
Table of content
- Palliative medicine
- ⛲ Basics of palliative medicine
- 💮 Symptoms & symptom control
- 🗣️ Communication
- ⌛ Imminent death - ”the last hours”
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Palliative medicine
⛲ Basics of palliative medicine
total pain includes the:
- physical,
- emotional (psychological),
- social and
- spiritual dimensions of distress.
spiritual pain = existential suffering 📷
{kind=link}

⇒ A distinction based on clinical observations is made between suffering and physical distress (aka physical pain vs. the other 3 types)
⇒ The relief of suffering & cure of disease = twin obligations of a medical profession
approach to → IMPROVE QUALITY OF LIFE of people
with a LIFE-THREATENING/-LIMITING ILLNESS (and Ø ONLY TERMINAL ILLNESSES!)
LIFE LIMITING CONDITIONS = progressive conditions with Ø reasonable hope of cure and which the person will likely die from.

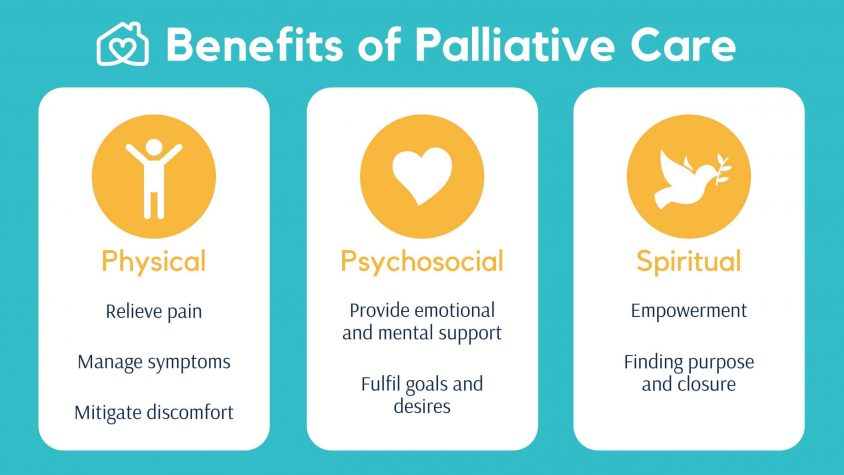
⇒ HOLISTIC APPROACH: 📷 Assessment, Prevention & TX of PHYSICAL + PSYCHO-SOCIAL (=social + emotional) + SPIRITUAL PAIN 📷
{kind=link}
{kind=link}
Definitions of palliative care:
"Palliative care is the active holistic care of individuals across all ages with serious health-related suffering (SHS) due to severe illness, and especially of those near the end of life.”
“Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial, and spiritual.”
{kind=link}
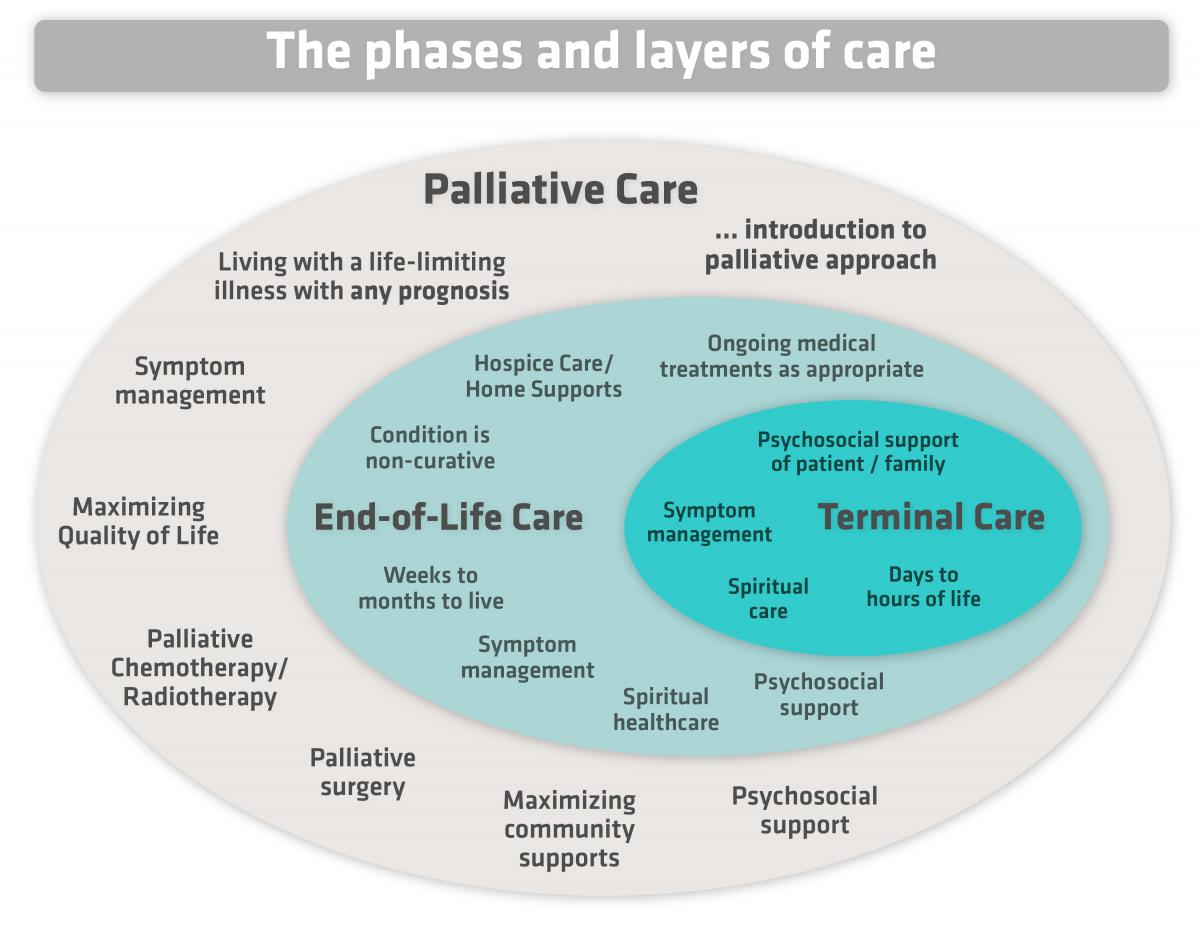
PALLIATIVE
- ANY TIME after Dgx
- includ. LIFE PROLONGING Tx
HOSPICE
- prognosis ≤ 6 MONTH
- COMFORT + SUPPORT
- Hospice care can be provided in various settings: at home or in a facility (nursing homes, hospitals, and dedicated hospice centers)
- A team of professionals, including nurses, doctors, social workers, spiritual advisors, and trained volunteers, provide ⇒ medical, emotional, and spiritual support.
Palliative care can provide assistance at any stage of illness
⇒ most effective when offered shortly after a person receives a diagnosis.
