





Obstetrics & Neonatology
🤱🏼 Obstetrics
Q. Which of the following statements are true?
- A. Human placenta is a villous, chorionic type.
- B. Human placenta produces hormones (chorionic gonadotropin hormone (hCG), human placental lactogen hormone (hPL)).
- C. The origin of the placenta is exclusively maternal.
- D. The origin of the placenta is exclusively foetal.
- E. Placental formation ends at the beginning of the second trimester.
Note: Period of placental formation – day 13 - end of 4th month.
18. * Where does the fecundation take place?
- A. It starts in the ovary with the release of the egg and ends inside the uterus.
- B. It takes place in the terminal third of the fallopian tube.
- C. It starts in the fallopian tube and ends inside the uterus.
- D. It takes place inside the uterus.
- E. None of the above are true.
- Gravida: total count of pregnancies
- Nulliparous: a woman who was never pregnant
- Multiparous: has been pregnant more than a single time
- Para: count of “completed” pregnancies (lasting 20 weeks or more)
- Ex. G2P1 (2 times pregnant, 1 delivery + 1 not-delivered (yet))
- GA: Weeks since last menstrual period (Conception = 2 after last period)
- Embyronic Age: conception at day 0

Classification ⇒ 📷
EDD = last menstruation + 10 days - 3 month (or + 9 month)
Example: LMP = July 10, 2023 + 10 days + 9 months = probable date of birth: April 16, 2024.

1st T: 1-12w
2nd T: 13-27w
3rd T: 28w-birth
Q. Which of the signs listed below enable an accurate diagnosis of pregnancy in the second trimester?
A. Increased volume of the uterus
B. Objectifying perception and active fetal movements
C. Palpation of fetal parts
D. Softening of the cervix
E. Listening of the fetal heart using cardiotocography
Q. Which of the signs listed below enable an accurate diagnosis of pregnancy in the second trimester?
A. Increased volume of the uterus
B. Objectifying perception and active fetal movements
C. Palpation of fetal parts
D. Softening of the cervix
E. Listening of the fetal heart using cardiotocography
1st TRIMESTER:
2nd+3rd TRIMESTER:
BIOMETRIC MARKERS (via US)→ estimate fetal weights
- Biparietal diameter (BPD) 📷
- Head circumference
- abdominal circumference
- femur lenght
⇒ freq. used for growth assessment (compared to 1st T dating)
FUNDAL HEIGHT ⇒ 📷
- 14 weeks: Uterus above pubic symphysis.
- 16 weeks: Uterus between pubic bone and belly button.
- 22-24 weeks: Uterus around umbilicus.
- 32 weeks: Uterus middle between umbilicus and xiphoid.
- 40 weeks: Uterus 3-4 finger sides below xiphoid appendix, umbilical scar may fade.
What are the changes in the organ systems?

Late → SUPINE Hypotension baby compresses of IVC → ↓Preload ⇒ ↓Output
Q. Which of the following statements are false regarding the changes at the level of the cardiovascular system during pregnancy?
A. Cardiac output gradually declines.
B. Cardiac output rise.
C. Increasing volume expansion.
D. Decreased volume expansion.
E. Ejection decreases after 30 SA.
Which of the following statements are false regarding the changes at the level of the cardiovascular system during pregnancy?
A. Cardiac output gradually declines.
B. Cardiac output rise.
C. Increasing volume expansion.
D. Decreased volume expansion.
E. Ejection decreases after 30 SA.
Minute ventilation increases = TV x RR
- More CO2 to exhale → ↑tidal volume → ↓CO2 → respir. alkalosis
- Renal compensation (↓ HCO3) →Normal / slightly ↑ pH
- VOLUME: blood from maternal circulation → placenta → ↑renin (mother) → retention
- ↑GFR → ↑renal blood flow → ↓BUN + crea
Q. Which of the hematological modifications listed below are found in a normal pregnancy?
A. Decreased leukocytes B. Increased number of leukocytes C. Hypercoagulability D. Normocoagulabilitity E. Hemodilution with decreased red blood cell count
Q. Which of the hematological modifications listed below are found in a normal pregnancy?
A. Decreased leukocytes B. Increased number of leukocytes C. Hypercoagulability D. Normocoagulabilitity E. Hemodilution with decreased red blood cell count

hCG(alpha unit) → stimulated TSH-Receptor → ↑ FREE T4 + ↓TSH

⇒ 📷
- Rise in TBG (due to estrogen)
- Rise in total thyroid hormone levels
- hCG stimulates thyroid (same alpha unit as TSH)
- ↑ free T4 → ↓ TSH
Generally safe
Contraindicated only in certain patients:
- Cervical insufficiency
- Placenta previa
- Hypertension in pregnancy
- Multiple gestation
- ↑ weight gain assoc. with:
- macrosomnia + C-section
- Gestational Hypertension
- Gestational diabetes
- ↓ weight gain assoc. with:
- ↓birth weight
- preterm
- Metabolism and Emotional Effects:
- Altered metabolism of catecholamines, steroid hormones, and the endorphin system can lead to:
- Sleep disturbances
- Fatigue
- Emotional lability
- Character disorders
- Postpartum Depression:
- Potential risk of occurrence
- First Trimester Symptoms:
- Central origin of morning sickness and vomiting
- State of drowsiness
- Vagotonia in the neurovegetative system
- Second Trimester Mood:
- Possible states of good mood and euphoria
- Third Trimester Changes:
- Depressive manifestations
- Chronic fatigue
- Sympatotony in the neurovegetative system
- Parathyroid: Experiences hypertrophy leading to increased parathormone concentration, resulting in hypercalcemia. The placenta acts as a calcium pump.
- Adrenal Hormones: Maternal cortisol rises, impacting total and free calcium levels. Maternal total calcium decreases due to decreased albumin, but the proportion of free ionized active calcium remains constant due to Parathyroid Hormone (PTH).
- Vascular Changes: Vascularization increases substantially from the start of pregnancy, leading to hypertrophy.
- Gonadotropic Hormones: Serum levels, especially LH, decrease due to prolactin inhibition. Cyclic secretion ceases, leaving only continuous basal secretion.
- Prolactin: Serum levels increase progressively, losing pulsatile characteristics. Prepares the mammary gland and supports the yellow gestational body.
- TSH (Thyroid Stimulating Hormone): Levels do not rise during pregnancy.
- Growth Hormone (GH): Alongside hPL (human placental lactogen) and prolactin, it forms the lactogenic hormone complex.
- Melanocyte Stimulating Hormone (MSH): Secretion doesn't seem to be altered.
- Oxytocin: Plays an essential role in myometrial action during labor and supports uterine dynamics.
- Pancreas: Carbohydrate metabolism is influenced early on by increased estrogen and progesterone, leading to beta-pancreatic hyperplasia.
- Placenta: Functions as an endocrine gland, synthesizing hormones that reach both maternal and fetal circulation. Cytotrophoblast and Syncytiotrophoblast: Synthesize various neurohormones resembling hypothalamic and pituitary functions, releasing hormones like hG, HPL, TSH-like substances.
- Basal Metabolism: Increases by 10-20%, leading to decreased alkaline reserve and a propensity towards acidosis.
- Carbohydrate Metabolism: Influenced by hormones from the pancreas, adrenal, pituitary, and placenta, highlighting changes in carbohydrate metabolism. Glycemia generally remains within normal limits, necessitating an oral hyperglycemia test if blood sugar changes occur (hyperglycemia).
- Lipid Metabolism: Lipemia escalates due to increased HPL and chorionic GH, affecting lipid storage and lipolysis.
- Protein Metabolism: Essential for fetal growth and development, requiring a high-protein diet (1.5 g/kg/day). Total serum protein levels decrease to 55-60 g/l, impacting the albumin-globulin ratio.
- Water and Electrolyte Metabolism: Total water increases up to 7 liters during term pregnancy, mostly in extracellular water. Plasma volume rises until 7 months, followed by a decrease, causing reduced hematocrit. Water retention occurs during pregnancy, while Na, Cl, and K values remain unchanged.
- Phosphor-Calcium Metabolism: Calcium and phosphatemia decrease by 10%, causing an increase in calcium concentration and "physiological hyperparathyroidism."
- Magnesium Metabolism: Low serum Mg levels may contribute to miscarriage or preterm delivery.
- Iron Metabolism: Fetal reliance on maternal iron reserves increases iron needs in pregnant women. Hemoglobin decreases due to hemodilution; values below 11 g% indicate anemia during pregnancy.
- Gastroesophageal Reflux Disease (GERD): Attributed to heightened intra-abdominal pressure and progesterone's effects, including decreased sphincter tone and delayed gastric emptying.
- Increased Gallstones: Progesterone leads to heightened gallbladder stasis, causing a rise in gallstone occurrence.
- Constipation and Hemorrhoids: Progesterone contributes to decreased GI motility, resulting in constipation and the development of hemorrhoids.
- Gingival Hypertrophy and Pregnancy Gingivitis: Hormonal factors like estrogens cause edema and bleeding, while progesterone enlarges the periodontal space.
- Dental Cavities: Elevated calcium transfer from mother to fetus may lead to increased dental cavities.
34-37: twice a month
>37: weekly
Q. What is the correct rhythm of monitoring for a normal pregnancy?
A. Monthly between 20 to 32 weeks of gestation (SA) B. Bimonthly between 20 to 32 weeks of gestation (SA) C. Bimonthly between 34-37 weeks of gestation (SA) D. Weekly between 35-41 weeks of gestation (SA) E. Weekly after 37 weeks of gestation (SA)
- Establish baseline
- Exclude anemia
- Exclude iron deficiency & thalassemia(↓ MCV + normal iron)
(if pre-pregnant anemia: ↑severity of dilutional anemia during pregnancy)
⇒ Markers:
- RBC markers
- Hb + Hct
- MCV
- Plts

💪🏼 DOMINANT 📷

- Excessive bleeding between mother and fetus may necessitate an increased dosage of RhoGAM.
- Rosette Examination:
- Quantitative assessment
- If bleeding between mother and fetus is less than 2 ml -> Result is negative
- If bleeding is more than 2 ml -> Proceed to: Kleinhauer-Betke Evaluation
- Kleinhauer-Betke Evaluation:
- Assesses the ratio of fetal to maternal red blood cells present in the mother's bloodstream.
- If the ratio is significantly high, administer an extra dose of RhoGAM.
This method helps figure out how much baby's blood mixes with the mom's blood. Baby's blood and mom's blood react differently to acid. When we treat a blood sample with acid, mom's blood goes kinda invisible, but the baby's blood stays and turns a pinkish color. By looking under a microscope, we can count these pink cells and figure out the percentage of baby's blood in the mom's sample.

Ø Ab → prevention with RhoGAM +Ab → Is the baby Rh+? (Fater,baby testing) ⇒ confirmed if: Father homozygous 📷 or baby + Ab

*RhoGAM = 300 microg IM
- Serial Ab titers
- A positive titer (>1:16) for Rh antibodies indicates an elevated risk of fetal hemolytic anemia.
- A titer of ≥ 1/32 signifies isoimmunization,
- A titer > 1/64 suggests a heightened risk of fetal harm.
- A continual increase of titer in stady-state possibly leading to fetal harm.
- A sudden drastic decrease in the titer could indicate a very high transfer of antibodies into the fetal circulation, potentially resulting in fetal harm.
- Fetal trans-cranial MCA Doppler (↑flow = anemia) 📷
- Umbilical cord sampling → Fetal Hb/Hct 📷
⇒ if sev. anemia → fetal transfusion 📷 & early delivery (>35w)
HEMOLYSIS (↑bili + LDH) →Anemia → HYPOXIA
- 🫀 Heart failure (due to anemia) → Hydrops fetalis 📷 📷 (→ ↑uterus size)
- pleural, pericardial effusion
- ascitis + periph edema
- Compensatory: 🥮 Placentomegaly + 🍑 HSM (hepatosplenomegaly)
- 🚨 Fetal distress + Jaundice (hemolysis) → first 24h of life
- ↑MCA flow velocity = sev. ANEMIA

Severe cases of isoimmunization can lead to fetal hydrops, characterized by edema in at least two fetal compartments due to fetal heart failure secondary to anemia. Another potential consequence is erythroblastosis fetalis, which involves moderate to severe immune-mediated hemolytic anemia in the fetus.
🫀 Heart failure → fluid accumulation
- Pleural effusion
- Pericardial effusion
- Ascites
- Polyhydramnios
🍑 + 🥮 Compensatory
- Polyhydramnios
- Hepatosplenomegaly
- Increased placental size
👶🏽 Fetal distress
- Fetal heart rhythm disorders or the absence of FHR and fetal death
⇒ MCA Doppler to assess degree of fetal anemia
Q. Which of the following statements regarding isoimmunization are true?
A. Amniocentesis to a Rh-positive woman requires administration of anti Rh immunoglobulin.
B. Isoimmunization in a patient with decreasing antibody titer is a favorable prognostic factor.
C. In the situation of fetal Rh isoimmunization, it may occur with low serum proteins and clotting disorders.
D. In the situation of fetal Rh isoimmunization, it may cause hydrops and anasarca.
E. Isoimmunization prophylaxis involves administration of anti D immunoglobulin within 48 hours postpartum (? within 72h)
A. Amniocentesis to a Rh-positive woman requires administration of anti Rh immunoglobulin.
B. Isoimmunization in a patient with decreasing antibody titer is a favorable prognostic factor.
C. In the situation of fetal Rh isoimmunization, it may occur with low serum proteins and clotting disorders.
D. In the situation of fetal Rh isoimmunization, it may cause hydrops and anasarca.
E. Isoimmunization prophylaxis involves administration of anti D immunoglobulin within 48 hours postpartum (? within 72h)
Q. Choose the correct affirmations towards Rhesus incompatibility:
A. IgM cross the placenta and destroy the fetal erythrocytes.
B. The mild form of hemolytic disease represent half of the cases/involve anemia and hyperbilirubinemia.
C. Fetal hydrops does not appear when Hb is between 7 and 12 g/dl.
D. If the bilirubin level is more than 25 mg/dl, the term newborn is at risk for kernicterus.
E. No risk if there is, in the same time, ABO incompatibility, and neonatal.
A. IgM cross the placenta and destroy the fetal erythrocytes.
B. The mild form of hemolytic disease represent half of the cases/involve anemia and hyperbilirubinemia.
C. Fetal hydrops does not appear when Hb is between 7 and 12 g/dl.
D. If the bilirubin level is more than 25 mg/dl, the term newborn is at risk for kernicterus.
E. No risk if there is, in the same time, ABO incompatibility, and neonatal.
- 🥐 pyelonephritis
- ⏲️ premature birth (infection → premature rupture of membranes)
Q. Which statements are true about Asymptomatic bacteriuria?
A. Located in the lower urinary tract B. It doesn't influence the pregnancy C. Can induce adverse birth patterns, neonatal mortality, and morbidity D. The treatment isn't necessary in all cases E. Oral antibiotics are administered
A. Located in the lower urinary tract B. It doesn't influence the pregnancy C. Can induce adverse birth patterns, neonatal mortality, and morbidity D. The treatment isn't necessary in all cases E. Oral antibiotics are administered

- Rubella + Varicella
- HIV
- Syphilis
- Chlamydia + Gonorrhea
- HPV
- Hep B
- others depending on mother: TSH, HbA1c, genetic
Gestational Diabetes Testing:
- Screening: 50-gram one-hour glucose challenge test (GCT)
- Done between 24 to 28 weeks.
- Take a 50-gram sugar drink (no need to be on an empty stomach).
- Blood sugar is checked an hour later.
- If blood sugar is between 130 to 140 mg/dL or more (can change depending on the lab) -> go to the diagnostic test.
- Diagnostic test: 100-gram three-hour oral glucose tolerance test (GTT)
- Begin after fasting for 6 hours.
- Test blood sugar at the start, then after 1, 2, and 3 hours of drinking a 100-gram sugar drink.
- If two or more of these tests show high levels -> diagnosis of gestational diabetes.
↓
Evaluation Standards for 100g 3-hour Glucose Tolerance Test (GTT):
Measurement Time | Threshold (mg/dL) |
Before Eating | 95 |
After 1 hour | 180 |
After 2 hours | 155 |
After 3 hours | 140 |
Group B Strep (GBS) ⇒ rectovaginal cultures at 36-37 weeks
Down syndrome (trisomy 21) Edward syndrome (trisomy 18) Ptau syndrome (trisomy 13)
- Maternal 🩸 serum markers
- Alpha-fetoprotein (AFP)
- Varies with gestational age
- Measured as multiples of median (MoM)
- Reduced AFP (< 0.5 MoM)
- Possible chromosomal anomalies: Trisomy 21, Trisomy 18
- Fetal demise potential
- Incorrect gestational dating
- Increased AFP (> 2.5 MoM)
- Neural tube defects
- Abdominal wall defects (e.g., gastroschisis)
- Multiple gestations
- Gestational dating errors
- Free B-human chorionic gonadotrophin (free B-hCG)
- Unconjugated estriol
- Inhibin A
- Pregnancy-associated plasma protein-A (PAPP-A)
- Fetal 🦇 US findings ⇒ ↑ Nuchal translucency (+others*) 📷
- 🧬 Cell free DNA (”modern type”) ⇒ more expensive, but ↑Se+Sp
main causes for ↑ nuchal translucency: Turner sy, Trisomies (13,18,21), Skeletal dysplasia
Fetal cranicaudal lenght (CCL) 📷 : its the head-pelvis distance, which is a crucial parameter for assessing fetal development. In the majority of cases, fetuses with genetic disorders exhibit growth abnormalities. Severe conditions, such as Edwards syndrome (Trisomy 18) or Patau syndrome (Trisomy 13), often result in pronounced growth disorders.
Nasal bone:
The nasal bone, specifically the hard portion located at the root of the nose, is visualized through ultrasound as a white line immediately below the skin. Since no single ultrasound marker is pathognomonic for a chromosomal aberration, there has been a strategic introduction of combined tests in contemporary medical practice. These tests involve the integration of ultrasound markers and blood markers to enhance the diagnostic accuracy of such conditions

Cell-free DNA (cfDNA) consists of small DNA fragments that circulate freely in bodily fluids like blood, urine, and saliva. These fragments are released when cells die and break down. In pregnancy, a portion of cfDNA comes from the fetus and can be used for non-invasive prenatal testing (NIPT) to detect genetic conditions without invasive procedures.
⇒ Do Ø use: BEFORE 10w or in OBESE women ⇒ low fetal DNA in both
1st→ combined
2nd → quad + fully integrated

📖 Book:
- Double Test:
- Conducted between 11 and 14 weeks of gestation.
- Includes the assessment of nuchal translucency, CCL (crown-rump length), and nasal bone, along with the serum markers PAPPA and free beta hCG.
- Triple Test:
- Performed between 16 and 18 weeks of gestation.
- Involves measurements of fetal cranial circumference, biparietal diameter, abdominal circumference, and femoral length.
- Additionally, it assesses maternal serum markers, including alpha-fetoprotein (AFP), human chorionic gonadotropin (hCG), and free estriol fraction (uE3).
- 1st and 2nd Trimester Dry Test:
- Comprises two complex screening tests designed to evaluate the risk of having a child with chromosomal abnormalities and screen for carriers of genetic disorders.
- The 1st-trimester dry test is conducted between 11-13 weeks + 6 days of gestation.
- The 2nd-trimester dry test is performed between 14-20 weeks + 6 days of gestation.
- Both tests assess genetic conditions like cystic fibrosis and non-syndromic congenital deafness by analyzing maternal serum.
Procedure | Chorionic Villus Sampling (CVS) | Amniocentesis |
Sample | Obtains sample of the placenta | Obtains fetal cells in amniotic fluid |
Approach | Transabdominal or transcervical approaches (varies by operator preference and anatomy, transcervical = ↑abortion risk) | Transabdominal aspiration |
Timing | 10 - 13 weeks | 15 - 20 weeks* |
Risk of fetal loss | ~ 1:100
(higher risk) | 0.1% to 0.3% (~1:500) |
Sample quality | - | Sample should be clear,
⇒ green/brown fluid associated with adverse outcomes (intra-amniotic hemorrhage → ↑risk for spontan. abortion/fetal death) |
Complications | maternal: bleeding or infection,
fetus: bands or limb amputation |

→ Alternative: Cordocentesis 📷
Cordocentesis:
- Also known as percutaneous umbilical blood sampling.
- Technique involves puncturing the umbilical vein as close as possible to the placental insertion of the umbilical cord to avoid injuring the fetus.
- Typically performed starting at 16 weeks of gestation.
- Results can be obtained within 72 hours.
Complications:
- Approximately 2% of procedures may result in spontaneous abortion.
- Other potential complications include hemorrhage and infections.
⇒ ALL:

- DTP (Diph, tetanus, pertuss) ⇒ SINGLE DOSE → 27-36w
- INFLUENZA (inactivated → i.m.)


