




Pharmacology II

🫁 Respiratory System
→ 📷
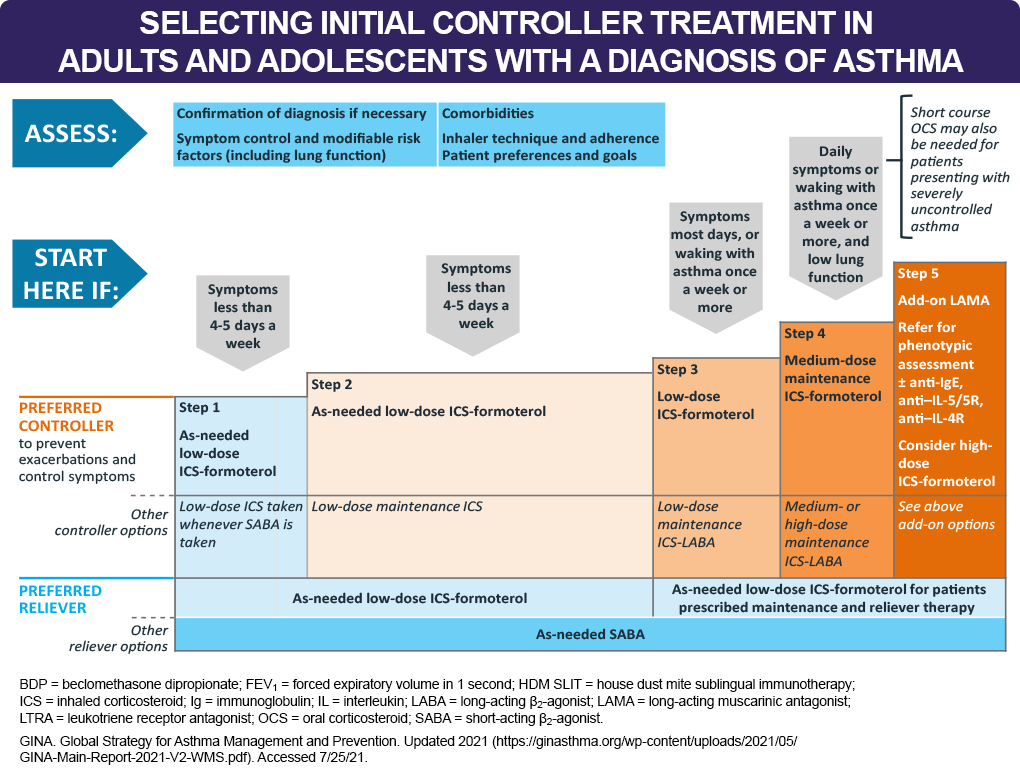
- intermittent
- mild Persistent
- moderate persistent
- severe persist.
- status asthmaticus

- short acting b2 agonist (salbutamol/albuterol)
- systemic steroids (methyl-prednisone oral or hydrocortisone i.v.)
- anticholinergics (iptratropium bromide)
- Methylxanthines
+Epinephrine
→ 📷
- Inhaled steroids (fluticasone/budesoide)
- Long acting b2 agonist (salmeterol/formoterol)
- Leukotriene Modifier (Montekast; Zileuton)
- Theophylline
- Systemic steroids
MABs (Omalizumab) (+ Chromes)
Allergen specific immunotherapy
H1 antagonists
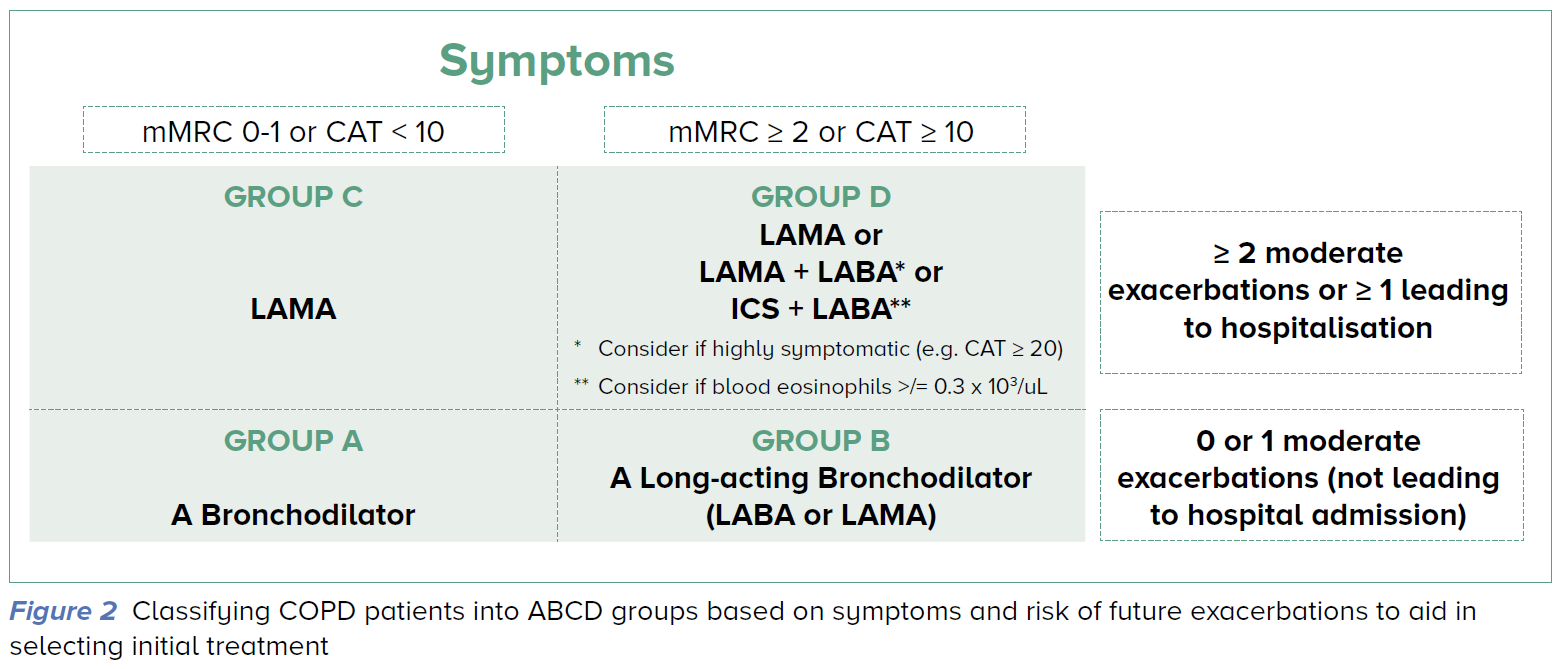
spirometry:
Post-bronchodilator FEV/FVC < 0.7
assessment of airlow limitation
Grade | FEV (% predicted) |
GOLD 1 | ≥80 |
GOLD 2 | 50-79 |
GOLD 3 | 30-49 |
GOLD 4 | <30 |
SABA + SAMA
steroids
(theophylline i.v.)
(AB if purulent sputum)
T
↑cAMP (via adenylyl cyclase stimulation) → ↓Ca release 📷 → SM relaxation
FFFF → thats why steroids are needed
↓R activity (downregulation) + tachyphylaxis
inhaled
- severe persistent asthma
- children
- short (4-6h)
- long, (8-12h)
- ultralong (12-24h)
exacerbation of asthma + COPD
Controllertherapy
in asthma (+ICS)
COPD ( mono or with LAMA/ICS → see above)
(exception: Formoterol combination can be given in exacerbation)

COPD
usually not → but sometimes if high doses or systemic administration!
- Heart -tachycardia -palpitation, -arrhythmias
- Skeletal muscles -tremor -muscles cramps
- CNS -headache -anxiety
salbutamol
2 puffs PRN, 3-5min interval; Ømore than 8 puffs/day
Terbutaline
Dont disTERB me while sniffing The BUTtER-LINE
status asthmaticus
(when refractory to classic treatment - salbutamol)
Fenoterol (another SABA)
(1) Salmeterol
(2) Formoterol
(Salute ∝ Salmeterol)
(Formation ∝ Formoterol)
controllertherapy in asthma + copd
(+/- together with ICS)
formoterol + ICS (budesonide/beclomethasone)
→ can be given in exacerbation + controller therapy of asthma
Formoterol can also be with SAMA in COPD or bronchitis w/ spasm
COPD
Antimuscarinic (LAMA) or steroids (ICS)
- Indacaterol
- Olodaterol
- Vilanterol
- Carmoterol
"Carmo + Krooked sagen Ola zum Villain Inder-Kater"
(Carmo + kooked = ultrageil = ultralong)
block m1 + m3 📷 → bronchodilation + ↓mucous secretion (via vagus)
- COPD #1 exacerbation (SAMA) + controller ( LAMA (+SAMA in A))
- Severe asthma attacks (SAMA)
- Persistent asthma (+b2)
short: ipratropium bromide
long: tiotropim bromide
↑hyperreactivity after treatment stop
(+antimuscuarinic symptoms)
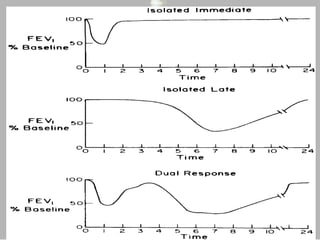
early + late
(1)Non-selective PDE inhibitor
(2) Adenosine receptor antagonist
(3) Histone deacetylases activitation
(∴ ↑ cAMP)
⇒ Bronchodilation
⇒ + anti-inflammatory effect:
inhibits NF-kB translocation, increases IL-10 release, Anti-oxidative, Induces apoptosis of neutrophils and eosinophils)
- CNS stimulation
- Diuretic effect * → ↓Preload
- ↑HR
☕
oral + IV!
iv → asthma + COPD reliever
oral → asthma + (COPD controller)
MAINLY RELIEVER THERAPY never 1st line
(CAVE: narrow therapeutic index! → more of a last resort)
genetic + environmental factors → means inter-personal variability (→ not really predictable)
(1) CNS effects incl. tremor (+agitation, insomnia, seizures)
(2) Tachycardia + Arrhythmias
→ like to much coffee
hypotension (↓preload + ↑HR→ ↓output)+ seizure (refractory; due to ↑CNS)
chest pain + death (heart affected)
>20
seizures (more prone than acute tox)
prophylactic diazepam (2nd line: barbiturate)
- Epilepsy
- Acute MI + IHD
- Hypertension
- Cave: elderly + newborns
- tea/coffee consumption
Amino-phylline
(1) ↓ Inflammation (2) ↓ Leukocyte infiltration (Importantly, they also upregulate (2 receptors)
T (alone or in combination)
severe + freq. exacerbation (Stage D)
- oral + iv → asthma exacerbation
- iv → status asthmatic, patient is vomiting
- Systemic → COPD exacerbation
- oral → controller in chronic severe asthma (step 5)
oral → methylprednisolone + prednisone
iv → hydrocortisone, methylprednisolone sodium succinate
T
T
- oral candidiasis
- dysphonia
- ↓bone density
- Fluticasonide
- Budesonide
- Flunisolide
- Controller - asthma
- alternative for ICS in NSAID induced asthma

- asthma + allergic rhinitis
LTBA (IL-8 also potent neutrophil chemoattractant. IL-8 looks like IL-B)
LTC4, D4, E4 (Also ↑ Airway vascular permeability and mucus production)
CysLT1. (= Leukotriene receptor)
receptor for LT-D4, -C4, -E4. 📷
Montelukast + Zafirlukast
- Systemic Eosinophilia
- Vasculitis (Churg-strauss)
- Neuro-psychiatric symptoms
esp. in children
nightmares, sleep disturbance, mood disorders, aggressive behavior
Monte ist verrückt rot und reitet auf nem strauss
Zileuton
↓LT A4,B4 + C4,D4,E4
(sie läuten an den Dino-Eiern)
↑Liver enzymes (hepatotox)
Aspirin (NSAIDs in general)
inhibition of COX shifts the AA metabolism to the LOX leukotriene pathway (exaggerated in aspirin-induced asthma)
Mild-moderate asthma persistent
On Mast cells:
↓Histamine release by mastcells
💪 stabilizing mast cells ( ↓ mast cell “degranulation”)
↓bronchial hyperreactivity in (long term)
F → early + later
T
Methylxanthines
inhaled
- lungs: cough + bronchospasm
- more above: laryngeal edema + bitter taste
- headache + nausea
Farbe zu Inhalieren schadet Rachen, Lungen und Kopf
Omalizumab
→ bindings prevents mast cell sensitization (IgE cant bind to mastcells → no degranualation)
moderate - severe persist. asthma (controller)
s.c. (every 2-4weks)
F → well tolerated
children <6y
(Nimm keine Süßigkeiten von Omas an)
Benralizumab
Mepolizumab, Reslizumab
Severe eosinophilic asthma
sc or iv.
administer allergens → progressive dose inc.
(for houst dust mites)
asthma PLUS allergic rhinitis
sedation
Cetirizine, Loratadine
asthma→ prevention of this progression is one Tx goal
H1 antihistamines 2nd gen (orally or nasaly)
Corticosteroids (intranasal)
- Leukotrien modifier → asthma + allergic rhinitis
- Alpha 1 agonist → acute rhinitis (cave: tachyphilaxis)
(+antimuscarinics + chromes)
T
intermittent + persistent
- EPistaxis
- candidiasis
Budesonide, Fluticasone
(→ inhalatory)
- 🐝 H1 antihistamines
- 🦥 Antimuscarinics *

- 🌨️ Mast cell degranulation inhibitors (Chromes)

