




ENT
👃🏼 Nose
- Obstruction / Congestion
- septal defects + malformation
- tumors (malignant + benign)
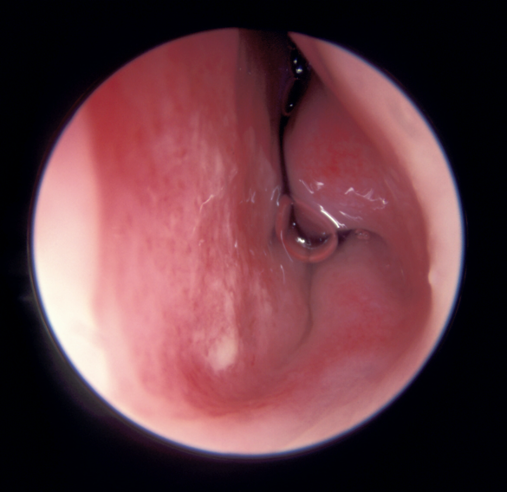
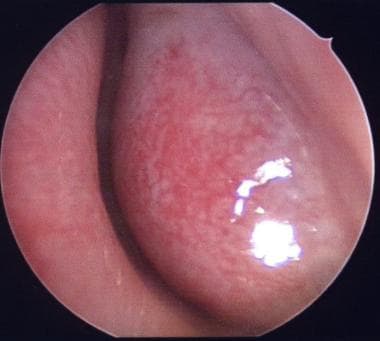
- turbinate hypertrophy
- polyp
- choanal atresia
- chemic injury
- Rhinosinusitis
- Discharge
- headache
- smell abnormalities
MECHANICAL:
FUNCTIONAL









⇒ Appearance of membranes + Work-up + Tx are same as pharyngeal (Antitox + ABs)
- Syphilis
- Tuberculosis
- Rhinoscleroma
- Leprosy


necrotizing granuloma
localized → URT
disseminated → pulmonary + sytemic symptoms
cANCA
localized → TMP-SMX

disseminated → TMP-SMX + CYC + Predni
Which of the following statements is false?
a) Sarcoidosis is a systemic disorder made up of epithelioid granulomas. b) ESR in Wegener's granulomatosis is low. c) Nasal endoscopy is mandatory in allergic rhinitis diagnosis. d) A medical treatment for allergic rhinitis is 25-50mg of chlorpheniramine. e) Anterior choanal polyps arise from the posterior lateral wall.
B → ESR = ↑
non-caseating “epitheloid” 📷
check granuloma directly, look for the lung + URT structures
⇒ biopsy + CT, ENT exam
Hydroxychlorochin, MTX, Steroids
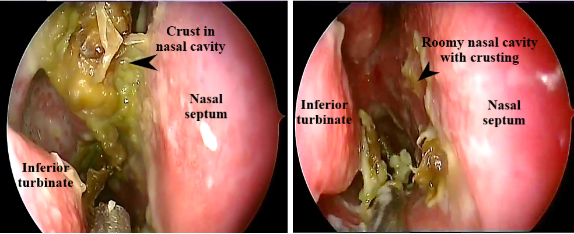
Local: saline irrigation, crust removal, intranasal steroids

Q. Which of the following drugs are prescribed in allergic rhinitis? A. Topical steroids B. Oral antihistamines C. Topical anticholinergic agents D. NSAIDs E. Antileukotrienes

- idiopathic
- drug-induced
- hormonal
- non-allergic occupational
- NARES (non allergic occupational rhinitis)
- Similar symptoms to allergic rhinitis
- >20% eos in nasal smear
- BUT: ØIgE Ab + neg. skin test
topical vasoconstrictures
strong vasoconstriction → rebound vasodilation → over time loss of vascular tone
⇒ hypertrophy of nasal mucosa
⇒ hyper-reactivity
Estrogen → vascular enlargement → obstruction / hypersecretion
Q. The term NARES refers to a nasal condition characterized by:
A. Symptoms similar to allergic rhinitis B. Positive c-ANCA test C. The presence of high levels of serum late antibodies (IgE) D. The presence of more than 20% eosinophils in the nasal smears E. Frequent association with asthma and aspirin intolerance
A + D
- The most aggressive form of nasal polyposis
- believed to be caused by an anomaly in the arachidonic acid cascade, resulting in excessive production of leukotrienes.
CF