- SYMPTOM CONTROL + LIFE-PROLONGING INVTERVENTIONS
- Symptoms → pain + other
- LIFE-prolonging Tx → chemo, RT, complication
- Improve quality of life and positively impact the course of illness.
- It is applicable early in the illness and can be used alongside other life-prolonging therapies like chemotherapy or radiation.
- HOLISTIC APPROACH
- Affirms life and acknowledges dying as a natural process
- Integrates psychological and spiritual aspects of care
- Utilizes a team approach to address patient and family needs
“Holistic means the patient is viewed as a person with Physical, psychological, social, spiritual and cultural gifts and needs which are special to that person. Each of these aspects must be taken into account. “ (Anne Merriman, 2006)
aspects of holistic needs: physical, social psychological (emotional) and spiritual 📷
{kind=link}
1.) SHORT period of heavy decline ⇒ CANCER 2.) LONG term limitation w/ INTERMITTENT EPISODES ⇒ ORGAN FAILURE (heart, lung) 3.) PROLONGED DWINDLING ⇒ FRAIL elderly + DEMENTIA
⇒ Palliative care interventions benefit patients early in the trajectory of a life-limiting or life-threatening illness, as well as patients with good performance status.
Level | Description |
Level 1:
Palliative Care Approach | Provided in any location or setting by all healthcare professionals as part of their role and using a palliative care approach. |
Level 2:
General Palliative Care | Provided in any location, using a palliative care approach by healthcare professionals who have additional knowledge of palliative care principles and use this as part of their role. |
Level 3:
Specialist Palliative Care | Provided by healthcare professionals who work solely in palliative care and have extensive knowledge and skills in this specialty. |
everywhere 🤡
- Hospitals
- Nursing homes
- Outpatient palliative care clinics
- Certain other specialized clinics
- At home
- Which is the main disease? For how long does the patient suffer from it? What does the patient and family know about it?