⇒ Other vaccines only if never immunized ⇒ Avoid Live + HPV vaccine

- The FDA classifies medicines for use during pregnancy into specific groups.
- Group A: Believed safe based on human research. (Note: Such drugs are rare.)
- Group B: Considered safe in studies not involving humans.
- Group C: Uncertainty remains; safety isn't confirmed.
- Group D: There's evidence suggesting potential harm.
- Group X: Definitely unsafe during pregnancy.
- These meds have shown harmful effects in both animals and people.
- The negative impacts clearly surpass any potential benefits.
Drug | Category | Effect |
CV drugs | ||
ACEi & ARBs | D | 1st T → malformations
2nd T → Oligohydramnios (due to renal failure) → Potter’s syndrome* 📷 |
Statins | X | CNS + limb deformities |
Warfarin
(use LMWH as an anticoagulant in pregnancy) | D | - Fetal hemorrhage + spont. abortion
- Optic atrophy
- Warfarin embryopathy ** |
Antibiotics | ||
Aminoglycosides | 1st T: Permanent deafness | |
Tetracycline | Accumulation in bones
teeth discoloration | |
Fluroquinolones | Fetal cartilage damage | |
TMP-SMX | ↓ Folate → neural tube def.
Displacemement bili from albumin → Kernicterus | |
Antiepileptics
(all may affect) | most = D | |
Valproic acids, Carbamazepin + Phenobarbital | D | ↓ Folic acid → Neural tube def (↑↑dose folate acid during pregnancy - Normal recommendation: 400 mcg/day; High risk mothers: 4mg/day) |
Phenytoin | Fetal Hydantoin syndrome = Abnormal facial*** 📷 + growth def. | |
Lithium | D | Ebstein’s anomaly **** 📷 |
Immunomodulators | ||
MTX | X | ↓Folic acid → neural tube def.
(⇒ used for ABORTION in ECTOPIC preg) |
Thalidomide (Contergan)
| X | Limb deformities
• Amelia: absence of limb
• Micromelia: short limbs
• Phocomelia: abnormal limb |
Hyperthyroidism drugs | ||
Methimazole | D | Aplasia cutis ***** 📷 + Neonatal hypothyroidism
(⇒ PTU in 1st T; Methimazole in 2nd) |
Derma drugs | ||
Isotretinoin (vit A derivate) | X | 20% → spont. abortion
20-30% of live birth
→ abnormal facial (low ears, wide-spaced eyes)
→ congenital heart di.,
→ hydrocephalus |
Vitamin A | during 1st T:
spont. abbortion
microcephaly
heart | |
Caffein | Crosses placenta → can ↑wakefulness
NORMAL intake = Øharm |
Potters sy: 📷
- During the 1st trimester, multiple congenital malformations are detected.
- In the 2nd/3rd trimester, a condition known as oligohydramnios arises due to decreased amniotic fluid.
- This suggests impaired fetal kidney function.
- This situation can progress to Potter's syndrome.
- Consequences might include underdeveloped lungs and anomalies in bones or limbs.
- Abnormalities observed in bones and joints.
- Presence of "dotted growth plates": observed as tiny, round shapes in X-ray.
- Underdeveloped nasal structure.
- Shortened limbs.
- Cleft lip and cleft palate
- Wide-spaced eyes
- Broad short nose
- Malformed ears

Aplasia cutis: 📷
Øepidermis on scalp ⇒ mainly at 1 local point ⇒ missing patch of hair/skin
Fetal Alcohol Spectrum Disorder (FASD):
- A collection of disorders linked to alcohol consumption during pregnancy.
- Fetal alcohol syndrome (FAS): One of the main conditions within FASD.
- Partial fetal alcohol syndrome (pFAS): A subtype where not all symptoms of FAS are present.
- Alcohol-related neurodevelopmental disorder (ARND): Problems with brain development due to alcohol exposure.
- Neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE): Behavioral issues stemming from in-utero alcohol exposure.
- Alcohol-related birth defects (ARBD): Physical birth defects (i.e.e heart defect) due to alcohol exposure during pregnancy.
- There are two main harmful substances in cigarettes: nicotine and carbon monoxide.
- These toxins can reduce the amount of oxygen the baby receives.
- Nicotine causes the blood vessels to constrict, which reduces blood flow to the placenta.
- Carbon monoxide reduces the oxygen-carrying capacity of blood cells.
IUGR/Low birthweight:
- In about 20% of cases, smoking has been identified as the cause.
Placental Issues:
- Abruption: The placenta detaches prematurely.
- Previa: The placenta covers the cervix.
Other potential outcomes:
- Early breaking of the water sac, or premature rupture of membranes.
- Going into labor before the due date.
- A well-known link with Sudden Infant Death Syndrome (SIDS).
Stimulants:
- They lead to vasoconstriction
- Potential outcomes include:
- Restricted fetal growth, leading to lower birth weight.
- Complications with the placenta, known as placental abruption.
- Birth before the due date.
- The unfortunate event of losing the pregnancy.
- The use of certain substances is advised against during pregnancy.
- Potential effects on brain development are noted.
- Limited information available on the potential risks and safety.
F ❌
- X-rays, CT scans:
- Small doses → no harm.
- Harm threshold → unclear.
- 8 to 15 weeks, high doses → microcephaly, growth restriction, intellectual challenges.
- Scans → use lead shields for fetus protection.
- Methylmercury in fish/seafood.
- Cooking → doesn't remove.
- Mothers → usually unaffected.
- Fetus's brain → sensitive to mercury.
- Effects → developmental delays.
- Severe cases → blindness, deafness, cerebral palsy.
- Canned tuna = mercury-tested, considered safe.
Performed to evaluate fetal health ↘ Identifies risk factors ↘
- Intrauterine death
- Fetal hypoxia ↘ Guides medical actions ↘
- Interventions to prevent complications
- Possible early delivery
- Influences delivery method ↘
- Vaginal or cesarean
Continue HR monitoring of fetus
(if fetus moves → HR increases)
after 32weeks GA → intact autonomous nervous system
Reactive ⇒ 📷
- 2 instances of increased fetal heart rate (accelerations) in a 20-minute span.
- A rise of 15 beats / minute above the baseline.
- Each increase should last for at least 15 seconds.
→ A positive sign for the well-being of the fetus.
→ Typically suggests no immediate need for urgent delivery.
Non-Reactive ⇒ 📷
- Inadequate accelerations observed after 40 minutes of monitoring.
- May result from the baby being asleep or facing potential risks!
- Possible follow-up actions:
- Repeating the test in 30 minutes.
- Considering vibroacoustic stimulation.
- Exploring further assessments such as a biophysical profile.
- Fetal movement: There should be ≥ 3 distinct movements observed in a 30-minute period.
- Fetal tone: The fetus should display >1 extension of an extremity or the spine, followed by a return to a flexed position.
- Fetal breathing: There should be >1 episode of chest expansion lasting ≥ 30 seconds.
- Amniotic fluid volume: The single deepest fluid pocket should measure ≥ 2 centimeters.
Maximum score = 10 out of 10 8 to 10 normal • 2 points deduction allowed for movement, tone, or breathing • Not amniotic fluid 6 = equivocal (usually repeated 24 hours) 0 - 4 = abnormal (consider delivery)
Q. * The fetal biophysical profile includes five parameters, except:
- A. Fetal respiratory movements
- B. Fetal tonus
- C. Quantity of amniotic fluid (deepest pocket of amniotic fluid at ultrasound examination)
- D. Aspect of the placenta at ultrasound examination
- E. Non-stress test (NST)
- A. Fetal respiratory movements
- B. Fetal tonus
- C. Quantity of amniotic fluid (deepest pocket of amniotic fluid at ultrasound examination)
- D. Aspect of the placenta at ultrasound examination
- E. Non-stress test (NST)
- Evaluation involves the nonstress test and assessment of amniotic fluid volume exclusively.
- Focus on the parameters with the highest predictive value for outcomes.
- Exclude problem when both parameters are normal
⇒ If 1 parameter is abnormal → consider further assessments.
- rarely employed test to assess the safety of a vaginal delivery.
- Involves monitoring fetal heart rate following oxytocin or nipple stimulation.
- Late heart rate decelerations 📷 can signal hypoxia → C-section due to an inability to tolerate labor.
- Utilizes Doppler ultrasound technology.
- Assesses flow velocity and direction.
- Normal flow maintains a continuous forward direction.
- Abnormalities include absent or reversed diastolic flow. 📷
- Absence of end-diastolic flow velocity (AEDV).
- Reversal of end-diastolic flow velocity (REDV) indicates impending fetal demise.
⇒ Typically necessitates urgent delivery.
In some cases, one twin may not survive in the womb.
- Natural resorption of the fetus or embryo, often referred to as the "vanishing twin" phenomenon.
- Ultimately, a single baby is delivered.
hcg
- Dizygotic twins: Two siblings resulting from the fertilization of two separate ova (2 zygotes) by two distinct sperm cells. Also known as "fraternal twins."
- Monozygotic twins: Twins emerging from a single zygote that divides into two. These are often referred to as "identical twins."
The timing of cleavage plays a role in determining chorionicity (the number of chorions) and amnionicity (the number of amnions) using the acronym SCAB.
- Cleavage within 0-4 days results in separate chorion and amnion.
- Cleavage within 4-8 days leads to a shared chorion.
- Cleavage within 8-12 days results in a shared amnion.
- Cleavage occurring at 13+ days leads to a shared body, resulting in conjoined twins.
- Maternal risks include gestational hypertension, preeclampsia, placenta previa, and the likelihood of a cesarean delivery.
- Fetal risks encompass preterm delivery, growth restriction, and congenital anomalies.
monochorionic
(more common in diamniotic than in monoamniotic)
Imbalanced blood flow due to arteriovenous anastomoses in the placenta, which are vascular connections between twins.
- In the recipient twin, there's an excess of blood leading to polyhydramnios and organ enlargement, resulting in hypervolemia and potentially heart failure.
- In the donor twin, there's a decrease of blood volume, leading to oligohydramnios and growth restriction.
⇒ single placenta
⇒ fluid pockets discreptancy:
- twin 1: fluid pocket <2cm
- twin 2: fluid picket >8cm
Fetal laser coagulation 📷
- is a procedure involving the elimination of anastomoses.
- It effectively separates the placenta into two parts.
- This procedure is associated with significant risks and is typically reserved for severe discordance between twins.
Amnioreduction 📷
- involves the removal of excess amniotic fluid to address polyhydramnios.
- It can enhance maternal breathing and reduce pressure on the cervix.
- This procedure is associated with a reduced risk of preterm delivery.
- The choice of delivery method depends on the positioning of the twins.
- The presenting twin, often referred to as twin A, is the one closest to the cervix.
- The non-presenting twin, or twin B, is positioned furthest from the cervix.
- If both twins are vertex → vaginal delivery
- If one twin is vertex and the other is not, it may involve a trial of vaginal delivery or a cesarean delivery.
- Indications for C-section even if both vertex:
- Collision: Both twins in vertex presentation can result in their heads being blocked by a similar advance above the pelvic rim. 📷
- Compaction: This occurs when both heads are blocked by a similar advance below the pelvic rim. 📷
- Impaction: The second fetus may block the advancement of the first twin after engagement. 📷
- When twin A is not in the vertex position, a cesarean delivery is typically recommended.
Q: Select the correct sentences regarding twin pregnancy delivery.
A. When the first fetus is in breech and the second is in cephalic presentation, there is a risk for locking phenomena during vaginal delivery, and the cesarean section is preferred.
B. If both fetuses are in cephalic presentation, there is a risk of collision, and if this occurs after the onset of labor, the cesarean section is the correct choice.
C. When the first fetus is in breech and the second is in cephalic presentation, there is a risk for compaction during vaginal delivery.
D. If the second fetus is in transverse lie, the cesarean section is not mandatory.
E. The acute fetal distress of only one fetus doesn't mean that a vaginal delivery is not possible.
A. When the first fetus is in breech and the second is in cephalic presentation, there is a risk for locking phenomena during vaginal delivery, and the cesarean section is preferred.
B. If both fetuses are in cephalic presentation, there is a risk of collision, and if this occurs after the onset of labor, the cesarean section is the correct choice.
C. When the first fetus is in breech and the second is in cephalic presentation, there is a risk for compaction during vaginal delivery.
D. If the second fetus is in transverse lie, the cesarean section is not mandatory.
E. The acute fetal distress of only one fetus doesn't mean that a vaginal delivery is not possible.
Q. Select the correct answers:
A. The incidence of multiple pregnancy increased in the last two decades, also due to widespread assisted reproductive techniques. B. The monochorionic twin pregnancy implies two separate placentas. C. Conjoined twins are the result of early separation of a unique embryo in the first 3 days. D. The positive diagnosis of a twin pregnancy is definitive only at the end of the first trimester due to vanishing twin phenomena, which is possible during the first weeks of a multiple pregnancy. E. Dizygotic twin pregnancy is always bichorionic
A. The incidence of multiple pregnancy increased in the last two decades, also due to widespread assisted reproductive techniques. B. The monochorionic twin pregnancy implies two separate placentas. C. Conjoined twins are the result of early separation of a unique embryo in the first 3 days. D. The positive diagnosis of a twin pregnancy is definitive only at the end of the first trimester due to vanishing twin phenomena, which is possible during the first weeks of a multiple pregnancy. E. Dizygotic twin pregnancy is always bichorionic
Q. Select the false sentences regarding multiple pregnancy:
A. Preeclampsia is less frequent in multiple pregnancies when compared with singleton pregnancies. B. Preterm deliveries are more frequent with twin pregnancies. C. Iron-deficiency anemia is more frequent in singleton pregnancies than in twin pregnancies. D. The fourth stage of labor after the vaginal delivery of twins is characterized by a lower risk of bleeding due to the usually smaller size of the fetuses. E. Hemorrhage is more frequent after vaginal delivery of twins.
A. Preeclampsia is less frequent in multiple pregnancies when compared with singleton pregnancies. B. Preterm deliveries are more frequent with twin pregnancies. C. Iron-deficiency anemia is more frequent in singleton pregnancies than in twin pregnancies. D. The fourth stage of labor after the vaginal delivery of twins is characterized by a lower risk of bleeding due to the usually smaller size of the fetuses. E. Hemorrhage is more frequent after vaginal delivery of twins.
- It refers to the loss of a viable uterine pregnancy before 20 weeks, sometimes occurring in the second trimester, but mainly in the first trimester (before 12 weeks).
- It is often recognized through declining serial hCG levels or via US
- Clinically, it manifests as vaginal bleeding + pelvic cramping
- Pelvic abdominal pain caused by uterine contractions
- Metrorrhagia (uterine bleeding between menstrual periods)
- Changes in the cervix
- Valve examination - ovular fragments can be revealed at the external cervical orifice
- Vaginal examination - estimates the volume of the uterus in relation to the gestational age, the consistency of the uterus (usually the uterus is contracted).
/w=1920,quality=90,fit=scale-down)
Risk factors:
- Classics
- Maternal age exceeding 35 years.
- Previous pregnancy loss.
- Smoking and alcohol use.
- Maternal health conditions such as infections, diabetes, and obesity, Thyroid-related issues, Thrombophilias.

Type | Description | Cervical Status |
Complete | Bleeding and complete passage of sac and placenta. Cervix is closed and bleeding stopped. | Closed |
Threatened | Vaginal bleeding + cramping. Cervix is closed and soft | Closed |
Inevitable | Increasing bleeding and cramps ‡ rupture of membranes. Cervix is closed until products start to be expelled, then external os opens. | Initially closed, then opens as products are expelled |
Missed | No bleeding (fetal death in the uterus). Cervix is closed. | Closed |
Incomplete | Extremely heavy bleeding and cramps + passage of tissue noticed. | Open |
Recurrent | 2-3 consecutive spontaneous abortions | |
Septic | Contents of uterus infected - infrequent | Open (may be infected) |


DDx for Bleeding:
- other 1st Trimester causes Ectopic pregnancy (EP) Hydatidiform mole
- Gyn causes Uterine fibroids Cervical polyp Cervical erosions Dysfunctional bleeding Ovarian tumors
- Hemorrhagic complications: These can range from heavy bleeding to severe hemorrhage and even septic shock in some cases.
- Infectious complications: Miscarriages can lead to infections such as endometritis (inflammation of the inner lining of the uterus), salpingitis (inflammation of the fallopian tubes), and pelviperitonitis (inflammation of the pelvic peritoneum).
- Late complications:
- Pelvic inflammatory disease (PID): An infection that can affect the female reproductive organs, including the uterus, fallopian tubes, and ovaries. PID can lead to chronic pelvic pain and infertility if left untreated.
- Infertility: Recurrent miscarriages or complications from miscarriages can sometimes result in infertility, making it difficult for a woman to conceive in the future.
- Depression: Miscarriages can have a significant emotional impact on individuals, leading to feelings of grief, sadness, and depression.
Pregnancy OUTSIDE uterus & endometrium
⇒ Most common: Fallopian tube → Ampulla
80% ampulla, 10% isthmus, 5% fimbriae
Other locations: 📷
- Fallopian tube damage
- A history of previous ectopic pregnancy.
- Tubal blockage or obstruction.
- Tubal ligation (although pregnancy is rare).
- Prior tubal surgery related to tumors.
- Pelvic inflammatory disease.
- The use of IUDs
- others:
- infertility treatments
- structural (fibroids, adhesions, anatomical abnormalities)
- smoking (not alcohol!)
Overall: lower risk of pregnancy with IUDs → However, if pregnancy does occur, there's a heightened risk of it being ectopic.
Q. Causes of ectopic pregnancy may be: A. Prior tubal surgeries B. Alcohol abuse C. Intestinal inflammatory disease D. Ovarian pathologies E. Infertility treatment
A. Prior tubal surgeries B. Alcohol abuse C. Intestinal inflammatory disease D. Ovarian pathologies E. Infertility treatment

- symptoms typically appear in the first trimester.
- These symptoms may include:
- Vaginal bleeding.
- Abdominal pain, which can sometimes resemble appendicitis.
- Abnormal human chorionic gonadotropin (hCG) levels based on gestational dates.
- Ectopic pregnancies often exhibit smaller-than-expected increases in hCG levels ⇒ An increase of less than 35% in hCG levels over 48 hours may suggest an ectopic pregnancy.
- Normally, hCG should double every 72 hours.
- Fever: Detected in approximately 20% of patients, with temperatures exceeding 38.0°C.
- Abdominal Pain: Occurs in 90% of cases, can be continuous or colicky in nature.
- Tenderness: Noted during bimanual examination and cervical motion tenderness.
- Menstrual Cycle Abnormalities: Presence of amenorrhea followed by scant bleeding that is darker in appearance.
- Pregnancy Signs
- Subjective Pregnancy Signs: Nausea, vomiting, and breast tension are common.
- Gynecological Examination: Presence of signs indicative of pregnancy.
- Chadwick's Sign: Bluish discoloration of the cervix and vagina due to pelvic vasculature engorgement, typically visible from the 6th week of gestation (WG).
- Hegar's Sign: Softening of the cervical isthmus observed between 6-8 WG.
- Uterine Volume: Enlarged uterus noted, but the volume is smaller compared to the duration of amenorrhea.
- Adnexal Mass: Palpable in 50% of cases. Additionally, in half of the patients, a mass attributable to the corpus luteum may be palpated on the side opposite the ectopic pregnancy.
- Peritoneal Irritation: Signs indicative of irritation in the peritoneal cavity.
(shock, pain, rebound tenderness + guarding)
Clinical Signs:
- Laffont sign: Pelvic abdominal pain radiating into the shoulder.
- Ody sign: Pain in the anterior fundus of the vaginal sac, especially during urination.
- Proust sign: Violent pain on palpation of the vaginal sac, in the backside, known as "Douglas' scream."
- Mondor sign: A floating sensation of the uterus (due to hemoperitoneum).
In case of rupture of an ectopic pregnancy, there can be an acute abdomen with intensified pain and abdominal relaxation.
Culdocentesis: 📷 Culdocentesis is a diagnostic procedure where the bottom of the pouch of Douglas (cul-de-sac) is punctured, and the characteristics of the aspirated fluid are examined. If the aspirate contains uncoagulated, non-coagulable blood or clots, it confirms the diagnosis of hemoperitoneum, which can be indicative of a ruptured ectopic pregnancy.

TVUS: 📷
- Transvaginal Ultrasound (TVUS): While TVUS is a valuable diagnostic tool, it may sometimes be non-diagnostic if the pregnancy is too small to localize, or if a spontaneous abortion has occurred.
- Follow hCG Levels: Human chorionic gonadotropin (hCG) levels are monitored. They are typically measured every 48 hours.
- Falling hCG Levels: If hCG levels are falling, it indicates a nonviable pregnancy. This could be indicative of a miscarriage.
- Slowly Rising hCG Levels: If hCG levels are rising slowly, it suggests the possibility of an ectopic pregnancy.
- Repeat TVUS: A repeat transvaginal ultrasound may be performed to identify whether the pregnancy is intrauterine or ectopic.


Laparoscopic Salpingostomy:
- This procedure is commonly performed using laparoscopy.
- It involves a linear salpingostomy followed by the removal of the ectopic pregnancy, while preserving the affected fallopian tube.
- The goal is to save the tube if possible while removing the pregnancy.
Salpingectomy:
- Salpingectomy is considered if the fallopian tube is severely compromised or if the patient has a history of another tubal ectopic pregnancy.
- In this case, the entire fallopian tube is surgically removed.
Monitoring BhCG Levels:
- After surgery, BhCG (human chorionic gonadotropin) levels are monitored until they become undetectable.
- In about 15% of cases, residual trophoblast tissue may remain after surgery, which is why ongoing monitoring is essential.
Immunoprophylaxis with Rhogam:
- If the patient is Rh-negative and Rh-positive fetal blood is involved (as can happen in ectopic pregnancies), immunoprophylaxis with anti-D Immunoglobulin (Rhogam) is recommended to prevent Rh sensitization.
Laparotomy in Certain Cases:
- In some situations, such as hemodynamic instability or a history of pelvic surgery, laparotomy (open abdominal surgery) may be recommended instead of laparoscopy.
- A rare form of pregnancy.
- Associated with trophoblastic placental neoplasms.
- Typically benign → molar pregnancies.
- In rare instances, it may be malignant (see types)
Complete (more common) | Partial | |
Patho | Fertilization “empty” egg → only paternal chromosomes
Ømaternal chromosome → Øfetal tissue
Øfetal drainage = ↑↑SWOLLEN villi | Fertilization normal egg by 2 sperms → paternal+ maternal chromosomes → fetal tissue/drainage ⇒ LESS SWOLLEN villi |
Karyogram | 46, XX (haploid) | triploid (69,XXX/XXY/XYY) |
Immunostaining | p57 negative -
• Cyclin dependent kinase
• Only expressed by maternal chromosomes | p57 positive + |
Clinic | - ↑uterus: Size/date discrepancy (uterus to big for stage)
- Bleeding (painless)
- Hyperemesis gravidarum
- Theca lutein cysts (hcg stimul. ovaries)
- Hyperthyroidism (hcg stimul. TSH receptor)
- Preeclampsia (BEFORE 20w) | - n/↓ uterus
n May be normal (some villi drainage to fetus)
↓ May be small for gestational age (slow growth of fetus) |
b-hcg | MARKED ↑↑ (>100.000) | Ømarked ↑ (less common) |
US | “clusters of grapes” 📷+ “sandstorm” appearance (swollen villi)
Doppler → abnormal placent. vessels
ovarian cysts | - fetus might be seen (but small)
- oligoamnionitis
- abnormal placenta (cysts=molar degen.)
- hemorrhage |
Risk of malignancy | 10-20% * | <4% |
When assessing the risk of persistent post-evacuation Gestational Trophoblastic Neoplasia (GTN), healthcare providers consider the following parameters:
- Local Uterine Invasion: GTN invading more than 31% of the uterine wall increases the risk.
- BhCG Level: High levels of beta-human chorionic gonadotropin (BhCG) exceeding 100,000 IU/L indicate an elevated risk.
- Enlarged Uterus: An enlarged uterus, often due to trophoblastic tissue, is associated with a higher risk.
- Prominent Theca-Lutein Cysts: The presence of these cysts in the ovaries can indicate a more aggressive form of GTN and is a risk factor.
- Treatment often involves uterine suction curettage.
- Options in special situation:
- In rare cases, a hysterectomy may be necessary.
- Most cases don't necessitate chemotherapy → reserved for high-risk patients (suggestive signs of a higher likelihood of choriocarcinoma) → Treatment options include methotrexate or actinomycin D.
+Contraception (see next question)
- Monitor hCG levels → until return normal (which can take up to six months)
- If there's a plateau in hCG levels, it could indicate an invasive mole or choriocarcinoma.
- After treatment, contraception is recommended.
A new pregnancy can cause hCG levels to rise → challenging to confirm the resolution of a molar pregnancy.
⇒ Typically, the advice is to avoid pregnancies for at least one year.

