

Table of content
- Infectious Diseases
- 💊 PHARMA Tx
- 📍 FOCUS OF INFECTION
- 🫁 Respiratory tract
- 🫀Heart
- 🍤 Gastrointestinal tract
- 🎈Urinary tract
- 🧠 Nervous system
- 🖐🏾 Skin
- 🦴 Bones
- 🔥 Sepsis & Fever
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Infectious Diseases
💊 PHARMA Tx
- ✏️ Penicillin (= natural penicillins)
- ⚕️Beta-lactamase resistent Penicillins (= staph. penicillins)
- 🎸 Extended-spectrum penicillins (Aminopenicillins, other penicillins) & beta-lactamase inhibitors
- 🦑 Cephalosporins
- 🤖 Monobactams & 🚘 Carbapenems
- 🚌 Vancomycin (Glycopeptides)
- 👮🏼♂️Daptomycin
- 🚴🏾Tetracyclines
- 🦅 Macrolides
- 🧼 Clindamycin
- 🚧 Linezolid
- 🤺 Aminoglycosides
- 🧻🥚 TMP-SMX: Trimethoprim-sulfamethoxazole (Bactrim (Cotrim))
- 🌷Fluoroquinolones
- 🚇 Metronidazole
- HSV & Varicella (Aciclovir, Valaciclovir, Famciclovir 👪♻️)
- CMV (Ganciclovir 🥫♻️, Val-ganclovir, Foscarnet 🏎️🥅, Cidofovir)
- Interferon alpha
-"vir" + -"vudin"
Adolf geht vor und singt Tenor, (Adefovir + Tenofovir)
die Ente spielt Klavir (Entecavir) und das Lamm telefoniert(2x) mit Hudini (Lamivudin + Telbivudin)
- inhibit HBV-DNA polymerase
- Teno, Ade, Lami → also inhibit reverse transcriptase

- Teno
- Lami
- Ade → esp. in Lami-resistance strains

Entecavir + Adefovir
All -vir's
- Entecavir
- Tenofovir
- Adefovir
The fovirs
Teno + Ade
Lami → incr. Transferases when stopped
Telbi → Myopathy + incr. CK


Guanosin analog
→ interference with GTP synthesis
→ inhibit capping of viral mRNA
→ inhibit RNA polymerase *
- Ribavirin + IFN alpha (hepC)
- decompensated cirrhosis:
- Sofosbuvir
- NS5A protease inhib.
"Der Mexikaner lag wohl auch auf dem Sofa shit + er liebt tomatenlastiges (hemolytic anemia)Chili con carne
- hemolytic anemia
- pruritus +rash
- depression
"Auch ihm wurde an der Niere geknabbert, außerdem chillt oben in der Ecke ne Tarantula und er hat ein großes Herz. Tomaten hat er wohl zuviel gegessen"
- Anemia
- RF
- heart disease
- pregnancy (Teratogenic)
-buvir
(b für 5B; Bu = boobs)
"Da sah ich das Sofa"
Sofosbuvir + Dasabuvir
- sofa → all
"Uhr überm Sofa"
yes, uridine analogue
- NS5A inhibitors: daclata,ledip,velpat,-asvir
- Ribavirin (in decomp. cirrhosis)
- Simeprevir
"Erschöpft(Asthenia) auf dem Sofa, aber das Sofa hat Bettwanzen(itching) arrrrg das juckt. Plötzlich kommt ein Amigo (Amiodaron) und haut ihm aufs Herz"
- asthenia
- itching (pruritus)
- cardiac arrest with amiodarone
"Die Sofa-Bettwanzen knabbern an der Niere, wie ne Maus(GFR<30)"
GFR <30
-asvir
(A für 5A, as = ass)
"Ein lediger Dackel-Welpe sitzt an der Elbe"
- Daclatasvir
- Velpatasvir
- Ledipasvir
- Elbasvir
Daclatasvir + Velpatasvir
"Der Dackel Welpe der ist ja auch süß af"
all with sofosbuvir
except: Elbasvir - Grazoprevir
"Merke: in cirrhosis immer mit Riba, außer die NS3"
A für ja
yes, with ribavirin
- fatigue
- headache
- CYP450 inhib
"Vom ganzen Arschfick ist der kleine Dackel müde und hat Kopfschmerzen" "Schau mal was im Hintergrund parkt"
-previr
(act before the others → hence "pre")
2, but 1. generation replaced in HCV treatment
side effects!
- anemia
- rush + hyperbili
- Dysgeusia
Simeprevir ("simmering") → Sofosbuvir
Grazoprevir ("kratzt sich am Bein") → Elbasvir
"An der Feuerstelle ist das CYP450-Auto, eine Kamera + eine LFT Fahne"
- CYP450 inhibition
- Photosensitivity + Rash (Sime)
- incr. Transaminases +bili (Grazo)
nope
Transaminases ↑. (side effec)




(Sketchy Pharm > Antimicrobials)







(Sketchy Pharm > Antimicrobials)





Systemic fungal infection?
↓
Invasive ASPERGILLIOSIS? → Voriconazole
↓
CANDIDEMIA? → Echinocandins
↓
OTHER? → Amphotericin B
📍 FOCUS OF INFECTION
🫁 Respiratory tract
🧫 1) BACTERIAL
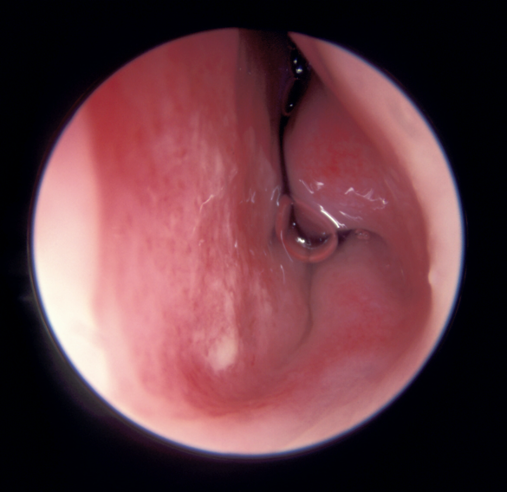
Clinical presentation:
- 🧣Signs of Infection:
- Clinical exam: Hyperremia + Congestion (+ pus) 📷
- Symptoms + Signs:
- Pharyngitis:
- like viral: dysphagia, odynophagia (sore throat)
- petechia (on pallate) 📷
- Tonsillitis
- 🧫Specific signs of bacterial infection:
- PUS
- HIGH Fever
- ↑LN
- Exanthem (⇒scarlet fever) aka scalantiform rash 📷
- Ø viral symptoms! (Øcough, Ørhinorrhea, Ø hoarseness)
⇒ Etiology: Strep. pyogenes (aka beta hemolytic GAS)

Acute viral tonsillopharyngitis: children <5 years and young adults Acute GAS tonsillopharyngitis: children aged 5-15 years; rare in children aged < 2years
Centor score
The Centor score is a clinical prediction tool used to estimate the probability of a streptococcal infection in patients with a sore throat.
A score of 0-1 is considered low risk, 2-3 is moderate risk, and 4-5 is high risk.
- The score is calculated based on the presence or absence of four clinical criteria: fever, tonsillar exudates, tender anterior cervical lymphadenopathy, and absence of cough.
- Another criteria used in the score is the patient's age, with younger patients (<15 years old) being assigned a higher point value. This is because streptococcal infections are more common in younger individuals. Specifically, patients under 3 years old are assigned 1 point in the Centor score.
- Each of these criteria is assigned a point value, and the total score is used to estimate the likelihood of a streptococcal infection.
<3years:
- 👃🏽 nasal congestion
- 🤒 low grade fever
- 🟢 cervical ↑LN
<1year:
- 🍔 ↓ appetite
- 🤒 low grade fever
- 👨👨👦👦 older siblings/contact with GAS
- Local spread
- 2)👂🏼 Otitis media 📷+ Mastoiditis
- 3) 🎛️ Sinusitis 📷
- 4) 💪🏼 Necrotizing fasciitis 📷
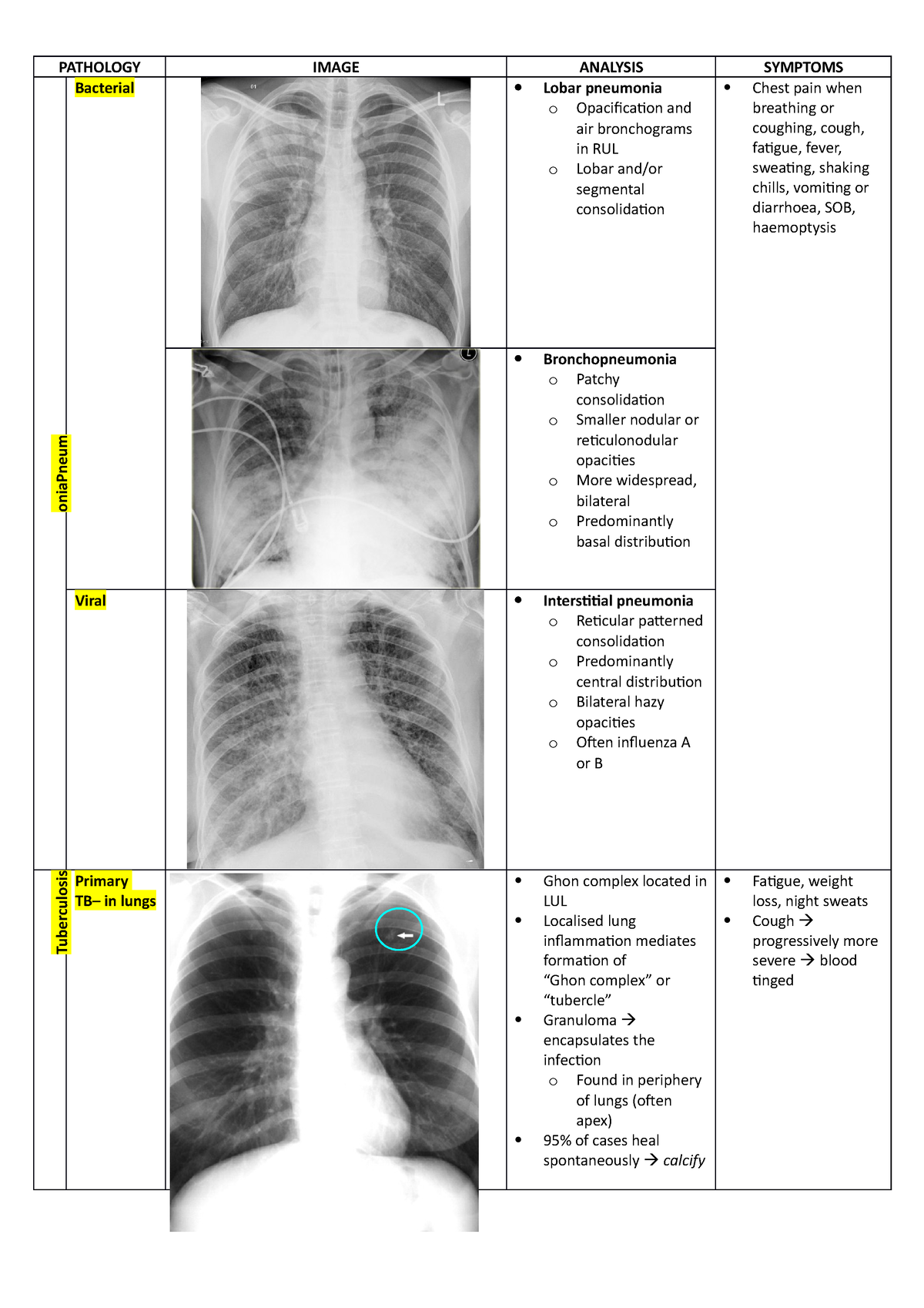
- 5) Pneumonia 📷
- Systemic complications
- Pharyngitis signs + non-specific inflammatory
- +- GI signs
- 3) ⛑️ Auto-immune
- Rheumatic fever 📷 (JONES)
- PANDAS: neuropsychiatric disorder

aka “streptococcal bacteremia”
1. TOXIC Shock-signs(i.e. ↓BP+fever) + Exanthem (measle-like) 2. Evolution: - skin desquamation - multi-organ failure ☠️
erythrogenic toxin
(makes you red 👹)
→ 🩸hematuria → RF ⇒ 🥐 ↓GFR → 💳 ↑Crea

