
Table of content
- Psychiatry
- Psychiatric Therapy
- 🗣️ Psycho-Therapy
- 💊 Pharma Treatment
- Psychiatric Disorders
- 🎭 Mood disorders
- 😱 Anxiety disorders
- 😵💫 Psychotic disorders
- 👹 Personality disorders
- 🕳️ Dissociative Disorder
- 🍺 Alcohol & Substance abuse
- 👵🏽 Disorders of consciousness, memory & cognition
- 🐣 Pediatric psychiatry
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Psychiatry
Psychiatric Therapy
🗣️ Psycho-Therapy
A treatment approach for individuals experiencing mental or physical challenges, focused on achieving symptom relief through interpersonal interactions with another person.
studies suggest that up to 60-90% of therapy outcome is due to common factors with only 10-40% due to specific factors common factors are:
- warmth (unconditional positive regard),
- accurate empathy,
- genuineness,
- goodness of fit,
- relationship with provider predicts positive outcomes
⇒ see PS48 in Toronto notes for more information!
💊 Pharma Treatment
block D2-R
FGAs → D1+D2
SGAs → D2 (selective → less SE)
(Clozapine → D4)
- ⚙️ Extrapyramidal
- 🍼 ↑PRL → amenorrhea, gynecomastia
- ❤️ CV
- ↓BP
- ventricular arrhythmias (torsades)
- ⚡ Seizures
- 💤 M-cholinolytic effect → Sedation
- ⌛ Agranulocytosis (clozapine)
- 👨🏽🌾 NMS 📷→ give muscle relexants, stop antipsychotic → switch to 2nd gen after 2w
→ Acathisia (restlessness) → benzos, BB or switch to 2nd gen
→ Parkinsonims → ↓dose, switch to 2nd gen or anticholinergics
→ acute dystonia (torticolis, spasm, grimaces) → give anticholinergics
→ tardive dyskinesia (irreversible extrapyramidal; the ones above are reversible) → switch to 2nd gen
SGAS:
- also ↓negative symptoms (FGAs only positive)
- ↓ extrapyramidal symptoms, PRL, NMS
- ↓anti-cholinergic SE
- ↓Seizures
- ↓Relapse
⇒ BUT SGA → ↑ metabolic SE
High potentcy → haloperidol
low potency → Chlorpromazine
more side effects because less specific to D2-R
(low potency ↑ sedating + hypotension)
- Haloperidol (most important)
- "azines" and "penthixols"
- Chlorpromazine (=Phenothiazine)
- Levomepromazine
- Flupenthixol
- Zuclopenthixol
Long acting FGAs
anti-psychotic | sedative | anti-emetic | |
Haloperidol | ↑↑ | - | ↑↑ |
Chlorpromazin | ↑ | ↑↑ | ↑↑ |
Haloperidol → ↑↑antipsychotic + ↑↑antiemetic
Chlorpromazine → ↑↑sedative, ↑↑antiemetic ↑antipsychotic
Levomepromazin→ ↑↑sedative, ↓antipsychotic (weak), mild analgesic
-Penthixol → ↑sedative, ↑antipsychotic, ↑anxiolytic
- Clozapine
- Quetiapine
- Olanzapine
- Risperidone
- Aripiprazol
- Ziprasidone
- All → like FGA
- torsades but ↓seizures
- but ↓ Extrapyramidal+Anticholinergic, PRL, NMS
- SPECIFIC:
- “APINES” (cloza, olanz,queti,)⇒ 🧈 metabolic synd
- 🚽 CLOZAPINE → ⌛ Agranulocytosis + ⚡ SEIZURES
block Serotonin reuptake
F → benzos are indicate in acute condition (fast action)
(SSRI need 1-2month to be effective) [bocsan: antidepressant effect - 2-4weeks])
⇒ LONG TERM TREATMENT
- Depression
- Anxiety disorders (not acute!, if acute →benzos)
- Panic attack disorder
- PTSD
- OCD (higher doses)
- Bulemia
- Fluoxetine
- Paroxetine
- Sertraline
- Citalopram
All similar effectiveness → consider SIDE EFFECTS:
- fewest drug interaction → citalopram escitalopram
- pregnancy → sertraline
- most activating, no tapering requried (long half-life) → Fluoxetine
- OCD → max dose SSRI (or even higher)
sertaline + paroxetine (the 2 in the middle)
Serotonin Syndrome 📷 → Hyperthermia, HT + ↑neuromusc. activity (↑reflexes)
→ MAO + TCA ↑risk ⇒ dont give with them
→ Treat with: Cyproheptadine (Der lächelnde Cipro hebt Nadine)
LESS SIDE EFFECT
(no cardiovascular + antimuscarinic side effect)
- 🙂 Serotonin syndrome 📷
- 🍤 GI
- nausea, diarrhea,
- ↑ weight
- 🍆 sexual dysfunction
- 🚰 SIADH. 📷
- ↑/↓🧠
- ↑ insomnia, Aggression
- drowsiness
- One must be vigilant over the first 2 weeks of therapy.
- Neuro-vegetative symptoms may start to resolve during this period, but emotional and cognitive symptoms may not.
- There's a mention that patients, especially children/adolescents, might be at risk for suicidal behavior during this time.
- Concerning the onset of effect:
- Relief from neuro-vegetative/physical symptoms occurs between 1 to 3 weeks.
- Relief from emotional/cognitive symptoms happens between 2 to 6 weeks.
↑suicidal ideation on starting therapy ⇒ give benzos
flu-like symptoms + others (FINISH)
FINISH Flu-like symptoms Insomnia Nausea Imbalance Sensory disturbances Hyperarousal (anxiety/agitation)
- Amitriptylin + Nortriptylin
- Imipramine, Desipramin, Clomipramine
(secondary amines have less M-cholinolytic side effects)
- Block Serotonin +NE re-uptake → antidepressive
- block H1 → sedation, ↑weight
- M-cholinolytic → urinary retention, dry mouth, constipation, blurred vision
- Block alpha 1 → Hypotension
- SSRI resistant Depression (SSRI are #1line)
- OCD (SSRI = #1line)
- Severe chronic pain
- Anxiety disorder, incl Bulimia+Enuresis
- ADHD (Stimulants = first line)
- ❤️Cardiotoxicity
- Arrhythmias (i.e. torsades)→ can be fatal
- myocardial depression
- AV block
- Serot.+NE effect:
- tremor + sweating
- tachycardia
- ⚡ seizures
- Anti-cholinergic effect (=M-cholinolytic)
- dry mouth
- constipation
- urinary retention
- blurred vision
- Alpha 1-adrenergic effect → Orthostatic hypotension D + dizziness
- Anti-histaminic: weight gain, sedation
- ↑ → then ↓ 🧠
- CNS stimulation + Convulsion
- → Sedation
- mood inversion + muscle tremor
- supportive → Saline solution + electrolytes
- symptomatic
- convulsion → diazepam (iv)
- Arrhythmias → Lidocaine + Porpranolol
- Anti-cholinergic symptoms (coma) → Physostigmine
- fibromyalgia + neuropathic pain (i.e. in diabetes)
- Depression
- Anxiety disorders
Like SSRI + ↑sympathetic (HT+↑HR, dry mouth, sweating, ↓appetite)
- Venlafaxin (Wendler macht faxen)
- Duloxetine (Zwei Oxen-Teens)
+Desvenlafaxine
"Wendler macht faxen mit zwei oxen-teens."
Buproprion
(NET DAT = Nor-epinephrin + Dopamine) (Ball pro = Buproprion)
No only NE+Dopa (NET+DAT)
It causes less..
↓ 😴 sedation
↓ 🧈 weight gain
↓ 🍆 sexual dysfunction (only delayed ejaculation as SE)
SSRI
(also useful in depression + low energy because ↑CNS effect aka less sedating)
- Nicotine dependance
- weight loss (off-label)
- ADHD
- neuropathic pain
- ↑🧠
- ❤️ CV
- Hypotension + dizziness
- Tachycardia, arrhythmia
- 🍤 GI
- N/V, diarrhea, pain
- dry mouth
- Fever
- GU: delayed sexual ejaculation
⇒ ⚡ Convulsion
anxiety disorders (including BULEMIA) → stimulation effect
Trazodone + Mirtazapin

