





Gynaecology


- Adrenarche: Increased secretion of androgens produced by the adrenal cortex, typically occurring about 2 years before gonadarche. Adrenarche is considered the trigger of puberty.
- Gonadarche: Alteration of steroid feedback action, leading to an increase in gonadal sexual steroids, starting at around 8 years of age.
- Thelarche: The development of breasts.
- Pubarche: The appearance of pubic hair, typically followed by axillary hair two years later.
- Growth Spurt: A period of rapid growth.
- Menarche: The first menstruation, typically occurring around 12.5 years of age when sufficient estradiol is secreted for endometrial proliferation. Ovulatory cycles occur when positive estradiol feedback develops. Initially, menstrual cycles can be irregular in terms of timing and length, and the first cycles are generally anovulatory.
Define the following:
- Onset:
- Occurs before the age of 8 years.
- Characterized by early pubic hair development.
- Minimal growth of axillary hair (normal puberty timing).
- Bone Growth and Maturation:
- Slightly advanced compared to typical development.
- Secondary Sex Characteristics:
- Absent during this stage.
- Signs of Virilization:
- May include the development of secondary male characteristics or the absence/regression of secondary female sexual characteristics, such as clitoral hypertrophy.
- Typical Progression:
- Often evolves toward normal puberty.
- Etiology:
- Primarily associated with premature adrenarche, unrelated to gonadal stimulation.
- May also be associated with underlying hypothalamic disorders.
- Slight Increases in Breast Development During Childhood:
- Characterized by minor breast development without concurrent nipple and areola development and pigmentation.
- Absence of Other Secondary Sex Characteristics:
- Secondary sexual characteristics beyond slight breast development are not present.
- Progression and Regression:
- This condition may either spontaneously regress or progress towards normal puberty.
- Etiology:
- Typically attributed to an unexplained increase in estrogen levels.
Tx: If etiological: suppress estrogen release
True isosexual prec. puberty | Isosexual prec. pseudo-puberty | Heterosexual prec. pseudo-puberty | |
Cause | HP-axis activation | Ovarian E↑ produc. (Ø axis activation) ⇒ i.e. ovarian tumor | ↑E by other tissue: adrenal tumor (/ ovarian tumor) or hyperplasia |
FSH/LH | ↑ | normal | normal |
Bone age | ↑ | ↑ | ↑ |
normal development (only ↓stature in relation to age) | VIRILIZATION | ||
Exclude intracranial tumor (*neuro signs?) |
⇒ Tx = Etiological
- LATE onset (→ see primary amenorrhea)
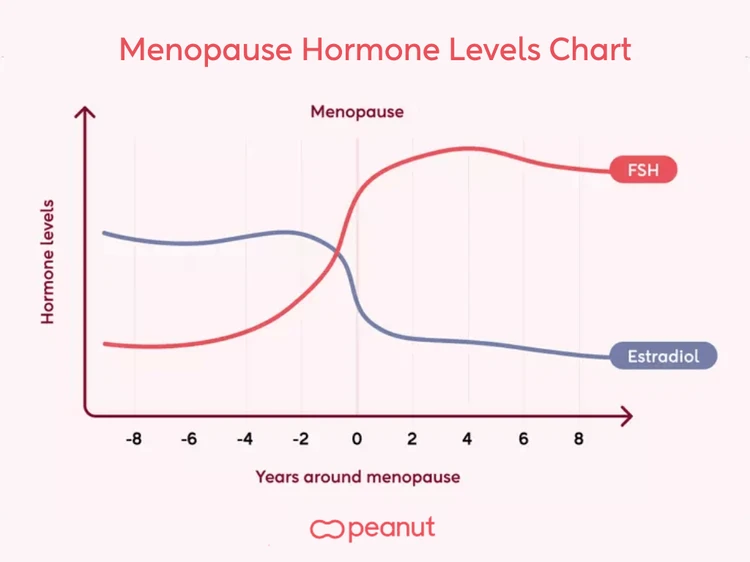
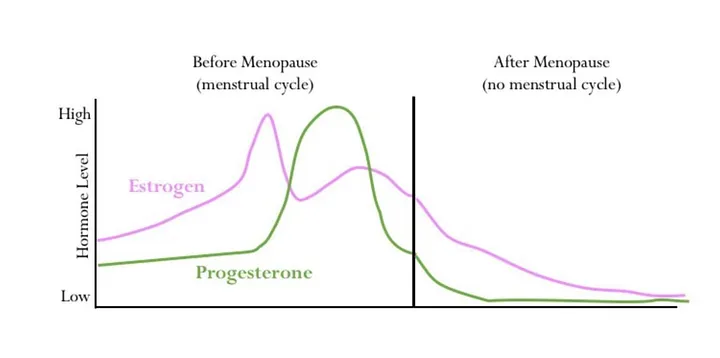
- depletion of ovarian follicles → permanent cessation of menstrual periods
- Usually preceded by irregular menses
- Median age around 50 years
- ↓ levels of estrogens and progesterone from ovaries → Evtl. FSH and LH levels will be elevated

- Usually preceded by irregular menses
- Patho:
- Ø luteal phase → Ø progesterone release → continued estrogen release
- Ø progesterone withdrawal for normal menses → Endometrial growth → abnormal uterine bleeding
- Other signs & symptoms
- Hot flashes (vasomotor sympoms)
- Usually lasts only a few minutes
- Associated with ↓ in estrogen
- Vaginal atrophy
- loss of estrogen stimulation → Thin, dry or friable
- Tx: topical estrogen
- Fatigue
- Dgx: usually clinically ⇒ 12 months of amenorrhea Ø due to other cause
- hCG
- FSH
- TSH
- Prolactin
- Serum hormone level changes are not required for diagnosis:
- ↑ FSH
- FSH:LH ratio > 1.
⇒ Women under 45: exclude other causes of amenorrhea
⇒ 📷
FSH ↑ more than LH.
due to ↓E:
- Osteoporosis
- Cardiovascular disease
- Dyslipidemia: ↓ HDL, ↑ LDL
- lifestyle modification
- herbal supplements
- Tx of hot flashes
- Ø for long-term prevention ⇒ Risk > benefits for osteoporosis / CAD
- Estrogens and/or progestins
- Estrogens: ↓ menopausal symptoms
- Progestin if intact uterus:
- Prevents endometrial hyperplasia (↓cancer risk) & bleeding
- Not required if post-hysterectomy
- CV (DVT, stroke, MI)
- breast cancer
- History: Hormone-sensitive breast/endometrial cancer
- CV:
- coagulopathy
- history DVT, PE, stroke, CAD
- Metabolic
- liver d.
- kidney d.
- Unexplained vaginal bleeding (E → ↑bleeding)
**preperation details


- biphosphonates / Vit D (osteoporosis prevention)
Perimenopause
(”Climacterium”) | Menopause | Postmenopause | |
Duration | Last years before stabilization of amenorrhea | Permanent cessation of menstruation | Begins 10 years after menopause onset |
Menstruation | Excessive or decreased menstrual flow | Cessation of menstruation | Absent menstrual flow |
Hormones | Relatively normal or slightly decreased estrogens | Low estrogen and progesterone | Very low estrogen, progesterone and inhibin |
Low progesterone | Very low inhibin* | FSH and LH normalize due to pituitary involution | |
FSH increase parallels inhibin decrease | Significantly increased FSH, high LH | During postmenopause, signs of uterovaginal atrophy develop | |
Symptoms | Reduction of fertility | Vasomotor disorders may occur (hot flushes) | Signs of uterovaginal atrophy and general senescence |


