





Radiology II
🫁 Lung
more infos below
- Bone abnormalities? (scoliosis, rib fx)?
- Thorax size? (↑ - emphysema)
- chest wall mass? (obtuse angle - Bernou sign)
- bone deformities
- Kypo-scolisosis / scoliosis 📷
- pectus excavatum 📷
- Rib deformities / fractures 📷
- emphysema (↑size) 📷
- chest diameter↑
- Diaphragm: flattening
- Ribs
- Horizontal disposition
- widened intercostal spaces
- → usually 7-8 ant. ribs seen → >8 in emphysema
- heart: vertical (falls down)
- hyperlucencies w/ visible vessel (might not be that obvious)
- Chest wall tumors 📷
⇒ (might overlay pathology)
if in the middle → CT might be needed to differentiate intra-pulmo vs. chest wall (see later)
- ↑opacity?
- heart
- vessels
- LN
- tumor
- shifted?
- atelectasis
- pleural effusion, pneu
- adhesions (pleural)
- dynamic alterations?
- complete?
- incomplete?
- inspiratory bronchial stenosis → towards stenosis
- expiratory bronchial stenosis → towards opposite side
more infos below
- elevation?
- flat? (emphysema)
- costophrenic angle?
- mobility? (Hinge signs = costophrenic symphysis)
- Elevation of hemidiaphram?
- >1,5(-2)cm height compared to contralat.→ pathologic 📷
- Etiology: Pleural effusion (→US!), phrenic n. paralysis, hepatomegaly
- ↓ mobility?
- check with fluroscopy or 2xrays (inspir. + expir.)
- adhesions? (peridiaphgramatic inflammation→fibrosis)
→ HINGE SIGN (costrophrenic symphysis) 📷
pic 1: inspiration pic 2: expiration
- Localization
- chestwall: Bernou sign = obtuse angle 📷 (betw. border of lung and mass)
- pulmonary: acute angle 📷
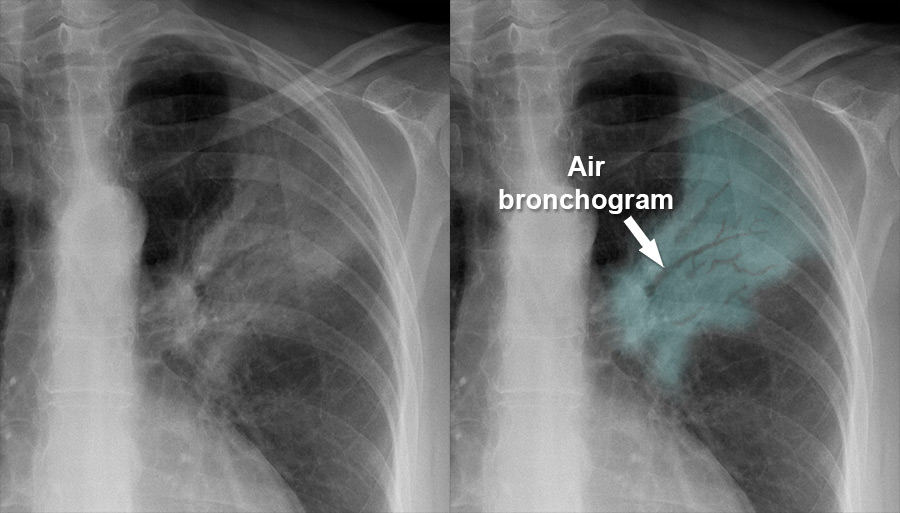
- Silhouette sign 📷→ contour blurred when 2 object in contact (if Ø→ superimposed)
- diffuse
- How many lesions? (number)
- Whats the form of the lesion? Size? homogenous/inomogenous
- border / contour?
- relation with sourrunding
- Intensity compared to heart
- Localisation: Pulmonary region in PA, lobes, segments, fissures (PA and LL)
- Number: How many lesions?
- Shape: Systematized or non-systematized
- Size: Dimensions of the lesion
- Contour/Outline: Sharp, sharp and linear (fissure), ill-defined, regular/irregular (infiltrating, lobulated)
- Structure: Homogeneous or inhomogeneous
- Nature: Fatty, soft tissue, bony (calcium)
- Intensity: Greater than, less than, or equal to the heart
- Relation with Surrounding Structures: Relationship with adjacent structures
- localized?
- vessel vs. Ø vessel?
- vessels → emphysema
- Øvessel → enclosed air cavity (sharp outline - wall)
- diffuse?
- vessel vs Øvessel + uni vs. bilat
- vessels
- bilat → emphysema 📷, ac. asthma
- unilat → stenosis main bronchus
- assoc. signs
- ↑size: thorax + pulmonary volume
- Air trapping: ↓Insp.+exp. difference
- pulmonary arteries abnormalities
- Øvessels
- lateral → pneumothorax (see below)
- intra-pulmonary → large cavity/air cyst
“
- Localization: circumscribed / diffuse
- Number: for circumscribed lesions
- Dimensions: for circumscribed
- Outline: for circumscribed (thin/thick wall)
- Structure: with/without vessels
- Relation with the surrounding structures
- Dynamic: size decreased/increased at inspiration/expiration maneuvers”
- Mixed cyst
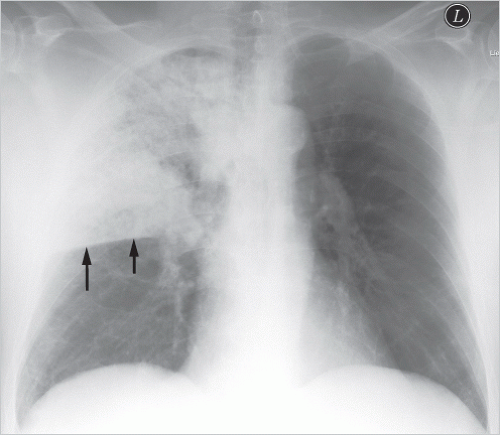
- Partially evacuated abcess 📷
- if completely evacuated ⇒ air cavity
- if Ø evacuated → cant be seen!
- walls?
- thick irregular → recent abscess
- thin + calcification → chronic abscess
- Partially evacuated hydatic cyst (+waterlily sign → wavy 📷)
- if completely evacuate ⇒ air + small opacity
- if Ø evacuated → homogenous opacity
- Infected air cyst
- Hydropneumothorax 📷 📷

Straight surface = Abscess Wavy surface = Ruptured hydatid cyst
- Prominence of pulmonary vessel?
- large vessels?
→ see pleural syndrome
pneumo, effusion?


thickened bronchial wall
⇒ w/ shift towards (inspiratory valve) ⇒obstructive atelectasis (when complete)
⇒ or hyperinflation w/ shift away (expir. valve)

thickening of bronchial walls: 📷 peribronchial “cuffing” (in asthma & chronic bronchitis)

DIRECT SIGNS:
- ↓volume: pulmo+thoracic
- Øair bronchogram
- if lobar / systemized:
- retraction of fissures (inverted S) 📷
- triangle-shape
INDIRECT SIGNS:
- Diffuse / non-systemized + non-confluent
- low intensity
- DDx features interstial syndrome vs. bronchopneumonia:
- sharp border (??)
- slow evolution
→ see also “interstital pneumonia”

Xray, US, CT
- lateral hyperlucency
- Ø Pulmonary pattern (Øvessels)
- medial = adjacent lung (visc. pleura edge visible)
- lat = parietal pleura
- Lung collapse (atelectasis) towards hilum
- diaphram compression + incr. intercostal space
- Etiology:
- Trauma
- Spontaneous (i.e. emphysema)
- Ømediastinal shift
- if Mediastinal shift ⇒ 🚑 Tension-Pneumothorax!
F - clinical
- Cardiac
- Tumor
- Infection (exudates)

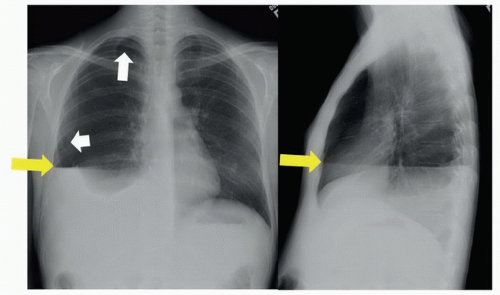
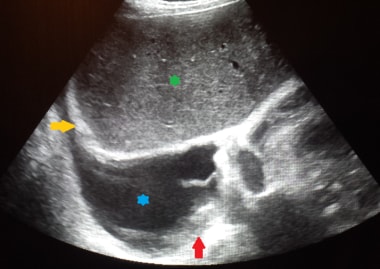
SMALL: 📷
⇒ Diaphragm
- blurred outline
- loss of costro-phrenic angle
- mobility testing (→ DDx: CP-symphisis)
- ↓motility of diaphragm
- effusion moves with diaphragm
MEDIUM: 📷
⇒ ascends on lat thorax
- concave + blurred upper outline
- mobile opacity ( with position )
- Øair-bronchogram
LARGE: 📷
⇒ Apex reached
- Mediastinal shift away
- ↑Volume
⇒ if Ø shift → consider assoc. atelectasis

Mixed image (Pneu + Effusion) ⇒ Basis + lat changes
- Inf: Opaque
- Sup: Radiolucent (Pneu signs)
- AIR FLUID LEVEL (unlike pleural effusion)
- free vs. loculated!
FROM INSIDE OR OUTSIDE
- Lung parenchyma
- intercostal + intermammary vessels
same as pleural effusion
- Inflammatory non-suppurative pneumonia
- Inflammatory suppurative pneumonia
- Primary: abscess, pulmonary gangrene, diffuse pulmonary suppuration
- Secondary: complication of pneumonia, bronchiectasis, pulmonary cysts




- Peribronchial + perivascular thickening (interstital edema)
- reticular infrahilar band (opaque)
- micro/macronodular opacities

