

Table of content
- Neurosurgery
- 🚗 Traumatic Brain Injury (TBI)
- 🩸 Hemorrhagic stroke
- 🧠 Brain tumors
- 🎍 Spine pathologies
- 👶🏽 Congenital malformations of the CNS
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Neurosurgery
🚗 Traumatic Brain Injury (TBI)
- Delaceration(tear) + concussion ⇒ paranchyma + blood vessel (laceration) destruction ⇒ aggravating lesion
- Diffuse axonal injury (DAI) ⇒ brain rapidly shifts inside the skull as an injury is occurring (rotation movement?) 📷
- Hemorrhage 📷
Mechanisms 1.) Direct → commin. fracture (dmg to underlying parenchyma) + Penetrating wound + foreign body (gun shot) 📷 2.) Indirect → Countercoup 📷
⇒ WHITE MATTER (WM) lesion (scissoring of axons) ⇒ inconclusive CT + severe neuro detoriation
⇒ aggrevating lesion
WHICH AREA IS AFFECTED? ⇒ Type 1-3
Type 1: SUBCORTICAL WM
Type 2: entire CORPUS CALLOSUM
Type 3: BRAINSTEM affected
(epidural, subdural,subarachnoid, intraparenchymal)
- Direct (scissoring ✂️) ⇒ bony canal fx ⇒ instant symptoms
- Indirect (compression / edema) ⇒ delayed symptoms
- Linear fx
- Comminuted fx
- Depressed (intrusive)
- Extrusive
- Gunshot (exit wound larger!)
- Skull base (CSF fistulas to nose/ear → Meningitis risk!)
- Cut
- Contusion
- Scalping 📷
- Gunshot
Emergency management:
- Shave the head and clean the wound
- Administer local anesthesia
- Explore the wound and address any leakage of cerebrospinal fluid or cerebral mass by suturing ⇒ neurosurgery
- Remove foreign objects
- Perform scalp suturing in two levels: galea and skin 📷
- Address tissue loss by sliding adjacent scalp to close the gap
- Clean and suture gunshot wounds, referring to neurosurgery if necessary
- Administer antibiotics and tetanus prophylaxis
- Apply a bandage for two days
- Remove sutures after 6-7 days
- Check GCS ⇒ mild, moderate, severe TBI
- Facial bone injury
- Vertebro-medullary trauma → aware + FND or comatose
- Chest, Abdomen + Limb injuries ⇒ PRIORITY!!! ⇒ shock
- CT ⇒ pathologic findings?
- Admission / emergency Tx → home, 24h hospital, neurosurgical, ICU
- Grade 0 - No risk, no loss of consciousness → send home 🏡
- Grade 0 - With risk (alcohol/drugs, age, anticoagulant, NS (VP shunts)) → CT + Hospital 🏥 (24h)
- Grade 1 - Minimal loss of consciousness = retrograde amnesia, headache, vomiting, scalp wounds → hospital 🏥
- Grade 2 - GCS 14-13 for 30 min, no focal deficit → hospital 🏥 until amelioration
Algorithm:

Type | Description | CT Findings |
I | Diffuse lesion | normal CT |
II | Diffuse lesion | Visible cisterns, midline shift < 5mm, no cerebral lesions > 25 cm³ |
III | Diffuse lesion | Cerebral edema, midline shift < 5mm, compressed cisterns, cerebral lesions < 25 cm³ |
IV | Diffuse lesion | Medial line > 5mm, cerebral lesions < 25 cm³ |
V | Massive lesion | Surgically evacuated lesions |
VI | Massive lesion | Unevacuated mass lesion > 25 cmv |

Minor TBI (Ø focal neurologic deficit / CSF fistulae):
- Epidural hematoma: (Single greatest neurosurgery emergency)
- meningeal a. / dural sinus / fx
- 3 stages: initial Ø conciousness → silent gap → worsening
- good prognosis
- Acute subdural hematoma
- venous parenchym vessel (corticodural bridging veins)
- direct coma with worsening
- bad prognosis
- Subtypes:
- Subacute (assoc. with brain atrophy): after 2-3 days ⇒ 3 stages ⇒ good prognosis
- Chronic: 3 weeks after ⇒ pseudotumoral/pseudodemetic/oligosymptomatic clinical presentation ⇒ good prognosis
- Pseudo-TU: ICH + progressive focal deficit
- Pseudo-dementia: neurological symptoms resembling dementia, psychiatric disorders
- Oligosymptomatic: headache, motor deficit, etc
- Intraparenchymal hematoma
- cerebral vessel ⇒ progressive!
