

- Dermatology
- ⛲ Basics of Dermatology
- 🥫Acne & Rosacea
- 🦠 Skin Infections
- ❄️ Papulo-Squamous lesions
- ☄️ Dermatitis / Eczema
- 🛡️ Auto-Immune Dermatosis
- 🐝 Hypersensitivity reactions
- 💇🏽♀️ Alopecia & 🐄 Pigmentation disorders
- 🧬 Genetic disorders
- 🦀 Tumors
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Dermatology
⛲ Basics of Dermatology


LESION | CHARACTERISTICS | DIAMETER |
FLAT | ||
🫓 Macule | flat (Øpalpable)
other color than surroundings | <1cm |
🩹 Patch | flat (Øpalpable)
other color than surroundings | >1cm |
PALPABLE / ELEVATED | ||
⚾ Papule | palpable | <1cm |
🏀 Nodule | palpable (elavated) | >1cm
(diameter AND depth) |
🥿 Plaque | palpable (+- elevated) | >1cm |
BLISTER | ||
🐡 Vesicle | blister
(fluid-containing) | ≤ 0.5 cm |
🐂 Bulla | blister
(fluid-containing) | > 0.5 cm |
OTHERS | ||
🎡 Wheal | papule or plaque
pruritic + red
TRANSIENT | |
🐠 Pustule | vesicle with pus |
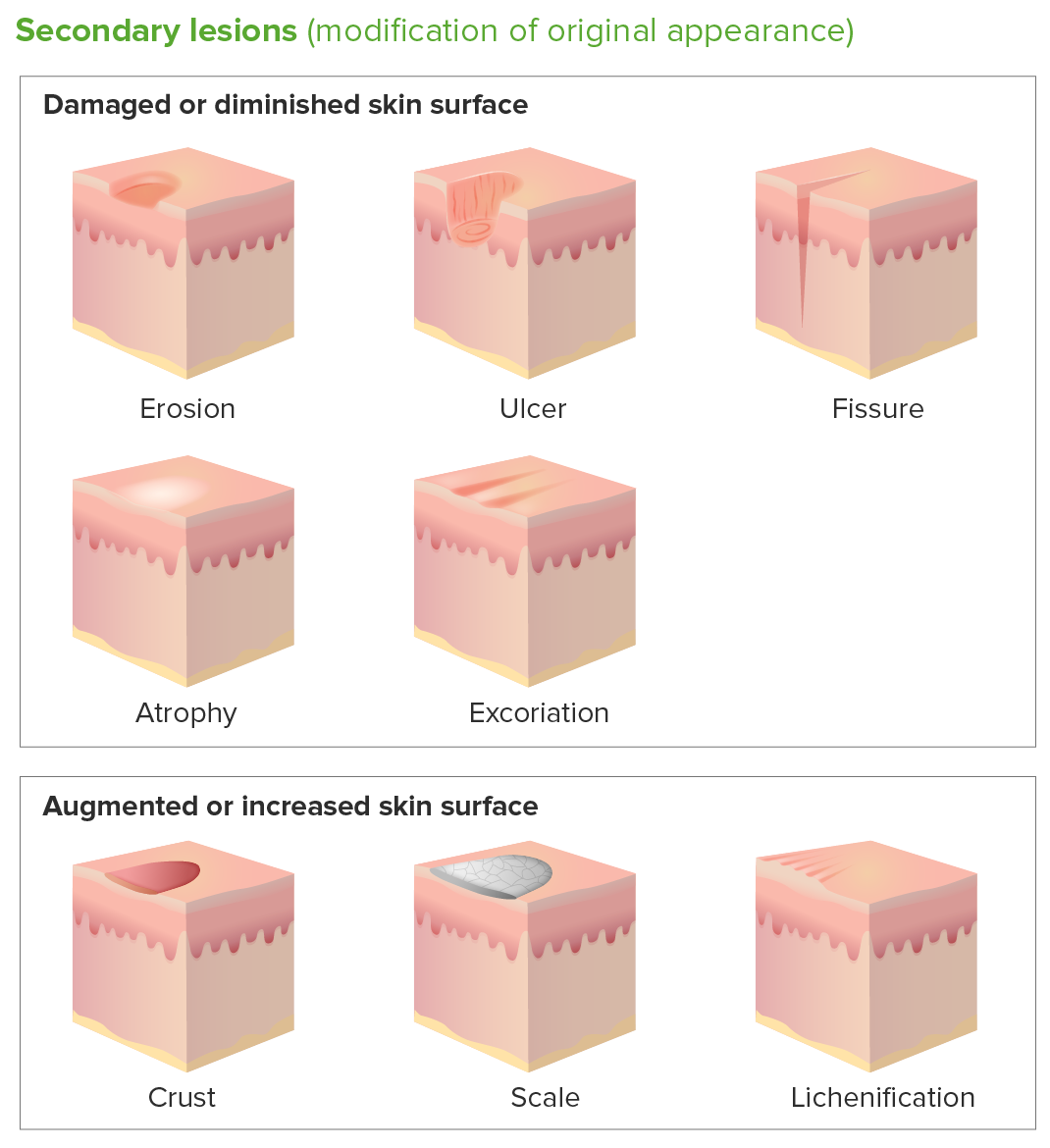
LESION | CHARACTERISTICS | LAYERS |
❄️ Scale | flaky white scales | thickend stratum corneum |
🍯 Crust | yellow/brown
= dried exudate (pus,blood) | |
Fissure | linear crack | epidermis → dermis |
Excoriation
(scratch mark) | abrasion due to mechanical force | epidermis (+/- dermis) |
Ulcer | round/irregular deep lesion | epidermis → dermis (scar) |
Erosion | epidermis (Øscar) | |
Necrosis | black, yellowish/brown | |
Skin atrophy | Thinning of skin
Øinflammation | |
Scar | new connective tissue
(if overgrowth beyond borders of scar = keloid) |
🩸 Hemorrhage | ||||
Hematoma 📷 | Bleeding into (subcut. tissue, muscle, organ tissue, cavity) | |||
Purpura
(subtype of hematoma, non-blanching 📷) | Non-palpable purpura | Petechia 📷 | flat, red-purple
<3mm ( pinpoint) | |
Echymosis 📷 | flat, red-purple
>5mm | |||
Palpable purpura 📷 | raised, red-purple | |||
🥵 Rashes | ||||
Exanthem 📷 | extend + uniform
(local or general) | |||
Enanthem 📷 | mucous membranes only | |||
Erythema 📷 | red due to vasodilation
BLANCHING | |||
Erythroderma 📷 | generalized reddening | |||
Maculopapular rash 📷 | rash with palpable + non-palpable lesion <1cm | |||
Others | ||||
non-contagious dermatitis
+ PRURITIS, erythema + papule | ||||
thickening of skin
accentuated skin markings |
*non-blanching = does Ø blanch after pressure-application 📷

POTENCY
Potency | Agent |
Super high | Clobetasol propionate (Dermovate) |
High | Fluocinonide |
Medium | Triamcinolone |
Low | Hydrocortisone
Fluocinolone acetonide
Desonide |
Agent | Hydrocortisone | Triamcinolone | Clobetasol |
Potency | Low | Medium | High |
Indication | For mild and chronic dermatoses and for use on the face & intertriginous areas | For intermediate severity dermatoses
(Øface; Øintertriginous) | For more severe dermatoses
(Øface; Øintertriginous) |
- Super high potency (class I) used for severe dermatoses in nonfacial and nonintertriginous areas such as scalp, palms, soles, and thick plaques on extensor surfaces.
- Medium to high potency steroids (classes II-V) appropriate for mild to moderate dermatoses in nonfacial and nonintertriginous areas, and can be used on flexural surfaces for limited periods.
- Low potency steroids (classes VI, VII) can be used for large areas and on thinner skin, including the face, eyelids, genital area, and intertriginous areas.

- Super high potency: treat for less than 3 weeks
- High and medium potency: treat for less than 6-8 weeks
- Low potency: treat facial, intertriginous, and genital dermatoses for 1-2 week intervals to avoid side effects like skin atrophy, telangiectasia, and steroid-induced acne
- Stop tx when skin condition resolves (to avoid rebound/flares) → if necessary, taper with gradual reduction of potency and dosing frequency
1) Depends on Size of Lesion ⇒ Estimate BSA (body surface area)
2)Give Dose according to finger tip unit (FTU) 📷
1 FTU = 2% BSA = 500mg topical steroid
2 FTU = 4%BSA = 1g
..for each dose
e.g., you treat an area of skin the size of 8 adult hands. You will need 4 FTUs for each dose. (This is 2 g per dose. If the dose is once a day, then a 30 g tube should last for about 15 days of treatment).
🥫Acne & Rosacea
Puberty → ↑ 💪🏽 Androgen
↓
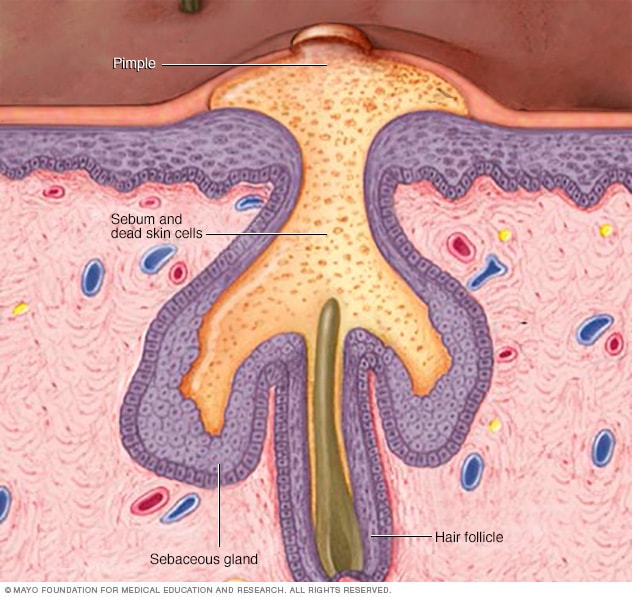
→ Sebaceous glands enlarge → ↑ 🌽 Sebum
→ Keratinocytes (around hair shaft) produce → 🥥 ↑Keratin
⇒ 🚧 Blocks ducts ⇒ 🟡 Comedones 📷


↓
⇒ 🧫 Bacterial growth (Sebum = growth medium)⇒ Propionibacterium (=cutibacterium) acnes + Staphylococcus epidermidis
Propionibacterium acnes:

Steph epidermidis:

↓
⇒ 🔥 Inflammation of comedones 📷
- 👐🏽 Open comedos = ⚫ blackheads
- 🚪 Closed comedos (by skin) = ⚪ whiteheads
- 🔥 Inflammatory lesions = 🔴 papules / pustules / nodule / abscess / cyst
COMEDONAL ACNE 📷


PAPULO-PUSTULAR ACNE 📷







ACNE EXCORIEE: 📷


TYPE | LESION | COMMON LOCATION | SCARRING | SPECIAL |
🟡 COMEDONAL acne | 🟡 COMEDONES
(rarely inflamm.) | 👴🏽 FACE | onset: early in puberty | |
🔴 PAPULOPUSTULAR acne | 🔥 INFLAMMATORY
→ PAPULES/PUSTUL.
+/- NODULES
(+/- comedones) | 👴🏽 FACE
🧰 CHEST
🗼 BACK | +/- | |
🟢 Acne CONGLOBATA | 🔥 INFLAMMATORY
→ PAPULES/PUSTUL.
→ NODULES
→ ABSCESS
(+/- comedones) | 👴🏽 FACE
🧰 CHEST
🗼 BACK | ☑️ YES
(atrophic+keloidal) | 💥 PAINFUL lesions
🕰️ CHRONIC course
M>F |
🩸 Acne FULMINANS | 🔥 INFLAMMATORY
SUDDEN onset:
→ CONFLUENT ABSCESSES
⇒ 🩸 HEMORRHAGIC NECROSIS | 👴🏽 FACE
🧣 NECK
🗼 BACK | (☑️ yes) | - 💥 PAINFUL LESIONS
- ♻️ SYSTEMIC SIGNS
→ 🤒 fever
→ 👾 ↑Leukos
→ 🦴 joint pain+swelling |
👉🏽 Acne EXCORIEE | 🕳️ EXCORIATION/ ULCER
(w/ hemorrh. crust) | 👴🏽 FACE
🧰 CHEST | ☑️ YES
(+pigment. chan.) | cause: 👉🏽 SQUEEZING/
SCRATCHING “away”
F>M |
💊 DRUG-INDUCED acne | 🔥 INFLAMMATORY
(might → acne fulminans) | +/- | causing agents:
- 🌝 steroids
- ⚡ phenytoin
- 🏂🏽 Lithium
- 🫁 Isoniazid (anti-TB)
- 💡 halogenated drugs
(sedatives, asthma-drugs)
- 🅱️ Vit B (↑dose)
- 🧪 chemo
|
✅ - Healing
🪢 - Scarring (atrophic or keloidal scars)
🐄 - ↑Pigmentation
TOPICAL TX
- 👁️ Retinoids (Vit A deriv.) ⇒ Isotretinoin (Accutane) → ↓ keratin production
⇒ CAVE: 🕷️ TERATOGENIC

→ SE: irritation → 👹 erythema, burning, scaling


- 🧫 AB ⇒ Clinda, Erythro → ↓colonization → Do Ø combine with syst. AB!
- ⭐🛢️ Benzoyl peroxide (topical) → comedolytic + bactericidal
- 🕶️ Azelaic Acid → comedolytic + anti-inflamm.
- 🧢 Salicylic Acid → keratolytic


SYSTEMIC TX
- 👁️ Isotretinoin
- 🧫 AB ⇒ Minocycline [tetracycline] (alternative: Doxy → but ↑SE)
- 💊 Oral contraceptives

→ SE: 👄 cheilitis, 👀 dry eyes, 👃🏽 dry nose xerosis, 🧈↑ triglycerides + cholesterol.
PATHO = complex + poorly understood
leads to ⇒ 🔥 INFLAMMATION OF THE SKIN (dermatitis)
→following factors are assoc.:

- 😳 FACIAL FLUSHING 📷 (transitory erythema)←🍷 ENVIRONMENTAL TRIGGER (i.e. ALCOHOL, SUN, temp)
- GRADE 1: Rosacea Erythematosa 📷 👃🏽 CHRONIC REDNESS (nose + cheeks) +/- TELEANGIECTASIS
- GRADE 2: (Rosacea Papulopustulosa)📷 🔴 PAPULES & 🟡 PUSTULES (due to Demodex folliculorum)
- 👃🏽 PHYMATOUS ROSACEA 📷


→ Chronic inflammation → Skin(sebaceous) hypertrophy + fibrosis → mainly involving 👃🏽 = Rhino-phyma:
- Celtics and Northern Europeans: greatest risk
- Affects light-skinned individuals
- Avoid:
- 🍷 trigger (sun, alcohol,..)
- 🥴 topical use of irritating cleansing agents, topical alcoholic solutions, topical corticosteroids.
- 🔦 LASER THERAPY
TOPICAL
- 🧫 AB ⇒ Minocycline
- 🕶️ Azelaic Acid→ comedolytic + anti-inflamm.
- Demodex folliculorum? → 🌲 Ivermectine = Anti-parasitic
SYSTEMIC
- 👁️ Isoretinoin
- 🧫 AB ⇒ Minocycline, Metronidazole
- 🚁 H.Pylori-Tx
🦠 Skin Infections

Layer | Etiology + Pathology | Signs + Symptoms | Location | TYPICAL patient | Specials | |
Impetigo contagiosa 📷 | Epidermis
(below S. corneum) | S.Aureus or GAS
→Neutrophils beneath S. corneum | Macule → vesicles → rupture
⇒ “honey-colored” crust (dried sebum) | Face + extremities | child | ↑↑ contagious
DDx: Herpes Simplex |
Bullous Impetigo 📷 | Epidermis
(S. Granulosum) | S.Aureus
→ Exfoliative Toxin (cleaved desmoglein 1 complex) desmosome damage
→ keratinocyte de-attachment → fluid in space | Bulla / blister (Nikolsky +) on erythem. base
clear → cloudy → pus → rupture
→ crust
↑LN | Face, neck, hands
Trunk involved | child | Øscar
|
Scalded skin synd. (SSSS) 📷 | Epidermis | S. Aureus
→ DIFFUSE exfoliative toxin | Infectious signs: Fever + Diffuse Erythema
large Bulla (Nikolsky +) → rupture
→ Sloughing/peeling of skin
| diffuse
| newborn or child
(3-7d post-natal) | Øscar
(Øinvolvement of dermis or basal layer of epidermis)
**in contrast to Staphyloccal toxic shock syndrome (SSSS vs. STSS)
DDx SJS |
Erysipel 📷 | Dermis - SUPERFICIAL
(+superfic. lymphatic) | GAS
Skin break/trauma → bacterial entry
or endogenous (sinusitis, pharyngitis,etc) → facial erysipel | FAST onset
↑LOCAL SIGNS → painful, warm, red
Rash ⇒ clear DEMARCATION + elevated borders + spread over time
↑↑ SYSTEMIC SIGNS | LEG (unilat. after fall)
or FACE 😊 | child or older adults | Variants: bullosum + gangrenosum + chronic recurr.
DDx: cellulitis, compartment sy, hypodermitis |
Cellulitis 📷 | Dermis - DEEP
+- subcut. fat | S.Aureus or GAS
Skin break/trauma → bacterial entry | SLOWER onset
↑LOCAL SIGNS → painful, warm, red
Rash ⇒ ILL-DEFINED + spread over time + Øelevated borders
SYSTEMIC (uncommon, less than erysipel) → ↑LN | LEG (unilat) | middle-age + eldery (↓immunity) | ⇒ Complication: Thrombophlebitis, Elephantiasis (if recurr), deeper extension
⇒ Systemic: Staph Aureus / GAS complications |
Dermis or Subtaneous | S.Aureus
→ pus collection (Np+bact)
→ may complicate cellulitis/erysipel | 💥 red + painful nodule w/ central yellow plug
tense + raised skin
🔥 fever + ↑LN
⇒ central plug DRAINS SPONT. ⇒ SCAR
| - multiple = FURUNCULOSIS ⇒
→ Permissive factors for FURUNCULOSIS → ↓immunity (atopic dermatitis, Diabet, HIV,..)
- ↑risk: sepsis, cavern. sinus thromb., endocarditis | |||
Necrotizing Fasciitis 📷 | Fascia
(+subc. fat) | Anaerobes (Clostridium..) → after surgery in immunocompromised
GAS (or S.Aureus)→ after skin injury in otherwise healthy
→ Necrosis of tissue above fascia | 1) rash → color changes: red → purple/blue → black
+-bulla
2) pain + tenderness ⇒ out of proportion to rash
3) Crepitus when pressed (bact. gases)
(fever + local infectious signs)
4) Hypo-esthesia | ↓immunity . post-surgery
or
after skin injury | ⇒ IMAGING! (+muscle enzyms, renal)
quick, uncontrolled spread along fascia ⇒ SEPTIC SHOCK
pain eventually stops when nerves are destroyed
|
furuncle: abscess due to folliculitis
carbuncle → multiple follicles infected ⇒ multiple pustules on inflamed plaque
Disease | Tx |
Impetigo contagiosa | Topical AB (i.e. fucidic acid)
Systemic oral AB (amoxi-clav, erythro, clinda, doxy, tmp-smx) |
Bullous Impetigo | Topical AB (fucidic acid)
Systemic oral AB (amoxi-clav) |
Scalded skin synd. | Systemic oral AB (Vanco) |
Erysipel | Systemic oral AB
- penicillin G, or other betalac (cefalexin, amoxi, erythro)
- + clinda
→ 1-2w (duration) |
Cellulitis | systemic oral AB
- cephalexin, amoxi-clav, Oxa/Nafcillin if S.Aureus
- + clinda |
Abscess (Furuncle / Carbuncle) | topical anti-septic/AB
systemic oral AB (Clinda, doxy, TMP-SMX)
incision + drainage required |
Necrotizing Fasciitis | 🚑 !
- syst. i.v. AB (Penicillin+Clinda)
→ urgent surgical debridement
(if mixed (anaerob+aerob) = Pip/Taz+Vanco or Cefotax + Clinda) |

folliculitis (superficial)
→ pustules (yellow papules) where you can find body-hair w/ periph. erythema
→ caused by S. Aureus
+/- crusts