Benign | Malignant | |
Border | sharp | irregular |
Structure | homogenous, solitary, round | heterogenous |
calcifications | hamartoma | (”scar cancer”) |
sourrundings | Ø | - rib lysis
- pleural effusion
- LN (hilum)
- pulmo mets |
growth | slow | faster (2x 3-6m) |
Complications | central necrosis
|
- Adenoma 📷
- Fibroma
- Hamartoma
- Lipoma
- Chondroma
- Central / Hilar
- exobronchial (outside of bronchi)
- endobronchial (involving bronchi)
- complete = obstructive atelectasis 📷
- incomplete
- expiratory valve → hyperlucency
- inspiratory valve → hypoventilation + pneumonia
- Peripheral
- Malignant outline! (irregular outline, spicules, “tail”) ⇒ see illustration in lecture
- Bronchialveolar 📷
- diffuse
- patchy or might be confluent
⇒ compare above
→ bronchoscopy!
CLASSIC
- cough, dyspnea, hemoptysis
- pleuritic pain
- B- symptoms
- extension signs: recurr. laryngeal, phrenic n, dysphagia, SVC syndrome, pleural+pericardial effusion
- paraneoplastic syndrome
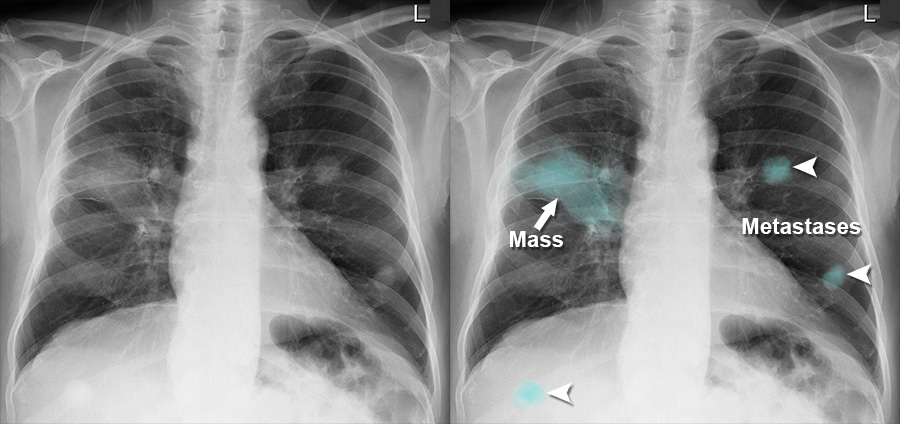
- Benign masses
- mets
INVADE sourrundings
- chest wall
- mediastinum
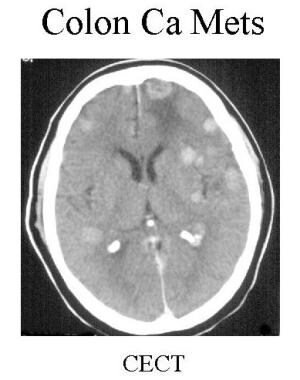
METS:
- Head
- Liver + adrenals
- bone
- Lung
- common mets
- lymphangitis carcinomatosis 📷
- Breast cancer
- Bone cancer
- Thyroid cancer
- Seminoma and prostate cancer
- Uterine cancer
- Digestive tract cancer
- Renal cancer
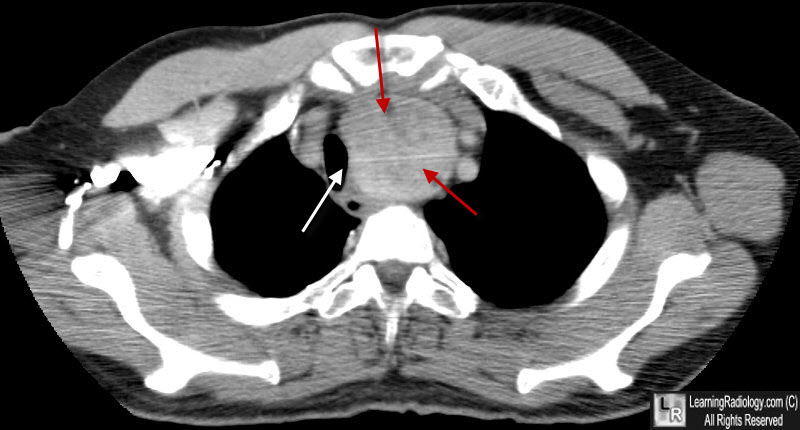
🫀 Mediastinum
- SUP mediastinum ⇒ Sup. vena cava syndrome
- MIDDLE mediast ⇒ bronchi + recurr. laryngeal n. compression
- INF mediast. ⇒ Inf. vena cava syndrome
- Xray (PA, LL) → identification
- CT +con→ characterization, extension, LN, (bone involvement)
- MRI +con → Spinal / nervous system


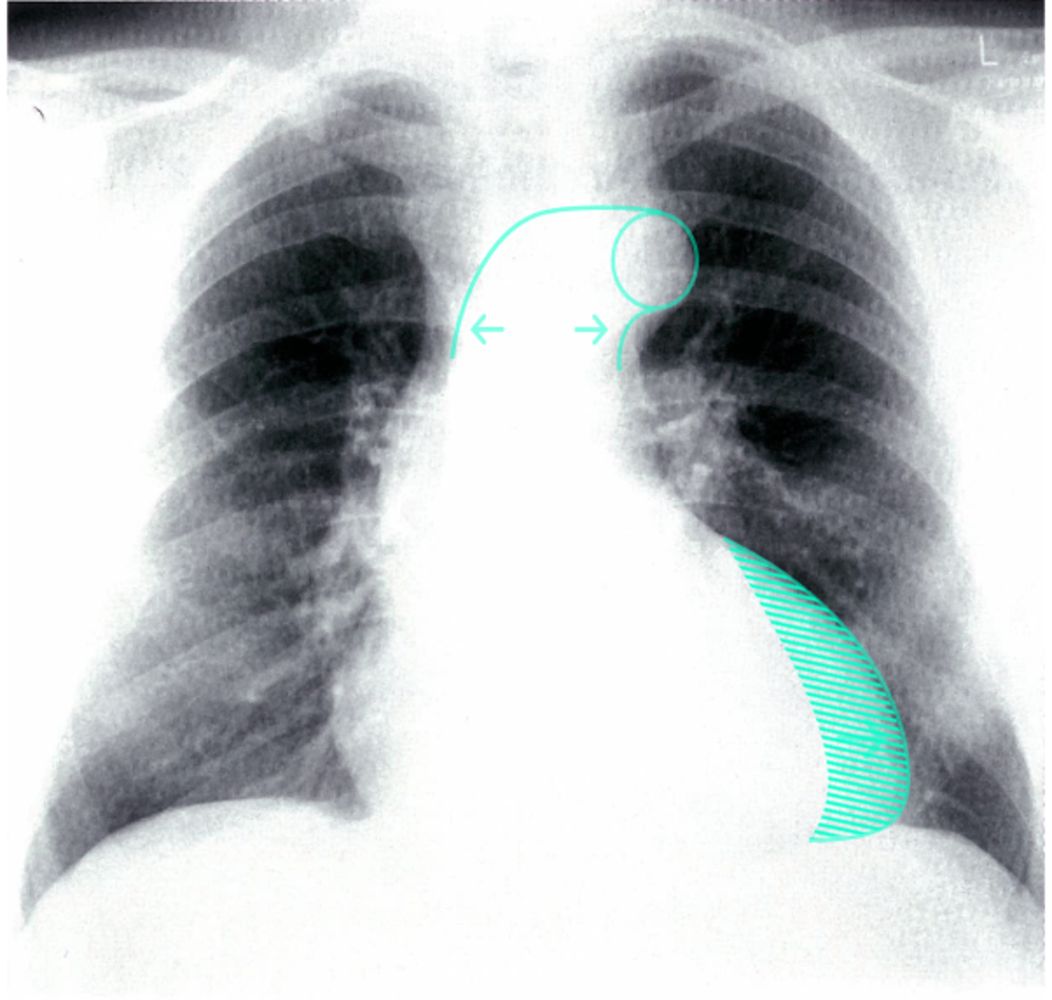
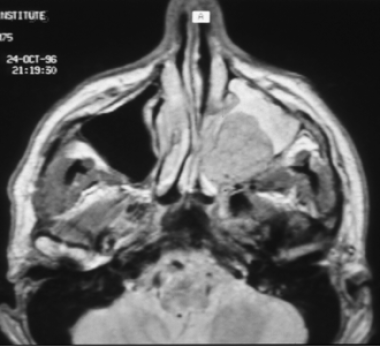
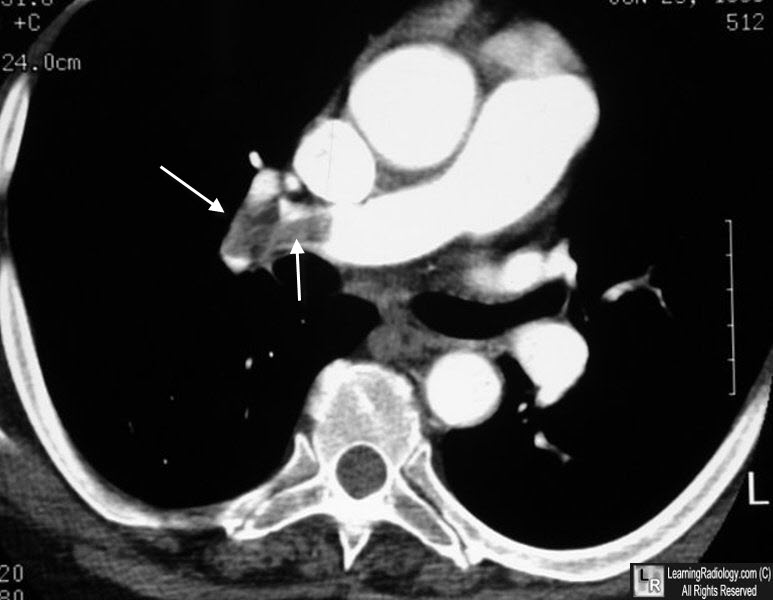
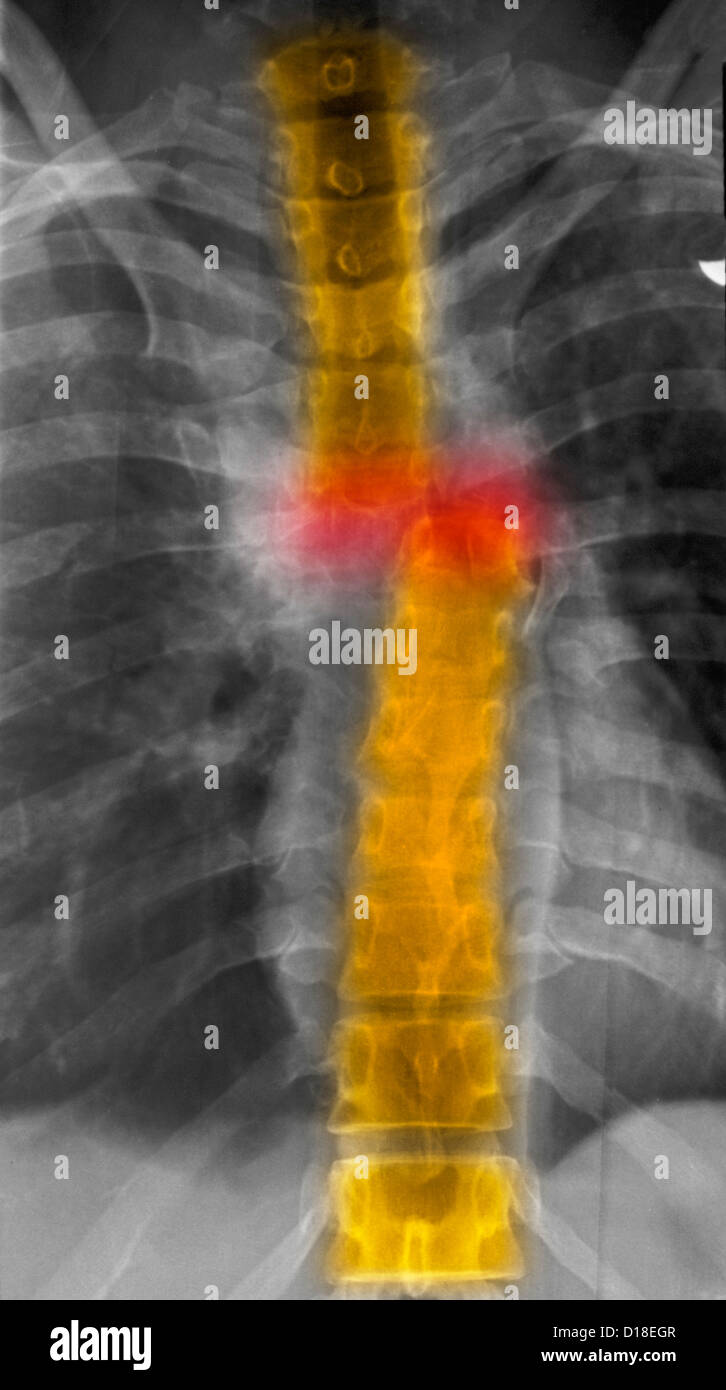
- Enlarged mass in ant. mediastinum (enhancing) [red arrows]
- Mass effect → trachea (Dislocation/compression) [white arrow]
- retrosternal goiter vs. tumor?
- homogenous → retrosternal goiter
- inhomogenous cervical LN? invasive? → tumor
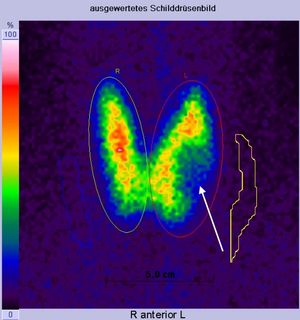
scinti 📷
more details later
anterior middle 📷 (anterior to asc. aorta on AP view)
- Hyperplasia 📷
- Cyst 📷
- Thymoma 📷
- Carcinoma 📷
- Teratoma 📷
→ global enlarged → normal shape/outline
→ fluid density → wall calcification
→ benign features, → homogenous contrast uptake → +/- calcifications

