





Anaesthesiology & Intensive Care
💉 Types of anesthesia
Inhaled or IV
Anesthesia encompasses three essential reversible components:
- immobility
- amnesia
- unconsciousness
BIS-Monitor (BIS = bispectral index) 📷
{kind=link}
- 0 = Øbrain activity; 100 = awake
- BIS GOAL during SURGERY = 40-60
→ too high (= too little anesthesia)→ pain + awake
→ too low (= too much anesthesia) → SEE + prolonged waking-up
(= monitor to measure brain response during anesthesia ⇒ adjustment of drug dosages)
The BIS index, also known as the bispectral index, is used to evaluate the depth of anesthesia and monitor cerebral function during anesthesia. It measures the brain's response to anesthesia and helps adjust drug dosages accordingly. The BIS index ranges from 0 to 100, with 0 indicating no brain activity and 100 indicating full wakefulness.
During surgery, the goal of the BIS index is usually to maintain a range of 40-60. If the index is too high (above 60), it may indicate that there is too little anesthesia, which can result in the patient experiencing pain and being awake during the procedure. On the other hand, if the index is too low (below 40), it may indicate that there is too much anesthesia, which can lead to prolonged waking up after the surgery.
- INDUCTION
- put patient asleep (usually propofol (children: sevoflurane) + fentanyl)
- give muscle relaxant (rocuronium or succi)
- consider adjuvants (midazolam or lidocaine)
- intubate
- MAINTENANCE
- keep patient asleep iv/inhaled - or combination (usually propfol or inhaled + fentanyl)
- EMERGENCE
- Stop anesthetics
- stop +/- reverse neuromuscular blockade
- Extubate
- Terminate general anesthesia and extubation
- Discontinue all drug and volatile agents
- Administer reversal agents for non-depolarizing relaxants
- Ensure normal neuromuscular function and hemodynamic status
- Confirm spontaneous breathing with adequate rate and tidal volume
- Provide ventilation with 100% oxygen for 3-5 minutes
- Suction secretions from the pharynx
- Deflate cuff and remove endotracheal tube on inspiration
- Confirm adequate breathing after extubation and use a mask for oxygen delivery
- Ensure proper positioning of the patient during transfer
lidocaine:

- Previous surgery and anesthesia, including adverse reactions to specific drugs, difficulties with tracheal intubation, postoperative pain or nausea
- Medication use, including potential drug interactions and insights into medical conditions
- Known allergies or side effects of medications
- Recent history of upper respiratory tract infections, which increases the risk of bronchospasm and laryngospasm after laryngeal instrumentation, particularly in children and the elderly

{kind=link}
AIRWAY EVALUATION score ⇒ HOW DIFFICULT IS THE INTUBATION? (class = ascending difficulty)
{kind=link}
3-3-2 rule → difficult airway?
Evaluate the 3-3-2 rule: This aspect of airway education involves three measurements — the distance between the upper and lower incisors, the distance between the hyoid bone and the chin, and the distance from the thyroid cartilage to the floor of the mouth. Each measurement is assessed using the provider’s fingers and can be done fairly quickly. At least three fingers should be able to fit between the patient’s upper and lower incisors. This doesn’t mean the caregiver must stick their hand in the patient’s mouth. The measurement can be done by holding the index, middle and ring fingers closely together, opening the patient’s mouth by gently pulling down the chin and determining if at least three fingers would fit. Using the fingers held together, assess the distance from the hyoid bone to the chin (should be at least three fingers) and the distance from the thyroid cartilage to the floor of the mouth (at least two fingers). Any measurement that is less than 3-3-2 indicates potential difficulty with airway management.
Pre-operative assessment:
- 🦷 Examine dentition, noting any loose teeth, caps, or crowns that may cause dental damage.
- 🧣Evaluate the upper airway for anatomical abnormalities that could pose difficulties during tracheal intubation.
- 🫀🫁 Be aware that certain diseases, such as ischemic heart disease, heart failure, chronic obstructive pulmonary disease (COPD), and asthma, may worsen during and after surgery.
- Consider assessing cardiorespiratory compromise by having the patient walk up two flights of stairs.
- Elicit information about uncontrolled hypertension, heart valve pathology, arrhythmias, wheezing, chest crackles, tachypnea, and cyanosis, as these may require further investigations.
- Recognize the implications of obesity, diabetes, and liver failure in the pre-operative assessment.
Test | Indications |
BCC | Major surgery requiring group screen or cross match; chronic cardiovascular, pulmonary, renal, or hepatic disease; malignancy; known or suspected anemia; bleeding diathesis or myelosuppression; patient less than 1 year of age |
Sickle cell screen | Genetically predisposed patient (hemoglobin electrophoresis if screen is positive) |
INR, aPTT | Anticoagulant therapy, bleeding diathesis, liver disease |
Electrolytes and | Hypertension, renal disease, diabetes, pituitary or adrenal disease, |
creatinine | digoxin or diuretic therapy or other drug therapies affecting electrolytes; age>50 |
Fasting glucose level | Diabetes (should be repeated on day of surgery) |
Pregnancy (beta-HCG) | Women of childbearing age |
ECG | Heart disease, hypertension, diabetes, other risk factors for cardiac disease (may include age), subarachnoid hemorrhage, CVA, head trauma, age (male>40 y.o., female >50 y.o.) |
Echocardiography | CHF, cardiomyopathy, valvular pathology, limited cardiac reserve, stroke of unknown etiology |
Chest radiography | Cardiac or pulmonary disease, malignancy, age >60 |
ASA Classification (Pre-OP assessement)
Class I: Fit and healthy individual
Class II: Patient with mild systemic disease
Class III: Patient with severe systemic disease
Class IV: Patient with incapacitating systemic disease
Class V: Moribund patient not expected to survive more than 24h
Class VI: Brain death patient


Pre-operative fasting guidelines:
- 8 hours after a meal that includes meat, fried or fatty foods
- 6 hours after a light meal (such as toast, crackers, and clear fluids) or after ingestion of infant formula or nonhuman milk
- 4 hours after ingestion of breast milk
- 2 hours after clear fluids (water, black coffee, tea, carbonated beverages, juice without pulp)
- 💠 ACEi
- 🍌🌊 K+ sparing diuretics
- 🕰️🍬 Hypoglycemic drugs (long acting)
- 🐀 MAOi
- 🪖 Warfarin
- 💊 Oral contraceptives / hormone replacement
how do you assess the risk for complications in..
- Independent predictors of cardiovascular complications: IHD, heart failure, high-risk surgery, insulin treatment, cerebrovascular disease, preoperative creatinine > 177


Disease Process | Risk in Perioperative Period | Important Considerations |
Autonomic Neuropathy | Delayed gastric emptying- aspiration, Painless myocardial ischaemia- silent infarction, Apnoea | Antacid and prokinetic premedication, Investigate for coronary artery disease, Supplement oxygen and monitor breathing |
Peripheral Neuropathy | Pressure necrosis, Increased sensitivity to local anaesthetics | Protect pressure points, Document neuropathies and decrease local anaesthetic dosage |
Vascular Disease | Acute vascular events – MI, CVA | Maintain coronary, renal and cerebral perfusion pressure |
Nephropathy | Acute renal failure | Maintain intravascular volume, Osmotic diuresis may occur with hyperglycaemia, Avoid nephrotoxic drugs |
Immunocompromised | Infection | Antibiotic prophylaxis and treat infection |
Stiff Joints including cervical spine | Difficult intubation and airway management | Avoidance of general anaesthesia if possible |
- Difficulties in obesity:
- Difficult to ventilate and intubate
- Restrictive lung disease
- Obstructive sleep apnea
- Pulmonary emboli
- Atelactasis, aspiration, and infection
- Effects on the heart:
- Increased cardiac work
- Cor pulmonale
- Ischemic heart disease
- Arrhythmias
- Cardiac failure
- Endocrine implications:
- Diabetes mellitus
- Thrombophilia is more prevalent than bleeding tendencies.
- It is crucial to collaborate with a hematologist early on.
- Identify patients at risk of thrombophilia before surgery and manage their risk factors accordingly.
- Patients undergoing major surgery should generally receive thrombosis prophylaxis.
best indicator post-op lung function: exercise tolerance
smoking cessation: 8 weeks pre-surgery

- Alcoholism increases perioperative risk.
- Blood glucose should be checked in patients with a history of excessive alcohol use.
- Alcohol withdrawal syndrome is a life-threatening emergency.
- Cocaine causes a marked increase in sympathetic tone, with its attendant problems.
- Water and electrolyte derangement follow ecstasy ingestion.
- Chronic opiate use results in tolerance and may not be the ideal opportunity to combat addiction during acute hospital admission.
- Cannabis and tobacco use can lead to severe chronic obstructive disease.
- Universal precautions in blood collection
- Avoid reusing disposable equipment or potentially contaminated items
- Healthcare workers should be vaccinated against HBV
- Early post-exposure antiretroviral prophylaxis reduces the risk of HIV infection
- Fluranes ⇒ SEVO-flurane, iso-flurane, des-flurane
SEVOFLURANE:

- NO (nitrous oxide)
🩸 1. BLOOD solublity

⇒ ↑ blood solubility (↓partial pressure) = SLOWER onset +offset
⇒ represented by BLOOD:GAS COEFFICIENT (↑=slower)
→ blood solubility + BGC:
Fluranes = ↑
NO = ↓
(ex. NO = ↓solubility/B:Gc ⇒ quick onset + offset; Fluranes slow onset + delayed offset)
🧠 2. LIPID solubility

