




Oncology & Radiotherapy
Onco Lab
- chemical RF
- tobacco
- cyclophosphamide
- others
- Infections
- repeated UTI (ex. due to stone)
- parasitic → schistosoma = flatworm
- Metabolic
- dietary: ↑fat ↓fluid
- abnormal tryptophan metabolism
urothelial carcinomas (95%)
(5% = SCC, AdenoCa, etc.)
- non-muscle invasive (insitu + exophytic)
- muscle invasive (→local extension, lymphatic spread, mets)
- hematuria
- gross ⇒ considered BladderCa until proven otherwise
- microscopic
- irritative bladder symptoms (dysuria, ↑freq.)
- advanced:
- pelvic / bony pain (bone invasion)
- leg edema (illiac vessel compression)
- flank pain (uretereal obstruction → hydronephorosis)
- Urinary cytology (missed 30% of + cases)
- Cytoscopy + TUR-B → muscle invasive or not?
- Imaging
- CT → abdomen, pelvis + thorax
- MRI + Pet → abdomen + pelvis
- Bone scinti (if bony pain)
- Lab:
- Renal + liver function
- CBC
- T4b or
- Any N + or
- M +
Non-muscle invasive or muscle-invasive?
↓
→ non-muscle invasive:
TUR-B +/- intravesical chemoT/BCG vaccine
→ muscle invasive:
- Cystectomy + pelvic LN
- Bladder preservation: maximal TUR-B + neoadj. chemo/CRT
Mets? → Chemo + ImmunoTx
Age, Black,
Western diet,
FH, genetic (BRCA1,2)
- urinary symptoms
- obstructive symptoms (weak stream, incomplete emptying)
- UTI (freq + urgency, dysuria)
- advanced → lumbar pain (bone mets/ para-aortic LN mets)
- DRE
- PSA
- Endorectal US
- Biopsy (US guided, fusion) → At least 6 core
- MRI (pelvic or whole body)
- CT (chest, abdomen)
- Bone Scinti (if clinic, PSA>20 or intermediate risk)
- PET
Bone Mets:
SPINAL COMPRESSION SUSPECTED → CT MRI → confirm bone Mets + compression
Emergency treatment!! → surgery/ RT (within 48h)
Grading of aggressiveness / differentiation
G1-G5
(Most common + second most common)
→ Risk + Tx assessment
Patients urinary symptoms before treatment → if very symptomatic → don’t start RT give Hormone first
Low: Gleason <7 PSA <10
Intermediate: Gleason=7; PSA 10-20
High Gleason >7 PSA >20
Take into consideration
- Gleason
- PSA
- TNM
- Life expectancy + comorbidites
- Surgery (robotic, lapa, classic)
- Radiotherapy (ext +/- brachy)
- Hormonal (adrogen deprivation - surgical or LHRH agonist, anti-androgens)
Metastatic + hormone resistance → chemo
- systemic
- hormone
- chemo
- target
- palliative RT
CT (+/- markers for prostate) or MRI before each fraction
→ compare with baseline target volume +/- corrections
High dose - iridium needle (temporary)
Low dose - palladium/ iodine seeds (permanent)
Classic (inflammation, strictures/stenosis, fistula)
ESP rectum bladder
- undescended testicle = cryptorchidism
- FH + genetic → Klienefelters
- already cancer related: CIS or previous cancer of the testicles
GERM CELL TUMORS
- Seminoma
- non-Seminoma
both → betaHCG + LDH
non-seminoma → alpha-fetoprotein! (seminoma does not produce AFP!)
seminoma → LN spread + Ø hematogenous
non-seminoma → LN + hematogenous
follow the route:
liver → lung → bone + brain
- Epididymitis / Orchitis (inflamm. of testicles or epididymus)
- Painless mass
- Lumbar pain (para-aortic LN involv)
- Gynecomastia (due to ↑bHCG)
- Mets- + B-symptomatic
- history + physical exam
- palpation of testicles + inguinal LN
- US
- CT chest, abdomen, pelvis
- Lab **→ Tumor markers (bHCG, AFP, LDH) + CBC, liver+renal function
- neuro signs → MRI(brain)
- bone pain → Scinti
DONT TAKE A BIOPSY!!!!! (↑risk of dissemination)
Histo → AFTER REMOVAL of the testicles
Stage 1: N0
Stage 2: N+
Stage 3: M+
Unilateral radical orchiectomy
Seminoma → consider adjuvant RT or Chemo
→ chemo only if M+
Non-Seminoma → consider adjuvant chemo
BLEOMYCIN!
SURGERY → fistula
CHEMO → hema + non-hema (GI, lung fibrosis, Nephro-, neuro-, oto- tox)
RT → secondary Lymphome
- #1 SCC → exocervix
- AdenoCa → endocervix
HPV
- vaccination
- papsmear
- + hpv test
- dont smoke
- condome + limited sexual partners