*patho
The incubation period of diphtheria is 2-4 days.
- ONSET: It has an insidious onset with sore throat and mild pharyngeal inflammation.
- A diagnostic feature is the 'wash-leather' elevated greyish-green membrane on the tonsils, called a 🧁 pseudo membrane. 📷
- ❤️ Tachycardia, despite modest fever, is a sign of myocarditis.
- 🌕 Neuropathy
→ The pseudo membrane has a well-defined edge, firm and adherent, surrounded by a zone of inflammation. It can extend to the larynx, trachea, or bronchia → airway obstruction.
⇒ 🐂 Swelling of the neck ('bull-neck') 📷 ⇒ 🟢 tender enlargement of the lymph nodes may occur.
There are three types of diphtheria:
- 🧣Pharyngeal diphtheria: Insidious onset of exudative pharyngitis. Exudate spreads to form adherent, malignant “pseudo membrane”: removal of the membrane reveals a bleeding, edematous mucosa. It can lead to respiratory obstruction and death by asphyxiation. Fever is not high, but the patient appears toxic.
- 🎙️ Laryngeal diphtheria: Either an extension of pharyngeal form (often) or the only site involved (rarely). Symptoms include mild fever (with little absorption of toxin), dyspnea, hoarseness, and a barking cough. The pseudomembrane can lead to airway obstruction, coma, and death.
- 💪🏼 Cutaneous diphtheria: Skin infections are quite common in the tropics and are probably responsible for the high levels of natural immunity found in these populations. Skin infections may be manifested by a scaling rash or by ulcers with clearly demarcated edges and pseudomembrane. 📷
- ↑Inflammatory markers
- ↓Plts
- severe cases: Damage of heart tissue ⇒ ↑LDH, CK, proteinuria
⇒ CULTURE (naso-pharyng. swab) ⇒ Löfflers ⇒ SMEAR + GRAM stain
The treatment for diphtheria should begin once appropriate swabs have been taken, before waiting for microbiological confirmation. Strict isolation should be used as pseudo membranes are highly contagious.
Antitoxin and antibiotics should be used for the neutralization of free toxin, elimination of further toxin production, and to control local infection.
Diphtheria antitoxin is produced in immunized horses. It will not neutralize toxin that is already fixed to tissues but will neutralize circulating toxin. Early use will prevent the progression of the disease. The earlier, the better.
For moderate disease ⇒ 16.000-40.000-100.000 U i.m. mild cases ⇒ 4.000-8.000 U.
Antibiotics like penicillin/amoxicillin or macrolides (erythromycin) should be used for two weeks to eradicate the bacteria and prevent further toxin production.
- Gram negativ Bacilli:
- Fusiform bacilli,
- Bacteroides ssp
- Spirochets (Treponema, Borrelia)
bacterial overcrowding due to:
- poor oral hygiene
- malnutrition
- AB → ✏️ Penicillin + 🚃 Metronidazole
- oral hygiene
- topical disinfectants

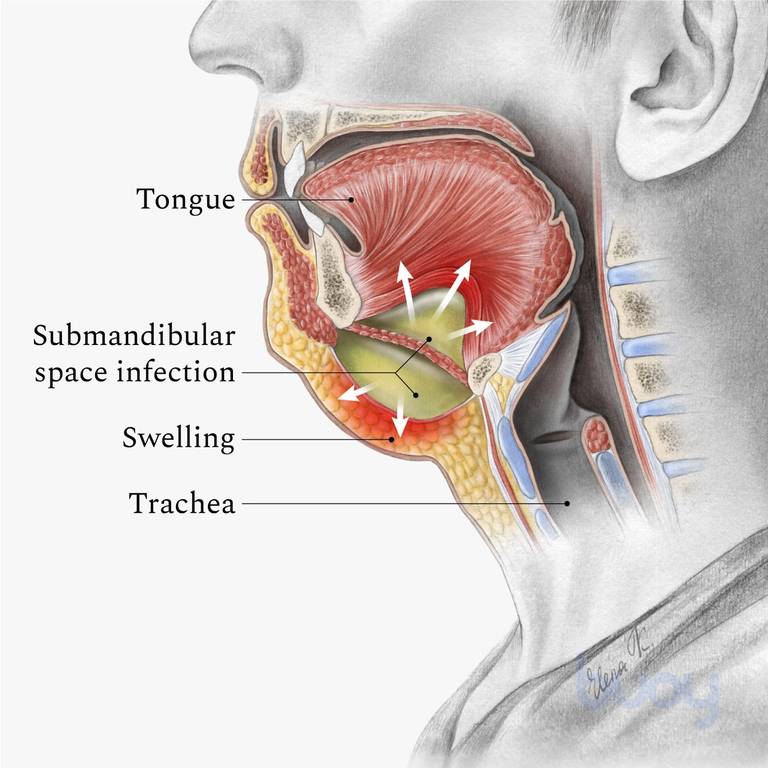
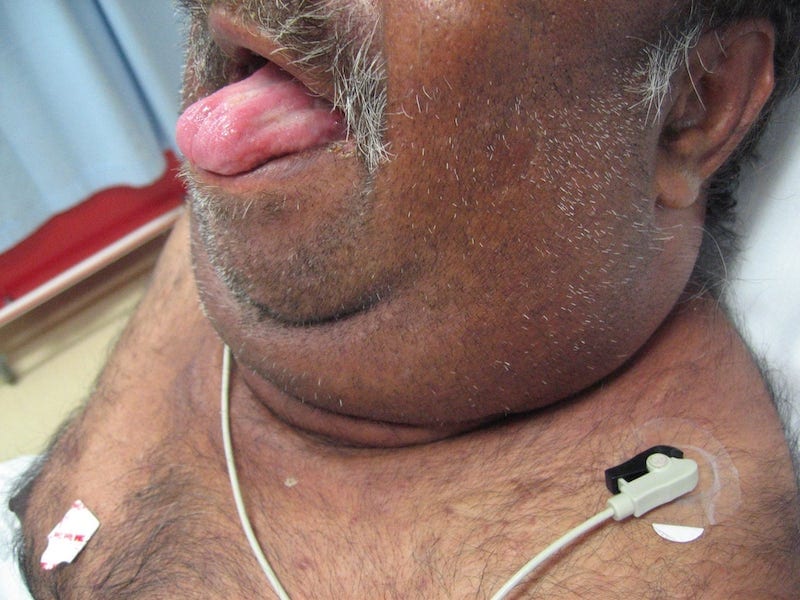
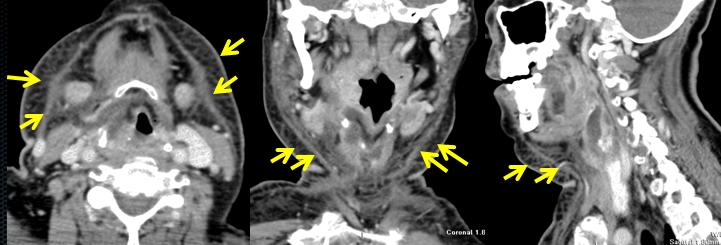
- Bilateral “wood-like” swelling
- double chin appearance
- Tongue protrusion (airway obstruction)
- Fever
- ØLN + ØAbscess
1) CT 📷
2)🩸 Blood + 💉 Needle aspiration ⇒ 🧫 CULTURE
🔪 SURGERY + 💊 AB

- Arcanobacter haemolyticum
- Pathogen: Arcanobacter haemolyticum
- Similar to GAS pharyngitis
- Occurs in adolescents and young adults
- Clinical features:
- Pharyngeal erythema and exudate
- Fever
- Cervical lymphadenopathy
- Distinguishing feature: Rash (>50%)
- Scarlet fever-ish
- Macular/maculopapular
- Involves distal extremities, typically extensor surfaces
- Spares palms and soles
- Rarely causes severe infections (e.g., pneumonia and pyomyositis)
- Can be a confecting agent

- 🎿 WALKING PNEUMONIA: M. pneumoniae + C. pneumoniae
- young adults <30y
- xray worse than clinical symptoms (=”walking pneumonia”)
clinical differentiator: history of recurrent pharyngitis
→ Patchy infiltrates on xray
⇒ Tx Macrolides
→ also causes walking pneumonia
🦠 2) VIRAL


Clinical presentation:
- signs of Infection: classic Pharyngitis
- Clinical exam: Hyperremia + Congestion
- Symptoms + Signs: dysphagia, odynophagia (sore throat)
- 🦠Specific viral signs
- 🌬️ cough (dry)
- ↕️ Assoc. rhinitis + laryngitis
- 👃🏼Rhinitis + sinusitis: rhinorrhea + nasal obstruction + sneezing sinus pressure
- 🎙️ laryngitis: dysphonia
- 💩 Diarrhea (nausea, vomiting)
- if adenovirus → conjunctivits
- +/- fever (if present LOW-grade)
Special viral + pedi: (esp if <6y)
- Irritability
- Feeding difficulties ! (nasal obstruct. / odynophagia)
- +/- ↑LN
⇒ usually Ø other systemic manifestations (digestive, LN, exanthem)
Criteria | Infants | Older Children (≥6 years) |
Onset | Often presents with fever | Symptoms include dry nasal passages and scratchy throat |
Clinical Manifestations | Varied symptom presentation | Less variability in symptoms |
Nasal Inflammation Symptoms | Nasal discharge common | Nasal obstruction is more prominent |
Fever | More frequent occurrence | Less frequently observed |
Behavioral Changes | Irritability and restlessness are more common | Less commonly irritable or restless |
Feeding and Sleeping Patterns | More likely to have difficulties | Fewer difficulties with feeding and sleep |
Lymph Node Enlargement | More commonly observed | Less commonly observed |
Etiology: (RACI) - rhinovirus (30–80%), - coronaviruses (≈ 15%) - influenza viruses (10–15%) - adenoviruses (5%) - others
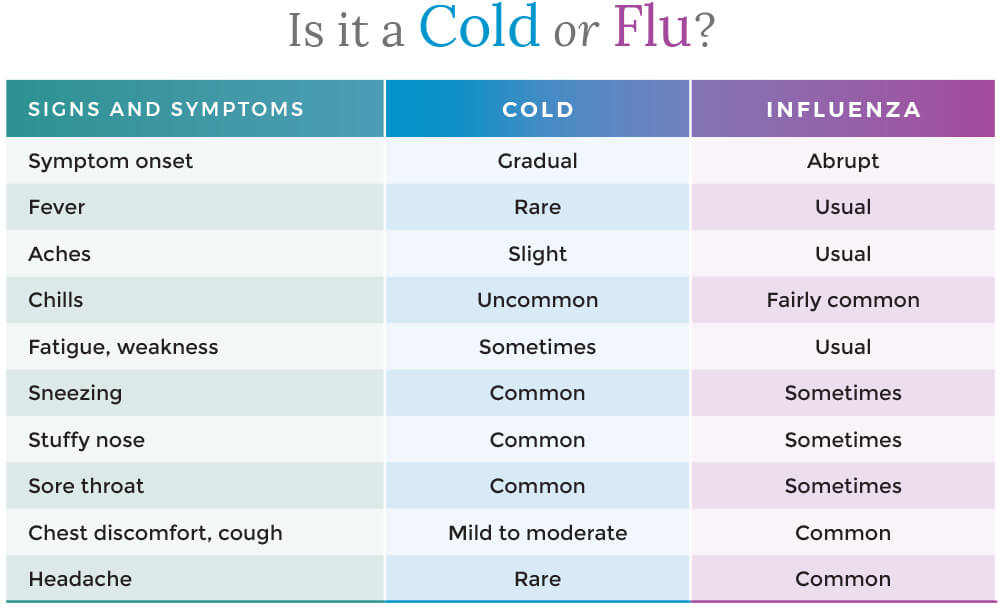
CLINICAL DIAGNOSIS:
- Rhinitis signs
- Pharyngitis signs
- Minimal/Ø systemic signs (fever, headache, myalgia)
- Exclusion of DDx
- Non-infectious rhinitis → allergic, vasomotor, etc.
- Influenza
- bacterial pharyngitis
- Measles + Pertussis
- Any other respiratory infection w/ common cold = prodrome
Self-limited after 1w (adults) / 10-14d (infants)

- Influenza viruses are classified into four types: A, B, C, and D.
- Types A and B are responsible for seasonal epidemics of influenza, while type C causes mild respiratory illness and type D primarily affects animals.
⇒ A causes ENDEMIC + PANDEMICS (Ag drift + shift) ⇒ B only ENDEMICS (Ag drift only)

Antigenic DRIFT = point mutation Antigenic SHIFT = segments shared → new formation
- 🫁 Respiratory: croup, bronchiolitis, primary influenza pneumonia – early (12-24 h), severe, hemorrhagic alveolitis with ARDS !
- mild interstitial prominence
- to poorly defined, 1- to 2-cm patchy areas of consolidation
- to extensive airspace disease due to hemorrhagic pulmonary edema
- cavity formation suggests bacterial superinfection with Staphylococcus
- pleural effusion is rare and usually represents bacterial infection
- characteristic appearance of ARDS: multifocal bilateral air-space opacities, in a predominantly perihilar and lower zone distribution = ground-glass opacity
- differential diagnosis includes: infection (common complication of ARDS), cardiogenic pulmonary edema, differentiation can be impossible in some cases
- causes of ARDS include: trauma, septicemia, hypovolemic shock, fat embolism, near-drowning, burns, viral pneumonia (influenza, SARS-CoV2, VZV), pancreatitis, oxygen toxicity, disseminated intravascular coagulopathy
- ARDS mortality is high, around 50%
- many survivors develop chronic lung disease, with damaged lung healing by fibrosis
- 🧠 Neurological: neuritis, 🐻 Guillain-Barre sd, transverse myelitis, encephalitis, cranial nerves palsies
- ❤️ Cardiac: myocarditis, pericarditis
- 💪🏼 Myositis, rhabdomyolysis (> in children, > with type B)

