
Table of content
- Rheumatology
- Poly-Articular Arthropathies Connective tissue disorders (CTD)
- Mono-Articular Arthropathies
- Oligoarticular Arthropathies Spondyloarthritis (SpA)
- Systemic Vasculitis
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Rheumatology

- Life-threatening organ involvement: → attack: Steroids + Cyclophosphamide/Myocophenolate
- SLE + mild severity = Hydroxychlorquine
- RA = MTX
- #2 lines: every cDMARD might be used (depends on location+severity)
→ Last resort: IVIG, Plasmapheresis, Rituximab, Stem cell transplant
→ maintenance: AZA/Mycophenolate
Poly-Articular Arthropathies Connective tissue disorders (CTD)
- OA
- systemic rheumatic disease (RA, SLE etc.)
- SpA (Spondyloarthritis)
- Infectious (esp. viral)
- Fibromyalgia
- Autoinflammatory (Still’s, famillial mediterranean fever)
- Metabolic diseases (Gout, Pseudogout)
- Deposition diseases (Amyloidosis, Mucopolysaccharidoses)
- Drug-induced diseases (drug induced vasculitides)
- Hep B+C
- Parvo-Virus + Rubella (endemic?)
- DGI (disseminated gonococcal infection → usually monoarthritis if not disseminated)
- Alphaviruses, EBV, initial phase of Chlamydia/Gonorrhea, early Lime disease
- Reactive Arthritis, acute rheumatic fever (Group A Strep)
- systemic disorders
- involve immunological & inflammatory processes
- unknown etiology
- RA
- SLE
- Scleroderma (systemic sclerosis - SSc)
- Dermato- + Poly-Myositis (DM/PM)
- Sjogren Syndrome
- Mixed CTD
- Relapsing Polychondritis
clinic → RA + SLE + Scleroderma + PM/DM
Ab → Anti-U1-RNP Ab
Ø fullfill classification criteria
→ e.x. lupus-like synd.
overlap syndrome = criteria for ≥2 CTD
→ ex. Rhupus (RA+SLE)
obvious shit:
- Arthralgia + Myalgia
- Rash (skin)
- Inflammatory syndrome (i.e. antibodies)
- B-symptoms
special shit: (but acutally more specific for a certain CTD)
- Raynauds
- Sicca
- Serositis
Yes → dont test for it if Ø clinical manifestations
“> 90% of patients who were referred to a tertiary rheumatology clinic for a positive ANA test result had no evidence for an ANA-associated rheumatic disease.”
T
(95-98%)
T (ANA=highly sensitive but not specific !)
HLA-DR4 (mnemonic: DRive 4 Rheuma 🚗 💨 )
- Auto-Ab (RF, ACPA[Anti-CCP] )

- Complex formation + Environmental triggers
1. INFLAMMATORY INFILTRATE → fluid in the joint + bone marrow edema
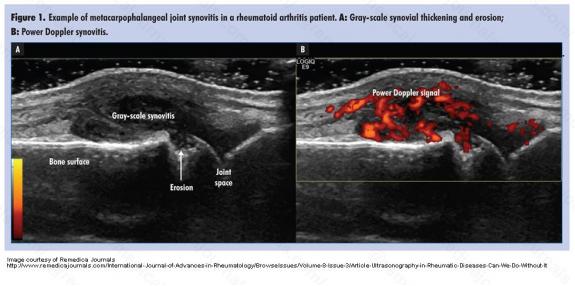
- SYNOVIAL HYPERTROPHY + PANNUS 📷
⇒ bone erosions + cartilage dmg (→narrow joint space)
- 🚬
- viruses + bacteria

female 35-50y
6weeks
(otherwise it could be an infection)
small joints (hand + feet) + later large joints (elbow, spine, knees, ankle , foot)
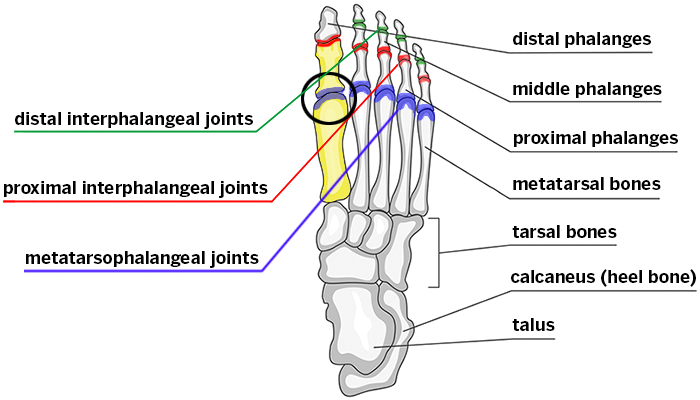
- MCP
- PIP
- Wrist
MTP📷 (+ankle)
symmetrical
(OA=asymetrical)

INFLAMMATORY PAIN
↓pain with activity
↑pain with rest (worse during night+morning)
(opposite to mechanical pain in OA)
>60min
- Ulnar deviation
- Boutonniere deformity
- Swan neck deformity
- Z shaped thumb
- MCP subluxation
Nodules 📷→ filled with cholesterol when you biopsy them
RF/ACPA + HLA DR4 +

- General B-symptoms
- Derma → nodules
- CV → various heart pathologies + vasculitis
- Lungs
- Eye
- Osteoporosis
- Hema: anemia, ↑plts
- Neuromuscular
- ”General manifestations: Fever, lymphadenopathy, weight loss, fatigue
- Dermatological: Palmar erythema, rheumatoid nodules, purpura
- Ocular: Episcleritis, scleritis, nodules in the sclera, scleromalacia perforans, keratoconjunctivitis sicca
- Neuromuscular: Carpal tunnel syndrome, peripheral neuropathy, mononeuritis multiplex, inflammatory myopathy
- Bone: Osteoporosis
- Cardiovascular: Pericarditis, myocarditis, conduction defects, valvular defects, coronary vasculitis, nodules
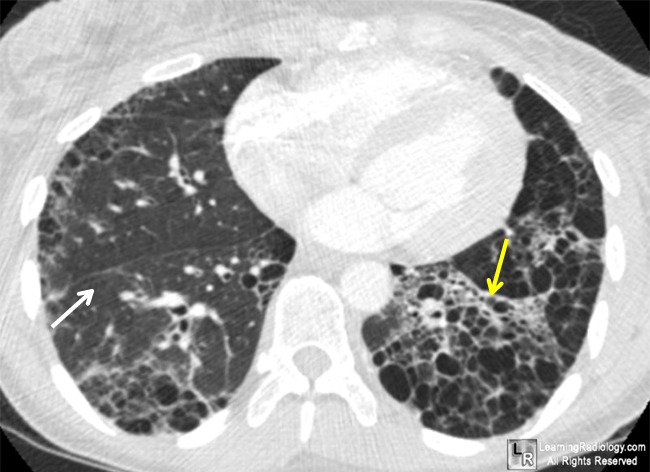
- Pulmonary: Pleural effusion, interstitial lung disease, nodular lung disease, obstructive lung disease
- Hematologic: Anemia (normocytic, normochromic), thrombocytosis, thrombocytopenia and leucopenia in Felty's syndrome; leukocytosis in Still's disease; lymphoma (Hodgkin and non-Hodgkin)
- Other EAM: Amyloidosis”
if location: C1, C2 → probably RA
→ Xray
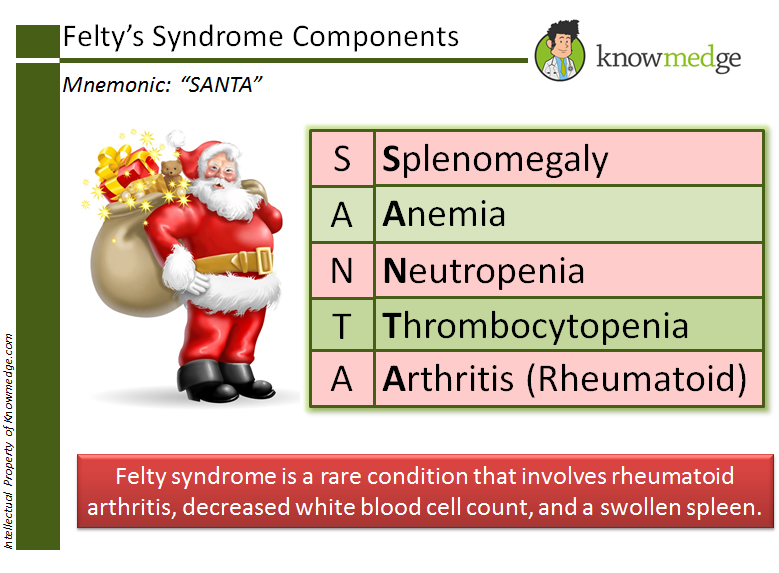
Felty = RA + Neutropenia + Splenomegaly + ↓Plts 📷
Still’s = RA + ↑Np + evanescent (”salmon”) rash + fever (39°>1w)

