







Palliative medicine
- Palliative medicine
- ⛲ Basics of palliative medicine 🔓
- 💮 Symptoms & symptom control
- 🗣️ Communication 🔒
- ⌛ Imminent death - ”the last hours” 🔒
⛲ Basics of palliative medicine 🔓
- ❔ Basic definitions
- 🎏 Dgx & Tx Principles
💮 Symptoms & symptom control
- Disease-related (cancer or Ø-malignant)
- Tx-related
- Complications due to illness (indirectly disease-related)
- Co-morbidities
DDx of breakthrough pain:
- Incident pain: Transitory pain caused by specific movements or activities related to the underlying condition (e.g., bone metastases, changes of dressings)
- Opioid end-of-dose pain: Pain that occurs when levels of opioids in the blood are decreasing toward the end of a dose interval
⏱️ ACUTE → noxious stimuli from recently damaged tissue
→ DISTRESSED appearance
→ CHANGES in VITALS
🕰️ CHRONIC → beyond expected healing period
→ Ø DISTRESSED
→ Ø CHANGES in vital

- Nociceptive pain:
- 🗡️ Somatic pain → sharp/localized
- Musculo-skeletal 🦴 💪🏼
- Vascular 🩸 (artery + vein)
- Visceral pain → dull/diffuse
- 🪞 Referred (radiated, mirrored) pain
- 🔥 Neuropathic pain → burning
- Central
- Peripheral
- Sympathetic
- 🗡️ + 🔥 Mixed (nociceptive + neuropathic)
- 🤪 Psychogenic
(bone, joint, peri-articular; muscle, skin)
⇒visceral ORGANS (i.e. ❤️)
- somatic → 🔪 localized + sharp
- visceral → diffuse, dull +- radiation + autonomic signs
- neuropathic → intermittend / permanent + 🔥 burning OR aching, numb, stabbing, shock-like
+ NEURO-SIGNS (sensory,motor, reflexes)
+/- 💦 autonomic changes in sympath. (vasomotor+sweating, trophic changes)
+/- 🧦 distal hypesthesia (periph)
- somatic → 🔪 localized + sharp
- visceral → diffuse, dull +- radiation + autonomic signs
- neuropathic → intermittend / permanent + 🔥 burning OR aching, numb, stabbing, shock-like
+ NEURO-SIGNS (sensory,motor, reflexes)
+/- 💦 autonomic changes in sympath. (vasomotor+sweating, trophic changes)
+/- 🧦 distal hypesthesia (periph)
↓
- 2) SYMPTOMATIC Tx:
- Neuropathic-pain → Anticonvulsants + antidepressants + steroids
- Spasticity → Muscle relexants
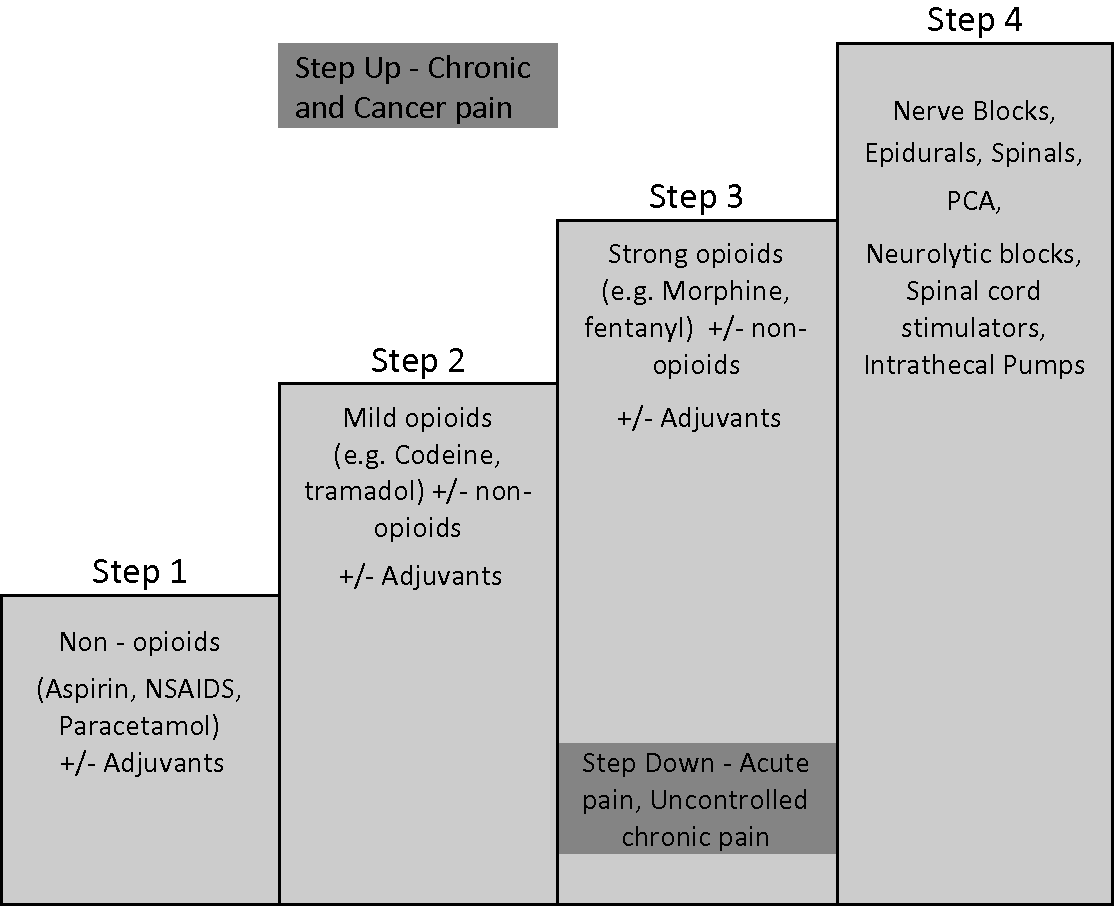
- STEP 3 OPIATES (i.e. morphine) ⇒ every 4h
- STEP 1+2 ⇒ every 6h
physical therapy
•Massage •Stretching •Heat •Splints and physical supports •TENS •Aids and appliances (hoist, wheel chair, walking frame etc...) •Wound care
*For the individual: right dose = satisfactory pain relief + minimum SE
*Attention to detail: incl. regular administration, PRN availability (rescue dose), SE anticipation (prophylactic laxatives + PRN anti-emetics)
parenteral → subcutaneous
{kind=link}
*PCA
(+biphosphonates in bone mets)
MILD PAIN = <3 ⇒ step 1
MOD. PAIN = 4-6⇒ step 2
SEV. PAIN >7 ⇒ step 3
GENERAL RULES:
STAGE 1:
1000 mg = 1g PO every 6 hours =4000mg/day
(=max dose)
400 mg PO every 6 h
(=max dose)
Stage 2:
50mg every 6h
30mg every 6h