⇒ Influenza-virus pneumonia (primary)


- Infection of respiratory tract
- Sinusitis + Otitis
- Bronchitis
- Pneumonia (S.AUREUS!) / bronchopneumonia
- toxic shock syndrome (TSS) frequently reported during last epidemics due to some modifications of colonization and replication of toxins producers staphylococci induced by A and B viruses
- pregnancy severe evolution, double lethality teratogenic potential
- Exacerbation of underlying chronic diseases - COPD, asthma, cystic fibrosis (=risk groups → vaccination!)
- Influenza A, B viruses/ VZV + salicylates
- Acute encephalopathy + fatty degenerative liver failure
- Affects frequently children as well as other ages
- Other viral / atypical bacterial
- Covid-19
- Common cold
- Respiratory infections with adenoviruses, RSV, enterov, parainfluenza viruses
- Atypical pneumonia (Mycoplasma, chlamydia, legionella)
- Other disease’s onset with respiratory catarrh: measles, varicella
- Systemic infections
- Systemic disease’s onset: leptospirosis, brucella, typhoid fever
- Flu-like infectious diseases: TB, HAV, sepsis
- Influenza can be diagnosed through laboratory tests, including
- rapid antigen tests,
- PCR (viral Ag detection)
- Ø SEROLOGY!
-
viral culture. - Clinical evaluation and epidemiological factors (SEASONAL) are also taken into consideration for diagnosis.
- ✳️ Identification of groups of risk for severe forms, complications
- 🛏️Supportative
- Isolation
- Bed rest
- Diet
- Medication differentiated according to clinical forms – common/complicated/severe
- 💊Antivirals
- Protein
M2inhibitors:Amantadine, Rimantadine⇒ #not anymore! - NA inhibitors: Oseltamivir (Tamiflu), Zanamivir, Peramivir – iv, Favipiravir
- Endonucleases inhibitors: Baloxavir
- FAVIPIRAVIR (Avigan)
- Laninamivir (Inavir)
- Peramivir (Rapiacta, Peramiflu)
- Endonucleases inhibitors: Baloxavir
- severe forms: 🌝steroids


- High-risk groups: Children under 2 years old, adults 65 years and older, pregnant women (up to 2 weeks postpartum), residents of nursing homes and long-term care facilities.
- Medical conditions: Asthma, neurological and neurodevelopmental conditions, chronic obstructive pulmonary disease (COPD) and cystic fibrosis, heart disease (including congenital heart disease, congestive heart failure, and coronary artery disease), blood disorders (such as sickle cell disease), endocrine disorders (such as diabetes), weakened immune system (due to diseases, medications, or HIV/AIDS), kidney disorders, liver disorders, metabolic disorders, extreme obesity (BMI of 40 or more).
Complications of the flu include:
- Pneumonia
- Bronchitis
- Sinus infections
- Ear infections
- Worsening of chronic medical conditions, such as heart disease, asthma, or diabetes
- In rare cases, the flu can lead to respiratory failure, sepsis + multiorgan failre
Basic measures: 📷
ANNUALLY SEASONAL INFLUENZA 💉VACCINATION
→ IM (inactivated) quadrivalent → Intra-nasal (live attenuated) [! in pregnancy]
every person ≥6 month should get vaccination
incubation period: 5 days
contagious: 2 days before symptoms
- 🧣 URT VIRAL signs (”influenza like”)
- cough + sore throat
- congested nose (+- taste dysfunction)
- fever, muscle aches, fatigue, headache
- assoc. GI symtoms
- 🫁VIRAL PNEUMONIA signs (see below)
- dyspnea +- wheezing + cough
- assoc. URT (⇒ see “1.” ↑)
→ more common: young → a + b; elderly → c + d
- 🥍 RAPID-Ag or PCR
- Lab:
- Inflammatory markers?
- Lymphocytes?
- Thrombocytes?
- LDH?
- Liver, renal?
- Imaging ⇒ CT (or Xray) ⇒ GROUND GLASS OPACITIES: BILATERAL + PERIPHERAL 📷
Stage | Characteristics |
Asymptomatic or presymptomatic infection | Positive virologic test for SARS-CoV-2 (ie, NAAT or antigen test) but no symptoms consistent with COVID-19 |
Mild illness | ØLUNG, only URT + systemic:
Varied symptoms (eg, fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste or smell) but no shortness of breath, dyspnea, or abnormal chest imaging |
Moderate illnes | LUNG, but Ø severe
SpO2 ≥ 94% and lower respiratory disease evidenced by clinical assessment or imaging |
Severe illness | LUNG severe
Severe hypoxemia (SpO2 < 94%, PaO2/FiO2 < 300 mm Hg, respiratory rate > 30 breaths/min, or lung infiltrates > 50%) |
Critical illness or organ failure | ORGAN FAILURE / SEPTIC SHOCK
Respiratory failure, septic shock, and/or multiorgan dysfunction |
In a multivariate analysis comparing 16 critical COVID-19 cases with 310 asymptomatic, mild, or severe cases, the following predictors of increased disease severity were identified:
- Older age (P = 0.002)
- Lymphocyte declines correlated with high levels of IL-6 and IL-8 in patients exhibiting severe/critical disease.
- ↗️ symptomatic
- 🌝 corticosteroids systemic + other immunomodulator (IVIG, JAK-inhib)
- 🦠 anti-viral ⇒ 🐏 remdesivir + 💧convalescent plasma
Remdesivir:
A nucleotide analog → inhibits RNA synthesis. Has been shown to have in vitro activity against SARS-CoV-2. Its clinical efficacy is not well understood.

Convalescent plasma:

(Prevention = Vaccination)
- persistent cough
- fatigue














- ⛄3) Irritative pharyngitis
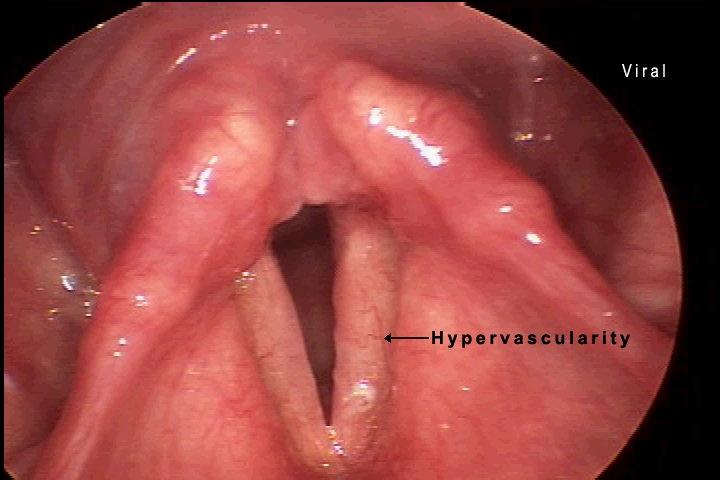
Acute (simple) laryngitis
Laryngoscopy: 📷
Etiology: COMMON COLD (VIRAL)
Patient: older children!
- viral infection signs

- LARYNGEAL signs
- hoarseness
- BARKING COUGH (seal-like)
- ØAIRWAY obstruction
- assoc. / prodrome nasopharyngitis
(Østridor, Ødyspnea, Ørespir. distress)
= self limited (1w)
⇒ Symptomatic Tx (hydration, inhalation, avoid irritants, vocal rest)

*Signs of respiratory distress → 📷
*Tripod → 📷
SUBGLOTTIC:
VIRAL → mainly: Parainfluenza virus 📸 (less common RSV 🪦 or others)
Inflammation + edema ⇒ 📷 narrowed subglottic area (obstruction)
⇒ more severe in smaller children (small larynx→ edema more impact of luman narrowing)
Clinical Indicator | Mild Severity | Moderate Severity | Severe Severity |
Stridor | Observable when agitated | Notable at rest | Present at rest (occasionally biphasic) |
Tachypnea | Absent | Mild presence | Moderate to severe |
Retractions | Absent | Mild to moderate | Severe |
Mental Status | Restlessness upon disturbance | Restless without disturbance | Lethargy |
- Viral → pneumonia, bronchiolitis
- bacterial → pneumonia, bronchiolitis, tracheitis, otitis media
- dehydration
- <0,5y
- moderate / severe
- poor oral intake / dehydration
- Toxic + high fever ⇒ DDx bacterial (membranous + epiglottitis)
- steroid refractory
- Øpossible at home
- other obstructive laryngitis
- other causes for airways obstruction
- abscess (peritonsillar, retropharyngeal)
- foreign body
- angioedema
- external compression
- other causes for laryngeal irritation
- GERD
- congenital anomalies
Non-inflammatory subglottic edema
contraction of larynx muscles
⇒ triggers/RF = laryngeal irritants: allergic, viral, adenoids, GERD, FH
- Membranous bacterial croup (Chevalier Jackson laryngo-tracheo-bronchitis)
- Diptheria
(Staph aureus)
SUPRAGLOTTIC:
- Acute epiglottis
→ 🅱️ Hemophilus influenza B
Pathology | Clinical Course | Stridor (Intensity) |
Viral Croup | Self-limited disease; worse at night | Yes (mild to severe) |
Spasmodic Croup | Short duration; recurrences | Yes (moderate to severe) |
Membranous Croup | More rapid deterioration compared to viral croup | Yes (moderate to severe) |
Epiglottitis | Rapidly progressive; respiratory arrest can occur within hours | Yes (often not severe) |
‼️ be careful with them → stress → trigger airway obstruction
contraction of laryngeal muscles or aspiration of saliva → apnea → resp. arrest
⇒ only performed when airways secured
⇒ in epiglottitis: only performed on ICU!!
NOT COMPULSARY!
LAB:
- Deyhydration?
- Oxygenation? (SpO2)
- Inflammatory lab?
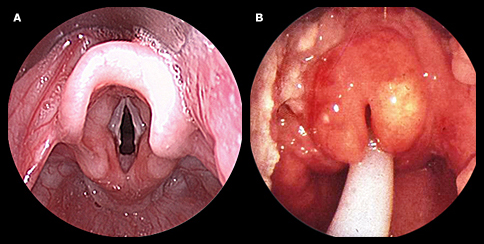
PARACLINICAL: (usually Ø recomm. in viral)
⇒ Xray
⇒ laryngoscopy 📷(+oropharyngoscopy)
left picture = viral croup
right picture = epiglottitis

- Steroids
- epinephrine
- humidified air
- intubation + ventilation
- hydration + O2
Mild Croup:
- Manage anxiety in infants.
- Utilize cool mist inhalation.
- Position infant in upright posture for sleep.
- Encourage cool air inhalation during colder months.
- Administer Dexamethasone:
- Effective in reducing airway inflammation within 6 hours.
- Available as oral syrup, IV, or IM.
Moderate to Severe Croup:
- Hospitalization is necessary for severe cases.
- Use inhaled racemic epinephrine:
- Efficient in reducing airway inflammation; faster than Dexamethasone.
- Apply Dexamethasone.
- Offer humidified air or oxygen when needed.
- Administer IV fluids to counteract dehydration.
- Intubation is vital when there's a risk to the airway (occurs in less than 3% of severe croup cases).
Note: Intubation can be challenging in severe croup due to narrowing of the subglottic region. An anesthesiologist's assistance is crucial.
- Rapidly improves without Tx (<1h)
- Symptomatic
- Cold night air
- Humidified air


- Single therapy often suggested with a third-generation cephalosporin (examples include cefotaxime, ceftriaxone) or a beta-lactam combined with a beta-lactamase inhibitor (such as ampicillin/sulbactam, amoxicillin/clavulanate, piperacillin/tazobactam).
- If there's a penicillin allergy in patients, opt for a fluoroquinolone like levofloxacin.
- To counteract MRSA, consider adding an antibiotic with anti-MRSA properties, e.g., vancomycin or clindamycin.
- Intubation in Severe Croup:
- Intubation is indicated when airway compromise is imminent.
- This procedure is required in less than 3% of infants with severe croup.
- A noteworthy point is the difficulty of intubation in severe croup due to subglottic narrowing. It emphasizes the importance of having an anesthesiologist present during the process, indicating the complexities and potential challenges of this procedure.
child presenting with stridor + respiratory distress
↓
- laryngeal signs? → croup → recurrent/Øprodrome → pseudocroup →common cold prodrome → croup → viral croup prodrome + high fever → membranous (also respect age; <3y ⇒ 0,5-3y - viral croup+pseudo; 0.5-7 - epiglottitis)
- muffled voice + drooling/dysphagia + Ø cough + high fever? → epiglottitis
↓
[SKIP Lab + Paraclinical exams to Ø aggrevate respiratory distress!!]
↓
Tx:
- pseudocroup → usually ØTx needed(symptomatic → humidified air, cold air at night
- Rest → steroids, epinephrine, humidified air, intubation + ventilation, hydration + O2
- epiglottitis + membranous croup → AB (Amoxi/Cephalorsporine)