⇒ Both ANA +
⇒ Felty’s RF +
⇒ Stills’s RF -

- handicapped
- after 2 years → mod. handicaped
- some after 10 years → sev. handicaped
- some during first 10y → incapable of profess. life
- psychological disorders
- CV events
MI, stroke
- polycyclic (70%): intermittent or continuous, incomplete remission or progression
- monocyclic (20%): Significant remission in 1st year
- progressive(10%) = malignant: Continuous, generalized; poor prognosis
- ESR + CRP
- CBC → Anemia, ↑plts (n/↑ leukos)
- Rheumatoid factor (RF) → If RF neg.→ its probably Ø RA
- Anti-CCP ( ACPA)→ if CCP is pos. → its probably RA
- erosions?
- panus?
- deformities?
- periarticular osteopenia/osteoporosis?
- narrow joint space
US
pulse doppler → suggestive if PD+ 📷
also shows fluid collection + synovial hypertrophy
- Arthrocentesis → inflammatory joint: Np >2k but < 50k
- MRI → bone marrow edema (earliest sign of imflammation aka early detection of joint inflammation in RA)
Xray + US
(rarely MRI)
XRAY (+MRI)
- Lab → ESR + CRP
- US
- MRI
1887:
≥4 criteria for ≥6weeks:
- Morning stiffness: >1 hour
- Arthritis of ≥ 3 joints
- Arthritis of small joints (RC, MCP, PIP, and hand arthritis)
- Symmetric arthritis
- Rheumatoid nodules
- Rheumatoid factor positive
- Specific radiographic changes (erosions)
2010:
≥ 6 = definite RA
- Joint distribution:
- 1 large joint - 0p
- 2-10 large joints- 1p
- 1-3 small joints (large joints not counted)- 2p
- 4-10 small joints (large joints not counted)- 3p
- 10 joints (at least one small joint)- 5p
- Serology:
- Negative RF AND negative ACPA- 0p
- Low positive RF OR low positive ACPA- 2p
- High positive RF OR high positive ACPA- 3p
- Symptom duration:
- <6 weeks- 0p
- ≥6 weeks- 1p
- Acute phase reactants:
- Normal CRP AND normal ESR- 0p
- Abnormal CRP OR abnormal ESR- 1p
predni + NSAID(symptomatic)
GI, cardiac, renal

#1 line MTX → everbody

#2 line add-on other cDMARDS
#3 line bDMARDS (biologics) → inflixi-, rituximab 📷
#4 line tsDMARDS → Jak inhibitors

T
CV → CV drugs
osteoporosis → anti-osteoporotic drugs
Hep B +C
folic acid


- adequately vaccinated?
- TB test?

- Fungi?
→ if you downregulate the immunesysteme these things will fuck the patient up
- infections
- herpes zoster
- thromboembolism (if CV-RF)




can be assoc. with lupus
→ thrombosis
→ fetal loss
→ thrombocytopenia
→ anti-phospholipid Ab (anti-cadiolipin, lupus anticoagulant)
→ (livedo reticularis)
“SOAPBRAIN MD” 📷


anti-phospholipid
- CNS: Aseptic meningitis, Cerebrovascular disease, Demyelinating syndrome, Headache (including migraine and benign intracranial hypertension), Movement disorder (chorea), Myelopathy, Seizure disorder, Acute confusional state, Anxiety disorder, Cognitive dysfunction, Mood disorder, Psychosis
- PNS: Acute inflammatory demyelinating polyradiculoneuropathy (Guillain-Barré syndrome), Autonomic disorder, Mononeuropathy (single/multiplex), Myasthenia gravis, Neuropathy (cranial), Plexopathy, Polyneuropathy
check anti-phoslipid Ab + Neuro-workup

- The lupus band test is performed on a skin biopsy using direct immunofluorescence staining.
- It helps to distinguish between systemic lupus erythematosus (SLE) and cutaneous lupus.
- In SLE, the lupus band test is positive in both involved and uninvolved skin.
- In cutaneous lupus, only the involved skin shows a positive result.
- The test detects the deposition of IgG and complement at the dermoepidermal junction.

- Infections
- CNS vasculitis
- Artherosclerosis → CV-events
- Kidney failure
yes
(but classic for scleroderma (systemic sclerosis) + mixed connective tissue disorders)
Follow up: Complement + dsDNA
Renal activity: Protein-/Hematuria





(+lifestyle measures in general + stress coping mechanism)!

(double click)

+DM + skin atrophy/strechmarks/easy bruising

Ro/La + Cardiolipin → CLOSE HEART monitoring

safe → hydroxychlorquin, steroids, AZA
(cyclosporin → pregnancy warning but no general contraindication)