50=lasso
30=maus
tramadol = tram/train
codein = syrup
Stage 3:
old lecture:
<65y ⇒ 10mg oral + 5mg injectable
>65y ⇒ 5mg oral + 2.5mg inject.
Amboss: STARTING DOSE : Immediate-release morphine 2.5–10 mg PO every 4 hours as needed

Morphine 2–10 mg SC/IV every 4 hours as needed
for breakthrough pain (incident or predicted)
→ additional immediate-release of the opioid used ⇒ 1/6 of total daily dose
⇒alternative: buccal/intranasal fentanyl
ex. 10mg every 4h = 60mg/day ⇒ rescue dose = 10mg
constipation ⇒ LAXATIVES
#1 Softener (docusate) + Stimulant (senna, bisacodyl)
#2 Add Osmotic agent (PEG, Lactulose)
Nausea/vomiting ⇒ 🤢 PROKINETIC ANTIEMETIC since opoids → constipation
⇒ metoclopramide / domperidone
⇒ give with opioid for first 1-2weeks
OR
Antipsychotic (Haloperidol)
Other SE: Sedation, Opioid induced neurotoxicity (stop/change opioid)
↓
- 3) Adress OTHER HOLISTIC aspects 😇
↓
- 4) REASSESS ♻️ (SE + pain adjustment)
- 💨 Dyspnea
- 🌬️ Cough
- 👄 Oral problems
- 🤢 Nausea, vomiting & anorexia
- 🪠Constipation
- 💩 Diarrhea
- 😴 Fatigue
- 😱 Anxiety
🗣️ Communication 🔒
- 🗞️ Delivering BAD NEWS
- 🎯 Negotiate GOALS OF CARE
⌛ Imminent death - ”the last hours” 🔒
- 👀 RECOGNIZING imminent death
- 😓 LOSS & GRIEF