




Neurology
🎗️ Basics
Upper & lower motor neuron lesion
- Nervous (UMN + LMN)
- NM-Junction (myasthenia gravis)
- Muscular
- functional

- Hemiplegic stiff (circumductive) gait
- Arms flexed + pronated
- Legs extended + adducted
⇒ Elastic: regain initial position after mobilized
⇒ clasp-knife phenomena might be seen


Mental status & speech
details: see → alterations of conciousness
- orientation in space, time + person
- GCS 📷
- speech? understanding?
- aphasia (→ which type?)
- dysarthria (→ what type?)
- thought processes?
Dysarthria | Etiology | Speech |
Flaccid | acute stroke, myasthenia | nasal, breathy |
Spastic | small bilat. stroke, tumor | slurred, low pitch, slow |
Ataxic | cerebellar pathology | irregular “scanning” speech (explosion + pauses) |
Extrapyramidal | monotonous, sudden start/stop | |
Mixed | combination of above |
✅=impaired: 🚨

Type of aphasia | SPEECH | UNDERSTAND | REPEAT | LOCATION |
Broca | ✅ | - | ✅ | inf. frontal gyrus (broca) |
Wernicke | - | ✅ | ✅ | sup. temporal gyrus(wernicke) |
Global | ✅ | ✅ | ✅ | broca,wernicke, arc. fasciculus |
Conductive (Arcu. fasc.) | - | - | ✅ | parietal (arcuate fasciculus) |
Transcortical motor | ✅ | - | - | suppl. motor (frontal) w/ broca intact |
Transcortical sensory | - | ✅ | temporal lobe w/ wernicke intact | |
Transcortical mixed | ✅ | ✅ | - | broca, wernicke, arc. fasc. intact (watershed areas affected) |
Anomic | - | - | - | Ølocalization possible |
Cranial nerves
1 - Olfactory
- identify aroma
2 - Optic
OPTHA EXAM
- Visual acuity:
- count finger, see hand movement,
- perceive light
- Snellen chart,
- Color vision: Ishiara plates
- Visual field assessment → hemianopsia?: ⇒ Confrontation (finger 📷) (or perimetry)
- Pupillary reflex
- Papilla - Fundoscopy 📷→ check optic nerve + disk

3,4,6 - Oculomotor, trochlear, abducens
- Eye-movement:
- Follow finger
- Pupillary reflex + Accomodation pupillary reflex (+convergence)
- CN3 palsy (surgical CN3 palsy + occular trauma)
- Adie’s pupil (Tonic pupil)
- Atropine
- Horners (Ptosis, miosis, anhydrosis)
- Painful horner = Carotid + cervical dissection → compression pericarotid sympathetic plexus ⇒ 🚑
- Apical lung tumor
- Vestibulo-ocular reflex (turn head + fixate point 📷)
- Diploplia (CN 3-6)?
- Ptosis + anisocoric pupils + divergent strabismus ?(CN3)
- tilted head in vertical plain (contralat)?📷 (esp. when looking down + medial) ext.rotated + up? (CN4)
- tilted head in horizontal plain (ipsilat)? convergent strabismus?
(paresis? not smooth?, nystagmus?)
📷 aka saccadic movement!
paresis:


MYDRIASIS: > IN LIGHT (large pupil abnormal)

MIOSIS: > IN DARK (small pupil abnormal)
Ptosis:

lat rectus → CN6 sup oblique → CN4 rest → CN3
5 - Trigemial
- Facial sensory 📷 : light touch test at 3 different spots: Forehead(V1), Cheek (V2)+ Jaw (V3) → Q-tip: sharp or soft side? hypoesthesia?
- Motor (V3): open + close mouth (masseter asymmetry? pain on palaption? open against resistance)
- jaw reflex 📷
- Corneal reflexes → pat. look away → touch cornea with twisted wooden
- both eyes blink→ normal
- stimulated eye open & contralat. eye closed → CN7
- both open / reduction in corneal sensation → V1

7 - Facial
- facial motor: smile (w/ teeth), pull eye-brows up, pop cheeks, close eyes tight
- Sensory tongue: taste (sweet, salty, sour) ant 2/3
8 - Vestibulocochlear

Hearing (cochlea)
- conductive vs. sensorineuronal vs. central deafness
- normal hearing from conversation?
- Tuning fork: Weber + Rinne
- whisper test (2 syllables)
- (+balance: Romberg)
Vestibular:
- nystagmus → horizontal or rotatory? (see below)
- vertigo + nausea
- ↑by movement
- sense of inbalance
- 1 position w/ 1 eye close → ↓vertigo+nausea
- Tinnitus?
- posture + gait? → romberg (towards lesion), difficulties when making a turn
- Hallpike maneuver 📷⇒ vertigo? ⇒ periph. lesion
Quickly move the patient from sitting to recumbent position, with the head tilted at a 30 to 40-degree angle over the end of the table and 30 to 45 degrees to one side.
9, 10 - Glossoph. + Vagus
- both:
- swallow (pharynx muscles) 📷 → 9-sup ; 10-inf
- Cough + gag reflex
- 10 → say “ahhhh”: uvula + soft pallate: deviation? symmetrical?
- 9: taste bitter (post 1/3 + parotid autonomic fibers)
gag reflex:


- 10: Phonation: Hoarseness? Cough? (+ alot parasympathetic fibers + sensory)
parasymp. fibers:
- Afferent fibers: Visceral sensation from the intestines, stomach, esophagus, tongue, part of the pharynx, lungs, bronchi, trachea, and larynx.
- Efferent fibers: Control secretion of glands in the mucosa of the larynx, pharynx, gut from the esophagus to the colon at the splenic flexure, pancreas, liver, and lungs; control acid secretion of the stomach; slowing of the heart rate; innervate smooth muscle of the airway (bronchoconstriction, airway opening) and gut (peristalsis coordination).
11 - Accessory
Trapezius + SCM (C2-C4)
- trapezius:
- one shoulder below level? winging of scapula away? pain?
- hands on shoulder + pull against resistant up.
- arm abduction
- SCM: rotate neck lateral against resitance (chin) → weakness when turning oppsite side
12 - Hypoglossal
Tongue muscles
- deviation? (towards lesion!)
- fasciculations? atrophy?
- patient press tongue against inside of cheeck → resistance from outside
- test speech + say fast “ticker ticker ticker”
- if bilateral → motor nuclei lesion
- assoc. painful horner?
Motor, Coordination & Reflexes
1. MOTOR:
1. Appearance 👁️
- atrophy? 📷
- abnormal movements
- voluntary movement (watch patient doing normal shit)
- Tremor (rhythmic)
- Resting → Parkinsons
- Intention (ataxic) → Cerebellar
- Postural → Essential
- Chorea → huntington/sydenham chorea (see below), drug-induced (L-DOPA, antipsychotics)
- Athetosis → Basal ganglia lesion, drug induced (L-DOPA, antipsychotics)
- Ballismus → acute subthalamic nuclei lesion
- Dystonia (→abnormal posture)
- torticollis
- laryngeal muscle (dysphonia)
- writers cramp
- drug induced
- Myoclonus → cerebral hypoxia, creutzfeldt jakob, metabolic, neurodegenerative, physiological
- Tics → turrette
- fasziculations?
- abnormal posture? (dystonia?)


Chorea:




⇒ Tx: Botox


2. Strenght 💪
- Muscle power grading 0-5
→ upper + lower extremity → go “through every joint”
Muscle power grading:
- 0: no contraction (complete paralysis)
- 1: flicker or trace of contraction
- 2: active movement, with gravity eliminated
- 3: active movement against gravity
- 4: active movement against gravity and moderate resistance
- 5: normal power (full range of motion against gravity and full resistance)

- Pronator drift 📷
The pronation or lowering of one arm while raising both arms horizontally up to shoulder level, palms facing upwards, with the eyes closed (for 30 seconds) is indicative of paresis. → Mingazzini sign
- Legs: Global testing

3. Tone → passive ROM 🎵
- spasticity? (pyramidal tract)
- velocity dependent
- clasp-knife phenomenon
- flexor upper limb + extensor lower limb
- rigidity (extrapyramidal)
- velocity independent
- constant? → lead pipe rigidity
- cogwheel rigidity
- Extreme stiffness of the joint of the limb
- Difficulty in movement
- Jerky movement resembling ratcheted rotation of a cogwheel when flexed/extended by examiner
- hypotonia/flaccid? (peripheral (lower motor neuron), cerebellum)

initial resistance due to increased muscle tone followed by a sudden decrease in resistance
Increase in tone that is constant throughout the passive movement
- Clonus? → combined with muscle weakness, increased muscle tone, or pathological reflexes? → UMN lesion
Clonus:

- Clonus: Rhythmic contractions and relaxations of a muscle group.
- Myoclonus: Sudden jerks of a muscle or group of muscles.
- Myoclonus is associated with metabolic abnormalities.
- Clonus is a sustained rhythmic reflex response to muscle stretching.
- Clonus and myoclonus are different types of abnormal muscle movements.
2. COORDINATION: Cerebellum
⇒ see also cerebellar syndrome!
⇒ look for ataxia (gait, limb, trunk)
⇒ DAMAGE TO CEREBLLUM OR CONECTING PATHWAYS
1. Finger-nose + Finger-Finger test 📷→ dysmetria/tremor? 👆🏼
→ miss or overshoot? (dysmetria) → cerebellar
→ tremor? (intention (cerebellar) vs. kinetic))
intention:

kinetic:

- finger-nose: patient touch nose
- finger-finger: alternate bet. betw. nose and examiners moving finger as quickly as possible
2. Heel-knee shin test 📷→ ataxia? 🦵🏼
touch the opposite knee with heel + slide down
3. Rapid alternating movements📷 🤚🏼
→ cant perform? (dysdiadochokinesia) ⇒ cerebellar/corticospional tract
dysdiadochokinesia:

4. Sit up lying in bed without using hands
- trunk ataxia?
5. Romberg 📷 (feet next to each other, hold arm forwards, close eyes) → ataxia? 💃🏼

→ cerebellar ataxia: eyes open → uncontrollable swaying
Cerebellar ataxia
- Impaired coordination of muscle movement due to central nervous system disorders
- This impairment cannot be compensated for visually, resulting in unchanged swaying of the patient regardless of the eyes being open or closed.
→ sensory ataxia: eyes closed → patient starts swaying/swaying incr. / falls (immediatly)
Sensory ataxia: Dorsal columns and proprioception impairment
- Loss of sensory coordination in muscle movements
- Visual compensation for lack of sensory control
- Swaying increases with closed eyes
→ vestibular disorder: eyes closed → fall sideways (towards ipsilat. side) (after few seconds)

3. Reflexes
Deep tendon reflexes (DTR) - monosynaptic → UMN vs. LMN, NMJ + muscular?
- Grade DTR: 0 - 4+ (1-5)
- /0: Areflexia (no response even with reinforcement)
- /1+: Hyporeflexia (weak response)
- /2+: Brisk reponse (normal)
- /3+ Hyperreflexia (very brisk reponse)
- /4+ Clonus (repeating series brisk reflexs)
- Significant asymmetry between both sides
- Difference between upper and lower extremities
- Other signs of LMN lesion affecting the same zone
- ↑ - UMN lesion
- +/- reflex spreading
- Reflex response extends beyond the muscle typically involved (to another muscle group)
- Examples include finger flexion during biceps reflex and hip adductor contraction during knee reflex
- ↓/Ø - LMN AND acute UMN
- 1 reflex diminished → nerve root, sciatic nerv
- multiple reflexes diminied → multiple roots (i.e. polyneuropathy)
- inverted reflex = absent but spreading - combined UMN+LMN
- Combination of missing the tested reflex with spreading of the reflex to a muscle at a lower level.
- Example: When testing biceps reflex, biceps doesnt react but triceps response appears.
- pendular reflex (knee jerk) - cerebellum
- elderly ⇒ ↓/absent lower DTR → look for other assoc. signs

- cant get a reflex? → try Jendrassik Maneuver 📷
Cutaneous reflex 📷 - polysynaptic → Nerve root?
Polysynaptic reflexes exhibit habituation, where the response to repeated stimuli gradually diminishes and eventually disappears.
→ this reflex circuit mediates withdrawal from painful stimulus
- Abdominal, cremaster, anal, bulbocavernous
- contraction of muscle group → normal
- ↓/Ø contraction → Nerve root lesion (LMN or reflex arc lesion)
- Abdominal reflexes are tested by lightly stroking the anterior abdominal wall in specific areas, and a normal response is the contraction of the abdominal muscles.
- Normal conditions: obesity, previous abdominal surgery, frequent pregnancies, aged
- Pathologic condition: pyramidal tract lesion, thoracic root interruption
- The cremasteric reflex is elicited by stroking the inner part of the thigh, resulting in the contraction of the cremaster muscle.
- The anal reflex is elicited by stroking the skin around the anus, resulting in contraction of the anal sphincter muscles.
- The bulhocaverosus reflex is elicited by squeezing the penis or clitoris, resulting in contractions of the pelvic floor muscles.
Absence of abdominal reflexes:
Pathologic reflexes/ Pyramidal tract signs
- Babinski? 📷
- Rossolimo? 📷
- Plantar flexion of last 4 fingers upon percussion of the plantar surface with a hammer
- Presence of the reflex indicates a pyramidal lesion
- primitive (infant) reflexes? → diffuse cerebral disorder (frontal lobe + pyramidal tract)
- Grasp Reflex
- The grasp reflex is obtained by gently inserting the examiner's hand into the palm of the patient's hand.
- With a positive response, the patient grasps the examiner's hand with variable strength and continues to grasp as the examiner's hand is moved.
- Ability to release the grip voluntarily depends on the activity of the reflex.
- Palmo-Mental Reflex
- The palmo-mental reflex occurs when a tactile stimulus is drawn from the thenar eminence at the wrist up to the base of the thumb.
- There is ipsilateral contraction of the orbicularis oris and mentalis muscles.
- The skin over the chin wrinkles, and the corner of the mouth elevates slightly.
- Snout Reflex
- The snout reflex is elicited by tapping the upper lip lightly.
- The muscles around the mouth and base of the nose contract.
- The contraction of the muscles causes the mouth to resemble a snout (protrusion of the lips).
- Suck Reflex
- The suck reflex is elicited by lightly touching or tapping on the lips with an object such as a tongue blade, reflex hammer, or the examiner's finger.
- It consists of sucking movements by the lips when they are stroked or touched.
Gait & Stance
Gait/Stance examination
Stance:
- Romberg 📷 → sensory (proprioceptive) vs. cerebellar vs. vestibular ataxia?
- Positive Romberg: Impaired coordination when eyes are closed, swaying or swaying increases, indicates sensory ataxia, increased tendency to fall sideways (indicative of vestibular disorder, falls towards the side of the lesion).
- Negative Romberg: Closing the eyes does not affect balance, swaying does not increase.
- Uncontrollable swaying, even with eyes open, indicative of cerebellar ataxia.
- Pull-test (postural reflexes)
- Normal pull-test: patient recovers balance by stepping backward
- Mild loss of postural reflexes (pull test +): patient requires several steps backward to recover balance
- Severe loss of postural reflexes (pull test +++ and risk of falls): patient falls if not caught by examiner
(see above)
Gait:
Abnormal gait patterns (8)
- small + slow steps (bradykinesia) → shuffling
- cant turn with a single step
- “frozen posture”: leaning forwards, knees+ hips bent, arms flexed
- difficulties in step-initiation (rigidity)
ATAXIA:
- wide base
- irregular + uncoordinated movement
- unsteadiness, lateral swaying, arms+ legs flung
→ cerebellar vs. sensory ataxia:
CEREBELLAR ataxia:
- staggering gait
- - Romberg (fall with eyes open)
- Øsensory symptoms (like in sensory ataxia)
- + Deep tendon reflexes (lost in sensory) → pendular
- also check tandem (heel-toe), tremor, heal-shin, rapid alternating movement
- assoc. cerebellar signs (DANISH)
SENSORY ataxia → dorsal column / periph. neuropathies
dorsal column

- stomping gait
The patient may lift the leg higher than usual and slam the foot onto the floor because of deficits in proprioception
- + Romberg
- exacerbated when can’t see feet (i.e. in the dark)
- sensory signs + no reflexes
- (Dysmetria, intention tremor, limb ataxia might also be present in sensory ataxia)
FRONTAL LOBE ATAXIA (dementia)
- + stiffness
- narrow base
- primitive infant reflexes
→ vs. other ataxias
- Inherited: spino-cerebellar atrophy, Friedreich ataxia
- Acquired:
- Stroke (affecting the cerebellum and brainstem connections)
- Tumors (cerebellum, brainstem)
- Immune (multiple sclerosis with cerebellar or spinal lesions, paraneoplastic syndromes)
- Toxic: Lead, alcoholism, anticonvulsants, cytostatics
- Deficiency: Hypothyroidism, vitamins B1, B12, E
cant walk on heals (foot drop) 📷 ⇒ weakness foot dorsiflexion
→ patient has to step high (so foot doesnt drag)
⇒ unilat foot drop: L5 radioculopathy or sciatic nerve palsy
⇒ bilat footdrop: periph. neuropathy
- Waddling towards both sides while walking
- Trendlenburg + : pelvis drop towards unaffected side ⇒ gluteus medius + minimus weakness 📷
walking with irregular, jerky movement
patients do Ø fall → balance Ø affected
symmetric shuffling + upright posutre
- Painful gait: Lombalgic patients walk carefully with a stiff back and trunk bent to one side.
- Orthopedic gait: Seen in patients with coxarthrosis, hip surgery, or a shortened limb. The patient limps and may use a walking stick.
Sensory
Spinothalamic + dorsal columns

- Both: dull vs. sharp pain discrimination (i.e. broken q tip/pinprick) → dull: dorsal → sharp: spinothalamic
Dorsal colum
- Fine touch (fingertip, cotton)
- “say yes when touched”
- check bilat (assymetry?)
- Vibration: Tunig fork (pallhypesthesia?)
- Proprioception: DIP of hand + feet moved up and down by the examiner with closed eyes of the patient (DIP positional change sensed)
Spinothalamic:
- Temperature(+pain) cold vs. warm object
Cortical sensory signs:
DISCRIMINATIVE SENSATION:
- 1 vs 2 points discimination? (compass)
Two-point discrimination test: Assess the ability to distinguish two points. Gradually reduce the distance between the prongs of a compass.
- touch an area while eyes closed → let patient retouch the area (topagnosia?)
- write a number on their palm (figure writing) with eyes closed (angraphesthesia?)
- feel object → texture, size, shape (asterognosia?)
- touch right, then left, then both (sensory extinction/inattention)
- Touch the patient (eyes closed) on the right side (arm, leg), and then touch the left side in the same point
- If able to recognize each independently, touch him on both sides at the same time
- Normally: recognizes R, L, and both
- Sensory inattention: recognizes R, L, but not both → Parietal lobe lesion
⇒ Interpretation
Character of sensory deficit (How does it feel?):
- Pain → thalamic, radicular, (sometimes parietal)
- ↑ response → hyperalgesia
- ↑threshhold to perceive (when perceived: severe ↑pain) → hyperpathia
- abnormal sensation → paresthesia (all)
- unpleasant sensation through normal stimulus→ dysesthesia
- ↑ perception (sensitivity) → hyperesthesia
- ↓ perception → hypoesthesia
- Complete senosry loss = Anesthesia

e.g., itching, burning, pain , electric shock
Localization
- fixed zones? (dermatomes/nerve zones)
- single nerve area? → mono-neuropathic
- bilat. symmetric glove + socking? → poly-neuropathic
- Sensory impairment: bilateral and length-dependent
- Begins symmetrically at the most distal aspect of the lower extremities and ascends proximally
- "Glove and stocking" sensory loss
- Accompanied by motor and reflex loss (usually the peripheral nerves are sensory-motor)
- Associated with diabetic neuropathy
- radicular pain + incomplete sensory loss in dermatome →nerve root
- Signs of spinal cord sensory syndrome? → see below
- Starting at a LEVEL → BELOW (sublesional syndrome)
- Differences in dorsal vs. spinothalamic perception
- assoc. wearkness? (corticospinal)
- trauma, syphillis?
- Signs of brain stem sensory syndrome?
- Altern syndrome? (CN → ipsilat; periph → contralat)
- others → see below
- Signs of thalamic sensory syndrome?
- complete hemisensory loss (all sensations: body + face)
- Thalamic pain + hyperpathia (contralat)
- Signs of Cortical sensory syndrome?
- abnormal: discriminitive touch = tactile agnosia
- sensory inattention / extinction
Meningism
- Stiff neck (nuchal rigidity) → cant flex neck forwards
- Headache
- Photophobia (eye pain when exposed to bright light)
Nerve root irritation
check for spinal root compression:

- Lasegue 📷(straight leg raise <45°) → streched sciatic nerve → + back RADIATING down the ipsilat. leg ⇒ L5-S1 irritation
- Crossed Lasegue 📷 (crossed straight leg raise <45° of the unaffected leg) ⇒ pain radiating in contralat. extended leg (affected leg)
- If Lasegue + → Bragard test 📷 → lower leg slightly until pain gone → dorsiflex foot ⇒ + pain → L5-S1 irritation
- If Pseudo-Lasegue + (= Aching pain in the back of leg >60° (hamstring area not back pain) ⇒ hamstring pathology
Positive Lasegue + Positive Bragard ⇒ Neurological etiology likely
Positive Pseudo-Lasegue + Negative Bragard ⇒ Muscular etiology likely
Nystagmus
Spontaneous nystagmus 📺 = Øprovocation + in all direction of gaze
- Peripheral Vestibular
- jerk (with slow + fast phase)
- horizontal: a type of jerk nystagmus in which the eyes move horizontally
- torsional: a type of jerk nystagmus with rotary oscillations of the eye along its anteroposterior axis (clockwise, counterclockwise)
- + Vertigo (mild vs. intense)
- partially suppressed with visual fixation
- Central vestibular
- jerk or pendular 📺 ⇒ multidirection
- A type of nystagmus characterized by sinusoidal oscillating movements of one or both eyes.
- Often associated with multiple sclerosis.
- Always considered pathological.
- Acquired pendular nystagmus indicates a central lesion.
- -↓Vertigo
- Ø supression with visual fixation
- assoc. neuro signs
Nystagmus: a slow movement of the eyes towards a defined direction followed by a fast, corrective movement backward.
→ name of the nystagmus is determined by the direction of movement in the fast phase, i.e., left- beating, right-beating, downbeat, upbeat
→ usually mixed horizontal torsional(rotatory) (rare: vertical)
→ UNIDIRECTIONAL AWAY from lesion
Pendular nystagmus:
→ esp. if pure horizontal, rotational, vertical
Gaze-evoked nystagmus 📺
- test oculomotor eye movement to extreme horizontal point of gaze
- jerk nystagmus > 20s ⇒ brainstem/cerebellum pathology