Erythrasma
→ due to Diphteroids or Porphyrines
→ in SKIN FOLDS

groin, axilla, gluteal cleft, intramammary folds & umbilicus
⇒ 🟤 red/brown MACULES → coalescent → PATCHES with SHARP BORDER 〰️
⇒ smooth surface or fine scales
⇒ +- pruritus
⇒ Dgx: 🪵 💡Wood-light exam → coral-red fluorescence 📷
⇒ Tx: 🧫 Local AB (imidazole) + systemic Ab (erythro, clinda)
- Early syphilis
- Primary syphilis
- Secondary syphilis
- Latency phase
- Late syphilis
- Tertiary syphilis
- Neurosyphilis
- Congenital syphilis

CLINIC:


Gumma 📷
Other:
- Tuberous syphilids (Tubero-serpinginous 📷 and tubero-ulcero-serpinginous 📷)
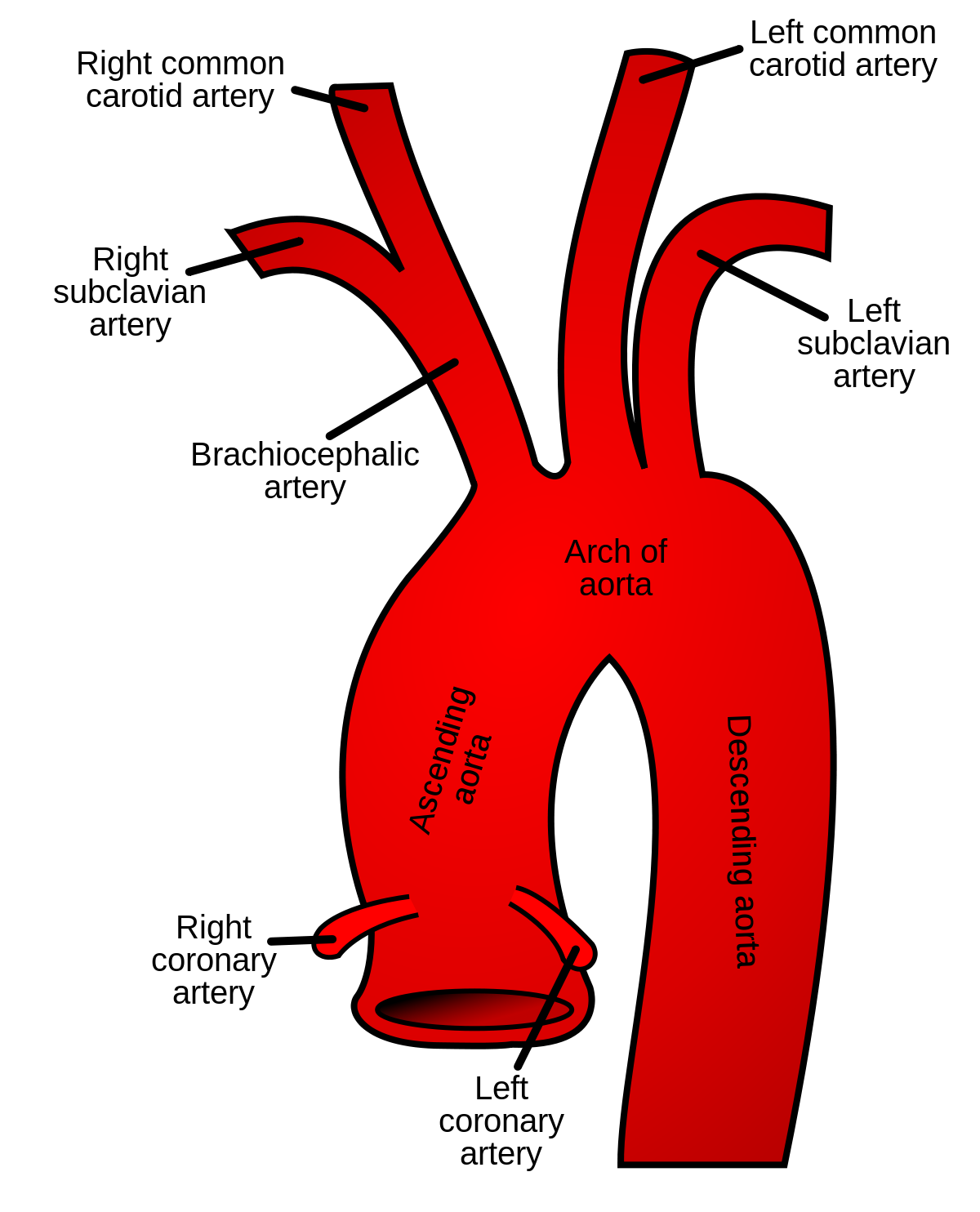
- Cardiac
- Aortitis
tubero-serpiginous: -red, brows -flat-topped red papules -progress periph. -heal centrally with atopy + pigm. changes
tubero-ulcero-serpinginous
- same as tubero-serpiginous +ULCER

- Focal Gumma
- Meningo-vasc. Syphilis
- General paresis
- Argyll-Robertson pupil
- Deafness
- Tabes dorsalis

early: <2 yo
late: >2 yo

- FLUORESCENT microscopy
- DARK FIELD microscopy
- 🫀 NON-TREPONEMAL SEROLOGIC TEST (non-specific ⇒ cardiolipin reaction)
- VDRL
- RPR
- Treponema cannot be grown
- Tests for serum reaction to cardiolipin antigen
- Presence of syphilis antibodies leads to reaction
- May get false positive results due to conditions like lupus or viral infections
- Venereal Disease Research Laboratory (VDRL) test
- Rapid Plasma Reagin (RPR) test
- Results are either given as a specific measurement or simply reactive/non-reactive
- Continues until birth
- 🪱 TREPONEMAL SEROLOGIC TEST (specific)
- FTA-ABS (IgM + IgG)
- TP-EIA
- Identifies antibodies against particular treponemal agents
- Precise examination
- Fluorescent Treponemal Antibody Absorption (FTA-ABS)
- T. pallidum Enzyme Immunoassay (TP-EIA)
- Outcomes: “Active” or “Inactive”
- Most efficient during initial stage of the disease.
Non-Treponemal Serologic Tests
Treponemal Serologic Tests
Neurosyphilis? → Lumbar puncture ⇒ VDRL
LATENT syphilis → Treponemal serologic test +
- Signs: clinic + radiological
- 🩸 IgM ⇒ VDRL infant > mother
- 💉 CSF → VDRL
Penicillin G benzathine - 💪🏽I.M. (2,4 Mill. IU )
→ 1x / week for 2-3w
- Early syphilis→ day 1 + 8 (2 doses)
- Late syphilis → day 1, 8 + 15 (3 doses)










Clinic, DDx, Tx, Complications?
- clear VESICLES (👄 mouth + face) on erythematous base 📷
- ↑LN (painful)
⇒”Zoster-like” evolution: PRODROME (burning, pain, tingling) → after 24-48h: vesicles → rupture + CRUST
⇒ duration = 1w & Øscarring
→ other body-parts when contact 📷

DDx:
Herpes zoster, hand-foot-mouth disease, aphte
Tx:
👉🏽 TOPICAL acyclovir
Complications:
- SPREAD → 🧠 + dissemination





Shingles:
Dermatomal pattern: Symptoms often affect dermatomes from Th3 to L3.
- Pain: Dull, pulling, sometimes intense pain in the affected ganglion area.
- Paresthesia
- Vesicles
- Skin lesions are pinhead to rice-sized, clear blisters
- Vesicles are on an erythematous base.
♻️ SYSTEMIC acyclovir (or others)


TYPICAL EVOLUTION:
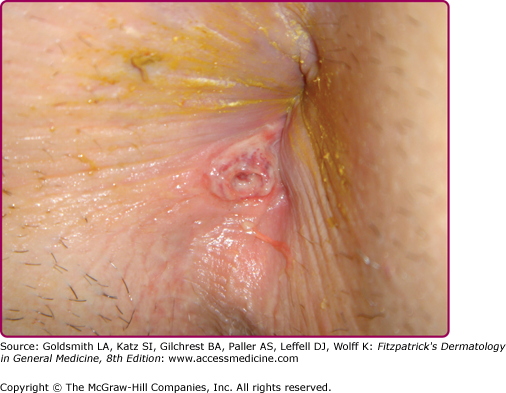
initial small red papule → new lesions: Cauliflower-like (vegetations with irreg. surface + border) → become ERODED + FOUL-smelling ⇒ +/- 🦀 malignant change
Locations:
1) Genital 📷
2) Peri-anal 📷
3) Oral cavity 📷
DDx:
- Fordyce spots are harmless and painless sebaceous glands.
- They appear as white/yellow small bumps or spots on the inside of lips or cheeks, gums, or genitalia.
- They are common and present in approximately 80% of adults.
Tx:
👉🏽 local:
- 🧊 CRYO-therapy
→ if numerous → curettage, laser surgery, electrocoagulation
- 💊 : LOCAL cytostatics → salicylic acid (keratinolytic), 5-FU, trichloroacetic acid, podophyllin




- 🔰 Immune modifiers → imiquimod,

♻️ systemic:
- against virus → interferon alpha

- 💉 Vaccination (Cervarix, Gardasil)
KOH microscopy:
- Diagnostic test for fungal infections
- Detects dermatophyte infections of skin, hair, and nails
- Involves applying sample to slide, adding KOH, and observing under microscope
- KOH dissolves skin cells, making fungal hyphae visible
⇒ Tinea: 📷
⇒ Candida (yeast cells): 📷
Sabouraud medium:
- Growth medium used in microbiology to cultivate fungi (specifically dermatophytes and other filamentous fungi)
- Developed by Pierre Sabouraud in the late 19th century
- Contains a mixture of nutrients (e.g., peptones, glucose, and agar) that support fungal growth
- Optimal pH for the growth of many fungi (slightly acidic)

Dermatophytes: Epidermophiton, Tricophyton,Microsporum

= SUPERFICIAL FUNGAL INFECTION
Malassezia furfur

Clinic, Dgx, DDx, Tx*?
CLINIC:
1) MACULA (well-defined + VARIOUS COLOR) ⇒ form PATCHES 📷
2) SCALES on 📷 ↑HYPER-PIGMENTED PATCHES 📷 → if tanned (scales prevent tanning)→ ↓HYPO-PIGMENTED 📷
DGx:
Wood lamp → green fluorescence 📷
DDx:
- P-SQ-lesions
- psoriasis (guttate)
- ptyriasis rosea
- seborr. dermatiti
- Vitiligo (↓pigm.)
Tx:
- TOPICAL 🪝 selenium sulphide (shampoo)
or

- ORAL 🍄 antifungals → Imidazoles (✈️ fluconazol)
CLINICAL SUBTYPES of tinea pedis:
1) INTERDIGITAL (chronic interdigital scaling) 📷
1.1)FISSURES + erosions
1.2) On gray-white skin with SCALES
→ DDx: candidiasis (stage 4)
2) DYSHYDROTIC 📷
2.1) large BLISTERS
2.2) EROSIONS with → ERYTHEMATOUS + SCALY BORDER
→ DDx: psoriasis (pustular)
3) HYPERKERATOTIC 📷
3.1) THICK, DRY, SCALY PLAQUE
3.2) ERYTHEMATOUS BORDER
3.3) NAIL involvement is common ⇒ Onycho-gryphosis 📷
Onychogryphosis: hypertrophy of nails resembling claws or a ram's horn.
→ DDx: psoriasis, dry skin(xerosis)
⚠️ Complications: 🧫 Super-Infection + recurrent ERYSIPEL
1) Erythematous patch ⇒ INNER THIGHS, SCORTUM, PERINEUM 📷
2) SCALY “ACTIVE” BORDER 📷
⇒ DDx:
- Erythrasma 📷
- candida intertrigo
⇒ Tx: Terbinafine (or others) ⇒ SYSTEMIC or LOCAL
- Topical: Terbinafine 1% cream, miconazole, clotrimazole, ketoconazole, and econazole for 2-4 weeks.
- Systemic: Itraconazole (100 mg daily) or terbinafine (250 mg daily) for 2 weeks.
1) INFLAMMATORY TYPE: KERION CELSI 📷
1.1) ROUND + ERYTHEMATOUS patch (well circumscribed)⇒ SCARRING ALLOPECIA (hair = same lenght)

1.2) SCALES
1.3) INFLAMMATORY LESIONS → Pustules, Nodules = secondary 🧫 STAPH. INFECTION
⇒other locations: BEARD kerion celsi (tinea barbae) 📷
OTHER CLINICAL VARIANTS:
trichophyton:
- INFLAMMATORY → see 1)
- NON-INFLAMM. ENDOTRIX 📷

- NON-INFLAMMATORY ECTOTHRIX - MICROSPORIA 📷

Dgx = KOH, woodlamp
⇒ DDx: Alopecia arata, psoriasis
Tx: oral (systemic) griseofulvin (= prevent scarring allopecia)
⇒ Dgx → scrape + microscopy (KOH)
- Examination of scales:
- Used for the diagnosis of fungal infections
- Clean the skin with alcohol and allow it to dry
- Scrape the skin with a scalpel blade
- Place the sample on a clean blade
- Apply 10 or 20% KOH to dissolve the keratin
- Warming the blade can accelerate the process
- Direct microscopic examination
- Confirmation:
- Culture the sample on special media (Sabouraud)
⇒ DDx:
⇒ Tx → Terbinafin (TOPICAL or SYSTEMIC) or Azoles

Location (Variants)? Tx?
CLINICAL VARIANTS
1) 👄ORAL candidiasis 📷
WHITE PLAQUE w/ ERYTHEMA → scraped off → EROSIONS + BLEEDING
2) 🍆GENITAL candidiasis 📷
Balanitis with → CIRCULAR DESQUAMATION (& MULTIPLE VESICLES not seen in image)
3) 🐣 INTERTRIGOS candidiasis (Diaper dermatitits) 📷
ERYTHEMA w/ SCALES
4)💅🏽 PARONYCHIA candidiasis 📷
DYSTROPHIC nail w/ → peri-ungal (around nails) SCALES & Onychomycosis

⇒ Tx: ✈️ Fluconazole → SYSTEMIC or LOCAL (🚽 or local clotrimazole)
Clinic, Variants, Dgx, Tx*?
- Warm bed or bath exacerbates pruritus due to increased mite activity.
- Pruritus can occur in areas without mites due to allergenic antigens released on mite trails.
CLINIC:
1) BURROWS (linear, 2-15mm) 📷 = “tunnels” w/ EXCORIATIONS → basically everywhere
2) Erythematous PAPULES at ENTRY site📷
3) DARK VESICLES at END of burrow (female mite is there) 📷
4) SECONDARY EXANTHEM 📷
- buttock
- lateral trunk
- prox. extremities
- “belt region”
VARIANTS:
⇒ Dgx = microscopy + dermoscopy 📷
⇒ Tx:
- systemic: 🌲 IVERMECTINE (anti-parasitic)

- local:⭐ BENZYL BENZOATE, 🦪 PERMETHRIN, others

→ Tx for entire family 👩👩👧👧
→ wash clothes
HEADLICE - CLINIC
1) erythematous PAPULES 📷
2) NITS (eggs) 📷
3) LICE might be seen 📷
SUBTYPES: → location
- BODY-lice
- PUBIC-lice (phtirius pubic)
→ EXCORIATION + papules/nodules → scars
→ !! VECTORS of trench fever + typus

→ EXCORIATION + macules
⇒ DDx: Eczema
⇒ Tx:
- local: 🦪 PERMETHRIN or others

inhibits Na+ channel deactivation → neuronal membrane depolarization
others:

- Nit COMBS
❄️ Papulo-Squamous lesions
SQUAMOUS = they all have ❄️ SCALES 📷

❓poorly understood → Combination of genetic and environmental factors ⇒ trigger factors*
→ Believed to be 🛡️autoimmune ⇒ Strong association with HLA-C
⇒ 🕰️ 🔥 CHRONIC INFLAMMATION

- 🥿 PLAQUE
- 〰️ Well-demarcated
- 🍣 Pink/salmon-colored
- ❄️ Silver-white SCALES
1. 🦵🏽 areas exposed to trauma/friction: ellbow, knee, legs, lumbosacral , palms+soles, ⇒ usually ØFACE
severe variants are marked in red:
- 🥇 Plaque psoriasis (80-90%) = Psoriasis vulgaris
- Nail psoriasis
- psoriatric arthropathy
- 💧 Guttate psoriasis 📷
- 🪙 Numular psoriasis 📷
- 💆🏽♂️ Scalp psoriasis 📷 📷⇒ ØHair-loss
- 💪🏽 Flexural (Inverse) psoriasis 📷⇒ ØSCALES
- ✋🏽 Palmo-Plantar psoriasis 📷 📷
- ✋🏽🟡 Pustular Palmo-Plantar psoriasis 📷 📷
- 🟡 Generalized pustular psoriasis 📷 📷⇒ trigger: 💊
- 🗯️ Erythrodermic psoriasis 📷 📷⇒ >90% skin surface; w/ desquamation ⇒ trigger: stop 💊
- Other: Genital muscosa 📷 + face psoriasis 📷

