
Table of content
- Emergency Medicine
- ⛲ Basics of Emergency Medicine
- 💔 Cardic arrest & CPR
- 🍫 Shock
- 💥 Trauma
- 🔥 Burns
- 🧪 Intoxication
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Emergency Medicine
⛲ Basics of Emergency Medicine
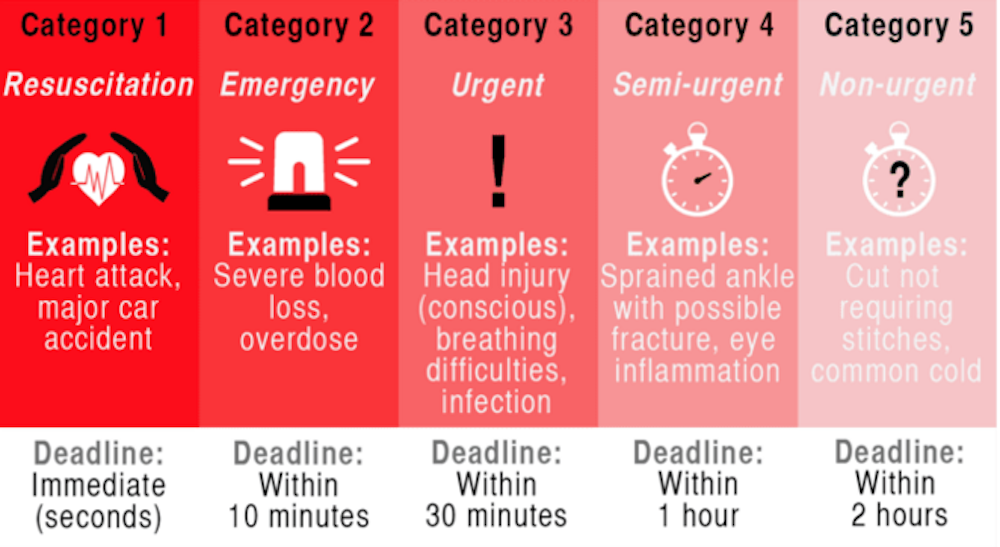
Level 1 - RESCUSCITATION
→ IMMEDIATE lifesaving intervention required
SCR, severe chest pain, massive vomiting of blood, sudden loss of consciousness, major trauma with hypotension
→ 0 min until Tx
Level 2 - CRITICAL
→ serious RISK, altered MENTAL STATUS or intense PAIN (incl. stroke)/turn 2
Acute dyspnea, abdominal/chest acute pain, acute confusion → Repeat triage until the patient is seen by the emergency doctor.
→ 15 min until Tx
Level 3 - URGENT
→ STABLE vitals, ≥2 Resources required
stable vitals:
Average abdominal pain, hemodynamically stable closed abdominal trauma, headache, fever, back pain, extremity injuries
resources:

→ 60 min (1h) until Tx
Level 4 - NOT URGENT
→ STABLE vitals, 1 Resource required
No risk of developing critical state -Sore throat, minor collisions, chronic disease, acne
→ 120min (2h) until Tx
Level 5 - CONSULT
→ ØEmergency Tx required (vaccination, social case, recipes)
→ 240min (4h) until Tx
Color | Level | Time |
RED | I | 0 min |
YELLOW | II | 15 min |
GREEN | III | 60 min - 1h |
BLUE | IV | 120 min - 2h |
WHITE | V | 240 min - 4h |
VITALS | MENTAL STATUS | |
Critical | INSTABLE VITALS | UNCONCIOUS |
Serious damage | INSTABLE vitals | altered mental state |
Almost good (convenient) | stable + n vitals | awake + unconfortable |
Good | stable + n vitals | awake + talks |
Unlimited | wait to be assessed |
ABCDE Assessment
What are the steps to consider in..
- ⤵️ OPEN Airway
- without device (subluxation/hyperextension)
- tubus
- 🪀 Remove FOREIGN BODY
- 👀 Inspection
- Assymmetry?
- Trachea deviation
- 🩺Auscultation, percussion (pneuo, hemothorax, stridor etc.)
- B- PARAMETER
- 💨 SpO2
- ⏱️ RR
- 🩸bleeding? ⇒ only treat PROFUSE bleeding during primary evaluation
- Uncontrolled bleeding can pose a life-threatening situation.
- In the initial assessment, the primary concern is profuse bleeding.
- Focus should be on the total volume of blood loss, rather than the speed of bleeding.
- 💪🏼Assess perfusion
- Pulse (central + periph)
- BP
- Recap
- skin color, temp, hydration
- 🔵 Assess preload:
- Jugular vein
- 🩺 ❤️- murmors? muffled heart sounds?

- 🥶 Hypothermia?
- 💦 Wet?
- 🧪 Toxic environment?
- 💊Medications?
- exposure: rash, edema, petechia
- BGA
- Biological markers (e.g., troponine , SCA, coagulopathies, sepsis (procalcitonine))
- Rapid urination tests
- Biochemistry with rapid tests
- Ultrasound
- Radiographs
aka life-threatening condition
what are 🚩 in..
- Sudden onset of headache
- Known history of aneurysm
- Family history
Category | Compressive Myelopathies: Spinal Cord Compression | Compressive Myelopathies: Conus Medullaris Syndrome | Cauda Equina Syndrome |
Etiology | Various factors can lead to spinal distress, like degenerative disk anomalies, vertebral disruptions, and more. | The spinal cord at vertebral levels T1–L2 might face distress due to injuries or coccygeal spinal segment issues. | Distress can occur in the cauda equina, especially in nerve fibers L3–S5. Disk herniation or tumors are frequent causes. |
Onset | Symptoms can appear bilaterally and might be intermittent. | Bilateral and sudden onset of symptoms. | Gradual onset, usually unilateral. |
Pain | Bilateral pain primarily in the neck or back. | Predominantly bilateral lower back pain with the possibility of intense radicular pain. | Unilateral lower back pain, with potential for intense radicular discomfort. |
Motor symptoms | Bilateral paralysis potential below the distressed spinal segment, alongside heightened reflexes and a distinct Babinski sign. | Bilateral heightened reflex actions in the lower limbs, potential muscle spasms, and an absent Achilles reflex. | Asymmetric flaccid paralysis of the legs and possible muscle atrophy. |
Sensory symptoms | Bilateral diminished sensation below the distressed area. | Bilateral general numbness and potential sensory dissociation. | Saddle anesthesia with potential uneven numbness in the lower limb dermatomic regions. |
Urogenital and rectal symptoms | Dysfunctions like urinary or bowel movement urgency, retention, or the opposite. | Early bladder and fecal inconsistencies. | Late urinary retention, altered bowel movements due to sphincter control issues, reduced anal reflexes, and bulbocavernosus reflex problems. |
🧠NEURO
- FND (i.e. BILATERAL paresis /paresthesia → i.e. cauda equina, unilat. if herniated disc)
- abnormal reflexes (= UMN lesion)
UMN (Upper motor neuron):