- Typically presents with vaginal bleeding and/or elevated hCG levels.
- Diagnosis is often confirmed through 🦇pelvic US (Each type = distinct characteristics)
- There's a potential for metastasis to the 🫁 lungs. ⇒ chest X-ray.
🦇pelvic US (Each type = distinct characteristics)
single agent chemotherapy (MTX or actinomycin D)
- These tumors typically arise after a molar pregnancy.
- usually after COMPLETE MOLE
- Rare: after partial, abortion, or normal pregnancy
- They involve swollen chorionic villi that invade the uterine wall (myometrium). ⇒ vaginal bleeding.
→ Approximately 5% of cases have the potential to metastasize.
- b-hCG → plateau +rise after prev. molar pregnancy tx
- US 📷 → Mass (poorly defined) → Invades myometrium

desire fertility-preservation → 💊 Chemo (MTX or Actinomycin D)
alternative → hysterectomy
- rarely-occurring malignant gestational tumor 📷 → composed of syncytiotrophoblast and cytotrophoblast cells.
- Characterized by the absence of villi formation.
- Most frequently develops following a complete molar pregnancy.
- Early & extensive mets (hematogenous) → mainly 🫁
vaginal bleeding + 🫁mets: cough + hemoptysis
other sites:
- Vagina (30%):
- Symptoms: Vaginal bleeding is a common symptom, and "blue lesions" may be present in the vaginal area.
- Pelvis (20%):
- Symptoms: In cases where the pelvic area is affected, rectal bleeding may occur if the bowel is invaded. These lesions can be detected by ultrasound imaging.
- Liver (10%):
- Symptoms: Liver involvement may lead to modifications in liver tissue samples. Ultrasound imaging can reveal signs of liver involvement.
- Brain (10%):
- Symptoms: Brain metastases can cause symptoms such as headaches, dizziness, and seizures. Imaging techniques like CT scans or MRI can detect signs of brain involvement.
- b-hCG → plateau +rise after prev. molar pregnancy tx
Treatment for low-risk forms typically involves single-agent chemotherapy: MTX or actinomycin D.
→ The majority of patients (>90%) achieve a cure with chemotherapy.
- A seldom-occurring germ cell tumor (develop in either the ovary or testes)
- Originates from germ cells that differentiate into trophoblasts.
- histological = gestational choriocarcinoma.
- Produces beta-human chorionic gonadotropin (B-hCG).
- It is often deadly☠️.
- Treatment and cure can be challenging.
- Trophoblast proliferation BUT Ø formation of villi
- Typically occurs after non-molar abortion or pregnancy
- May occur months / years after pregnancy
*intermediate trophoblast
🔪 Hysterectomy often needed
(poor response to chemo)
- Detachment = Prior to delivery
- Blood loss from maternal circulation
→ no blood to fetus
→ contraction of uterus (triggered by bleeding)
⇒ life-threatening condition for both fetus and mother
- 🔂 previous PD
- 🤰🏼 maternal disorders
- 😷 pre-existing placental RF (HT, pre-eclampisa,vasoconstrictor[smoking, cocaine])
- 👛 uterus d. (structural, C-section)
- 🚗 Trauma
- ⬇️ rapid decrompression (twin)
Q. Regarding the diagnosis of premature detachment of a normally situated placenta (abruptio placentae), the symptoms found in the obstetrical syndrome may include:
A. Pain B. Relaxed uterus C. The disappearance of fetal movements or altered fetal heart rate D. Vaginal bleeding (not necessarily in all cases) E. Lowering of the fundus of the uterus
A. Pain B. Relaxed uterus C. The disappearance of fetal movements or altered fetal heart rate D. Vaginal bleeding (not necessarily in all cases) E. Lowering of the fundus of the uterus
- Fetal distress → might lead to demise
- Maternal
- Hypovolemic shock (maternal)
- DIC
- Cortical necrosis
- lack of blood flow leading to kidney cortex damage → Acute kidney failure • Linked to decreased blood supply and clotting disorders • Commonly linked with placenta detachment
- Symptoms include:
- ARF and Absence of urination (anuria)
- Flank pain
- Blood in urine (possibly macroscopic)
- US ⇒📷 retroplacental hematoma (but not reliable)
- +- MRI
- Other: coagulation markers, renal markers, hepatic markers, fetal heart mornitoring
Sexton's Classification:
- Depending on the detached placental surface:
- Stage I: Detachment of 1/6 of the placental surface.
- Stage II: Detachment of up to 50% of the placental surface.
- Stage III: Detachment of over 50%.
Page's Classification:
- Based on severity (bleeding, contraction, FHB, coagulat.):
- Stage 0: Infraclinical (subclinical) hematoma recognized post-delivery.
- Stage I: Characterized by an irritable uterus with slight contraction and general stability, ↓bleeding, FHB present
- Stage II: Features a contracted uterus, without shock, but friable blood clots (more bleeding), FHB altered
- Stage III: Defined by uteroplacental apoplexy (Couvelaire syndrome 📷), a state of shock, and potential coagulation disorders, FHB undetectable
❤️ Fetal HR monitoring
🚿 Fluids +-blood, coagulation correction
↓
🪡 Amniotomy (artificial membrane rupture)
↓
🚚 DELIVERY
- unstable (hypotension, coagulopathy) → 🔪 C-section
- stable → 🦪 vaginal or 🔪C-section
choice betw. vaginal + C-section:
Depends on multiple factors → fetal status, weeks of gestation
- Definition: Placenta goes before baby
- Location: Near or at cervical opening
- Attachment: Lower section of womb
- Normal: Positioned >2 cm away from cervix
- Complete: Fully covering cervical opening
- Partial: Covers part of the cervix
- Marginal: Reaches cervix edge
- Low: Border within 2 cm of opening
- history of:
- Placenta previa
- Cesarean delivery
- past pregnancy
- uterine operations
⇒ Ø💥pain

⇒ ⏱️ PRETERM LABOR
Premature rupture of membranes, which can lead to premature birth, chorioamnionitis, umbilical cord prolapse
⇒ Dgx: 🦇 US → might also show co-existing placenta accreta (perform US before exam → AVOID contact: Ø vaginal touch, speculum, insertion of foreign structures [i.e. mesh])
Q. When dealing with a case of placenta praevia with hemorrhage, which of the following should be avoided?
A. Vaginal touch B. Placement of a vaginal mesh (tampon for vaginal tightening) C. Speculum examination D. Transport of the patient in an anti-Trendelenburg position (reverse Trendelenburg) E. A quick intravenous line (IV catheter for the administration of fluids)
A. Vaginal touch B. Placement of a vaginal mesh (tampon for vaginal tightening) C. Speculum examination D. Transport of the patient in an anti-Trendelenburg position (reverse Trendelenburg) E. A quick intravenous line (IV catheter for the administration of fluids)
🩸BLEEDING → prevention + Tx
- avoid sex, strenous tasks + extended standing
- if bleeding → fluids/RBC transfusion
All types + abund. bleeding→ 🔪 Scheduled C-section (36-37w → if accreta at 34-35w) exception: Low lying (lateral) + Øabundant bleeding → Amniotomy + vaginal
(fetals vessel near os (<2cm) within velamentous cord)
- Apt test with NaOH can determine the source of bleeding:
- Pink supernatant indicates fetal bleeding
- Yellow supernatant indicates maternal bleeding
- Wright stain on blood smear:
- Presence of nucleated red blood cells suggests fetal blood (blood taken from cord, not from mother)




- 🍮 Cervical lesions + other non-obstetric
- Placenta previa 30%
- Abruptio placentae 25%
- Spontaneous abortion < 15%
- Cervical lesions (cervicitis, polyps, ectropion, cervical cancer): 8-10%
- Vulvovaginal varices: 2-4%
- Uterine rupture < 5%
- Local trauma: < 5%
- Cervical changes at the onset of labor: < 5%
- Vasa previa < 1%
- ❌ Spontaneous ABORTION (Miscarriage)
Q. The most common causes of bleeding in the second half of pregnancy are:
A. Local trauma B. Abruption placenta (Detachment of the normally inserted placenta) C. Cervicitis D. Placenta previa E. Vulvo-vaginal varicosities
A. Local trauma B. Abruption placenta (Detachment of the normally inserted placenta) C. Cervicitis D. Placenta previa E. Vulvo-vaginal varicosities
- Mild cases of nausea are referred to as "morning sickness."
- Itching
- Jaundice, colurice urine, discolored faces
- Nausea, vomiting
- Without hepatomegaly, or abdominal pain
- Signs disappear in postpartum
- ↑ Conjug. bilirubin, AP, transaminases, bile acids may be elevated
- QT interval (TQ) may be extended
- Does not affect fetal development
- In severe cases of vomiting, are named hyperemesis gravidarum.
- Excessive vomiting can result in hypovolemia
- This condition may lead to significant weight loss.
Biological picture:
- Multifactorial with hormonal, immunologic, and psychologic components.
- Rapidly rising B-hCG + estrogen levels may be implicated.
→ Alkalosis? / Hypokalemia?
→ Ketones (urinary)?
Thiamine def. → Wernicke’s encephalopathy (but few cases reported only)
#1 Lifestyle (eat when hungry, avoid trigger)
↓
#2 Antiemetics:
- 🥇Doxylamine-pyridoxine
- Doxylamine: anti-histamine
- Pyridoxine: vitamin B6 (improves nausea through unknown mechanism)
- Severe → classic antiemetics (Onda/DopaAgonist)
DM: pregnancy makes PRE-EXISTING DM worse
GD: Diabetes onset DURING pregnancy
⇒ Gestational during pregnancy: 2-3 Trimester
Decreased response of mother to insulin (probably to ↑ gluc delivery to fetus)
Etiology: Anti-insulin factors produced by placenta and high maternal cortisol levels create increased peripheral insulin resistance, leading to GDM and/or exacerbating pre-existing DM.
- Screening is conducted using serum glucose testing.
- The presence of glycosuria is normal during pregnancy.
- Hemoglobin A1c has limited utility in pregnancy.
Gestational Diabetes Testing:
- Screening: 50-gram one-hour glucose challenge test (GCT)
- Done between 24 to 28 weeks.
- Take a 50-gram sugar drink (no need to be on an empty stomach).
- Blood sugar is checked an hour later.
- If blood sugar is between 130 to 140 mg/dL or more (can change depending on the lab) -> go to the diagnostic test.
- Diagnostic test: 100-gram three-hour oral glucose tolerance test (GTT)
- Begin after fasting for 6 hours.
- Test blood sugar at the start, then after 1, 2, and 3 hours of drinking a 100-gram sugar drink.
- If two or more of these tests show high levels -> diagnosis of gestational diabetes.
↓
Evaluation Standards for 100g 3-hour Glucose Tolerance Test (GTT):
Measurement Time | Threshold (mg/dL) |
Before Eating | 95 |
After 1 hour | 180 |
After 2 hours | 155 |
After 3 hours | 140 |
- ↕️ BIG BABY
- LARGE for GA
- Macrosomnia
- Polyhydramniosis
- 🏮🥐Pre-eclampsia
- ↓🍬Neonatal HYPOglycemia
- 🏗️ Congenital defects
- 🫀 heart
- 🧜🏼♀️ Sacral agenesis (caudal regression synd.)
⇒Spont. Abbortion, Stillbirth, preterm
⇒ Birthtrauma ⇒ Shoulder dystocia + other ⇒ C-section
⇒ Transposition of the great arteries (TGA), Other: Ventricular septal defects (VSDs), Truncus arteriosus, Tricuspid atresia, Patent ductus arteriosus (PDA)
+/- SIRENOMELIA (fusion of legs) +/- Neural tube defect

Q. Influence of diabetes mellitus on pregnancy may include: a. Abortion b. Postterm delivery c. Amniosis d. Macrosomy e. Postpartum hemorrhagic complications
a. Abortion b. Postterm delivery (→ preterm) c. Amniosis (→ poly) d. Macrosomy e. Postpartum hemorrhagic complications
>30% over Target values?
Targets: Fasting < 95 1hr postprandial <140 2h postprandial <120
↓
- no ⇒ Diet + Exercise
+ yes ⇒ Insulin (+- Metformine)
- Diabetes typically resolves after childbirth.
- However, there is an elevated risk of developing DM2 following delivery.
⇒ Screening for postpartum diabetes is recommended with a 2-hour glucose tolerance test (GTT) conducted 6-12 weeks after giving birth.

- During pregnancy, women with normal blood pressure levels often experience a reduction in blood pressure, predominantly at the end of the first trimester. This decline is attributed to significantly increased vasodilation, a compensatory mechanism for the increased plasma volume associated with pregnancy.
- The decrease in blood pressure is notable, generally falling by 5 to 10 mm Hg, and this reduced level is maintained throughout the pregnancy until the onset of the third trimester.
- As the third trimester progresses, blood pressure typically begins to return to the levels noted pre-pregnancy. This pattern is consistent with the physiological changes and demands of late pregnancy on the maternal cardiovascular system.
- For women with pre-existing chronic hypertension, the blood pressure pattern during pregnancy mirrors this general trend. However, around 33% of these women will experience a normalization of their blood pressure during pregnancy, while another 33% will continue to have unchanged blood pressure readings. The remaining third are at an increased risk of developing preeclampsia, a serious hypertensive disorder of pregnancy characterized by high blood pressure and often a significant amount of protein in the urine.
- Chronic HT → BEFORE 20w + PERSISTS >12w postpartum
- Chronic kidney disease (e.g., glomerulonephritis, reflux nephropathy, and adult polycystic kidney disease).
- Renal artery stenosis.
- Systemic diseases with renal involvement (e.g., diabetes mellitus, systemic lupus erythematosus).
- Endocrine disorders (e.g., pheochromocytoma, Cushing's syndrome, primary hyperaldosteronism, hyperthyroidism, hypothyroidism, hyperparathyroidism, acromegaly).
- Coarctation of the aorta.
- Certain medications and substances (e.g., decongestants, steroids, licorice, cocaine, methamphetamines).
- Gestational HT → AFTER 20w + RESOLVES <12w postpartum
a. Essential Hypertension: This includes women who enter pregnancy while already on antihypertensive therapy, and the cause remains unknown. They typically have lower systolic (sBP) and/or diastolic blood pressure (dBP).
b. Secondary Hypertension: This type may have identifiable causes, such as:
- Absolute BP increase in pregnancy is defined as ≥ 140 mmHg for systolic BP (sBP) and/or ≥ 90 mmHg for diastolic BP (dBP).
- Relative BP growth, though not part of the formal definition, is considered abnormal when it exceeds 30 mmHg for sBP or 15 mmHg for dBP compared to baseline values.
- Women with relative BP growth should be evaluated for signs of preeclampsia, a potentially serious condition.
- BP values should be consistently elevated in at least two different examinations.
- BP measurements should be taken with the patient in a seated position using an appropriately sized cuff.
- Automatic BP measurement systems are not recommended for pregnancy monitoring due to the potential underestimation of true BP values.
Hypertension Type | Systolic BP (sBP) | Diastolic BP (dBP) | Notes |
Moderate Hypertension | 141 mmHg to 159 mmHg | 91 mmHg to 109 mmHg | |
Severe Hypertension | ≥ 160 mmHg | ≥ 110 mmHg | |
≥ 170 mmHg | ≥ 110 mmHg | Medical emergency requiring urgent treatment | |
White Coat Hypertension | Normal in non-clinical setting | Normal in non-clinical setting | Assessed by 24-hour ambulatory BP monitoring or home BP monitoring using a validated device |
It can lead to reduced placental perfusion.
→ Elevated risk of unfavorable fetal outcomes.
→ These outcomes may include fetal growth restriction, oligohydramnios (low amniotic fluid), and placental abruption.
- proteins (urinary)
- CBC, Renal (incl. uric acid) + liver markers (incl. coagulation)
→ not treated until BP >160/105 (or end-organ damage signs) #1 Labetalol / Methyldopa


#2 Nifedipine #3 alpha + beta blocker → Ø ARBs, ACEi or diuretics
- Labetalol i.v. (SE: bradycardia)
- Hydralazine i.v. (doesnt cause bradycardia → alternative for labetol if bradycardia present)
- Nifedipine p.o.
🥮 PLACENTAL ABNORMALITY (abnormal invasion/transformation of spiral aa. 📷+ other factors) ⇒ ↓PERFUSION (placental)⇒ release circulation substances ⇒ MATERNAL endothelial dysfunct. = VASOSPASM + COAGULATION ⇒ Endorgan-failure (incl. kidney)
- Hypertension
- Proteinuria
- End-organ dysfunction


- 🏛️ HISTORY
- prior eclampsia
- FH
- 1️⃣ FIRST pregnany (nulli)
- 👶🏼👶🏼 MULTIPLE gestations
- 🏮Maternal HT-assoc. conditions • Diabetes • Hypertension • Obesity • Chronic kidney disease • 🐺 Lupus/Antiphospholipid syndrome
- Positive PREDICTIVE TEST
- Uterine Artery Doppler Studies: These are used to anticipate the faulty trophoblastic invasion of the spiral arteries, a factor in PE development. The studies look for notches in the uterine artery waveform, with bilateral notches being significant for early-onset PE.
- Postural Test - Roll-over Test: This test measures the increase in diastolic blood pressure (DBP) when a pregnant woman moves from a lateral recumbent to a supine position. A rise in DBP by 20 mmHg or more increases PE risk.
- Isometric Exercise Test: Similar to the roll-over test, this involves handgrip exercises that increase vascular reactivity.
- Angiotensin Test: Measures vascular reactivity to angiotensin II, with a dosage increase required in PE patients.
- Measurement of Angiogenic Factors: Research focuses on sFLT and PlGF levels. A high sFLT/PlGF ratio suggests high risk for PE and severe maternal complications.
- Other Biological Tests: Include markers like hyperuricemia.

⇒ Calculation of Average SBP: Blood pressure is used to gauge PE risk, with an average BP above 90 mmHg being suggestive for PE.
- There's no unified standard for high risk. In routine: ≥1 Risk Factor (RF)
- Start after the 12th week but before the 28th week.
- Preferably by the 16th week.
- Continued every day until the baby is born
- 👶🏼 Fetal
- 🥮 Placental insufficiency (↓perfusion)
- 🎑Placental detachment
- 🤰🏼Maternal ⇒ Endorgan dysfunction
- 🫁 edema + 🫀HF
- 🍑liver failure
- 🍽️ DIC
- 🧠stroke
- 🥐RF
⇒ Growth restric. + Oligohydramnios
- Blood pressure: Systolic ≥ 165 mmHg or Diastolic ≥ 115 mmHg
- Recorded at least twice, 4 hours apart while resting.
- New brain or eyesight issues:
- Blind spots, vision loss
- Intense headache
- Altered AST/ALT levels
- Platelet count < 100,000
- Kidney failure
- Pulmonary edema
- Fetal weight below the 5th percentile (sev. IUGR)
- Oligohydramnios, characterized by a maximum vertical pouch of less than 2 cm of amniotic fluid.
- Biophysical score of less than 4 out of 10 in two assessments conducted at 6-hour intervals.
- Presence of reversed diastolic flow in the umbilical artery for fetuses under 32 weeks gestation or its absence for fetuses over 32 weeks gestation.
- Abnormal findings on non-stress test (NST), such as late or variable decelerations or the absence of short-term variability.
- Intrauterine fetal death
↓ - no → TERM-delivery (>37w) + 🧲 IV magnesium sulfate (at delivery)

+ yesIMMEDIATE delivery (<34w)
Patho: Related to blood flow/endothelial dysfunction (Exact etiology of seizures Ø clear)
during 3rd T or postpartum(44%)
- HT Tx
- 🧲 IV magnesium sulfate (seizures) ; alternative: benzos
- = 🥇 Most effective drug for preeclampsia.
- Often administered for prevention in preeclampsia.
- Inhibits acetylcholine release, which may lead to hyporeflexia or drowsiness.
- ! Cave in renal impairment: Magnesium Toxicity
- Rare if renal function is normal.
- Clinical assessment for magnesium toxicity should be conducted every one to two hours.
- Check deep tendon reflexes and signs of paralysis or abnormal cardiac conditions.
- Serum magnesium levels should be monitored, especially in women with renal insufficiency.
- Therapeutic range for serum magnesium is 4.8 to 8.4 mg/dL.
- The antidote for magnesium toxicity is calcium gluconate.
- Calcium gluconate is used in cases of severe cardiac toxicity, such as cardiac arrest.
- 🚚 Rapid Delivery (do Ø wait for stabilization)
Hemolysis, Elevated Liver enzymes, Low Platelet count
- Microangiopathic hemolytic anemia
- Fragmented red cells (💔 Schistocytes) 📷
- ↑ bilirubin
- ↓ haptoglobin
- Thrombocytopenia (due to plts consumption)
Gestational Thrombocytopenia
- Harmless condition
- Presents in third trimester
- Platelet accumulation in spleen & placenta
- No symptoms
- Platelet number: 100,000 - 150,000
- Treatment not needed
- Might restrict epidural use
Development of systemic features of preeclampsia after 20 weeks gestation in a woman with pre-existing hypertension
reminder: chronic HT = before 20w
😉
Q. Which of the following statements are false in relationship with eclamptic seizures?
A. It can be the first symptom of preeclampsia.
B. The treatment will start after the MRI and CT results.
C. The delivery will be vaginal.
D. Magnesium sulfate is the best choice for preventing relapses.
E. It defines the occurence of coagulation disorder in a preeclamptic patient
ABCE
Q. * Which of the following drugs represents the main treatment for chronic hypertension associated with pregnancy? a. Calcium channel blockers b. Magnesium sulfate c. Central anti-hypertensives (methyldopa or clonidine) d. Diuretics e. Hydralazine
C
- Highest transmission risk in the third trimester (but most severe if infected in the 1st trimester)
- Only problematic if: primary infection during pregnancy
SEROLOGY ⇒ IgG+ & IgM+(both!!)/turn 2
IgM + | IgM - | |
IgG + | Follow up with IgG Aviditiy | No risk
! in severe
immunodepreson |
IgG - | IgM without
signiticance
The same as IgM (-),
IgG (-) | Advise to minimise
acquisition
Repeat serology in 2nd
and 3rd T |
↓ ⇒ follow up with: IgG Avidity test
⇒ If HIGH ⇒ Ø Risk (infection >3-5 month)
⇒ If LOW ⇒ RECENT infection ⇒ SPIRAMYCIN
⇒ >15w prior to gestation: Amniocentes. + PCR
⇒ PCR - : SPIRAMYCIN till birth
⇒ PCR + : Pyrimethamine + sulfadiazine + folinic acid
Q. Risk of transplacental transfer of toxoplasmosis is greatest in:
a. 1st trimester b. 2nd trimester c. End of pregnancy evolution d. Birth process e. In case of PROM
C
early: <2 yo
late: >2 yo

- FLUORESCENT microscopy
- DARK FIELD microscopy
- 🫀 NON-TREPONEMAL SEROLOGIC TEST (non-specific ⇒ cardiolipin reaction)
- VDRL
- RPR
- Treponema cannot be grown
- Tests for serum reaction to cardiolipin antigen
- Presence of syphilis antibodies leads to reaction
- May get false positive results due to conditions like lupus or viral infections
- Venereal Disease Research Laboratory (VDRL) test
- Rapid Plasma Reagin (RPR) test
- Results are either given as a specific measurement or simply reactive/non-reactive
- Continues until birth
- 🪱 TREPONEMAL SEROLOGIC TEST (specific)
- FTA-ABS (IgM + IgG)
- TP-EIA
- Identifies antibodies against particular treponemal agents
- Precise examination
- Fluorescent Treponemal Antibody Absorption (FTA-ABS)
- T. pallidum Enzyme Immunoassay (TP-EIA)
- Outcomes: “Active” or “Inactive”
- Most efficient during initial stage of the disease.
Non-Treponemal Serologic Tests
Treponemal Serologic Tests
Neurosyphilis? → Lumbar puncture ⇒ VDRL
LATENT syphilis → Treponemal serologic test +
- Signs: clinic + radiological
- 🩸 IgM ⇒ VDRL infant > mother
- 💉 CSF → VDRL
Penicillin G benzathine - 💪🏽I.M. (2,4 Mill. IU )
→ 1x / week for 2-3w
- Early syphilis→ day 1 + 8 (2 doses)
- Late syphilis → day 1, 8 + 15 (3 doses)