- Vulva + Vagina
- Penis
- Anus
- Oropharynx
16 + 18
- ↑ sexual activity
- early onset
- multiple partners
- other viruses → herpes simplex, HIV
- smoking
- immundef. + Vit A+C def.
- multiparity
pap test
colposcopy → punch biopsy or Conization → described as cervical intra-epithelial neoplasia (CIN)
CIN I (mild)→ follow up
CIN II (mild-moderate) + III (severe) → conization or cryo or LEEP
- asymptomatic woman: ages 20-65 yo
- starting at 3yrs after first sexxxual intercourse
- woman >70 yo may stop screening of cytology was normal the last 10 yrs
VAGINA → BLADDER; URETHER, RECTUM; ILLIAC VESSELS
- abnormal vaginal bleeding
- vaginal discharge (leucorrhea)
- B-symptoms (weightloss, appetite, fatigue, anemia)
→ after sexual intercourse + intermenstrual, menorrhagia,
INVASIVE:
- urinary symptoms (dysuria, ↑freq., hematuria)
- Rectal invasion → constipation, rectorrhagia
- lumbar pain → Hydronephrosis (acute RF) or para-aortic mets
- unilat. leg edema (illiac vessel compression
- gynecological exam
- DRE
- abdomen/pelvis CT + contrast or MRI /PET
- CT/ Xray thorax
- advanced: cystoscopy / rectoscopy
- Lab: CBC, renal+liver markers, urine samples, CA125, CEA
FIGO
Stage 1: confined to cervix
1a microscopic tumor
1b1 ≤4cm
1b2 >4cm
Stage 2: beyond cervix
2a: Øparametrial invasion
2b: parametrial invasion
Stage 3a → lower 1/3 of vagina
Stage 3b → pelvic side wall OR hydronephrosis
Stage 4
4a: spread to rectum / bladder
4b: distant mets
para-aortic
Main treatment modalities: Surgery (Conization or TH+BSO) AND/OR RT/RCT
(⇒ in 2B ⇒ RCT (+/- surgery))
1A
- Total hysterectomary
- OR Conization (young)
- OR Brachytherapy
1B - IIA
- Surgery (Total hysterectomy + bilat. salpingo-oophorectomy + pelvic LN) + adjuvant RT
- OR RCT
2B-4A
- RCT(+/- followed by surgery)
4b
- palliative Chemo or RT
- targeted therapy (bevaciuzumab)
classics
acute: inflammation of sourrunding structures:
- colitis
- cystitis
- vaginitis
late: stenosis + fistula
- vaginal + urethral stenosis
- rectovaginal + vesicovaginal fistula
⇒ unbalanced/high Estrogen (ENDOMET) + genetic+FH!
ENDOMET:
- elderly
- nulliparity (never been pregnant)
- Diabetes*
- Obesity*
- menstrual abnormalities OR vaginal bleeding after menopause
- estrogen monotherapy*, late onset menopause
- hyperTension *
- genetic: lynch synd. II( HNPCC )
- FH: endometrial cancer
AdenoCa
- abnormal vaginal bleeding
- in menopause = probably endometrial Ca (until proven otherwise)
- vaginal discharge (leukorhea)
- compressive symptoms → parametrial invasion → ureteral obstruction
- Gyn-exam + DRE
- Imaging
- US (abdominal)
- Chest Xray / CT
- MRI / CT / PET → pelvis + abdomen
- rectoscopy + cystoscopy (advanced)
- Lab
- CA125
- CBC
- renal+liver
- Biopsy (curettage)
- pelvic
- para-aortic
TNM
FIGO
operable → TH+BSO +/- adjuvant RT or Chemo
non-operable/extrauterine → RT (+/- surgery after)
Limited to uterus
Operable
→ Surgery (TH+BSO)
- total hysterectomy
- +bilat. slpingo-oophorectomy
- +/- pelvic/para-aortic LN dissection
→ +/- adjuvant Radiotherapy → external + brachy
→ Chemotherapy
Non-operable
Radiotherapy (ext + brachy)
Extra-uterine
Radiotherapy +/- Surgery after
Brachytherapy, also called internal radiation therapy, places radioactive material directly inside or next to the tumor. It uses a higher total dose of radiation to treat a smaller area than external beam radiation therapy (EBRT) which directs high-energy x-ray beams at a tumor from outside the body.
temporary → sticks (iridium) - high intensitiy
permanent → seeds (iodine) - low intensity
+ femoral head fx
acute: inflammation of sourrunding structures:
- colitis
- cystitis
- vaginitis
late: stenosis + fistula
- vaginal + urethral stenosis
- rectovaginal + vasicovaginal fistula
- instestinal occlusion/perforation
- femoral head fracture
- regular follow up → 1stY: every 3m; Next years: every 6
- clinical exam
- xray
- US
- CT
- CA-125
- educate about recurrence symptoms
- educate about SE of Tx (RT)
- reduce RF (HT, obesity+DM, estrogen monotherapy)
- FH + Genetic: BRCA1+2 + Lynch
- Elevated number of ovulations
- early menarche + late menopause
- nulliparity
- lifestyle + obesity
oral contraceptives
breastfeeding + parity
serous AdenoCa
- salpinx + uterus
- peritoneum
- Mass
- Abdominal pain + distension/bloating
- abnormal vaginal bleeding (metorrhagia, post-menopause)
- urinary symptpoms (freq+urgency)
- B-symptoms
- Late: Ascitis+bowel obstruction + dyspnea (due to ascitis/pleurisy)
- physical (pelvic) exam
- US (pelvic + endovaginal)
- CT /MRI pelvis/abdomen
- Chest Xray
- Lab: CA-125
CONTRAINDICATED! → might cause direct spread to peritoneum
→ HISTO AFTER surgery!
Surgery
- TH + BSO + LN (paraaortic+pelvic)
- omentectomy
- all involved organs + peritoneal mets
+/- adjuvant chemo
- HIGH ESTROGEN
- Benign BREAST DISEASES (hyperplastia, CIS etc)
- GENETIC: BRCA1+2 + Lynch
- Lifestyle: alcohol + smoking
- Radiation
→ ENDOGENOUS: obesity, nulliparity, early menarche/last menopause, late 1stpregnancy
→ EXOGENOUS: Estrogen replacement (after menoP) or contraception
Follow the lymphathic route
- lung + pleural
- bone
- CNS
- liver
- mass + pain
- palpable axill. LN
- retraction nipple
- discharge
- skin
- skin ulcers
- “orange peel” + red skin
- advanced: bone pain +dyspnea
- normal-risk woman: Mammography from age 40, annually
- high-risk woman: Mammography from age 30, annually
- Breast-US: from age 35, annually, complementary to mammography
- palpation (breast + axilla)
- Mammography (2 planes) + US
- Biopsy
- Lab:
- Tumor markers: CA 15-3, CEA (+ CBC/liver/renal)
- Hormone-Receptor testing → Estrogen + Progesteron R
- HER2 testing
- Imaging for Mets
- CT (chest, abdomen, pelvis)
- Scinti (bones)
- MRT (brain+breast)
- PET
dye into Tumor that leads to sentinel LN
- Surgery
- Radical mastectomy + LN
- Breast conservation + LN → adjuvant RT
- neoadjuvant / adjuvant RT or Chemo
- Hormonal Tx (if hormone R +) → oophorectomy or LHRH analogues
- Targeted Tx: Trastuzumab (if HER2+) → in comb. with chemo or Hormone
(”trust her too”)
- Hema
- GI
- Heart
- osteoporosis
- endometrial cancer
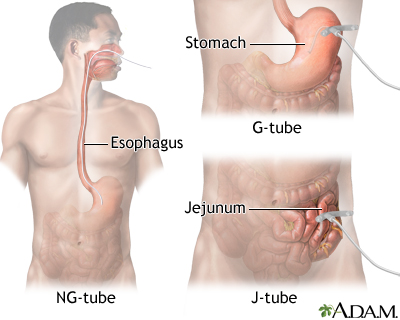
- Esophageal patholgy: GERD, Barrets, caustic esophagitis, functional
- hot drink/food,
- alcohol/smoking
classics (invasion sourrundigs - fistulas)
- dysphagia (solid first) + odynophagia
- tracheal invasion/compression: cough dyspnea, hemoptysis
- recurr. laryngeal n.: dysphonia
- B-symptoms
- Endoscopy + Biopsy
- Endoscopic US: T+N
- CT of esophagus (cervical, thorax, upper abdomen)
- Barium swallow → strictures, mass?
- Lab: classics (liver/renal/CBC)
- local → endoscopic
- Neoadjuvant RCT + Subtotal/total esophagectomy +LN (+pull up/ colonic interposition)
- Cervical esophagus (cant do surgery) → RCT
- Trustuzumab (if Her2+ adenoCa)
Palliative → RT, Stent
- HP
- age,
- lifestyle
- Smoking, alcohol,
- preserved food (salty+spice),
- decreased HCl (biermer anemia),
- prior gastric surgery (at suture),
- genetics (Lynch, familiar gastric cancer syndrome),
liver +lung
bone +brain
- classic: bleeding (hematemesis), pain + B-symptoms
- anemia
- compressive: gastric outlet obstruction, esophago-gastric junction obstruction
- invasive signs → rupture into peritoneal cavity
- LN **→ paraumbilical (sister mary Joseph n.), virchow N., axillary
- Met symotomatic (dyspnea, aszitis etc)
- endoscopy + biopsy
- T+N → EUS + abdominal US
- M → CT thorax,abdomen,pelvis (or Chest Xray instead of Ct throax - that a general rule!)
- Lab:
- Tumor marker: CEA, CA19-9 + classics (CBC,renal/liver)
- HER2+ ?
- Fecal occult blood test
- Cardiac** workup (EKG, Echo-EF?) → 5-FU can cause coronary spasm
→ Exploratory Laproscopy**
→ PET
- Limited: mucosa/submucosa → endoscopic resection
- Advanced ⇒ Neoadjuv. + adjuv. Chemo + Surgery:
- Radical gastrectomy + D2 lymphadenctomy (=d1 (Right side +liver ) + left side, splenic a.)
- Øoperable? → try to downstage with CRT
- HER2+ →Trastuzumab
- Palliative: RT OR subtotal gastrectomy
FH + Genetic → FAP, Lynch (HNPCC), BRCA1+2
Premalignant conditions → IBDs + Polyps
Lifestyle (smoking, alk, diabetes) + Diet
Age+black
Bacterioides fragilis
indications for genetic counseling:
- + FH for CRC
- <50y
Any colorectal cancer patient younger than 50 should consider genetic counseling to evaluate the need for genetic testing. In addition, any colorectal cancer patient with a family history of cancer should consider genetic counseling for similar reasons
DEPENDING ON LOCATION
pain | Soft stools /diarrhea | Constipation/Obstruction | Bleeding | Pencil stools | |
Asc. colon | ✅ | ✅ | occult | ||
Desc. colon | ✅ | ✅ | hematochezia | ✅ | |
Rectum | ✅ (tenesmus) | ✅ | ✅ | hematochezia | ✅ |
- asc. colon:
- soft stool + Ø obstruction
- pain
- anemia (occult bleeding)
- palpable mass
- desc. colon
- constipation + obstruction
- pain
- hematochezia + pencil stools
- DRE
- Colo + biopsy
- rigid proctoscopy for rectal tumors → distance anal verge
- T + N stage:
- MRI (pelvic)
- Endorectal US
- M-stage:
- CT thorax, abdomen M-stage(liver,lung)
(like gastric)
CEA (for follow up esp. if it was high before)
CA19-9
+classic lab (CBC/renal/liver)
Increased CEA (false positive)
Colon: surgery → adjuvant chemo
Rectum: neoadjuvant RT → surgery → +/- adjuvant chemo
Surgery → circumferential margins
If Mets → oligo vs. multi (if Oligo-still curable, multi - palliative)
- rectum
- Mesorectum
- Presacral Space
- LN → int. illiac + obturator
⇒ RT alone (short-course) or combined CT-RT (long course)
(RT fraction shemes: RT Short course (↑Gy ↓Fractions) or RT long course (↓Gy ↑Fractions))
⇒ followed OR preceded by Chemo
Classics
inflammation, strictures/stenosis, fistula
If you can’t perform colo (obstructing tumor) - do colo within 6m after surgery ⇒ THERE COULD BE SECONDARY MALIGNANCY IN THE INTESTINE
fused with “RT Lab”
- Smoking
- Former radiation (RT or radon-exposure)
- Asbestos
- Genetic + FH
- Pulmonary diseases
- other cancer
- NSCLC (ex. adenoCa + SCC)
- SCLC
- brain
- liver
- bones
- Lung
- Melanoma
- Renal
- Breast
- Dypnea
- cough + hemoptysis
- pleuritic pain (if periph. tumor)
- Recurr. infections**
- B-symptomatic
- obstruction: trachea, esophagus
- Paraneoplastic syndrome **
- Horner synd.
Always CT if any symptom!!
Cushings ← ACTH-release by SCLC
tumor induced hypercalcemia ← parathyroid hormone-related protein by SCC
bronchoscopy,
EBUS, EUS,
mediastinoscopy,
Transthoracic (US/CT guided)
- Biopsy - bronchoscopy, EBUS, EUS, mediastinoscopy, Transthoracic (US/CT guided)
- If NSCLC →and if adenoCA → look for mutations (I.e. EGFR) → there’s target tx!!
- CT (abdomen + chest if not done by XRAY)
- PET
- MRI (brain)
- Lab**
- Tumor markers:
- LDH
- NSE → SCLC
- CYFRA-21 → SCC
- CEA → AdenoCa
- classics (CBC/renal/liver)
SCLC (or AdenoCa)
NSCLC
- resectable? → surgery +/- adjuvant chemo OR RT
- unresectable? → try to downstage: RCT
- M1? ⇒ Chemo + targeted therapy (bevakizumab = avastin)
→ Oligometastatic? → ABLATION!
→ Brain: stereotactic RT or surgery
→ liver: Radiofrequency ablation
SCLC
limited? → RCT
extensive? → Chemo + targeted
classics: Lung, esophagus, heart + ribs
short:
- pneumonitis, esophagitis, heart
long:
- pericardial fibrosis
- lung fibrosis
- rib fracture + osteonecrosis****
- esophageal, tracheal strictures
- 2nd cancer
RT Lab
- 🚬
- 🍺
- HPV
- Neck mass
- Dysphagia + odynophagia
- ear pain - referred otalgia
- bleeding
- dysarthria (extension → tongue)
- trismus aka lockjaw (extension → pterygoid muscles)
- B-symptoms
T1N1
T:
≤2cm → T1
>2cm - 4cm → T2
≥4cm or extension to epiglottis→ T3
invasion of larynx or others → T4 (a+b)
N:
unilat + all ≤6cm → N1
contra/bilat. + all ≤6cm → N2
>6cm → N3
M:
absent → M0
present → M1
Tumors caused by HPV → p16 + (on immunohistochemistry)
⇒ different Tx!
- CT or MRI + contrast
- biopsy
- check p16
- consider PET for dist. M
ECOG PS
→ ask for:
weight loss? (+fatigue?)
physical acitivity?
→ walking
→ self-care
work capacity?
⇒ decides which Tx can be done