⇒ pure vertical ⇒ midbrain
⇒ pure horizontal ⇒ pontomedullary
- Pure upbeat, pure downbeat, and pure horizontal nystagmus are characteristic of central lesions.
- Mixed horizontal and torsional nystagmus patterns are typical of peripheral lesions.
Nystagmus provoked by external stimuli
→ caloric test ⇒ COWS (=physiological)
horizontal jerk nystagmus caused by infusing cold or warm water into the external ear canal

- Quantitative = arousal / responsiveness
- Alert - normal response
- Obtundation - stimulation → delayed answer
- Stupor - only reaction to repeated “hard” stimuli, eyes can open
- Coma - complete unresponsiveness
- Qualitative = “content” of mental function
- Delirium (acute confusional + agitated state) - fragmented attention, conc. + memore
- acute onset, fluctuant abnormal attention(worse at night)
- mental disturbances
- ↓ attention
- disorganzied thinking
- hallucinations/illusion
- level of conciousness/psychomotoractivity ↑/↓
- ↓perception
- memory disturbance:
- esp. diorientation to time
- ↓ short-term memory
- sleep disturbances: reversal of day-night cycle
- Neuro patho (stroke, epilepsy, trauma)
- Metabolic + drugs
- Infections (herpes)
- Perioperative
Ø perception
Ø reactivity
PLUS autonomic troubles
(⇒corneal + pupillary reflex might be preserved)
- Locked-in syndrome (see below)
- Øvoluntary movement response to stimuli
- Ø comprehension/expression
- Return of sleep eye cycle (periodical eye opening)
- brainstem + hypothalamic (autonomic) function preserved; cortical function ↓
⇒ ONLY REFLEXIVE MOVEMENTS
→persist. veg. state aka “Unresponsive wakeful state”
>1m ⇒ “persistent”
>6/12m ⇒ “permanent
- Catatonia (psych) → muted, ↓motor activity(maintain 1 position)
- CNS Damage (ext. or int.)
- diffuse cortical,
- midbrain, dienchephalon (thalamus),
- reticular system (brainstem)
- Systemic: metabolic, toxins
⇒ ASSYMETRICAL COMA (see exam findings)
⇒ SYMMETRICAL COMA
- External causes:
- Trauma
- Infections
- Tox
- Internal causes:
- Metabolic
- Space-occupying brain lesion (stroke, tumor, bleeding)
- Brainstem lesion (reticular - stroke, tumor)
GCS ≤8 📷
PLUS: Øresponse to verbal OR Øeye opening
ETIOLOGY SEARCH:
- trauma signs?
- fever? (infect)
- seizure signs? → tongue bite
- metabolic signs?
- intox signs?
- BP? (+HR) → BP↑:stroke, hypertensive encephalopathy → BP↓: bleeding, MI, tox, sepsis
- hypothermia? (intox, barbiturate)
- Breathing?
→ smells?

→ skin changes?
→sweating? tremor?

→ cheyne-stokes? → cerebral hemisphere / thalamus(diencephalon) (hyperventilation ↔ hypoventilation + apnea)
→ apneustic breathing? → bulbopontine (↑insp + pause ↔ end-expir. pause) → central neurogenic hyperventilation
- face assymetries? (wrinkles, folds)
- compress asc. mandible → induce grimacing (assymetry?)
- Muscle tone during noxious stimuli
(uni-/bilat.; spont./during noxious stimuli
- Decorticate rigidity → high lesion (subcortical, cerebral white matter) ; brainstem+pyramidal tr. are intact!
- Decerebrate rigidity → brainstem (pons + midbrain) lesion
⇒ 📷
3. Eye (pupils + gaze deviation)?
- Øblinking Ørestitance against passive opening
- pupil:
- size?
- o: bilat. arrective mydriasis → midbrain / atropin intox
- -: punctiform myosis → pons
- anisocoria?
- unilat mydriasis + Øreactive → CN3 / midbrain
- unilat. myosis → hypothalamus to cervical spinal cord
- conjugate lat. deviate 📷→ towards lesion / Strabismus


4. Reflex testing
- pupillary reflex? → midbrain lesion absent vs. present
- corneal reflex? → normal: both eyes blink → absent: pons (CN5, CN7 = reflex centers)
- Oculovestibular reflex? (caloric) 📷→ cold water in ear →normal: cold water pouring into the left ear leads to eye movement to the left and a direction of the nystagmus is on the right (opposite side) → absent: pons
- Cough reflex? → medulla (CN9,10 reflex centers)
- Oculocephalic / Vestibulo-ocular reflex(”dolls eye”)? 📷→ sudden rotation head → normal: eye move oppsite direction (visual fixation) → absent/delayed: brainstem nuclei + CN 3+6, CN8

(in awake patients: jerk correction nystagmus towards midline)

- EMERGENCY CT → IF FND!
- MRI: structural, infection?
- Lab-Screening:
- INFECTION: CBC + inflammatory lab
- consider CSF analysis
- consider blood cultures
- METABOLIC: liver function, BGA, Gluc, Elektroly, urea, crea
- TOX-screening (urine)
- Funduscopy
- EEG (seizure suspected)
- Stabilize vital function
- etiological Tx
- Hypoglycemia: glucose 30% iv 30 ml
- Epileptic seizure: Clonazepam iv 1 mg, Diazepam iv 10 mg or intrarectal
- Opioid overdose: Naloxone iv
- Benzodiazepine overdose: Flumazenil iv
- Alcoholic intoxication: Vitamin B1 500-1000 mg iv
- Trauma: neurosurgical advice
- “Coma Cocktail”:
- D - 50% Dextrose (D50): 1 amp IV after finger stick
- O - Oxygen at high flow (place on monitor to include pulse oximetry)
- N - Naloxone (Narcan): 0.4 to 2 mg IV initially
- T - Thiamine: 100mg IV (prevents Wernicke's)
- Treat suspected seizures: Lorazepam or Diazepam
- Coma (preceding) with known irreversible cause
- Ø Potentially reversible cause
- Complete loss of brain function
- isoelectric EEG (”electrocerebral silence”)
- brainstem:
- Ø spontaneous respiration
- Ø brainstem reflex
- Øcerebral blood flow (contrast angio)
primary → since childhood
psycho-physiological
“sleep attacks“
irresistible desire to fall asleep in inappropriate circumstances and places (while talking, driving, eating, walking); few minutes duration; patient feels refreshed on waking
- sudden loss of all voluntary muscle tone (Øresp.) for seconds
- Øloss of conciousness
→patient may fall,
- Sleepwalking - usually children
- Sleep terrors (pavor nocturnus) - usually children
- Sleep terrors (pavor nocturnus):
- Occurs in children aged 5-7 years, may persist into adulthood
- Familial history
- Symptoms: sudden sitting up in bed, dilated pupils, rapid pulse, frightened expression
- Includes motor and autonomic features
- REM sleep behavior disorders - usually elderly (act out the dreams) - i.e. neuro-degenerative diseases

A REM sleep parasomnia characterized by the absence of paralysis during the REM phase of sleep, leading to individuals acting out their dreams. Common in older individuals, symptoms may include talking, yelling, kicking, and self-injury.
- Compressive neuro signs
- Horner
- FND + seizures
- ↑ICP (papilledema)
- Thunderclap + Meningeal signs + Fever?
- Temporal artery tenderness?
Mnemonic: “PHANTOMS”:
- Pattern change, progressively worse, papilledema
- Horner syndrome (history of cancer, HIV, or lyme)
- Altered mental status, analgesics refractory
- Neurological deficits
- Temporal artery tenderness, Triggered by cough, exertion, or sexual intercourse
- Onset > 50 yr, thunderclap (worst headache)
- Meningeal signs, mid-dilated pupil (AACG)
- Systemic symptoms and signs (e.g., fever, myalgia), seizures
- + REDFLAG ⇒ IMAGING / Lumbar puncture
- Thunderclap → CT
- Papilledema (ICP) → CT/MRI
- Meningitis / SAH → consider Lumbar puncture
- (Giant cell a. → temporal arty biopsy)
- ØREDFLAG:
- exclude drugs + extracranial cause (↓Gluc, CO-intox, COPD)
- Duration (<3h/>4h?; days?)
- Location (uni vs. bilat, eye vs. larger area)
- Assoc. signs
- photophobia, aura, prodrome?
- post. neck-muscles tight?
- eye: lacrimation or horner?
- Tx of Migraine + Trigeminal → Triptans + Ergots
- Tx of Tension → analgesic + muscle relaxants
⇒ DDx migrain, tension, cluster 📷 :
Migraine prophylaxis: 📷
- prodrome
- Migraine prodrome occurs 24 to 48 hours prior to the onset of headache.
- Symptoms of migraine prodrome include increased yawning, euphoria, depression, irritability, food cravings, anorexia, and constipation.
- aura (neuro symptoms) - 25%
- headache
- postdrome (tired)

- unilat.
- throbbing / pulsatile
- >4h
- assoc. symptoms:
- nausea/vomiting
- photophobia (+ sound) = photophonophobia
ØAura = common migraine
- unilat onset →might spread bilat.

With Aura (25%)
- mainly visual aura scintillating scotoma 📷

- unilat. headache follows
- Paroxysmal hemicrania (cluster like, but short duration) →
- Headaches: rare, unilateral, short duration (10-30 minutes), episodic
- Pain: severe, throbbing quality, maximal in the orbital region
- Accompanied by autonomic features: lacrimation, myosis, nasal or conjunctival congestion
- More attacks per day
- Predominant in women
- Chronic daily
- chronic migraine
- medication-overuse
- During specif. situations
- Hypnic headache (during sleep)
- Cold stimulus (”brain freeze”)
- Exertional
- Cough
- Assoc. w/ sexual intercourse 😉
Tx: indomethacin

-#1 MRI → for every cerebral abnormality (esp. spinal cord lesions)
⇒ MOST SENSITIVE
-CT → bleeding suspected (i.e. trauma) or for exclusion (i.e. stroke)
pregnancy? → NO CT! (relative contraind.)
metallic implants (pacemaker) → NO MRI
- Parkinson 📷 + Alzheimer
- DDx Tumor vs. radiation necrosis
Risks:
- Stroke (occulusion, embolism) 📷
- Bleeding (perforation/dissection)
- RF
⇒ contraindications: anticoagulation + RF
⇒ but its indicated in both types of stroke with indication for endovasc. procedure (occlusion/dissection/aneurysm)
Indications:
- Infection/Inflammation?
- Diagnostic: MS, subarachnoid hemorrhage (SAH)
Contraindications:
- ↑ICP - Mass lesion (cerebral, spinal)
- Anticoagulation (spinal hematoma!)
⬆️ UMN lesions:
upper motor neuron lesions
parkinsons + alzheimer
- Amaurosis fugax → retinal a. occlusion (due to thromboembolism from cartotid a. , heart) → sudden + reversible
- Migraine ⇒ Retinal a. spasm
- Giant cell arteritis
- Optha causes
→ followed by headache
incongruous → optic chiasm lesion
⇒ pituitary adema
homonimous (congruous) → behind optic chiasm
⇒ optic tract (behind chiasm)/ optic radiation
⇒ temporal / parietal / occipital ⇒ Thalamus
In addition to: Basics > Neurological examination > Cranial nerves (see above)
- Ptosis
- DOWN + OUT ⇒ DIVERGENT STRABISMUS 📷
- blown (or normal) pupil
- + pain → susp. for acute compression (aneurysm, cerebral edema)
cerebral edema:

- Midbrain lesion → structural (esp. aneurysm)
- Intra-cavernous lesion 📷 → assoc. w/ CN 4+6 palsy + V1+V2
- Intra-orbital → structural(trauma, vascular, tumor, infection)


PUPIL INVOLVEMENT!
- Medical: vascular lesion more deep→ spares parasympathetic fibres (normal pupil)
- surgical: compressive lesion→ involv. superfical medial part (parasymp fibers) → mydriasis (aka “blown pupil” - sunopposed sympathetic activity)


Complete ipsilat + contralat ptosis
- Trochlear (4)
- intra-cavernous pathology
- vascular → diabetes, brainstem-stroke (pons)
- Compression → bleeding, tumor, ↑ICP
- Frontal (contralat)→ voluntary eye movements:
- Parietal / occipital (ipsilat)→ Automatic / pursuit eye movement: ⇒ slow (maintain fixation on moving object - ipsilat)
- Vestibular + Cerebrallar → Compensatory reflexes (compensate head movement to maintain fix)
- Brainstem → Integration(MLF) 📷from higher input (1.-3.)
- Midbrain → Vertical + Medial (convergence) gaze control
- Pons → Lat. gaze control
⇒ rapid (change fixation point - contralateral)

⇒ Eyes move together
BOTH EYES!! → symmetrical limitatation in one direction = CONJUGATE DEVIATION (horizontal or vertical)
- Horizontal gaze deviation (L-R)
- During seizure (contralat. frontal foci): jerking towards contracting limb (away from lesion)
- looks aways from hemiparesis (towards lesion) → Cortex (frontal lobe)
- looks towards hemiparesis (away from Lesion) → Pons
- Vertical gaze deviation (U-D)
- Midbrain lesion
- Internuclear opthalmoplegia (assymetric)
→ i.e. Perinaud syndrome (Øupward) 📷
- primary/idiopathic (essential)
- secondary (symptomatic)
microlesion trigemnial ganglia or post. root
(i.e.due to microtrauma )
- Compression (tumor, aneurysm, etc.)
- MS plaque touching CN5
- Infection → Herpes zoster opthalmicus 📷
- Trauma
- Clinic:
- Idiopathic: - Between attacks pain free - Neuro-exam = normal
- Secondary: - continous sensation (mild pain betw. attack) - neuro exam abnormal (hypoesthesia, loss of corneal reflex)
- MRI ⇒ look for lesion !
#1 Carbamazepin
- Alternatives: Other anticonvulsants
- Refractory: Surgery/ RF
Refractory cases successfully treated with various procedures:
- Radiofrequency ablation of the Gasserian ganglion
- Gamma knife
- CyberKnife
- Surgical nerve decompression
- Percutaneous thizotomy
- herpes zoster → aciclovir i.v.
face, ear, taste, tears
- facial muscles
- stapedius muscle (ear)
- taste (Øbitter) ant 2/3 tongue
- lacrimal gland
- PERIPHERAL (Facial n + facial n brainstem nuclei)
- whole face + ipsilat weakness
- forehead → Øwrinkling
- cant close eyes (lagophthalmia)
- cant smile/whiste
- OTHER FACIAL NERVE DYSFUNCTION!
- dry eye
- hyperacusis
- saliva drooling
- loss of taste ant 2/3
- Bell’s phenomena 📷
upward eye movement when attempting to close the eyes
- CENTRAL
- only lower part + contralat (same side as hemiparesis)
- look at flat nasolabial fold + assymetric smile (forehead muscle normal)
- Pyramidal syndrome + cortical signs
- Øother facial nerve dysfunction signs

- Idiopathic = Bell’s palsy
- ↓Inflammatory swelling → Steroids 🌝
- Kill the virus → Acyclovir 🦠
- Protect the cornea (↓tears) → eye patching, artificial tears 🥲
- Secondary
- Infection
- Herpes zoster → + pain + vesicles ext. auditory canal ⇒ Acyclovir
- Lyme (Neuro-borreliosis) → + fever + circular eruption + Serum Ab ⇒ AB
- Inflammation
- Compression
🦠 - inflammation CN7 → swelling → entrapment + ischemia ⇒ ACUTE ONSET but usually benign course
🦠 → 🌕 ⇒ 🔥 + 💦 → ↘️
- Visual system (head position)
- Proprioception (joint position)
- Posture + gait (vestibulo-cerebellum)
- Peripheral: Labyrinth or vestibular nerve (internal ear, intracranial) ⇒ nystagmus unidirectional
- Central: Pons (CN8 nuclei) or connection betw. CN8 + higher centers ⇒ nystagmus multidirection
Peripheral
(harmonic) | Central
(dysharmonic) | |
Vertigo | intense | moderate |
Cochlear signs | present | absent |
Nystagmus | horizontal or horizontal-rotatory
unidirectional | purely rotator or vertical
multidirectional |
Slow deviation of eyes, Index deviation, Romberg sign | lateralized to affected side | Ølateralized |
Other neuro signs | absent | present |
- Stroke (ischemic+hemorrh) →(brainstem:) vestibular nuclei OR cerebellum
- Trauma
- MS
- Drug induced → Anticonvulsants
- Infection
- Tumor
- Migraine
- Dysphagia + Dysphonia
- unilateral Øgag reflex
dysphonia:

- taste post 1/3
- dry mouth (parotid)
→ CN9 root compression (structural cause) 📷
Paroxysmal severe pain
⇒ in SENSORY TERRITORY: Base of tongue, tonsilar fossa + pharynx + reffered ear pain
⇒ caused by Activity of pharynx muscles: chewing/swallowing/yawning
- Dysphonia / Hoarseness (ENT exam: unilateral vocal cord paralysis)
- Dysphagia (unilat. paralysis uvula + soft pallate)
- ⇒ deviation uvula: curtain signs 📷
- Pharynx + Larynx: Unilat. sensory loss
- unilat. Øgag reflex
⇒ Hypoglossal palsy: see above
PAINFUL HORNER
→ CN12 close to carotid artery 📷 → carotid dissection
- Trombotic → classic CV-RF
- large vessel artherosclerosis
- small vessel artherosclerosis
- carotid artery stenosis
- Embolic (→ small OR large vessel occlusion)
- Carotid artery
- atherosclerosis (can be embolic or thrombotic)
- dissection
- Heart
- Afib/Aflutter
- Valve path.
- Other
- Non-artherosclerotic vasculopathies (i.e. vasculitis)
- hypercoagulability/hematologic diseases
- Undetermined etiology
- sudden onset FND
- lasting 10-20min (up to 24h)
- ØBrain dmg!
Carotid TIA (#1)
- mono-ocular blindness (amarosis fugax)
- hemispheric syndrome aka classic: aphasia, hemiparesis
Vertebrobasilar TIA
- brainstem/cerebellar syndrome (ataxia, diploplia)
- visual (homonymous hemianopsia)
more infos carotid + vertebrobasilar artery → later








Type of stroke | Location | Symptoms |
Pure motor (#1) | - Int. capsule (post. limb)
- basis pontis | contralat. hemiparesis face + extremities |
Pure sensory | - Thalamus | contralat. paresthesia/numbness face + extremities |
mixed sensorimotor | - Thalamus + Int. capsule (post. limb) | contral. hemiparesis (pyramidal) + paresthesia/numbness |
ataxic hemiparesis (#2) | - Int. capsule (post. limb)
- corona radiata
- basis pontis | ipsilat. hemiparesis + cerebellar symp** (ataxia, gait instability)
leg > arm |
dysarthria / clumsy hand | - Pons | Contral. lower face + hand hemiparesis
⇒ Dysarthria + clumsy hand (writing)
(+/- ipsilat. hyperreflex + Babinski)
arm > leg |


any type but:

corticobulbar tract:

- Stroke #1: ischemic / hemorrhagic
- MS
- Tumors
- etc.
- cranial nerves and/or cranial nerve nuclei
- major brainstem tracts (white matter)
reticular activating system
Ipsilateral cranial n. findings
Contralat. Periph. Motor/sensory
Exception: CN IV - contralat. sup. Oblique
Midbrain syndromes
Tracts | Nuclei / Nerv | Physiological centers | Arteries affected | |
Weber (ventral) | 1. corticospinal
→ contralat. hemiparesis
2. corticobulbar | 1. CN3 (not nucleus)
→ ipsilat. CN3 palsy | - | PCA
(Post. cerebral a.) |
Benedikt (paramedian) | 1. Corticospinal
→ contralat. paresis | 1. CN3 palsy (nerv)
2. red nucleus+ substantia nigra
→ contralat. parkinsonism | - | PCA |
Parinaud (dorsal) | sup. colliculi/ med. long. fasciculus (eye movement control)
→ vertigal gaze palsy
→ Eyelid retraction
→ convergence-retraction nystagmus | - | PCA, compression in children (i.e pinealoma) |
Pontine syndromes
Tracts | Nuclei/Nerv | Physiological centers | Arteries affected | |
Locked-in (ant + bilat.) | 1. corticospinal
→ quadriplegia
2. corticobulbar
→ anarthria (cant move+ speak; except eyes → pat. is aware+can feel) | CN6 (nerv not nuclei)
→ horizontal eye movement restriction | - | - Basilar a. (stroke, trauma),
- Central pontine myelinosis (after rapid hypoNa+ correction) |
Raymond (medial) | 1. corticospinal
→ contralat hemiparesis | CN6 palsy
→ ipsilat. lat rectus paresis
| ||
Millard-Gubler (medial) | 1. corticospinal
→ contralat. hemiparesis
| CN6 palsy
→ ipsilat. lat rectus paresis + diploplia
CN7 palsy
→ ipsilat. facial palsy | Basilar | |
Marie-Fox (lat) | 1..spinothalamic → pain +temp
2. cerebellar → ipsilat. ataxia
3. (corticospinal) | NUCLEI:
CN5 - pain+temp
CN7 - face palsy
CN8 - hearing loss, vertigo, nystagmus
| AICA |
Medullary syndromes
Tracts | Nuclei | Physiological centers | Artery affected | |
Wallenberg (lateral) | 1. spinothalamic
→ contralat. periph. paresthesia (pain+temp)
2. spinocerebellar/inf cerebellar peduncle
→ ipsilat. ataxia
3. hypothalamospinal
→ ipsilat. horner | 1. ambiguus (CN9+10)
→ hoarse voice + dysphagia
2. vestibular (Deiter’s)(CN8)
→ vertigo + nystagmus
3. CN5 (nucl+ nerv)
→ ipsilat. face paresthesia (pain+temp) | Reticular formation
→ ↓conciousness | Vertebral, PICA |
Dejerine (medial) | 1. corticospinal → contralat. paresis
2. medial leminiscus (dorsal colum)
→ paresthesia (other than pain+temp) | CN12 nerv → ipsilat. tongue deviation, dysarthria |
- Dysphagia
- Ataxia
- Nystagmus
- Vertigo
- Anaesthesia
- Horner's syndrome
- Convergence of all sensory input before → cortex
- Integration of cerebellar information (movement control)
→ Cortical activation
- SENSORY #1:
- contralat. thalamic pain (burning)
- Hyperalgesia
- Hyperpathy
- paresthesia/hypoesthesia
- unstable thalamic hand
- NEURO-PSYCH (like right + left cortical lesion)
- LEFT: thalamic aphasia (jargon speech)
- RIGHT: thalamic neglect, visuo spatial disorientation
- BILAT: somnolence, coma, amnestic syndrome
- nearby structure damage: INT. CAPSULE → contral. hemiparesis


amnestic syd:

D - Dysdiadochokinesia + Dysmetria + Dysarthria
A - Ataxia (gait, trunk, limb [clumsy hand])
N - Nystagmus + oculomotor dysfunction
I - intention tremor
S - slurred speech
H - hypotonia (pendular reflexes)



stroke + neurodegenerative disorders
occupational Tx



more discrete agnosia ⇒ Gerstmann syndrome

- Primary motor area: Hemiparesis
- Premotor: Contralat. Apraxia/↓Spontaneity
- Primitive reflexes (pathological prehension)
- Oculomotor area: looks towards lesion, away from hemiparesis (see above)
- Broca’s aphasia
- Gait abnormalities (seems to “forgot how to walk”)
- Sphincter dysfunction
- Motor behaviour abnormalities
- Imitate examiner's gestures
- Automatic behaviors
- Manipulation of any found object (utilization behavior)
- Lack of initiative for moving
- Apathy
- Lack of interest
- ↓Insticts → bulimia, sphincter dysfunction, sexual dysfunction
- Personality changes → AGRESSIVE, SOCIAL DISINHIBItiON, INAPPROPRIATE JOKES
COGNITIVE CHANGES
(inability abstract thinking, cant solve problems, attention defiicit)
- SENSORY loss (sensory cortex)
- Apraxias (Ideational, dressing, constructional) + Agonias (tactile)
- Alexia + Acalculia (left parietal)
- Homonimous hemianopsia (contralat)


- AUDITORY: “Cortical deafness”
- VESTIBULAR dysfunction
- Wernicke’s aphasia
- HYPOCAMPUS + LIMBIC SY: emotion + behavior disorders + memory disorders
Disorders of emotions and behavior: rage, aggressive outbursts, suspiciousness, poor judgment, indifference to others' feelings.
- homonimous hemianopia (contralat)

VISUAL (RECEPTIVE + ASSOCIATIVE)
- RECEPTIVE:
- “Cortical blindness”,
- Homonimous hemianopia/quadrant- (contralateral visual field loss)
- ASSOCIATIVE
- Illusions / Hallucinations
- Loss of topographic memory (right occip. → spatial)
- Hypo/Hyper-Glycemia
- MI
- Neuro-vascular path.:
- periph. neuropathy
- decr. circulation
- Nerve Compression
- spinal stenosis / herniated disk
- Tumor
- Subdural hematoma
- thoracic outlet syn
- Hemiplegic migraine
- Todds’ paralysis (in postictal phase of seizure)
- Conversion disorder (=functional)
- CT → Ischemic vs. hemorrhagic 📷
- other ischemic signs
- consider additional exams
- time of onset? ⇒ tPA? mechanial thrombectomy?
- Control BP + Anti-platelet
- ↓ICP + Tx of other complications
- Etiology search? (Next day (or earlier)) + specific Tx
- Rehab
- general chronic Tx post-stroke (2nd. prophylaxis)


Hyperdense MCA: 📷
Loss of gray-white matter differentiation: 📷
MRI DWI (early phase): 📷
Ischemic penumbra: 📷
diffusion-perfusion mismatch (penumbra = blue): 📷


GRADUAL PROGRESSION!
variable onset (progressive vs. brutal)
Cushing triad 📷
- ↑BP (sys)
- Bradycardia
- Respir. Alteration (Cheyenne-stokes) → brainstem herniating
- Perfusion pressure of the brain (CPP) is the difference between mean arterial pressure (MAP) and intracranial pressure (ICP).
- An increase in ICP leads to a decrease in brain perfusion pressure, resulting in reduced cerebral blood flow and oxygen supply to the neurons.
- To prevent this, the systemic blood pressure is often dramatically increased to maintain a constant ratio of MAP to ICP.
- However, this further elevates the ICP, creating a vicious cycle where the arterial pressure must continue to rise.
- hernation → damage to brainstem → Respiratory alterations (respiratory centers in brainstem)
Other signs
- Headache (progressive, hard to control with analgesics)
- Blurred vision (papilledema)
- Nausea/vomiting
- Consciousness alteration



- Trauma
- Aneurysm rupture
- AVM (arterio-venous-malformations)
saccular (berry) aneurysm = congential
7mm
classfication:
small <10
large 10-25
giant >25
- Thunderclap headache
- Meningeal signs
- Neck stiffness (= nuchal rigidity)
- Kernig sign
- Brudzinski sign
- Photophobia
- Nausea + Vomiting
- Fever (due to irritation of meninges) + lethargy/↓ consciousness
Sudden, severely painful headache (often described by patients as the worst headache they have ever experienced)

⇒ 📷
+/- FND ⇒ “cerbro-meningeal hemorrhage” (further evolution see below) ← if blood ruptures into parenchyma + leads to mass effect
- Physical exertion
- Cough
- Defecation
- Sexual intercourse
- Prolonged sun exposure
- INFECTIOUS MENINGITIS (fever, lumbar puncture for dg)
- Other causes for headache:
- migraine
- cluster headache
- paroxysmal hemicrania
- exercise-induced headache




CT Subarachnoid hemorrhage: 📷
- Rebleeding (max risk in first 24h → 14d)
- Vasospasm (7-10d) → secondary ischemic stroke
- Nimodipine (CCB)
- magnesium sulphate
- Triple-H
- Hypervolemia
- hemodilution
- Anti-hypertensives
- Hydrocephalus 📷 → might require drainage
- acute obstructive (min - h)
- chronic communicating (weeks-m)


⇒ Monitor with transcranial Doppler
VERY BAD ☹️
- 20% mortality rate within the first 24 hours
- 40% mortality rate within the first week
- 50% of survivors experienced significant disabilities and had recurrent aneurysms
congenital malformation → direct communication betw. arteries&veins + NO capillary network
⇒ AVM can rupture
children / young adult
→ usually ruptures betw. age 30-40
superficial or in parenchyma
→ thats why it can cause ICH + SAH!
T → symptoms before rupture!
FOCAL NEURO SIGNS:
- focal seizure + FND
- hemicrania (unilat. headache)
+bruit on skull auscultation
💡 Like SAH PLUS FND
⇒ cerebro-meningeal hemorrhage: “meningeal signs” + FND
REMOVE THEM:
- surgery
- gamma-knife (stereotactic RT)
- endovascular embolization
Thrombus in sinuses 📷 📷 → ↓ cerebral drainage → ↑ intracranial pressure → hemorrhage (+ other clinical features)
congestion within venous system of the brain → blood stasis → ↓ cerbral perfusion → cerebral edema and/or infarcts/stroke
- Headache
- Signs of ↑ICP
- VISUAL: Bilat. papilledema + other vision imparment
- ↓Conciousness
- nausea + vomiting
- Neurologic deficits
- Seizure + FND (focal OR generalized)
- Cranial nerve syndromes (i.e. blown pupil - CN3)
- Cavernous sinus syndrome
- Compression of cranial nerves (III, IV, V1, V2) passing through the cavernous sinus
- Symptoms: ophthalmoplegia, conjunctival congestion, proposis, sensory loss in the trigeminal area (forehead and cheek), Horner syndrome
- Conditions related to the cavernous sinus can cause CSS, such as cavernous sinus thrombosis, carotid-cavernous fistula, and cerebral metastases.
- Diplopia
- Tinnitus
- Unilateral deafness
- Facial palsy
- Infectious (spread from sourrounding source)
- ↑ back-pressure in the veins ⇒ EYE SWELLING + PAIN:
- Swelling Conjunctiva
- Exophthalmus
- periorbital pain
- edema with vein dilation
- Compressive signs
- Signs of CN palsies
- Painful ophthalmoplegia = unilat. periorbital headache + partial/paresis of one occulomotor nerve (CN 3+4)
- ØCorneal reflexes (V1 involvement)
- ØCorneal + Øupper facial sensation (V1+V2)
- Horner’s syndrome 📷
- Seizures + ↓conciousness
- Non-infectious: Hypercoaguable states
- ↑Estrogen: oral contraceptives, pregnancy, postpartum period
- Elevated estrogen levels and changes in blood composition during delivery and due to thrombokinases released by the placenta may increase the risk of cerebral venous thrombosis (CVT).
- Cesarean delivery is the recommended procedure for women diagnosed with CVT.
- pregnant woman
- headache
- seizure
- alternating FND (mono-/hemiplegia: esp. lower limb)
- abnormal Blood, Coagulation, Blood vessel: Hematologic + Autoimmune + hemostatic diseases
- malginancies


CN3 - Occulomotor
CN4 - Trochlear
CN6 - Abducens
CN-5 (V1+V2) - Trigeminal
⇒ visual disturbances
sup. saggital sinus thrombosis
→ might be focal or generalized

- Anticoagulation
- ↓ICP 📷
- Infectious? → AB
- anti-convulsant prophylaxis

F
MS is a chronic neurologic disease which evolves throughout several decades Natural history studies: time from onset to wheelchair is 15-20 years
F
MS causes the accumulation of irreversible disability over time whereas survival is only slightly affected.
- Patient age: 11-50y (mainly 25-40)
- Relapse + remission pattern
- Optic neuritis (unilat)
- Pyramidal syndrome (UMN)
- Sensory syndrome
- Lhermitte sign
- MS-hug
- Motor syndrome → esp. lower limbs
- fatigue after walking
- Cerebellar syndrome
- Brainstem syndrome
- Internuclear opthalmoplegia
- Uhtoff phenomenon
- Sphincter disturbance (retention or urgency)
- Fatigue Øeffort-related
electric shock in the back and/or limbs during neck flexion


- (mainly) unilat. ↓/Ø vision
- +/- pain
- diploplia
- marcus gunn pupil

classic
(mainly bilat. involvement)




reversible exacerbation of neuro-symptoms due to ↑ bodyTemp
(i.e. exercise, fever)




- sensory + motor
- optic neuritis
- spinal cord syndrome
- CIS ⇒ first suggestive clinical episode

- RR-MS
- SP-MS
- PP-MS
incidental imaging finding suggestive for MS
Øclinic (past+current)
- Infection (i.e. borelliosis)
- Inflammatory disorder (i.e. ADEM, SLE, vasculitis)
- granulomatous disease
same as MS acute exacerbation
#1 steroids
#2 plasmapheresis


- MRI
- not confirmed by MRI:
- CSF analysis
- Oligoclonal bands
- ↑IgG
- normal cell-count
- VEP (↓latency)
visual evoked potentials

*Oligoclonal bands: 📷

- Interferon + Glatiramer
- Oral drugs
- Teriflunomide
- Di-methyl fumarate
- Fingolimod
- Mabs
- Ocrelizumab
- Natalizumab
- Alemtuzumab
- Special shit
- SP-MS → Siponimod
- if severe MS→ Mitoxantrone (🫀-tox)
Teri(-flunomide) and Natali(-zumab) are Glad(iramer) to be on the inter-phone (Interferone) 📞

#1 steroid i.v.
#2 plasmapheresis

⇒ see also Neurosurgery
❌ total cord transection syndrome
→ Spinal shock = classic acute UMN signs + sensory loss + autonomic (bladder):
- acute:
- ØMOTOR: flaccid paraplegia + ØReflexes
- ØSENSORY
- autonomic signs (urinary retention [overfill incontinence], bowel), babinski +
- days/week → spasticity, ↑Reflexes
→ sometimes: only ↓ below; hyperesthesia/-algesia
⇒ if above C3 → respiratory failure
⇒ C2-C5 → hypotension

lateral hemisection syndrome (stabbing wound)
- ipsilateral → weakness (corticospinal)
- ipsilateral → vibration/proprioception (dorsal colum)
- contralat → pain + temp + light touch (spinothalamic)
- Øbladder symp (autonomic) → only unilat. involvment of autonomic fibers
BILATERAL:
- medial CST: weakness arms > legs 📷

- SUSPENDED:
- reflex Ø at the level of lesion (reflex arc from dorsal → ventral horn) 📷
- Ø pain + temp (crossing spino-thalamic fibers) in specif. dermatoma ⇒ “suspended-sensory level” = minimal sensory decit
- Ø bladder symptoms (no involvment of autonomic fibers)

- Etiology: Syringomyelia , degenerative lesions
syringomyelia:

- corticospinal → weakness + reflex changes
- desc. autonomic tracts → bladder dysfunction
- spinothalamic → pain temp
⇒ all bilateral
- corticospinal → UMN signs (depending on acute vs. chronic)
- dorsal colum → ataxia + paresthesia (proprio + vibration)
- autonomic fibers → bladder incontinence
- Etiology: TABES (neurosyphillis)
- Lesion below L2
- ØMotor Ø Reflex (bilat.)
- ØSensory ⇒ 🏇🏽 SADDLE ANESTHESIA 📷
- ØAutonomic ⇒ bladder bowel
⇒ IMPAIRMENT spinal cord/nerves at LEVEL OF LESION
- limited motor neuron signs
- only 1 Reflex absent
- transversal dysesthesia (dermatome?)

- unilateral radicular (radiating) pain in fixed area
- ↑by cough + at night
DAMAGE TO ASCENDING/DESCENDING TRACTS
pyramidal tracts → paraplegia / hemiparesis
spinothalamic + dorsal → sensory loss
autonomic → sphincter control loss
⇒ VERTEBRAL BONE LESION
⇒ pain
⇒ ↓mobility,
⇒ paravertebral stiffness
SPINAL SHOCK
- Ømotor: complete paralysis below
- Øsensory: anesthesia
- Øreflexes
- Øsphincter control
- Dg: MRI 📷
- Tx:
- before surgery:
- i.v. steroids (↓spinal edema)
- ventilatory support if above C4
- SURGERY
- Rehabilitation
- back pain
- radicular pain +/- weakness
- 🚑 ACUTE SPINAL CORD COMPRESSION ⇒ acute UMN signs
TRANSVERSE → complete below
- Infectious
- viral (a lot of them; i.e. CMV, HIV)
- bacterial
- (neuro-) syphillis
- TBC
- Lyme
- fungi / parasites
- Autoimmune
- MS
- SLE
- Vasculitis
- Sarcoidosis

- MRI contrast → edema
- Lumbar puncture → CSF anaylsis
- Lab → inflammatory vs. autoimmune

- ↓Edema → i.v. steroids
- Etiology specific Tx
⇒ abscess in epidural space (venous plexus); Staph Aureus
- distal spread (seeding via bloodstream)
- vertebral infection (osteomyelitis)
- direct inoculation (invasive procedures)
epidural anesthesia, spinal surgery, paravertebral injections
- back pain + tenderness
- menigeal signs + fever
- bilat. motor → paraplegia
- Lab → Infection marker
- MRI
surgery + AB
MEDIAL hernation → spinal cord compression
⇒ pain + tenderness + neuro signs
MRI 📷 ⇒ 🔪 surgery
- trauma
- anticoagulation Tx
- AVM rupture
Transverse myelitis (complete or partial signs)
- pre-monitory signs might be present (”spinal TIAs/claudications”)
- sudden onset
→ paraparesis + numbness after walking (↓w/ rest)
→ acute UMN signs: bilat. weakness, Øreflexes
→ pain (radiating)
→ dissociated sensory loss: pain + temp loss (dorsal column spared) d
degenerative changes (joint thickening, osteophytes, ligament hypertrophy)
↓
Spinal canal narrowing
↓
<13mm → myelopathy
↓
microtraumas & compression of vessels (ischemia)
microtraumas:

- progressive onset / old patient
- UMN signs → assymetric spasticity (drag 1 leg), → bilat. reflex / babinski
- sensory signs (paresthesia)
- neck pain
- Lhermitte
- MRI → Diagnosis
- Xray
- EMG + ENG
mild → collor
progressive → surgery
COMPRESSION OF:
- nerve roots: radicular (radiating) pain
- CST: UMN signs
- spinothalamic: unilat. sensory
- unexplained spinal cord syndrome → slowly progressive
- radicular pain
- pyramidal signs
- sensory
- dorsal lumbar region
- male >50
DG: MRI, angigraphy
Tx: Embolisation
congenital fluid-filled cyst (tubular) within spinal cord (cervical)
⇒ enlarges → compression gray matter
CENTRAL CORD SYNDROME + ant. horn ⇒ BILATERAL
- Early: Spinothalamic → Dissociating sensory loss
- “cape-like” distribution (neck, shoulders, arms - cervical region)

- in Evolution:
- LMN: muscle atrophy + flaccid paresis
- UMN: weakness + Pyramidal signs
MRI + EMG
decompression SURGERY
⇒ tubes: drain fluid from canal to subarachnoid space 📷
Demyelinationg dorsal + lateral (CST) columns ⇒ subacute lesion
- Dorsal colum
- sensory loss→ paresthesia, vibration, proprioception
- Sensory ataxia → pos. Romberg
- chronic UMN signs (later)
TRANSVERSE MYELITIS
→ paraparesis (spastic)
→ numbness + paresthesia (lower limb)
Other cerebral pathologies
default: GABA inhibits movement
→ DOPA inhibits GABA ⇒ movement stimulation
→ Ach stimulates GABA ⇒ movement inhibition



- Bradykinesia/akinesia
- shuffling small gait (↓speed+amplitude)
- difficulty initiating steps
- mask-like facies,
- freezing (transient inability to walk)
- micrographia (small effortful handwriting)
- dragging of one leg(if unilat.)
- Rigidity
- cogwheel
- led pipe
- Lead pipe rigidity: constant increase in muscle tone throughout passive movement
- Cogwheel rigidity: Difficulty in movement due to joint stiffness; extreme stiffness of the joint, movement is jerky and resembles ratcheted rotation of a cogwheel
- Resting tremor (pill rolling)
- Postural/gait instability (shuffling steps, , fall over when walk)
- Postural instability refers to imbalance and loss of postural reflexes.
- It is assessed by having patients stand with their eyes open and pulling their shoulders back toward the examiner.
- Patients should be ready for the displacement and aim to regain their balance as quickly as possible.
- Taking 1 or 2 steps backward to regain balance is considered normal.
- The examiner should be prepared to provide support if patients are unable to regain balance.
- Non-motor signs
- Neuropsychiatric (depression, dementia)
- Sleep disturbances
- NERVES
- Hyposmia (can’t smell) - EARLY SIGN
- sensory symptoms
- autonomic dysfunction (i.e. orthostatic hypotension, constipation)
F! → clinical dgx
(MRI only if unsure)
Bradykinesia

+ 1 OTHER (Rigidity OR Tremor(resting)
+ Ø exclusion criteria
- 2️⃣ Secondary parkinsonism
- drug-induced (antipsychotics)
- Vascular (small lesions in basal ganglia)
- Neurodegenerative
- Metabolic: Huntingtons + Wilsons
- Infections (i.e. creutzfeldt-jakob)
- Toxin-induced (i.e. pesticides)
- Essenstial tremor
- ➕Parkinson-Plus syndromes
- 🎛️ cerbellar signs (i.e. cerebellar ataxia)
- 🧠 cortical signs (aphasia, apraxia)
- 🦵🏼 restricted to lower limb >3y
- etc.