Perimenopause or Climacterium
- A comprehensive term encompassing three distinct phases: perimenopause, menopause, and postmenopause.
- Represents the transitional period from reproductive maturity to the onset of senescence.
- Impaired ovarian function before 40 years
- Clinic & Tx similar to menopause
- Causes:
- Familial
- Chemo- or radiotherapy
- Autoimmune or Genetic disorders (Fragile X carriers, Turners)
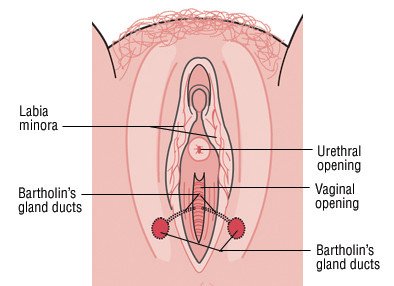
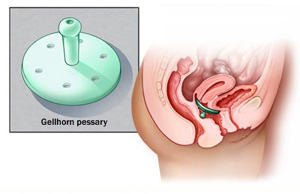
- Vagina
- center of vagina (equal anterior and posterior distance to walls)
- at 8-10cm depth (compared to introit of vagina)
- Abnormal location: tumor? (uterine, adjacent organs)
Condition | Non-Pregnant Woman | Cervical Fibroids 📷 | Pregnant Woman |
Cervical Consistency | Firm, Elastic | Rough | Softened |
⇒ 📷
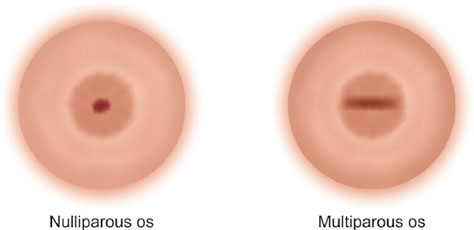
- Nulli: Conical + punctiform ext. orrifice
- Multi: Cylindrical/Bivalve + transverse ext. orrifice
- Dimensions:
- An important marker is the comparison between the length of the cervix and that of the uterine body.
- In adult women, a normal ratio is 1:2.
- This ratio is reversed in girls.
- Mobility:
- The cervix is mobile in all directions.
- It allows for a 2-3 cm displacement.
- Pouches
Anterversion flexion 📷 vs Retroversion flexion 📷! → Anteversion-flexion: easily palpated; Retroversion-flexion: difficult to palpate
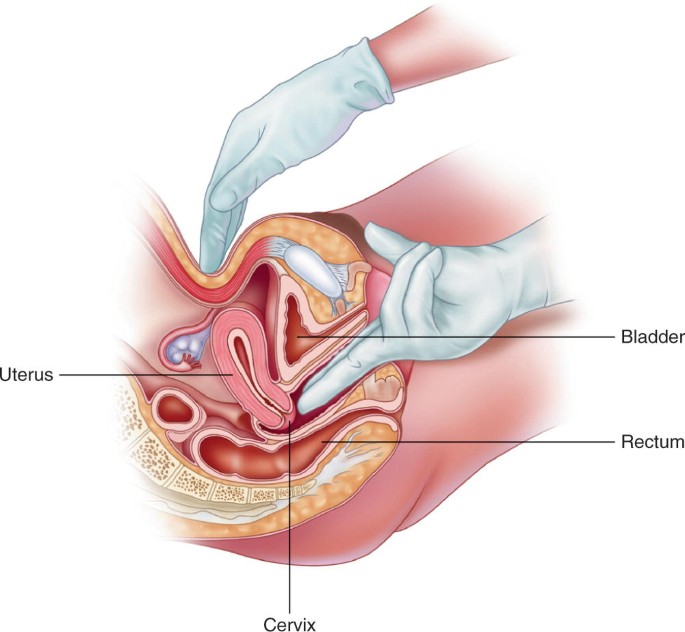
- Anteversion-Flexion:
- Typically, the uterus can be easily palpated between the two exploratory hands in most cases.
- Retroversion-Flexion:
- In situations involving retroversion-flexion, the uterus may pose challenges in palpation between the two exploratory hands or even become inaccessible.
- Efforts can be made to retrieve the uterine body, although success may be limited, particularly when evident adherences are present.
- Measurement Difficulty:
- The size of the uterus can be easily measured through bimanual examination in an anteverted uterus.
- In contrast, it is more challenging to measure the size of a retroverted uterus, which often feels larger during vaginal touch.
- Expressing Uterine Size:
- To convey the size of the uterus accurately, one can compare it to that of a pregnant uterus of a specific gestational age.
- Uterine Volume:
- The volume of the uterus may vary:
- Small: Occurs before puberty or during menopause.
- Large: Notably during pregnancy, in cases of tumors in the uterine body or cervix, or due to metritis.
- Position:
- Located in the medio-sagittal plane, below the superior strait.
- It can be laterally deviated to the right or left.
- Shape:
- Typically piriform in shape.
- May be deformed in the presence of uterine fibroids.
- Consistency (similar to the cervix)
- In a non-pregnant uterus, it is firm and elastic, .
- In the case of uterine fibroids, it may feel rough.
- Mobility:
- A normal uterus is mobile in both the medio-sagittal and lateral planes.
- Limitation of mobility can occur due to various factors including uterine tumors, adnexal tumors, pregnancy, PID, peritonitis, or scarring.
- Sensitivity:
- The normal uterus is typically painless.
- Pain in the uterus can be associated with inflammatory processes, endometritis, uterine abscess, while non-complicated uterine fibroids may not cause pain.
- Palpating the Adnexa:
- Adnexa examination involves bimanual palpation in the lateral recto-uterine pouches, directed towards the walls of the excavation.
- Normal Findings:
- In a normal examination, the ovaries are the only structures palpated.
- Ovaries typically have a size similar to that of almonds.
- The normal fallopian tube is not typically palpable.
- Detecting Tumor Formation:
- When a tumor formation is detected laterally to the uterus, it's important to differentiate whether it originates from the adnexa or is part of the uterine body.
- Differentiation Indicators:
- A separation ditch is typically present between an adnexal mass and the uterine body.
- In the case of a uterine formation, this ditch is not present, and the formation moves along with the mobilization of the cervix.
- Shape:
- Cystic or solid ovarian tumors typically exhibit a round or oval shape.
- Inflammatory formations tend to be elongated and sensitive.
- Consistency:
- The consistency can provide insights:
- Cystic tumors may feel renitent.
- Solid tumors may have a rough texture.
- Tubo-ovarian abscesses may feel fluctuant.
- Mobility:
- Mobility can vary:
- Present in benign tumors.
- Reduced in malignant tumors, pelvic inflammatory processes, or intraligamentary tumors.
- Sensitivity:
- Sensitivity is an important factor:
- Ovarian tumors are typically painless.
- Adnexal inflammatory masses often cause pain.
- Torsion of ovarian masses can be painful.
- Size:
- The size of the adnexal formation should also be assessed.
- Step I - Exploration of the Vagina:
- Systematic characterization of vaginal walls.
- Step II - Examination of the Cervix:
- Utilizing a circular motion around it.
- This examination can reveal aspects related to direction, size, and volume.
- Step III - Examination of the Retro-Uterine Pouches:
- Conducted with a deep circular motion.
- Includes the examination of the pouch of Douglas.
- Step IV - Exploration of the Uterine Body:
- Requires bimanual check.
- Most information is provided by the abdominal hand.
- Step V - Exploration of the Adnexa:
- Conducted through bimanual evaluation.
- The main function is fulfilled by the vaginal fingers.
- Coitus interruptus
- Method Description:
- This method involves withdrawing the penis from the vagina before ejaculation, requiring precise control over the timing of ejaculation.
- Effectiveness:
- The effectiveness of this method is relatively low.
- It is associated with the possibility of encountering sperm cells with fecundation potential in the pre-ejaculate fluid.
- Success with this method is contingent upon the perfect control of ejaculation.
- Coitus reservatus (absence of ejaculation)
- Method Description:
- This method is primarily based on controlling nerves to delay ejaculation and determining the absence of such control.
- Regional Prevalence:
- It is frequently encountered in East and Central Asia.
- Training Requirement:
- Successful implementation of this method necessitates intensive training, which goes beyond the aspect of nerve control.
- Postcoital showers/douching
extremely low effectiveness
- Rhythm (calendar) method
- Method Description:
- This method is based on observations made regarding fertility periods over the preceding 6-12 menstrual cycles.
- It involves identifying and establishing fertile days within these cycles.
- Applicability:
- This method is suitable for women with regular menstrual cycles.
- However, its effectiveness tends to decrease in women with menstrual disorders.
- Breastfeeding
- Breastfeeding as Contraception:
- Using breastfeeding as contraception is a natural method.
- It provides protection against pregnancy without side effects.
- Encourages using other contraceptives when necessary.
- Conditions for Protection:
- Natural protection occurs when:
- Frequent breastfeeding (8-10 times a day, including once at night).
- Time between feedings doesn't exceed 4 hours during the day and 6 hours at night.
- Correct breastfeeding technique.
- Baby is under 6 months old.
- Menstruation hasn't resumed.
- Mechanism:
- Breastfeeding suppresses ovulation during lactation.
- It increases prolactin, reduces GnRH release, and inhibits follicular maturation.
- Periodical abstinence through:
- Temperature rhythm (basal body temperature) method
- Measure temperature daily at the same time, ideally in the morning after waking up, and record the data on a graph.
- During ovulation, basal temperature increases by 0.2 - 0.4°C and stays elevated until menstruation begins.
- The most fertile period (when sexual contact should be avoided) spans from 3 days before ovulation to 3 days after ovulation.
- Cervical mucus (Billings) method
- This method relies on evaluating changes in cervical mucus throughout the menstrual cycle.
- During ovulation, cervical mucus is stretchy (Insler score of 5-7 cm), clear, and feels moist.
- After ovulation, cervical mucus becomes thick or disappears.
- Sympto-thermal method
- Palpation of the cervix
- This method involves observing changes in the cervix throughout the menstrual cycle.
- Self-palpation of the cervix is performed to assess consistency and the cervical orifice.
- Key observations include:
- Postmenstrual: Firm cervix, descended into the vagina, closed cervical orifice.
- Ovulation: Moistened and softened cervix, cervical orifice with a dimple and slight opening, high cervix position that is challenging to access.
- Postovulatory: Cervix becomes firm again, and the cervical orifice closes.
Basal Body Temperature Method
Cervical Mucus Method:
Cervical Observations Method
Q. What are the natural methods of contraception? A. Combined oral contraceptives. B. Rhythm method (calendar method). C. Periodic abstinence. D. Postcoital douching. E. Withdrawal method.
Q. What are the advantages of breastfeeding as a natural method of contraception? A. It has no side effects. B. It can be used after weaning. C. It does not require material expenses. D. It prevents pregnancy by 100% in the five-year period after childbirth. (correct would be: 85-100% first month) E. It effectively prevents pregnancy for at least 6 months, possibly even longer if breastfeeding is frequent both day and night.
- Condom
- Description:
- The most widely used barrier method.
- Made of latex, available in various assortments, with a cylindrical shape.
- Can be plain or treated with lubricant or spermicides.
- Advantages:
- Effective in protecting against STDs.
- Easy to use and available over the counter.
- Can assist in treating premature ejaculation.
- Can prevent cervical intraepithelial neoplasia and HPV infection.
- Vaginal Diaphragms 📷
- Description:
- Made of rubber, available in flat, spiraled, or arched shapes.
- Various sizes for cervix adaptation.
- Requires spermicide application before use.
- Disadvantages:
- Requires proper instructions for use.
- May trigger allergic reactions.
- Demands special hygiene measures.
- Cervical caps 📷
Cervical Caps:
- Applied directly onto the cervix.
- Used by women who have difficulty using the diaphragm.
- Made of rubber.
- Size must correspond to that of the cervix.
- Requires treatment of the vagina with spermicides.
- Female condom 📷
Female Condom (Femidom, Femy):
- A barrier method designed for single use.
- Made of polyurethane with a tubular shape.
- Applied before intercourse.
- Provides protection against STDs.
- Spermicides (chemical)
Chemical Barrier Methods - Spermicides:
- Spermicides contain chemicals that immobilize or destroy sperm cells before they reach the cervix (e.g., nonoxynol, menfegol, benzalkonium chloride).
- Enhance the effectiveness of other barrier contraceptives.
- Available in various forms:
- Pellets
- Foams
- Gels and creams
- Suppositories tablets
- Disadvantages:
- Irritation and allergic reactions.
- Excessive vaginal lubrication.
- Potential sexual discomfort.
Mixed Barrier Methods - Contraceptive Sponge:
- An occlusive (mechanical) device infused with spermicide.
Number of unwanted pregnancies occurring in 100 women that correctly use a certain contraceptive method during a 12-month period.
Pearl index for different contraceptive methods: Hormonal contraception = 0,5 - 1 IUDs = 0.5 - 2 Barrier methods = 3 - 20 Natural methods = 1 - 20 Surgical sterilisation = 0,5
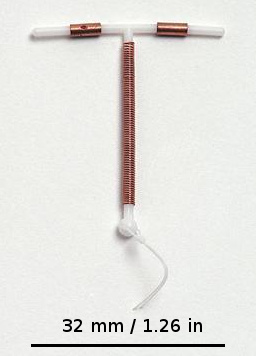
⇒ 📷
Polyethylene frame with LNG ⇒ Thickened cervical mucus (barrier) and impaired implantation
- Reduce fertility by thickening cervical mucus.
- Modify utero-tubal liquid, preventing sperm cell migration.
- Induce atrophy of the endometrium, reducing the chance of zygote implantation.