- 5-HT receptor antagonist → 5-HT 2a+ 5-HT 2c
- Inhibit 5-HT Re-uptake
- Sedation (also H1 blocker)
- hypotension + priapism + sexual dysfunction
- serotonic syndrome
rapid
MOA = alpha2 blocker → ↑Serotonine + NE release (presynaptic)
but also 5-HT2a+c + 5-HT-3
Depression WITH insomnia, agitation
⇒ Bind als H1-R → sedation
(H1 blocker effects)
Weight gain
sedation + dizziness
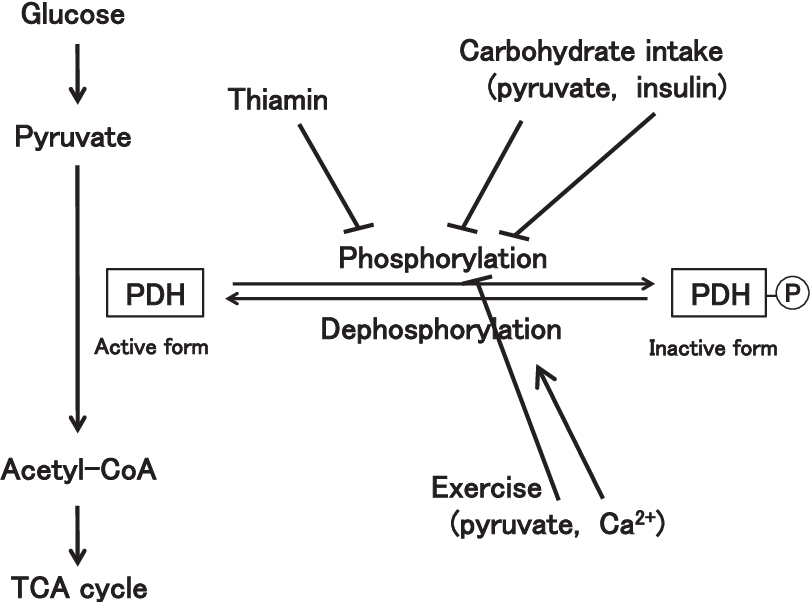
*thiamine rich food = wine, cheese
- optimization: adjust dosage to maximum tolerated or highest therapeutic dose.
- augmentation: introducing a drug that isn't labeled as an antidepressant to a treatment strategy (i.e. thyroid hormone, lithium, atypical antipsychotics (aripiprazole, quetiapine, olanzapine, risperidone))
- combination: incorporating another antidepressant into a current treatment plan (i.e. the inclusion of bupropion or mirtazapine to an SSRI or SNRI)
- switch: alter the main antidepressant (either within the same type or a different one).
- note: it's pivotal to comprehensively address depression signs (i.e., achieve remission) to minimize the likelihood of returning symptoms.
#1
Option A: SSRI / other atypical AD
Option B: TCA or Trazodone
↓
#2
⇒ Increase dose until maximum dose (max. tolerated or max. therapeutic)
⇒ switch
→ Option A with Option B
→ use DUAL anti-depressants (i.e. venlafaxin, mirtazapin, etc)
↓
#3
⇒ combine 2 AD from OPTION 1
⇒ Thyroid hormones
↓
#4
Antipsychotic (quetiapine), Mood stabilizers (lamitrigine), Es-ketamine
+/- AD from Option A
*adjuvant = augmentation
bipolar mood disorder (manic episodes)
- 🏂🏽 Lithium #1
- ⚡ valproic acid, lamotrigin, carbamazepin
→ pregnancy = #1 lamotrigine
LT - 🦋 ↓(low) thyroid
H - 🫀 Heart anomaly (Ebstein)
I - 🚰 Insipidus (nephrogrenic (DI)
UM - 👋🏽 Unwanted Movement → Tremor
Excretion ⇒ 🥐 kidney (⚠️ drug interaction - 🧯, 🌊)
- lamitrigine
- Antipsychotics (halo)
- 😱 Acute Anxiolytics → Benzos
Psychiatric Disorders
🎭 Mood disorders

*MDD = Major depressive disorder
F - more common in woman
False statement
⇒ M=F (equally distributed)
childhood → somatic, irritability, social withdrawal
adolescents → “ATYPICAL” ⇒ ↑eating + ↑sleep (see below)
elderly → “TYPICAL”/ MELANCHOLIC features ⇒ ANHEDONIA = ↓ interest + pleasure ⇒ ↓eat+sleep

MANIA | HYPOMANIA | |
↑/irritablemood + ↑energy/activity | ✅ | ✅ |
duration | ≥ 1 WEEK | ≥ 4 DAYS |
complete functional impairment | ✅ | Ø |
hospitalization required | ✅ | Ø |
psychotic features | +/- | Ø |
PLUS ≥3 OTHER CRITERIA MET (see “DIG FAST” below)
- 🧠 NEURO
- 🧑🏽🦼MS
- 🦀frontal lobe tumor
- 🦋+🌝 ENDOCRINE
- hyperthyroidism
- cushings
- 🍻 alcohol
- ❄️ cocaine + other amphetamines
- 🧫 Tuberculostatics
- 🎭 anti-depressants
- 🌝 steroid-hormones
- Secondary to other PSYCHIATRIC CAUSES


Mood disorder with..
- Catatonic features (immobility etc.)
- Psychotic features (hallucination+dellusion)
- Melancholic pattern (typical depression)
- Seasonal pattern
- Postpartum




- Mild: Some difficulty in continuing with normal activities
- Moderate: Considerable difficulty in continuing normal activities but still able to function in some domains
- Severe: Unable to continue normal activities
- Antidepressant (SSRI or other) → mainly Fluoxetine (Prozac)
- Psychotherapy
- ECT
⇒more details: see Tx-approach above!
⇒ See psychotherapy types above!
- Chronic ⇒ Mood stabilizers ⇒ see above
- Agitated ⇒ Antipsychotic (quetiapine, olanzapine)
- in depressive episodes there might be an anti-depressant added, but usually not used in bipolar!
- Psychotherapy
- ECT
#1 Lithitium
#2 Valproic acid, Carbamazepin, Lamotrigin
Case 1: A 33-year-old woman has been feeling down for the past six months. She has lost interest in activities she used to enjoy and has trouble sleeping at night. She feels tired all the time and has lost a significant amount of weight. She has also been having thoughts of self-harm.
Case 2: A 25-year-old man has been experiencing episodes of intense excitement and energy for the past year. He has been spending money impulsively, engaging in risky behaviors, and feeling irritable and angry when he doesn't get his way. He has also been experiencing difficulty sleeping but feels wide awake in the middle of the night.
Case 3: A 45-year-old man has been feeling sad and hopeless for most of his life. He has trouble sleeping and finds it difficult to motivate himself to do anything. He has a history of alcohol abuse and has recently been feeling more hopeless and helpless than usual.
Case 4: A 30-year-old woman has been experiencing periods of low mood, irritability, and trouble sleeping for the past two years. She has also been feeling self-critical and lacks confidence in her abilities. She has been struggling to keep up with her daily responsibilities and has been feeling overwhelmed. Sometimes he has periods of an elevated mood. during these episodes she talks way more than usual, her husband reports.
Case 5: A 40-year-old man has been experiencing mood swings for the past ten years. He has periods of high energy and activity, followed by periods of low mood and decreased energy. He has been struggling to keep up with work and relationships and has a history of substance abuse. He tells you, that he already had a major depressive episode in the past.
Case 1: Major Depressive Disorder Case 2: Bipolar I Disorder Case 3: Dysthymic Disorder Case 4: Cyclothymic Disorder Case 5: Bipolar II Disorder
😱 Anxiety disorders