- 🎽 Leukotriens modifier

stimulation alpha1-R → vasoconstriction
acute episodes of allergic rhinitis → produce tachyphylaxis + rebound congestion
- Systemic → Sympathetic symptoms (↑CNS, ↑BP, ↑HR)
- Long term → atrophic rhinitis 📷
Pseudoephedrine
in mild intermittend → h1-antihistamines, decongestant
rest → + steroids, chromes +- Leukotrien inhib(if asthma)
⇒ 📷
CNS → ↓cough reflex
(some also periph → ↓sensitive receptor on bronchial mucosa)
DRY COUGH
⇒ BUT FIND UNDERLYING CAUSE!! (more important)
CNS → mu-R stimulation → ↓cough
also periph. effect
T
- Respiratory depression
- Constipation
- Bronchospasm
- Dry bronchial secretion
- ↓ciliary acitivity
- dependence
- Respiratory failure
- ASTHMA (bronchospasm!!)
- Children <12
Oxeladine 📷
CNS but ↓SE
- no sedation, analgesia
- no respiratory depression
- no constipation
- no dependance
N-acetylcystein (NAC)
- reduce the disulfide bridges that bind glycoproteins to other proteins (such as albumin and IgA) 📷
- act as antioxidants → reduces airway inflammation
- Ac + chronic bronchitis
- COPD
- Acetaminophen (Paracetamol) intoxictation
- Cystic fibrosis
Bronchospasm + GI
- Diarrhea
- Nausea+vomiting
- ASTHMA
- unconcious patient (cant cough out)
🫀 Cardiovascular System
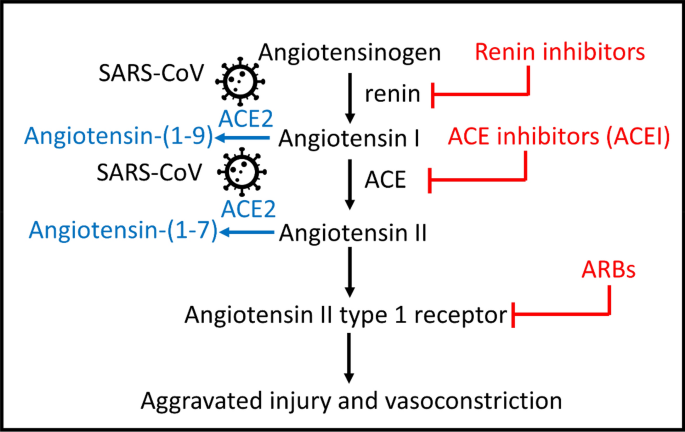
"-pril"
Inhibits ACE (→ Ø Angiotension I into II) 📷
↑Na/HCO3 in PCT
indirect also via aldosteron → ↑Na/↓K exchanger

(1) Dilate efferent (and a little afferent) arteriole
⇒ ↓ GFR

⇒ ↑renal blood flow

(4) ↓ Aldosterone release + ↓ADH
⇒ ↓ Na+/HCO3- reabsorption in PCT
(6) On myocardium + vessels→ antiproliferative + protective

(7) ↓Sympathetic tone + ↓Catecholamines
(8) General ↓vasoconstriction (exception see below)
⇒ ↓BP,
⇒ ↓pre- + afterload
⇒ improved cardiac function
ACEi have Ø influence on cerebral + coronary blood flow
(1) Heart failure (with EF <45%) #1 line therapy

(2) Myocardial infarction + Stroke


(3) Hypertension #1 line therapy
(4) Diabetic nephropathy
(5) Patients with high CV Risk (w/o ventricular dysfunction)

Yes
(By inhibiting AngII mediated cardiac remodeling)
Albuminuria with BP >130/80
Dry cough (Due to increased bradykinin → lung irritation)
Fainting
(Sudden drop in AngII ⇒ Vasodilation ⇒ Syncope)
Hyperkalemia
(1) ↑ Creatinine
(2) Hyperkalemia
- Bilateral renal artery stenosis
- ↓Na + Hypovolemia

neutropenia
in patients with collagen or renal disease
rash
metallic tase
Hereditary angioedema (C1 esterase deficiency) or personal history of angioedema
No, teratogenic 🕷️
- Bilateral renal stenosis
- Chronic renal insuff → with Crea>3 mg/dl
>6 mmol/l
NSAIDs → afferent arteriole vasoconstriction
K sparing diuretics → ↑risk for HyperK+Hypotension
other diuretics → ↑risk for Hypotension (precaution!)
K-salts
- Mild Hypotension
- chronic renal insuff but Crea<3 (dose reduction might be necessary)
- HyperK but K<6
- If given together with diuretics + alcohol → hypotension
- BP
- Elektrolytes
- Crea
T
→ ↑after a fews days (if hospitalized)
→ ↑in week intervals (if ambulatory)
"Der Chef von Pril-Mann (Filmann) ist El Capto (Der Captian).
El Capto (Captain) sagt: "Eh, Nala, Foss I no an"
- Capto-pril group
- Enala-pril group
- Fosino-pril (phosphor group)
they are grouped according to their chemical-bond

- Capto-pril
- Zofeno-pril
"El Capto ist ein großer Zoo-Fan"
capto 2-3doses /day
zofeno single dose
zofeno ⇒ produg
zofeno ⇒ lower dosage needed
Enala-pril
Lisino-pril (=2nd generation ACEi)
Rami-pril
"Weil der Captain (E)Nala nicht anfassen will, geht Nala zu Lissi und Rami.
- long T1/2
- single administration / day
- prodrug
50-100 mg/d (2-3 doses)

Weil El Capto so ein Tier-Fan ist, jagt er manchmal mit einem Lasso und einer Tasse bewaffnet eine Sau.
(Major-System Code)
5mg
30mg
"Der Captain sagt: Alle anderen sind Mäuse"
Zofeno 30 (in HT maitenance)
Enala 10-40
Lisino 5-40
enalapril
Nala wickelt Lissi und Rami mit ivy (Efeu) ein
"-sartan"
Block Angiotensin-II R Type 1. 📷
⇒ Vasodilation + ↓BP
- AT1 - mainly in vessels and myocardium, but also in the brain, kidney
- AT2 - in the suprarenal gland, kidney and CNS, involved in vascular proliferation
→ ARBs - higher affinity for AT1 receptors compared with AT2
- ARBs more in AT1-Receptor deactivation (Angiotensin II is also activated through alternative routes by blocking only ACE)
- Activation of AT2-Receptor still possible
- ØInfluence on Bradikinin (↓cough) 📷
See ACEi
F → maximal effect after 3-4weeks
F, same efficacy
ARBs
same indication:

- HT (moderate-severe)
- Post-MI
- Cardiac failure
- Diabetic nephropathy
- Patients with arterosclerotic CV-Disease (second. prophylaxis)
exceptions:
- only post-MI not acute MI
- Cardiac failure with EF<40 (ACEi EF<45)
→ See ACE inhibitors
- hypotension
- hyperkalemia
- renal failure
- teratogenic
- cough + angioedema (rare; less than ACEi)
ACEi more SEs
Same as ACEi
Same as ACEi
NSAIDs, K-Salts, diuretics, etc.
Dont to that 💩 (acutally its possible but not recommended → dont tell bocsan 🤫)
Sa(r)tan says: "Tellmi where the Cande(candy) is or I'r be (I'll be) climbing your Lo(w) val(wall).
- Lo-sartan
- Val-sartan
- Irbe-sartan
- Telmi-sartan
- Cande-sartan
25-100mg/d 1-2doses (Compare Captopril: 2-3doses)
"Von der lowen Mauer sieht man den Niel. Im Niel schwimmt die Tasse mit der Sau. (Sie ist ElCapto entkommen, aber jetzt übernimmt Satan)"
- muscle pain
- nasal congestion
Irbe-sartan
(even prevent renal disease progression)
"I + r in Irbe stands for liver + kidney" (even though its actually an "L")
Act on pro-renin/renin-specific receptors → inhibit renin → ↓Angiotensinogen into Angiotensin I

Aliskiren
"Ali ist beim Ski-Rennen"
(Das -Ren steht für Renin)
F → ↑renin-levels (negative feedback)
diarrhea (high dose) 💩
Hypertension (similiar efficacy to other hypertensives)
First ACEI → not tolerated (I.e dry cough) → ARB → both not tolerated (I.e angioedema) → Renin inhibitors

⇒ 📷
block voltage gates L-type Ca-Channel
Dihydropyridines → smooth muscles → Vasodilation of vessels
Non-Dihydropyridines → cardic muscles → ↓contractability of heart + ↓AV+Sinus conduction (→Bradycardia)
"-dipine" ('-dipine' = Dihydropyrine)
Verapamil = non-dihydropyridine
Diltiazem = non-dihydropyridine
(Verapamil > Diltiazam for angina)
(Diltiazem = 2 = Affects both smooth muscle and heart)
- Amlo-dipine (amo)
- Nife-dipine (knife)
- Felo-dipine (fehler)
- Lercani-dipine (Leer kann ich)
- Nicar-dipine (Nie mit dem car)
- Isra-dipine (israel)
"Amo (Amlo) mit dem Nife (knife) abzustechen war ein Felo (Fehler). Jetzt ist das Auto leer. Ler canI (leer kann ich) Ni mit dem Car (nie mit dem car ) nach Isra(el) fahren.
(1) Hypertension (both types)
- esp. in elderly
- also in patients with asthma! (beta-bl are contraindicated)
(2) Malignant hypertension
dihydropyridine → nicar-dipin
(3) Hypertension in pregnancy
Nifedipine
(4) Raynaud's
dihydropyridine
(5) Cerebrovascular diseases → esp. Subarachnoid hemorrhage / Post-hemoragic stroke
Nimodipine
(6) Angina
- Stable angina (Dihydropyridinic + non-dihydropyric)
- unstable angina (cave: nifedipine)
- MI (if contraindication for betablocker) → give non-dihydropy.
- Prinzmetal angina

nifedipine can exacerbate myocardial ischemia (caused byreflex tachycardia) ⇒ avoid in patients with unstable angina or MI
(7) Arrhythmia (esp. supraventricular arrythmias)
Non-dihydropyridines
(8) Migraine prophylaxis
Verapamil (Verapamil for Very-Painful-Migraines)
→ 💡 remember: elderly, asthmatic, metabolic disturbances, pregnancy
- elderly (often + thiazide)
- isolated syst. HT
- HT + PAD
- HT + Angina
- HT + cerebro-vascular disease (good stroke prevention!)
- HT + SVT
- HT + asthma (favor bronchodilation)
(1) Lightheadedness and headache
(2) Peripheral edema

(3) Reflex tachycardia
Nifedipine
(1) Constipation (2) Gingival hypertrophy
esp. when associated with beta-blockers!
⇒ cause bradycardia + AV-blocks
T (esp. non-dihydropyridinics)
except: Amlodipine + Felodipine
Digoxin
short acting → hypertensive crisis (sublingually)
slow release → long term hypertension
Amlodipine

→ long T1/2 → one dose/day
3-10 mg/day
"Amo hinterlässt nichts an seine Nachkommen außer seine Muh-Tasse. 📷
i.v. Nicardipine
(or Clevidipine; not mentioned by the prof)
Felodipine → higher specificity for vessels + Øeffect on heart
(Felodipine Fessels)
Lercanidipine
Nicardipine
(=angia + HT emergency)
Isradipine 🇮🇱
Isradipine 🇮🇱
Diltiazem
(i.e. in kidney artherosclerosis, diabetic nephropathy + CRF)
- non-selective
- selective
- selective or non-selective +vasodilation
- ↑NO
- Alpha1 block
- Ca-channel block
- Beta2 agonist
⇒. 📷
- ↑NO - Nebivolol
- Alpha1 block - Carvediolol + labetalol (+celiprolol)
- Ca-channel block - Betaxolol, Carvedilol
- Beta2 agonist - celiprolol
A-BEAM + Nebivolol
A-BEAM: Atenolol, Betaxolol, Esmolol, Acebutolol, Metoprolol
Nevbivolol is the exception. However, it's memorable as it also induces NO release
(1) Carvedilol
(2) Labetalol
(Notice this class differs from the "-olol" suffix)
propanolol
- ↓Contractability
- ↓SA- & AV-Node activity ⇒ ↓HR
- ↓Renin → ↓Angiotensin II + ↓Aldosteron→ ↓Periperal resistance + ↓Plasma volume
- ↓Sympathetic activity (CNS inhib. → ↓catecholamines))

⇒ ↓Cardiac output

⇒ ↓Periph. resistance

⇒ ↓Plasma volume ↓

⇒ ↓ Blood pressure
⇒ ↓Cardiac remodeling

⇒ ↓Myocardial oxygen demand
(1) Prevents remodeling due to ↓catecholamines (↓sympathetic activity (CNS inhibition) + ↓AngII (see (2))
(2) ↓ Renin ( → ↓fluid overload and AngII mediated remodeling) ⇒ ↓aferload+preload
(3) ↓Oxygen demand → due to ↓SA+↓AV+↓Contractility
- Atenolol
- Bisprolol
- Esmolol
- Acebutolol
- Metoprolol
- Nebivolol (+↑NO → vasodilation)
- Celiprolol (+a1-blocker ; +beta2-agonist)
- Propranolol (b1+b2)
- Carvedilol (b1+b2+a1-blocker)
- Labetalol (b1+b2+a1-blocker)
- Sotalol (b1+b2+K-channel-blocker)
N-BAM
Nebivolol > bisoprolol > atenolol > metoprolol
- Propanolol
- Carvedilol
- Metoprolol
→ can cross BBB
→ cave: in liver disease (liver metabolism)
- Atenolol
- Sotalol
→ no BBB-cross
→ cave: in renal diseases (renal elimination)
if lipophylic → short T1/2
if hydrophilic → long T1/2
⇒ in general 3-6h T1/2
hyrophilic → low variability
lipophilic → high variability
50-300 mg/day
Lasso - MausSau
Ich fang in der Metro mit dem Lasso ne Maus, die auf ner Sau reitet.
50mg
alpha-beta Lasso (50) 🪢
(1) CHF
Carvedilol, Bisoprolol, Metoprolol
Carve + BM + Nebi
2,3,4
→ Start low dose → ↑progressively
(2) MI, ACS, Post-MI
- chronic stable angina (↓oxygen demand)
A + M
Atenolol + metoprolol
- hypertension
- HF
- Ischemic heart disease (Post-MI, chronic stable angina)
- A-fib
- sotalol (esp with arrhythmia)
- carvedilol
- Celeprolol
- arrhythmias (SVT + ventricular arrhytmias)
- Class II = A-BEAM;
- Class III = sotalol (+amiodaron)
- hypertrophic obstructive cardiomyopathy
labetalol i.v.

