
Table of content
- Nephrology
- 🧶 Glomerular syndromes
- 🥇 Primary glomerular diseases
- 🥈 Secondary glomerular diseases
- 🚇 Tubulo-intestinal kidney disease
- 🩸Vascular nephropathies
- 💥 Acute renal injury
- 🕰️ Chronic renal injury
- 🔁 Renal replacement therapy
- 💧 Hydro-electrolytic disturbances
- 🧪 Acid-base disturbances
- 🧬 Hereditary Nephropathies
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Nephrology
🥇Albumin(most abundant), 🥈Globulins, 🥉fibrinogen(least abundant)
γ > β > α
→ “The lightest globulins are the alpha globulins, which typically have molecular weights of around 93 kDa, while the heaviest class of globulins are the gamma globulins, which typically weigh about 1193 kDa”
number of pores ↑, size doesn't
⇒ only albumin starts leaking because it’s the smallest plasma proteins, globulins dont leak→ only albuminuria
size of pores increases, +/- number
albumin + globulins leak
α → HDL + Lipoprotein a
β → VLDL, LDL, IDL
3,5g/24h → that's why only at that threshhold edema develops due to hypoalbuminemia
(proteinuria below 3,5g/24h is called sub-nephrotic range proteinuria, ≥3,5g/24h is called nephrotic range proteinuria)
hydrostatic → fluid pressure that want's to leave capillary
colloid osmotic/oncotic pressure: pressure gradient exerted by the plasma proteins (esp. albumin) that pulls/keeps fluid into the capillary
⇒ pitting edema due to low oncotic p or high hydrostatic p (HT)

lymphatics blocked
normal oncotic + hydrostatic p
edema is made out of fluid and proteins: lymphatics usually drain a small amount of plasma proteins which are drawn into the intestitium together with the fluid that is pushed into the interstitium by the hydrostatic pressure → non-pitting edema
edema due to low oncotic or high hydrostatic p only made out of fluid and no proteins
HSR I: reaction of antigen/allergen with IgE on mastcell, may lead to anaphylaxis
HSR II: reaction of IgG or IgM with Ag at a fixed place = immune-complex formation in situ
HSR III: reaction of igG or igM with Ag in circulation = ICF in circulation —> then deposition in severeal possible places
⇒ Type II + III may lead to Gl.Nephritis (Ag either intrinsic, planted and Ab will reach the side and form IC or ICF within circulation then get planted in glomerulus
Type II HSR
Megalin (in the pits inbetween the footprocesses of the podocytes)
Collagen type IV (basement membrane) - Anti-GBM (Good-Pasteur)
e.g. against mesangial cells, endothelial cells or podocytes
injured cells produce substances (ROS, proteases, etc.) that damage the glomerulus
e.g. minimal change disease (see below)
Autoantibodies against Properdin ⇒ overstimulization of alternative complement pathway
Properdin ist ein Gammaglobulin, das eine wichtige Rolle bei der Steuerung des Komplementsystems spielt. Es stabilisiert die Proteasen der alternativen Komplementaktivierung. Es erfüllt Aufgaben im Rahmen der Immunabwehr, indem es die Phagozytose beeinflusst. Das Protein fördert die Anlagerung von Komplementfaktor C3b an Faktor B und unterstützt das Assembly von C3bBb.
activation of classic complement pathway → formation of membrane attach complexes (MAC) = "b-parts" → cell lysis
C3a + C5a → activation mastcells and release of reactive component (PG, Platelet activating factor, ROS, Lysosome enzymes, leukotriens)
C5a → attraction of Neutrophils and release of reactive component (PG, Platelet activating factor, ROS, Lysosome enzymes, leukotriens, IL, TNF) → activtion of Macrophages → more reactive substances and further cell damage
Thrombos → Microthrombi → ischemic events
Mesengial cells will produce reactive substances too (ROS, PG, Leukotriens)
Growth factor production by mesengial cells, macrophages and Lymphocytes → excessive proliferation of mesengial cells → compression of glomerular capillaries
diffuse = all glomeruli are involved
focal = <50% glomeruli are involved, but others are not
global: the whole glomerulus is affected
segmental: <50% of the glomerular tuft is affected
hypercellularity due to immune cells / proliferating cells (due to damage)
- Proteinuria >3,5g/24h
- Hypoalbuminemia <3g (+/- hypoproteinemia <6g/dl)
- Edema
normal serum albumin is 3,5 - 5,4 g/dl
↓ albumin → efflux water into interstitium → ↓ blood V → RAAS activation 📷
→Renin → activation Angiotensin → increased hydrostaic pressure
→ Aldosteron: Na + H2O retention
→ More fluid eflux out of vessels
→ hyperosmolarity (Na etc) of blood → triggers ADH → more H2O retention → more water efflux
edema is not caused by incr. hydrostatic capillary pressure but by low oncotic pressure → edema is not gravity dependend
👁️ peri-orbital (= loose tissue) → fluid efflux in the loose tissue doesn't ↑ the local pressure first → more fluid can accumulate
Periorbital (albumin-related edema doesn't follow gravity)
↓
Peripheral pitting
Pleural/Pericardial effusion + ascites
↓
Anasarca = generalized edema
- hyperlipidemia/dylipidema + xanthoma/xanthelasma, (+lipiduria arterioscleorsis+CAD risk)
- hypercoagulable state → increased risk of thrombosis
- Incr. susceptibility to infections
- Frothy urine (foam on beer 🍺)
- hypocalcemia + anemia→ in chronic stages
- symptoms of underlying diseases (e.g. malar rash in lupus)
- hyperlipid → compensatory synthesis by liver to restore normal oncotic pressure + urinary loss of lypolysis enzymes
- hypercoagulation/thrombosis → urinary loss antithrombin III/protein C+S + hepatic synth. of procoagulant factors due to compensation + coagulations-cascade-activation due to glomeruli mediated lesions
- infections → urinary loss of IgG, reduced complement activity, complement urine loss, reduced Tcell function + proteins malnutrition(due to loss)
- Hypocalcemia → due to Vit-D deciciency → incr. PTH → incr. bone resorption
- Anemia due to loss of transferrin + less EPO
F - Azotemia and hypertension are uncommon initially, but their presence may indicate advanced disease
Hematuria might also be present
minimal change, focal segmental glomerulosclerosis, membranous nephropathy
can manifest as nephrotic or nephritic sy., like diffuse proliferative GN (in lupus)
minimal change
FSGS
focal segmental glomerulosclerosis
Membranous nephropathy (MN)
most common etiology depends on age:
Children | Minimal change |
Young adults | MN |
Old adults | FSGS |
Diabetic nephropathy, amyloid np., lupus nephritis + diffuse proliferative GN
lupus can also manifest as nephritic synd.
qualitative: urine dipstick
quantitative: 24-hours urine protein evaluation
hematuria

hematuria with acanthocytes + RBC cast

FSGS + membranous nephropathy
🤡 hemoconcentration due to plasma volume loss
secondary cause of nephrotic syndrome (e.g., SLE, other inflammatory conditions, or malignancy).
ATIII, proteins S, plasminogen → decreased antithrombotic factors (urinary losses)
fibrinogen, d-dimer→ increased procoagulant factors (compens. synthesis)
LDL, TG → increased (compens. synthesis)
decr in chonic → no activation by the kidney
incr. ESR + CRP, WBC may suggest underlying infection, inflammatory condition, or vasculitis.
see etiologies below
Immunological screening:
- ANA, anti-dsDNA
- C3, C4
- ANCA
- rheumatoid factors
- ASLO (antistreptolysin O)
- no secondary cause found
- also in lupus to differentiate the types
- advanced CKD → fibrotic tissue on → biopsy doesn't give good tissue
- hyperechogenic small kidney on US <9cm
- severe uncontrollable HT
- uncontrollable bleeding diathesis (Neigung)
- Infection: Hydronephrosis, bilateral cysts, acitve renal/perirenal infection
- solitary kidney
sodium + fluid restriction
diuretics (furosemid = first line)
consider i.v. albumin
RAAS inhibitation: ACEI (ramipril) or ARB (losartan)
- AKI, aprupt onset of NS (like minimal change)
- hyperkalemia
not to much, not to little
Patients with nephrotic syndrome are at risk of protein malnutrition. While lowering dietary protein intake can lead to a reduction in proteinuria, very low-protein diets should be avoided because of the increased risk of malnutrition. High protein intake may help offset urinary protein loss, but very high-protein diets are discouraged because of the risk of worsening proteinuria.
usually resolves after treatment of underlying cause + reduction of proteinuria
→ Lipid lowering therapy: Statins (eg. atorvastation)
3.0 g/L
prophylactic anticoagulation (e.g. heparin)
- vaccination → influenz + pneumococcal
- consider AB-therapy
- Sodium + fluid restriction
- Diuretics
- RAAS-inhib (ARB , ACEI)
- Statins
- Anticoagulation
additional: i.v. albumin, protein diet, vaccines
see etiologies below
artherosclerotic complication → MI, stroke
FSGS + membranous nephropathy
increased size (+/- number)→ non-selective proteinuria + hematuria
glomerular inflammation → GBM disruption
inflammated glomeruli swell up (inflammatory infiltrate, clots,..) → less blood flow to the kidney → decr. GFR
- Hematuria with acanthocytes
- RBC casts
- Hypertension → mild to moderate Edema + oliguria
- Renal insufficiency (decr. GFR): esp. Azotemia + Crea (+ anemia)
- Oliguria: inflammatory infiltrates reduce fluid movement across the membrane (↓ GFR) → oliguria + pyuria (leukocyturia)
- mild - moderate Proteinuria <3,5g/24h
A type of dysmorphic red blood cell characterized by irregular, thorn-like cytoplasmic projections.
RBC are stuck inside tubules 📷 → increase pressure from the fluid → get compressed with proteins
decreased GFR →less water excretion
→ activation RAAS due to less effective volume+Na reaching macula dense
→ Angiotensin → incr. BP
→ Aldosteron → water + sodium retention
GFR is reduced → you cant piss out se proteins
Possible development into Nephritic syndrome → Check for hematuria+ acanthocytes, RBC cast , Azotemia!
OR due to renal failure
attraction of macrophages + cytokines
stimulation epithelial cells → growth factor
⇒ extreme cellular proliferation in urinary space ⇒ cellular crescent ⇒ rapidly progressive GN ⇒ rapid renal failure + Uremia
post-streptococcal / post-infectious GN
IgA Nephropathy (Berger disease)
= Rapidly progressive GN
- Goodpasture
- Small vessel vasculitis
- immune complex mediated diseases (like Lupus, IgA nephropathy, post-strep GN)
→ more details RPGN
Alport
- All causes for RPGN
- Lupus
- Alport
→ dont forget about Lupus which can manifest as diffuse proliferative GN
Nephritic sediment:
- Hematuria + acanthocytes
- RBC cast
- Mild to moderate proteinuria
- sterile pyuria +/- WBC
- no RBC cast + acathocytes
bright red or pink urine, the occurrence of blood clots, normal RBC morphology, and the absence of RBC casts.
- high Crea (low GFR)
- Azotemia with inc. BUN
- Specific: Complement, ANA, ANCA, anti-GBM etc
- when nonspecific disease pattern to confirm diagnosis
- lupus - classification
ACE-I or ARB
diuretics
Low sodium diet + water restrictrion
immunosuppression
plasmapheresis to remove antibodies
dialysis, transplantation
🥇 Primary glomerular diseases
Non-proliferative
typically nephrotic syndrome
- child 4-8y
- heavy proteinuria + edema
normal
steroids
excellent herr specht wenn du treatest
ofc, makes 10-20% of adult nephrotic syndrome, but in the exam its gonna be child for sure ;)
reabsorbed lipoproteins → lipid accumulation
(hence the term "lipoid nephrosis" as a synonym of minimal change d.)
idiopathic / primary
NSAID, penicilliam, lithium
Hodkin's lymphoma → inc. cytokines
- allergy (sting 🐝 🦂 , vaccination)
- malignancies: lymphoma, leukemia, tumor
abnormal T-cells are activated due to previous infection (e.g. upper resp. trakt) → production of cytokines
→ damage of the footprocesses → effacement of the podocyte + structural changes of slit diaphragm
→ less polyanions (negative charges) are produced → albuminuria (negative charge + small) = selective proteinuria (bigger immunoglobulins can't pass)
- pure nephrotic syndrome (no nephritic sediment)
- Sudden onset selective proteinuria + renal edema
- normal renal function (GFR, Crea, Urea normal)
children 1-12 → MCD should be presumed if no other suspicion
- adults
- children with: concomitant nephritic syndrome, RF, steroid resistance (no response after 8 week)
Electronmicroscopy
(IF negative, light microscopy show nothing)
all normal/no findings
diffuse loss and effacement of foot processes
- non-specific treatment for nephrotic syndrome
- Corticosteroids
- Etiology if secondary
1mg/kg predni / 24h ; 3-4month → progressively less 6month ⇒ lower relapse + avoid adrenal suppression
relapse
remission→30days continued at same dose→lower dose progressively
→ in total 3month
- frequent relapse >4x/year
- steroid dependent → relapse when decr dosage or after therapy
- steroid resistance→ no response after 8 weeks
⇒ Immunsupressiva:
Cyclophosphamide → Eliminierung regulatorischer T-Zellen und Inhibition von T-Zell-Wachstumsfaktoren
or Cyclosporin → inhibits cytokine synthesis
Mycophenolat
wirkt als Inhibitor der Inosinmonophosphat-Dehydrogenase (IMPDH) und hemmt dadurch die Synthese von Guanosin.
B- und T-Lymphozyten sind in ihrem Wachstumsprozess aber auf eben diese Nukleotide (wie Guanosin) angewiesen. Dadurch sinkt deren Gehalt stark ab und eine effektive Immunreaktion ist unmöglich.
high mortality rate! → Infection + thromboembolism
>80%, 1-2 years
more than half!
- podocyte injury → scarring → proteinuria → progressive chronic kidney disease
4% total ESRD
most common prim.GN cause of ESRD
- idiopathic - probably due to circulating permeability factors
- genetic - mutation in specific podocyte genes
- Viral infections (HIV, HepC, EBV, CMV)
- Drug-induced (Heroin, anabolic steroids)
- Adaptive due to:
- reflux nephropath, any advanced renal disease
- vascular abnormalities (hypertension, thrombus, stenosis, microangiopathies..)
- Obesity
IDIOPATHIC → prop. circulating permeability factors → podocyte lesion
dysfunction
detachment
foot process effacement
→ parietel cell cover GBM
→ synechia (cellular adhesion of Bowman's capsule with tuft)