- What treatment did the patient follow?
- Does the patient have other associated diseases?
↓
- What medications does the patient take?
- What medications did the patient use in the past? Which medications did have a positive impact?
- Were there any side effects to some medications? (allergy!!!)
↓
- How is the patient coping with the disease? Does the patient have emotional support? Does the patient have any spiritual concern? Fear of death?
- What are the patient's goals and objectives?
↓
- What is the general condition of the patient? Did the patient lose a significant amount of weight?
- Is the patient attentive and able to communicate clearly?
- How is the patient's mobility? What is the patient capable of doing by himself?
- According to the physical examination, what are the factors that may cause/provoke the symptoms?
↓
- Concentrate on the symptoms and problems that have the biggest impact on the patient's quality of life.
- Try to figure out what can be the cause of each symptom.
- Elaborate and discuss with the patient a clear plan targeting each of his problems. If a new problem surfaces, reevaluate the patient to figure the cause.
{kind=link}

- TREAT disease → ↓Symptoms
- Chemotherapy/Radiotherapy can be beneficial in improving the patient's quality of life, even if it does not offer a curative outcome.
- Certain diseases may lead to treatable complications, such as pneumonia requiring antibiotics for cough improvement or constipation management to alleviate abdominal pain.
- CARE
- Symptom control can be achieved through well-rounded care and not solely relying on medications.
- Genuine care and attention to detail play a crucial role in improving the patient's medical condition.
- Human-to-human interaction, with kind, honest words and active listening, holds significant value.
- Medical care at the patient's home can involve family, friends, healthcare professionals, and volunteers.
- The palliative medical team collaborates with the patient's support system to provide comprehensive care.
- DRUGS
- GIVE medications with a beneficial effect that outweighs the side effects.
- EDUCATE patients and caregivers about the medications.
- LIMIT the number of medications.
- REASSESS symptoms and medications in a regular interval.
EVALUATE
- holistic
- symptoms
- SPIKES - effective communication: patient involvement
- Patient communication: Address the patient's desired amount of information, level of involvement in decision making, and their ideas and concerns about symptoms.
- Understand Patient's Desires: Begin by clearly understanding what the patient wishes to know and address.
- Communicate Clearly: Provide information about the illness tailored to the patient's preferences, ensuring it's comprehensible without relying on complex medical jargon.
- Define Care Objectives: Establish care goals that enhance the patient's quality of life, such as comfort, sleep, and mobility.
- Prioritize Treatment: When multiple symptoms exist, identify and target the symptom of greatest concern to the patient first.
- Discuss Treatment Options: Review all possible treatments, highlighting their benefits and risks, and consider the patient's decision-making preferences.