- Levo +/- carbidopa
- Dopa-agonists (Ropinerole, promipexole)
- COMT-i (”-capones”)
- MAO-B-i (Selegeline)
- Ach-i (benztropine) - young
- 🥓 GI + ulcer (!ulcer bleeding)
- ❤️Arrhythmia
- 🚗 Autonomic: Orthostatic Hypotension
- 🤪 ↑Neuropsychiatic symptoms + Ø😴 insomnia
- DYKINESIAS

- Response fluctuations: on-off phenomena
- wearing off
- “delayed on”
⇒ therapeutic windows narrows when the disease progresses
- Periods of efficacy with alternating periods of reoccurrence of parkinsonism = “On-periods” (controlled) and “off-periods” (recurrence)
- Wearing-off effect: levodopa effect ends before the next dose
- Delayed-on effect: levodopa effect is delayed
- Multi-system atrophy
- MSA-C → + cerebellar
- MSA-P → + UMN (dysarthria + pyramidal) + Tx refractory
- Shy-Drager syndromes → Autonomic: urinary incontinency + orthost. hypot.
- Progressive supranuclear palsy → + upgaze palsy = Benedikt syndrome (midbrain syndrome)
- corticobasal degeneration → + apraxia, coginitive, alien limb, myoclonus
- dementia with lewy bodies → + demetia, visual hallucinations
alien limb:

- Hoehn + Yahr scale
- UPDRS (United Parkinson Disease Rating Scale)

- ACTION tremor ☝🏼
- improvement after small amount of alcohol 🍺
Sydenhams = manifestations of rheumatic fever→ recent URT-infection?
- YOUNG ADULT (35-45y) + FH⇒ main DDx point
- Chorea (dykinesia)
- Psychiatric troubles
- Dementia (later)
copper chelating agents
⇒ D-Peniciliamine or Trientine
UMN:
- Precentral gyrus (& prefrontal) motor neurons
prefrontal neurons: involved in planning / orchestrating the signals of the upper and lower motor neurons.
- axon degeneration
LMN: ant. horn + brainstem neuron degeneration
- Age >50y
- #1 limbs onset → arms/legs (80%) → motor signs: cramps, weakness, falling
- #2 bulbar onset (20%)
- Emotional lability (involuntary outburst of laughing/crying) + depression
→ bulbar signs(CN9+10,12) (hoareseness, dysphagia, dysarthria, tongue atrophy)
- Signs of LMN lesion
- classic LMN signs (fasciulations, ↓reflexes, ↓muscle tone)
- classic UMN signs (i.e. spasticity)
- ØSENSORY Signs


OTHER LESIONS AT THE TYPICAL LOCATIONS
- brainstem
- spinal cord
- neuro- + myo-pathies
- EMG ⇒ NORMAL sensory + abnormal motor
- structural etiology exclusion → MRI
- DMT (↓progression)
- Riluzole
- early onset + rapid progressive? → Edaravon
- Symptomatic Tx
- Pain → analgesics
- muscle cramps → levetiracetam
- dysphagia → diet-modif., PEG
- Mood alteration → SSRI/ TCA
- Respiratory insuff → non-invasive ventilation
- Spasticity → muscle relaxants (baclofene)
- sialorrhea → anti-cholinergic (atropin)

⇒ both have unknown mechanism of action in ALS

cognitive alteration → acquired + persistent + progressive
- memory impairment
- cortical signs (see above)
- aphasia
- apraxia
- agnosia
>70y

- Forgetfulness
- Cortical signs (parietal/temporal)
- aphasia (parietal)
- apraxia (parietal)
- agnosia (parietal + temporal)
- Hypocampus: Sleep + personality/mood changes ⇒ paranoia
- Neuropsychological testing → ↓memory + verbral skills
- CT/MRI 📷
- EEG → slowed (diffuse)
- CSF → normal
→ hippocampus atrophy → enlarged lat. ventricle (temporal horns) → (indirect due to atrophy)
- Ach-esterase inhibitors (mild-mod)
- Donepezil
- Rivastigmine
- Galantamine
- NMDA-R antagonist (mod-sev / add-on)
- Memantine
- blocks excess glutamatergic transmission (blocks excitatory signals)
- may have neuroprotective effects

- Frontotemporal dementia
- Parkinsonian dementia
- Dementia with lews bodies
- Huntingtons
- vascular → FND + cortical signs
- Inflammatory: infectious, autoimmune
- metabolic,
- traumatic


CEREBELLUM (+/- spinal cord)
EARLY ATAXIA!
childhood / early adult
Friedreich ataxia (AR)

- 🎛️ + 🫀
(cerebellar dysfunction + Cardiomyopathies)
→ ataxic gait, clumsiness, ↓reflexes, dysarthria

⇒ see neurologic exam → typical for cerebellar
- claw foot 📷

- Nerve conduction studies
- MRI ⇒ exclusion cerebellar tumor)
- Coenzyme Q and vitamin E supplementation
- Gene therapy for neurological disorders
- Foot orthoses for gait improvement
- Genetic /idiopathic & Congenital(+perinatal)
- Genetic
- 5-20y
- Øother neuro signs
- FH+
- congenital = malformation
- infancy / early childhood
- structural (gross abnormalities / features of underlying disease)
- head trauma ( young + old) + tumor → compressive hemorrhage
- strokes, degenerative disease (old)
- Metabolic
- immune / infection
(DM, Elektrolytes dysbalance, waste product accumulation (kidney), nutritinal def., phenylketonuria, intox / withdrawl)
provoked → immediate preceeding cause
unprovoked → unknow etiology OR pre-existing (progressive) cause
ANY OF THE FOLLOWING:
- ≥2 seizures (unprovoked/reflex) >24h apart
- 1 unprovoked seizure and similar recurrance risk as “1.”
- EEG abnormalities (inter-ictal)
- Neuro-exam abnormalities
- seizure during sleep
- Symptomatic secondary cause (tumor, prior CNS infection)
epileptic seizures ≥5min (for tonic-clonic)
(Øconciousness in this time aka generalized)
Status epilepticus is a seizure that lasts ≥ 5 minutes or a series of seizures in rapid succession without full neurological recovery in the interictal period
Focal (unilateral → may spread) | Generalized (bilat) | |
Origin | Single hemisphere | Both hemisphere |
Awareness | aware or impaired | Ø |
Symptoms | Motor (↑/↓)
Non-motor (sensory, cognitive, autonomic) | Motor (Tonic clonic or other motor)
Non-motor |
- clonic: sustain rhythmic jerking (automatism movement - i.e. lip smacking, automated movements)
- unilat. body
- may spread prox. (”jacksonian march”)
- tonic: ↑tone (sec-min)
- atonic: ↓/Ø muscle tone
- myoclonic - short brief single / series of muscle contraction (jerks)
- hyperkinetic: irregular large amplitude (”chorea-like”)
- automatism: repeating automatic actions
Øtonic-clonic
- Sensory (somatosensory, visual, auditory, olfactory, gustatory, vestibular)
- Cognitive → cortical symp (aphasia, agnosia, memory, hallucination, alexia, etc)
- Emotional (everything imaginable; unapproriate bursts of laughter)
- Autonomic
(cardiac, GI, cutaneous, respiratory, urination, lacrimation, etc)
- Tonic-clonic (”grand mal”) - 1-3min
- Tonic (w/ expiratory sound in beginning)
- Atonic → brief ”drop attack” or unilateral sagging (seconds-min)
- Myoclonic → brief (seconds) jerk
- Epileptic spasms → on awakening sudden brief flexion, extension or mixed proximal + truncal muscles
Øhyperkinetic + Ø automatism
- Typical absence
- abrupt onset + offset of conciousness-loss (5-10(15) sec)
- multiple times a day
- memory impaired (retrograde)
- +/- assoc. features
- +/- minor clonic movement (twitching) of face + eye muscles
- +/- automatisms
- Øpost-ictal phase
- Atypical absence
- Less abrupt onset + offset
- Less loss of conciousness
- ASSOCIATED w/ loss of muscle tone (head, trunk, limb)
- Myoclonic absence
- jerks → shoulder + arms
- with tonic abduction → lifting of arms during seizure
(i.e. starring with variable loss of conc.)
→ history taking from observing person + patient!
- Before:
- trigger? (syndrome?)
- aura? (Ø in generalized)
- During:
- duration of seizure? etc
- trauma during seizure?
- ↓/Øconciousness? (awarness, memory, response, sense of self)
- After:
- UMN signs ? (FND, aphasia) →structural
- classic postical?
→ talk + response + comprehend? retrograde amnesia? autonomic?
- look for trauma
- Aspiration? → SpO2 + auscultation
- CV workup (ECG → rhythm+ rate, pulse, BP, prolonget QT? carotid murmors?)
- Neurowork-up: diffuse vs. focal? (see below) ⇒ assymetries (face, pupillary)
⇒ aphasia? ⇒ pronator drift
⇒ Babinski might be + (normal)
- EEG
- Background: asyymetry + slowing
- Interictal phase → Spikes, sharp waves, spike-wave-complex 📷
- Sleep deprivation provocation
- MRI → structural abnormality?
- Lab (gluc, tox, electrolytes, CBC)
- fever/infection? → Lumbar puncture
- others
A group of paroxysmal, reversible, neurological symptoms that typically precede an attack of migraine or seizure and vary in intensity and duration.
⇒ Aura can manifest with a multitude of symptoms: e.g., visual (e.g., flashing lights, scotoma), motor (e.g., paresis), somatosensory (e.g., paresthesia), vestibular (e.g., dizziness), vocal (e.g., aphasia), or olfactory (e.g., hyperosmia) symptoms.
NON-EPILEPTIC SPELLS:
- Febrile seizures !!🤒
- tremor
- DDx: loss of conciousness ⇒ vasovagal, arrhythmias, autonomic dysfunction
- Aural: migraine
- motor: TIA
- psychological disorders
F
Focal (unilateral → may spread) | Generalized (bilat) | |
Origin | Single hemisphere | Both hemisphere |
Awareness | aware or impaired | Ø |
Symptoms | Motor (↑/↓)
Non-motor (sensory, cognitive, autonomic) | Motor (Tonic clonic or other motor)
Non-motor |
- clonic: sustain rhythmic jerking (automatism movement - i.e. lip smacking, automated movements)
- unilat. body
- may spread prox. (”jacksonian march”)
- tonic: ↑tone (sec-min)
- atonic: ↓/Ø muscle tone
- myoclonic - short brief single / series of muscle contraction (jerks)
- hyperkinetic: irregular large amplitude (”chorea-like”)
- automatism: repeating automatic actions
Øtonic-clonic
- Sensory (somatosensory, visual, auditory, olfactory, gustatory, vestibular)
- Cognitive → cortical symp (aphasia, agnosia, memory, hallucination, alexia, etc)
- Emotional (everything imaginable; unapproriate bursts of laughter)
- Autonomic
(cardiac, GI, cutaneous, respiratory, urination, lacrimation, etc)
- Tonic-clonic (”grand mal”) - 1-3min
- Tonic (w/ expiratory sound in beginning)
- Atonic → brief ”drop attack” or unilateral sagging (seconds-min)
- Myoclonic → brief (seconds) jerk
- Epileptic spasms → on awakening sudden brief flexion, extension or mixed proximal + truncal muscles
Øhyperkinetic + Ø automatism
- Typical absence
- abrupt onset + offset of conciousness-loss (5-10(15) sec)
- multiple times a day
- memory impaired (retrograde)
- +/- assoc. features
- +/- minor clonic movement (twitching) of face + eye muscles
- +/- automatisms
- Øpost-ictal phase
- Atypical absence
- Less abrupt onset + offset
- Less loss of conciousness
- ASSOCIATED w/ loss of muscle tone (head, trunk, limb)
- Myoclonic absence
- jerks → shoulder + arms
- with tonic abduction → lifting of arms during seizure
(i.e. starring with variable loss of conc.)
- Generalized epilepsy
- = generalized seizure type
- typical findings: EEG (interictal/inctal)
- FH+ ?
- types: Childhood Absence Epilepse, Juvenile Absence Epilensy, Juvenile Myoclonic Epilepsy, Generalized Tonic-Clonic Seizures Alone
- Focal epilepsy
- = focal seizure type
- typical findings: EEG (interictal)
- structural cause? (→ imaging!!)
- Combined (both)
- general + focal seizure type
- typical EEG findings for both
- Cause: Syndrome (Dravet + Lennox)
WEST SYNDROME (starts after 3-12m) - general poor prognosis, Tx: vigabatrin/benzos
- Spasm
- ↓Development
- EEG: Hypsarrytmia (severe chaotic brain activity) 📷
- ≥2 seizures (in <24h)
- 1 unprovoked + 1 of the following:
- EEG abnormalities (inter-ictal: epileptic form)
- Symptomatic secondary cause (tumor, prior CNS infection)
- Neuro-exam abnormalities
- seizure during sleep
- FH+
avoid triggers
- sleep
- avoid drugs+alcohol
- ↓stress
- others
caution in dangerous situation
- driving
- swimming/bathing
psychological

2 seizure free years
- Ketonic diet
- Vagus n. stimulator (refr. FOCAL)
- Surgery
- resection of focus (pot. curable)
- partial resection of region to prevent spread(palliative)
- esp in MESIAL TEMPORAL LOBE EPILEPSY !!
>5min OR ≥2 discrete seizures w/ incomplete conciousness recovery
#1 Benzos (after 5min)
↓
#2 Anti-epileptics (25min later (after 30-40min))
Non-pharma: clear environment, put something under head, let him shake → after: lat. decubitus
- First seizure?
- trauma?
- dyspnea?
- Drug indication (≥5min, ≥2 seizure)?
- mainly normal children
- all drugs have teratogenic risk
- stick to monotherapy
- add-on: folate
⬇️ LMN lesion
lower motor neuron lesions
- Radicular pain
- Weakness + Sensory loss → in specific territory
- ↓Reflexes at the the level
→provoked by root test: Straight leg raise 📷
⇒ ALL SIGNS PRESENT = COMPLETE LESION
⇒ ONLY RADICULAR PAIN ⇒ PARTIAL LESION
- Degenerative
- Trauma → traction injury
- Disk Herniation (minor trauma)
- Neoplasm: Meningeal spread
- Infection
- Diabetic

SPONDYLOSIS (OA) aka DEGENERATIVE ⇒ narrowed cervical canals
(+/- trauma)
Pain | Sensory loss | Motor weakness | ↓Reflex | |
C5 | Medial scapula | lat. (ant.) shoulder | Deltoid (+Biceps) | (Biceps) |
C6 | shoulder → ant arm → lat. forarm + thumb | thumb + index | Biceps | Biceps |
C7 | Post. arm | dorsal middle finger | triceps | triceps |
C8 | medial arm + finger 5 | finger 4+5 | finger flexors (interoseus) | - |
- Structural cause → MRI / Xray
- Root specific → EMG, ENG (conduction studies)
80% → spontaneous improvement
#1 Conservative Tx:
- Symptomatic Drugs: Anti-inflammatory, analgesics, muscle relaxants
- Immobilization: ↓physical acitvity + cervical collar
↓
spinal cord involv.? refractory?
↓
#2 SURGERY
L4-S1
⇒ post.-LATERAL disc herniation OR degenerative
- PAIN
- back
- sciatic
- Sensory loss: dermatome
- Straight-leg +
- PAIN
- L5 → lat. leg → lat. malleolus
- S1 → pos. leg → heel
- Sensory + Weakness:
- L5: Dorsum (dorsal sensory + dorsiflexor weakn.)
- S1: Plantar (plantar sensory+ plantarflexor)
- Reflex:
- L5: ↓/Ø Achilles refl.
- S1: ↓/Ø Medioplantar refl.


SAME AS CERVICAL
- Structural MRI / Xray
- Where’s the lesion → EMG + ENG
#1 Conservative:
- short immobilization → PHYSIO!
- Symptomatic drugs: NSAIDS, analgesics, muscle relax
↓
Cauda equina syndrome (sphincter dist.)?, foot drop? conservative Tx refractory?
↓
#2Surgery
Preceeding GI / URT infection → molecular mimicri
⇒ Autoimmune-mediated demyelinating of periph nerves + nerve roots
- Bacterial Infection: Campylobacter jejuni, Mycoplasma pneumonia
- Viral Infection: Cytomegalovirus, Epstein-Barr Virus
- LMN signs
- progressive WEAKNESS: Lower limbs → ascends prox. (arms, face, oropharynx, respiratory)
- Ø reflexes (LMN)
- CN involvent
- bulbar
- facial symp.
- paresthesia / sensory → ascending
- autonomic symptoms


- Days - 4w: Progression
- Plateau phase: 2-4w
- recovery phase:
→ mild to severe (tetraplegia)
Nerve conduction:
- absent F-waves (roots)
- disseminated conduction blocks (like the lesions)
- ↓Amplitude
CSF Analysis ⇒ albuminocytologic dissociation

- Progressive weakness legs + arms
- ØReflexes
- abnormal conduction studies
- albuminocytologic dissociation
- Plasmapheresis
- IVIG (0,4g/kg for 5d)
- Supportative care + Symptomatic Tx
SLOW RECOVERY: after 1y → 70% recovered
= UMN lesion (spinal cord syndrome)
below L1 (end of spinal cord = conus medullars)
⇒ continues as cauda equina = bunde from which lumbar + sacral nerve roots arise
COMPRESSION OF CAUDA EQ. ⇒
- UMN signs↓/Ømotor → bilat. legs (Paraparesis/-plegia)
- Øreflexes
- Øsensory → legs, ass, perineum
- “saddle-anesthesia” 📷 (medial buttocks + perianal)
- acute:
- sudden onset bilat. pain in specif. areas
- Straight leg (lasegue) +
- chronic:
- continous low back pain
- “spinal claudication”
- autonomic: bladder, bowel, sexual
Sensory loss restricted to medial buttocks and perianal area
“Spinal (neurogenic) claudication: Low back, buttock, and leg pain and/or paresthesias produced by walking or standing; relieved by sitting and resting for many minutes; patient position: bent forward on walking (spinal canal gets maximum opening)”
- ACUTE CAUSES FOR COMPRESSION
- disc herniation (central!)
- vertebral collapse (mets)
- Trauma
- Spinal hematoma
- CHRONIC CAUSES FOR COMPRESSION
- Spinal stenosis (DEGENERATIVE)
- Neoplasm:
- Pelvic tumors (infiltration)
- vertebral mets
- Meningeal carcinomatosis
- Abscess
- Congential malformation
- Compression
- Trauma → traction
- idiopathic
- COMPLETE VS. PARTIAL (motor, sensory, reflex)
- Complete:
- complete arm flaccid paralysis
- Øreflexes
- Øsensory
- Partial
- Autonomic disurbances (trophic skin, Horner)
Superior | Inferior | |
Weakness | scapula, deltoid, biceps | wrist + hand |
Absent Reflex | biceps | finger flexor |
Sensory loss | lat. upper limb | medial forarm + hand |
- EMG + ENG
- Imaging: MRI, CT
- Nerve avulsion ? 📷→ Surgery
- Symptomatic Tx
- Physio
- Orthesis
- Analgesics (if metastatic)
- Steroids (if idiopathic)
- Lumbar plexopathy
- ext. Compression / Entrapment #1
- Superficial locations within extremities (e.g., ulnar nerve at elbow, median nerve at wrist, peroneal nerve at fibular head)
- Proximity to areas used for medical interventions (e.g., radial nerves at IV injection sites)
- Diabetes
- Tumor infiltration
- nerve ischemia
- vasculitis