- incontinence (💩 + 🥐) → in autonomc nerve damage (cauda equina)
🤒 FEVER
Q. RED FLAG Clinical Signs for Lumbar Pain:
A. Right crural paresis B. Bilious vomiting C. Acute constipation (DD) D. Fever >38°C E. Incontinence
ADE

RISK FOR
- ❤️?
- ↓🌊 (hypovolemia)?
- or 🐼Anemia?
(BNP>300, Bradycardia, chest pain, patholog. Q, ↓SpO2)
(Anemia, DRE → blood)
💔 Cardic arrest & CPR
- 🪗 Airway obstruction
- 🫁Abnormal Breathing
- ❤️ Heart diseases
10% 📷
🤷🏼 Basic life support (BLS)

🚑 Advanced life support (ALS)


💊
40
Vasopressin- if the health system agree 40 I.U. i.v. single use
Magnesium:
Indications:
- Torsades de pointes
- hypomagnesiemia possible and
- shock refract. VFib or
- VT
- Digoxin intox
Dosage:
shock refractory Vfib: Mg sulfate 2g i.v. for 1-2min (dosage can be repeated after 10-15min)
Sodium Bicarbonate
Indications:
- Severe metabolic acidosis (pH <7.1)
- Hyperkalemia
- Special circumstances
- Overdose of tricyclic antidepressants
- Cardiac arrest induced by cocaine
Dosage:
0.5 to 1 mEq / kgc to 10 min in CPR 50 mmol (50 ml of 8.4%) i.v.


🦇
hypovolemia
tension pneu + tamponade

🚫
20min of asystolie
O2
- O2 (10-15l)
- Adrenalin im or iv
- Fluids
- antihistamines, steroids, bronchodilators

Change EKG | Serum K value (mEq/l) |
Where high, sharp T's | 5.5 - 6.5 |
Where P small/absent, PR extension | 6.5 - 7.5 |
QRS wide | 7.0 - 8.0 |
Sine wave pattern | → imminent cardiac arrest |

or salbutamol
Sabutamol promotes the uptake of potassium into cells by activating the beta-2 adrenergic receptors. These receptors are responsible for triggering the sodium-potassium pump, which transports potassium from the extracellular space into the intracellular space, effectively reducing the concentration of potassium in the blood.
Grade | Temperature Range | Description |
1 | 35°C - 32°C | Mild: conscious, shivering |
2 | 32°C - 28°C | Moderate: altered mental status |
3 | 28°C - 24°C | Severe: unconscious, vital signs present |
4 | Below 24°C | SCR or "no flow state": minimal vital signs, weak/slow/irregular pulse, unmeasurable blood pressure |
5 | Below 13.7°C | Irreversible hypothermia: death |