⇒ ↑ lipid solubility = ↑POTENCY (= less drug concentration needed)
⇒ represented by OIL:GAS COEFFICIENT (↑=↑potency)
Fluranes = ↑ lipid-sol / OGC
NO = ↓ lipid-sol / OGC
⇒ + INVERSLY RELATED to MAC:
↓MAC = ↑POTENCY (=↓concentration needed)
(ex. NO = ↓solubility/O:Gc = ↑ MAC ⇒ ↑ CONC. needed; fluranes = lower conc. needed)
- 🫁 resp → ↓TIDAL (ØRR) + ↑CO2
- ❤️ myocardial → ↓OUTPUT
⇒ 🤒 fever
⇒ 💪 muscle rigidity
⇒ MUSCLE damage ⇒ ↑CK + K
⇒ including ❤️ ⇒ Tachycardia + ↑BP
→ Tx: Dantrolene, O2, stop drug
- 🍤 ⇒ 🤮nausea/vomitng
- 💨 ↑volume in airspace (due to rapid diffusion into airspaces) ⇒ Ø give in pneu + abdominal distension !
↑ Volume in airspace:

- Halothene → Hepatotox
- Methoxyflurane→ Nephrotox
- Enflurane → seizures
- Induction drugs
- Propofol (only i.v. drug that can be used for maintenance too)
- Etomidate
- Ketamine
- Adjuvant drugs
- Opioids
- Benzodiazepines
- Lidocaine
- 🤮 anti-emetics
- ⚡ anti-convulsant
- 🌕 anti-pruritic (opiods SE)
- 🫁 bronchodilator (good in asthma)
- 🧠 ↓ICP
- 🫁 DEPRESSION
- 🫀 VASODILATION ⇒ HYPOTENSION (compare volatile = ↓output) , minimal HR change
- 💥 injection PAIN→ +- lidocaine / opioids
→ unlikely with central infusion
- 🤮 n + v
- 📐 acute adrenal insuff (transient): cave if adrenal insuff or chronic steroid use
- 💪 myoclonic movement (due subcortical inhib → prevent with opioids/benzos)
- 💥 injection PAIN→ give +- lidocaine / opioids to
→ unlikely with central infusion

- ↑↑🫀 sympathetic activity (↑ HR, BP, SVR, bronchiodilation)
- 🧠 CNS + 🫁 Resp. depression
- ↑↑Analgesia (prop+etom=none)
- rapid onset + offset (like others)
Symph activity: cave in IHD, HT, pulmonary HT, RHF!
Emergence reactions (when “waking up”) → nightmares & vivid dream, hallucination, disorientation ⇒ reduce with benzos (co-administered)
- Sodium thiopental (Pentothal): Ultra-short acting thiobarbiturate-hypnotic. Decreases time CI channels open facilitating GABA and suppressing glutamic acid. Decreases cerebral metabolism, blood flow, cerebral perfusion, cardiac output, blood pressure, reflex tachycardia, and respiration. Popular for induction. Used for control of convulsive states.
- Indications: Induction of anesthesia, control of convulsive states.
- Caution: Allergy to barbiturates, uncontrolled hypotension, shock, cardiac failure, porphyria, liver disease, status asthmaticus, myxedema.
Induction: Etomidate/Propofol (+- adjuv.)
Paralysis: Succi/Rocuronium
- Preoxygenate the patient: spontaneous ventilation with 100% oxygen for 3-5 minutes
- Apply Sellick's maneuver: pressure on cricoid cartilage 📷
- Administer induction agent (propofol, etomidate, thiopental) plus muscle relaxant (succinylcholine, rocuronium)
- Intubate shortly after administration of muscle relaxant
- Inflate cuff, verify correct placement of ETT
- Release cricoid pressure
🥇 Fentanyl (iv) → SEDATION + ANALGESIA + NO AMNESIA
midazolam i.v.
⇒ anxiolytic, sedation, amnesia, anticonvulsant
usage: short procedures (i.e. endoscopy) / i.v. infusion for longer (as adjuvant)
Adjuvant usage:
- Less pain from propofol / etomidate IV injection
- Suppressed cough reflex (good for intubation)
SE:
- ↓BP (stronger hypotensive effects of other anesthetics)
- Afib (ventricular rate increased in these patients!)
😶🌫️ Sorry about that, but old exam question

Anaesthetics | GABA A | K2P channel | Glycine | NMDA |
Intravenous anaesthetics | ||||
Barbiturates | + | Ø | + | - |
Propofol | + | Ø | + | - |
Etomidate | + | Ø | + | Ø |
Benzodiazepine | + | Ø | - | Ø |
Volatile anaesthetics | ||||
Ether | + | + | + | - |
Ether derivatives | + | + | + | - |
Halogenated hydrocarbons | + | + | + | - |
Others | ||||
Ketamine | Ø | Ø | Ø | - |
Nitrous oxide | Ø | + | + | - |
GABA ⇒ Cl- influx into cell ⇒ ↑threshhold
Glycine (=GABAs brother) receptors are responsible for fast inhibitory neurotransmission in the CNS, predominantly in the spinal cord and brainstem. Similar to GABA, glycine also activates anion channels (Cl− and conducting) that lead to hyperpolarization, thereby suppressing neuronal firing.
K2P = Two-pore-domain potassium channel ⇒ leakage K+ channel out of cell ⇒ ↑threshhold
NMDA = Gutamate-R = exitatory



- Non-depolarizing NMBAs • Rocuronium • Vecuronium • Atracurium • Cisatracurium
- Depolarizing NMBAs • Succinylcholine
{kind=link}
- Ach-Receptor-ANTAgonist (nicotinic receptors) ⇒ Acetylcholine can not bind to ACh-Receptor because its blocked → flaccid paresis
- No muscle depolarization occurs
- can be reversed by blocking Ach-esterase
steroidal vs benzylisoquinoliunium (”benz ⭐”) compound
Steroidal = “Curonium” (Rocuronium, Vecuronium)
benzylisoquinoliunium = “curium” (Atracurium, Cis-atracurium)
Onset | Excretion | Side effects | |
Steroidal Compounds | |||
Rocuronium | Rapid (like succinylcholine) | Mostly biliary, some renal | CAVE in: liver/renal failure |
Vecuronium | Slower onset than rocuronium | Biliary and renal excretion | CAVE in: liver/renal failure |
Benzylisoquinolinium Compounds | |||
Atracurium | Hoffman elimination 📷
(spont. non-enzymatic in inactive metabolite =”self destruction mechanism”)
⇒ can be given in liver/renal failure) | Histamine release (flushing, hypotension, tachycardia) | |
Cisatracurium (more potent than atracurium) | Hoffman elimination 📷
⇒ can be given in liver/renal failure) | Ø histamine release |
Classification | Drug | Onset (min) | Duration of Action (min) | Metabolism |
Short-acting | Mivacurium | 1-1.5 | 15-20 | Plasma pseudocholinesterase |
Gantacurium | <1 | 10 | Rapid endogenous cysteine adduct formation and slower ester hydrolysis | |
Intermediate-acting | Rocuronium | 1 | 60 | None, primarily biliary excretion unchanged |
Vecuronium | 1.5 | 60 | Liver deacetylation to small extent | |
Atracurium | 1-1.5 | 45-60 | Hoffman degradation, ester hydrolysis | |
Cisatracurium | 2 | 60-90 | Hoffman degradation | |
Long-acting | Pancuronium | 4-5 | 90 | Liver deacetylation to small extent |
Doxacurium | 3-5 | 90-120 | None, excreted unchanged in urine and bile | |
Pipecuronium | 3-5 | 80-90 | Partial hepatic metabolism, mostly excreted unchanged |

- Ach-E inhibitor i.e. Neostigmin (causes Ach flooding of synapse) + atropin (added to prevent muscarinic action → only on nicotinic receptor)
- if steroidal compound (VE- + RO-curonium)→ Sugammadex
- ❤️ - asystole (+bradycarardia)
- 🐝 - Allergic reaction
Sugammadex:
MOA: Inactivation by bindings + encapsulation (Øreceptor action possible no more)
⇒ Ø cholinergic SE
⇒ faster onset compared to neostigmine
SE:
- Assess neuromuscular blockade → Under anesthesia
- Devices like "Innervator" → Apply stimulations
- Four electrical stimulations: T1 to T4 → Usually ulnar nerve
- T1 = first electrical stimulation
- T4 = fourth electrical stimulation
- Fade → Decrease in twitch amplitude from T1 to T4 (T4 = lowest twitch amplitude)
- More drug → Less muscle contraction (T1 twitch is lost at the end, T4 first)
- All receptors blocked → No twitch
- Recovery → T1 returns first → T4 returns last
- Long + strong stimulation: high frequency nerve-stimulation for 5sec
- If Ø NMB (normal) = tetany (sustained contraction)
- If Blocked = Ø/weak/non-sustainable contraction
{kind=link}
Ach-Agonist ⇒ sustained depolarization → fasziculations followed by ⇒ flaccid paralysis
- FAST ONSET + WASHOUT (useful for temp. paralysis as bolus)
- onset: 30sec → paralysis: 1-2min
- duration: 10min
- FASZICULATION
- CAN Ø BE REVERSED: Ømetabolized by Ach-E!! ⇒ butyryl-cholin-E 📷
- Ø TRAIN OF FOUR

- 🧠 ↑ICP
- 🍌 Hyperkalemia (depolarization → leakage of K+)
- burned/stroke → ↑nicotinic receptor + ↑Risk for Hyperkalemia
- 🌡️ Malignant hyperthermia (like inhaled) → rigidity + fever
- 💪🏽 Myalgia
- Stimulates 🕌 MUSCARINIC R (similar to neostigmine)