{kind=link}
{kind=link}
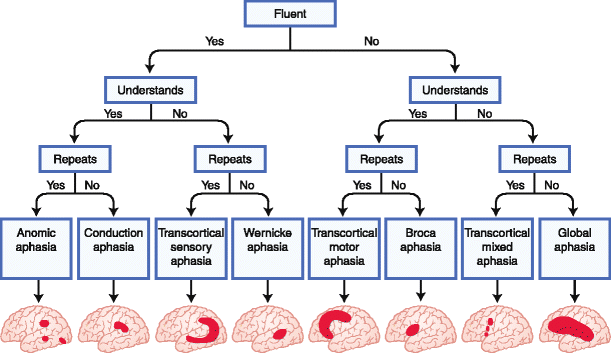{kind=link}
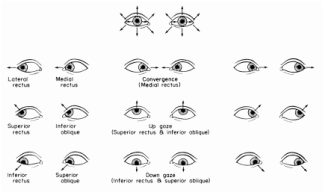{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
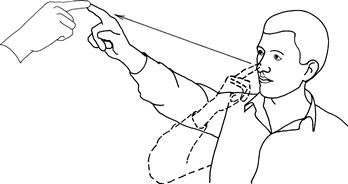{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
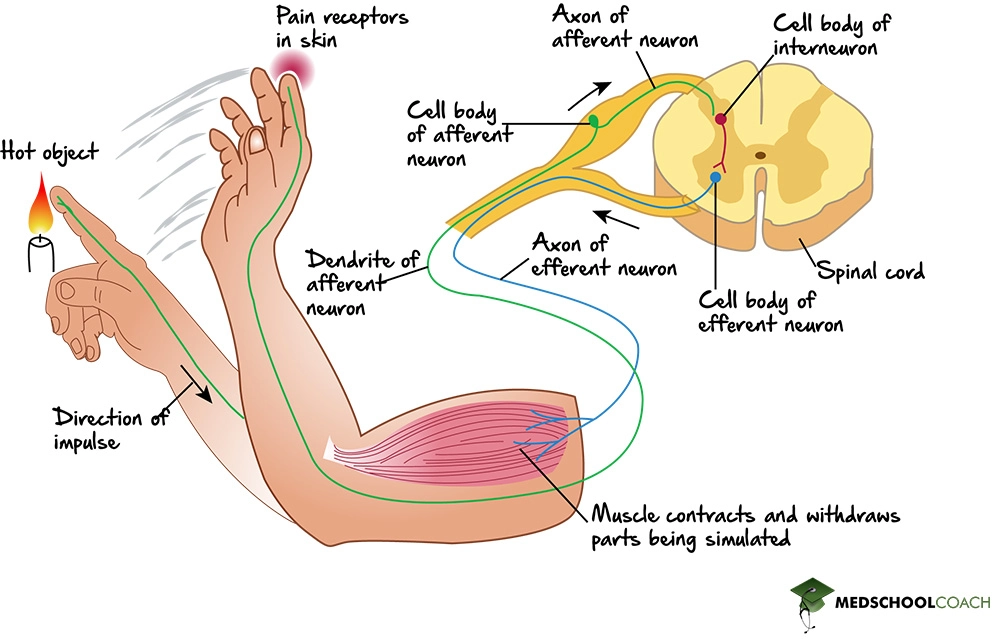{kind=link}
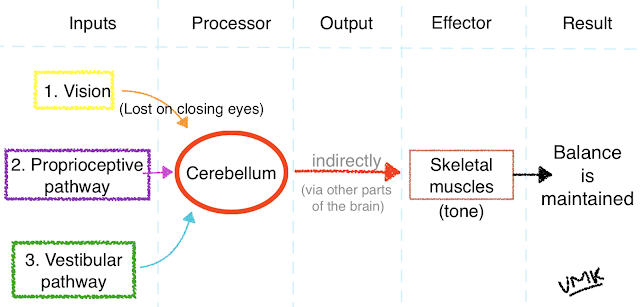{kind=link}
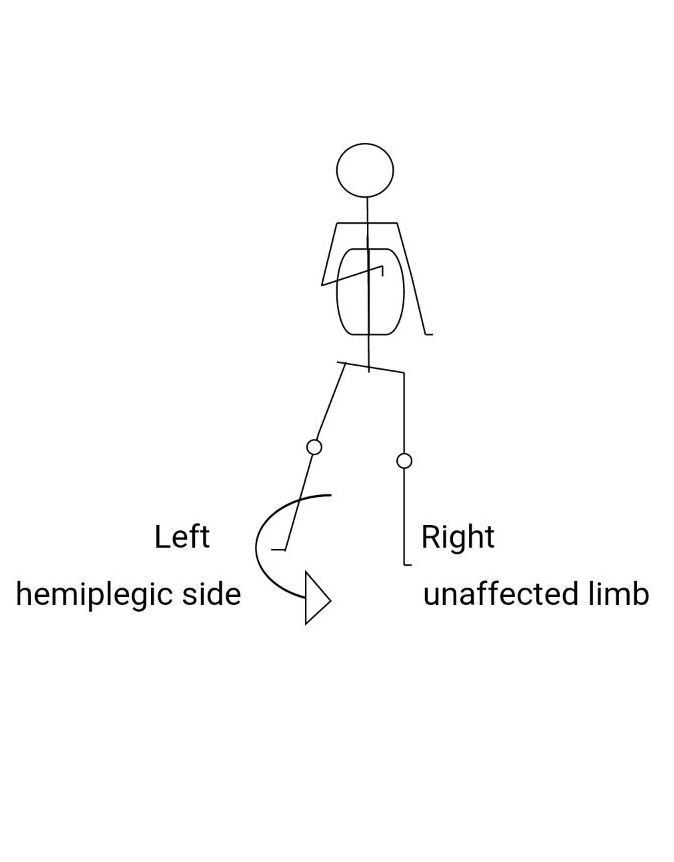{kind=link}
{kind=link}
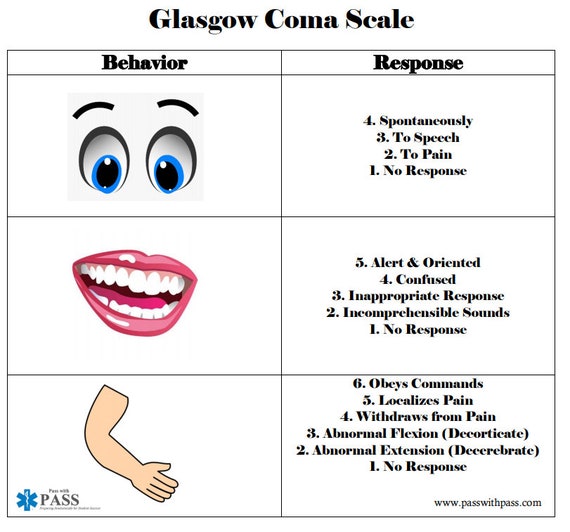{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
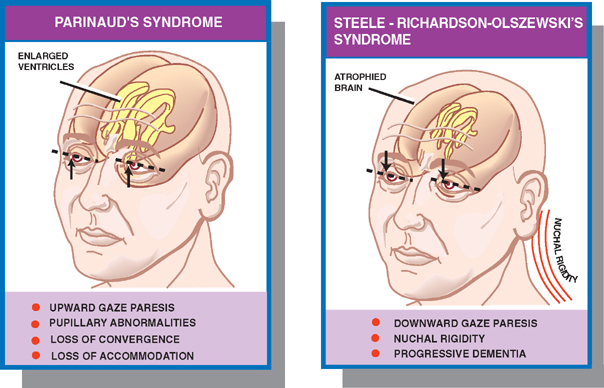{kind=link}
{kind=link}
{kind=link}
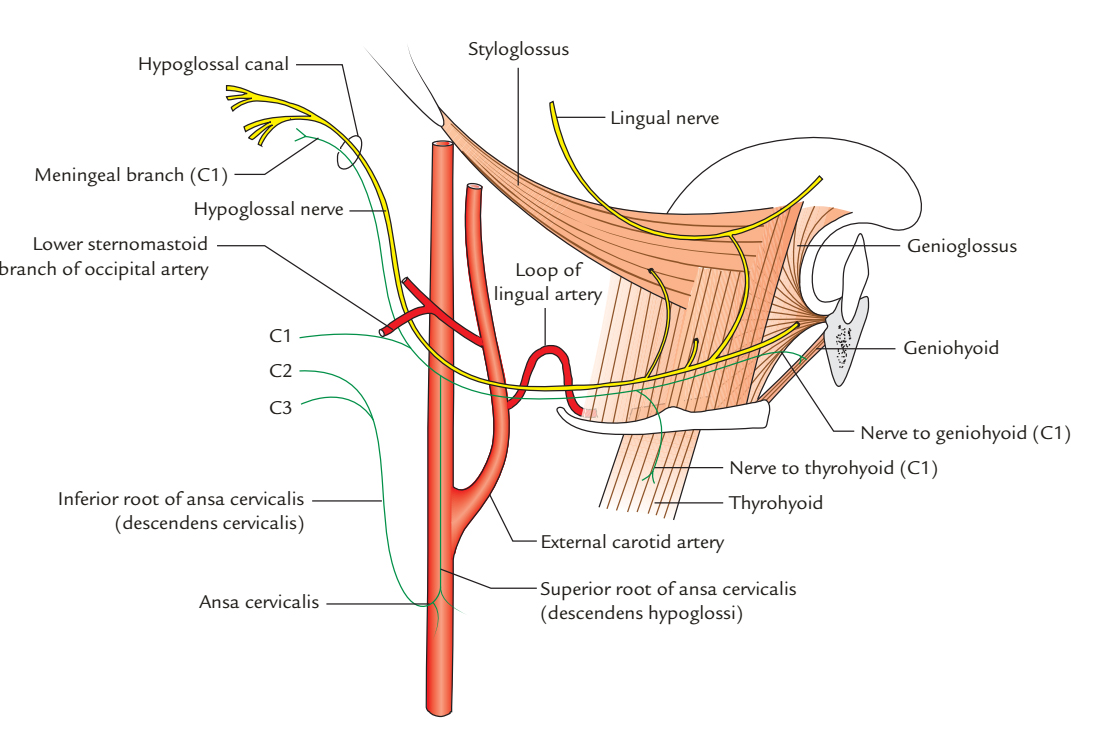{kind=link}
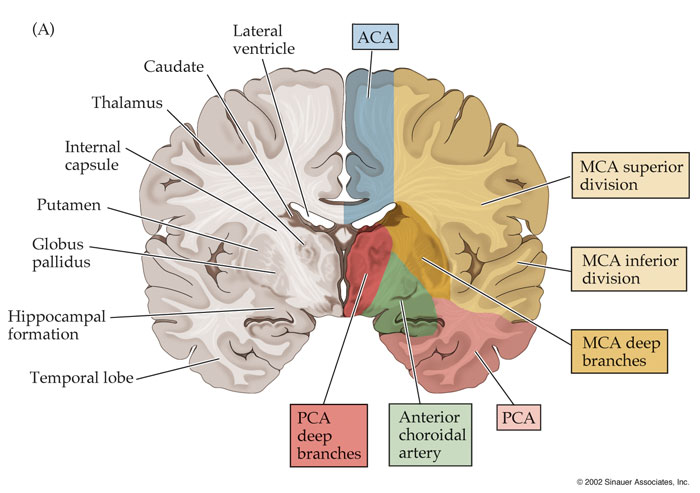{kind=link}
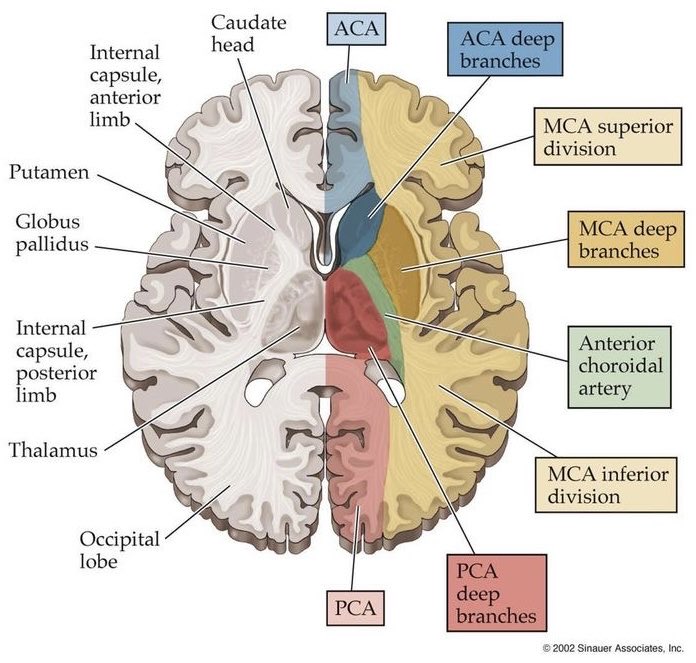{kind=link}
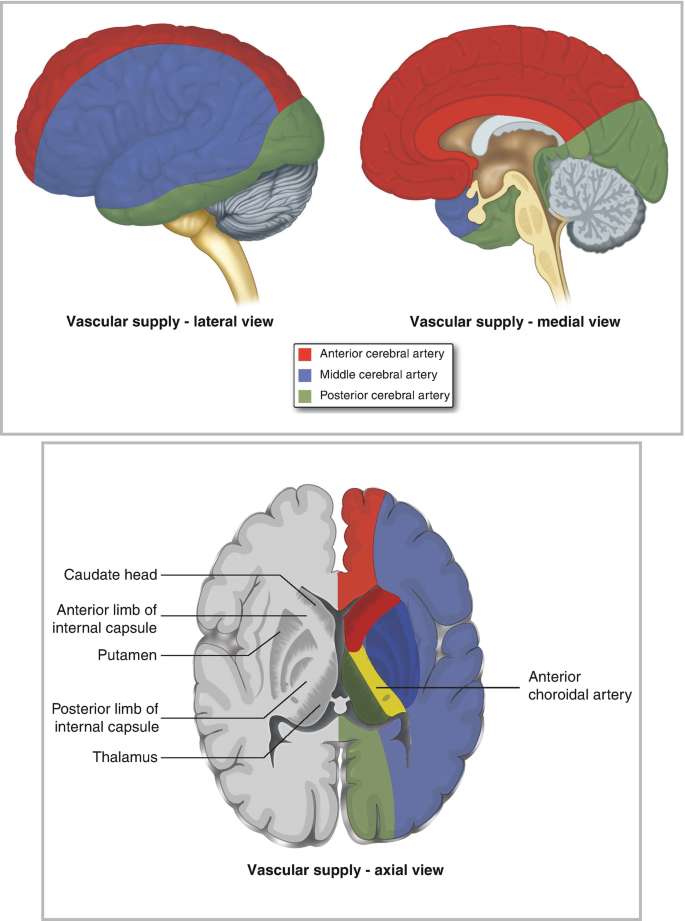{kind=link}
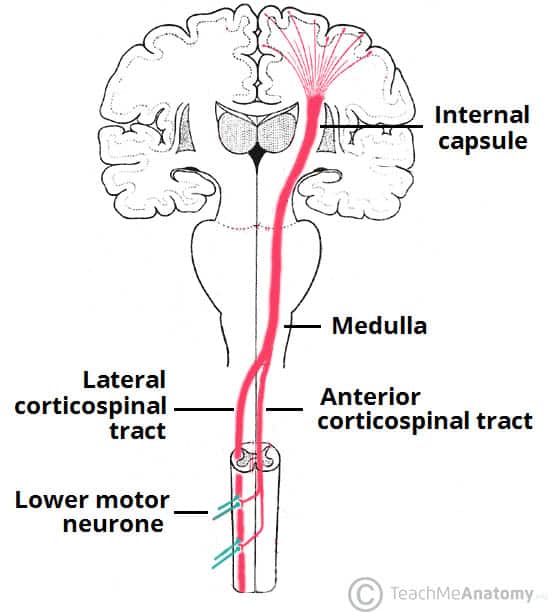{kind=link}
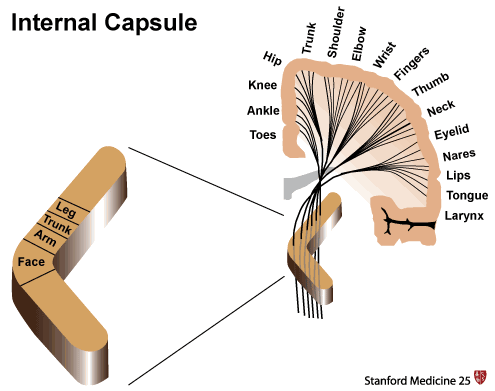{kind=link}
{kind=link}
{kind=link}
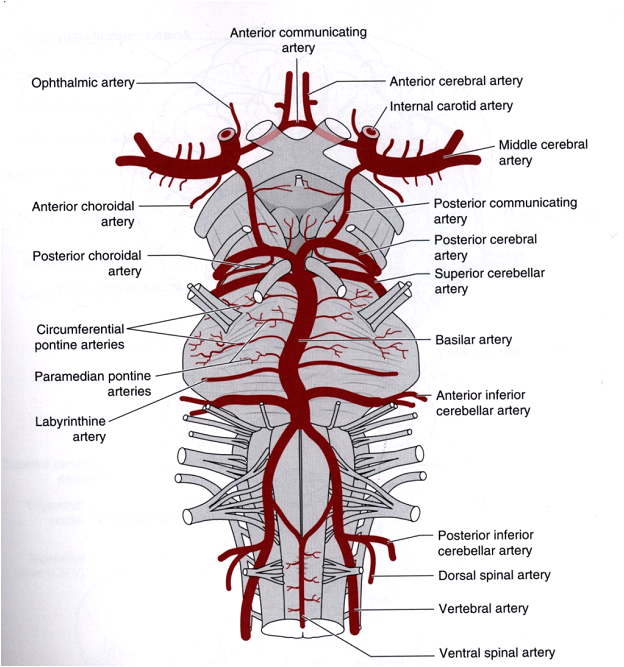{kind=link}
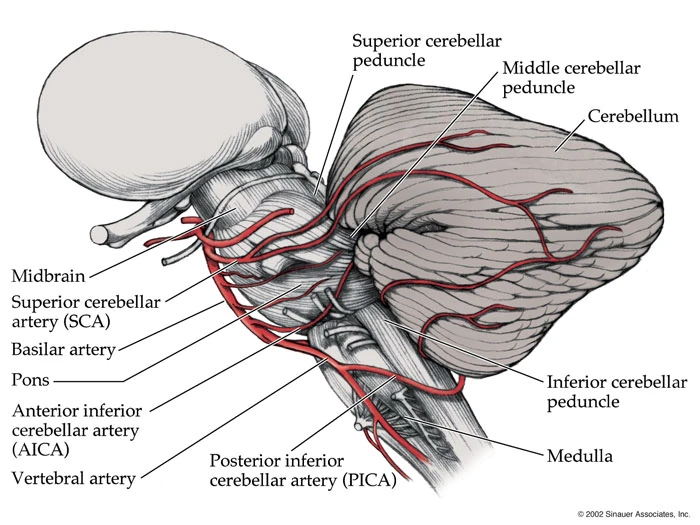{kind=link}
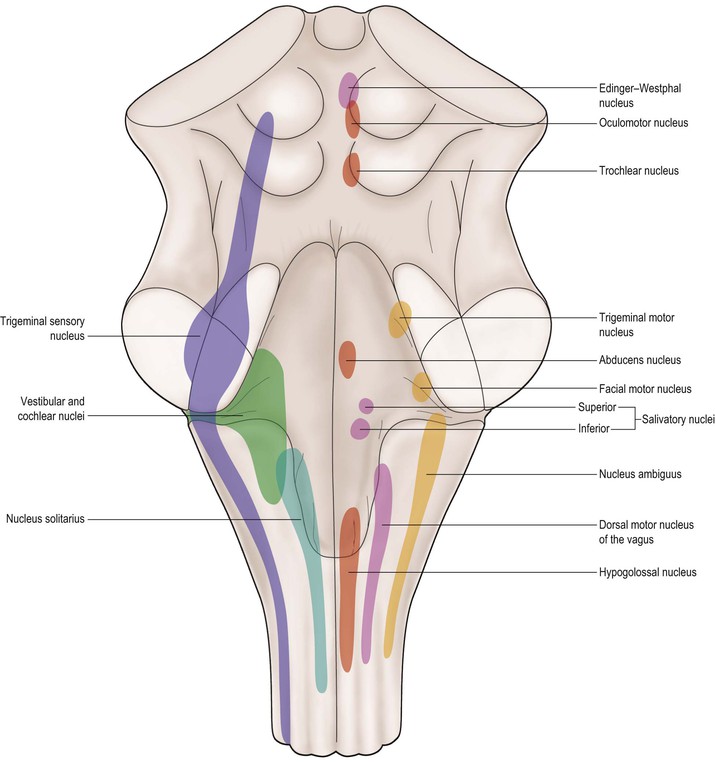{kind=link}
{kind=link}
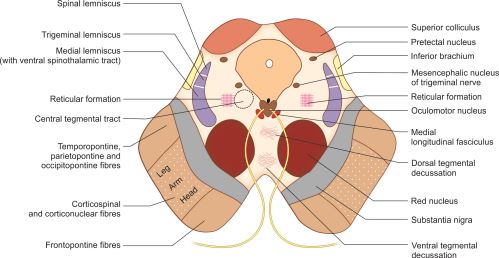{kind=link}
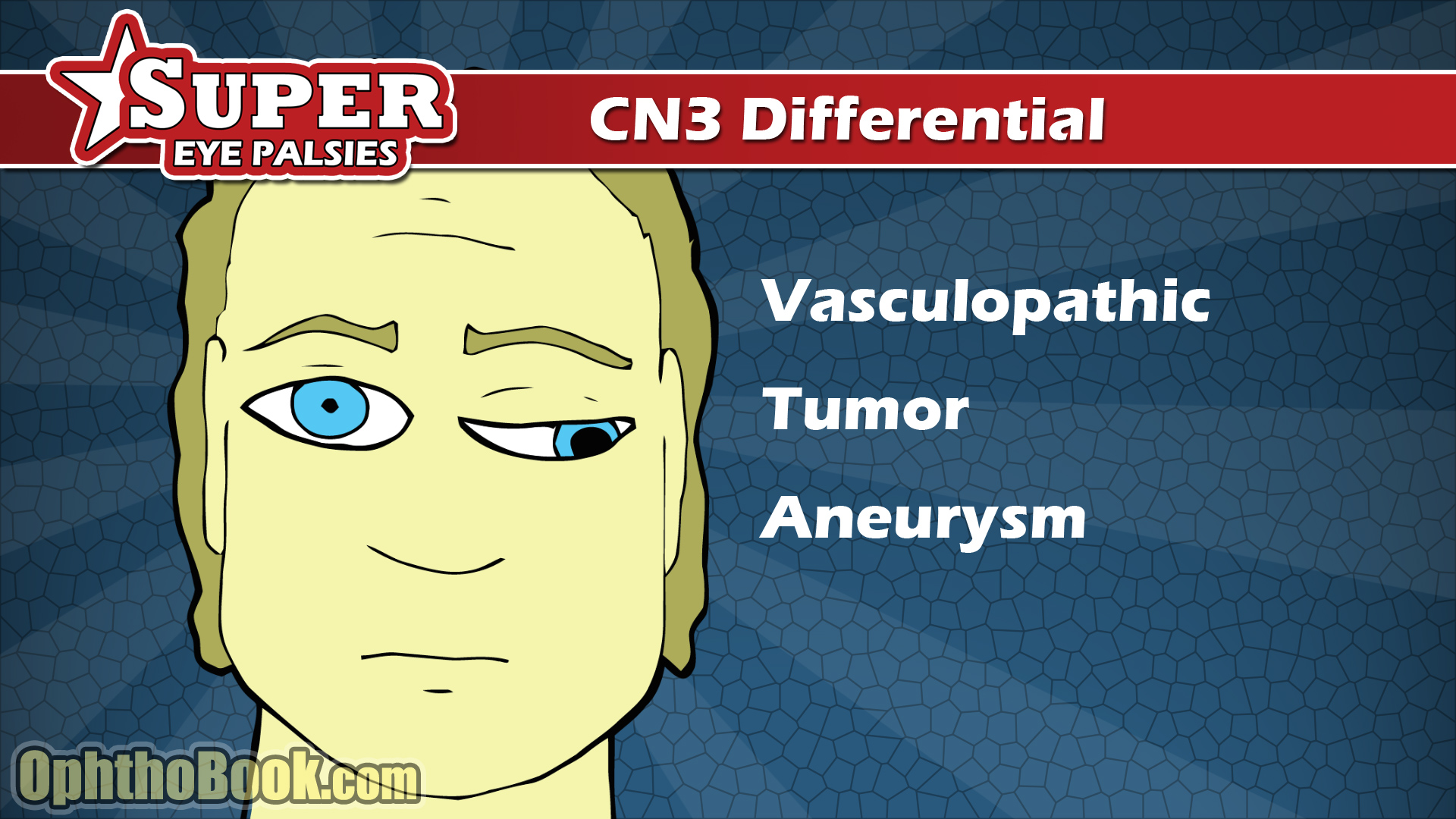{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
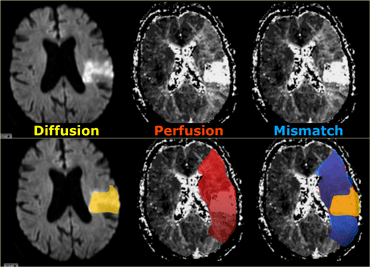{kind=link}
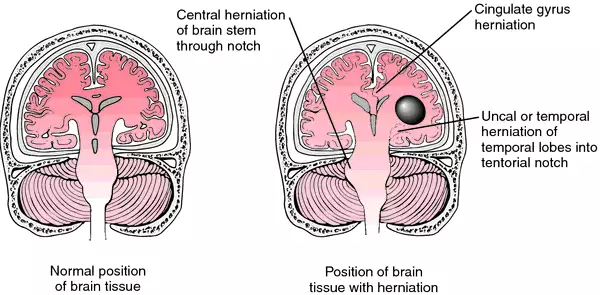{kind=link}
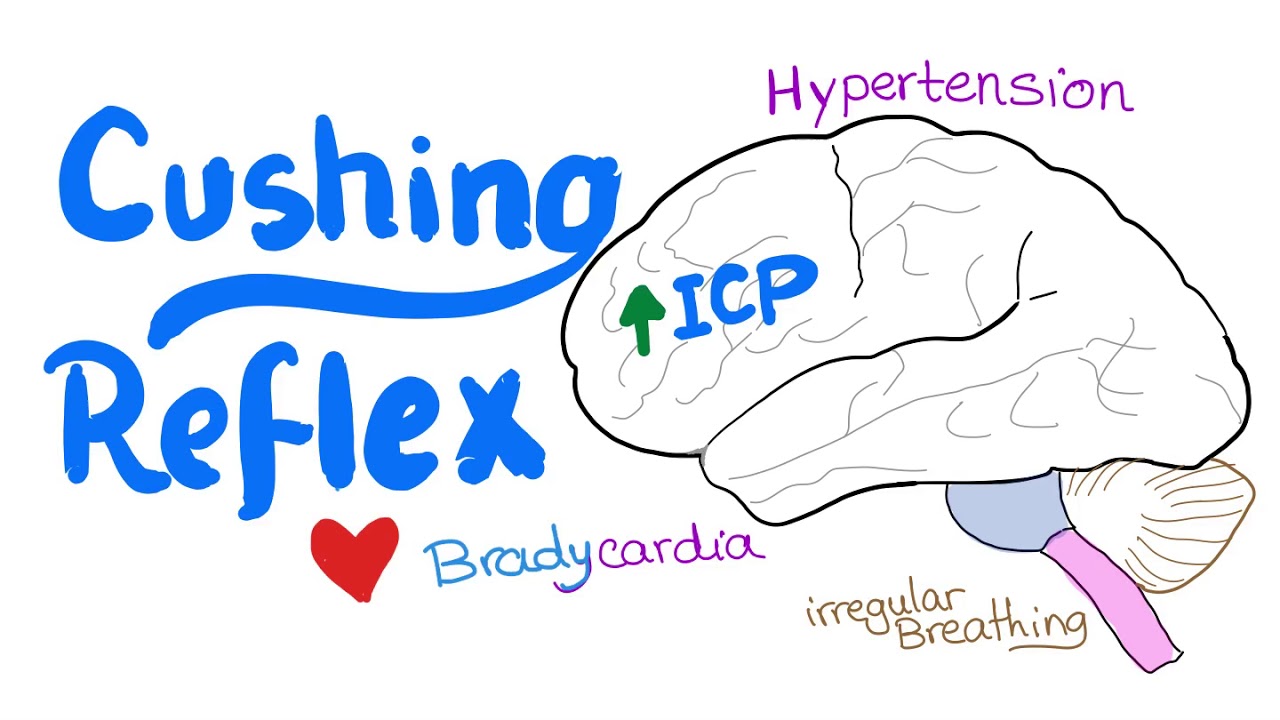{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