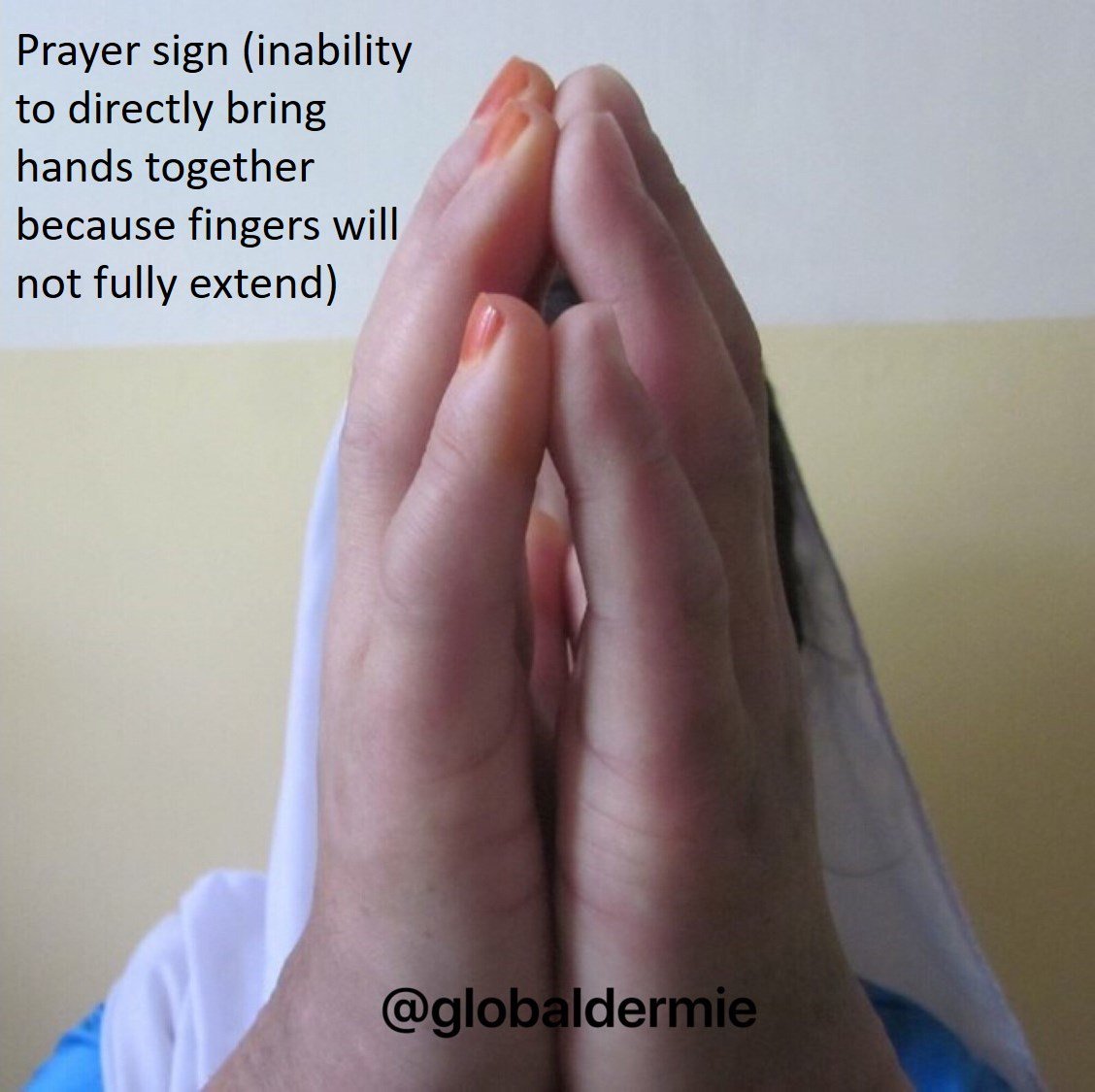
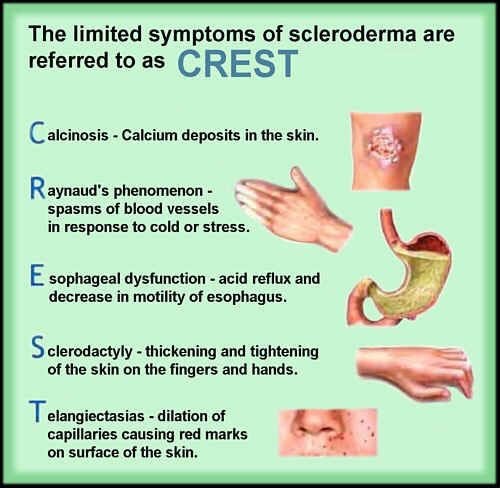
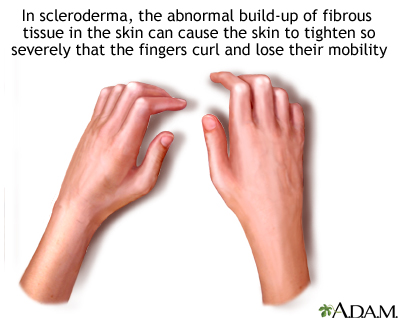
“aka systemic scleros is (SSc)”
collagen depositions → stiffness where it deposits
Raynauds
(white → blue → red, triggered by stress+cold)
Secondary Raynauds:
- Signs for inflammatory rheumatic disease → clinic, ANA+, ESR↑
- > 30y
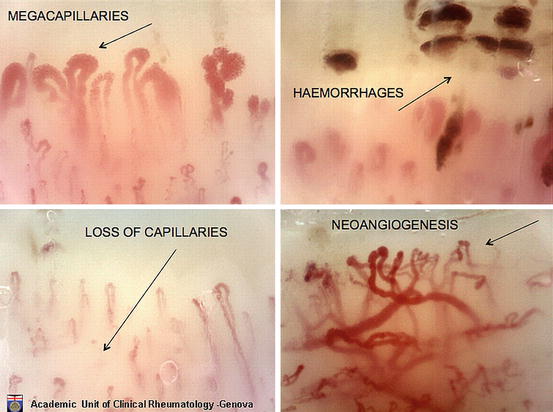
- Signs of ischemic episodes:
- capillaries normal in primary RF
- abnormal in secondary RF
→ clinic: painful + asymetric
→ Ulcers + Gangrene + pitting scars
→ Abnormal nail-fold capillaries
- Edematous phase : Puffy edema in the fingers
- Indurative phase: skin becomes thickened. The skin appears shiny and tight. Skin creases are lost. Erythema may be present. In limited scleroderma, this process continues slowly for many years.
- Atrophic phase: Late in the course of scleroderma, the skin becomes fragile and lax as it enters the atrophic phase. Patients with limited scleroderma find that the advancement of skin disease occurs slowly, over many years. By definition, skin involvement remains distal to the elbows and knees, although it can involve the face and neck.
LCSS → mainly limited to face, forarms, hand, feet DCSS → diffuse (everywhere)
LCSS → Raynauds YEARS(>1y) before skin involvement
DCSS → Raynauds max. 1y before skin involv. (or concomitant or after)
Raynauds in LCSS appears >1y before skin
Raynauds in DCSS appears randomly (before (<1y),during or after)
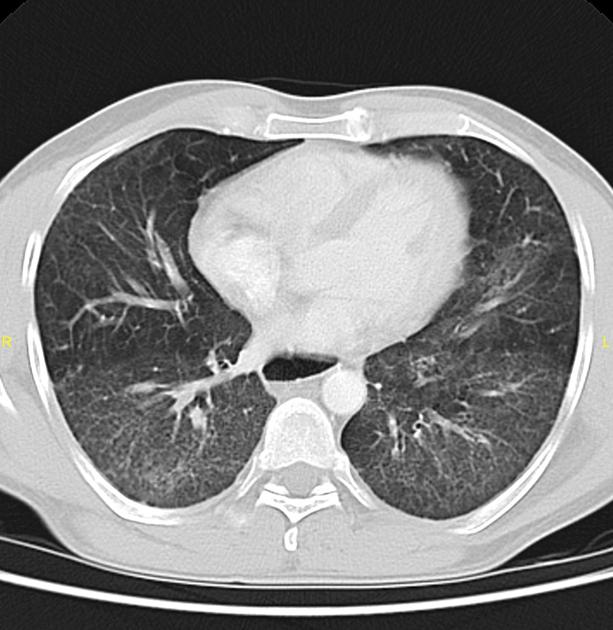
DCSC = LCSS +visceral involvement (lung, heart, kidney)
→ lungs → interstitial lung disease +/- PHT
→ heart
→ myocardial fibrosis → restrictive cardiomyopathy(DCSS) + conduction abnormalities(LCSS)
→ pericardial effusion
→ valvular abnormalities (rarely symptomatic)
→ early Atherosclerosis
→ kidney → sclerodermal renal crisis (SRC)
→ GI
→ esoph. reflux → esophagitis→ strictures + Barrets
→ hypomotility
→ esoph. hypomotility
→ gastroparesis, intestinal pseudo-obstruction,
→bacterial overgrowith, diarrhea
→ malabsorption, weight loss
LCSS→ PHT w/o any damage to the lungs
DCSS→ Interstitial lung disease → secondary PHT (but PHT is act. rare in DCSS)
- GI endoscopy
- Manometry → esoph. hypomotility?
- Barium swallow → esoph. strictures
- Abdominal Xray/CT
- ECG + holter → conduction abnormalities?
- Echo → pericardial effusion + fibrosis? valves?
- MRI → earlier detection than echo
- NT-proBNP → if HF
rapidly progressive RF + malignant HT + ↑Renin(plasma)
- RF → ↑Crea +/- proteinuria/hematuria
- general HT signs
- Retinopathy
- microangiopathic hemolytic anemia
Severe arterial hypertension with abrupt onset
→ Clinical manifestations: headaches, malaise, encephalopathy (confusion, neurologic signs), pulmonary edema
severe form of SSc, CV-D, polymerase 3, steroids
- DCSS
- rapidly progressive cutaneous
- duration <4y
- Anti-RNA polymerase 3 Ab
- CV impairment
- Anemia
- Heart-involvement
- ↑↑dose steroids
- LCSS (CREST) → Anti-Centromere
- DCSS (Scleroderma) → Anti-Scl70 (=topoisomerase)
- Anti-RNA polymerase 3 (↑SRC risk)
(ANA)
F → never give steroids in renal crisis caused by scleroderma! → precipitates further 🚑
→ give ACEi
there is none 🤡→ only symptomatic
⇒ SYMPTOMATIC TREATMENT FOR...?:
nothing 🤡
Penicillamin
PPI
- Eating behavior + diet
- Prokinetics
- Recurrent diarrhea or pseudo obstruction → AB + pro-biotics
non-pharma:
- avoid cold+stress exposure
- avoid digital trauma
- Øsmoking
- stop vasoconstrictive drugs
pharma:
- #1 CCB
- PG-analogs (i.e Ilprost)
Endothelin-R antagonist (Bosentan)
→ refractory? → combination with: PDE5-inhibitor (Viagra)
ACEi
→ refract.?→ Dialysis / kidney-transplant
- like in lupus nephritis
- induction: Cyclophosphamide
- Maintenance: AZA
- Alternative: Myocophenolate mofetil
- bDMARDS: Tocilizumab (Anti-IL6)
- Anti-fibrotics (TK-inhibitor: Nintedanib)
- Bosetarn + viagra
- Iloprost
(like digital ulcers)
- 📜 rapid progressive cutaneous
- 🫁 Interstitial lung diseases
- 💪🏽 joint/muscle inflamm.
- 🫀heart inflamm.
- cDMARDS = classic
- Cyclophosphamide, AZA, Mycophenolate
- MTX + Cyclosporin A
- bDMARDS
- Tocilizumab (interstital lung D)
- Rituximab (others)
= same as #2line lupus/lupusnephritis
pulmonary involvement (25%)
unknown etiology → inflammation of:
→ muscles
→ skin (if skin manifestations present = dermatomyositis)
→ visceral organs

- Heliotrope rash 📷 📷
- hand joints, ellbow, knee: Gottron's papules 📷 📷
- Shawl sign 📷 + V sign 📷 → UV-exposed areas (4)
- prox. symmetrical muscle weakness (5)
- visceral involvement (6)
- Nails = Cuticular overgrowth 📷 + Manicure sign 📷(teleangiectasis around nails)

→painless + subacute
Herr V (v sign) mit seinem Schal 🧣 (Shawl sign) fliegt im Heli über den Tropen 🚁 🏝 (Heliotrope). Er kann nicht aufstehen und selber laufen deswegen Heli (Proxy Sym. Muscle weakness). Er will zu seiner Ischen Gutrun Pap (Gottron Papules) zur Manicure 💅 .
onset: local swelling
later: muscle atrophy + muscular contractures
occular muscles
inflammation + pain ⇒ BUT NEVER EROSIVE
(somehow like lupus) 🐺
T
- Lungs
- GI
- Heart - rare
Interstitial lung disease
(like scleroderma)
esophageal dysmotility
diarrhea + constipation

⇒ can be assoc. with almost every 🦀 malignancy (screen!)
lymphomas, breast cancer, ovary, lungs, colon, gastric cancers
Anti-synthetase syndrome (ASS)
PM/DM + 🫁 Interstitial lung diease
check muscle + antibodies
- CK ↑ + other muscle enzymes (LDH, AST, ALT)
- EMG
- Muscles biopsy (DDx betw. PM + DM)

- MSA (Myositis-specific-Ab):
- Antisynthetase Ab → Anti-Jo + Anti-Mi
- Anti-SRP
- MAA (Myositis-assoc.-Ab):
- ANA (i.e. anti-PM-Scl)
anti-Jo
- non-pharma: muscle exercise
- #1 steroids
- #2 Immunosuppressives → MTX + AZA
- pulmonary involvement? → like lupus-nephritis (cyclophosphamide + Myophenolate)
- cutaneous → like lupus #1: hydroxychloroquine
- #3 iv.Ig, Plasmapheresis, stem cell
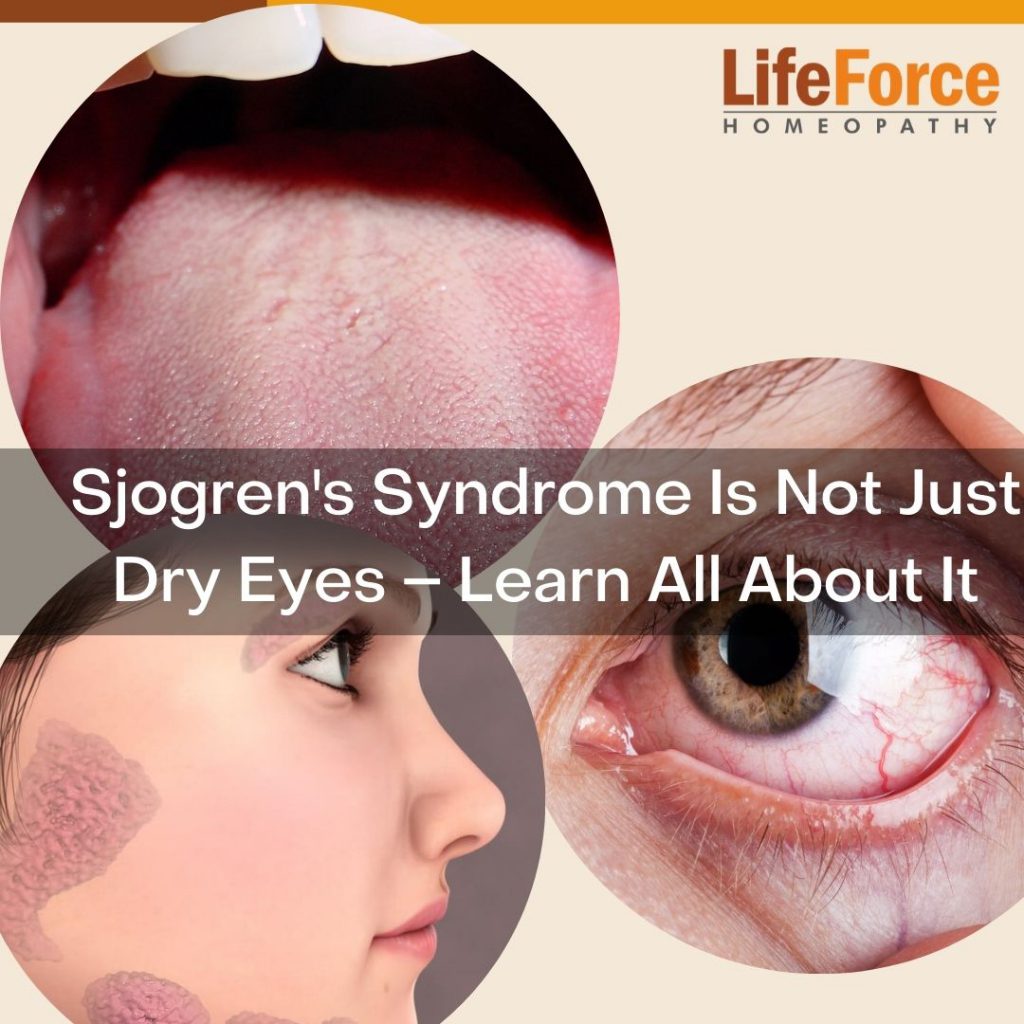
(pronounced “show-grins” syndrome)
Lymphoplasmocytic (mononuclear cells) infiltration of the exocrine glands (i.e. salivary glands) 📷→ destruction
- 👁️ Dry eyes (Xerophthalmia)
- 👅 Dry mouth (xerostomia)