- external - room, blankets
- internal - iv fluid (42°C), gastric/peritoneal/ pleural/ vesical lavage (40°C), oxygen & warm air
- start with 5 RESCUE BREATHS (in lecture = 2??)
- warm fluids
- Dry before shock
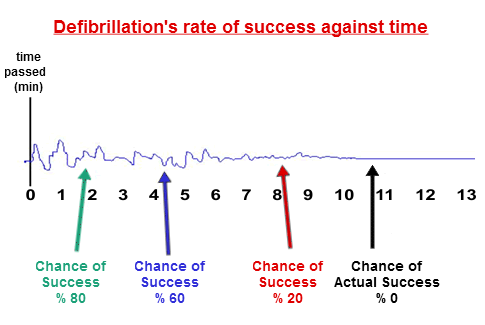
4J/kg
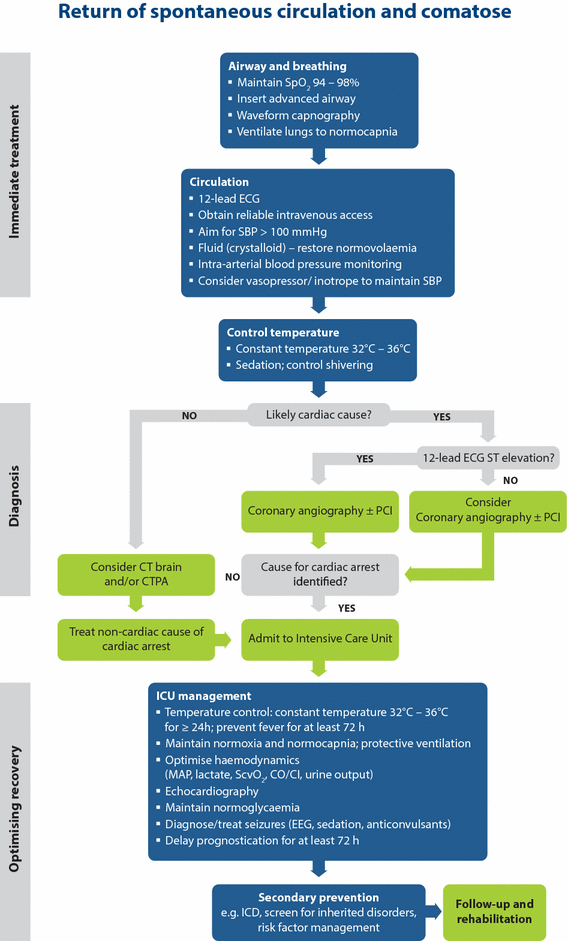
“return of spontaneous circulation”
🍫 Shock
merged with ATI
Disorder of circulatory system → inadequate organ perfusion + tissue hypoxia → metabolic disturb. → irreversible organ damage
1) Hypotension
2) Signs of end-organ hypoperfusion:
🧠brain : altered conciousness or other mental disturbance, weakness, dizziness, nausea
🥐kidney ⇒ 🚱 oliguria
💪skin ⇒ 🧊 cold, mottled, clammy/diaphoretic+ ↓recap time
→ exception: distributive⇒ 🥵 might be warm+flushed+ normal recap
3) Specific signs depending on type of shock (see below)
Pre-Shock
compensated, non-progressive shock
appears IMMEDIATELY after triggering event
Compensatory mechanisms only:
- Peripheral vasoconstriction
- 💪 🧊 cold + clammy + ↓recap
- may be absent in distributive shock ❗
- ❤️ ↑HR
- 🥐 Oliguria
Shock
decompensated, progressive shock
- ✨ ↓BP
- Hypoperfusion →🍼 Lactic acidosis (high AG metabolic acidosis)
⇒ 🧠 Altert mental stage
⇒ DIC
⇒ worsening tachypnea
End-organ dysfunction
irreversible shock
ORGAN FAILURE due to ISCHEMIA, INFLAMM. MEDIATOR + REPERFUSION INJURY
- 🧠 - autonomic dysfunction
- 🧠 - ↓/↑ activity
- ⇒ ❤️ - ↓↓output
- ⇒ 🫁 ⇒ ARDS ⇒ micro-thrombi
- ⇒ 🥐 ⇒ ischemia, oliguria, ↑↑RAAS + tubular necrosis
- ⇒ 🍑 ⇒ ischemia ⇒ ↑transaminases
- ⇒ 🍤 ⇒ ischemia ⇒ translocation of gut bacteria ⇒ septic shock
- ⇒ 🩸 (coagulation) ⇒ DIC + Thrombocytopenia
- Volume
- Shift ⇒ DISTRIBUTIVE shock
- Capillary leakage ⇒ SEPTIC shock
- Vascular tone dysregulation
- Loss ⇒ HYPOVOLEMIC shock
- Blood ⇒ HEMORRHAGIC shock
- Body fluids (i.e. GI) ⇒ NON-HEMORRHAGIC NON-TRAUMATIC shock
- Plasma (i.e. burns) ⇒ NON-HEMORRHAGIC TRAUMATIC shock
- Output
- Cardiac ⇒ CARDIOGENIC shock
- Myocardium (i.e. MI)
- Conduction system → arrhythmias
- valves
- Extracardiac ⇒ OBSTRUCTIVE shock
- Impaired filling ⇒ TAMPONADE
- ↑after-load ⇒ (massive) PE
- Obstruction of venous retunr ⇒ TENSION PNEU
⇒ ANAPHYLACTIC shock
⇒ NEUROGENIC shock
TYPE | CAUSES |
💧 HYPOVOLEMIC | - fluid loss (GI, burns)
- hemorrhage (esp TRAUMA) |
❤️ CARDIOGENIC | - cardiac ischemia
- arrhythmias
- valvulopathies
- cardiotoxic substances (see toxins) |
🚧 OBSTRUCTIVE | - cardiac tamponade
- PE
- tension pneu |
🔥 SEPTIC | - infection
- bacteremia |
🤧 ANAPHYLACTIC | - exposure to allergens
(food, sting, drug) |
🧠NEUROGENIC | CNS injury:
- traumatic brain injury
- intracerebral hemorrh.
- spinal cord injury |
- hypodynamic shock = all shocks, except distributive
- hyperdynamic shock = distributive
→ ↓ CO
→ ↑ SVR
→ ↑O2 extraction + lactic acidosis
→ variable CO (see next question)
→ ↓ SVR
→ normal O2 extraction
TYPE | OUTPUT | PRE-LOAD (PCWP or JVP) | AFTER-LOAD
(SVR) |
💧 HYPOVOLEMIC | ↓ | ↓ | ↑ |
❤️ CARDIOGENIC | ↓↓ | ↑ | ↑ |
🚧 OBSTRUCTIVE | ↓↓ | ↑ or ↓ | ↑ |
🔥🤧🧠 DISTRIBUTIVE | 🧠 ↓
🔥 🤧 early:↑ ; late: ↓ | ↓ | ↓↓ |
Gap between systolic + diastolic BP
⇒ wide in distributive
⇒ narrow in cardiogenic (+others)
💪 skin perfusion | 🚹 jugular v. | ⭐ specific | |
💧 HYPOVOLEMIC | 🧊 cold + diaphoretic + ↑recap
↓tugor+dry membranes
| Ødistended | -signs of cause (bleeding, diarrhea)
-Shock index (HR/BP) > 0.9 |
❤️ CARDIOGENIC | 🧊 cold + diaphoretic + ↑recap | distended + ↑JVP | -HF signs (i.e. dyspnea)
-signs of cause (chest pain, palpitations, murmor)
-mechanical complication (mitral insuff, septal/free wall rupture + taponade, aneurysm) |
🚧 OBSTRUCTIVE | 🧊 cold + diaphoretic + ↑recap | distended + ↑JVP | -signs of cause (chest pain, ↓breath sounds, tracheal deviation, muffled heart sounds, DVT signs) |
🔥 SEPTIC | early: 🥵 warm + flushed
late: 🧊 cold + pale + ↑recap | -🤒 sepsis signs (fever, SIRS criteria)
Source signs(signs of pneumonia, UTI, menigitis) | |
🤧 ANAPHYLACTIC | 👹 rash + flushed + edematous | 🫁 - stridor, wheezing, cough
💩 - vomiting + diarrhea | |
🧠NEUROGENIC | 🥵 warm + flushed | ↓❤️ BRADYCARDIA
neurological-deficits |
The patient is placed in supine position with the torso elevated to 45 degrees and the head rotated away from the examiner. Tangential lighting can help elicit the finding. Determine the vertical distance between the upper limit of visible distention of the internal jugular vein and the sternal angle. A distance > 4 cm is considered elevated.
- Systemic inflammatory response syndrome (SIRS):
- Diagnosis: ≥ 2 of the following 4 criteria:
- Temperature: > 38°C or < 36°C
- Heart rate: > 90/min
- Respiratory rate: > 20/min or PaCO2 < 32 mm Hg
- White blood cell count: > 12,000/mm3, < 4000/mm3, and/or > 10% band cells
- Sepsis: SIRS criteria + suspected or confirmed underlying infection
- Severe sepsis: Sepsis + organ dysfunction (at least one organ or system)