→ hyalinosis 📷 + sclerosis
nope → some progressive bullshit
nephrotic syndrome
RF
HT,
proteinuria (subnephrotic)
obesetity related,
nephritic with hematuria
Biopsy
focal + segmental distribution of hyalinosis + sclerosis lesions (Terminology - what does focal segmental mean?)
- Perihilar variant = Perihilar sclerosis and hyalinosis; adaptive FSGS
- Tip lesion variant = Tip lesion alone; in idiopathic FSGS, in Caucasian patients, has best prognosis
- Collapsing variant = Collapse and extracapillary visceral epithelial hypercellularity; has the worst progression rate to ESRD
- Cellular variant = Endocapillary hypercellularity
- NOS (not otherwise specified) variant - most common variant.
diffuse effacement of footprocesses
patchy effacement
false negative → only biopsy of areas without abnormalities → >15 glomeruli!
primary → generally good response to immunosupressive (esp. glucocorticoids) + RAAS
secondary → symptomatic + etiological treatment → ACEI/ARB (decr. glomerular pressure)
- ACEI / ARB
- sodium restriction
Predni
ACEI + ARB
Cyclosporin
mycophenolate, rituximab
depends in etiology
ACEI + ARB
statins
sodium restriction
underlying etiology
75% → very poor prognosis
50%
30% recurrence after (esp. primary idiopathic!)
→ give immunosupression!!
GBM thickening in response to igG + complement deposition
→ no cellular proliferation!
highest, 30%
FSGS 25%
MCD 13%
middle-aged + elderly males
- Anti-PLA2R
- Anti-Thrombospondin (THSD7A)
- Anti-Neutral endopeptidase
MAID 👧
Malignancies (CA, Lymphoma, Leukemia)
Autoimmune (Lupus etc.)
Infections (HepC+B; HIV, siphilis, parasites)
Drugs/Toxins (NSAID, penicillamin, lithium, Captopril(ACEI)
linked to active disease + risk for renal failure
pretty certain
high specificity
75%
immunosupressive therapy might cause worsening if the etiology is an infection or cancer
cancer-associated MN has usually no tumor symptoms 🤓
Lung, prostate, digestive
PLA2R, THSD7A, neutral endopeptidase
- nephrotic syndrome presentation
- evtl. hematura + HT
normal at presentation → may develop into CKD
Anti-PLA2R
thickening GBM / capillary loops
no cellular proliferation, excudation or necrosis
(spike - dome pattern: subepithelial deposits seperated by BM projections → can be seen better in EM)
global, diffuse, granular (spincled) pattern of IgG + complement along subepithelial GBM; (epithelial side)
- CV-events → thrombolism, renal vein thrombosis, Pulmonary emoblism
- Chronic KD progression
albumin levels → low albumin = high risk
PE: ≤4g/24h
CC normal for 6 month
PE: 4-8g/24h for >6month
CC: (near) normal for 6-12month
PE: >8g/24h for 3 month
and/OR CC reduces over 3 month
nonspecific + prophylactic anticoagulation
+/- immunosupression → depends on severity
Corticosteroids + cylclophosphamide
nonspecific NS:
ACEI or ARB
Statins
for 6 month
immunosupression
non-remitted after 6 month
severe symtpoms
progressive renal insufficiency
GFR<30 + evidence of sclerosis
- Ponticelli: monthly alternation steroids + cyclophosphamide
- other immune supressive
- Calcineurin inhibitors (cyclosporin)
- Rituximab
- Mycophenolate
DM, Myelotoxicity, infections, cancer
nephrotoxicity!
B-cells
at least as effective in remission as ponticelli
very good → progressive renal insufficiency only 10%
30% my friend
GFR + Albuminuria
- severe chronic proteinuria
- reduced GFR → further declining
Proliferative
typically nephritic syndrome
→ not relevant for exam
LM
immune complexes or complement factors
mesangium + capillary wall → mesengial proliferation + capillary wall remodeling
one of the least common types of GN
mainly in children
IMMUNERESPONSE TO CHRONIC ANTIGENS OR COMPLEMENT DYSREGULATION!
- system immune diseases (SLE,..)
- chronic infections (HCV,HCB,HIV)
- monoclonal gammopathies
- complement dysregulation
- Neoplasms (myeloma, lymphoma, leukemia)
- IG-mediated: SLE, monoclonal gammopathy, idiopathic, → usually both IgG + complement
- Complement-mediated: dense deposit diseases, igG (nephritic factor) that stabilized C3 convertase → activation + depletion + deposition in BM
→ Both can occour: Infectious, Tumors, SLE, hereditary disease (sickle-c) → We still talk about type 1 if we have immune-complexes AND complement subendothelial
[3. Immune-complexes + complement subendo + subepith.]
mesangium and glomerular subendothelial space
- most common nephritic sy, severe forms can be nephrotic sy
- also only microscopic hematuria or mild proteinuria possible
- severe GN with HT + reduced GFR possible too
⇒ very broad spectrum → microscopy is important
ESP. C3 IN ALL CASES
look for specific markers for secondary causes! (infections, SLE,...)
- diffuse cellular proliferation ( mesengial + endothelial + Monocytes)
- lobular appearance of the tuft + thick capillary walls
⇒ evtl. tram-track-appearance
black arrow = duplication of GBM (tram track)
LM (silver stain) + EM
Mesengial interpositions between endothelium + GBM → replication of GBM → double outline in silver stain
stains IG + complement (both positive)
→ esp. in viral, monoclonal gammopathy, or autoimmune
Yes
antiphosphlipid syndrome
healing phase of uremic syndrome
scleroderma
transplant glomerulopathy
Underlying cause → differentiation of type 1 + 2 can help, to evaluate appropriate therapy
- RAAS inhibitor if mild (non-nephrotic proteinuria, normal crea + BP)
- Predni if nephrotic or renal insuff
- Cyclophosphamide + low dose predni if rapidly progressive renal diseases
- alternative: Mycofenoplate + Rituximab
- nephrotic syndrome
- ↑Crea
- ↓GFR
- HT at presentation
- crescents (due to ruptured GBM!)
mainly nephritic
(nephrotic sydrome → rare)
Berger disease
very low
20% of all ESRD!
Pentru ca very high prevalence → most common primary GN
- The cause is still not entirely understood.
- Most likely mechanism: increased number of defective, circulating IgA antibodies are synthesized (often triggered by mucosal infections, i.e., upper respiratory tract and gastrointestinal infections) -> IgA antibodies form immune complexes that deposit in the kidney -> glomerulonephritis (typeIII hypersensitivity reaction)
- inflammations:
- Cirrhosis
- GI (inflammatory bowel)
- Psoriasis
- Immune (ankylosing spondylitis)
- infectious (HIV, Hep b+c)
- malignancies
- Incr. synthesis of abnormal IgA due to Glactose deficient IgA1)
- reduced clearance
→ aggregation + mesangial trapping
→ Anti-glycan antibodies against IgA → ICF in mesengium
→ Cytokines, mesangial proliferation → Complement activation
→ RIP
yes, has been demonstrated in at least some cases
occurs within 2 days of a febrile mucosal illness!
DD: Post-streptococcal GN → 10-20 days after infection(esp. tonsillitis)
- Assymptomatic → only change in laboratory parameters (e.g. microscopic hematuria+proteinuria→ can already have decr. renal function at presentation
- Reccurent episodes of:
- Macroscopic hematuria
- flank pain
- fever (usually low grade)
- Nephritic syndrome
- → esp. in relation to infection (GI + respir.)
- esp. in children
- Can progress to RPGN and/or nephrotic syn. (10% of patients)
- ARF with macroscopic hematuria
- 50% → develop ESRD within 20-25years
- Post-streptococcal → low C3,C4 10-20days post infections
- Lupus → low C3,C4, dsDNA, ANA
- MPGN
⇒ in IgA C3 usually normal because its not activated that extremly
Normal or MEST-C
- normal glomerulus
- Mesengial hypercellularity → assymptomatic
- Endocapillary hypercellularitý → acute GN
- Segmental glomerulosclerosis- chronic GN or ESRD
- Tubular atrophy + interstitial fibrosis
- Crescents → RPGN (crescent in 1/3 but only 5% have ≥50% crescent (to classify for RPGN))
mesengial diffuse global deposits of IgA 📷
→ Aim: reduce proteinuria, symptoms + complications
- ACEI/ARB for 3-6 month → ↓Proteinuria + ↓BP
- tonsillectomy if reccurrent
- (Statins → ↓cholesterol)
if RAAS-inhibit shows no improvement after 6month
- persistant proteinuria >1g/day after 6 month of ACEI
- Nephrotic syn + GFR >50
- Esp. budesonide
Immunsupressiva!
Predni for 3 days → then monthly i.v. cyclophosmaide for 6 month → maintenance treatment with azathiprine
Calcineurine inhibotrs (cyclosporin) + Rituximab
Renal replacement therapy / kidney transplantation in ESRD
Yes, but slow progression also nicht so schlimm lel
varies widely
1/3 → complete remission
1/3 → benign chronic persistant hematuria + proteinuria <1g/24h
1/3 → progressive decline in GFR → ESRD in 20years
HT
How bad is the proteinuria?
Inital renal function impairment
don't forget about the genetic IgA-NP
IgA in small vessels (capillary, venules, arterioles)
Same as IgA NP
in most cases symptomatic
→ renal manifestations same as IgA NP
🥈 Secondary glomerular diseases
biopsy
skin, joints, MSK, heart, lungs, NS, any other..
SLICC classification 📷 [Systemic lupus international collaborating clinics]
- 4 out of 17
- at least one out of each group
biopsy + ANA or dsDNA pos.
80%
20-60%
Tubulointerstitial disease + Vascular diseases (thrombotic microangiopathy)
jap
- complement activation
- leucocytes infiltration, cytokines, procoagulant factors
= infiltration + proliferation → inflammatory glomerular disease
Glomerular injury, but no inflammation 🤡
any of..
- persistent proteinuria (>3+ dipstick, >0,5g/day)
- active urinary sediment (RBC cast)
- Hypocomplementemia
- ANA, anti-dsDNA, Anti-Sm
biopsy
Antiphospholipid syndrome 📷 → Thrombotic prhoylaxis
full house pattern (igG/A/M, C3, C4, C1q) in mesangium, capillary loop, tubules
minimal mesangial
mesangial proliferative
Focal + diffuse lupus nephritis
Mesangial + subendothelial
nephrotic
lupus membranous NP
subepithelial → see membranous NP
Advanced sclorsing
Sclerosis → bland sediment
minimal mesengial LN
mesengial
only in IF + EM
LM negativ
all normal
Mesangial proliferative LN
Hematuria and/or proteinuria
mesangial hypercellularity, matrix expansion
good👍🏽
Focal lupus nephritis
hematuria, proteinuria
nephrotic sy
HT
Renal insufficiency in 50%
active (proliferative)
chronic (sclerosing)
mixed
endo- or extracapillry GN with <50% of glomeruli affected
focal subendothelial + mesangial depositions
depends on severity
diffuse lupus nephritis
hematuria + proteinuria in all!
Nephrotic sy
HT
RF
→ most common type + severe
proliferative endo- + extracapillary proliferation >50% of glomeruli
segmental or global
active or chronic
poor (even treated might develop in ESRD)
Lupus membranos nephropathy
nephrotic sy (evtl. with HT + Hematuria)
diffuse thickening of capillary wall (+/- mesangial prolif) → see membranous NP
full house staining
EM → subepithelial depsits (evtl. some eubedothelial+mesangial)
Advanced sclerosing LN
global >90%
slowly progressive RI, proteinuria + bland sediment
Tubulointerstital lesions
- hypercellularity
- inflammatory infiltrate
- cellular crescent
- hyaline thrombi
- fibrinoid necrosis
- hematoxylin body
- glomerulosclerosis
- fibrotic crescent
- tubular atrophy
- interstital fibrosis
nonspecific - ACEI, ARB
if nephrotic syndrome → corticosteoroid or calcineurin inhib(cyclosporin)
- nonspecific
- Immunosuppressive:
- induction: corticosteroids + cyclophosmadie or mycofenolat mofetil (MMF)
- maintenance: corticosteroids + azathiprine or MMF
corticosteroids + immunosuppressive (cyclophosphamide, cyclosporin, MMF, azath) for 1-2 years
no immunosupression!
renal replacement in ESRD, transplantation when no sign of activity
- Hydroxyclorochine in any class (against onset, relapses, ESRD)
- NSAID in skin/joint involvement
- Plasmapheresis in RPRF-associated LN, anitphosphlipidic syndrome, hemolytic-uremic syndrome
like initial regimen
→ if resistance: Rituximab, etc.
high crea
HT
Nephrotic range proteinura
Anemia
Black, hispanic
Class IV, crescents + associated tubulinterstital
ANA, Anti-dsDNA, C3, C4, Proteinuria, urinary sediment, Crea, eGFR, biopsy
- acute nephritic syndrome →Acantocytes+RBC-casts, non-nephritic proteinuria
- glomeruloar crescent formation with progression to renal failure within weeks to month ⇒ ACUTE RENAL FAILURE

≥2 layers of proliferating cells in Bowman's space
- proliferation of epitelial cells (parietal)
- Mp
= cellular crescent
- fibrinoid necrosis of the capillaries

= fibro-cellular crescent
Types:
- Anti-GBM-mediated: Goodpasture
- Immune complex mediated: Lupus, IgA nephropathy, post-strep GN [LAP]
- Pauci-Immune:
→ igG linear pattern along GBM

→ granular complement deposition in capillary wall 📷
systemic small vessel vasculitides including: microscopic polyangiitis, eosinophilic granulomatosis with polyangiitis (EGPA), and granulomatosis with polyangiitis (GPA)
→negative/little immunofluorescence pattern
in all types → crescent formation 📷
- poor prognosis (if untreated)
- Tx:
- Anticoagulation
- Plasmapheresis + Immunosuppressants
- Dialysis
- Transplant
- poor prognosis
- behaves like Anti-GBM ealry
- relapses like ANCA-vasculitis
Pulmonary-renal syndrome (Anti-GBM + Anti-ABM)
can be also isolated
general: 60-70y
also: young in their late 20
Collagen Type IV
(noncollagenous domain of alpha3-chain)
Injury of the GBM → necrosis, inflammation + proliferation of epith. cells in bowmann's space → sclerosis
→ More intense + rapid/sudden
- explosive hemoptysis
- dyspnoe
- hematuria
- drop in Hb
non-nephrotic proteinuria
nephritic sediment (acantho, RBCcast)
after upper respiratory infection
smoking + hydrocarbon (Kohlenwasserstoff)
biopsy
- Steroids
- Cyclophosamide
- Plasmapheresis
nope, no maintenance immunosupressive therapy indicated
- dialysis-depent patient
- 100% crescent + no pulmonary hemorrhage
worse if:
- >50% with advanced fibrosis → fibrocellular crescent
- Crea > 5-6
- Oliguria + acute dialyisis indication
→ see Lupus, IgA nephropathy, post-strep GN
antineutrophil cytoplasmasmic antibodies
unknown → probabaly genetic + environment
C-ANCA → proteinase 3 (PR3) → Wegeners: polyangitis with granulomatosis
P-ANCA → Myeloperoxidase (MPO) → Microscopic polyangitis
secondary hit
→ infections, silica exposre, etc. ⇒ Damage due to Np, Leu, alternate complement pathway
⇒ Any tissue and organ in the body.
”Signs and symptoms of necrotizing small vessel vasculitis are cutaneous purpura, nodules and ulcerations, anemia, peripheral neuropathy (mononeuritis multiplex), abdominal pain and blood in stool, hematuria, proteinuria and renal insufficiency, hemoptysis and pulmonary infiltrates or nodules, myalgias and arthralgias. In PR3-ANCA positive patients, upper respiratory tract symptoms (necrotizing hemorrhagic sinusitis, otitis media, cranial nerve entrapment, sub-glottic stenosis, nasal ulcers and crusting) can be present.”
crescent + fibrinoid necrosis in severe types
negative (type 3 - pauci)
- corticosteroids + cyclophosphamide
- plasmapheresis
- in PR3-ANCA/p-anca → better rituximab (instead of CP)
Azathioprine, (or alternative: MMF)
Corticosteroids + rituximab
CS + CP
>12month complete extrarenal remission
PR3/C-ANCA
lung diseases + hemoptysis
GN
ß-pleated sheet fibrillar proteins
proteases can only cleave alpha-structured proteins
→ ß-pleated proteins can't be removed → insoluble
→ accumulation → locally or widely(multiorgan failure)
from mild albumiuria - nephrotic syndrome
- chronic inflammation (AA) → incr. no. of Serum amyloid A (SAA)
- multiple myeloma (AL)→Abnormal plasma-cells → abnormal proteins → amyloidosis
- hereditary: esp. fibrinogen A-alpha mutation

alzheimer
congo red
amyloid P component

non-branching fibrils 📷
rare shit
yes in risk group:
cause for 17% of nephrotic syndrome in patients over 65y
MONOCLONAL GAMMOPATHY (esp. du to multiple myeloma 20%)
⇒ Free light chains (esp. Lambda, kappa)
GBM + Mesengium
become thick
→ tissue toxicity
multiple myeloma -syndrome
peri-orbital brusing (due to thrombocytopenia?)
macroglossia
edema
nephrotic syndrome
cardiac dysfunction
nerve abnormalities
- serum free light chain test - detects 98%
- Serum + urine proteins electophoresis
Serum amyloid P scintigraphy 📷

BIOPSY of:
bonemarrow, kidney, liver, fat, fums,..
ye, 80%
proteins - variable range
mild albuminuria - nephrotic syndrome
bland sediment
Bence-Jones proteins
- Fanconi Syndrome due to Bence-Jones proteins which obstruct the tubular lumen → NaK-pump insufficiency → resorption impared
⇒ renal tubular acidosis
ne nicht wirklich
- neg. for Ig + complement
- positive for lambda or kappa (not both simultaneously)
non-branching amyloid fibrils 📷
- classic nephrotic nonspecific (RAAS,diuretics)
- myeloma specific → chemo, stem cell transpl.
- RRT/transplant
- if myeloma → myeloma protocol (chemotherapy)
- Symptomatic (diuretics, Anti-Proteinuric agents(ACEI/ARB), dialysis)
- stem cell transplantation
- kidney transplantation
→ Election therapy: CyBorD
- cardiac (arrhythmias, blocks, failure)
- ESRD
- extra-renal manifestations:
- neuropathy
- carpal tunnel
- hepatomegaly
- macroglosia
- pulmonary infiltrations
- clotting abnormalty
“DER FETTE KRIECHENDE TUNNEL MENSCH”
only 30%
nephritic
- poststrep-GN
- infective endocarditis -relatedGN
- shunt nephritis
rare
children 6-10y
Strep + Staph
HIV, Hep B+C
Post-streptococcal GN
acute 10-20d
- Upper resp. tract infection, GAS (pyogenes)
- 1-4 weeks ago (DD: IgA NP - days after)
Blood:
- ↑ Anti-SLO
- ↓ C3
supportive/symptomatic treatment
- sodium + fluid restriction
- Loop diuretics (esp. when edema)
Give vasodilators
probably hyperternsive encephalopathy
- when other treatment doesn't correct the fluid overload
- Uremia → might develop uremic encephalopathy
corticosteroids (methylpredni)
Only in chronic, recurrent infections
Antibiotics , Antimicrobials
Alles entspannt, usually resolves within 6 weeks
Fluid overload leads to:
- Hypertensive encephalopathy
- Heart failure
- Pulmonary edema
nephritic syndrome lead to:
- ARF
- HbA1c ≥6,5 or
- fasting Glu >126 or
- Glu ≥200 at any time
- leads to sclerosis + fibrosis
- progressive albuminuria
→ HT + renal insuff
- other GN
- Neurogenic bladder (neuropathy) → obstruction
- UTI
- Vascular nephropathies
- Papillary necrosis
nephrotic
type 2 → 90%
hell yea, the most common
- genetic
- poor glycemic control
- HT
- Proteinuria
- low GFR
- Incr. Proteinintake
- metabolic syndrome (hyperlipid, obesity, smoking)
Chronic hyperglycemia → non-enzymatic glycosylation (NEG) of the basement membrane (protein glycation) → increased permeability and thickening of the basement membrane and stiffening of the efferent arteriole → hyperfiltration (increase in GFR) → increase in intraglomerular pressure → progressive glomerular hypertrophy, increase in renal size, and glomerular scarring (glomerulosclerosis), GBM thickening, mesangial matrix expensian, podocyte injury → worsening of filtration capacity
keine! 🤡praaaaank
- proteinuria esp. macroscopic/severely inc. albuminuria >300mg / 24h
- Renal edema
- HT
- RF → ESRD with uremic syndrome
microalbuminuria
30-300mg/24h
diabetes: crea + proteine increase at the same time.
if not increase at the same time ⇒ unlikely to be diabetes
albuminuria/24h ⇒ 30-300g/24h
albumin/crea ratio ⇒ 30-300mg/g
only when blood sugar levels are high
→ not related to diabetic nephropathy
nope, only levels over 300mg/day, → urinary exame might be normal, despite microalbuminuria
every year
albuminuria → albumin/crea ratio (when there is no infection present)
→ abnormal test ⇒ again in 3-6 month
- exercise
- fever
- UTI
- HT
→ if presentation with hematuria!
type 1 → 90%
type 2 → 60%
that it might NOT be diabetic nephropathy
- severely incr. albumin + bland urinary sediment OR
- moderatly increased albuminuria + retinopathy
noooo
- proteinuria in less than 5 years after DM-1 diagnosis
- no retinopathy in DM-1
- active urinary sediment (nephritic)
- ACUTE onset of RF/nephrotic sy → albumin >3,5g/24h (crea usually normal)
- clinic of another systemic disease
Check for secondary causes → blood test + antigens + antibodies, complement etc.
if nothing → idiopathic → biopsy
normal / incr. size
normal echogenicity of parenchyma (even in ESRD)
Class I: GBM thickening
Class II: Mesangial expansion
Class III: Kimmelstiel-Wilson=nodular intercapillary glomerulosclerosis (<50% of one glomerulus)
Class IV: Advanced sclerosis
glomerulosclerosis starts diffuse and than becomes nodular
Hyaline thickening of efferent and afferent arteriole → narrowing + vasdilation of afferent
⇒ Interglomerular hypertension
negativ OR non-specific linear IgG (low intensity)
- thickend GBM
- Mesanagial expansion
nephortic + chronic + diabetic specific management
- lifestyle → keine faules, fettes, ungesundes, rauchendes schwein mehr
- hyperglycemic control
- ACEI, Arb, Diuretics
- statins
- Low protein diet (0.8 g/kg/day)
- Treatment of anemia + hPTH
- planning RRT
- adjustment to GFR
- Metformin lactic acidosis in decr. GFR (better switch to insulin)
nope
10-12 ml/min/year