Q. The main bacteria involved in the etiology of acute rhinosinusitis are:
A. Haemophilus influenzae B. Moraxella catarrhalis C. Group A beta-hemolytic streptococci D. Staphylococcus aureus E. Streptococcus pneumoniae
ABDE
Q. Which of the following symptoms are frequently reported by patients with acute bacterial rhinosinusitis?
A. Nasal obstruction B. Profuse, watery chinorrhoca C. Facial pain, pressure D. Sneezing E. Post-nasal drip
A+C
12 or more
(≥3month)
with or without nasal polyps
CRSwNP
CRSsNP
- other rhinitis (allergic/non-allergic)
- immun-def.
- chronic syst. diseases that affect the nose: Wegeners/sarcoidosis
- Topical Steroids
- Classic symptomatic Tx(nasal douche, decongestants)
- acute exacerbation→ AB
- partially/uncontrolled → biologics

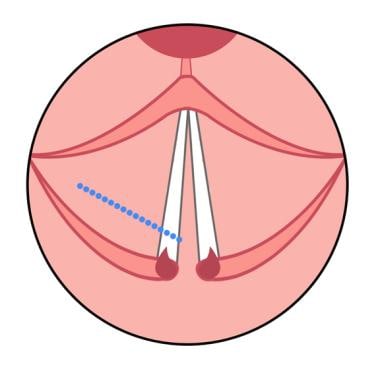
- Surgery: Endoscopic sinus surgery (FESS) 📷
- The main principle of Functional Endoscopic Sinus Surgery (FESS) is to surgically remove the affected areas at the level of the ostiomeatal complex.
- FESS aims to relieve obstruction of the ostia, restore natural sinus drainage, ventilation, and overall nasal physiology.
- The surgical procedure is performed endoscopically, targeting only the diseased regions.
- noninvasive
- mycetoma (fungus ball)
- allergic fungal
- invasive:
- chronic invasive
- acute fulminant invasive 📷
all of them except. acute fulminant
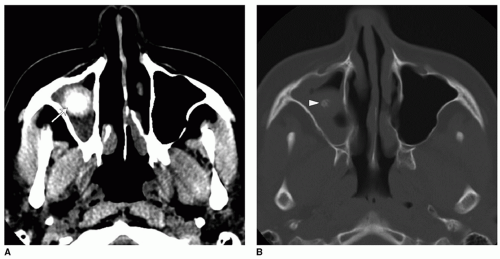
MRI / CT 📷
”Fungus ball in soft tissue and bone windows. A: Axial CT image with soft tissue windows shows a right maxillary sinus high-density rounded mass (arrow). B: Axial CT image with bone windows shows central calcification (arrowhead) within the mass. Note that the fungus ball and mucosa have different density appearances on soft tissue window, which cannot be appreciated on bone windows. On bone windows, the calcifications and bony structures are more conspicuous.”
skull base + orbit
fungal ball → surgery
invasive forms → surgery + antifungals
allergic form → surgery + antifungals PLUS steroids
Mycetoma | allergic fungal | chronic invasive | acute fulminant | |
Surgery | ✅ | ✅ | ✅ | ✅ |
Anti-fungals | (not required) | ✅ | ✅ | ✅ |
steroids | ✅ |
- squamous papilloma (nasal vestibule) + inverted papilloma
- Commonly arises at the level of the lateral nasal wall
- Presents as a unilateral polyp
- Locally aggressive, causing bony erosion of the lateral wall
- High propensity for recurrence after removal
- Associated with malignancy in 15% of cases
- osteoma (sinus)
- hemangioma (septum)
- angiofibroma (juvenile?)
Inverted papilloma:
maxillary sinus → SCC
Unilateral!
- obstruction
- discharge + epistaxis
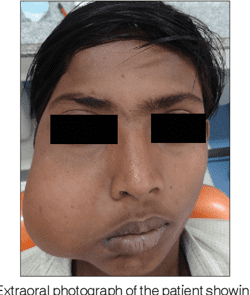
- swelling in the face ⇒ facial asymetry
- loose teath
- neurological compressive symptoms (diploplia, numbness of cheek)