- RCT (combined RT + chemo)
- Surgery (if operable)
- Chemo (TPF, cisplatin)
→ consider brachythery in recurrent cancer
Depends on clinical target volume → high vs. intermidate vs. low risk
50 - 70 Gy
p16+ → lower doses
High-risk CTV (including GTV) = 70Gy Intermediate-risk CTV = 60 Gy Low-risk CTV = 50 Gy *in study: lower doses for p16+ tumours
- hairloss
- skin + mucous membrane (radiation dermatitis + mucositis)
- mouth → mucositis, xerostomia, dysgeusia
- edema (larynx)
- conjunctivitis
- 2nd c → mandibular sarcoma
dental care+ classics
- regular follow-up
- avoid RF
- explain possible symptoms of recurrance + late RT toxicities
- food (special food needed)
⇒ unbalanced/high Estrogen (ENDOMET) + genetic+FH!
ENDOMET:
- elderly
- nulliparity (never been pregnant)
- Diabetes*
- Obesity*
- menstrual abnormalities OR vaginal bleeding after menopause
- estrogen monotherapy*, late onset menopause
- hyperTension *
- genetic: lynch synd. II( HNPCC )
- FH: endometrial cancer
AdenoCa
- abnormal vaginal bleeding
- in menopause = probably endometrial Ca (until proven otherwise)
- vaginal discharge (leukorhea)
- compressive symptoms → parametrial invasion → ureteral obstruction
- Gyn-exam + DRE
- Imaging
- US (abdominal)
- Chest Xray / CT
- MRI / CT / PET → pelvis + abdomen
- rectoscopy + cystoscopy (advanced)
- Lab
- CA125
- CBC
- renal+liver
- Biopsy (curettage)
- pelvic
- para-aortic
TNM
FIGO
operable → TH+BSO +/- adjuvant RT or Chemo
non-operable/extrauterine → RT (+/- surgery after)
Limited to uterus
Operable
→ Surgery (TH+BSO)
- total hysterectomy
- +bilat. slpingo-oophorectomy
- +/- pelvic/para-aortic LN dissection
→ +/- adjuvant Radiotherapy → external + brachy
→ Chemotherapy
Non-operable
Radiotherapy (ext + brachy)
Extra-uterine
Radiotherapy +/- Surgery after
Brachytherapy, also called internal radiation therapy, places radioactive material directly inside or next to the tumor. It uses a higher total dose of radiation to treat a smaller area than external beam radiation therapy (EBRT) which directs high-energy x-ray beams at a tumor from outside the body.
temporary → sticks (iridium) - high intensitiy
permanent → seeds (iodine) - low intensity
+ femoral head fx
acute: inflammation of sourrunding structures:
- colitis
- cystitis
- vaginitis
late: stenosis + fistula
- vaginal + urethral stenosis
- rectovaginal + vasicovaginal fistula
- instestinal occlusion/perforation
- femoral head fracture
- regular follow up → 1stY: every 3m; Next years: every 6
- clinical exam
- xray
- US
- CT
- CA-125
- educate about recurrence symptoms
- educate about SE of Tx (RT)
- reduce RF (HT, obesity+DM, estrogen monotherapy)
- naso-or oropharyngel cancer → regional extension to LN
- Lymphoma
- Lipoma/Liposarcoma
Nose, nerves, trismus + general
DEPENDS ON EXTENSION
- Nose:
- bleeding
- obstruction
- Cranial nerve involvement
- Cranial nerve palsies
- facial pain & headache
- Eye: Vision Problems
- Ear
- hearing loss
- recurr. ear infection
- Trismus
- LN + DISTANT METS SIGNS
- EBV
- diet: salted/preserved food (nitrosamides)
- FH + genetic
- (Smoking + Alcohol )
MRI +CT → most common origin Rosenmüller fossa
PET
→ nerv + skull involvement most common!
ECOG PS
→ ask for:
weight loss? (+fatigue?)
physical acitivity?
→ walking
→ self-care
work capacity?
⇒ decides which Tx can be done

Concurrent Radiotherapy +/- adjuvant chemo
OR
Induction Chemo + adjuvant RCT
(never surgery for NPcancer!)
see above
gliomas + meningiomas = 80%
children → infratentorial (+spinal cord)
adults → supratentorial
Glioma → brain
Meningioma → spinal cord
- skull
- Falx
- Tentorium
CSF!!
(hema-exceptional; NEVER LYMPHATIC)
High-dose IONISING RADIATION
(non-ionising radiation might also be a RF but not clear yet (ex. 📲)
- Genetic - i.e. Lynch synd., Neurofibromatosis (NF1+2), MEN
- >65y
- ↑estrogen → meningioma
- MRI = gold standard
- CT
- Biopsy
- thick + irregular margins
- enhancing +
- central necrotic/hemorrhagic core
- sourrunded by edema
- infiltrative
neurological abnormalities
- seizures
- headache
- focal neuro deficiency symptoms (paresthesia, vision disturbance + unlit. dilated pupils)
- neuro-psychiatric
+/- B-symtoms
- Clinical: Karnofksy index > 60% + <60y = curative
- histo type: LGG vs. HGG (vs GBM)
- Extend of resection (complete vs. incomplete)
according to histology:
Astrocytoma, oligo-astrocytoma, oligo-dendroglioma
- Low grade (LGG) → 1+2
- High grade (HGG) - anaplastic → 3
- Glioblastoma multiforme (GBM) → Grade 4
another index for to estimate PS
→ ask for:
weight loss? (+fatigue?)
physical acitivity? → walking, self-care
work capacity?
⇒ decides which Tx can be done

- LGG → Resection (+ observation or RT or RCT)
- HGG → Resection + RT/RCT
- GBM → Resection + RCT (with TMZ) or only RT
contralateral extension → becomes in-operable ⇒ only RT + Chemo possible
- Anti-edema → Dexamethasone (+/- Manitol)
- Anti-epileptics → i.e. Carbamazepine, Gabapentin
Hair, skin, neuro,
Acute:
- Hair loss
- Fatigue
- nausea
- cutaneous burns
Late:
- neurological impariment
- neurocognitive decline
- vision loss
- 2nd cancer
- Radiation necrosis (less frequent)
30 x 2 Gy
>90% recurr within irradiated target volume
Consider oligometastatic stereotactic RT
yes → ulcerated + compression
- SCC → ulcerated + slow growing
- Basal cell Ca → slow growing
- Melanoma → assymetric dark spots or nodular
- SKIN IRRITATION:
- sun exposure
- chronic skin inflammation
- others: chemicals (arsenic) + burn scars
- Genetic (blonde+white skin, xeroderma pigmentosum)
- immunosuppresion
SCC more likely for deep invasion + LN/distant spread (aka highly lymphophil)
BCC → ØLN + Ødistant mets
Surgery if possible
if N+ → adjuvant RT
at least 4-6mm
Lymphatic spread → recurrance
LN drainage ex lower limb-› inguinal LN upper limb -› axila forehead-› preauricular/ parotid gland
yes, bc N+
- avoid RF + use sunprotection
- self-exam skin+LN
- more often follow up in regional diseases!
FH + Genetic → FAP, Lynch (HNPCC)
Lifestyle + Diet
Occupation
Age+black
indications for genetic counseling:
- + FH for CRC
- <50y
Any colorectal cancer patient younger than 50 should consider genetic counseling to evaluate the need for genetic testing. In addition, any colorectal cancer patient with a family history of cancer should consider genetic counseling for similar reasons
- Endoscopy + biopsy
- dRE
- MRI (pelvic)- T,N-Stage
- Or Endorectal US - T-stage
- CT thorax, abdomen M-stage(liver,lung)
CEA (for follow up esp. if it was high before)
Increased CEA (false positive)
<T3 + N0 → surgery only
T3 or N+ → neoadjuvant RT → surgery 6-8w later → +/- adjuvant chemo
Surgery → circumferential margins
If Mets → oligo vs. multi (if Oligo-still curable, multi - palliative)
- rectum
- Mesorectum
- Presacral Space
- LN → int. illiac + obturator
⇒ RT alone (short-course) or combined CT-RT (long course)
(RT fraction shemes: RT Short course (↑Gy ↓Fractions) or RT long course (↓Gy ↑Fractions))
⇒ followed OR preceded by Chemo
Classics
inflammation, strictures/stenosis, fistula
If you can’t perform colo (obstructing tumor) - do colo within 6m after surgery ⇒ THERE COULD BE SECONDARY MALIGNANCY IN THE INTESTINE
AdenoCA
Age, Black,
Western diet,
FH, genetic (BRCA1,2)
- urinary symptoms
- obstructive symptoms (weak stream, incomplete emptying)
- UTI (freq + urgency, dysuria)
- advanced → lumbar pain (bone mets/ para-aortic LN mets)
- DRE
- PSA
- Endorectal US
- Biopsy (US guided, fusion) → At least 6 core
- MRI (pelvic or whole body)
- CT (chest, abdomen)
- Bone Scinti (if clinic, PSA>20 or intermediate risk)
- PET
Bone Mets:
SPINAL COMPRESSION SUSPECTED → CT MRI → confirm bone Mets + compression
Emergency treatment!! → surgery/ RT (within 48h)
Grading of aggressiveness / differentiation
G1-G5
(Most common + second most common)
→ Risk + Tx assessment
Patients urinary symptoms before treatment → if very symptomatic → don’t start RT give Hormone first
Low: Gleason <7 PSA <10
Intermediate: Gleason=7; PSA 10-20
High Gleason >7 PSA >20
Take into consideration
- Gleason
- PSA
- TNM
- Life expectancy + comorbidites
- Surgery (robotic, lapa, classic)
- Radiotherapy (ext +/- brachy)
- Hormonal (adrogen deprivation - surgical or LHRH agonist, anti-androgens)
Metastatic + hormone resistance → chemo
- systemic
- hormone
- chemo
- target
- palliative RT
CT (+/- markers for prostate) or MRI before each fraction
→ compare with baseline target volume +/- corrections
High dose - iridium needle (temporary)
Low dose - palladium/ iodine seeds (permanent)
Classic (inflammation, strictures/stenosis, fistula)
ESP rectum bladder
- #1 SCC → exocervix
- AdenoCa → endocervix
HPV
- vaccination
- papsmear
- + hpv test
- dont smoke
- condome + limited sexual partners
- Vulva + Vagina
- Penis
- Anus
- Oropharynx
16 + 18
- ↑ sexual activity
- early onset
- multiple partners
- other viruses → herpes simplex, HIV
- smoking
- immundef. + Vit A+C def.
- multiparity
pap test
colposcopy → punch biopsy or Conization → described as cervical intra-epithelial neoplasia (CIN)
CIN I (mild)→ follow up
CIN II (mild-moderate) + III (severe) → conization or cryo or LEEP
- asymptomatic woman: ages 20-65 yo
- starting at 3yrs after first sexxxual intercourse
- woman >70 yo may stop screening of cytology was normal the last 10 yrs
VAGINA → BLADDER; URETHER, RECTUM; ILLIAC VESSELS
- abnormal vaginal bleeding
- vaginal discharge (leucorrhea)
- B-symptoms (weightloss, appetite, fatigue, anemia)
→ after sexual intercourse + intermenstrual, menorrhagia,
INVASIVE:
- urinary symptoms (dysuria, ↑freq., hematuria)
- Rectal invasion → constipation, rectorrhagia
- lumbar pain → Hydronephrosis (acute RF) or para-aortic mets
- unilat. leg edema (illiac vessel compression
- gynecological exam
- DRE
- abdomen/pelvis CT + contrast or MRI /PET
- CT/ Xray thorax
- advanced: cystoscopy / rectoscopy
- Lab: CBC, renal+liver markers, urine samples, CA125, CEA
FIGO
Stage 1: confined to cervix
1a microscopic tumor
1b1 ≤4cm
1b2 >4cm
Stage 2: beyond cervix
2a: Øparametrial invasion
2b: parametrial invasion
Stage 3a → lower 1/3 of vagina
Stage 3b → pelvic side wall OR hydronephrosis
Stage 4
4a: spread to rectum / bladder
4b: distant mets
para-aortic
Main treatment modalities: Surgery (Conization or TH+BSO) AND/OR RT/RCT
(⇒ in 2B ⇒ RCT (+/- surgery))
1A
- Total hysterectomary
- OR Conization (young)
- OR Brachytherapy
1B - IIA
- Surgery (Total hysterectomy + bilat. salpingo-oophorectomy + pelvic LN) + adjuvant RT
- OR RCT
2B-4A
- RCT(+/- followed by surgery)
4b
- palliative Chemo or RT
- targeted therapy (bevaciuzumab)
classics
acute: inflammation of sourrunding structures:
- colitis
- cystitis
- vaginitis
late: stenosis + fistula
- vaginal + urethral stenosis
- rectovaginal + vesicovaginal fistula
fused with “Onco Lab”
- Smoking
- Former radiation (RT or radon-exposure)
- Asbestos
- Genetic + FH
- Pulmonary diseases
- other cancer
- NSCLC (ex. adenoCa + SCC)
- SCLC
- brain
- liver
- bones
- Lung
- Melanoma
- Renal
- Breast
- Dypnea
- cough + hemoptysis
- pleuritic pain (if periph. tumor)
- Recurr. infections**
- B-symptomatic
- obstruction: trachea, esophagus
- Paraneoplastic syndrome **
- Horner synd.
Always CT if any symptom!!
Cushings ← ACTH-release by SCLC
tumor induced hypercalcemia ← parathyroid hormone-related protein by SCC
bronchoscopy,
EBUS, EUS,
mediastinoscopy,
Transthoracic (US/CT guided)
- Biopsy - bronchoscopy, EBUS, EUS, mediastinoscopy, Transthoracic (US/CT guided)
- If NSCLC →and if adenoCA → look for mutations (I.e. EGFR) → there’s target tx!!
- CT (abdomen + chest if not done by XRAY)
- PET
- MRI (brain)
- Lab**
- Tumor markers:
- LDH
- NSE → SCLC
- CYFRA-21 → SCC
- CEA → AdenoCa
- classics (CBC/renal/liver)
SCLC (or AdenoCa)
NSCLC
- resectable? → surgery +/- adjuvant chemo OR RT
- unresectable? → try to downstage: RCT
- M1? ⇒ Chemo + targeted therapy (bevakizumab = avastin)
→ Oligometastatic? → ABLATION!
→ Brain: stereotactic RT or surgery
→ liver: Radiofrequency ablation
SCLC
limited? → RCT
extensive? → Chemo + targeted
classics: Lung, esophagus, heart + ribs
short:
- pneumonitis, esophagitis, heart
long:
- pericardial fibrosis
- lung fibrosis
- rib fracture + osteonecrosis****
- esophageal, tracheal strictures
- 2nd cancer
- Regular follow up
- Avoid RF
- Education about:
- Recurring symptoms
- Tx SE
🎗️ Cancer Basics
Carcinogenesis, Trials, Epidemiology (Onco) & Precursors (RT) are fused in “Cancer Basics”
- Dysplasia: anarchic growth
- Neoplasia: Abnormal growth of cells
- Anaplastic: Lack of cellular differentiation
multiple subclones within 1 tumor sample 📷
→ different characteristics
↓
cancer → acidic
normal → alkaline
- substate-dependent
- contact-inhibition
- density-dependent inhibition 📷
breast + ovarian
(prostate, colorectal)