→ but only rate control not rhythm
- mitral prolapse (if + palpitations/anxiety)

Labetalol
(1) Migraines*
(2) Thyroid storm
(3) Tremor*
(4) Glaucoma (Timolol)
(5) Portal HT* (due to ↓Output → Splanchnic vasoconstriction)
(6) Dissected aortic aneurysm *
(7) Anxiety *
propanolol
🛡️ AV block
(1) ⇒ Heart block
(2) Exacerbate asthma
(3) Impotence
(4) Bradycardia (Cave: Might cause HF decompensation if ↓contractility or ↓HR)

(5) Reduced effort tolerance + Aggravation of PAD (↓Cardiac output)
(6) CNS-side effects
fatigue, sleep disorder, depression
→ makes sense since betablocker slow the shit down (thats why they are used in anxiety)
→ esp for lipophilic compound!
- asthma
- Prinzmetal angina (due to vasospasm)*

- AV-block , bradycardia
- decompensated HF
- Depression
- COPD
- compensated HF
- Diabetes (mask + cause hypogylcemia) + metabolic synd.
- pregnancy (→ give labetalol)
- athletes
nope - contraindicated
Although beta-1 selective blockers are safer than nonselective beta blockers, they should still be used with caution in patients with asthma, particularly in those with severe obstruction or markedly reduced pulmonary function at baseline
Lipids
↑VLDL ↓HDL
(sympathetic blockage)
Partial agonists (e.g. pindolol, acebutolol)
- Hypotension
- Bradycardia + AV-Block
- Convulsion

- Glucagon + Atropine (Cardiac reversal)
- Pace-maker
- Anticonvulsant
- alpha-agonist or beta-agonists (↑BP)
*beta agonist:

- exercise induced hypoglycemia
- masking of hypoglycemia symptoms
(BB → ↓gluconeogensis/glucolysis + ↓lipolyisis)
not abruptly! → progressively ↓ over 10-14days
⇒ if abruptply → REBOUND SYMPTOMS → angina, MI, arrhythmia, sudden death, HT
persistent elevation of systolic and diastolic blood pressure (BP) over 140/90 mmHg
T
- Essential hypertension - 85 - 90%
- Secondary hypertension: renal, endocrine, cardiovascular 10-15%
- sex (male)
- age
- history of CVD
- hereditary
- ↑Lipidemia
- Smoke 🚬
- DM
- obesity
- alcohol
- ↑sodium intake
<5g
- CHF
- MI + STROKE
- Renal failure
- HT encephalopathy
- Aortic aneurysm
(⇒ CV, RENAL + CEREBRAL DAMAGE)
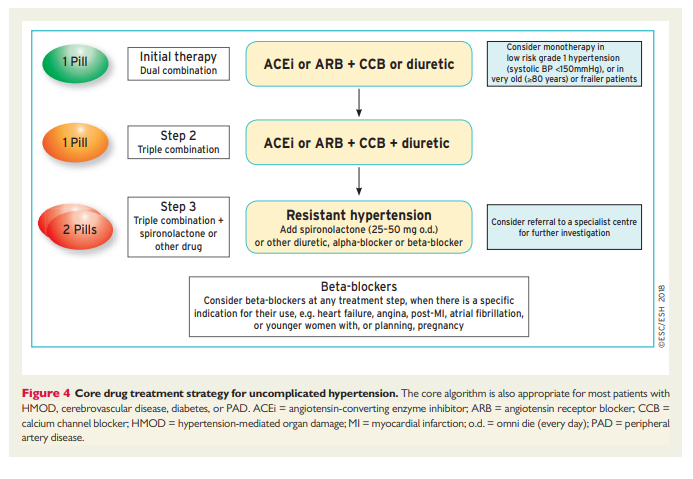
ABCD Rule
ACEi
BB
CCB
Diuretics
most cases → <140/90
DM, CRF, acute MI, stroke → <130/80 (↓10)
- ↓salt (Na, Ca, K)
- weight↓
- Øalcohol, cigaretts, coffee
- ↓cholesterol + saturated fats
- exercise
- stress control
SBP / DBP
1: 140-160 / 90-100
2: 160-180 / 100-110
3: ≥180 / ≥110
- High normal (130-140) → Lifestyle (consider drug if very high risk)
- Grade 1 HT
- Grade 2 HT
- Grade 3 HT
→ If ØCVD, CKD, Organ damage, Diabetes → first lifestyle → then drugs
→ If CVD, CKD, Organ damage, Diabetes → Lifestyle+Drugs
→ If <3RF AND If ØCVD, CKD, Organ damage, Diabetes → Lifestyle first → then drugs
→ If ≥ 3 RF OR CVD, CKD, Organ damage, Diabetes → Lifestyle+Drugs
→ Lifestyle + Drugs


Risk | Any of the following: |
Very High Risk | - Clinical CV-Disease (ACS, MI, stroke, aneurysm, PAD)
- Imaging → plaques >50% stenosis
- DM + organ dmg (i.e. proteinuria)
- Severe CKD (GFR<30)
- SCORE > 10% |
High Risk | - ↑ of a single RF esp.:
→ cholesterol > 310,
→ familiar ↑cholesterolemia,
→ Grade 3 HT
- LVH (hypertensive)
- Moderate CKD (GFR 30-59)
- SCORE 5-10% |
Moderate Risk | - Grade 2 HT
- SCORE 1-4% |
Low Risk | SCORE < 1% |
- All patients → lifestyle + RF correction
- Mild HT + Low-Moderate Risk → 1. Non-pharmacological → reduction failed? → pharmacological
- High + very high CV-Risk → directly pharmacological
📷 ⇒ 10y risk of fatal CVD
⇒ male, age, BP, cholesterol, smoker (fat old smoking male with ↑BP + cholesterol)
→. 📷
- (Mono therapy only in BP<140/90)
- ACE/ARB + CCB/Diuretic
- ACEi/ARB + CCB + Diuretic
- Spirono or other 2nd line (see later)
*consider beta blocker if HF, ischemic diseases, afib
(1) Heart failure (2) Diabetics (3) MI
↓vascular resistance → vasodilation
- Blacks + Elderly (+ calcium channel blockers)
- CHF
- Low plasma renin

mild-moderate → 12,5-25mg/d
severe → 50mg/d
+OTHER AGENTS (i.e. ACEi, beta-blocker)
"Ne Tonne schwimmt im Nil und der Typ mit den weißen Beinen zieht sie mit dem Lasso raus"
CHLORTHALIDONE:
Longer effect (24h vs. 12h)
also better vasodilator effect
but ↑hyperkalemia
Indapamide
can be given in renal failure
↑vasodilation
↓diuretic effect
↓side effects
- Ø Response to thiazides
- RF
- Rapid diuretic effect is needed
- i.e. ac. pulmonary edema,
- HF
- Hypertensive emergency
- Hypercalcemia
Clinical Parameter | Thiazide | Furosemide |
Diuretic potency | + | +++ |
Antihypertensive effect | ++ | + |
Renal blood flow and GFR | May fall | May rise |
Effective in renal failure | No | Yes |
Effective for hypercalciuria | Yes | No |
Effective for hypercalcemia | No | Yes |
Torasemid → prolonged effect
Collecting Duct
- ENaC → ↑Na+ reabsorption
- K- channel → ↑K+ excretion
- ↑ Na/K pump (basolat.)
- H+ ATPase → ↑ H+ excretion
(-) Lumenal voltage
(Na+ reabsorption ⇒ (-) Lumenal voltage ⇒ Pulls K+ through channels)
Amiloride
Triamterene
"A ride with Milo (Amiloride) and Terry in the tram"
Amiloride + Hydrochlorothiazide
Triamterene + Hydrochlorothiazide
Mineral corticoid antagonists → Eplerenone + Spironolactone
- Resistent hypertension treatment
- Hypokalemia due to other diuretics (give combination i.e. thiazide+spiro)
- Cardiac failure → cardioprotective: inhibit fibrosis + remodeling induced by hyperaldosteronism
- MI with LVD → reduced mortality
- HT due to primary or secondary Hyperaldosteronism (edema)
- Eplerenon more specific inhibition of MR
- and lower affinity for Androgen+progesteron R ⇒ less side effects (i.e gynecomastia)
digoxin (lower K)

- Steroids
- Betablocker
- ACEi
- NSAIDs
(NSAID,ACEi+betablocker → ↓aldosterone → ↑K)
Thiazide (+ ACEi)
if >140 → ACEi/ARB + Thiazide/CCB
#2+#3 line
- prevention Hypo-K
- ↓ Cardiac remodeling
METABOLIC RF (i.e. Ions, Uric acid, Gluc, TG+Cholesterol → see Side effects)
⇒ See above, extrainfos:
renin activiy in plasma (high renin = high antihypertensive effect)
HT PLUS
- HF
- (history of) MI
- diabetic nephropathy
- high renin levels
- eldery
- PAD
- Afib
- Hypercholesterolemia

HT PLUS
- children >6y + adolescents
ACE + CBB/Thiazide
- Enalapril + Amlodipine/HCT
- Ramipril + Amlodipine /HCT
saaaaame shit 😎
⇒ See above, extrainfos:
Decrease BP via:
- ↓Cardiac output (SA,AV,contractability)
- ↓Renin (beta 1) → ↓periph resistance + volume
- ↓sympathetic activity → ↓output + resistance
→ see above
⇒ syncope
(reflex tachycardia + orthostatic hypotension)
peripheral resistance↓ only after 1-2 weeks
⇒ initially even ↑periph reisitance
- HT + tachycardia (i.e. SVT)
- counteracts reflex tachycardia due to other antihypertensive agents (due to vasodilation)
high
⇒ See above, extrainfos:
dihydropyridinic CCB
DHP-CCB (dihydropyridinic)
→ esp. if others are contraindicated (metabolic, asthma etc.) →
see also CCB-Indications above
- elderly (often + thiazide)
- isolated syst. HT
- HT + PAD ****(with ACEi; BB are contraindicated)
- HT + Angina (or BB)
- HT + cerebro-vascular disease (good stroke prevention!)
- HT + SVT (or BB)
- HT + asthma (favor bronchodilation)
Nifedipine
F
(except: amlodipine + felodipine)
Vasodilation (+venodilation) → ↓preload+afterload ⇒ BP
↓lipid profile values (total chol, LDL, TG)

-"osin"
- Prazosin (most important)
- Terazosin
- Doxazosin
- Tamsulosin
- Urapidil
"Ich sitze mit Atze Praze (Prazosin) auf der Teraze (terazosin). Neben uns chillen die Dogs (Doxazosin) und ich denk mir nur boah Tam (tamsulosin) geil hier. Und ich sage zu Praze: YoU rap + I deal (Urapidil)
Urapidil also have CNS effect:
→ sympatholytic effect (via stimulation of Serotonin-R)
- SIDE EFFECTS TO DIURETICS (diabetes, gout) OR BETA BLOCKERS (asthma)
- HT + BPH
- aggrevation of IHD → give with betablocker! (reflex tachycardia)

- Orthostatic hypotension → syncope ("first dose phenomena")
- headache + dizziness
- Sexual dysfunction (alpha-R in the 🍆)
- nasal congestion
- HT crisis
- perioperative HT
- pre-eclampsia

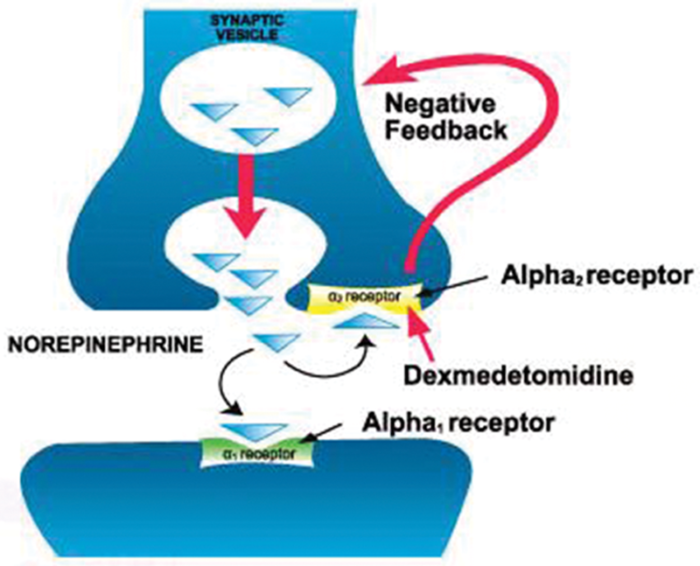
stimulation of alpha2-R and/or Imidazoline type 1-R
→. 📷
- transient HT + ↑periph. resistance
- then ↓BP
no changes in periph resistance!
↓HR + ↓Cardiac-Output
F → actually ↑reabsorption of water + sodium → ↑blood volume
F
→ normal renal blood flow
→ BUT ↓Renin is true
F → no influence on postural reflexes
- HT (moderate-severe)
- opiates withdrawal