- 🦜 Parotid swelling

- Past radiation + HepC → dry eyes + mouth
- Diabetes → dry mouth + parotid
- red eye
- ulceration
- perforation → dry keratoconjunctivitis 📷
- oral candidiasis
- dental: caries + peridontitis

- MALT (also is a NHL)

- NHL
- Check for Ab:
- ANA, RF
- Anti-Ro, Anti-La
- Hypergammaglobulinema
- ↓ complement
- Cryoglobulinemia
- SLE
- RA
- Scleroderma
- DM/PM
- Eye:
- ☂️ Schirmer test 📷→ can they make their own tears?
- Use small calibrated filter paper strips inserted under the lower lid for 5 minutes
- Less than 5 mm moistening of the paper indicates classification criterion for the disease
- 🌹 Rose Bengal test + Slit lamp → ulceration?
- Salivary gland
ALL OTHER CLASSICS! (above)

- Artificial tears
- Artificial saliva + gum + Tx candidiasis
- Extraglandular:
- mild: NSAIDs + Hydroxychloroquin
- mod-severe: Steroids +/- cDMARDS
MTX, AZA, MMF, CYC (depending on site and severity of organ system involvement)
≥2 CTD aspects
overlapping clinic of systemic sclerosis, SLE, and polymyositis
↑ anti-U1 RNP

like SSc + PM
- Arthralgia
- “Scleroderma-like” HAND → hand edema, sclerodactyly, raynauds
- “PM-like” → Myositis
CAN PRESENT LIKE EVERY CTD
- Raynauds + Myositis
- polyarthritis + edema (symmetrical)
- all kinds of CTD cutaneous manifestations
- ILD + PH
- GI manifestations (dymotility)
- Cardiac involvement
- Sjögrens
PHT → regular echo check-ups
raynauds
Tx like the constituent CTD
recurrent inflammation cartilage → destruction cartilagenous tissue
- Ear
- outer ear → “cauliflower” ears 📷 (bilat. aricular chondritis)
- inner ear → cochlear + vestibular dmg
- Eye → Conjuncitivits + (-itis)
conjunctivitis, keratitis, episcleritis, uveitis, chemosis
- Nose → “saddle nose” (nasal septum collapse) 📷
- Trachea + Larynx collapse → ❗respiratory failure
- Arthritis
- CV*
- Renal*
- Systemic vasculitis*
clinic + histo
empiric immunosuppressiva
tracheostomy
- Female (betw. 30-50y)
- specific Pain
- generalized (axial + extremities bilat.) aka pain “all over”
- diffuse widespread (hard to describe)
- chronic
- other distribution then polyarthropathies - little joint focus
- worse AFTER activity
- Fatigue
- Sleep problems
- Anxiety
- Psychosomatic diseases
- IBS
- Migraines
- RLS
- Raynauds
- etc.


IN GENERAL NORMAL!!

there might be some tender points
weird radiation of the pain

- Primary
- Secondary
- other inflammatory rheumatic D (RA,SLE, AS)
- OA
- Hypothyroidism
unclear (but non-immune + non-inflammatory)
→ central sensitization (↑CNS response to simulus) → hyperalgesia + allodynia

→ impaired desc. inhib. pain pathways
→ disturbances of neurotransmitters
⇒ ↑ pain perception
→ psychological + behavioral response → new or different region of chronic pain
ENVIRONMENTAL TRIGGERS + BAD SLEEP
Cold Warm Temperature changes Humidity Non-restorative sleep Noise Oter factors: light, smells, touch
exclusion




usually not needed
evtl for DDx:
- CBC + ESR
- Elektrolytes
- specific Ab (RF, ANA)
- Thyroid markers
- muscle enzymes
- Hepatitis C serology
- Lympe serology
- Self management:
- exercises + physio
- sleep education
- cognitive behavioral therapy (CBT)
- avoid trigger
- Drugs
- Anti-depressents + Anti-convulsants (for the treatment of chronic pain)
- TCA
- SSRI
- SNRI (psychiatric + pain)
- Gabapentin + Pregabalin ( pain)
- OTC pain-relievers:
- NSAIDS + Paracetamol

(double click to zoom)

Mono-Articular Arthropathies
INFLAMMATORY + mono-articular
- red
- hot
- swollen
- tender
- toxic
Inflammatory → Septic, Crystals
Non-inflammatory (1-2 joints) → OA, trauma
Non-Articular → Bursitis, Tendonitis

💉 arthrocentesis → synovial fluid examination
- Cellulitis overlying the joint
- Skin lesions or dermatitis overlying the joint
- Known bacteremia
- Adjacent osteomyelitis
- Uncontrolled coagulopathy
- Joint prosthesis (relative contraindication, arthrocentesis preferably done by an orthopedist)
String test → low viscosity 📷
Total leuko count + PMN proportion:
Category | Appearance | WBCs, cells/µL | PMN cells |
Normal | Clear | < 150 | < 0.25 |
Noninflammatory (OA, trauma) | Clear | < 3000 | < 0.25 |
Inflammatory | Cloudy | > 3000 | < 0.75 |
Purulent (septic) | Cloudy | > 50,000 | > 0.9 |
Hemorrhagic | Bloody | > 2000 | ~ 0.3 |
CULTUREEEEEES
- GRAM
- for gonococcal → GRAM + hemoculture + uretral, rectal, oropharynx culture
F → sepsis might be present at the same time → !esp. when sepsis-symptomatic present
- Crystal deposition and sepsis can coexist, so it is important to culture synovial fluid if sepsis is suspected clinically.
- In undiagnosed joint effusions, it is recommended to search for PPD and MSU crystals.
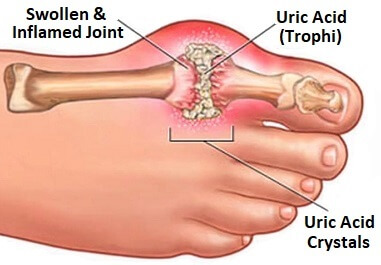
Inflammatory:
men >40y
(in women delayed → after menopause)
1-15%

... of uric acid
- non-modifiable RF:
- male
- age
- +FH
- genetic predisposition
- Hyperuricemia
- ↑intake:
- food (meat + seefood)
- alcohol
- ↓excretion:
- RF
- Obesity
- Hypertension

(double click)


*TLS

- Recurrent arthritis attacks
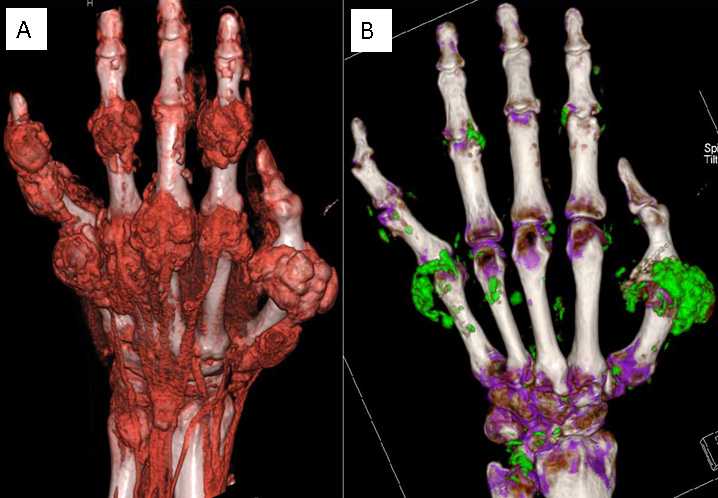
- Tophi
- Renal damage
- Renal stones (Nephrolithiasis)
metabolic syndrome (also tumor lysis Sdr.)
→ HT + dyslipidemia
Gout is associated with: Hypertriglyceridemia Low HDL-cholesterol Obesity Hypertension Insulin resistance
ischemic heart diseases → gout might cause MI
(metabolic sy)
acute gout attacks → PODAGRA 📷 (=pain in MTP [or distal interphalangeal joint])