Stage | Symptoms |
Catarrhal stage
(1-2 weeks) | Nonspecific symptoms similar to an upper respiratory infection (mild cough, watery nasal discharge, low-grade fever), possibly conjunctivitis |
Paroxysmal stage
(2-6 weeks) | Intense paroxysmal coughing (often occurring at night), followed by a deep and loud inhalation or high-pitched whooping sound, accompanied by tongue protrusion, gagging, and struggling for breath, possibly accompanied by cyanosis increases in frequency and severity throughout the stage, followed by the expulsion of phlegm or posttussive vomiting (risk of dehydration), potential bleeding of the conjunctiva, petechiae, and venous congestion, infants (<6 months) may only develop apnea and not the characteristic cough |
Convalescent stage
(weeks to months) | Progressive reduction of symptoms, coughing attacks may persist over several weeks before resolving |

Prevention: 💉 DTP vaccine




“Coughing man”



- Atypical pneumonia → patchy infiltrate
- Hyponatremia
- Neurological symptoms
- Diarrhea
- High fever
Confirmation: Rapid urine antigen test
Macrolides or Fluros

- D-K:
- Cervicitis/Urethritis (Dysuria, discharge)
- Neonatal: Conjunctivitis + Pneumonia
- L1, L2, L3
- Lymphgranuloma venerum:
- A-C
- Trachoma ⇒ Blindness! (in low resource contries)
→ Complication: PID, Fitz-Hugh curtis perihepatitis
early: painless ulcers late: tender “buboes” (swollen inguinal+femoral LN)


🦅 Macrolides


self-limited
- Advanced age (>65)
- Hospitalization for pneumonia required within 1 year
- Serious underlying conditions:
- Chronic lung, heart, liver, or renal disease
- Diabetes mellitus
- Malnutrition
- Recurrent aspiration
- Alcoholism
- Renal insufficiency
- Immunodeficiency (including complications of splenectomy)
- Hypoxemia or hypercapnia
- Anemia
- Cystic fibrosis
- Physical findings:
- Tachypnea (>30/min)
- Hypotension
- Fever (>38.3°C)
- Altered level of consciousness
- Laboratory findings:
- Leucocytosis (>30,000 cells/mm3)
- Leukopenia (<4,000 cells/mm3)
- Neutropenia (<1,000 cells/mm3)
- Radiographic findings:
- 2 or more lobes involved
- Significant pleural effusions
- Cavitation
- Rapid spread
- Other complications:
- Mechanical ventilation
- ARDS (Acute Respiratory Distress Syndrome)

F → valuable!
⇒ Dg: PLEURAL effusion +pneumonia( consolidation, interstital pneumonia)
⇒ DDx: pneumothorax, atelectasis, cysts, tumors

CLINIC:

PARA-CLINIC:


- Walking pneumonia ⇒ Mycoplasma + Legionella
- Leptospirosis
- HSV

🏥 when:
- <6️⃣Ⓜ️ Age ≤ 6 months.
- 🚨 Severe OR complicated pneumonia.
- 🕰Associated chronic diseases
- ❌Failure to respond to initial ambulatory antibiotic treatment.
Tx:
⇒ 💊 supportive treatment + AB

🐑 sheep or other animals

- Edema factor (EF) Toxin:
- Increases intracellular cAMP levels
- Causes extracellular fluid accumulation (edema)
- Inhibits host defenses and phagocytosis
- Lethal factor (LF) exotoxin:
- Acts as a protease
- Cleaves MAP Kinase, a signal transduction protein responsible for cell growth
- Results in necrosis and black eschar formation



Feature | Malignant Pustula | Malignant Edema | Bullous Anthrax |
Lesion appearance | erythematous macule -> pruritic papule -> vesicle with serosanguineous/hemorrhagic contents -> necrotic eschar surrounded by new vesicles -> Chaussier crown "lenticular" crust | enormous gelatinous, painless edema covered with frills and troubles, deforms region | blisters/bullae with serohemorrhagic content, ulceration and necrosis on edematous background and infiltrated |
Initial lesion | painless erythematous macule | discrete/absent (↓/Øeschar) | - |
Regional adenopathy | painful | - | - |
General manifestations | reduced/absent: fever, headache, myo-arthralgia | fever, chills, tachycardia, tachypnea, toxic state | - |
Death | untreated -> death in 4-5 days by septicemia and infectious shock
or by asphyxia or glottic edema | - |

- inflammatory markers
- 🔬 ⇒ Gram + Bacillus (”box car” shaped)
- 🧫 culture + PCR
- 🛡️ Serology (ELISA) ⇒Anti-LF + Anti-EF

⇒ 🌊 Malignant edema
⇒ 🧠 Meningitis
🫀Heart
- Infection of the heart's endocardial surface, which includes the valvular, septal, and mural(wall) surfaces.
- Characterized by septic vegetation: lesion composed of platelets, fibrin, microorganisms, and inflammatory cells.

IE pathophysiology involves three stages:
- transient bacteremia
- bacterial multiplication
- septic vegetation formation, and local destruction and systemic embolization.
⇒ Many microorganisms associated with IE produce biofilms, which allow bacterial populations to embed within an extracellular polysaccharide slime-like matrix, protect bacteria from host immune defenses, impede antimicrobial efficacy, and hide resistant persister organisms. Biofilm-forming capacity is now recognized as an important determinant of virulence in the development of staphylococcal device-related infections.
- The incidence of IE is difficult to ascertain and varies according to location (6-10/100,000).
- Despite trends toward earlier diagnosis and surgical intervention, 1-year mortality (10-30%) has not improved in over two decades.
- IE is more common in males than in females,
- and may occur in persons of any age and increasingly common in elderly.
- More than one-half of cases now occur in patients without known heart disease.
There are four different classifications of IE:
- ⛵ Native Valve IE,
- 🦾 Prosthetic Valve IE,
- 💉 Intravenous drug abuse (IVDA) IE,
- 🏥 and Nosocomial IE.
- Native Valve IE can be classified based on the localization and presence/absence of a device.
- The different types include left/right heart IE, mitral valve IE, aortic valve IE, tricuspid valve IE, and pulmonary valve IE.
- Prosthetic Valve IE can be classified based on the timing of onset.
- The different types include early (<12 months) and late (>12 months) onset.
- Device-associated IE can be classified based on the type of device. The different types include pacemaker IE.
Other types of device-associated Infective Endocarditis (IE) include prosthetic valve IE, central venous catheter-associated IE, hemodialysis-related IE, and implantable cardioverter-defibrillator IE.
- Community Acquired IE refers to onset of symptoms and signs before 48 hours of admittance,
- while Health-care Associated IE refers to onset of symptoms and signs after 48 hours of admittance.
- Rheumatic heart disease
- Prosthetic heart valves
- Degenerative cardiac lesions
- Congenital heart defects
- Intravenous catheterization/ shunt procedures
- IV drug use
The different extra-cardiac risk factors of bacteremia include dental procedures, respiratory procedures, gastrointestinal procedures, genitourinary procedures, and invasive procedures.

- IE has a "1000 faces disease" and can present with non-specific symptoms such as fever, general altered state, and weight loss.
- Complications may represent the first manifestation.
The complications of IE include
- ❤️ heart complications
- heart failure,
- periannular complications.
- ♻️ septic emboli
- kidney failure
- stroke
- septic shock




- 🍢 Staph. Aureus
- 🦾Staph. Epidermidis & Saprophyticus
- 🃏Strep. Viridans

- 🦀 Strep. Gallolyticus
- 🏛️ Enterococcus
- ✋🏼 HACEK organism

- 🐆 Bartonella henselae
- 🐏 Coxiella burnetii (Q-fever)
- 🍄 Fungal (Aspergillus, Candida)
possible culture negative bacteria:
– HACEK organisms – Nutritionally deficient Streptococcus sp Atypical + Zoonotics: – Coxiella burnetii – Chlamydia psittaci – Mycoplasma sp – Legionella pneumophila – Brucella sp – Bartonella sp – Tropheryma whipplei
- Gram neg. bacterial
- culture-negative IE
- fungal IE
The different types of Gram-negative bacteria associated with IE include the HACEK group and typical Gram-negative bacilli such as E. coli and Klebsiella.
The different types of culture-negative IE include HACEK organisms, nutritionally deficient Streptococcus sp, Coxiella burnetii, Chlamydia psittaci, Mycoplasma sp, Legionella pneumophila, Brucella sp, Bartonella sp, and Tropheryma whipplei.

⇒ 🤯 DUKE = 🐻⏲️ BE(R* ) TIMER 📷
*major = also new valvular regurgitation

NATIVE ⇒ Vanco + Genta PROSTHETIC early ⇒ Vanco + Genta + CEFEPIME + RIFAMPIN late ⇒ Vanco + Ceftriaxone


*Tx of native → Gentamycin + Vanco/B-lactam is an option too!
Surgery is recommended for patients with IE who have
- cardiogenic shock + severe heart failure
- severe
- valve regurgitation,
- prosthesis dysfunction,
- extensions
- peri-, intra-cardiac fistula,
- valvular and annular abscess,
- non-controlled infection + abscess,
- peri-valvular dysfunction,
- vegetation >10 mm
- embolic event
🍤 Gastrointestinal tract
- Pre-formed toxin (Ø bacteria present)
- Bacteria present (toxin produced in intestine)
- others → see “Bacterial gastroenteritis” for more details)
- Staphylococcus species, Listeria and Campylobacter are commonly found in cheese.
- Salmonella species are often found in eggs and mayonnaise.
- Ground beef can be contaminated with EHEC.
- Campylobacter species and Salmonella are commonly found in poultry.
- Pork can be contaminated with Clostridium perfringens and Yersinia enterocolitica.
- Seafood, Oysters can carry Vibrio species
- Vegetables can be contaminated with Clostridium perfringens.
- Bacillus species are sometimes found in fried rice.
from meats, mayonaise, salad, cream filled pastries
from reheated fried rice



Certain bacteria are associated with specific types of food, leading to food poisoning.
Please note that this information is for study purposes and should not be used as medical advice.
1) 🚿 Rehydration (iv or oral - depending on severity)
Grade | Mild | Moderate | Severe |
Volume Deficit (Infants) | 5% (50 mL/kg) | 10% (100 mL/kg) | 15% (150 mL/kg) |
Volume Deficit (Older Children) | 3% (30 mL/kg) | 6% (60 mL/kg) | 9% (90 mL/kg) |
Clinical Signs: Tears | Present | Reduced/absent | Absent |
Clinical Signs: Eyes | Normal | Sunken | Very sunken |
Clinical Signs: Skin Touch | Normal | Dry | Clammy |
Clinical Signs: Skin Elasticity | Pinch retracts immediately | Pinch retracts slowly (tenting) | Pinch retracts very slowly |
Clinical Signs: Buccal Mucosa/Lips | Moist/dry | Dry | Very dry/cracked |
Clinical Signs: Anterior Fontanelle | Flat | Soft | Sunken |
Clinical Signs: Respiratory Rate | Normal | Normal/increased | Increased |
Clinical Signs: Respiratory Amplitude | Normal | Deep | Deep |
Clinical Signs: Heart Rate | Normal | Slightly increased | Increased |
Clinical Signs: Pulse Amplitude | Normal | Weak | Feeble/impalpable |
Clinical Signs: Capillary Refill Time | <2 seconds | 2-3 seconds | >3 seconds |
Clinical Signs: Blood Pressure | Normal | Normal/low | Low |
Clinical Signs: Diuresis | Normal/mild decrease | Oliguria | Severe oliguria |
Clinical Signs: Mental Status | Alert, restless | Drowsy | Drowsy, lethargic, obtunded |
if in doubt classify in the more severe grade
2) BRAT diet 📷
GI- infection:






- local
- rectal prolapse
- intussusception
- toxic megacolon
- systemic:
- sepsis
- seizures
- glomerulonephritis + reactive arthritis
- HUS



- 🔬microscopy + Gram stain
- 🧫 Culture (stool + blood)
- 🔰 +-serological (elisa, agglutination test) + PCR
- US for DDx (appendicitis)
bipolar staining (safety-pin appearance) 📷
- 🤺 Aminoglycosides,

- 🌷Fluros,
- 🦑 Cephalos 3rd,
- 🧻🥚TMP-SMX
- 🥸 Curved-shaped
- 🚿 REHYDRATION
- AB (🚴🏼♂️Doxy/🌷Fluro/🦅Macrolide)
- Prevention in endemic areas: Vaccine (Dukoral, shanchol)





fecal oral (poor sanitation → gets into food)
Tx:
Special forms:
C. difficile infection causes toxic megacolon through the action of its toxins, particularly toxins A and B. These toxins cause damage and inflammation to the colon lining, leading to ulcerations and erosions. As the inflammation worsens, it can result in the colon becoming dilated and distended, leading to the development of toxic megacolon. The toxins also impair the function of the smooth muscle of the colon, which can contribute to the development of megacolon. Overall, the exact mechanism by which C. difficile causes toxic megacolon is not fully understood, but it is believed to be related to the toxins' impact on the colon's inflammatory response and smooth muscle function.
- Recurrent = easier but chronic evolution
- ↑ sensitivity tests: GDH (with EIA) or PCR (toxin)
- ↑specifictiy: Toxin (with EIA)
- Toxin detection / determination
- detection → EIA
- determination → PCR
- C.diff detection
- glutamate dehydrogenase = GDH test → EIA
cultureonly in research