Disorder | CBT | SSRI | Benzos | Other | #2 drugs |
Panic D. | ✔️ | ✔️ | ✔️ | TCA | |
PTSD | ✔️ | ✔️ | Ø | Prazosin
(↓ night mares)
EXPOSURE tx | - anti-psychotics
- anti-convulsants |
ASD | ✔️ | Ø | Ø | ||
OCD | ✔️ | ✔️ | Ø | higher doses | - busprione
- lithium
- benzos |
PHOBIAS | ✔️ | ✔️
(agoraph) | +- | EXPOSURE therapy | |
SOCIAL anxiety | ✔️ | ✔️ | +-
(if performance eg, anxiety restricted to public speaking) | BB (betablocker)
(if performance)
EXPOSURE Tx | |
ADJUSTMENT | ✔️ | +- | +- | ||
GAD | ✔️ | ✔️ | +- | - anti-psychotics
- anti-convulsants |
Case 1: A 35-year-old man has been experiencing intense fear and avoidance of certain situations, such as crowded places and public transportation, for the past two years. He has also been experiencing physical symptoms, such as sweating and heart palpitations, in these situations.
Case 2: A 27-year-old woman has been experiencing intrusive and distressing thoughts, images, and urges related to contamination and germs for the past year. She has been engaging in repetitive behaviors, such as excessive hand-washing, to try to alleviate her anxiety.
Case 3: A 32-year-old man has been feeling overwhelmed with worry and anxiety for the past six months. He has trouble sleeping and finds it difficult to concentrate on his work. He has been experiencing physical symptoms, such as headaches and muscle tension, as a result of his anxiety.
Case 4: A 25-year-old woman has been experiencing symptoms of distress and difficulty functioning since witnessing a traumatic event three weeks ago. She has been having nightmares, flashbacks, and difficulty sleeping. She has also been feeling jumpy and on edge and has been avoiding things that remind her of the event.
Case 5: A 28-year-old veteran named Jack was deployed to a war zone for two years and experienced several traumatic events while serving in the military. After returning home, he has been experiencing distressing memories, nightmares, and flashbacks of the traumatic events. He has been feeling on edge and easily startled, and has been avoiding things that remind him of the traumatic events. He has also been feeling disconnected from others and has been experiencing feelings of guilt and shame related to his experiences in the war zone. Jack has been struggling to adjust to civilian life and has been experiencing difficulty sleeping and concentration difficulties. He has also been experiencing physical symptoms, such as headaches and muscle tension, as a result of his PTSD. Jack has been feeling overwhelmed and hopeless and has been having thoughts of suicide.
Case 6: A 30-year-old woman has been feeling overwhelmed and sad since a recent significant life change. She has been struggling to adjust to her new circumstances and has been feeling hopeless and helpless. She has also been experiencing physical symptoms, such as fatigue and difficulty sleeping.
Case 7: A 40-year-old man has been experiencing intense fear and avoidance of social situations, such as public speaking and parties, for the past five years. He has been feeling self-conscious and worried about being judged by others in these situations.
Case 8: A 45-year-old woman has been experiencing sudden, intense, and excessive panic attacks for the past year. She has been avoiding certain situations, such as driving and being alone, because of her fear of having another panic attack.
Case 1: Agoraphobia Case 2: Obsessive-Compulsive Disorder (OCD) Case 3: Generalized Anxiety Disorder (GAD) Case 4: Acute Stress Disorder (ASD) Case 5: PTSD Case 6: Adjustment Disorder Case 7: Social Anxiety Disorder (Social Phobia) Case 8: Panic Disorder
🍔 Eating disorders
Anorexia nervosa
- Fear of weight gain + body image distortion (=”delusional-like”)→ calorie restrictions
- ↓ BMI
- 2 types:
- binge-eating/purging type: vomiting, diuretics
- restriction type: excessive exercise + diet
- cave: refeeding syndrome! + other


Bulimia nervosa
- Craving + food preocupation → Reccur. episode of BINGE eating in short periode of time → compensatory PURGING (vomiting, laxatives, diuretics)
- BMI = n/ slightly↑ body weight
- at least weekly over 3m
- ← Often history of anorexia n.
- 🥕 NUTRITIONAL rehab
- 🗣️ Psycho-Tx
- 🙂 SSRI
- Anorexia → consider 😵💫 anti-psychotic

Case 1: A 25-year-old woman named Emily has been experiencing recurrent episodes of binge eating, followed by purging behaviors, such as self-induced vomiting or excessive exercise, for the past two years. She has been feeling ashamed and guilty about her binge eating and purging behaviors and has been trying to hide them from others.
Emily has been feeling overwhelmed and hopeless and has been having thoughts of suicide. She has been experiencing physical symptoms, such as gastrointestinal distress, electrolyte imbalances, and dental problems, as a result of her binge eating and purging behaviors.
Case 2: A 22-year-old woman named Sarah has been experiencing an intense fear of gaining weight and a distorted body image for the past year. She has been restricting her food intake and has been engaging in excessive exercise to try to lose weight. Despite her efforts, she has been feeling unhappy with her body and has been continuing to restrict her food intake.
Sarah has lost a significant amount of weight and has been experiencing physical symptoms, such as fatigue, cold intolerance, and irregular menstrual cycles. She has been feeling overwhelmed and hopeless and has been having thoughts of suicide.
Case 1: Bulimia Nervosa
Case 2: Anorexia Nervosa
😵💫 Psychotic disorders
- Delusions 📷
- Hallucinations (primary= auditory, secondary = visual / olfactory[in tempor. lobe epilepsy])
- Disorganized though/speech (/behavior)
Types of delusions:
- persecutory
- Most common form of delusional disorder
- Belief of being followed, spied on, poisoned or drugged, harassed, or conspired against
- jealous
- Individuals with this subtype exhibit a persistent delusional belief that their spouses or partners are being unfaithful. This delusion is often based on misinterpreted and insignificant pieces of evidence, which are used to justify the belief.
- This subtype of delusional disorder can be difficult to treat and may only show improvement in cases of separation, divorce, or the death of the suspected partner.
- egomaniac
- Delusions of being loved by another
- More common in women, but can affect men as well
- Belief that a perceived suitor, often of higher social status, is in love with the individual
- Can become the central focus of the individual's life
- Onset can be sudden
- somatic
- Delusional disorder with somatic delusions is known as monosymptomatic hypochondriacal psychosis.
- This disorder is characterized by a greater degree of impairment in reality compared to other conditions with hypochondriacal symptoms.
- The terminology used is essential to understand for the exam.
- others
- Delusions of Infestations
- Delusions of Dysmorphophobia
- Delusions of Foul Body Odors or Halitosis
M > F
Positive Symptoms | Delusions, Hallucinations |
Negative Symptoms | Flat affect, Avolition, Anhedonia, Social withdrawal |
Disorganization | Formal thought disturbances, Bizarre behavior |
Affective Symptoms | Dysphoria, Affective inversion, Paradoxical affectivity, Ambivalence |
Cognitive Symptoms | Memory disturbances, Attention deficits, Planning and problem-solving difficulties |



- Catatonic type
- Disorganized type (worst Prognosis)
- Paranoid type 🥇 (most common, best Prognosis)
- Undifferentiated type
- Residual type
Negative symptoms often persist after Tx despite the resolution of positive symptoms.

Characteristics | TYPE 1 | TYPE 2 |
↑/↓ pre-dom. symptoms | ↑positive | ↓negative |
👨👩👧👧 Family history | + | Ø |
📉 prognosis + drug-response | better | worse |
⏰ symptom-onset | later, but acute | earlier |
👓 intellectual impairment | Ø | +/- |
🧠assoc. brain abnormality | ↑dopa | structural abnormalities |
- Premorbid
- Prodromal
- Syndromal
- Chronic / Residual
- 🗣️Psycho-Tx →Øin acute setting
- individual
- CBT + cognitive remediation
- FAMILY therapy
- 🗣️Psycho-social rehab
- ECT (if tx-resistent)

Anti-psychotic (FGA or SGA) ⇒ Ø#1 → choice of drug depends on TOLERABILITY + TARGET SYMPTOMS + PRIOR AP-USE (1st+2nd gen = comparable efficacy)