→ inhomogenous → WELL DEFINED OR INVASIVE/mets → inhomogenous contrast uptake

→ fat + calcifications → cystic (uni or poly)
Middle mediastinum 📷
- Infectious
- Malignancy
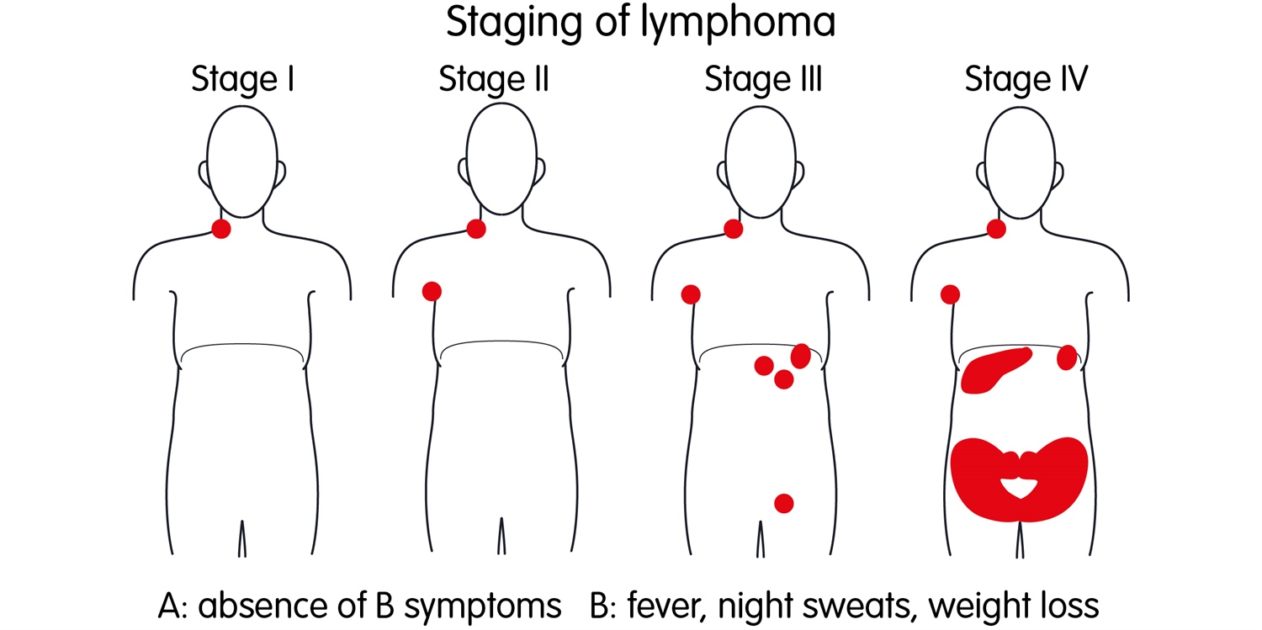
- Primary: Lymphoma (HL+NHL)
- Secondary LN mets
- Granulomatous
- Sarcoidosis
- Silicosis (egg shell)
Stage | LN group | extralymphatic region |
1 | 1 ———> OR: | 1 |
2 | 2 ———>OR: 1+
(same side diaphragm) | 1
|
3 | 2
(both sides diaphragm) | +/- (spleen) |
4 | +/- | multiple organs |
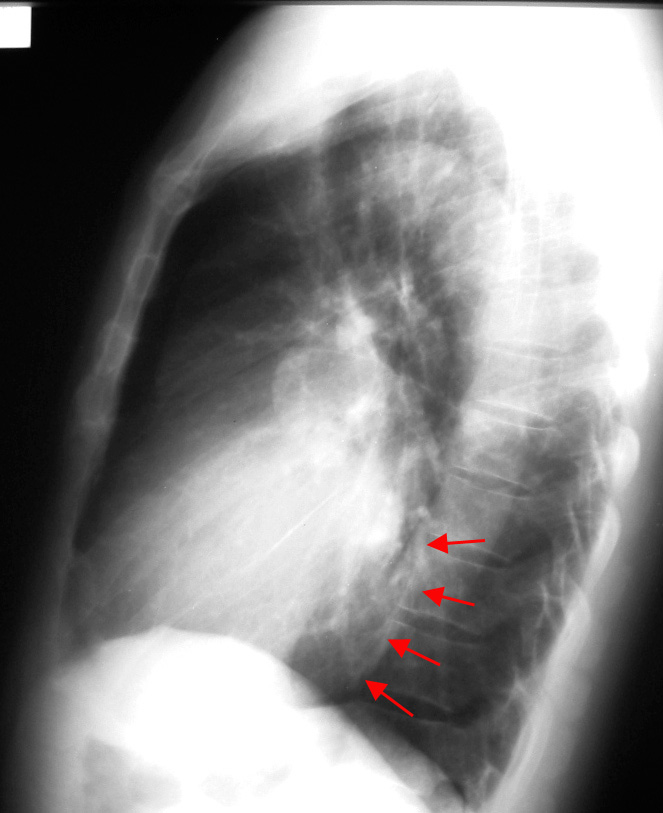
Posterior mediastinum (paravertebral) 📷
- Periph nerves → Neurofibroma + Schwannoma (Neurinoma)
- Sympathetic → Neuroblastoma
- opacity (paravertebral)
- Øsilhouette sign (behind heart)
- round/oval
Pathology of other structures in post. mediastinum
→ esophagus, thoracic aorta, spine
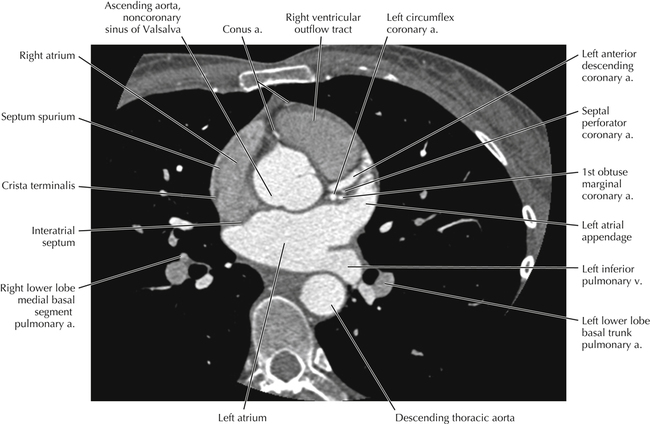
🫀 Heart
Soft tissue evaluation!
- MYOCARD
- MI
- hypertrophy (+wall function)
- tumor invasion (also pericardal tumor)
- SEPTUM
- defects? 📷
- Other imaging exams: echo, xray, scinti, angio, catheter
→ see below
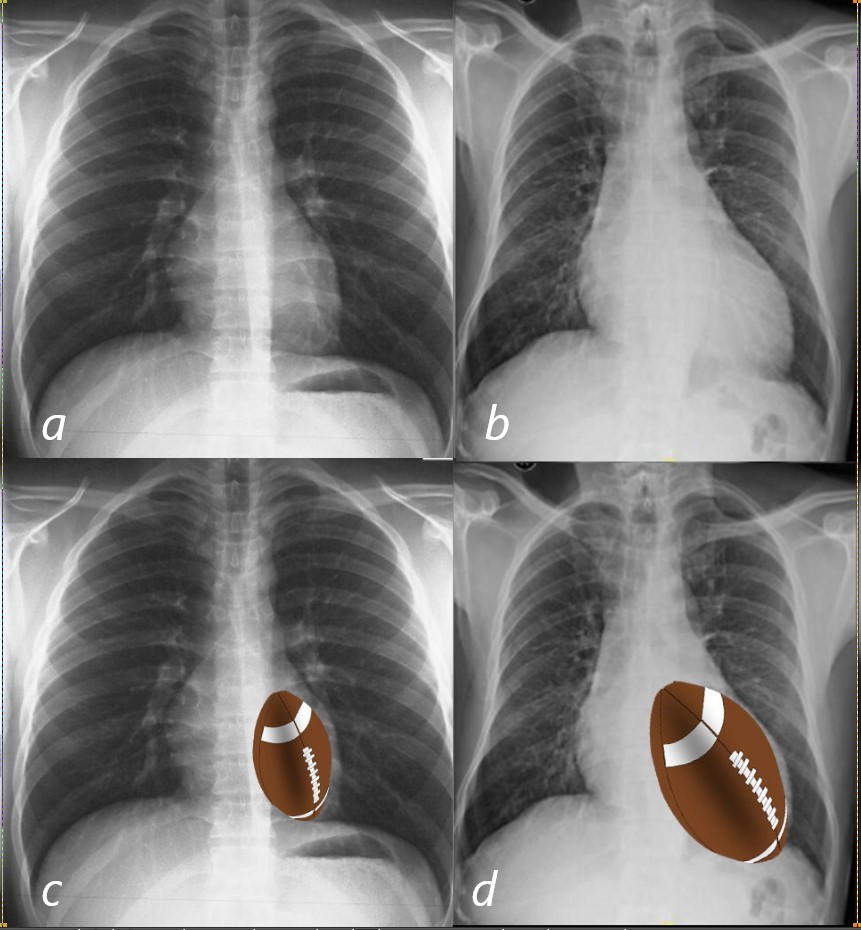
LEFT → Backwards (retrocardial)
Right → Forwards (retrosternal)
⇒ touches >1/3 of retrosternal clearspace (inner ant. chest wall) 📷
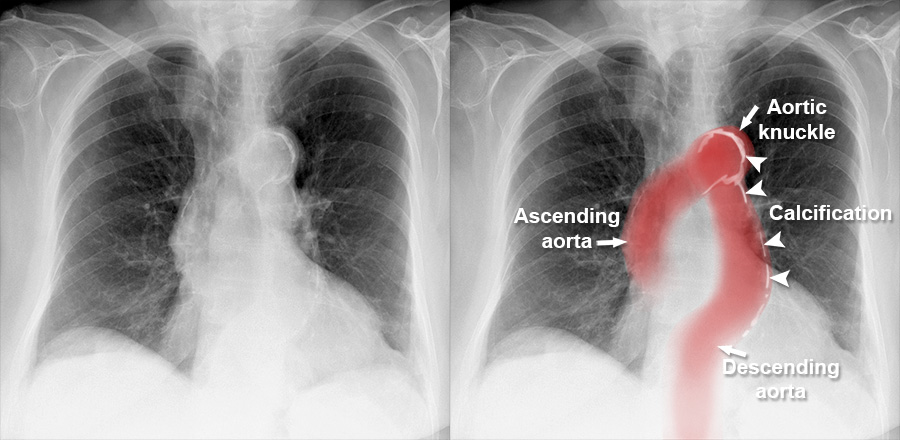
- Aortic knob: >35mm distance to lateral. air border of trachea 📷 📷
- ↑Pressure/Flow
- Aortical wall abnormalities
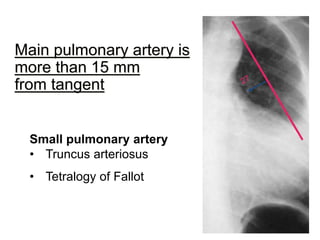
- Main Pulmonary artery (might not be seen)
→ Normal: 0-15mm medial from tangent line (aortic knob→LV) 📷 📷
→ If extends beyond (convexity?) ⇒ Pulmonary artery HT (↑Pressure/flow)
Venous → pulmonary capillary p >(10-)12
Arteral → PAP systolic >25 OR PAP median >15
- Oligemia ⇒ ↓blood into lungs (obstrucion (PA stenosis), ↓V (hypovolemia +R-L shunt)
- Hyperemia
- Venous PHT
- Arterial PHT
- venous PHT (LV congestion)
- Obstruction
- embolism
- Primary PHT
⇒↑blood into lung (PA regurg, ↑V( hypervolemia, L-R shunt)
⇒ LV congestion (mitral stenosis, LV failure)
Lung | Hili | Vessels | Felix rim (Fleischer signs) | |
Oligemia 📷 | Hyperlucent periph. (Westernmark) | small + frail | small (+ not filled) | enlarged PA 📷 |
Hyperemia 📷 | Hyperlucent (relative) | Arterial hili | dilated + redistribution (cephalization) | Ø |
mild venous PHT (12-18mmhg) 📷 | Venous hilum | visible pattern + redistribution
(cephalization) 📷 | Ø | |
moderate venous PHT
(18-25) 📷 | 1. interstital edema
→ Kerley A+ B, blurred hilum (cuffing) , vascular opacities
2. pleural effusion (free/loculated)
📷 | “ | “ | |
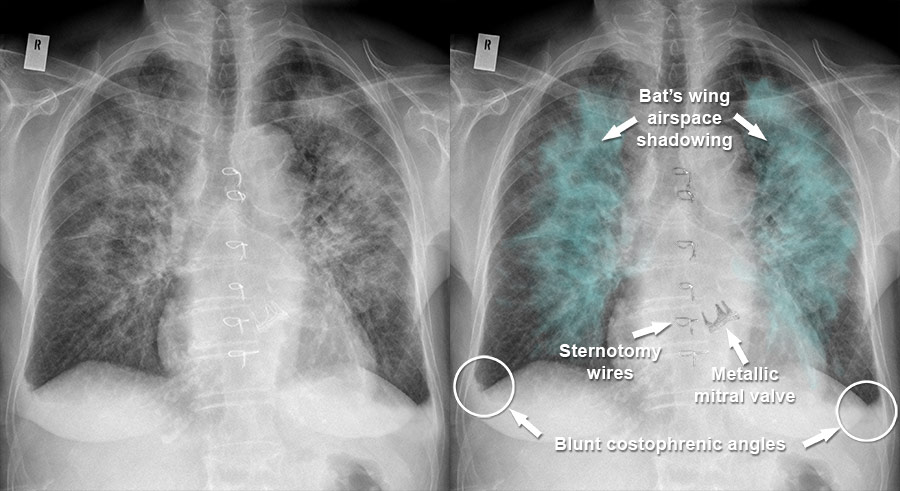
severe venous PHT (>25) 📷 | (acute) alveolar edema
→ air-space filling syndrome
→ central Bat/butterfly wing | “ | “ | |