- Hyperkeratosis (↑s.corneum)
- Parakeratosis = RETAINED NUCLEI in s.corneum
- Acanthosis = ↑epidermis
- ↑ S. spinosum
- ↓/Ø S. granulosum
- Dermis blood vessel → surface ⇒ scale breaks → BLEEDING = AUSPITZ SIGN
- Np from Dermis → S.corneum ⇒ MUNRO MICRO-ABSCESSESS
- 👉🏽 TOPICAL
- 🥟 Keratolytics → Salicylic acid
- 🌝 steroids
- 🍦 Calcipotriol (VitD analogue)
- 🔆 Phototherapy
- Narrowband UVB therapy
- PUVA therapy
- ♻️ SYSTEMIC ⇒ IF >30% or COMPLICATED FORM
- Retinoids (Acitretin)
- Immunosuppressives
- MTX
- Cyclosporin
- Biologicals
- ❄️OTHER PAPULO-SQUAMOUS LESION
- Ptyriasis Rosea (+ Syphillis)
- Lichen Planus (esp. w/ Guttate form)
- Seborrheic dermatitis (hard esp. with face psoriasis→ look for distant sites)
- ☄️ DERMATITIS ⇒ esp. NUMMULAR eczema (Øscales, crumbled borders, pruritus, lichenification, other location)
- 🎾 Lymphoma (B or T cell) ⇒ BIOPSY + SCREENING-TEST
(“lichen” = tree moss, “planus” = flat)

❓unknown
→ assoc. w/ 🦛 HEP C
⇒ ⇒ 🕰️ 🔥 CHRONIC INFLAMMATION
⇒ resolves spont. over YEARS (lecture = 6-12 month)
→ Extremities → bilat + sym.
- 💪🏽 arm → wrist
- 🦵🏽leg → ankle
- 🍑 lumbo-sacral area
→ 6 P’s:
- Papules or Plaques
- Purple
- Pruritic !!
- Polygonal + irregular borders but well-demarked
- Planar (flat-topped)
⇒ 💥 KOEBNER’s signs (= new papules develop at site of trauma)
⇒ 🕸️ WICKHAM’s sign (= wickham’s striae after paraffin oil application on lesion)
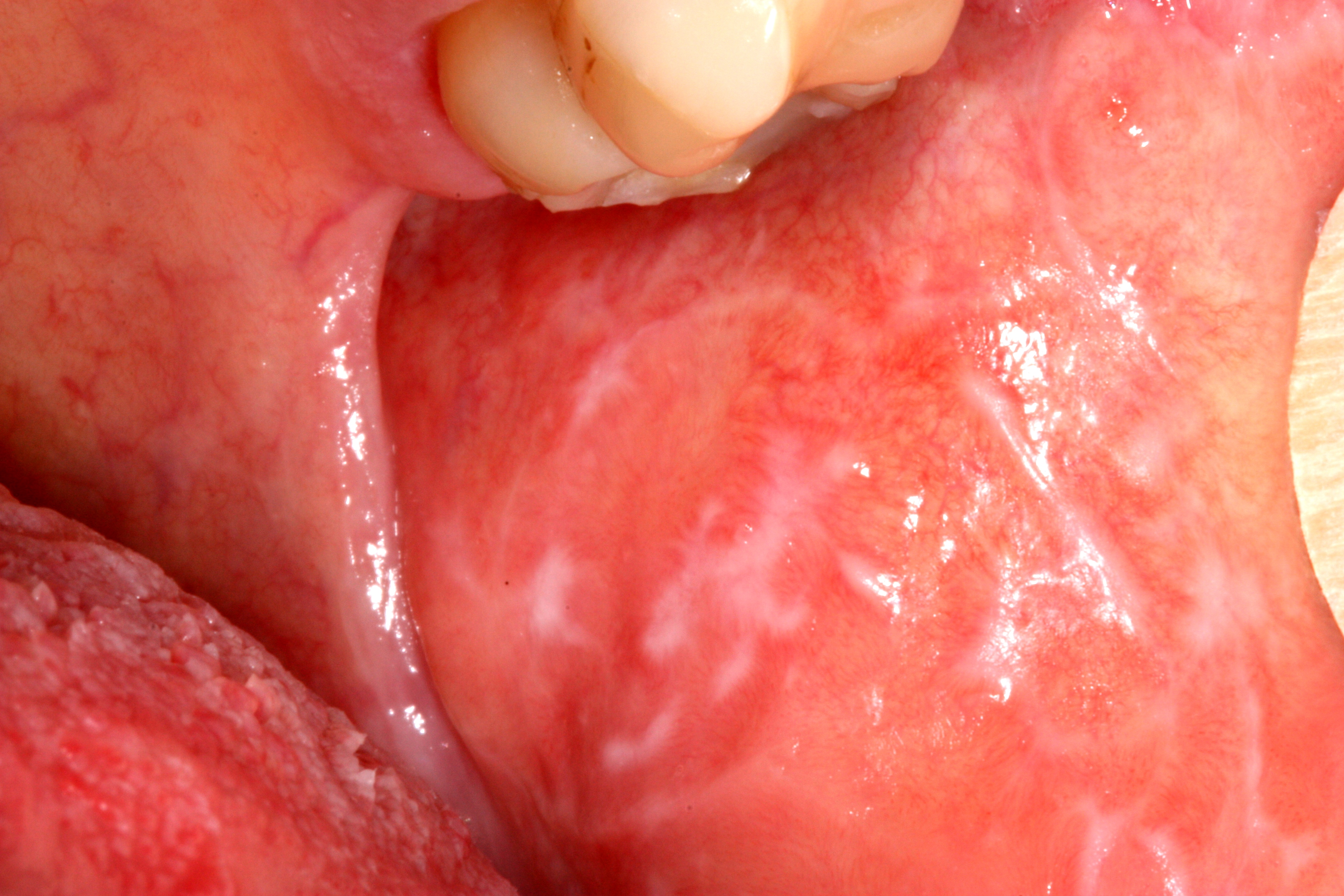
2) 👄 MUCOSA
- oral
- glans penis
⇒ 🕸️ WICKHAM STRIAE (due to hypergranulosis) 📷

3) 💅🏽 NAILS 📷
- longitudinal RIDGING
- subungal HYPERKERATOSIS

- Hyperkeratosis (↑s.corneum)
- Hypergranulosis (↑s.granulosum)
- at dermal-epidermal junction:
- Lymphocytes
- “Sawtooth” pattern of rete ridges*
rete ridges

Public domain

#1 🌝 STEROID
→ SYSTEMIC (alternative: retinoid)
→ TOPICAL
#2 🔆 Phototherapy (UV light)
#sympt⇒ for PRURITUS:
- 🐝 Anti-Histamines
- 😴 sedatives/anxiolytics (pat. cant sleep bc of itching)
- Palmo-plantar LP 📷 📷
- Plano-Pilaris LP 📷
- Nails LP 📷
Scaly patches, well demarcated, sometimes erosive, fissured
Affect the scalp: Small pink plaque covered with a very adherent scaly coating, scarring alopecia and atrophy Can affect the entire scalp
is not very rare, Can be isolated Irreversible destruction of the nail apparatus Acquired dorsal pterygium
- Psoriasis (guttate)
- Scabies
❓unknown (possibly 🦠-HERPES)
⇒ ⏱️ ACUTE RASH + skin lesion
⇒ SELF-LIMITED: resolves spont. over 2-3 MONTH
1) HERALD PATCH 📷
- SINGLE lesion
- red/salmon colored
- well-demarked
- SCALES with CENTRAL ATROPHY
⇒ 🧰 chest OR🗼back OR 🧣neck
↓
after days (10-15)
↓
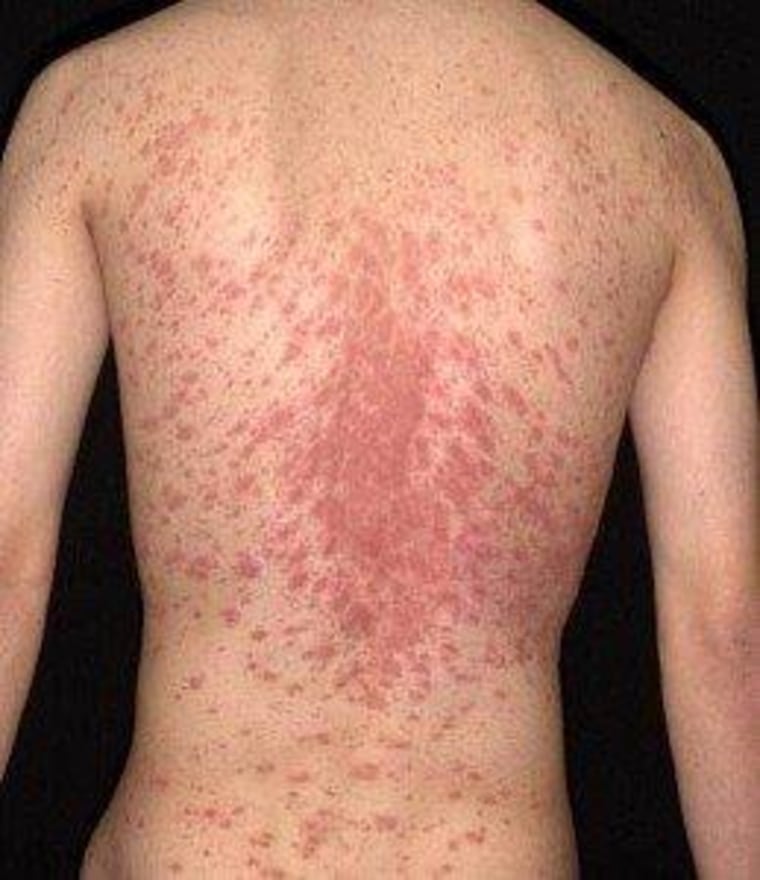
2) GROUPS of multiple SIMILIAR + SMALLER lesions on TRUNK (NEVER OVER ELBOW/KNEE) 📷
⇒ develop SCALE = “TRAILING” ; Øcentral atrophy



⇒ 3) 🎄 CHRISTMAS TREE DISTRIBUTION (follow SKIN LINES on back) 📷 📷
self-limited ⇒ usually ØTx needed
if atypical form ⇒ 🌝 TOPICAL steroids, Phototherapy (pruritus), Erythromycin (if prolonged)

Syphilis + HIV ⇒ serology has to be done!!
Patho: Poorly understood pathogenesis, No inflammation of sebaceous glands but assoc. with them (adolescents + >50y)
→ Associated with fungal infection by Malassezia

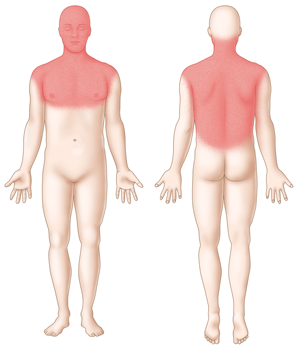
PRURITIC (if sev. burning), erythematous PLAQUE with yellow SCALE (flaky skin) 📷

INFANTILE FORM (ISD):
⇒ 1) “CRADLE CAP” 📷(thick adherent scale → Øpruritus )
⇒ 2) Rash in SKIN FOLDS of TRUNK + EXTREMETIES 📷
⇒ resolves spont. (in contrast to adolescent/adult = chronic relapsing)
Tx:
Topical → 🍄 antifungal (ketonazole) + 🌝 steroids , keratinolytics, calcineurin inhib.
(if severe →systemic steroids/retinoids)
- Syphillis (secondary)
- other DDx: eczema + tinea corporis
☄️ Dermatitis / Eczema
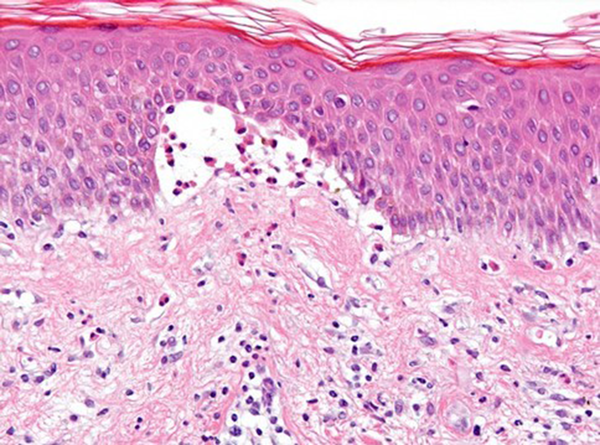
Exogenous:
Hypersensitivity type 4 (delayed reaction)
⇒ PRURITUS + LOCALIZED to area of skin contact with allergen 📷(poison ivy, nickel, detergents, chromium)
→ otherwise like atopic dermatitis:

Dgx:
Patch test 📷
Tx:
- avoid allergen
- 🌝 steroids → local or systemic (depending on localized or widespread)
Aspect | ICD (Irritant Contact Dermatitis) | ACD (Allergic Contact Dermatitis) |
Symptoms | Burning stinging, prickling, pain and soreness of the skin (pruritus may be present) | Pruritus is the main symptom of ACD |
Clinical Course | - Appears after first exposure, especially with strong irritants | - Sensitizing exposure(s) is required |
- Lesions appear rapidly, usually within minutes to a few hours after exposure, delayed reactions can be seen | - Clinical lesions appear after re-presentation of the antigen to already primed (memory) T cells
- Lesions usually appear 24–72 hours after the last exposure, but may be as early as 5 hours or as late as 7 days | |
- Characterized by a decrecendo phenomenon | - Allergic reactions characterized by a crescendo phenomenon, slower resolution | |
- Reaches its peak quickly and then starts to heal | ||
Risk Factors | Everyone is at risk | Genetically predisposed individuals are at risk |
Mechanism | Nonimmunologic mechanism: Physical and chemical alteration of epidermis | Delayed hypersensitivity reaction |
Exposure Required | Few to many, depends on individual's ability to maintain an effective epidermal barrier | One or several to cause Sensitization |
Nature of Substance | Organic solvent, soaps, acids usually high concentration required | Low molecular weight hapten (metal, formalin, epoxy, etc.), may be very low concentration |
Lesion Appearance | Rapid (few hours after exposure), monomorphical, well-defined to site of exposure | Not so rapid, polymorphical, poor-defined, spreading in the periphery, may become generalized |
Management | Trial of avoidance | Trial of avoidance, patch testing |
Protection and reduced incidence of exposure | Complete avoidance |

- Photosensitivity dermatitis
Endogenous:
Clinic, Dgx, Tx*, Cx?
hypersensitivity disorder
chronic → flares + remissions
⇒ PATCHES / PLAQUES → erythematous + Pruritus (+dry)
- 1) baby 📷 📷→ face (cheeks) + scalp, extensor:
- 2) children/ adults 📷 📷 📷 → lichenified (thickened) plaques/papules +/- scaling, +/-excoriation
- children: skin flexures (i.e. popliteal fossa), dorsal Arm+hand( wirst, elbows), feet
- adults: trunk, face with Dennie Morgan sign* 📷 , skin flexures, hands(dorsal), feet
→ patch or papulo-vesicular plaque → +/- scaling, +/-excoriation
Dennie Morgan sign: small creases along lower eyelids
(⇒ high risk if Filaggrin gene mutation)
filaggrin = protein in stratum corneum
if mutation → filaggrin deficiency →impaired skin barrier → higher risk of eczema
Dgx: ↑IgE, Family history of atopic disorder
Tx:
- Topical
- Hydration(emollients)
- steroids🌝 / anti-histamines
- Calcineurin inhibitors (Tacrolismus, Pimecrolimus)
- systemic (classics)→ 🌝 steroids, DMARDs, biologicals
Pime → mild/mod AD
Tacro → mod/sev AD
- 📸Phototherapy

- identify + eliminate trigger,
Complications:
- 👁️ cornea scarring, cateracts, keratoconjunc.
- 🦠 infections → HSV, S.Aureus, fungal
- Hand + exfoliation dermatitis

- Xerosis (dry skin)
- Fissures
- Erythema
- Itching
- Legs
- Elderly
Patho: Related to itching/scratching but assoc. with multiple etiologies → Rule them out
- Bidirectional relationship with emotional and psychological factors
- Other dermatoses: Atopic dermatitis, Contact dermatitis, Pemphigoid nodularis, Psoriasis, Candida, and Tinea infections
- Systemic causes of pruritus:
- Renal insufficiency
- Hyper- or hypothyroidism
- Liver failure
- Hepatitis B and C viruses even without liver failure
- HIV disease
- Helicobacter, mycobacterial or parasitic infection
- Underlying hematologic or solid-organ malignancy, including Hodgkin disease, gastric and bladder cancers, celiac disease and/or dermatitis herpetiformis
⇒ HARD, pruritic NODULES 📷 : hyperkeratotic or crateriform w/ overlying excoriation
→ extremities (extensor surf), abdomen, sacrum (Øupper back)
Tx: → #1 control pruritus 🦟
#1 topical → 🌝steroids or non-steroid antipuritic (menthol)
#2 intra-lesional steroids, cryo, topical calcineurin-inhib(tacrolismus)
refract → phototherapy, immunosuppressants
emolients, sedating anti-histamines
keep nails short
Tx: topical 🌝 steroids
- Chronic Venous Insufficiency (CVI) is caused by peripheral venous hypertension in the superficial and/or deep venous system.
- It can be primary or secondary, with the latter being mainly due to post-thrombotic syndrome.
- Venous reflux, obstruction, or limitation of muscle-ankle function contribute to the development of CVI.
- CVI leads to capillary dilation and the deposition of fluids, erythrocytes, and protein in the interstitial tissue.
- This causes inflammation, pigmentation, and increased collagen synthesis by fibroblasts.
- Impaired microcirculation and hypoxia in sclerotic areas can result in ulcerations and impaired wound healing.
- Stasis eczema 📷
- Corona Phlebectatica Paraplantaris 📷 : Perimalleolar and periplantar telangiectases indicating dilated superficial blood vessels.
- Dermite Ocre (Increased Pigmentation)📷 : Erythrocyte extravasation leading to hemosiderin deposits in the skin. Initial petechiae and purpura transition to yellow-brown discoloration.
- Hypodermitis📷 : Chronic, noninfectious inflammation of subcutaneous tissue on the lower calf, causing painful skin thickening. Distinguishable from erysipelas by the absence of systemic features. Progresses to lipodermatosclerosis over time.
- Lipodermatosclerosis📷 : Skin adhesion to subcutaneous tissue, preventing pinching or lifting. May involve entire lower leg, causing 'piano leg' or 'inverted champagne bottle leg' appearance due to constriction and proximal swelling.
- Atrophie Blanche📷 : Porcelain white, atrophic skin areas overlying fibrosis, often with hyperpigmented periphery. These patches may be several centimeters in size and become depressed.
- Patchyderma and Hyperkeratosis📷 : Response to chronic edema and lymphatic overload, resulting in skin thickening, papillomatous and verrucous changes. Recurrent erysipelas may lead to elephantiasis and further lymphatic damage.
- Venous Leg Ulcer📷 : Commonly located on the lower calf around the ankle, representing a frequent site for venous ulcers.
- Topical Therapy for Ulcers:
- Debridement: Employ mechanical debridement for necrotic tissue removal when necessary. alternative: Enzymatic Agents → Utilize proteolytic enzyme preparations, notably collagenases, for non-complex cases.
- Desinfection: Apply agents such as silver nitrate or chlorhexidine for disinfection.
- Epithelial Growth Promotion: Use treatments containing silver sulfadiazine, urea, or essential vitamins to foster granulation and re-epithelialization.
- Skin Grafting: Consider grafting to expedite the healing of clean, well-prepared ulcerative wounds.
- Topical Dermatitis Management:
- Corticosteroids: Utilize protective creams and moderate potency corticosteroid formulations for effective management.
- Chronic Venous Insufficiency Interventions:
- Elevation: Encourage nightly leg elevation to aid edema reduction.
- Muscle Activation/Mobilization: Advocate for patient engagement in activities like walking or swimming to activate muscle and joint pumps.
- Compression Therapy: Implement compression bandages or stockings to assist fluid reabsorption and reduce inflammation.
- Venotonic Medication: Consider venoactive drugs, such as micronized diosmin, for symptomatic relief.
- Surgical Consideration: Assess for potential surgical intervention when indicated.
🛡️ Auto-Immune Dermatosis
- Autoimmune blistering diseases: ABD
- Abnormal humoral reactivity: erythema multiforme, toxic epidermal necrolysis, photosensitivity, arthropod bites
- Genodermatoses: EB simplex, junctional & dystrophic, Incontinentia pigmenti, Hailey-Hailey disease
- Ischemia: non-inflammatory (coma), inflammatory (vasculitis)
- Skin infections: herpes simplex, bullous impetigo
- Metabolic conditions: porphyrias, diabetes, glucagonoma, bullous amyloidosis
- Physical and chemical factors: thermal, chemical, electrical, frictional injuries, radiation dermatitis