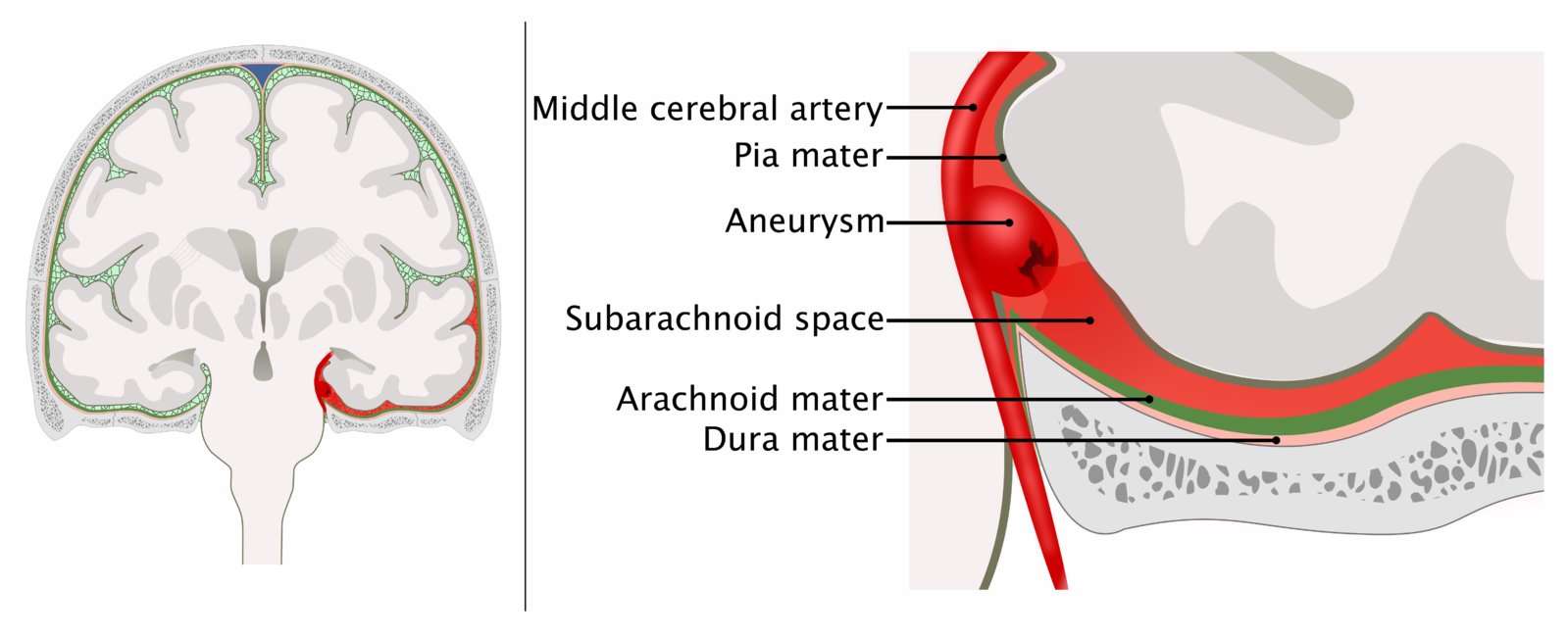{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
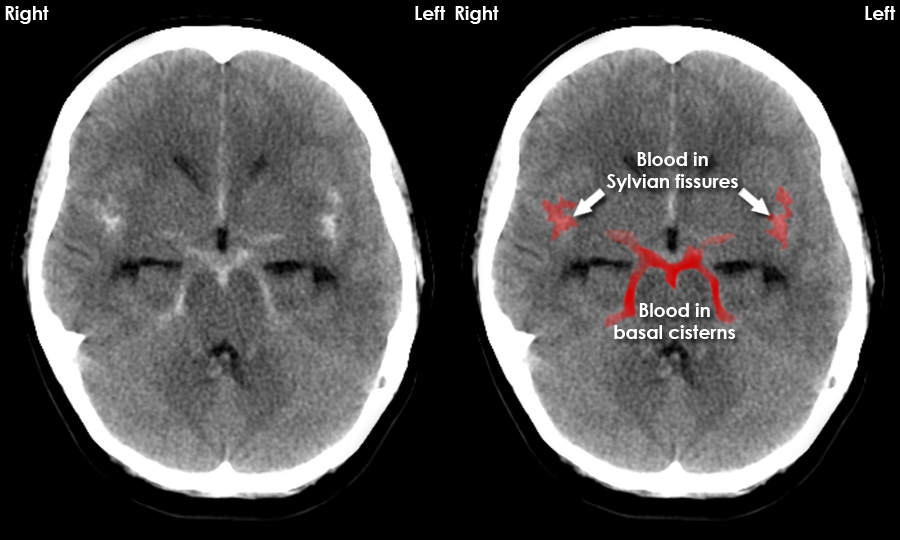{kind=link}
{kind=link}
{kind=link}
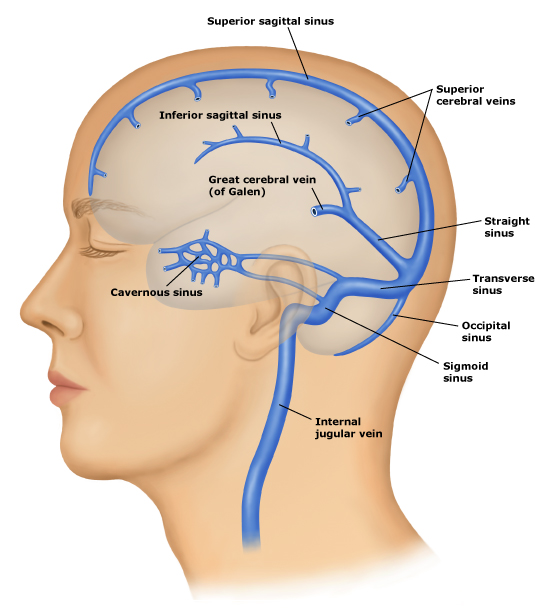{kind=link}
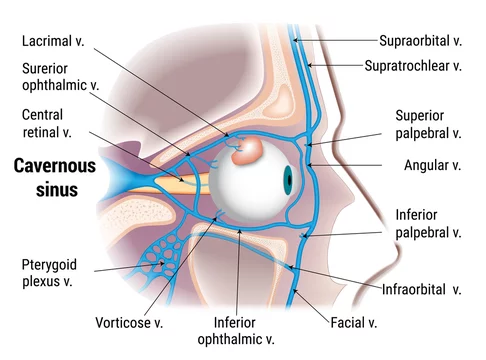{kind=link}
{kind=link}
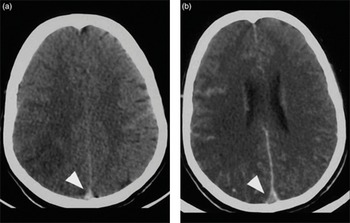{kind=link}
{kind=link}
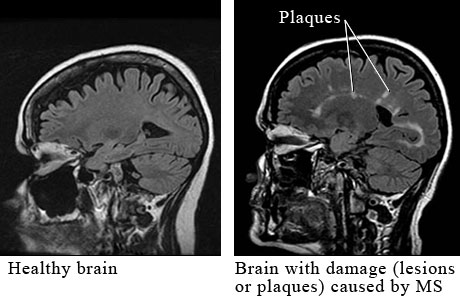{kind=link}
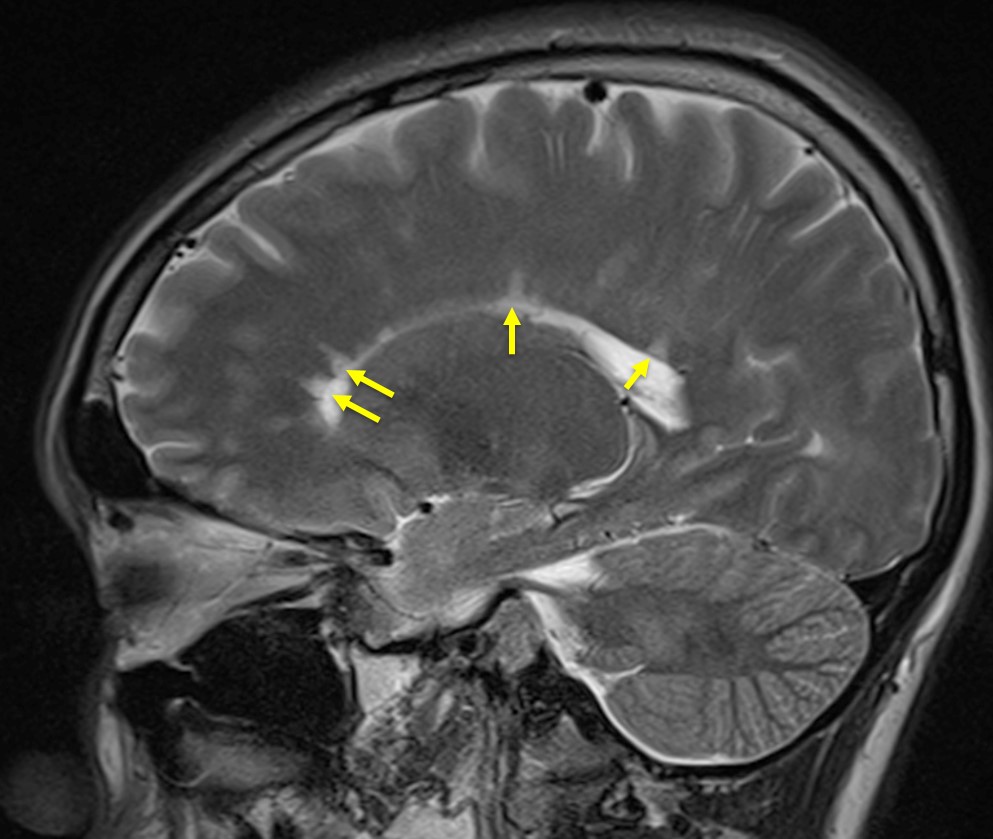{kind=link}
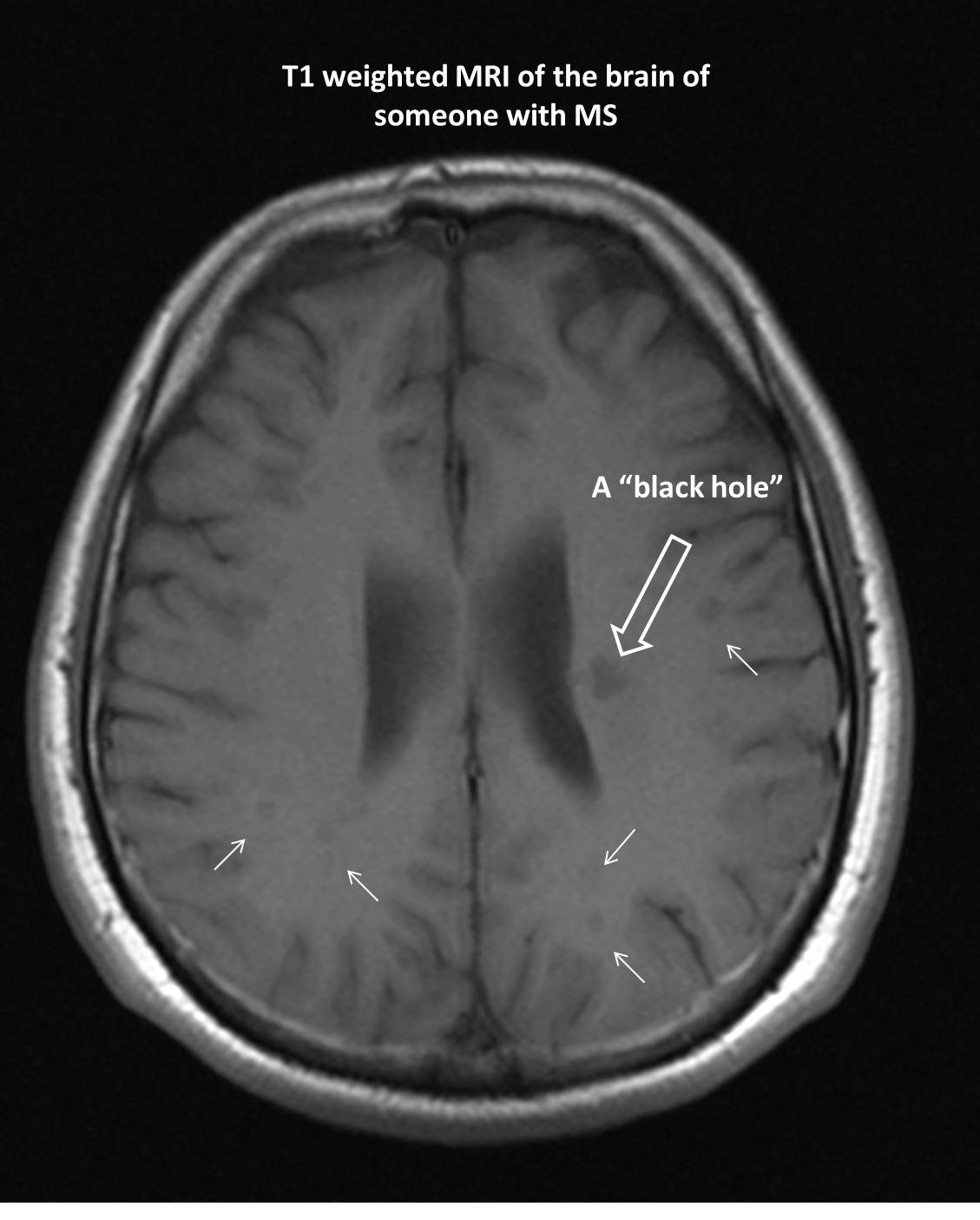{kind=link}
{kind=link}
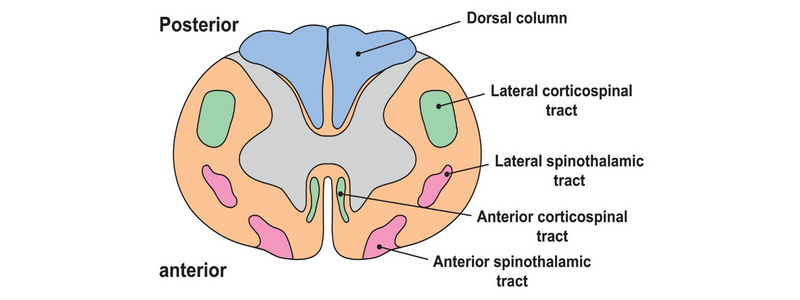{kind=link}
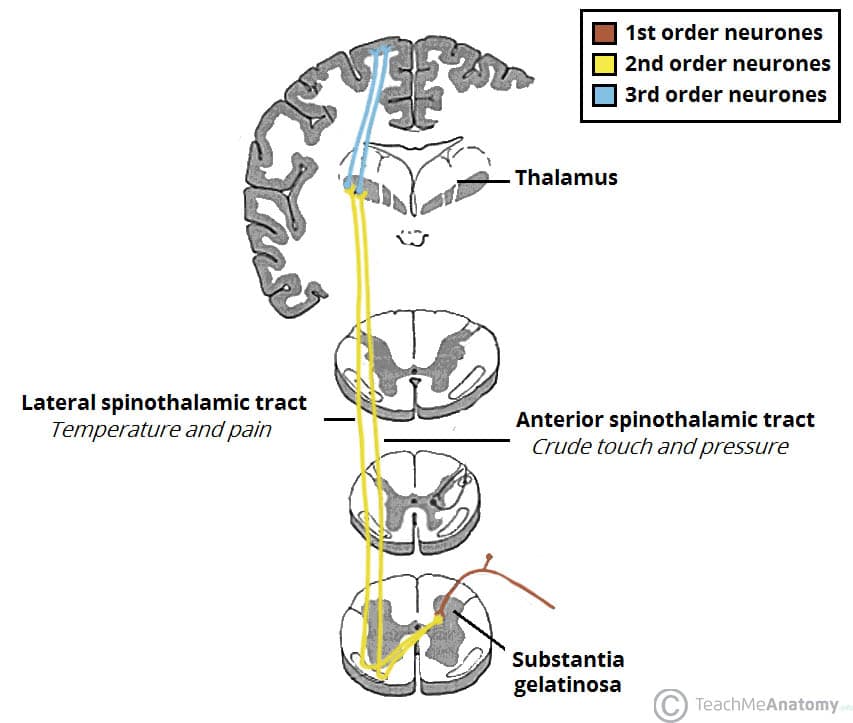{kind=link}
{kind=link}
{kind=link}
{kind=link}
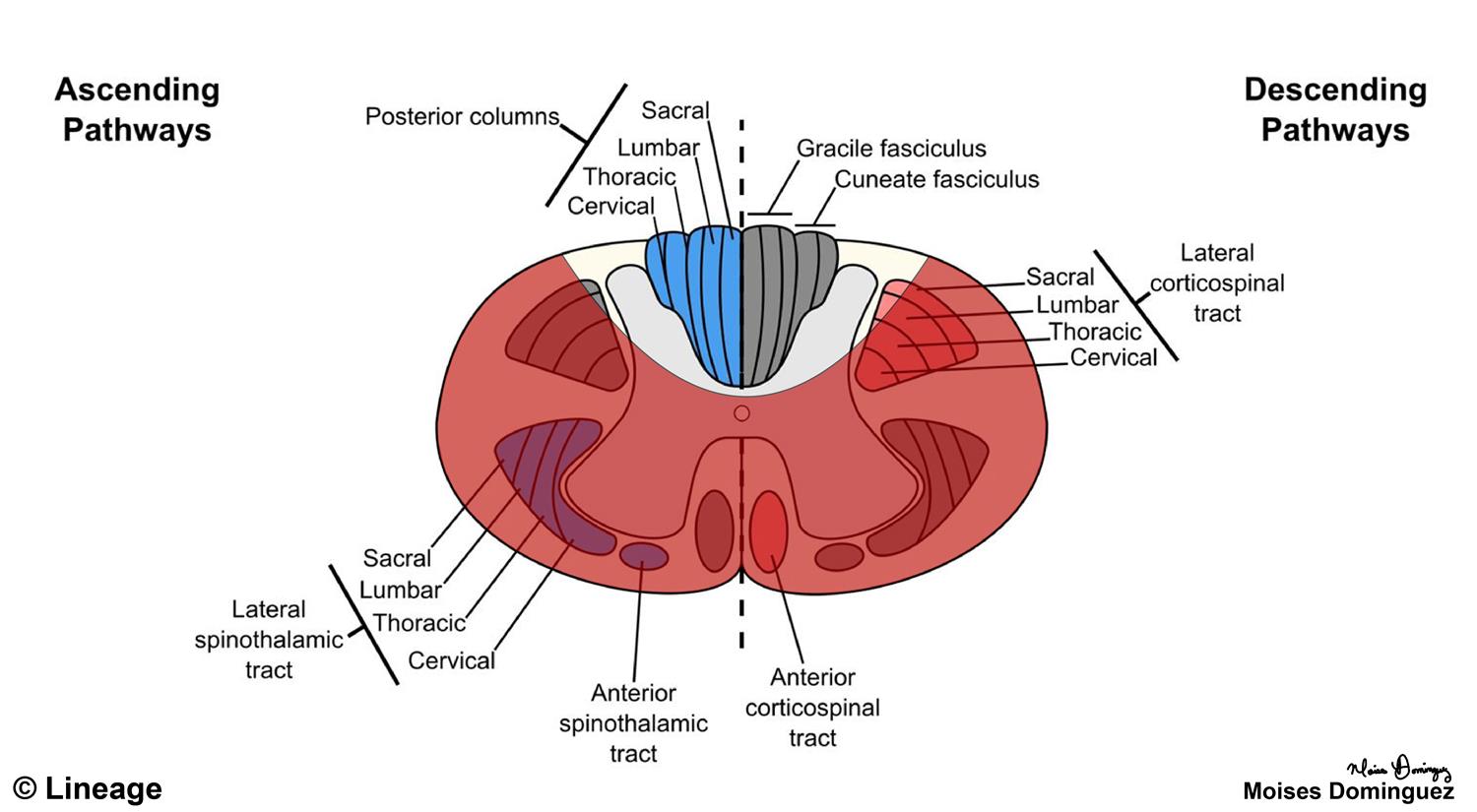{kind=link}
{kind=link}
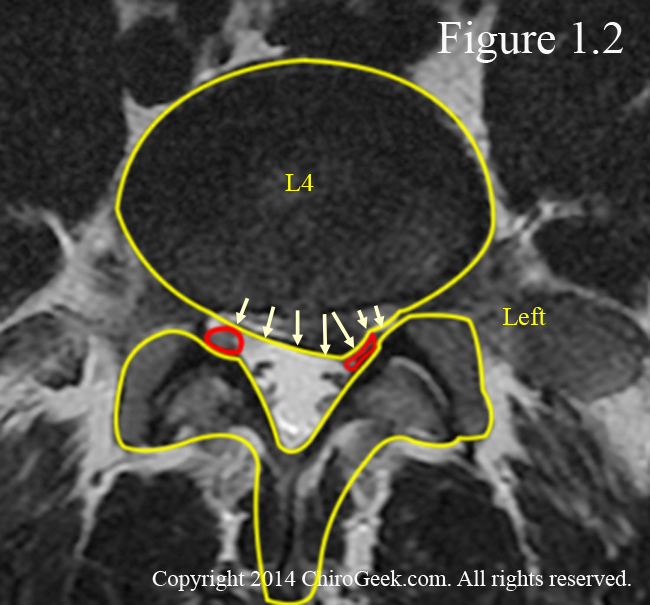{kind=link}
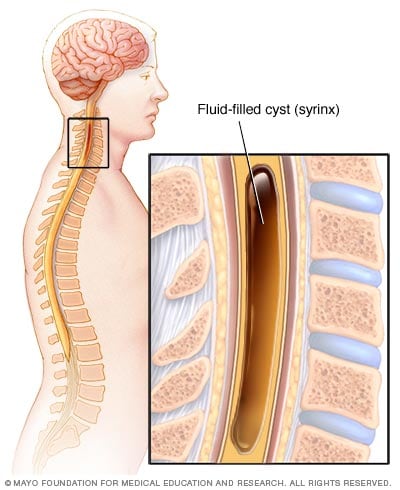{kind=link}
{kind=link}
{kind=link}
{kind=link}
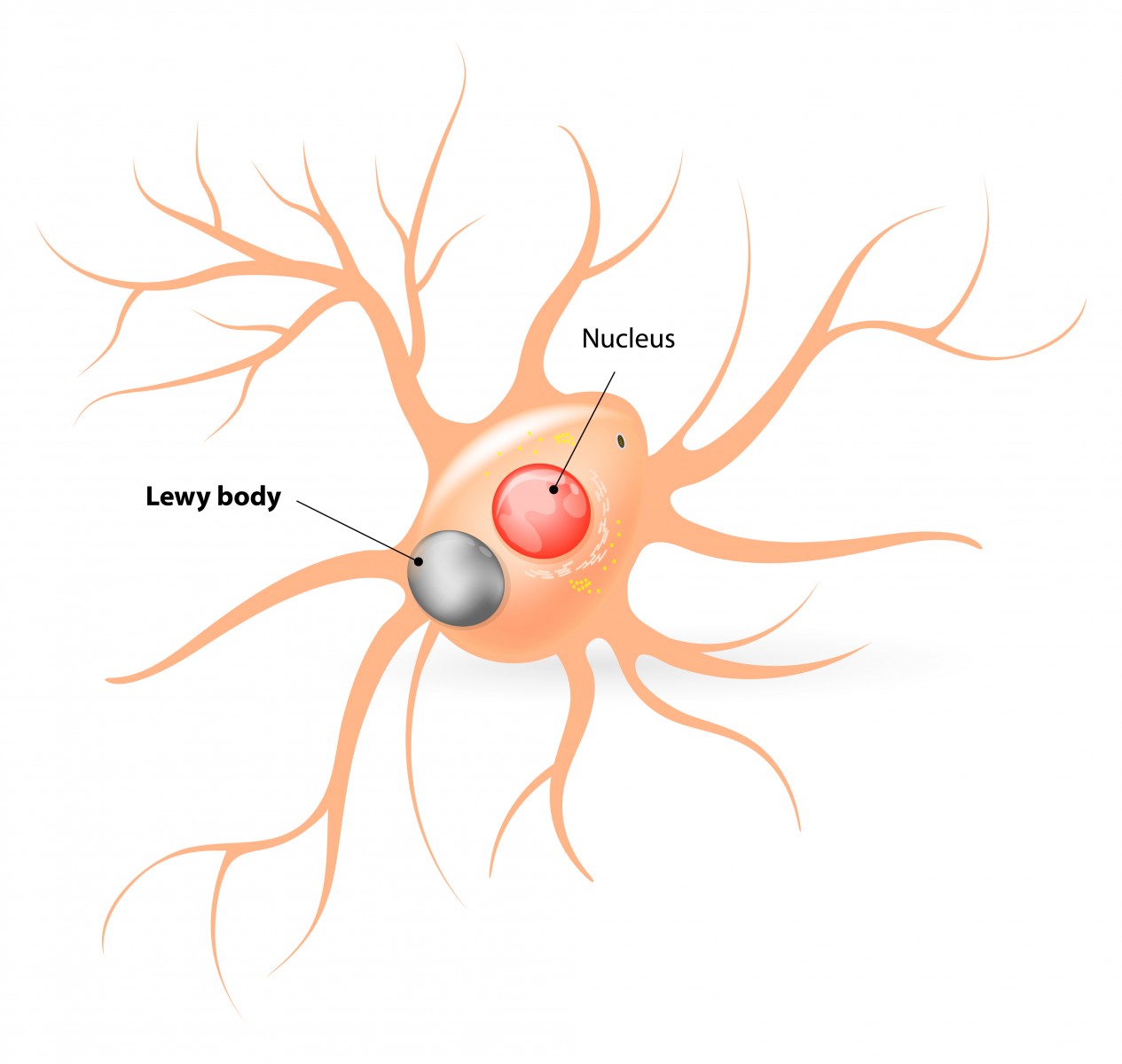{kind=link}
{kind=link}
{kind=link}
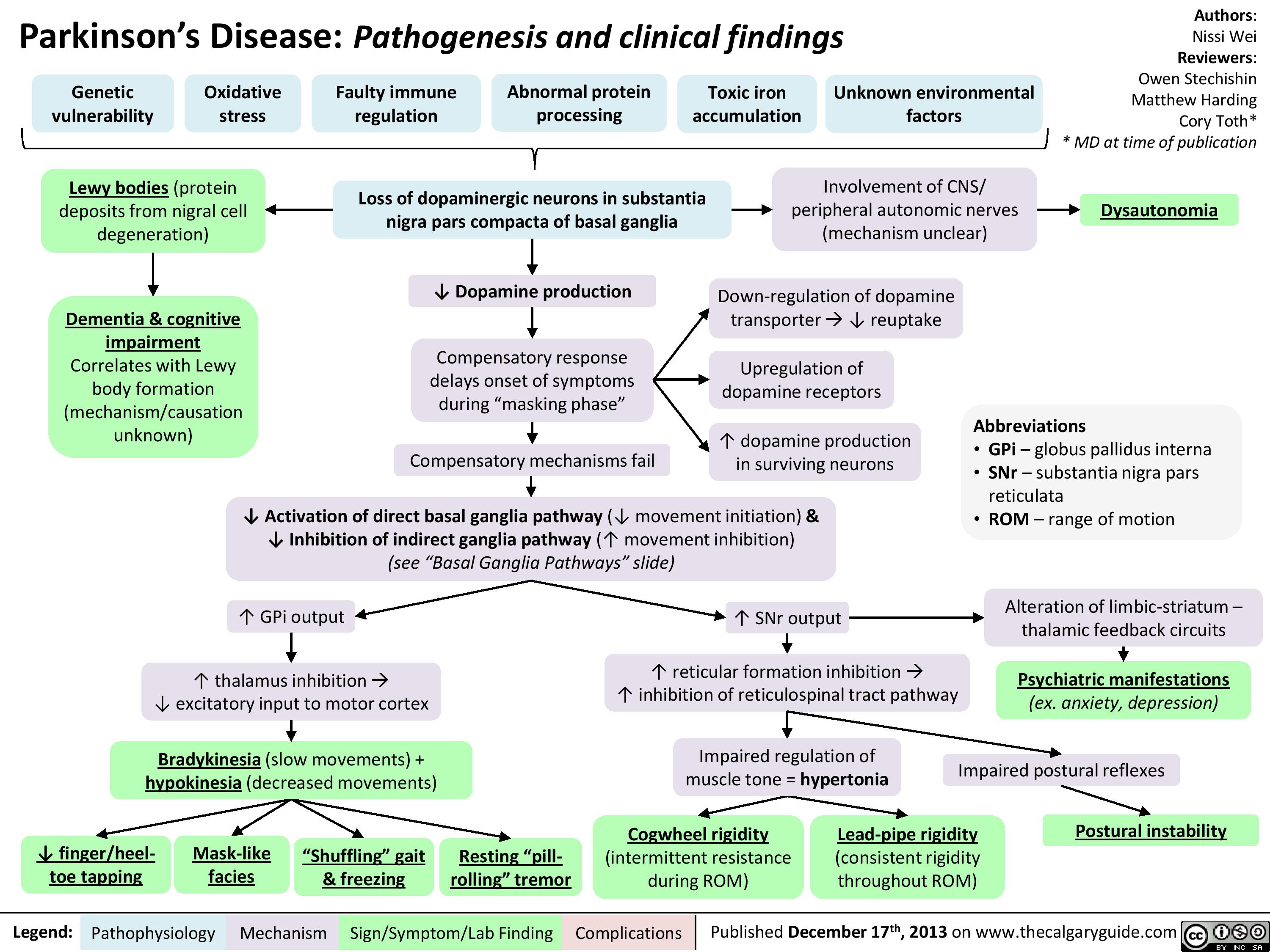{kind=link}
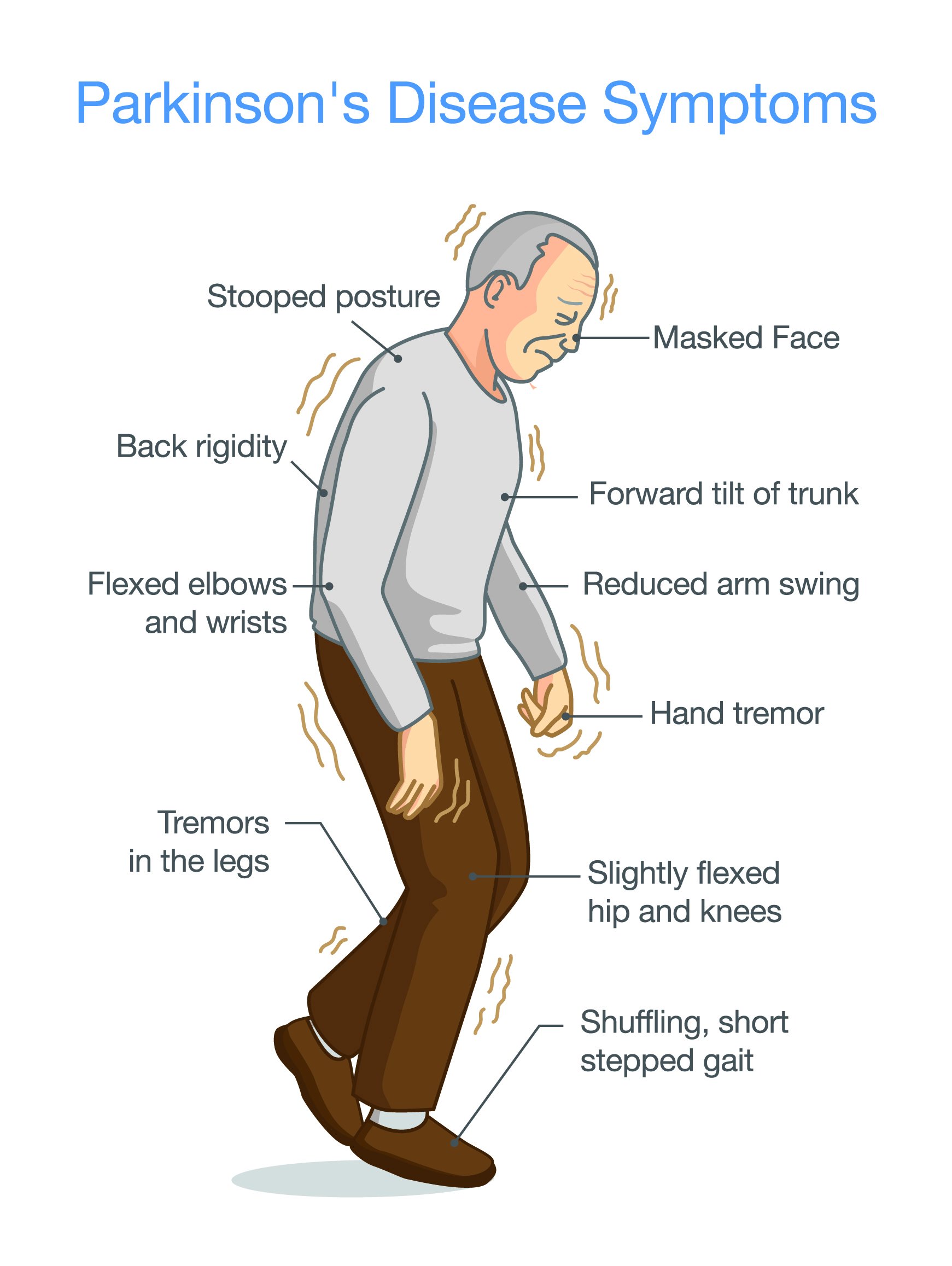{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
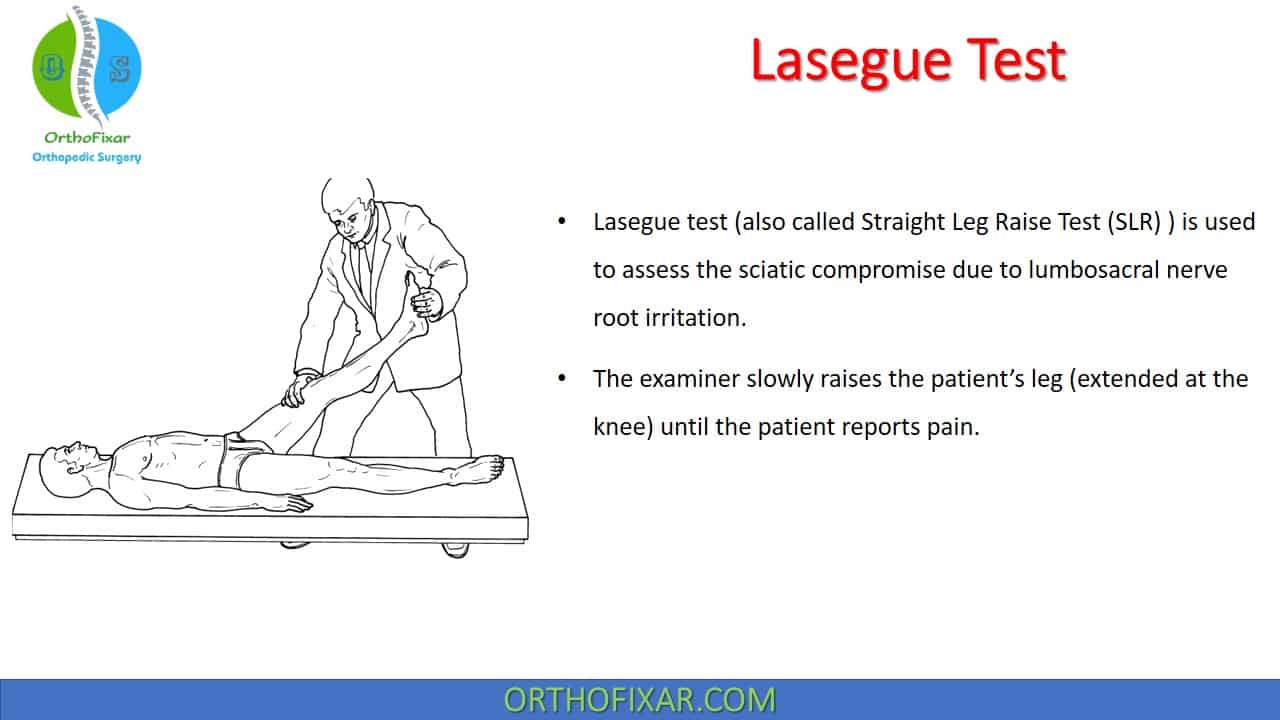{kind=link}
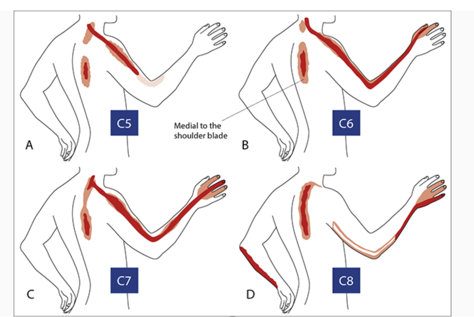{kind=link}
{kind=link}
{kind=link}
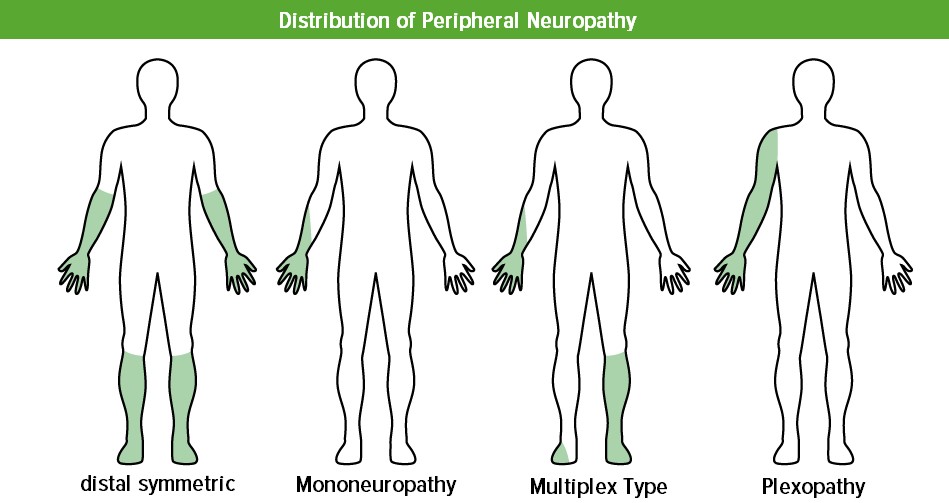{kind=link}
{kind=link}
{kind=link}
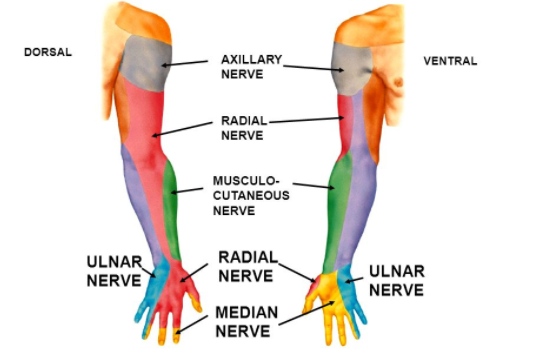{kind=link}
ENG (conduction studies)→ ↓conduction velocity at wrist