- progressive ↓ conciousness (Tiredness → coma )
- prognosis: poor
- Decompression craniotomy
- Epidural + acute subdural ⇒ large craniotomy
- subacute subdural + intraparenchymal ⇒ craniotomy
- Chronic subdrul ⇒ Minimal craniotomy / external drainage / lavage / port (SEPS)
- ↓GCS by 2 points
- Pupil dilation
- MIdline shift >5mm Or Volume >30ml (≥type 4)
- Temporal / Temporo-parietal location?
- hemostatis + evaluation of hematoma
- infectious control
T
F → suture up + send them asap
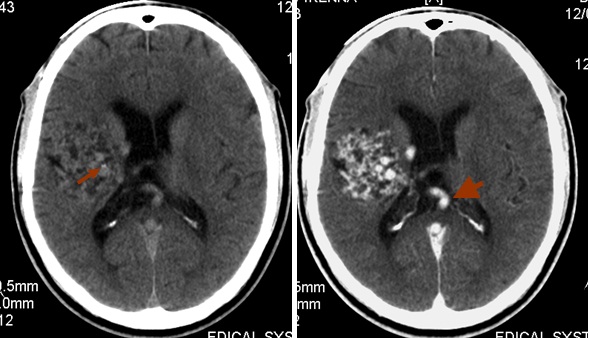
🩸 Hemorrhagic stroke
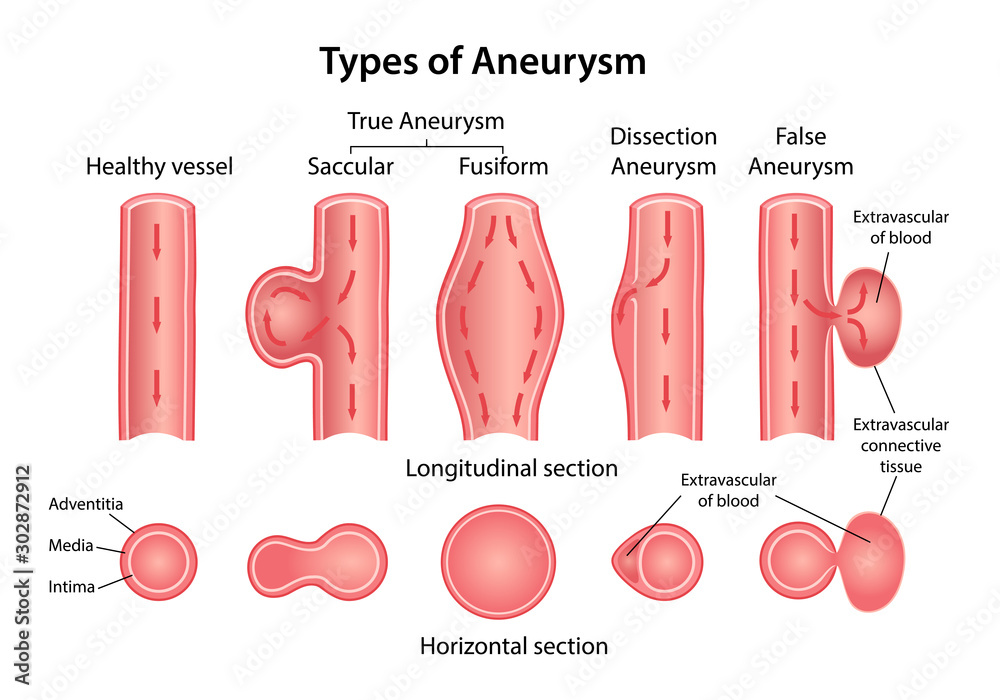
- Aneurysm (SAH) (#1)
- HT (primary intra-parenchymal) [+Amyloidosis]
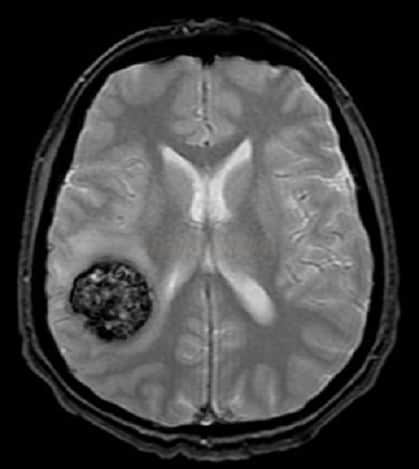
- AVM (parenchymal / SAH)