TREAT
- correct what can be corrected
CARE
- Advance care planing (ACP)
- keep the TEAM informed about patient status
- ask for help
→ determine future care + Tx decision that alignt with patients wishes
(i.e. writing down of own wishes for future treatment they might want to refuse, like CPR)
local guidelines when
consult with the palliative care team
DRUGS
- regular + PRN (as needed)
- keep it as simple as possible (less drugs)
- Evaluate regularly + adjust
💮 Symptoms & symptom control
- Disease-related (cancer or Ø-malignant)
- Tx-related
- Complications due to illness (indirectly disease-related)
- Co-morbidities
DDx of breakthrough pain:
- Incident pain: Transitory pain caused by specific movements or activities related to the underlying condition (e.g., bone metastases, changes of dressings)
- Opioid end-of-dose pain: Pain that occurs when levels of opioids in the blood are decreasing toward the end of a dose interval
⏱️ ACUTE → noxious stimuli from recently damaged tissue
→ DISTRESSED appearance
→ CHANGES in VITALS
🕰️ CHRONIC → beyond expected healing period
→ Ø DISTRESSED
→ Ø CHANGES in vital

- Nociceptive pain:
- 🗡️ Somatic pain → sharp/localized
- Musculo-skeletal 🦴 💪🏼
- Vascular 🩸 (artery + vein)
- Visceral pain → dull/diffuse
- 🪞 Referred (radiated, mirrored) pain
- 🔥 Neuropathic pain → burning
- Central
- Peripheral
- Sympathetic
- 🗡️ + 🔥 Mixed (nociceptive + neuropathic)
- 🤪 Psychogenic
(bone, joint, peri-articular; muscle, skin)
⇒visceral ORGANS (i.e. ❤️)
- somatic → 🔪 localized + sharp
- visceral → diffuse, dull +- radiation + autonomic signs
- neuropathic → intermittend / permanent + 🔥 burning OR aching, numb, stabbing, shock-like
+ NEURO-SIGNS (sensory,motor, reflexes)
+/- 💦 autonomic changes in sympath. (vasomotor+sweating, trophic changes)
+/- 🧦 distal hypesthesia (periph)
- somatic → 🔪 localized + sharp
- visceral → diffuse, dull +- radiation + autonomic signs
- neuropathic → intermittend / permanent + 🔥 burning OR aching, numb, stabbing, shock-like
+ NEURO-SIGNS (sensory,motor, reflexes)
+/- 💦 autonomic changes in sympath. (vasomotor+sweating, trophic changes)
+/- 🧦 distal hypesthesia (periph)
↓
- 2) SYMPTOMATIC Tx:
- Neuropathic-pain → Anticonvulsants + antidepressants + steroids
- Spasticity → Muscle relexants
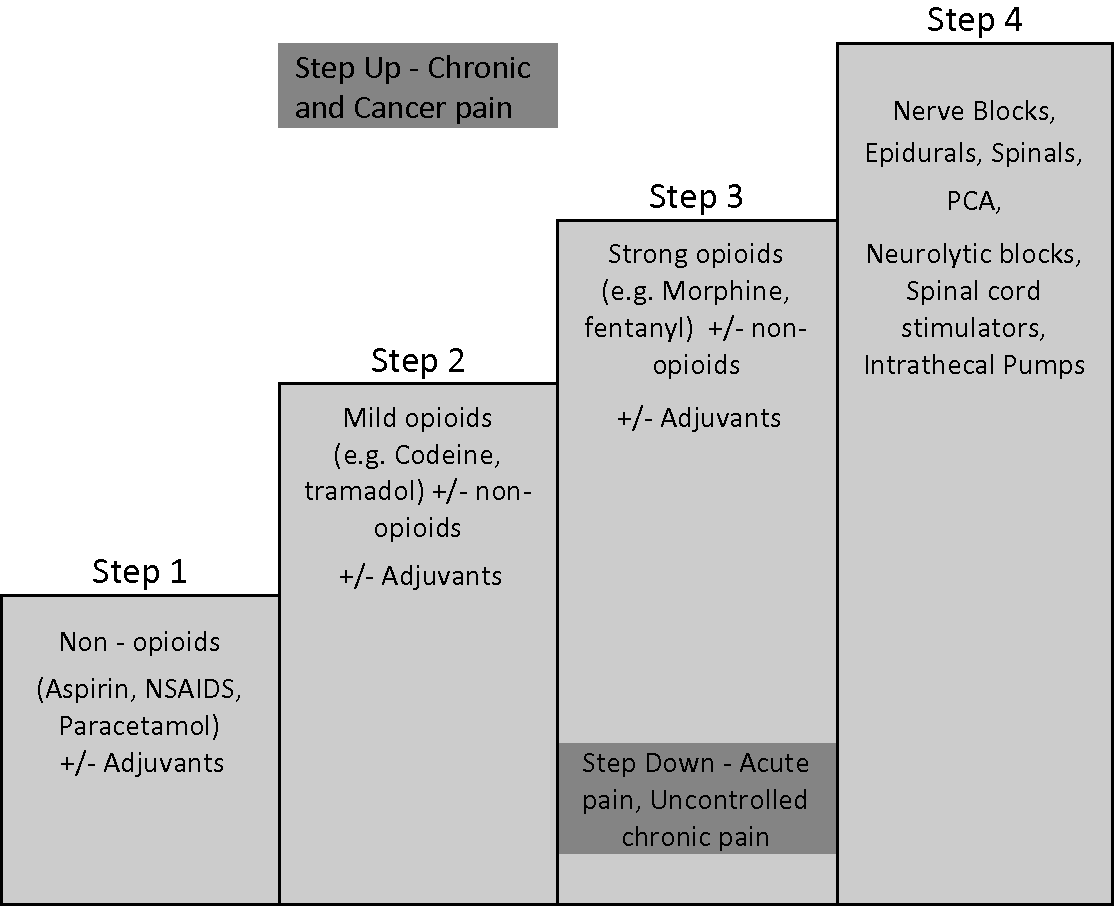
- STEP 3 OPIATES (i.e. morphine) ⇒ every 4h
- STEP 1+2 ⇒ every 6h
physical therapy
•Massage •Stretching •Heat •Splints and physical supports •TENS •Aids and appliances (hoist, wheel chair, walking frame etc...) •Wound care
*For the individual: right dose = satisfactory pain relief + minimum SE
*Attention to detail: incl. regular administration, PRN availability (rescue dose), SE anticipation (prophylactic laxatives + PRN anti-emetics)
parenteral → subcutaneous
{kind=link}
*PCA
(+biphosphonates in bone mets)
MILD PAIN = <3 ⇒ step 1
MOD. PAIN = 4-6⇒ step 2
SEV. PAIN >7 ⇒ step 3
GENERAL RULES:
STAGE 1:
1000 mg = 1g PO every 6 hours =4000mg/day
(=max dose)
400 mg PO every 6 h
(=max dose)
Stage 2:
50mg every 6h
30mg every 6h

50=lasso
30=maus
tramadol = tram/train
codein = syrup
Stage 3:
old lecture:
<65y ⇒ 10mg oral + 5mg injectable
>65y ⇒ 5mg oral + 2.5mg inject.