- ↑uric acid
- Øsigns+sy: Ø arthritis, Ø tophi, Ø renal
Gout risk is associated with serum uric acid concentration:
- > 7 mg/dL (0.42 mmol/L) for men
- > 6 mg/dL (0.36 mmol/L) for women
- acute hyperuricemia (ex. TLS)
- Uric acid > 12
intense pain:
- FOOT
- PODAGRA (MTP or DIP)
- or: prox. foot (tarsus, ankle)
- KNEE
- PROX. ARMS+HANDS
- ELLBOW
- WRIST
- FINGER
Inflammation of the surrounding tissue:
- tendonitis
- cellulitis
→ stretching + gnawing + tightening
The intervals between attacks of gouty arthritis are referred to as intercritical periods. A patient who has intercritical gout simply has gout that has caused attack(s) of gout in the past, but is asymptomatic at the time the doctor is evaluating the patient.
- ↑uric acid levels
- +crystals in the joints (but asymptom.)
- attacks are:
→ polyarticular
→ longer
→ more severe
- tophi around the joints (intra-articular + soft tissue)
- leads to disability
- Progressive destruction of the joints
(arthrocentesis+) synovial fluid analysis
ARTHROCENTESIS of gout:
- >2k WBC but <50k
- Ø Germs (negative microscopy+culture)
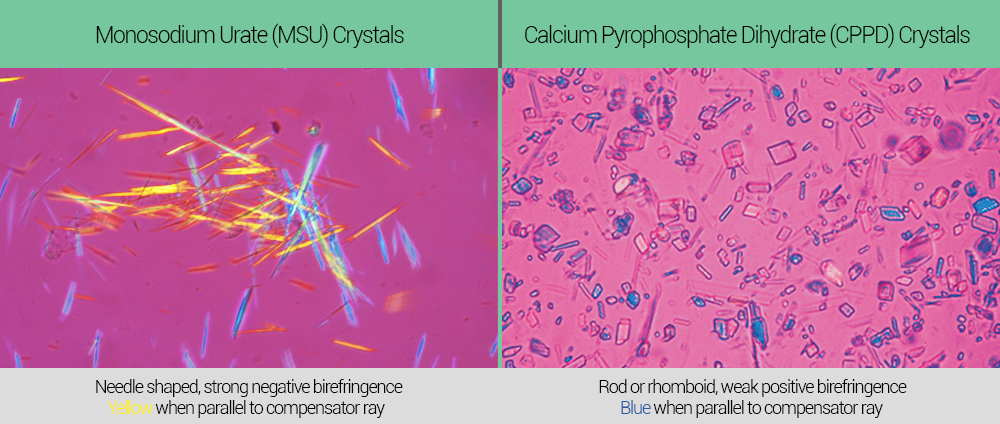
- + Crystals (under polarizing microscopy)

POLARIZED LIGHT MICROSCOPY:
- Gout: mono-sodium urate + negative birefringent
- Pseudo-Gout: Ca-pyro-phosphate + pos. birefringent

CHECK URIC ACID + KIDNEY + METABOLIC SYND. + DDx Septic 👍🏼
- Uric acid → serum + urinary
- Renal function
- Inflammatory (Leukos) → DDx septic (+hemoleucogram→ exclude proliferative hema disorders)

- Metabolic syndrome profile → Lipid + Gluc profile
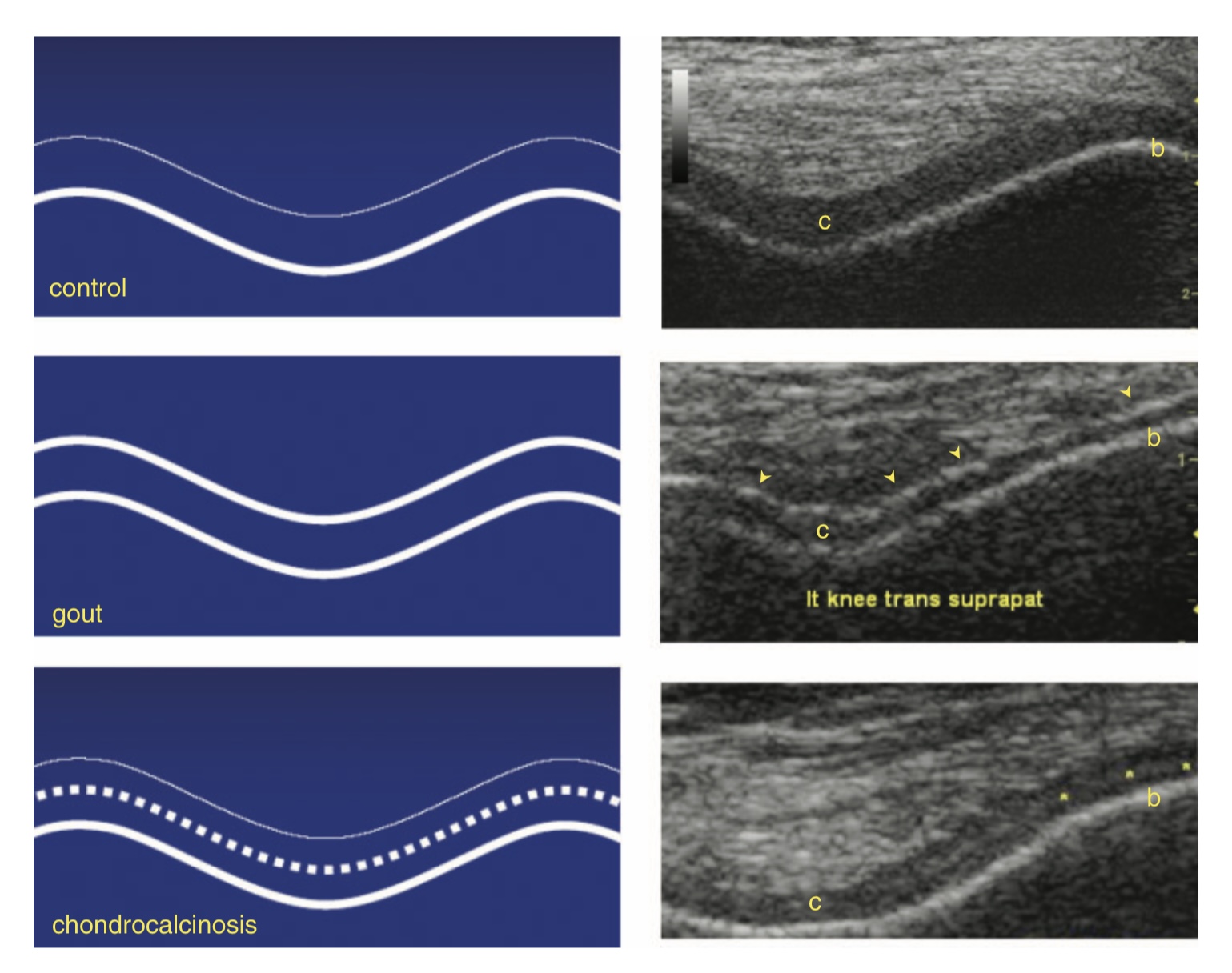
- synovial fluid can Ø be aspirated → Dgx of Gout via US (only during intercritical period)
- Dgx tophi (Øaspiration needed)
- DDx pseudogout
- Gout = double-contour sign 📷
- Tx monitoring
- appreciate dissolution of tophi → Tx adjustment accordingly

- ↓Uric acid
- ↓Inflammation during flairs
- prophylaxis of flairs
- Tx of associated disorders (metabolic synd)
Colchicine, NSAIDS, steroids


- Lifestyle (esp. diet + Ø alcohol) + stop thiazides

- Urate-lowering: #1Allopurinol or Febuxostat
-2nd line: Uricosuric drugs: Benzbromarone, Probenecid, Sulfinpyrazone
→in moderate RF; allergy to allopurinol
→ contraindicated if ↑urinary uric acid (↑ stone risk)
-3rd line: pegylated Uricase (severe refractory chronic)

- Prophylaxis → #1 Colchicine or NSAIDs (or Steroids)
-2nd line: Canakinumab (≥3 attacks/year and #1 line fails)


at the same time urate-lowering therapy is started
at least 6 month
<6
- hypersensitivity syndrome
- 👺 SJS [steven johnson syd]
(can trigger acute gout attack)
- hypertensive Tx → losartan (uricosuric effect)
- hyperlipidemia Tx → fenofibrate (uricosuric effect)
- Chondrocalcinosis: Calcium pyrophosphate deposits in joint spaces (in cartilage) with radiological appearance
- Pseudogout: Acute arthritis caused by the release of calcium pyrophosphate in the joint
- Pyrophosphatic arthropathy: Structural lesions associated with calcium pyrophosphate deposits
old (>60y)
KNEES
(and fist: triangular fibrocartilage)
DEGENERATIVE X-RAY FINDINGS
- Calcification → of connective tissue: ligaments, tendons, capsule
- joint-space narrowing (assymetrical)
- osteophytes
- subchondral sclerosis
- calcium-pyro-phosphate crystals
- small sticks
- weak positive birefringence
Gout | Chondrocalcinosis | |
Male:Female | way more common in male (7-9:1) | almost same (1,4:1) |
Maximum Incidence Age | 40-50 years | > 60 years |
Predilect joints | MTP I | Knee |
Serum uric acid | ↑ | normal |
Radiological appearance | ||
Calcification | Usually absent | Present |
Erosions | Can be characteristic | Often degenerative |
Crystals | ||
Type | Monosodium urate | Calcium pyrophosphate |
Shape | Acycular | Small sticks |
Birefringence | Intense negative | Weakly positive |