- most common
- ↑progression
- cant be inhibited by common drugs
- ↑mortality
- repare
- apoptosis
- survival of retarded cell (!)
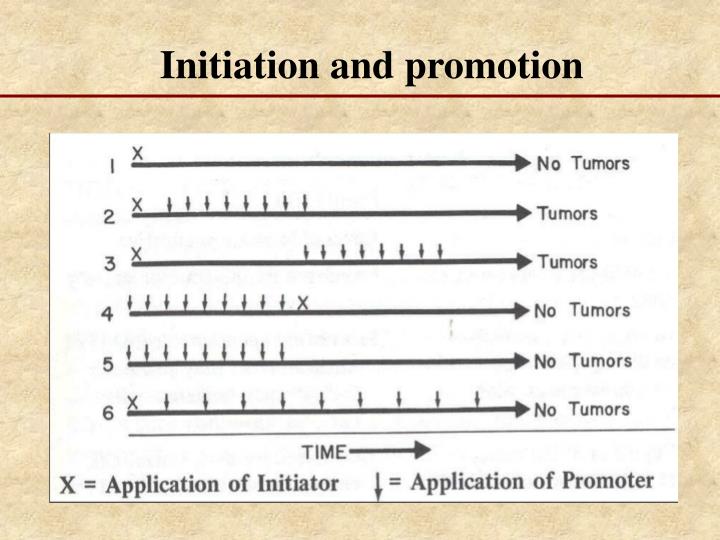
- carcinogenic agents (initiation agent) → irreversible DNA lesion
- Cocarcinogenic agent (incomplete carcinogen+promotor) → irreversible DNA lesion
- Radiation

- UV
- Viruses, Bacteria, Parasites


- Asbestosis
- Chemicals (complete vs. incomplete)
complete:

incomplete:

Øpreneoplastic lesion
Fusobacterium
mitogen agents (promoter) → stimulation of proliferation
⇒ first tumor cell
⇒ REVERSIBLE!
⇒ dose-dependent
⇒ØDNA-Damage
Initiators vs. Promoters:
Initiators | Promoters |
Carcinogenic agents that cause permanent DNA damage | Non-carcinogenic by themselves |
Induce mutations in DNA (by DNA damage) | Do not directly affect DNA |
Rapid and irreversible changes | Reversible changes |
Not sufficient for tumor formation by themselves | Induce tumors in initiated cells |
Play a role in the early stages of tumor development | Contribute to tumor formation in initiated cells |
Act as the first step in the multi-step process | Act as the second step in the multi-step process |
Survival of one clone → growth
- environment

- ANGIOGENIC SUPPORT

T
- (Proto-) Oncogenes ↑

- Supressor ↓
- Apoptosis ↓
- DNA repair ↓
- Gatekeepers (ex. p53)
- Caretakers (ex. BRCA)
- Landscapers
Subtypes:
i.e BRCA1, FAP

- Caretaker genes stabilize the genome. Mutations in caretaker genes lead to genomic instability.
- Gatekeeper genes prevent the growth of potential cancer cells and the accumulation of mutations that promote increased cellular proliferation.
- Landscaper genes, when mutated, create a stromal environment that supports unregulated cell proliferation.
oncogene → dominant → 1 chromosome is enough
suppressor → recessive → both need to be affected
T
Nuclear transcription factors aka genes that control the DNA transcription ⇒ ↑transcription → uncontrolled growth
CDK 📷
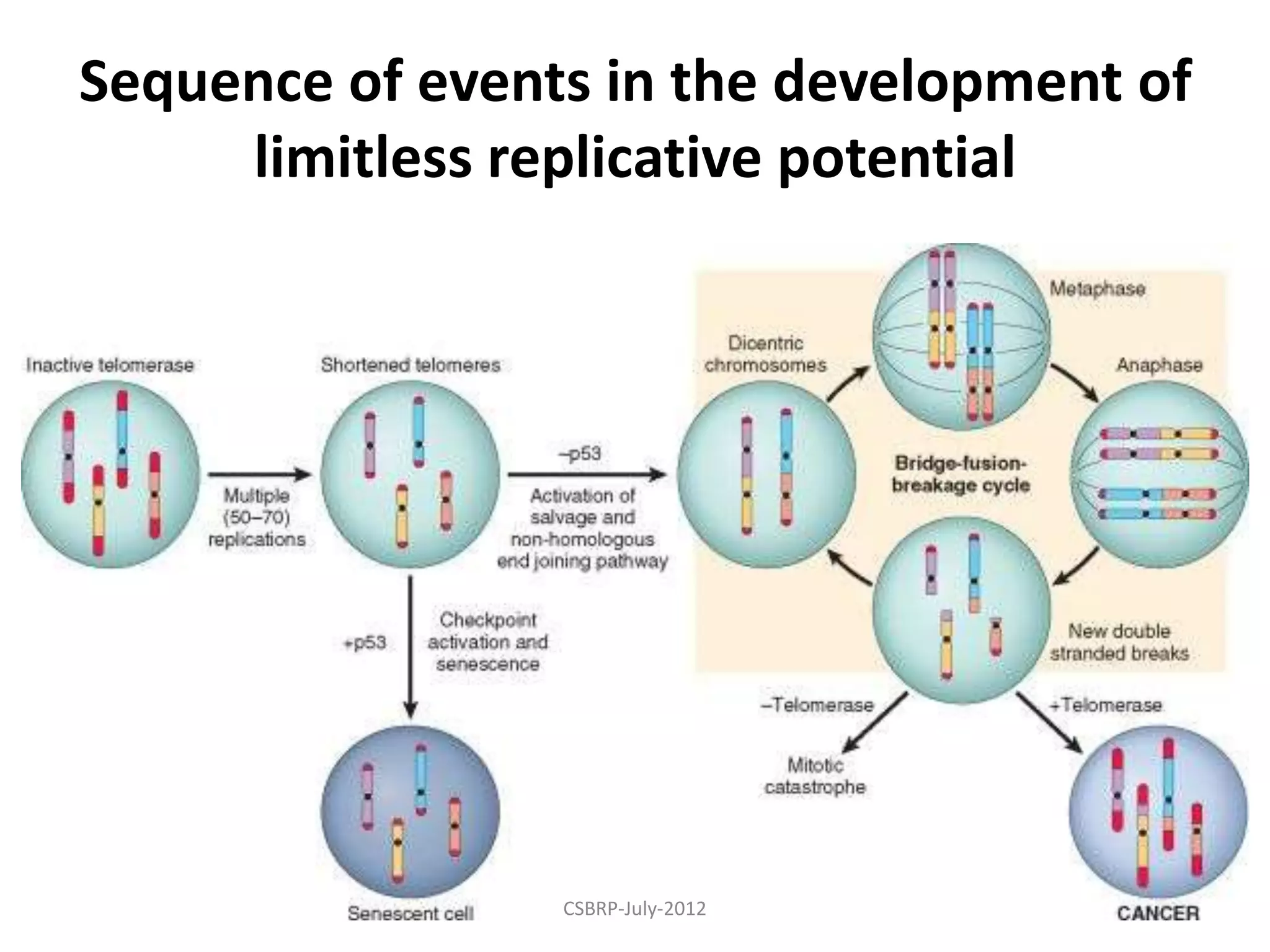
absent checkpoints (p53) → skips nonreplicative senescence → innapriate DNA repair (connects 2 ends of chromosomes w/o the telomers) → dicentric chromosomes
- Replication of somatic cells without telomerase leads to telomere shortening.
- Competent checkpoints induce cell cycle arrest and nonreplicative senescence.
- Absence of checkpoints activates DNA repair pathways, resulting in formation of dicentric chromosomes.
dicentric chromosomes → new brakes in chromosomes → genetic instability
⇒ Ø telomerase → mitotic catastrophe