Amboss: STARTING DOSE : Immediate-release morphine 2.5–10 mg PO every 4 hours as needed

Morphine 2–10 mg SC/IV every 4 hours as needed
for breakthrough pain (incident or predicted)
→ additional immediate-release of the opioid used ⇒ 1/6 of total daily dose
⇒alternative: buccal/intranasal fentanyl
ex. 10mg every 4h = 60mg/day ⇒ rescue dose = 10mg
constipation ⇒ LAXATIVES
#1 Softener (docusate) + Stimulant (senna, bisacodyl)
#2 Add Osmotic agent (PEG, Lactulose)
Nausea/vomiting ⇒ 🤢 PROKINETIC ANTIEMETIC since opoids → constipation
⇒ metoclopramide / domperidone
⇒ give with opioid for first 1-2weeks
OR
Antipsychotic (Haloperidol)
Other SE: Sedation, Opioid induced neurotoxicity (stop/change opioid)
↓
- 3) Adress OTHER HOLISTIC aspects 😇
↓
- 4) REASSESS ♻️ (SE + pain adjustment)
- PHYSICAL PATHOLOGY
- Pulmonary disease
- Cardiovascular disease
- Muscle problems: weakness of respiratory muscles due to cachexia, phrenic nerve palsy
- Anemia
- Fever
- Treatment side effects: radiation, chemotherapy, surgery
- Other symptoms: pain, insomnia, fatigue
- OTHER HOLISTIC ASPECTS
- PSYCHOLOGICAL
- SOCIAL
- SPIRITUAL
→ see family medicine: dyspnea
Anxiety, panic attacks, depression
Financial, family concerns etc.
Suffering, existential distress
AB
Steroids + bronchodilatiors
transfusions (blood)
pallative chemo, RT, hormonal
steroids
stent or LASER for bronchial/tracheal obstruction
lymphangitis carcinomatosis:

aspiration
diuretics
anticoagulation
↓
- physio
- walking aids
- chest vibrations
- neuro-electrical muscle stimulation
- breathing training
- Opioids have been found to be effective in improving dyspnea in palliative care patients.
- Clinical experience and studies support the use of oral morphine sulfate in total daily doses of 10mg to 30mg for dyspnea relief.
- Dose titration for opioids in dyspnea is similar to opioid use in analgesia, but with lower doses (e.g., starting dose of 2.5mg every 4 hours) and smaller dose increments.
- In frail elderly patients, starting doses as low as 1.25mg every 4 hours may be appropriate.
- Daily doses up to 15mg have been effective in many patients.
OPIOIDS
starting dose = LOW
- lorazepam 0.5mg
- diazepam 2mg
⇒ if end of life ⇒ midazolam continous infusion (subcutaneous)
SSRI
<90% ⇒ oxygen
<94 ⇒ (piped??) air = oxygen
- Dyspnea may not correlate with hypoxemia.
- Response of dyspnea to supplemental oxygen varies.
- Some patients find supplemental oxygen helpful for dyspnea, while others do not.
- Issues with supplemental oxygen can include restriction due to being attached to an oxygen source, inhibition of communication, and discomfort (e.g., dry mouth, sore nose or ears from tubing).
- A minority of patients require continuous oxygen inhalation.