- glaucoma

- migraine

- post-menopausal flushing

- Dry mouth
- Depression
- Sedation
→ all signs of sympatholytic acitivity
- rebound HT (if sudden stop of treatment)
- Alpha blockers
- Digoxin (big ass bradycardia)
- Depression
- Pregnancy
- Drivers
alpha 2 agonist
→ ↓periph resistance → ↓BP
T
- HT in PREGNANCY
- HT + RENAL FAILURE
- HT emergencies
1g/day single administration (evening)
("=1 Seil")
Sedation (cns depression)
Dry mouth
rare: hemolytic anemia + hepatitis
Depression + hepatic failure
imidazoline type 1 receptor stimulation
SYMPATHOLYTIC
- ↓symph tone → ↓periph. resistance → vasodilation
- ↓Catecholamines
- conduction disorders + bradycardia
- angina (severe)
- Dry mouth
- sedation
- headache
like others
unknown → perhabs ↓Ca release from SR + ↑NO release
Arteriolar vasodilation → Reduction of BP (esp. diastolic) → ↓afterload
vasodilation → hypotension → reflex tachycardia + ↑renin → consider beta-blocker
- Severe HT
- HT in pregnancy (pre-eclamsia)
- CHF (if ACEi and ARBs are not tolerated) → give together with nitrates
everything that exacerbates when reflex tachycardia happens
- elderly
- IHD
→ due to reflex tachycardia which leads to ↑oxygen demand → exacerbation of these conditions
- Hypotension → Headache, dizziness + fainting
- Reflex tachycardia → tachycardia, palpitations, angina, CHF(if not with nitrate)
- Drug-induced lupus
- (hemolytic anemia, polyneuropathy, rapidly progressive glomerulonephritis)
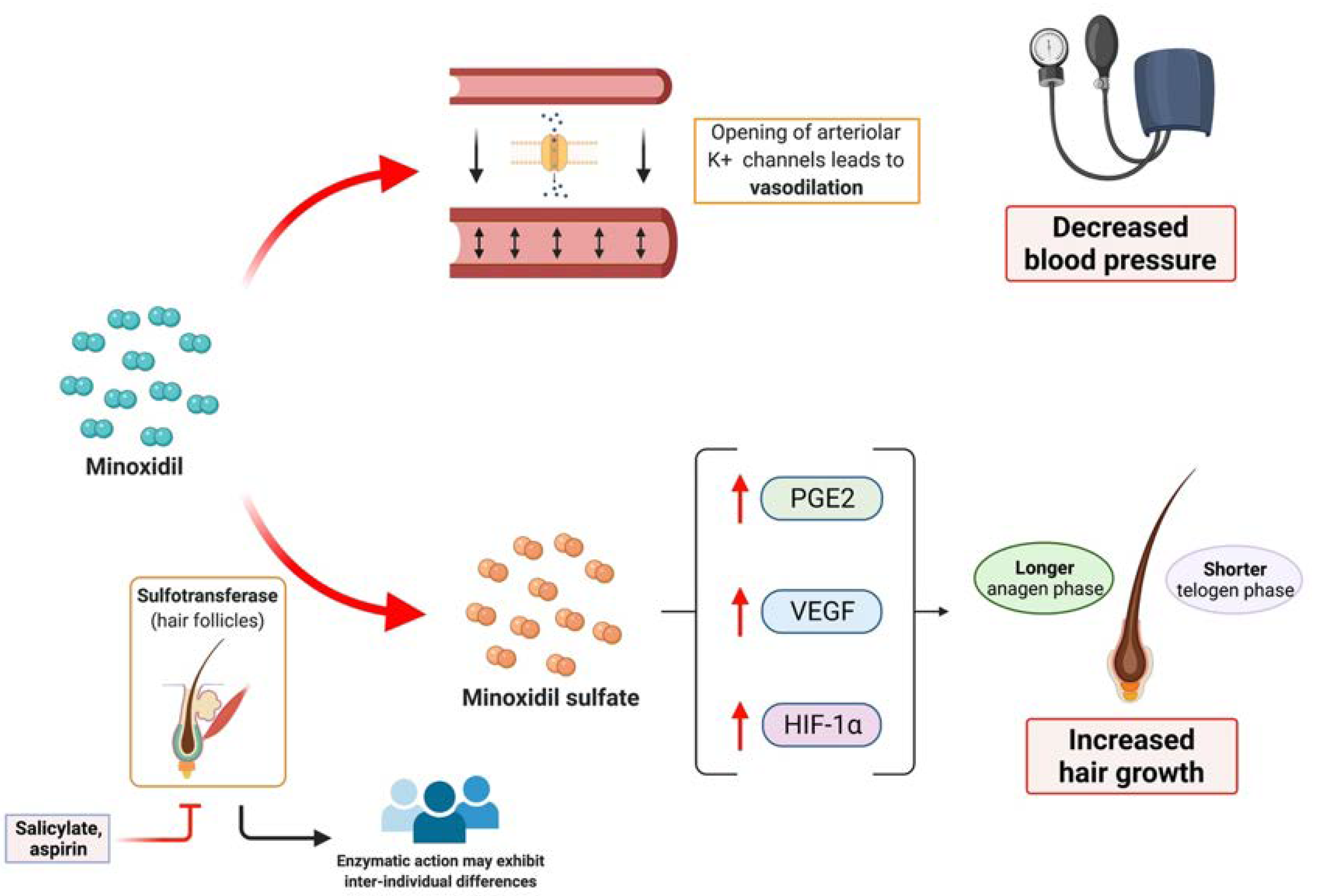
active K channel on vessel SM → arteriolar Vasodilation. 📷
Reflex tachycardia → ↑↑cardiac output
no influence!
"last kidney resort"
- Severe HT + end stage renal failre + no response to other drugs
drugs that ↓preload or reduce reflex tachycardia
→ betablockers
→ diuretics
- Edema (give loop diuretics)
- Tachycardia
- Hypertrichosis

↑NO → ↑cGMP → arteriolar + venous dilation → ↓pre+afterload
GFR + renal blood flow maintained!
- Hypertensive emergencies
- Aortic dissection (give with beta blocker)
- Acute pulmonary edema ("both side release")
- Severe CHF (↓oxygen demand)
- After acute MI
only iv infusion (continous)
→ rapid metabolism by light
Onset of action - within 30 sec, maintenance for 2 minutes
- Hypotension
- Cyanide poisoning
- Methyldopa
- Nifedipine
- Labetalol
hydralazine i.v.
ACEi, ARBs, diuretics
laut sketchy: CCB + diuretic (thiazide)
bocsan: ACEi + diuretic
→ depends on comorbidities (i.e. HF → ACEi)
hypovolemia
orthostatic hypotension (+reflex tach)
Endorgan damage
PLUS
Systolic > 180 mmHg OR Diastolic >120 mmHg
LAUT BOCSAN: ≥220/120
(1) β1 antagonists
(2) Combined α / β antagonists
⇒ ESMOLOL / LABETALOL
NICARDIPINE
Hydralazine
(+ Labetalol)
Administer β1 antagonist
Lower by 25%
Diastolic not less then 100
oral antihypertensives
- Contraceptives
- NSAIDs (due to ↓Pg)
- Nasal decongestants (alpha-agonist (pseudoephedrine))
- MAOi (due to ↑tyramine)

- TCA (due to ↑Epinephrine)

- Corticosteroids (↑↑RAAS)

- Coronary dilation (↑O2 delivery)
- ↓Pre + Afterload (↓O2 demand)
- Heart depression (↓O2 demand)
NBC → Nitrates, BB, CCB
+other (other anti-anginal, antiplatelets, statins)
stabilize atherosclerotic plaques
🧨 Nitrates
↑NO → ↑cGMP →↓intracellular Ca++ → Myosin light chain dephosphorylation → no interaction with actin → vasodilation
also:
↑NO→↓platelet aggregation
- ↓↓Preload → ↓O2 demand #MAIN EFFECT
- Coronary artery dilation → ↑O2-supply

- ↓Afterload (indirect or direct at ↑dosis)

vasodilation arterioles → ↓BP → reflex tachycardia → ischemia aggravation
- Prevent coronary spasm (prinz metal)
- ↑Blood supply in ischemic regions + favor collaterals

NITRATES DONT CAUSE THAT!! because they dont affect the arterioles
A phenomenon in which long-standing coronary artery disease requires maximal coronary arterial dilation distal to the stenosis to maintain normal function. Administration of vasodilators (e.g., dipyridamole) causes dilation of normal vessels, thereby resulting in shunting of blood to well-perfused myocardium. Subsequent myocardial ischemia downstream of the pathologically dilated vessels manifests as angina.
⇒ 📷
- improves coronary endothelial dysfunction + ↓platelet agg.
- ↓ remodeling
- relax bronchi, GI, GU
⇒ 📷
sublingual or IV
(oral bioavailability low as shit (liver metabolism))
oral (or transdermal)
=slow onset + long action
- Nitroglycerine
- Isosorbide dinitrate
nitroglycerin
(+nitroprusside)
sublingual → stable angina + prinz metal (variant)
iv → emergency: acute MI, unstable angina, ac. pulmonary edema, malignant hypertension (+cardiac/neurological surgery)
- Nitroglycerin (can also be given transdermally(TSS))
- Isosorbide dinitrate
- Isosorbide mononitrate (maintenance only)
- Pentaerithrityl tetranitrate (maintenance only) lower effic. than ISDN+ISMN
- All types of angina (stable, unstable, variant aka prinzmetal)
- ACS (acute MI + post-MI)
- Hypertensive emergency
- Some congestive HF (but not hypertrophic obstructive!)
→ Ø in RV-infarction!!

- throbbing headache, flushing, tinnitus
- dizziness, orthostatic hypotension → might produce reflex tachycardia (↑ischemia) → give beta blocker
- Methemoglobinemia
Hypovolemia + Hypotension
+certain drugs → see below
QUICK TOLERANCE AKA TACHYPHYLAXIS → do short periods of interruption to restore sensitivity (during night i.e.)
(demonstrated only for long acting compounds (oral)
- after chronic administration
- discontiuation → vasospasm → NEVER SUDDENLY INTERUPT
- Inhibit CYP450 → Not with PDE-5 Inhibitors → suffix: afil (sildeafil, vardeafil, tadalafil) → severe Hypotension
- Alpha 1 blockers (except tamsulosin)
only high → low bioavailability otherwise
endothelial dysfunction
See above
↓contraction+HR → ↓O2 demand (esp. during effort)
(also antiplatelet + antiarrhythmic + antihypertensive effect)
- stable angina → #1 line chronic treatment
- Acute MI+Post-MI
- Unstable MI
→ esp. with arrhythmias or HT
Carvedilol or Metoprolol
Metoprolol + Bisoprolol → esp ↓mortality + progression to HF
See above
Angina
- Stable angina (Dihydropyridinic + non-dihydropyric)
- unstable angina (cave: nifedipine)
- Prinzmetal angina
- #2 line MI (if contraindication for betablocker) → give non-dihydropy.

WHEN ESP A CCB?
- Angina + Arrhythmia (esp. supraventricular arrythmias)
- Angina + Hypertension (NDP-CCB, DP-CCB)
- also in patients with asthma! (beta-bl are contraindicated)
Non-dihydropyridines
Dihydropyridines → ↓afterload + ↓oxygen demand
Nifedipine Amlodipine Felodipine Tacidinine Verapamil Dultiazem
→ if intolerance to BB + HR>70
- Chronic stable angina
- CHF (NYHA II-IV)
- With atenolol (combined therapy)
→ if normal sinus rhythm + HR >70
bradycardia
<50 BPM
add on therapy in patient with IHD + ↑HBA1c
can also be considered as an alternative to BB or as add-on if first line fails
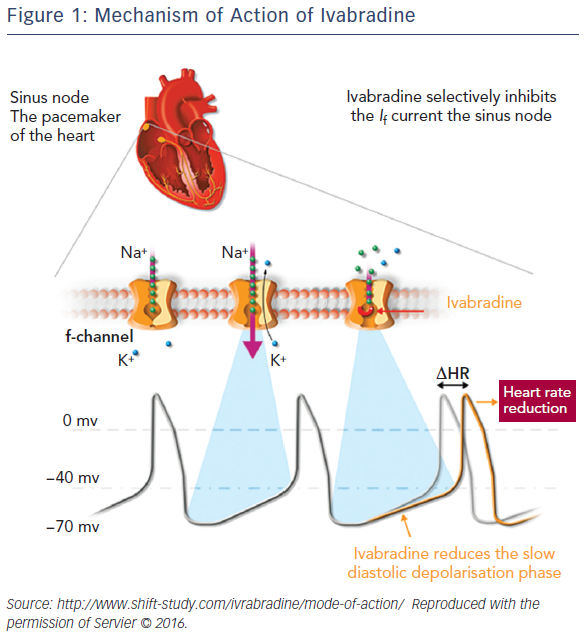
→ 📷
select. inhibitor of tardive (late inward) Na current → ↓Ca (intracell) → ↓wall tension → ↓O2 demand + ↑tolerance to effort
⇒ Øchange in HR + BP!
Reduces MVO (without altering heart rate or BP): Inhibition of late inward sodium channels on cardiac myocytes → ↓ calcium influx via sodium-calcium channel pump → ↓ wall stress and MVO
- Constipation
- dizziness + headache
- with CYP inhibitors (metabolism via CYP3A4)
- (can exacerbate) QT-prolongation + arrhythmias
- hepatic failure
↑Gluc oxidation → good for ischemic tissue
coronary vasodilation
• ↓ free fatty acids oxidation • Favors glucose oxidation in ischemic conditions • Improve myocardial hypoxic cell metabolism • Vasodilation of coronary arteries
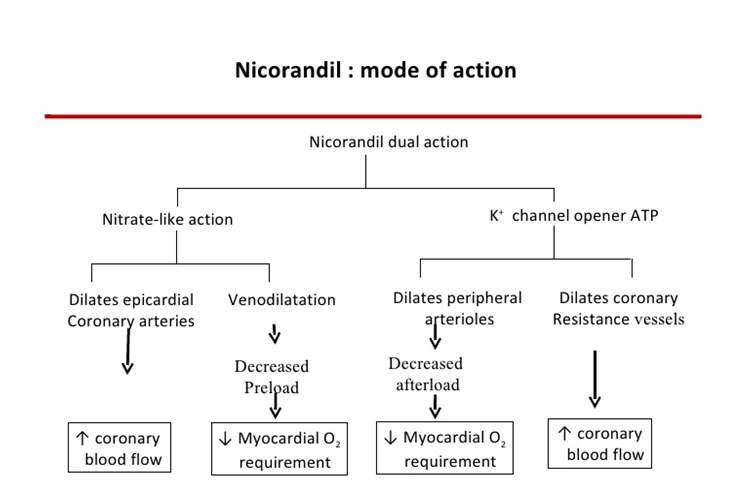
Nitrates
Parkinson, tremor
- ↑NO → vasodilation → ↓preload + ↑coronary flow
- K-channel opener → ↓afterload + ↑coronary flow
symptomatic patients already on anti-angina treatment (add-on)
Mucosa ulceration
headache + flushing
Nitrates
BUT DIFFERENT CHEMICAL STRUCTURE
AND NO TOLERANCE
not routinely used
→ oral angina maintenance therapy
- DM
- HF
- history of acute MI
„Ibra hat 3 Met-Brötchen gegessen und rennt jetzt zu Nico (braucht mehr).“