LAB:
- ↑Lactate ⇒ Metabolic acidosis
- CBC, inflammatory lab → hemorrhage, sepsis?
- cultures (BEFORE AB tx)
- troponin → cardiac?
OTHER
- EKG + Echo→ cardiac? obstructive?
- FAST → hemorrhage?
- CT Brain, Abdomen → neurogenic? septic? 3rd space fluid loss (pancreas, obstruction)?
- Chest Xray → obstructive? cardiac? sepsis (pneumonia)?
- other exams depending on etiology
Parameter | Class I | Class II | Class III | Class IV |
Blood loss (mL) | Up to 750 | 750–1500 | 1500–2000 | > 2000 |
Blood loss (% blood volume) | Up to 15% | 15–30% | 30–40% | > 40% |
Pulse rate | < 100 | 100–120 | 120–140 | > 140 |
Blood pressure | Normal | Normal | Decreased | Decreased |
Pulse pressure (mm Hg) | Normal or increased | Decreased | Decreased | Decreased |
Respiratory rate | 14–20 | 20–30 | 30–40 | > 35 |
Urine output (mL/h) | > 30 | 20–30 | 5–15 | Negligible |
CNS/mental status | Slightly anxious | Mildly anxious | Anxious, confused | Confused, lethargic |
Fluid replacement | Crystalloid | Crystalloid | Crystalloid and blood | Crystalloid and blood |
Stage 1 (+2) ⇒ 🌊fluids
Stage (2+) 3 ⇒ 🌊fluids + 🩸blood
Stage 4 ⇒ 🌊fluid + 🩸blood + 🔪surgery (hemostasis)
Normal volume:
- adults: 7% of ideal body weight (approximately 5 I / kg for 70)
- children: 8% of ideal weight (approx. 80 mL / kg)
Q. 4th stage of hemorrhagic shock is defined by:
(A) Low systolic blood pressure
(B) Normal diastolic blood pressure
(C) Diuresis 5-15 ml/h
(D) Heart rate > 140 /min
(E) Heart rate <100 /min
AD
primary evaluation! (first ABCDE)
Type of shock | Treatment |
💦 Hypovolemic: | 1. 🌊Fluids
(i.v. location depending on injury or CV catheter)
2. 🩸 hemorrhage
-Blood transfusion
-Hemostatic control (emergency surgery🔪) |
❤️ Cardiogenic: | 1. ⚠️ check fluid responsiveness
(dry = output problem vs. wet = congestion problem)
2. Output maintenance (preload, afterload, contractility)
- 🏵️ Inotropes (Dobutamin, Milrinone)
-🔺 Vasopressors (NE)
-⚠️ Diuretics (only if sysBP >90)
3. Definite tx: PCTA, stents, thrombolysis
4. OTHERS
(oxygen, AB +electroly. correction, arrythmia correction, Mechanical assistant devices) |
🚧 Obstructive: | 1. 🌊 Fluids
2. 🪡 Relieving intervention
-Pericardiocentesis
-Thoracostomy
-Thrombolysis |
🔥 Septic shock: | 1. 🌊 Fluids
2. 🔺 Vasopressors (NE, vasopressin, ØE!)
3. 🧫 infection
-AB
-Infectious source control
4. OTHERS
(consider FFP or Platelets if DIC; steroid if adrenal dysfunction, ventilation in ARDS, sedation, analgesia, glycemic control, bicarb if acidosis, ulcer. + DVT prophylaxis) |
🤧 Anaphylactic: | Initial:
1. 🌊Fluids
2. 🫀 Epinephrine bolus (if refract. other vasopressor)
3. Stop the exposure + airway maintanance
LATER:
- 🐝 Anti-histamines, 🌝steroids, 🎺 bronchodilators
- 🔺vasopressor (NE, vasopressin) |
🧠 Neurogenic: | 1. 🌊 Fluid
2. 🔺 Vasopressors (NE, vasopressin)
3. 🥀 Atropine (for bradycardia) |
- ⬇️ Injury below the diaphragm:
- 1 above: At least 1 i.v. line should be placed in a tributary of the superior vena cava.
- ⬆️ Thoracoabdominal damage:
- 1 above: At least one i.v. access site should be above the diaphragm.
- 1 below: One access below the diaphragm.
→ Never i.v. access in injured limb

The content of Na Osmolarity pH The amount of water provided Glucose requirements (calories) Anticipated rate of administration
Ringer Lactate
- large quantities + prolonged
- lactic acidosis
- Ø in RF, high need of free water, in transfusion line + hyperK
Saline solution
- RF
- hyponatremia , hyper
- transfusion line
- !! → hyperchloremic acidosis + hypokalemia
emergency:
- unnoticed loss of fluids (i.e. hemorrage after fracture)
- ventilation problem
- wrong Dgx
- other type of shock
- Addison crisis + DKA
- Hypothermia