- In moderate to severe hypoxia (SaO2 < 90%), oxygen is better than air and should be offered if the patient wants to use it (usually 2-4 L/min prescribed).
- In mildly hypoxia (SaO2 90-94%), piped air appears to be as beneficial as oxygen.
↓
- 3) Adress OTHER HOLISTIC aspects
- General measures: air humidification, avoiding smoke, avoiding dehydration, comfort
- Medication: - Secretostimulating expectorants: Ipeca - Secretolytic expectorants Acetylcysteine - Central antitussives Codeine , Methadone, Dextromethorphan - Nebulized local aesthetics Xylene, Bupivacaine - Paroxetine, Amitriptyline, Gabapentin
{kind=link}
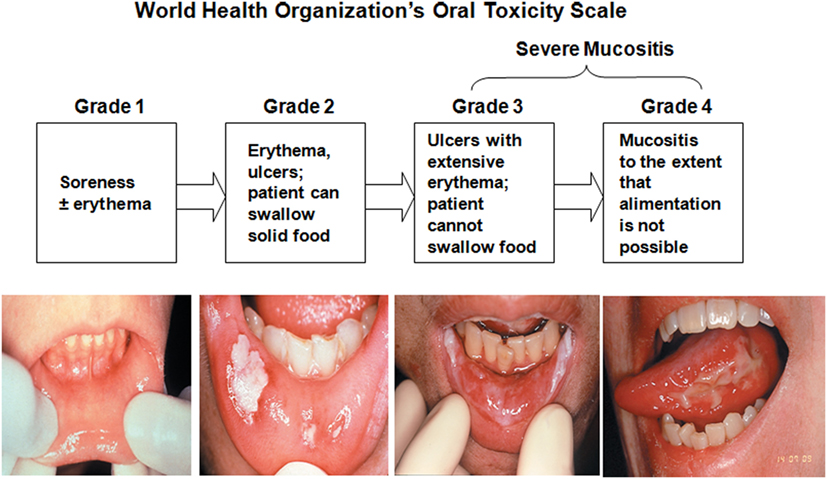
- Grade 0: No oral mucositis
- Grade 1: Erythema and Soreness
- Grade 2: Ulcers, able to eat solids
- Grade 3: Ulcers, requires liquid diet (due to mucositis)
- Grade 4: Ulcers, alimentation not possible (due to mucositis)
{kind=link}
CAUSE: Chemo (ØRT)
⇒ HYPO-GEUSIA; A-GEUSIA; DYS-GEUISIA
⇒ ↓NUTRITIONAL INTAKE
{kind=link}
SYMPTOMATIC
- ↑Oral hygiene, soft diet, high caloric drinks, NGT
- Dry mouth → fluid, gum, gels, artifical saliva
- pain → ice, mouth rinses + local anesthetic, systemic analgesic
- infection → anti-fungal, anti-viral
⇒ Intestinal obstruction 🚧 (+constipation)
⇒ + Gastroparesis (stasis)
⇒ infection 🦠

⇒ ↑ICP (intracranial pressure)
(i.e due to tumor)
⇒ Opioids, Digoxin, +AB + NSAID + SSRI

- uremia 🥐
- Ketosis 🍬
- electrolyte-disturbances
- ↑Ca 🍦
- ↓Na 🧂

Drug | D2 receptor antagonist | H1 receptor antagonist | ACh Muscarinic antagonist | 5HT receptor antagonist |
Domperidone (Prokinetic) | ++ | 0 | 0 | 0 |
Metoclopramide (Prokinetic) | ++ | 0 | 0 | + (5HT3) |
Ondansetron (5HT3 antagonist) | 0 | 0 | 0 | +++ |
Cyclizine (Antihistamine antimuscarinic) | 0 | ++ | ++ | 0 |
Haloperidol (Antipsychotic) | +++ | 0 | 0 | 0 |
Prochlorperazine (Antipsychotic) | ++ | + | 0 | 0 |
Levomepromazine (Antipsychotic) | ++ | +++ | ++ | +++ (5HT2) |
Hyoscine (Antimuscarinic) | 0 | 0 | +++ | 0 |
prokinetic (i.e. Metoclopramide)
PROKINETIC ANTIEMETIC since opoids → constipation
⇒ metoclopramide / domperidone
⇒ give with opioid for first 1-2weeks
OR
Antipsychotic (Haloperidol)
- CORRECT disturbance
- 💊
⇒ Consider drug that act on CTZ = D2 ⇒ Metoclopramide (prokinetic) OR Haloperidol
🥇ORAL PREFERRED
#2 ⇒ PARENTERAL (subcutaneus) if ⇒ SEVERE, ØTOLERATE, ↓ABSORPTION
(consider continous subcut. infusion)
- If Severe nausea, patient cant tolerate oral → parenteral antiemetics
- If oral medication is not tolerated, consider the subcutaneous route.