#2 ORALLY 👄 ⇒ 🚇 Metronidazol (only in non-severe forms) if FULMINANT: ⇒ 🚌 Vanco oral 👄 PLUS 🚇 Metronidazol I.V. 🌀 if RECURRENT: ⇒ 🔄 switch ABs or ⏰ give Vanco longer (additive rifaximine and fecal transplant can also be considered)
*newer guidelines propose 🦊 Fidoxamicin as #1 Tx
Fidoxamicin:


- 🐋 NORO-virus
- 🛥️ Rota-virus
- 👃🏼 Adeno-virus
- ✨Astro-virus
- Short incubation (1-4 days)
- Self-limited Evolution 1-10 days
- Sudden onset of 🤮 vomiting AND 💩diarrhea, abdominal pain.
- 🌊WATERY stools, ↑VOLUME ,Ø BLOOD (rarely)
- +/-fever.
- Complications:
✓ Dehydration especially in children and the elderly ✓ Intestinal intussusception.
- Rapid Ag,
- PCR (multiplex)
- ELISA (serology)

Test Method | Mechanism | What It Detects | Uses |
Rapid Antigen Detection Test | Uses specific antibodies to detect a viral protein antigen in a patient's sample | Viral protein antigens | Diagnosing infectious diseases such as influenza, strep throat, and COVID-19 |
Polymerase Chain Reaction (PCR) | Amplifies and detects specific nucleic acid sequences from a patient's sample | Viral RNA or DNA | Diagnosing infectious diseases, detecting genetic disorders, and identifying bacteria and viruses |
Enzyme Immune Assay (EIA) | Uses specific antibodies to detect the presence of a particular antigen or antibody in a patient's sample | Antigens or antibodies | Diagnosing infectious diseases, detecting autoimmune disorders, and identifying food allergies |
symptomatic
- 🦠
- Hep-A,B,C,D,E
- Generalized Lymphadenopathy (incl liver)
- 🍺 EBV + 🛒CMV
- 🧙🏼♂️HIV
- 🤒 Yellow fever
- 🦠HSV
- 🧫
- 🐳 Leptospirosis
- 🐄 Brucella
- 🐏 Coxiella (Q-fever)

- Primary
- 🛡️ autoimmune
- 🦀 malignancy
- 👁️ Wilsons
- 🫐 Budd-Chiari
- Secondary
- 💊Drug-induced
- 🎋 bile duct pathology
- 🅾️ ischemic
- 🤰🏼 pregnancy

- Inflammatory markers?
- Hepatolysis?
- ↑ Transaminases: ALT >> AST
- LDH = mod. ↑ (DDx: HF, shock)
- Cholestasis?
- Bilirubin
- GGT + ALP
- Liver function test?
- Coagulation: INR (PT), Fibrinogen
- Ammonia (BUN)
- ↓ Proteins
- Albumin
- Cholinesterase
- Fibrinogen


- Prothrombin Index (PI): Less than 50% indicates rapid liver function deterioration.
- Alanine Aminotransferase (ALT/AST): Elevated levels may suggest liver damage or inflammation.
- Total Bilirubin (Bi): Levels above 4 mg/dL can indicate liver dysfunction.
- Ammonia: Normal range is 50-100 mcg%. Elevated levels may suggest hepatic encephalopathy.
- Hypoproteinemia: Reduced protein levels in the blood, signifying potential liver disease, malnutrition, or other metabolic disorders.
- Hypofibrinogenemia: Low levels of fibrinogen, affecting blood clot formation.
- Hypoalbuminemia: Low albumin levels, often a sign of chronic liver disease.
- Low cholinesterase: Indicative of liver dysfunction.
- Resistant Hypoglycemia: Persistent low blood sugar levels despite intake, may indicate hyperinsulinism.
- Metabolic Acidosis: Abnormal acidity in the body fluids indicated by low potassium (K) and sodium (Na) levels.
- Leukocytosis with Neutrophilia: Increased white blood cells and a higher proportion of neutrophils, often signaling infection or inflammation.
1. self-limited? → symptomatic (incl. vitamins)
2. Correction:
- 🌼Hyper- Ammonia
- protein restriction
- non-resorbable AB (i.e. Rifaximin)
- 🧠cerebral edema → mannitol, furosemide
- 🩸hemorrhage → Vit K
- 🍬Hypo-Glyc
- 🥐Heptorenal syndrome (RF) 📷 → dialysis, liquid+salt restriction, AB + Electroly. correction
- 🧫superinfection → culture + AB
- ❌ Fulminant, cholestatis, allergic, extra-hepatic or immune? → 🌝 Steroids
3. Etiological Tx
⇒ Anti-virals (see below)
4. Liver transplant







- Classic signs of Hepatitis (Hepatomegaly, jaundice, dark urine, pale stools, bleeding, neuro, etc)
- “Rheuma”-Prodrome:
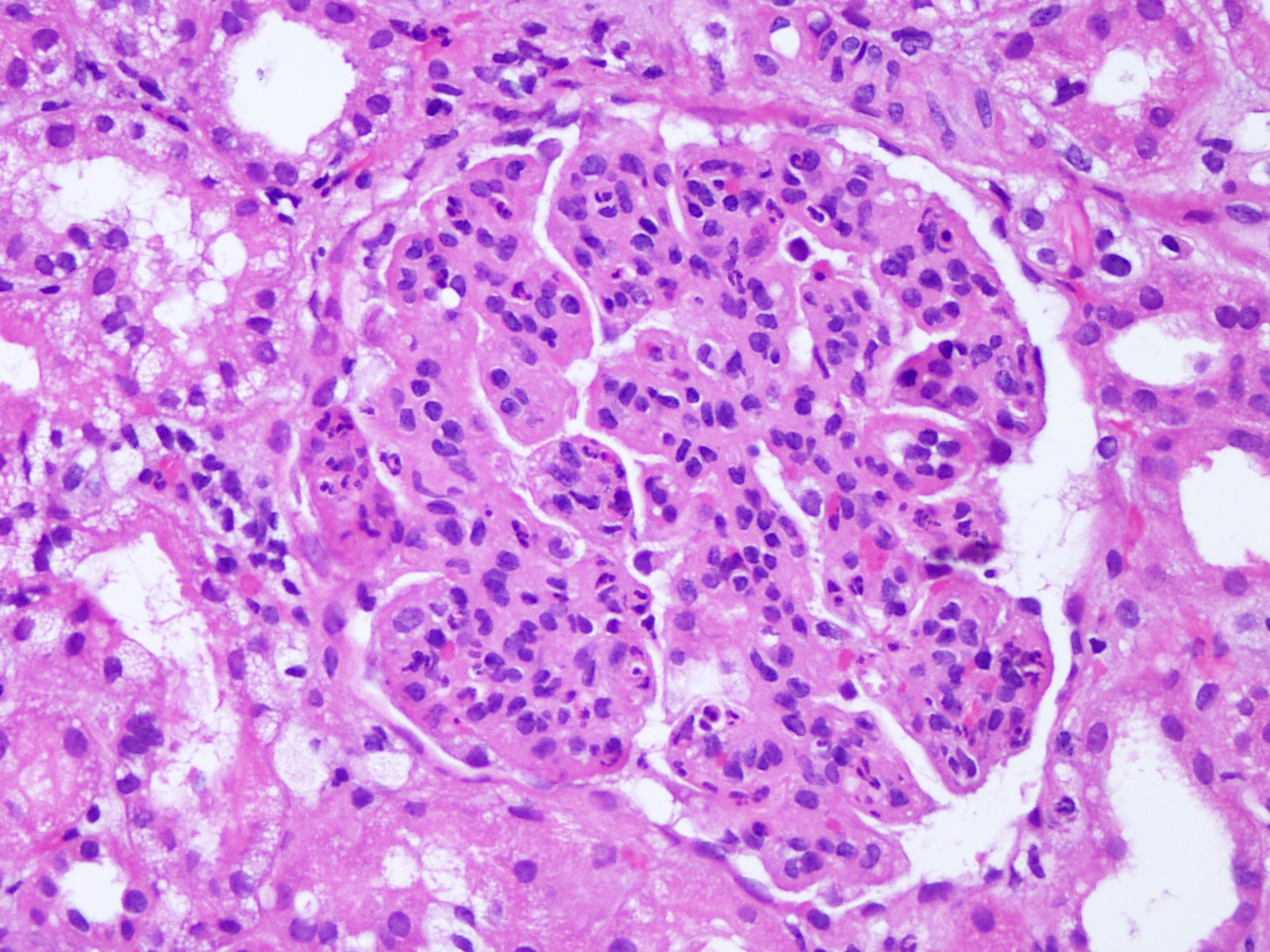
- PN (polyarteritis nodosa)📷
- GN (membranous + membrano-proliferative)
- Rash (pruritic)
- Arthralgia/Arthritis
- Fever
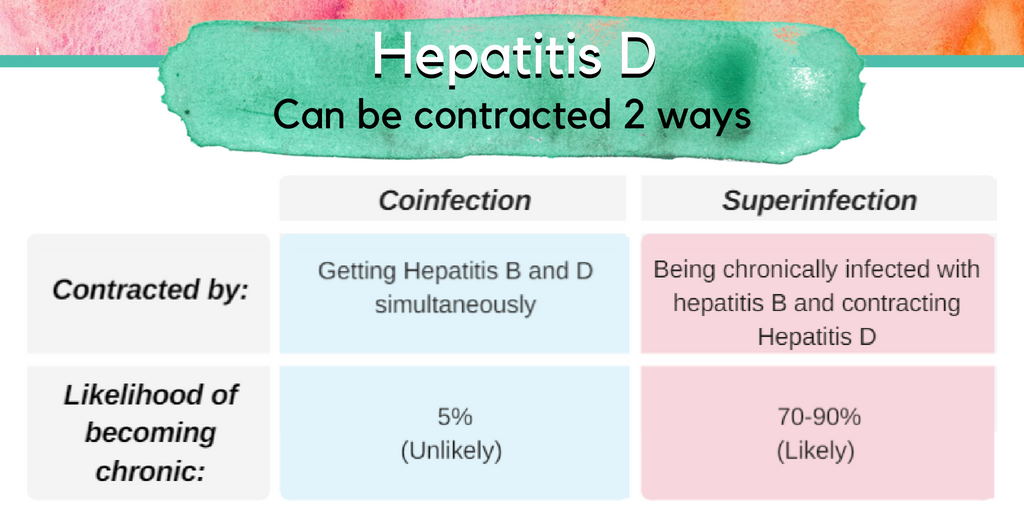
- ⇒ 🦛 HepD (co-infection or superinfection)
- 🕰️ CHRONIC HEPATITIS ⇒ 🦀 HCC
- adults ⇒ rarely (5-10%)
- 🐣 NEWBORNS ⇒ very common! (90-95%)
- The onset of acute hepatitis B is typically insidious.
- Clinical manifestations of acute infection vary depending on age.
- Jaundice is less common in children under 5 years old (less than 10%) and more common in older children and adults (30%-50%).
- Most cases of acute hepatitis B (approximately 70%) are either subclinical or anicteric.
- Severe fulminant forms of acute hepatitis B occur in a small percentage of cases (0.1-0.5%).
- The majority of adults with acute hepatitis B (90-95%) experience complete recovery, characterized by clearance of hepatitis B surface antigen (HBsAg) and production of anti-HBs, indicating future immunity against the infection.
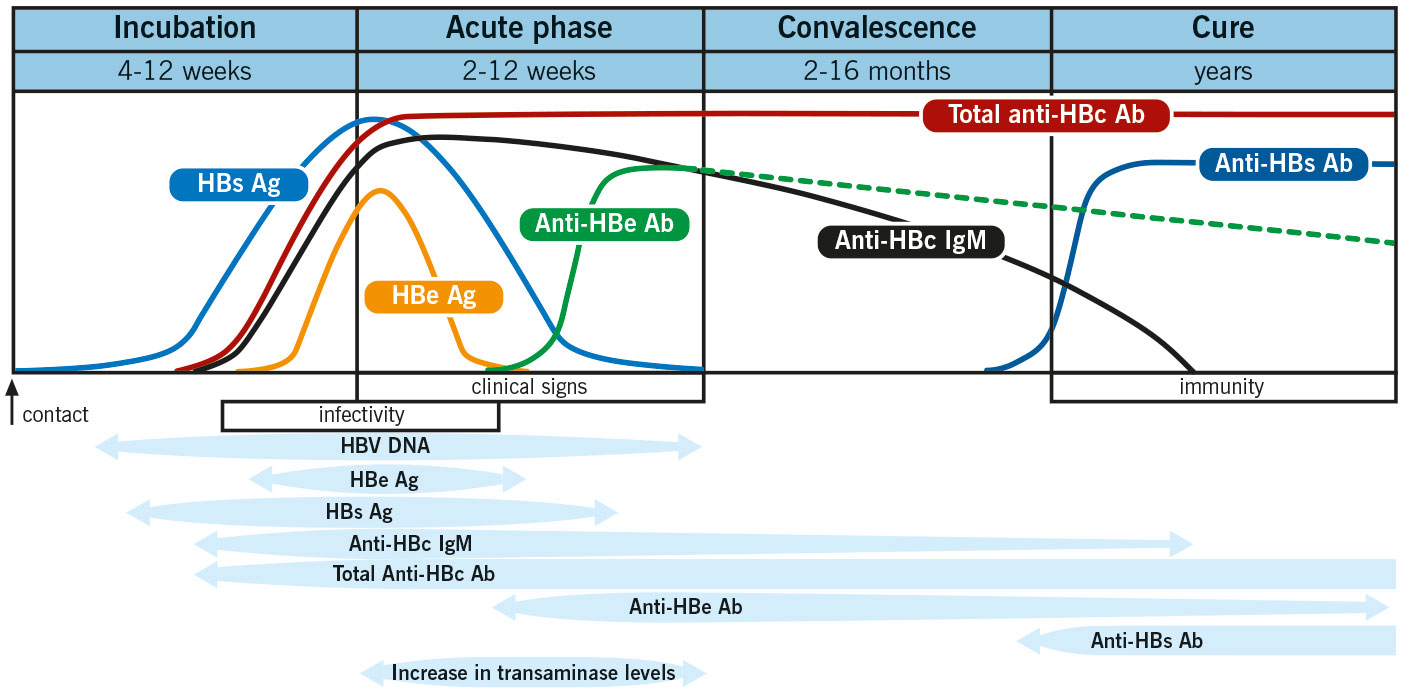
- Screening for acute infection:
- If positive: detemine transmissibility
- Acute vs. chronic (persistence)
HBsAg + anti-HBc IgM
HbeAg + HBV DNA
anti-Hbc IgM vs IgG