→ + telomerase → cancer

microsatellite instability (MSI) → ex. Lynch syd

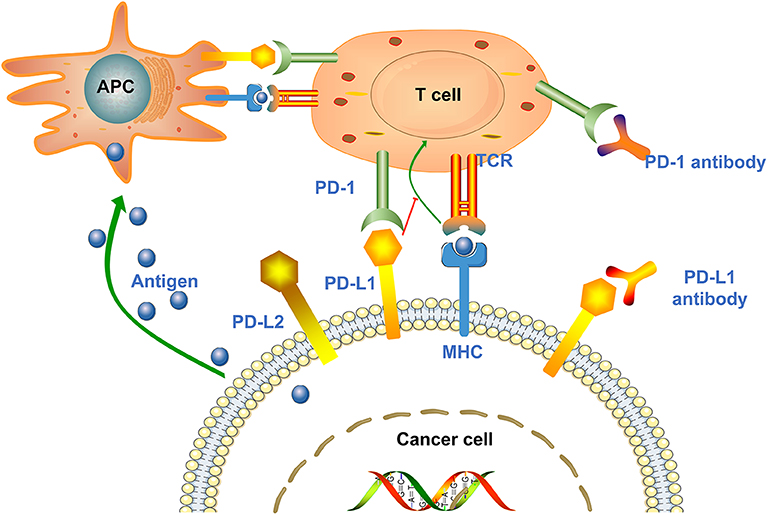
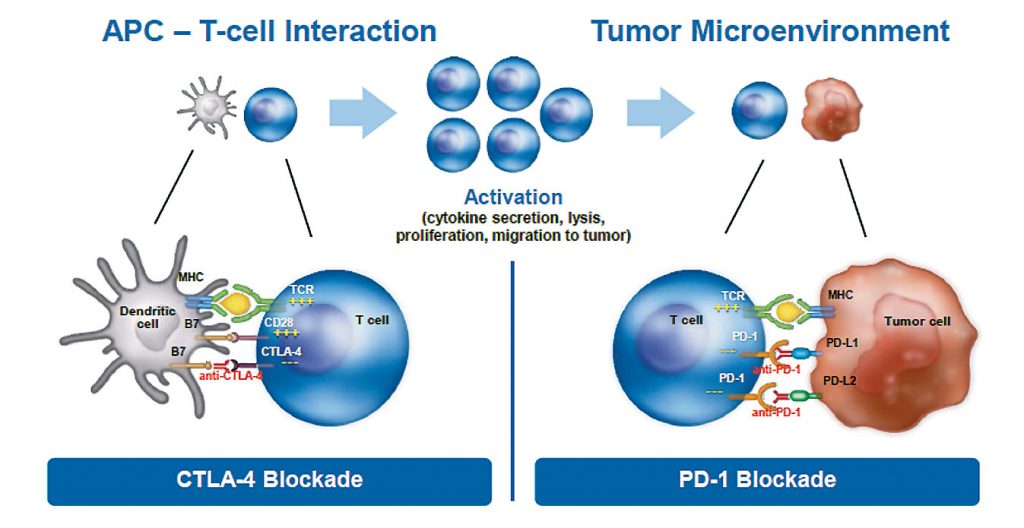
→ PDL1 over-expression by cancer cells prevent immune reaction by T-Cells (prevent interaction of T-cell receptor with MHC proteins of tumor cell via binding of PD-1 R on T-cell ⇒ thereby preventing cancer cell death
→ PD-1 blockade → T-cell activation (cant be blocked anymore)
example of PD-1 blocker:

→ PD-L1 blockade
- Melanoma
- NSCLC
- Nasopharyngeal
- Lynch (CRC,Endometrian, ovarian, skin)
- Glioblastoma
- Colon cancer
- HCC
- Urothelial
Growth factor
(autocrine secretion)
Shortening of telomeres → Cell death after max. 60-70x cycles
(telomerase → no cell death → cancer)
cyclophosphamide

(antidote against acrolein = MESNA)

need activation (secondary origin)
→ pro-carcinogen
→ ultimate carcinogen → directly acts
⇒ i.e. (Nitros-)Amide
Aflatoxin B

children + young adults
- physical:
- Radiation + UV radiation
- Mechanical (asbestos) or chemical (gastric acid in esophagus) microinjuries
- chemical:
- tobacco
- alchohol
- food + obesity
- aflatoxin
- salted fish
- red meat
- industrial products
- mineral oil
- wood dust
- etc.
- others:
- chemotherapy
- estrogen compounds
- analgesics
- amphetamines
- pollution
- biological:
- schistosoma → bladder
- HepB+C, HPV, EBV, Herpes, HIV




- Lung cancer
- Oral cavity cancer
- Oropharyngeal cancer
- Esophageal cancer
- Laryngeal cancer
- Urinary bladder cancer
- Where it goes through (mouth, pharynx, larynx, esophagus, colon, rectum)
- Where it gets metabolized (liver)
- lung
- breast
- prostate
↓ cancer-risk
(high intake→ ↑ cancer-risk)
no
- High glycemic-index diet associated with increased risk of ovarian, endometrial, breast, colorectal, pancreatic, and lung cancers
- Limit processed foods and refined sugars
↑↑fibers
fruits + vegetables
- Fiber-rich diets have shown an association with a protective effect in colon cancer.
- High intakes of vegetables were inversely associated with colon cancer risk.
- High fiber diets tend to be lower in meat, fat, and refined carbohydrates.
- Increased consumption of fruits and vegetables is associated with lower risk of cancers of the oral cavity, esophagus, stomach, colon, rectum, and bladder.
- Evidence for the association between fruit and vegetable consumption and hormone-related cancers such as breast and prostate cancer is less strong.
- Genetic
- Immunologic
- Endocrine
- Lynch 1+2 (NPCRC)

- FAP (PCRC)
- MEN 1, 2a, 2b 📷
- congenital immun-deficiencies
- ataxia teleangiectasis
- Wiskitt-Aldrich disease (Lymphoma)
- AIDS + Kaposi sarcoma
- intermittent imuno-supression (treatment, post-infection, etc)
↑ Estrogen → breast + endometrial cancer
↑ no. of ovulations

T
T
(exception: thyroid > F)
Prostate
Lung
GI (CRC)
breast
cervix
lymphoma + leukemia
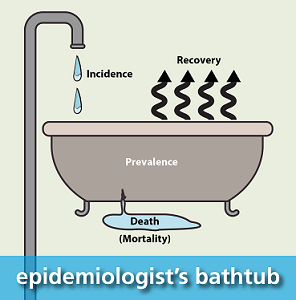
- Incidence
- Prevalence
- Mortality
- Potential life years lost
- incidence = new cases / 100k
- prevalence = number of cases / 100k = incidence x survival (medium duration)
→ ↑ w/ incidence + duration
→↓ w/ mortality
PLYL = 65y - years at death
⇒ measures impact of disease esp. in young
ANALYTICAL ECOLOGICAL
instant “photo” of the data at a certain moment in time
does NOT link etiology to diseases!!
Retrospective or prospective:
patient group free of diseases + exposure to risk factor
→ follow-up
(exposure→incidence)
How much higher is your risk for developing a type of cancer if you are exposed to a specific RF / the risk of a non-exposed person developing that type of cancer
RR = Fraction between the number of cancer cases in exposed individuals (A) and the number of cancer cases in non-exposed individuals (B)
Possibility of RR control by the measures taken by the community
80-90%
(aka 80-90% modifiable!)
theres a control group
LINKS:
exposure group → disease
control → disease
(in cohort there is only exposure→disease w/o control)

- efficacy + toxicity (SE) - Drug characteristics
- (FDA)approval - Drug approval
- Role of the drug in clinical practice - Drug in practice
- post-registration/marketing efficacy + toxicity - Drug post-study- evaluation
Determine Toxicity → MTD (maximum tolerated dose)
⇒ define optimal dose+ administration-schedule → 80% MTD for phase II
- rapid escalation of low doses
- slower escalation of higher doses
⇒ dose is escalated until a maximum tolerated dose (MTD)

objective response rate = partial or complete response (RECIST)

aka how good does the drug work?
New treatment vs. Gold-standard on survival:

→ better (superiority)
OR
→ not-better (equivalence; non-inferiority)
Randomized (+/- double blinded) → balanced groups
risk stratification

post-registration (post-marketing) studies
⇒ detect rare but serious side effects