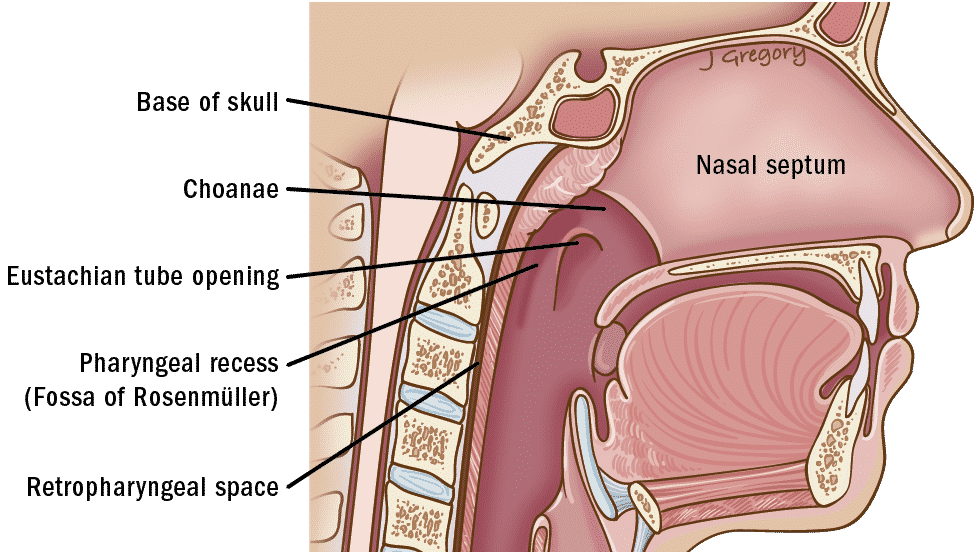
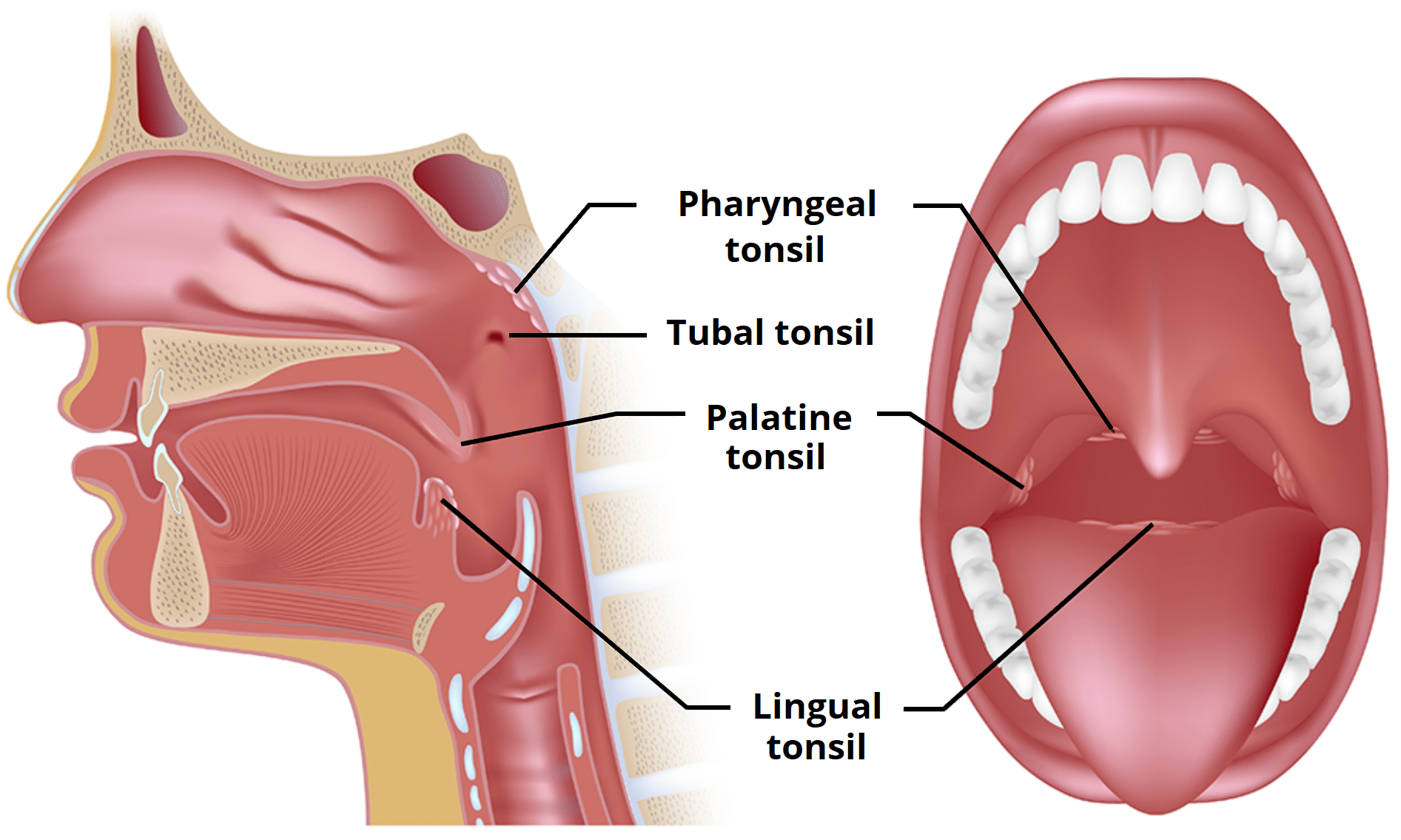
🧣 Pharynx