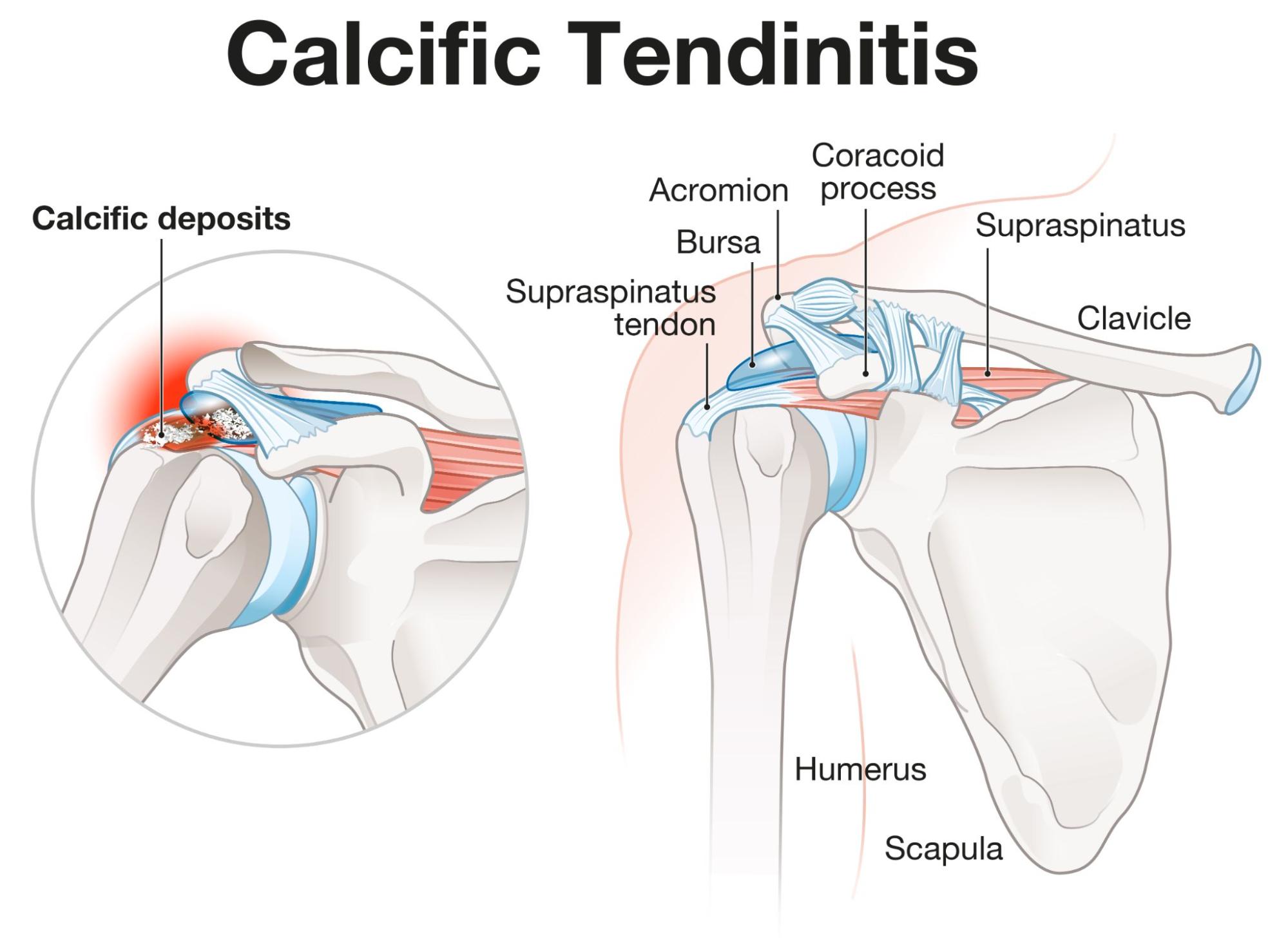
Calcific tendinitis
(HA-deposition in tendons)
Rotator cuff → 80% Supraspinatus 📷
“shiny coin” appearance with alizarin red 📷
Øbirefringend
- NSAIDS and/or intra-articular steroids
- US-guided aspiration
- surgery
OA

F
Caused by bacteria, mycobacteria, fungi or parasites

monoarticular (20% = polyarticular)


- pain
- loss of function
- swelling
- warmth
- red
- +/- fever
STAPH AUREUS
typical patient:
- remote infection in patients with ↓immunity (elderly, small children, immuncompromised)
- iv drug user
- direct innoculation (trauma, surgery)

- genitourinary diseases is often asymptomatic
- tenosynovitis hands + ankles

- rash📷
- migratory polyarthritis
- fever

- Arthrocentesis → synovial fluid analysis
⇒ Culture + GRAM (joint + blood )

- Arthrocentesis → synovial fluid analysis
⇒ 🔬 GRAM - & 🧫 hemo-cultures + (chocalate agar) → also of oropharynx, rectum, vagina
⇒ PCR
- Consider imaging in all cases (MRI/CT)

- 1) 💉Joint drainage
F → start before: HISTORY + typical patient ‼️
⇒ GRAM STAIN !!!

Cefriaxone single I.M. dose !
⇒ Doxy / Azithro to cover Chlamydia
Gram-Neg. Rods: Cover pseudomonas⇒ 🖼️🪐 PSEUDOMONAS-BETALACTAMS (Ceftazidime, Cefepime, Piperacillin-tazobactam)
negative (unclear) Gram stain ⇒ COVER ALL ⇒ 🖼️🪐 PSEUDOMONAS-BETALACTAMS + 🚌 VANCO (cover MRSA)
Degenerative:

degenerative disease → focal cartilage loss
→ bone erosions
→ bone repair → osteophytes

F → can be mono, oligo + poly!!!
T
- hand → CMC1, PIP + DIP (MCP might also be involved esp MCP2+3)
- spine
- hip
- knee

- swollen + tender joint
- mechanical pain (worse with activity, better w/ rest)
- restricted movement
- morning stiffness <30min
- deformities (i.e. Heberden + Bouchard nodules)
- Øextra-articular manifestations + Øsystemic inflamm. signs ‼️

- radiation towards medial thigh above the knee
- ↓int. rot + adduction (cant bring it in)
- patrick’s test + 📷
- Patrick's test or FABER test is used to assess hip joint or sacroiliac joint pathology.
- The test involves flexing the tested leg and abducting and externally rotating the thigh.
- If anterior pain is felt on the same side, it suggests a hip joint disorder.
- If posterior pain is felt around the contralateral side of the sacroiliac joint, it suggests dysfunction in that joint.

- episodic inflammation
- Baker cyst
- muscle hypotrophy (quadrizeps)
- deformation + instability

Direct Dgx of OA =
pain + morn. stiffness <30m + funct. limitation + 1 more typical
Xray
- Joint space narrowing
- Subchondral sclerosis
- subchondral cysts
- Osteophytes


- >65y?
- Comorbidities?
- Steroids?
- History ulcer/bleeding?
KIDNEY!
- >65y?
- ↓Renal function → ↑Crea?
- CV overload: HT+CHF?
- Drugs: Diuretics, ACEi?
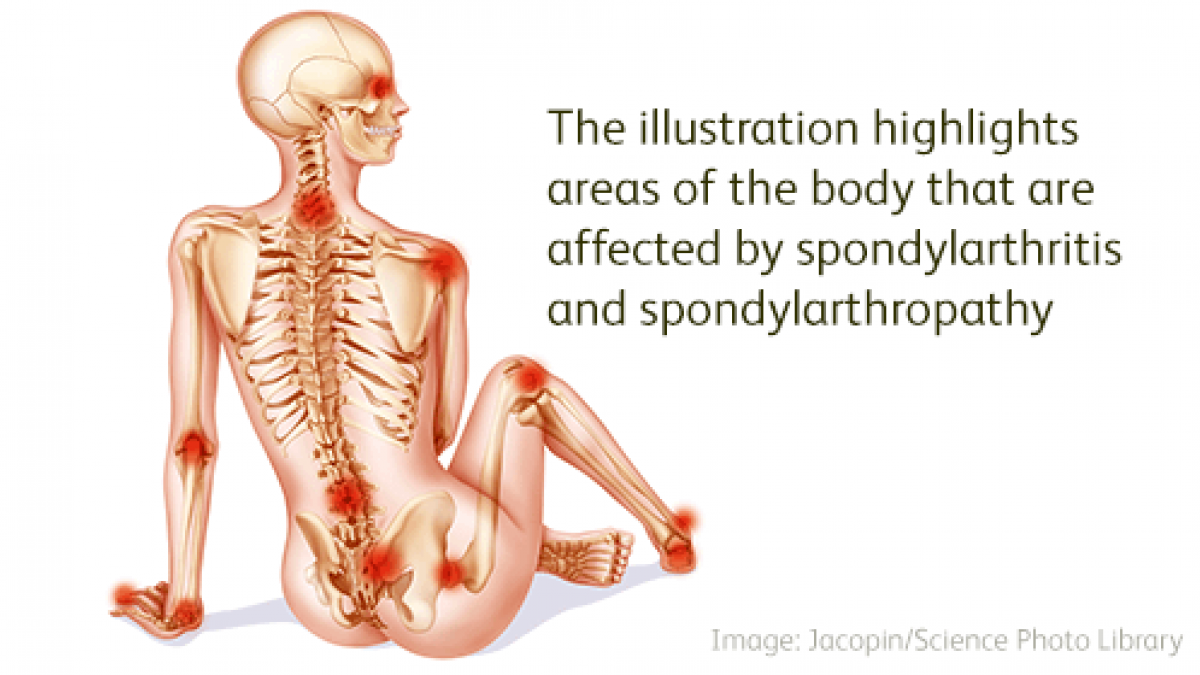
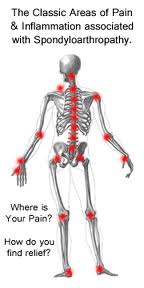
Oligoarticular Arthropathies Spondyloarthritis (SpA)
T
(difference to the others!)
- Suspicion of cancer / inflamm / trauma?
- age: <20 or >50y
- B-symptoms (cancer, inflammatory)
- noctural (inflammatory + cancer)
- PMH
- cancer, osteoporsis, steroids
- trauma/recent infection
- Periph neuro def. (i.e paresthesia, motor deficit, radiation)
→ activity → ↓pain in inflammatory but not in cancer
look for etiology (imaging - esp. Xray + MRI) → immediate Tx!
<6w
(also Ø RF + ANA check)
2-4 joints
asymetrical
- Common variable back pain
- OA
- discprolapse
- SpA
PAIR
- Psoriatric arthritis
- Ankylosing spondylitis
- IBD associated ankylosing spondylitis/SpA