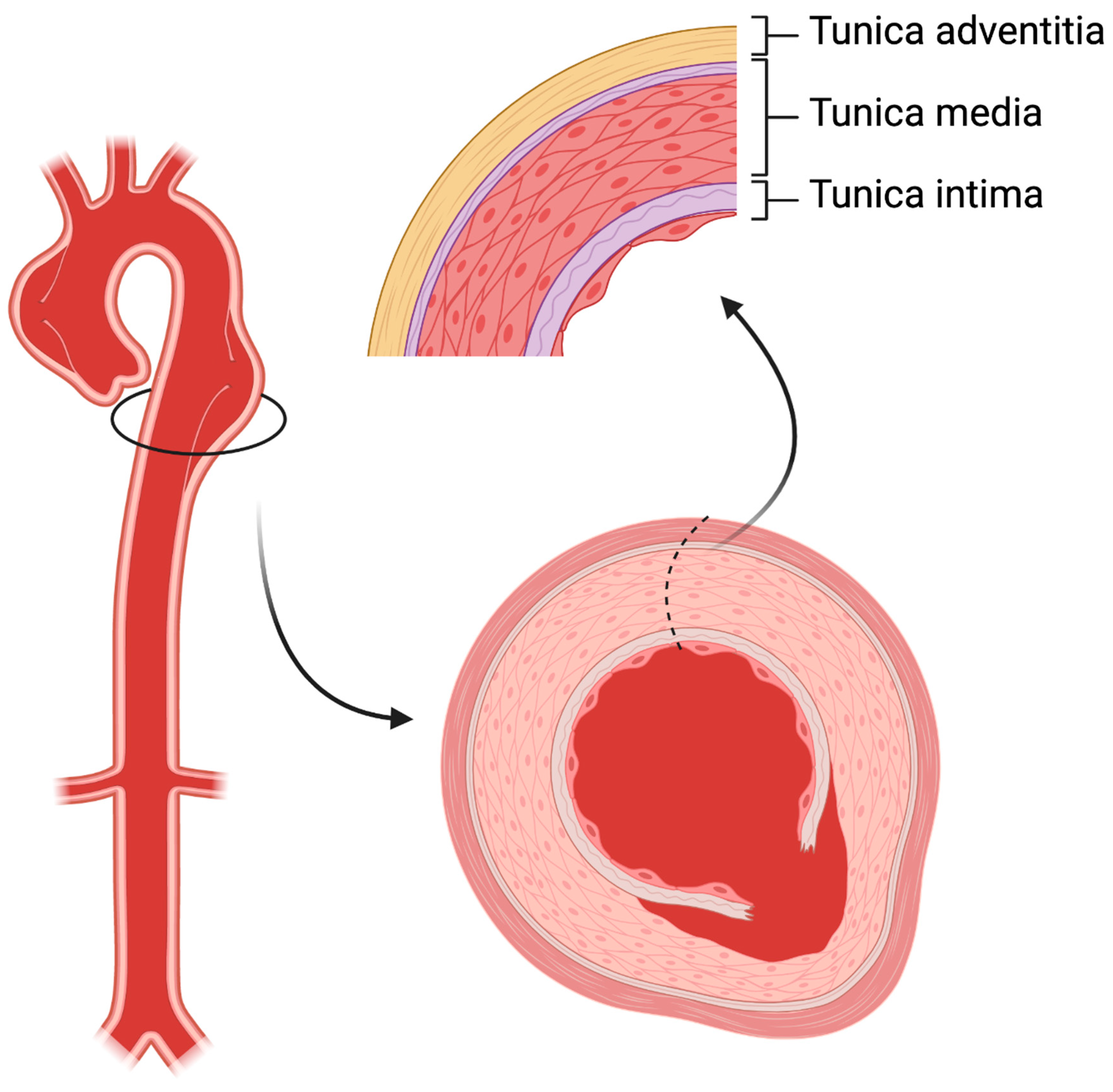
intima + adventitia 📷
dome (apex) 📷 = minimal resistance area
5-10mm
Classification - dimensions: • <3 mm (microaneurysm) • 4 - 6 mm (small) • 7 - 10 mm (medium) • 11 - 24 mm (large) • >25 mm (GIANT)
- Bleeding → SAH
- Cerebral herniation (transtentorial → brainstem)
- Acute hydrocephalus (sylvian aqueduct obstruction)
- Vasospasm (Critical period day 4-12)) ⇒ ischemia ⇒ ↓neuro-status
- Rebleeding → 70% die at rebleed
- Chronic hydrocephalus (due to malabsorption, Øobstruction)
- Thunderclap headache
- Meningeal syndrome
- ↑ICP → Neurologic deficit + Loss of conciousness
Survival rates:
GOOD (SV 96%) - grades 1-2 MEDIUM (SV 90%) - grade 3 POOR (SV 72%) - grade 4 RESERVED (SV 50 %) - grade 5