albuminuria severity
annual risk:
- No nephropathy - 1% risk of death; 2% risk to progress;
- Microalbuminuria-3% risk of death; 2,8% risk to progress; Macroalbuminuria - 5% risk of death; 2,3% risk to progress;
- ESRD- 19% risk of death.
arm wie n schwein
Prostate - PSA
Lung tumor - xray esp. in young
breast cancer
🚇 Tubulo-intestinal kidney disease
immune-mediated infammation → infiltrate in kidney intersititium → ARF
15%
- Drugs 75% - not necessarily nephrotox but hypersensitivity reaction
- Autoimmune (SLE, Sjögren syn)
- Systemic Infections (CMV,EBV,Legionella,Strep)
- TIN with uveitis syndrome (TINU syndrome) 📷
TINU syndrome • TINU (Tubulolnterstitial Nephritis + Uveitis) • First described in 1975, by Dobrin • More than 150 cases were reported Pathogenesis • Unknown • Renal tubular & ciliary body epithelia: electrolyte transporters sensitive to carbonic anhydrase inhibitors -> share common autoantibody? • Cell-mediated immunity, delayed-type hypersensitivity?
Risk factors No identifiable risk factors have been found • Infection (Chlamydia, EBV), drugs (antibiotics, NSAIDs), "goreisan," • Autoimmune diseases (hypoparathyroidism, hyperthyroidism, IgG4-related autoimmune disease, RA)
- AB → Penicillin, Cephalosporins
- NSAID
- Diuretics
- Hypersensitivity reaction to drug
- Drug mimic nephritogenic AG
- Drugs are trapped in interstitium
- Acute cellular injury caused by infection (often associated with obstruction or reflux)
⇒ Ag-Ab-complex → immuneresponse + infiltrate → tubular injury
- Rash
- Fever
- Eosinophilia
in acute kidney injury
Big variation in clinical picture: asymptomatic - RF
- Microhematuria,
- Eosinophilia (Hypersensitivity),
- Leukocytecast +Leukocyturia,
- mild proteinuria = Tubular proteinuria <1,5g/24h
- Glycosuria
- Phophaturia
- Aminoaciduria
Na/k-P:
→ Hyperkalemia
→sodium wasting
→ Acidosis (distal tubular)
Aquaporin:
→ nephrogenic diabetes insipidus
when diagnosis is not clear
→ definite dg by biopsy
highly suggestive!
T-Lym, Mp, Mc, Eos, Np
→ interstitium → edema
→ tubular BM→ Tubulointerstitial nephritis → necrosis tubular cells (!!epithelial cells + casts still indicate Ac. tubular necrosis ATN)
Drug withdrawal
→ kidney bioposy + glucocorticoids
Antimicrobial treatment
RRT → hemodialysis
and other supportative treatment
Just easy money drug withdrawl
- inflammation tubules + interstitium
- slow progressive chronic renal failure (month-years)
chronic nephrtox (exo- + endotoxin)
infection + obstruction → PyeloN + Papillary N
- chronic nephrotoxic drugs (calcineurin, nsaid, lithium)
- toxins (uremia, Chronic uric acid nephropathy)
- papillary necrosis
- infections + obstructions
- malignancies
- Balkan/chinese herbs und die anderen verrückten
Etiology → Renal cell injury → Expression new local antigens → inflammatory infiltrate, cytokines in interstitium + tubules
- focal tubular atrophy
- interstitial edema
- peritubular + glomerular sclerosis
- Mp+Ly (Mononuclear) infiltrate
advanced:
- interstitial fibrosis
- FSGS
- in certain cases:
- papillary necrosis
- granulomas
- most common
- chronic NSAID + Acetaminophen
- Typical
- Anemia
- Transitional cell Ca
Coagulative necrosis
Calcification
Analgesic microangiopathy → thickend BM of vessels
DM, Analgesic abuse, obstructed urinary tract, pyelonephritis* → cagulative necrosis pyramids + papilla
POSTCARDS:
- pyelonephritis,
- obstruction of the urogenital tract,
- sickle cell disease,
- tuberculosis,
- cirrhosis of the liver,
- analgesia/alcohol abuse,
- renal vein thrombosis, Renal transplant rejection
- diabetes mellitus, and
- systemic vasculitis.
- recurrent pyelonephritis
- obstruction
- reflux
IVP → scarring, irregular contour
if ureteral dilation → chronic VU reflux
if stones, tumors → obstructive cause
🦀 CRAB
- (Hyper)calcemia
- Renal insuff
- anemia
- bone lesions
- Leukocyturia, w/o bacteriuria, mild proteinuria → bland sediment
- Fanconi sy: Proximal tubular dysfunction + glycosuria, amnoaciduria, phosphatura, proximal renal tubular acidosis)
- HT
- slow progression to ESRD
- Assymetric renal involvement → obstruction, reflux only affect one kidney
- small, atropic kidney
- etiology + supportative
- AB in reflux + obstructrion
- surgical intervention
Fused with Urology - UTI
- outside hospital aquired + hospital aquired
- sensible germs + resistance germs
bacteriuria + leucocyturo
→ repeat exam!
could be do to contamination of sample or contamination via catheter
- atypical germs
- other inflammatory causes → stone, tumor, irradiation damage, nephrologic D
G- → E.coli, Klebsiella, Enterobacter, Proteus
G+ →Enterococc(Klebs, Pseudomonas), StaphAureus
*most common - assiciated with infection outside hospital, others are nosocomial
- Neisseria gonorrhea
- clamydia
- staph + strep
cloudy 📷, bad smell
+/- hematuria
dipstick (leukoC-esterase, nitrite)
- Vesicoureteral reflux
- Obstruction: Disruption urinary flow
- foreign body (catheter, ureteral stent, nephrostomy)
- NM: neurologic bladder + sphincter abnormality
- female RF
- postmenopausal
- pregnancy
→ When SEPSIS → check for obstruction/Abcess → treat immediately
CT: can detect: gas-forming abcess, hemorrhage, obstruction, anatomic factors
- reflux
- obstruction
- pregnancy
- pre-urologic procedure
- neutropenia
- recent transplant
acute pyelonephritis in 25-40%!
→premature delivery, low birth weigh, baby mortality
! SCREEEEEEENING bidde
Amoxi-Clavu or Phosphomycin
no Fluros, no TMP in first trimester
all have bacteriuria → absent/minimal symptoms
Remove catheter, do intermittent cathetering, only treat when symptomatic (fever,dysuria)
malformation
- intercourse
- bowel disorders
- contraceptives
- gyn-infections
- foreign body in urethra+bladder
e.coli
pollakiuria
dysuria - burning
⇒ lower urinary tract signs
cloudy urine
+/- hematuria
fever, lumbar pain → acute pyelonephritis
dipstick - leukos+Nit
culture
- AB
- analgesic - NSAID or more
FluroQui
- TMP-SMX
- Norfloxaxin
- Amoxi + clavulanic acid
- FluroQui
- onset of symptoms
Acute:
- systemic inflammatory response → fever, Np
- AUR
- Urinanalysis Nit +
Chronic
- no acute phase reaction
- local symptoms
- Leu in semen+germs
abacterial chronic prostatitis
- Urethritis (see urology)
Testicular Ca + Torsion
like APN but with acute scrotum 📷
secondary to acute or chronic bacterial prostatitis
- sterile leucocyturia
- cloud urine, chronic
- extreme pollakiuria
- small bladder
- Forunier gangrene
bacterial inflammation of PC-epithelium + renal parenchyma
- obstructive
- non-obstrive (reflux, attypical)
obstruction → impaired urine flow → ascending bacterial infection + microabcess
- colic pain
- sign of systemic infect → Sepsis (HypoT, TC, TPn), fever, chills
- lower urinary tract sign (dysuria, pollakiuria, freq.)
- lumbar flank pain, costovertebral tenderness - giordano
- pyuria
- history of recent cystitis
- nausea + vomiting
SOFA ≥2 ⇒ suggests poorer outcome and should alert of possible infection (when previously unknon)
- CBC
- Crea + BUN, Electrolytes
- BGA
- inflammatory markers: Lac, CRP, Glu
- Bili + Coagulation test
- Urinanalyis + culture (2 sets)
- IV AB
- FluroQ
- Aminoglycoside (+ amoxi)
- Cephalos
- Pathogen specific - Vanco, linezolid
- Give Volume
- Address Electrolyte abnormalities
- Decompression of obstruction (see Hydronephrosis)
- cant get through in stable pat
- unstable patient
- pyonephrosis (pus)
DM, Immunosupressed, eldery
DM, posttransplant kindey
- Atropy + scars
- HT + CKD
- Renal abcess
- papillary necrosis
- perinephric phlegon
- pyonephrosis
- septic shock
hematogenous , staph
- high fever
- nephromegaly + back pain
urineanalyis
US
CT
perinephric phlegmon
no improvement on AB therapüy
pus outside the renal capsule
back pain US + CT
purulent destruction renal parenchyma → nephrectomy + AB needed
- Procalcitonin → incr. in big amount of bacterial, fungal + parasitis
- AB asap!
→ start empiricial broad spectrum early → then adapt to antibiogram
- give volume
- vasopressor (NE,dobutamin)
- evtl. cortisone in renal failure
fused version with Urology
crystalline mineral deposits → migrate + obstruct UT → renal colic pain
Classic: Colic wave pain+ Hematuria
severe: UREMIC SYNDROME + SEPSIS
can vary widly:
- inc. urgency + freq
- diffuse abdominal pain
- nausea
- testicular pain
- uremic syndrome
= site of pain
- Diet
- reduced water intake
- HT
- DM
- disorders leading to high Ca