- Causes amenorrhea & improves abnormal uterine bleeding (good option if woman with heavy menses)
- Safest & most effective type of contraception
5 y
⇒ 📷

- ectopic pregnancy (if fails) - Inflammation/Infection → PID, Irritation leukorrhea - embedding in myometrium
- PROGESTIN only contraceptives
- COMBINATION oral contraceptives (P+Estrogen)
Progestin only | Combination (P+E) | |
Mechanism | • Thickens cervical mucous
• Thins endometrium to prevent implantation
• High dose blocks LH surge → absence of ovulation | • ↓ follicular growth (Øovulation) + luteolysis (E → ↓FSH; P → ↓LH)
• ↑ effects of progestins
• Main benefit: stabilizes endometrium ⇒ Less breakthrough bleeding |
Examples & Aministration | • Mini pill (norethindrone)
→ Thickens cervical mucous for 20 hours
→ Must be taken same time every day
• Implant (etonogestrel)
→ Placed in upper arm - 3-year lifespan
→ Rarely used due to irregular bleeding
• Injection: Depo Provera (medroxyprogesterone)
→ Given every 3 months
→ Irregular bleeding + weight gain | *24/4 formulations
→ monophasic/sequential/phased |
Side effects | - Irregular bleeding or amenorrhea
- Depo (Inject.) = ↓bone density (given with VitD/Calcium, Exercise)
- Mood/ Libido changes
(SE = rare in LNG IUD) | - Nausea + vomiting
- Breakthrough bleeding (if ↓estrogen component) or amenorrhea
- HT (mild) + ↑LDL/↓HDL
- Thrombosis |
Benefits | - ↑ HDL / ↓ LDL
- can be given in postpartum
- don't cause estrogen side effects | - ↓ cancer risk for ovarian + endometrial
- bleeding regulation (↓severity + irregularity)
- ↓acne |
Indications | Only in women with estrogen Contraindic. or postpartum in breastfeeding (E contraindic.) | 🥇 for hormonal contraception if Øcontraindication |
Estrogen Contraindications | ——- | Estrogen contraindications
- Smokers > 35y or non-smokers >40
- Vascular → HT or thrombosis history (DVT,PE, STROKE, MI)
- bleeding that is → undetermined or metrorrhagia
- Estrogen receptor + Cancer → Breast & Hepatocellular ADENOMA
- Liver patho
• Migraine with aura (↑thrombo risk)
- 4w prior surgery
- breastfeeding |
Types of Combined Oral Contraceptives (COC):
- Monophasic (Monodose):
- Contain the same amount of hormones in each tablet.
- Sequential:
- Imitate the hormonal profile of the menstrual cycle.
- Contain only estrogen in the first tablets, while the others have more progesterone and also some estrogen.
- Phased (Two-Phased or Three-Phased):
- Contain different doses of hormones, simulating the menstrual cycle.
COC Regimen Options:
- 24 Days of Hormone Pills + 4 Days of Placebo Pills.
- 21 Days of Active Pills + 7 Days of Placebo Pills.
The mechanism of combined oral contraceptives is due to A. Inhibition of ovulation B. Modification of cervical mucus (hostile mucus which does not allow the passage of sperm) C. Hyperplasia of the endometrium D. Hypermotility of the tubes E. Luteolysis
Contraindications for the use of combined oral contraceptives: A. Women under 35 years B. Thrombophlebitis C. Hepatic tumors D. Unexplained abdominal vaginal bleeding E. History of vascular cerebral thrombosis
The contraindications for the use of combined oral contraceptive pills are: A. History of thrombophlebitis B. Estrogen-dependent neoplasms C. History of cerebrovascular accidents D. Hypermenorrhea (Metrorrhagia) E. Within 3-4 weeks prior to surgery
Variety of surgical techniues: Abdominal, vaginal or transvaginal access:
Abdominal:
- Mini Laparotomy:
- Conducted on days 3-4 postpartum.
- Involves a reduced-size abdominal incision.
- Subsequently, the two Fallopian tubes are sectioned.
- Laparoscopy
- Laparotomy
Vaginal:
- Colpotomy
- Culdoscopy
Transvaginal:
Hysteroscopy:
- Involves a hysteroscope and a special insertion.
- Catheterizes both Fallopian tubes through the tubal ostia.
- The synthetic material inserted causes fibrosis.
- The technique is irreversible.
Q. Female sterilization is a surgical procedure that provides permanent contraception and can be performed by A. Interventional radiology B. Laparoscopy C. Minilaparotomy D. Rectoscopy E. Hysteroscopy
• Goal: disruption of Fallopian tubes → Low failure rate • Often done postpartum • Also performed outside pregnancy ("interval") • Reversible in some cases based on technique
- Medical Conditions Posing Risks in Pregnancy:
- These are medical conditions that elevate risks during potential pregnancies.
- Obstetrical Indications - Repeated Caesarean Sections:
- Permanent contraception may be recommended for individuals with a history of multiple caesarean sections.
- Genetic Indications - Family History of Transmissible Diseases:
- When there is a family history of genetic diseases with high transmission risk, permanent contraception can be considered.
- Contraceptive Indications - Intolerance to Other Methods:
- Permanent contraception becomes an option for individuals who cannot tolerate or use other contraceptive methods effectively.
⤴️ ectopic pregnancy
other:
- Complications due to the surgical procedure.
- Hormonal disorders, which can be debatable and may result from ovarian vascularity being affected.
- Menstrual changes.
- Possibility of tubal repermeabilisation.
- Ligation of bilateral vas deferens 📷
- Usually outpatient under local anesthesia
- Semen analysis 3 months postoperatively to confirm sterility
- If still sperm at 3 months → follow-up test 1 - 2 months later
⇒ Failure: if sperm at follow-up after > 20 ejaculations and > 3 months
Becomes effective only after 20 ejaculations or 3 months post-surgery.
⇒ Use alternate method of contraception until semen analysis
F → USUALLY permanent • Rare cases of recanalization (~ 0.2% of patients) • Reversal possible in some cases
- Lactational amenorrhea (unreliable)
- Barrier contraception
- Common options: IUD (copper or LNG) or progestin implant📷
→ Ø Estrogen avoided for at least 1 month postpartum • ↑ thrombotic risk • ↓ milk production
- Represents the deliberate termination of pregnancy.
- Occurs before the conceptus is sufficiently developed to survive.
- The termination method is chosen to ensure the impossibility of survival of the conceptus.
Q. Which is the correct definition of abortion:
a. Willing interruption of pregnancy in the first 12 weeks of gestation.
b. Spontaneous or induced termination of pregnancy before fetal viability.
c. Spontaneous termination of pregnancy before 20 weeks of gestation.
d. Induced termination of pregnancy before 20 weeks of gestation.
e. Pregnancy termination in the first 8 weeks of gestation.
Termination of Pregnancy in Romania:
- According to the law, termination of pregnancy at the request of the pregnant woman is legally permitted up to 3 months of pregnancy (14 weeks gestation).
- Termination after three months of pregnancy is allowed only under certain conditions.
- To save the life, health, or body integrity of the pregnant woman that cannot be saved otherwise.
- When interrupting the course of pregnancy is required for therapeutic reasons
- If pregnant woman is unable to express her will, and interruption of the pregnancy course is required for therapeutic reasons
- Pregnancy Dgx (Clinic, US, +-beta HCG)
- Determine GA (has to be <14weeks)
- History & Paraclinic
- Documentation includes a thorough examination of the physiological and pathological personal history of the current pregnancy.
- Paraclinical testing involves a comprehensive set of assessments, including:
- Pregnancy test.
- Urine analysis.
- CBC
- Blood group and Rhesus factor determination.
- Optional:
- serological tests for syphilis, Chlamydia Trachomatis, or Neisseria Gonorrhea.
- Cytotumoral examination.
- Informed consent (for termination)
Method | Mechanism | Timing | Risks | Benefits |
Medical abortion | Antiprogesterone (Mifeprestol) + Prostaglandins (Misoprostol)
→ active uterus → contractions | first 63 days (9 weeks) | Failure rate = 1,3-7,5% | ↓Morbidity+Mortality |
Menstrual aspiration | ENDOMETRIAL
aspiration | first 42 days (6 weeks) | Failure rate (0,5-3%) | ↑Safety, Øanesthesia needed |
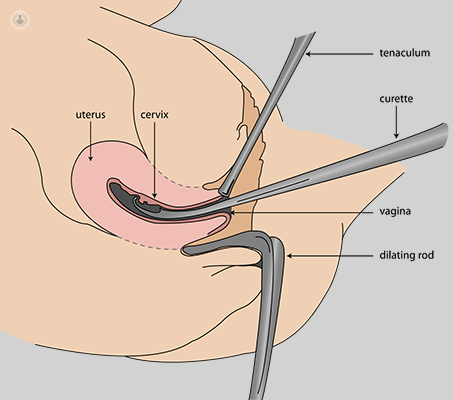
Vacuum aspiration | Cervical DILATION + Aspiration of GESTATIONAL SACK | 1. Trimester | HIGHEST SAFETY & EFFICANCY (↓failure, short, ↓blood loss, ↓ complications) | |
Dilation & Curretage | Cervical DILATION + Uterine SCRAPING | 1.Trimester
(when Vacuum can Ø be performed) | ↑blood loss
longer
↑tissue injury
UTERINE SYNECHIAS | |
Intramniotic instillation | Aspiration Amniotic fluid → Replacement with hypertonic NaCl solution | 2. Trimester (only) | ↑↑COMPLCATIONS (20%!):
- bleeding, infection, injury
- incomplete placental elimination
- Hyponatremia | |
Intravaginal Prostagland. | PGE2 or Misoprostol (intravaginally) → | 2. Trimester | - GI SE
- Live conception productions | |
Hysterotomy/Hysterectomy | Open/Remove uterus | 2. Trimester (only in complications or when others fail) | ↑Morbidity + Mortality |
IMMEDIATE:
- Damage to Cervix or Uterus
- HEMORRHAGE (due to lesions or uterine atony)
- UTERINE PERFORATION (might lead to hemoperitoneum)
- Cervical lesions
- Anesthetic risk
LATE:
- THIRD DAY syndrome (painful contraction + metorrhagia after vaccum/D&C)
- This syndrome is characterized by the occurrence of hematometra due to cervical spasm following vacuum aspiration or dilation and curettage.
- It manifests through painful uterine contractions associated with metrorrhagia.
- INFECTION
- others
placental retention, Rhesus iso- immunization, infertility, psycho-affective sequelae.
- Vaginal Agenesis (Aplasia) 📷
- Complete
- Muellerin agenesis (only UPPER part)
- Vaginal Septa 📷
- Longitudinal
- These septa have a mid-sagittal orientation within the vagina.
- They can be either partial or complete and may result in a "double vagina" appearance.
- Longitudinal septa can be associated with malformations of the uterine body or cervix.
- Diagnosis may be delayed if external genitalia appear normal, with symptoms such as dyspareunia (pain during intercourse) or dystocia during childbirth leading to diagnosis.
- Treatment typically involves the surgical incision of these septa.
- Transverse (→ see amenorrhea)
Longitudinal Septa:
- Morphologically, the uterus exhibits small dimensions and often assumes a hyper-anteverted or hyper-retroverted position.
- This condition is frequently linked to symptoms such as amenorrhea (absence of menstruation), dysmenorrhea (painful menstruation), infertility, or miscarriage.
- Uterine hypoplasia may also co-occur with other forms of pelvic-genital hypoplasia.
- RARE: These are uncommon disorders and often go undiagnosed.
- The most prevalent types of disorders in this category include:
- Complete or partial aplasia of one or both fallopian tube horns, often associated with the absence of the corresponding hemi-uterus or even the entire uterus.
- Duplication of the fallopian tube.
- Accessory fallopian tube.
- Rudimentary fallopian tube, where the tubes appear as fibro-muscular cords without a lumen.
- Infantile fallopian tubes.
- Anomalies involving the ovaries often coincide with chromosomal abnormalities of the sex chromosomes, such as X and Y.
- The most prevalent ovarian malformations include:
- Agenesia (Disgenesis): Absence or underdevelopment of the ovaries.
- Accessory Ovaries: Presence of extra ovarian tissue.📷
- Mislocated Ovaries: Ovaries are positioned retroperitoneally, typically at the lower pole of the kidneys.
= 💥 PAINFUL menstruation
all disorders that accompany menstrual period ⇒ pain is most common symptom

