







Nephrology
- Nephrology
- 🧶 Glomerular syndromes
- 🥇 Primary glomerular diseases 🔒
- 🥈 Secondary glomerular diseases 🔒
- 🚇 Tubulo-intestinal kidney disease 🔒
- 🩸Vascular nephropathies 🔒
- 💥 Acute renal injury 🔒
- 🕰️ Chronic renal injury 🔒
- 🔁 Renal replacement therapy 🔒
- 💧 Hydro-electrolytic disturbances 🔒
- 🧪 Acid-base disturbances 🔒
- 🧬 Hereditary Nephropathies 🔒
🧶 Glomerular syndromes
- 1. General 🔒
- 2. Mechanisms of injury 🔒
- Proteinuria >3,5g/24h
- Hypoalbuminemia <3g (+/- hypoproteinemia <6g/dl)
- Edema
normal serum albumin is 3,5 - 5,4 g/dl
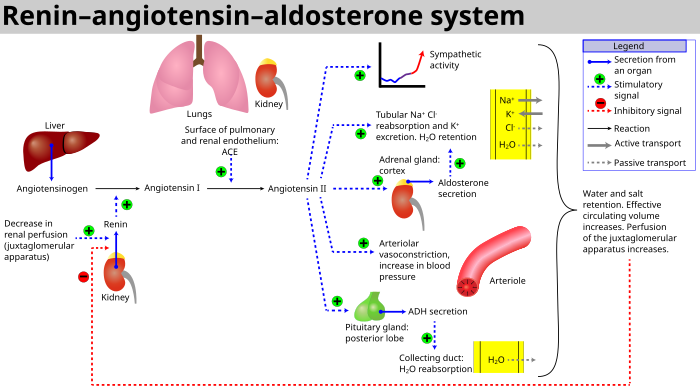
↓ albumin → efflux water into interstitium → ↓ blood V → RAAS activation 📷
→Renin → activation Angiotensin → increased hydrostaic pressure
→ Aldosteron: Na + H2O retention
→ More fluid eflux out of vessels
→ hyperosmolarity (Na etc) of blood → triggers ADH → more H2O retention → more water efflux
edema is not caused by incr. hydrostatic capillary pressure but by low oncotic pressure → edema is not gravity dependend
👁️ peri-orbital (= loose tissue) → fluid efflux in the loose tissue doesn't ↑ the local pressure first → more fluid can accumulate
Periorbital (albumin-related edema doesn't follow gravity)
↓
Peripheral pitting
Pleural/Pericardial effusion + ascites
↓
Anasarca = generalized edema
- hyperlipidemia/dylipidema + xanthoma/xanthelasma, (+lipiduria arterioscleorsis+CAD risk)
- hypercoagulable state → increased risk of thrombosis
- Incr. susceptibility to infections
- Frothy urine (foam on beer 🍺)
- hypocalcemia + anemia→ in chronic stages
- symptoms of underlying diseases (e.g. malar rash in lupus)
- hyperlipid → compensatory synthesis by liver to restore normal oncotic pressure + urinary loss of lypolysis enzymes
- hypercoagulation/thrombosis → urinary loss antithrombin III/protein C+S + hepatic synth. of procoagulant factors due to compensation + coagulations-cascade-activation due to glomeruli mediated lesions
- infections → urinary loss of IgG, reduced complement activity, complement urine loss, reduced Tcell function + proteins malnutrition(due to loss)
- Hypocalcemia → due to Vit-D deciciency → incr. PTH → incr. bone resorption
- Anemia due to loss of transferrin + less EPO
F - Azotemia and hypertension are uncommon initially, but their presence may indicate advanced disease
Hematuria might also be present
minimal change, focal segmental glomerulosclerosis, membranous nephropathy
can manifest as nephrotic or nephritic sy., like diffuse proliferative GN (in lupus)
minimal change
FSGS
focal segmental glomerulosclerosis
Membranous nephropathy (MN)
most common etiology depends on age:
Children | Minimal change |
Young adults | MN |
Old adults | FSGS |
Diabetic nephropathy, amyloid np., lupus nephritis + diffuse proliferative GN
lupus can also manifest as nephritic synd.
qualitative: urine dipstick
quantitative: 24-hours urine protein evaluation
hematuria