Nitrate + BB
→ to avoid nitrate tolerance + reflex tachycardia
→ in the evening LA-BB(Atenolol, Metoprolol)
not very used → if necessary non-dihydropyridic
BB + dihydropyrines! → counters reflex tachycardia
Ønot with non-dihydropy.! → bradycardia + HF
severe angina → but cave: difficult to control
- Step: BB or CCB
- Step: BB+ DHP-CCB
- Step: Add #2 line drug
↑ HR (>80)
#1 BB or CCB
#2 BB + CCB
#3 BB + Ivabradine
↓HR (<50)
#1 DHP-CCB
#2 Switch to LAN
#3 DHP-CCB + LAN
#4 Add Nicorandil, ranolazine or trimetazidine
#1 BB
#2 BB+LAN or BB + Ivabradine
#3 Add another #2 line
#1 BB or non-DHP-CCB (both low dose)
#2 Switch to ivabradine, ranolazine or trimetazidine
#3 combine two #2 line drugs
→ antiproliferatives
- Paclitaxel
inhibits cellular proliferation by binding to and stabilizing polymerized microtubules.
- Sirolimus
binds to the cytosolic immunophilin FKBP12 - inhibiting cell cycle progression
- 🚭
- 💪🏼
- control diabetes + HT
- Statins
- Antiplatelets
- PERIPHERAL VASODILATORS (symptomatic)
- BB can also be considered in IHD + HF
- Vasodilation
- Antiplatelet
Pentoxyphillin + PGs
"Das Nafri-PiG wiegt 5 (Penta) Cilo und ist antiplatelet + vasodilation"
inhibit PDEs → ↑cAMP
→ vasodilation
→ antiplatelet
→ ↓fibrinogen
→ ↑deformability of RBC (squeeeeeeze)
Claudication
- Dizziness+ hypotension → reflex tachycardia → angina
- bleeding (↓fibrin+platelets)
- HT (?)
- with oral anticoagulants+antiplatelets
inhibit PDE3 → ↑cAMP
→ antiplatelet + vasodilation
→ ↓TG+↑HDL
Claudication
↓risk of stroke
5HT2-R blocker → vasodilation + antiplatelet
Claudication
symptomatic treatment of cogn. deficit after ischemic stroke
adjuvant for raynauds (with d-CCB)
Alprostadil
- Claudication
- Ulceration
- CHD
- Sexual dysfunction
- Apnea
- Hypotension
- bradycardia
- hyperthermia

Also check out cerebral vasodilator - Nimodipine (see CCB)
Block Na+ channels
↓ Rate of rise of AP
↑Effect on rapidly depolarizing tissue
↑HR → ↓Phase 0 upstroke
None
class I antiarrhythmics affect the Na+ dependent cardiac action potential (Ø action at the SA and AV nodes)
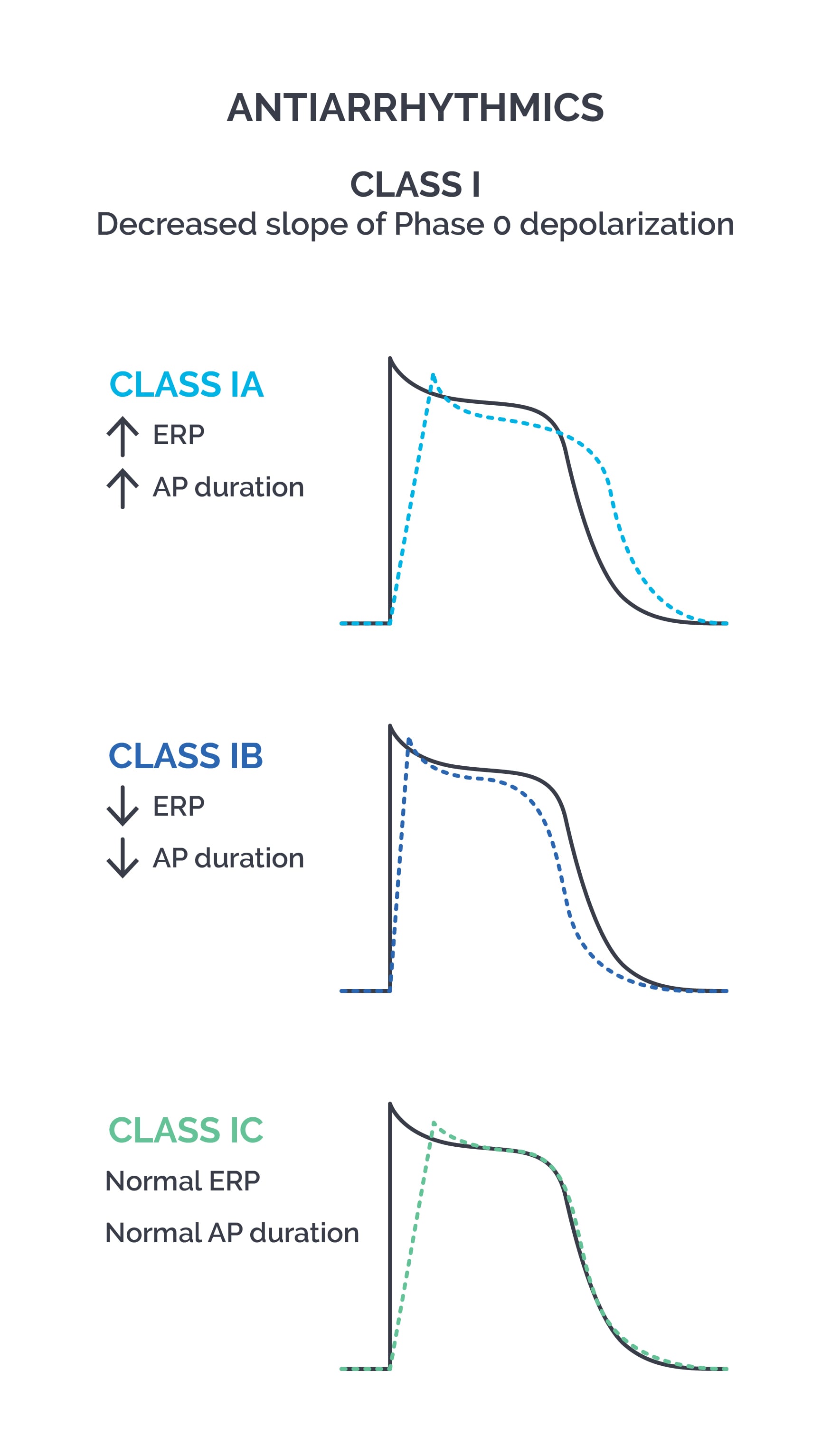
Widened QRS complex (↓AP conduction velocity)
- C → slow dissociated from the channel: strong use-dependence,drastic slowing of the phase 0 upstroke
- A → intermediate dissociated from the channel: intermediate use-dependence, moderate slowing of the phase 0 upstroke
- B → rapid dissociated from channel: slow use-dependence, minor slowing of the phase 0 upstroke
(CAB)
Ia → Atrium + Ventricles
Ib → Ventricles
Ic → Atrium + Ventricles
IA
A → ↑ AP duration (↑phase 2+3), ↑ERP
B → ↓ AP duration (↓phase 2+3), ↓ERP
C → Normal AP duration → normal ERP
- Quinidine
- Procainamide
- Disopyramide
Blocking K+ channels → ↑phase 2 + 3 of cardiac AP
WPW (Wolff-Parkinson-White syndrome)
T → ↑↑ side effects
- Ventricular arrhythmias caused by:
- brugada
- short QT
- Afib/Flutter if refractory SVT → conversion/maintaince sinus rhyth.
- Cinchonism: Tinnitus, headache, dizziness
- Thrombocytopenia
- Torsades / QT prolongation (but actually all class IA can cause torsades!!)
- PR + QRS prolongation
- GI-side effects (nausea, vomiting,diarrhea)
- hepatitis, agioneuritic edema, fever
- Ventricular arrhythmias (more efficient than Quinidine)
- Ventricular premature beats
ganglion blocking → ↓BP
⇒ give i.v. in HT (esp. in LVD)
- Lupus like syndrome
- similar adverse as quinidine:
- GI
- Fever + hepatitis
- agranulocytosis
Disopyramide
(↓inotropic effect due to ↑antimuscarinic effect)

- Torsades
- Ventricular arrhythmias
- atropin-like activity → urinary retention, dry mouth, blurred vision, constipation, exacerbate glaucoma
→ Afib/Aflutter (maintain sinus rhyth.) → Prevent VT
‼️ NOT USED as #1 LINE ANTIARRHYTHMIC
(Diso → atrial; procain → ventricle; Qinidine → atrium + ventricle)
- Lidocaine
- Mexiletine
- Phenytoin
i.v. (bc. extensive first-pass)
oral
ischemia induced ventricular arrhythmias
(post-MI complication!)
Bocsan:
- termination of VT,
- prevention Vfib after cardioversion in acute ischemia

- chronic ventricular arrhythmias
- prolonged QT syndrome
- Neurological SE ↑→ paresthesias, tremor, convulsion (esp in rapid administration)
- hypotension (large doses)
- pro-arrhythmic effect (uncommon)
F
esp. Na
(+ K but normal ERP!)
- Flecainide
- Propafenon
- Afib (+flutter+tachycardia)→ Rhythm control
- VT + V-Extrasystoles
(with normal heart)
exacerbation of arrhythmia (even with normal dose)
- arrhythmia exacerbation
- metallic taste
- constipation
weak beta-blocker (structural similarities to propranolol)
PRE-EXISTING HEART DISEASES
- Structural
- Ischemic
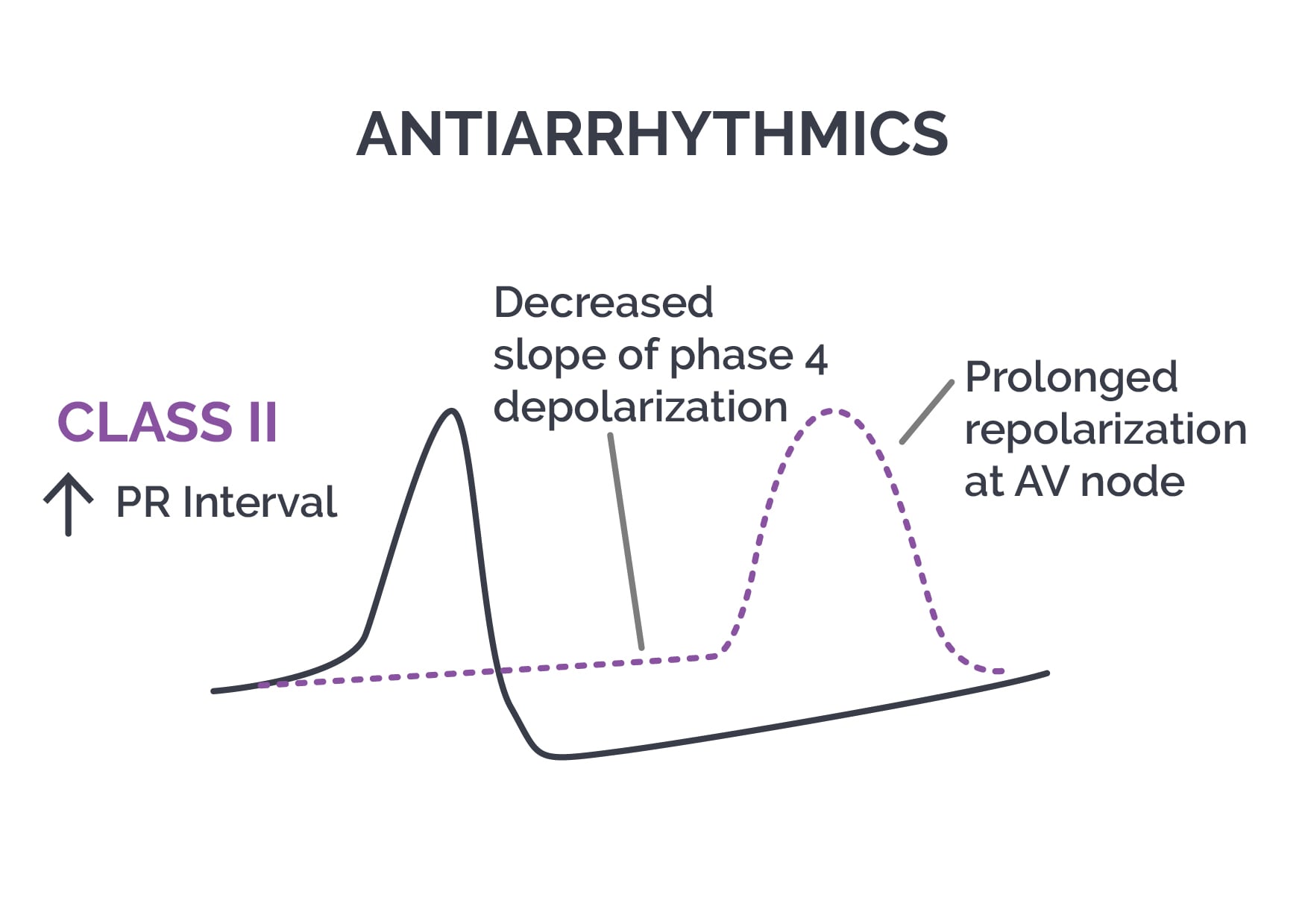
Prolongs nodal phase 4 📷
(Via reducing sympathetic input to SA/AV node via ↓cAMP → ↓Ca++)
AV node (Although they do affect SA too)
Supraventricular
i.e., atrial fibrillation, flutter, SV-premature beats)
BUT RATE CONTROL!! only in RVR