⇒ use any (except clozapin → only if resistent)
→ often Haloperidol or Olanzapine IM
Besides Clozapine, ECT can also be used if Tx resistent
same drug + dose for next 6 month
Duration of the treatment
- First-episode schizophrenia: 1–2 years of antipsychotic treatment
- Second episode: 2-5 years of treatment
- Multiple-episode schizophrenia patients-undefinite/lifetime
👹 Personality disorders
Personality Traits Fixed patterns of behavior Way of interacting with environment (+socializing) No significant distress or impaired function Positive traits: kind, confident Negative traits: lazy, rude Person often aware of own traits
Personality Disorders Fixed patterns of behavior Way of interacting with environment (+socializing) Cause distress or impaired function Person often unaware All treated with psychotherapy Difficult to treat ("enduring") Often strains doctor-patient relationship
- Cluster A (Weird)
- types: Paranoid, schizoid, schizotypal
- Odd and eccentric behavior
- ⇒ associated with SCHIZOPHRENIA
- Cluster B (Wild)
- types: Antisocial, borderline, histrionic, narcissistic
- Dramatic, erratic behavior
- ⇒ assoc. with MOOD DISORDERS & SUBSTANCE ABUSE
- Cluster C (Worried)
- types: Avoidant, obsessive-compulsive, dependent
- Anxious, fearful behavior
- ⇒ assoc. with ANXIETY DISORDERS
Personality Disorder | 👀 PARANOID | 🧘🏽 SCHIZOID | 🔮 SCHIZO-TYPAL |
Mnemonic | “Accusatory” | “Alone” | “Awkward” |
Hallmark | DISTRUST of others | CHOOSES social isolation | ODD + MAGICAL beliefs |
Other features | - guarded
- suspicious / ↑ vigilance
- cynical world-view | - does Ø enjoy close relationships or sex
- ↓/Ø hobbies
- detachment + flat affect
| - social anxiety → ↓friends
- superstitious (telepathy + sixth sense)
- IDEAS OF REFERENCE (events have “special meaning”)
- interpersonal awkwardness |
Ego defense | Projection
Attributing unacceptable thoughts to others ⇒ Often accuses others of being suspicious | ||
DDx | 😵💫 (Psychotic) Persecutory Delusion
→ more “absurd” belief that somebody is after you” despite contrary evidence | 🙅🏽♂️ Avoidant PD
→ CHOOSES (DOES Ø WANT) vs. WANTS but CAN’T
(also DDx with 🔮Schizo-typal) | 😵💫 Psychotic (Delusion)
→ shizo-typal: open to challenge beliefs; Øhallucination, Ø cognitive impairment |
Key differences: Schizoid vs Schizotypal vs Schizophrenia
- Thought Form:
- Schizoid: Organized thoughts.
- Schizotypal: Thoughts are organized but can be vague and circumstantial.
- Schizophrenia: Disorganized thinking pattern, often tangent, with loosening of associations.
- Thought Content:
- Schizoid: No evidence of psychosis.
- Schizotypal: While no psychosis, there may be ideas of reference, paranoid ideation, odd beliefs, and magical thinking.
- Schizophrenia: Characterized by psychosis and hallucinations.
- Relationships:
- Schizoid: Prefers solitude, lacking the desire for social relationships.
- Schizotypal: Has an interest in relationships but struggles socially, lacking close ties.
- Schizophrenia: Socially marginalized, not by choice, but due to symptoms.
Personality Disorder | 😈 Anti-social | 🔪 Borderline | 💃🏽 Histrionic | 🪞 Narcissistic |
Mnemonic | “Bad”; Antisocial = sociopath | “Borderline” | “FaBulous” | “Best” |
Gender dominant | M>F | F>M | ||
Hallmark | disregards RIGHTS of OTHERS | UNSTABLE MOOD & RELATIONSHIPS | ATTENTION seeking | INFLATED sense of SELF |
Ego defense | Splitting (all good or bad) * | |||
Other features | - CRIMINALITY
- IMPULSIVE, manipulative + Ø remorse
- must be >18y w/ CONDUCT DISORDER onset before 15y | - Fear of ABANDONMENT
- “emotional EMPTINESS”
- Impulsivity (Spending sprees, sex with strangers)
⇒ Self-mutilation
⇒ SUICIDE (gestures or attempts: Relates to fear of abandonment
→ "You don't care about me, so I'll kill myself”) | - wants to be CENTER OF ATTENTION (Talks loudly, tells wild stories, uses hand gestures)
- inapropriate sexually provocative behavior
- very concerned with PHYSICAL APPEARANCE (Exotic outfits, shoes, hats) | - grandiosity + sense of entitlement
- Ø EMPATHY
- needs ADMIRATION
⇒ CRITICISM ⇒ RAGE/DEFENSIVENESS
|
DDx | Conduct Disorder
→ if <18y = conduct d. | 🎭 Bipolar
→ Bipolar: mood changes over longer periodes (vs. quicker fluctuations in mood sometimes hours) | 😵💫 (Psychotic) Grandiosity Delusion |
Splitting = people either all good or all bad (black&white thinking)
Personality Disorder | 🙅🏽♂️ Avoidant | 🎛️ Obsessive-Compulsive | 👫 Dependant |
Mnemonic | "Cowardly” | “Compulsive” | “Clingy” |
Hallmark | social isolation due to feelings of “INADEQUACY” | PERFECTIONISM, ORDER & CONTROL (Loves "To Do" lists, Always needs a plan) | DEPEND on OTHERS |
Other features | - “social inhibition”
- afraid people dont like them / embarrasment → struggle relationships | → INFLEXIBLE at work/relationship
- EGO-SYNTONIC (behavior → goals)
ØIntrusive thoughts
Øcompulsions (repetitive behavior) | - ↓self-confidence + struggle self-care
- cant make decision on their on, “no opinion”, “you decide”
→ ABUSIVE relationships |
DDx | 🧘🏽 Schizoid PD
→ avoidant = WANT to socialize but CAN’T!
😱Social anxiety (no feelings of inadequacy, no persistent fixed pattern but only 6m needed; to DDx trials for social anxiety tx and see if it gets away→ if not: avoidant PD | OCD *
→ OCD = ego-dystonic + intrusive thoughts + repetitive behaviors
(OCPD = ego-syntonic, Øintrusive th. + Ørepetitive behaviors |
- Ego-Syntonic or Ego-Dystonic:
- OCPD (Ego-syntonic): Behavior and feelings aligned with one's self-image.
- OCD (Ego-dystonic): Behavior and feelings in conflict with one's self-image.
- Thought Content:
- OCPD: Obsessional thinking, no compulsions, strict routine and rigidity in day-to-day matters, more perfectionistic and rigid.
- OCD: Obsessions and compulsions, rituals, anxiety provoking unwanted intrusive thoughts.
🕳️ Dissociative Disorder
- Detachment from reality
- Feeling "like I was outside my own body"
- Extreme cases: becoming another person
- New name, age, job, etc.
- Often associated with psychological trauma
- May allow victim to cope with trauma
- Tx for all =Psychotherapy

🍺 Alcohol & Substance abuse
Defined by a maladaptive patterns:
- Tolerance: Building resistance to substance.
- Withdrawal: Negative effects when not using.
- Cravings: Strong desires for the substance.
- Overuse: Consuming more than intended.
- Desire vs. Inability: Wanting to reduce but failing.
- Time: Large amount of time spent acquiring or using.
- Functioning: Reduced capabilities at work/home.
- Conflicts: Strains in relationships due to use.
- Activities: Reduction in hobbies/leisure activities.
- Danger: Usage in hazardous situations.
- Awareness & Continuation: Use despite recognizing harm.
Dgx: ≥2 of the criteria should have been met in the past year.
- Pre-contemplation: denying of the problem
- Contemplation: acknowledging the problem but still not willing to make change
- Preparation/determination: preparing to change behavior
- Action/willpower: changing behavior
- Maintenance: maintaining changed behavior
- Relapse:(if applicable) returning to old behaviors and abandoning changes → back to pre-contemplation
Calculation for this statement 🤡
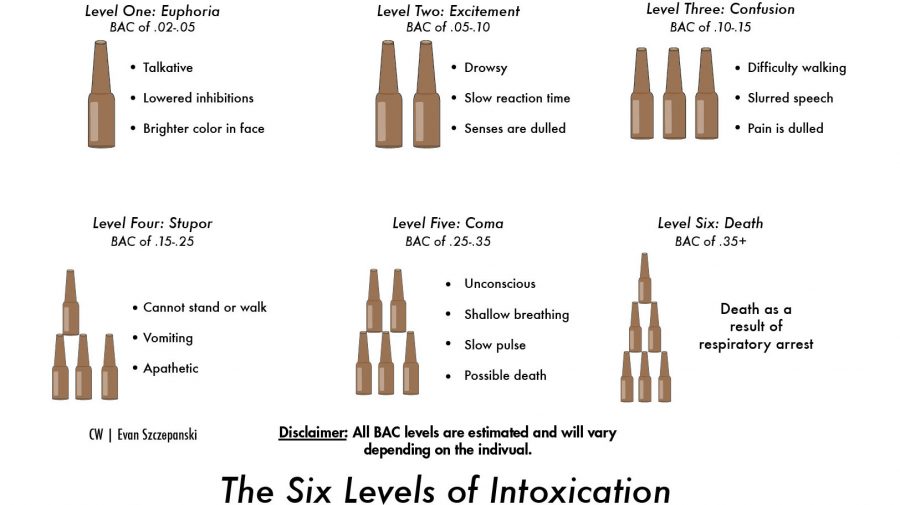
The Six Levels of Intoxication (Based on Beerpong)
1x Beerpong game is 10 Cups
Two Teams
Each Team 2 x 0,33 Liter beer
Each player 1x Beer
Result: Max 3 rounds of beerpong in a row pls!
1 Bottle beer = 0,33 Liter BAC = 0.2-0.5 1 Game = Euphoria
2 Bottle beer = 0,66 Liter. BAC = 0.5-1 2 Games= Excitement
3 Bottle beer = 0,99 Liter BAC = 1- 1.5 3 Games = Confusion
4 Bottle beer = 1,32 Liter BAC = 1.5-2.5 4 Games = Stupor
5 Bottle beer = 1,65 Liter BAC = 2.5-3.5 5 Games = Coma
6 Bottle beer =1,98 Liter BAC = > 3.5-3.5 6 Games = Death