⭐ Star sign ⇒ 📷
Brain angioography = gold standard
brain angio-CT = imaging standard
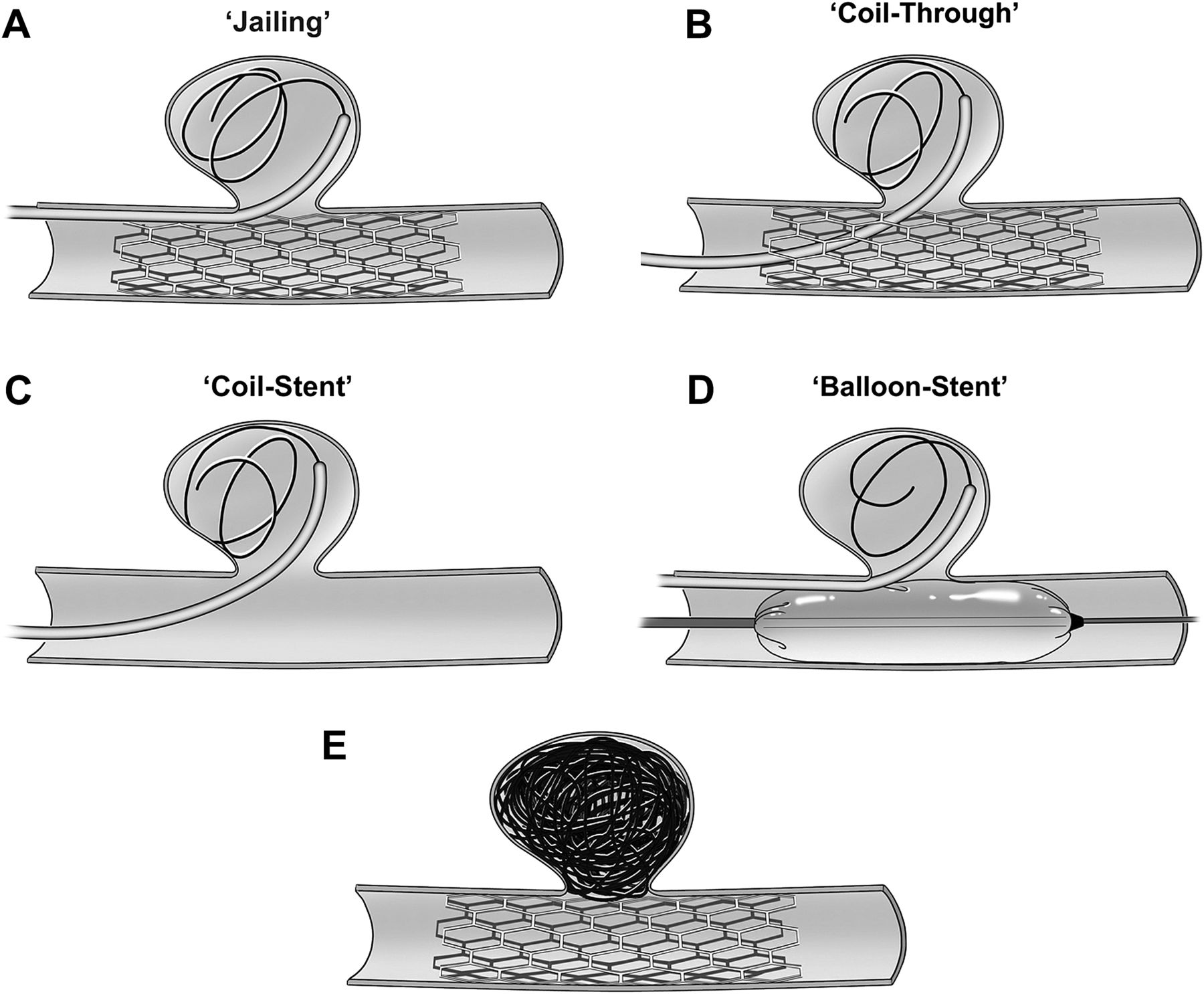
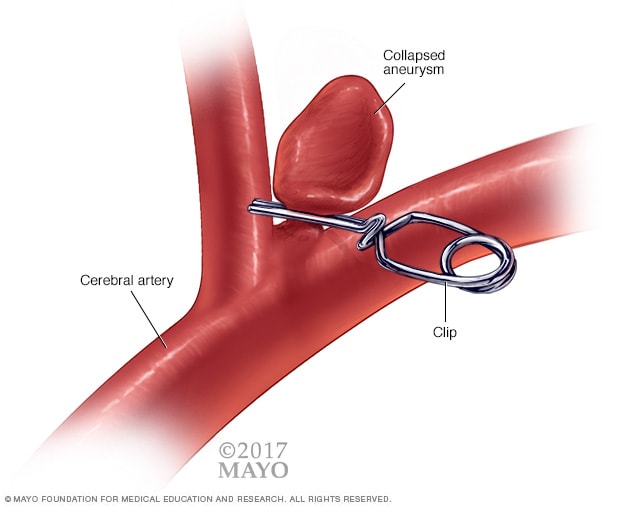
clipping 📷 ⇒ aneurysm neck
- coiling fails
- Aneurysm: large neck, giant aneurysm
- Location: MCA OR Ant. circulation+young (life expectancy >15y)
angiography
- ↑Survival w/o disability
- ↓ hospitalization
- ↓short-term complication
- ↑risk for Re-permeabilization
- Need for pre-angiography
- ↑cost (long term)
- Progressive neurologic deficit (Epilepsy, headache, FND)
- Children → Vascular steal → cardiac insuff.
- There is an effect of impaired perfusion of the cerebral tissue surrounding the AVM ⇒ diversion to AVM = vascular steal phenomenon
- Vascular steal is said to be the cause of progressive neuro deficits and psychiatric behaviors/manifestations seen in some AVM patients
Vascular steal:
⇒ PICTURE
- Embolization (endovascular)
- Gamma-knife
- Surgery
Grading:
- AVM size
- small (<3cm) = 1pt.
- medium (3-6cm) = 2pt.
- large (>6cm) = 3pt.
- Adjacent parenchyma eloquence
- non-eloquent = 0pt.
- eloquent = 1pt.
- Venous drainage
- superficial = 0pt.
- deep = 1pt.
⇒ add points together = grade
Tx depending on grade:
Grade 1-2 = minor operative risk, other options: radiosurg. / endovasc. Grade 3 = surgery Grade 4 = surgery (high risk) Grade 5 = selective embolization + surgery / embolization/ observe
T ⇒ symptoms may persist + repermeabilization!