- Ventricular tachycardia (RVR)
- prolonged QT ? like 1b mexilitide
esmolol iv. = short-acting b1
(can be given for rate control or in acute arrhytmias)
↑PR interval
sotalol → prolonges AP as well (class 3 property)
NON-SELECTIVE!
- Amiodarone
- Dronedarone
- Satalol
- Dofe-tilide
- Ibu-tilide
Inhibit cardiac K+ channels → prolonged phase 2 and 3 of cardiac action potential → prolonged refractory period
AMIODARON
(thats why it ↓HR PLUS ↓AV-conduction)
Amiodaron can be given in structural or ischemic heart diseases with Afib!!!
Supraventricular and ventricular
RHYTHM CONTROL
- Supraventricular: PSVT, Afib, Aflutter
- Malignant VE, VT (incl. VT after MI → compare Ib)
- Vfib prophylaxis after resuscitation
(1) Neurological side effects
(2) Gray corneal deposits
(3) Hypo/Hyperthyroidism
(4) Pulmonary fibrosis
(5) Heart block*
(6) Induce heart failure*
(7) Hypersensitivity hepatitis
(8) Gray-blue skin discoloration
(9) Photodermatitis
Amiodarone
Amiodarone (probably due to 4x effect)
oral or iv
Dronedaron
→ stronger anti-adrenergic (b1)
→ prolonged QT more prone (dose-dependet)
→ GI symptoms
- SVT with RVR rate control
- VE + prevention of VT (#2/3 line)
"pure" lKr-blocker 📷→ slowed repolarization

(no relevant effect on others)
Afib maintainance of sinus rhythm
- ↓dosage basen on CrCl
- ECG monitoring (continous)
Ibu also activates slow inward sodium
F - rapidly cleared (halftime 6h)
acute conversion afib/aflutter (i.v.) → ESP. FLUTTER
ECG monitoring
- Diltiazem
- Verapamil
- Galopamil
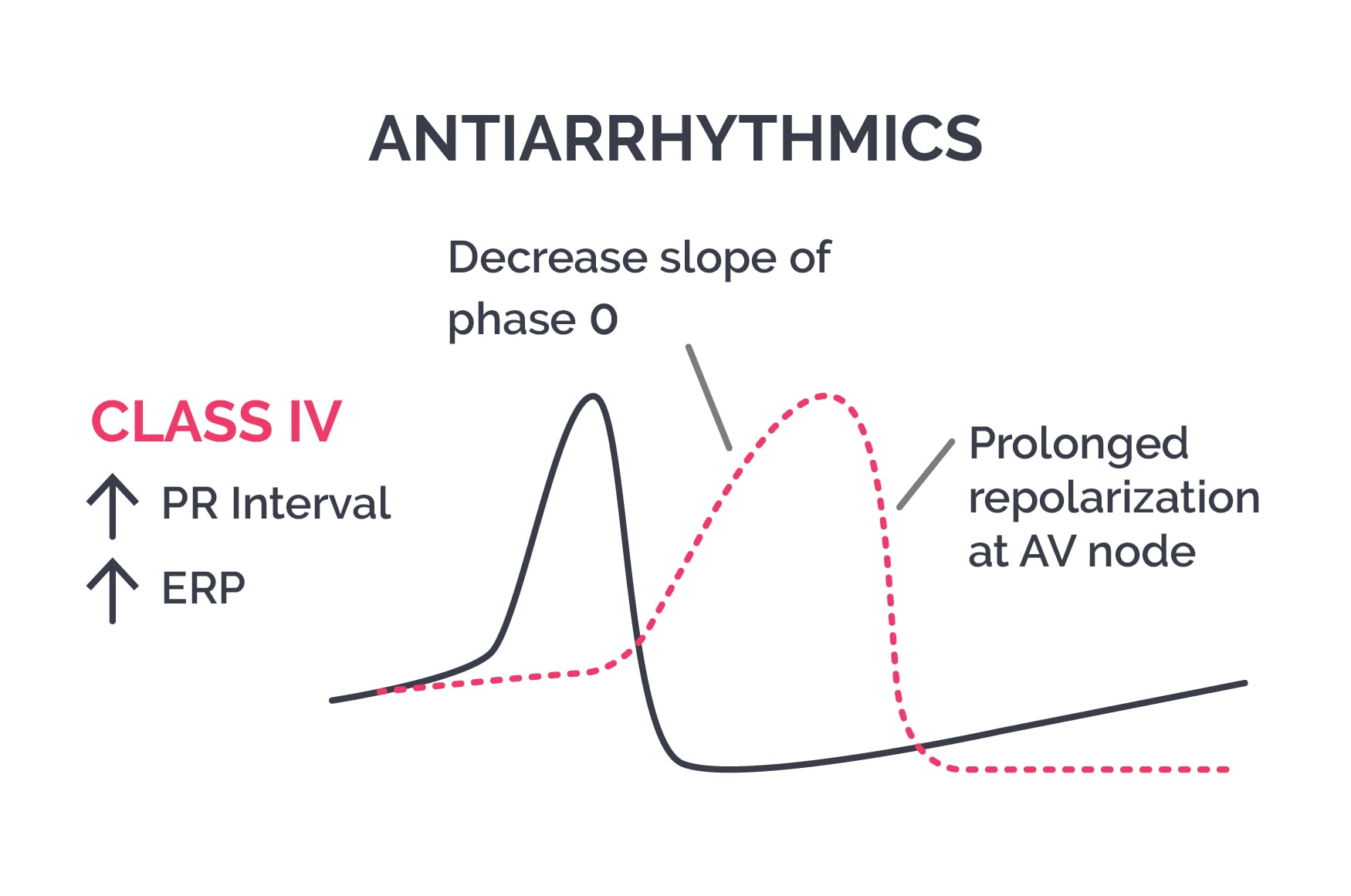
Calcium channel blockers → ↓AP upstroke + ↑ERP in SA/AV. 📷
SVT with RVR (i.e. afib) → RATE CONTROL
(also useful in HT due to periph effect)
AV node
↑PR → cave AV-block
(like DHP + Verapamil (constipation)
constipation
nervousness
periph. edema
diltiazem (less periph vasodilation+ ↓effect on heart compared to verapamil)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
alternative for beta-antagonist (Øtolerated or contraindication)
↑ Parasympathetic effects (vagus) → AV inhib
RATE CONTROL
↓ ERP in myocardial cells + ↓conduction in purkinje (slight rhythm control???)
A1-Receptor (on myocardium and SA + AV nodes)
(1) ↑ Outwart K+current
(2) ↓ Inward Ca2+ current
(Both factors inhibit cardiac action potential → hyperpolarizations, suppressed Ca-dependent AP )
AV-node
(decreased AV conduction, prolonged AV refractory period)
SVT → esp. PSVT (AV re-entry)→ give iv bolus
vasodilation (via A2 receptors)
(1) Cutaneous flushing
(2) Shortness of breath/Chest pain (due to bronchospasm)
(3) Hypotension + headache
(4) High grade AV-block
(5) Afib*
Methylxanthines (Caffeine, Theophylline)
- Torsades de pointes
- arrhythmia induced by digoxin
SVT
F only atrial → conversion afib
- Calcium chloride → VT due to ↑K
- Atropine → in bradycardia??
- Epinephrin → cardiac arrest
- Isoproterenol → AV-Block
- ACEi + ARBS → prevent new Afib in CHF, HT, LVH
IHD + HT
Activation RAAS, BNP, sympathetic NS
- ↑Preload (retention (RAAS) + congestion if diastolic)
- ↑Afterload (symph + RAAS) → excessive vasoconstriction
- ↑Contractabilty + HR (due ↓output)
- LVH → remodeling
{kind=link}
→. 📷
{kind=link}
→ 📷
{kind=link}
arrhythmias
ACEi + BB + Diuretics (ABD)
1st LINE
- arteriolar + venous dilation → ↓pre+afterload
- ↓symph. activity
- ↑diuretic effect (↓aldosteron)
- ↓remodeling
- antiproliferative effects + improve endothelial dysfunction
- vascular protective effect
also see above
- HF with LV-dysfunction aka systolic HF NYHA II-IV (+EF<40%) → #1 line
- CHF #1 line (+diuretics if edema aka diastolic dysfunction)
- Post-MI HF (EF doesn't matter)
- Prophylactic in patient with ↑risk for developing HF (ACC/AHA Stage A) (HT, IHD, dyslipidemia, DM)
2+3 → enalapril, lisinopril, ramipril (aka 2nd generation ACEi
4 → ramipril (,trandolapril)
Just give ramipril 5mg in HF and you are gucci
start small → ↑in a few days/weeks (hospital/ambulatory)
- BP
- Electrolytes
- Crea
ACEi not tolerated
candesartan, valsartan
(esp in NYHA3+4 + post-MI)
- mild-severe HF (NYHA II-IV) together with ACEi + diuretics → but caution in NYHA IIIb + IV!
- post MI → now asymptomatic LV-dysfunction
- HEMODYNAMICALLY STABLE (no acute decomp. in last 2-4w; Ø/minimal water retention)
NOT IN ACUTE HF
1/10 of maintenance dose → ↑slowly+progressively
(and Øsudden discontinuation!!)
continue with lower dose
stop the BB!
- Metoprolol
- Bisoprolol
- Carvedilol
- Nebivolol
A-BEAM + Nebivolol + Carvedilol
↓afterload (due to ↓periph vascular resistance)
False, except Spironolactone
- Spironolactone (+Eplerone)
- Furosemide
- Other loop diuretics (Torasemide)
- Thiazides + Indapamide
- K sparing diuretics
T
slow release tbl preferred
Nope give furo!
(dont give thiazide if crea >1,6)
HyperK+ 🍌
- Congestive HF NYHA II-IV
- EF < 35% in systolic HF
K+ and renal function
ACEi/ARBs + BB
edema
acute HF → give as perfusion or bolus
rapid onset, short term effect
Oral or parenteral
Spirono
- Ototoxicity aka deafness (dont combine with other ototoxic drugs i.e. aminoglycosides!)
- Low Na, K, Mg, Ca
- Hypovolemia
- interstitial nephritis
- Hyperuricemia
- Sulfa allergy
Ototoxicity, Hypokalemia, Hypomagnesemia, Dehydration, Allergy (sulfa), metabolic Alkalosis, Nephritis (interstitial), Gout.
Bumetanide
Torasemide
antiandrogenic
T → used to ↑ diuretic effect of other groups
ACEi
Triamterene + Amiloride
"A ride with Milo (Amiloride) and Terry in the tram"
- non-compliance
- ↑Na intake
- ↓renal flow due to
- ↓Cardiac output
- when starting/increasing ACEi therapy
- severe hypotension
- Renal pathology (r.artery stenosis, etc.)
daily:
- diuresis
- body weight
- sodium + water intake
- electrolytes + crea
2nd Line
HFrEF & persistent / worsening symptoms despite adequate teatment regimen with #1-line drugs.
ARB
valsartan + sacubitril
{kind=link}
impair breakdown of NP + Ang-II (+Substance P) → ↑NP+Ang-II

→ ARB to block Ang-II effects on AT1 receptor
→ NP effect:
- natiuresis
- vasodilation
- ↓sympathetic activity
↓ 👌
- Positive inotropic (contractability)
- negative chronotropic (↓SA)
- negative dromotropic (↓AV)
- positive batmotropic (→automatism in cardiac tissue → Atrial or V arrhythmias)
- Positive tonotropic (↑Tonus + ↓size of the heart→better oxygen consumption)
{kind=link}
inhibits Na+/K+- ATPases in cardiomyocytes → Increased intracellular Na+ levels→ reduce the efficacy of Na+/Ca2+ exchangers → higher intracellular Ca2+ concentrations.
⇒ the force of contraction becomes stronger (positive inotropic effect)
↓periph. sympathetic activity → ↓vascular resistance
(parasympatic effect on the heart → thats why ↓AV+SA↓
- sinus bradycardia
- prolonged PR (av depression)
- ↓QT interval (↓ventricular AP)
- ST depression + T inversion (altered repolarization) ⇒ “scooped” concave ST segment
Digitoxin → liposoluble → good absorption+bioavailability, steady state conc. takes 1month
Digoxin → less liposoluble → variable bioavailability (!prolonged in eldery + renal insuff), stead state conc take 1week
Maintenance dose = eliminated amount /day
HF PLUS
- Low cardiac output (esp. systolic dysfunction)

- SVT (Afib, Aflutter, PSVT) - rate control
- Ac. pulmonary edema (pulmonary pressure decrease)
F - Ø influence the survival period but ↑ quality of life!
- Arrhytmias → Ventricular premature beats, bigeminism, VT+Vfib
- bradycardia,
- AV-Block
- GI: nausea + vomiting
- visual disturbance (objects appear yellow) + psychosis
- skin erruptions
- Ventricular arrhythmias
- freq. ventricular premature beats
- VT
- WPW with Afib → Risk for Vfib!
- Bradycardia
- AV block
- hypertrophic cardiomyopathy *
- aorta stenosis *
- constrictive pericarditis *
- cave with: amiodarone (III), quinidine (Ia) + verapamil (NDCCB) and diuretics→↓renal clearance of digoxin*
- Correct K
- Antidigitalis Antibody
- Lidocaine (Ib)
- Propafenone (Ic)
- Propranolol (non-selective betablocker)
- elderly
- renal insuff
- patient under amiodarone, quinide or verapamil
- overdose
ACEi or ARBs are not tolerate
↓preload (venous dilation)
↓afterload (higher doses)
coronary vasodilation
- ISDN
- Nitroglycerine
- Nitroprusside
ISDN → in CHF together with hydralazine (due to tolerance)
Nitro → acute MI-induced HF, acute LHF
Nitroprusside → HF due to ↑periph resistance, MI-induced HF
- hypotension
- methemoglobinemia (cyanide intox)

↓periph. + pulmonary resistance → ↓afterload
oral or iv (emergency)
see above
I nahm eine Millionen Rhinozeros
(one in a million)
Inhibit PDEIII → ↑cAMP → ↑contractability + vasodilation (↓afterload)
- Acute HF with systolic dysfunction (iv)
→ BUT:
- only used in ICU for short-term → fast tolerance
- in some contries even withdrawn
Acute heartfailure + instable
IV only!
1,5-10 → renal, coronary, cerebral dilation
10 → b1 → ↑contractability, mild ↑HR, ↑AV-conduction, ⇒ mild ↑BP, ↑Cardiac output
>15 → a1 → vasoconstriction (↑periph. resistance)
- Severe HF → esp. in oliguric
- Acute pulmonary edema
- All types of shocks (except anaphylactic shock) → esp. in oliguric patient
- Peripheric Sympathetic effects
- Tachycardia
- Arrhythmias
- Angina
- Tremor
- HT
- ischemic necrosis (paravenous perfusion)
Already increased dopa/sympathetic problem
- Hyperthyroidism
- Pheochromocytoma
- Tachyarrhythmias
- MAOi