- CNS depressant
- Slurred speech
- Incoordination
- Unsteady gait
- Stupor
- Coma
C2(alcohol/ethanol)-poisoning = ↑↑ blood alcohol conc. (very high) ⇒ 🫁respiratory depression → can be fatal ☠️
ethanol = 2 carbon 📷

- 🍌 Banana-Bag (thiamine (B1), folate (B9), Mg)
- 💦 IV FLUIDS (gluc5%, Ringer, saline)
- 😴 BENZOS
- +- Carbamazepin (seizures)
- +- Antipsychotics (only if HALLUCINATION/sev. AGITATION) - ⚠️ ⇒ ⚡ (↓ seizures-threshhold)
(Wernicke precipitated by Gluc without Thiamine)



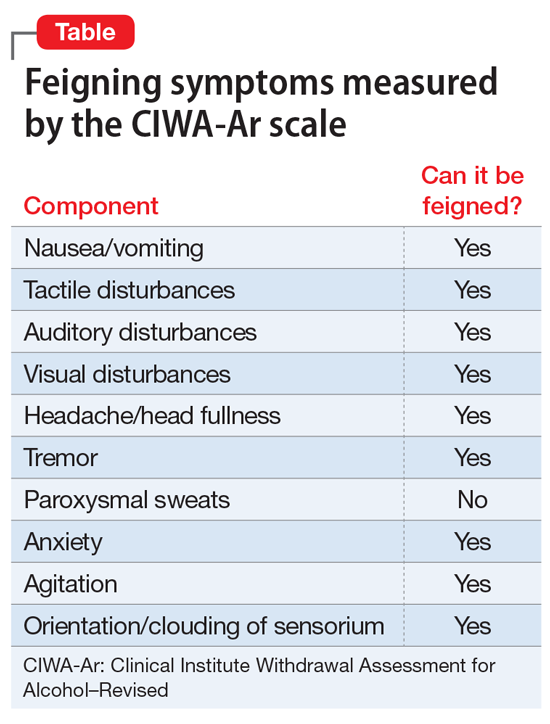
CIWA: 📷
- AST* + GGT (return to normal after abstinence: AST = 7days, GGT = 2-6weeks)
- ↑MCV
- Hypertension (Tx resistent)
*AST>ALT
- 1. 👭 ↓ FUNCTIONING

- Gastrointestinal Manifestations:
- Gastritis
- Hepatitis
- Cirrhosis
- Pancreatitis
- Cardiac Abnormalities:
- Dilated Cardiomyopathy
- Refractory Hypertension
- Types of Malignancies:
- Esophageal Cancers
- Oropharyngeal Cancers
- Wernicke Korsakoff
- Wernicke = encephalopathy (acute)
- Korsakoff = neurological damage (chronic)
- Associated with Thiamine (B1) deficiency + alcohol use ⇒ Atrophy of mamillary bodies + damage to thalamus
- Clinic:
- Wernicke:
- visual / nystagmus
- confusion
- ataxia
- REVERSIBLE (thiamine)
- Korsakoff Amnesia
- RECENT memory esp effected (memory more in the past less effected) + ANTEROGRADE: New memories can Ø be formed
- CONFABULATION (unable to remember → make things up)
- APATHY: ØInterest/concern
- PERMANENT (irreversible)
Korsakoff syndrome is a late development in patients with persistent vitamin B1 deficiency. It is most often seen in thiamine deficiency due to chronic heavy alcohol use.
- Confabulation: Patients produce fabricated memories to fill in lapses of memory.
- Anterograde and retrograde amnesia (anterograde is more common than retrograde)
- Personality changes (in frontal lobe lesions): apathy, indifference, decrease in executive function
- Disorientation to time, place, and person
- Hallucinations
Wernicke's COAT: Confusion, Oculomotor dysfunction, Ataxia, and Thiamine administration (see Treatment section)Korsakoff's CART: Confabulation, Anterograde and Retrograde amnesia, and altered Temper
Although often grouped together as a single syndrome (Wernicke-Korsakoff syndrome), the two conditions are distinct entities with different presentations, and, while both are due to severe chronic thiamine deficiency, Wernicke encephalopathy is reversible whereas Korsakoff syndrome is not.
- 🎭 mood d.
- 😱 anxiety d.
- 😵💫 psychotic d.
- 🍆 sexual dysf.
- 👵🏽 perisisten amnesic disorder (Wernicke-Korsakoff)
- 🗣️ Support groups, CBT, Family tx
- Relapse reducing drugs
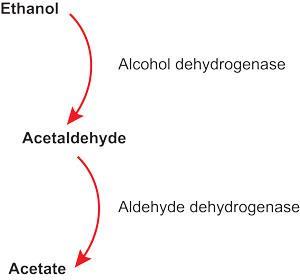
- 🥚🥚🇮🇷 disulfiram (antabuse)
- 👕 Naltrexone + Nalmefene
- ⛺ 🌹 🍽️ Acamprosate
- 🚗 Carbamazepin
- Baclofen
Inhibition Aldehyde dehydrogenase 📷→ ↑Acetaldehyde → Catecholamine release → Sweating + flushing + palpation

Naltrexone: Long acting OPIOID AGONIST → ↑ effects of alcohol
⇒ administered to PREVENT RELAPSES (p.o.)
Nalmefene: Unlike naltrexone, nalmefene is not only antagonist at the mu- and delta-opioid receptors but a partial agonist at the kappa opioid receptor. The function of the kappa receptor is not entirely clear, but it may be relevant to the motivational aspects of alcoholism. Nalmefene is useful in the reduction in both heavydrinking days and total alcohol consumption.
mechnism Ø fully understood → Modulates NMDA receptors affected by alcohol
SE: diarrhea

Other Screening Tools: AUDIT + MAST
- A 54-year-old woman with a history of alcohol abuse has been drinking heavily for the past 10 years. She reports experiencing tremors, anxiety, sweating, and insomnia since she stopped drinking two days ago.
- A 35-year-old man has been drinking heavily for the past 5 years. He reports drinking every day, often starting in the morning and continuing until he passes out at night. He has lost interest in hobbies and has strained relationships with friends and family due to his alcohol use.
- A 42-year-old man presents to the emergency department with confusion, slurred speech, unsteady gait, and nystagmus. His breath smells of alcohol, and his blood alcohol level is found to be 250 mg/dL.
1 → withdrawal
2 → use disorder
3 → intox
1) ⬇️ Depressants
- 🍺 Alcohol
- 🌈 Opioids → opioid R (mu, kappa and delta)→ drug of abuse = heroin
2) ⬆️ Stimulants

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
3) 🖼️ ”Hallucinogens”
- 🥦 Cannabis → canabinoid R
- 🍄 Lysernig acid diethylamine (LSD) + Psilocybin, others
- 🥰 MDMA (Ectasy) → ↑serotonin (↑release + ↓reuptake)
- Phencyclidine (Angel dust)