THERAPEUTIC ALTERNATIVES:



die Ente spielt Klavir (Entecavir) und das Lamm telefoniert(2x = bi) mit Hudini (Lamivudin + Telbivudin)

- Interferons
- Bulevirtide
- Lonafarnib
On the 🧑🏼🌾 Loner-farm (Lonafarnib) lives only the 🐂 bull D in wires that are tight (Bulevirtide) . (Bull is lonely = HepD needs another virus (HepB)

- 🙅🏼 Mainly ASYMPTOMATIC
- or 🍑 CLASSIC LIVER SIGNS
complications:
- 🕰️ CHRONIC (65-70%)⇒ cirrhosis + HCC
- ❄️ Cryoglobulinemia





⇒ Like EBV

- Monospot neg. (DDx EBV)
- non-specific
- ↑Lymphos
- ↑Liver markers
- Urine sediment → owls eye inclusion
- PCR
- Serology IgM/IgG (esp. screen in pregnancy!)
#1 Ganciclovir 🥫♻️ (iv) OR Val-Ganciclovir (oral)
→ resistent? → Foscarnet 🏎️ 🥅
→ alternative: Cidofovir
- 🍺 EBV
- 🦠 HSV
- 🧙🏼♂️HIV
- 🤒 Yellow fever
contamination of water with animal urine → water sports in tropical regions
CLINICAL FORMS:


STAGE 1
(Septicemic, Leprospiremic) | STAGE 2
(Organic, Immune, Leprospiruric) | |
🪱 Leprospires present in | 🩸BLOOD & 🧠 CNS
(Øurine) | 🥐 URINE
(present at renal tubules) |
- 🐏 Coxiella burnetii (Q-fever)
- Initially: Fever, chills, anorexia ⇒ undulating fever!
- spread through endothelial organs → enlarged spleen, liver, LN
- chronic infection → Osteomyelitis
🚴🏽♂️ Doxy + 🔫 Rifampin
🎈Urinary tract
Bacteriuria | UTI | |
Definition | Presence of microorganisms in urine
(same germs as UTI → see below
** extra:
P (+ Enterococ)→ in male; K (+all other) + Gardneralla → in female) | Microbial invasion of any of the tissues extending from the urethral orifice to the renal cortex |
Significance | Significant bacteriuria: the number of bacteria in the urine collected ≥ 10^5 CFU / ml;
CATHETER-related BACTERIURIA -> 10^2 CFU / ml | Clinical symptoms may include frequent urination, painful urination, and lower abdominal pain.
Upper UTI might present with positive giordano, oliguria, fever or signs of sepsis. |
Asymptomatic cases | Asymptomatic bacteriuria: significant bacteriuria without clinical symptoms
Prevalence:
- Catheter
- UT abnormalities
- Elderly
- Hemodialysis | Asymptomatic UTI can occur but is less common |
Diagnosis | Urine culture test | Urine culture test and/or imaging tests such as CT scan or ultrasound |
Treatment | Only if symptoms! | Antibiotics are usually prescribed for symptomatic UTI |
Etiology:
Female:
- E. coli
- Other Enterobacteriaceae • Klebsiella pn
- Enterococcus spp
- Streptococcus grup B
- Staphylococcus coagulazo neg
- Gardnerella vaginalis
Patients with indwelling devices:
- Pseudomonas
- Proteus m.
Males
- Enterococcus ssp.
- Other BNM - Proteus mirabilis
Infection Type | Etiology | Predominant Bacteria | Favoring Factors |
↑ Ascending (97%) | Mainly Gram-negative bacteria | E.Coli (80%), Proteus spp, Klebsiella spp, Enterobacter spp, Serratia marcescens, Pseudomonas aeruginosa
ØGram neg (Enterococcus, Staph epidermidis, Candida) | OBSTRUCTION:
Vesicoureteral reflux, foreign bodies, instrumentation of urinary tract/endoscopy, bladder catheterisation |
↓ Descending (3%)
(hematogenous spread → microabscesses) | Gram-positive bacteria & Fungi | Staphylococcus spp, Streptococcus spp, Candida spp | Kidney trauma, obstructions, diabetes, immunosuppression |
- 🔥 inflammatory + 🥐 renal markers
- 📃 Urinary Strip Exam - Dipstick
- THE PRESENCE OF 🧨 NITRITES → Enterobacteriaceae
- ⚪ LEUKOCYTIC ESTERASE TEST → Bacteriuria
- 🐈 CATALASE TEST
- 🧫 Urine culture (+blood cultures)
- 🔬 MICROSCOPIC EXAMINATION OF URINARY SEDIMENT ⇒ Leukos + GRAM STAIN
- ABACTERIAL LEUKOCYTURIA (sterile pyuria) → Urinary tract inflammation - tumors, stones, prostatitis, orchiepididymitis, renal TB, chlamydia trachomatis
- 🦇 Imaging examinations - abdominal ultrasound/CT/MRI








🧫 URO-culture
- 🧻🥚TMP-SMX
- 🌷 Fluros
- 🚴🏼Tetracyclins
- 🤺 Aminogylcosides
- NOT IN SKETCHY!:
- 🚘 Imipenem
- 🦅some Macrolides (Clarithro + Spira-mycin)
- 🚧Linezolid


- 🦑 Cephalos (1. + 2. GEN)
- 🔫 Amoxi-clav
- 🧨 Nitrofurantoin (⚠️ cave: Last weeks of pregnancy → 🍅 hemolytics anemia)
- 🥚 Fosfomycin
same as complicated pyelonephritis (see above)
- Pip-Taz
- Cephalos (3. + 4. GEN)
- if complicated → Meropenem, Ertapenem

Screening for asymptomatic bacteriuria

- Vesico-uretheral reflux
- Obstructive uropathies
- pyureteral junction syndrome, megaureter, ureteral duplications
- Posterior urethral valve
- Lithiasis
- Renal malformations (horseshoe kidneys, polycystic kidneys, renal hypodysplasia)
- Phimosis
- Chronic constipation
- Neurogenic bladder
- Micturition dysfunctions
- Incomplete perineal hygiene
- 🖼️ IMAGING - also possible prenatal!
- 🧫URO-CULTURE
- inflammatory makers
- 🔪SURGICAL CORRECTION of abnormality
- 💊 AB:
Infant / Young → Amoxi / Cephalos
Older child→ Biseptol, Nitrofurantin → Ø-obstructive: 3-6m → obstructive: 6-12m (or until surgery) → malformation: life-long
⇒ Follow up: multiple cultures if recurrence or high risk
🧠 Nervous system
- 🔥INFECTIOUS syndrome: fever, chills
- 🦢 MENINIGEAL signs:
- ⏫ ↑ICP signs
- headache
- photophobia
- papilloedema → blurred vision
- vomiting +/-nausea,
- Cushings triad (↓HR + ↑pulse pressure (↑sysBP) + irregular breathing)
- (fontanelle bulging in babies)
- 🧠CEREBRAL signs: FND, ↓conciousness, seizures, neuro-psych
- 🦵🏼 PETECHIA / purpura (meningococcal)


- Abscesses
- Brain damage
- Coma
- Death
- Hearing loss (partial or total)
- Recurrent seizures (epilepsy)
- Problems with memory and concentration
- Co-ordination, movement, and balance problems
- Learning difficulties and behavioral problems
- Vision loss (partial or total)
- Loss of limbs (amputation may be necessary)
- Bone and joint problems (such as arthritis)
- Kidney problems
- 🧫 Bacterial
- newborns → 🧑🏾🚀S. agalactiae + 🥤E.coli + 🎅🏾Listeria
- Children → like #1 (but 🕵🏾 N.mening > 🎠 S.pneu)
- adults → #1 🎠🕵🏾🍒
- elderly + ↓immunity → like #1 🎠🕵🏾 (excl. H.influenza) + 🎅🏾Listeria
- Intracranial manipulation / CSF shunts → Staph ⇒ 🦾Coagulase-neg + 🍢Aureus
- close contacts → 🕵🏾N.mening
- Basilar skull fx → 🎠 S.pneumoniae + 🥧 GAS
- Rodents → 🐳 Leptospirosis
- TBC? → tuberculous menigitis (often with central cranial n. palsy)
- 🦠 viral, 🍄 fungal
- 👻Mumps
- Incubation Phase:
- Duration: 7-14 days on average.
- Characteristics: Asymptomatic or minor non-specific symptoms.
- Prodrome or Minor Illness Phase (corresponding to viremia):
- Duration: 2-4 days.
- Symptoms: Fever (39-40 degrees Celsius), myalgias, pharyngitis, diarrhea, and meningeal irritation signs.
- Note: Typically self-limited.
- Latency Period:
- Duration: 2-4 days.
- Characteristics: Asymptomatic phase before major illness onset.
- Major Disease Phase:
- Symptoms: Recurrent fever, subsequent paralysis, muscle hypotonia, asymmetric/proximal muscle atrophy, intense pain, abolished reflexes, preserved sensitivity, meningeal irritation, and possible cardiac and gastrointestinal manifestations.
- Reversal of Paralysis Phase:
- Onset: 10-14 days after major disease onset.
- Duration: Can last months to years, with 50% of paralysis recovering in the first 3 months and up to 75% within 1 year.
- Sequelae Period:
- Conditions: Permanent paralysis with muscle atrophy, limb deformations, tendon retractions, and various deformities (equine foot, valgus, flat foot, lordosis, kyphosis, scoliosis).
- Post-Polio Syndrome (PPS):
- Onset: 25-30 years after acute illness.
- Manifestations: Muscle weakness, pain, and atrophy. About one-third of recovered patients may present symptoms.
- 🕊️Coxsackie-virus
- 🦜Echo-virus
- 🍄 candida
#1 🎠S.pneumonia >🕵🏾N.menigitidis > 🍒H.influenza
Depending on age:



Polio Clinical Progression Timeline




- Lumbar puncture → CSF analysis
- Bacterial: ↑↑WBC (>80% PMNs); ↓Gluc; ↑↑Proteins
- Viral ↑WBC (Lymphos predominant); n Gluc; ↑Proteins
- Exclude other DDx ⇒ +/- Imaging (CT, MRI)
** also: Blood culture + culture from suspected primary infection focus
⇒ INDICATIONS: ↑ICP, basilar fracture, paranasal sinuses, CNS complications (hydrocephalus, stroke, abscess, thrombosis etc)
- Empiric Tx (depends on predisposing factor & GRAM STAIN + AGE
- Target Tx
- S pneumoniae → Penicillin G, Ceftriaxone, Vancomycin
- H influenzae → Ceftriaxone
- N meningitidis → Penicillin G
- L monocytogenes → Ampicillin + aminoglycoside
- S. agalactiae → Ampicillin + aminoglycoside
- Enterobacteriaceae → Ceftriaxone + aminoglycoside
- P aeruginosa → Ceftazidime + aminoglycoside

(if young / old ⇒ add AMPICILLIN to cover Listeria)
0-4w ⇒ Ampicillin plus Cefotaxime
Amipicillin:

Cefotaxime:

Age 1-3 m ⇒ Ampicillin plus cefotaxime plus vancomycin
AMpicillin:

Cefotaxime:

Vanco:

3m to 50 y ⇒ Ceftriaxone / cefotaxime plus vancomycin
Age older than 50 y (or ↓immunity) ⇒ Ampicillin plus ceftriax/cefotaxime plus vanco
Ampicillin:

Neurosurgery, head trauma, or CSF shunt ⇒ Vancomycin plus ceftazidime/meropenem
Vanco:

Ceftazidime:

Meropenem:

- 🌝 Dexamethasone ⇒ efficacy only proven in 🍒 H.influenza!
- 🍩 Manitol
- 🌊 Furosemid
⇒ severe: ANY NEURO-SIGN can be present
Sudden fever, Severe headache, Nausea and vomiting, Stiff neck, Bulging in the soft spots (fontanels of the skull in infants), Drowsiness, Confusion and disorientation, Seizures, Coma.