Shingles:
Dermatomal pattern: Symptoms often affect dermatomes from Th3 to L3.
- Pain: Dull, pulling, sometimes intense pain in the affected ganglion area.
- Paresthesia
- Vesicles
- Skin lesions are pinhead to rice-sized, clear blisters
- Vesicles are on an erythematous base.
♻️ SYSTEMIC acyclovir (or others)


- Confirm:
- Management: Infection during..
- First half → reassurance
- >20w → US (weekly!): if hyrops or anemia-signs (↑flow MCA): RBC transfusions (intrauterine)
Serology (IgM) or Amniocentesis + PCR (if sev. anemia signs)

↓


(*anemia signs)









(infection during FIRST trimester)
- ❤️ Congenital heart disease: patent ductus arteriosus, septal defects.
- 👁️ Eye lesions: microphthalmia, cataract, glaucoma, chorioretinitis.
- 👂 Hearing impairment: deafness.
+ blueberry muffin rash 📷
- 💀microcephalia
- 🫀myocarditis
- 🍑hepatosplenomegly, jaundice
- 🦴BM: Amegakaryocytic thrombocytopenic purpura
- 🧠
- autism/mental retardation
- epilepsy

Virus can be detect in:
- Pharynx: 7d before until 7 days after rash
- Blood: 7d before until day of rash
- Stool: 4d before until 4d after rash (in children w/ subclinical infection)
→ Most contagious from: day of rash until 7d after
⇒ Infection = lifelong immunity
Q. What part of pregnancy has the highest malformation risk for rubella infection?
a. 3rd trimester b. After 20 gestational weeks c. 1st trimester d. 2nd trimester e. 1 month before birth
c

⇒ Like EBV

- Monospot neg. (DDx EBV)
- non-specific
- ↑Lymphos
- ↑Liver markers
- Urine sediment → owls eye inclusion
- PCR
- Serology IgM/IgG (esp. screen in pregnancy!)
#1 Ganciclovir 🥫♻️ (iv) OR Val-Ganciclovir (oral)
→ resistent? → Foscarnet 🏎️ 🥅
→ alternative: Cidofovir

Serology + PCR ↑ risk if primary infection ⇒ Antibodies neg ⇒ PCR for confirmation (Øserology)
Serological Diagnosis:
- Viral antigen (ELISA)
- Viral DNA
- HSV in cell culture
Serological Markers:
- IgM appears early and can persist for 3-8 weeks.
- IgG appears after 7-21 days from primary infections and persists for an undefined period.
- Acute infection is characterized by the presence of IgM and a significant increase in IgG levels within 2-4 weeks.
Histopathological Diagnosis: Can be made from the examination of lesions.
Any History of genital herpes? (prior or during pregnancy) ⇒ ♻️ Suppressive Tx (Acyclovir): >36w until delivery
↓
Active genital lesions or symptoms (pain, burning)?
↓
+ yes: 🔪 C-section (after onset of labor)
- no: 🦪 vaginal can be considered
Routine First Pregnancy Visit: rubella, chickenpox, and syphilis
- Rubella: Detection of antibodies
- Chickenpox (Varicella): Identification of antibodies
- Syphilis: Using tests RPR/VDRL
Further Tests Depending on Medical Practice
- Toxoplasmosis, Herpes Simplex Virus (HSV), Parvovirus B19, Cytomegalovirus (CMV)
Hormonal Effects on the Urinary System
- Progesterone leading to slowed urine flow
- Softening of muscles in the urinary system
Potential Urinary Conditions During Pregnancy
- Silent urinary infections, bladder infections, or kidney infections
Most common bacteria: E. coli 🥇 Others: S. saprophyticus, GBS, enterococcus
first prenatal visit screening (via urinary culture)
- 🥐 pyelonephritis
- ⏲️ premature birth (infection → premature rupture of membranes)
Q. Asymptomatic bacteriuria
A. Is located in the lower urinary tract
B. It doesn't influence the pregnancy
C. Can induce a birth pattern, neonatal mortality, and morbidity
D. The treatment isn't necessary in all the cases
E. We administer oral antibiotics
A, C, E
Nitrofurantoin or Fosfomycin
→ adjust according to culture results
Pyelonephritis
- Manifests in 2% of pregnancies
- Common reason for hospital admission
Treatment
- Intravenous AB (broad-spec): Ceftriaxone, Cefepime, and the combination of Ampicillin-Gentamycin
- Administration of fluids iv
- Reappearance of the condition is common → Prophylactic antibiotics are often prescribed until childbirth
- 🪨 Lithiasis
Acute Liver Failure in Third Trimester
- Uncommon cause of acute liver failure during the third trimester of pregnancy
- Characterized by fat accumulation in liver cells
- Persistent nausea and vomiting
- Other symptoms can include jaundice or hepatic encephalopathy
- Lab results often show abnormal liver function tests (LFTs) and elevated bilirubin levels
- Immediate induction of birth along with additional supportive care
- Pregnancy progression can result in severe liver failure
- Most patients recover post-delivery.
2nd half of pregnancy
- Jaundice
- Colurice urine
- Discolored faces
- Itching, Nausea / Vomiting
- Absence (Ø) of
- hepatomegaly
- abdominal pain
- Signs tend to disappear in the postpartum period
Biological Picture:
- ↑Bile acids
- ↑ Conjugated bilirubin
- ↑ Alkaline phosphatase (AP)
- ↑ Transaminases
Ø Effect on Fetal Development!
- Antihistamines
- Cholestyramine
- Vitamin K
Fetal demise / Preterm birth
⇒ To prevent: deliver fetus when it reaches term
- classic signs: nausea/vomiting, pain
- ⭐Special: pain located in RUQ (displaced due to baby) 📷
spont. pain or on palpation
🦇 US 📷 (if inconclusive → MRI) ⇒ NEVER CT❗
Tx: 🔪 Surgery
- Diagnosis challenging in the second and third trimesters due to anatomical changes in the maternal body.
- Appendix position shifts upward and rotates during pregnancy.
- In the third trimester, it can be located near the right kidney.
- Pregnancy-related changes blur the symptoms.
- Progesterone reduces peritoneal irritation.
- Uterine contractions can facilitate germ spread and appendix perforation.
Q. Acute appendicitis in pregnancy: A. It is easy to diagnose, especially in the second and third trimester of gestations. B. The most important sign is nausea. C. The surgical treatment is necessary. D. If there is a delay of the diagnostic, the local infection tends to generalize. E. The incision for appendectomy is always done at the level of the McBurney point (classic incision).
C, D
Hypo/Hyperthyroidism → no screening needed
Hyperemesis Gravidum
- Linked to elevated hCG levels which activate the thyroid.
- Low TSH and potentially increased T4 levels can be observed.
- Thyroid tests are typically avoided in patients with Hyperemesis Gravidum.

- Pregnancy increase NYHA status by one level. 📷T
- Cardiopathy in NYHA class I or II is compatible with pregnancy.
- Types of cardiac problems:
- Mitral valve issues are the most frequent cardiac lesions in pregnancy.
- Stenotic lesions tend to cause more complications than insufficiencies.
- Pulmonary issues are the most common cardiac complication in pregnancy.
- Beta-blockers are the recommended treatment during pregnancy.
Q. The following regarding pregnancy and heart disease associations are true:
A. Pregnancy is not allowed for women suffering from cardiac insufficiency NYHA II class.
B. Pregnancy increases the NYHA classification by one grade.
C. Stenosis injuries determine complications.
D. Surgical treatment is crucial.
E. Pregnancy doesn't affect heart disease.
B, C
- 🫁 Resp. (pneumonia, TBC)
- 🩸 Blood → Anemia (iron/folate/B12) + DVT

Class | Medications |
A | None |
B | Argatroban, Fondaparinux, Clopidogrel, LMWH |
C | Aspirin (1st and 2nd trimesters), Heparin, Dabigatran (Direct thrombin inhibitor), Abciximab (Glycoprotein IIb/IIIa Inhibitor), Rivaroxaban (Anti-FXa) |
D | Aspirin (in 3rd trimester), Aggrenox (aspirin+dipyridamole), Warfarin (warfarin embryopathy) |
X | Warfarin (warfarin embryopathy) |
Maternal | Fetal | Adnexal | Idiopathic |
Preexisting or pregnancy-induced hypertension | Chromosomal abnormalities | Placenta praevia | 50% of cases have Ø evident cause |
Diabetes mellitus | Genetic syndromes | Retroplacental hematoma | |
Antiphospholipid syndrome | Viral, bacterial infections, etc. | Placental tumors (placental chorioangioma) | |
Thrombophilia | Metabolic diseases | Cord accidents (cord thrombosis) | |
Cardiac pathology with repercussions on placental perfusion | |||
Toxic substance consumption |
Q. Which of the following changes regarding intrauterine fetal death is correct? A. Vilous edema B. The disappearance of vilous capillaries C. Vascular changes, thrombosis D. Proliferation and stromal sclerosis E. All the answer are correct
E
- ⬇️ Intra-uterine growth restriction (see later)
- 🌊 Abnormal amniotic fluid volume (see later)
- 🔴 Fetal-maternal incompatibility (see before)
Q. Which of the following clinical elements define imminence of abortion (threatened abortion)? a. Painful UC, metrorrhagia, without uterine cervix alterations b. Reduced bleeding with clots, opened uterine cervix c. Opened cervix d. Ruptured membranes e. Fever, abdominal pain
A
- Labor begins when ≥1 regular uterine contractions every 10 minutes
- Cervix modifications (effacement & dilation up to 10cm)
- Gelatinous plug is expelled
- Membrane rupture may occur spontaneously.
Braxton-Hicks Contractions
= Contractions but no cervical modifications.
- Typically aren't felt until the 3rd trimester.
- Can be detected or palpated as early as 18 weeks.
- They are irregular in nature.
- Usually do not intensify or occur more frequently as time progresses.
- Relief with anti-spasmodics
Dgx workup:
The initial assessment includes an ultrasound and cervix check.
→ A follow-up might involve a non-stress test.
→ If the test results are reactive, no specific intervention is typically required; patients can usually be sent home.
Stage | Description | For First-Time Mothers (Nulliparous) | For Those With Previous Deliveries (Multiparous) |
1. Stage (Latent) | Onset of labor leading up to around 4-6 cm cervix dilation | Typically less than 20 hrs (commonly 10-12 hrs) | Often less than 14 hrs (commonly 6-8 hrs) |
1. Stage (Active) | From around 4-6 cm up to when the cervix dilation is fully 10 cm | About 4-6 hrs (usually more than 1-1.2 cm every hr) | About 2-3 hrs (often more than 1.2-1.5 cm every hr) |
2. Stage | When the cervix dilation is fully dilated until the delivery of the baby | Typically less than 2 hrs (3 hrs if under epidural) | Often less than 1 hr (2 hrs if under epidural) |
3. Stage | Following the baby's birth until the placenta is delivered | Often less than 30 minutes | Generally faster in multiparous, with exceptions in the 3rd stage |
4. Stage (Immediate postpartum)* | After the placenta's delivery. Activities include monitoring vital signs and bleeding, ensuring the uterus is contracted, inspecting the placenta for completeness, and noting the 3rd and 4th stages are most dangerous due to potential hemorrhage. |
- first postpartum hour.
- Monitor vital signs and bleeding; Repair lacerations if necessary.
- Ensure the uterus is contracted by palpating it and monitoring uterine bleeding.
- Inspect the placenta for completeness and check the umbilical cord for the presence of 2 arteries and 1 vein.
- Pay close attention to the 3rd and 4th stages of labor, as they can be dangerous to the mother, particularly in terms of hemorrhage.
Phase | Name | Characteristics |
0 | Myometrial Silence | |
- Uterine muscles silent | ||
- Cervix rigid, closed | ||
- Lasts from week 36 to 38 | ||
1 | Myometrial Activation | |
- Uterus preparing for labor | ||
- Softening, maturation of cervix | ||
- Oxytocin receptors and Gap Junctions | ||
2 | Stimulation of Labor | |
- Uterotonines initiate contraction | ||
- Dilatation of cervix, delivery | ||
3 | Puerperium | |
- Contractile activity for involution | ||
- Restoration of fertility |
↑Contraction | ↑Relaxation |
Estrogen | Progesterone ( +hCG) |
Oxytoxin | CRH (→ACTH→adrenal) |
Prostaglandin (E2) | Prostacyclin I2 |
Alpha-R | Beta-R |




Defintion: Relationship Long axis baby to long axis mother
📷 ⇒ Longitudinal, Oblique, Transverse
Fetal Presentation
- Description: Part of the fetus overlying the pelvic inlet.
- Most Common Presentation:
- Type: Longitudinal
- Specific: Cephalic
- Breech Presentation:
- Type: Longitudinal
- Specific: Buttocks presenting
- Vertex
- Sinciput (military)
- Brow
- Facial
- Vertex Presentation
- Fetal vertex is the presenting part.
- Note: This is a subtype of cephalic presentation and is considered the NORMAL presentation.
- Malpresentation
- Presenting part is not the vertex.
- Usually require C-section
- Types include:
- Breech
- Transverse/oblique lie
- Face or brow presentation
- Occiput (O): The most common cephalic presentation, often referred to as vertex or flexed head presentation. The skull is flexed towards the trunk, with the small fontanelle as the central point, engaging with a diameter of suboccipito-bregmatic (~9.5 cm).
- Brow (B): Known as sinciput or military presentation, it involves an indifferent attitude of the skull to the trunk, with neither flexion nor deflection. The large (bregmatic) fontanelle is central in this presentation, and the engagement diameter is suboccipito-frontal (~11.5 cm).
- Nose (N): This is a brow presentation characterized by a moderate deflection of the fetal skull, with the forehead at the center of the presentation. The diameter of engagement is mento-vertical (occipito-mental ~13-13.5 cm), which is not compatible with a vaginal delivery at term.
- Mentum (M): Also called facial presentation, it involves an extreme deflection of the skull, with the chin (mentum) presenting. The engagement diameter is submentobregmatic (~9.5 cm).
- Sacrum (S): For breech presentations, where the buttocks or feet of the fetus enter the pelvis first.
- Acromion (A): For humeral presentation, which involves the shoulder of the fetus.
- Complete breech presentation (full-flexed): The fetus's pelvis is in the pelvic inlet plane, with the lower limbs in a "Turkish position" or "cannonball position." This means the thighs are flexed on the abdomen, legs crossed, and feet flexed on the legs.
- Frank breech presentation (extended): In this presentation, the fetus presents with the pelvis, while the lower limbs are extended along the body, resembling a "splint" position. The thighs are flexed on the abdomen, and the legs are extended.
- Incomplete breech: One of the baby's legs is flexed, while the other is in extension.
- Footling breech: This presentation is less common and may involve the fetus presenting with one or both feet first, and sometimes even with the knees first (referred to as knee presentation).
- Occurs when the fetus is positioned transversely in the uterus. This means that the baby's shoulder comes into the lower segment of the uterus. This presentation is relatively rare, with a frequency of about 0.5% (approximately 1 in 300 pregnancies near term).
- In this presentation, the two fetal poles are located on the two flanks of the maternal abdomen, and the reference point for the shoulder is the acromion.
- It's important to note that in about 15-17% of these cases, the presentation may change from a transverse lie to a different presentation at the onset of labor.
- Shoulder presentation is more commonly found in multiparous patients (those who have had multiple pregnancies).

Step | Process | Details |
1 | Adjustment | The pregnant woman adjusts to the hands of the examiner; assessing the consistency of the uterine wall. |
2 | Delimitation | Delimiting the high uterine fundus (HUF) and comparing it to several markers: pubic symphysis, umbilicus, xiphoid appendix. |
3 | Palpation (Lower Uterus) | Palpation of the lower pole of the uterus (the inferior segment) to establish presentation.
- Skull: Round, regular, undepressible, rough pseudo-tumoral formation.
- Pelvis: Irregular pseudo-tumoral formation, uneven consistency, depressible.
- Transverse Layout: The lower segment is empty. |
4 | Uterine Fundal Region Palpation | Revealing the fetal pole, which is identified at this level. |
5 | Uterine Flank Palpation | - Fetal Back: Regular plane, rough surface, convex, undepressible.
- Small Fetal Parts: Irregular region, depressible. |
Fetal position refers to the relationship between the fetal presenting part the right, left or transverse side of maternal pelvis. In the case of vertex/occipital presentation, the positions are as follows:
- Left occiput anterior (LOA) - 60% 🥇
- Right occiput anterior (ROA) - 20%
- Right occiput posterior (ROP) - 15%
- Left occiput posterior (LOP) - 5%
- Left occiput transverse (LOT)
- Right occiput transverse (ROT)
These positions describe the orientation of the baby's head as it descends through the birth canal during labor.
- Mobile: Presentation did not make contact with the pelvic inlet and is mobile at the vaginal examination.
- Applied: Presentation took contact with the pelvic inlet but can be displaced (mobilized) at the vaginal examination.
- Fixed: Presentation took contact with the pelvic inlet and cannot be mobilized at the vaginal examination.
- Engaged: The widest transverse diameter of the presentation passes through the pelvic inlet (sup. strait).
- Descended: Presentation reaches the pelvic outlet (inferior straight).
After a failed attempt to mobilize, the two fingers can be slightly opened between the presentation and the concavity of the sacrum (Farabeuf 3 sign).
The two palpating fingers of the examiner can be inserted between the presentation and the concavity of the sacrum (Farabeuf 2 sign or classical Farabeuf sign). 📷
Only one of the two palpating fingers of the examiner can be inserted between the presentation and the concavity of the sacrum (Farabeuf 1 sign).
- Farabeuf 3: This space allows the insertion of three fingers, indicating that the presentation is fixed at most.
- Farabeuf 2: This space allows the insertion of two fingers, indicating that the presentation is engaged and has passed through the pelvic inlet.
- Farabeuf 1: This space allows the insertion of one finger, indicating that the presentation is descended, possibly reaching the pelvic outlet or inferior straight.
Fetal Station:
- Description: Assessment of the leading edge of the presenting part of the fetus.
- Measured in centimeters of the leading edge of the presenting part.
- Reference Point: Ischial spines of the maternal pelvis.
- Above or Below: Measurements are either above or below the level of the ischial spines.
- Significance:
- Station 0 (0 centimeter): At level of ischial spines 📷 → engaged
- Negative: Leading edge is inside the uterus → mobile,applied or fixed
- Positive: Leading edge is outside the uterus →descended
- Range: 5 to +5.
Presentation Type | Description | Characteristics |
Synclitism | The sagittal suture is located midway between the promontory and the pubic symphysis. The plane of the biparietal diameter is parallel to the plane of the inlet. | - Sagittal suture centered between promontory and pubic symphysis.
- Biparietal diameter plane parallel to the inlet. |
Asynclitism - Anterior | Lateral flexion of the fetal head causes the anterior parietal bone to present first. | - Lateral flexion leads to posterior inclination of the head.
- Sagittal suture closer to the promontory. |
Asynclitism - Posterior | Lateral flexion of the fetal head causes the posterior parietal bone to engage first. | - Lateral flexion leads to anterior inclination of the head.
- Sagittal suture closer to the pubic symphysis. |
Cervical assessment:
⇒Maximum Score: 13
Cervical Status | 0 | 1 | 2 | 3 |
Dilatation | Closed | 1-2 cm | 3-4 cm | > 5 cm |
Effacement | < 30% | 30-50% | 50-80% | > 80% |
Station | -3 | -2 | -1 or 0 | ≥ +1 |
Consistency | Firm | Intermediate | Soft | - |
Position | Posterior | Intermediate | Anterior | - |
Progresses → until 10cm
Effacement:
- Refers to the thinning of the cervix during the labor process.
- Normal cervix: 4 cm in length.
- As labor progresses, the cervix undergoes changes: it thins out, softens, and shortens.
"Bloody Show":
- This term describes a discharge that contains blood-tinted mucus.
- It is linked to the commencement of effacement.
The cervix can be
firm (similar to the feel of a nose), medium (akin to lips), or soft (resembling the texture of butter). → The soft consistency is typically expected at the time of delivery.
posterior, anterior, midposition
- Engagement:
- This is the initial step where the widest diameter of the fetal head (the biparietal diameter) aligns with the widest diameter of the maternal pelvis. Essentially, the baby's head settles or "engages" into the mother's pelvis, beginning its journey through the birth canal.
- Flexion:
- As the baby's head comes into contact with the cervix and pelvic floor, it bends forward, tucking the chin to its chest. This movement ensures the smallest diameter of the fetal head (the suboccipitobregmatic diameter) presents to the pelvis, aiding in the progression of labor.
- Descent:
- This refers to the downward movement of the fetus through the birth canal. It is influenced by several factors, including uterine contractions, maternal pushing, and the resistance of the pelvic floor.
- Internal Rotation:
- The fetal head, initially aligned transversely, rotates to align with the mother's sagittal plane. This is largely due to the shape of the maternal pelvis and the forces from the pelvic muscles. By the end of internal rotation, the baby's head is typically facing the mother's back.
- Extension:
- Once the fetal head reaches the base of the pelvis, it begins to extend (tilt backwards). This allows the head to navigate the curve of the pubic symphysis, leading to the birth of the head with the face following the occiput.
- External Rotation/Restitution:
- After the head is born, it rotates back to its original transverse position (restitution) and then continues to rotate even further (external rotation) to align the baby's shoulders with the mother's pelvis.
- Expulsion:
- Following the external rotation, the anterior shoulder is delivered under the pubic symphysis, followed by the posterior shoulder. The rest of the body then follows easily, completing the birth process.
- Generalized flexion (= normal attitude)
- Skull moderately flexed on the trunk
- Spine slightly bent anteriorly
- Forearms flexed on the arms anterior to the chest
- Thighs flexed on the trunk
- Lower legs flexed on the thighs and crossed
- Cephalic extremity and the pelvis with flexed lower limbs form an ovoid shape
- Attitude of the cephalic pole in relationship with the spine:
- Flexed (physiological, tendency to assume fully flexed posture)
- Antermediate (neutral or "military")
- Moderate extension
MCQs:
* The diameter of engagement of the fetal skull in cranial presentation is:
- A. Occipito-bregmatic
- B. Suboccipito-bregmatic
- C. Occipito-frontal
- D. Supraoccipito-mentonier
- E. Supraoccipito-obregmatic
B
The transverse lie:
- A. Is a distocyc lie
- B. Occurs in 45% of all monofetal deliveries
- C. Can occur in the presence of a voluminous uterine fibroma
- D. Allows the vaginal delivery up to 3500 g
- E. Is a eutocyc lie
AC
* The smallest antero-posterior diameter of the fetal skull is:
- A. The occipito-mentonier diameter
- B. The occipito-frontal diameter
- C. The suboccipito-bregmatic diameter
- D. The submentum-bregmatic diameter
- E. The biparietal diameter
C
Select the correct answers:
- A. Vaginal delivery by conduplicatio corpore mechanism is possible with live, term, normal weight fetuses after a positive diagnostic of transverse lie with ruptured membranes
- B. Transverse lie and ruptured membranes with a live, term, live fetus implies emergency c-section
- C. Breech presentation has the sacrum as reference (not hallmark)
- D. One of the reasons for increased obstetrical trauma with vaginal delivery is that the most voluminous part of the foetus (the foetal head) is the last one to be delivered
- E. In complete breech the legs are parallel with the body of the foetus
BCD