INTOXICATION
DRUG | EYES | MAIN ABUSE EFFECT | CLINIC | TX |
DEPRESSANTS: | ||||
🌈 Opiods | 👁️ 🤏🏽 “PIN-POINT” (bc depressant)
→ if severe intox → dilation | 😁 EUPHORIA
+
ANALGESIA
| ⬇️ DEPRESSANT effects:
◦ 🫁 respiratory → ↓RR
◦ 🧠 CNS → 😴 sedation(or euphoric) , 👅 slurred speech +
⚡seizures
◦ 🧣 Gag- + cough-reflex + ↓secretion (mouth, nose)
◦ 🍤 GI → 🤢 n/v, 🪠 constipation → ↓bowel sounds
◦💪🏽 : 🥵 flushed + warm | 👕 Naloxone or Nalmefene
⇒ 👁️ pupils + 🫁 RR should react promptly
(⚠️ may cause withdrawal if too ↑ dose)
naloxon = short acting antagonist, multiple doses might be needed
naltrexon = long action, sometimes given to prevent relapse
Nalmefene = long acting, can be given intox as a single dose |
STIMULANTS: | ||||
❄️ Cocaine | 👁️ 👌🏽 DILATED | 😁 EUPHORIA
+
ANALGESIA | ⬆️ STIMULANT effects:
- 🔋 ↑alertness + wakeful, insomnia (↓sleep-need)
⇒ “BAD TRIP”
→ 🖼️ Hallucinations(tactile - "Bugs crawling on my skin”),
→ paranoia, agitation
🆙 AUTONOMIC↑
- ❤️ ↑BP, ↑HR → ⚠️ Angina* → ☠️
- 🤒 fever (↑muscle activ. + ↑central DOPA)⇒ ⚠️⚡ seizures + 💪🏽Rhabdomyolysis
- ↓ 🍔 Appetite | 😱 Benzos,
😵💫#2Anti-psychotics
🎹 Labetalol (if❤️)
mixed alpha-beta blocker
(pure beta blocker is controversial)
context: theory
⇒ cocain acts as alpha + beta agonist (↑HR + ↑ BP)
→ if only beta-blockade (beta 2 usually cause vasodilation) ⇒ un-opposed alpha action ⇒ further vasoconstriction ⇒ myocardial ischemia |
🦷Amphetamines | 👁️ 👌🏽 DILATED | 😁 EUPHORIA
Øanalgesic
| SAME AS COCAINE:
⬆️ STIMULANT effects:
- 🔋↑alertness + wakeful,
⇒ “BAD TRIP”
→ 🖼️ Hallucinations(tactile),
→ AGITATION, paranoia
🆙 AUTONOMIC↑
- ❤️ ↑BP, ↑HR → ⚠️ Angina → ☠️
- 🤒 fever ⇒ ⇒ ⚠️⚡ seizures + 💪🏽Rhabdomyolysis
- ↓ 🍔 Appetite
- 🦷 fractures teeth + skin excoriation(meth)
| 😱 Benzos
😵💫#2Anti-psychotics |
HALLUCINOGENS: | ||||
🥦 MARIJUANA | 👁️ 🍎 red conjuctiva (+-dilated) | 😁 EUPHORIA
(+mild analgesia, antiemetic) | 🖼️ ↓:
⇒ paranoid delusion, “slowed” time, ↑sensation, hallucinations (rarely),
- anxiety, de-personalization/-realization, tachycardia
→ 🛋️ social withdrawal
- 👄 DRY MOUTH + 🍔 ↑APPETITE
| supportative (fluid+ elect) |
🍄 LSD + Psilocybin | 👁️ 👌🏽 DILATED | 😁 EUPHORIA
Ø analgesic | 🖼️↑↑= “TRIP” :
⇒ 🖼️ hallucinations/illusions
⇒ ⭕ expanded conciousess
⇒ 👂🏽 Synesthesia (a blending of the senses -
"Hearing" colors or 'seeing" sounds)
⇒ 👻 Depersonalization/derealization
⇒ “BAD TRIP” ⇒ ⇒ anxiety, paranoia, psychosis
⇒ ❤️ ↑autonomic (HR, sweating, burred vision)
⇒ 📸 Flashbacks after stopping drug (usually Ø disturbing) | supportative (fluid+electro)
😱 Benzos
😵💫Anti-psychotics |
🥰 MDMA | 👁️ 👌🏽 DILATED | 😁 EUPHORIA
Ø analgesic | 🖼️↓ :
⇒ distorted time + senses, hallucinations
⬆️ STIMULANT EFFECT:
- 🔋 Hyperactivity + Disinhibition, sexual desire
- ❤️ ↑BP, ↑HR
- 🤒 fever
🦷 bruxism (kiefern)
🧂 ↓Na (dilutional = due to ↑thrist + ↑ADH-secretion) ⇒ ⚡ seizures + ☠️
🍑 Heptotox
⇒ ⚠️ SEROTONIN-SYND.! | supportative |
Angina:

WITHDRAWAL
DRUG | KEYWORD | EYES | CLINIC | TX |
🌈 Opiods | ⇒ REVERSAL
| 👁️👌🏽 DILATED | → COWS scale*:
REVERSAL of EFFECTS:
- 🧠 restless, anxiety, “achy feeling”, ↑pain sensitivity
- 💦 ↑lacrimation + ↑rhinorrhea, sweating
- 🥱 yawning,
- 🍤 GI (nausea, 💩diarrhea, cramps)
- 💪🏽piloerrection
| 1)*OPIOID AGONIST
- 🪙 Methadone
- 🧒🏽 Buprenorphine(+naloxone)
2)*Clonidine (alpha 2 agonist) → sweating + GI
3) 😱 Benzos → anxiety + insomnia |
⬆️ Stimulants (🦷 + ❄️) | ⇒ ↓stimulation | - ⬇️ post-use “CRASH”
→ depression, lethargy, anxiety
- 🍔 ↑APPETITE
- 😴 insomnia, Sleep disturbance + 🎆 vivid nightmares
-(🐽 perforated nasal septum) | ||
🥦 MARIJUANA | - 🎭depression
- ⬆️ anxiety, irritability, insomnia
- 🍔 ↓APPETITE | - 😱 Anxiolytics
- ⚡ mood-stabilizer (valproate; gabapentin if dependence)
- 🥦 Dronabiol
(also used in:
→ chemo n/v
→ HIV (↑appetite)
→ Glaucoma | ||
Ø WITHDRAWAL FOR LSD | ||||
🥰 MDMA | ⬇️ post-use “CRASH” → depression, fatigue anxiety, ↓concentration
- 🍔 changes in appetite
- 🦷 jaw-soreness |
COWS = Clinically oriented withdrawal scale 📷 → mild vs mod vs sev. withdrawal:
{kind=link}
Methadone (oral)= Long acting opioid with ↓ abuse potention→ ↓Craving
Buprenorphine (sublingual) = long acting partial agonist (agonist + antagonist effect)
→ Combined with naloxone to prevent abuse
Clonidine → ↓sweating, cramps, diarrhea + n/v (Øeffect on other symptoms)

Q. Which statements are true for opiod withdrawal syndrome: A. The appropriate management ist with alpha 2 adrenergic agonists B. The appropriate management is with antipsychotics C. Characteristic symptoms are autonomic instability, insomnia, drug-craving D. The onset is 24-48h E. The duration is 5-10days
ACE
- A 32-year-old man presents to the emergency department with chest pain, dilated pupils, sweating, and agitation. He reports using cocaine earlier in the day.
- A 25-year-old woman reports feeling anxious, irritable, and experiencing muscle aches, runny nose, and watery eyes since she stopped using opioids two days ago.
- A 26-year-old man presents to the emergency department with confusion, paranoia, and visual hallucinations. He reports taking LSD earlier in the day.
- A 35-year-old woman reports feeling euphoric and having increased energy and talkativeness after using MDMA at a party.
- A 28-year-old man presents to the emergency department with chest pain and shortness of breath. He reports using marijuana earlier in the day.
- A 40-year-old man reports feeling irritable, restless, and experiencing insomnia since he stopped using cocaine two days ago.
- A 24-year-old woman presents to the emergency department with drowsiness and confusion. She reports taking opioids earlier in the day.
- A 30-year-old man reports feeling anxious and paranoid after using marijuana at a concert.
👵🏽 Disorders of consciousness, memory & cognition
- 👁️ ATTENTION + AWARENESS disturbance → distractibility → disorientation (time, place, rarely person)
- 🧠 COGNITION disturbance (memory, language, perception etc. → see dementia)
PLUS
⇒ develops RAPIDLY ⏱️
⇒ FLUCTUATE over a day
⇒ EVIDENCE for CAUSE (med. condition, intox/ withdrawal) ⇒ exclusion DDx (other neuro or psych causes)
OTHER FEATURES:
- 🎭 AFFECTIVE disturbances (anxiety, fear, depression, irritability, anger, euphoria, apathy)
- 😵💫 PSYCHOTIC-LIKE symptoms delusions, misinterpretations, illusions, and hallucinations (visual hallucinations are organic until proven otherwise)
- 🕺🏽 PSYCHO-MOTOR ACTIVITY disturb. groping/picking at clothes, attempts to get out of bed when unsafe, sudden movements, sluggishness, lethargy
- 😴 SLEEP/WAKE disturbance
{kind=link}
“I WATCH DEATH” ⇒ 📷
{kind=link}
Aspect | Psychosis | Delirium |
Type of Hallucinations | Auditory hallucinations that are structured and consistent | Visual or tactile hallucinations |
Onset | Gradual onset (unless substance induced) | Acute onset |
History of Psychosis | Personal or family history of psychosis | No previous history of psychosis |
Additional Factors | History of a prodrome (insidious functional decline) | Sleep/wake changes, More global cognitive impairment, Recent medical illness/medication changes |
Delirium
⏱️ acute
🤷🏽♂️ disorientation
〰️ fluctuation in symptoms
↓👁️ impared conscious
🔼 Transient sleep disturb
🔃 REVERSIBLE
Dementia
🕰️ chronic
disorientation = later
⚖️ stable symptoms
n 👁️ normal concsious
🔄 inversion sleep-wakeful rhythm
❌ PERMANENT
1) Treat UNDERLYING CONDITION
2)🥇 HALOPERIDOL
#2 atypical antipsychotics, Tiapride