Flu-like prodrome




- Non-arthropod-borne
- 👼🏼 HSV-1 & HSV-2
- Pain: Dull, pulling, sometimes intense pain in the affected ganglion area.
- Paresthesia
- Vesicles
- Skin lesions are pinhead to rice-sized, clear blisters
- Vesicles are on an erythematous base.
- 🍺 EBV - HHV4
- 🛒 CMV - HHV5
- ❤️ Congenital heart disease: patent ductus arteriosus, septal defects.
- 👁️ Eye lesions: microphthalmia, cataract, glaucoma, chorioretinitis.
- 👂 Hearing impairment: deafness.
- 💀microcephalia
- 🫀myocarditis
- 🍑hepatosplenomegly, jaundice
- 🦴BM: Amegakaryocytic thrombocytopenic purpura
- 🧠
- autism/mental retardation
- epilepsy
- 🦩 Polio-virus
- 🕊️Coxsackie-virus
- 🦜Echo-virus
- 🦷 Flu (influenza)
- Arthropod-borne
- 🐴 Toga → EQUINE
- 🥍 Bunya → La crosse
- Flavi
- West-Neil
- St. Louis + Japanese
- (TBE)
- Tick-borne encephalitis (flavi)
- TBE virus (FSME)


Shingles:
Dermatomal pattern: Symptoms often affect dermatomes from Th3 to L3.
♻️ SYSTEMIC acyclovir (or others)



↓ - after







MMR (mumps, measles, rubella)
Detection of the virus depending on timing:

(infection during FIRST trimester)
+ blueberry muffin rash 📷


↓
↓
↓



serum + spinal fluid ⇒ DIRECT IF (immunoflorescence)



*in children (<8y) ⇒ Amoxi !
- 🐱 Toxoplasmosis
🥫 canned food ⇒ ingestion of (pre-formed) toxin
(exception: in babys = spores in honey → see next Q.)
DESCENDING FLACCID PARALYSIS (purely PNS!)
→ 4D’s: diploplia, dysphagia, dysarthria, dyspnea
⇒ Ø CNS/Meningeal + ØSENSORY + Ø FEVER

⇒ “Floppy Baby syndrome” (spores in honey)
- Babies: Ingest spores
- Adults: Ingest pre-formed antigen (toxin) from improperly canned foods
- Rapidly identify botulinum toxin in samples from serum, GI (vomit, gastric acid, stool), or suspicious foods → ELISA, PCR
- Pathological EMG findings in affected muscles support the diagnosis.
BIG IV:

- All → Symptomatic (Ventilation, Fluids, Electrolytes)
- Food-born ⇒ 🐎 Horse-derived botulism antitoxin
- Wound botulism ⇒ 🐎 Horse-derived botulism antitoxin +/- 🔪 surgical debridement, +/- 💊 AB if superinfection
- Infant botulism ⇒ 👶🏼 IV human botulism immune globulin (BIG-IV)
• 1 - 3 months of hospitalization. • Complete resolution of symptoms in 6 months.

*C.tetani spores

- 🔪 Wound care → Toilet
- 💊 AB → 🚇 Metronidazole or ✏️ Penicillin G
- 🧪 Anti-toxin → anti-tetanus human IgG
- 💉 Vaccine (DTP)
- 🏹 Symptomatic ⇒ ICU 🏥
- Spasms:
- ↑Autonomic activity:
→ Benzos, NMJ blocker (Dantrolene) → Ventilation
→ Beta-blocker (Propranolol, Metoprolol)


Polio Clinical Progression Timeline
- Incubation Phase:
- Duration: 7-14 days on average.
- Characteristics: Asymptomatic or minor non-specific symptoms.
- Prodrome or Minor Illness Phase (corresponding to viremia):
- Duration: 2-4 days.
- Symptoms: Fever (39-40 degrees Celsius), myalgias, pharyngitis, diarrhea, and meningeal irritation signs.
- Note: Typically self-limited.
- Latency Period:
- Duration: 2-4 days.
- Characteristics: Asymptomatic phase before major illness onset.
- Major Disease Phase:
- Symptoms: Recurrent fever, subsequent paralysis, muscle hypotonia, asymmetric/proximal muscle atrophy, intense pain, abolished reflexes, preserved sensitivity, meningeal irritation, and possible cardiac and gastrointestinal manifestations.
- Reversal of Paralysis Phase:
- Onset: 10-14 days after major disease onset.
- Duration: Can last months to years, with 50% of paralysis recovering in the first 3 months and up to 75% within 1 year.
- Sequelae Period:
- Conditions: Permanent paralysis with muscle atrophy, limb deformations, tendon retractions, and various deformities (equine foot, valgus, flat foot, lordosis, kyphosis, scoliosis).
- Post-Polio Syndrome (PPS):
- Onset: 25-30 years after acute illness.
- Manifestations: Muscle weakness, pain, and atrophy. About one-third of recovered patients may present symptoms.


🖐🏾 Skin

Layer | Etiology + Pathology | Signs + Symptoms | Location | TYPICAL patient | Specials | |
Impetigo contagiosa 📷 | Epidermis
(below S. corneum) | S.Aureus or GAS
→Neutrophils beneath S. corneum | Macule → vesicles → rupture
⇒ “honey-colored” crust (dried sebum) | Face + extremities | child | ↑↑ contagious
DDx: Herpes Simplex |
Bullous Impetigo 📷 | Epidermis
(S. Granulosum) | S.Aureus
→ Exfoliative Toxin (cleaved desmoglein 1 complex) desmosome damage
→ keratinocyte de-attachment → fluid in space | Bulla / blister (Nikolsky +) on erythem. base
clear → cloudy → pus → rupture
→ crust
↑LN | Face, neck, hands
Trunk involved | child | Øscar
|
Scalded skin synd. (SSSS) 📷 | Epidermis | S. Aureus
→ DIFFUSE exfoliative toxin | Infectious signs: Fever + Diffuse Erythema
large Bulla (Nikolsky +) → rupture
→ Sloughing/peeling of skin
| diffuse
| newborn or child
(3-7d post-natal) | Øscar
(Øinvolvement of dermis or basal layer of epidermis)
**in contrast to Staphyloccal toxic shock syndrome (SSSS vs. STSS)
DDx SJS |
Erysipel 📷 | Dermis - SUPERFICIAL
(+superfic. lymphatic) | GAS
Skin break/trauma → bacterial entry
or endogenous (sinusitis, pharyngitis,etc) → facial erysipel | FAST onset
↑LOCAL SIGNS → painful, warm, red
Rash ⇒ clear DEMARCATION + elevated borders + spread over time
↑↑ SYSTEMIC SIGNS | LEG (unilat. after fall)
or FACE 😊 | child or older adults | Variants: bullosum + gangrenosum + chronic recurr.
DDx: cellulitis, compartment sy, hypodermitis |
Cellulitis 📷 | Dermis - DEEP
+- subcut. fat | S.Aureus or GAS
Skin break/trauma → bacterial entry | SLOWER onset
↑LOCAL SIGNS → painful, warm, red
Rash ⇒ ILL-DEFINED + spread over time + Øelevated borders
SYSTEMIC (uncommon, less than erysipel) → ↑LN | LEG (unilat) | middle-age + eldery (↓immunity) | ⇒ Complication: Thrombophlebitis, Elephantiasis (if recurr), deeper extension
⇒ Systemic: Staph Aureus / GAS complications |
Dermis or Subtaneous | S.Aureus
→ pus collection (Np+bact)
→ may complicate cellulitis/erysipel | 💥 red + painful nodule w/ central yellow plug
tense + raised skin
🔥 fever + ↑LN
⇒ central plug DRAINS SPONT. ⇒ SCAR
| - multiple = FURUNCULOSIS ⇒
→ Permissive factors for FURUNCULOSIS → ↓immunity (atopic dermatitis, Diabet, HIV,..)
- ↑risk: sepsis, cavern. sinus thromb., endocarditis | |||
Necrotizing Fasciitis 📷 | Fascia
(+subc. fat) | Anaerobes (Clostridium..) → after surgery in immunocompromised
GAS (or S.Aureus)→ after skin injury in otherwise healthy
→ Necrosis of tissue above fascia | 1) rash → color changes: red → purple/blue → black
+-bulla
2) pain + tenderness ⇒ out of proportion to rash
3) Crepitus when pressed (bact. gases)
(fever + local infectious signs)
4) Hypo-esthesia | ↓immunity . post-surgery
or
after skin injury | ⇒ IMAGING! (+muscle enzyms, renal)
quick, uncontrolled spread along fascia ⇒ SEPTIC SHOCK
pain eventually stops when nerves are destroyed
|
furuncle: abscess due to folliculitis
carbuncle → multiple follicles infected ⇒ multiple pustules on inflamed plaque
Disease | Tx |
Impetigo contagiosa | Topical AB (i.e. fucidic acid)
Systemic oral AB (amoxi-clav, erythro, clinda, doxy, tmp-smx) |
Bullous Impetigo | Topical AB (fucidic acid)
Systemic oral AB (amoxi-clav) |
Scalded skin synd. | Systemic oral AB (Vanco) |
Erysipel | Systemic oral AB
- penicillin G, or other betalac (cefalexin, amoxi, erythro)
- + clinda
→ 1-2w (duration) |
Cellulitis | systemic oral AB
- cephalexin, amoxi-clav, Oxa/Nafcillin if S.Aureus
- + clinda |
Abscess (Furuncle / Carbuncle) | topical anti-septic/AB
systemic oral AB (Clinda, doxy, TMP-SMX)
incision + drainage required |
Necrotizing Fasciitis | 🚑 !
- syst. i.v. AB (Penicillin+Clinda)
→ urgent surgical debridement
(if mixed (anaerob+aerob) = Pip/Taz+Vanco or Cefotax + Clinda) |

- 🏹 Borrelia burgdorferi (Lyme’s disease)
- 🪓 Bacillus Anthracis
- 👻 Measles (RubeOla) & Mumps (Paramyxo-viridae)
- Day 0-1: Prodrome begins.
- Days 2-3: Koplik spots appear.
- Days 4-5: Morbilliform rash appears.
- Day 6: Koplik spots regress.
- Days 7-8: Rash is most intense.
- Day 10: Rash begins to resolve.
- Approximately 1/3 of postpubertal male patients develop unilateral orchitis.
- Orchitis usually follows parotitis, but it may precede parotitis or occur in the absence of parotitis.
- It typically appears in the first week, but it can occur in the second or third week.
- Bilateral orchitis is less common.
- Gonadal atrophy may follow orchitis, but sterility is rare even with bilateral involvement.
- Orchitis is accompanied by high fever, severe pain, swelling, nausea, vomiting, and abdominal pain.
- Fever and gonadal swelling usually resolve in 1 week, but tenderness may persist.
T
erythrogenic toxin
(makes you red 👹)
- Pharyngitis signs + non-specific inflammatory
- +- GI signs
STREP THROAT:


TONGUE:

characteristic course: (total = 7d)
Day 0-2:
WHITE coat
(w/ red prominent papillae)
Day 2-5
RED due to desquam. (w/ prominent papillae)
Day 5-7
NORMAL




(infection during FIRST trimester)
- ❤️ Congenital heart disease: patent ductus arteriosus, septal defects.
- 👁️ Eye lesions: microphthalmia, cataract, glaucoma, chorioretinitis.
- 👂 Hearing impairment: deafness.
+ blueberry muffin rash 📷
- 💀microcephalia
- 🫀myocarditis
- 🍑hepatosplenomegly, jaundice
- 🦴BM: Amegakaryocytic thrombocytopenic purpura
- 🧠
- autism/mental retardation
- epilepsy
Detection of the virus depending on timing:




Shingles:
Dermatomal pattern: Symptoms often affect dermatomes from Th3 to L3.
- Pain: Dull, pulling, sometimes intense pain in the affected ganglion area.
- Paresthesia
- Vesicles
- Skin lesions are pinhead to rice-sized, clear blisters
- Vesicles are on an erythematous base.
♻️ SYSTEMIC acyclovir (or others)


🔦 Torch infection
Primary infection

Latent phase:

AIDS:
Screening: ELISA
Confirmation: Western Blot/Differentiation Assey
- ACUTE HIV INFECTION: HIV ELISA negative
- ASYMPTOMATIC STAGE: HIV ELISA positive
- SYMPTOMATIC STAGE: HIV ELISA positive


NRTIs: Tenofovir Emtricitabine Abacavir Lamivudine Zidovudine
NNRTIs: Efavirenz Nevirapine Etravirine Rilpivirine
PIs: Darunavir Atazanavir Ritonavir Lopinavir
Interrase inhibitors: Raltegravir Dolutegravir
Fusion Inhibitors: Enfuvirtide
CCR5 Inhibitors: Maraviroc
mnemonic:


The existence of viral sanctuaries is an obstacle in infection eradication bc it does not only resides in CD4+ T cells ⇒ sanctuaries: CNS, male genital tract, intestinal tract + lymphoid tissue.