- 💂🏽♂️ CO-MORBIDITIES-related
- Sore throat
- Damage to the mouth or teeth
- Cerebral hypoxia
- Death
- Oesophageal intubation
- Air embolism
- Gas embolism
- Vertigo in ENT surgery
- Hyponatremia in urological surgery (TURP syndrome)
- Neurological deficits in neurosurgery
- Postoperative ileus in major abdominal surgery (intestinal resections, fistulae, pulmonary aspiration)
- 🐝Anaphylaxis
- 🧠confusion+memory loss + dizziness
- 🤢 vomiting
- 🌰 bladder problem
- 🌡️ malignant hyperthermia
- …
{kind=link}
{kind=link}
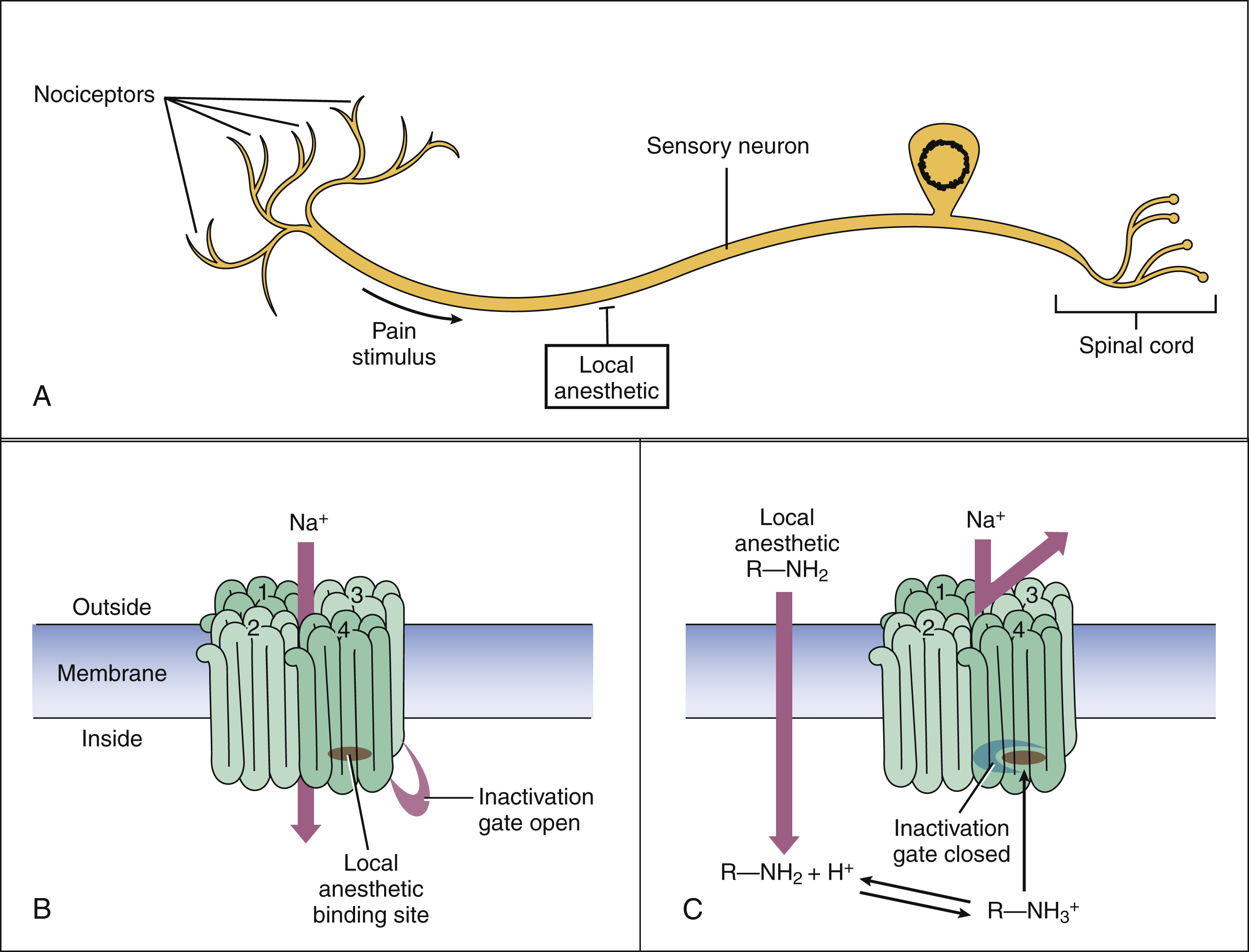
- Amides • Lidocaine • Bupivacaine • Mepivacaine
- Esters • Tetracaine • Procaine • Benzocaine
In chronological order:
- Sympathetic block (vasodilatation)
- Loss of pain and temperature sensation
- Loss of proprioception
- Loss of touch and pressure sensation
- Loss of motor function
ADRENALIN (causes vasoconstriction → less bleeding & less washout)
- 🅾️ END-CAPILLARIES
- 🫀 CV disease
- 🦋 HYPER-THYROIDISM
-Local infiltration of skin flaps -Block of a digit or penis -Block of the foot or toe
-hyperthyroidism / marked arrhythmia
-compromised nerve blood flow from diabetes / atheriosclerosis
also to reverse hypotension due to sympathetic blockade
↑potency + duration → ↑ lipid solubility
↑onset of action → ↓ lipid solubility
ex. ↑lipid solubility → lesser drug needed, SLOW onset, SLOW washout (=↑duration)
- Potency: Ability of the local anesthetic (LA) to penetrate membranes, influenced by lipid solubility, molecular size, number of halides to aromatic ring, and ester linkage.
- Onset of action: Determined by pKa (closest to physiological pH) and lipid solubility of the LA.
- Duration of action: Influenced by lipid solubility of the LA (not cleared by blood flow).

Esters → 1.💧 Plasma → 2. 🥐 Kidney
Amides → 1. 🍑 Liver → 2. 🥐 Kidney
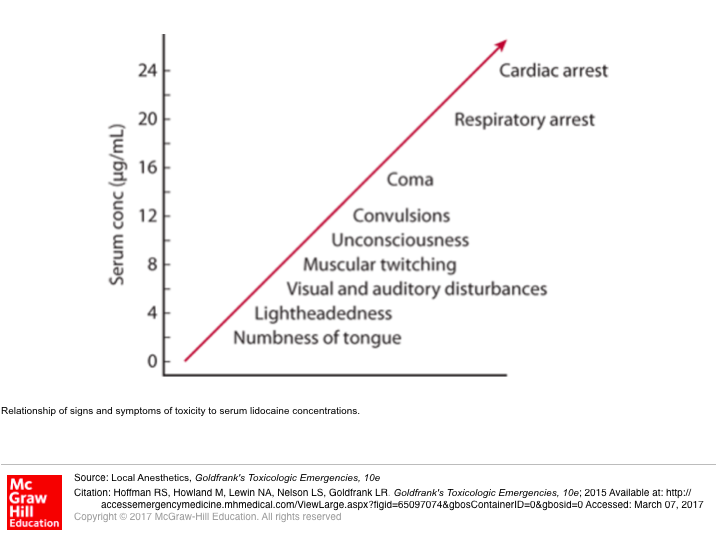
Systemic SE (injection in blood vessel by accident or overdose) ⇒ but RARE
Block INHIBITORY synapses ⇒ EXCITATION (later coma)
{kind=link}
- Variable HR/BP effect
- ↑HR + ↑BP
- ↓HR + ↓BP
- Arrhythmias / Asystole
- Most cardiotox = Bupivacaine