Øbenzos → aggrevate confusion+cognitive funcction
A 75-year-old man is brought to the emergency room by his family after they noticed changes in his behavior. He has been confused, disoriented, and easily agitated over the past few days. Upon examination, the patient is found to have a fever and an elevated heart rate. He is also experiencing difficulty sleeping and has been seeing and hearing things that are not there. The emergency room physician suspects that the patient is experiencing delirium, a sudden and severe change in mental function that can be caused by a medical condition or medication use.
Further evaluation reveals that the patient has a urinary tract infection, which is causing the fever and delirium. He is started on antibiotics to treat the infection, as well as medications to manage his symptoms of confusion, agitation, and sleep disturbances. The patient's delirium improves over the next few days as the infection is treated and his body begins to recover. He is then transferred to a rehabilitation center for further treatment and recovery.


1)
Patient: Mr. John Doe, 68 years old Medical history: smoking, hypertension, stroke
Presenting complaint: Mr. Doe was brought to the clinic by his wife, who noticed that he was having difficulty with planning and organizing daily tasks, as well as with memory recall. He also showed signs of confusion and disorientation.
Examination: Upon evaluation, Mr. Doe was found to have trouble with coordination and balance, as well as difficulty with understanding spoken language and expressing his thoughts. Neurological examination revealed mild weakness in the right arm and leg, and imaging tests showed evidence of multiple small strokes.
2) Patient: Mrs. Jane Smith, 76 years old Medical history: hypertension, diabetes, mild cognitive impairment
Presenting complaint: Mrs. Smith was brought to the clinic by her daughter, who noticed her memory loss and confusion. The patient was also having trouble performing daily activities such as cooking and taking care of herself.
Examination: Upon evaluation, Mrs. Smith was disoriented to time and place. She had difficulty recalling recent events and recognizing familiar faces. She also showed signs of forgetfulness, repeating the same questions multiple times. Neurological examination revealed mild difficulty with coordination and imbalance.
1) vascular dementia
2) alzheimer
🐣 Pediatric psychiatry
❓ unknown, multifactoral → neurodevelopmental disorder
M>F
Assoc. with:
- 🕯️ TORCH infections
- ⚡ Epilepsy
- 🧬 GENETIC SYNDROMES:
- Fragile X sy
- Down’s sy
- Rett’s sy
- 👶🏽 ↑ head-circumference


- others
- Phenylketonuria (PKU)
- Histidinemia
- Creatine Deficiency
- Metabolic Purine Disorder
- Mitochondrial Disorders
- Storage Diseases (Ceroid, Polysaccharides)
- Fragile X
- Down Syndrome
- Turner Syndrome
- Angelman Syndrome
- Prader Willi
- Neurofibromatosis
- Tuber Sclerosis
- Soto Syndrome
- William's Syndrome
- Congenital Rubella
- Infantile Spasms
- Lennox Gastaut
- Landau-Kleffner
1) 💬 SOCIAL-COMMUNICATION DEFICITS in MULTIPLE SETTINGS
- 🗣️ Social-emotional RECIPROCITY
- Failure of back-and-forth conversation
- Reduced sharing of interests, emotions
- 👀 NON-VERBAL
- Abnormal eye contact or body language
- 👬 RELATIONSHIPS
- Difficulty making friends
- Lack of interest in peers
2) 🔁 RESTRICTED, REPETITIVE patterns
- 🔄 ROUTINES
- Insistence on sameness,
- unwavering adherence to routines
- inflexible
- 🔎 INTEREST
- Preoccupation with certain objects, interests
- 👋🏽 MOVEMENTS / SPEECH
- Repetitive movements, use of objects
- phrases, echolalia
- 🔇 SENSORY
- ↑/↓ reactivity to sensory input
- Indifference to pain/temperature
- Adverse response to specific sounds or textures
- unusual interest in sensory aspects of environment
- Excessive smelling or touching of objects
- Visual fascination with lights or movement
3) onset during EARLY developmental period, 4) IMPAIRED FUNCTIONING 5) exlude DDX → intellectual disability or global develop. delay, ODD
+/- 🧠 ↓INTELLECTUAL ABILITY
Some skills weak (i.e. verbal communication, reasoning)
⇒ Do Ø REACH MILESTONES

+/- 🏝️ ↑ABILITY IN SPECIFIC SKILLS = SAVANTS
Some patients have special skills in one area Memory, music, art, math Classic example: determining day of week for given date
- 🕺🏽 Early behavioral / educational intervention
- 💊 SYMPTOMATIC drugs
- 😵💫 Atypical Antipsychotics ⇒🍓 RISPERIDONE,🤫 ARIPRIPRAZOL
- ❄️ Stimulants (if ADHD features)
- 🙂 SSRIs (if anxiety, OC-features)
- 💤 Melatonin (if insomnia)
- ⚡ anti-epileptics (if seizure)