🧩 Dg-Workup & Tx-Evaluation
⇒ direct=mass vs. indirect=other cancer signs
- direct signs → see/feel T, N (or M)
- indirect signs → see/feel effect of cancer
- bleeding,
- discharge,
- compression,
- neurologic signs
- B-symptoms,
- paraneoplastic synd.
- detect tumor (feel/see)
- Suggestive special signs? → aditional exam needed
→ if neg. → further dg-workup (imaging, lab)
- RF? → FH, Lifestyle, Diet, Environment/profession, etc.
- Main symptoms?
- Pre-neoplastic conditions/lesions? (polyps, leucoplasia, CIN, Barrets)
- Lab
- Imaging
- MRI
- CT
- US
- PET
- scinti
⇒ tumor resence? size? spread (local, regional, distant)?
- Endoscopy
- FNA → cytology
- Biopsy → histo + special tumor characteristics
STANDARDIZATION FOR:
- Tx-decision + evaluation/response
- Prognosis
- size
- invasiveness (adj. structures)
- number of involved structures
superficial → clinical exam
partially accessible to palpation → imaging and/or intrstrumental
deep → imaging!
- number (single vs. multiple)
- size
- location (regional vs. extra-regional)
- mobility (fixed or non-adherent)
- breast+ENT → Palpation
- deep → Imaging
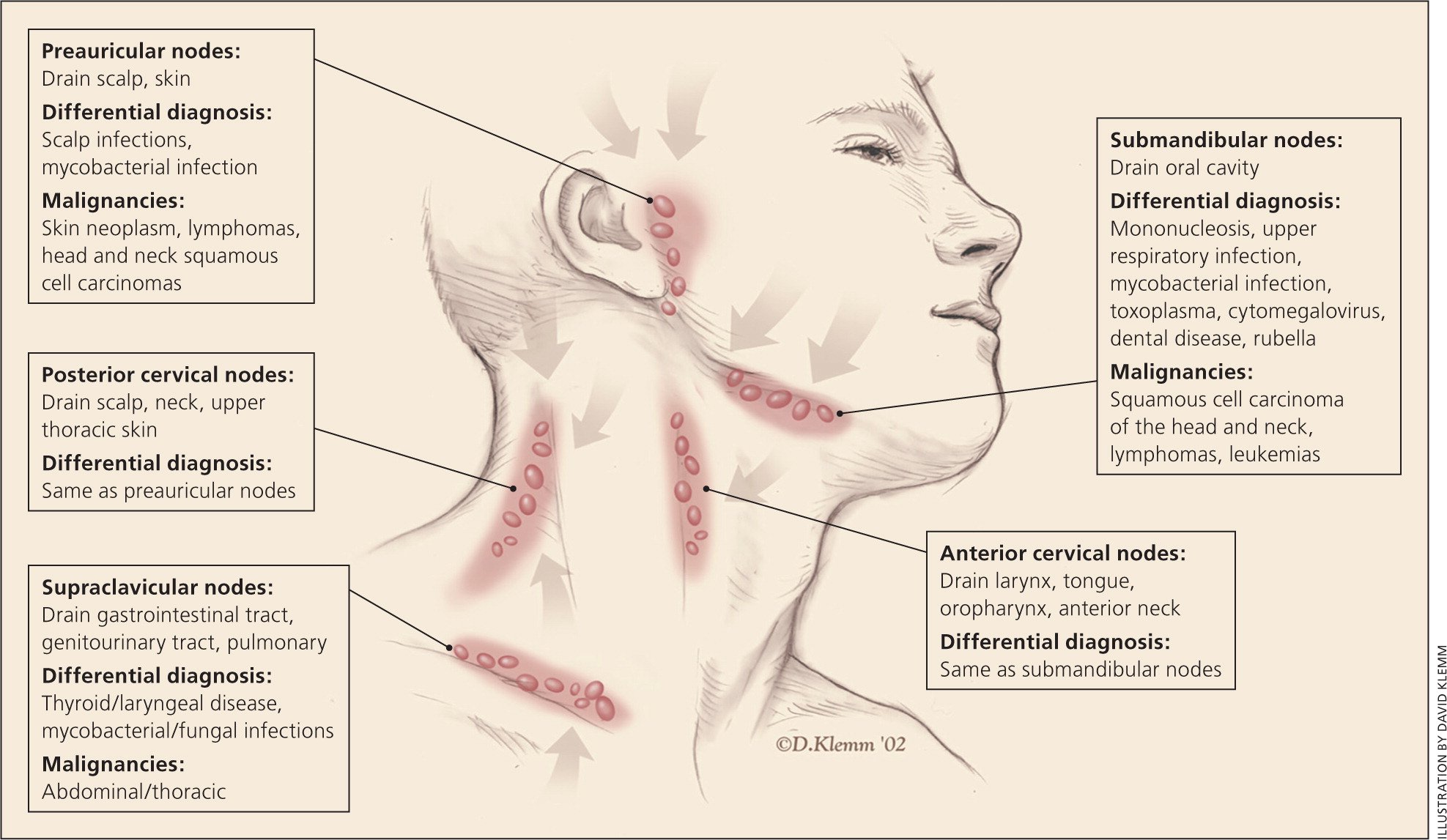
>[1]cm in [short] axis.
Abdomen + Thorax
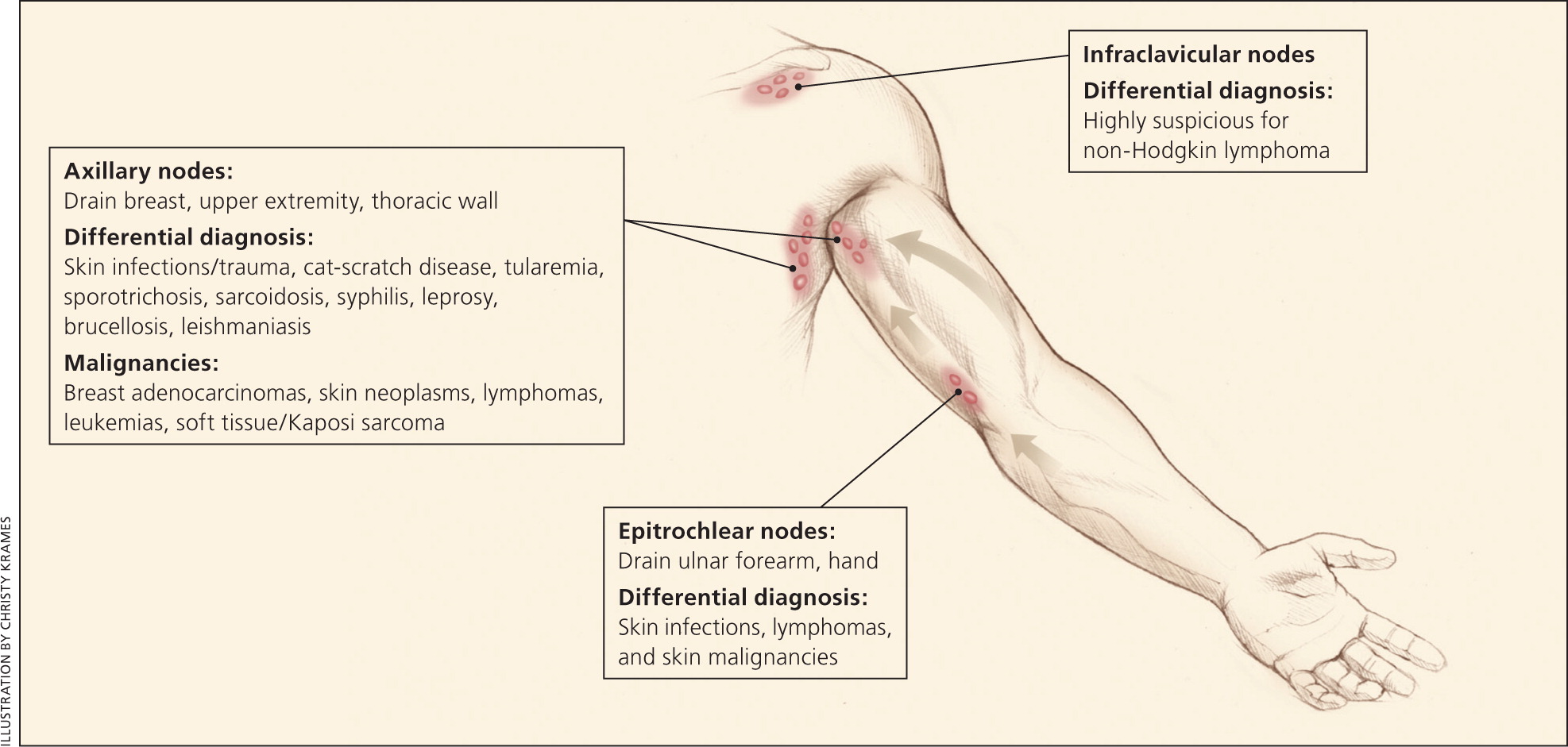
axillary 📷
- male, white, >40y
- Generalized lymphadenopathy (≥2 regions)
- Lymphadenopathy ≥4-6w* (Øreturn to baselike after 12w)
- B-Symptoms
- supraclavicular location
- Lungs
- Liver
- Bone
- Brain
- distant LN (extra-regional LN)
Notice that CT catches almost everything → order scinti if bone involvement suspected
MRI for brain
CT | MRI | US | Xray | Scinti/PET | |
Lung | ✅ | ✅ | |||
Liver | ✅ | ✅ | ✅ | ||
Bone | ✅ | ✅ | ✅ | ||
Brain | ✅ | ✅#1 | |||
distant LN | ✅ | ✅ | ✅ |
F → does not modify
pathological TNM after chemo/RT
TNM after recurrance
less advanced
clinical stages (0-IV)
0 = in situ
1 = small tumor (Ø N,M + Ø BM invasion)
2 = local/regional extension minimum (BM invasion)
3 = local/regional extension important (LN +)
4 = extra-regional (M)
- Brain tumor
- Endometrial + Cervix
- ST sarcomas
CLINICAL STAGING:
early stage → 0-IIb
locally advanced → IIIa-IIIc
metastatic → IV
TNM:
early stage → T≤2 N≤1 (OR T3N0)
locally advanced → T1/2 N2+; T3N+, T4N0, or N3
metastatic → M1
- History → how fast did the symptoms progress?
- Inflammatory signs (edema, congestion)
- Imaging → RECIST: measure size + progression of size
- Lab → monitor tumor markers
ECOG performance index scale
→ ask for:
weight loss? (+fatigue?)
physical acitivity? → walking, self-care
work capacity?
⇒ decides which Tx can be done

Local:
- Surgery
- RT
Systemic:
- Chemo
- Hormone
- Immuno + Targeted Tx
- Other (cryo, HIFU, RFA)
RO= ideal R1= microscopic residual disease R2= MACROscopic residual disease
- acute complications / toxicity
- tumor regression (RECIST)
- natural tumor history
- risk of recurrence
- Immediate post-tx → first control after 2month
- Maximum risk → 2m - 5y
- relative security → >5y
Year 1: every 3m (4x/y)
Year 2-3: every 3-6m (2-4x/y)
Year 4-5: every 6m-1y (1-2/y)
⇒ in lab:
year 1-2 = every 3m
year 3-5 = every 6m
- aggressiveness of tumor
- Tx-fails