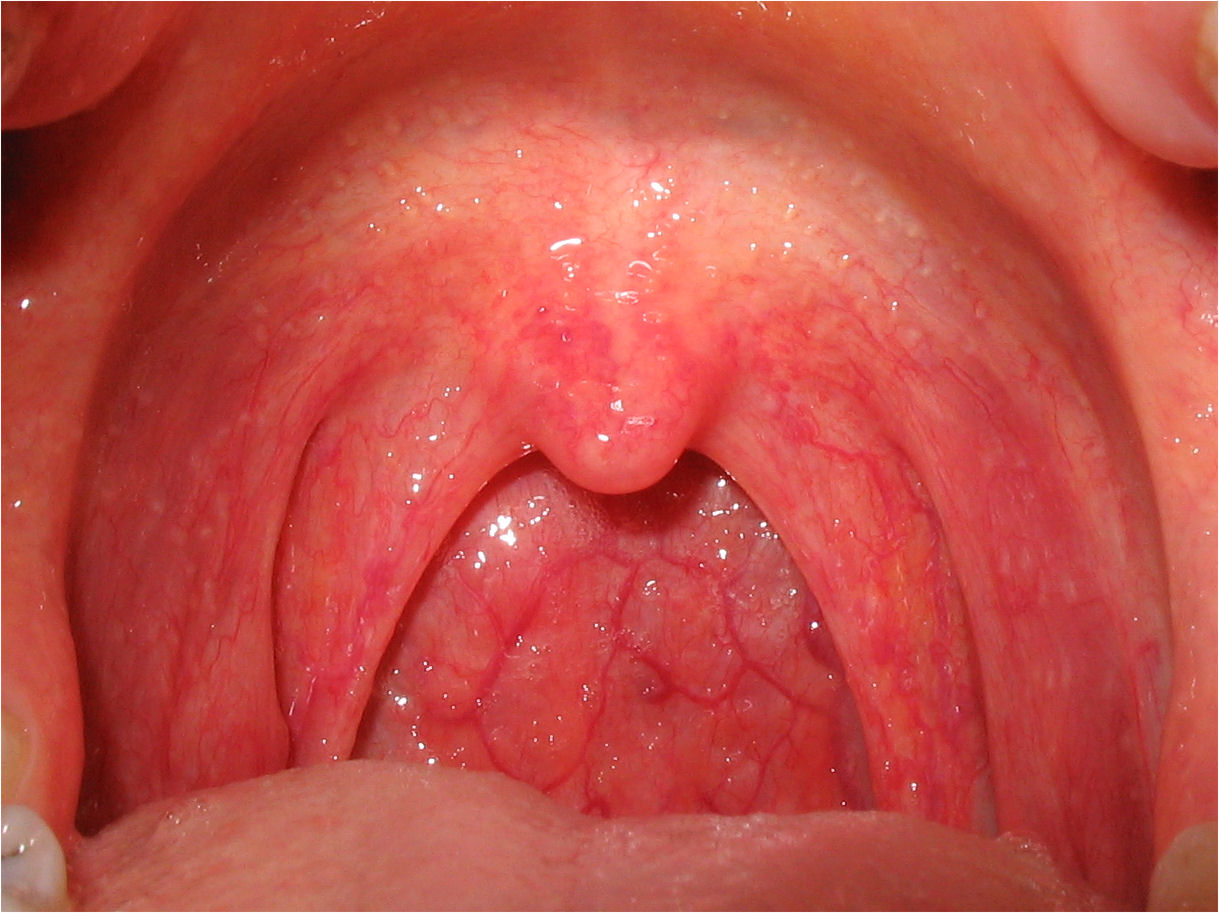
Q. Regarding follicular tonsillitis:
a) The inefction is present diffusely. b) The disease is often contagious. c) Streptococcus pyogenes can cause high fever and chills. d) The tonsils are enlarged and erythematous. e) Can be diagnosed via lab technique using swab techniques.
BCDE