Decresed periph sympathetic tone, increased HEart
- ↑Output + slide tachycardia
- ↓pre+afterload
- ↓pulmonary pressure
- ↓sympathetic tone
- ↑diuresis
ACUTE
- acute HF after MI
- acute episodes of CHF
→ if not oliguric (compare Dopamine)
Nesiritide = BNP analogue → ↑cGMP → vasodilation (vessels, kidney + other organs)
→ ↓pulmonary + periph resistance → ↓cardiac output
iv → acute HF
- Hypotension
- Headache
- severe hypotension
- cardiogenic shock
- Same special stuff as digoxin:
- aortic stenosis
- constricitve pericarditis
- hypertrophic cardiomyopathy
{kind=link}
🧠 Nervous System
persistent (chronic) insomnia
- ↑slow-wave sleep
- ↓REM
6 month
T → Barbiturates incr dependence+toxicity
"-olam" (except. oxazepam)
- Triazolam
- Midazolam
- Oxazepam
- Alprazolam (intermediate)
💥 ATOM
LA: Diazepam
Intermediate: Alpa + Lora
short: mida
Long acting BZD (T1/2 >24h) | Intermediate-acting BZD (10-20h) | Short acting BZD (<8h) |
Diazepam | Estolazepam | Triazolam |
Clonazepam | Lorazepam | Oxazepam |
Chlordiazepoxid | Temazepam | Midazolam |
Flurazepam | Alprazolam |
Was geht lange? → Die Diashow zwischen Klo und Flur
Welche Presentation geht mittellange → Die von Lora mit dem Thema: Who (e)stole the Alpakas?
liver 🍑 (long acting BZD form active metabolites)
stimulate GABA-A receptor (allosteric site)
BZD = GABA-A R agonist ⇒ potentiate GABA-A transmission in CNS
↑Cl
GABA-A = Chloride channel
GABA (and glycine) is a major inhibitory neurotransmitter
↑ Opening frequency
(not duration like barbiturates)
oral, iv, rectal
hepatic oxidation followed by glucoronide conjugation
(some directly conjugated → Øactive metabolites)

(1) Anxiety
(2) Panic disorder
- ↓Anxiety + aggression → Anxiety + PD, Alcohol withdrawal
- Sedative/hypnotic → Insomnia
- Muscle relaxing → spastic diseases
- Anticonvulsive → seizures
- Anesthesia (induction + maintenance i.v.)
Induce anterograde amnesia
(can be used for conscious sedation i.e. wisdom-teeth extraction)
- Diazepam
- Midazolam
- Lorazepam
Clonazepam
Midazolam (short acting)
oral (insomnia)
i.m. (anesthetic induction)
i.v. (endoscopy)
Nitrazepam + Flu-nitrazepam
Diazepam
anxiolytic → Diazepam
Anti-Seizures → Clonazepam
anesthesia → midazolam
hypnotics → nitrazepam
oral
iv + im → administer slowly!
Alprazolam
weeks
(due to dependance)
- Sedation
- ↓Psychomotor performance → cave: drivers!*
- Confusion + Headache
- Anterograde amnesia
- Dependance
- Mild euphoria
- Muscle weakness
- Acute intox → ataxia, speech difficulties, coma (moderate CNS depression)
alcohol
FLUMAZENIL
competitive antagonist of BZD recept. → reverses BZD induced sedation (but precipitates seizures)
i.v.
post-OP → to reverse BZD effect
Portal encephalopathy

in some patients → ↑irritability+ aggression
esp. with SA-BZD (Triazolam)
F → ↑in SA-BZD
but occur after longer treatment (few month)
short acting → 1-3 days
long acting → 1-2weeks
CNS stimulation symptoms:
agitation, anxiety, insomnia, headache, tremor, convulsion
slow dose reduction
For anxiolytic (+anticonvulsion)→ Pregabalin (anti-epileptic drug)
For insomnia → melatonin or zolpidem during dose reduction
MYASTHENIA GRAVIS
Caution: drivers + elderly(small dose)
(1) Zolpidem
(2) Zaleplon
(3) esZopiclone + Zopiclone
"Der Zoll-Piet bekommt seinen Zahlen-Lohn und er sagt: ich ess die Suppe meines Klons"
same as benzos (same allosteric site on GABA-A)
No → other allosteric site of GABA-A
INSOMNIA (💤)
Have largely replaced benzodiazepine (BZD) in the treatment of insomnia. They are less effective as anticonvulsants or muscle relaxants due to their relative selectivity for GABA receptors with α1 subunit.
Zolpidem → ONLY SEDATIVE without anticonvulsant, muscle relaxing, anxylytic
Zopiclone → all of BZD (hypno, sedative, anxyo, amnesic, muscle relax, anticonvulsant)
esZopiclone ⇒ long term treatment possible
zolpidem → only short term for both
zaleplon → only for induction (or if administered when patient awake)
headache
xerostomia (dry mouth)
memory impariment
→ aka kiff-kopf
short period of time
Residual daytime sedation/amnesia
MILD REBOUND INSOMNIA
"verklatscht"
Zaleplone
short → only induction insomnia treatment
Minimally → esp. in high doses long term therapy
Flumazenil (same as BZD)
same as BZD
Ramelteon (melatonin)
Activation of MT1 and MT2 melatonin receptors (located in the suprachiasmatic nucleus of the hypothalamus) (these Melatonin receptor maintain the circadian rhythm)
→ no tolerance, no impairment next day (), no rebound insomnia, no withdrawal symptoms ⇒ safe in geriatric patients
Bind GABA-A R (other allosteric site then benzos)
→ Cl influx → CNS inhibition
low dose → sedative
high dose → hypnotic
Phenobarbital oral or im
NEVER IV!!! (Cardiac + resp. depression)
↑CYP450 activity → dose adjustment (i.e. warfarin, statins)
↑glucuronyl transferase activity → can be used for neonatal jaundice
long acting (8h)
Tiopental → general anesthesia (induction)
- Tolerance + dependance (1-2weeks) ⇒ withdrawal syndrome (agitation, tremor)
- allergy
- residual sedation after awakening
ACUTE INTOX (lethal dose = 5-10mg):
- Cardiac + respiratory depression/insufficiency → arrest
- bronchial hypersecretion + infection lung complications
- Hypotension, fainting, CVcollapse, coma
- muscular relax (no deep reflexes)
- renal insuff
- Gastric lavage / induction of vomiting
- sympathmimetics
- mechanical ventilation
- bicarbonates (acidosis-CO2 retention ; &buffering hco3 bind drug > renal excretion)
- dialysis
- antibiotics (prevention lung compl)
- hepatic porphyria
- liver failure
- renal failure
Ethomidate (+fenta) → i.v. (no pulmonary or vascular depression)
Propofol → induction + maintenace (long term sedation)
remember H1-blocker + pregablin
Others: Ethomidate, Clomethiazole, Propofol, H1 antihistamines, Doxepin, Pregabalin, Ritanserin, Agomelatine, and Suvorexant.
Antidepressants like SSRIs and SNRIs are first-line treatments for various anxiety disorders. Older antidepressants are effective but have more side effects. Buspiron is an anxiolytic with weak sedative effects, while other tranquilizers like hydroxyzine are used for different situations. B Adrenergic antagonists have limited use due to significant side effects.
depression + mania. 📷
:max_bytes(150000):strip_icc()/379962-bipolar-disorder-symptoms-and-diagnosis-5b1150af3418c60037552e47.png){kind=link}
aka manic-depressive
- Amitriptylin + Nortriptylin
- Imipramine, Desipramin, Clomipramine
(secondary amines have less M-cholinolytic side effects)
- Block Serotonin +NE re-uptake → antidepressive
- block H1 → sedation, ↑weight
- M-cholinolytic → urinary retention, dry mouth, constipation, blurred vision
- Block alpha 1 → Hypotension
Cardiotox! 🧪
→ sev. ventricular arrhythmias
→ >QT → Torsades
→ inverse/flat T (myocardial depression)
→ prolonged PR (AV-block)
prolonged T1/2 → single dose in chronic treatment
T → after 2-3weeks
- SSRI resistant Depression (SSRI are #1line)
- OCD (SSRI = #1line)
- Severe chronic pain
- Anxiety disorder, incl Bulimia+Enuresis
- ADHD (Stimulants = first line)
- ❤️Cardiotoxicity
- Arrhythmias (i.e. torsades)→ can be fatal
- myocardial depression
- AV block
- Serot.+NE effect:
- tremor + sweating
- tachycardia
- ⚡ seizures
- Anti-cholinergic effect (=M-cholinolytic)
- dry mouth
- constipation
- urinary retention
- blurred vision
- Alpha 1-adrenergic effect → Orthostatic hypotension D + dizziness
- Anti-histaminic: weight gain, sedation
- ↑ → then ↓ 🧠
- CNS stimulation + Convulsion
- → Sedation
- mood inversion + muscle tremor
- extra-pyramidal symptoms
- convulsion
- fever
- hypotension
- coma/death
- arrhythmias
- electrolyte imbalance
2g
- supportive → Saline solution + electrolytes
- symptomatic
- convulsion → diazepam (iv)
- Arrhythmias → Lidocaine + Porpranolol
- Anti-cholinergic symptoms (coma) → Physostigmine
block Serotonin reuptake
F → benzos are indicate in acute condition (fast action)
(SSRI need 1-2month to be effective) [bocsan: antidepressant effect - 2-4weeks])
⇒ LONG TERM TREATMENT
- Depression
- Anxiety disorders (not acute!, if acute →benzos)
- Panic attack disorder
- PTSD
- OCD (higher doses)
- Bulemia
- Fluoxetine
- Paroxetine
- Sertraline
- Citalopram
All similar effectiveness → consider SIDE EFFECTS:
- fewest drug interaction → citalopram escitalopram
- pregnancy → sertraline
- most activating, no tapering requried (long half-life) → Fluoxetine
- OCD → max dose SSRI (or even higher)
sertaline + paroxetine (the 2 in the middle)
Serotonin Syndrome 📷 → Hyperthermia, HT + ↑neuromusc. activity (↑reflexes)
{kind=link}
→ MAO + TCA ↑risk ⇒ dont give with them
→ Treat with: Cyproheptadine (Der lächelnde Cipro hebt Nadine)
LESS SIDE EFFECT
(no cardiovascular + antimuscarinic side effect)
- 🙂 Serotonin syndrome 📷
- 🍤 GI
- nausea, diarrhea,
- ↑ weight
- 🍆 sexual dysfunction
- 🚰 SIADH. 📷
- ↑/↓🧠
- ↑ insomnia, Aggression
- drowsiness
- One must be vigilant over the first 2 weeks of therapy.
- Neuro-vegetative symptoms may start to resolve during this period, but emotional and cognitive symptoms may not.
- There's a mention that patients, especially children/adolescents, might be at risk for suicidal behavior during this time.
- Concerning the onset of effect:
- Relief from neuro-vegetative/physical symptoms occurs between 1 to 3 weeks.
- Relief from emotional/cognitive symptoms happens between 2 to 6 weeks.
↑suicidal ideation on starting therapy ⇒ give benzos
flu-like symptoms + others (FINISH)
FINISH Flu-like symptoms Insomnia Nausea Imbalance Sensory disturbances Hyperarousal (anxiety/agitation)
- fibromyalgia + neuropathic pain (i.e. in diabetes)
- Depression
- Anxiety disorders
Like SSRI + ↑sympathetic (HT+↑HR, dry mouth, sweating, ↓appetite)
- Venlafaxin (Wendler macht faxen)
- Duloxetine (Zwei Oxen-Teens)
+Desvenlafaxine
"Wendler macht faxen mit zwei oxen-teens."
dulexetine → next to dual coper/scanner
Trazodone + Mirtazapin