☢️ Radiotherapy
survival
The abscopal effect is a hypothesis in the treatment of metastatic cancer whereby shrinkage of untreated tumors occurs concurrently with shrinkage of tumors within the scope of the localized treatment.
🧱 Treatment
SYMPATHETIC EFFECTS:
- ↑metabolism → muscle wasting
- Heart: ↑HR
- Lungs: Tachypnea + superficial breathing
- Vascular: ↑thrombo-embolic risk
- Kidney: water+Na retention
- GI: ↓motility
- Immune system ↓
- Anxiety + Depression
- Sleep deprivation
Definition: "Increasing pain experienced by patients with well-controlled chronic pain under medication."
- Duration of Breakthrough Cancer Pain (BTCP): 30 minutes (range: 1-240 minutes)
- Intensity: Maximal for 3-5 minutes
- Moderate to severe pain
- Multiple episodes of BTCP per day
- somatic
- Most frequent
- Intense
- Dull and aching
- Influenced by movements and touch
- Localized
- visceral
- Visceral pain characterized by deep squeeze, pressure, or aching
- Movement does not influence the pain
- Profound pain sensation
- neuropathic
- Nerve or central nervous system (SNC) lesion
- Repetitive discharge
- Electrical discharge
- Hyperesthesia or hypoesthesia at the skin level
- referred/reported
- Pain reported by patient
- Specific nerve innervation
- Superficial location
- Similar to neuropathic pain
Bone, muscles, and ligaments
lesion of nerves (CNS/PNS)
→ compression, transection, infiltration, ischemia
- burning,
- tingling,
- shooting,
- stabbing,
- electrical,
- pins and needles
- oxaliplatin
- paclitaxel
- bortezomib

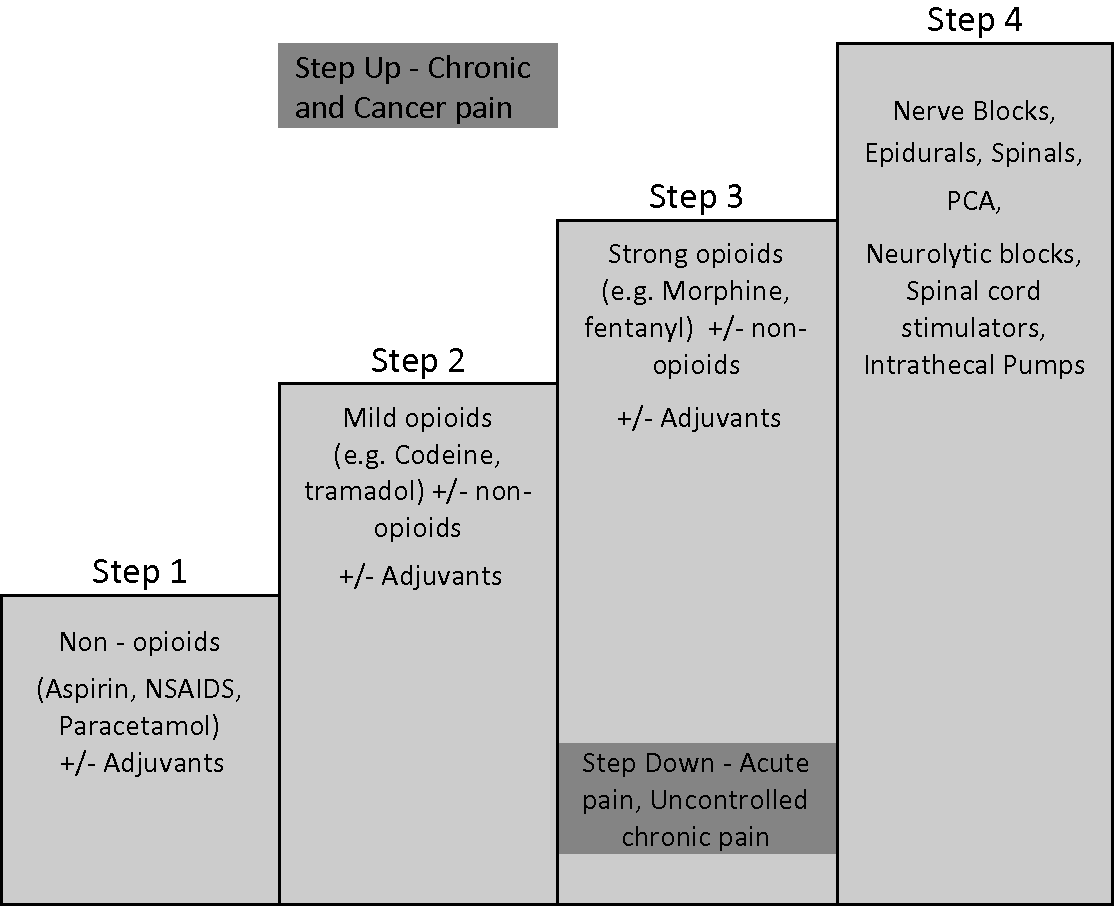
- NSAID +/- adjuvant*
- Opioid (weak) +/- adjuvant
- Opioid (strong) +/- adjuvant
*adjuvant (non-analgesics) = antidepressants, anti-epileptics

rapidly
cutaneous infection
oral + i.v. cant be used → but still constant need for analgesics
- Respiratory depression
- GI
- Constipation
- Nausea + Vomiting
- CNS
- Sedation
- Seizure
- Urinary retention

+many others
prokinetics (+enema)
(prophylactic)
anti-emetics
(vomiting+nausea usually occurs at the beginning of Tx with opioids)
stimulants (coffee, CNS stimulant drugs)
(sedation usually occurs at the beginning of Tx with opioids)
change opiods
bladder catheter
Reduce dose (try not to stop opioid tx)
→Naloxon if needed
benzos
- respiratory insuff.
- asthma
- obesity + sleep apnea
- paralytic ileus
- allergy
- Amitriptylin (TCA)
- Pregabalin + Gabapentin (Anti-convulsant)
- (SNRIs)

pre-existing cardiac disease

neuropsychiatric SE occur

- Classics (Opioids + NSAIDS)
- Biphosphonates
- Steroids
- Calcitonin
- compression
- pathological fracture
- Osteoneocrosis of the Jaw
- ↓kidney function
primary tumor or mets ⇒
spinal cord
↑↑


one at a time
“ie: q2-5 days, until good effect or adverse effects or max dose reached”

chemo-sensitivity


NSCLC
osteosarcoma
UCNT

(gastric)
mets: high risk OR micromets eradication



neoadjuvant + adjuvant

gastric
( i know it doesnt make sense)






T








(in orange)


*Performance status: 📷


aquired

every 4-6 wks


T (T + N)
→ but M (mets) can be also treated with RT
30%
(noice)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
area of irradiation = GTV + CTV + PTV 📷
{kind=link}

→ IONISATION → DNA + cell damage → cellular dysfunction + apoptosis
cellular dysfunction:

direct parencymal lesion → (inflammation )atrophy
indirect vascular lesion → fibrosis → atrophy
normal:
quicker+better repair
faster repopulation
Fractionation RT → 1fr (=1,8-2Gy)/day for 5days/w → repair
Protracting RT for 5-8w → repopulation
(⇒50-80Gy in total)
- morpholgy of the tumor (macro)
- histology (ex. seminoma, lymphoma)
- volume (↑Gy in macroscopic tumor)
- replication organs (ovaries, testies)
- sensory organs (eyes, ear, spinal cord)
- the big 4 (🫀, 🫁, kidney, liver)
ACUTE → INFLAMMATION
CHRONIC → FIBROSIS, FISTULA + 2ND CANCER
acute:
- skin + mucosa → burn, necrosis, stomatitis
- GI → radiation enteritis, radiation proctitis
- Lungs → radiation pneumonitis
- Hema → pancytopenia (bone marrow dmg)
- Genitourinary → ↓Fertility
chronic:
- secondary cancer
- fibrosis (obstructions)
early stages!! (I-II)
- Seminoma
- Skin cancer (Ømelanoma)
- Lymphomas (NHL, Hodgkin)
- Cervix
- ENT
After the big curative beam-blast of the radiotherapy machine Mrs Hodkins has semen on her skin, cervix, and pharynx (where else would it be?)

- Adjuvant
- Neoadjuvant
- palliative
- brachytherapy
- Endocavitary (lung, pharynx, uterus)*
- Interstitial: Breast, prostate+rectum
- Contact: skin *
- local complications → compression + bleeding**
- Multiple Mets
less than extensive M1 → ≤4mets in ≤3 organs
⇒ stereotatic high dose ablative RT → curative intent
Stereotactic radiotherapy (ST) gives radiotherapy from many different angles around the body. The beams meet at the tumour. This means the tumour receives a high dose of radiation and the tissues around it receive a much lower dose
- Cell-signaling molecules „Cogk 🍆“
- growth factors(GF)
- oncogenes
- cell cycles proteins
- kinases
- Apoptosis molecules
- Bcl-2
- Bax
- p53
- Transcription molecules „Histo-DNO Meth 🦖“
- DNA-methyltransferase
- Histone deacetilation
- Angiogenesis + Mets molecules
- Angiogenic factors + receptors (VEGF(R))
- Metalloproteases

small molecules (”-ib”)
→ Kinase inhibitors (ex. TKI)
- some kind of GF block:
- anti-HER1 (anti-EGFR)
- anti HER2
- VEGF
- VEGFR
- Anti-CD20 (rituximab)


- BreastC
- GastricC
→ trastuzumab
NHL
( can be used in lymphoma + Leukemia)
VEGF Trap blocks a protein called VEGF, which may prevent the growth of new blood vessels that tumors need to grow.
It is also called a “Receptor-like”.
ACTIVATION OF T-CELLS (+Ag-presenting cells) → KILLING OF THE TUMOR
{kind=link}
{kind=link}
Sipuleucel-T,