- 🧠mental status
- 🩸 perfusion
- Vitals (RR, HR, Resp-rate)
- Diuresis
- Periph perfusion: recap-time
- CVP
- Start primary evaluation - ABC(DE)
- Start Tx during primary evaluation
- Evalulate FLUID LOSS
- Figure out TYPE of shock
- Assess RESPONSE to Tx
↓
↓
↓
↓
- Vitals
- HR
- BP invasive → Ø good indicator of tissue perfusions
- CVC
- Pulmonary artery catheter
- SvO2 = mixed venous saturation
- Lactate (arterial)
- VO2 = O2 consumption
- DO2 = O2 delivery
- CO2 clearance
- SvO2 (Mixed Venous Saturation): It is a measure of the oxygen saturation of venous blood returning to the heart. It indicates the balance between oxygen delivery and consumption in the tissues.
- Lactate (Arterial): Lactate is a byproduct of anaerobic metabolism and is measured in arterial blood. Elevated levels of lactate can indicate tissue hypoxia or inadequate oxygen delivery.
- VO2 (O2 Consumption): VO2 represents the amount of oxygen consumed by the body per unit of time. It reflects the metabolic needs of the tissues and is an important parameter to monitor during anesthesia.
- DO2 (O2 Delivery): DO2 is a measure of the amount of oxygen delivered to the tissues per unit of time. It depends on cardiac output, hemoglobin concentration, and arterial oxygen content.
- CO2 Clearance: CO2 clearance refers to the removal of carbon dioxide from the body. It is an important parameter to monitor during anesthesia as elevated levels of CO2 can indicate inadequate ventilation.
💥 Trauma
25x
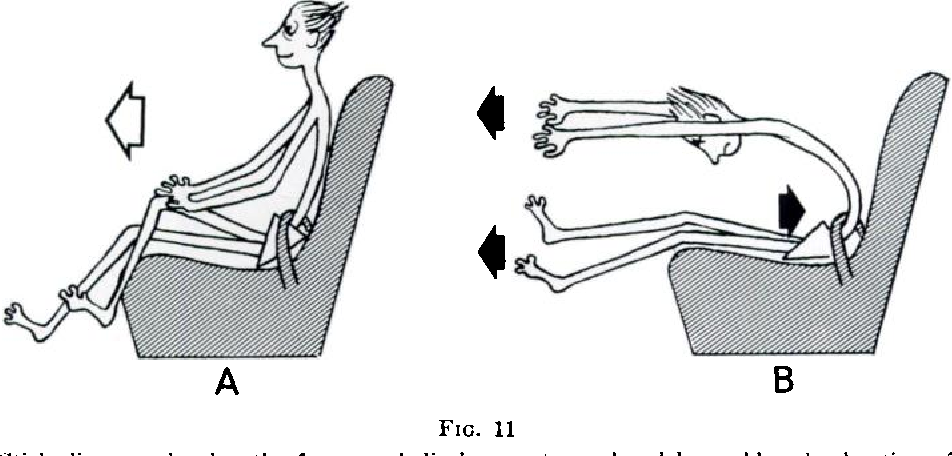
- Injuries that result after the second impact (body hits the ground outside the car) ⇒ even more severe than the initial impact
- Distance between the victim and the vehicle ⇒ indicates how fast the car was going & how much energy was absorbed by the victim
- 1 out of 13 ejected victims: spinal injuries
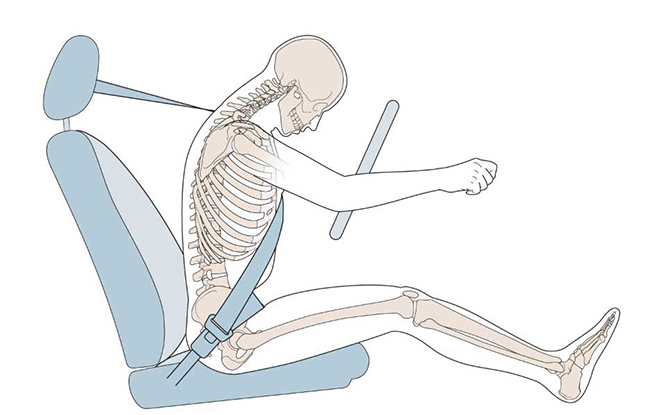
- SEAT BELT injury
- lumbar spine compression fractures
- Compression injuries of abdominal organs
- Rupture of diaphragm
- MOTORCYCLE → head ☠️, spinal, extremity📷 trauma
If too high:
lap belt's worn alone → Severe trauma to the head, face, and neck since (Ø shoulder strap to stop the forward momentum of upper body)
If the shoulder belt is worn alone→ Severe C-spine injuries, Decapitation
- location
- lenght of blade
- angle of penetration
stab wounds that entered upper abdomen may have reached organs in thoracic cavity
Stab wounds below the 4th intercostal space may affect abdominal organs (highest level of the diaphragm).
- Vehicle damage
- Fall greater than 15 feet
- Auto vs. Pedestrian
- Ejected from a vehicle
- Survivor of a fatal accident
- Penetrating chest, abdominal, or upper extremity trauma; Knife wound or other sharp object
↓
SELF-PROTECTION ensured?
↓
UNCONCIOUS? (verbal + tactile stimulation)
→ yes → OPEN airway → BREATHING? → no ⇒ CPR-Algorithm; yes ⇒ lateral decubitus
↓
no, concious
↓
cABCDE Assessment