- 5-HT receptor antagonist → 5-HT 2a+ 5-HT 2c
- Inhibit 5-HT Re-uptake
- Sedation (also H1 blocker)
- hypotension + priapism + sexual dysfunction
- serotonic syndrome
rapid
MOA = alpha2 blocker → ↑Serotonine + NE release (presynaptic)
but also 5-HT2a+c + 5-HT-3
Depression WITH insomnia, agitation
⇒ Bind als H1-R → sedation
(H1 blocker effects)
Weight gain
sedation + dizziness
bone marrow depression → do regular CBC
Buproprion
(NET DAT = Nor-epinephrin + Dopamine) (Ball pro = Buproprion)
No only NE+Dopa (NET+DAT)
It causes less..
↓ 😴 sedation
↓ 🧈 weight gain
↓ 🍆 sexual dysfunction (only delayed ejaculation as SE)
SSRI
(also useful in depression + low energy because ↑CNS effect aka less sedating)
- Nicotine dependance
- weight loss (off-label)
- ADHD
- neuropathic pain
- ↑🧠
- ❤️ CV
- Hypotension + dizziness
- Tachycardia, arrhythmia
- 🍤 GI
- N/V, diarrhea, pain
- dry mouth
- Fever
- GU: delayed sexual ejaculation
⇒ ⚡ Convulsion
Atomoxetine +Reboxetine
(Rebecca die NE-Bitch reitet auf einem Atom-Ochse)
ADHD (or give TCA instead)
PATIENT WITH DEPRESSION + PSYCHOTIC DISORDER ⇒ SGA+SSRI
→ combination of antidepressant + antipsychotic
→ aripiprazole/quetiapine (SGA) + SSRI/SNRI
→ olanzapine (SGA) + fluoxetine (SSRI)
⇒ 📷
:max_bytes(150000):strip_icc()/what-are-the-symptoms-of-schizophrenia-2953120-e15ca22957ec44ff8969cf9b8ac24568.jpg){kind=link}
Positive Symptoms | Negative Symptoms |
Hallucinations (voices that ask to do some actions) | Social isolation |
Thinking disturbances (bizarre ideas, irrational conclusions) | Lack of emotions |
Bizarre behavior, aggression, stereotypes | Lack of will |
block D2-R
FGAs → D1+D2
SGAs → D2 (selective → less SE)
(Clozapine → D4)
- ⚙️ Extrapyramidal
- 🍼 ↑PRL → amenorrhea, gynecomastia
- ❤️ CV
- ↓BP
- ventricular arrhythmias (torsades)
- ⚡ Seizures
- 💤 M-cholinolytic effect → Sedation
- ⌛ Agranulocytosis (clozapine)
- 👨🏽🌾 NMS (neuroleptic malignant syndrome) → give muscle relexants, stop antipsychotic → switch to 2nd gen after 2w
→ Acathisia (restlessness) → benzos, BB or switch to 2nd gen
→ Parkinsonims → ↓dose, switch to 2nd gen or anticholinergics
→ acute dystonia (torticolis, spasm, grimaces) → give anticholinergics
→ tardive dyskinesia (irreversible extrapyramidal; the ones above are reversible) → switch to 2nd gen
SGAS:
- also ↓negative symptoms (FGAs only positive)
- ↓ extrapyramidal symptoms, PRL, NMS
- ↓anti-cholinergic SE
- ↓Seizures
- ↓Relapse
⇒ BUT SGA → ↑ metabolic SE
- Antipsychotic → improve delirium, hallucination, aggression etc.
- Anti-nausea (i.e. haloperidol, olanzapin, phenothiazine)
- Hyperthermia induction (compare malignant neuroleptic syndrome later)
- M-cholinolytic symptoms
- Antihistaminic effects
- Alpha-adrenolytic → hypotenion
- Antiserotonic (SGAs)
- ↑PRL
- Extrapyramidal symptoms
- Schizophrenia → acute + chronic
- Mania (adjunctive to SSRI)
- Antiemetics (haloperidol, chlorpromazine, prochlorperazine)
- Neuroleptanalgesia (Droperidolul)
- Behaviour disturbance in Alzheimer (↑neurpsychiatric SE)
- closed angle glaucoma
- BPH
- constipation
⇒ antimuscarinics effects
Yes, in MANIA
- acute mania (high dose → almost max dose)
- refractory mania (lower dose)
- i.e. olanzapine + clozapine adjunctive (+SSRI)
- i.e quetiapine → mono
(see also above)
High potentcy → haloperidol
low potency → Chlorpromazine
more side effects because less specific to D2-R
(low potency ↑ sedating + hypotension)
- Haloperidol (most important)
- "azines" and "penthixols"
- Chlorpromazine (=Phenothiazine)
- Levomepromazine
- Flupenthixol
- Zuclopenthixol
Long acting FGAs
anti-psychotic | sedative | anti-emetic | |
Haloperidol | ↑↑ | - | ↑↑ |
Chlorpromazin | ↑ | ↑↑ | ↑↑ |
Haloperidol → ↑↑antipsychotic + ↑↑antiemetic
Chlorpromazine → ↑↑sedative, ↑↑antiemetic ↑antipsychotic
Levomepromazin→ ↑↑sedative, ↓antipsychotic (weak), mild analgesic
-Penthixol → ↑sedative, ↑antipsychotic, ↑anxiolytic
- Clozapine
- Quetiapine
- Olanzapine
- Risperidone
- Aripiprazol
- Ziprasidone
Acute schizophrenia → rapid control (injectable)
(→give max. for 3days)
same as clozapine
Schizophrenia (non responders) → act on pos+neg symptoms
Mania
(can be given with SSRI)
- D4 blocker
- 5-HT2 blocker
- Alpha 1 blocker → orthostatic hypotension
- m-cholinergic R blocker → urinary retention, blurred vision, dry mouth..
5-HT2 + D2
F
valproic acid
carbamazepine
lamotrigine (for bipolar)
- #1 mania in bipolar disease (+Neuroleptics + BZD)
- Acute mania
- Adjuvant in depression (with SSRI)
individualized (high inter-interindividual plasmatic variations)
T. 📷
{kind=link}
- Neuro: Tremor, ataxia, aphasia, psychosis(high dose)
- hypothyroidism
- Renal lesions
- edema + bradycardia
- skin eruptions
- cyanosis
- hepatomegaly
- Nephrogenic diabetes insipidus
(excreted in breastmilk → child lethargy)
⇒ 📷
{kind=link}
- L-Dopa → decarboxylation into DOPA (in periphery + centrally)
- Dopa-Agonists: Ropeinirole, Pramipexole, Bromocryptide, Pergolide, Rotigitin, Apomorphin
- INITIAL FIRST LINE TREATMENT!
- Amantadin → block NMDA → ↓reuptake + ↑Dopamin + antimuscarinic
- Selegiline + Rasagilin
- Tolcarpone + Entecapone → COMT-inhibitor
- Carbidopa → decarboxylase inhibitor → ↓periph conversion → more dopa bioavailability
Rigidity + bradykinesia
Øcognitive
No → other drugs are better
Øtoxic metabolites, Øconversion needed, ↓response fluctuations, ↑effect
RLS
Acromegaly + Hyperprolactemia
(it ↓PRL via D1 + partial D2 agonism)
↑emesis
rigidity, bradykinesia + tremor
mild PD + young individual
(cave: ↑adverse effects of LEVO-Dopa)
Yes or in combination with l-dopa
- GI + ulcer (!ulcer bleeding)
- Arrhythmia
- Orthostatic Hypotension
- ↑Neuropsychiatic symptoms + insomnia
- L-DOPA + carbidopa
- D2-Agonists
⇒ treatment: SGA
↑neuropsychiatric
↓others
- GI + ulcer (!ulcer bleeding)
- Arrhythmia
- Orthostatic Hypotension
- ↑Neuropsychiatic symptoms + insomnia
T → also combine with other drugs to ↓L-Dopa dosis
Tol → COMT CNS + periphery
Enta → COMT periphery only
hepatic failure → give entecapone
- Response fluctuations: on-off phenomena
- wearing off

⇒ therapeutic windows narrows when the disease progresses
- Schizophrenia / Psychosis
- Ulcer
- Cardiac diseases (L-Dopa + carbidopa)
- Hypotension
- TCA + SSRI
- (driver)
no → doesnt do shit
combine them → i.e. ↓L-dopa dose needed
- Trihexaphenidyl
- Benztropine
⇒ anticholinergic
Parkinsonism produced by Anti-psychotics
- BPH
- closed angle glaucoma
- GI-obstruction
- Øtogether with TCA + H1-Blocker
tremor + rigidity
- Topiramate → Bind GABA-A, Carbonic anhydrase inhibitor, Ca-channel blocker, ↑Na channel inactivation
- Felbamate → Ca-blocker (t-type +voltage), NMDA blocker, ↑GABA
- Valproic acid → ↑GABA + ↑Na-channel inactivation
↑GABA:

- Lamotrigine → Ca-blocker, ↑Na-ch. inactivation, NMDA blocker
- Levetiracetam, Brivaracetam → SV2A protein inhibitor
- Parampanel → AMPA-R blocker
Levetiracetam also blocks Ca-channels
Tobi trinkt ne Mate in Fellbach auf dem FestiVal. Das Lama trinkt einen Gin. Dann fährt er im Elevator hoch zum Tier-Race. Das River-Race-Team B ist auch dabei. Aber sie dürfen nicht fahren: es liegt an der Pain-Ampel.
- Generalized seizures
- focal seizures
- juvenile epilepsy
- GI
- ↑appetite + weight gain
- Liver toxicity
- pancreatitis
- tremor
- teratogenic *
- Anemia/↓thrombos → bleeding
- dysmenorrhea
- rash +allopecia
- insomnia + fatigue
- confusion + ↑CNS
- weight loss
- closed angle glaucoma
- renal/urinary stones
- GI
- aplastic anemia
- hepatic failure
"Bist am saufen in Fellbach und kotzt in nen plastik eimer der aussieht wie ne liver"

- Skin rash, SJS
- GI
- Diplopia
- Ataxia
- somnolence
- dizziness
⇒ 📷
{kind=link}
- Carbamazepin → Na-channel blocker
- Oxacarbazepin (+m-cholinolytic)
- Eslicarbazepin
- seizures: partial/focal (+ tonic-clonic)
- Trigeminal neuralgia
- Cancer pain
- Phenytoin → Na channel blocker, Ca blocker, ↓Serotonin, ↑DOPA
- Maintanance status epileptics
- Zonisamide → Na channel blocker
- Gabapentin + Pregabalin → Ca channel blocker
- partial seizures
- Post herpetic pain
- chronic pain
- neuropathie (i.e. diabetic)
- fibromyalgia
- Tiagabin → ↓GABA re-uptake (↑GABA)
- Vigabatrin → ↓Gaba transaminase (↑GABA)
- infant seizures
- refractory partial seizures (add-on)
partial seizures (adjuvant) → like RUFI
(0 order elimination)
new partial epilepsy
refractory partial seizures (add-on)
- Rufinamide
refractory partial seizures (add-on)

- Agranulocytosis + aplastic anema
- Diploplia
- Ataxia + drowsiness
- agressiveness*
- SJS + rash
- teratogenic → neural tube defect
- drug-induced lupus
- Dress-syndrome (+eosinophilia)
- ↑Na+H2O retention
- CYP 450 induction
- convulsion *
- respiratory depression, coma *
- less SE
- but m-cholinolytic
GI, neuropsycho + visual
"Der Esel hat Nie GV (geschlechtsverkehr)"
- osteoporosis
- GI
- DRESS
- ataxia + dizziness
- lupus-like syndrome
- Urticaria + SJS/TEN
- gingival hyperplasia
- hypovitaminose (folate def → megaloblastic anemia)
- teratogenic
- trigeminal neuralgia
- CYP450 induction
- diploplia
You can use the following to remember the features of PHENYTOIN: cytochrome P450 interaction, Hirsutism, Enlarged gums (gingival hyperplasia), Nystagmus, Yellow-browning of skin(melasma), Teratogenicity, Osteomalacia, Interacts with folate, Neuropathy
Neuropsych, skin, GI
- neuropsych
- ataxia
- atralgia/myalgia*
- GI
- ↓Leukos *
"Zeus ist n bisschen verrücjt und schwankt durch die gegend. Weil ihm alle muskeln so weh tun kotzt und stolpert über ein paar Leukos die auf dem Boden schlafen"
Blindness
neuropsych
"Raffi ist n bisschen crazy im Kopf und kotzt schon von einem Bier"
neuropsych + GI
- Status epilepticus (acute )→ i.v. benzos #1 line → #2line phenobarbital (barbiturate)
- benzos → resitant epilepsy
- barbiturates → drug-induced epilepsy in children + in combination with phenytoin


partial seizures
refractory (add-on)
- Neuropsych
- Blue-gray pigmentations (skin,nail,lips) → esp. after chronic high dose
Acetazolamide
minor seizures (short term)
short term: parastesia, headache, dizziness, anorexia, polyuria (like being drunk )
long term: kidney dmg → acidosis, electrolyte dysbalance

"Kleiner (Minor Seizures)Atze tatze der besoffen ist und ne niere hinter sich her schleif
Ethosuximide ( bocsan: Valproate)
valproate + Lamotrigine
block Ca T-Type channel
95-100% (yeaaaaaah)
- GI
- fatigue + somnolence
- photosensitivity
- parkinsonim
- euphoria
GABA-B agonist
spinal injury + MS
neuropsychiatric
- Benzodiazepines
- alpha 2 agonist
spinal cord injury + MS
↓Ach release
- spastic neuromuscular D.
- achalasia
- strabismus
- larynx dystonia
periph. muscle relaxation

"Christine hat n Brief von ihrem Ex bekommen: Der Brief war um ein Spinal-Cord gewickelt. Christine ist genervt von ihm (MS) und schmeißt den Brief in den Ofen (Baclofen), der er ist echt verrückt. In der Peripherie chillt Dante. Neben Dante steht Herr Schnadro Botox. Er zuckt n bisschen rum, schielt und kann nicht schlucken. AUßerdem hat er echt ne hohe Stimme (war er etwa noch nicht im stimmbruch??)"
- Intoxication phase
- Release of reward neurotransmitters and associated mechanisms in accumbens nucleus
- Determine stimuli- response type effects in dorsal striatum
- The essential neurotransmitters involved in this mechanism - dopamine and endogenous opioids
- Withdrawal (negative affect stage)
- Activation of structure in the amygdala
- Negative conditioning depends on the release of neurotransmitters: corticotrophin release facto norepinephrine and dynorphin
- Stage of preoccupation/anticipation (craving)
- strengthening the conditioning of the baso-lateral amygdala - processing of contextual information by the hippocampus
- Executive control depends on the prefrontal cortex and includes representation of possible events, representation of results, as well as their value and subjective states associated with drug abuse.(desire and probably feelings)
defined as the need to use the substance to avoid withdrawal syndrome (withdrawal)
short
it is manifested by specific behavioral disorders, sometimes of a psychotic nature, which may occur in the case of prolonged use of the substance of abuse.
- Abuse+addiction → fail obligations, drive high, continued despite social problems
- Harmful → harms somatic + mental health
- Benzos
- Methadone
- Antiepileptics: Topiramate, Gabapentin
- Methadone (both)
- Buprenorphin

- Nicotin R agonists

- Naltrexone + Acamprosat + disulfiram

Naloxone i.v. (+symptomatic treatment)
opioid receptor ANTAGONIST
→ good to block effects but not so efficient to maintain abstinence
Clonidine (alpha 2 agonist→ ↓symp. activity)
opioid receptor agonist
(risk of addiction! → lower risk with buprenorphine than with methadone)
there are none🤡
→ symptomatic treatment
- Agitation + Anxiety → BZD (Dia-,lorazepam)
- Psychotic manifestations → low dose high potency neuroleptics (azin)
- Øhaloperidol!! (↑hyperthermia, diskinesia, seizures)
- Hyperthermia → cooling, dantrolene
- Hypertension → usually no treatment, HT treatment if:
- organ lesion → Nitro, alpha blocker + beta blocker, CCB, diuretics
- no organ lesion but BP >180→ Captopril
{kind=link}
{kind=link}