- calcium oxalate - most common 75%
- calcium phosphate - 15%
- uric acid - 10%
- struvite, cystein - rare
- hypercalciuria + oxalaluria due to any cause (hPTH)
- obstruction of the ureter or UPJ
- animal protein intake, vitC + D intake
Proteus + Klebsiella (Urease-producing) → only in upper UTI
- Ions (Ca, P)
- Urea + Crea
- Uric acid
- PTH
- CRP, WBC
- Hb, Hct
- Dipstick - Hematuria
- Infection (Leu, nitrate,ph,culture)
US → Hydronephrosis? Stone?
→ CT (without contrast) → Confirm diagosi(stone/hydronephrosis)
KUB → radioopague; in uric acid → detection with IVP
with contrast: Retrograde pyelography or UroCT → if stone removal is planned
PAIN + DECOMPRESSION + AB
- Pain control → NSAID, Opiates, warming,
- MET: alpha-blocker + ca-channel blocker 📷
- UTI + Sepsis → AB
- Prevention + Recurrance
- Diet →VitC, animal prot, Na, Ca, purine in uric acid
- sufficient Fluid intake → 2.5-3L/day
- sodium restriction if high excretion
- Drugs → thiazide (↓urinary Ca elimination)
- Lifestyle advide → normal BMI
- treat Hyperparathyroidsm
- Urologic intervention
signs of sepsis!! → Urosepsis
no delay it until sepsis is resolved
→ exception: sepsis + abscess
- urine culture
- urine microscopy
→ exclude UTI / treat prior to removal therapy
→ give AB prophylaxis
evtl. stop antithrombotic therapy
→ 📷
infections, refractory pain, decr. renal function
offer stenitng / perc. nephrostomy
renal + prox ureteral stones
stone density >1000HU
stone >10mm
- pregnancy
- bleeding diatheses
- UTI
- anatomical obstruction distal to stone (e.g. ureteral stricture)
increase power session by session
ureteral + renal stones >10mm
ureteral trauma + residual fragments
uncomplicated cases, no trauma, stone-free procedure
renal stone >20mm → percutaneous nephrolithotomy
→ Precise assessment of the stone with contrast (retrograde/CT)
calyx tear
- Ultima ratio - in rare cases, when others fails
- UPJ obstruction → concomitant reconstructive surgery
uric acid stones, alkanization of the urine
🩸Vascular nephropathies
chronic: hypertensive NS, renal artery sclerosis+ischemic nephropathy
acute: acute hypertensive NS
- Chronic • Hypertensive nephrosclerosis • Renal artery sclerosis and ischemic nephropathy •Antiphospholipidic syndrome •Cholesterol crystals emoli
- Acute/ Rapidly progressive •Acute hypertensive nephrosclerosis •Thrombotic microangiopathies •Sclerodermic renal crisis
- Chronic essential hypertension (HT)
- Proteinuria (<1-1.5g/day)
- Progressive renal insufficiency (slowly progressive)
up to 30%
→ 12- 30% of patients with dialyzed patients with ESRD are caused by hypertensive nephrosclerosis
- HT present BEFORE renal involvement
- sign secondary to HT:
- Hypertensive retinopathy
- Left ventricular hypertrophy
- no other cause of renal diseases
- progressive renal damage (crea +urea)
- prexisting CKD
- HT
- black race
- Relatively normal urine sediment (+/- microscopic hematuria)
- Proteinuria <1-1,5 g/24 hours
- Ultrasound: Symmetrical small kidneys
nope,not indicated
- Treat hypertension
- Decrease cardiovascular risk
- Slow the progression of CKD
- Treat the complications of CKD
- lifestyle change (low salt+protein, sport)
- treat aggravating factors
- infection
- avoid toxins, drugs, dehydration
- BP control
- ACEI, ARB if proteinuria
- calcium channel blocker, loop diuretics, betablockers
if crea rise more than 30% → suspect bilateral arterial stenosis📷
⇒ otherwise continue
slow progression to ESRD
→ other complications associated with HT (also malignant hypertension → acute hypetensive nephrosclerosis
- malignant hypertension due to stop of antihypertensive drugs → BP >180/120
- RF, Hematuria, high proteinuria
- HT-ecephalopathy, Cardiac failure, retinal hemorrhage
Hell no
fibrinoid necrosis 📷 → only in bloodvessel
Light micrograph reveals fibrinoid necrosis in the preglomerular afferent arteriole in acute hypertensive nephrosclerosis. The normal muscle layer of the media has been replaced by the fibrinoid material.
- normal protein
- different sizes of right + left kidney
- hypertension
Patholo (see below) → reduction of renal artery lumen → decrease perfusion of kidney → RAAS activation → intrarenal ischemia
>50-55 years
ASc already elsewhere
commonly proximal main renal artery 📷 (green arrow)
total occlusion
- HTN
- Declining renal function => ESRD
- ARF after initiation antihypertensive drug's (ACEi/ARB)
- Flash pulmonary edema
- Surgery
- Percutaneous transluminal renal angioplastia (PTRA) +- stent 📷
- renovascular hypertension
- ischemic nephropathy
bilateral (or unilateral stenosis and single kindey that works)
- Age at onset of HT below 30 or above 55
- Acute HT
- Abrupt onset of HTN or acceleration of previously stable/ well controlled BP
- Severe/refractory hypertension to an appropriate 3 drugs regimen
- Malignant HTN
- Recurrent "flush pulmonary edema"
- Acute renal failure after RAAS inhibition treatment (creatinine rise >50% baseline value within 1 week after ACE/ARBS treatment)
- Moderate/severe hypertension in a patient with generalized atherosclerosis/ or asymmetry in renal size >1.5cm
- Systolic-diastolic abdominal bruit (sensitivity 40%, specificity 99%)
- clinical
- Doppler, angio MRI/CT
- contrast angiography 📷 - gold standard, but invasive
⇒ how severe is the stenosis? → treatment
contrast medium: further deterioration of renal function / allergy
Renal arteriography - gold standard
- confirmation of diagnosis and cause of renal artery stenosis (if >75% stenosis + clinical context => indication for intervention)
- extent of intrarenal vascular disease
- ACEI + ARB
- diuretic
⇒ if crea > 30% stop ACEI,ARB!
- bilateral high grade ( > 75%) arterial stenosis/ or unilateral in solitary kidney
- uncontrolled HT with optimal treatment (3-5 drugs)
- progressive decline in GF/ rapid raise in serum creatinine during HT treatment
- severe decrease in GFR after ACEI/ARBs therapy
- recurrent congestive heart failure => repeated "flush pulmonary edema"
- kidney size >9 cm
- before advance kidney failure (creatinine more>3-4mg/di indicates irreversible lesions)
💥 Acute renal injury
- hours - days
- high crea + urea
- oliguria
- “Deterioration of renalfunction over a period of hours to days, resulting in the failure of the kidney: • to excrete nitrogenous waste products and • to maintain fluid and electrolvte homeostasis • Rapid deterioration of renal function
- "azotemia" (accumulation of nitrogenous wastes)
- elevated BUN and Creatinine levels N levels?
- decreased urine output (usually but not always)”
normal values:
Crea 0,6 -1,2
BUN 10-20
Urea 20-40
yes, in recovery phase or in disturbed tubular reabsorption
- Anuria - no urine output or less than 100ml/24 h
- Oliguria - less than 500ml urine output/24 h or less than 20ml/h
- Polyuria - more than 2.5L/24 hours
75-90%
- SCr increase ≥0,3 in 48h
- ≥1,5x incr. SCr baseline within 7 days (known or presumed)
- Urine output <0,5 ml/kg/h for 6 hours
Stage 1. Serum creatinine is 1.5-1.9 times baseline or ≥0.3 mg/dl increase or urine output <0.5 ml/kg/h for 6-12 hours
Stage 2. Serum creatinine is 2.0-2.9 times baseline or urine output is 0.5 ml/kg/h for > 12 hours
Stage 3. Serum creatinine is 3.0 times baseline or increase in serum creatinine to > 4.0 mg/dl or initiation of renal replacement therapy or urine output <0.3 ml/kg/h for ≥ 24 hours or anuria for ≥12 hours.
Risk factors:
- Dehydration
- old, black, femals
- CKD
- Chronic lung, heart, liver D
- DM
- Cancer
- Anemia
Exposure Factors:
- LOW BLOOD VOLUME (Sepsis, shock, burns)
- surgery
- nephrotoxic agents
- Radiocontrastagent
- Test patients at increased risk for AKI to detect AKI
- Measurements of SCr
- Urine output
- Frequency and duration of monitoring
- Individualized
- Based on patient risk and clinical course
- Evaluate patients 3 months after AKI for resolution, new onset, or worsening of pre-existing CKD
- If CKD-CKD guidelines
- If not - increased risk of CKD
- Hyaline casts can be seen in normal pts (=NOT abnormal)
- UA in prerenal ARF is normal
- Prerenal: causes 21% of ARF in hosp. pts
- Reversible
- Prevent ATN with volume replacement
- Fluid boluses or continuous IVF
- Monitor Uop
- low Volume (depletion)
- low cardiac output
- vasodilation
- intrarenal-artery modification
• Hemorrhage • Renal losses (diuretics, polyuria) • GI losses (vomiting, diarrhea) • Cutaneous losses (burns, Stevens-Johnson syndrome) • "Third spacing"; Pancreatitis, severe hypoalbuminemia
• Heart failure; Cardiogenic shock, tamponade • Pulmonary embolus • Acute myocardial infarction • Severe valvular heart disease • Abdominal compartment syndrome (tense ascites)
• Drugs (antihypertensives, anestesics) • Sepsis, septic shock • Anafilactic shock • Cirrhosis
- Aferent arteriole vasoconstriction:
- NSAIDs, Cox inhibitors, cyclosporin, iodine contrast dye, hypercalcemia, noradrenalin
- Eferent arteriole vasodilation:
- ACEI, ARB, hepatic cirrhosis
acute tubular necrosis
ischemia or nephrotoxic agents
ischemia → due to prerenal cause
→ endogenous → hemepigments, myeloma chains
→exogenous → Nephrotoxic substances:
AB(aminogylcosides, cyclosporn), Contrast, Poisons
necrosis → occlusion of the tubular lumen by casts + cell debris
WBC casts 📷 : cells in cast have nuclei (unlike RBC casts) ⇒ pathognomonic for AIN!
75% due to drugs hypersensitivity → not due to nephrotoxicity
(AB: Penicillin, Cephalosporin, amoxi, Ciproflox, Methicillin, NSAID.. actually could be any drug)
25% rest (Infections, systemic diseases)
Symptoms:
- Painless hematuria
- Flank pain
- Sterile pyuria
- Peripheral eosinophilia
- Rash
- Fever
- Arthralgias
Diagnosis:
- Urinary exam: Leukocyturia (+leuko casts), Eosinophiluria, proteinuria, hematuria
Urine culture- Histology: diffuse interstitial inflammatory infiltrate (T lymphocytes, monocytes) E
tubular proteinuria is generally < 1 g/24 h
biopsy
→ only do in high crea → better stop the drug + see what happens
- stop the causative drug
- if no improvement within 3-7days → biopsy + steroids
- treat infection if present
- supportative (fluids, metabolic correction, dialysis)
Bilateral renal artery stenosis
Malignant HT / Acute hypertensive nephrosclerosis
...and some
Small vessels:
- Thrombotic microangiopaties (HUS, TTP), DIC
- malignant arterial hypertension
- Cortical necrosis
- sclerodermic renal crisis
- cholesterol cristals emboli
Large arteries:
- renal artery thrombosis/emboli
- Bilateral renal vein thrombosis polyarteritis nodosa
- Compresion on renal vein
see urology du latzko
- Intratubular obstruction:
- Oxalate, uric acid (tumor lysis syndrome)
- Drugs - sulfamide, methotrexate, acyclovir
- Light chains
- Ureteric obstruction:
- Stone disease, clot
- Tumor
- Fibrosis
- Ligation during pelvic surgery, tumors (cervical cancer)
- Bladder neck obstruction:
- Benign prostatic hypertrophy (BPH)
- Cancer of the prostate
- Neurogenic bladder
- Drugs (Tricyclic antidepressants, ganglion blockers)
- Bladder tumor
- Stone disease, hemorrhage/clot
- Urethral obstruction:
- Phimosis
- Strictures
- Tumors
- Digestive
- Pericarditis
- Encephalopathy
- Digestive manifestations: nausea, vomiting, diaree, uremic foetor, anorexia, hiccups, GI bleeding
- Pericarditis: precordial pain, cough, fever, tamponade
- CSN symptoms: disorientation, confusion, seizures, coma, delirium
- oliguria with concomitant HTN, edema
- Electrolyte: Hyperkalemia, HypoNa, Metabolic Acidosis
- CV-complications: HF, Arythmias, Pericarditis, HT
- Lung-complications: edema, pneumia, pleuritis
- Uremic encephalopathy + digestive problems
- Hematologic: Anemia, Thrombocytopenia
- Infections: Pyelonephrtis, UTI, pneumonia
Acute or chronic?
- History
- Eco: small kidneys?
- Anemia; HPTH - CBC, PTH
exclude other causes B12, iron, etc.
Obstructive?
- Complete anuria?
- Palpable U bladder?
- Renal US: Hydronephrosis?
Hypovolemia?
- TA, Puls, jugular veins, CVP, response to fluids
- Urea: creatinine; NaEF
Parenchymatous cause?
- History and exam
- Dipstick, microscopy (RBCs, hematic casts, eozinofils, proteinuria)
contrast dye → CT or MRI:
- Renal asymmetry
- vascular ATS disease
- Lumbar pain
- Macroscopic hematuria
- Anuria
ACUTE or CHRONIC? ⇒ Obstruction? ⇒ Euvolemia? ⇒ Any elements of other renal parenchymatous disease (not ATN)? ⇒ Vascular oclusion?
- density >1018;
- normal/hyalin casts
- ATN: density<1012, Granular casts,"muddy" brown, epithelial cells
- AIN: eozinofiluria, leucocitary casts
- GN: proteinuria, hematuria, hematic casts
- VASCULAR: normal/hematuria
no, you need special stain
AIN
- Pigmenturia (rhabdomyolisis, hemolysis)
- Uricozuria(tumor lysis sd)
- normal/hematuria, leucocyte, hyalin, granular casts
- Bland sediment: pre-renal azotemia, urinary outlet obstruction
- Red blood cell (RBC) casts, dysmorphic red blood cells or proteinuria: acute glomerulonephritis, small vessel vasculitis
- White blood cells and casts: acute interstitial nephritis, acute pyelonephritis
- Renal tubular epithelial cells and casts, pigmented granular (*muddy brown") casts: acute tubular necrosis
- Pigmenturia: postrenal AKI due to rhabdomyolisis, hemolysis
Urinary indices | Prerenal AKI | ATN |
U Density | >1020 | <1010 |
U Osm | >500 | <350 |
U Na (mEq/l) | <20 | >40 |
FE Na % | <1 | >2 |
FE uree % | <35 | >35 |
Uree s/creat s | >10 | <15 |
not necessary in most cases when AKI is prerenal, postrenal or ATN
INDICATION:
- Suspician renal cause other than ATN
- Oliguria>3weeks, no obstruction
- AKI renal cause - unknown etiology
- Posttransplant
→(AcGN, Vasc, thrombosis, AIN, Lupus)
Histo of ATN: 📷
- Infection
- hemorrhage
- AV-fistula
- Correct hydric and electrolyte disorders
- Fluid administration - if fluid loss
- Diuretics in high doses, hemodialysis - if fluid overload
- Correct hyperkalemia, hyponatremia, etc.
- Correct metabolic acidosis - bicarbonate, HD
- Treat anemia
- Prevent infections
- Etiology
- vasopressin + isotonic crystalloids→ in low fluid
- hemodynamic + oxgenitc parameter treatment
- not to many but not to less proteins
- Diuretics in V-overload
- NO Nephrotoxic drugs! → Aminoglycosides, Antifungal drugs!
- RRT
Aim
- Remove nitrogenous waste products
- Correct electrolyte imbalance
- Correct acidosis
- Remove water if fluid overload
⇒ Initiate RRT emergently when life-threatening changes in fluid, electrolyte, and acid-base balance exist ⇒ Consider the broader clinical context, the presence of conditions that can be modified with RRT, and trends of laboratory tests-rather than single BUN and creatinine thresholds alone-when making the decision to start RT
- Absolute indications for renal replacement therapy in AKI:
- Refractory volume overload
- Severe and refractory metabolic acidosis
- Severe and refractory hyperkalemia
- Uremic state: encephalopathy, pericarditis
- Relative indications for renal replacement therapy in AKI:
- Severe azotemia without uremic manifestations; absolute thresholds based on azotemia are not well defined
- Need for larger volumes of fluids for drug administration and for nutrition in oliguric patients
Ultrasound guided catheter in jugular or femoral vein
→ Check with chest xray
Continous RRT, rather than intermittent
etiology, patient, severity, kidney injury markers, compliction (multi organ failure, DIC)
every third
15%, every 6. person
→ 50% in dialysis dependend patient (age, multiorganfailure)
= impairment of renal function within 48-72hours after intravenous contrast administration
- Patient related AKI risk factors:
- Preexisting renal insufficiency
- Diabetes mellitus
- Proteinuria
- Intravascular volume depletion
- Reduced cardiac output
- Concomitant nephrotoxins
- Procedure related AKI risk factors:
- Increased dose of radiocontrast
- Multiple procedures within 72 hours
- Intra-arterial administration
- Type of radiocontrast
- Selection of contrast agent
- low risk contrast (low osmolality non-ionic or iso-osmolar) agents
- Volume administration
- I.v. isotonic crystalloid - dose of 1-1.5 mL/kg/h for 6 to 12h preprocedure, intraprocedure, and for 6 to 12h postprocedure
- Pharmacologic therapy
- may include anti-oxidants (eg. N-acetylcysteine), statins, vasodilators, adenosine antagonists or, iron binders
- none of them has enough evidence in studies of preventing AKI
- Avoidance of concomitant nephrotoxins
🕰️ Chronic renal injury
Markers of damage: >3month
MAINLY CREA + URINANALYSIS
- Albuminuria
- Urine sediment abnormalities
- Ions abnormalities
- Histology abnormalities
- Ultrasound
- Kidney transplant history
or
GFR: <60 for >3month
Either of the following present for >3 months.
- Markers of kidney damage (one or more): Albuminuria (AER >30 mg/24 hours; ACR >30 mg/g)
- Urine sediment abnormalities
- Electrolyte and other abnormalities due to tubular disorders A
- Abnormalities detected by histology
- Structural abnormalities detected by imaging
- History of kidney transplantation MPROVING or
- GFR<60mL/min/1,73m2
Stage | Descriere | GFR (mL/min/1.73m^2) |
1 | Renal damage with normal or increased GFR | > 90 |
2 | Mild ↓ of GFR | 60-89 |
3 | Moderate ↓ of GFR | 30-59 |
4 | Severe ↓ of GFR | 15-29 |
5 | End-Stage | < 15 or dialysis |
Albumin-crea ratio (mg/g) | |
A1 | <30 |
A2 | 30-300* |
A3 | >300** |
* Relative to young adult level. ACR 30-300 mg/g for > 3 months indicates CKD. ** Including nephrotic syndrome (albumin excretion ACR > 2220 mg/g)
- high Crea + decr. GFR for >3 month
- Ultrasound → small kidney, hyperechoic
- Anemia (normochromic, normocytic)
- high PTH (due to low VitD→HypoCa2+→high PTH)
Causes of CKD in the US | Incidence |
Diabetic nephropathy | 44% |
Hypertensive nephropathy | 28% |
Glomerulonephritis | 8% |
Polycystic kidney disease | 2% |
Urological disease | 0.5% |
Other causes | amyloidosis, toxins, chronic inflammation |
FSGN
Membranous
Lupus
• Diabetes 37.47% • High Blood Pressure 25.1% • Glomerulonephritis 16.34% • Cystic Kidney 4.69% • Other/Unknown/Missing 16.39%
- Metabolic syndrome characterics (4)
- autoimmune
- cancer
- infections (esp. viral like HBC, HBC, HIV)
- acute renal insuff
- drugs
- stones
- age/race/family history
DM, HT, systemic disease, family history of renal D
- UA: Urinary Albumin/Creatinine
- Proteinuria/24 h: Proteinuria in a 24-hour urine collection
- Urinary Sediment: Hematuria (red blood cells in the urine), leukocyturia (white blood cells in the urine), casts
- Renal US: Renal ultrasound
- Serum and urinary Electrolytes (Na, K, Ca, P) & pH: Levels of electrolytes (sodium, potassium, calcium, phosphorus) and pH in the blood and urine
- Glucose, Chest X-ray, abdominal and heart ultrasound; tumor markers
- ANA: Antinuclear Antibodies
- C3, C4: Complement components
- SP: Serum Protein
- UPEF: Urinary Protein Electrophoresis with Immunofixation
IF: Serum + urinary elektrophoresis in amyloidosis + multiple myeloma
- Small kidneys, reduced parenchimatous index
- In DM, Amyloidosis → enlarged kidney
- Symmetrically small kidneys with thin granular cortex and increased peripelvic fat
- Effacement of the limit between cortical and medullary area
Nephrogenic systemic fibrosis (NSF), also known as nephrogenic fibrosing dermopathy, is a complication of gadolinium-based contrast agents used in MRI. It is characterized by "firm, erythematous, and indurated plaques of the skin associated with subcutaneous edema" 1.
CT → only in tumor suspicion
MRI → only in renal artery stenosis suspecion, Gardulinum(contrast) can cause systemic nephrogenic fibrosis
no, risk is higher then benefit
hylainization / fibrosis of glomeruli
atrophy of tubules
- Evidence of glomerular disease without diabetes
- sudden onset of nephrotic sd or glomerular hematuria
For staging:
Accumulation of uremic toxins
- Urea
- Creatinine
- Uric acid
and approx. 1 million more
from Creatinine
- Directly:
- Endogenous creatinine clearance
- Inulin or other radioactive molecules clearance
- Indirectly - estimated (eGFR) - it uses
- Serum creatinine and equations:
- Cockroft-Gault
- MDRD
- CKD-EPI
- Cysatin C and equations
- albumin/creatinine ratio
- proteine/creatinine ratio
- Urinary dipstick
→ taken from morning urine
dipstick + → ACR + → albuminuria/24h or proteinuria/24h
Work-up:
Check for etiology, see above
Ions
pH
Heart-US
ECG
Cell blood count
mineral markers
- Filtration
- Water excretion + electrolyte excretion
- EPO
- RAAS
- Vit-D activation
the lower the GFR the higher the risk für den shit
- HTA or HTN
- Volume depletion (infections, diarrhea, vomiting, diuretics)
- Cardiac insufficiency
- Drugs (ACEI, NSAIDs, contrast dye, aminoglycosides, CsA, etc.)
- Urinary tract obstruction
- Others (atheroembolism)
alter schwarzer mann mit doofer nephropathy und schon zu beginn schlechter niere
- Underlying nephropathy
- Initial renal function
- Male gender
- Age
- Blacks
most important:
- HTN
- Proteinuria
- Hyperproteic diet
- Glycemic control in diabetic patients
others:
- Dyslipidemia
- Obesity
- Hyperuricemia
- Smoking
- Anemia
- Iron toxicity
- Acidosis
- Phospho-calcic
- Prostaglandin metabolism disturbance
- Fluid overload
- Elevated waste, such as:
- urea
- creatinine
- potassium
- Changes in hormone levels controlling:
- blood pressure
- making red blood cells
- uptake of calcium
none, because most of them are in stage 1-3.
clinical manifestation are present mainly in stage 4-5.
- Specific to primary renal disease
- HTN
- Specific to primary renal disease
- HTN (more freq. than stage 1)
- HTN (rule, 50-60%)
- decr. calcium absorbtion and fosforus excretion
- incr. PTH
- decr. 25(OH)D and 1,25(OH) 2D
- Spontanous decr. of protein intake
- Renal anemia
- Left ventricular hypertrophy
same as previous stage, but more pronounced, plus:
- Metabolic acidosis
- hyperkaliemia
- malnutrition
From the previous stage, more pronounced and severe, plus:
- Hydro-saline retention
- Meeting in
- Anorexia, vomiting
- Pruritus
- Nausea, vomiting
- Fatigability
- Uremic pericarditis
- Uremic encephalopathy => MALNUTRITION
- Clinical
- SGA
- Anthropometric indices
- Serum albumin
- Cholesterol
diagnosis of exclusion
you don't check for EPO in blood because in stage 4 + 5 you always have decreased EPO
→ better exclude by looking for iron, B12, folic acid, bleeding, etc.
- Ca, Phosphate, PTH, Vitamine
- Vascular or soft tissue calcification!
KDIGO: I. ROD = exclusively alteration of bone morphology associated with CKD, evaluated through histo-morphometry II. CKD-MBD = mineral and bone metabolism abnormality secondary to CKD - consists of:
- Lab tests for mineral metabolism (Ca, P, iPTH, vitamin D)
- Bone
- Vascular or soft tissue calcification -> evaluation for extraskeletal calcification becomes an essential element in mineral metabolism disturbances approach in CKD patient
- classification based on these elements (L, LB, LC, LBC)
- Bone pain - diffuse continuous
- Bone deformities
- Fractures on pathologic bone
- Proximal muscle weakness
- Renal dwarfism
- Increase survival
- Increase quality of life
- Underlying renal disease treatment:
- Slow CKD progression rate
- Prophylaxis and treatment of complications
- Prophylaxis and treatment of associated diseases
- Prepare the patient for renal replacement therapy
- Renal replacement therapy
- Conservative treatment
Non-pharmacological treatment:
- Diet: Reduction of salt intake
- Physical activity
Pharmacological treatment:
- #1 ACEI/ARB are the first therapeutic line in:
- CKD stages 1-5 associated with albuminuria >30 mg/24h, in hypertension patients
- CKD stages 1-5 when albuminuria >300 mg/24h, in diabetes mellitus patients, even if blood pressure is not high.
- #2 Diuretics
- #3 Calcium channel blockers or beta blockers ´
low proteins
Salt <2g Na+
Evaluate the need to restrict K*
Low phosphorus diet <800mg/day (meat, fastfood, fish, cheese, milk, cola, seeds)
check the HbA1c development over time
Glycemia control: HbA1c = 7%
- Exception: patients with high risk of hypoglycemia, low life expectancy, severe comorbidities.
- DM: multifactorial therapy = ARB/ACEI + statins + antiplatelet.
Life style
- Reach optimal body weight (BMI 20-25)
- Reduce salt intake (<5-6g/day)
- Physical activity (30min × 5/week)
- Reduce alchool consumption
- Stop smoking
- very important in nephrotic sy
- CKD 2-4 → statins reduce cardiac risk
- chronic dialysis → no real benefit
Dyslipidemia and Cardiovascular Morbidity
- Chronic dialysis patients do not benefit from statin treatment (e.g., 4D study).
- Treatment for CKD stages 2-4 reduces cardiac mortality and morbidity.
- Dyslipidemia is common in glomerular diseases (nephrotic syndrome), and controlling it reduces morbidity and mortality associated with atherosclerosis.
- Too less water (at least 500ml)
- NSAID
- Contrast
- ACEI/ARB in dehydration
- Avoid Dehydration
- Ensure adequate infection treatment
- Avoid nephrotoxins such as aminoglycosides and NSAIDs
- Avoid iodate contrast dye
- In the presence of dehydration, even in the absence of renovascular disease, ACE or ARB can worsen renal dysfunction
- Prophylactics: to avoid/correct blood loss.
- Treatment with:
- Injectable iron (Venofer), Folic Acid, B12, B2, B6, vit C
- Erythropoetin (EPO)
11-12 g/dI. Levels > 13 → increased mortality
Bicarbonate po
- Diet
- Hemodialysis
- Phophorus binder
- Vitamin D substitutes
- Calciumimetics
- Biophosphonates
- Parathyroidectomie
Cardiac
Aterioscl
⇒ ATS - antiaggregant BNP, Troponin - interpreted with caution if GFR < 60 To benefit from the same invasive investigations ACOMI - periodic evaluation Meeting
dose adjustment to GFR
Uremia → modified absorption
incr. volume of distribution
decr. protein binding
kidney dependend excretion drugs
caution in cancer tx!
- Dialyisis vs transplant
- Hemodialyisis vs perioteneal diaylsis
- Protect veins for possible AV-fistula
- Viral markers + vaccination
- Education to choose between dialysis or transplantation
- Hemodialysis vs Peritoneal Dialysis
- Protect veins when RFG < 60 ml/min
- Choose an appropriate moment to realize vascular access or PD catheter insertion
- Evaluation of viral markers (AgHbs, Anti-HCV, Anti-HIV) and HBV vaccination
Other:
- Pericarditis
- Hyperkalemia and acidosis resistant to treatment
- Pruritus
- Hypervolemia resistant to treatment (acute pulmonary edema, hypertension)
- Deterioration of nutritional status refractory to dietary intervention (nausea, vomiting, inappetence)
- Cognitive dysfunction (advanced encephalopathy)
- Peripheral neuropathy
- Hemorrhagic diathesis
- Glomerular filtration rate between 5 and 10 ml/min
- best survival advantage
- take immunosupression
In patients who refuse renal replacement therapy, palliative care is provided. This includes:
- Symptom control
- Psychological, spiritual, and social care
- Family involvement in the caring unit (including bereavement)
- "Advance care planning"
- "End-of-life care"
Bad progression factors: low GFR, etiology, stage, albuminuria other risk factors
⇒ 📷
Death = far more common than ESRD
🔁 Renal replacement therapy
Chronic renal replacement treatments:
Other extracorporeal purification techniques:
⇒end-stage renal D (stage 5)
- GFR <15ml/min (can be different in each country)
- Uremia manifestation (pericarditis,malnutrition, hypervolemia, hyperkalemia, metabloc acidosis, resistance to conservatory treatment, pruritus, encephalopathy/neuropathy)
corrects ions
fluid overload removal
waste product removal
3 x 4h / week
dry weight = after session → check every time to set the right ultrafiltration rate and compare to ideal weight + weight gain inbetween sessions
Urea reduction rate should be at least 70% per session
- Hb 11.5-12 g/dl
- Ca, P, PTH within limits
- Patient status, lack of complications/hospitalizations
- Dry/ideal weight = Euvolemia and BP control
- spKt/V > 1.4
- URR > 70% (urea reduction rate)
- Hb 11.5-12 g/dl
- Ca, P, PTH within limits
- Patient status, lack of complications/hospitalizations
- Dialyzer
- Dialysis solution
- Tubing for transport of blood and dialysis solution
- Machine to power and monitor the procedure
- Diffusion
- Different concentrations become equal over time if solute transfer is possible
- Ultrafiltration
- Water transfer occurs due to a pressure gradient across the pores of the membrane, generated by the dialysis machine
- Convection
- Solutes are transported with water flux
semipermeable membrane
- Cellulose: cellulose, cellulose acetate
- Synthetic: polysulfone, polyacrylonitrile, polymethylmethacrylate, polycarbonate, polyamide
Several types of dialyzers with different characteristics are available:
- Membrane materials
- Surface area
- Ultrafiltration coefficient
- Blood volume capacity
- Clearance of various substances
more water removal → choose ultrafiltration
- The filter type
- High vs low efficiency: high mb S (small pores) and high blood debit
- High vs low flux: big pores
- washes out the porrous capillaries of the dialyzer allowing changes with the blood compartment
- obtained from
- purified water
- dialysate concentrate
Removes aluminum, chloramine, fluoride, copper, zinc, electrolytes, as well as bacterial fragments and endotoxins.
- The first filter contains gravel and activated charcoal, which retains chloride and 5-micron impurities from tap water.
- The next two filters (alternating) contain resins saturated with sodium, eliminating calcium and magnesium to provide softened water.
- The reverse osmosis machine has a semi-permeable membrane with 0.0001-micron pores. Under pressure in the water compartment, water passes through the membrane at a rate of 270 liters per hour, purifying it from bacteria, viruses, and heavy metals, resulting in ultrapure water.
native (AV-fistula), AV-graft, CVC
An AV graft is a looped, plastic tube that connects an artery to a vein. A vascular surgeon performs AV graft surgery.
Seldinger technique
- Guidewire into internal jugular
Native AVF
- prolonged patient survival
- fewer infections reduced costs
- improved clearances
- Infections
- Thrombosis
- Aneurisms
- Stenosis
- Steal sd
- Venous edema
- cardiac failure (incr. venous load)
steal sd = due ischemia → check 6 P's

venous edema + cardiac failure due to increased venous pressure
Fistula aneurysm → might cause rupture
Fistula has to be closed!
- Hypo- or HT
- Nausea vomiting
- pain (head, thoracic lumbar)
- pruritus
- Disequilibrium syndrome
- Hypoxemia, Hypoglycemia, Hemolysis
- Anaphylaxis
- Electrolyte disturb → arrhthymias
- Cardiovascular complications due to Uremia + HT
- GI inflamm + bleeding
- infections
- Restless leg syndrome
- Hypoglycemia + Proteinmalnutritian
- Anema
- Ion abnormalities
- Endocarditis
- Pericarditis in uremic dialysis patients
- Hypertension; ischemic cardiopathy, congestive cardiac failure
- Gastritis (stress in HD, Hb in HPTH), colonic diverticulosis; gastrointestinal bleeding due to heparin; hemosiderosis
- Bacterial: vascular access; respiratory, urinary tract
- Viral: hepatitis B, C, CMV, HIV
Cardiovascular (due to AVF, HPTH, VC, HE & AB disequilibrium; accelerated AT):
Digestive:
Infectious:
InflammationEndocrine (infertility) Neurological (restless legs syndrome) Metabolic: hypoglycemia in HD; insulin need in diabetic HD patients; protein malnutrition; increased tryptophan Anemia
Mineral metabolism
Anemia/ HPTH treatment
- normal calories + normal proteins
- fluid restrictions
- Restriction for Na, K, Phosphate
adjusted dose to renal function
- Avoid IM administration - hematoma risk due to anticoagulant therapy.
- Pay attention to IV administration: DO NOT use in AVF (arteriovenous fistula).
- Preserve venous access.
- Vaccinations - for Hepatitis B
- Monitor ALAT, ASAT, viral markers
- Initiate antiviral treatment before renal transplantation
10%
(90% HD)
- children ≤ 2y
- residual renal function
- without signif. comorbidities
- difficult vascular access (DM)
- CV-diseases
kids can't stay at the dialysis
Better hemodynamic tolerance
peritoneum already fucked up
poor quality peritoneum (previous big abdominal surgery → fibrosis)
- only once a month they have to go to the center
- better tolerance
- longer preservation of resudual renal function + vascular access site
- less severe infections
“In 1968, Tenckhoff revolutionized the field of peritoneal dialysis (PD) by introducing a permanent catheter and a method of implantation that, for the first time, allowed relatively long periods of usage with a significant reduction in infections. The catheters are made of silicone rubber and usually have two cuffs with a straight tunnel configuration (tunnel in the peri-umbilical area and an internal part).”
same as HD but additioanlly Osmosis
→ hyprerosmolar peritoneal dialysis solution → water moves from peritoneal capillaries
- Diffusion (toxins move into peritoneal fluid)
- Convection (solvent drag)
- Ultrafiltration
⇒ These processes facilitate the transfer of water, solutes, and toxins during peritoneal dialysis.
Changes - between peritoneal capillaries and dialysis solution:
- Osmosis:
- Water transfer occurs due to different concentrations between the peritoneal capillary network and the hyperosmolar peritoneal dialysis solution.
- Diffusion:
- Solute transfer from the peritoneal capillary network into the PD fluid.
- Toxin removal and solute clearance occur simultaneously with water removal.
- Convection:
- Solutes are transported with water flux, known as "solvent drag" during ultrafiltration.
- Ultrafiltration:
- Fluid movement in response to an osmotic force.
- Aquaporins are responsible for 40-50% of total UF, while small pores account for 50-60%.
- UF volumes can be modified by using different osmotically active solutions.
water, osmotic agents (gluc), electrolytes(no K), buffer (lactate) → inc. osmotic pressure gradient
- chronic ambulatory peritoneal dialyisis (CAPD) → 4 changes a day
- or automated peritoneal dialysis (ADP) → noctural or continous
infections = most common ⇒ most common Peritonitis
exit site infection
Diagnosis:
- cloudy fluid in bag (effluent)
- abdominal pain
- Leucocytosis
- Culture of effluent pos
Treatment: AB (+ antifungal prophylaxis)
Refractory P → cloudy fluid persists → fungal, mycobac, catheter removal
- Diagnosis: At least 2 of the following 3 elements:
- Clinical features: cloudy effluent, abdominal pain
- Effluent cell count: WBC > 100/L, with >50% neutrophils
- Positive dialysis effluent culture. Bacteremia is rare.
- Peritonitis treatment:
- Immediate empiric antibiotic therapy INTRAPERITONEAL and heparin.
- Must cover Gram-positive and Gram-negative microorganisms: Vancomycin or a cephalosporin + third-generation cephalosporin or aminoglycoside.
- Often, Cefazolin and Ceftazidime are administered in the same bag.
- Refractory peritonitis:
- Symptoms and cloudy fluid persist for more than 4-5 days.
- Causes can include fungal or mycobacteria, polymicrobial peritonitis, and chemical peritonitis.
- Catheter removal is recommended for relapsing peritonitis, refractory peritonitis, and fungal peritonitis.
- Anti-fungal prophylaxis (with Nystatin or Fluconazole) is recommended when PD patients receive antibiotic courses to prevent fungal peritonitis.
- Outflow failure
- Leaks → hydrothorax, abdominal wall edema
- Hernias
- Encapsulating peritoneal sclerosis "interstitial cocoon"
- Bloody effluent
- hypokalemia