arterial PHT 📷 | Hyperlucent
(periph collapse) = Westermarck sign) |
Large + „Amputated” = embolus
(Goodwin/Knuckle sign)
| ↓periph. vessels
Pulmonary artery >15mm from tangent | enlarged PA (ri. desc. pulmonary artery) 📷 |
Pulmonary Arterial Congestion | Pulmonary Venous Congestion |
Active congestion | Passive congestion |
Pulmonary arterial hypertension | Pulmonary venous hypertension |
Constricted arterial vessels | Prominence and thickening of upper lobe vessels |
Dilated hilar trunks | Prominence of lower lobed vessels |
Pulmonary vasculature on CXR findings | Hazy hilar vessels present |
Seen in ASD, VSD, PDA | Seen in left sided obstruction such as mitral or aortic valve defects regurgitation and stenosis |
Roentgen features of Kerley A, B, C lines | |
Kerley B Lines= pulmonary venous pressure is at 17- 20 mmHg | |
Pulmonary edema= > 25 mmHg |
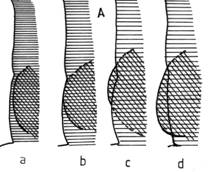
- apex lifted boot shaped (”coeur en sabot”)
- prominent pulmonary artery (aPHT)
- retrosternal space filling (LL)
- LA enlargment
- covex/straight appendix
- double-density sign
- elevation left main bronchus + ↑carina angle
- Venous pulmonary hypertension
- upper zone venous enlaregment
- pulmonary edema
- Progresses: arterial pulmonary HT, RV hypetrophy, trikuspid regurg
- LA enlargement (see above)
- Venous pulmonary hypertension
- upper zone vein enlargemen
- acute:edema
- LV enlargement
- LV enlargement (hypertrophy → later dilation)
- post-stenotic dilation
- later: pulmonary venous cong
- global enlargement (w/ clear margins)
- “lying on diaphragm” - shape change
- +/- signs of HF (clinic + radio)
- congestion (vPHT→ aPHT)
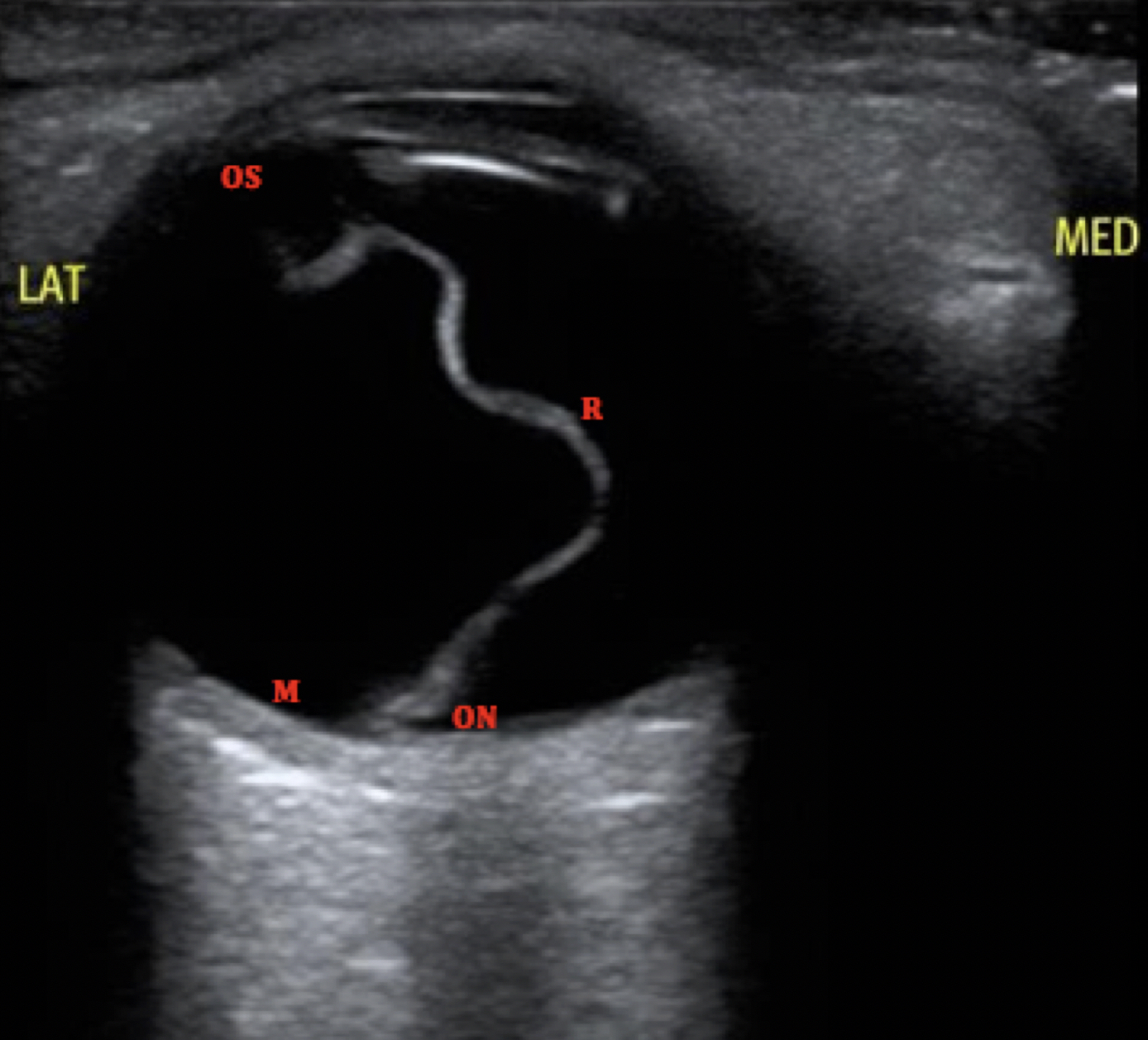
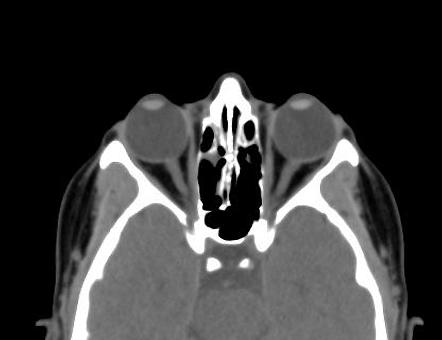
🧣 Head & Neck
- Optic nerve
- Optic vein
- Eye muscles
- Lacrimal gland (look for classic malignant signs)
- eye ball (shape/outline, position, symmetry, walls, post. fat)
#1 US (with doppler, 2D, elaso) → thyroid + LN (see pathologic LN)
→ nodules? → #2 scinti (”cold” vs. “hot” nodule) 📷
→ malignant? → #3 CT/MRI (con) 📷
⇒ extension? ⇒ LN?
- Morphology?
- Size?
- Symmetry?
- Homogenous? (cysts/nodules?)
- Extension?
- Blood vessels? (common cartoid + IJV) 📷
- cervical LN?
🌶️ Blood vessels
- int. thrombus / embolus /spasm
- aneurysm + dissection
- hemodynamic changes → ↑clotting
- ext. compression
Leriche synd:
- Aorto-femoral obstruction → bilat.
- RICH COLLATERALS!
- Clinic:
- first sign = impotence
- Pain buttocks + lumbar → DDx lumbar disk
→ stenosis / occlusion
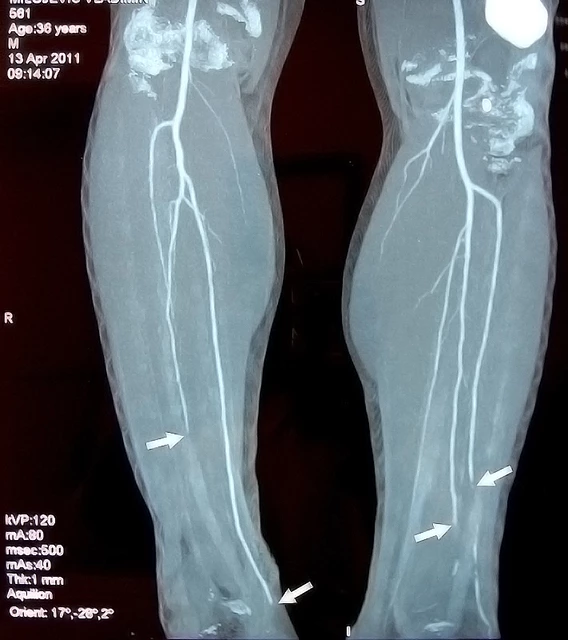
Burger D. (thrombangitis oblit.)
- Small terminal vessel → small caliber
- POOR COLLATERALS
- Clinic: young male, smoker
→ “spiral-like” + multiple thrombi