Which of the following are false?
- A. Presentation is defined as the part of the fetus that takes contact with the pelvic inlet (superior strait).
- B. Presentation takes into consideration a fix point of the pelvic inlet and the foetal back.
- C. Position of the fetus takes into consideration a fix point from the presentation relative to the right or left half of the maternal pelvis.
- D. Foetal lie represents the orientation of the presentation with respect to the sciatic spines.
- E. For each fetal position there are three varieties of positions: anterior, transverse and posterior.
BDE (= false statements)





❗ Depends on Bishop Score ⇒ 📷
Bishop >6 ⇒ OXYTOCIN (+- Amniotomy if Ø spont. rupture [ROM])
Oxytocin:
- Potential complications:
- Hyperstimulation or tetanic contraction
- Uterine muscle fatigue or uterine atony leading to PPH (postpartum hemorrhage)
- Vasopressin-like action causing anti-diuresis
Amniotomy:
- Amniotomy: Artificial rupture of membranes to stimulate prostaglandin synthesis and secretion
- More efficient when combined with intravenous oxytocin
- Considered as an initial measure if the cervix is open and ripped and the head is present at the cervix
→ oxytocin can also be used if inadeq. contractions during labor (= augmentation of labor)
Side Effects of Oxytocin:
- Increased Contraction Rate (Tachysystole):
- Observing more than 5 contractions within an average of 10 minutes over a half-hour span.
- Potential risks include hypox and acidosis for the fetus.
- There's a minimal chance it might lead to a rupture of the uterus.
- Suggested management: decrease oxytocin dosage or incorporate terbutaline.
- Salt Level Discrepancies (Hyponatremia):
- Has molecular similarities to ADH.
- Decreased Blood Pressure (Hypotension):
- Oxytocin can cause the blood vessels to relax.
- Tiredness/Fatigue in Mothers:
spinal / epidural 📷 →bupivacaine + fentanyl
- Maternal:
- Obstructive tumors of the pelvic canal (pelvic cyst or fibroid, placenta praevia, neoplasms, bone tumors)
- Active herpetic lesions on vulva
- Invasive cervical cancer
- Previous uterine surgery (most common - C/S)
- Maternal medical conditions (cardiomyopathy, eclampsia, HELLP syndrome)
- Transmissible disease (poorly controlled HIV, B Hepatitis)
- Previous 3rd / 4th perineal tear
- Pregnancy obtained after treatments for infertility
- Maternal-fetal:
- Failure to progress
- Antepartum hemorrhage (placenta praevia, vasa praevia, placental abruption)
- Maternal diabetes with a fetal estimated weight > 4500g
- Cephalopelvic disproportion
- Fetal:
- Abnormal fetal heart tracing
- Malpresentation (breech presentation, transverse lie or oblique lie, cord prolapse)
- Congenital anomalies
- Multiple gestations (twin pregnancy- when the first fetus is not a cephalic presentation)
- Intrauterine growth restriction with very low birth weight.
Short-term:
→ Classics
Complications related to anesthesia:
- Hemorrhage (average blood loss ~ 1000ml)
- Infection (UTI, wound, endometritis) - Single dose prophylactic antibiotic should be used
- Injury to surrounding structures (bowel, bladder, ureter, uterus)
- Thromboembolism (DVT, PE)
- Increased recovery time (hospitalization period)
- Maternal mortality (<0.1%)
Long-Term:
- Scarring
- ↑Risk in subseq. prengnacy → uterine rupture, placenta previa/accreta, placental abruption
- Risk of uterine rupture (<1%) with low transverse incision.
⇒ often C-section (if prior vertical (classic) incison → C-section mandatory! if lower uterine transverse → trial of labor after cesarean (TOLAC)
uterine rupture:
Indications:
- Fetal:
- Atypical or abnormal fetal heart rate tracing, evidence of fetal compromise
- Consider in cases of prolonged second stage due to poor contractions or failure of fetal head rotation
- Maternal:
- Need to avoid voluntary expulsive effort in conditions such as cardiac, cerebrovascular disease, eclampsia, or previous uterine surgery
- Exhaustion, lack of cooperation, and excessive analgesia may impair pushing effort
Devices: 📷
- Forceps:
- Obstetric tool for prehension, traction, and expulsion of the fetal skull in cases where expedited completion of birth is necessary due to maternal or fetal reasons.
- Vacuum extraction:
- Obstetric tool for traction and flexion used to extract the fetus during the expulsion stage of labor when expedited completion of birth is necessary due to maternal or fetal reasons.
- Serves as an alternative to forceps delivery and aids in maternal pushing.
Forceps | Vacuum Extraction | |
PROS | - Higher overall success rate for vaginal delivery
- Decreased incidence of fetal morbidity | - Easier to apply
- Less anesthesia required
- Less maternal soft-tissue injury compared to forceps |
CONS | - Greater incidence of maternal injury | - Contraindicated if fetus at risk for coagulation defect (fetal bleeding)
- Suitable only for vertex presentations
- Maternal pushing required
- Contraindicated in preterm delivery |
= rupture of the amniotic sac

- May occur spontaneously after onset of labor: SROM
- Before onset of labor (pre-labor): PROM
- Before 37 weeks (premature) + pre-labor: PPROM
- Artificial (amniotomy) rupture: AROM
↓GA → ↑Latency → Choriamnionitis
- Nitrazine test: 📷
- Application of vaginal secretion to Nitrazine test strips.
- Amniotic liquid displays a heightened pH interval, between 7.0 and 7.3.
- The testing strip adopts a blue hue when the pH level of the fluid is elevated.
- Fern test: 📷
- Mixing vaginal secretion with estrogen.
- Upon Rupture of Membranes (ROM), a distinctive "fern-shaped" design is visible microscopically.
- Dye tests
- Introduction of dye directly into the amniotic pouch via the belly.
- When the test is positive, a tinted liquid manifests in the vaginal area.
ROM before contractions after 37w (Øsame as PPROM)
↑Risk of chorioamnionitis
↓

ROM before contractation before 37w
→ 30% of preterm birth present like this
- Preterm
- Placental detachment
- Amniotic infection
- Umbilical cord prolapse
👉🏼 digital (vaginal touch)

- 🎒 Chorioamnionitis
- 🥐 Asymptomatic bacteriuria & UTI
- 👛 Postpartum endometritis
- 📛 Neonatal sepsis
ALL woman at 35-37w → take vaginal & anorectal swabs → GBS culture
- confirmed positive culture during pregnancy or GBS infect. detected during prengancy.
- Prior record of a neonate affected by GBS.
- GBS status unknown at birth + accompanied by any of these symptoms:
- Fever
- Preterm delivery.
- Early rupture of the membranes prior to labor onset (PPROM).
- Extended time of ROM, lasting over 18 hours.
- Detected GBS through intrapartum testing (NAAT).
Penicillin allergy?
↓
↓
No ⇒ #🥇 ⇒ 🎸 Ampicillin / ✏️PenicillinG
Yes → risk of anaphylaxis?
↓ ↓LOW risk (rash) ⇒ 1stG🦑: Cefazoline ↑HIGH risk ⇒ 🚌Vanco (r)
Infection of chorion, amnion and amniotic fluid
Infection → Chorion, amnion, amniotic fluid
⇒ typically AFTER ROM (”protection shield” lost)
Polymicrobial → G- & G+
GBS
- Systemic
- 🤒 Fever
- ❤️Tachycardia → maternal AND FETAL (>160) 📷
- ⚪ Leukocytosis
- Rarely → 📛 bacteremia (GBS, E.coli)
- Local
- uterine TENDERness
- PURULENT/bad-smelling amniotic fluid
⇒ Gold standard: 🔬Gram + 🧫Culture of amniotic fluid
usually 🔪 C-section (vaginal only if mother + fetus stable)
↓
🎸Ampi plus 🤺Genta +/- 🚇/🧼 Metro or Clinda (if C-section)
Intrapartum → Ampi + Genta
C-section → Clinda / Metro (to cover anerobes)
only if PPROM <34w ⇒ Prophylactic 💊 ABs
(Ø prophylaxis if >34w)
⇒ see: Preterm pre-labor rupture of membranes (PPROM)
- Childbirth prior to completing 37 weeks.
- Risk factors
- Primary RF: History of premature delivery.
- Additional RF:
- Multiple gestation
- Infections like UTI or asymptomatic bacteriuria.
- Cervical abnormalities
- Shortened cervical lenght (often referred to as cervical insufficiency).
- Past procedures on the cervix (like for CIN) done less than 6 months ago.
- Excessive amniotic fluid (polyhydramniosis).
- Habitual tobacco use.

+- premature rupture of membranes (PPROM)

*Other tocolytics: Nitric axoid (Nitro); Oxytocin antagonist (Atosiban)
Q. Which of the following statements are false?
A. Beta-mimetics are administered in the case of premature labour up to 37 weeks. B. Beta-mimetic medication is administered in the event of premature labour up to 34 weeks. C. Calcium channel inhibitors are not tocolytic. D. Atosiban is an antiocitocic. E. Mg sulphate is administered as a tocolytic in preterm labour in a bolus of 1-2 mg.
AC (=false)
- Progesterone therapy ⇒ Preserves a calm uterus → ↓ ROM likelyhood.
- Cervical cerclage ⇒ Operative enforcement of the cervix. 📷
Late ≥41w
Post ≥42w
- perinatal mortality
- big baby (macrosomnia)
- dysmaturity syndrome
- Postmaturity syndrome: Fetal weight loss (not below 10th percentile), reduced subcutaneous fat, scaling, dry skin from placental insufficiency, long thin body, open-eyed, alert and worried look, long nails, palms and soles wrinkled.
- Risks in postterm pregnancies: Meconium aspiration syndrome, intrauterine infection, asphyxia, placental insufficiency, placental aging and infarction with subsequent fetal death, macrosomia followed by dystocic complications if a vaginal delivery is attempted, fetal distress, operative deliveries, stillbirth.
41w → Expectant 42w or Fetal abnormalities → C-section / Induction Maternal age >40y → Delivery at 40w
Question: Which of the following mechanisms listed triggers premature birth?
- A. Overactive uterus
- B. Premature rupture of the membranes
- C. Urogenital infections
- D. Bleeding occurring in the third trimester of pregnancy
- E. Hyperprolactinemia
ABC
Question: Which of the following statements are false regarding the prevention of premature labor in 34 to 37 weeks?
- A. Beta-mimetics are administered in the case of premature labor up to 37 weeks
- B. Beta-mimetic medication is administered in the event of premature labor up to 34 weeks
- C. Calcium channel inhibitors are not tocolytic
- D. Atosiban is an antiotocic
- E. Magnesium sulfate is administered as a bolus of 1-2 mg in preterm labor
AC = false
Question: Which of the following are false regarding the latent period (latency) in a case of premature rupture of membranes?
- A. The smaller the gestational age, the smaller the latency
- B. The smaller the gestational age, the bigger the latency
- C. The bigger the gestational age, the smaller the latency
- D. When the latency prolongs the infectious risk is smaller
- E. When the latency prolongs the infectious risk is higher
AD

placental / during delivery (like HIV)
The greatest transmission risk to fetus ⇒ 3rd trimester

- Classic signs of Hepatitis (Hepatomegaly, jaundice, dark urine, pale stools, bleeding, neuro, etc)
- “Rheuma”-Prodrome

🕰️ CHRONIC HEPATITIS
- adults ⇒ rarely (5-10%)
- 🐣 NEWBORNS ⇒ very common! (90-95%) → esp if infection during birth
placental (↓common than hepB) or during birth (intrapartum)
(placental only if ↑↑viremia)

Ø intervention ↓ vertical transmission → only prevention = tx of chronic HepC before pregnancy
during DELIVERY 🚚 (Øplacental)

Conjunctivitis → 1-2w postpartum
Pneumonia → 4-12w postpartum
First prenatal visit ⇒ Screening: cervical swab → NAAT)
If neonatal (Øscreening, transmission during delivery): Conjunct. & Nasopharynx swab → NAAT
- During Screening:
- Neonatal:
🦅 Azithromycin (p.o. 1g single dose) ⇒ ØDoxy🕷️
+partner tx
→ repeat testing after 2w
🦅Erythromycin (p.o.)

Dgx: Swab → NAAT
Tx:
Ceftriax + Azithromycin
For neonatal: Prophylactic erythromycine eye drops at birth or if present Ceftriaxone (iv/im single dose)
- usually spread via 🦟mosquito bite.
- Especially risky during the 1st trimester.
- Mothers who contract the virus often show no symptoms.
- Virus targets the 🧠fetal brain:
- Smaller than normal head size.
- Diminished thickness of the brain layers.
- Solid deposits observed in the brain.
→ It's typical for babies to have a 🔒closed anterior fontanelle.
- Dgx method: PCR analysis of fluids like baby's blood, urine, or spinal fluid.
- Tx strategy: Supportive methods.
- Protection measure: Refrain from trips to high-risk areas.
- Key areas of transmission: Mainly Central and South America
Q. An infectious disease can affect the fetus or the neonate by:
A. Transplacental transfer of germs or toxins B. Damaging the placenta C. Upward infection - chorioamnionitis D. Postpartum uterine infection E. After delivery through milk and breastfeeding
ACE
Normal: 110-160 BPM
Bradyc: <110
Tachyc: >160
Short acceleration = benign (due to fetal movement)
Persistent tachycardia 📷⇒ rule out causes (i.e. anemia, maternal infection)
Variability is due to activity of the autonomic nervous system
Classification: 📷
Classification | Criteria |
Category I | - Heart rate baseline: 110 to 160/min |
- Moderate variability | |
- Absence of late or variable deceleration | |
Category II | - Doesn't fulfill Category I/III parameters |
Category III | - Heart rate: Bradycardic |
- Sinusoidal pattern | |
- Recurrent variable or late deceleration |
- 🚿 O2 + Fluids (maternal) → ↑perfusion +O2 to fetus
- ⬇️ Pressure
- POSITIONAL CHANGE
- STOP uterine CONTRACTIONS → stop oxytoxin, → consider tocolytic (terbulatin)
- Prepare 🚌Delivery→ 🔪C-section
- Green amniotic fluid (meconium)
- Doppler changes in umbilical artery (i.e. reversal of flow)
- Prolapse of the umbilical cord is a critical obstetric emergency characterized by the descent of the cord to a level adjacent to or below the presenting part, resulting in compression of the cord between the presenting part and the pelvis.
- The risk to the fetus is the compromised blood flow to and from the placenta, leading to hypoxia caused by physical compression or spasm of the blood vessels in the cord.
- Cord prolapse outside the vagina can also result in colder temperatures, which may induce spasm of the blood vessels in the cord.


- The most common method of diagnosis is through vaginal examination ⇒ Visible or palpable cord.
- FHR changes (variable decelerations, bradycardia, or both).
- The diagnosis of cord presentation can be made in cases with predisposing factors before rupture of the membranes by ultrasound.
- Cord-Decompression (immediate)
- Alleviate pressure on the presenting part on the cord by placing a digit in the vagina. Maintain this position until cesarean section.
- Keep the cord warm and moist by replacing it into the vagina and applying warm saline soaks.
- Position the mother in Trendelenburg or knee-to-chest position.
- Delivery ⇒ emergency C-section
it fetal demise or too premature (<22 GW), allow labour & delivery
Q. *The treatment for acute fetal distress does not include
- A. Myometrial relaxants
- B. Rapid delivery via C-section
- C. Induction of labor
- D. Lying on the left site
C
Dystotic delivery refers to the disturbance of the delivery mechanism through difficulties during labor, which can endanger the life of the mother and fetus. Dystocia is defined as any abnormality at birth of the cervix, uterus, fetus, and maternal pelvis, or combinations thereof.
Stage | Description | For First-Time Mothers (Nulliparous) | For Those With Previous Deliveries (Multiparous) |
1. Stage (Latent) | Onset of labor leading up to around 4-6 cm cervix dilation | Typically less than 20 hrs (commonly 10-12 hrs) | Often less than 14 hrs (commonly 6-8 hrs) |
1. Stage (Active) | From around 4-6 cm up to when the cervix dilation is fully 10 cm | About 4-6 hrs (usually more than 1-1.2 cm every hr) | About 2-3 hrs (often more than 1.2-1.5 cm every hr) |
2. Stage | When the cervix dilation is fully dilated until the delivery of the baby | Typically less than 2 hrs (3 hrs if under epidural) | Often less than 1 hr (2 hrs if under epidural) |
3. Stage | Following the baby's birth until the placenta is delivered | Often less than 30 minutes | Generally faster in multiparous, with exceptions in the 3rd stage |
4. Stage (Immediate postpartum) | After the placenta's delivery. Activities include monitoring vital signs and bleeding, ensuring the uterus is contracted, inspecting the placenta for completeness, and noting the 3rd and 4th stages are most dangerous due to potential hemorrhage. |
- Dynamic dystocia (↓contraction)
- Obstructive
- Bone dystocia
- Soft part dystocia
- Fetal dystocia
- Tumors causing dystocia
- Adnexal dystocia
- Umbilical cord
- Membranes + AF
Protected labor = labor phase takes more time
Labor arrest = Labor phase does progress further (secondary arrest)
Phases | Criteria |
Protracted Latent Phase | - Dilation less than 6 cm |
- Over 20 hours for first-time parenthood (nulliparenty) | |
- Over 14 hours for those with multiple parenthood experiences (multiparenty) | |
Protracted Active Phase | - Dilation of more than 6 cm |
- Dilation speed below 1 cm/hour | |
Arrested Active Phase | - No change in cervix for 4 or more hours despite strong contractions |
- No change in cervix for 6 or more hours in the absence of strong contractions |
Stage | Description | For First-Time Mothers (Nulliparous) | For Those With Previous Deliveries (Multiparous) |
1. Stage (Latent) | Onset of labor leading up to around 4-6 cm cervix dilation | Typically less than 20 hrs (commonly 10-12 hrs) | Often less than 14 hrs (commonly 6-8 hrs) |
1. Stage (Active) | From around 4-6 cm up to when the cervix dilation is fully 10 cm | About 4-6 hrs (usually more than 1-1.2 cm every hr) | About 2-3 hrs (often more than 1.2-1.5 cm every hr) |
2. Stage | When the cervix dilation is fully dilated until the delivery of the baby | Typically less than 2 hrs (3 hrs if under epidural) | Often less than 1 hr (2 hrs if under epidural) |
3. Stage | Following the baby's birth until the placenta is delivered | Often less than 30 minutes | Generally faster in multiparous, with exceptions in the 3rd stage |
4. Stage (Immediate postpartum) | After the placenta's delivery. Activities include monitoring vital signs and bleeding, ensuring the uterus is contracted, inspecting the placenta for completeness, and noting the 3rd and 4th stages are most dangerous due to potential hemorrhage. |
An increased BMI is assoc. with a prolonged 1st stage of labor!
Other causes:
- General causes:
- Neuro-hormonal disorders
- Obesity
- Preeclampsia (PE)
- Anaemia, avitaminosis
- Local causes:
- Uterine hypoplasia
- Uterine malformations, scars, tumors
- Polyhydramnios
- Gemellar (twin) pregnancy
Q. Which of the following represents local causes of dynamic dystocia?
A. Pre-eclampsia B. Polyhydramnios C. Uterine hypoplasia D. Obesity E. Multiple pregnancies
BCE
ONLY amniotomy if membranes Ø spontaneously ruptured yet
Active arrest → 🔪C-Section Protracted latent → 🏠home or 🏥 inpatient (→ oxytocin)
- “STUCK”
- Cephalopelvic disproportion: Fetal head to big for pelvis of mother
- Malposition of fetus (esp. occipitoposterior)
- ↓ PUSHING
- contractions Ø adequate
- effort of mother Ø adequate
- Bone dystocia
- Soft part dystocia
- Fetal dystocia
- Fetal excess due to macrosomia or generalized edema.
- Partial excess includes hydrocephaly and torso enlargement (goitre, hydrothorax, ascites).
- Limb procedence adjustment challenges during delivery may necessitate limb repositioning or cesarean section.
- Tumors causing dystocia (uterine/pelvic)
- Fibroids
- Ovarian Tumors
- Adnexal dystocia
- Umbilical cord
- Dystocia due to umbilical cord abnormalities
- Prolonged labor, lack of progress in presentation
- Possible complications: cord rupture, placental decollation, nuchal cord (cord wrapped around the neck)
- Umbilical cord in front of the presentation with intact membranes
- Cord descent causes compression between presenting part and cord
- Management: position mother in Trendelenburg or knee-to-chest position, alleviate pressure with vaginal digit, maintain until C/S
- In cephalic presentation: lift the skull above the cord; in pelvic presentation: attempt repositioning between contractions
- If fetal demise or too premature (<22 weeks), allow labor
- Cord tightening triggers fetal distress, possible intrauterine fetal death
- Membranes + Amniotic fluid
- Abnormal resistance of membranes
- Rupture may not occur upon complete dilation
- Prolonged labor or premature placental separation may occur
- Artificial rupture of membranes recommended at 4-6 cm dilation
- Polyhydramnios
- Can lead to dynamic dystocia
- Artificial rupture of membranes recommended at 3-4 cm dilation
- Puncture between uterine valve or speculum examination to avoid excessive loss of amniotic fluid
- Oligohydramnios
- Can lead to long, difficult labor with irregular uterine contractions
⇒ Both = Obstacle to fetus
⇒ 💊 Oxytoxin → ↑contraction or ⇒ “EVACUATE”
🦪 vaginally → Forceps/Vacuum 📷
🔪C-Section
- Symmetrical modifications
- Small pelvis due to developmental stop (infantile pelvis)
- Large pelvis due to excessive development
- Dysplastic pelvis (achondroplasia)
- Pelvis with aplasia of both sacral wings
- Double oblique pelvis - Robert ovalar
- Asymmetrical modifications
- Pelvis with aplasia of one sacral wing
- Symmetrical or asymmetrical modifications
- Covered pelvis due to modifications in the position of the spine
- Rachitic pelvis
- Osteomalacic pelvis
- Pelvis with ankylosing spondyloarthritis
- Kyphotic pelvis
- Lordotic pelvis
- Scoliotic pelvis
- Complex pelvis
- Spondylolisthesis
- Modified basin due to iliofemoral diseases (coxofemoral arthrosis, coxofemoral luxation)
- Modified basin due to diseases of the lower limbs (shortenings, amputations)
- Modifications following trauma, surgery, or vitiated consolidations
- External pelvimetry (normal):
- Internal pelvimetry:
- A. Bispinous diameter: 24cm
- B. Bisciatic diameter: 11 cm
- C. Bitrochanteric diameter: 32cm
- D. Bicrest diameter: 28 cm
- E. Baudeloque's antero-posterior diameter: 18 cm
Measured Diameter | Value (cm) |
Inter-spinous | 24 |
Inter-crestal | 28 |
Inter-trochanters | 32 |
Ischial inter-tuberosities | 11 |
Anteroposterior (external Baudeloque/obstetrical conjugate) | 20 |
Note: External pelvimetry is considered to have minor importance in modern obstetrics.
Pelvic Assessment | Adequate Characteristics | Inadequate Characteristics |
Pelvic Inlet | Diagonal conjugate >11.5cm; sacral promontory cannot be reached | Diagonal conjugate <11.5 cm; "sacral promontory reached" |
Midplane | Sacrum curved; sacrosciatic notch wide; ischial spines not prominent; bispinous diameter > 8.5cm; sidewalls divergent | Sacrum straight/shallow sacral concavity; sacrosciatic notch narrow; ischial spines prominent; interschial diameter < 8.5cm; sidewalls convergent |
Outlet | Intertuberosus diameter > 8.5cm; subpubic angle > 90 degrees; wide subpubic angle; coccyx moveable | Intertuberosus diameter < 8cm; subpubic angle < 90 degrees; narrow subpubic angle; coccyx not moveable |
Q. External pelvimetry provides the following data:
ACD
- Clinical evaluation method for predicting vaginal birth feasibility
- Assessing likelihood of cephalic presentation crossing the SS (engagement)
- Consideration of factors related to pelvis or fetus indicating difficult engagement
- Cephalic presentation
- "Borderline pelvis" with conjugata vera of 8-9 cm 📷
- Dilation of at least 4 cm
- Ruptured membranes
- Living fetus without fetal suffering
- Normal or medicinally adjusted uterine dynamics (antispasmodic)
- If the engagement of the presentation occurs within 2-4 hours without fetal station or maternal suffering, the delivery is considered a positive trial of labor ⇒ vaginal delivery = feasible
- If the engagement of the skull does not occur or there is fetal station or maternal suffering, the delivery is completed through a cesarean section and considered a negative trial of labor.
Q. *What is the obstetrical conduct in case of pelvic dystocia, with true conjugate <8 cm? a. Artificial rupture of membranes b. Vaginal birth c. Vaginal birth after labor test d. C-section e. C-section after labor test
d
Q. Select the correct sentences regarding the trial of labour:
A. It is a preclinical investigation that allows the evaluation of vaginal delivery.
B. It is the clinical assessment of the possibility of a vaginal delivery for a fetus in cephalic presentation and a pelvis on the verge of normality.
C. It is the clinical assessment of the possibility of a vaginal delivery for a fetus in cephalic presentation and a pelvis with conjugata vera below 8 cm.
D. If it is positive the vaginal delivery is sure.
E. If it is negative the solution is the cesarean section.
A, (D), E
- pelvi-perineal floor
- vulva
- vagina
- cervix (rigidity, obliteration, hypertrophy, deviation)
Fetal head is delivered but shoulders are stuck
⇒ +/- 🐢 turtle signs (retraction of head against perineum)