- Continuous subcutaneous infusion (CSCI) via a syringe driver can be used for persistent nausea.
- Seek advice from a specialist in palliative care if nausea does not improve.
- 💥pain during defecation
- 🎈bloating
- 💪straining
- 👀 sensation of incomple evacuation
<3x/w
- Usual bowel habit?
- Cause?
- 🥗 diet? + environmental?
- 💊 Drugs? (opiods)
- 🦀 Compression: Tumor?
- 🧠 Neuro signs?
- 🤪 psych?
(+ pain assessemt (SOCRATES))
- fluid + fibers
- physical activity
- other
To prevent or reduce constipation in palliative patients, prioritize patient privacy, comfort, and dignity, encourage physical activity within their limits, monitor fluid and fiber intake, be aware of constipating effects of medication and consider anticipatory prescribing, and provide patient and carer education. Once constipation is established, a combination of these measures is typically needed.
Laxatives
#1 Softener (docusate) + Stimulant (senna, bisacodyl)
#2 Add Osmotic agent (PEG, Lactulose)
- Acute diarrhea: ≤ 14 days
- Persistent diarrhea: > 14 days
- Chronic diarrhea: > 30 days
- 🥗
- 💊
- 🦀 tumor/radiation + 🚧
- 🔪 Malabsorption
- OTHER disease
- Motility + secretion modifying
- Absorbants
⇒ LOPERAMIDE 🐰
start with 4mg then → 2mg every 2-4h ⇒ for 12h = 3-6x (until resolved)

loperamide = 🐰
24 = niere (kidney) ⇒ start with 4mg, then 2 mg every 2-4h
codein
⇒ i.e. Methyl-cellulose
- PHYSICAL PATHOLOGY
- Anemia
- underlying disease (cancer, organ failure)
- infections, metabolic, endocrine
- drugs (opioids, benzos, antipsychotics, chemo)
- OTHER HOLISTIC ASPECTS
- PSYCHOLOGICAL
- SOCIAL
- SPIRITUAL
- 🥇 MAINLY 1) ETIOLOGICAL Tx (treat what is treatable)
↓
steroids
⇒ predni 40mg / day → only last for 2-4w
longer treatment (at this dose) → might lead to side effects (i.e. myopathy) ⇒ therefore, Ø recommended
↓
- 3) Adress OTHER HOLISTIC aspects
- Benzos
- TCA + SSRI
- Neuroleptics
🗣️ Communication
Setting → plan where to deliver the news
- Sit down and ensure privacy and adequate time for the conversation.
- Confirm medical facts and establish the purpose of the conversation to set goals for care.
- Plan what you will say and create a conducive environment.
- Prevent interruptions and determine if the patient would like others, such as parents, to be present.
Perception → what does the patient know?
- Start the conversation with an open-ended question to assess the patient's understanding of their illness and gather relevant information (i.e. “I'd like to start by having you tell me what you know about your illness.”)
- Inquire about the patient's knowledge and comprehension level, particularly for delivering difficult news.
- Consider rescheduling the discussion if the patient is unprepared or unable to comprehend new information.
Invitation → How much does the patient want to know?
- Start the conversation by asking about the patient's expectations for the future with their illness.
- Respect and support various patient preferences, including the decision to decline information or designate a spokesperson.
- Recognize that different individuals handle information differently based on factors such as race, ethnicity, culture, religion, socioeconomic status, age, and developmental level.
Knowledge → share news
- Avoid minimizing severity and vagueness
- Use confident and academic language
- Use language like:
- “I feel badly to have to tell you this, but the growth turned out to be cancer. “
- “I'm afraid the news is not good. “
- “The biopsy showed that you have colon cancer.”
- “Unfortunately, there's no question about the test results: it is cancer.”
- “The report is back, and it's not as we had hoped. It showed that there is cancer in your colon.”
- “I'm afraid I have bad news. The bone marrow biopsy shows that you have leukemia.”