- Hampton’s hump (focal subpleural density - evtl. triangular) & Knuckle sign (sharp cuttoff pulmonary artery) 📷
- Westermark signs (hyperlucent periph. vasc. → regional oligemia) 📷
- Indirect due to ↑ back pressure
- Pleural effusion 📷
- Elevated hemidiaphragm
- Signs of PH → Fleischner sign: Prominent PA + ↑diameter, cut-off
- ↑RV diameter
- angio → filling defect 📷
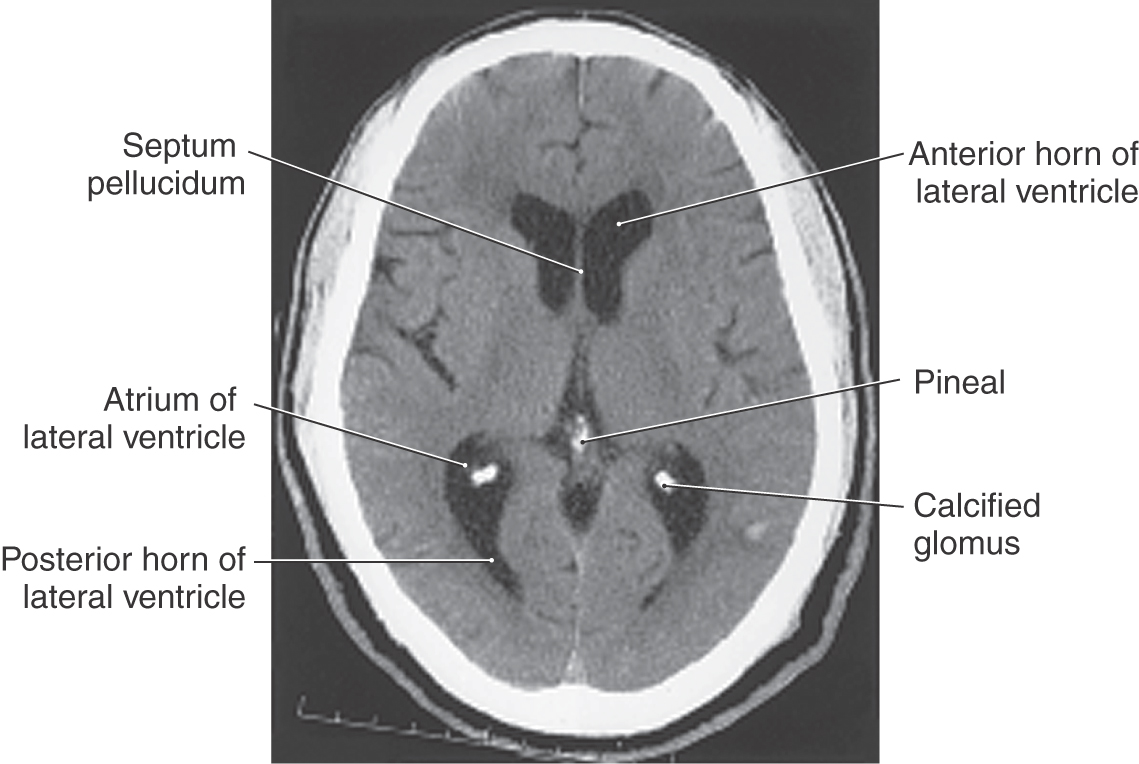
🧠 Neuro
- bone/calcifications
- fresh blood (first 7d)
- contrast
- foreign bodies
- (light gray: tentorium, venous sinuses)
- hemorrhage (subacute)
- cerebral → 20d
- meningeal (subarachnoid) → 5d
- Other isodense structure → tumors + pus
- chronic hemorrhage
- edema
- central necrosis (”behaves like fluid”)
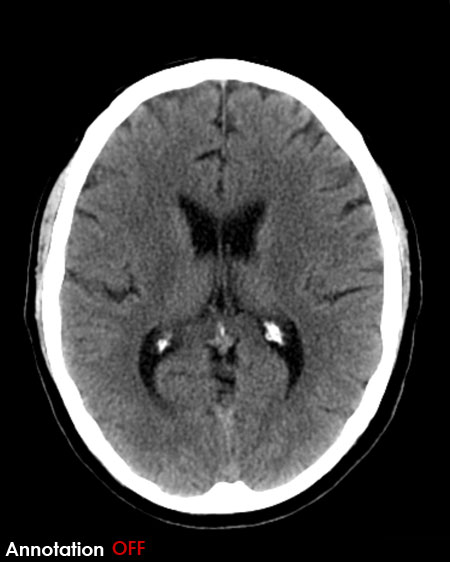
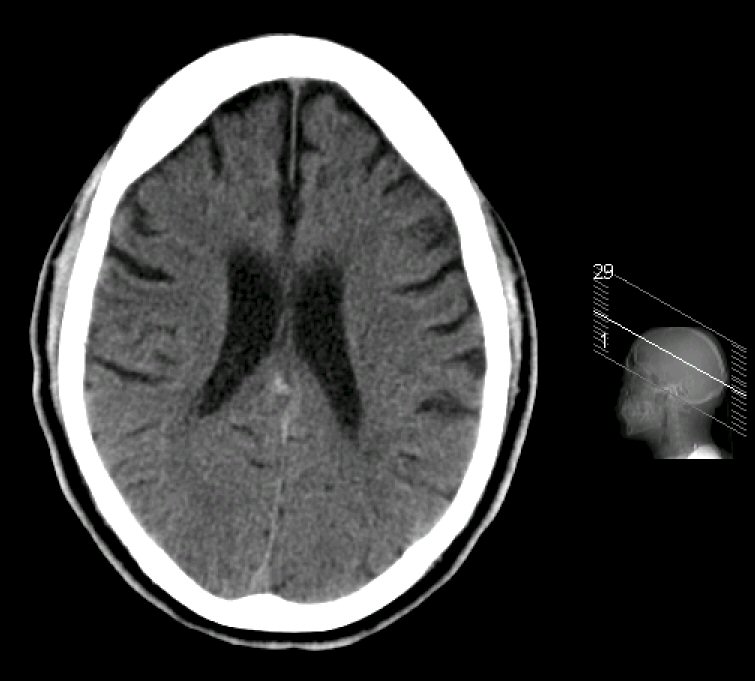
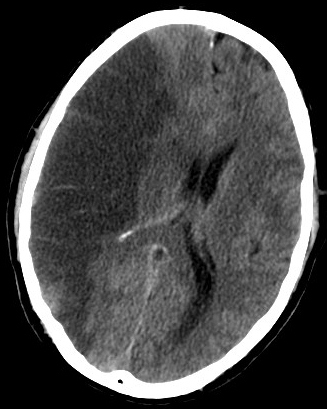
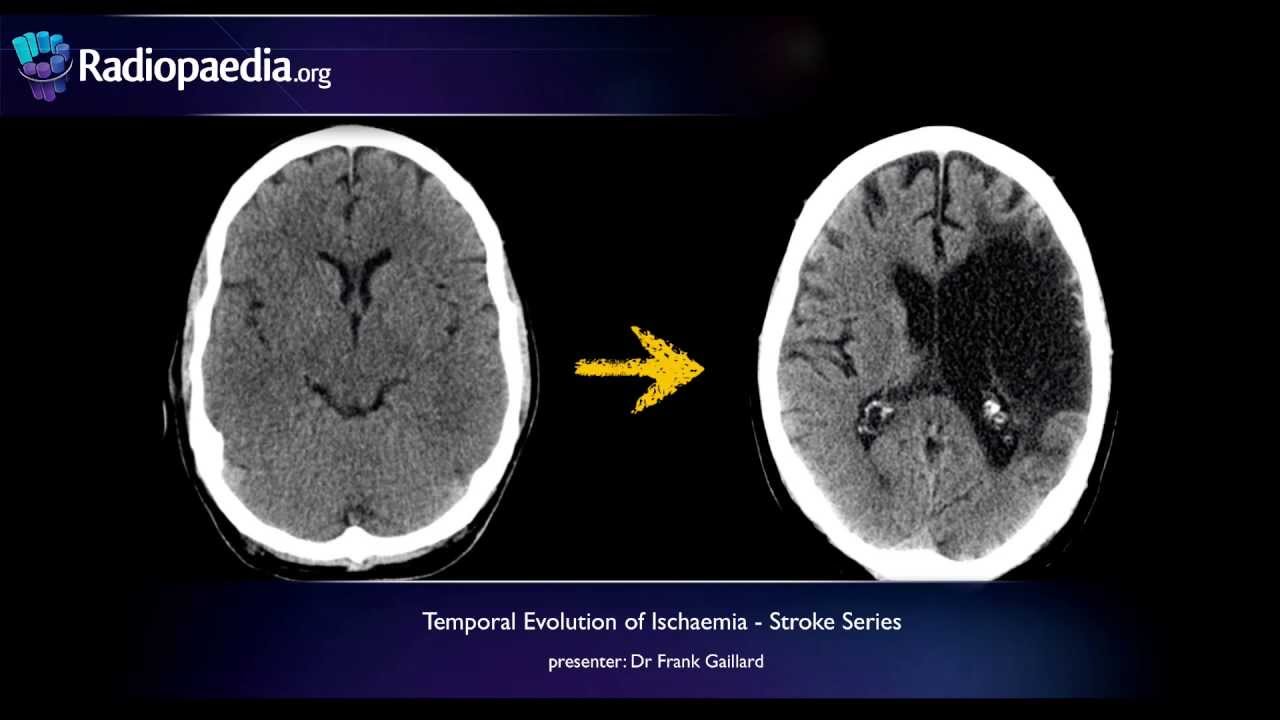
- ischemia
- Dead brain tisse
- ischemic lacuna + brain atrophy
- central necrosis: cystic tumor or met
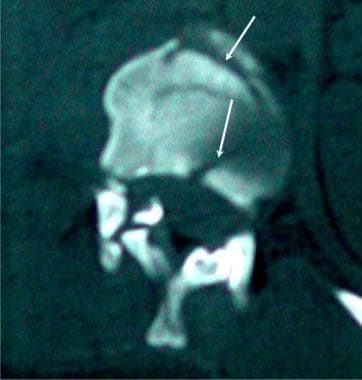
- arachnoid cyst 📷