pain during sex

Primary
- Crampy lower abdominal pain during menses + Ø identifiable disease to explain clinical picture
- Patho: ↑ uterine PG production → contractions and pain
- Treatment: - NSAIDs - COCs (progestins → relaxation of uterus) - non-pharma (exercise, massage)
Secondary
- Onset > 25 years
- Non-midline pain
- Ø other menstrual symptoms (nausea, headache)
- Abnormal uterine bleeding (AUB)
- Dyspareunia / dyschezia
- progression: symptoms get worse over time

- 🤰🏼Pregnancy
- 🍫 Endometriosis + Adenomyosis
- 👛 PID
- 🚧 Obstructed menstrual flow:
- Fibroids
- Obstructive polyps
- Uterine adhesions
- Cervical stenosis (post cervical surgery)
- Endometriosis
- Adenomyosis
- Uterine polyps
- Uterine anomalies (e.g., non-communicating uterine horn)
- Leiomyoma
- Intrauterine synechia
- Ovarian cysts
- Cervical stenosis
- Imperforate hymen
- Transverse vaginal septum
- Pelvic inflammatory disease
- IUD (copper)
- Foreign body

Ultrasound - ovarian endometrioma 📷

Common locations • Ovaries • Fallopian tubes • Uterus • Cul-de-sac (behind vagina) • Broad / uterosacral ligaments • Round ligaments • Sigmoid colon or appendix
- White, young, skinny, academic woman without kids 📷
- White woman
- Aged 30-40 (mainly > 25 years old)
- Possesses an increased educational level
- Thin
- Experiences regular ovulatory menstrual cycles
- Nulliparous (has not given birth)
- Congenital anomalies of the genital tract (obstructive)
- Abundant menstruation
- Family history (7-10 times increased risk if there is a affected 1st-degree relative)


- Dysmenorrhea
- Cyclic menstrual pelvic pain
- Classically 1 to 2 weeks before menses
- Out of proportion to bleeding
- Dyspareuria
- Painful intercourse
- Ectopic tissue near vagina
- Infertility
- Inflammatory changes impair fertility
- Dyschezia
- Painful defecation
- Ectopic tissue near rectum
- Dysuria
- Painful urination
- Ectopic tissue near bladder
- Improves at menopause and in pregnancy
- Increased risk of ovarian epithelial cancer
displaced*:


⇒ Negative sliding sign

BIOPSY =definite dgx (often only empirix Tx without definite Dgx)


Physical Exam
- May be normal
- Location-specific changes
- Vaginal tenderness
- Cervical motion tenderness (dull)
- Nodules along uterosacral ligaments 📷
- Ovarian /adnexal mass
- Normal uterus size (Enlarged uterus: adenomyosis)
- Anatomic distortions of uterus
- Lateral displacement
- Retroverted uterus
- May be caused by adhesions
External Endometriosis: External endometriosis can be further divided by location into:
- Genital:
- Ovary
- Fallopian tubes
- Broad ligaments
- Extra Genital:
- Rectum
- Urinary bladder
- Omentum
- Bowel loops
- Genital:
- Vulva
- Vagina
- Cervix
- Scars
- Extra Genital:
- Umbilicus
- Scars
- Liver
- Kidney
- Pleura
- Lung

- Easy: Recent isolated lesions
- Moderate: Affects both ovaries, with scars or retractile lesions
- Severe: Ovarian lesions over 2 cm with extensive scars and adhesions
- Stage I: Implants below 5 mm on the pelvic peritoneum, with minimal adhesions
- Stage IA: Endometriosis of the ovaries, but the rest of the small pelvis is free of disease
- Stage IB: Incipient disease of the fallopian tubes, which remain permeable
- Stage III: Extended adhesions with distortion of the tubes and ovaries
- Stage IV: Extra-genital disease involving the bladder, bowels, and lungs


- #1 Combination oral contraceptive pills (COCs) • Cause atrophy of endometrial tissue • Progestin-only • additive: Nonsteroidal anti-inflammatory drugs (NSAIDs)
- GnRH antagonists • ↓ LH/FSH production → ↓Estrogen → Improves endometriosis-related pain • Immediately effective (contrast with GnRH agonists) • SE: hot flashes, night sweats
- #2 GnRH Agonists • Binds to GnRH receptors in pituitary → Down-regulation →Pituitary desensitization → LH/FSH • Leads to amenorrhea and endometrial atrophy • May be given with estrogen/progestins • Minimizes hot flashes and menopausal symptoms
- Surgical removal (laparoscopically) • for refractory cases • definitive diagnosis & excludes other pathology • Remove endometrial tissue
Q. Choose the false statements regarding endometriosis:
A. Endometriosis is a disease in which an active, functional endometrial tissue is ectopically implanted outside the uterine cavity. (correct)
B. Endometriosis is a disease in which an active, functional endometrial tissue is ectopically implanted outside the uterus.
C. Congenital obstructive malformations of the genital tract constitute a risk factor for endometriosis. (correct)
D. In endometriosis, the ectopic endometrial tissue is transformed outside the uterine cavity, but it does not suffer the same cyclic modifications as the normal uterine endometrial tissue does.
E. The principle behind the treatment in endometriosis is to induce a state of endometrial hyperplasia.
Adenomyosis | Endometriosis | |
Patho | Endometrial tissue INSIDE uterus → MYOMETRIUM | Endometrial tissue OUTSIDE of uterine cavity |
Clinic | ||
Age | >40y (→Øinfertility) | >25y |
dysmenorrhea | ✅ | ✅ |
location specfic pain (dyspareuria, dyschezia) | ✅ | ✅ |
bleeding | ↑ (Menorrhagia)
drain through vagina | ↓ (out of proportion to dysmenorrhea)
Ødrainage through vagina |
Associated w/ | external Endometriosis (often co-exists) | Ovarian cancer |
Paraclinic | 🦇US (pelvic) → normal sized uterus |