- Diseases with intra-epidermal blistering
- Pemphigus vulgaris
- subtype = Pemphigus vegetans
- Pemphigus folicaceus
- subtype = Pemphigus erythematosus
- Paraneoplastic pemphigus
- Drug-induced pemphigus
- Diseases with subepidermal blistering
- Bullous pemphigoid
- Mucous membrane pemphigoid
- Linear IgA bullous dermatosis
- Epidermolysis bullosa acquisita
- Dermatitis herpetiformis


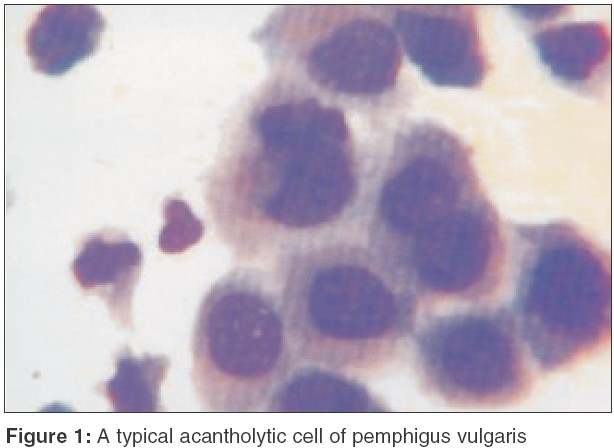
1) 🖖🏽 Pemphigus vulgaris:
- 30-60y (adults)
- Ab (IgG) against Desmoglein 1 + 3 (=component of desmosomes) ⇒ Acantholysis (loss of connections betw. keratinocytes) → disruption Stratum Spinosum 📷⇒ Fluid above BASAL layer with ROUNDED + FREE-FLOATING KERATINOCYTES 📷
2) ⛺ Bullous Pemphigoid
- 60-80y (elderly)

3) 🥖 Dermatitis Herpetiformis
🖖🏽 PV | ⛺ BP | 🥖 DH | |
👄 MUCOSA (ORAL) | + (in 70%) 📷 ⇒ dysphagia
👁️ & 🍆
(+- conjunctiva, genital) | - (in 80%)
| - |
BLISTER | flaccid (=not tense)📷→ burst easily
⇒ most bulla = ruptured → erosions + scabs | tense (less flaccid) 📷
⇒ more intact bullae, less ruptured
→ flexural skin areas
→ post-inflamm. ↑pigmentation | |
PRURITUS | + | + | |
Nikolsky sign* | + | - | |
Mortality | ↑↑
(due to infections, tx SE) | ↑
(infections, tx SE) | |
Subtype | rare: 🦀PARANEOPLASTIC bullous pemphigoid | ↑🦀 Lymphoma risk |
- An intact blister can be gently pressed to expand laterally
- Blistering can be artificially induced by rubbing normal skin.


🖖🏽 PV
⇒ Acantholysis
Fluid above BASAL layer with ROUNDED + FREE-FLOATING KERATINOCYTES
+ for IgG ⇒“RETICULAR” pattern (net-like)
+TZANK SMEAR 📷
⛺ BP
Fluid SUB-EPIDERMAL with EOSINOPHILS +lymphocytes
Øacantholysis
+ for IgG (+C3) ⇒ LINEAR at dermal-epidermal junction
🥖 DH
micro-abscesses (spaces) at tip of dermal papillae w/ NEUTROPHILS
IgA depositions
⇒ granular depositions at tip of dermal papillae
- Antibodies against tissue transglutaminase
- Antibodies against epidermal transglutaminase
- Clinical history and physical examination
- Cytologic smear - Tzanck
- Histopathology
- Direct and indirect immunofluorescence
- Immunoblotting: ELISA
↓
↓
↓
↓
↓
- Immunelectronic microscopy
PV:

PF:

🖖🏽PV
1)🌝 Predni (systemic - ↑dose)
→ 🦴 give with Calcium + Vit D
→ if >3m → Biphosphonates
2)🛡️ Immuno-supressives
→AZA, MM
→ Rituximab, IVIG, Plasmapheresis
⛺ BP
1)🌝 Predni (🥈systemic) → start with 🥇topical steroids 2)🛡️ Immuno-supressives
→ Rituximab, AZA
🥖 DH
1)🥖Gluten-free diet
2)🕺🏽 Dapsone
⇒ inhibitis neutrophils
Side Effects:
- Haemolytic anemia
- Methaemoglobinemia
- Peripheral neuropathy
→ check blood regularly
PV ⇒ fatal without Tx ☠️
BP ⇒ benign, usually well Tx-response
INTRA-EPIDERMAL:
Only Ab against Desmoglein 1 (Øagainst desmoglein 3 like PV)
🌝 steroids (🥇 systemic) - like PV
- topical steroids
🕺🏽 DAPSONE - UNLIKE PV

SUB-EPIDERMAL:
🛡️ Auto-Ab (IgG + C3) against components of BM
elderly (like BP)
🌝 steroids +/- 🛡️ Immunosuppressants
Linear IgA deposition → BM 📷
- 💊 drug-induced
- 👶🏽 Chronic bullous dermatosis of childhood
- 🧫 AB → Vanco + TMP-SMX
- ⚡ anti-convulsants: phenytoin + lithium
- ❤️ CV → furosemide, atorvastatin, captopril
- 🧯 NSAIDS → diclofenac
5y
most patients remit completely before the onset of puberty
like PF
🌝 systemic steroids
🕺🏽 dapsone
Ab against TYPE VII COLLAGEN

adult 40-60y (like pemphigous)
assoc. with other AI-disease
🌝 steroids (systemic)
🛡️ Immunosuppressants
💥 Avoid trauma
1) HYPERKERATOTIC PLAQUE 📷 with ERYTHEMA → face, ear, nose, scalp; rarely trunk + extremeties
- center: adhererent scale (painful when removed) → under scale = follicular plug
2) ATROPHY
- pigm. changes ⇒ periph: in time raised + red & center: pale + depressed (=atrophy) 📷
3) SCARRING ALOPECIA 📷
4) ORAL / lip lesions 📷
Variants:
- L. tumidus 📷→ only dermis, Øscar
- L. profundus 📷→ all subcutaneous layers
- Chilblain lupus 📷→ finger, “frostbite”-like
is considered a precancerous lesion (SCC)
Dgx:
- check ANA
- Anti-Ro,La + dsDNA, Sm, etc. → if present could be systemic
- IF → band like lesions DEJ (IgG+C3) 📷
DDx:
- Rosacea,
- seborrhea dermatitis
- psoriasis
- tinea, scarring allopecia
Tx
- 🌝 steroids ⇒ TOPICAL (↑↑potency) & SYSTEMIC
- 🦟 Hydroxychloroquine
- non-pharma: sun screen, hair transplant, lasery therapy

Cutaneous+mucosal findings:
- 1) MALAR RASH 📷 📷
- both cheeks and nose,
- indurated erythematous plaques,
- inflamed
- spares nasolabial folds
- discoid rash
- Ø scarring alopecia (in contrast to CCLE)
- bullous lesions
- hyperkeratotic painful macules on palm + soles (acral photosensitive lesions)
- vasculitis
- livedo reticularis (aka racemosa) 📷
- Oral ulcer (hard palate) 📷
Tx
- 🦟 Hydrochloroquine or DMARDS
- 🌝 steroids ⇒ SYSTEMIC
- 🧯NSAIDS
- non-pharma: sun screen, hair transplant, lasery therapy
Prognosis depends on
- artherosclerosis
- renal inv.
- infections
can be assoc. with lupus
→ thrombosis
→ fetal loss
→ thrombocytopenia
→ anti-phospholipid Ab (anti-cadiolipin, lupus anticoagulant)
→ (livedo reticularis)



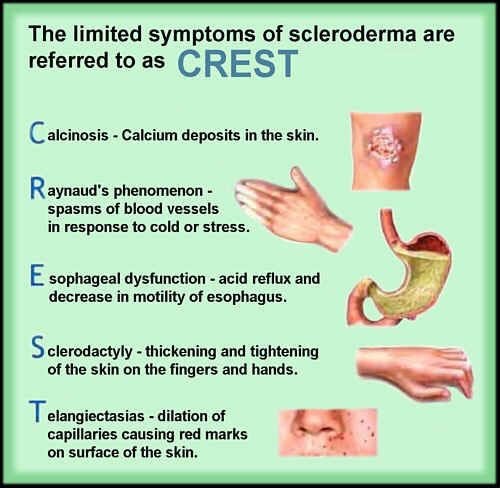
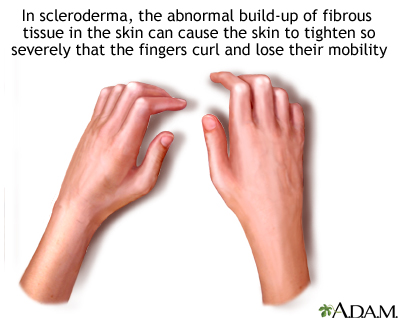
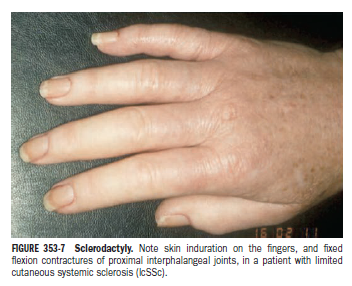
collagen depositions → stiffness where it deposits
- LCSS (CREST) → Anti-Centromere
- DCSS (Scleroderma) → Anti-Scl70 (=topoisomerase)
🖐🏽
💆🏽♀️
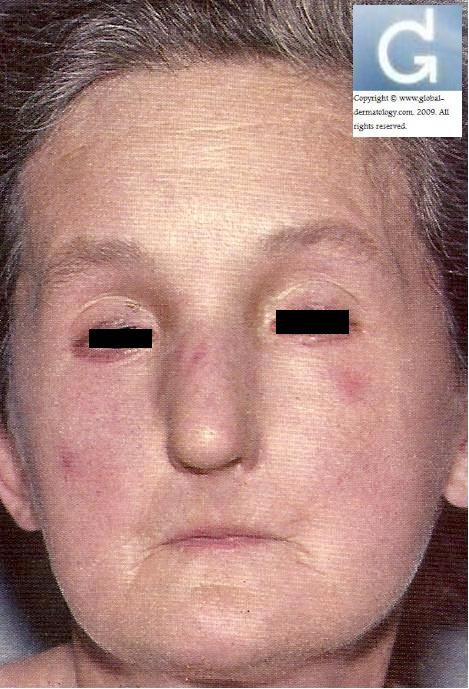
3) MASK-like facies 📷 📷→ loss of expression
3.1) MICROSTOMIA
3.2) perioral FOLDS
3.3) PEAK-LIKE appearance (🐦)
Tx = symptomatic
- Calcinosis → carbon dioxide LASER
- Raynauds → CCB
- Esophageal → PPI
- Fibrosis (i.e. sclerodactily) → phototherapy (UVA)
- Ulcer → PDE-5 inhibitors (-”afil”: tadalafil, sildenafil)
- if rapidly progressing = steroids (low dose)
LCSS → mainly limited to face, forarms, hand, feet
other visceral locations: eyes, teeth, larynx, GI
low dose 🌝 steroids,
if refract → DMARDs (cyclophosphamide, AZA, MTX)
Cause: IDIOPATHIC, maybe 🦂 Borrelia burgdorferi OR 💥 Trauma

ALL → ↕️ PATCHY PERIPH. EXPENDING ERYTHEMA
CLINICAL VARIANTS:
- PLAQUE-LIKE MORPHEA: 📷 📷→ central ivory plaque (=sclerotic area → atrophy) sourrounded by 1) liliac ring (blue-pink, violet)
- LINEAR MORPHEA: (En coup de sabre) 📷→ band like lesion from eyebrows to scalp ⇒ scarring alopecia, bone damage, abnormal neuro findings
- guttate morphea 📷
- disseminated morphea (generalized) 📷
- hemifacial atrophy 📷
COMPLICATIONS:
- 🐄 pigmentary changes
- 💪🏽 atrophy + deformities
→ evolution = persistent unpredictable but not permanent
Tx:
SYSTEMIC → 🧫 AB (high dose), 🌝steroids, DMARDs (hydroychloroquine, cyclosporin, MTX)
topical → first line PUVA, 🌝 steroids + emollients

2) GOTTRON PAPULES 📷

Systemic findings → sclerosis+calcifications of:
5) 💪🏽 prox. symmetrical muscle weakness
→painless + subacute
6) lung, heart, GI
Dgx: Anti-Jo + Anti-Mi-2
Anti-Jo:

Anti-Mi-2:

⇒ 7) SCREEN for underlying 🦀 MALIGNANCY
Tx:
🌝 steroids (high dose)
Dmards (MTX, AZA, MM, CYP), biological, ivig, hydroxychloroquin
→ Ø physical therapy!
- Clinic
- BIOPSY = Gold standard
- Angiography → if Øbiopsy possible (Takayasu, PAN)
- Lab:
- Inflammatory markers (ESR, CRP, etc)
- Organ markers (kidney, liver)
- ANCA
- Etiology: HepB+C serology + cultures
- Suggesting for immune-complexes
- RF + ANA
- Cryoglobulines
- Complement
- Giant cell (temporal) arteritis
- Takayasu arteritis


- Polyarteritis nodosa (PN)
- Kawasaki disease
- CNS vasculitis
- Burgers diseases
Hep B
all organs can be affects → NEVER LUNGS!!
most common:
🥐 renal artery
🍤 mesenterial artery
🌕 nerves
- Renal artery → HT (hematuria, oliguria, RF)
- mesenteric → GI pain + melena
- nerves → periph. neuropathy ⇒ MONONEURITIS MULTIPLEX 📷
- +SKIN LESIONS
- coronary arteries → MI
- Genitals → orchitis
- Arthralgia/Myalgia
Mononeuritis multiplex: painful, asymmetrical, asynchronous sensory and motor peripheral neuropathy
Asian <5y
CRASH and BURN on a KAWASAKI
- Conjunvtivits (bilat)
- Rash: Polymorphous non-vesicular
- Adenopathy (cervical)
- Strawberry tongue + cracked red lips
- Hand+foot: red palms + soles
- Burn: Fever >5d
⇒ 📷
CORONARIES!!
→ thrombosis → MI
→ Aneurysm → rupture
→ other 🫀-pathos: Myocarditis, Pericarditis, valvulopathy, arrythmias
- ANCA-ASSOCIATED small vessel vasculitis
- Granulomatosis with polyangitis (Wegeners)
- Microscopy polyangitis (MPA)
- Eosinophilic granulomatosis with polyangitis (Churg-Strauss)
- NON-ANCA-ASSOCIATED small vessel vasculitis
- IgA vasculitis (Henoch-Schonlein purpura)
- Cutaneous small vessel vasculitis (Leucocyto-Clastic vasculitis)
→ We”c”ners → “C”-man: nasopharynxm lung, kidney involvement & C-ANCA(anti-proteinase3)

most common vasculitis in children
FOLLOWING 🧣URT infection
IgA deposition


Histo ⇒ IF (IgA in dermis) 📷
IgA: usually self limited
⇒ but can be #1 NSAIDs → #2 Steroids → #3DMARDS can be given in severe forms of nephritis (Azathiprine) but usually not needed
consider anticoagulants