- ASYMPTOMATIC
- Hemorrhage
- Mass effect → headache + seizures, FND
observation
F ⇒ useless
#1 gamma knife
(⇒ surgery if emergency)
Anticoagulants!
(+classic CV-RF)
CT ⇒ exclusion DDx (aneurysm, AVM, tumor)
⇒ DYNAMIC EVALUATION! (repeat)
- Medical Tx
- vital function
- ↓ICP
- Anti-hypertensive drugs
- Correct Coagulation
- Surgery
- Clinical
- ↑ICP
- Neurolog. detoriation
- <50y
- Imaging:
- 10-30 cm3
- Location:
- Lobar
- Cerebellum
- Neurologic status on admission (↓Conciousness)
- Bleeding characteristics
- ↑Size
- Location (brainstem damage?, deep?)
- Origin (AVM>Aneurysm>PIH)
- Patient aspects
- Age + Comorbidities
- Coagulopathy
🧠 Brain tumors
benign → mass effect = tumor volume
malignant → mass effect > tumor volume (marked perilesional edema)
- benign characteristics (Øinvasion, well delineated, homog, minimal edema)
- ↑vascularized
- +/- calcification
- mass effect
T
neuroepithelial
- Major analgesics (opioids) → respiratory depression! ⇒ give minor analgesics
- Benzos (for seizures) → anti-epileptics instead
Symptomatic Tx
- ↓Edema: steroids, mannitol, furosemide
- Minor analgesics
- i.v. antiepileptics (+benzos)
- Decompression = Tumor removal
- obtain Histo
- Fix cerebral function + CSF course
⇒ Piecemeal removal (Øen-bloc) via microsurgery
(palliative tx → ↓iCP)
F
- <65y
- ≥1y progression-free
- Ø irrevers. neuro detoriation
- high enough performance index (karnofsky score
glioblastoma → any combination (surgery, RT, chemo)
meningioma → Removal: total (surgery) OR partial (surgery +RT)

Surgery
- Trans-sphenoidal
- Craniotomy
- Radiosurgery (gamma knife)
⇒ ❗ hypopituitarism
OR medical (depends on adenoma type)
- Prolactinoma: Treated with Bromocriptine
- Somatotrophic: Treated with Somatostatin
- Cushing's disease: Treated with Ketoconazole
🎍 Spine pathologies
= Vertebromedullary injury
- Forces
- Direct:
- Indirect:
- Hyperflexion
- Rapid deceleration
- stable fx
- with rotation → unstable (lig. lesion)
- Cervical location (thoraco-lumbar junction) ⇒ highest mobility areas
- Hyperextension
- Rapid aceleration / leaps in shallow water
- Axial compression
- Falling from height
- Scissoring
- Rotation + Lat. tilting
- Elongation (Distraction)
- Bleeding → Compression
- Ischemia (i.e. due to compression) ⇒ neuron alteration + apoptosis



⇒ unilateral impact → articulate process fx

⇒ assoc. with flexion + extension
see → Radio
Jefferson → C1 vertical burst
Ododontoid → dens (C2) flexion
Hangman → C2 peducle avulsion → moved forward from C3
- Vertebral lesion
- stable (flex, compression)
- unstable
- Medullary
- complete (complete loss of function below)
- incomplete
- Spinal shock
- C1 - C4: Cervical plexus (muscles of the neck and diaphragm)
- C5 - T1: Brachial plexus (muscles of the upper limb)
- T2 - T12: Intercostal muscles, subcostal muscles, abdominal wall muscles
- T7 - L1: Abdominal wall muscles
- L1 - L4 (+ram. S3): Lumbar plexus
- L5 - S3 (+ram. L4): Sacral plexus
- L2 - S5: Cauda Equina (muscles of the lower limb and innervation of the rectum, bladder, and genitalia)
- ØMOTOR: flaccid paralyis +
- Øreflex
- ØSENSORY: sensory loss
- ØAUTONOMIC: bladder / bowel
- Local signs
- pain + paravertebral contracture
- skin + ST injury (wound, contusion)
⇒ DOWNWARD from lesion ⇒ COMPLETE LOSS OF FUNCTION:
→ depending on type of spinal cord syndrome ⇒ see neuro
- MRI ⇒ Ø in emergencies
- CT (vascular → angio-CT; spinal cord compression → Myelo-CT)
- Xray ⇒ for surgical approach (detects only bone)
- Immobilize (esp Ø flexion)
- DVT prophylaxis
- Manage autonomic dysfunction
- Hypotension
- Vasodilatation
- Poikilothermia
- Paralytic ileus → NG tube
- Urinary retention → catheter
- QUICK transport ⇒ NEUROSURGERY
- Decompression
- Stabilzation
- Prevent Infection (+worsening)
- Spine INSTABILITY (→ neuro worsening)
- COMPRESSION: spinal cord / root
- OPEN Wound (CSF fistula)
- Open → clean, hemostasis, suture
- gunshut through abdomen? → sepetic risk
- gunshot through ST → only eplore if surgery indication
- C1-C2 lesion ⇒ Surgery within first 6 weeks!