(loss of O2 binding ability due to conversion of Fe2+ to Fe3+ in hemoglobine)
Clinic: Dyspnea: Ø Improvement with O2
→ When drawing blood ⇒ Blood = “Chocolate brown” 🍫
Tx: Methylene Blue 🔹
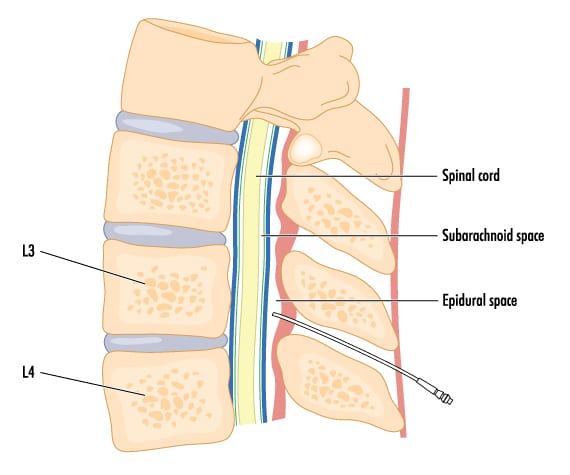
🗼 NEURO-AXIAL: SPINAL & EPIDURAL anesthesia
- ↓COMPLICATION: ↓risk for ❤️ +🫁 complication + other complications of GA
- ↑RECOVERY time
- cheeper
- Reduces risk for VTE, PE, cardiac complications, pulmonary complications, bleeding
- Allows earlier return of gastrointestinal function following surgery
- Advantages of Regional Anesthesia over GA:
- Safe, reliable technique in patients at risk of apnea, bradycardia, desaturation, cardiac or respiratory complications after GA
- Good alternative for day care surgeries
- Minimal risk of postoperative respiratory depression
- Limited stress response to surgery
- Cost-effective
Q. The epidural space: a. Is continuous from inside the skull to its caudal boundary b. Contains veins which act as collaterals when venous return via inferior cava is partially or completely obstructed c. Is bounded anteriorly by arachnoid mater d. Ends caudally at the sacrococcygeal membrane / ligament e. Has an abundant arterial blood supply
ABDE
{kind=link}
Spinal (intrathecal injection) → CSF in subarachnoid space
- single injection
- rapid onset
Epidural → in epidural space
- continuous infusion
- prolonged action
→ can be combined (initiation: spinal; maintenance: epidural)
{kind=link}
- Mainly used: Bupivacaine
- Adjuvants: Opiates (fentanyl, morphine)
Drug | Dose | Onset (min) | Peak effect (min) | Duration (hrs) | Advantages | Disadvantages |
Morphine | 0.1-0.25 mg | 30 | 60 | 12-24 | Long duration | Significant side effects; delayed respiratory depression; biphasic modality |
Fentanyl | 10-25 mcg | 5 | 10 | 2-3 | Rapid onset | Short duration |
Sufentanil | 5-10 mcg | 5 | 10 | 2-4 | Rapid onset; few side effects | Respiratory depression > fentanyl; sinusoidal fetal HR |
Meperidine | 10 mg | 10 | 15 | 4-5 | Rapid onset; potentiation of spinal anesthesia | Nausea and vomiting; pruritis significant |
- As the ligamentum flavum and dura are transversed, a change in resistance is noted, which may be described as a "pop" or a decrease in pressure.
- Once in the subarachnoid space, remove the stylet and cerebrospinal fluid (CSF) should appear.
- If CSF does not appear, rotate the needle 90 degrees until it appears. If still no CSF, replace the stylet.
- Assess the needle position: depth, midline trajectory.
- If off the midline, remove the needle and start over.
- If blood returns from the needle, wait to see if it clears. If not, reassess needle position.
- If the needle is midline, it may be in an epidural vein. Advance the needle slightly further to transverse the dura.
- If the needle is not midline, remove it and start over.
- 💥 postural HEADACHE (low pressure headache due to drop in CSF pressure due to leakage) → Tx: epidural blood patch (causing clotting at leakage point) +NSAIDS
- 🦵Transient pain/paresthesia in leg
- ♻️ Systemic toxicity of local anesthetics ⇒ 🧠 + ❤️
- → ❤️ → ↓BP
- 🧫 Infection → Spinal epidural abscess
- ⬆️ High Spinal / Total spinal
High Spinal:
- Anesthetic effect → spreads above T4
- Blocks → Sympathetic, Sensory, Motor
- Symptoms → Bradycardia, Hypotension, Dyspnea, Swallow/Speak issues
- Causes → Excessive anesthesia, Wrong needle/catheter position
- Occurs in → Spinal/Epidural anesthesia
Total Spinal:
- Extreme High Spinal
- Effect → Brain (intracranial anesthetic spread)
- Major Risk → Loss of consciousness
Comparison Criteria | Spinal | Epidural |
Cost | Cheaper | Expensive |
Onset of Action | Early | Delayed |
Technical Difficulty | Easier | Difficult |
Duration of Action | Less | Prolonged |
Quality of Block | Excellent | May be patchy |
Change of Level | Not possible after fixation | Can be possible |
Block Failure Rate | Less | High |
Post-dural Puncture Headache | Seen | Not seen |
Epidural Hematoma | Less likely | High incidence |
Total Spinal | Rare | High chance |
Intravascular Injection | Rare | High chance |
Drug Toxicity | Less | High |
Catheter Complications | Not seen | Present |
ABSOLUTE
- 🙅🏿♂️ patient → REFUSAL
- 🩸BLEEDING risk (coagulopathy)
- 🕯️ LOCAL INFECTION (at puncture site)
- ↑HYPOTENSION-RISK
- 🚱 HYPOVOLEMIA
- ⛵ VALVE-STENOSIS: aortic/mitral
RELATIVE
- 🤷🏾♂️ patient → UNCOOPERATIVE (incl. emotion instability)
- 🧠 NEURO defic.
- 📛 SEPSIS
- ⏳ LONG/Extensive surgery
Q. Spinal anesthesia is contraindicated in which of the following? a. Emotional instability b. Coagulopathies c. Lack of intravenous access d. Uncorrected hypertension e. Previous spinal surgery
BD
- Spinal and epidural anesthesia: associated with lower morbidity and mortality in major hip or knee surgery.
- Epidural space: not a continuous cylinder, contains discrete pockets of epidural fat.
- Mental model of spinal anatomy: helps locate spinal or epidural space.
- Hemodynamic effects: proportional to local anesthetic block.
- Patient variables: minimally affect spread of intrathecal and epidural medications.
- Unintended intrathecal injection: common cause of morbidity during epidural block.
- Early signs: of unintended intrathecal injection can be subtle.
- Intravenous injection: of local anesthetics can lead to seizures and cardiac arrest.
- Test doses and incremental injection: important safety steps.
- Increased risk: of spinal or epidural hematoma in patients receiving antithrombotic or thrombolytic medications.
🌾 PERIPHERAL NERVE BLOCK & IV regional anesthesia
Regional Anesthesia Techniques
- Peripheral Nerve Block: 📷
- Procedures focused on upper or lower limbs
- Using Ultrasound (US) 📷 📷 or a nerve stimulator to target a specific nerve or plexus
- Administration of a local anesthetic directly onto the nerve
- Intravenous Regional Anesthesia: 📷
- Serves as an alternative to the peripheral nerve block, especially for shorter interventions of under an hour
- Procedures like surgeries for the hand and forearm, such as carpal tunnel release
- Utilize a tourniquet to minimize blood flow back
- Administer a local anesthetic through an IV line in the hand
neuro-axial (epidural/spinal)
2nd trimester
- Surgery in the second trimester = ideal.
- First trimester poses risks of teratogenic effects.
- Third trimester surgery may trigger preterm labor.
- Emergency surgery can be performed at any stage of pregnancy.
- Mother's safety is the priority.
- Preoperative assessment for elderly patients: evaluation of co-existing medical conditions, cognitive assessment, review of current medication, assessment of cardiovascular and respiratory status, measurement of hemoglobin and electrolyte levels, chest X-ray, and electrocardiogram (ECG).
- Anesthetic techniques: consideration of regional techniques such as spinal anesthesia and epidural anesthesia to reduce postoperative complications.
- Awareness of the potential risk of postoperative cognitive dysfunction as a serious complication.
- Infants and children have anatomical, physiological, and pharmacological differences compared to adults.
- Anesthesia induction period can present challenges, including the potential development of laryngospasm, bradycardia, and apnea.
- Intravenous anesthesia induction may be limited in children due to their aversion to injections → EMLA cream (topical analgesia agent) minimize distress during induction
- Inhalation route of induction, particularly with sevoflurane, is commonly used in pediatric anesthesia.
- Regional anesthesia and nerve blocks are often used in conjunction with general anesthesia.
- Maintaining fluid balance and thermoregulation is crucial in pediatric anesthesia.
🔩 ICU Management
- temporal
- patho
→ chronic (>3m) vs acute (<6w)
chronic:

(post-OP pain = acute pain)
→ nociceptive vs. neuropathic
- 🪜 WHO-ladder 📷
- non-pharma tx

- 🫁Respiratory depression
- 🍤GI - pain, n/v, constipation → give antiemetic + laxative with opioids
- 🧠Neuro - sedation
- 🚱 Urinary retention
- 🪡pruritus
Q. Common side effects of opioids are: a. Renal insufficiency b. Urinary retention c. Liver toxicity d. Pruritus e. Asthma
BD
{kind=link}
{kind=link}
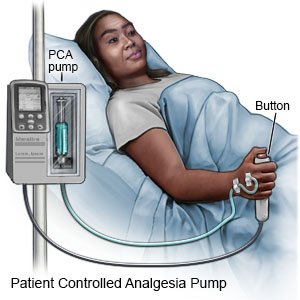
- It allows patients to self-administer pain medication by pressing a button (limited by lockout intervals to prevent OD)
- PCA is used for acute, chronic, postoperative, and labor pain.
- It provides flexibility and individualized pain control.
- Medication can be given through intravenous (IV) or epidural routes, peripheral nerve catheters and transdermally.
- Commonly used drugs include opioids, local anesthetics, and dissociatives.
- Morphine and hydromorphone are frequently used agents.
ABSOLUTE:
- ❓ patient does Ø understand
- 🐝 allergy to drugs
- 🦠 infection (systemic or LOCAL)
- 🔥/🗡️ LOCAL burn/trauma
- 🧠 Nerve-deficits or ↑ICP→ if catheter (epidural)
RELATIVE
- 🥐 CRF
- 🩸 anti-coagulants or bleeding disorder
- 👅 sleep apnea
- Indication: Opioid overdose
- Mechanism of action: Competitive inhibition of opioid receptors, primarily mu-opioid receptors
- Naloxone: Short-acting with a half-life of 1 hour; effects of narcotics may return when naloxone wears off (closely observe the patient following administration)
- Naltrexone: Longer-acting with a half-life of 10 hours; return of opioid effects = less likely
- Side effects = Opioid withdrawal: Nausea, agitation, sweating, tachycardia, hypertension, reemergence of pain, pulmonary edema, seizures (which essentially represent opioid withdrawal)
🫁 Respiratory insufficiency
GAS-EXCHANGE
Parameter | Type 1 (hypoxemic respiratory failure) | Type 2 (hypercapnic respiratory failure) |
Description | Failure marked by hypoxemia and either normocapnia or hypocapnia in arterial blood samples. | Failure marked by hypercapnia and either normoxemia or hypoxemia in arterial blood samples. |
PaO2 | < 60 mm Hg | Normal or < 80 mm Hg |
PaCO2 | Normal or <33 mm Hg | > 50 mm Hg |
TEMPORAL CLASSIFICATION:
- Acute: Development over minutes-hours;
- Chronic: Development chronically (from chronic illness i.e. COPD)