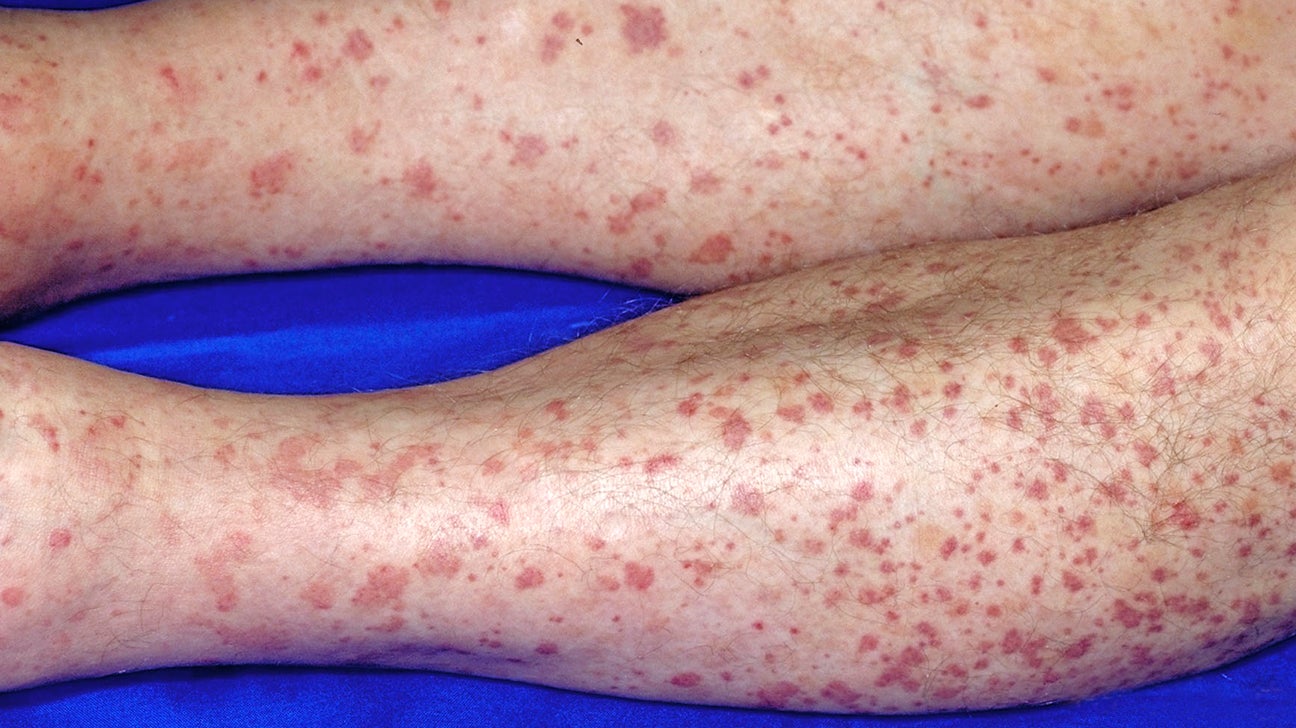
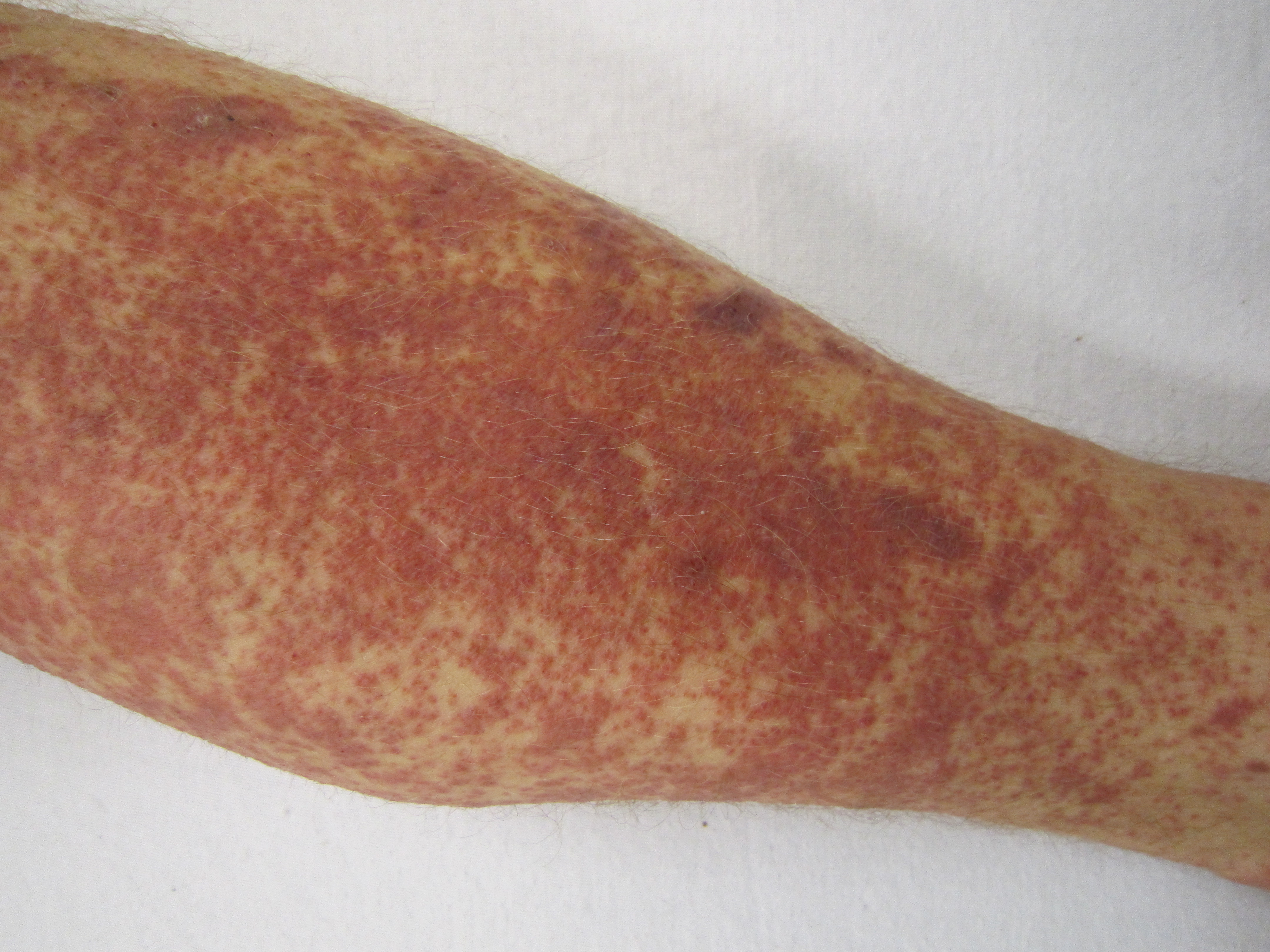
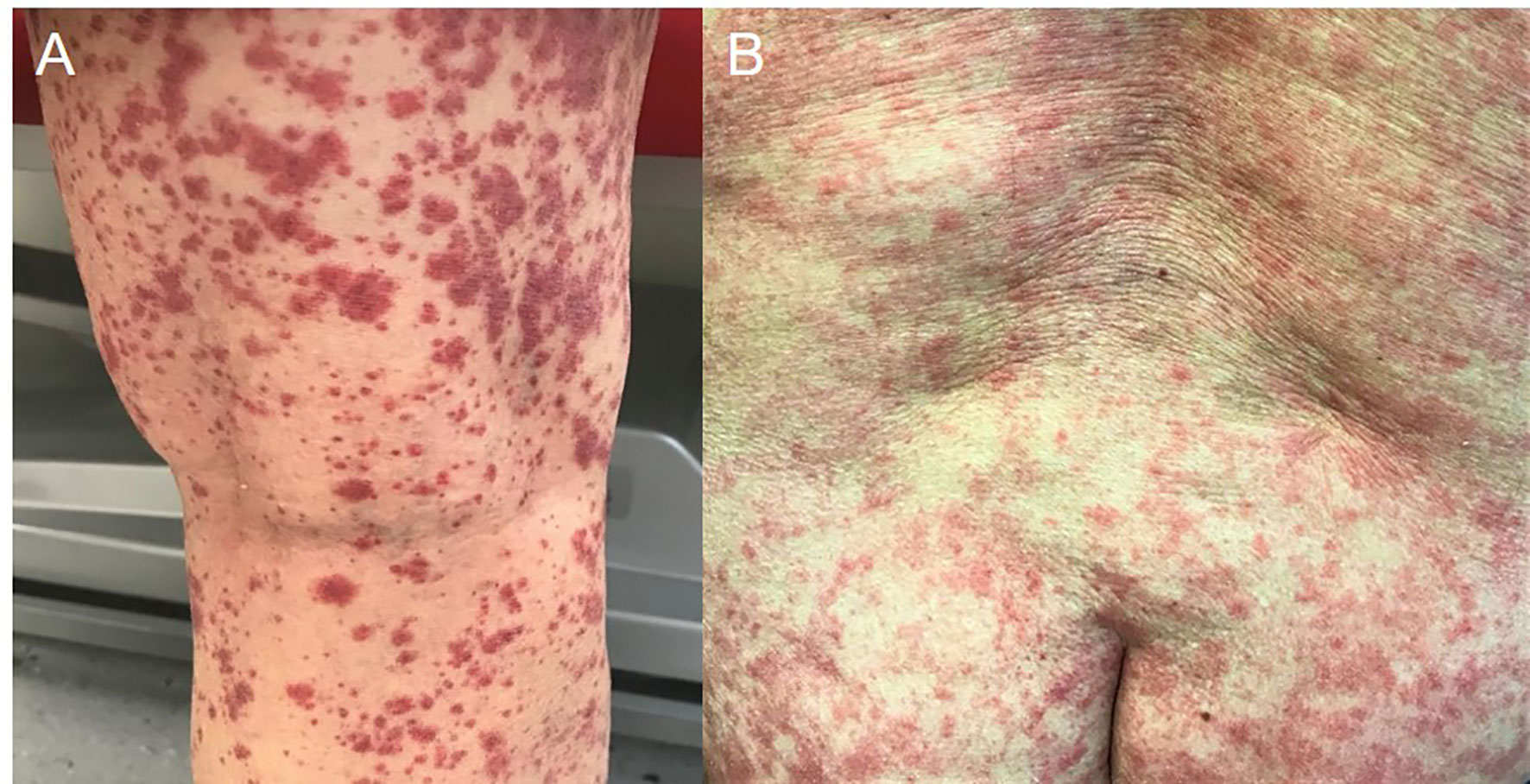
Trigger (drugs, infection) ⇒ immune complexes ⇒ PALPABLE PURPURA (like IgA)
- occurs 7-10 days after certain medications or infections.
- Immune complex-mediated leukocytoclastic vasculitis.
- Symptoms include palpable purpura.
- No visceral involvement.
- Late involvement indicates systemic vasculitis.
- B-symptoms (like all)
- Systemic symptoms might be presents → 🍤 GI, 🥐 renal, 🌕 neuro ⇒ ↑↑suspicion for SYSTEMIC VASCULITIS
1) PALPABLE PURPURA: 📷 📷 📷 → MACULES + PAPULES (pruritic) → SYMMETRICAL → Non-Blanching
⇒ heals with scars + ↑↓pigment. 2) +/- other vasculitis skin lesion (necrosis, blisters, livedo reticularis)
- like IgA → Steroids + AZA(or other)
- Colchicine (oral)
- non-pharma: remove trigger, elevate legs, compressive stockings
>85% → resolve (w-m)
10% → chronic recurr.
- ✏️ Psoriasis
🐝 Hypersensitivity reactions
🐝 Type I (immediate allergic reaction, IgE-mediated) → Prick test, specific IgE

Wheal = papule or plaque, pruritic + red, TRANSIENT

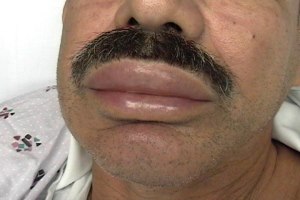
Urticaria = (Raised, red, pruritic, transient [diminishes in 1d]) Wheals +/- Angioedema (extension in deep dermis or subcutaneous)
Angioedema = deep mucocutaneous edema(swelling) →+/-pain but Øpruritus
Type 1: Allergic skin reaction to exog. Ag (to food, drugs [NSAIDs,ACEi], sting, infections, contactants, etc) → Mastcell degranul. + Histamine release
might be hypersensitivity type 2 in CHRONIC spontaneous ( +induced) assoc with;→ IgG against IgE or IgE-R on mastcells 📷→ Histamine, depending on activation of complement cascade)
Ø epidermis involvement
DERMIS:
- EDEMA (dilated blood vessel)
- DILATED LYMPHVESSEL (compensatory to drain edema)
⇒ can appear ALONE or component of ANAPHYLAXIS (wheezing, mucosal swelling, hypotension, syncope) ⇒ bc type 1 hypersensitivity ⇒ acute + self-limited (transient [around 24h])
HETEROGENIC (Raised, red, pruritic, transient) Wheals 📷 📷
- location: PERI-ORBITAL, LIPS, tongue, pharynx, LARYNX
- +/-pain
- Øpruritus
+- → urticarial VASCULITIS → if recurr. urticarial lesion that stay for >24h
→ histo: leukocytoclastic vasculitis
NON-CUTEANOUS FINDINGS:
- GI → infection = trigger
- Pharynx → bradikinin-induced
- signs of ANAPHYLAXIS (wheezing, hypotension, syncope)
- SPONTEANEOUS
- ACUTE → <6w
- CHRONIC → recurrent for >6w
DDx:
- other subtypes of urticaria
- other drug eruption (see type 4)
Dgx: Clinic + PRICK test + specific IgE
Tx:
- acute = self-limited
- induced → avoidance of stimuli or repetititve exposure to slight stimuli
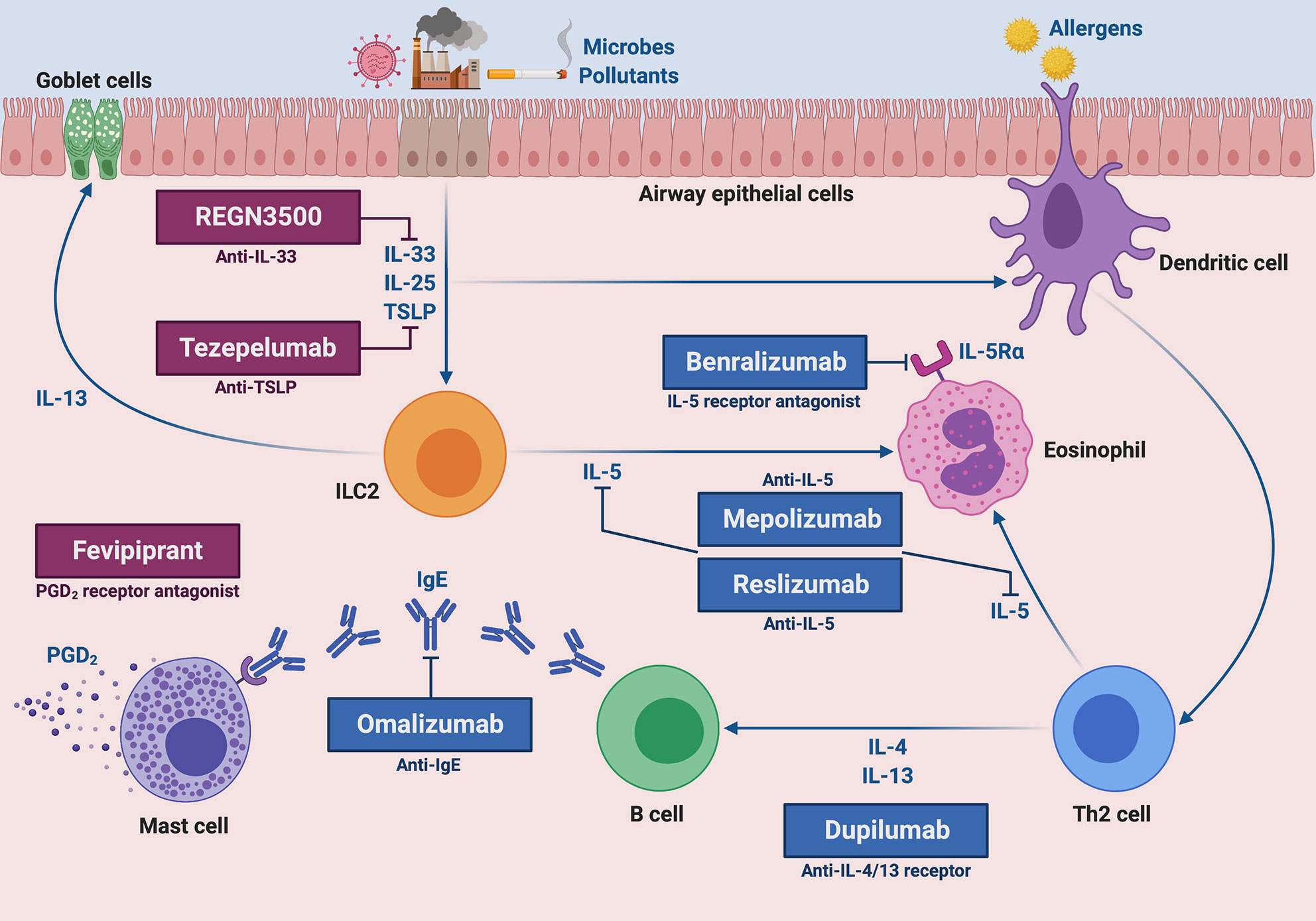
- 🥇Antihistamines (H1-Bl. 2nd gen) +- Montelukast, Omalizumab, Steroids

- mild-severe
- intermittent / persistent
→ i.e mild persistent, moderate intermittent, etc.
Mild intermittent → Allergen avoidance, 2nd gen Antihistamine, Decongestant, Chromes Other more severe forms 📷: → like mild intermittent PLUS addition of:
Intranasal steroids (fluticasone) Antileukotriens, Immunomodulators
- examples: Montelukast, Zafirlukast, Zileuton (LOX inhib)
- Block synthesis or block receptors of leukotriens
- effect: anti-inflammatory, ↓eosinophils action
- indication: rhinitis, asthma, urticaria, preventive (i.e. effort induced asthma)
i.e., Omalizumab is used in asthma & chronic urticaria
Types
- Local (injected) → Subcutan. administration
- Non-injected:
- Oral (tablets or drops)
- Sublingual immunotherapy (SLIT)
Indications:
- preventive: insect sting
- therapeutic: allergic asthma, rhinoconjunctivits
subcutan. → > 5 years
SLIT → > 3 years
Steroid NASAL SPRAY
- most effective drug for allergic rhinitis
- take several hours
Q. Choose the false statement: DDx of allergic rhinitis include:
- A. Infectious rhinitis, viral
- B. Vasomotor rhinitis
- C. Drug-induced rhinitis / rhinitis medicamentosa
- D. Eosinophilic nonallergic rhinitis
- E. Nasal tumors
E
Suspect asthma if:
RECURRENT coughing, wheezing, dyspnea, chest tightness
→ REVERSIBLE: relieved by bronchodilator → on spirometry seen by ↑FEV1 >12% + >200ml post-bronchodilator
Mediators of asthma:
- according to “thoracic key”: 📷
- according to lecture:
- Preformed (involved in early response)
- histamine
- cytokines (IL-1, IL-3, IL-5; GM-CSF; TNFalpha)
- enzymes (triptase, peroxidase, exoglycosidase, chimase, arylsulfatase)
- New-formed (involved in late response with EOSINOPHILS)
- Leukotriens
- Prostaglandins (PG-D2)
- PAF
- eicosanoids (HETE)
- In asthma, during the immediate response induced by the allergens, which of the following participate? a. Eosinophils b. Histamine c. Leukotrienes d. PMN (cytokines) e. Heparin
- Preformed mediators in allergies are: a. PAF (new formed) b. Histamine c. Leukotrienes (new formed) d. Enzymes (tryptase, chumase peroxidase...) e. Prostaglandins (new formed)
- H1 receptors produce: a. Smooth muscle contraction (guts, bronchi), mucus secretions, increased vascular permeability b. Stimulate acid secretions by the stomach (H2) c. Modulate neurotransmitters transmission to the presynaptic extremities d. Late effect in allergic cascade e. Production of O2 free radicals
BD
BD
AC
- 🐝 Atopic Dermatitis (type 1+4)
- IgE-mediated
- Systemic: Anaphylaxis
- Oral Allergy Syndrome
- Immediate gastrointestinal allergy
- Asthma/rhinitis
- Urticaria
- Morbilliform rashes and flushing
- Contact urticaria
- Eosinophilic esophagitis
- Eosinophilic gastritis
- Eosinophilic gastroenteritis
- Atopic dermatitis
- Cell-mediated (Non-IgE mediated)
- Protein-Induced Enterocolitis
- Protein-Induced Enteropathy
- Eosinophilic proctitis
- Dermatitis herpetiformis
- Contact dermatitis
1. Allergens involved in 90% of food allergies are:
a. Cows milk
b. Fish
c. Wheat
d. Penicillin
e. Tartrazine (food coloring)
ABC
2. Allergens in cows milk are:
a. Prophilins
b. Casein
c. Alpha lactoglobuline
d. Beta lactoglobuline
e. Ovomucoide
BCD
Oral allergic Syndrome (Pollen-fruits, latex-fruits):
- Edema of oral mucosa after consuming fresh fruits and vegetables in individuals allergic to pollens
- Allergens are destroyed by cooking
- Cross-reactivity between pollen and fruits/vegetables
- Systemic reactions are rare
Q. Peanuts allergy:
a. Cross reactivity with nuts: 25% b. Cross reactivity with vegetables: 5% c. Induces severe clinical picture d. Exists only in children e. Decreasing prevalence
AC
- Eviction
- Symptomatic Tx
- Epinephrines
- H1-Blocker
- Steroids
- Long term
- Omalizumab (Anti-IgE)
- Oral immunotheraphy w/ food (or patch)