Antepartum | Intrapartum |
History of shoulder dystocia at a previous birth | Prolonged dilation period |
Fetal macrosomia | Precipitated fetal expulsion period (<20 min) |
Diabetes | Instrumental vaginal birth (forceps, vacuum extractor) |
Obesity (BMI > 30 kg/m2) or Excessive maternal weight gain | Prolonged fetal expulsion period (>2h for nulliparous, >1h for multiparous) |
Prolonged pregnancy | Use of oxytocin to stimulate uterine dynamics |
Multiparity | |
Induction of labor |
How do you perform the following maneuvers?
- flexion and abduction of thighs
- suprapubic pressure
Posteriorly, at the level of the sacred concavity (most accessible portion of the pelvis)
- Insertion of the posterior or anterior hand into the vagina ( along dorsal face of the fetal shoulder → Internal rotation (adduction) by approximately 30% until shoulders positioned in the oblique diameter of the pelvis
- Rotation determines adduction of the shoulders → Reduction of the biaacromial diameter
Hand is inserted into the vagina in the attempt to give birth to the posterior upper limb (not just shoulder).
- The Woods maneuver is an extension of the later Rubin maneuver.
- By applying pressure on the dorsal face of the posterior shoulder, the fetal trunk is rotated by at least 180 degrees, causing shoulder adduction.
- #3 Cleftotomy, Symphysotomy, Zavanelli maneuvers

→ see above
↓ Limited movements
- 💪🏼 Structural (fibroma)
- ↓🌊Oligohydramnios

↑Excess movements
- ⬇️ Fetal growth restriction (small fetus - IUGR)
- ↑🌊 Polyhydramniosis
- prior pregnancy (“lax uterus”)
Ø Contraindications for cephalic version → Cephalic version 📷 + vaginal delivery
Contraindications/Cephalic version unsuccessful → C-section
Relative Contraindication | Absolute Contraindications |
Active labor: Contractions might be temporarily stopped using terbutaline. | - Previous vertical cut cesarean delivery |
- Prior surgical removal of a uterine tumor (myomectomy) | |
- Presence of the placenta over the cervix (placenta previa) |
- Placental detachment
- Umbilical cord compression
- ROM
- Uterine rupture
RhoGAM
fetal weight (estimated) under 10th percentile for GA
- small for GA infant (SGA)
- neonatal mortality + morbidity risk ↑
20-30% ⇒ Symmetric (early = 2nd T): all organs and body parts affected (proportionally) → INTRINSIC (= fetal causes)
Fetal (intrinsic) causes:
- chromosomal abnormalities
- congenital infections
70-80% ⇒ 🥇 Asymmetric (late = 3rd T): head growth preserved (”head-sparing”) → EXTRINSIC (malnutrition → maternal causes i.e. placental insufficiency)
Extrinsic “maternal” causes:
malnutrition of fetus due to placental insufficiency (i.e. diabetes or HT)
Headsparing: fetal WEIGHT is most affected (lenght not so much)

- Maternal (15%): Includes preexisting or induced hypertension, diabetes mellitus, cyanogenic heart diseases, vascular involvement in autoimmune diseases, hemoglobinopathies, toxic substance consumption, chronic hypoxia, pulmonary insufficiency, and malnutrition.
- Fetal (25%): Encompasses chromosomal abnormalities like trisomy 21, 13, 18, genetic syndromes, congenital malformations, fetal infections (TORCH), and cases of multiple pregnancy.
- Placental (35%): Features conditions like placenta praevia, single umbilical artery, velamentous umbilical cord insertion, primary placental hypoplasia, and retroplacental hematoma.
- Idiopathic (25%): Represents cases where no detectable cause is found, leaving the complications unexplained
Clinical Diagnosis:
- Measurement of uterine fundus height (decreased) is a key indicator; normal growth is about 4 cm monthly until week 32.
- Height of the fundus should be around 16 cm at 20 weeks, 20 cm at 25 weeks, 24 cm at 28 weeks, and 28 cm at 32 weeks.
- A reduction in the expected height of the fundus can suggest growth restriction.
Ultrasound Diagnosis:
- Ultrasound is crucial for confirming or ruling out IUGR.
- Accurate gestational age is established, with first-trimester ultrasound being vital.
- Biometric parameters (biparietal diameter, femoral lenght and abdominal circumference) are measured and compared to standard growth curves.
- Intrauterine growth restriction (IUGR) can be classified as symmetrical or asymmetrical.
- Symmetrical IUGR requires further evaluations such as morphological ultrasound, amniocentesis & karyotyping, infectious disease testing, and consideration of pregnancy termination for severe cases.
- Asymmetrical IUGR requires continuous monitoring of the fetus to determine the optimal time for delivery.
- Clinical parameters, ultrasound parameters, and fetal heart rate monitoring are used to assess the intrauterine fetal status.
- Ultrasound: Placental appearance & Amniotic fluid amount → Doppler is important for evaluating vascular causes of IUGR, including examining uterine, umbilical, and middle cerebral arteries, as well as the umbilical vein and venous duct.
- Monitoring the fetal heart rate helps detect acute intrapartum fetal distress.
- The timing of delivery is based on gestational age and the degree of fetal distress.
AFI = Amniotic fluid index 📷
- Measurement of the amniotic fluid using the abdominal quadrants: divide the abdominal wall into four quadrants and measure the deepest pocket in each quadrant. Sum up the values obtained.
- Normal range for the amniotic fluid index (AFI): 5-25 cm.
Oligo: AFI <5cm
Poly: AFI >25cm
Measurement of the largest deepest pocket normal: is 2-8 cm. The upper limit admitted as normal is 2000 ml and the lower limit is 200 ml.
Oligohydramnios | Polyhydramnios | |
Causes | ||
First trimester | - Rare | |
Second trimester | - Decreased fetal urine production | - Decreased fetal swallowing (intestinal atresia) |
- Renal agenesis | - Fetal anemia | |
- Cystic kidneys | - High fetal cardiac output due to fetal urine production | |
- Posterior urethral valves | - Alloimmunization, B19 infection | |
Third trimester | - PROM | - Maternal diabetes |
- Placental insufficiency | - Multiple gestation | |
- Twin-twin transfusion syndrome |
Oligohydramnios | Polyhydramnios | |
Consequences/Associations | Associated with poor outcomes | May cause premature rupture of membranes |
- Umbilical cord compression | Associated with preterm delivery | |
- Placental insufficiency | or fetal malpresentation | |
- Meconium aspiration | ||
- Potter sequence |
Oligohydramniosis
⇒ Delivery at term or shortly before (36-37w) → hydration of mother (↑AF volume) → rarely: saline infusion
Polyhydramniosis
mild → spont. resolution
severe (AFI >35) and compressive symp: → Amnioreduction → Indomethacin (reduces amniotic fluid; but only before 32w → otherwise: ductus art. closure!)
Q. *Therapeutical target of intrauterine growth restriction (IUGR) does not include?
a. Reviewing and restoring data to confirm the diagnosis b. Determination of abnormal karyotype c. Assessment of morphological abnormalities d. Evaluation of possible etiologic factors e. Antibiotic treatment
e
- In most of the cases, foetal obstetrical trauma caused by mechanical forces such as compression or traction on the cranial extremity of the foetus.
- Prompt diagnosis and appropriate management can help reduce the long-term consequences of foetal obstetrical trauma.
- Low fever for first 24h
- polyuria for first 2-3d
- breast swelling → firm, tender
- mild hair loss → stops after 1-5m
Q. *In normal puerperium, one of the following changes may appear: A. Polyuria during the first 2-3 days B. Placental hormones are eliminated within the first hour C. Progression of the pubic symphysial diastasis D. Hypopigmentation E. Blood volume decreases immediately
A

severe → special interventions:
- balloon tamponade (intra-uterine)
- arterial embolization
- hysterectomy
- tranexamic acid

>500ml blood loss with vaginal delivery or >1000ml blood loss with C-section
Bleeding with signs of hypovelemia within 24h after birth → rarely: shock / Sheehan syd
Tx = Etiological
- 🥇 Uterine atony
- Others
- Genitourinary trauma
- Coagulation pathology
- Retained membranes/placenta

Pituitary gland during pregnancy is more susceptible because it enlarges naturally during pregnancy!
- ↓ PRL ⇒ ØLactation
- ↓GnRH ⇒ Amenorrhea, loss of pubic hair
- ↓TSH ⇒ weight loss
💊hormone replacement
After delivery ⇒ uterus contracts to stop bleeding If Øcontraction (atony) ⇒ bleeding
examples for each:
- ) Macrosomnia, mulitple babies
- ) prolonged labor, too much oxytocin
- ) structural (i.e. fibroids), drugs
+ 🎒 Chorioamnionitis
Oxytocin + Massage (of uterus)
+/- Additional Uterotonics:
- Methly-Ergonovine
Øin HT history ⇒ SE: ↑BP
- PG-analogs: Carboprostol / Misoprostol
Carboprostol ⇒ contraindication = asthma
Misoprostol ⇒ Ø contraindication in HT or asthma
+/- Hemorrhage control if sev. (balloon, emboliz, hysterectomy)
- Uterus inverts completely
- fundus of the uterus pushes through the cervix
- Solid, circular mass coming out of the vaginal opening
- Results in intense bleeding
- 1st degree: inverted fundus up to cervix
- 2nd degree: body of the uterus protrudes through cervix into the vagina
- 3rd degree: prolapse of the inverted uterus outside the vulva
- 4th degree: the vaginal walls participate in inversion
- multiple gestation
- iatrogenic: excessive cord traction
- Uterine rupture (see above)
- Cervical lesions
- Vaginal lesions
- Perineal lesions
- Puerperal hematomas
- Uterine inversion
- Symphysial lesions
- Postpartum fistulae
- breech
- instruments used
- macrosomnia
- …
- Apply manual pressure
- Repair via surgery
↑production + consumption of platelets = low-key “DIC” (chronially compensated)
⇒ Small bleeding ⇒ ↑DIC risk (clotting factors consumed by bleeding)
test if bleeding = prolonged:
Plts count + coagulation markers (INR, PT, aPPT)
Normal: Placenta attached to decidua 📷 + expelled after delivery by uterine contraction
Abnormal “decidualization” ⇒ Placenta attached to myometrium + is retained ⇒ postpartum bleeding 🩸
- Prev. C-Section esp. if together with placenta previa
- other uterine surgery

- Placenta A-CCRETA 🥇
- Attached to myometrium (Øpenetration)
- Placenta IN-CRETA
- Penetration of myometrium
- Placenta PER-CRETA
- Penetrates through myometrium into serosa (+- invasion of rectum/bladder)
📖 ❗ CAVE book says:
“Placenta accreta: the chorionic villi penetrate the inner 1/3 of the myometer; Placenta increta: the placenta penetrates the outer 1/3 of the myometer; Placenta percreta: the chorionic villi reach the peritoneum.”
🦇prenatal US
Massive maternal hemorrheage ⇒ shock, DIC (happens bc remaining part of placenta breaks into piece)
placenta undelivered after 30 min postpartum, often accompanied by heavy bleeding
- Endometrial lining damage (endometritis, curettage).
- Placental abnormalities (insertion of the placenta in the lower segment, excess volume, or placental surface).
- Abnormal uterine contractions during labor (prolonged labor, grand multiparity, womb malformations, fibroids, multiple gestations, general anesthetic).
- Other mechanisms of retained placenta (bladder distension, genital hematomas).
Fetal cells/debris + amniotic fluid → enter circulation of mother → anaphylactoid inflammatory reaction 📷
→ happens during or shortly after labor
→ often fatal ☠️
- Phase: Respiratory distress & Shock (Hypox + ↓BP)
- Phase: Hemorrhagic (bleeding + DIC) & Seizures
- Supportive measures: high flow of oxygen, ventilation support, fluid resuscitation, inotropic support, intubation, coagulopathy correction
- Obstetrical treatment:
- Dead fetus: expulsion is expected
- Alive fetus: emergency c-section
Bleeding >24h after delivery
Causes:
- Subinvolution
- Retained products of conception
- Endometritis
- Uterine involution: Return of the uterus to its non-pregnant size and state
- Lochia (postpartum vaginal discharge) = normal (cause: superficial decidua layer sheds)
- Lochia rubra (first 3 to 4 days): red color, similar to menstrual blood
- Lochia serosa (day 4 up to 2 weeks): pinkish-brown and watery
- Lochia alba (weeks): yellow
Inadequate physiologic closure and sloughing → late postpartum bleeding
- Retained product of conception
- Endometritis
- low fever for <24h after birth = normal
- Postpartum fever: ≥38°C for >24h
💊AB + Debridement/Drainage/Irrigation
This occurs due to the early closure of the cervical canal. The retained lochia becomes superinfected.

- fever
- local:
- discharge (”foul”, purulent)
- uterine tenderness
- leucocytosis

Toxic shock synd
⇒ ↓BP + rash/desquamation
breast feeding 🥛 ⇒ Skin-Trauma AROUND NIPPLE

Abscess 🎾 ⇒ Drainage
S.Aureus → 🦑 Cephalexin (Gen1) / dicloxacillin
⇒ CONTINUE 🥛nursing
cystitis / pyelonephritis
often the cause for prolonged fever after delivery (>24h) → normal Dgx + Tx workup
- Parietal factors: Endothelial injury
- Preexisting venous wall lesions
- Venous wall inflammation
- Venous stasis present in pregnancy
- State of hypercoagulability in pregnancy and the postpartum period
45. One of the following is a favoring (not decisive) factor for thromboembolism (deep vein thrombosis) in pathological puerperium:
- A. Age
- B. Parietal factor
- C. Hypercoagulability
- D. Venous stasis factor
- E. Hypocoagulability
A = risk factor and not decisive
Risk factors: • A history of venous thromboembolis • Age >35 years • Obesity • Presence of infections • Immobilization/prolonged rest in bed • Dehydration/shock • Thrombophilia
Thrombosis + infection in ovarian / deep pelvic vv.
Criteria | Ovarian vein SPT | Deep septic pelvic thrombophlebitis |
Timing | Occurs within 1 week of delivery | |
Symptoms | Acutely ill patient with fever and abdominal pain localized to affected side | Subtle presentation:
Fever but patients often Ø acutely ill-appearing |
Palpation | Pelvis tender to palpation
"Rope-like mass" on examination from uterus to lateral abdomen | Ø tenderness |
Diagnosis | Clinical + CT/MRI | Often dgx of exclusion (confused for endometritis → poor response to AB; response to anticoagulant)
Pelvic imaging may be normal |
- Other thrombotic: Superficial + deep thrombophlebitis, PE
- Relative rest
- Compression stockings
- Anti-Inflammatory drugs (phenylbutazone) - locally and systemic
- Anticoagulants (topical): Lasonil, Hepathrombin

Treatment
Q. Choose the false statements from below:
A. Superficial vein thrombosis is treated with anticoagulants.
B. Repeated vaginal touch and intrauterine maneuvers represent risk factors for postpartum endometritis.
C. Postpartum endometritis is characterized by inappropriately regressed uterus, abundant lochia, abdominal pain, and fever.
D. Duration of treatment of endometritis is continuous until the normalization of the laboratory analysis.
E. Determinant factors for deep vein thrombosis in the postpartum period are: endothelial factors, stasis, and hypercoagulability.
ADE (= false statements)
- Parametritis (pelvic cellulitis)
- Adnexitis
- Pelviperitonitis
- Generalized puerperal peritonitis
- Septicemia, Speticopyemia
- Anuria since 6h after delivery → pudendal nerve injury (birth trauma)
- improves over time
- intermitt. urinary catheter needed
- Type I: Pelvic inlet stretching
- Type II: Enlargement > 2 cm, pelvic bone fracture, rupture of anterior ligaments of symphysis
- Type III: Rupture of posterior ligaments of symphysis, displacement of iliac bone
Dgx: Clinic or Xray
Tx: Analgesics + Physio + Orthosis
Aspect | Postpartum Blues | Postpartum Depression | Postpartum Psychosis |
Prevalence | Common (in many studies, up to 85%) | Less common (~15% of cases) | Very rare (0.1 to 0.2% of births) |
Symptoms | Low mood, trouble sleeping, tiredness, difficulty focusing | Persistent mood disturbances after 14 days | Delusions, hallucinations, disorganized thinking |
Onset | Begins 2-3 days post-delivery | After 14 days post-delivery | Within 14 days after birth |
Duration | Resolves in 14 days | ||
Risk Factors | Women with a known psychiatric condition, particularly bipolar disorder. Risk increases if medications are stopped during pregnancy. | ||
Treatment | Supportive care | CBT and medications (SSRIs) | Requires hospitalization due to risk factors like potential for self-harm and danger to the baby. Medication (antipsychotics) and ECT are treatments. |
Q. Find the exception regarding prophylactic treatments in pathological puerperium A. Avoid repeated vaginal exams B. Avoid obstetric maternal trauma C. Correction of anemia D. Anti-inflammatory and antibiotic treatment E. Avoid loss of blood
D
Q. Choose the correct statements from below A. Lochiometria is characterized by purulent vaginal discharge B. Breast abscess requires exclusively medical treatment C. Pelviperitonitis occurred during puerperium requires surgery D. Deep vein thrombosis during puerperium can be treated by thrombolysis E. Medical treatment of postpartum endometritis requires the association between clindamycin and cephalosporin
CD