Organ System | Causes of Hypercapnia | Causes of Hypoxemia |
Pulmonary | Airway obstruction
- Lung diseases (e.g., COPD, asthma exacerbation, bronchiolitis, aspiration, bronchiectasis)
- Upper airway obstruction (e.g., laryngospasm, angioedema, anaphylaxis, croup, epiglottitis) | - Impaired alveolar diffusion (e.g., pulmonary edema, pneumonia) |
- Right-to-left shunt (Pulmonary: e.g., ARDS, pulmonary contusions/hemorrhage, lung collapse, tension pneumothorax; Intracardiac: e.g., Eisenmenger syndrome) | ||
- V/Q mismatch (e.g., severe pneumonia, pulmonary edema, pulmonary embolism, atelectasis) | ||
CNS | - CNS depression (e.g., drugs, cerebral herniation, stroke) | - Hypoventilation (related to hypercapnia causes) |
Muscular | - Respiratory muscle weakness (e.g., myasthenia gravis, Guillain-Barré syndrome, ALS, cervical spinal cord injury) | |
Chest Wall | - Decreased chest wall compliance (e.g., rib fractures, seizures, obesity hypoventilation syndrome) | |
Other | - Electrolyte disturbances | - Decreased FiO2 (e.g. high altitude illness) |
- Respiratory distress (dyspnea, tachypnea, grunting+nasal flaring, accessory muscles + rib retractions, tripod)
- Airway compromise symptomatic (i.e. inspiratory stridor, gasping)
- CNS: Respiratory drive changed
- Pulse oximetry, Capnography
- BGA
- Imaging (of lung)
- Chest X-ray (Rx)
- CT scan (СТ)
- Pulmonary scintigraphy
- Microbiological cultures of tracheal aspirates/BAL
Hypoxemic
Target ⇒ PaO2>65 or SaO2 >92%
- ETIOLOGY
- O2
- Ventilation
- non-invasive ⇒ NPPV (CPAP)
- invasive ⇒ Intubation (endotrach.
NPPV=Noninvasive positive pressure ventilation
Hypercapnic
Target ⇒ pH >7,25-7,3
- mainly ETIOLOGY
- upper airway desobstruc.
- lower (smaller) airways → bronchodilators + anti-cholinergics
- drainage (if effusion)
- Ventilation if 🧠
- normal neuro status + mild neuro deficits ⇒ CPAP
- altered neuro status or severe deficits ⇒ invasive
🤿 Ventilation
⇒ Effects on TIDAL VOLUME + Ø on RR (if spontaneous controlled)

⇒ ↑inspiratory pressure, ↑inspiratory time, ↑O2/CO2 exchange (recruitment)
⇒ extrinsic PEEP keeps lung open during end of expiration (i.e. in COPD, athelectasis) ⇒ ↑PEEP

- Elevation in airway pressures:
- Aids gas exchange (alveolar recruitment, stenting).
- Possibility of lung injury from the ventilator, notably barotrauma.
- Increase in pulmonary artery pressure.
- Ascendancy in pulmonary vascular resistance.
- Augmentation of intrathoracic pressure:
- Diminishes venous return → ↓output → reduced organ perfusion
- Potential for gastric distension and elevated risk of vomiting/aspiration.
T
CPAP = only one airway pressure = equivalent to PEEP. BIPAP = 2 pressure cycle.
respiratory insufficiency with…
- ↑ breathing work (RR>35)
- Altered bronchial secretions (COPD exacerbation, cardiogenic edema, atelectasis)
- obstruc. sleep apnea
- ØSpontaneous breathing
- ↓ airway protection (Upper airway obstruction, Aspiration risk (GI bleeding, secretion not removable, vomiting) → Intubation needed
- ↓mask seal efficiency (facial deformity/trauma/surgery)
- ↑Risk for Pressure side effects (recent surgery in GI-tract or upper airways, CV instability, arrhythmia)
- SPONTANEOUS by the patient (MAINLY)
- CONTROLLED by ventilator
VOLUME vs. PRESSURE CONTROLLED
- Breathing initiation:
- Controlled breathing: initiated by the ventilator
- Spontaneous breathing: initiated by the patient
- Modulation of controlled breaths:
- Pressure vs. volume
- Management of spontaneous breaths:
- Assisted Ventilation with pressure support
- 🫁 lung injury → baro trauma, volumo trauma, shear stress (VILI)
- ❤️ ↓output
- 😵💫 - stress
- Barotrauma and volutrauma
- Reduction of cardiac output
- Ventilation-associated pneumonia
- Stress and anxiety
- Ventilation-induced lung injury (VILE) - shear stress
female = 50%
male = 60%
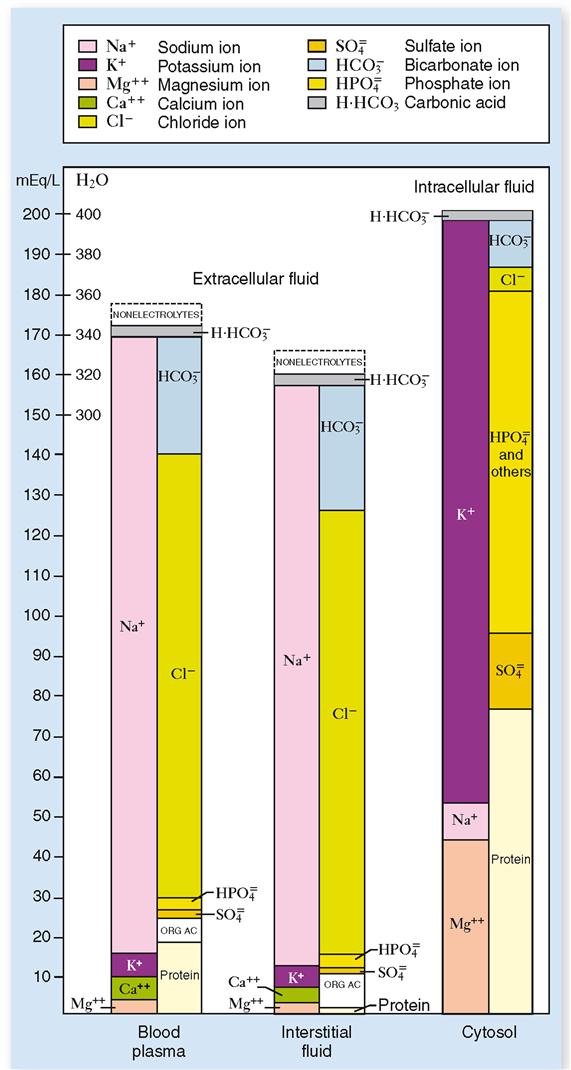
Electrolytes + Proteins
{kind=link}
Plasma vs. interstital: plasma more proteins, interstital more Cl
Fluid
{kind=link}
Q. What is true from the following sentences? a. The total body water content is similar in women and men. b. Potassium is the major intracellular cation. c. Chloride is the major intracellular anion. d. Plasma sodium concentration is the principal determinant of the effective osmolarity of extracellular fluid. e. The protein content is similar in the intracellular and extracellular compartments of the body.
(A)BD total body water average: men 60%; woman 55%
- Osmolality indicates the concentration of all particles dissolved in body fluid (per kg).
- It is routinely measured in clinical laboratories for the differential diagnosis of disorders related to hydrolytic balance regulation, renal function, and small-molecule poisonings.
- The formula for calculating osmolality is 2(Na) + glucose/18 + BUN/1.8.
- The normal range for serum osmolality is 275 to 295 mOsm/kg.

- CO derived parameters
Co-derived parameters are physiological measurements that are calculated or derived from other measured parameters. They provide additional information and insights about the patient's condition. Some examples of co-derived parameters include:
- Cardiac Output (CO): It is calculated based on the measurement of stroke volume and heart rate. CO represents the volume of blood pumped by the heart per minute.
- Stroke Volume Variation (SVV): It is derived from the variations in stroke volume during the respiratory cycle. SVV can indicate fluid responsiveness and help guide fluid management in critically ill patients.
- Systemic Vascular Resistance (SVR): It is calculated using the mean arterial pressure and cardiac output. SVR represents the resistance that the blood encounters as it flows through the systemic circulation.
- Oxygen Delivery (DO2): It is calculated by multiplying the arterial oxygen content by the cardiac output. DO2 represents the amount of oxygen delivered to the tissues per minute.
Feature | Crystalloids | Colloids |
Definition | Salt solutions with variable electrolyte compositions
→ distribution in ECF | Solutions with larger molecules such as proteins (i.e. albumin) or non-protein colloids (i.e. starches)
→ intravascular distribution |
Intravascular Compartment Stay | Less than an hour; rapidly excreted if renal function is normal | Remain within the circulation; do not freely cross vascular endothelium |
Osmolarity Classification | Isotonic, hypertonic, or hypotonic | N/A |
Usage Recommendation | For routine replacement and resuscitation
Balanced crystalloid (e.g., Ringer's lactate) preferred over saline | Controversial due to recent evidence:
Protein colloids like albumin used; non-protein colloids should be avoided |
Volume Replacement | 3 mL crystalloid per 1 mL of blood loss (3:1 replacement) | 1:1 ratio (infusion:blood loss) in terms of intravascular volume replacement |
Specific Products | Ringer’s lactate, normal saline | Albumin, gelatin solutions, dextrans, hydroxyethyl starch (HES) |
Metabolic Acidosis Risk | Hyperchloremic metabolic acidosis possible with large volumes | N/A |
Renal Function Impact | Rapid excretion if renal function is normal | Use of certain colloids (e.g., HES) controversial due to renal side effects |
Coagulation | N/A | Potential coagulopathic side effects |
Safety and Efficacy | Generally considered safe | Lack of definitive studies; safety and efficacy concerns ⇒ Routine use avoided |
Q. Crystalloid solutions: a. Are often implicated in anaphylactic reactions b. Maintain euvolemia in patients with blood loss (replacement ratio 3:1) c. Are cheaper than colloids d. Ringer's lactate may lead to hypochloremic metabolic acidosis e. Distribute within the intracellular fluid (ICF) compartment
ABC
Ringer Lactate
- large quantities + prolonged
- lactic acidosis
- Ø in: RF, high need of free water, in transfusion line + hyperK
- Ringer Lactate is the preferred choice for rapid bolus injection in large quantities.
- It is suitable for situations requiring increased and prolonged volume, such as burns.
- Ringer Lactate can be used for mild to moderate acidosis caused by volume depletion.
- It can be administered in quantities of over 40 L per 24 hours without affecting electrolyte levels.
- Ringer Lactate is contraindicated in renal failure due to its potassium content.
- It helps maintain glucose levels and is necessary for water intake of more than 100 ml per liter.
- Lactic acidosis is not a contraindication for Ringer Lactate.
- Transfusion with Ringer Lactate may cause coagulation in the same infusion line.
- Ringer Lactate is often preferred over Sodium Chloride (Normal Saline) in cases of acute dehydration.
Saline solution
- RF
- hyponatremia
- transfusion line
- !! → hyperchloremic acidosis + hypokalemia
- Indications: volume depletion in patients with renal or undefined status of renal function, moderate hyponatremia due to depletion of volume, fluid vehicle for transfusion on the same line, dilution medium for IV phenytoin
- Contraindications: prolonged administration leading to hyperchloremic acidosis and hypokalemia, sensitivity to sodium (CHF - congestive heart failure or hypertension)
- Requires buffer solution (0.9% NaCI pH = 4)
- Requires maintaining serum potassium
- Sensitivity to Na (CHF - congestive heart failure or hypertension)
- Requires maintaining blood glucose
- Preoperative fasting time should be considered in the total fluid volume that needs to be compensated.
- Patients with fever, sweating, gastrointestinal losses, polyuria, and hyperventilation require increased fluid requirements.
- Decreased fluid requirements are necessary for patients with renal insufficiency and heart failure, as they cannot excrete large volumes of free water or tolerate fluid overload.
{kind=link}
Percentage of Body Water Loss | Severity | Signs and Symptoms |
3% | Mild | Decreased skin turgor, dry mucous membranes, sunken eyes, dry tongue, reduced sweating |
6% | Moderate | Oliguria, orthostatic hypotension, tachycardia, low volume pulse, cool extremities, reduced filling of peripheral veins and CVP, hemoconcentration, apathy |
9% | Severe | Profound oliguria or anuria and compromised CNS function with or without altered sensorium |
Fluid Deficit (in liters) = [(Current Sodium - Desired Sodium) / Desired Sodium] * Body Weight (in kg) * 0.6
→ only possible in isotonic fluid deficits.
4 mL/kgBW/hour for the first 10 kilograms
2 mL/kgBW/hour for the next 10 kilograms
1 mL/kgBW/hour for the each kilogram over 20kg.
i.e., 22 kg child who was fatsed for three hours need: 4 x 10 +2x 10 + 2= 62 mL of fluid/hour × 4 hours= 248 mL of free water.
fluid loss during surgery