⇒ 📷

**SERM = Selective Estrogen Receptor Modulator (or SPRM → Progesteron)
- Multiparity
- Age (late reproductive period, 40-50 years)
- Hyperestrogenism
- Coexistence of leiomyomas, endometrial hyperplasia, endometrial cancer
- Uterine trauma at birth
- Prior surgical interventions involving the uterine cavity
- Previous acute PID
- Age < 30 years
- Risk factors for STI (chlamydia and gonorrhea)
- “Introduction”
- Vaginal douching
- IUD (within the first 10 days after insertion)
- Invasive gynecologic procedures (D&C, endometrial biopsy)
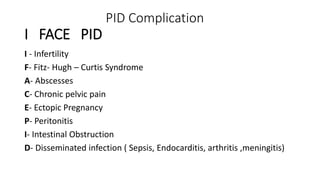
- Pelvic PAIN (Ønecessarily during menstruation)
- SYSTEMIC signs → fever, chills, ↑leukos
→ RUQ pain → Fitz-Hugh-Curtis (Perihepatitis) 📷
Spread of infection ⇒ Inflammation of liver capsule
Tx = same as PID
Definite Dgx: laparoscopy: "Violin string" adhesions
Gyn exam:
- TENDERNESS:
- Cervical motion (🛋️ ”Chandelier” signs) tenderness
- Uterine / Adnexal tenderness
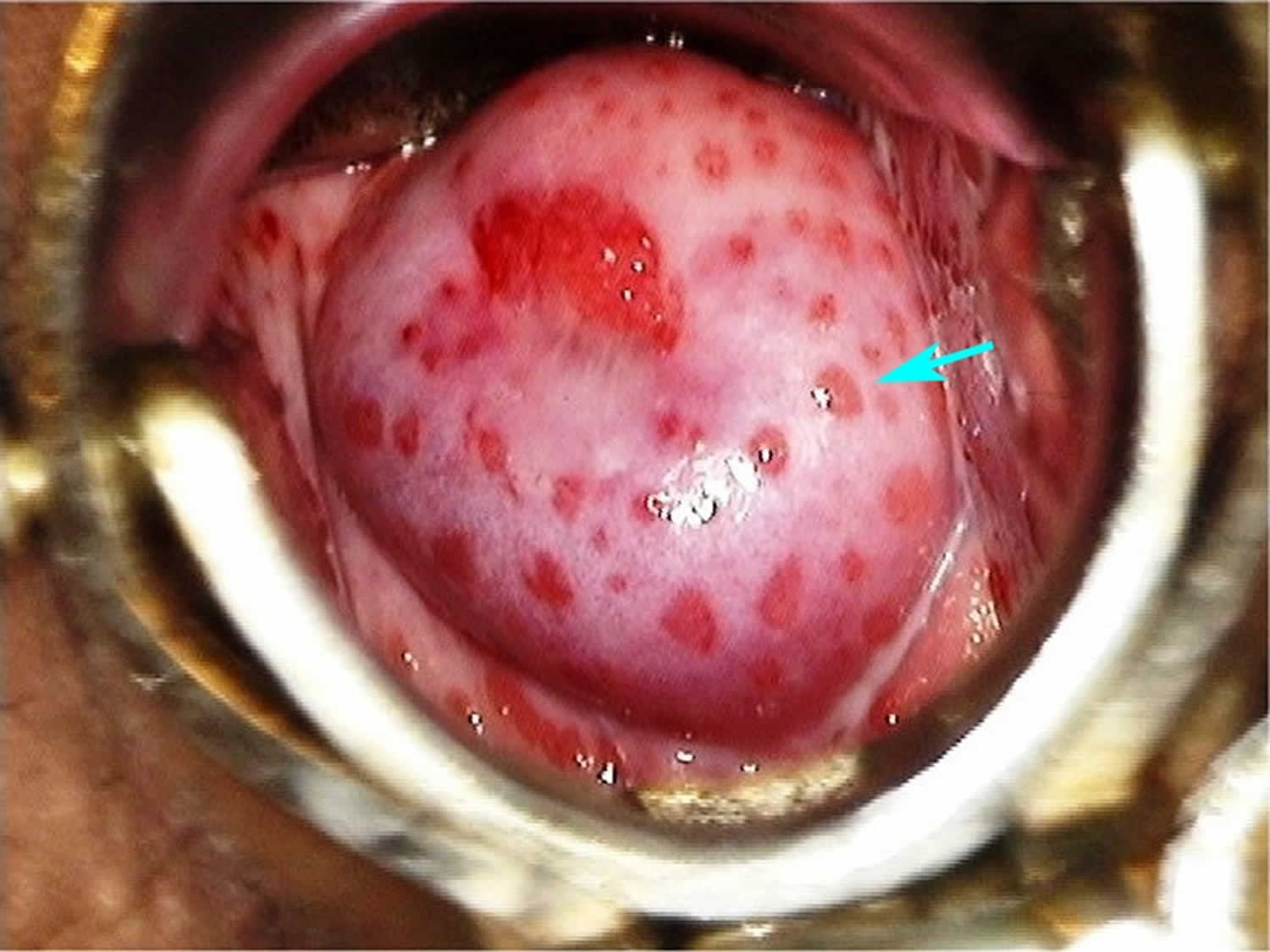
- purulent DISCHARGE 📷 + CERVICAL BLEEDING (”spotting”)

MINIMUM:
- PAIN (pelvic/lower abdominal)
- TENDERNESS (severe cervical motion / uterine / adnexal)
Additional:
- Temperature > 38°C (101°F)
- Mucopurulent cervical discharge
- Leucocytosis > 10,000
- Elevated ESR (>15 mm/h) or CRP (> 3 mg/L)
- Cul-de-sac fluid, pelvic abscess, or inflammatory mass on ultrasound or gynecological examination
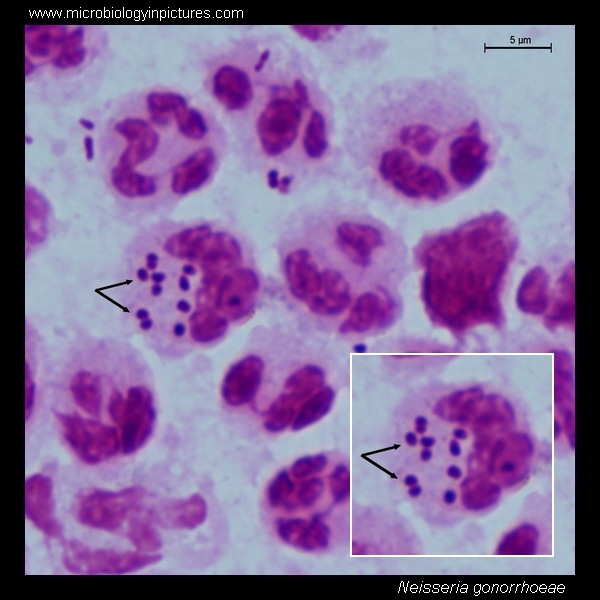
- Positive Gram stain or laboratory documentation of cervical infection with Neisseria gonorrhoeae, Chlamydia trachomatis (NAAT = Dgx tool of choice), or culture for the latter or another vaginal abnormal flora
- High-risk partner
If severe (↑fever, n/v, ↑pain, hospitaliz):
→ 🦇 TRANSVAGINAL US ⇒ EXCLUDE Tubo-Ovarian Abscess
Inflammatory mass in fallopian tubes or ovary → Similar clinic to PID
⇒ May rupture → peritonitis
DDx pelvic pain
- Ectopic pregnancy
- Adnexal complications (torsion, bleeding)
- Appendicitis or other types of acute abdomen involving lower abdominal pain
- Endometriosis
- Enteritis
- Septic incomplete abortion
- Diverticular abscess
HIV, Gonorrhea, Chlamydia
cover G+ (chlamydia), G- (gonorrhea), & anaerobes
inpatient → “Foxy doxy” = cefoxitin (iv) + doxy (po)
outpatient → Ceftriax (im) + doxy (po) [=standard gonorrhea+chlamydia tx]
#1
Regimen A: cefoxitin 2g IV q6h + doxycycline 100mg IV/PO q12h
Regimen B: clindamycin 900mg IV q8h + gentamicin loading dose 2 mg/kg IV/IM followed by 1.5 mg/kg IV/IM q8h
↓
#2 (Ø response to ABs)
Laparoscopic drainage
↓
#3
Surgery (options: salpingectomy, total abdominal hysterectomy, bilateral salpingo-oophorectomy)

- Before puberty
- During pregnancy and lactation
- During menopause

Definition | |
Primary Amenorrhea | - Absence of menarche by the age of 14 years, without developed secondary sex characteristics
OR
- absence of menarche by the age of 16 years, with developed secondary sex characteristics |
Secondary Amenorrhea | Appearance of amenorrhea after a period of regular menstrual cycles |

Location | Primary | Secondary |
🤰🏼 Pregnancy (+Lactation) | ✅ | ✅ |
🧠 Hypothalamic-pituitary | 1) Functional hypothalamic amenorrhea
2) Constitutional Delay of puberty
3) GnRH deficiency
4) Hyperprolactinemia
5) Tumors (craniopharyngioma 📷) | 1) Functional hypothalamic amenorrhea
2) Hyperprolactinemia (prolactinoma or antipsychotics)
3) Sheehan synd (post-partum pituitary infarction)
4) Tumors |
🥚 Ovaries | 1) Turner synd
2) Radio/Chemo (in childhood) | 1) Menopause (+ primary ovarian insufficiency)
2) PCOS |
🚧 Anatomic
(obstruction) | 1) Upper genital tract:
- Mullerian agenesis
2) Lower genital tract:
- Imperforate hymen
- Transverse vaginal septum | 1) Asherman syndrome (uterine adhesions) |
🧪 Hormonal | XY w/ female appearance but Ø ovaries:
1) Androgen insensitivity
2) 5-alpha-reductase deficiency | 1) Thyroid + Parathyroid (↑/↓)
2) ↑Steroids (drugs, cushings)
3) Cirrhosis (metabolic disruption) |
💊 Drugs | Sprinolactone (Anti-Androgenic)
Antipsychotics (↑PRL)
Steroids |
beta hcg
All ↓
TEMPORARY defect in GnRH release from hypothalamus
= familiar (family members that are “late bloomers” too) ⇒ Evtl. NORMAL PUBERTY at LATER age
boys (if in female → amenorrhea)
- X-ray of the left hand and wrist
- Determination of bone age based on population norms
- Utilized in children with abnormal growth patterns
- If bone age is less than chronologic age, it may indicate constitutional delay of growth and puberty, with the expectation of eventual growth catch-up.
- If bone age is identical to chronologic age, it may suggest familial short stature.
GnRH deficiency + 👃🏼Anosmia
Autosomal dominant, autosomal recessive, and X-linked forms
boys (if in female → amenorrhea)
↑Stress → ↓GnRH

Stress = Eating disorder, excessive exercise, weight loss, emotional stress
secondary
↑PRL → ↓GnRH → ↓LSH/FSH
🚱Amenorrhea + 🍼 Galactorrhea
- 🐄 Prolactinoma
- Often only 🍼galactorrhea and 🚱amenorrhea
- +- Headaches or 👁️ visual loss
- Diagnosis: MRI
- 💊😵💫 Antipsychotics (Dopamine blockade -> ↑ prolactin)
- Tumor
- Sheehan
↑FSH/LH (compensatory)
Q. Which endocrine organ has an abnormal function in women with amenorrhea with both FSH and LH high values?
A. hypothalamus
B. hypophysis
C. ovaries
D. uterus
E. suprarenal glands
- Turner syndrome +chemo/RT
- Menopause
Genetics + Diet/Obesity
↓
- Insulin Resistance → Diabetes
- ↑LH + ↓FSH → ↑Androgens
→ ↑Testosterone → Hirsutism + Acne
→ ↑Estrogens → ↑LH
↓
↓FSH:
→ Anovulation (Amenorrhea + Infertility)
→ Cysts