↓Signal in both seq. (T1+T2)
Diffusion weighted (DW) MRI
- hyperdensity within blood vessel (hyperdense artery+vizualisation)
- Vasogenic edema (later cytotoxic edema): loss of grey & white differentiation → hypodense area
- CT + T1 → hypodense/-intense
- T2 → hyperintense
- edema & mass effect → loss of sulci +- ventricle compression
- sharply demarked area
- black (similar to CSF → T2 hyperintense)
- +- contrast enhancing rim
- Hemorrhagic stroke (see “Trauma”)
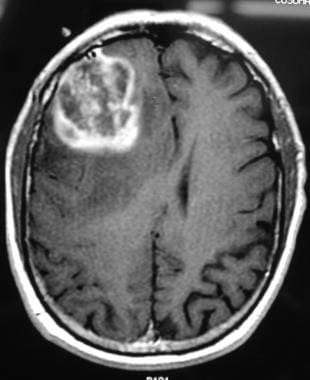
- approx. round well delineated lesion often at parasagittal convexity or falx
- hyper-isodense
- homogenous enhancing (compared to brain parenchyma)
- calcifications*

- dural tail

- mass effect

- Hypodense Halo (edema)

- 🫁 lung cancer
- 🍈 breast cancer
- 👻 malignant melanoma
#1 in:
- Trauma
- bone tumor suspected
- fracture line (dark)
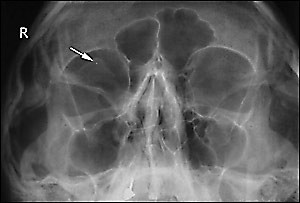
- opcities in sinuses? (indirect sign of fx)
- Soft tissue changes?
Acute: hyperdense = white (fresh blood)
days - 1 month = Subacute: Isodense
> 1 m. Chronic: hypodense = dark (w/ time loses its density d/t breakdown of hemoglobin)
- between dura & skull
- arterial bleeding (middle meningeal a.)
- bi-convex (lemon shaped) (contained within sutures)
- Mass effect (midline shift + compression of ventricles)
dural attachments/reflections:

- if contains air → mastoid / sinus fracture
- swirl sign if active extravasation of blood 📷⇒ immediate surgery!