Fluid responsiveness assessment:
- Indicators of intravascular volume deficit: hypotension, oliguria, reduction of ET CO2, lactic acidosis, and low SevO2.
- Response to fluid resuscitation:
- Increase in blood pressure and alleviation of compensatory tachycardia.
- Return of ET CO2 value to normal.
- Positive response (↑ of BP) to passive leg raising test indicates persistent intravascular fluid deficit.
- Increase in urinary output.

Acute HyperNa: over 24h
Chronic HyperNa: over 48-72h
- RBCs: Increase Hb by 1 g/dL per per unit (= 300ml)
- Platelets: Increase platelet count by 5000-10000/dL per unit
- Fresh frozen plasma: Contains all clotting factors, increases coagulation factors value by 15-30% per 10-15 mL/kgBW
- Cryoprecipitate: Increases levels of fibrinogen, factor VIII, and factor XIII by 150-250 mg per unit of cryoprecipitate
⇒ <7
- The appropriate triggers for transfusion have been extensively debated in recent years.
- For young, healthy patients, a hemoglobin level of 7g/dL= threshold for transfusion.
- However, in patients with conditions such as coronary artery disease, sepsis, or CNS dysfunction (including cerebral vascular disease), transfusion should be considered earlier.
- Other factors to consider for transfusion include serum lactate levels and central venous oxygen saturation (SvcO2).
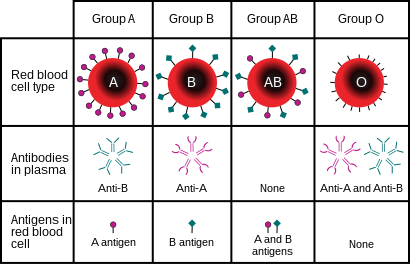
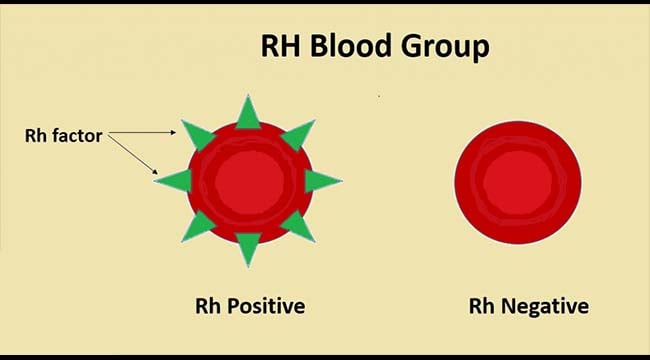
- Selection of Red Cells for Transfusion:
- Group and screen: Determines blood group, Rh status, and presence of auto- or alloantibodies in patient's plasma
- Cross-match: Mixes recipient's blood with potential donor blood to look for agglutination (takes 30-45 minutes)
{kind=link}
{kind=link}


- 🩸Acute hemolytic tranfusion reactions (ABO incompatibility)
- 🤒Febrile Nonhemolytic transfuison reaction (alloantibodies to WBC, plts or plasma Ags → cytocines)
- 🐝 Allergic Nonhemolytic Transfusion Reactions (IgE alloantibodies to plasma proteins → mastcellactivation → histamine release)
- 🫁 Transfusion-Related Acute Lung Injury (leads to release of mediators → ↑capillary permeability)
1. Acute Hemolytic Transfusion Reactions
- Caused by: ABO incompatibility, leading to intravascular hemolysis.
- Common Symptoms: Fever, chills, hypotension, back/flank pain, hemoglobinuria.
- Risks: Most often due to incorrect patient identification.
- Treatment:
- Stop transfusion
- Check for clerical errors
- Retest blood specimen
- Provide vigorous IV fluids & inotropes
- Maintain urine output with diuretics and other agents.
2. Febrile Nonhemolytic Transfusion Reactions
- Cause: Antibodies reacting to WBC, platelets, or other donor plasma antigens.
- Common Symptoms: Fever, facial flushing, headache, myalgia, chills, hypotension, and more.
- Onset: Within 6 hours of transfusion.
- Treatment:
- Rule out hemolytic reaction or infection
- Adjust transfusion rate based on severity and symptoms
- Give antipyretics as needed.
3. Allergic Nonhemolytic Transfusion Reactions
- Cause: Antibodies (IgE) reacting to donor plasma proteins, causing mast cell activation.
- Occurrence: Commonly in individuals with multiple transfusions or multiparous women.
- Common Symptoms: Urticaria, fever, potential anaphylactoid reactions.
- Treatment:
- Varies from slowing transfusion rate to providing medications such as diphenhydramine, steroids, and more, based on severity.
4. Transfusion-Related Acute Lung Injury (TRALI)
- Definition: New-onset lung injury during or within 6 hours post-transfusion.
- Common Symptoms: Severe hypoxemia, bilateral pulmonary edema on imaging.
- Cause: Binding of donor Abs to recipient's WBCs, increasing capillary permeability in lungs.
- Onset: Resolves within 24-72 hours post-transfusion.
- Risks: Leading cause of transfusion-related morbidity and mortality.
- Treatment: Supportive therapy with oxygen; testing for patient and donor will be arranged.


- 🌊 Circulatory overload
- 🍋 Citrate Toxicity
- 🧫 Bacterial infection
- 🍌 Hyperkalemia
- 🍷 Dilutional Coagulopathy
- Transfusion-Associated Circulatory Overload:
- Caused by: Impaired cardiac function and/or rapid transfusion.
- Symptoms: Dyspnea, orthopnea, hypertension, tachycardia, crackles in lungs, increased venous pressure.
- Incidence: 1/100.
- Risk Factors: Age >70 years, heart failure, history of MI, renal failure, positive fluid balance.
- Treatment: Stop transfusion, administer diuretics and oxygen. Transfuse at a slower rate and use diuretics for prevention.
- Citrate Toxicity:
- Occurs in: Massive transfusion, especially in liver disease patients who can't clear citrate from blood.
- Mechanism: Citrate binds to calcium leading to hypocalcemia symptoms and coagulopathy.
- Treatment: Administer IV calcium gluconate 1 g.
- Bacterial Infection:
- Common Bacteria: Gram-positive (e.g., S. aureus, S. epidermidis, Bacillus cereus) and Gram-negative (e.g., Klebsiella, Serratia, Pseudomonas, Yersinia).
- Risk: 1/100000 for RBCs and 1/10000 for platelets.
- Important Note: Never store blood >4 hours after it leaves the blood bank.
- Treatment: Stop transfusion, conduct blood cultures, and give IV antibiotics and fluids.
- Hyperkalemia:
- Caused by: Potassium release from stored RBCs.
- Risk: Increases with storage time and decreases if blood is irradiated. Higher risk with older blood.
- Incidence: Occurs in 5% of patients receiving massive transfusions.
- Dilutional Coagulopathy:
- Occurs in: Massive transfusions (>10 units).
- Mechanism: The transfused pRBCs lack clotting factors, fibrinogen, cryoprecipitate, or platelets.
- Treatment: Fresh plasma (FP), cryoprecipitate, and platelets.