- ⤵️ OPEN Airway
- without device (subluxation/hyperextension)
- tubus, cricotomy
- 🪀 Remove FOREIGN BODY
- 👀 Inspection
- Assymmetric movement?
- Trachea deviation
- 🩺Auscultation, percussion (pneuo, hemothorax, stridor etc.)
- 💨 SpO2
- ⏱️ RR
- bleeding? ⇒ only treat PROFUSE bleeding during primary evaluation
- Assess perfusion
- Pulse (central + periph)
- BP
- Recap
- skin color, temp, hydration
- Assess preload:
- Jugular vein
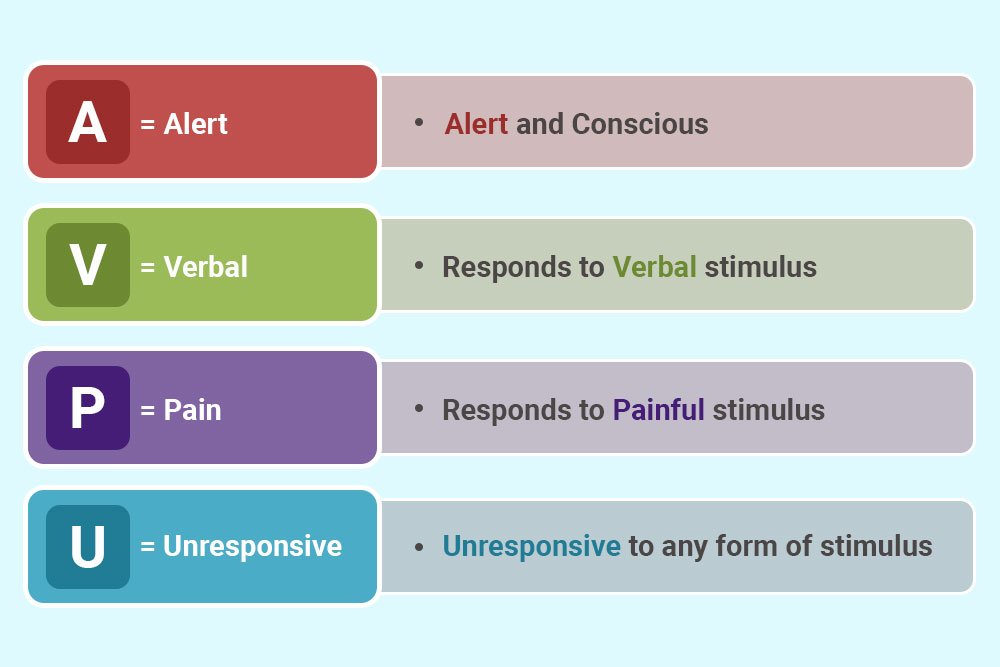
- Status: GCS + AVPU
- Neuro exam :
- Pupil? (small/big, anisocoric?)
- FND?
- head injury?
- Glycemia?
- back in axis
- Hypothermia? → ext+int. warming
- Wet?
- Toxic environment?
- Medications?
- exposure: rash, edema, petechia
→ unstable → fluids + CPR
↓
stable
↓
SECONDARY ASSESSMENT

- Periorbital ecchymosis (raccoon eyes)
- Retroauricular ecchymosis (Battle sign)
- Otorrhagia / Otorhinolaryngology
- SCALP ONLY → COMPRESSION sterile compress + bandage 📷
- FRACTURE (bone can be seen)→ ØCOMPRESSION!

- DIRECT COMPRESSION
- ARTERY (prox.) COMPRESSION
- Tourniquet ⇒ release every 20MIN
→ controlled? → fixate with gauze
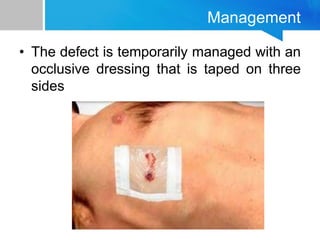
Apply a non-porous occlusive dressing over the wound (such as plastic, or foil from space blanket) and tape it down on 3 sides.
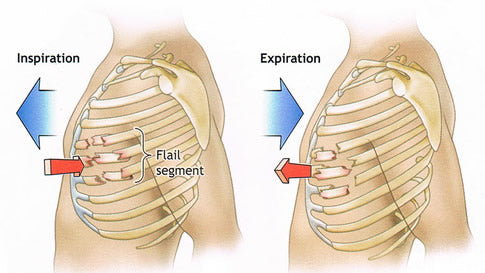
Flail Chest: 📷
- Disruption of bone continuity in at least 2 adjacent ribs in at least 2 places
- Clinic: Paradoxical movement (during breathing, the rib cage moves in reverse to the rest of the rib cage)
- Treatment:
- Oxygen
- Analgesia
- Leucoplast wide: like a hashtag "#"

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- immobilize


- Foreign bodies in the body should NOT be removed
- To minimize movement during transport, secure the foreign body with several rolls of gauze wrapped around it ⇒ # gauze
- If a foreign body is penetrating a limb, consider potential bone injury. After fixing the object, immobilize the entire limb with a splint.
{kind=link}
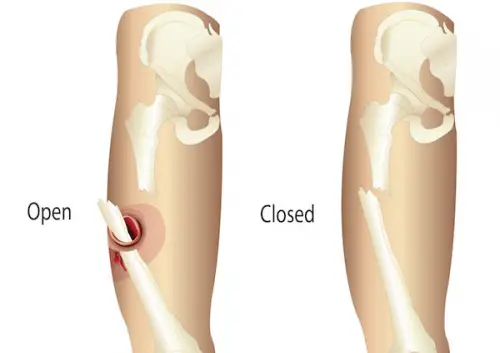
- OPEN fx
- CLOSED fx
- bone crackles
- disruption of continuity
- abnormal mobility
- Øforce transmission
⇒ put in AXIS + SPLINT
- Ø pressure → sterile compresses
- control hemorrhage → prox. artery pressure
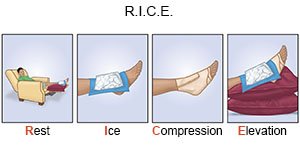
- position in axis + immobilize
- Control hemorrhage by applying pressure on proximal vasculature
- Administer analgesia
- Properly position the patient in the anatomical axis
- Cover the fractured bone with sterile compresses
- Perform PMS assessment (evaluate distal pulse palpation, motor function, and sensory function)
- Apply a vacuum splint to immobilize the limb
- Consider volume resuscitation if hypotension occurs due to fractures of large bones (e.g., femur, humerus)