- Analgesics: Nsaids, Aspirin, Opiates
- Antibiotics: Amoxi, Penicillin, Sulfa drugs, tetracycline
- History
- Paraclinic
- clinical: skin test, provocation test
- Lab:
- Immunoassay of Triptase & Ig
- LTT (lyphocyte transformation test)
- Objective: Measure the functional activity of lymphocytes in response to an antigen, infectious agent, or drug.
- Method: Expose lymphocytes to the specific antigen and observe the resulting response.
- Response: Look for changes in lymphocyte size or shape and the release of specific chemicals from the cell.
- BAT (Basophil activation test)
- Blood sample exposed to an allergen
- Monitor basophils for increase in size and production of histamine

- Immune Aggregates (Type 3 Hypersensitivity)
- IVIG
- Dextran
- Cytotoxic (Type 2 Hypersensitivity)
- Post-transfusion reactions to cells → ABO system (IgG, IgM)
- Non-allergic (Direct Degranulation of mast cells / other mechanisms)
- Contrast Substances (with high or low molecular weight)
- ACE-i.
- Opioids
- Neuromuscular blocking agents
- Gaz Etilen oxyde in tubes for dialysis
- Protamine
- Substances from dialysis membranes (poli. acrilonitrile sulfonate, poli-metilmetacrila)
- Physical Factors: Exercise, temperature
Signs & Sympt. | |
Skin | Pruritus, urticaria, angioedema, flushing |
Eye | Pruritus, tearing, redness |
Respiratory | Rhinitis, pharyngeal edema |
Cardiovascular | Arrhythmias, cardiac arrest |
GI | Nausea, emesis, cramps, diarrhea |
GU | Urgency, cramps |
- Majority: sudden onset, within 60 minutes of exposure
- Biphasic phenomenon 📷
- Second phase of mediator release, occurring 3-4 hours after initial exposure
- Mortality: 0,65 to 2%
💉 Allergo-Therapy
🚫 1. Eviction ⇒ ↓↓/REMOVE EXPOSURE
↓
💊 2. Pharma Tx
🌝 steroids
🐝 2️⃣nd gen. H1️⃣-Blocker → 👃🏾 rhinitis, 🥛 food
🌨️ cromes → 👃🏾rhinitis (,🌬️ asthma)
🎽 leukotriene modifiers →👃🏾rhinitis, 🌬️asthma, 🎡urticaria (chronic)
👵🏾 biologicals (omalizumab) → 👃🏾rhinitis, 🌬️asthma, 🎡urticaria (chronic)
💢 Epinephrine → anaphylaxis
Tx algorithm of acute anaphylaxis:
- Administer IM epinephrine and repeat as needed
- Stop offending trigger
- Administer supplemental oxygen
- Airway management
- Start basic airway maneuvers
- Consult anesthesia/ENT for assistance with intubation
- Secure airway using techniques for difficult airway
- Administer bronchodilators
- Position supine if tolerated
- IV fluid resuscitation
- Continuous epinephrine infusion for refractory shock
- Consider adjunctive treatment (steroids, antihistamines)
- Continuous telemetry and pulse oximetry
- Close clinical monitoring for biphasic reaction
- Transfer to ICU or medical service
↓
💉 3. Specific therpy → Immunotherapy with allergens (👃🏾rhinitis, 🌬️asthma, 🥛 food)
↓
↪️ 4. Prophylaxis
Early introduction of peanuts significantly ↓ frequency of development of peanut allergy (among children at ↑ risk for this allergy & modulated immune responses to peanuts)

Q. Adrenaline: a. Alpha and beta adrenergic stimulant b. Produces vasodilation (vasoconstriction) c. Produces bronchodilation d. Produces vasoconstriction and reduced extravascular extravasation e. Is essential in the treatment of anaphylactic shock
ACDE
Q. Emergency bag of an allergic patient: a. Adrenaline b. Cortisone c. Fluids d. Antihistamines e. Chromes (mastcell stabilizers)
AD
Q. Peanuts allergy: a. Cross reactivity with nuts 25% b. Cross reactivity with vegetables 5% c. Induces severe clinical picture d. Exists only in children e. Decreasing prevalence
AC
🔗 Type II (cytotoxic, IgM/G-mediated)
- 🎈 Auto-immune blistering disease
- Systemic: goodpasteur, rheumatic fever, graves, myasthenia gravis, hemolytic anemia(i.e. drug induced)
⛓️ Type III (immune complexes, IgG+Ag depositions)
- 🐺 CTD (lupus, RA,..)
- 🌶️ Vasculitis (PAN, drug-induced)
- 🥐 Nephropathies (PSGN, IgA, Membranous)
- 🏊🏾♂️ serum-sickness (drug induced)
🦖 Type IV (delayed allergic reaction, T-cell mediated) → Patch test
- Allergic contact dermatitis
- Atopic Dermatitis (type 1+4)
Most common: Urticaria (type 1) and Exanthematous eruption (type 4)
trigger = drugs (usually)
⇒ necrosis of epidermis (🚨 dehydration + infections) ⇒ nikolsky+
prodrome (fever, flu-like, light sensitivity, dysphagia)
→ after 1-3d:
⇒ if ≥30% BSA invovled = 4) TEN
ICU → supportative 🤡
2-6w after drug
Morbiliform [measles-like] eruption + SYSTEMIC (multiple organs → failure) 📷 systemic signs include: FEVER + ↑LN
- Maculopapular rash (>3 weeks after starting therapy with limited number of drugs)
- Prolonged clinical symptoms after discontinuation of causative drug
- Fever (>38°C)
- Liver abnormalities (ALT >100 U/L)
- Leukocyte abnormalities (at least one present):
- Leukocytosis (>11 x 109/L)
- Atypical lymphocytes (>5%)
- Eosinophilia (>1.5 x 109/L)
- Lymphadenopathy
- HHV-6 reactivation
Tx:
- stop drug
- 🌝 steroids systemic
- antipyretics
TRIGGER → reactive TYPE IV hypersensitive reaction (delayed) → Np chemotaxis → granuloma (& Type III? → complexes in venules of septa)
⇒ PANNICULITIS
TRIGGER:
- ❓idiop.
- 🧫 strep, histoplasmosis
- 🛡️ AI
- 💩 IBDs
- 🌶️ vasculitis (Behcet , PAN)
- ⚰️ sarcoidosis
- 🤰🏽 pregnancy + 💊 contracept.
- 🦀 malignancy
1) INFLAMMATORY NODULE (warm, painful, red) 📷 → POORLY-defined → Location: legs, arms → do Ø cause tissue destruction
2) SYSTEMIC signs: 🤒. fever +🦴arthralgia
- Other panniculitis

- Vasculitis
- Erysipel
- Superfical thrombophlebitis
- Symptomatic
- 🧯 NSAIDS
- 🍌 Potassium iodine
- 🌝 topical steroids
- If severe → SYSTEMIC STEROIDS, Colchicine (steroid-sparing), biologicals
- nonpharma: rest, leg elevation, compressive stocking
↓ pain, arthralgia, fever
- 🥇 Infections
- 🦠 HSV, Hep, EBV
- 🧫 Mycopl. pneum., Salmonella, TB
- 🍄
- 💊 drugs (i.e. steroids)
⇒ assoc. with 3.💩 IBD + 4. 🦀 neoplasia
MINOR EM
⇒ multiple 🎯 TARGET LESIONS 📷
→start: extremities (hands, feeet) → spread to center of body (centripetal spread)

→ CENTRAL: dark = hemorrhage, necrosis, vesicle
→ SURROUNDING: pale, cyanotic area
→ OUTER RING: erythematous
MAJOR EM
→ Laboratory findings & histopathology are nonspecific

COURSE | RECURRENCE | |
MINOR | rapid resulution | ↑ |
MAJOR | severe | ↓ |
- Remove trigger (+antiviral prophylaxis if herpes simplex)
- Topical antiseptics, steroids
- if sev → Systemic Steroids (⚠️ can be a trigger for EM)
⛓️ Non-Allergic Hypersensitivity (direct release of histamine from mastcells)
Non-allergic = Direct Degranulation of mast cells / other mechanisms
- Contrast Substances (with high or low molecular weight)
- ACE-i.
- Opioids
- Neuromuscular blocking agents
- Gaz Etilen oxyde in tubes for dialysis
- Protamine
- Substances from dialysis membranes (poli. acrilonitrile sulfonate, poli-metilmetacrila)
- Physical Factors: Exercise, temperature
- Infection-induced urticaria
💇🏽♀️ Alopecia & 🐄 Pigmentation disorders
- Intrinistic (genetic) alopecia
- Acquired alopecia
- Physiological: postpartum, newborn
- Febrile illness: typhoid fever, malaria, TB, HIV
- Physical or emotional stress: major surgery, bleeding, accidents, difficult births, severe diets, starvation
- Drugs: oral retinoids, antithyroids, IECA, beta-blockers, hypolipemiants, ACO, anticonvulsants, amphetamines
- Disease: hypo/hyperthyroidism, LES, syphilis, kidney or liver failure
- Nutrition: iron deficiency, zinc deficiency, malnutrition
- Others: hair dye, short anagen syndrome
- MINOXIDIL (direct arterial vasodilator)
- only for men → FINASTERIDE (5alpha-reductase blocker)
- only for women → ANTI-ANDROGENS (i.e. Spironolactone)
- TRANSPLANT, platelet rich plasma (PRP), laser
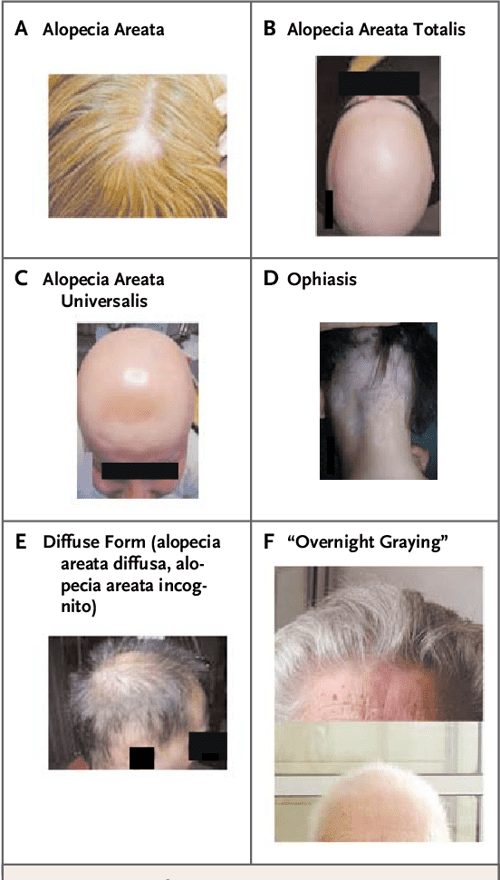
- A: Alopecia Areata - Hair loss plaques (single/multiple); white skin (Øatrophy), hair can be removed easily
- B: Alopecia Areata Totalis - entire scalp
- C: Alopecia Areata Universalis - entire body hair (including eye-brows + -lashes)
- D: Ophiasis - occipital involvement (↓Tx response)
- E: Diffuse Form (alopecia areata diffusa, alopecia areata incognito) - diffuse hair loss with visible plaques
- F: Overnight graying
- & Nail Changes: Trachyonychia = “sandpaper” nails 📷
- TOPICAL/INTRA-LESIONAL 🌝 steroids
- if severe (totalis, universalis or progressive): ⇒ PULSTHERAPY with 🌝 STEROIDS (systemic) or other DMARDS, 📸 Phototherapy
- Cosmetic camouflage → tattoos (eyelashes + eyebrows), wigs
Chemo (kills rapidly dividing cell) → rapidly after: Anagen activity stopped → Exogen hair (hair loss) 📷
rapidly dividing cells:

⇒ diffuse: ENTIRE SCALP
Dgx:
⇒ + HAIR-PULL TEST 📷 = indication for ↑ number of hair in telogen or exogen stage.

DDx: DIFFUSE Alopecia areata
ØTx ⇒ spont. REGROWTH in 3-6m
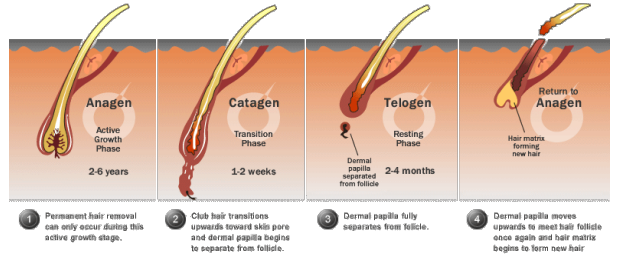
2-3m after ⚡TRIGGER → premature termination of anagen → direct entry in Telogen stage (skips catagen) 📷 (→ fall out over 12m)
⚡ Trigger:
⇒ loose up to 50% of terminal hair
Dgx:
⇒ + HAIR PULL TEST → telogen hairs
⇒ TRICHOGRAM: >25% telogen hairs
Tx → correct CAUSE
→ spont. REGROWTH in 12-18m (slower than anagen effluvium)
Patho: 5-DHT effect


⇒ SHORTENED anagen 📷
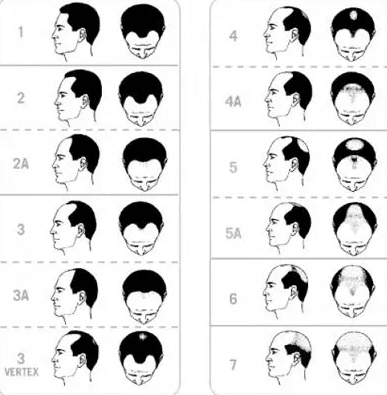
⇒ terminal hair turns → VELLUS-like hair = “Miniaturization” 📷 1) Bitemporal "M” pattern of recession

2) CROWN: circular patch
Dgx = clinical
Tx:
extend anagen
shortens telogen
thickens terminal hair (vellus-like)
SE: scalp irritation, hypertrichosis, dandruff
decrease conversion testosterone → DHT
SE: decr. libido, erectile dysf, gynecomastia
Pat: probably 🛡️ AI destruction of hair follicles
⇒ Assoc. with other AI disease: 🦋 hashimoto, graves 🐄 vitiligo 🐺 lupus
⇒ Anywhere → CIRCULAR patch with → EXCLAMATION POINT 📷 📷
⇒ SUDDEN onset
PATTERNS of hair loss: 📷
Dgx = clinic
⇒ unpredictable evolution (might regrow or never regrow)
Tx:
→ other topicals tx: immunotherapy (DPC = Diphencipron), minoxidil, cryo



multifactorial (thought to be AUTOIMMUNE) ⇒ destruction of melanocytes
⇒ assoc. with other AI disorders ⇒ 🦋 THYROID!!
- Universalis → whole body
- Generalized
- 🥇 V. vulgaris → multiple lesion in SYMMETRICAL pattern
- Acrofacial v. → Distal FINGER + Facial Orifices (circumferential)
- mixed
- Localized
- focal → few in ONE AREA
- mucosal → ONLY mucous membranes
- segmental → unilat. dermatome
White macules 📷 📷→ well defined, homogenous depigmentation
⇒ in ☀️-exposed areas
⇒ precipitated by stress factors
physical trauma, sunburn, psychological stress, inflammation, pregnancy, contraceptives
⇒ +/- Koebner’s phenomenon

Dgx:
- 🪵 Wood lamp 📷 (rarely histo)

- Workup → 🦋 Thyroid (T4, TSH, Thyroid-Ab)
DDx: → other causes for hypopigmentation (tinea vesicolor, secondary syphilis, post-inflammatory(i.e. chornic lupus)
Tx:
- Pigmentations Promoting
- Phototherapy
- Topical steroids
- Vit D
- Calcineurin-inhib
- Surgery → graft or mini-graft
- Non-pharma → concealer + sun protection
Brown macule 📷 → symmetric on the face
→IRREGULAR border
⇒ Assoc. with 🤰🏽 pregnancy + 💊 oral contracept.
☀️ -exposed areas:
Tx:
- Hypopigmentation drug (hydroquinone, tretinoin, azelaic acid, rucinol, kojic acid)
- Sunscreen
🧬 Genetic disorders
EBS → EB simplex JEB → junctional EB DEB → dystrophic EB
at birth / during early life ⇒ BLISTERS of SKIN + MUCOSA(except: AD dystropic)

- Intraepidermal
- Hands and feet blisters that occur after friction or minor trauma associated with excessive sweating.
- Can be generalized in some patients with a severe phenotype.
- Blisters are localized in the upper layer of the skin (intraepidermal) with hemidesmosomes below.
- Healing occurs without scarring
- Acral (extremities) blistering
- Atrophy
- Dyspigmentation
- Poikiloderma
- Photosensitivity
- Gingival fragility
- Palmo-plantar keratoderma
- Squamous cell carcinoma
- blisters in basement membrane (lamina lucida)
- Severe form - Herlitz: widespread hemorrhagic blisters of the skin and mucosa present at or soon after birth; patients die due to infections and protein loss
- Less severe form - Non-Herlitz: widespread spontaneous or mechanically induced blistering, mucosal involvement, skin atrophy, and alopecia
- Mutation of laminin 332 and collagen XVII
- subepidermal →scarring
- Subtypes:
- EBD AR
- Subepidermal blisters of skin and mucosa
- Extremely fragile skin with large flaccid hemorrhagic blisters
- Shortened life expectancy
- Healing with scars, discolorations, and milia
- Loss of dermatoglyphic patterns
- Severe anemia, constipation, malnutrition, dental abnormalities
- Ulceration and constriction of hands and feet leading to deformities and syndactyly
- Increased risk of squamous cell carcinoma
- EBD AD
- Good prognosis
- Diminished blistering activity with age
- Presence of milia, scars, and nail dystrophy
- No mucosal involvement, normal teeth
- avoid skin trauma
- wound care (dressing, emolients..)
- topical antibiotic & steroids
- Mucosa and Teeth: Consume semi-liquid foods, practice early dental care, and use laxatives if needed.
- Surgical Approach: Consider syndactyly and contractures as potential complications and address them accordingly.
🧬 → ↑ keratinization
⇒ DRY (xerosis)
⇒ generalized desquamatoion ⇒ SCALY skin
- NON-CONGENITAL (→ onset in first months of life)
- CONGENITAL