similar
ESRD
- RF actually reversible
- active cancer, infection
- low life expectancy
- drug addiction, psychatric disorder
life expectancy
Ne auch 70 jährige haben noch bock
autoimmune disease → solve before transplant
(Active ANCA-associated vasculites or SLE need to be adequately treated; after few months of inactivity, transplantation can be realized Primary oxalosis - combined kidney-liver transplantation - AL amyloidosis - renal transplant after succesful stem cell transplantation)
- Blood, Liver function, count, coagulation,..
- Infections
- Screening for cancer
- pregnancy
no longer routine, only in:
- large PolycysticKD
- severe proteinuria
- Chronic reflux disease
- Recurrent infection with nephrolithiasis
living donor (30%)
deceased donor (70%)
- No vascular diseases!
- no infections
- GFR ≥80
- general healthy
- imaging of renal vasculature
- HLA typing + cross matching
children (growth impact)+ HLA zero mismatch
absolute: infections + malignancies
relative: old, vascular abnormalities (HT, DM)
iliac fossa
started before or at time of transplant
#1 IL-2 Receptor antagonists (basiliximab)
Lymphocyte depleting antibodies (antithymocyte globulins, alemtuzumab)
calcineurin inhibitors (cyclosporin + tacrolismus)
antiproliferation (Mycophenolic acid, azathiprine)
steroids
- Rejection (hyperacute, acute, chronic)
- Surgical complication → Renal artery stenosis, urine leakage, ureteral stenosis
- Drugs → Nephrotox (Calcineurin-Inh)
- Recurrance kidney diseases
- Infection
- Malignancy
- HT
- Liver D
excellent progrnosis, longer lifespan
Death mainly due to Cardiac diseases not kidney failure
acute kidney injury, intox, fluid overload (HF) + sepsis
→ NOT IN CHRONIC
esp. in intensive care
hemodynamic instability in acute kidney injury
intoxications!
Seperation plasma from cells → remove antibodies or toxins → replace with fresh frozen plasma or albumin
Goodpasture, SLE, Recur. FSGS, others
💧 Hydro-electrolytic disturbances
Osmolality =(2 X Na) + glucose/18 + BUN/2.8
Urea = BUN x 2,14
270-290 mosm/kg water
if we suspect pathological condition
compare it to calculated Osmolarity
if there is a difference bigger than 10 (m>calc.) ⇒ Elevated osmolal gap
- exogenous solutes (Ethanol, methanol, anti-freeze)
- Mannitol, i.v. IgG
- other absorbed irrigants
500-800
→ Thirst + ADH → KEEP THE WATER
<120
- ADH-indep.: serum+urine osmolal<100 → water intox, kidney failure
- ADH-dep.: serum <100 urine >100 → SIADH+others
Water intoxication is the cause of hyponatremia when urine osmolality is <100 mOsm/kg.
- Psychotic polydipsia
- Infants fed dilute formula
- Beer potomania
- Tea and toast diet plus large water intake.
Hyponatremia with urine that is not maximally dilute and urine osmolality >100 mOsm/kg.
- Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
- Upregulated AVP secretion.
HIGH ADH SECRETION due to
- Hypovolemic → Sodium loss:
- Extra-renal → diarrhea, burn, fever
- Renal → Diuretics (thiazides), Addison, Salt wasting
- Hypervolemic →Edema: HF, Cirrhosis, nephrotic
- Euvolemic → SIADH, Adrenal insuff, Hypothyroid

- Hypotonic hyponatremia
- Urine osmolality above 100 mOsmol/kg
- Clinical euvolemia
- Lab correlates of euvolemia: low BUN and low serum uric acid
- Urine Na matches intake and is typically > 30 mEq/L/24h
- Exclude other causes of hyponatremia
- Malginancies
- Infections
- Neurological disorder (inflamm, degen)
- Psychotic disorder
- Drugs: SSRI, Antidepressant, NSAID, Cyclophosphamide
- Pulmonary small cell carcinoma, head and neck cancers, aspergyllosis, pneumonia, tuberculosis
- Neurological disorders (degenerative, inflammation), psychosis
- Medications like selective serotonin reuptake inhibitors, tricyclic antidepressants, NSAIDs, oxytocin, carbamazepine or, cvclophosphamide
- general aim: treat etiology, Take more salt, consume/excrete less water
- ADH-R-Antagonis: Conivaptan, Tolvaptan
- Urea, Lithium
Therapies to raise the serum sodium: fluid restriction, intravenous hypertonic saline, high solute intake, oral salt tablets, salt plus Meets. loop diuretic
- cerebral edema with seizures +- herniation of brain
- pulmonary edema with respiratory arrest
- loss of organic osmolytes minimizes brain swelling → adaptation complete in 2 days
- non-neuro: myocardial fibrosis, osteoporosis, falls, fractures and earl senescence
⇒ rapid correction causes osmotic demyelination
Water restriction, diuretics, hemodialysis
in water intox, Edema (HF,Cirr,NS)
i.v. saline
in Sodium loss
- Apoptosis of astrocytes
- chronic Hyponatriemia is corrected to quickly
- 2-6 days after correction
- Pontine symptoms: Swallowing difficulties, Locked in syndrome (Quadriplegia+Anarthria)
- Extrapontine symptoms: periph. neurological abnormalities (seizures, behavior, movement)
4-6 meq/l /day
NOT MORE THAN 10-12
Desmopressin
>160
children
elderly → neurologic patients
frail+critically ill patients (can't drink water, etc.)
rare!
extreme water loss or sodium intake
- Salt poisoning
- Diabetes insipidus without water replacement
water losing disorders
- Central DI
- Nephrogenic DI (Autosomal recessive + x-linked)
- Vasopressin antagonist
- Loss of medullary conc. → kidney diseases, Loop diuretics
- Pregnancy → Vasopressinase
polyuria + low osmolality
Diabetes insipidus (DI) = elimination of large volumes (ranging from 3-20 Liters/day) of dilute urine (urine osmolality < 300 mOsm/kg)
idiopathic
any trauma to pituitary gland
tumor
ischemia
autoimmune
idiopathic
lithium
hypercalcemia
DD: polydipsia, central-DI, nephrogenic DI

- Central → Desmopressin nasal
- Nephrogenic → Etiology, Thiazide diuretica, Nsaids

→ neurologic abnormalities
- brain hemorrhages
- demyelination with apoptosis of astrocytes
- brain produces intracellular osmolytes to minimize shrinkage → adaption in 3days
- Loss of accumulated osmolytes: take >24h
- Rapid correction ⇒ brain edema → infants rehydration seizures
actually corrected by fluid
12
- Etiology of DI/ADH-Antagonist (see above)
- Fluid overload? → diuretics + water restriction
- Dehydrated? → fluid replacement
- in chronic → water access? drink rhytm + dextrose or saline solution
<2,5
- Decresed intake
- Losses:
- Diarrhea
- Vomiting
- Renal abnormalities (Diuretics, hyperaldosteronism..)
- Diuretics
- Alkalosis → H+ raus aus der zelle, K+ rinn da
- Insulin
- Beta-2 agonists → Affect NaK-Pump
- Thyrotoxicosis
- HypoMg
pulyuria + polydipsia → less Na+H2O reabsorption
- Muscle weakness, sometimes with paralysis or rhabdomyolysis
- Fatigue and constipation
- Cardiac arrhythmias with syncope or palpitations
- Polyuria and polydipsia
- Decreased urinary concentrating ability
- Direct stimulus to thirst
- Volume depletion
- Hypokalemic nephropathy with interstitial renal disease
- End-stage renal disease in 5% after more than 20 years
- underlying etiology
- stop diuretic (take Spironolacton instead)
- Give Mg if ↓Mg
- K-rich diet
<2,5
5
6,5
- Renal failure
- ↓Aldosteron (Spironolactone, Addison, type 4 renal tubular acidosis)
- Low Volume → low distal sodium+water delivery( → decreased sodium, K+ exchange)
- Metabolic acidosis
- Beta blockers
- insulin deficiency, ↑Bloodsugar, ↑Blood-Osmolarity
- Tissue injury → Rhabdomyolyis, hemolysis, tumor lysis
- Digoxin (Blocked NaK pump), Succi (K+ efflux)
- Genetic (Periodic paralysis)