- Menstrual cycle with Ø ovulation
- No corpus luteum → No switch to progesterone secretion → Excessive endometrial growth from estrogen (unopposed growth = Øprogesterone) → irregular bleeding
2 ouf of 3 required:
- 🚱 Oligo-/Amenorrhea
- 💪🏼 ↑Androgens: Lab or Clinic (hirsutism, acne)
- 🎈 Polycystic ovaries by ultrasound 📷
Other potential findings:
- LH and FSH may be within normal range
- LH:FSH ratio usually > 2:1 or 3:1
- ↑ estrogens
- 📐Non-classic congenital adrenal hyperplasia (21-hydroxylase defic.) 📷
- Measure 17-hydroxyprogesterone
- High level (greater than 200 ng/dL) suggest NCCAH
- 🦀 Androgen-secreting tumors
- Ovarian or adrenal tumors
- Often very high serum testosterone (> 150 ng/dL)
1) Insulin resistence / Diabetes Tx
- ⚖️ weight loss
- Drugs:
- 💊 ORAL CONTRACEPTIVES (supress LH → ↓androgens)
- 🌊 SPIRONOLACTONE (block androgens)
- 🍬 if diabetes → METFORMIN and thiazolidinediones (GLITAZONES)
2) Infertility Tx
- #1 ⚖️ weight loss (→ ↓ estrogen)
- #2 🥚 Ovulation-triggering drugs: Clomiphene, Letrozole

- 🍬 Diabetes including Acanthosis nigricans

- 🦀 Endometrial cancer (endometrial hyperplasia)

administration of Progestin (oral / im)
⇒ if BLEEDING (within 7 days) = ANOVULATION (i.e. PCOS)

⇒ if Ø BLEEDING = OVARIAN FAILURE [ØE product.] (i.e. Menopause) OR ANATOMIC OBSTRUCTION (i.e. Asherman → see later)

→ External genitalia + Ovaries = normal
→ Ø cervix + uterus (+fallopian tubes)
→ Shortened vaginal canal or small pouch or dimple at vaginal opening 📷
- Amenorrhea (primary)
- Normal secondary sexual characteritics (Ovarian functional → normal hormones)

Imperforate hymen | Transverse vaginal septum |
Amenorrhea | Amenorrhea |
cyclic pelvic PAIN (dysmenorrhea) | cyclic pelvic PAIN (dysmenorrhea) |
BULGING obstruction on exam (+- pseudotumor = retrograde blood-accumulation) | SEPTUM on exam |
XY ⇒ ØOvaries → ØMenstrual cycle
Mutation of Androgen receptor in XY individuals:
- Testis stay in abdomen ⇒ Øinternal female genitals (”blind vagina”) → Øovaries ⇒ amenorrhea → Sertoli cells produce Müllerian-inhibiting hormone → ØUterus/Cervix/Fallopian tube
- Ø response to androgens → female external appearance → Øinternal/external male genitals
- Amenorrhea (at puberty)
- Female appearance
- ↑Testosteron (at puberty)
- ØArmpit/Pubic Hair
- ↑ Breast development


🦇 US → ØUterus/Cervix
🧬 Karyotyping → XY
🧪 Lab: ↑Testosterone
Remove testes at puberty
Autosomal recessive disorder
46,XY individual able to make testosterone ⇒ but Ø DHT (important for EXTERNAL male genitals)
⇒ Ø male EXTERNAL genitalia (⇒ mainly female instead)

⇒ NORMAL INTERNAL male genitalia: Testes present > variable location with blind ending vagina
⇒ At Puberty: Testosterone produced ⇒ MASCULINIZATION (muscles, hirsutism, deep voice, phallic growth)
🧬 Karyotype 🧪 Lab: ⇒ normal Testo; ↑Testo/DHT ratio
Multiple mechanism → ANOVULATION
Supression of GnRH → ↓LH/FSH → ↓Estrogen
- Cushings
- drugs
⇒ METABOLIC: DISRUPTION of SEX-HORMONE BALANCE
→ variable levels of T, E + PRL

- Anti-androgen ⇒ disrupts estrogen/androgen balance
- May stimulate progesterone receptors
- 😵💫 Antipsychotics
- 🌝 steroids

T ⇒ 🥇SCC
F ❌ ⇒ SLOW spread (usually STAYS NEAR VAGINA)
T ✅
⇒ DDx with skin BIOPSY ⇒ Tx: 🔪 excision or ☢️ Radio/Brachy


⇒ Vaginitis
- 🥇 = 🧫 Infection (incl. STDs)
- 🧪 Irritation/Allergy
- 🪛 Foreign body
- 🍬 Diabetes

Alteration of vaginal flora → ↓ in lactobacilli (maintain low pH) → ↑ growth of other species: esp. Gram-negative rods ⇒ Major G- rod: Gardnerella vaginalis
- Sexual activity (Vaginosis is not classified as STD! [Ø specific pathogen])
- Vaginal Douching
- Smoking
- Thin, white, yellow, homogeneous discharge
- Presence of clue cells on microscopy 📷 (Epithelial cells studded with bacteria)
- Vaginal fluid pH > 4.5
- Fishy odor release upon adding 10% potassium hydroxide (KOH) solution









Risk factors* ⇒ ↓Immunity ⇒ Overgrowth Candida albicans (mainly - 90%)

*Risk factors:
- 💊AB
- 🍬Diabetes
- 👾 Immunosuppression
ph = NORMAL (in contrast to Vaginosis + Trichomonas)
🔬 → KOH wetmount ⇒ Pseudohyphae 📷 (KOH wet mount negative in Vaginosis + Trichomonas);
rarely culture is done
💊 → Antifungals (Oral 🐒 fluconazol or other topical azoles)



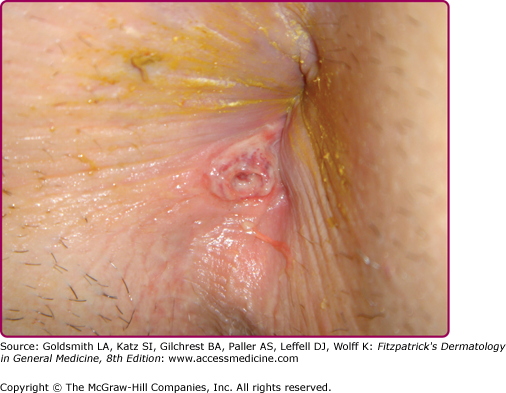
Gumma 📷
Other:
- Tuberous syphilids (Tubero-serpinginous 📷 and tubero-ulcero-serpinginous 📷)
- Cardiac
- Aortitis
tubero-serpiginous: -red, brows -flat-topped red papules -progress periph. -heal centrally with atopy + pigm. changes
tubero-ulcero-serpinginous
- same as tubero-serpiginous +ULCER

- Focal Gumma
- Meningo-vasc. Syphilis
- General paresis
- Argyll-Robertson pupil
- Deafness
- Tabes dorsalis

early: <2 yo
late: >2 yo

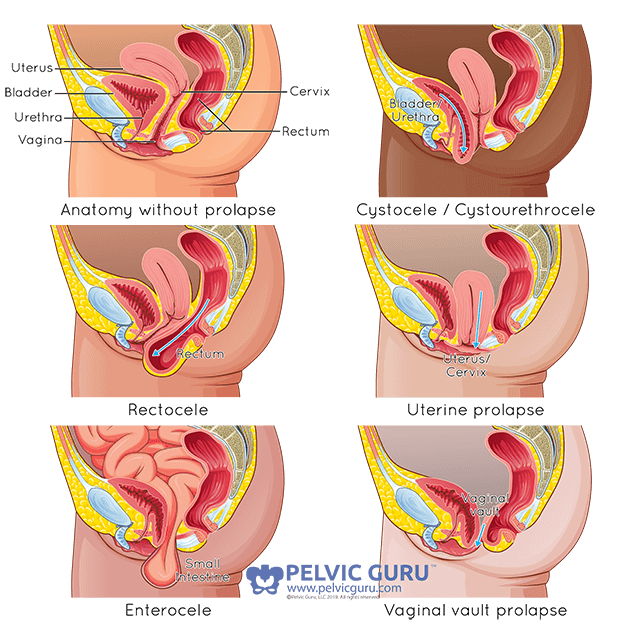
descent of pelvic organs (herniation) to or beyond the vaginal walls
- Vaginal wall prolapse
- Anterior vaginal wall prolapse: herniated anterior vaginal wall, which is often associated with
- cystocele (descent of the bladder)
- urethrocele (descent of the urethra);
- Posterior vaginal wall prolapse: herniated posterior vaginal wall, which is associated with
- enterocele (herniated section of the intestines);
- rectocele (descent of the rectum)
- Uterine prolapse: descent of the uterus
- Vaginal vault prolapse: descent of the apex of the vagina (often after hysterectomy)
→ can be due to weakness of the pubocervical fascia 📷
→ can be due to weakness of the rectovaginal fascia 📷
- 🕳️ Pelvic floor WEAKNESS
- Gestational characteristics: ligaments + pelvic floor extension&relaxation during birth
- Conjunctive tissue abnormalities
- conjunctive tissue DEFICIENCIES
- Endocrine: E-DEFICIENCY→ ATROPHY of conj. tissue
- 💥 Pelvic floor TRAUMA
- during Birth
- Iatrogenic (surgery, brutal maneuvers, incorrect forceps use)
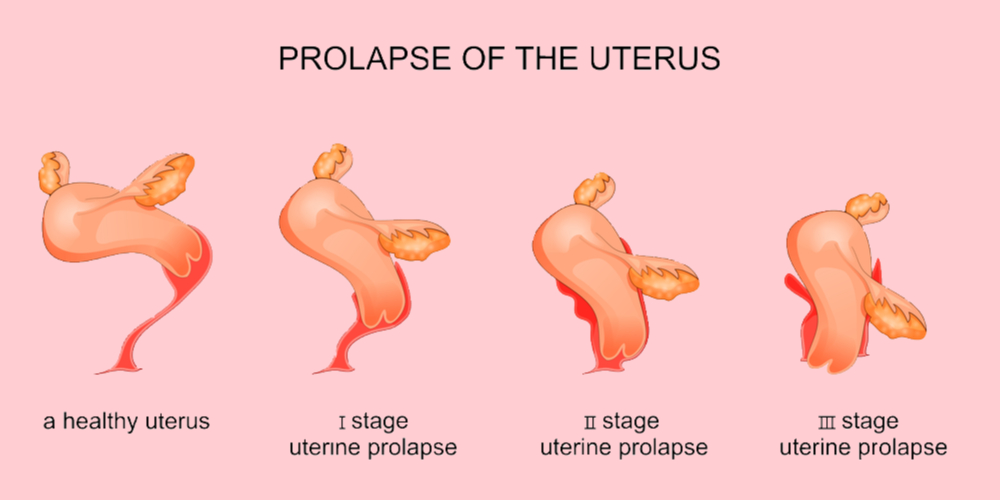
Degree | Description |
I | Uterus is descending but behind vaginal introit |
II | Uterine cervix is at the level of the vaginal introit |
III | Uterus is completely exteriorized |
- loose weight
- avoid constipation (↑fibers+fluids)
- Østraining during defacation
- Øheavy lifting
- control coughing
- Pelvic Floor Repair Surgery: This procedure involves the repair of weakened pelvic floor tissues. It is typically performed through the vaginal route but can sometimes be done abdominally. The surgeon may use your own tissue, donor tissue, or synthetic materials to reinforce weakened pelvic structures and support your pelvic organs.
- Hysterectomy: In certain cases of uterine prolapse, a hysterectomy may be recommended. While hysterectomy is generally considered safe, it is important to be aware that all surgeries carry some risk of complications.
- STRESS incontinency ⇒ ↓strenght of pelvic floor muscles ⇒ cant hold during stress (i.e. cough)
- URGE incontinency ⇒ sudden urge
- other types
- mixed
- transient (drugs, infections, stool impaction, restricted mobility)
- functional (↓mobility, cant reach)
- Confusion
- Dementia
- Impaired eyesight
- Limited mobility
- Poor dexterity
- bedwetting (young children)
- structural (malformation)
Functional incontinence can result from various factors, including:
- Most will clear infection within 12 months
- Some will have infection persist ⇒ Cervical cancer:
- HPV 16: 50% of cases
- HPV 18: 20% of cases
- Others: HPV 31, 33, 45, 52, and 58
- Related to Sexual behaviour
- HPV infection or history of other STD
- sex at young age
- multiple partners
- Smoking
- Immunodeficiency
- Hormonal factors
Q. It isn't a risk factor for cervical intra-epithelial neoplasia (CIN) A. HPV infection B. Smoking C. Immunosuppression D. Hormonal factors E. High socioeconomic level
→ E) Low socioeconomic level (only listed for carcinoma; Ø CIN)