{kind=link}
- remove object from pocket
- PULSE → PELVIC BINDER → PULSE

- Øpressure → cover with sterile moist (saline) compresses
- Put head in front (↓pressure)
- BGA
- EKG
- Urinary catheter (output)
- (e)FAST Ultrasound
↓
- 💥 headache?
- pupil
- conjunctiva
- pain, photophobia, blurred vision?
- flaring?
- rhinorrhea?
- cyanotic?
- salivation / drooling?
- smell of breath
- sore troat?
- 🎶 stridor?
- 🧵 ”pulling” neck muscles?
- ↑ BREATHING WORK ⇒ retractions, ↑RR?
- Central cyanosis 📷

LOOK FOR:
- Stridor
- Wheezing, rhonchi, rales
- Decreased breath sounds
- Central cyanosis
- Burning in the chest or chest pain
- Chest pain?
- HR + Rhythm?
- Assess perfusion
- Pulse
- Recap
- skin color, temp, hydration
- BP
- painful?
- distended?
- tense + rigid?
- vomiting / diarrhea?
- urinary/fecal incontinence?
- instability → pelvic binder
- mental status?
- Syncope? Sudden collapse?
- Dizziness?
- seizure?
- Muscle twitching?
- sensory function?
skin = painful, burning numb or tingly?
- skin lesions? (erythema - allergy?, vescles, bullae, necrosis)
- always immobilze one joint above + one joint below
- apply traction
- check PMS after

US, CT, XRay
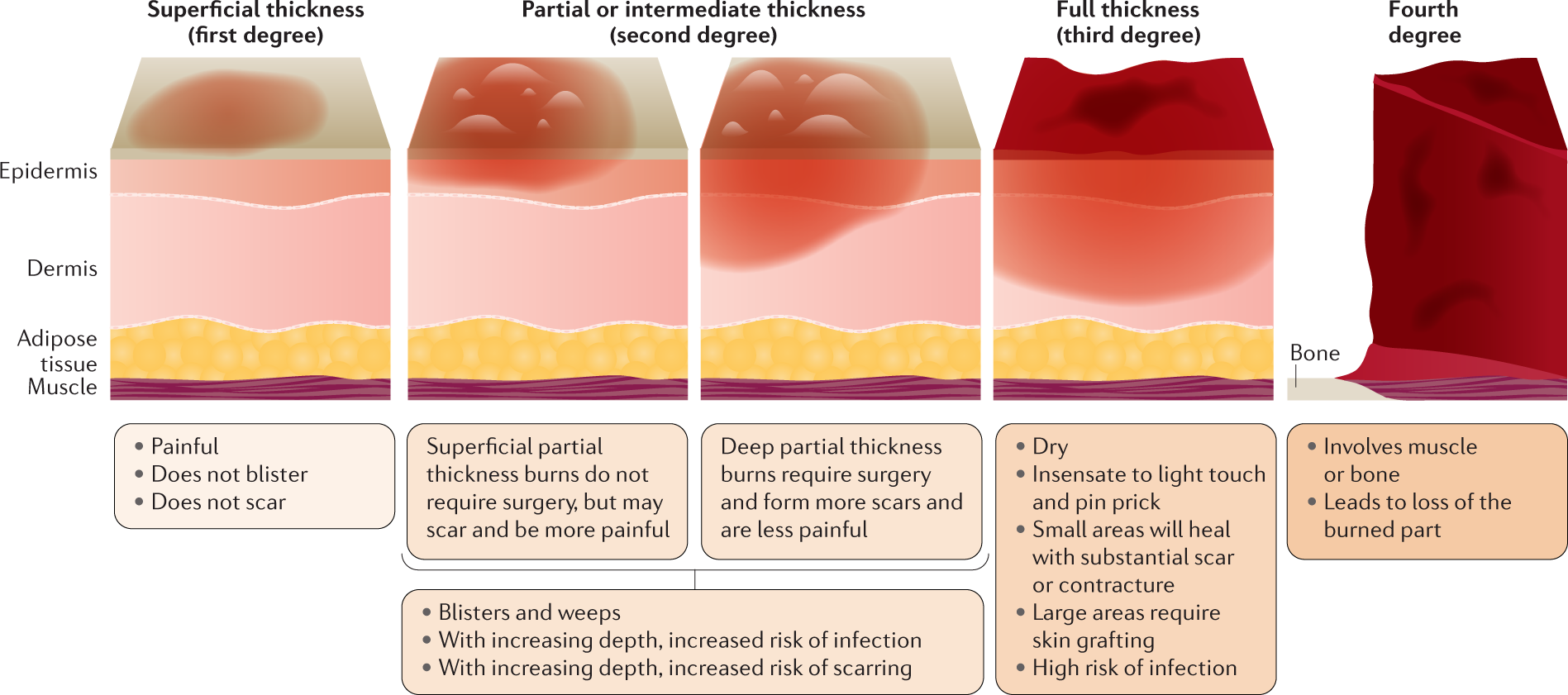
🔥 Burns
- EXTERNAL:
- 💪skin burns
- 🫁 airway burns
- INTERNAL:
- face, mouth, neck burns
- Ø facial + nasal HAIR
- COAL on lips, nose, pharynx
- BLACK SPUTUM
- Abnormal RESPIRATORY SOUND (wheezing, rale, stridor)
- progresive encephalopathy → death
- memory + personality changes
- edema
- infarct
- hypovolemic shock
- septic shock
🧠 CEREBRAL DYSFUNCTION