{kind=link}
hematuria with acanthocytes + RBC cast

FSGS + membranous nephropathy
🤡 hemoconcentration due to plasma volume loss
secondary cause of nephrotic syndrome (e.g., SLE, other inflammatory conditions, or malignancy).
ATIII, proteins S, plasminogen → decreased antithrombotic factors (urinary losses)
fibrinogen, d-dimer→ increased procoagulant factors (compens. synthesis)
LDL, TG → increased (compens. synthesis)
decr in chonic → no activation by the kidney
incr. ESR + CRP, WBC may suggest underlying infection, inflammatory condition, or vasculitis.
see etiologies below
Immunological screening:
- ANA, anti-dsDNA
- C3, C4
- ANCA
- rheumatoid factors
- ASLO (antistreptolysin O)
- no secondary cause found
- also in lupus to differentiate the types
- advanced CKD → fibrotic tissue on → biopsy doesn't give good tissue
- hyperechogenic small kidney on US <9cm
- severe uncontrollable HT
- uncontrollable bleeding diathesis (Neigung)
- Infection: Hydronephrosis, bilateral cysts, acitve renal/perirenal infection
- solitary kidney
sodium + fluid restriction
diuretics (furosemid = first line)
consider i.v. albumin
RAAS inhibitation: ACEI (ramipril) or ARB (losartan)
- AKI, aprupt onset of NS (like minimal change)
- hyperkalemia
not to much, not to little
Patients with nephrotic syndrome are at risk of protein malnutrition. While lowering dietary protein intake can lead to a reduction in proteinuria, very low-protein diets should be avoided because of the increased risk of malnutrition. High protein intake may help offset urinary protein loss, but very high-protein diets are discouraged because of the risk of worsening proteinuria.
usually resolves after treatment of underlying cause + reduction of proteinuria
→ Lipid lowering therapy: Statins (eg. atorvastation)
3.0 g/L
prophylactic anticoagulation (e.g. heparin)
- vaccination → influenz + pneumococcal
- consider AB-therapy
- Sodium + fluid restriction
- Diuretics
- RAAS-inhib (ARB , ACEI)
- Statins
- Anticoagulation
additional: i.v. albumin, protein diet, vaccines
see etiologies below
artherosclerotic complication → MI, stroke
FSGS + membranous nephropathy
increased size (+/- number)→ non-selective proteinuria + hematuria
glomerular inflammation → GBM disruption
inflammated glomeruli swell up (inflammatory infiltrate, clots,..) → less blood flow to the kidney → decr. GFR
- Hematuria with acanthocytes
- RBC casts
- Hypertension → mild to moderate Edema + oliguria
- Renal insufficiency (decr. GFR): esp. Azotemia + Crea (+ anemia)
- Oliguria: inflammatory infiltrates reduce fluid movement across the membrane (↓ GFR) → oliguria + pyuria (leukocyturia)
- mild - moderate Proteinuria <3,5g/24h
A type of dysmorphic red blood cell characterized by irregular, thorn-like cytoplasmic projections.
RBC are stuck inside tubules 📷 → increase pressure from the fluid → get compressed with proteins
{kind=link}
decreased GFR →less water excretion
→ activation RAAS due to less effective volume+Na reaching macula dense
→ Angiotensin → incr. BP
→ Aldosteron → water + sodium retention
GFR is reduced → you cant piss out se proteins
Possible development into Nephritic syndrome → Check for hematuria+ acanthocytes, RBC cast , Azotemia!
OR due to renal failure
attraction of macrophages + cytokines
stimulation epithelial cells → growth factor
⇒ extreme cellular proliferation in urinary space ⇒ cellular crescent ⇒ rapidly progressive GN ⇒ rapid renal failure + Uremia
post-streptococcal / post-infectious GN
IgA Nephropathy (Berger disease)
= Rapidly progressive GN
- Goodpasture
- Small vessel vasculitis
- immune complex mediated diseases (like Lupus, IgA nephropathy, post-strep GN)
→ more details RPGN
Alport
- All causes for RPGN
- Lupus
- Alport
→ dont forget about Lupus which can manifest as diffuse proliferative GN
Nephritic sediment:
- Hematuria + acanthocytes
- RBC cast
- Mild to moderate proteinuria
- sterile pyuria +/- WBC
- no RBC cast + acathocytes
bright red or pink urine, the occurrence of blood clots, normal RBC morphology, and the absence of RBC casts.
- high Crea (low GFR)
- Azotemia with inc. BUN
- Specific: Complement, ANA, ANCA, anti-GBM etc
- when nonspecific disease pattern to confirm diagnosis
- lupus - classification
ACE-I or ARB
diuretics
Low sodium diet + water restrictrion
immunosuppression
plasmapheresis to remove antibodies
dialysis, transplantation
🥇 Primary glomerular diseases 🔒
Non-proliferative
- 1. Minimal change disease
- 2. Focal segmental glomerulosclerosis
- 3. Membranous nephropathy
Proliferative
- 1. Membranoproliferative glomerulonephritis
- 2 . IgA nephropathy
🥈 Secondary glomerular diseases 🔒
- 1. Lupus Nephritis
- 2. Rapidly progressive GN
- 3. Renal amyloidosis
- 4. Infectious-related GN
- 5. Diabetic kidney disease
- 6. Neoplasia associated glomerular disease
- 7. Hereditary glomerulopathy: Alport syndrome, Fabry disease
🚇 Tubulo-intestinal kidney disease 🔒
- 1. Acute interstitial nephritis
- 2. Chronic tubulointestinal nephropathies
- 3. Urinary tract infections
- 4. Uro/Renal lithiasis
🩸Vascular nephropathies 🔒
- 1. General
- 2. Hypertensive nephrosclerosis
- 3. Acute hypertensive nephrosclerosis
- 4. Renal artery stenosis
💥 Acute renal injury 🔒
- 1. Definition
- 2. Staging
- 3. Etiology
- 4. Clinical presentation
- 5. Diagnosis
- 6. Management
- 7. Prognosis
- 8. Contrast-associated acuted kidney injury
🕰️ Chronic renal injury 🔒
- 1.General
- 2.Chronicity
- 3.Etiologies and risk factors
- 4.CKD Assessment
- 5.Pathophysiology
- 6.CDK progression
- 7.Management
- 8.Evolution and prognosis of CDK
🔁 Renal replacement therapy 🔒
- 1. General
- 2.Hemodialysis (HD)
- 3.Peritoneal Dialysis (PD)
- 4.Renal transplantation
- 5.Other blood purification techniques
💧 Hydro-electrolytic disturbances 🔒
- 1. General
- 2. Hyponatriemia
- 3. Hypernatriemia
- 4. Hypokaliemia
- 5. Hyperkaliemia
- 6. Hypercalcemia
🧪 Acid-base disturbances 🔒
- 1. Definitions
- 2. Metabolic acidosis
- 3. Respiatory acidosis
- 4. Respiratory alkalosis
- 5. Metabolic alkalosis
🧬 Hereditary Nephropathies 🔒
- General
- Autosomal dominant polycystic kidney diseases
- Alport syndrome
- Fabry diseases
- Tuberous sclerosis complex