{kind=link}
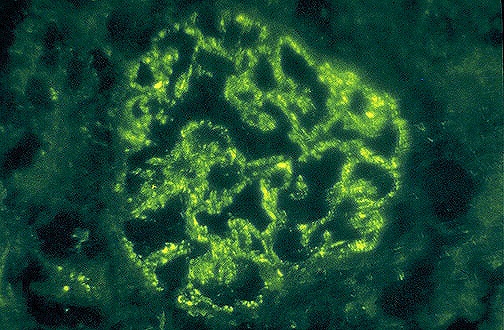{kind=link}
{kind=link}
{kind=link}
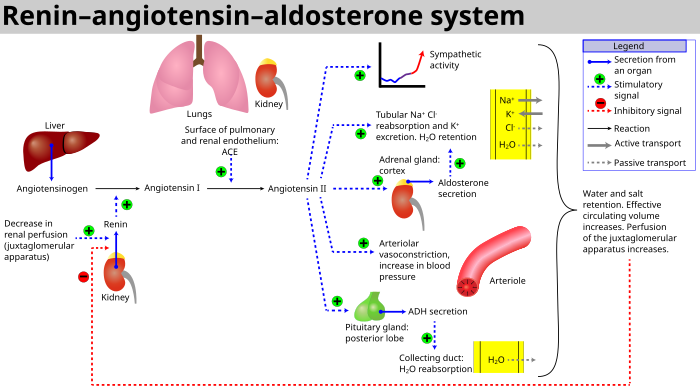{kind=link}
{kind=link}
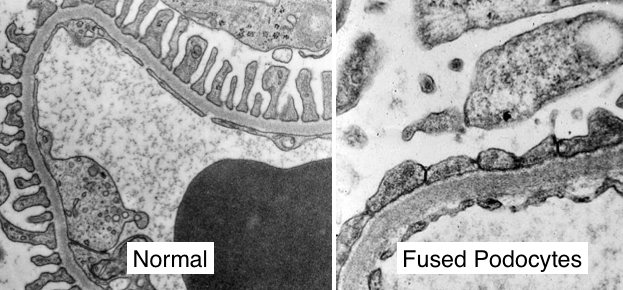{kind=link}
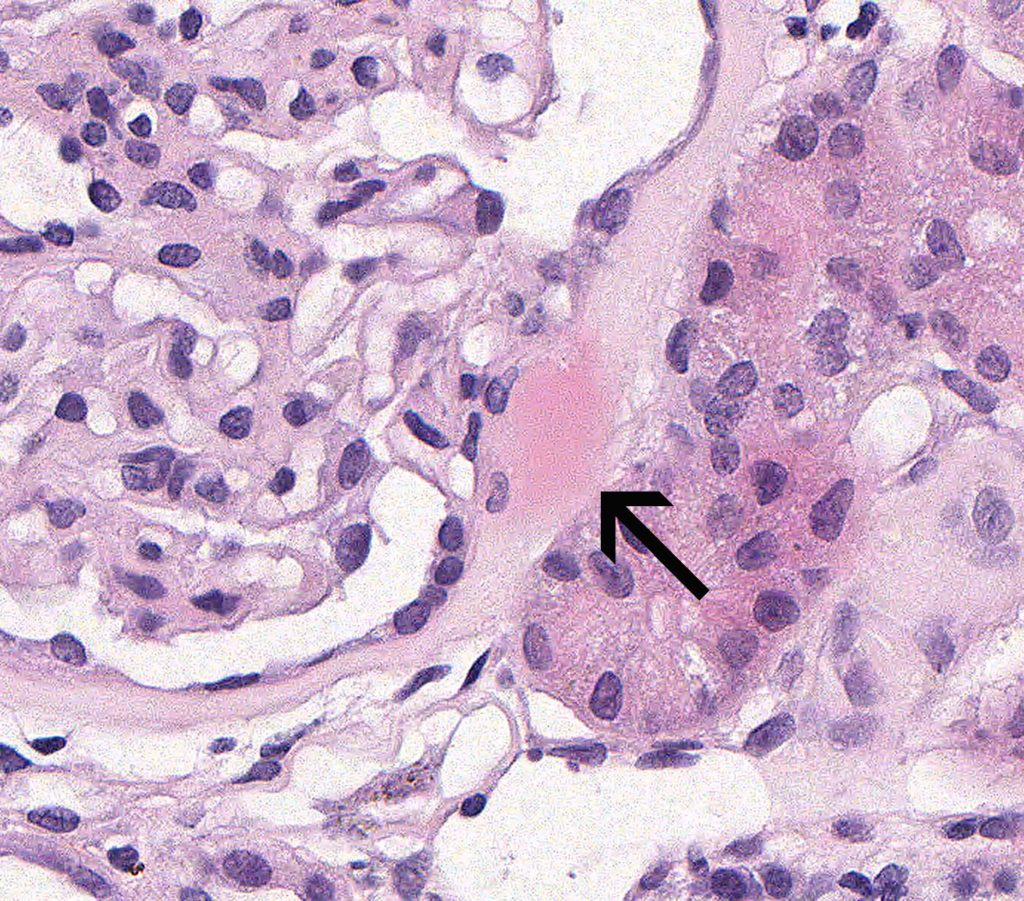{kind=link}
{kind=link}
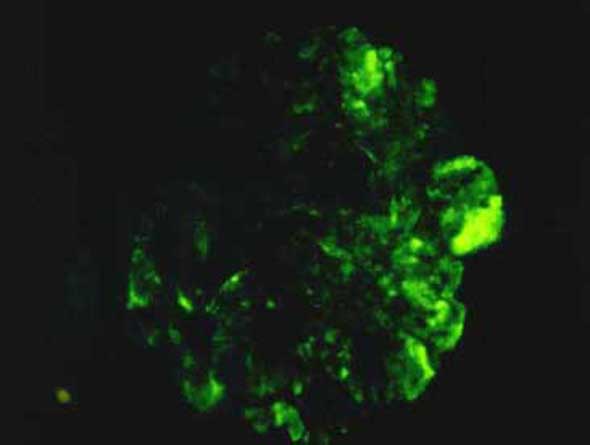{kind=link}
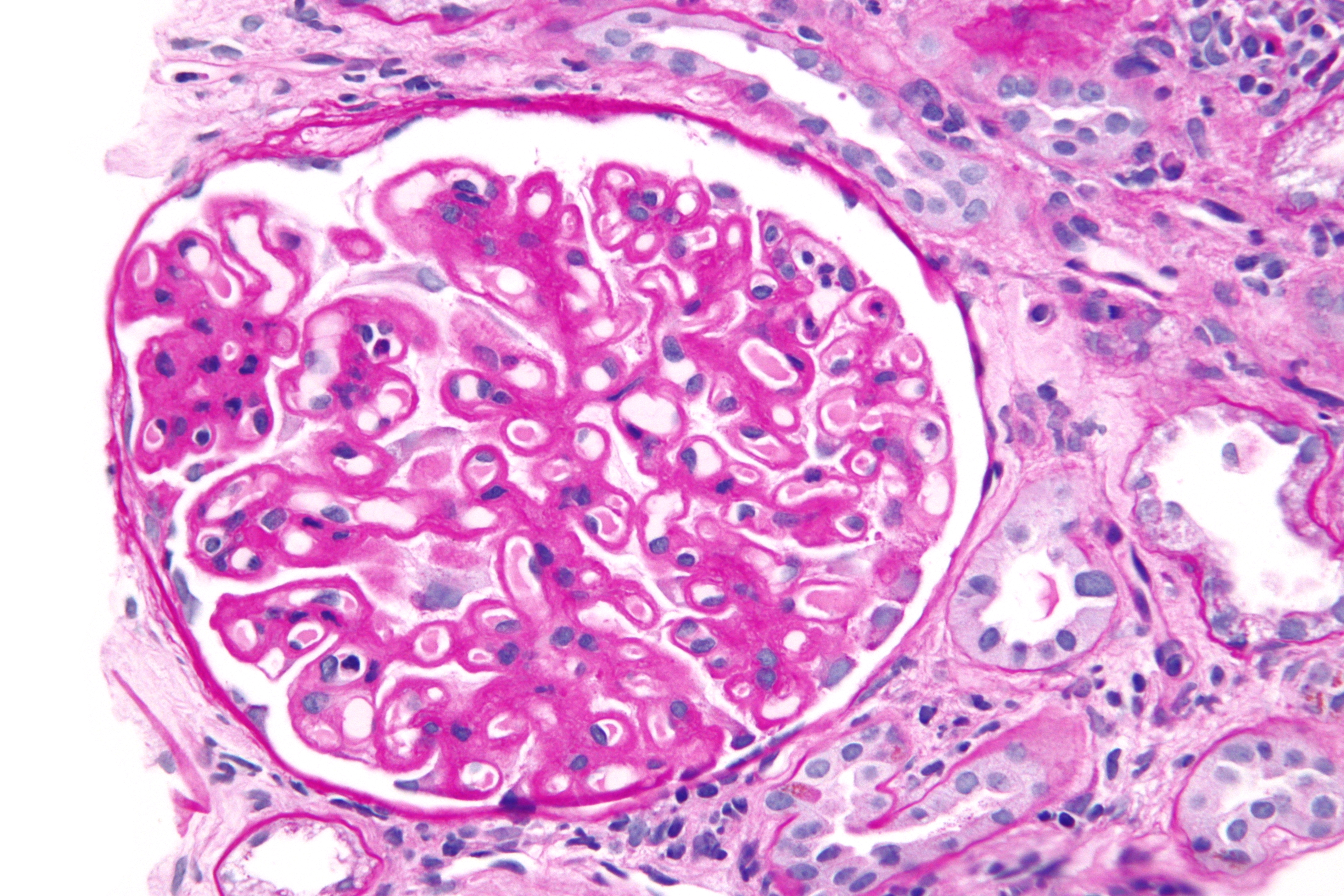{kind=link}
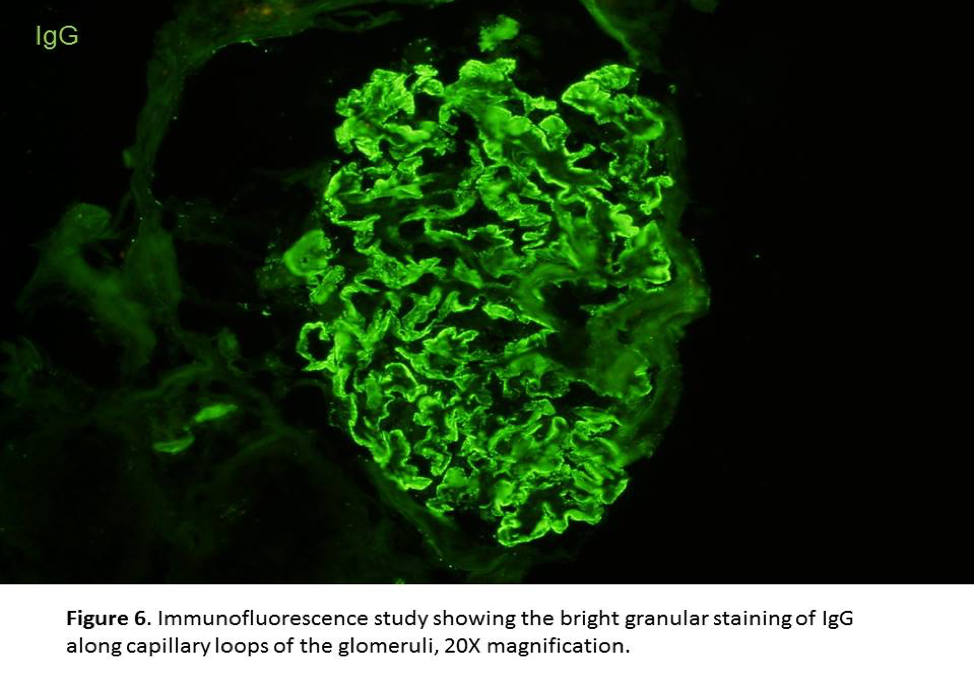{kind=link}
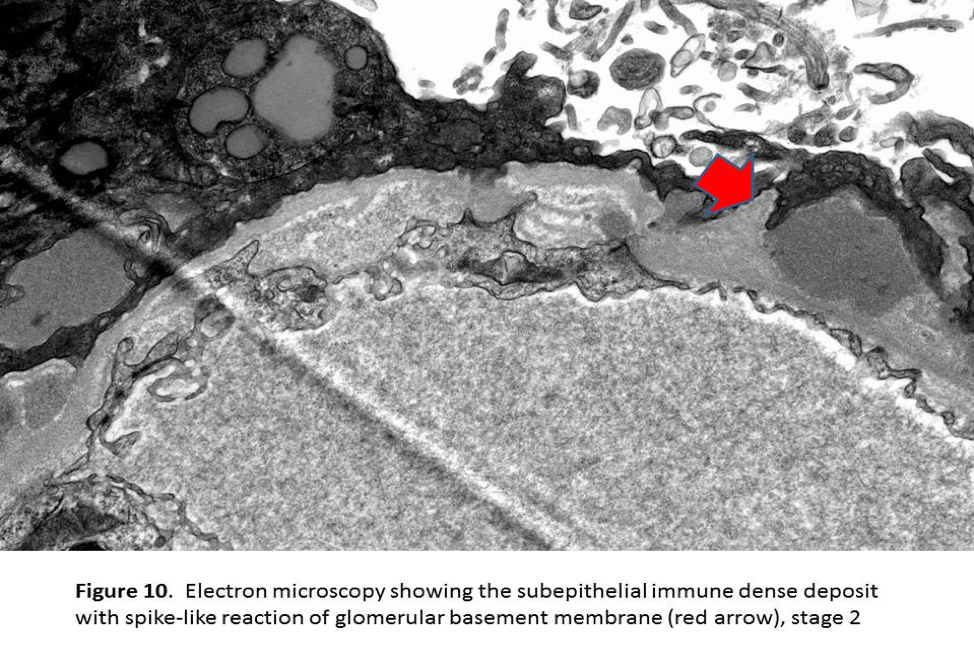{kind=link}
{kind=link}
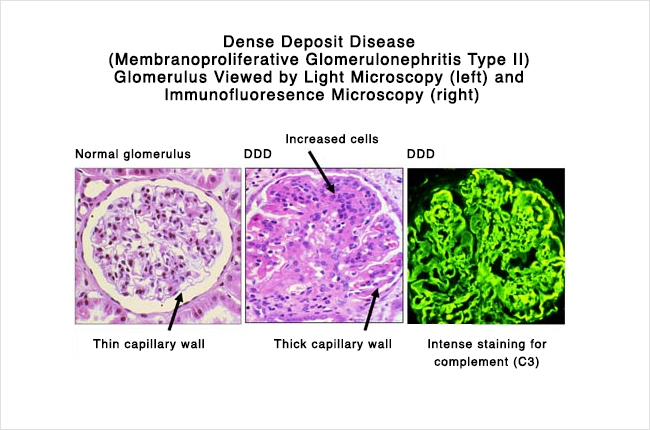{kind=link}
{kind=link}
{kind=link}
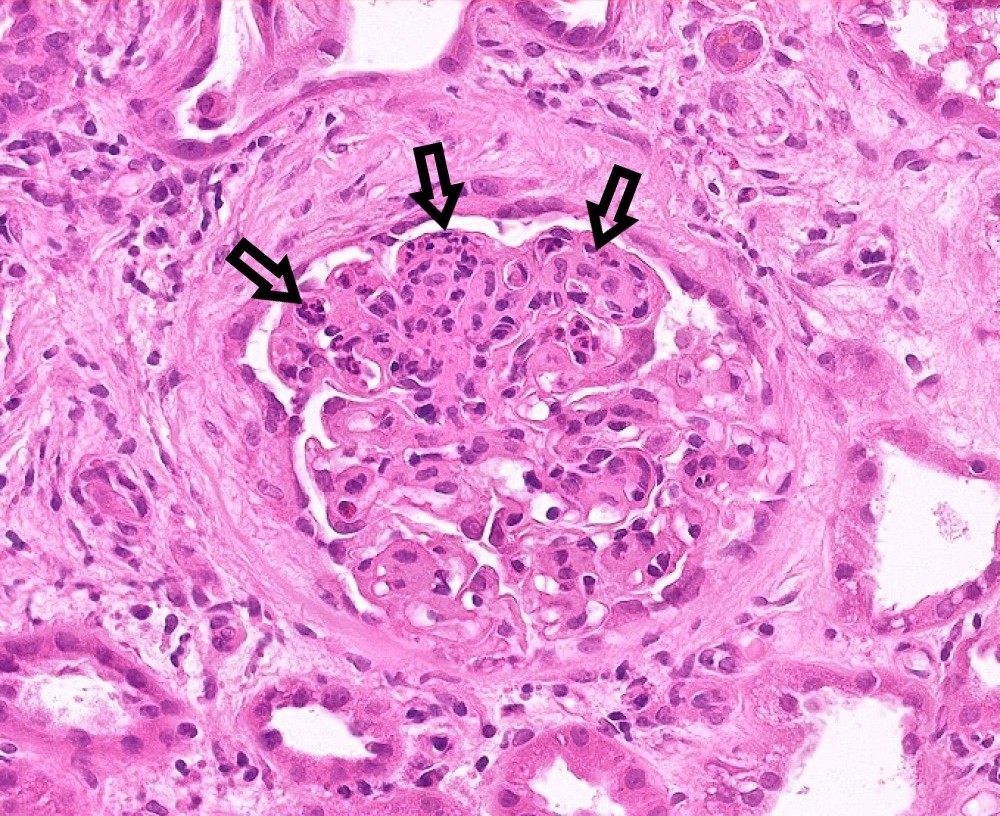{kind=link}
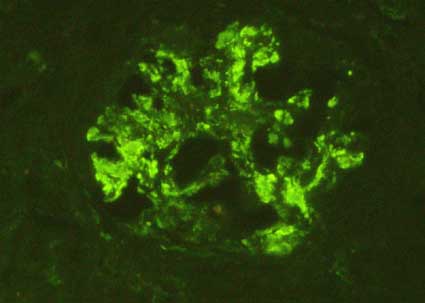{kind=link}
{kind=link}
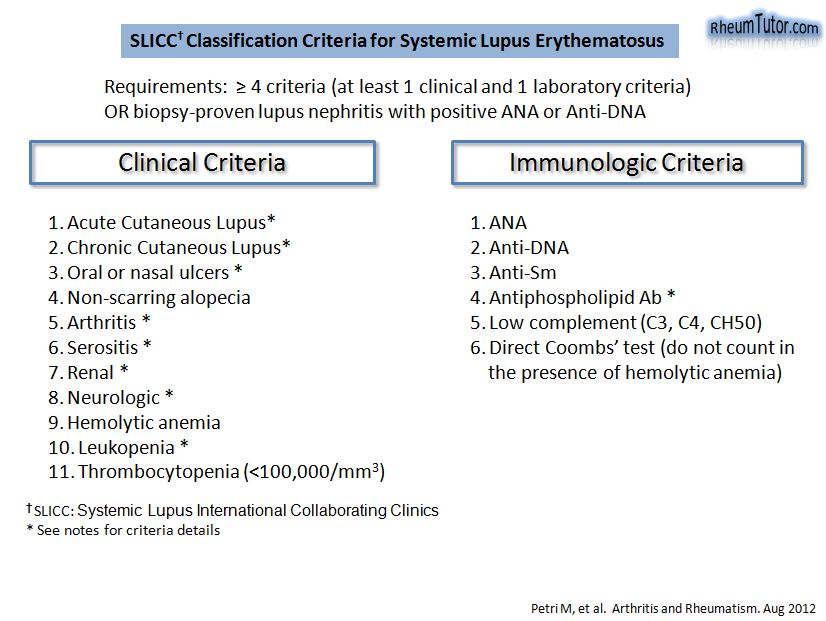{kind=link}
{kind=link}
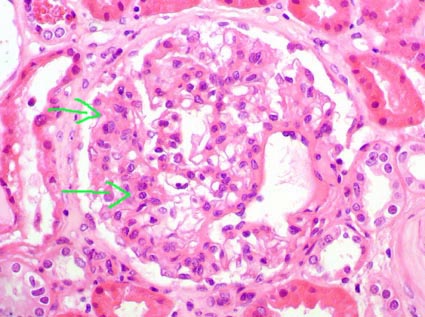{kind=link}
{kind=link}
{kind=link}
{kind=link}
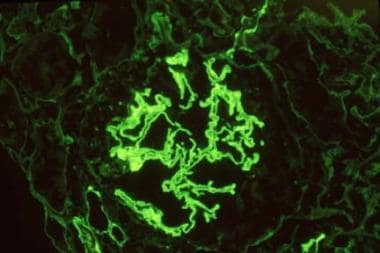{kind=link}
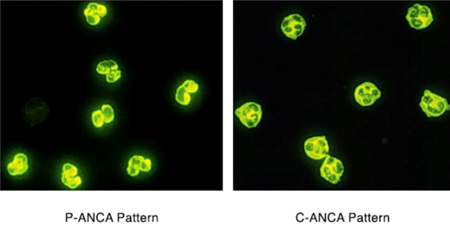{kind=link}
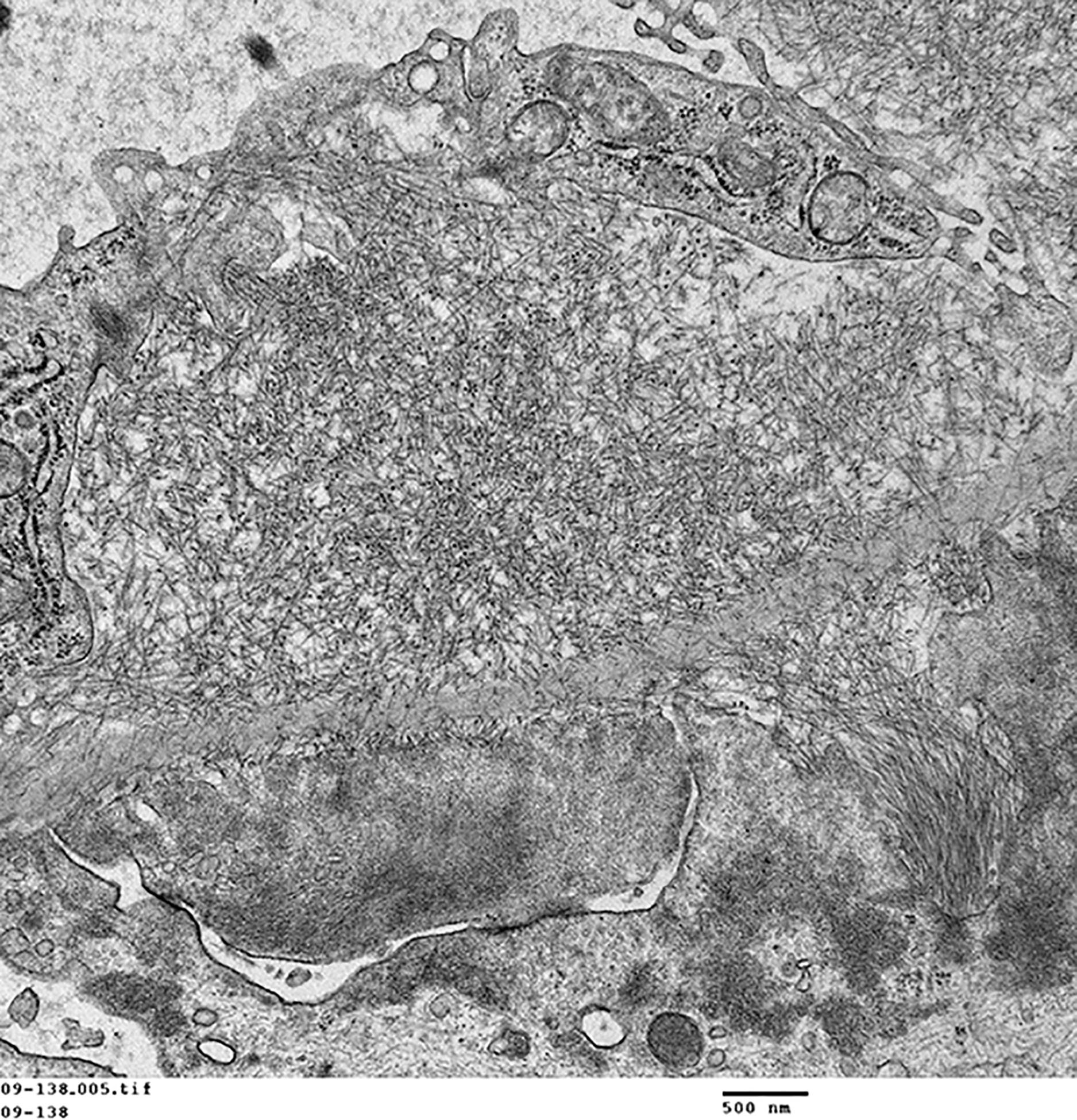{kind=link}
{kind=link}
{kind=link}
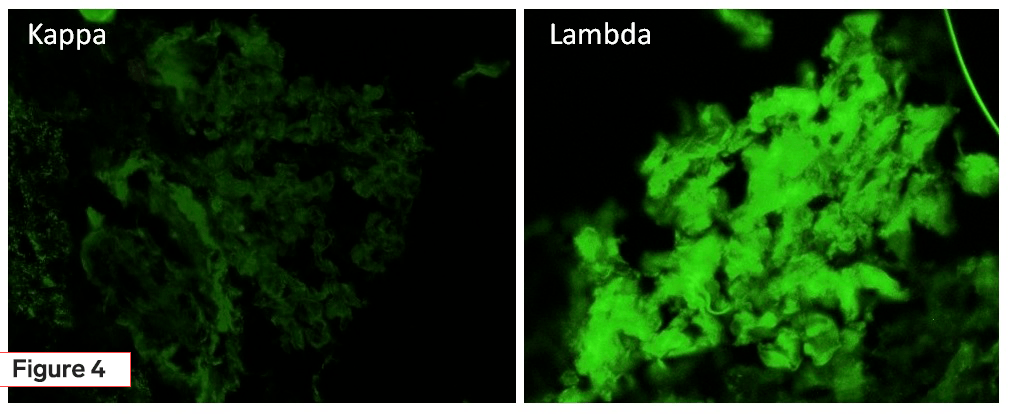{kind=link}
{kind=link}
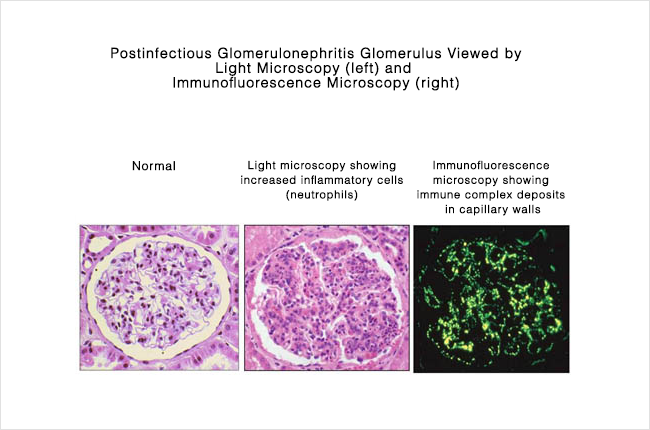{kind=link}
{kind=link}
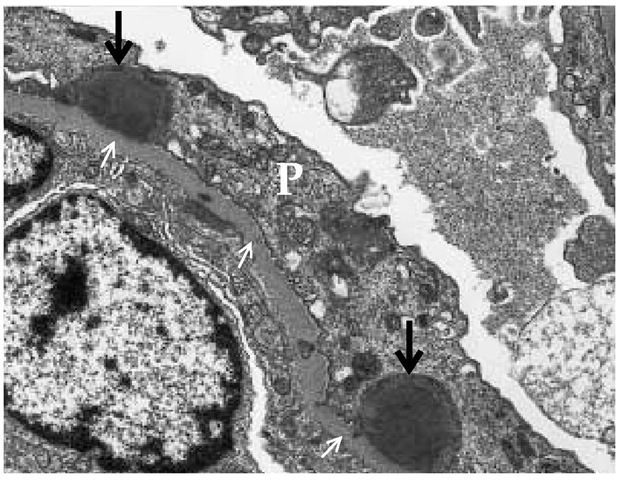{kind=link}
{kind=link}
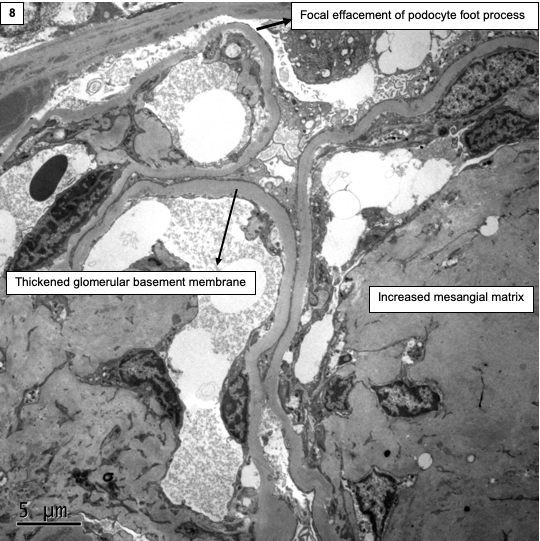{kind=link}
{kind=link}
{kind=link}
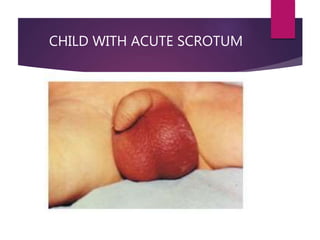{kind=link}
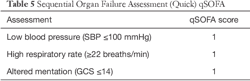{kind=link}
{kind=link}
{kind=link}
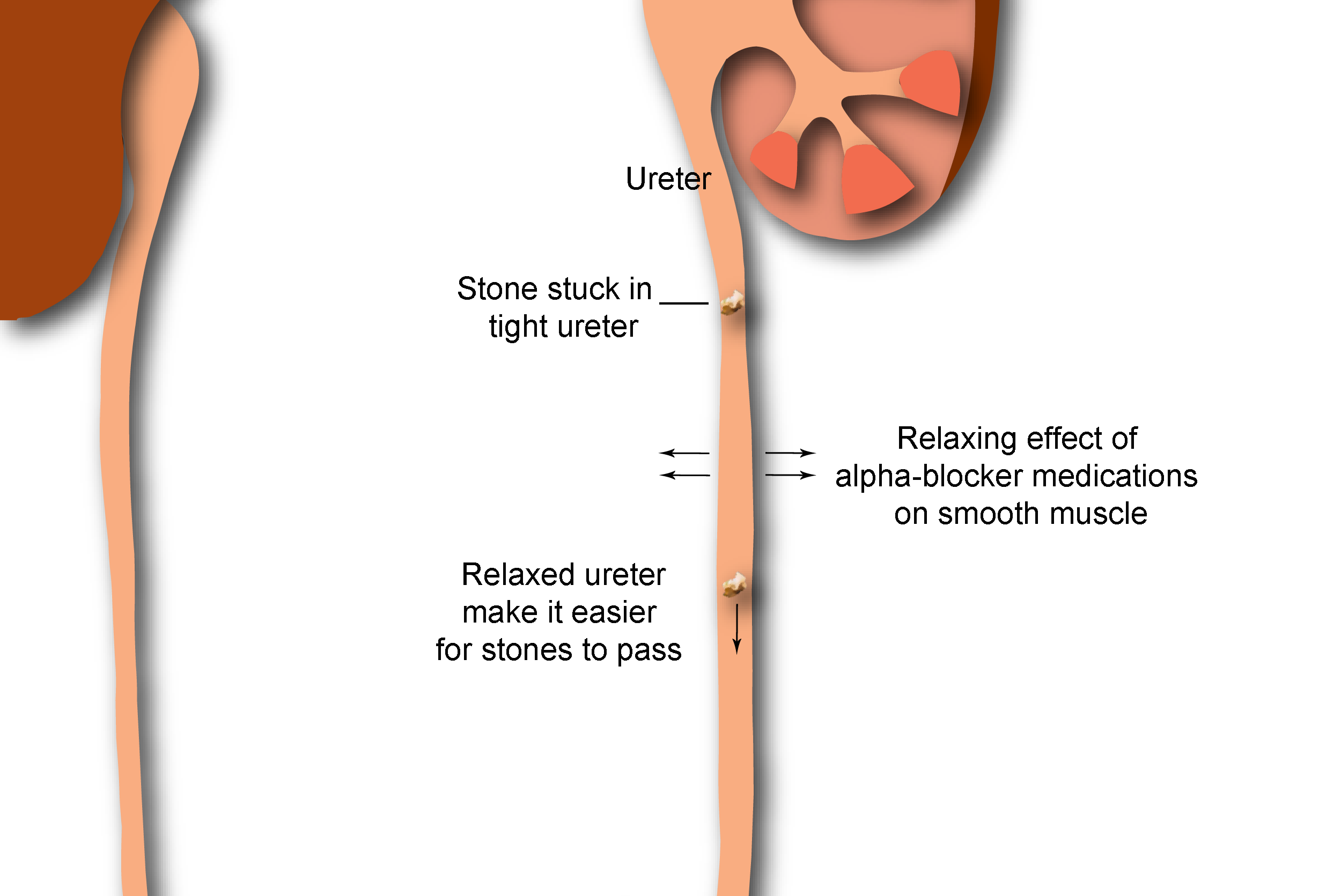{kind=link}
{kind=link}
{kind=link}
{kind=link}
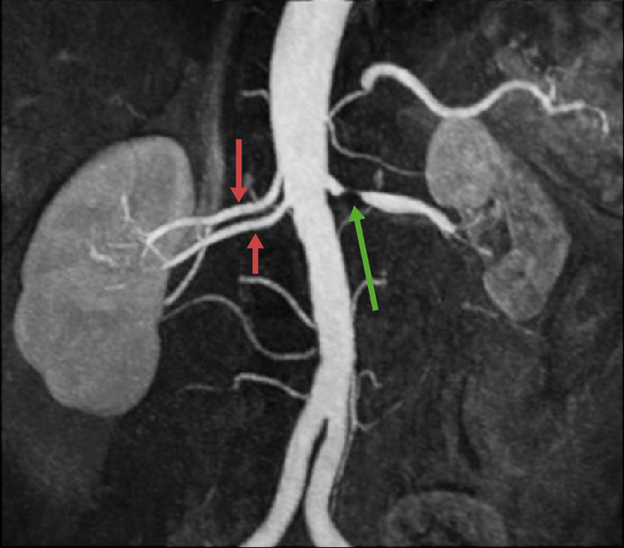{kind=link}
{kind=link}
{kind=link}
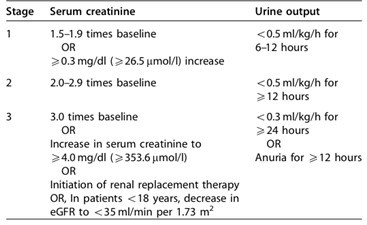{kind=link}
{kind=link}
{kind=link}
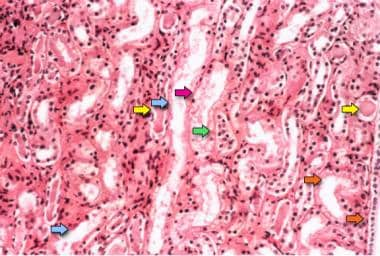{kind=link}
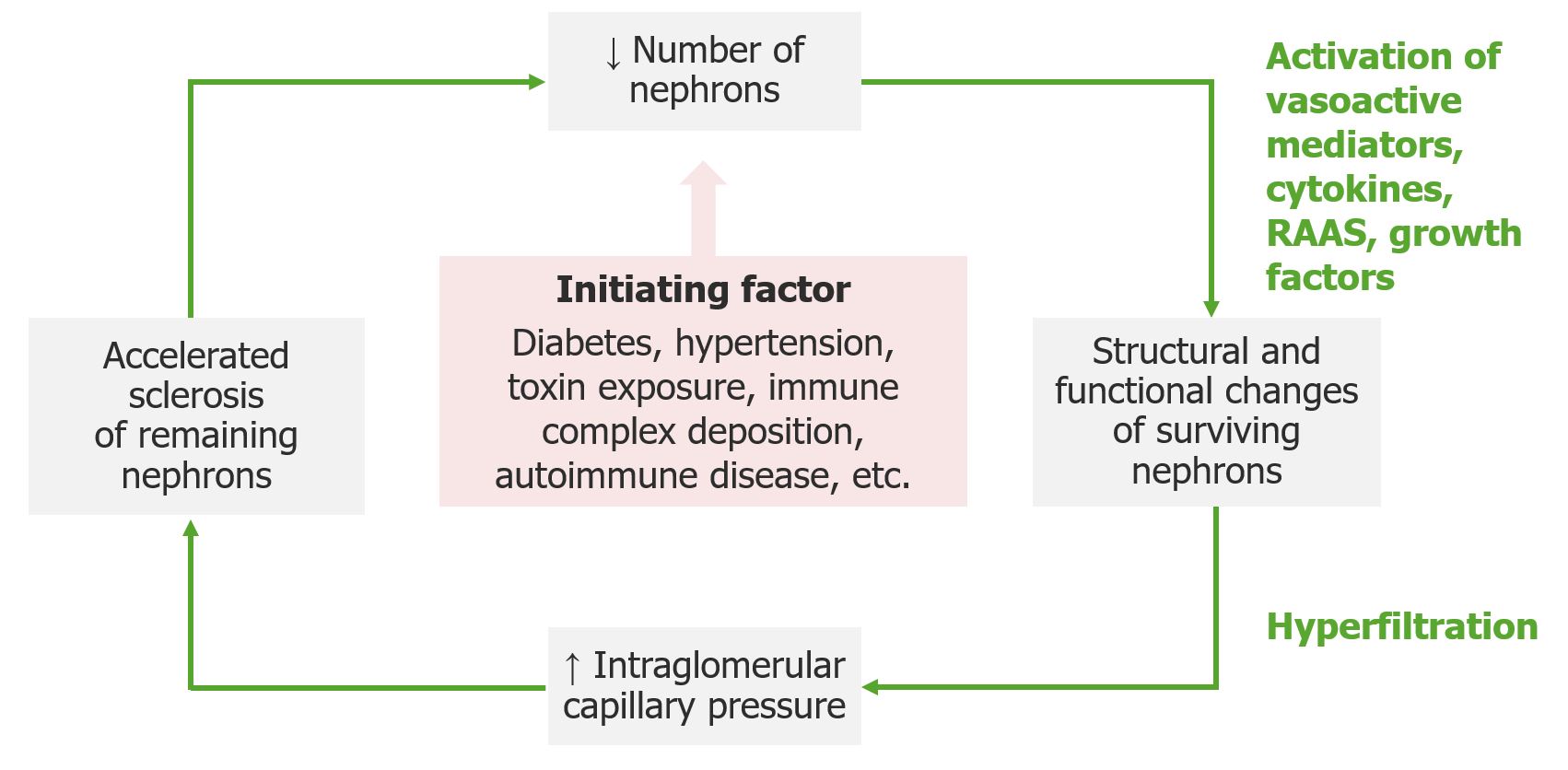{kind=link}
{kind=link}
{kind=link}
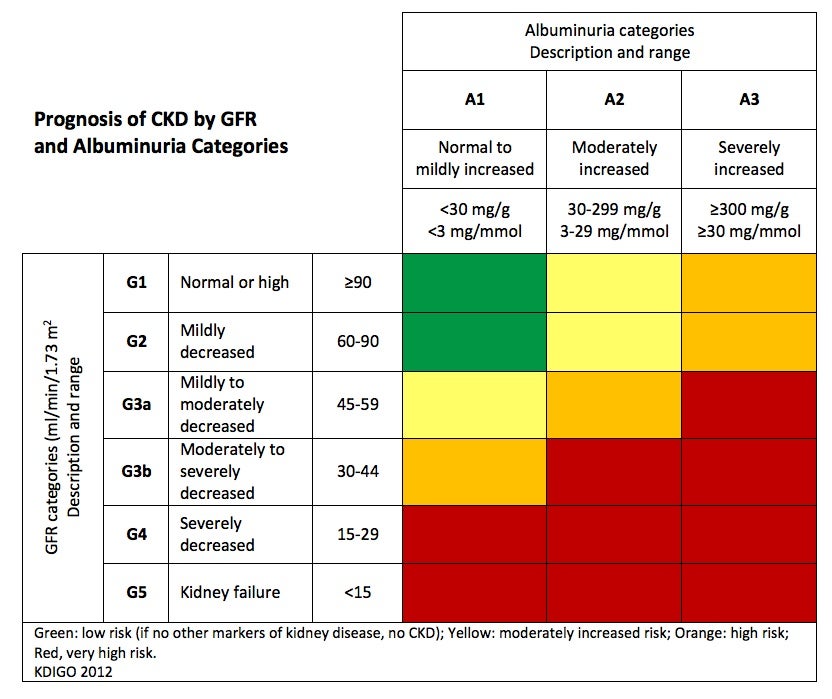{kind=link}
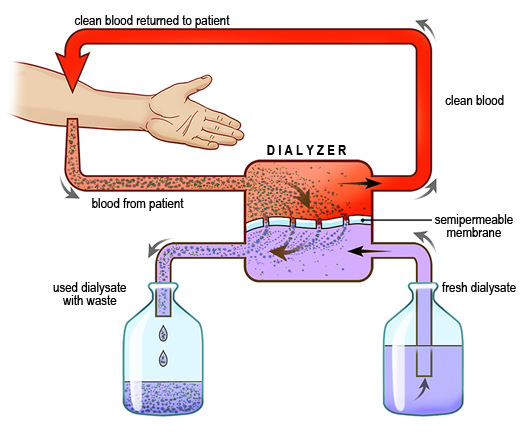{kind=link}
{kind=link}
{kind=link}
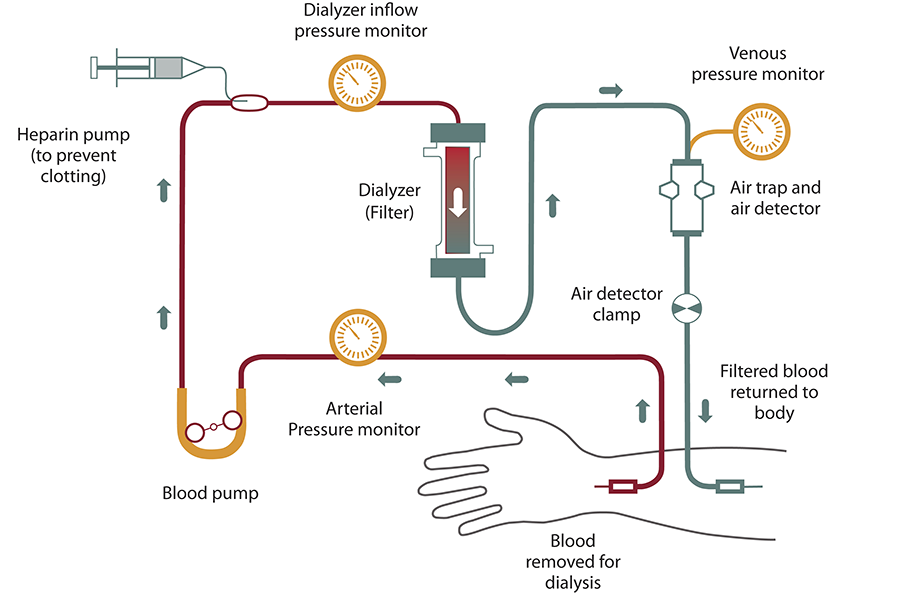{kind=link}
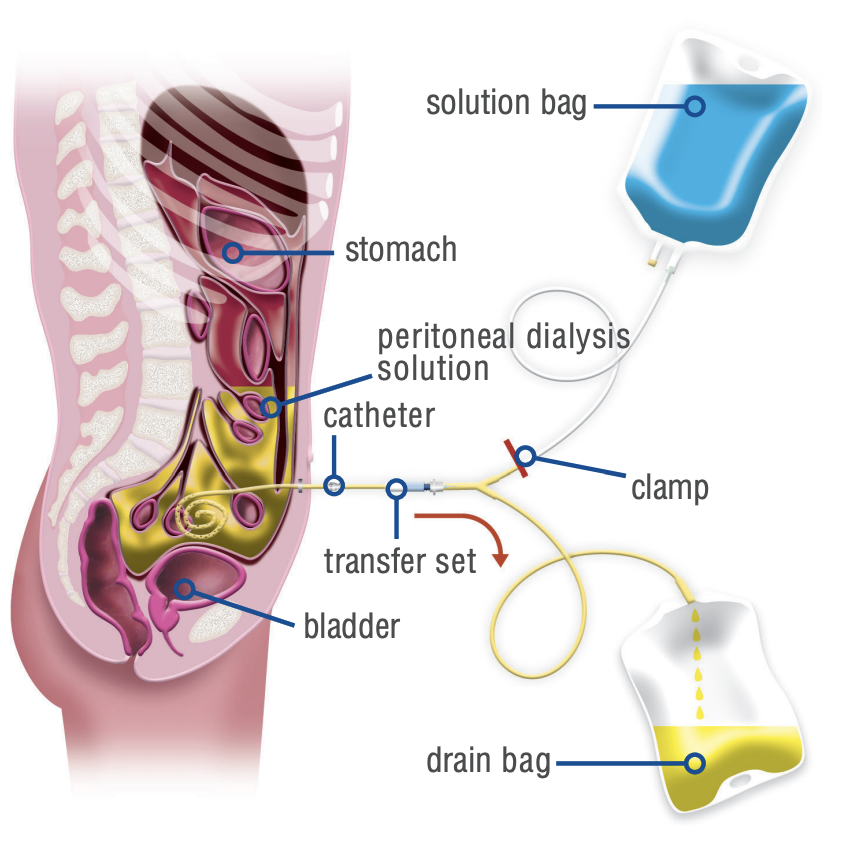{kind=link}
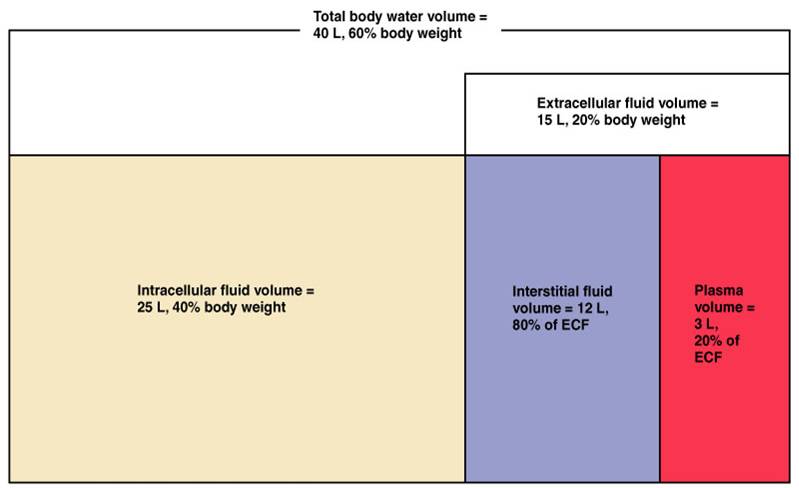{kind=link}
{kind=link}
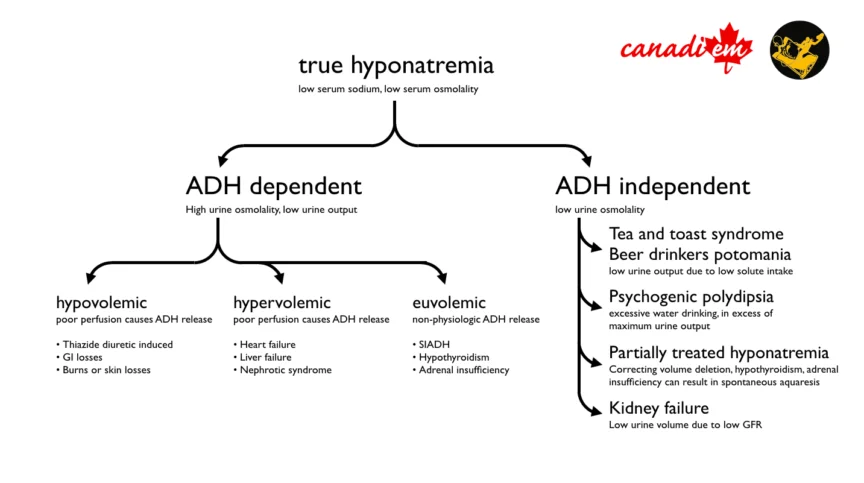{kind=link}
{kind=link}
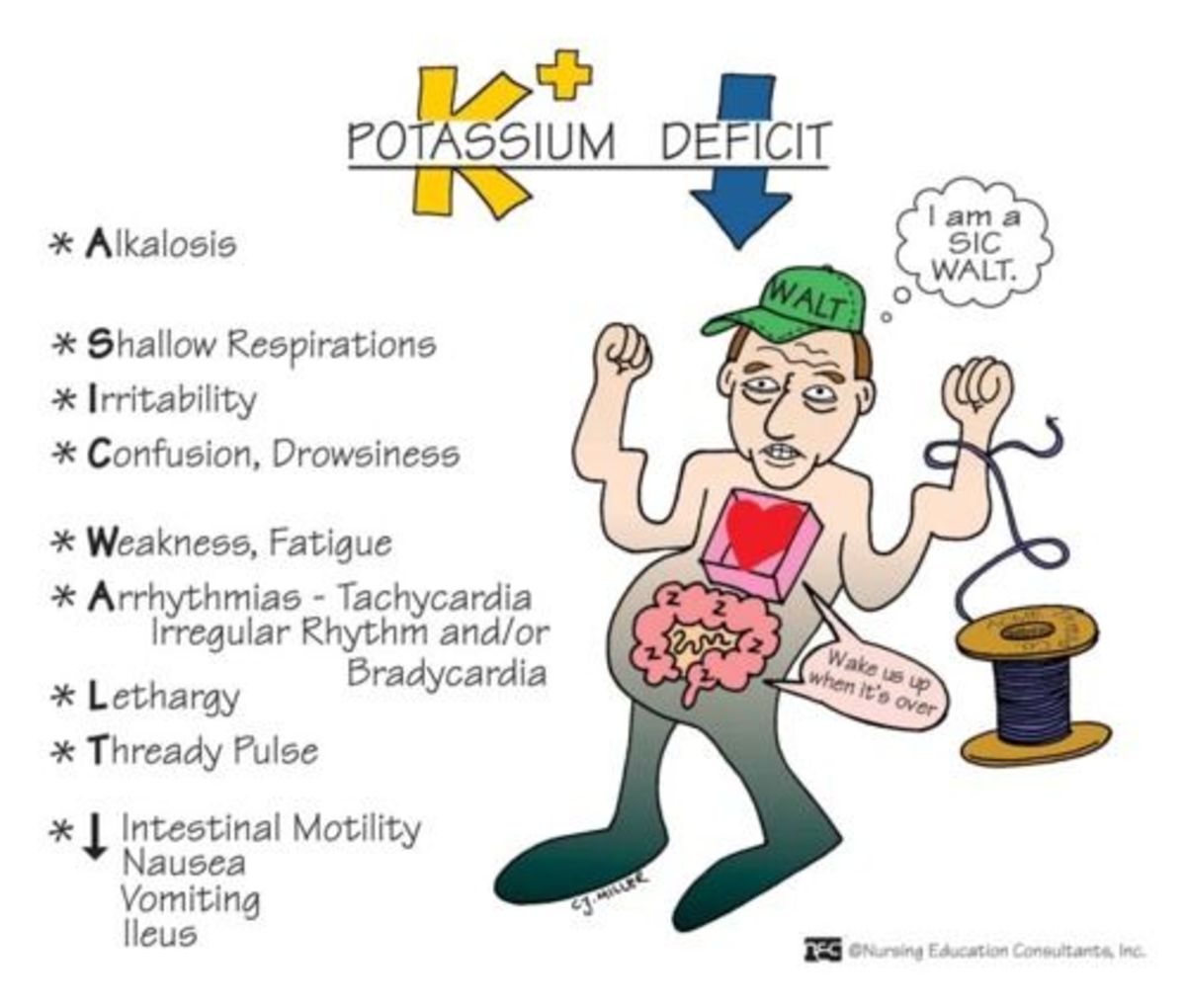{kind=link}
{kind=link}
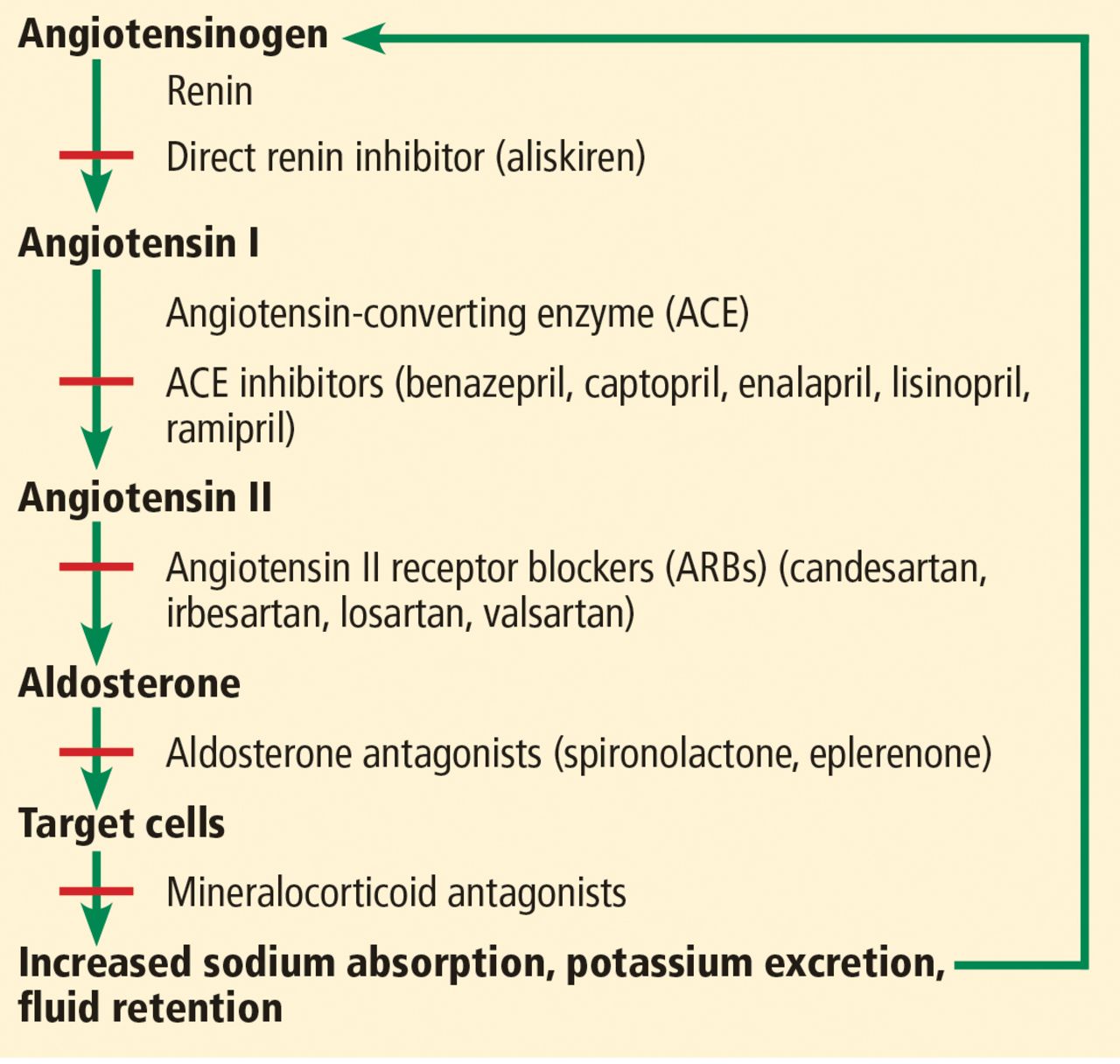{kind=link}
{kind=link}
Spurious hyperkalemia can appear due to fist clenching or tourniquet
Wenn die Erys platzen beim abbinden
- Cardiac toxicity
- Muscle warkness + paralysis
- metabolic acidosis
- high, narrow T wave + short QT-interval
- K>7: wide QRS, AV-blocks
- Vfib, bradycardia, asytole
- Antagonize membrane effects
- Bring K+ into cells
- Decrease total K+
Restriction of K intake through diet and stopping hyperkalemiant medication
- Bicarbonate
- Furosemide
- Fludrocortisone