🩸 Delayed hemolytic
🫖 Graft vs. Host disease
- Delayed Hemolytic
- Cause: Alloantibodies to minor antigens such as Rh, Kell, Duffy, and Kidd.
- Occurrence: Level of antibodies (Ab) during transfusion may be too low to detect and cause hemolysis. However, the Ab levels can increase later due to secondary stimuli, leading to extravascular hemolysis.
- Onset: 3-14 days post-transfusion.
- Presentation: Anemia and mild jaundice.
- Treatment: No specific treatment. It's essential to remember this reaction for future transfusions.
- Note: Serologic transfusion reactions are the development of alloantibodies without overt hemolysis.
- Transfusion-Associated Graft Versus Host Disease
- Cause: Transfused T-lymphocytes recognize and act against the "host" (the recipient of the transfusion).
- Onset: 4-30 days following transfusion.
- Risk: This typically happens in patients with severely compromised immune systems, like those with Hodgkin lymphoma or leukemia.
- Presentation: Fever, diarrhea, liver function abnormalities, rash, and pancytopenia.
- Prevention: Administering irradiated blood products can prevent this reaction.
🪨 Iron overload
🦠 Viral infection risk
Iron Overload:
- Definition: Iron overload refers to the accumulation of iron in the body due to various causes, one of which can be repeated blood transfusions.
- Causes: This condition can arise due to repeated transfusions over a long duration. Certain disorders like β-thalassemia major may necessitate frequent transfusions leading to iron overload.
- Complications: An excessive amount of iron in the body can result in secondary hemochromatosis.
- Treatment: The accumulated iron can be managed using iron chelators or through phlebotomy, especially if the individual no longer requires blood transfusion and isn't anemic.
Viral Infection Risk:
- Definition: Viral infection risk refers to the potential of acquiring viral infections through blood transfusion.
- Associated Viruses:
- HBV (Hepatitis B Virus): 1 in 7,000,000 chance
- HCV (Hepatitis C Virus): 1 in 12,000,000 chance
- HIV (Human Immunodeficiency Virus): 1 in 20,000,000 chance
- HTLV (Human T-lymphotropic Virus): 1 in 60,000,000 chance
- Other Infections: There are also risks from other infections such as EBV (Epstein-Barr Virus), CMV (Cytomegalovirus), and WNV (West Nile Virus).
{kind=link}
- Evaluate blood pH (normal: 7.35-7.45).
- Evaluate HCO3 (normal: 22-28 mEq/L).
- Evaluate PCO2 (normal: 33-45 mmHg).
- Central causes: head trauma, brain ischemia, tumor
- Neuropathy and myopathy
- Neuro-muscular diseases: myasthenia gravis
- Thorax deformities: spondylitis, scoliosis
- Pleural abnormalities: large fluid collections
- Pulmonary conditions: pneumonia, bronchopneumonia, pulmonary edema, ARDS
- Airway obstruction: asthma, COPD, foreign bodies, laryngospasm
or excess co2 production
- HCO3 loss → diarrhea, renal (tubular acidosis)
- HCO3 consumed → extra / endogenous acids ⇒ ↑Anion gap
{kind=link}
vomiting + renal (diuretics)
Disorder of circulatory system → inadequate organ perfusion + tissue hypoxia → metabolic disturb. → irreversible organ damage
1) Hypotension
2) Signs of end-organ hypoperfusion:
🧠brain : altered conciousness or other mental disturbance, weakness, dizziness, nausea
🥐kidney ⇒ 🚱 oliguria
💪skin ⇒ 🧊 cold, mottled, clammy/diaphoretic+ ↓recap time
→ exception: distributive⇒ 🥵 might be warm+flushed+ normal recap
3) Specific signs depending on type of shock (see below)
Pre-Shock
compensated, non-progressive shock
appears IMMEDIATELY after triggering event
Compensatory mechanisms only:
- Peripheral vasoconstriction
- 💪 🧊 cold + clammy + ↓recap
- may be absent in distributive shock ❗
- ❤️ ↑HR
- 🥐 Oliguria
Shock
decompensated, progressive shock
- ✨ ↓BP
- Hypoperfusion →🍼 Lactic acidosis (high AG metabolic acidosis)
⇒ 🧠 Altert mental stage
⇒ DIC
⇒ worsening tachypnea
End-organ dysfunction
irreversible shock
ORGAN FAILURE due to ISCHEMIA, INFLAMM. MEDIATOR + REPERFUSION INJURY
- 🧠 - autonomic dysfunction
- 🧠 - ↓/↑ activity
- ⇒ ❤️ - ↓↓output
- ⇒ 🫁 ⇒ ARDS ⇒ micro-thrombi
- ⇒ 🥐 ⇒ ischemia, oliguria, ↑↑RAAS + tubular necrosis
- ⇒ 🍑 ⇒ ischemia ⇒ ↑transaminases
- ⇒ 🍤 ⇒ ischemia ⇒ translocation of gut bacteria ⇒ septic shock
- ⇒ 🩸 (coagulation) ⇒ DIC + Thrombocytopenia
- Volume
- Shift ⇒ DISTRIBUTIVE shock
- Capillary leakage ⇒ SEPTIC shock
- Vascular tone dysregulation
- Loss ⇒ HYPOVOLEMIC shock
- Blood ⇒ HEMORRHAGIC shock
- Body fluids (i.e. GI) ⇒ NON-HEMORRHAGIC NON-TRAUMATIC shock
- Plasma (i.e. burns) ⇒ NON-HEMORRHAGIC TRAUMATIC shock
- Output
- Cardiac ⇒ CARDIOGENIC shock
- Myocardium (i.e. MI)
- Conduction system → arrhythmias
- valves
- Extracardiac ⇒ OBSTRUCTIVE shock
- Impaired filling ⇒ TAMPONADE
- ↑after-load ⇒ (massive) PE
- Obstruction of venous retunr ⇒ TENSION PNEU
⇒ ANAPHYLACTIC shock
⇒ NEUROGENIC shock
TYPE | CAUSES |
💧 HYPOVOLEMIC | - fluid loss (GI, burns)
- hemorrhage (esp TRAUMA) |
❤️ CARDIOGENIC | - cardiac ischemia
- arrhythmias
- valvulopathies
- cardiotoxic substances (see toxins) |
🚧 OBSTRUCTIVE | - cardiac tamponade
- PE
- tension pneu |
🔥 SEPTIC | - infection
- bacteremia |
🤧 ANAPHYLACTIC | - exposure to allergens
(food, sting, drug) |
🧠NEUROGENIC | CNS injury:
- traumatic brain injury
- intracerebral hemorrh.
- spinal cord injury |
- hypodynamic shock = all shocks, except distributive
- hyperdynamic shock = distributive
→ ↓ CO
→ ↑ SVR
→ ↑O2 extraction + lactic acidosis
→ variable CO (see next question)
→ ↓ SVR
→ normal O2 extraction
TYPE | OUTPUT | PRE-LOAD (PCWP or JVP) | AFTER-LOAD
(SVR) |
💧 HYPOVOLEMIC | ↓ | ↓ | ↑ |
❤️ CARDIOGENIC | ↓↓ | ↑ | ↑ |
🚧 OBSTRUCTIVE | ↓↓ | ↑ or ↓ | ↑ |
🔥🤧🧠 DISTRIBUTIVE | 🧠 ↓
🔥 🤧 early:↑ ; late: ↓ | ↓ | ↓↓ |
Gap between systolic + diastolic BP
⇒ wide in distributive
⇒ narrow in cardiogenic (+others)
💪 skin perfusion | 🚹 jugular v. | ⭐ specific | |
💧 HYPOVOLEMIC | 🧊 cold + diaphoretic + ↑recap
↓tugor+dry membranes
| Ødistended | -signs of cause (bleeding, diarrhea)
-Shock index (HR/BP) > 0.9 |
❤️ CARDIOGENIC | 🧊 cold + diaphoretic + ↑recap | distended + ↑JVP | -HF signs (i.e. dyspnea)
-signs of cause (chest pain, palpitations, murmor)
-mechanical complication (mitral insuff, septal/free wall rupture + taponade, aneurysm) |
🚧 OBSTRUCTIVE | 🧊 cold + diaphoretic + ↑recap | distended + ↑JVP | -signs of cause (chest pain, ↓breath sounds, tracheal deviation, muffled heart sounds, DVT signs) |
🔥 SEPTIC | early: 🥵 warm + flushed
late: 🧊 cold + pale + ↑recap | -🤒 sepsis signs (fever, SIRS criteria)
Source signs(signs of pneumonia, UTI, menigitis) | |
🤧 ANAPHYLACTIC | 👹 rash + flushed + edematous | 🫁 - stridor, wheezing, cough
💩 - vomiting + diarrhea | |
🧠NEUROGENIC | 🥵 warm + flushed | ↓❤️ BRADYCARDIA
neurological-deficits |
{kind=link}
The patient is placed in supine position with the torso elevated to 45 degrees and the head rotated away from the examiner. Tangential lighting can help elicit the finding. Determine the vertical distance between the upper limit of visible distention of the internal jugular vein and the sternal angle. A distance > 4 cm is considered elevated.
- Systemic inflammatory response syndrome (SIRS):
- Diagnosis: ≥ 2 of the following 4 criteria:
- Temperature: > 38°C or < 36°C
- Heart rate: > 90/min
- Respiratory rate: > 20/min or PaCO2 < 32 mm Hg
- White blood cell count: > 12,000/mm3, < 4000/mm3, and/or > 10% band cells
- Sepsis: SIRS criteria + suspected or confirmed underlying infection
- Severe sepsis: Sepsis + organ dysfunction (at least one organ or system)