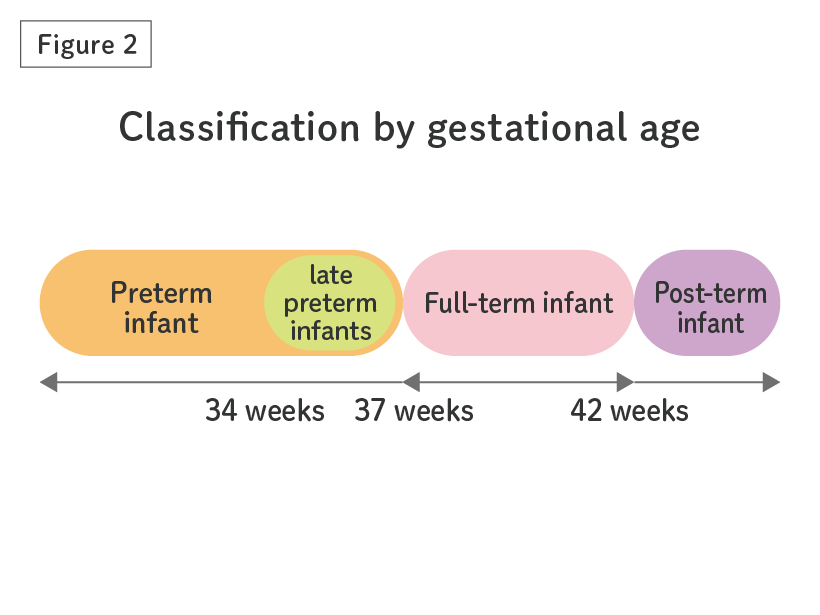{kind=link}
{kind=link}
{kind=link}
{kind=link}
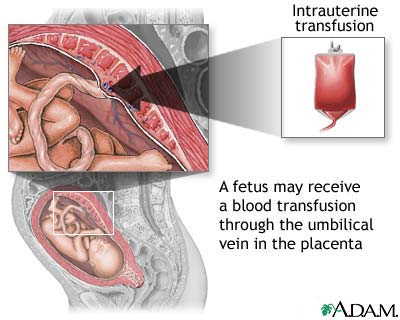{kind=link}
{kind=link}
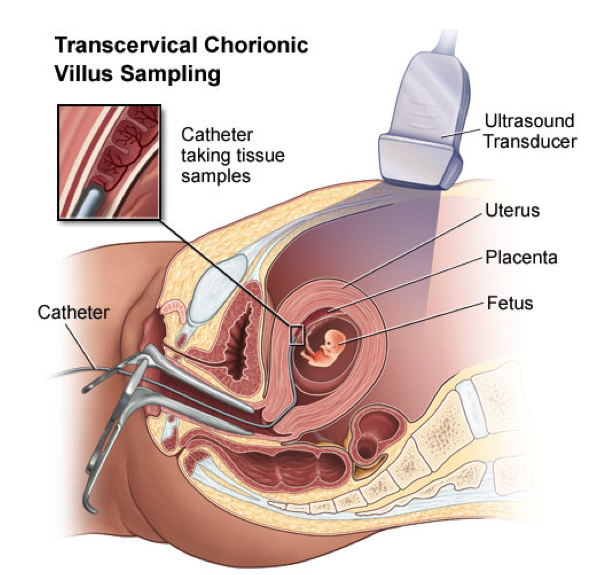{kind=link}
{kind=link}
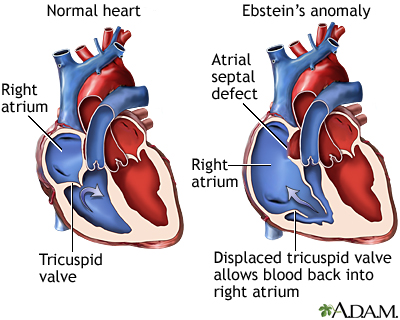{kind=link}
{kind=link}
{kind=link}
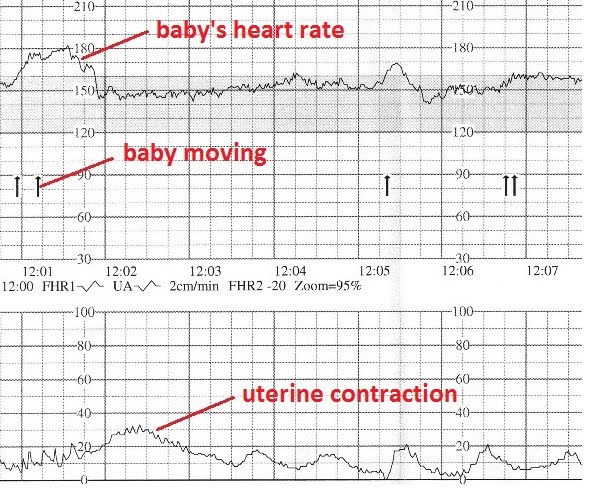{kind=link}
{kind=link}
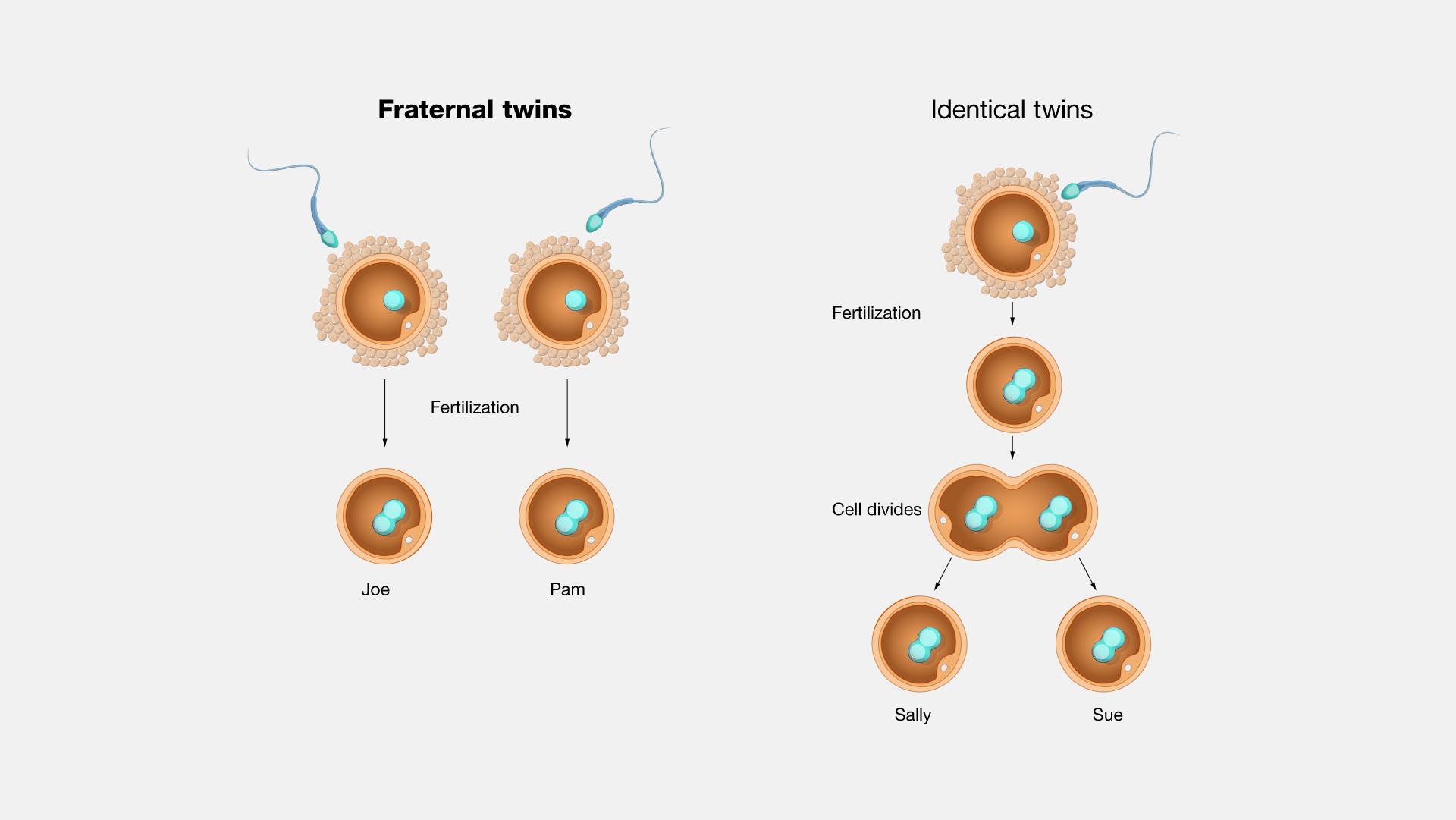{kind=link}
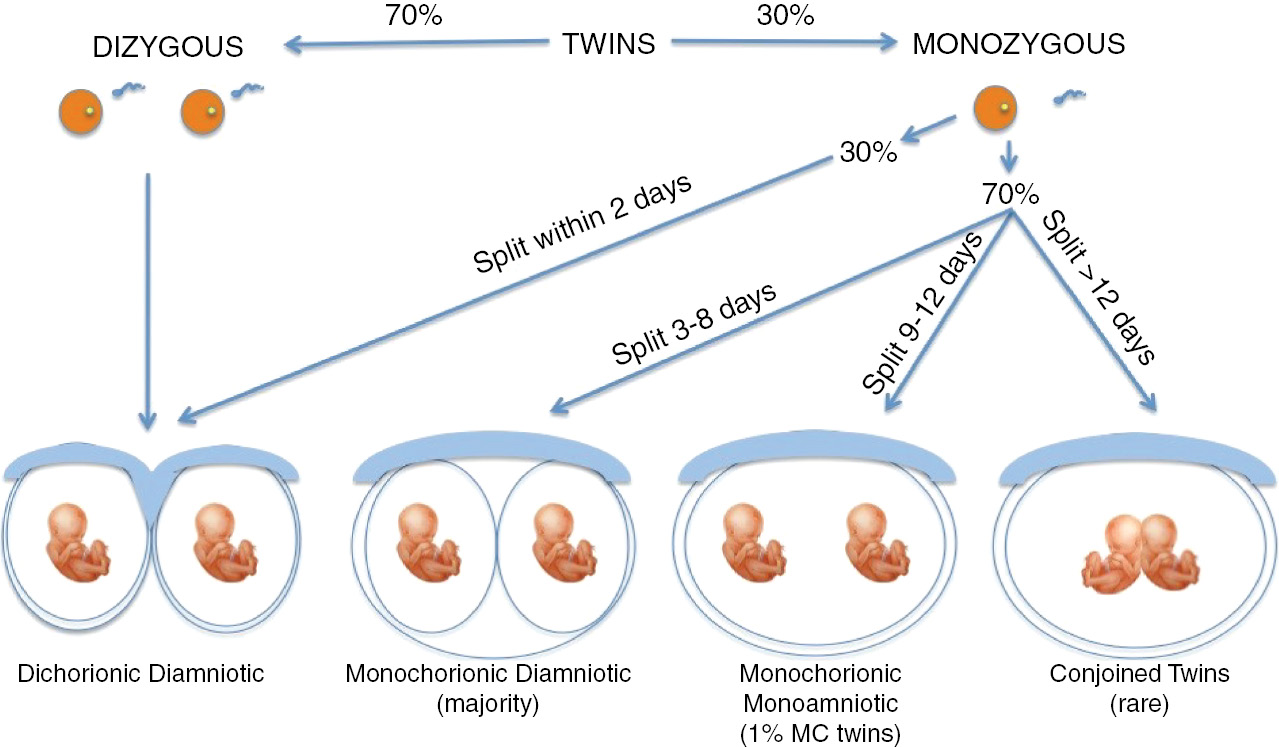{kind=link}
{kind=link}
{kind=link}
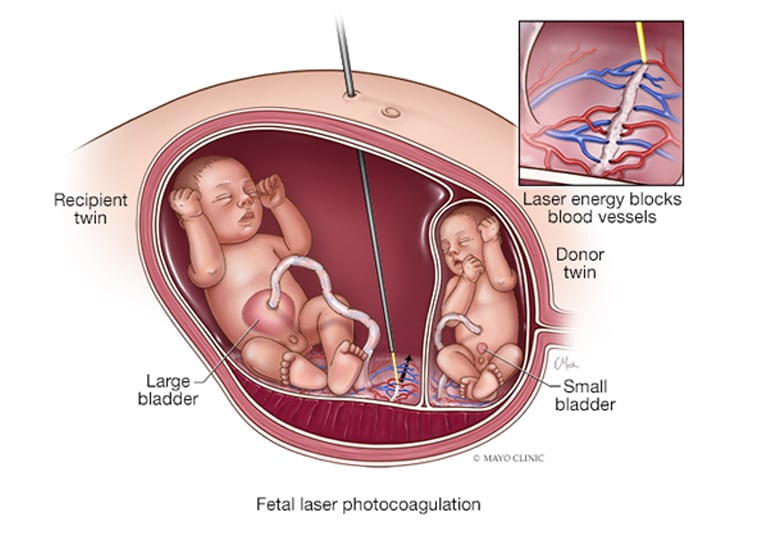{kind=link}
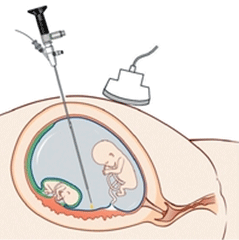{kind=link}
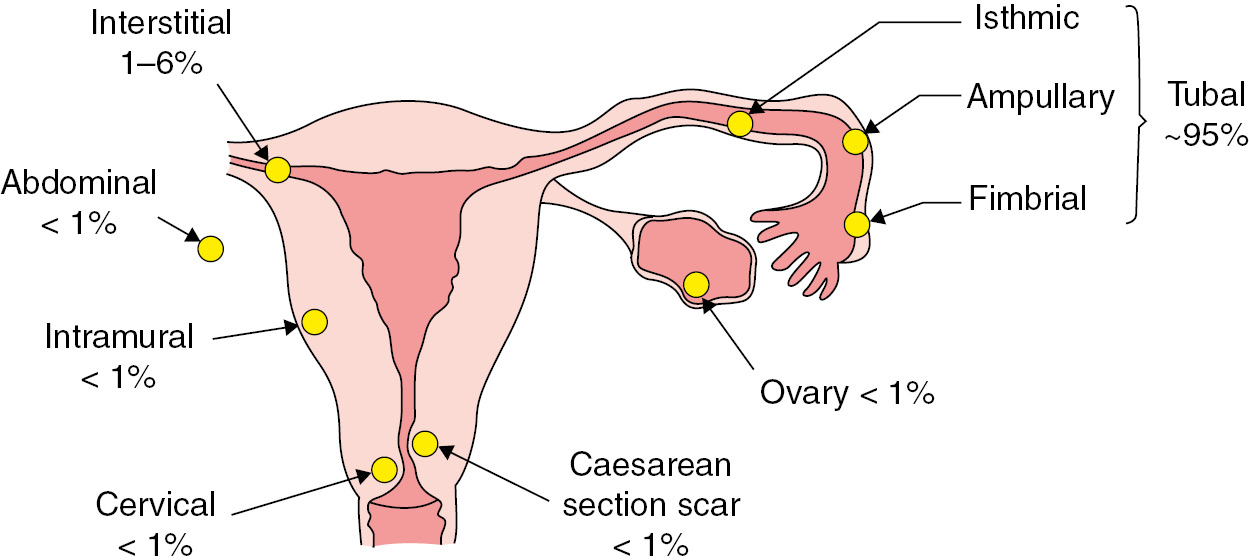{kind=link}
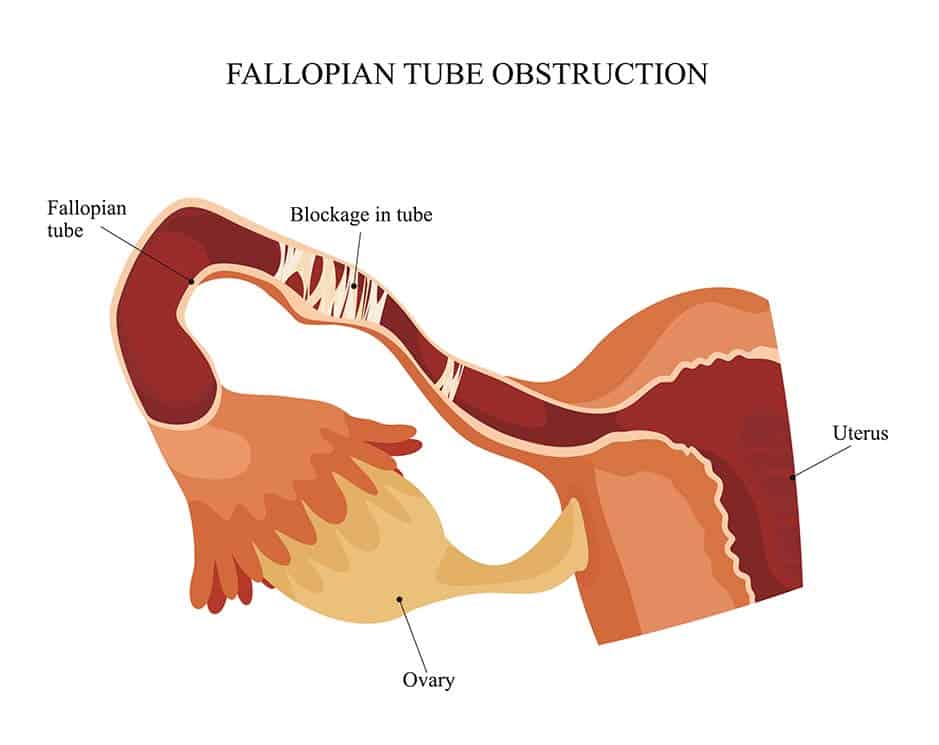{kind=link}
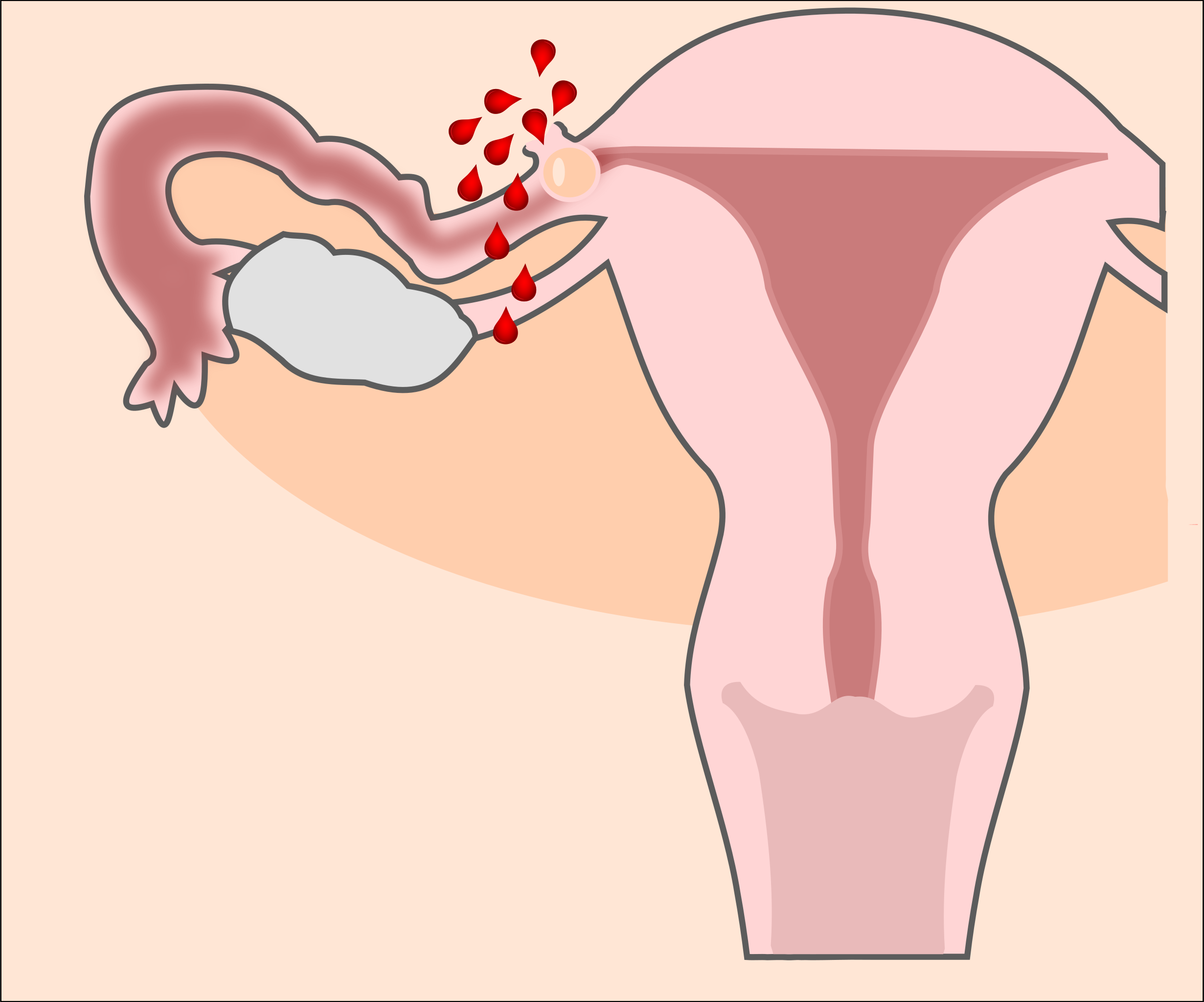{kind=link}
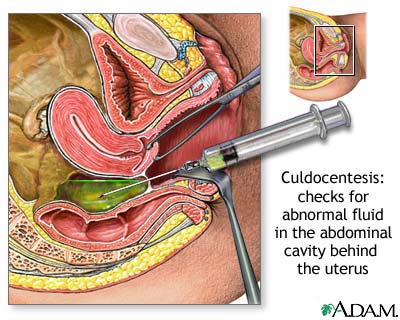{kind=link}
{kind=link}
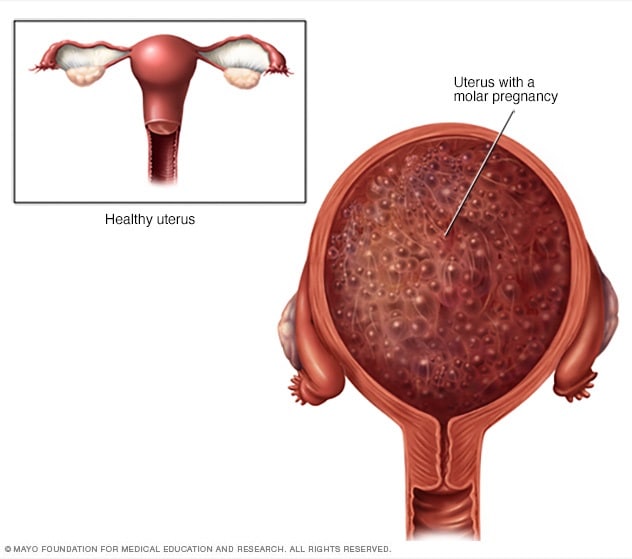{kind=link}
{kind=link}
{kind=link}
{kind=link}
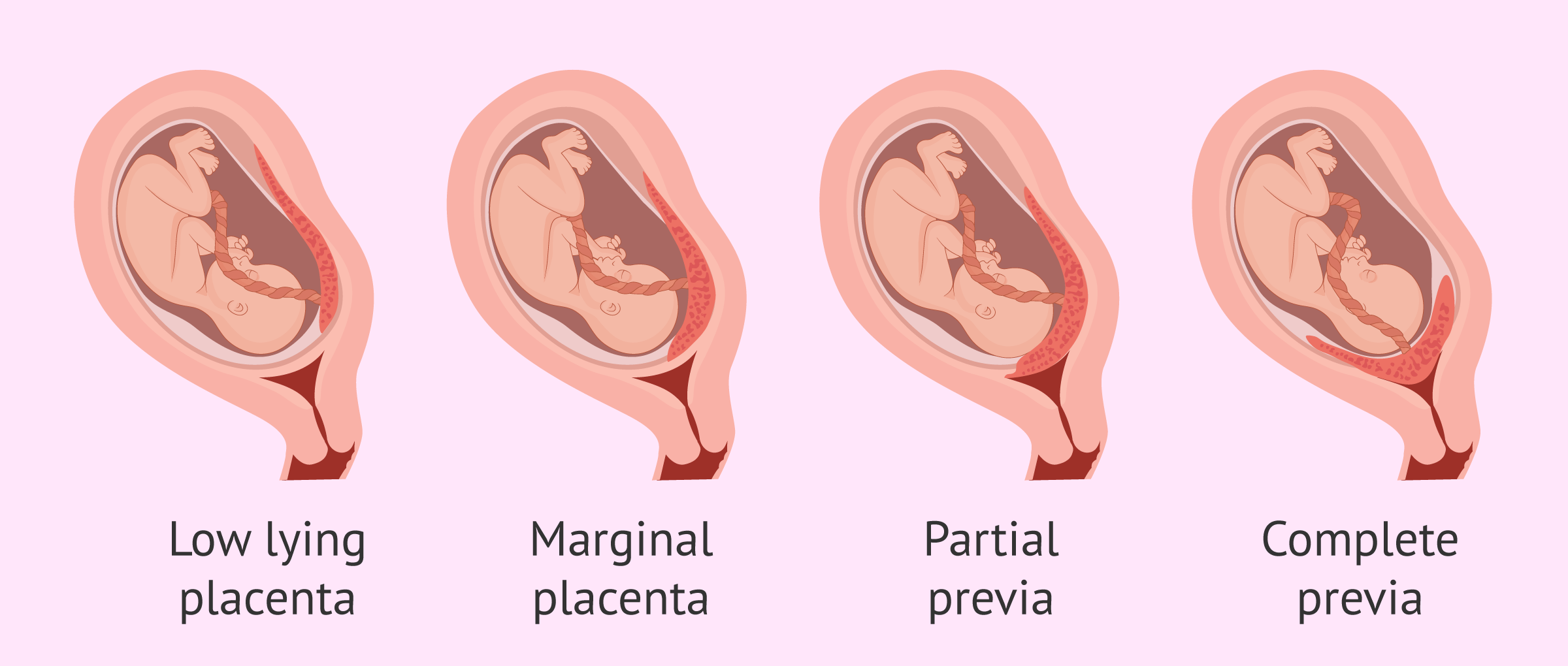{kind=link}
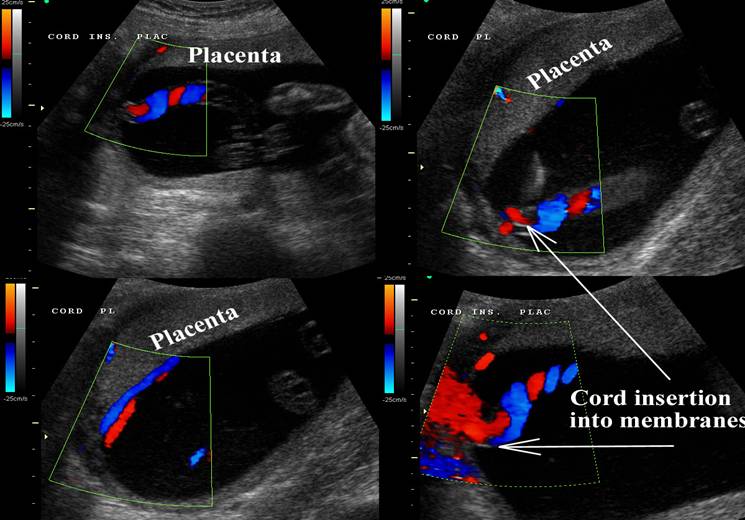{kind=link}
{kind=link}
{kind=link}
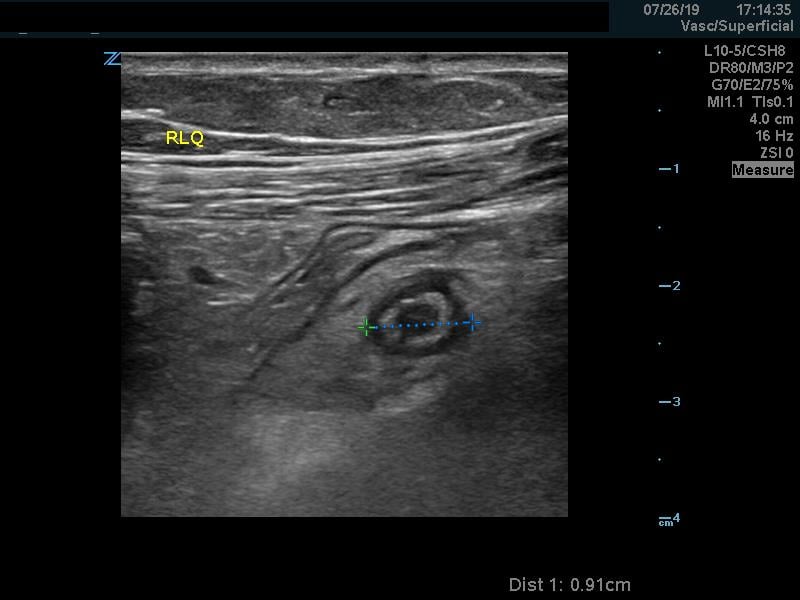{kind=link}