- Jefferson (C1) → ligament intact?
- Odontoid (Dens C2)
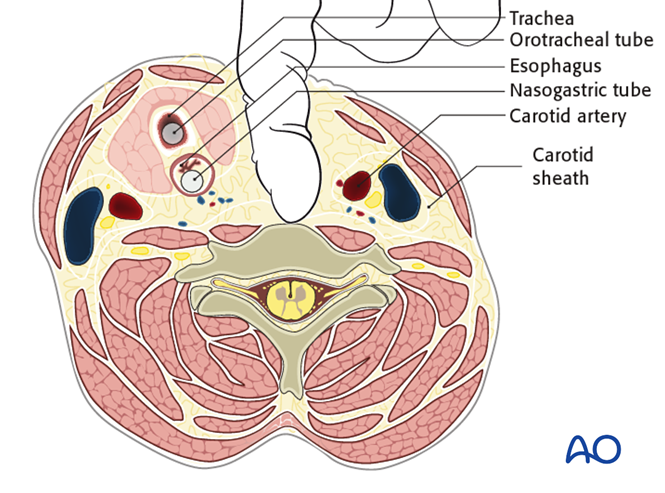
- post. aproach → fusion C1-C3
- ant aproach→ screw C2 body + dens 📷
- luxation? → ablation + C1-C3 fusion
- C3-C7 lesion
- Thoracolumbar lesion (esp. compression of nerves)
⇒ Ant. / post. or combined(complex) approach
⇒ depends on largest lesion! (i.e. ant →ant. approach)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Nerve damage
- CSF fistulas
- fusion system malfunction / instability
- General complication: bleeding, infection
{kind=link}
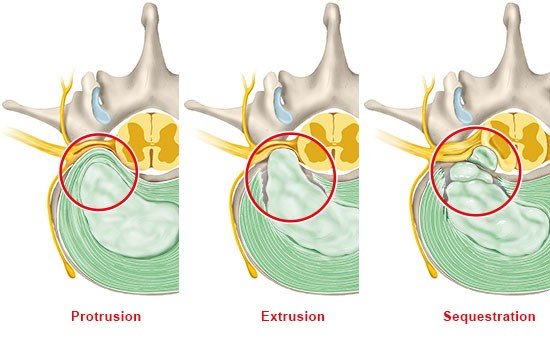
- Disc protrusion: protrusion of the nucleus pulposus through the annulus fibrosus
- Disc herniation/extrusion/prolapse: complete herniation of the nucleus pulposus through a tear in the annulus fibrosus
- Disc sequestration: extrusion of the nucleus pulposus and separation of fragments
- trauma
- occupational
- weight distribution problem
- posture
- tall / obese
- genetic
- Radiculopathy:
- Acute severe radicular pain (stabbing / electric shock) with radiation
- Cervical:
- ↓mobility,
- torticolis,
- L5 radioculopathy (L4-L5):
- Lumbago (vertebral syndrome) ⇒ Lasegue +
- Pain & Paresthesia in dermatome (toes 1-2 (-4))
- Fibular nerve paresis → cant walk on heels
- normal reflexes
- S1 Radiculopathy (L5-S1):
- Lumbago (vertebral syndrome) ⇒ Lasegue +
- Pain & Paresthesia in dermatome (popliteal space + toes 3-5)
- Tibial nerve paresis → cant walk on toes
- ↓/Ø Achilles t. reflex
- Cauda equina syndrome (🚑 ) (large median L2-L5)
- Paraparesis + Saddle anesthesia
- Ø Patellar + Achilles
- Myelopathy (esp. cervical) ⇒ Spinal cord syndromes (UMN + sensory + autonomic)
→ unilat. LMN signs + sensory loss in dermatome
{kind=link}
MRI
(CT, myeloCT, Myelography, Xray)
- Immobilization (+devices)
- Pain control
- Physio
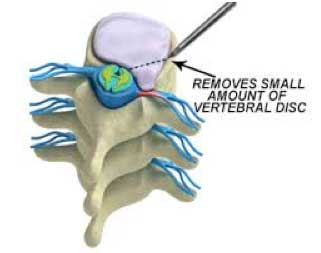