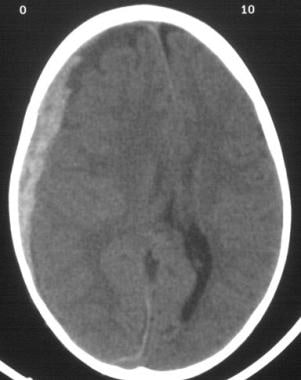
- between dura & arachnoid mater
- venous bleeding (cortical bridging veins)
- concave/crescent shape (concavity towards parenchyma) (not bound by sutures)
- midlineshift + compression of ventricles (might lead to brain herniation)
- crosses sutures
- Ø cross dural reflections (stops there)
- +/- underlying intra-parenchymal + interventricular bleeding
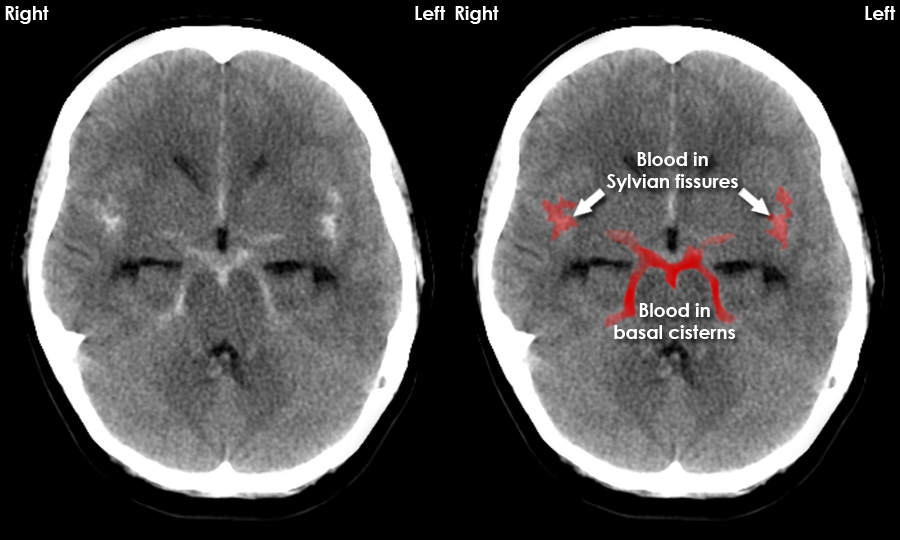
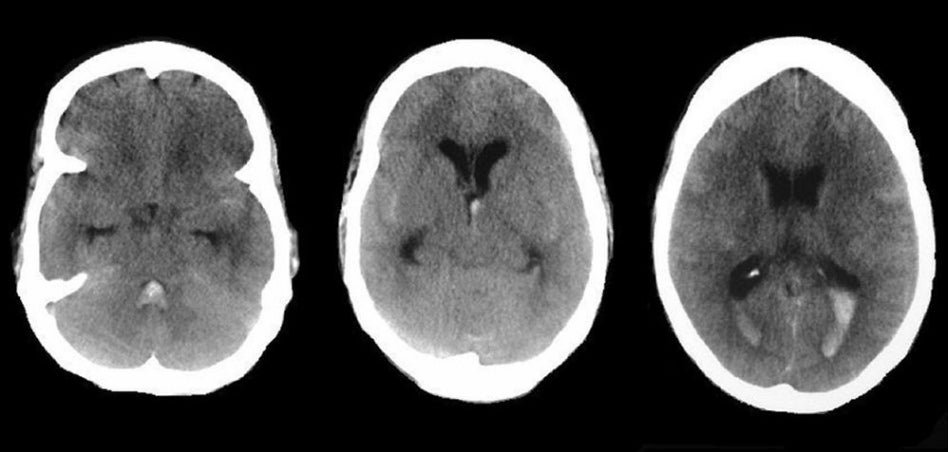
- within subarachnoid space (between arachnoid & pia mater)
- aterial bleeding
- blood within cisterns, sulci, ventricles
- hyperdense falx cerebri
- Etiology: aneurysm, trauma (subarachnoid a. damage or extension)
ANGIO (CT / MRI)
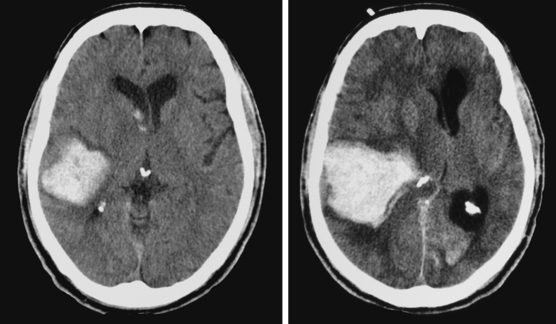
Intraparenchymal Hemorrhage/Hemorrhagic Stroke
- hyperdense accumulation within parenchyma (fresh blood)
- hypodense halo (perilesional vasogenic edema)
- not respecting vascular territory
- mass effect → midline shift + ventricle compr. + brainstem herniation
- compression of sulci/not visible anymore (edema)
- +/- intra-ventricular (ventricular flooding due to BBB disruption)
- resorption or lacuna (intense black “CSF-like”)

Feature | CT | MRI |
Contour of the disk | ++++ | +++ |
Hydration of the disk | + | ++++ |
Contour of the dural sac | ++ | +++ |
Contents of the dural sac | - | ++++ |
Nerve roots | +++ | +++ |
Bones | ++++ | ++ |
Para-vertebral regions | +++ | +++ |
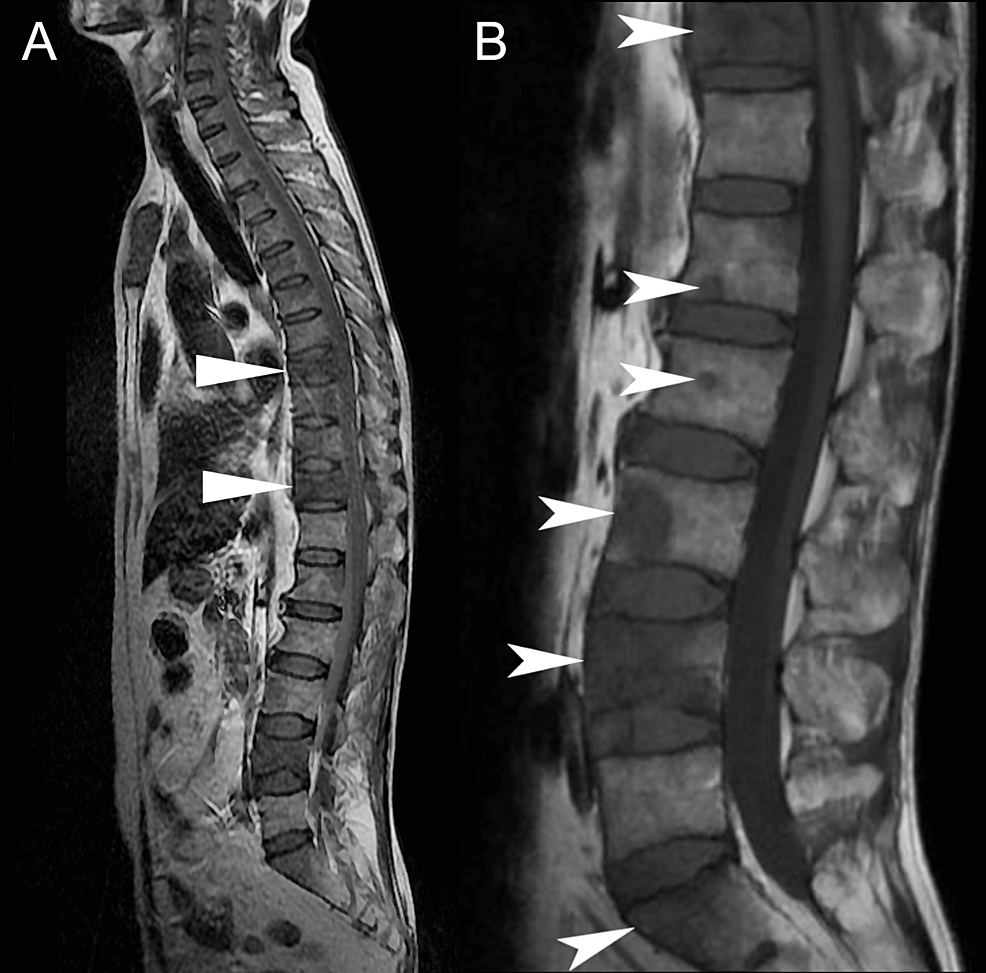
- post. displacement of IVD
- protrusion into spinal canal
- multiple lesion spread over entire column
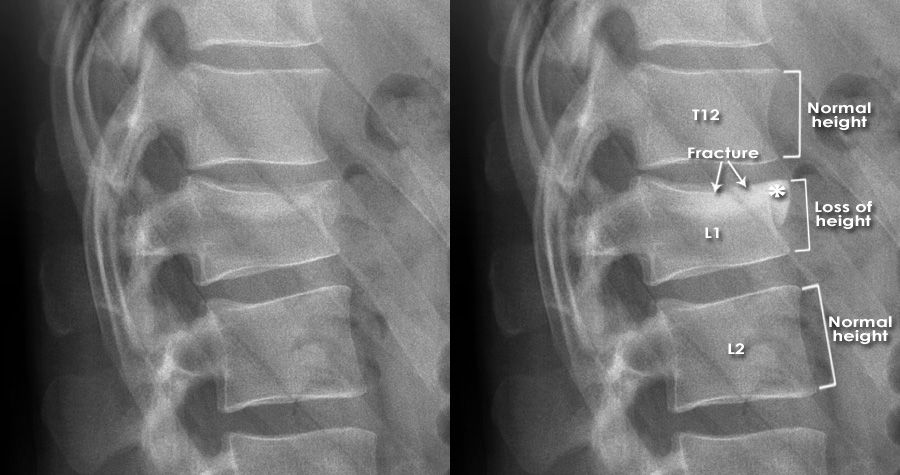
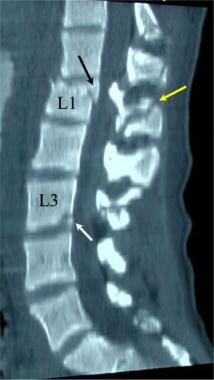
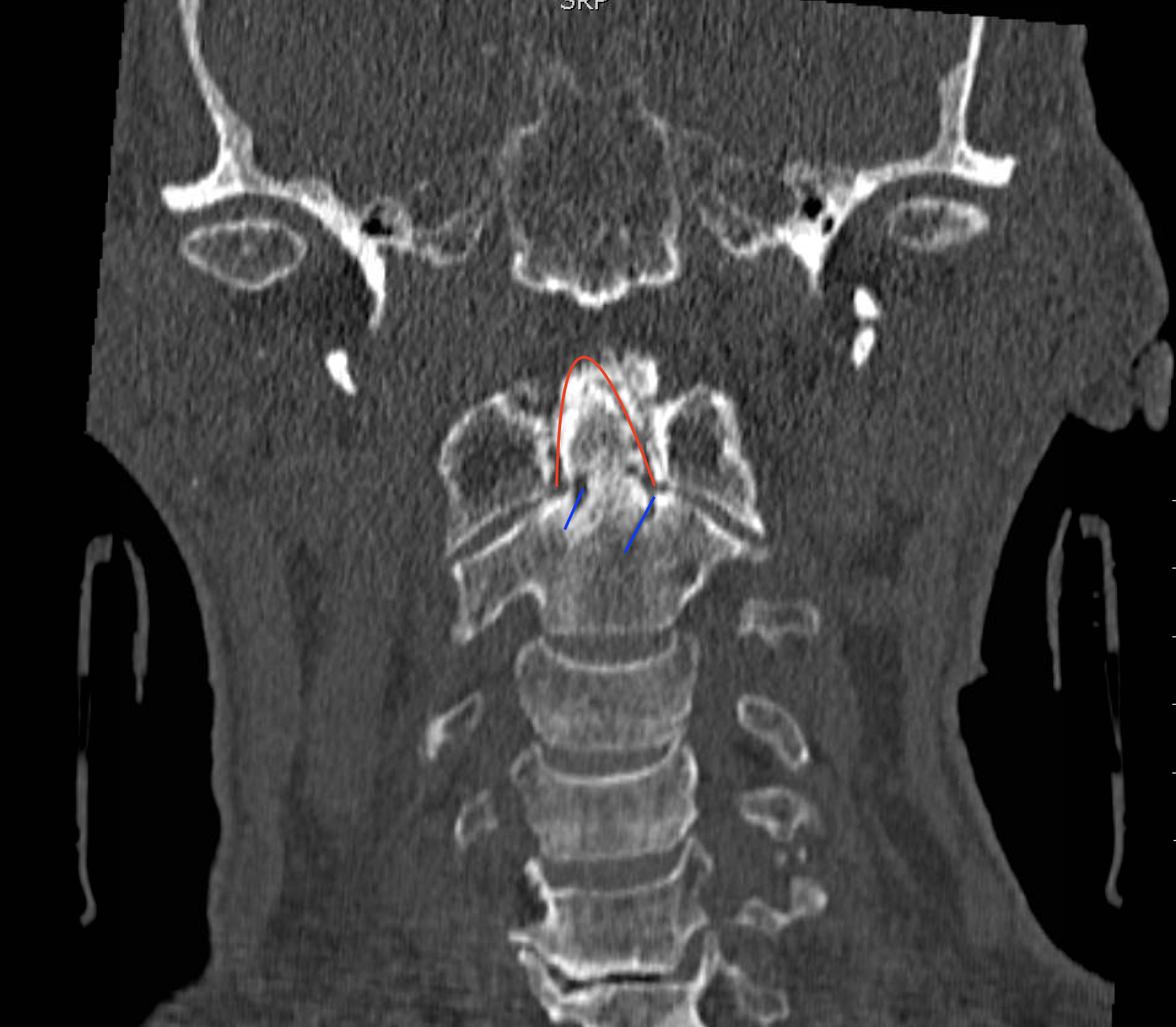
- compression fractures
- loss of height in the middle dimension (vertebral body)
- → height alteration of intravertebral space
- disrupted continuity of ant. line along vertebral bodies (missalignment)
- post. surface intact
- anterior wedging of the vertebral body