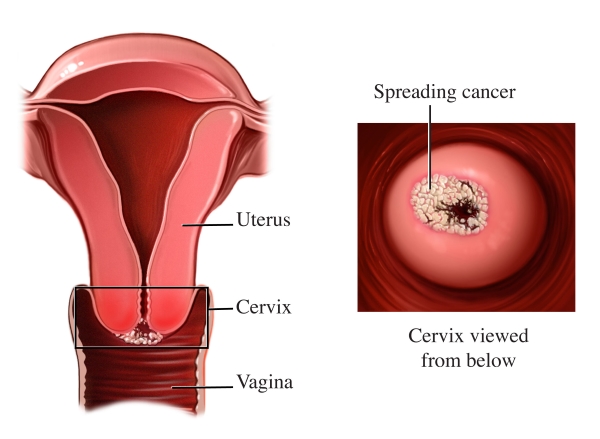
- Squamocolumnar junction
- Junction between squamous and columnar epithelium
- Endocervix: columnar epithelium
- Ectocervix: squamous epithelium
- Transformation zone
- SCJ moves from exposure to hormones
- TZ: area between original SCJ and new SCJ
- Most (95%) cancers arise here
Q. Which part of the cervix do cancerous lesions begin: a. Exocervix b. Endocervix c. Squamo -columnar junction d. External cervical ostium e. Internal cervical ostium
HPV testing (PCR) ⇒ identifies HPV-INFECTION (Øcellular changes)
PAP smear ⇒ epithelial CELL changes (Koilocytes) due to HPV 📷
Bethesda system “Squamous intraepithelial lesions” (SIL) | Cervical intraepithelial neoplasia (CIN) | WHO | |
Atypical cells | ASC-US + ASC-H | Atypia | Atypia |
Low grade lesion
⇒ 📷 | LSIL | CIN 1 | Koilocytes |
High grade lesion ⇒ 📷 | HSIL | CIN 2 + 3 | Moderate / Severe dysplasia + CIS |
Invasive carcinoma | When passing BM | When passing BM |
- CIN1 (corresponds to mild dysplasia)
- CIN2 (moderate dysplasia) - anomalies are present in the 2 / 3 basal epithelium.
- CIN3 (severe dysplasia and intraepithelial cancer) - anomalies are present in all epithelial structure.
→ the anomalies described are present in 1 / 3 basal epithelium, maintaining a mature aspect in superficial layers
- 🩸BLEEDING → irregular/heavy menses or POST-COITAL Discharge → initially watery, then bloody
- ↔️ Signs of INVASION → pain (pelvic/back), bladder & bowel signs (dysuria , dyschezia)

Other Investigations to Evaluate Tumor Extension:
- Pulmonary X-ray
- Urography, cystography, cystoscopy
- CT scan, MRI
- Renal and hepatic scintigraphy
- Barium enema (Irigography), rectoscopy
- Lymphography
Q. Which method allows a definitive diagnosis of cervical cancer? a. Colposcopy b. Lugol test c. Citotumoral test d. Histopathological exam e. Vaginal US
Q. What is the recommended treatment in cervical cancer stage IA2? a. Total hysterectomy b. Subtotal hysterectomy c. Wertheim total hysterectomy d. Endocervical curettage e. Cervical electrocoagulation

⇒ 📷
Q. Which of the following therapeutic methods is used to treat in situ carcinoma in a woman under 33 years old?
a. Total hysterectomy with bilateral adnexectomy b. Conization c. Cervical electrocoagulation d. Subtotal hysterectomy e. Wertheim total hysterectomy
- small elongated tumors on the cervix (usually benign )
- might cause
- bleeding
- abnormal pap smear
- Tx: Polypectomy
Screening → normal, like non-pregnant (abnormal PAP ⇒ colposcopy); if last screening >1y → screen in first 6w of pregnancy Biopsy ⇒ only if high risk APPEARANCE (Raised masses, ulcerative lesions) Excision ⇒ only considered if INVASIVE CA (beyond BM) → delay Tx for non-invasive (CIN1-3, LSIL+HSIL) until 6w after birth (via C-section)

Carcinoma Type | Treatment Approach and Details |
Micro invasive carcinoma | - Diagnostic conization, followed by a conservative approach until birth; colposcopy every 2 months.
- Birth when fetal viability is reached
⇒ caesarean section
⇒ followed by total hysterectomy.
- In case of early diagnosis, patient may choose radiotherapy, followed by miscarriage. |
Invasive carcinoma | Patient choice is fundamental:
- Radical surgery with lymphadenectomy in the 1st trimester.
- C-section in 3rd trimester, followed by radical surgery. |
Advanced carcinoma | - Subtotal hysterectomy (abortion) + radiotherapy
- If Dgx close to birth:
C-section → followed by total hysterectomy + radiotherapy
|


Risk Factors (↑E) | Protective Factors (↓E) |
Weight | Oral contraception |
Nulliparity / Infertility | Multiparity* |
Black race | Smoking** |




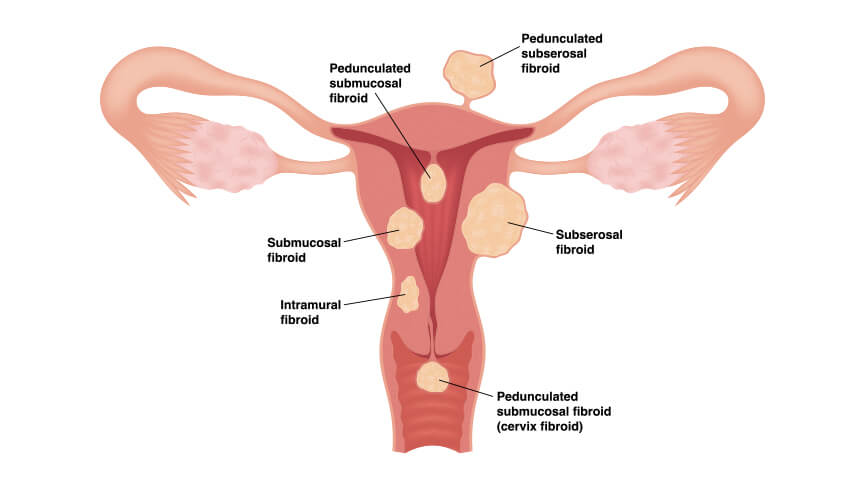
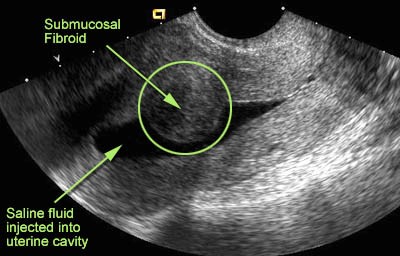
2) 🩸 BLEEDING (AUB)→ esp. submucosal

⇒ Exam: Pelvic mass (+- cervical fibroid visible)
Q. The excessive bleeding characteristic of menstrual disorders in a case of uterine fibroma is primarily due to:
a. Endometrial hyperplasia b. Chronic endometritis in a case of submucous fibroma c. The torsion of the fibroma d. Lack of elasticity at the level of the myometrium surrounding the fibroma e. Vascular ruptures inside the fibroma (??)