9-10,5
- Hyperparathyroidism (primary or secondary (low VitD in chronic renal insuff)
- Malignancy (solid tumors of the lung, esophagus, cervix, breast, and kidney producing PTHrP - cytokine-mediated local osteolysis associated with breast cancer, multiple myeloma, or other hematologic cancers)
- Vitamin D excess (Overdose+ Granulomatous D → Hodkin Lym, TBC)
DD between causes:
Check PTH, Tumor marker, VitD levels
{kind=link}
- Pancreatitis
- Peptic ulcer
- vascular calcifications
- HT
- Renal diseases (nephrolithiasis, nephrogenic DI)
→ >14
- i.v. rehydration
- Biphosphonate
- Calcitonin
- Hemodialysis
same, + glucocortioids if due to VitD excess
🧪 Acid-base disturbances
- Acidosis is any process that, if unopposed, will result in acidemia. Acidemia is defined as a serum pH < 7.35.
- Metabolic acidosis is the process that reduces the bicarbonate (HCO3) concentration and lowers the pH.
- Respiratory acidosis is the process that raises the partial pressure of CO2 (PCO2) and lowers the pH.
- Alkalosis is any process that, if unopposed, will generate alkalemia. Alkalemia is defined as a serum pH greater than 7.45.
- Metabolic alkalosis is a process that raises the HCO3 concentration and increases the pH.
- Respiratory alkalosis is a process that reduces the pCO2 and raises the pH.
- Arterial blood: pH = 7.36 - 7.44; HCO3 = 21 - 27 mEq/L; and PCO2 = 36 - 44 mmHg.
- Venous blood: pH is 0.02 - 0.04 pH units lower, the HCO3 is 1 - 2 mEq/L higher, and PCO2 is 3 - 8 mmHg higher than in arterial blood.
if HCO3 low → CO2 low, if HO3 high → CO2 high + vice versa
MetAc(low HCO3) → low CO2
MetAl(high HCO3) → high CO2
ResAc (high CO2) → high HCO3
ResAl (low CO3) → low HCO3
decr. HCO3
just last to digit of ph
Compensation rules are:
- pCO2 = 1.5 (HCO3-) + 8 ‡ 2
- pCO2 = last 2 digits of pH
High anion gap metabolic acidosis → accumulation of unmeasured anions
AG = [(Na+K)-(CI+HCO3)]= 8 +/- 2 mEg/l
renal failure
GOLD MARK
- Glycols (ethylene, propylene)
- Oxoproline (5-) (pyroglutamic acid)
- L- lactic acid (tissue hypoperfusion)
- D - lactic acid, generated from carbohydrates by Gl bacteria
- Methanol - formic acid
- Aspirin - multiple organic acids
- Renal failure (Uremia) - multiple organic and inorganic acids
- Ketoacidosis - B-OH-butyric and acetoacetic acid
- Renal tubular acidosis
- Early renal failure
- Bicarbonate GI losses
- Carboanhydrase inhibitors → Acetazolamide (mechanism see Type 2 RTA)
- Dilution acidosis