Vulgaris | X-linked recess. | Non-bullous | Bullous | |
Patho: | AD
(filaggrin mutation [protein that connects keratin]) | X-linked recess
⇒ males
(steroids sulfate disorder) | AR | AD |
Location: | Trunk + Extremities (extensor) ⇒ SYMMETRICAL
(Øflexural, Ø folds) | Face, trunk, extremities | Generalized Erythema | Generalized Erythema
Skin folds (vesicles) |
Palms + Soles | ↑palmo-plantar markings | spared | palmoplantar hyperkeratosis | spared |
Scales | light-gray | dark brown | LARGE yellow brown scales
→ prominent on extens. surf. | FINE yellow scales |
Clinical feautres | → assoc. with :
- follicular hyperkeratosis (keratosis pilaris)
- 🐝 ATOPIC DERMATITIS |
🥜 cryptorchidism, hypogonadism
👁️ corneal opacities
|
🏜️ Hypohydrosis,
💅🏽Nail dystrophy,
🧠 mental retardation |
Macerations + 🎈Blisters
|
Course: | IMPROVE in time (summer+puberty) | PERSISITENT → Øimprove |
- Topical → Keratinolytics + Emolients

- Systemic (if severe) → Retinoids
Dgx criteria → ≥2 of:
- At least 6 cafe-au-lait macules 📷 with diameter > 5 mm at young patients (before 2 puberty) and > 15 mm after puberty
- At least 2 neurofibromas 📷 or 1 plexiform neurofibroma
- Skinfold lentigines (axillary and inguinal)
- Optical Glioma
- At least 2 Lisch nodules 📷
- Bone lesions
- First-degree relative with the NF1
Tx:
🍇 neurofibroma → 🔪 excision
☕ cafe-au-lait → 🧊 cryo / 📡 laser
🦟 pruritus → 🐝 ketotifen (H1-blocker)
- “Clinical features:
- Cutaneous lesions:
- Facial angiofibromas 📷
- Tumors of nail folds (Koenen's tumors) 📷
- Hypopigmented macules 📷
- Cafe-au-lait macules
- Connective tissue nevus ("shagreen")
- Xanthomas
- Lymphangiomas
- Oral lesions: Gingival fibromas, depression of teeth enamel.
- Systemic involvement:
- CNS: Seizures, mental retardation.
- Cardiac: Rhabdomyomas, conduction blocks.
- Renal: Angiomyolipomas, cysts, renal failure, retroperitoneal hemorrhage.
- Ocular: Retinal hamartoma.
- Pulmonary: Lung lymphangiomatosis.
- Malignant diseases: Renal cell carcinoma, aggressive astrocytomas.
- Treatment:
- Removal of facial lesions: Surgery, dermabrasion, laser.
- Anticonvulsants for epilepsy.
- Surgical excision for symptomatic renal, brain, and cardiac tumors.
- Sirolimus or rapamycin for renal hemorrhagic tumors.
- Genetic counseling.”
🦀 Tumors
= benign skin tumor (in contrast to actinic keratosis = pre-cancerous)
⇒ Proliferation of IMMATURE keratinocytes → arise spont.
⇒ OLDER patient (40-50y)
⇒ common location: TRUNK, but can appear anywhere (face, neck, prox. extremities)
1) round PAPULE/PLAQUE → looks “STUCK ON” 📷
- well-demarcated
- dark with irregular surface ⇒ feel WAXY/GREASY
2) LESER-TRELAT signs = “explosive” onset of multiple SK lesions 📷 ⇒ assoc. with 🦀 (esp. gastric adenocarcinoma)
Biopsy: 📷
→ dark epithelial cells in epidermis (similiar to basal skin cells)
→ Keratin-filled cysts = 📯 HORN-CYSTS
Tx:
→ REMOVE → 🧊 Cryo, 🪒 Shave-excision, 🥄 Curretage, 📡 Laser
Malignant tumour development within a seborrheic keratosis (SK) is extremely rare.
→ present at birth
⇒ often with HAIR growing from lesion
Size: small, medium 📷, large or GIANT 📷 ⇒ THE BIGGER THE ↑ MELANOMA- RISK
if 🧠 CNS invovlement ⇒ Neurocutaneous melanosis (large congenital nevi + multiple small nevi + CNS defects (i.e. hydrocephalus)
Tx:
EXCISION (asap, prevent transformation) → several operations incl skin grafting
if SUPERFICIAL → DERMABRASION
- Junctional nevi Growth along dermal-epidermal junction Often found in 🐥 children
- Compound nevi Growth extends into dermis
- Intradermal nevi Loss of junctional lesion Found only in dermis Common in 🙆🏽♂️ adults

- Red-brown, dome-shaped nodule 📷
- Diameter less than 1 cm
- Found on the face or proximal limbs in children and young adults
- Appears gradually over a period of weeks to months
- Pale halo nevus: Nevus that develops a pale halo suddenly without an evident trigger, such as sunburn.
- Central nevus: The central nevus can either disappear or survive the immunologic attack.
- Repigmentation: Over time, the nevus may experience repigmentation.
- Ø Tx needed.
- Numerous small, dark papules and nodules on a light-brown patch on the trunk.
- Ø Tx required
- Small, blue-gray, sharply circumscribed, firm papule
- Usually present for many years
- Can be found on any body region, particularly acral areas
- Ø Tx necessary
- Very common skin types I and II
- Strong familial tendency (tendency to develop sunburns)
- Melanocytes in freckles produce more melanin, package it in larger melanosomes, and transfer it more efficiently to keratinocytes
- More apparent in the spring and blanch over the winter
- Flat tan-brown macules with irregular/bizarre borders
- Wide variation in size
- Typically found on the face, arms, shoulders, upper parts of the back, and lips
- Appears in childhood and tends to regress in older people
- Histopathology shows an increase of melanin in the basal layer
- Sunscreens are the recommended approach
- Large, oval, light-brown macules or patches, several cm to many cm in size
- Uniform color and smooth-rounded border
- Permanent skin lesions
- Seen in neurofibromatosis (≥6 lesions) and 10-15% of normal fair-skinned individuals
- Ø Tx required, laser therapy can be an option
- Location: Face, neck, upper part of the chest
- Large dilated follicle, usually dark, sometimes expanded into a cystic structure
- Treatment: Excision
- Clinical findings:
- Solitary, skin-colored lesion with a folded surface, often with a stalk, measuring mm-cm
- Multiple lesions - smaller, few mm in size
- Neck, axillae, groin, submammary region - overweight individuals
- Histopathology: Papillomatous acanthotic pattern; the dermis is normal
- Therapy: Tangential/scissors excision

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:max_bytes(150000):strip_icc()/plantar-warts-resized-56a315a85f9b58b7d0d04d6f-85edcc610ada498f887d524e00b8f7d2.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:max_bytes(150000):strip_icc()/pityriasis-versicolor-pink-07468ea10f4f40248ff14b593ef64787.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:max_bytes(150000):strip_icc()/VWH-DermNet-AllergicContactDermatitis-01-b5f408ff86a84e429ea924b2cbdda931.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:max_bytes(150000):strip_icc()/VWH-DermNetNZ-StasisDermatitis-01-9613e86280f549089b034145204c3a83.JPG){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:max_bytes(150000):strip_icc()/discoid-lupus-12-d036a1f968a746eca02378151c9f3db1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:max_bytes(150000):strip_icc()/3133-alt-7cf9740ed8ae46029426504e90c64b0a.JPG){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
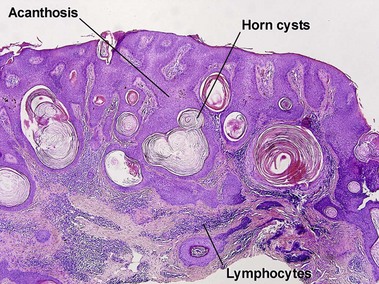{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
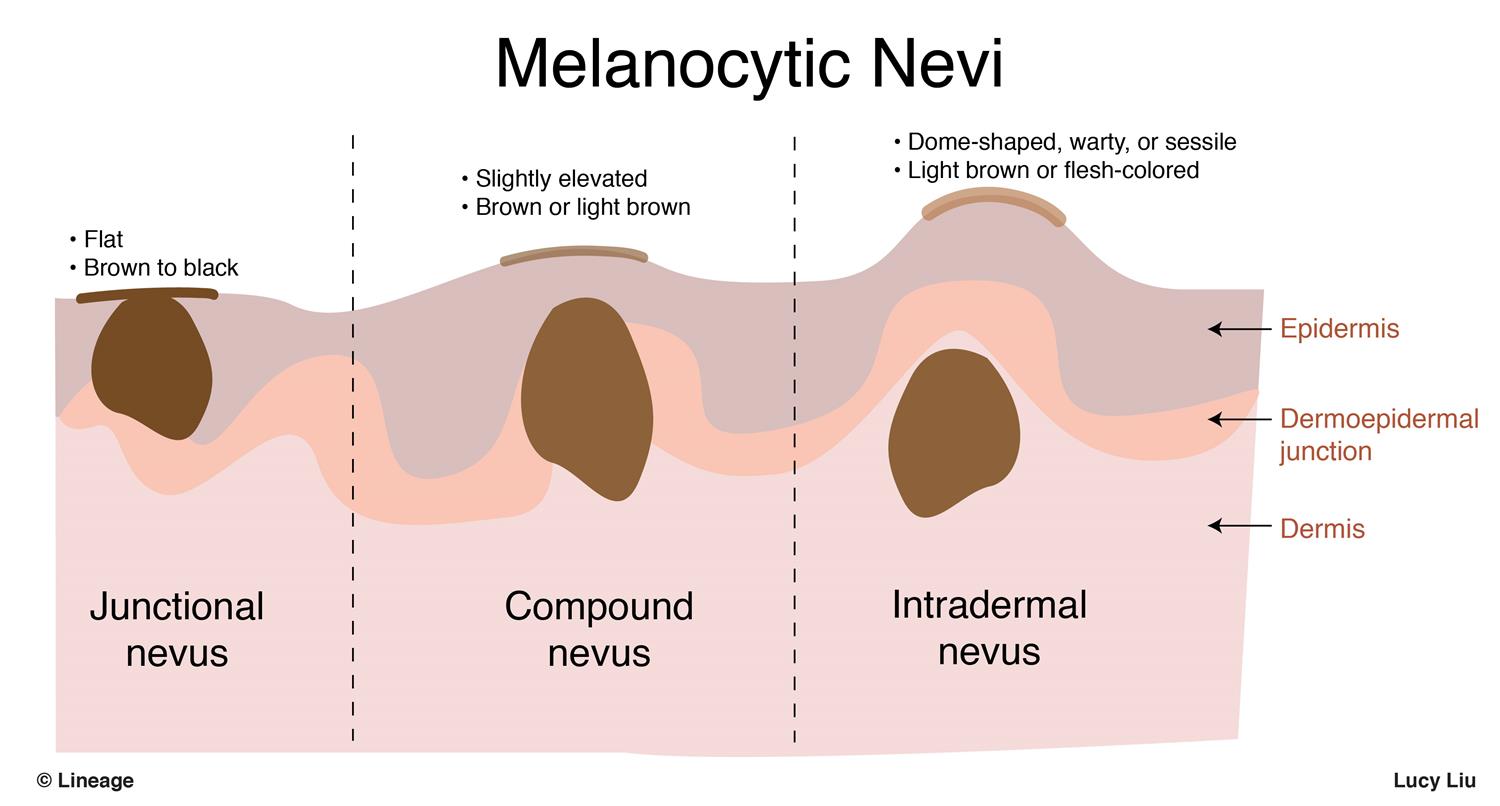{kind=link}
{kind=link}
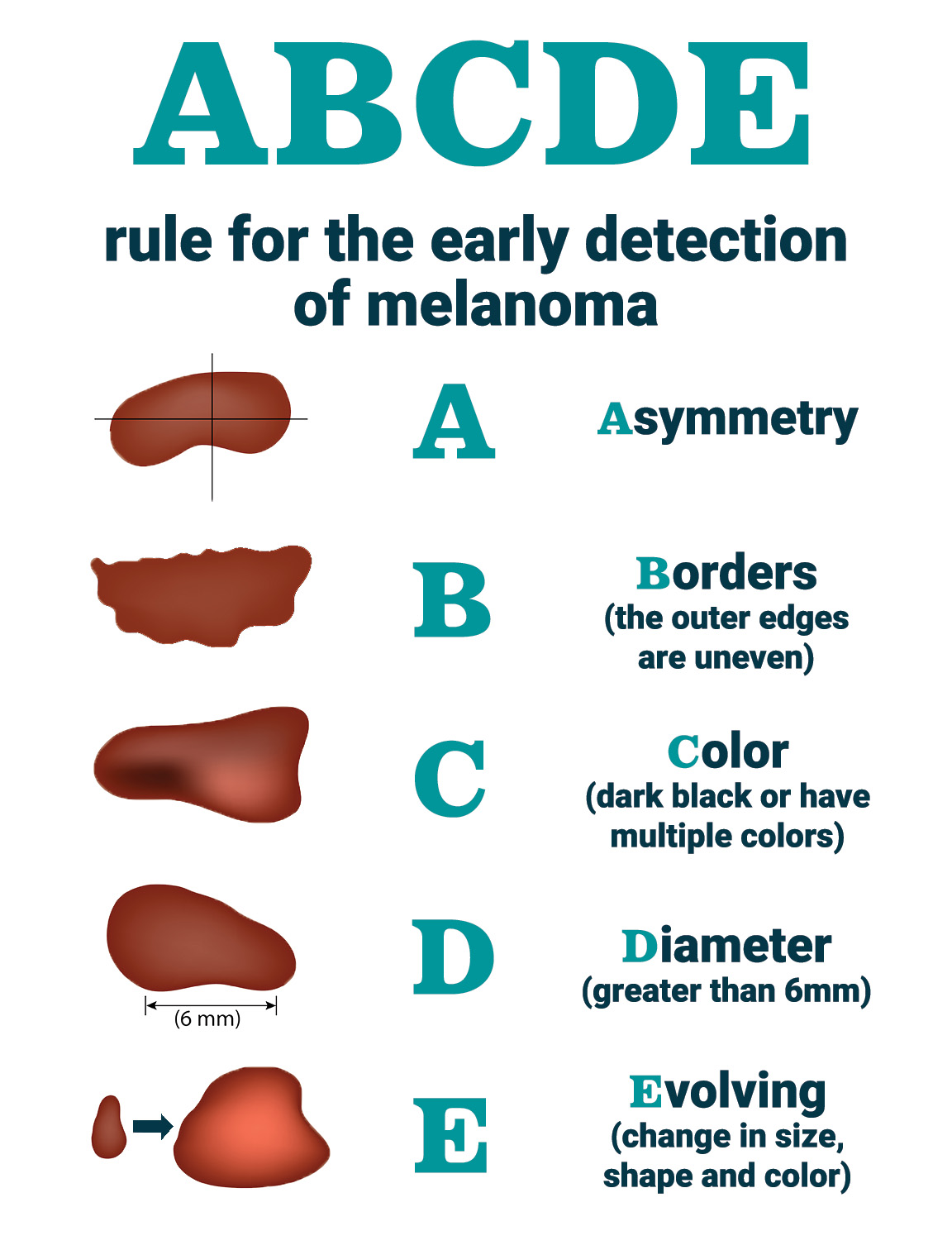{kind=link}
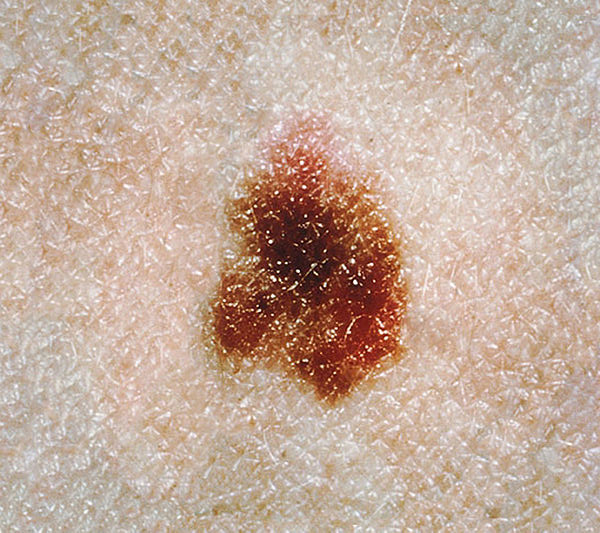{kind=link}
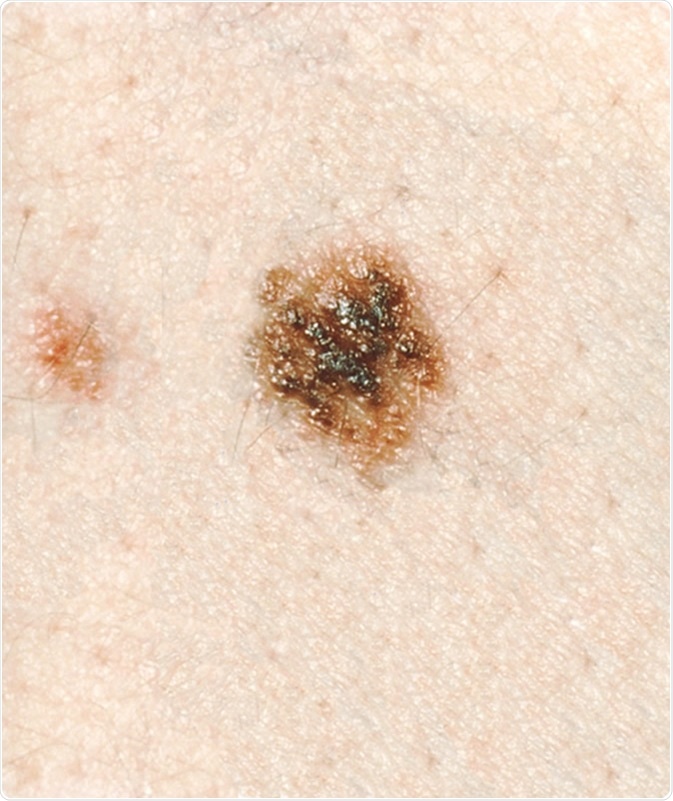{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
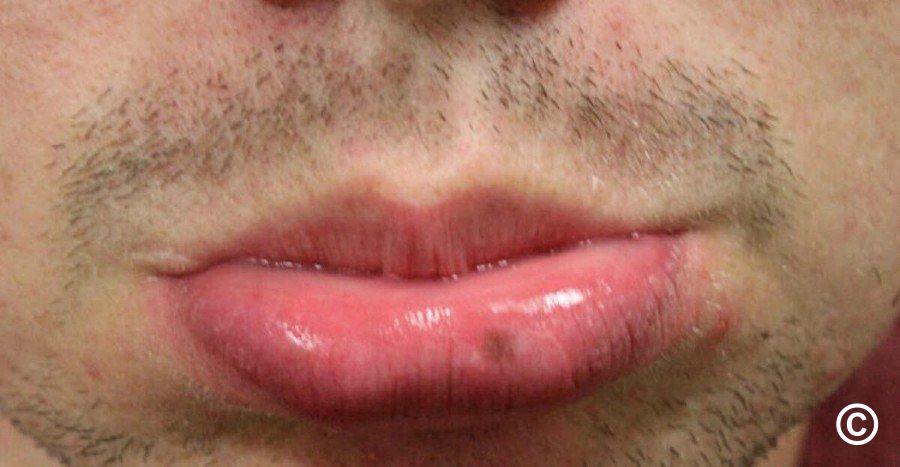{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:max_bytes(150000):strip_icc()/GettyImages-1323172866-a89d795cc9124a54ad75c7fcdb48847a.jpg){kind=link}
{kind=link}
- Clinical findings: Poorly defined tumor with a compressible slightly bumpy surface, usually located between the skin and subcutaneous fascia on the shoulders, over the ribs, on the back, and extensor surfaces of the forearms.
- Lipomatosis: Multiple lesions are observed, often associated with neurofibromatosis and other syndromes.
- Differential diagnosis: Cysts, which have a central pore and smooth surface.
- Therapy: Surgical excision is the recommended treatment.
{kind=link}
{kind=link}
- Most common cutaneous neural tumor
- Multiple lesions - associated with neurofibromatosis
- Clinical findings: Molluscoid nodules (soft nodules with or without central umbilication) that raise above the skin surface, can be pushed back into the skin, large firm or pedunculated
- Ø Tx or excision if necessary
{kind=link}
benign CAPILLARY proliferation/hemangioma (+most common vasc. malformation)
⇒ middle-aged/eldery (↑with age)
1) MULTIPLE red-violet DOME-SHAPED lesion → on TRUNK
→ May BLEED from trauma
Ø Tx needed
→ if cosmetic concern → remove ( laser, excision, electrosurgery)
{kind=link}
{kind=link}
LOBULAR CAPILLARY hemangioma
⇒ HYPERPLASIA of blood vessel to GROWTH STIMULI:
- Pregnancy → 👄 Gingiva
- Trauma (→fingers, palms, face, scalp etc)
- Soft + FRIABLE red PAPULE/NODULE (diameter <1cm) +/- stalk
if stalk: might bleed profusely
- w/ pale EPIDERMAL COLARETTE (surrounding skin at base)
DDx: Amelanotic melanoma
Tx:
- gingiva → regress spontaneous
- other lesion → REMOVE (excision, laser)
{kind=link}
excess proliferation of blood vessels in NEWBORNS (appears during first weeks of life or present from birth)
grows in the first month → REGRESSES (over 2-10y)
RED/VIOLET NODULAR or flat circumscribed
→ RUBBERY surface ⇒ SMOOTH or LOBULATED📷
{kind=link}
→ can be compressed (blanching)
Tx:
- Uncomplicated → WATCH + WAIT
- severe → SYSTEMIC: 🌝steroids, 🎺 BB (propranolol, atenolol)
- drug refractory → 📡 Laser (stops growth)🔪 surgery🧊 cryo
(Ø vascular tumor, but CAPILLARY MALFORMATION)
- Nevus simplex (stork bite, birth mark) 📷
- capillary malformation often eyelids or back of neck
- pink/red macule
- in up to 60% of infants → disappears in first few years
- Nevus Flammeus (Port wine stain) 📷 → Sturge-Weber syd
- dermal capillary + venule malformation
- unilated, blanching
- NO regression + grows with child growth
- Salmon patches
- Present at birth
- Locations: glabella, eyelids, nape of the neck
- Frequency: 1/3 of the neonates
- Persistence:
- Neck: persist for life
- Facial lesions: fade or disappear by the age of 2 years
{kind=link}
..jpg){kind=link}
☀️ → ATYPICAL keratinocytes ⇒ 🦀 SCC