CAR-T

T-VEC talimogene laherparepvec (melanoma)
Interferon alpha
IL2 (activate Tcells)
- skin manifestations (EGFR+VEGFR)
- HT (VEGF+VEGFR)
- HT
- proteinuria
- ↑bleeding risk
(2+3 could be all associat. with 1 for memorization)
allergic reaction
AUTOIMMUNE REACTION ⇒ inflammation of various organ + endocrinopathies
(endocrinopathies (Ex. hypo/hyperthyroidism), pneumonitis, colitis, hepatitis, nephritis, skin reactions)
IMMUNOSUPPRESSIVA
- steroids
- DMARS → infliximab, mycofenolate
BIOMARKERS → IS THE BIOMARKER AKA THE TARGET POSITIVE?
(Ex: Anti-PDL1 only works in PDL1 positive cancer)
⇒ NOT ALL CANCER OF ONE TYPE CAN BE TARGETED WITH THE TREATMENT WHEN TARGET DOESNT EXIST
surgical (ablative)
breast c → oophorectomy

prostate c → orchidectomy

Name examples for each type of tx (cancer type + drugs):
Progestin | Anti-Estrogens | Androgens | Anti-Adrogens | Estrogens | |
Breast | ✅ | ✅ | ✅ | ||
Prostate | ✅ | ✅ | ✅ | ||
Endometrial | ✅ |
LH-RH Agonist / Antagonist | Aromatase inhibitor | |
Breast | ✅ | ✅ |
Prostate | ✅ |
Aromatase is the enzyme that catalyzes a key aromatization step in the synthesis of estrogen. → Adrenal inhibition (in postmenopausal woman)

Tyroid cc → L-Thyrox → inhibits TSH → ↓tumor growth stimulation
- Steroids
- Metablic therapy

- impaired Tx → ↓Tx response, ↑SE + ↓healing + ↑complications
Side effects: chemotherapy, surgical wound healing, fistulas, treatment-resistant diarrhea, heart rate, BP, delays in administration, unplanned dose reductions, treatment abandonment.
- ↓General status + ↓survival
- Decreases performance index
- Decreases muscle strength
- Amplifies asthenia
- Weakens immunity - repeated and / or treatment-resistant infections
- Decreases quality of life
- Increases mortality
DEPRESSIVE:
- heart + lung
- muscles
- GI
- immunity
- Healing
- cognitive
- theromoregulation
- Tumors
- ENT + GI
- CNS (Brain mets) → induce nausea/vomiting
- Host reactivity
- Treatment (Surgery, RT, Chemo)
- Radiation enteritis
- Radiation colitis
- Xerostomia
- Radiation mucositis
- General causes:
- Stenosis
- Digestive enzyme disorders (pancreatitis, biliary disorders)
- ↑Cytokines (TNFalpha)
10%
RT → inflammation of the GI-mucosa + post-radiation recovery need + ↑catabolism
inflammation of GI mucosa:
CT → GI-tox + ↑catabolism
Surgery → stoma or resected parts

classic healthy diet
- Maintain a healthy body weight through balanced foods and beverages
- Moderate consumption of meat and red meat
- Include vegetables and fruits daily in the diet
- Prioritize whole grains over refined grains
- after gastric resection (total or subtotal)
- macrocytic anemia
- with certain cytostatica
T
Classic anamnesis + eating habits / weight loss
- PMH: surgeries? CV-RF? diseases?
- GI disorders?
- History of present illness
- Do you eat less? Nutritional intake <50% since >7days
- What have you been eating?
- How much weight loss? (>10%/6m = neg. prognostic factor)
- Dehydration → skin tugor
- muscle loss → Triceps/biceps thickness
Lab:
- ALBUMIN!! (long-term status) + prealbumin (short-term status)
- Transferrin → ↓ in severe malnutrition
- Liver enzymes
- Testosterone
Parameter | Details |
Albumin | • Easy and inexpensive to measure
• Covered by most reimbursement programs
• Extremely long half-life (~20 days); insensitive to short-term changes
• Insensitive to trauma- or stress-induced malnutrition (hypermetabolic state)
• Affected by over-hydration and dehydration; Often given as part of therapy
• Affected by non-nutritional factors (including liver and kidney disease) |
Prealbumin (Transthyretin) | • Short half-life (~2 days)
•Excellent sensitivity to nutritional status
• Very useful for classification/triage
• High proportion of essential amino acids
• Strongly depressed in patients with end-stage liver disease
• Depressed by infection/inflammation |
20-35 kcal/kgc
“das maul (35) snackt ne nase (20)”
EN alone or EN + PN = better than PN alone
maintenance → water every 4 h + with each meal
clogged → hot water
{kind=link}
- GI-disorders
- short bowel syndrome
- obstruction
- fistulas
- post-radiation recovery
- Enteral cant be performed
7-10days → if >10d OR not well-nourished ⇒ total pernteral nutrition
- risk for infection + thrombosis
- dysbalance betw. macro+micro nutrients
- liver + bone dmg prophylaxis needed
- ACTIVE cancer = hypercoagulability

- Chemo

- Cachectic patients → Immobilization
difficult !
→ lab markers
- Thrombos
- D-Dimer
- tissue facor *
- soluble P-selectin* (cell adhesion molecule)
- Factor VIII(8)*
→ gene mutations: factor VIII (8)+ V (5)
{kind=link}
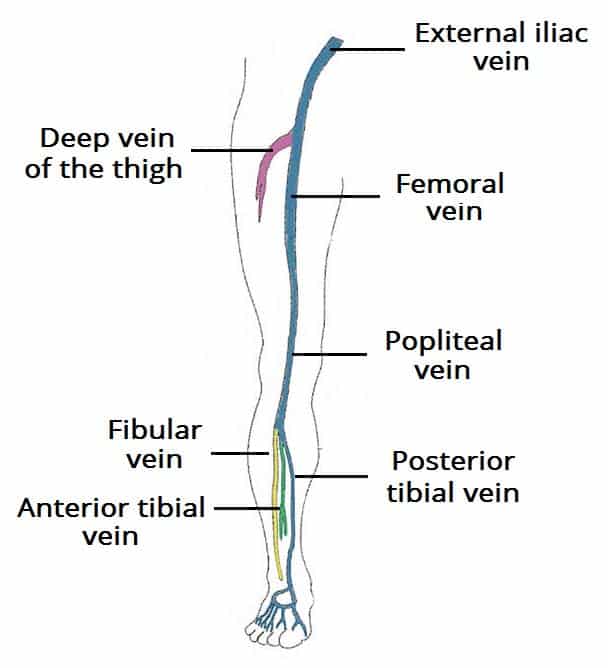
- calf v. (tibial (ant+post) + fibular)
- popliteal v.
- femoral
- illiac vein
US
compression + doppler
#1 = LMWH OR coumarin(Anti-VitK)

Ø iv Unfract. Heparin
LMWH → Factor Xa ( + aPPT)
Anti-VitK → INR
2-3
- venous compression (stockings)
- mobilisation
- Anticoagulation (LMWH)
- if thrombocytosis → ASS 300
- dyspnea
- cough
- pleural pain
CT angiography
severe cases → Thrombolysis or Resection

- head + neck
- Arms
- Sup. Thorax
{kind=link}
- SVC Compression by tumor
- lung cancer
- NHL + Hodkin
- extragonadel germcell tumors
- non-oncologic causes (thrombus, cardiac surgery, idiopathic,..)
- Xray - mediastinal mass
- CT / MRI = DGx 📷
BIOPSY
(through every way imaginable → depending on location)
- pleural aspiration
- bronchioscopy or EBUS
- trans-throacic (Ct-guided)
- Mediastinoscopy
- Thoracotomy
only SCLC palliative!
⇒ NSCLC → RT; Rest → Chemo
RT → NSCLC (12 Gy / 3 fractions)

Chemo → NHL/HL, Germ, palliative SCLC
- curative → NSCLC, NHL/HL, germ
- palliative → SCLC
- RT+chemo resistant → severe compression
- Areas treated with RT
- Prostate + Breast (DDx osteosclerotic mets)
- Lung
- Lymphoma + Myeloma
- Motor deficit → ex. walking difficulties
- pain
MRI → edema

Surgery + adjuv. RT, Dexamethasone
brain mets (mainly from lung cancer)
- general→ elevated head positioning
- anti-edema drugs→ Mannitol and Dexamethasone
Mannitol:

Dexamethasone:

- Tx mets → surgical resection, emergency ventriculostomy(if obstruct. hydrocephalus), whole brain radiation/stereotactic
- Hypercalcemia

- Hyperuricemia
- Tumor Lysis synd.
- Hypokalemia
- Hypoglycemia
- Adrenal failure → subacute Addison
- Tumor → paracrine secretion of PGE, TGF, IL6, TNF → bone resorption
- Treatment (ex. steroids)
Mild: 10.5-12 (mg%)
Mod: 12-15
Severe: >15
Mild → Hydration followed by diuretics (flush it out)
Moderate → hydration+diuretics + Zoledronic acid (Biphosp) i.v.

Severe
→ Øneurologic sym = moderate Tx
→ +neurologic sym = calcitonine OR dialysis
calcitonine:

Calcium is decreased due to increased Phosphorus (unbound phosphorus binds unbound Calcium→ relative Hypocalcemia)
A potentially life-threatening oncologic emergency: Rapid destruction of tumor cells → massive release of intracellular components
- Tumor cell lysis leads to the release of intracellular components into the bloodstream.
- Nucleic acids are converted to uric acid, causing hyperuricemia and the risk of acute kidney injury.
- Calcium is bound by phosphate, resulting in hypocalcemia and neuronal excitability, which increases the risk of seizures.
- Hyperphosphatemia leads to the formation of calcium phosphate crystals that obstruct renal tubules, causing acute kidney injury.
- Changes in resting membrane potential due to hyperkalemia increase the risk of cardiac arrhythmias.
⇒ Renal failure + Cardic arrhythmias
Metabolic disturbances:
↑Phosphorus, Uric acid + K AND ↓Ca (secondary to phosphorus binding)
- Febrile neutropenia→ GM-CSF, broad-spectrum ABs (let them grow +prevent infec)
- Febrile neutropenia definition:
- Fever: temperature ≥ 38.3°C (oral cavity) or ≥ 38.0°C sustained for at least 1 hour
- Neutropenia: absolute neutrophil count (ANC) < 500/μl or < 1000/μl with a predicted decline to < 500/μl within 48 hours
ABs:

- Anemia→ RBC transfusion
- Thrombocytopenia→ Platelet transfusion, Dexamethasone, Hemostatics
Dexa:

Hemostatics:

- UTI
- Cystitis (Aseptic) → i.e. after RT or chemo
- Neutropenia
- Male + old (BPH)
- Urologic procedures
- due to RT→ respect the limiting doses at bladder
- cytotoxic drugs→ chelating agents (MESNA)
- continuous saline lavage
- dimethyl-sulfoxid (aka DMSO)

- lidocaine/capasaicine→ against pain

Mama laudaaaa 🔊
{kind=link}