renal acid secretion
metabolic acidosis
Type 1: Distal tubule / Distal RTA: Defect in H+ secretion
Type 2: Proximal RTA: Defect in reabsorption of HCO3- due to Carboanhydrase-Deficiency
Type 3: Mixed 1. + 2. (rare)
Type 4: Hyperkalämic acidososis → Hypoaldosteronism/Resistance
LOW
yes type 2 is pretty slight, here its severe
acid buffering is even stronger → ↑↑Ca2+
→ Nephrolithiasis + -Calcinosis
→ Hypercalciuria
- Auto-immune (Rheumatoid arthritis, Sjögren's syndrome)
- Hypercalciuria
- obstructive uropathy
Na-Bicarbonate (NaHCO3)
- Carbonic anhydrase inhibitors
- Fanconi syndrome
- renal transplant
- genetic
- Myeloma
- Amyloidosis
due to acid buffering
→ Growth retardation, rickets, osteomalacia
Alkali supplement in growth periods
- generalized proximal tubular dysfunction
- hyperchloremic metabolic acidosis = proximal RTA
- phosphaturia with hypophosphatemia
- renal glucosuria
- aminoaciduria, tubular proteinuria
- Diabetes Mellitus
- Tubulointestinal nephropathy
- ACEI, Spironolactone, NSAID

- altered mental status
- CV-dysfunction → central constriction, periph dilation
- Hyperventilation
- Bone demineralization → Acid buffering
- hyperkalemia+hyponatremia → compensatory
- hypercatabolism

Mechanism of bone deminalization:
higher pCO2
inc. HCO3
ACUTE: ↑10 pCO2 → ↑1 HCO3
CHRONIC: ↑10 → ↑4
Any diseases that lead to a decr. in CO2 expiration
- COPD / Asthma
- CNS disorder: neuromuscular, drug induced (resp depression)
- Chest wall abnormalities
- Congenital central hypoventilation synrome
ACUTE: ↓10 pCO2 → ↓2 HCO3
CHRONIC; ↓10 → ↓5
- hyperventilation → decr. CO2
- Anxiety
- CNS
- Catecholamines
- Pregnancy , Progesterone
- Hyperthyroidsm
- Liver disease
- Sepsis, Endotoxemia, Hypoxia

high Hco3
incr. pCO2 (=HCO3 + 15)
- pCO2 increases by 0.6 mm Hg per 1 mEq/L increase of HCO3.
- pCO2 should increase to greater than 40 mmHg and is usually less than 55 mmHg.
- pCO2 is equal to HCO3 plus 15 when HCO3 is between 28-40 mmHg.
low Volume/Salt
low perceived volum/salt by the kidney
→ reabsorption salt&water + conc. urine
→ higher Volume → Higher GFR → ABility to excrete HCO3
- natrium bicarbonate infusions
- Ringers lactate (metabolism by the liver to bicarbonate)
- Antacids
- Steroids

- poor kidney function → no excretion
- VOMITING, CHLORID-WASTING DIARRHEA
- perceived extracellular fluid volume deficit (HCO3 needs Na to be excreted)
- OR Cloride deficit
- High Aldosterone
- high steroids
- aldosteron secreting adenoma
- Diuretics
- intermitted Cl concentration
- Bartter / Gitelman syndrome
- Hypotension + high chloride
→ Hypotension + Low urine chloride (<15)
⇒ give NaCl
→ Hypertension + high urine Chloride (>15)
→ NaCl unresponsive
Endogenous sources of HCO3
- Perceived extracellular fluid volume deficit (HCO3 cannot be excreted without Na) or a chloride deficit (minimal distal CI delivery)
- Vomiting 📷 or nasogastric suction/chloride-wasting diarrhea, villous adenoma
- Cystic fibrosis, Post-hypercapnia
- Persistent mineralocorticoid activity (stimulates H and K excretion)
- Volume expanded and hypertensive with high urine; he is NaCl unresponsive
- Aldosterone-secreting tumor/Cushing syndrome, exogenous steroids, Licorice
- Diuretics
- Drug activity is intermittent/urine [CI] fluctuant
- Volume contracted/hypotensive/with persistent high urine [CI]
- Bartter Syndrome
- Gittelman Syndrome
tubular dysfunction which leads to met.alk.
children
mimic chronic loop diuretics
- hypokalemic metabolic alkalosis
- increased Ca excretion
growth retardation
defective NaCl reabsorption
adults
mimics thiazide diuretics
- hypokalemia
- low Ca excretion
- Gitelman syndrome
- Tubular defect in NaCl reabsorption in the distal tubule
- Presents in adulthood
- Mimics chronic thiazide diuretic ingestion
- Manifests as metabolic alkalosis and severe hypokalemia
- Polyuria with normal concentrating ability
- Low urinary calcium excretion, renal magnesium wasting, and hypomagnesemia
- Symptoms include cramps of the arms and legs and fatigue.
- Treatment of patients with Barter and Gitelman syndromes typically involves
- Lifelong administration of a drug that blocks distal tubule potassium elimination (e.g., spironolactone)
- Supplementation with KCl and Mg
incr. function Sodium channal collecting tubule in childhood
→ HT, HypoK, metabolic acidosis
Tx: Amiloride/triamterene
Decreased cerebral blood flow (depleted volume)→ seizures, mental status, neuromuscular weakness
Arrythmias
Myocardial necrosis
Decreased cardiac putput → Hypotension
OTHER WAY AROUND
Compensatory:
respiratory depression
Hypoventilation
Atelectasis
Low K → Resp. Muscle fatique
Low Ca
incr. lactate
volume depletion
inc. anion gap
🧬 Hereditary Nephropathies
50%
15
hereditary nephropathy: characterized by formation of renal cysts in adults causing bilateral kidney enlargement and development of progressive renal failure.
! The most common hereditary nephropathy ⇒ The 4th leading cause of ESRD Prevalence: 1: 500 - 1: 1000 births PKD1 80-90% PKD2 10-20%
⇒ 📷
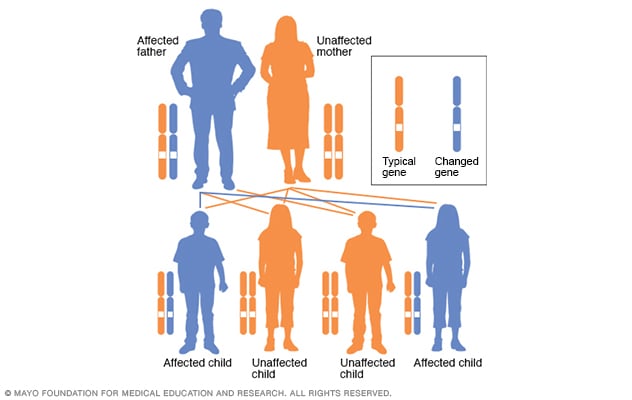{kind=link}
- Tubular dysfunction → polyuria, polydipsia, nocturia
- Lumbar pain
- Hypertension
- UTI
- Hematuria
- Nephrolithiasis
- Obstructive ARF (rare)
- Renal cell carcinoma (rare)
- Progressive renal failure → ESRD
- liver cyst
- brain aneurysm
- heart valvular abnormalities
- cysts elsewhere
symptomatically, drainage, when infected→AB
SUBARACHNOID HEMORRHAGE! at age 40y
⇒ SCREENING!
imaging → US
CT, MRI can be used substituially
Age | Cysts |
15-39 | ≥3 uni or bilat |
49-59 | ≥2 bilat |
≥60 | ≥4 bilat |
- Patients with PKD tend to experience frequent urinary tract infections.
- Cyst infections can be challenging to treat due to the limited penetration of many antibiotics into the cysts.
- However, lipophilic antibiotics such as quinolones (e.g., ciprofloxacin), trimethoprim, chloramphenicol, and vancomycin can effectively penetrate into the cysts.
- HT or hematura,pain,infection BEFORE the age 35
- enlarged kidney
- Proteinuria
- low GFR
- Multiple UTI
- Male
- Hypertension <35 years old
- First urological event <35 years old (hematuria, pain, infection)
- Younger age at baseline
- Increased total kidney volume
- Proteinuria
- PKD1 mutation
- Decreased GFR
- Multiple urinary tract infections
ADH → cyst growth
no ADH → no growth
high water intake, VasopressinR-blocker → no ADH
HT: RAAS inhib + sodium restric.
threat UTI, hematuria, nephroplith
surgical decompression in extrarenal
- Symptomatic treatment:
- Sodium restriction, statins, increased water intake
- Arterial hypertension: ACEI/ARBs, target BP <120/80mmHg
- Treat urinary tract infections, hematuria, nephrolithiasis
- Treatment of chronic renal insufficiency/ESRD: dialysis, transplantation
- Treatment of extrarenal complications
- Surgical decompression is indicated in very large cysts in patients with severe pain.
ADPKD Treatment:
- Vasopressin receptor 2 antagonist (Tolvaptan)
- It has a renoprotective effect and slows cyst growth through decreased fluid secretion.
- It can extend time to ESRD from 6.2 to 9 years.
- urine culture pos in AP, neg. in ICI
- AB!
Acute pielonephritis | Intrachistic infection |
Diffuse lumbar pain | Well localized lumbar pain |
Fever | Fever |
Positive urine culture | Negative urine culture |
Duration of treatment 10-14 day | Duration of treatment 4-6 weeks |
Antibiotics like in pyelonephritis | Antibiotics which penetrate into the cysts |
Additionally:
Nephrectomy is indicated only in patients with recurrent infections in association to renal failure, severe recurrent bleeding, or markedly enlarged kidneys with persistent and severe pain.
most of the time x-linked mutation of a alpha chain of collagen type 4
nephritic + progressive renal failure
- progressive renal failure (ESRD by the 15-35)
- hematuria (mainly presents as nephritic)
- proteinuria (can be up to nephrotic range)
- HT
→ check for extrarenal!
and Hypertension!
- Bilateral sensorineural hearing loss/deafness.
- Ocular manifestations: Anterior lenticonus 📷 - seen in 20-30% of males with Alport syndrome and is pathognomonic for the disease.
- Leiomyomatosis (2-5%): Benign tumors characterized by visceral smooth muscle overgrowth within the respiratory and gastrointestinal systems.
- Clinical : Family history of hematuria or Renal failure +/- sensorineural deafness
- Renal and skin biopsy
- Molecular genetic testing
- IGA Nephropathy
- Good Pasteur
- Thin basement membrane nephropathy
- Light microscopy and immunostaining = non-specific.
- Electron microscopy shows diffuse thickening of the GBM with splitting and lamellation 📷 = diagnostic for Alport syndrome.
non-specific
- In patients who develop end-stage renal disease transplantation/ dialisys
- RAS inhibitors (ACE/ ARBs) reduce proteinuria, slow down the progression of chronic renal failure
- x-linked transmission
- deficient galactosidase A 🌌 (lysosomal enzyme)
- deposition of Glycolipids (Glycosphingolipids) in lysosomes
→ multisystemic accumulation
- signs of periph polyneuropathy in fingers + toes
- blue black angiomatous macules
- upper eyelid edema
Pain, numbness of fingers and toes Telangiectasias on ears, conjunctiva Blue-black angiomatous macules or papules Edematous upper eyelids Raynaud phenomenon Ophthalmologic abnormalities
30-40
due to HT → LVH, Cardiomyopathy, Stroke
Renal insuff
proteinuria (usually sub-nephrotic)
hematuria
unexplained renal failure
- Low alpha-Gal A activity in leukocytes or plasma
- Mutation analysis of the alpha-Gal A gene
light microscopy → podocyte + tubular epithel. cell vacuolization
electronmicroscopy → zebra bodies (glycolipid deposits) 📷
Enzyme replacement tx → recombinant alpha-Gal A (slows progression) → Also given in patients with ESRD to reduce other organ involvement (cardiac/neurologic)