Round, red/brown lesions on ☀️-exposed areas

with HYPERKERATOTIC CRUST
VARIANTS with ↑↑🦀-RISK:
⇒ 👄 ACTINIC CHEILITIS 📷 → LOWER lip, crust, scales, fisures
{kind=link}
⇒ 🦏 CUTANEOUS HORN 📷 → HYPERTROPHIC AK or invasive SCC → 🔪 excision
{kind=link}
Biopsy: HYPERKERATOSIS, Epidermal cell DYPLASIA, PARAKERATOSIS
Tx:
1-5 lesions → CRYO (with liquid nitrogen)
≥6 lesions → 5FU, Imiquimod, 📸 Phototherapy
Imiquimod is a topical immune response modifier that works by activating immune cells such as dendritic cells and macrophages. The mechanism of action (MOA) of imiquimod can be described as follows:
- Imiquimod binds to specific receptors on the surface of immune cells, which leads to the release of cytokines, such as interferons and interleukins.
- The cytokines stimulate an immune response, including the activation of T cells, which then attack and eliminate the targeted cells.
- This immune response results in the destruction of virus-infected cells, cancer cells, and abnormal skin cells.
Genital warts: Imiquimod is used to treat genital and perianal warts caused by the human papillomavirus (HPV).
Actinic keratosis: Imiquimod is used to treat actinic keratosis, which is a precancerous condition that affects the skin.
others
- Topical retinoids
- Diclofenac gel
- Facial peeling
- Laser therapy
{kind=link}
{kind=link}
☀️sun-exposed areas (face, trunk)→ Ømucous membranes
WAXY, PINK, “PEARLY” papule/nodule 📷
{kind=link}

→ +/- TELE-ANGIECTASIS 📷
{kind=link}
→ +/- 3) central ULCERATION → CRUST 📷
{kind=link}
→ +/- “ROLLED” BORDERS (rounded + thickened, sometimes pearl-shaped) 📷
- ULCERATIVE 📷 : NON-HEALING INVASIVE
- Tendency for ulceration and destructive growth
- Ulcerative onset (clean-red, covered by purulent secretion)
- Location: Nasolabial fold, medial canthus, the ear in the evolution of a nodule
- Ø pain
- severe form = ULCUS TERBRANS 📷 → tissue destruction
- SCALING PATCH/PLAQUE = SUPERIFICAL / Pagetoid 📷
- Erythematous, crusted patches (1 or multiple)
- Slow growth rate
- Size ranges from a few millimeters to several centimeters
- Rare ulceration
- Pearl-like papules or fine hypopigmentation band at the periphery
- Typically found on the trunk and extremities
- CYSTIC 📷→ translucent, broad base, fine teleangiectasis, bluish-whitish, → eyelid+cheeck
- MORPHEA- / SCLERODERMI-FORM 📷→ atrophic scar, teleangiectasis → ↑↑aggressive
- PIGMENTED 📷 📷
- Melanin pigmentation of tumor and stromal cells
- Pearly border and telangiectases present but difficult to see
- Nevoid (Gorlin-Goltz synd) 📷 📷
- Multiple BCC (basal cell carcinoma)
- Early onset in the second or third decade of life
- Palmoplantar pits
- Large skull with frontal bossing
- Hypertelorism (widely spaced eyes)
- Enlarged mandible
- Acral epidermoid cysts
- Odontogenic keratocysts in the mandible and maxilla
- Calcification of the falx cerebri
- Medulloblastomas of the cerebellum
- Ovarian fibromas
⇒ slowly growing + invasive, rarely mets +recurr. → most of BCC found early + excised

DDx:
- SCC, Melanoma
- Variants & pre-malignant: Actinic keratosis, Keratoacanthoma, Bowen’s
- Seborrheic keratosis
- Lichen planus
- Morphea (localized scleroderma)
Biopsy: Palisading nuclei (aligned: cells at periphery of nest line up parallel) 📷 📷
{kind=link}
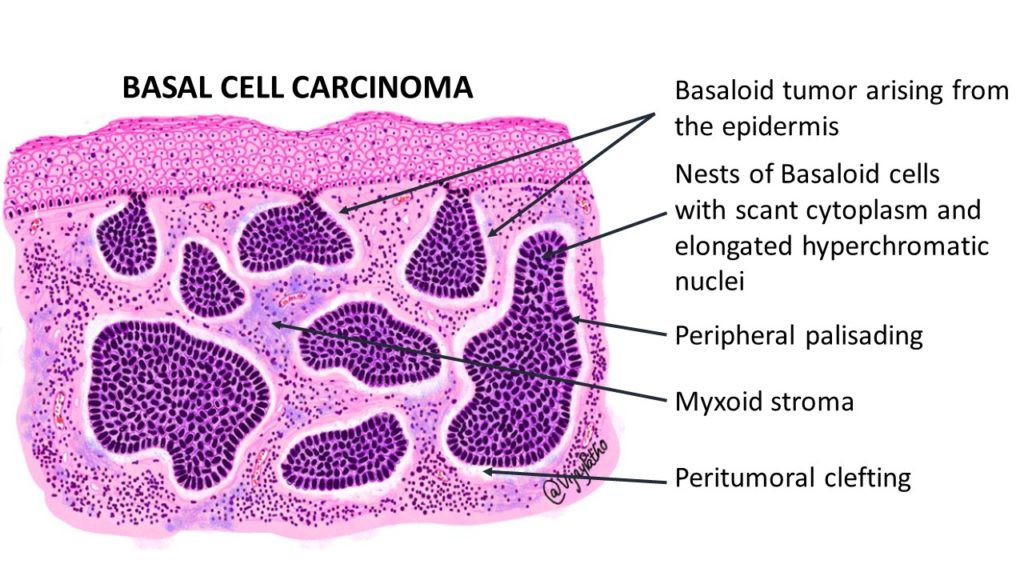{kind=link}
Tx:
high risk ⇒ EXISION (margin 3-5mm) or Mohs surgery 📷 (if 👃🏽👁️💆🏽♂️ 🦻🏽 special sites + sclerodermiform)
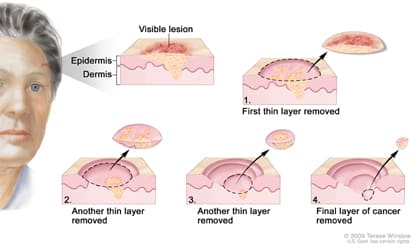{kind=link}
High risk: Large Recurr Specific location decr immunity

alternative: RT, chemo, cryp, electrocautery, laser, phototherapy
mets, recurr, Øexcise → VISMODEGIB
{kind=link}
{kind=link}
🧓🏽 older patient
risk factors: sun-exposure, ↓immunity, chronic skin inflammation, arsenic exposure
RED PLAQUE with SHARP BORDERS + SCALES
→ ULCERATION, BLEEDING, CRUSTING
→ location: ☀️exposed areas → face, LOWER lip, ears, hand

- Lower lip:
- sun exposure
- smoking
- Oral mucosa:
- Previous lesions (Glossitis, Oral lichen planus, Leukoplakia
- HPV infections
- smoking
- Penis:
- HPV infections
- Chronic inflammation (lichen planus, lichen sclerosus)
- Smegma
→ COMPRESSION → extrusion YELLOW WORM-LIKE MASSES (keratotic cells)
⇒ RAPID GROWTH ⇒ invasive, may spread to LN, rarely mets(but still more common than in BCC)
Biopsy: Keratin pearls 📷, atypical keratinocytes 📷
{kind=link}
{kind=link}
DDx:
- BCC, Melanoma (amelanotic)
- Variants & pre-malignant: Actinic keratosis, Keratoacanthoma, Bowen’s,
- Seborrheic keratosis
- Lichen planus,
Tx = 🔪 EXCISION (margin: 4-20mm)
alternative: RT (Øchemo → only palliative)
if small/low-risk → cryo, electrocoagulation, curretage
{kind=link}
benign tumor from hair follicles → self resolving (usually)
DOME-SHAPED NODULE → w/ CENTRAL HYPERKERATOSIS
⇒ RAPID GROWTH (weeks) ⇒ REGRESSION, sometimes aggressive
Tx: Follow up or surgery
{kind=link}
RED PLAQUE → WELL-DELINIATED + CRUST
(if ulceration or nodule → invasive)
Tx:
- REMOVAL → Excision, Cryo, curretage, electrocautery
- alternative: RT, laser
- TOPICAL → → 5FU, Imiquimod

{kind=link}
{kind=link}
{kind=link}
risk factors:
- ☀️ (esp. burns during childhood)
- 🦦 nevi → dysplastic or multiple (25% of melanoma develop from pre-exist. nevi)
- 🐻❄️ Light-sensitive skin types
1) ⇒ ABCDE

- 🥇 SUPERIFICIAL SPREADING (70%) 📷 ⇒ horizontal/radial growth in epidermis + upper dermis (→ vertical later)
- 🥈NODULAR (15-30%) 📷 ⇒ vertical growth !! (black, blue, pink-red ⇒ ulcerative + hemorrhagic nodule )
- 🦥 LENTIGO MALIGNA (large freckly)📷 → LENTIGO MALIGNA MELANOMA (>15%??)
- 🦶🏽 ACRAL LENTIGINOUS 📷 📷→ in DARK SKINNED: Palms, soles, under nail
- AMELANOTIC 📷 📷 ⇒ the “GREAT IMITATOR”: melanoma WITHOUT DARK pigment

⇒ SLOW growing → elderly; spreads darkens, becomes lump
→ Evolution is important
- 👁️ occular + 👄 muscous membranes melanoma

⇒ estimate RISK of METS 🫁 🍑 🧠= BRESLOW THICKNESS

the deeper the depth of tumor ⇒ higher risk of mets
Dgx: DERMOSCOPY 📷 + Biopsy 📷 ⇒ nest of melanocytes, atypical cells
{kind=link}
{kind=link}
- Excisional biopsy: performed with a 1-3 mm safety margin
- Incisional biopsy: used for specific anatomical areas (face, palms/soles, fingers, ear) or large lesions
- Shave-excision: suitable for lesions with a low degree of suspicion
TUMOR MARKER: S100, LDH, MIA
⇒ TNM workup
- LN (N) workup:
- Clinical examination
- Ultrasound of lymph nodes
- Sentinel lymph node technique
- Total lymphadenectomy
- Mets (M) workup:
- Clinical examination
- Laboratory assessment
- Abdominal echography
- Chest/bone radiography
- Bone/liver scintigraphy
- EEG
- CT, MRI, PET-CT
DDx:
- Nevus
- BCC
- actinic keratosis
- benign lesion
- seborrheic keratosis
- pyogenic grnauloma
Tx:
- EXCISION ⇒ WIDE margins
- stage 3 → Lymphadenectomy + adjuvant
- stage 4 → + RT + SYSTEMIC (Chemo, Targeted, Immuno)
- If V600E mutation ⇒ BRAF-inhibitors → Vemurafenib + Dabrafenib
Follow-up: 3m → 6m → yearly (all life)
{kind=link}
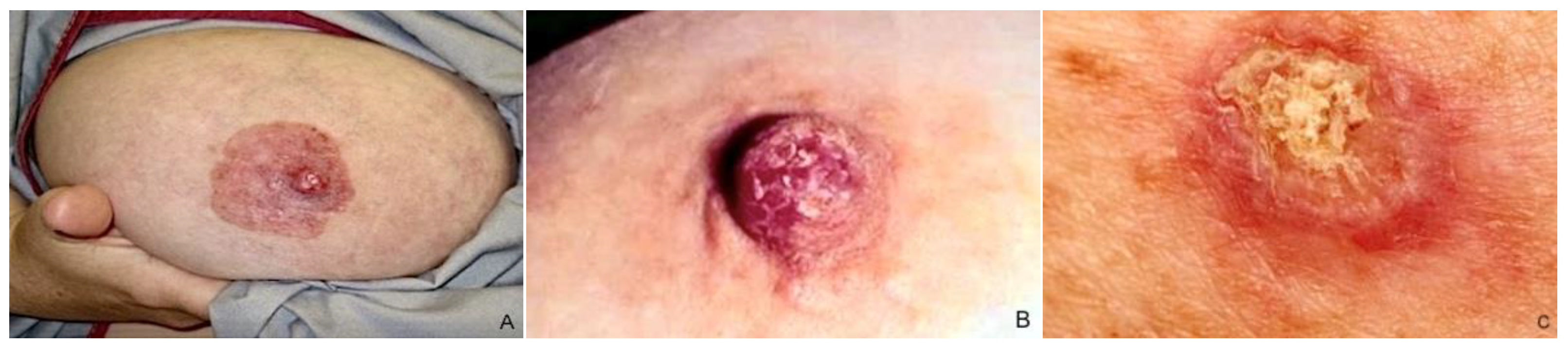{kind=link}
= Epidermal METASTASIS of AdenoCa
red, well-demarked, SCALING PLAQUE → expands slowly
→ becomes ERODED → covered with CRUST
TYPES:
1) Areola (unilat. padgets d. of the breast) ⇒ primary tumor = BREAST
2) Extra-mammary = PRIMARY or SECONDARY (rectal, gallbladder, urethra, cervix, prostate)
Dgx: Biopsy = intra-epithelial AdenoCA
Tx: underlying Tumor or wide EXCISION if Øtumor found

- Patch stage 📷
- Slowly growing round, oval, serpiginous, or polycyclic well-demarcated, red-violet patches
- Hypopigmented patches (in dark skin types)
- Fine wrinkling centrally and scales
- first asymptomatic, then uncontrollable itching
- Site: trunk, buttocks
- Plaque stage 📷
- Pre-existing patches infiltrated or new thicker lesions arise
- Sharply bordered, slightly elevated irregular plaques, red to violet or red-brown
- Expansion of lesions is slow and they increase in thickness
- Alopecia may be present
- Pruritus (itching) can occur
- Lymphadenopathy often observed
- Tumor stage 📷 📷
- End stage: large, thick tumors develop, either within pre-existing lesion or de novo
- Rapid growth, red-brown color, ulcerated
- Facial involvement: "leonine facies"
- Signs of systemic disease: lymphadenopathy, bone marrow infiltration, other organ involvement
- Severe, intractable pruritus
Clinic + SEQUENTIAL biopsies 🔪 + other paraclinic

- RT + chemo
- Topical
- Anti-neoplastics (bexarotene, nitrogenmustard, carmustine)
- 🌝 steroids
- Phototherapy
- rare
- in elderly patients
- ☠️ death in 2-3y
{kind=link}
{kind=link}
3) Palms + Soles: HYPERKERATOSIS 📷 + nail dystrophy
{kind=link}
4) Alopecia
5) ↑LN
Dgx:
- CLINIC
- BIOPSY (sezary cells 📷) + other paraclinical

- Paraclinic assessment:
- Immunophenotype and T-helper profile
- Molecular biology (monoclonal, identical T-cell population in skin, blood, and lymph nodes)
- Laboratory cell analysis (leukocytosis, lymphopenia, presence of Sezary cells)
DDx: drug reaction
Tx:
- EXTRA-CORPREAL PHOTOPHORESIS
- retinoids, phototherapy
- chemo