SYMPTOMATIC
- mild → splint + analgesics/anti-inflammatory
- severe → surgical decompression
{kind=link}
- Elbow entrapment (fracture, arthritis)
- Wrist entrapment (ulnar tunnel)
- ENG
- US: elbow
mild → symptomatic: immbolization + NSAIDS
severe → Surgery: nerve transposition
- Sensory loss: foot + lat. leg
- Weakness: all foot + ankle + knee flexion
- ØAchilles reflex
- Distal + symmetric
- sensory loss/paresthesia: “Stocking and gloves”
- motor weakness (foot drop, steppage)
- ↓/Ø Reflexes
→lower limbs > upper limbs (more affected + earlier)
- Alcoholic polyneuropathy = axonal + motor neuropathy
- Diabetic polyneuropathy = demyelinating, axonal + motor
- main form: sensory / sensory-motor
- others
- Uremic
- Amyloid
- Paraneoplastic
- EMG → nerve vs. muscle
- ENG → Axonal, demyelinating
- Complementary
- CSF analysis
- Nerve biopsy
- Biologic/immunologic/infectious/toxic laboratory tests for etiology
Ab against Ach-R → ↓ AchR stimulation → ↓action potentials → weakness
(assoc. with autoimmune disorders)


upward gaze:ptosis increased upon sustained upward gaze over time EMG: Decrement 📷
{kind=link}

Lambert Eaton Myasthenic Syndrome (LEMS)
→ weakness improves after exercise
→ assoc. with SCLC / other autoimmune disorders
to exclude SCLC:

Dystrophine gene mutation → X-linked recessive (males>femals) or sporadic
⇒ loss of functional dystrophine proteins 📷 → loss of cell membrane stabilization (sarcolemma) ⇒ damaged cells → creatine kinase escapes cells / Ca2+ enter ⇒ cell death
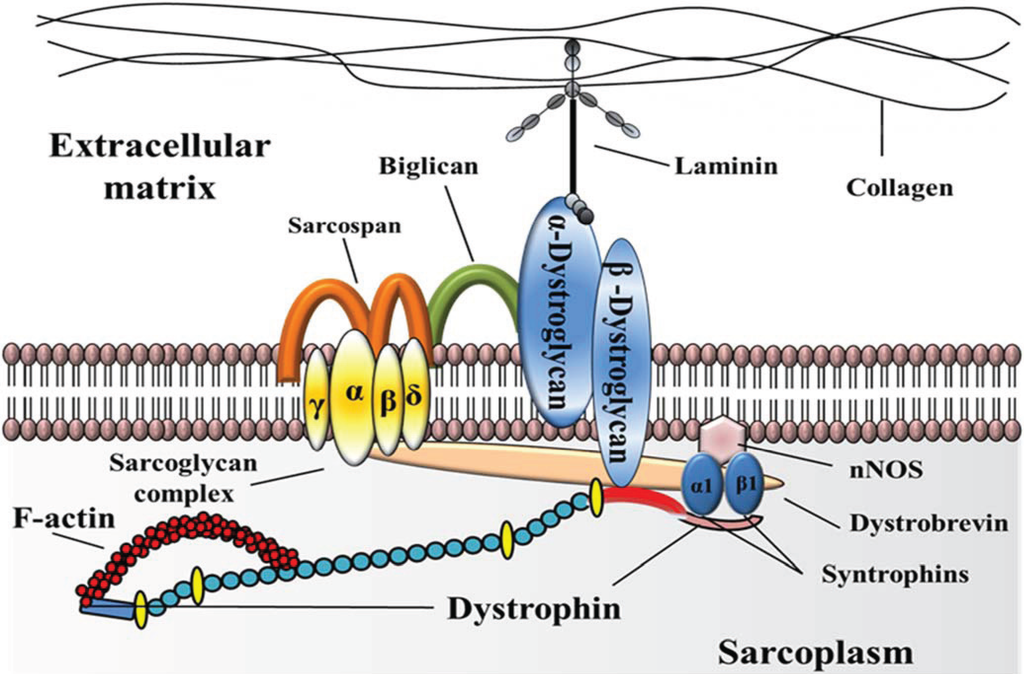{kind=link}
short term → muscle regeneration; long term: muscle atrophy (weakness)
⇒ Douche (Ødystrophin) → more severe, starts at age 3-5 (cant walk with 8-10y)
⇒ Becker (miss-shaped dystrophin) → milder, starts at age 7 (cant walk with 20-30y)
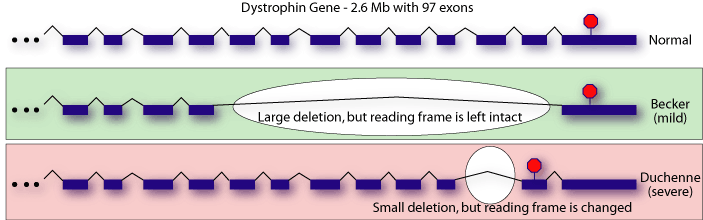{kind=link}
- Prox. muscle weakness (+paraspinal) ⇒ SYMMETRIC
HEART → cardiomyopathy, arrhythmias (dystrophin in heart muscles)
LUNG (diaphragm) → respiratory failure
- Normal nerve exams! ⇒ normal ENG + ØLMN signs
- EMG → ↓Amplitude+Location & Polyphasic
- Lab → ↑CK + ↑LDH
- Muscle biopsy
- Genetic mutation testing (Dytrophin)


- Steroids (oral) ⇒ slow degeneration
- physical therapy (↑ quality of life)
- genetic counseling
→ oxandrolone

Mutation of proteins that complex with dystrophin → expressed in:
Abnormal protein: myotonic dystrophy-protein-kinase
→ muscles
→ brain
→ heart
⇒ AD transmission

- Muscle dystrophy
- DISTAL!! → hand + foot drop initially
- spread upwards like in myasthenia gravis: facial + neck muscles
- Ptosis
- Long face
- Mournful expression
- Neck muscles deficit
- Mouth slack and tented
- Dysphagia
- Phonation troubles
- Masseter and temporalis atrophy
- Myotonia (delayed relaxation after contraction)
- sustained contraction → involuntary contraction → fades slowly
- percussion thenar eminence
- Systemic signs
Facial and neck muscles involvement leads to:
- EMG ⇒ “dive bomber” sound
repetitive bursts at needle insertion "dive bomber" sound at loudspeaker
- DNA analysis
- muscle biopsy
Symptomatic
- Myotonia → procainamide
- Supportative: ankle-foot orthesis
- CONTRAINDICATION: BB, Digox, TCA, Sedative!
- Facio-scapulo humeral
- girdle
- distal muscular dystrophy
- Ocular muscular dystrophy
mutation Ca-channel protein gene → ↓K (fluctuation) ⇒ relapsing flaccid paralysis
LOWER LIMB + HEAD MUSCLE PARALYSIS
- onset AT NIGHT → for hours
- after prev. exercise/carbohydrate rich meal
- Lab
- ↓K
- ↑CK during attack
- Provocation test → oral + insulin
Kalinor
🍼 Pediatric pathologies
“SYNDROME”-Appearance
ears, nose, jaw, lower hair border
- Abnormal earlobes: low amount of helixes, absence of earlobes, elongated upper part (rabbit's ear), low set ears
- Wide nose bridge: hypertelorism
- Prognatism
- Low hair border
{kind=link}
evaluates clinical-status of the newborn ⇒ standardization
(score = points; max 10 points)
- Appearance → cyanotic?
- Pulse → >100?
- Grimace (pullaway + cry) to stimulation
- Acitivity → movement? flexed?
- Respiration? → strong cry? irregular?
- shape?
- deformity? assymetry?
- Fontanels + Cranial sutures? bulging / widening? (↑ICP)
- Frontal fontanel → ≤ 2,5 x 3 cm (3x3cm)
- Posterior fontanel → not palpable after 2m
- Coronal + saggital suture closed?
- HC - Head circumference (occipitofrontal) ⇒ standardized graph
- 3m → ↑4cm
- 6m → ↑3cm
- 1y → ↑3cm
- Intracranial bruits? ⇒ pathological: assymetric + suppressed by carotid artery suppresion ;
- Intracranial hypertension (↑ICP)?
- Setting sun signs 📷(do repeated head nods)
- Tense + bulging ant. fontanelle OR saggital suture >0,5cm
→ saggital can be open but should be <0,5cm!
eyes down, white band of sclera above
smell → reaction? → tested if suspicion: frontal lobe tumor/trauma/infection
Visual acuity
- BRIGHT LIGHT RESPONSE:
- normal Pieper sign? (shut eye to powerful light)
- uninteressted in bright objects (light)? → Visual / cognitive defect
- >3m: Follow light stimulus?

- BLINDNESS? → Press on eyes with fist? +rolling movement of eye → Blind
- Blind infants exhibit auto stimulatory behavior, characterized by uncontrolled eye movements and disconjugate gaze.
- This behavior includes rolling movements of the eyes.
- Infants with blindness often display these eye movements.
- The eye movements are a distinct feature of blind infants.
⇒ Visual evoked potentials ⇒ type of dysfunction + localization
Visual field
- Double simultaneous stimulation abnormal? → homonimous hemianopsia

Pupillary reflex (present from birth)
- paradox reaction? → Congential syphilis
- red retinal reflex? (normal) 📷
- anisocoria?
- irregular form? → cataract
- Papilla fundoscopy
- Check visual milestones
- 3m - sustain eye contact
- 5m - “pbtdm”
- 7m roll over
- 8m sit w/o support
- 9m crawl
- EYE INSPECTION
- symmetry + width?
- Ptosis? (bilat → embryonic defect)
- Microphthalmus → infection (toxoplasmosis, CMV)
- Horners? → TB (cervical spin → symp. chain irritation)
- Pupil + reflex (see above)
- Suckling (with CN7+12)
- mandible + maxilla in contact?
- low mandible + Øsmaking sound + food falling out? → trigemnial nucleus trauma/↓developed
- assymetric sweating + flushing (Harlequin sign 📷)? → sensitive branch
- Rest like normal CN5-exam
- Facial sensory: light touch test at 3 different spots
- Motor (V3): open + close mouth (masseter asymmetry? pain on palaption? open against resistance)
- jaw reflex
- Corneal reflexes → pat. look away → touch cornea with twisted wooden
- both eyes blink→ normal
- stimulated eye open & contralat. eye closed → CN7
- both open / reduction in corneal sensation → V1
{kind=link}
Cochlear:
- Loud noise → shut eye? (=normal response)
- might cause abduction of arms (first phase Moro’s reflex)
- >4-5m → turn head towards sound
- abnormal langue development? (normal language = normal hearing)
Vestibular:
- Congenital reflexes: (see later)
- Moro’s r.
- Cervical-tonic r.
- tonic labyrinth r.
- protective r.
⇒ connect. vestibular, reticular formation, CN11, ant. horn neurons (cervical+lumbar)
- swallowing + phonation (muffled nasal cry)? → pseudobulbar or bulbar palsy
- Breathing abnormalities? ⇒ caudal medullary syndrome
“The child cannot swallow milk, chokes and coughs, milk pours out through his nose.”

CLASSIC
turn head + lift shoulder(older children)
torticolis?
Tongue movement?
signs of central paresis?
→ limited movement?
→ tense, indurated?
→ poor sucking-initiation
- INSPECTION:
- posture?
- symmetric limb movement?
- healthy newborn: embryo posture? ( predominant flexion & adduction of arm + legs)
- Muscle tone?
- Reflexes (tendon)
- The crossed adductor reflex is elicited when the patellar reflex is stimulated and results in contraction of the adductor muscles in the opposite leg.
- This response is normal until approximately 1 year of age.
- Persistent crossed adductor reflex, especially unilaterally, suggests the presence of difficulty in the corticospinal tract.
→ assymetry? absent? (LMN lesion)
→ crossed adductor reflex 📷 : <12m = normal
{kind=link}
ON BACK:
- Kussmaul’s: Snout r. (4m) → touch w/ finger mouth angle → tongue protrusion?
- Sucking reflex (4m)→ something in mouth
- Babkin: Palmar-mouth reflex → press on inside of hand (tenar) → open mouth?
⇒ sharp blow to table (20-30cm from childs head) → Phase 1: Arm abduction
→ Phase 2: Arm adduction (”hugs himself”)
(phase 2 can be absent in first week of life = normal)
📷 ⇒ turn childs head to one side → swordman posture: ipsilat: extendend (+↑tone); contralat: flexed
{kind=link}
⇒ until 6m
{kind=link}
VERTICAL:
→ 1. phase: flexion of legs
→ 2. phase: extension of legs against table
⇒ Automated ambulation: if legs stuck against each oter → leaning on toes (ballet dancer)
ON ABDOMEN:
- 1-1,5m → becomes head elevation reflex (lift head when laying on abdomen)
⇒ absent: UMN or LMN lesion
⇒ absent: UMN / LMN lesion
⇒ until 2m
- Reaction to hot/cold stimulus?
- reaction to stroking?
- reaction to eye + facial expression?
- Fontanel: Tense / pulsating?
- general hyperesthesia?
- ophistotonus 📷
- vertical liftet: hanging + ↑i + leg flexion
⇒ Ønuchal rigidity
⇒ < 4-6m: Kerning + Brudzinski + = normal
{kind=link}
{kind=link}
see above: Epilepsy
- Radiation
- Infection
- Hypoxia
- Head Trauma
- Classic birth RF: ↓weight, premature, multiple birth
- Assisted reproductive technology (ART)
- Infection: TORCH + FEVER of mother
- Asphyxia (hypox)
- ICH (intracranial hemorrhage)
- seizures

- Posture
- Oral refl.
- Strabismus
- Tone ↑
- Evolution (cong. reflexes + development: cognitive + grwoth)
- Reflex ↑
⇒ Interpretation: ≥4 ⇒ likely dgx of cerebral palsy later in life
- Posture (UMN) → fist w/ adducted thumb? 📷
- Oral motor → swallow? sucking? saliva drooling? chewing?
- Eye: Strabismus
- ↓Evolution/development (congential reflexs stay longer, automatic response appear later) → persistent palmar grasp, Moro, Magnus-Klein (assymetric tonic neck) → poor protective response (head) → poor equilibrium
- UMN signs
- Tone (muscle) → spastic extremities; BUT flaccid axial tone
- ↑Reflexes (tendon)
→ scissoring gait? 📷
{kind=link}
→ hyperextension of trunk?
- Spastic (70%)
- MCA cystic softening → cortical stroke ⇒ epilepsy + mental deficit
- subcortical → lateral ventricle enlargement
- UMN signs (pyramidal synd)
- hemiparesis + spasticity
- mainly distal limbs
- look for “hand preference”
- arms: Prehension → Ø princer grasp
- Excessive abduction of the arm
- Flexion at the wrist
- Hyperextension of the fingers, which are spread apart
- ↓Ipsilat. growth
- epilepsy + mental retardation
- scissoring gate, toe walk, or no walking
- ØEPILEPSY (uncommon)
- ØMENTAL RETARDATION
- bilat. spasticity (arms>legs)
- Bulbar symptoms (oral muscles)
- Ø SPEECH / dysarthria
- other CN palsies
- MICROCEPHALY + MENTAL RETARDATION
- Dyskinetic (athenoid)
- Ataxic
UMN lesion (signs) → (weakness +) spasticity → Stiff/tight muscles
⇒ strabismus + visual defect ⇒ if bilat. : “scissoring gait” + toe walk “ or not possible to walk (bc. calves + adductor m. = flexed)
(⇒ bleeding → compression)
(pre, peri-, post-natal etiology)
CT/MRI📷 /US
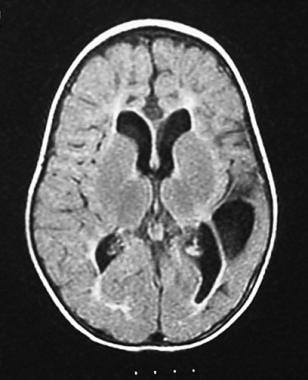{kind=link}
shows asymmetrical dilatation of the occipital horn of the left lateral ventricle, with loss of periventricular white matter

⇒ FACE IS SPARED!
mild → pincer grasp +
moderate → closed globally
severe → hand not used at all
preterm birth
{kind=link}
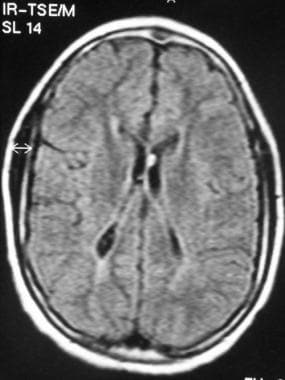{kind=link}
ARMS!
{kind=link}
Basal ganglia lesion (movement coordination + execution, posture)
→ ACTION Involuntary movement (basal ganglia usually initiate + prevent movement) → occur when attempt to move + try to maintain posture
⇒ Tremor + Dystonia + Chorea + Atetosis
Dystonia

Atetosis

Cerebellar → uncoordinated / movement + postural tone (cant hold balance)
Ø PYRAMIDAL → walk with 3-4y
Intellectual impairment but Ø SEVERE mental retardation
→ if severe mental r.: assoc. w seizure + microcephaly
MRI: Dandy walker malfomation (hypoplasia of cerebellum)
- Delayed + abnormal development (motor, cognitive)
- growth: unilat (hemiplegic); bilateral legs (arms = normal) (diplegic)
- feeding difficulties
- Ø/delayed bowel + bladder control
- epilepsy
- pain
- eating + sleeping disorders
Gross motor function classification system (level 1-5) ⇒ functional? assistive technology? wheelchair?
The five levels of mobility are as follows in decreasing order of mobility:
- Level 1: Able to walk without limitations.
- Level 2: Able to walk long distances but cannot run or jump. May need assistive devices such as braces when first learning to walk. May need a wheelchair outside of the home.
- Level 3: Able to sit with little support and is independent in standing. Able to "walk with adaptive assistance." Walking indoors requires "hand-held adaptive assistance." Requires wheeled assistance outdoors.
- Level 4: Limited self-mobility. Some support when sitting. Able to move independently with wheeled assistance.
- Level 5: Head and trunk limitations are severe. Need for assistive technology and manual help is extensive. May be able to control a motorized wheelchair.
- Drugs: Relax the muscles (therfor reducing pain) ⇒ Diazepam / Baclofen / Botox
- Physio → prevent contracture + dyskinesia, promote normal movement
- Ortho → splints + corrective surgery
- bone straightening (which are bend to do abnormal forces)
- nerve cutting → ↓spasms/movements
- Swallowing → PEG, NG tube
- Speech, behavioral + learning managemement
corrective surgery includes:
- ↑birthweight → trauma → epi- + subdural + intraparenchymal (”always” assoc. with SAH)
- preterm w/ asphyxia → intra-ventricular (assoc. with SAH & intracerebellar [hypox + ischemia])
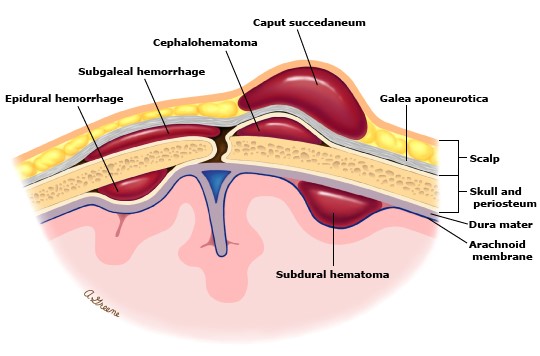{kind=link}
- Cephalhematoma: bone - periosteum
- Subgaleal: periosteum - aponeurosis
- caput succedaneum: aponeurosis skin
epidural
{kind=link}
COMPRESSIVE/↑PRESSURE SIGNS:
- ↓conciousness (stupor/coma) + irritability
- ↑ICP → bulging fontanelle
- brainstem → respiratory alteration
US, CT, MRI
F - most freq. cause in PRETERM babies (<37w)
rupture of blood vessel in germinal matrix (subependymal) 📷
{kind=link}
⇒ periventricular bleeding ⇒ intra-ventricular bleeding 📷
{kind=link}
(⇒ intraparenchymal bleeding)
- The germinal matrix is formed early during embryogenesis and serves as the site of glial and neuronal differentiation.
- Cells migrate peripherally from the germinal matrix to form the brain.
- The germinal matrix is densely cellular and vascular.
- Premature infants are at higher risk for germinal matrix hemorrhage due to weak-walled blood vessels in this region.
- Significant stress after birth can cause rupture of the blood vessels in the germinal matrix, leading to periventricular hemorrhage (PVH).
- Persistent bleeding can result in intraventricular hemorrhage (IVH) as the blood dissects into the adjacent lateral ventricles.
- The risk of hemorrhage in the germinal matrix decreases as gestational age progresses.
- At 32 weeks gestation, the germinal matrix is only present at the caudothalamic groove.
- By 35-36 weeks gestation, the germinal matrix has disappeared, reducing the risk of hemorrhage.
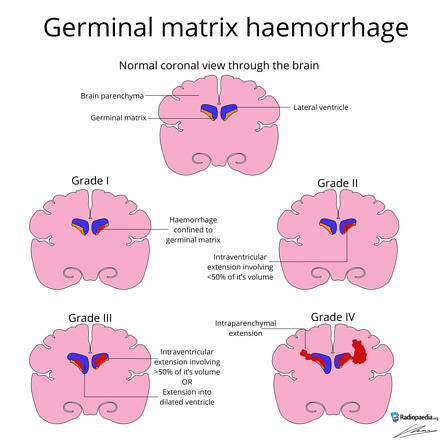{kind=link}
SIGNS OF COMPRESSION / ↑ICP
- can be acute (classical) or mild
- ↓Conciousness (acute vs milder)
aute: abrupt deterioration
milder: ↓ alertness, stupor/ irritability
- bulging ant. fontanelle
- Respiratory irregularities
- CN: eye movement abnormalities
- Hypotonia
- Fibrosis → post-hemorrhagic adhesive arachnoiditis → thickened + adherent to pia+dura matar ⇒ hydrocephalus
- If confined to subendymal area (grade 1) ⇒ periventricular cysts
- Neurodevelopmental abnormalities
US!!
(CT)
T
asphyxia ⇒ hypoxia + hypercapnia ⇒ acidosis → ↑Lactate + ↑glycolysis ⇒ decline of brain Gluc ⇒ brain lesion
- Periventricular leukomalacia (#1) 📷
- Trigone + occiptal horns 📷
- visual impairment (optic radiation)
- spastic diplegia (corona radiate leg portion)
- Basal ganglia (esp. globus pallidus + subthalamic nucleus 📷; common in kernicterus)
- Selective neural necrosis (localized / diffuse)
- Parasaggital pattern (affects arm-portion of corona radiata)
- Focal (MCA infarction)
⇒ lesion optic radiations 📷 + corona radiata 📷(portion for legs)
{kind=link}
→ might extend ⇒ ant. ventricular horn
→ lesion ⇒ gliosis (”scarring”)
Mild | Moderate | Severe | |
Mental Status | ↑↑ alertness | Lethargic | Coma/stupor |
Muscle Tone | Normal / slightly ↑ | Hypotonia | Hypotonia, flaccid |
Respiration | Normal | Periodic apnea | Irregular breathing |
Reflexes | ↓ sucking reflex | ↓ deep tendon reflexes
Weak/Ø neonatal reflexes | ↓ deep tendon reflexes
Ø neonatal reflexes |
Seizures | Ø | May occur within 24 hours postpartum | generalized (usually) |
Extra | Temporary (self-limitied) behavioral abnormalities (i.e. poor feeding, ↑ crying)
⇒ typically < 24h | Quick recovery (possible in 1-2 weeks) | 1. Ocular motor disturbances (i.e. nystagmus, bobbing);
2. Pupillary abnormalities (i.e. dilation, fixation, light unresponsiveness)
Symptoms may improve after 5 days postpartum;
if neonate survives → continued support needed |
mild (1) → good + Ø sequella
moderate (2) → unpredictable
severe (3) → poor
- Kidney + heart workup (metabolic damage)
- Seizure control
- ↓ICP - mannitol (Østeroids!)
Exessive traction of the
- neck ⇒ injury upper trunk (C5-C6 📷) = Erb palsy (#1)

- arm ⇒ injury lower trunk (C8-T1) = Klumpke palsy
- total = Erb + Klumpke
- can also be bilateral
⇒ ↓sensory + motor function
- Complete brachial plexus ⇒ complete flaccid paralysis + Horner 📷
- Erbs palsy 📷 ⇒ weakness C5-C6 myotomes ⇒ waiter’s tip position
- arm: adduction, internal rotation + extension
- Ømovement in shoulder + ellbow
- pronation + wirst + hand flexion
Horner syd:

if involving C3-C4 (severe avulsion) → phrenic nerve palsy
- Physical therapy
- w/ movement restricion
- splinting
- Surgery → Re-build
- Nerve graft reconstruction
- Nerve transfer
- Neurolysis (remove scar tissue)
- Other
- Neuromuscular electrical stimulation
- Botox