- 🦀 Malignancies: endometrial or surrounding (ovaries, bladder, rectum)
- ↗️ Ectopic pregnancy (or other pregnancy complications: molar pregnancy/abortion)
- 🏗️ Uterine malformations


- 📍Endometrial Polyps
- 🧺 Adenomyosis
- Uncommon malignant muscle tissue tumor of the uterus
- Typically found in women after menopause
- Often a singular large growth
- Can lead to symptoms similar to fibroids (bulk symptoms, post-menopausal bleeding)
- Higher likelihood when taking tamoxifen - a SERM (selective E-receptor modulator) used in treatments for breast cancer and infertility.
Estrogen drives endometrial growth; Growth opposed by progesterone ⇒ Excessive unopposed estrogen → abnormal growth:
- polyps
- hyperplasia
- carcinoma
- 🍳 Anovulation
- Common in PCOS
- menopause
- 🐖 Obesity
- Androgens to estrogens in adipose tissue
- 💊 Drugs
- Tamoxifen (SERM)
- Hormone replacement (pure E)
- 🦀 Estrogen-secreting tumors
(Ovaries produce estrogen, Ø progesterone)


- 0️⃣ Nulliparity

T
Hyperplastic growth of glands and stroma • Mainly benign • Little risk of malignancy (esp. post menopause) • exophytic mass projecting from endemtrium
- 🦀 Malignancy: Endometrial CA or sarcoma
- 🥮 Placental polyp (=fragment)
- ⚪ Submucosal fibromatous nodule (Fibroids)
Q. Differential diagnosis of endometrial polyps is made with:
A. Cervical polyp (??)
B. The subserous fibroma
C. Endometrial cancer
D. Endometriosis
E. The placental fragment
(A), C, E → cervical polyp is a type of endometrial polyp so its not really a DDx
Tx indications:


⇒ BIOPSY needed to differentiate (perform if 🩸 AUB + Risk factors)


Staging is established with different imaging modalities (US (thickness+vascularization, CT, MRI, PET)


- Germline mutation in DNA mismatch repair genes
- Increases the risk of colon cancer
- Elevated risk of endometrial cancer
- Regular endometrial sampling is recommended
(Most common non-colon malignancy associated with this syndrome) 📷
begin at age 30 to 35 or 10 years prior to the earliest family member
- Disease staging - the 5-year survival rate is 94% in stage I and 40% in stage III.
- Degree of histological differentiation.
- Presence of myometrial invasion.
- Presence of vascular invasion.
- Young age is associated with a better prognosis.
Q. Prognostic factors for endometrial cancer include:
A. Stadialization
B. Histopathological structure
C. Intense symptomatology
D. Myometrial invasion
E. Associated ovarian pathology
- 🥚 Ovarian causes (cyst, benign masses, malignancy)
- ✨ NEW tissue → 🍫 Endometriosis + 🥀Ectopic pregnancy
- 🟢 ABSCESS
- 🍤 bowel disorders
OVARIAN TORSION
- Intracystic hemorrhage/torsion ⇒ Rupture → pain+shock
- Compression of adj. structures
- Rotation of ovary around suspensory ligaments 📷
- Leads to ischemia and necrosis of ovary
- Acute onset pelvic pain with adnexal mass, +-radiation (flank+thigh)
- Classically waves of nausea and vomiting
- Major risk factor: ovarian mass (Especially if greater than 5 cm) → Also assoc. with ovulation induction (Can lead to large cysts)
- Functional ovarian cysts
- Follicular cyst
- Corpus luteal cysts
- Theca lutein cyst
- PCOS
→ Rare sub-type: Luteal phase cysts

Patho | PAIN | BLEEDING | |
Follicular | failure of ovarian rupture or rupture but resealed → cyst filled with E (stimulate endometrium) | ✅ | ↕️ IRREGULAR |
Corpus luteal | C.Luteum INVOLUTION fails → Cysts (mass + pain) → sustained Progesteron production (by C.Luteum) → Delayed/missed menstruation | ✅ | ❌ MISSED/DELAYED period
DDx with ectopic pregnancy (beta hcg+) |
Luteal phase | spont. BLEEDING into corpus luteal cysts → rapid enlargement → acute pain
→ if rupture → hemoperitoneum | ✅ | ❌ MISSED/DELAYED period |
Theca | Assoc. with ↑bhCG (twin, molar) → BILAT + MULTIPLE cysts: Luteinized theca cells with edema (theca hyperplasia)
⇒ cysts ↓ when beta hcg ↓ | ✅ | |
PCOS | → see PCOS
multiple cysts | ✅ | 🚱 AMENORRHEA |
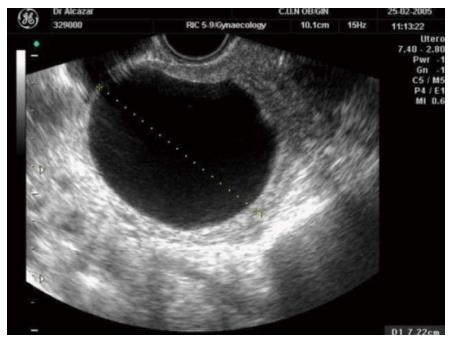
Ultrasound findings:
Follicular: 📷
- thin wall
- anechoic
- Vascularity (Doppler)
Corpus Luteal: 📷
- "RING OF FIRE": periph. vascularity (Doppler)
- thick walls
Luteal phase: 📷
- CENTER: hyperecho + heterogenous = agglutinated blood
Theca 📷
Hyperplasia of theca cells
Benign → Reassurance +/- Follow up +/- COC for functional cysts
Malignant → Surgical removal (mature teratoma, endometrioma, malignant tumor)
- Benign:
- 🥈 Teratoma → Dermoid cyst
- Stromal Tumors
- Granulosa cell tumor
- Sertoli-Leydig cell tumor
- Fibroma
- Malignant
- Immature Teratoma
- 🥇 Epithelial cell tumor
- Serous
- Mucinous
- Endometrioid
- Malignant: bilat, solid, not mobile, irregular, ascitis, demarcation notch (DDx endometrial)
- Benign: unilat, cystic consitency, mobile

/w=1920,quality=90,fit=scale-down)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- A secondary ovarian tumor originating from gastric, colon, or breast cancer.
- Incidence: 4-8%, often bilateral, may be associated with ascites.
- Clinical appearance: Well-defined, mobile, firm mass.
- Pathological anatomy: Predominantly solid with cystic, hemorrhagic, necrotic areas. Microscopically, it contains "signet-ring cells."
- Prognosis: Generally severe.
- Treatment: Surgical removal, with the primary gastric tumor also requiring surgical intervention.

Define the following terms:
Normal menstruation:

- Occurs every 24 to 38 days
- Variation less than 7 to 9 days
- Lasts up to 8 days
- Less than 80 ml of blood loss
frequent UB = more often than every 24 days
Polymenorrhea = menstrual cycles wit intervals of less than 21 days (aka more often than every 21days)
less often than every 28 days
irregular cycles > 35 days apart
more than 8 days
Heavy: >80ml / menstrual cycle (realistically not really measurable)
Hypermenorrhea = abundant menstrual flow, with a normal duration of menstruation, occurring at the normal date of menstruation
Heavy or Prolonged bleeding
- >80ml / cycle
- >8 days

bleeding between normal menses
heavy bleeding between normal menses
- STRUCTURAL
- Polyps
- Adenomyosis
- Leiomyoma (Fibroids)
- Malignancy/Hyperplasia
- FUNCTIONAL
- Coagulopathy
- Ovulatory dysfunction (Øovulation → Øprogesterone → “unopossed estrogen → irregular bleeding)
- Endometrial causes (if Øother cause)
- Iatrogenic (Drugs, IUD)
- NOS (Not other specified)

- 👵🏼 Post-menopausal woman
- 👩🏼 Pre-menopausal PLUS 🦀 RF (for endometrial CA) = excessive unopposed E
RF: Anovulatory cycles, Obesity, Nulliparity, Older age, Abnormal US lining thickness
Common Tx for many of the causes ⇒ COC

Access hemodynamic stability! → correct
Sexual response cycle ⇒ 📷
{kind=link}
absence of sexual desire
→ may occur after a period of normal sexual activity
Factors Contributing to Sexual Appetence Dysfunction:
- Diminution of estrogen production in women or testosterone production in both women and men.
- Senescence.
- Fatigue.
- Pregnancy.
- Medications:
- Antihypertensive drugs:
- Diuretics (e.g., Spironolactone).
- Methyldopa.
- Clonidine.
- Beta-blockers.
- Antipsychotics:
- Chlorpromazine.
- Risperidone.
- Antidepressants:
- Tricyclic antidepressants.
- Trazodone.
- Other drugs:
- Cimetidine.
- Steroids.
- Mental disorders ( depression and anxiety.
Types of Sexual Appetence Dysfunction:
- Hypoactive sexual disorder, often secondary to conditions like myocardial infarction or surgery (e.g., mastectomy or hysterectomy).
- Sexual aversion, which can result from sexual trauma and may involve various aspects of the sexual act (e.g., kissing, intromission).
- Symptoms include:
- Lack of vaginal lubrication.
- Reduced vaginal swelling.
- Diminished genital response to sexual stimulation.
- Both women with sexual arousal dysfunction and those without it exhibit similar psychological responses to erotic stimuli.
- Estrogen decrease (e.g., during lactation or postmenopause) is a major cause of sexual arousal disorders in women.
Anorgasmia:
- Defined as the absence of orgasm in at least 75% of cases following sexual excitement.
- Causes can be:
- Psychic (psychological factors).
- Physiological (e.g., menopause).
- Pharmacological, with antidepressants, particularly selective serotonin reuptake inhibitors, being a common culprit.
- Factors to consider when assessing anorgasmia include age, previous sexual experience, potential trauma, and adequacy of sexual stimulation.
- Women experiencing anorgasmia should be evaluated for organic or pharmacological causes.
Dysparunia → pain during intercourse
Vaginismus → involuntary spasm of vaginal muscles → dyspareunia (also pain during vaginal touch/valve insertion)
- Orientation Homosexuality: Primary attraction to individuals of the same sex.
- Inhibition Homosexuality: Occurs as a compromise due to fear or avoidance of partners of the opposite sex.
- Pseudohomosexuality: When individuals engage in same-sex relationships due to the absence of opposite-sex partners.
- Fetishism: Sexual excitement or gratification from inanimate objects (e.g., underwear) or specific body parts (e.g., foot).
- Pedophilia: Sexual arousal or satisfaction involving children.
- Zoophilia: Sexual arousal or gratification through sexual intercourse with animals.
- Exhibitionism: Sexual arousal or gratification derived from exposing one's body, especially the genitals.
- Voyeurism: Sexual arousal or gratification from observing others engaged in sexual activity.
- Masochism: Sexual arousal or gratification obtained from physical or mental pain, which can be self-inflicted.
- Sadism: Sexual arousal or gratification by causing physical or mental pain to others.