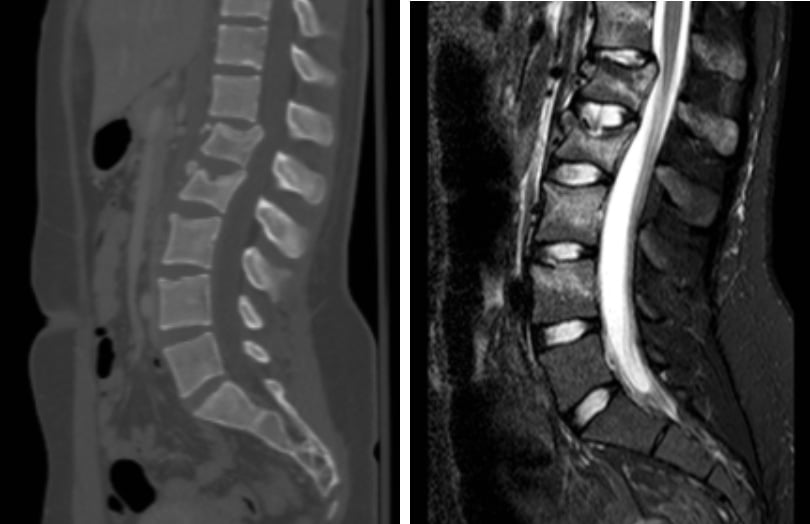
- Xray (bone lesion?)
- CT (bone lesion? fresh blood? compression: dura/spinal cord/ root?)
- MRI ( spinal cord? (compression/section/contusion) dural sac? disk? meninges? extradural hematoma?)
🚑 Emergencies
- US → FAST
- Xray → slight doubts → CT
- EXAMINATION OF CHOICE IS ALWAYS CT
4-9
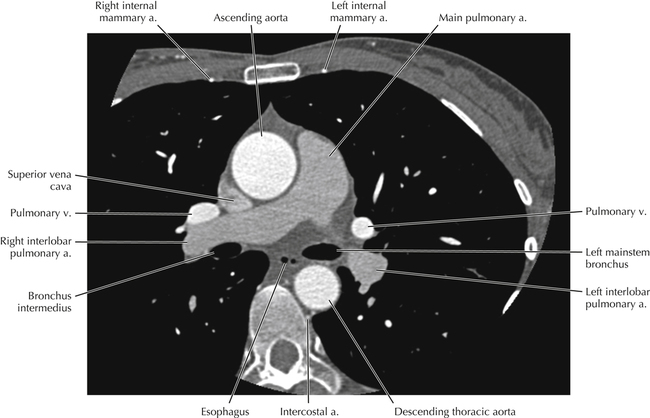
Trachea + Vessels
abdominal organs
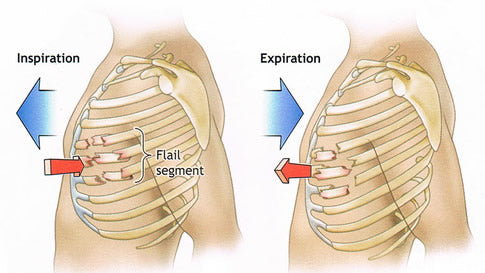
Flail chest or flail thoracic segment occurs when 3 or more contiguous ribs are fractured in 2 or more places. The fractured segment will sink into the chest with inspiration and expand out of the chest wall with expiration opposite to the normal chest wall movement.
in lecture it say 2 or more ribs (??)
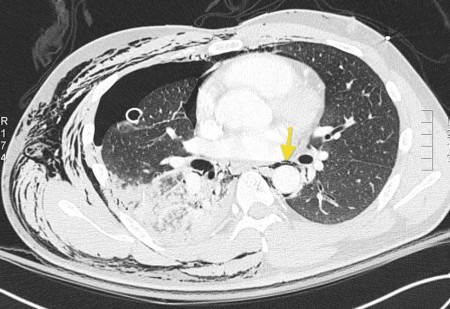
- Pneumothorax
- Hydropneumothorax
- Hemothorax

2-3d ; severe up to 14


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Pneumothorax (non-traumatic)
- Cardiogenic
- Hydrostatic (renal, hyperhydration)
- ARDS (↑capillary permeability)
- inflammation (chemical/allergic)
- Airspace-filling syndrome (see above)
- Central “bat wing” 📷
- Non-systemized (across fisures)
- Signs of atelectasis (consolidation, ↓lung volume, segment collapse)
- If expiratory valve (ball valve) →hyperinflation
- Infectious spread → Pleura + Neck
- Esophagus perforation
- Fatty stranding + edema: ↑density
- fluid collections
- w/ air inclusion → air fluid levels
- Maxillary (Le fort 1-3)
- Mandibular
- Nasal bone
- Infraorbital
- Zygomatic (malar)
→ see above
- intra-axial ⇒ intrapranchymal ⇒ blunt traumatic = cortical contusion
- extra-ax ⇒ outside of parenchyma (Epidural, subdural, subarachnoid+ventricular)
Intra-axial hemorrhage aka in CORTICAL CONTUSION
frontal + temporal
→ “glide” over rough surface of skull base
depressed fx
- Hemorrhage → necrosis phase (white)
- Resorption + Organization phase (iso)
- Defect stage (containing CSF - black)
- Aneurysmal subarachnoid hemorrhage (see above)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
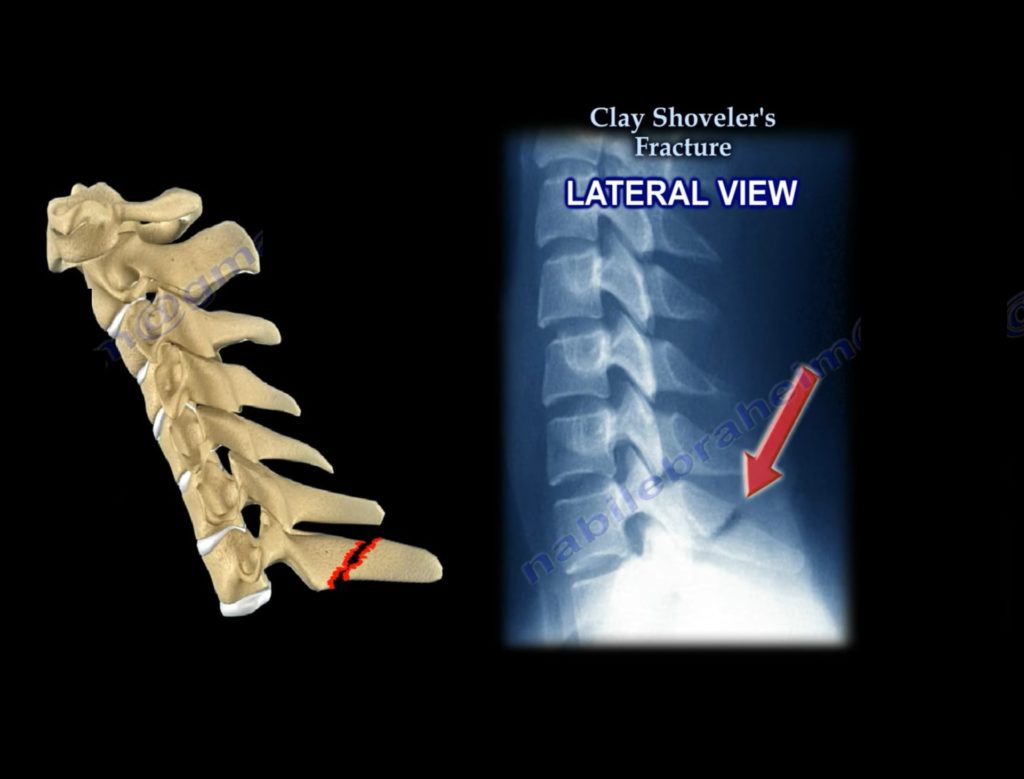
→ Chance fx 📷
{kind=link}