Alice is a 6-year-old girl. She was diagnosed with ASD at age 4 after her parents noticed that she was having difficulty developing language skills and engaging in social interactions. She has difficulty with social communication and impaired social interaction. She rarely makes eye contact and has difficulty engaging in back-and-forth conversations. She often appears distant and prefers to be alone. Alice tends to become overwhelmed and upset when faced with changes in her routine and has difficulty transitioning from one activity to another. She also has repetitive behaviors, such as hand-flapping, spinning, and rocking.
❓ unknown, multifactorial M>F
{kind=link}
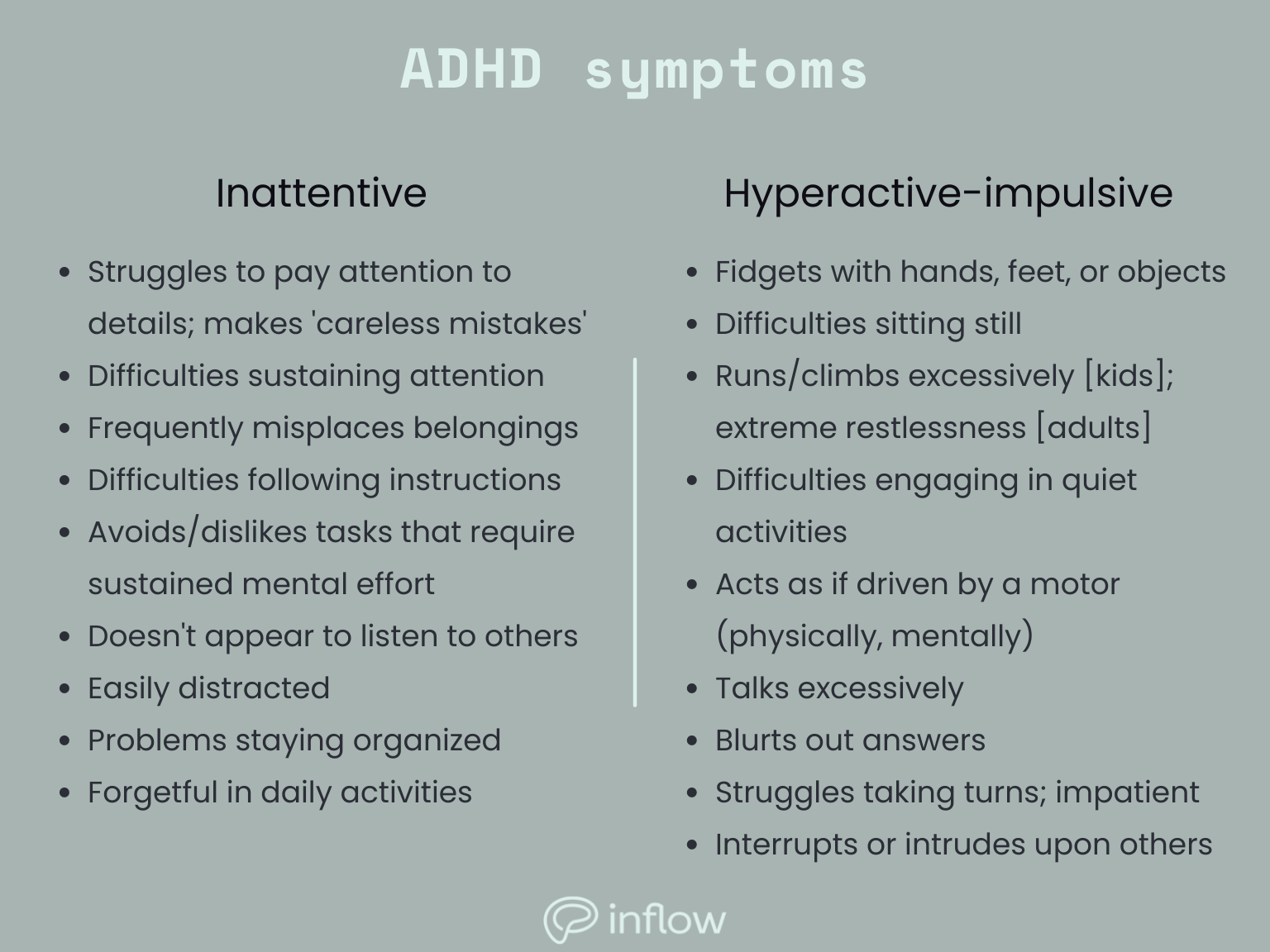
≥5/6 INATTENTIVE and/or HYPERACTIVE in MULTIPLE SETTINGS 📷
- Age <17 years: ≥6 symptoms in 1 or both categories
- Age >17 years: ≥5 symptoms in 1 or both categories
⇒ > 6 month ⇒ onset < 12y of age ⇒ IMPAIRED FUNCTIONING + exclude DDX ⚠️ compare attention to “DEVELOPMENTAL LEVEL” (differs)
- Pre-school: play < 3 mins, not listening, no sense of danger
- Primary school: activities < 10 mins, forgetful, distracted, restless, intrusive, disruptive
- Adolescence: attention < 30 mins, no focus/planning, fidgety, reckless
- Adult: incomplete details, restless, forgetful, impatient, accidents
#1 ❄️STIMULANTS = Methyphenidate (ritalin), Amphetamins (Adderall)
→ #2 NON-STIMULANTS: 🦬 Atomoxetine*, 2️⃣ Alpha2-Agonists* (Guanfacine, Clonidine) → ↓effectiveness, ↑SE, but ØABUSE
Atomoxetine:
- Selective norepinephrine re-uptake inhibitor
- Ø direct effects on dopamine systems in CNS
- May have ↓ insomnia & ↓ appetite
→ Normally Dopamine effects may cause euphoria → Less abuse potential
Alpha2-Agonist: ↓ norepinephrine release from synapse 📷 → Sedating and calming
{kind=link}

#2🕺🏽 Behavioral therapy
→ If Drug-refractory
→ #1 tx in younger children or milder cases
- ↓ 🍔 appetetite ⇒ ⚖️ weight loss
- 💤 Insomnia
- 🌈 ABUSE !
Jill is a 10-year-old female with Attention Deficit Hyperactivity Disorder (ADHD). She has had difficulty paying attention and staying on task since she was a young child (<12y). She often appears to be daydreaming and is easily distracted. She also has difficulty with organization and time management. She has a short attention span and often interrupts others when they are speaking. She often has difficulty following instructions and completing tasks. She has a history of impulsivity and often acts without thinking. Jill is currently receiving medication to help manage her symptoms and is also seeing a therapist to help her learn skills for managing her ADHD. She is also participating in a social skills group that focuses on teaching her how to interact appropriately with peers.
😈 ANTI-SOCIAL personality disorder

-RUNNING AWAY ”with limited prosocial emotions” if: - ØGUILT/REMORSE - ØCONCERN ABOUT CONSEQUENCES

🗣️ psychotherapy (CBT)
John is an 17-year-old male with conduct disorder. He has had difficulty following the rules at home and at school since he was a young child. He often gets into physical fights with peers and has been arrested multiple times for shoplifting and vandalism. He has a history of lying and stealing from family members and has struggled to maintain relationships with peers and adults. He often displays aggressive behavior and has difficulty controlling his temper. He has a history of substance abuse and has been in and out of treatment for his addiction. He has difficulty with empathy and remorse and often has difficulty understanding the consequences of his actions. John is receiving individual and family therapy, as well as medication to help manage his symptoms. He is also participating in a program that helps teach him skills for managing his emotions and behavior.
Enduring pattern of anger and irritability with argumentative, vindictive, and defiant behavior toward authority figures. Treatment: psychotherapy (eg, CBT).
>6m
Onset before age 10. Severe, recurrent temper outbursts out of proportion to situation. Child is constantly angry and irritable between outbursts. Treatment: CBT, stimulants, antipsychotics.
>1y
multifactoral
→ 🧠 NEURO DISORDER in children (↑DOPA in basal ganglia → impaired subcortical inhibition of movement)

Assoc. with ⇒ 🕺🏽 ADHD + OCD , (and anxiety, depression)

💃🏽 MOTOR
Sudden, quick movements Eye blink Head jerk Grimace
🗣️ SPEECH
Sudden, quick speech, usually few words Coprolalia: obscene language
- 🕺🏽 Behavioral therapy
- 💊 Drugs ⇒ only if ↓FUNCTIONING or DISCOMFORT
- 😵💫 Anti-psychotics (Haloperidol or Risperidone) ⇒ SE: tardive diskinesia
- 4️⃣:⭐ Tetrabenazine (benzamides - sulpide,tiapride) (”dopamine depletion”)⇒ Øtardive diskinesia
- 2️⃣ Alpha2-Agonists (see ADHD)

James is a 16-year-old male with Tourette Syndrome. He has had motor and vocal tics since he was a young child. His tics include shoulder shrugging, blinking, and grunting. He also has difficulty controlling his speech and often blurts out inappropriate words or phrases. He is often embarrassed by his tics and has difficulty managing his anxiety. He has difficulty concentrating and often fidgets when trying to complete tasks. He has a history of struggling in school due to his tics and difficulty with concentration. He is currently receiving medication to help manage his symptoms and is also seeing a therapist to help him learn coping strategies for managing his tics and anxiety. He is also participating in a social skills group that focuses on teaching him how to interact appropriately with peers.
Onset before age 5.
Anxiety disorder lasting ≥ 1 month
involving refraining from speech in certain situations despite speaking in other, usually more comfortable situations.
Development (eg, speech and language) not typically impaired.
Interferes with social, academic, and occupational tasks.
Commonly coexists with social anxiety disorder.
Treatment: behavioral, family, and play therapy; SSRIs.
Overwhelming fear of separation from home or attachment figure lasting ≥ 4 weeks(1m). (Can be normal behavior up to age 3–4.) → May lead to factitious physical complaints to avoid school.
Treatment: CBT, play therapy, family therapy.
Global cognitive deficits (vs specific learning disorder) that affect reasoning, memory, abstract thinking, judgment, language, learning.
→ Adaptive functioning is impaired, leading to major difficulties with education, employment, communication, socialization, independence.
Treatment: psychotherapy, occupational therapy, special education.
Onset during school-age years.
Inability to acquire or use information from a specific subject (eg, math, reading, writing) near age-expected proficiency for ≥ 6 months despite focused intervention.
General functioning and intelligence are normal (vs intellectual disability).
Treatment: academic support, counseling, extracurricular activities.