{kind=link}
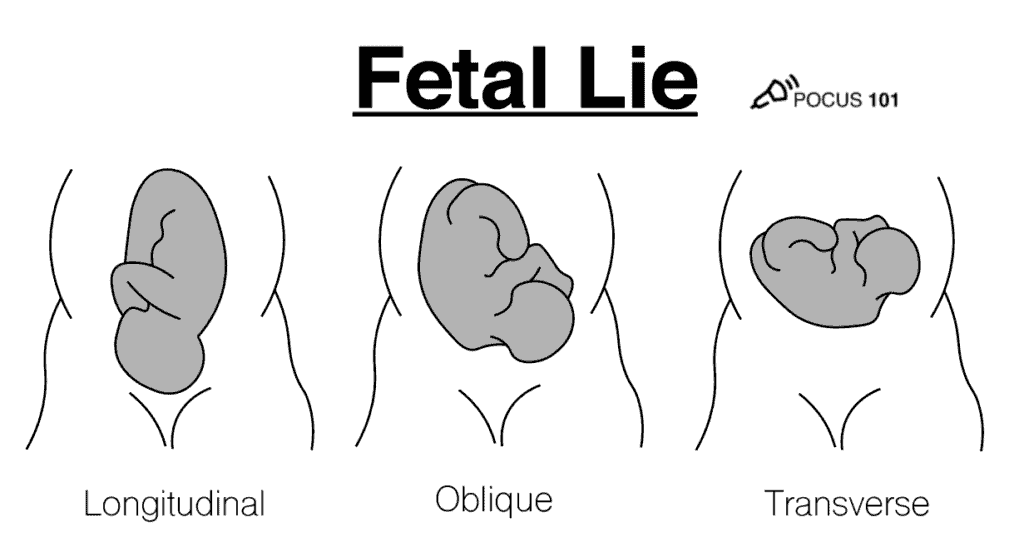{kind=link}
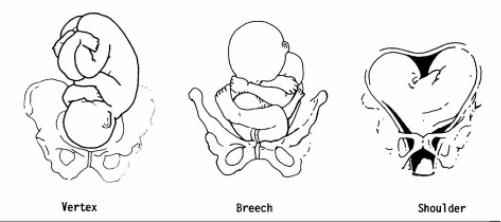{kind=link}
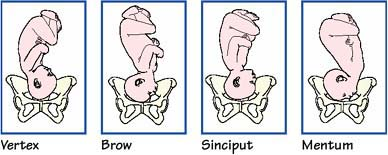{kind=link}
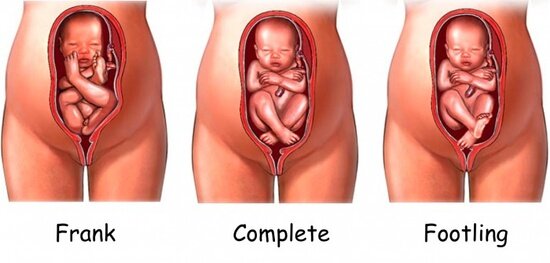{kind=link}
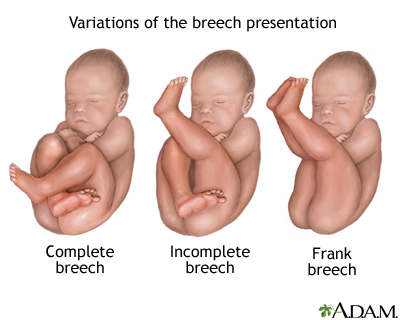{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
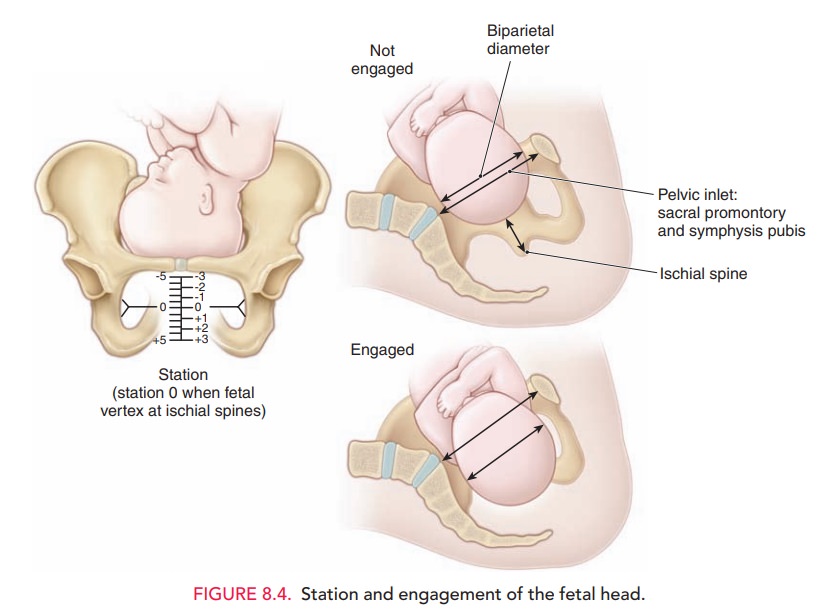{kind=link}
{kind=link}
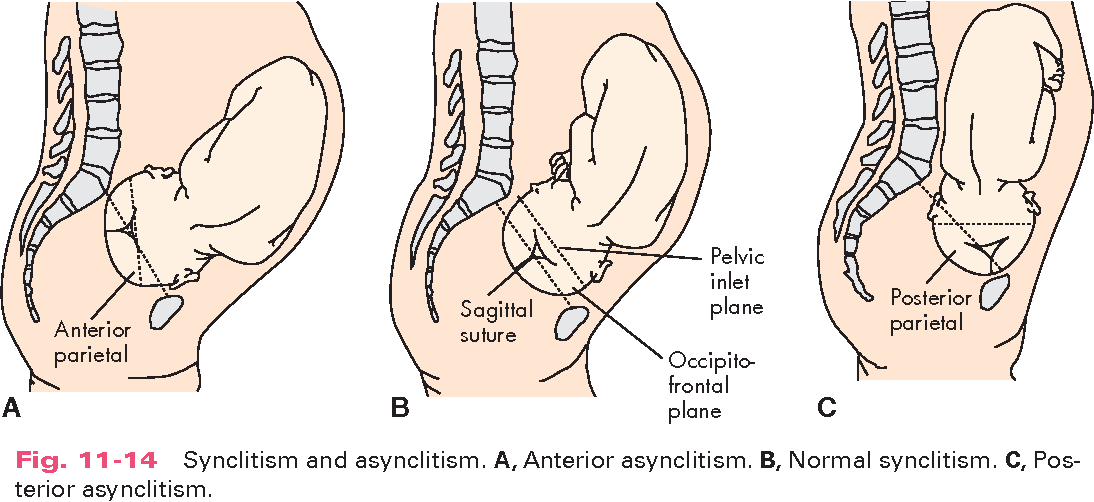{kind=link}
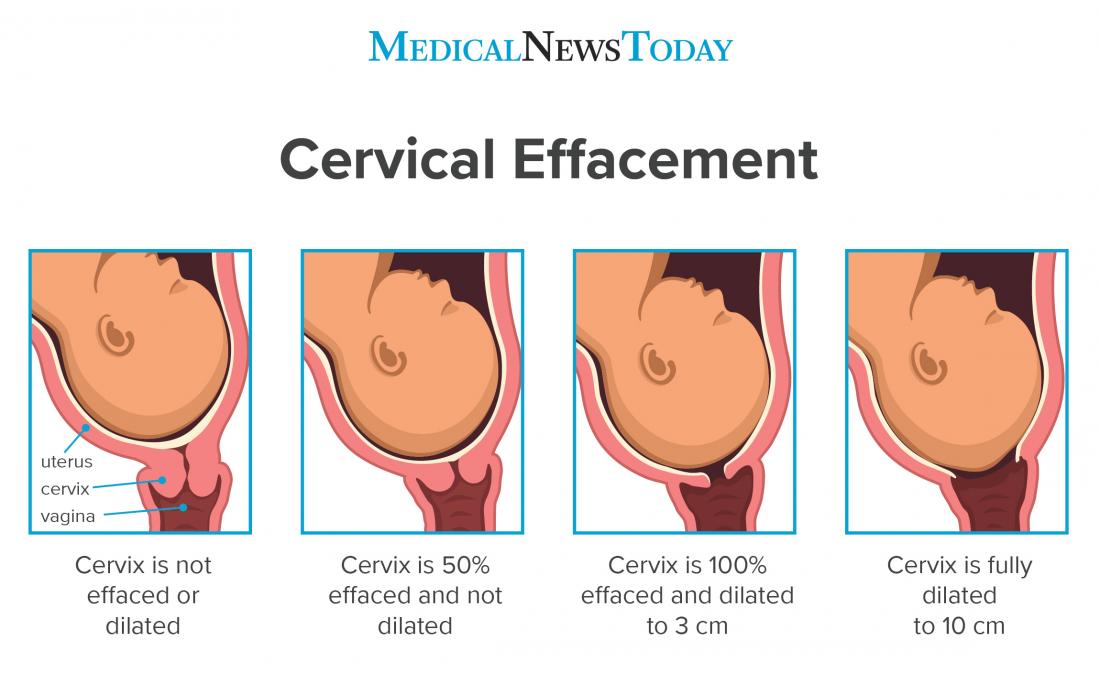{kind=link}
{kind=link}
{kind=link}
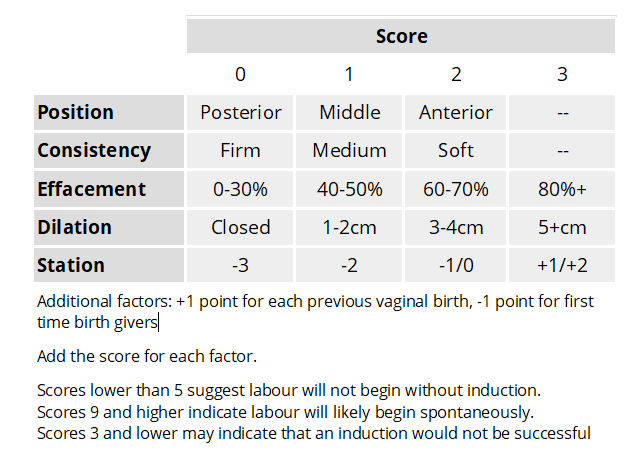{kind=link}
{kind=link}
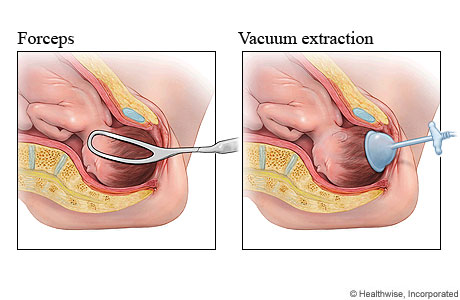{kind=link}
{kind=link}
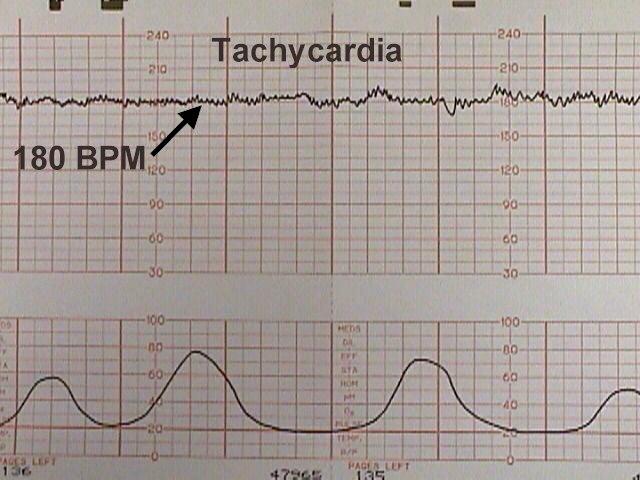{kind=link}
{kind=link}
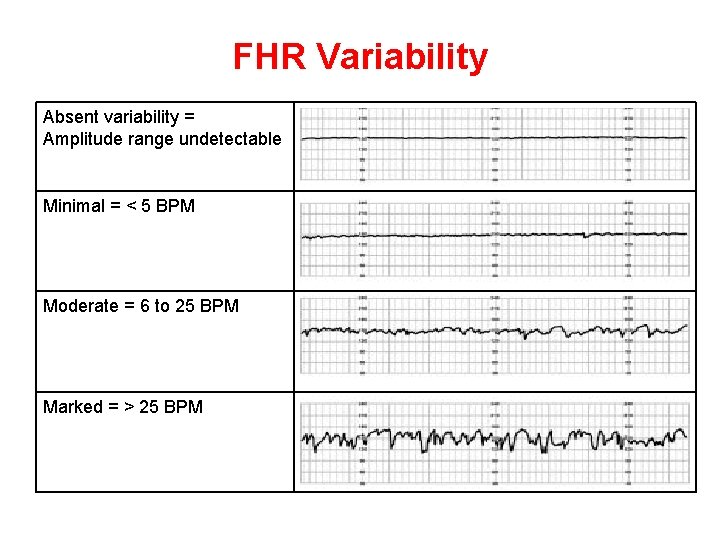{kind=link}
{kind=link}
{kind=link}
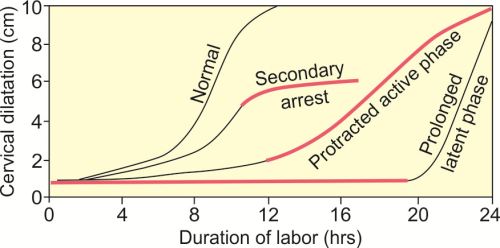{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
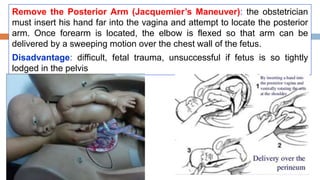{kind=link}
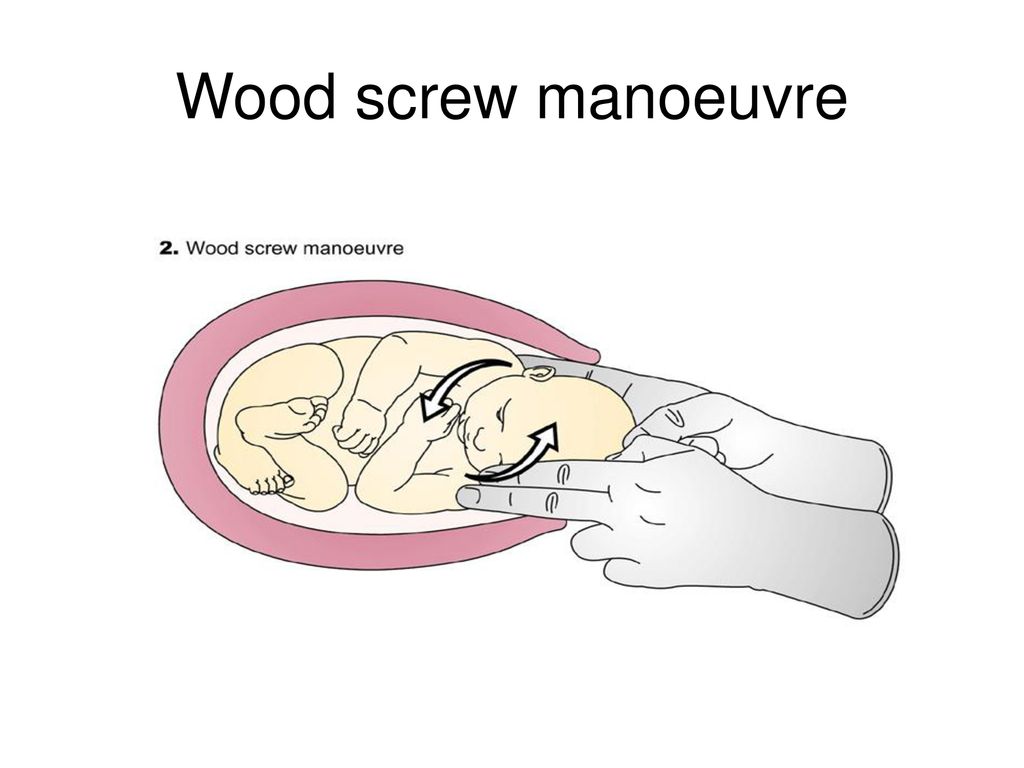{kind=link}
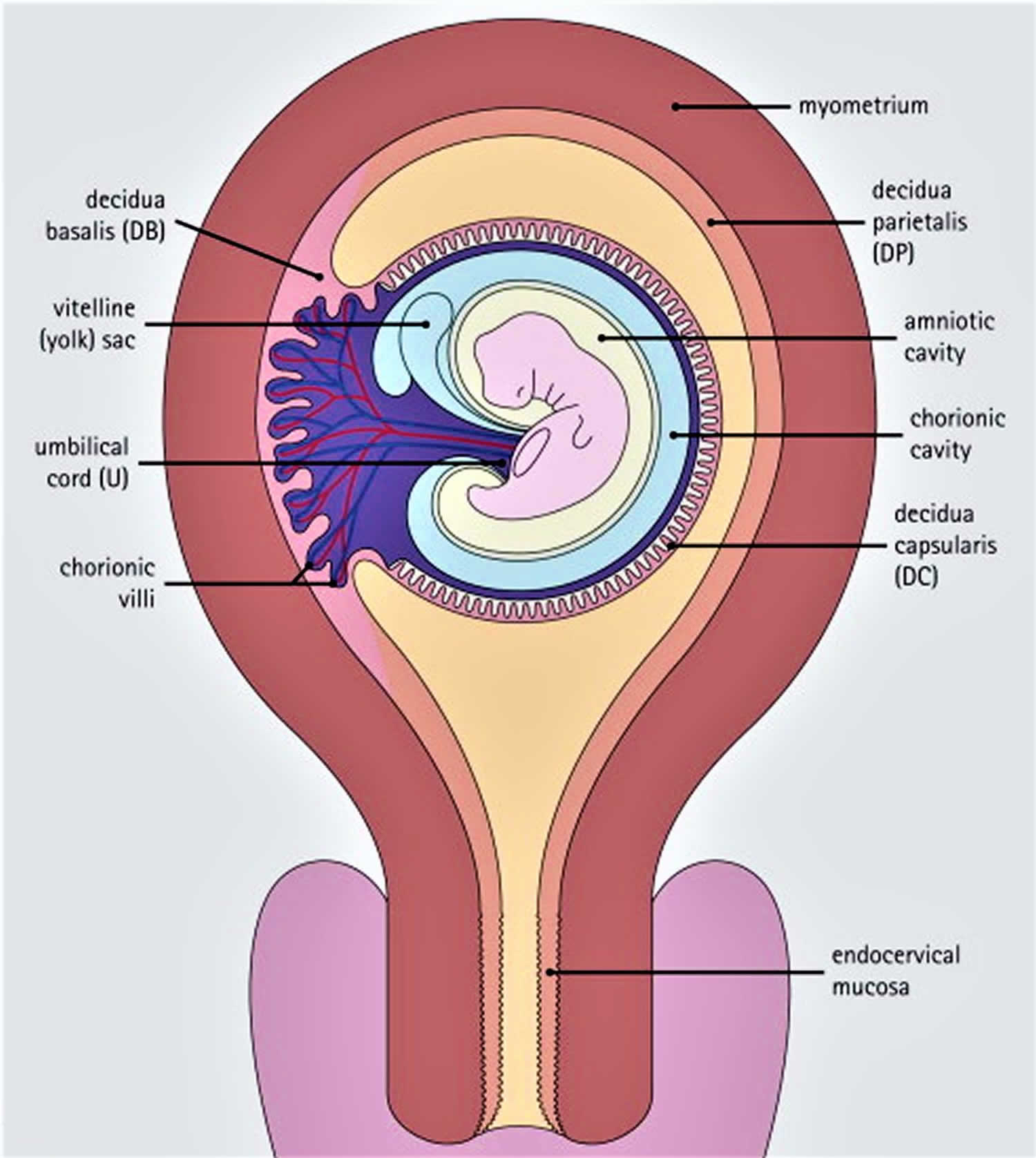{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}