- Inversion therapy 📷

- Refractory conservative tx
- FND
- severe pain
- compressive spinal emergencies
- Cauda equina syndrome
- spinal cord syndrome (myelopathy)
- Clinic + imaging concordance
{kind=link}
{kind=link}
{kind=link}
- Extradural (vertebra)
- intradural (schwannoma, meningioma)
- Intramedullary (glial origin, non-glial)
⇒ COMPRESSION:
- Pain (central, radicular, Lhermitte)
- FND ⇒ LMN & UMN signs below
- Sensory deficit below ⇒ depending on spinal cord syndrome
- Autonomic dysfunction
Indication: Radio-resistance, Øneuro-def.
Contraindication: low life expectancy, multiple lesion, altered general status
Neurosurgery ⇒ Medullary decompression
additional: tumor removal, histo, stability
Extra-dural (vertebral):
⇒ #1 Circumferential cord decompression (+ Reconstruction + stabilization) 📷
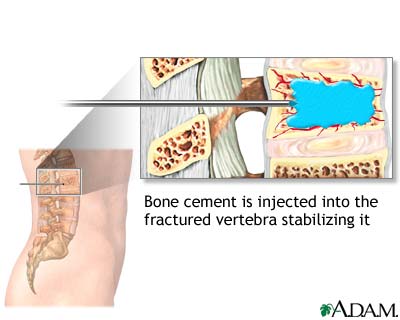
⇒ Vertebroplasty w/ PMMA cement injection 📷 ⇒ decompression (pain relief) + antitumoral effect
{kind=link}
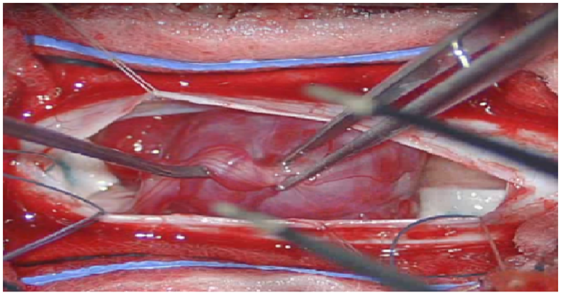
Intra-dural:
Microsurgery → total resection (post. approach w/ laminotomy/-ectomy) 📷
{kind=link}
Intra-medullary:
Complete resection 📷/ subtotal ablation(astrocytoma)
{kind=link}
complete resection:
ependymomas + hemangioblastomas
👶🏽 Congenital malformations of the CNS
Chiari 2 → cerebellar+ brainstem → caudal elongation + hernation of post. fossa contents → Hydrocephalus + Myelomeningocele 📷 (primary neurolation defect)
{kind=link}

Chiari 1 → cerebellar tonsills ↓ displacement → syringomyelia)
A. Obstructive hydrocephalus
B. Communicating hydrocephalus (↑secretion/↓resorption → infection, choroid plexus adenoma/carcinoma) → gate, dementia, incontinence (DIG)
- complete deficits → never recover
- mobility lower limb → able to walk
- sphincter disturbance from birth → entire life
- delayed complications
- UTI
- tethered cord syndrome