- Reactive arthritis
- Juvenile SpA
only ankylosing spondylitis + IBD assoc. = symmetrical
rest = assymetrical
Characteristics | AxSpA | Reactive arthritis | Juvenile SpA | Psoriatic arthritis | IBD associated SpA |
Age of debut | < 40 | 20-50 | 8-16 | 20-50 | Adult |
M/F Ratio | M:F = 3:1 | M > F | M > F | M = F | M = F |
Debut | insidious | acute | variable | variable | insidious |
Sacroiliitis or spondilitis | 100% | < 50% | < 50% | ~ 20% | < 20% |
Sacroiliitis symmetry | symmetric | Asymmetrical | variable | asymmetric | symmetric |
mainly reactive + psoriatic (+juvenile)
Characteristics | AxSpA | Reactive arthritis | Juvenile SpA | Psoriatic arthritis | IBD associated SpA |
Age of debut | < 40 | 20-50 | 8-16 | 20-50 | Adult |
M/F Ratio | M:F = 3:1 | M > F | M > F | M = F | M = F |
Debut | insidious | acute | variable | variable | insidious |
Sacroiliitis or spondilitis | 100% | < 50% | < 50% | ~ 20% | < 20% |
Sacroiliitis symmetry | symmetric | Asymmetrical | variable | asymmetric | symmetric |
Peripheral arthritis | ~ 25% | ~ 90% | ~ 90% | ~ 95% | 15%-25% |
You can copy and paste this into a word processor to maintain the table structure. If you need the table to be formatted in a specific way or to include additional data, please provide the details.
Characteristics | AxSpA | Reactive arthritis | Juvenile SpA | Psoriatic arthritis | IBD associated SpA |
Age of debut | < 40 | 20-50 | 8-16 | 20-50 | Adult |
M/F Ratio | M:F = 3:1 | M > F | M > F | M = F | M = F |
Debut | insidious | acute | variable | variable | insidious |
Sacroiliitis or spondilitis | 100% | < 50% | < 50% | ~ 20% | < 20% |
Sacroiliitis symmetry | symmetric | Asymmetrical | variable | asymmetric | symmetric |
Peripheral arthritis | ~ 25% | ~ 90% | ~ 90% | ~ 95% | 15%-25% |
Eye inolvement | 25-30% | ~ 50% | ~ 20% | ~20% | <15% |
T
(inflammation of the whole digit)
psoriatric + reactive
(can involve hands or feet → “sausage-like digits”)
all of them 🤡
inflammatory joint → pain+swelling & stiffness>60min
assymetrical → esp in lower limbs: knee, ankles, digits 📷
Common manifestations of SpA:
- Musculoskeletal manifestations:
- Inflammatory low back pain
- Peripheral arthritis
- Enthesitis
- Dactylitis
- Extra-skeletal manifestations:
- Cutaneous features
- Ocular features
- Intestinal features
- Genitourinary features
CV, kindey, GI
- Cardiovascular: aortitis, aortic regurgitation, conduction disturbances
- Kidney: IgA nephropathy, kidney amyloidosis
- Digestive: Inflammatory bowel diseases
⇒ deposition + IBD-relation
None 🤡 (no RF, no ANA)
HLA-B27 esp. + in ankylosing spondylitis
→ familiar!
→ there are also other markers: IL23R + ERAP1

+Ddx workup (non rheumatologic disease → common varibale back pain, OA, disc proloapse etc ⇒ look for clinic, red flags + MRI if necc.)
+Lab: Inflammatory markers (CRP/ESR)
MRT → early detection +active → bone marrow edema in osteitis
CT → chronic erosions + sclerosis
BOTH FOR DETECTION OF COMPLICATIONS! (fracture, anderson’)
Anderson' = Aseptic spondylodiscitis
Definite ankylosing spondylitis: If the radiological criterion is associated with at least 1 clinical criterion
peripheral skeletal arthritis (not in axial skeleton aka spine)
TNFalpha → infliximab ; IL-17 blocker → cosentyx
- Treatment for SpA must be personalized based on subtype, joint affectation (peripheral or axial), presence of extra-articular disease, and comorbidities.
- AxSpA: NSAIDs and biologic agents (TNFi and IL-17i).
- Peripheral SpA: NSAIDs, corticosteroids, cDMARDs (MTX, LEF, SSZ), biologics (TNFi, IL-17i, IL-12/23i), JAKi.
- signs of symmetrical sacroilitis
- signs of nerve compression
- radiation!
- alternating buttock pain
- good response to NSAIDs
- thorax + hip pain
- inflammatory pain + stiffness
- awaking in second half of the night
- stiffness >60
- ↑pain at night + rest → ↓with activity
- Inflammatory pain on axial skeleton
- Sacroiliac joint involvement
- Modification of vertebral spine at any level
- Arthritis on hip (coxitis) and shoulders
- Anterior thoracic pain due to involvement of chondrocostal joints and chondrosternal entheses.
ant. uveitis → unilateral + recurrent
⇒ can lead to synechias + visual loss

BASDAI & ASDAS
mainly chlamydia trachomatis
- Urogenital: Chlamydia trachomatis, Ureaplasma urealyticum
- Enterogenic: Salmonella, Shigella, Yersinia, Campylobacter, Clostridium
Reiter’s syndrome 📷
Keratoderma blennorrhagicum: Descuamative erythema on soles and palms 📷
only in chlaymdia-caused reactive arthritis

Relationship between infections and ReA
Postenteric (Gastrointestinal) | Postvenereal (Genitourinary) | |
Entrance | Gastrointestinal | Genitourinary |
M:F Ratio | 1:1 | 9:1 |
Infection | Symptomatic | Asymptomatic (60%) |
Frequency of RA post-infection | 1-15% | 5% |
Microorganisms | Yersinia, Salmonella, Shigella, Campylobacter | Chlamydia trachomatis |
Bacterial detection in synovial fluid | - | + |
#1 NSAIDs #2 intraarticular steroids #3 DMARDs (MTX/Sulfasalazine)
⇒short-term AB if trigger infection present → check the genitals bro

asymetric oligoarthrits
→ pencil-in-cup deformities 📷
- unilat. sacroiliitis
- axial parasyndesmophytes (bulky paramarginal spurs) 📷
T 👁️
F ⇒ Peripheral arthritis!!! (Øaxial!)
Peripheral Arthritis | Spondylitis | |
Prevalence | More common | Less common |
Gender Distribution | Equal ratio of males to females | More common in males |
Joint Involvement | Lower limbs more commonly affected | Spine and sacroiliac joints affected |
Type of Arthritis | Acute, self-limited, recurrent, migratory | Can be chronic, involving small and large joints |
Association | Correlates with inflammatory bowel disease's activity | Independent of inflammatory bowel disease's activity |
Extra-intestinal | Strongly associated with other extra-intestinal manifestations | Associated with uveitis, strongly associated with HLA B27 |
perform colo
ØNSAIDS! + Tx IBD → with sulfasalazin → infliximab
Systemic Vasculitis
- Clinic
- BIOPSY = Gold standard
- Angiography → if Øbiopsy possible (Takayasu, PAN)
- Lab:
- Inflammatory markers (ESR, CRP, etc)
- Organ markers (kidney, liver)
- ANCA
- Etiology: HepB+C serology + cultures
- Suggesting for immune-complexes
- RF + ANA
- Cryoglobulines
- Complement
- Giant cell (temporal) arteritis
- Takayasu arteritis

GC → Granuloma + fiboris of intima
Takayasu → Granuloma


1- Early inflammatory aka pre-pulseless phase
2- Late ischemic aka pulseless phase
early inflammatory → pseudoinfective signs+symptoms (non-specific) + self-limited
late ischemic: → Neuro signs + pulselessness
→ coronary
→ renal ischemia
→ mesenteric ischemia
polymyalgia rheumatica (PMR)
- Persistent pain (for at least 1 month) involving neck, shoulders, and pelvic girdle
- Morning stiffness lasting more than 1 hour
- Rapid response to prednisone (20 mg/day or less)
- Age over 50 years
- ESR (erythrocyte sedimentation rate) over 40 mm/hr
- Absence of other diseases causing similar musculoskeletal symptoms