*can also lead to PNEUMONIA in ↓IMMUNITY

- SEROLOGY ⇒ ↑IgG (IgM without significance) ⇒ acute infection = ↑↑IgG
- PCR → esp. in 🤰🏼 amnionic fluid pre-netal
- Culture + 🐁 mouse inoculation
- histo

⇒ qualitative test with ELISA ⇒ follow up with: IgG Avidity test





- Other
- Secondary syphilis
- Tuberculosis
- Leptospirosis
- Brucellosis
- Typhoid fever
- Tularemia
🦴 Bones
F
Caused by bacteria, mycobacteria, fungi or parasites

monoarticular (20% = polyarticular)


- pain
- loss of function
- swelling
- warmth
- red
- +/- fever
STAPH AUREUS
typical patient:
- remote infection in patients with ↓immunity (elderly, small children, immuncompromised)
- iv drug user
- direct innoculation (trauma, surgery)

- genitourinary diseases is often asymptomatic
- tenosynovitis hands + ankles

- rash📷
- migratory polyarthritis
- fever

- Arthrocentesis → synovial fluid analysis
⇒ Culture + GRAM (joint + blood )

- Arthrocentesis → synovial fluid analysis
⇒ 🔬 GRAM - & 🧫 hemo-cultures + (chocalate agar) → also of oropharynx, rectum, vagina
⇒ PCR
- Consider imaging in all cases (MRI/CT)

- 1) 💉Joint drainage
F → start before: HISTORY + typical patient ‼️
⇒ GRAM STAIN !!!

Cefriaxone single I.M. dose !
⇒ Doxy / Azithro to cover Chlamydia
Gram-Neg. Rods: Cover pseudomonas⇒ 🖼️🪐 PSEUDOMONAS-BETALACTAMS (Ceftazidime, Cefepime, Piperacillin-tazobactam)
negative (unclear) Gram stain ⇒ COVER ALL ⇒ 🖼️🪐 PSEUDOMONAS-BETALACTAMS + 🚌 VANCO (cover MRSA)
- Hematogenous
- Non-Hematogenous
- Contiguous spread: from adj. soft tissue or joints
- Direct inoculation: due to trauma/surgery
- other G+ cocci: Streptococci Enterococci
- GI- entero bacilli: Pseudomonas spp. Enterobacter spp. Proteus spp. Escherichia coli Serratia spp.
- Anaerobes: Finegoldia (Peptostreptococeus] spp., Clostridium spp., Bacteroides fragilis group.
- Mycobacterium tuberculosis
- Adults typically have nonspecific symptoms with a subacute-to-chronic course.
- Fever, chills, local swelling, and erythema near the affected bone are uncommon.
- Non-specific pain around the affected site with no systemic signs is common.
- A draining sinus tract may be present over the affected bone.
- The condition usually progresses over several months or years.
- Lab: ↑inflammatory markers
- 💉 SAMPLING → NEEDLE aspiration or surgical sampling (before AB-Tx!!)
- Imaging → CT / MRI
⇒ 🔬microscopy + Gram stain
⇒ 🧫 culture
- Staph
- MSSA → Oxacillin/Naficillin
- MRSA → Vanco
- Strep
- Penicillin sensitive → Penicillin
- Enterococci or penicillin resistent strep. → Ampi, Genta / Vanco
- Enterobacteriacea → Cetriaxone
- Pseudomonas → Cefepime, Imipenem
- Staph: Aureus, coagulase-neg.
- Strep
- TBC
- Brucella
- in IV drug users / Immunosuppressed ⇒ Gram- aerobic + Candida
- localized pain + tenderness
- fever
- motor / sensory deficits
- 🧲 MRI (or PET-CT)
- irregular contour (vertebral endplates)
- disc space narrowing & complete discal collapse
- edema within disc & vertebral plates
- 🔥 Inflammatory markers (ESR, WBC) → check for concom. infective endocarditis!
- 🧫Culture → #1 Blood #2 percut. biopsy
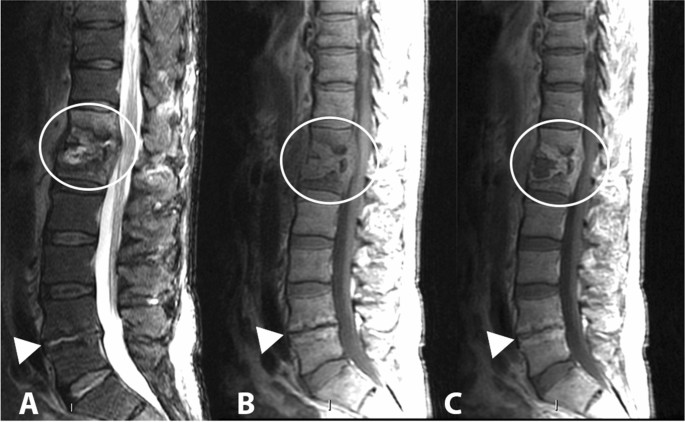
Spondylodiscitis
💊AB → see osteomyelitis DURATION: 6w
- MRI 📷⇒ paravertebral ST-ABSCESS 🍏
- Biopsy → Stain / Culture
- Xray (concom. pulmonary TB?)
- Staph Aureus
- Coagulase-neg. Staph
- Strep.
🔥 Sepsis & Fever
SIRS is diagnosed if ≥ 2 of the following 4 criteria are fulfilled:
- 🔥 Temperature: > 38°C↑ or < 36°C↓
- ⚪ White blood cell count: > 12,000/mm3, < 4000/mm3, and/or > 10% band cells
- ♥️ Heart rate: > 90/min
- 🫁 Respiratory rate: > 20/min or PaCO2 < 32 mm Hg

- Respiratory: Decreased Pa02 / Fi02 ratio, Need for supplemental oxygen
- Renal: Elevation serum creatinine, Decreased urine output, dialysis-dependent
- Coagulation system: Thrombocytopenia, DIC (disseminated intra-vascular coagulation)
- Metabolic: Lactic acidosis, Impaired gluconeogenesis and insulin resistance, poor control of blood sugar in diabetic patients
- Liver: Increased ALT, AST, bilirubin, Alk.P, LDH, CRP
- Gastrointestinal tract: Ileus, ulcers, ischemic bowel
- Cardiovascular system: Hypotension = Septic shock, Decreased myocardial contractility, Pooling of blood in the microcirculation
- Two phases of septic shock: Early hyperdynamic phase, Later hypodynamic phase
- Refractory septic shock: Shock >1 hr, and does not respond to fluid or pressor administration
The quick Sequential Organ Failure Assessment (qSOFA) score is a bedside prompt that may identify patients with suspected infections who are at greater risk for poor outcomes.
Parameter | Score |
🫁Respiratory rate ≥ 22/min | 1 |
♥️ Systolic blood pressure ≤ 100 mmHg | 1 |
🧠 Altered mentation (GCS <15) | 1 |

A qSOFA score ≥ 2 suggests a greater risk of poor outcomes such as prolonged ICU stay, need for mechanical ventilation, or death. The score can be calculated at the bedside with a simple physical exam, and can help clinicians identify patients who may require closer monitoring and more aggressive management.
- inflammatory markers → incl. procalcitonin
- Organ dysfunction marker
(leukos, esr, crp, fibrinogen)
(liver, renal, blood gas → lactic acidosis!)
- IMAGING → depending on suspected source
- lab markers + imaging (see “2.”)
- CLINIC
- Fever / hypothermia,
- Altered mental status
- CV: Tachycardia, hypotension, Bleeding, Heart failure
- Lungs: Hyperventilation, cough, cyanosis, acidosis, full-blown ARDS
- Kidneys: oliguria, anuria, tubular necrosis
- Liver: jaundice
- Gastrointestinal: nausea, vomiting, diarrhea, stress ulceration
- Skin: petechiae (suspect especially meningococcemia), ecthyma gangrenosum (Pseudomonas), generalized erythroderma (TSS)
- Systemic: lactic acidosis
What is the empiric Tx of …
COVER (mainly): ENTEROBACTERIACEA + Gram - aerobes ⇒ Pseudomonas + Enterococcus
🤺Aminoglycoside + 🪐 beta-lactam (3rd/4th gen cepahlo / pip-taz)/🌷fluros




COVER: S.pneu, N.mening. ,H.influenza, aerobic G- bacilli, Listeria
🦑3rd GEN Cephalo + 🚌 Vanco +- 🎸 Ampicillin


COVER: G+ cocci (incl. MRSA + Enterococci)
🚌Vanco + 🤺Gentamycin

COVER: G- bacilli, enterococcus, anerobes 🦑3rd GEN CEPHALO + 🤺Aminoglycoside + 🚇 Clinda/Metro

🦑3rd GEN CEPHALO + 🌷respiratory fluros / 🦅macrolide


COVER: MRSA + G- bacilli (incl. ESBL-E.coli, Pseudomonas, Klebsiella)
🚘 Carbapenem + 🚌vanco

COVER: Staph, Strep, anerobes, pseudomonas (in ↓immunity)
🦑1st GEN CEPHALO + 🧼 Clinda + 🤺Genta
COVER: capsulated → S.pneu, H.influenza, N.mening.
🦑3rd gen CEPHALO + 🚌Vanco

Cover: Staph (MRSA + Coagulase neg), enterococci, G- Bacilli (incl. Pseudomonas)
🚌Vanco + 🚘carbapenems
Cover: pseudomonas, MRSA, candida
🦑Ceftazidine/ 🚘carbapenem + 🚌 vanco + 🍄fluconazol
- 4) 🚿 Consider other Shock-Tx: - Fluids - Drugs ⇒ Vasopressors, Inotropics, Steroids, Gluc control
- 5) ⏬ Narrow down AB Tx ⇒ depending on culture results
Adults | Children |
>38,3 °C (intrarectal) | >38,3 °C |
>3 weeks | > 8days |
No proven etiology despite adequate investigations
(3days of hospitalization + ≥3 outpatient exams → including Xray, urine&blood culture) | No Dgx |
- TB
- Brucellosis
- Coxiella (Q-Fever)
- HIV infection
- Abdominal abscess
- Cat's scratch Disease
- EBV infection
- CMV infection
- Toxoplasmosis
- Extrapulmonary TB
- Subacute infectious endocarditis
- Vascular graft infections
- Abscessed tooth
- Chronic sinusitis
- Mastoiditis
- Chronic prostatitis
- Cholecystitis
- Discitis
- Whipple disease (Tropheryma whipplei, Gram neg. bacillus)
- Benign venereal lymphogranuloma (Chlamydia trachomatis)
- Giant cell arteritis
- Still’s disease
- Agammaglobulinemia / Variable immune deficiency
- Inflammatory bowel disease(Crohn's disease & UC)
- CNS dysfunction: Thermoregulation disorders, Epilepsy with fever, phenytoin response
- Diabetes insipidus
- Munchausen syndrome
- Kawasaki disease
1. Lymphomas
2. Kidney tumor
3. Acute myeloblastic leukemia
4. Multiple myeloma
5. Tumors of liver, breast, pancreas, colon, secondary determinations
- Thyroiditis (search ATPO)
- Drug induced fever (DRESS syndrome = Drug reaction with eosinophilia and systemic symptoms) → i.e. after Vanco
- Fever can occur weeks or months after starting medication
- Drug-induced fever is observed in about one-third of patients
- Common medications that can cause fever include antibiotics (sulfamides, penicillins, nitrofurantoin, vancomycin), antimalarials, barbiturate antiepileptics, phenytoin, iodine-based products, NSAIDs (salicylates), anti-HTA medications (methyldopa, hydralazine), and antiarrhythmics (quinine, procainamide)
- Increased eosinophils and rash
- Periodic hereditary fever
⇒ Fever typically resolves upon discontinuation of the medication
- Dgx-workup & Tx→ Depends on suspected / proven etiology



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



- Non-specific
- ↑ Liver marker
- ↓Eos
- ↓Thrombos
- Etiological:
- Rapid enzyme detection test: pLDH, HRP2, aldolase
- Blood smear + Giemsa 📷
- PCR
Serology→ only for past infection


= FEVER + COAGULOPATHY





- Nairoviridae (Crimean Congo hemorrhagic fever) & Phenuiviridae (Rift valley fever)