- Loss of capillary barrier in 🔥burns> 25% BSA (body surface area) → Local loss of capillary barrier appears around small burns
- Shock lasts 18-48 hours and then resolves spontaneously
- Probably caused by vasoactive mediators
depth and the surface area involved
{kind=link}
GRADE | LAYER | HEALING |
1 | EPIDERMIS outer layer | spont |
2 | EPIDERMIS complete (part of upper dermis) | spont |
3 | DERMIS partially
| healing if restoration sweat gland + hair follicle cells |
4 | DERMIS complete
(+- beyond) | >4cm→ Graft required |

{kind=link}
- 🔰 SELF-PROTECTION
- 🛡️ VICTIM PROTECTION
- ABCDE
(+breathing mask if possible)
(stop gas/current, remove from heat / explosive environment, fire extinguisher)

↓
- cABCDE
- remove CLOTHING 👕
- WATER on burned area 💦 (!!not until complete physical exam)
- ensure VENTILATION of AREA ♻️
- IMMOBILIZE + organize TRANSPORT
- CLASSIFICATION: DEPTH + SURFACE AREA
- determine body WEIGHT ⚖️
↓
- COLD WATER ⇒ RULE OF 10
- Apply cold water at 10°C for 10 minutes
- Maintain a distance of 10 cm
- Apply at an angle of 10°

- STERILE COMPRESSES
PARKLAND FORMULA:
cristalloids - RINGERS:
4ml x KG x %surface area
⇒ 1/2 in first 8h
⇒ 1/2 in the following 16h
ex. 70kg, 50% → 4x70x50 = 14.000ml → 7k in the first 8h, 7k in the following 16
opioids
⇒ ↓ catabolism & vascular stress
- ventilatory support if necessary
{kind=link}
- urinary output
- conciousness
- vitals
- CK (if compartment)
🧪 Intoxication
- BASIC MEASURES
- ABC(DE)
- O2
- i.v. access
- EKG → control arrhythmia
- Seizure? → benzos
- body cooling 🧊
- if exposure is clear → give antidote (…more details later)
↓

- ↓🧠 - coma
- ↓🫁 - Respiratory depression
- 🪡👁️ SMAAAALL pupils
- ❄️ Cocaine, Amphetamines, Ephedrine
- 🔋 Theophyllin
- 🎺 Salbutamol
- ↑🧠 Agitated
- 👁️ BIIIG Pupils
- 🥵 ↑temp
- ❤️ ↑HR + ↑BP

- salivation + lacrimation
- urination + defecation
- gastric cramping
- emesis
- (small pupils)
- PARASYMPT → ❤️ + 🫁 (bradycardia+ bronchospasm)

- 🛵 TCA
- 🐝 Anti-histamines
- 🌷 Belladonna → Atropine
- ↑🧠 delirium
- 👁️ BIIIG Pupils
- 🥵 flushed + hot skin
- 👄 dry mouth (+ other mucous membranes)
- PLUS ❤️ ↑HR
- Benzos
- Barbiturates
{kind=link}
- 🧠 confusion, coma
- 🫁 respiratory depression
- ❤️ ↓BP
- 🥶 ↓ temperature
- pupils variable
{kind=link}
- 👁️ BIG pupils
- 💩 diarrhea + cramps
- ❤️ tachycardia + piloerection
- alcohol: seizure
- insomnia
- etc.
- 7 main tox syndromes
- PUPILS
- DILATED → sympathomietic or anti-cholinergic or WITHDRAWAL or benzos
- CONSTRICTED → opioids, cholinergic or benzos
- OTHER sympathetics + parasympathetic signs?
- 💊INGESTION → type, amount, time
- 👏🏽 AT THE SCENE: symptoms?, pills?
- ❓ACCIDENTAL vs. INTENTIONAL?
- 📑 PMH (incl. psychiatric)
- 🖖🏼 VITALS (incl. rectal temp.)
- ❤️🫁 - edema, pneumonitis, bronchosapsm?
- 🧠 - ↑/↓?, Pupils?
- 💪 - color, moister, lesions, needle tracks
- 👄 oral muscosa burn?, breath smell
↓
{kind=link}
↓
→ irrigate eye + skin
- induce vomiting (Ipecac)
- gastric lavage (Øeffective >1h after ingestion)
- always indicated
⇒ DOES Ø WORK for:
- 🍺 alcohol
- 🍾 pesticides
- acid + alkalic subst.
- metals
The reduction of toxic absorption, as a principle of management in intoxications, carried out by: A. Administration of active charcoal B. No food intake for the next 6 hours C. Repeated fluid bolus administration D. Administration of antisecretory iv E. Gastric lavage in the first hour after toxic ingestion
- Ion trapping → salicilates
- Hemodialysis → methanol, ethylene glycole, salicilate, lithium
- Hemoperfusion (dialysis + charcoal filter) → phenobarbital, theophyllin
- Multidose Charcoal (every 4h) → phenobbarbital, theophyllin
to work: drug must have small volume distribution, minimum protein binding, low molecular weight (less than 500 daltons)
Ø limited by protein binding or molecular weight
To increase toxic elimination, hemoperfusion is indicated in the intoxication with: A. Paracetamol B. Diazepam C. Strychnine D. Tramadol E. Theophylline
Anti-dotes for..
naloxon 👕
- alpha blocker/ non selective BB (I.e. labetalol)
- benzos
- morphine

Atropine 🌺
Physo-STIGMIN
Flumazenil 🐩
o2 + hyperbaric chamber
n-acetylcystein
glucagon
hydroxycobalamin (Vit B12)
↓
To be discharged, patients must meet the following criteria:
- Medical-based on toxin:
- Normal vital signs and mental status after observation period
- No threat of delayed deterioration
- Psychosocial:
- No suicide risk
- Released to a competent adult
- In children and elderly, no concern for abuse or neglect