+ OTHER INFLAMMATORY MARKERS
AT LEAST 4:
- Age at onset > 50 years
- New headache
- Temporal artery abnormality (tenderness, ↓pulsation)
- ↑ ESR
- Abnormal artery biopsy (mononuclear cells, granulomatous inflammation, multinucleated giant cells)
AT LEAST 4:
- Age at onset < 40 years
- Claudication of extremities
- Decreased brachial arterial pulse
- BP difference > 10 mmHg
- Bruit over subclavian arteries or aorta
- Arteriogram abnormality (aorta or aortic branch or large extremity artery narrowing/occlusion → focal or segmental changes)
both: #1 steroids → #2 DMARDS (MTX) for maintainance if necessary
Takayasu: +Antiplatelets + #3 PTCA / Surgery

after steroids!!! → direct Tx dont wait → possible irreverible blindness
- Polyarteritis nodosa (PN)
- Kawasaki disease
- CNS vasculitis
- Burgers diseases
Hep B
complex mediated → focal segmental necrotizing vasculitis → Aneurysm (+thrombosis)
Alternating areas of necrotic vasculitis + fibrotic lesion (healed) ⇒ typical imaging appearance(see below)
all organs can be affects → NEVER LUNGS!!
most common:
🥐 renal artery
🍤 mesenterial artery
🌕 nerves
- Renal artery → HT (hematuria, oliguria, RF)
- mesenteric → GI pain + melena
- nerves → periph. neuropathy ⇒ MONONEURITIS MULTIPLEX 📷
- +SKIN LESIONS
- coronary arteries → MI
- Genitals → orchitis
- Arthralgia/Myalgia
Mononeuritis multiplex: painful, asymmetrical, asynchronous sensory and motor peripheral neuropathy
→ serology for surface Ag + (HBsAg)
ANCA/ANA negative
angigraphy (like takayasu)
string + pearls of renal artery


BIOPSY
EMG / ENG → for neuro-muscular evaluation
- Induction: cyclophosphamide + steroids
- Maintenence: AZA/ Myophenolate (+steroids?)
- Anti-HepB → Entecavir
- Organ specific Tx
- Uncontrolled BP
- Anuria (RF)
Asian <5y
CRASH and BURN on a KAWASAKI
- Conjunvtivits (bilat)
- Rash: Polymorphous non-vesicular
- Adenopathy (cervical)
- Strawberry tongue + cracked red lips
- Hand+foot: red palms + soles
- Burn: Fever >5d
⇒ 📷
CORONARIES!!
→ thrombosis → MI
→ Aneurysm → rupture
→ other 🫀-pathos: Myocarditis, Pericarditis, valvulopathy, arrythmias
ASS + IVIg
ASS:

⇒ if i.v.Ig fails → Inflixmab, i.v. steroids, plasmapheresis
⇒ if multiple/large coronary aneurysm → anticoagulation

Wegener (GPA) | MPA | Churg-Strauss (EGPA) | IgA | Cryo | |
“C-Disease”* | !relapses | Asthma | children, following URI | HepC | |
Necrotizing Granuloma | ✅ (giant c.) | Ø | ✅ (w/ Eos+giant) | Ø | Ø |
Necoritzing vasculitis | ✅ | ✅ | ✅ | Ø | Ø |
Eosinophilia | Ø | Ø | ✅❗ | Ø | Ø |
👃 (NP, URT) | ✅❗ | Ø | Ø | Ø | Ø |
🫁 | ✅ (nodules+DAH) | ✅ (ILD+DAH) | ✅ (non-excavating nodules. ØDAH!!) | Ø ❗ | Ø ❗ |
🥐 (kidney) | ✅ | ✅ | (rare) | ✅ | ✅ |
🫀 | ✅ | Ø(?) | ✅ | Ø❗ | Ø❗ |
⚡ periph. neuropathy:
mononeuritis multiplex | ✅ | ✅ | ✅ | ✅ | ✅ |
👁️ | ✅❗ | Ø (?) | Ø | Ø | Ø |
🦵🏼 skin (purpura, necrosis, blisters) | ✅ | ✅ | ✅ | ✅ | ✅ |
palpable purpura | Ø | ✅❗ | Ø (?) | ✅ | ✅ |
💩 GI | Ø | Ø | Ø (?) | ✅❗ | Ø |
ANCA | cANCA | pANCA | pANCA | Ø | Ø |
Complex deposition | Ø | Ø | Ø | IgA | IgG+IgM |
Glucocorticoids | ✅ | ✅ | ✅ | ✅ | ✅ |
Cyclophosphamide | ✅ | ✅ | ✅ | Ø❗ | ✅ |
NSAIDS | Ø | Ø | Ø | ✅❗ | Ø |
+HepC Tx |
“C-disease”*

- ❓ Idiopathic
- 🧫 Infection (bac + viral)
- 🛡️ systemic AI disease (CTD, IBD, primary biliary cirrhosis, etc)
- 💊 Drugs
- 🦀 Neoplasia (esp. HEMA-CANCER → leukemia, MM)
arteriols, capillaries + veins
(Ø aorta + its branches!)
- Granulomatosis with polyangitis (GPA=Wegeners granulomatosis)
- Microscopic polyangitis (MPA)
- Eosinophilic granulomatosis with polyangitis (EGPA=Churg-Strauss syndrome)
cANCA → proteinase 3
pANCA → MPO (myeloperoxidase)

Asthma! (+ periph. eosinophilia)→ adult on-set

- rhinitis + rhinosinusitis

- “saddle nose” deformities
- mucosal ulcers
- ear infection
- bilateral nodules (xray) = necrotizing granulomas
- cough, pain
- hemoptysis
- diffuse alveolar hemorrhage (rare but fatal)
nodules damage pulmonary small vessel → blood into alveoli → 🚑!!
diffuse alveolar hemorrhage (DAH) + Rapidly progressive GN

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rapidly progressive (focal+segmental) glomerulonephritis (necrotizing)
segmental fibrinoid necrosis 📷
{kind=link}
- Eye → proptosis, chemosis (unique for wegeners!)
- Arthralgías/myalgias
- Skin → livedo reticularis, (leg) ulcers
- CNS → aseptic menigitis
AT LEAST 3 POSITIVE FOR DG!
- Oral ulcer / nasal discharge (NP)
- XRay: nodules (lung)
- Microhematuria or proteinuria (kidney)
- Biopsy kidney or lung positive
RP GN (like wegeners) → might lead to HT
pulmonary capillaries → hemoptysis + diffuse alveolar hemorrhage (→pulmonary-renal syndrome)
+ILD! (unique feature)
no! - ØDAH!
(important difference)
AT LEAST 5:
Asthma-relating
- Asthma (in almost every patient)
- Eosinophilia
- Paranasal sinus abnormalitis
- Xray: infiltrates/non-excavating nodules
- Biopsy: Extra-vascular eosinophils
fibrosis + CHF
proteinase 3
C-ANCA (cytoplasmic anti-neutrophil cytoplasmic antibodies): Diffuse staining of the neutrophil cytoplasm 📷
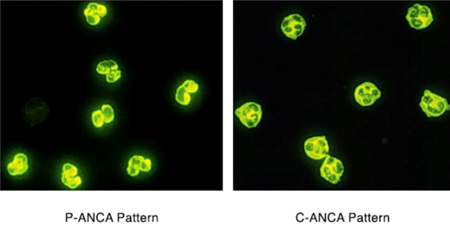{kind=link}
→Recognizes proteinase-3, which is present in the primary granules of the neutrophil.

all steroids + cyclophosphamide
alternative: other cDMARDS
step up: bDMARDS (Rituximab)

urinary bladder tox → hemorrhagic cystitis, carcinoma

- IgA vasculitis (Henloch-Schönlein purpura)
- Cryoglobulemic vasculitis → mixed type (II+III)
- Cryoglobulinemia is characterized by the presence of serum immunoglobulins, known as cryoglobulins, that precipitate at temperatures below 37°C and redissolve upon rewarming.
- There are three types of cryoglobulinemia:
- Type I: Monoclonal cryoglobulinemia without rheumatoid factor (RF) activity, associated with malignant hemopathies.
- Type II and III: Mixed cryoglobulinemia, consisting of both IgG and IgM with RF activity. Type II is monoclonal, while Type III is polyclonal. These types are associated with autoimmune diseases, chronic infections, and predispose to B-cell lymphoma.
- + small vessel cutaneous
most common vasculitis in children
FOLLOWING 🧣URT infection
Hep C
(compare with PAN → HepB)
It is also assoc with lupus, multiple myeloma and myeloproliferative disease
IgA → IgA
Cryo → IgG+M

temperature → low temperature
DETAILS:
IgA GN
→ (mainly presenting with isolated) hematuria
→ nephrotic synd
IgA deposition in intestinal submucosa → edema + hemorrhage → pain + melena → fecal occult blood test +
might even cause intussception
buttocks + legs
ulcers
glomerulonephritis (membranoproliferate)

- Lab:
- IgA
- inflammatory syndrome
- Skin biopsy → IgA depositions
- Urine → hematuria
- Lab:
- Serum Cryoglobulines
- RF + (eg. Creatinine)
- ↓C4
- HepC+
- Elektrophoresis: IgM kappa chains
- Biopsy → vessel / kidney
The big 4 C´s
IgA: usually self limited
⇒ but can be #1 NSAIDs → #2 Steroids → #3DMARDS can be given in severe forms of nephritis (Azathiprine) but usually not needed
NSAIDS for arthritis → relatively common in IgA
consider anticoagulants

all
(large, medium, small)
(arteries + veins)
neutrophil infiltrations (non-granulomatous )
→ tissue necrosis → blood clots + aneurysm
- recurr. Oral + genital ulcers
- Uveitis (panuveitis or post. uveitis) ⇒ might lead to vision loss
- Skin lesions
(features of lupus + SpA)
- Pseudofolliculitis
- Erythema nodosum
- Papulopustular lesions
PATERGY TEST 📷 (pin prick: skin lesion doesnt heal in 48h)
{kind=link}
Skin pathergy test positive: presence of erythematous papule or pustule at the site of needle prick after 48 hours
- CV → thrombosis + aneurysm
- arthritis
- GI (pain)
- CNS (meningitis)
- kidney
- Lung
- Steroids
- DMARDS
- if severe uveitis → Anti-TNF
- Anti-platelet/anticoagulants