Emotion → Respond to emotion
- Be prepared for emotional responses:
- Expect strong emotions and diverse reactions.
- Allow time for the person to react.
- Engage in active listening:
- Listen without interrupting.
- Encourage sharing of feelings.
- Use non-verbal cues to show empathy and support.
- Recognize normal reactions to difficult news:
- Emotional (Affective): Tears, anger, sadness, relief, etc.
- Cognitive: Denial, blame, guilt, fear, shame.
- Physiological (Psychophysiological): Fight-or-flight response.
- Facilitate communication:
- Validate their feelings: "This must be hard for you."
- Invite further discussion: "Would you like to talk about what you're feeling?"
- Offer support: "I'm here to help you through this."
- Provide reassurance in sensitive situations, especially to children:
- Comfort them about their family's emotions: "Your parents are sad now, but they'll feel better seeing you recover."
Subsequent → Make a plan + Follow up
Plan for the Next Steps:
Whenever possible, formulate three plans:
- Best-Case Scenario: Outline the steps for the optimal outcome.
- Worst-Case Scenario: Prepare for the most unfavorable circumstances.
- Unexpected Events: Address any unforeseen developments.
Additional Information:
- Treat symptoms and provide referrals as necessary.
- Discuss potential sources of support for the patient.
- Share contact information and schedule the next appointment.
Before concluding the session, assess:
- The patient's safety.
- The availability of support at home.
- The need to reiterate key information during future visits.
- Establish the Appropriate Setting: Begin the process.
- Inquiry and Discovery (Perception): Determine the patient and family's existing knowledge.
- Assess the Desire for Information (invitation): Understand their preferences.
- Advocacy: Explore life and care goals, while suggesting realistic objectives.
- Address Emotions with Empathy: Respond to emotional needs.
- Develop a Care Plan and Execute It: Create and implement a plan.
- Periodic Review and Revision: Regularly assess and adjust as needed.
Subsequent:
⌛ Imminent death - ”the last hours”
aka changes during dying process
{kind=link}
Early
- ↑💤 sleeping
- ↓🥗 loss of interest in drink+food
- ↑🧠 Delirium
- 🛌🏽 Difficulty mobilizing → bedbound
Late
- 🪰 Mottles extremities
- 💦 Terminal respiratory secretions (”death rattles”)
- 🫁 irregular breathing w/ apnea periodes
- 🧠 coma / terminal agitation
👂
Loss | Grief | Mourning | Bereavement | |
Definition | No longer having something | The normal process of reacting to the loss | The social expressions or acts expressive of grief | The period after a loss during which grief is experienced. |
Description | Tangible or Intangible
- Tangible losses are easily recognized (Body part, health, personal belongings)
- Intangible (Perceived/psychological) losses are less obvious (Loss of prestige, hope, faith) | Emotional response to loss
Involves emotional, cognitive, and behavioral processes and tasks
Experienced in waves, intensity decreases over time (No set schedule, progression varies among individuals) → Complicated grief without progress can be concerning | Social or cultural response to grief (Public or communal practices, like funerals) | A state of intense grief after the loss of a loved one
Acknowledged as a period of mourning (Exemplified by the widow receiving visitors during her bereavement; Desolation) |
{kind=link}
- Denial
- Anger
- Bargaining
- Depression
- Acceptance
- ANTICIPATORY grief → Progression through the stages of grief prior to the loss.
- Reflection on Life: Patients reviewing their life
- Preparation for the Future: Families looking ahead to a future without the dying person
- Emotional Closure: Expressing sentiments like "Forgive me, I forgive you, thank you, I love you, and goodbye"
- Cultural Variations: Different cultural backgrounds influencing how individuals cope
- Grief Reactions in Parents: May be mistaken for depression or imminent death, especially in cases involving terminally ill children.
- COMPLEX grief (chronic, traumatic) → extreme grief, strong longing for “normality”, strong impact on functional status
- DISENFRANCHISED (”suppressed”) grief → loss that can Ø be oppenly acknowledged
- Minimization of the loss (e.g., a loss not deemed significant, such as a non-death loss).
- Stigmatization of the relationship (e.g., an extramarital affair).
- Stigmatization of the cause of death (e.g., suicide).
- Lack of recognition of the grieving individual (e.g., a coworker or former partner).
- Stigmatization of the grieving process (e.g., criticism for not displaying outward grief or for exhibiting extreme grief responses).