LAB:
- ↑Lactate ⇒ Metabolic acidosis
- CBC, inflammatory lab → hemorrhage, sepsis?
- cultures (BEFORE AB tx)
- troponin → cardiac?
OTHER
- EKG + Echo→ cardiac? obstructive?
- FAST → hemorrhage?
- CT Brain, Abdomen → neurogenic? septic? 3rd space fluid loss (pancreas, obstruction)?
- Chest Xray → obstructive? cardiac? sepsis (pneumonia)?
- other exams depending on etiology
Parameter | Class I | Class II | Class III | Class IV |
Blood loss (mL) | Up to 750 | 750–1500 | 1500–2000 | > 2000 |
Blood loss (% blood volume) | Up to 15% | 15–30% | 30–40% | > 40% |
Pulse rate | < 100 | 100–120 | 120–140 | > 140 |
Blood pressure | Normal | Normal | Decreased | Decreased |
Pulse pressure (mm Hg) | Normal or increased | Decreased | Decreased | Decreased |
Respiratory rate | 14–20 | 20–30 | 30–40 | > 35 |
Urine output (mL/h) | > 30 | 20–30 | 5–15 | Negligible |
CNS/mental status | Slightly anxious | Mildly anxious | Anxious, confused | Confused, lethargic |
Fluid replacement | Crystalloid | Crystalloid | Crystalloid and blood | Crystalloid and blood |
Stage 1 (+2) ⇒ 🌊fluids
Stage (2+) 3 ⇒ 🌊fluids + 🩸blood
Stage 4 ⇒ 🌊fluid + 🩸blood + 🔪surgery (hemostasis)
Normal volume:
- adults: 7% of ideal body weight (approximately 5 I / kg for 70)
- children: 8% of ideal weight (approx. 80 mL / kg)
Q. 4th stage of hemorrhagic shock is defined by:
(A) Low systolic blood pressure
(B) Normal diastolic blood pressure
(C) Diuresis 5-15 ml/h
(D) Heart rate > 140 /min
(E) Heart rate <100 /min
AD
primary evaluation! (first ABCDE)
Type of shock | Treatment |
💦 Hypovolemic: | 1. 🌊Fluids
(i.v. location depending on injury or CV catheter)
2. 🩸 hemorrhage
-Blood transfusion
-Hemostatic control (emergency surgery🔪) |
❤️ Cardiogenic: | 1. ⚠️ check fluid responsiveness
(dry = output problem vs. wet = congestion problem)
2. Output maintenance (preload, afterload, contractility)
- 🏵️ Inotropes (Dobutamin, Milrinone)
-🔺 Vasopressors (NE)
-⚠️ Diuretics (only if sysBP >90)
3. Definite tx: PCTA, stents, thrombolysis
4. OTHERS
(oxygen, AB +electroly. correction, arrythmia correction, Mechanical assistant devices) |
🚧 Obstructive: | 1. 🌊 Fluids
2. 🪡 Relieving intervention
-Pericardiocentesis
-Thoracostomy
-Thrombolysis |
🔥 Septic shock: | 1. 🌊 Fluids
2. 🔺 Vasopressors (NE, vasopressin, ØE!)
3. 🧫 infection
-AB
-Infectious source control
4. OTHERS
(consider FFP or Platelets if DIC; steroid if adrenal dysfunction, ventilation in ARDS, sedation, analgesia, glycemic control, bicarb if acidosis, ulcer. + DVT prophylaxis) |
🤧 Anaphylactic: | Initial:
1. 🌊Fluids
2. 🫀 Epinephrine bolus (if refract. other vasopressor)
3. Stop the exposure + airway maintanance
LATER:
- 🐝 Anti-histamines, 🌝steroids, 🎺 bronchodilators
- 🔺vasopressor (NE, vasopressin) |
🧠 Neurogenic: | 1. 🌊 Fluid
2. 🔺 Vasopressors (NE, vasopressin)
3. 🥀 Atropine (for bradycardia) |
- ⬇️ Injury below the diaphragm:
- 1 above: At least 1 i.v. line should be placed in a tributary of the superior vena cava.
- ⬆️ Thoracoabdominal damage:
- 1 above: At least one i.v. access site should be above the diaphragm.
- 1 below: One access below the diaphragm.
→ Never i.v. access in injured limb

The content of Na Osmolarity pH The amount of water provided Glucose requirements (calories) Anticipated rate of administration
Ringer Lactate
- large quantities + prolonged
- lactic acidosis
- Ø in RF, high need of free water, in transfusion line + hyperK
Saline solution
- RF
- hyponatremia , hyper
- transfusion line
- !! → hyperchloremic acidosis + hypokalemia
emergency:
- unnoticed loss of fluids (i.e. hemorrage after fracture)
- ventilation problem
- wrong Dgx
- other type of shock
- Addison crisis + DKA
- Hypothermia

- 🧠mental status
- 🩸 perfusion
- Vitals (RR, HR, Resp-rate)
- Diuresis
- Periph perfusion: recap-time
- CVP
- Start primary evaluation - ABC(DE)
- Start Tx during primary evaluation
- Evalulate FLUID LOSS
- Figure out TYPE of shock
- Assess RESPONSE to Tx
{kind=link}
↓
↓
↓
↓
- Vitals
- HR
- BP invasive → Ø good indicator of tissue perfusions
- CVC
- Pulmonary artery catheter
- SvO2 = mixed venous saturation
- Lactate (arterial)
- VO2 = O2 consumption
- DO2 = O2 delivery
- CO2 clearance
- SvO2 (Mixed Venous Saturation): It is a measure of the oxygen saturation of venous blood returning to the heart. It indicates the balance between oxygen delivery and consumption in the tissues.
- Lactate (Arterial): Lactate is a byproduct of anaerobic metabolism and is measured in arterial blood. Elevated levels of lactate can indicate tissue hypoxia or inadequate oxygen delivery.
- VO2 (O2 Consumption): VO2 represents the amount of oxygen consumed by the body per unit of time. It reflects the metabolic needs of the tissues and is an important parameter to monitor during anesthesia.
- DO2 (O2 Delivery): DO2 is a measure of the amount of oxygen delivered to the tissues per unit of time. It depends on cardiac output, hemoglobin concentration, and arterial oxygen content.
- CO2 Clearance: CO2 clearance refers to the removal of carbon dioxide from the body. It is an important parameter to monitor during anesthesia as elevated levels of CO2 can indicate inadequate ventilation.
- Vitals
- HR
- BP invasive → Ø good indicator of tissue perfusions
- CVC
- Pulmonary artery catheter
- SvO2 = mixed venous saturation
- Lactate (arterial)
- VO2 = O2 consumption
- DO2 = O2 delivery
- CO2 clearance
- SvO2 (Mixed Venous Saturation): It is a measure of the oxygen saturation of venous blood returning to the heart. It indicates the balance between oxygen delivery and consumption in the tissues.
- Lactate (Arterial): Lactate is a byproduct of anaerobic metabolism and is measured in arterial blood. Elevated levels of lactate can indicate tissue hypoxia or inadequate oxygen delivery.
- VO2 (O2 Consumption): VO2 represents the amount of oxygen consumed by the body per unit of time. It reflects the metabolic needs of the tissues and is an important parameter to monitor during anesthesia.
- DO2 (O2 Delivery): DO2 is a measure of the amount of oxygen delivered to the tissues per unit of time. It depends on cardiac output, hemoglobin concentration, and arterial oxygen content.
- CO2 Clearance: CO2 clearance refers to the removal of carbon dioxide from the body. It is an important parameter to monitor during anesthesia as elevated levels of CO2 can indicate inadequate ventilation.
persistent failure of Tx of all REVERSIBLE factors → usually after 30min (emergency: 20min asystolie
End tidal CO2 (capnography)
End tidal CO2 less than 15 mmHg after 20 minutes of advanced life support predicts death in patients with pulseless electrical activity.
- Cardiac rhythm (ECG)
- Haemodynamic status (CVP, PAC, or minimal invasive monitoring)
- Blood gases: adequacy of ventilation, severity of acidosis and electrolyte derangements
- Chest X-ray: position of tracheal tube, CVP line, evidence of trauma, pneumothorax, cardiac failure (pulmonary edema), aspiration of gastric content
therapeutic hypothermia
T
F 🤡
- none 🧟
- CAUSE must be identified
- COMA (Øarrousal)
→ must be IRREVERSIBLE → Exclusion of REVERSIBLE conditions (hypothermia, metabolic, drugs)
- ØBrainstem reflexes
• no pupil response to light • no corneal reflex • no vestibulo-occular reflex • no cranial nerve motor function • no gag reflex • no cough reflex • no breathing efforts
- Apnea test ⇒ Øresp. drive
Apnea Testing:
- Purpose: Apnea testing is a crucial component in the evaluation of brain death. The main objective of the test is to measure brainstem activity, which plays a vital role in controlling respiration.
- Procedure: Before the test, the patient undergoes preoxygenation with 100% oxygen. After this step, the patient is disconnected from the ventilator and then closely observed for any signs of respiratory drive, such as gasps or visible chest movement.
- Duration & Assessment: Approximately 8 to 10 minutes after disconnecting the ventilator, an arterial blood gas reading is taken.
- Results Interpretation: If the pCO2 (partial pressure of carbon dioxide in arterial blood) surpasses 60 mm Hg and/or the pH falls below 7.30, and the patient still shows no respiratory drive when the mechanical ventilation assistance is absent, the apnea test is considered positive. This means there's an absence of respiratory drive, supporting the diagnosis of brain death.
Q. The diagnosis of brain stem death includes the following criteria:
a. Apnea testing does not confirm the diagnosis of brain stem death. b. Testing of brain stem reflexes is mandatory. c. Preconditions and exclusion criteria have to be met. d. The diagnosis is made clinically. e. Cardiac arrest must be identified in every patient. f. The patient has a GCS of 3 repeatedly. g. Patients must be hypothermic. h. Patients must be sedated. i. Apnea should occur within 1 minute with alteration of blood gases. j. Absence of corneal reflex. k. Delta wave EEG. l. Absence of pupillary reflex. m. Hypothermia. n. Apnea in unsedated ventilated patients.
BCDFJI
(Major cardiovascular instability may occur in the brain stem dead patient) 📷
{kind=link}
🎉 CONGRATULATIONS YOU MADE IT! NOW YOU’RE PART OF THE ICU GANG !