STREP THROAT:
TONGUE:
characteristic course:

Exanthema
Starts on 👹 face (SPARES PERIORAL! = Filatov mask)
↓
⇒ spreads rapidly over entire body ⇒ GENERALIZED (measle-like) → TEXTURE: “ 🧽 SANDPAPER” (micropapules) → +- pruritus
↓
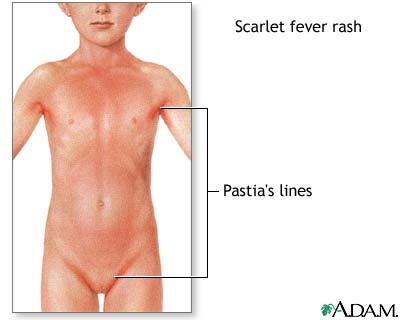
3) ⇒ after generalization ⇒ becomes more insense around skin folds: “🍝 PASTIA’S LINES”
↓
4) DESQUAMATION: ❄️ flaking of the face → after 1w: ✋🏼desquamation on hand 📷


Q. Infectious mononucleosis is characterized by:
A. Generalized tender lymphadenopathy B. A unilateral painful tonsillar ulceration C. Leukocytosis D. Positive Paul Bunnell test E. Ampicillin-based antibiotics are used if of bacterial superinfections are present


Fusiform bacilli + spirochaetes
Treponema vincentii, Spirochaeta denticulata, Fusobacterium necrophorum
bacterial overcrowding due to:
- poor oral hygiene (young adults)
- chronic dental/gingiva infection
- immunosuppressed
unilateral pharyngitis !!!
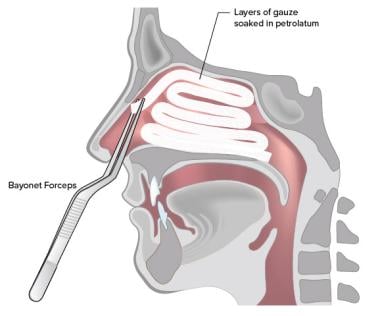
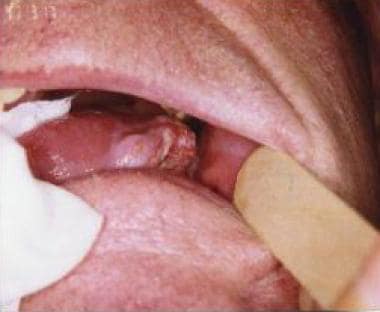
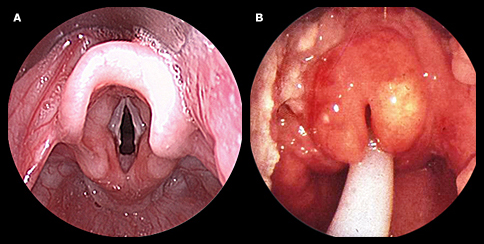
- Pseudomembranous 📷
- slow onset sore troat + fever
- oropharyngoscopy → necrotizing false membrane on one tonsil
- Ulcerative 📷
- ulceration with yellowish exudate
Q. Vincent's Angina evolves in stages. Which of the following statements is correct regarding Vincent's Angina? a) Evolves in 3 stages b) It is often seen in the elderly b) It has a gradual onset c) Fever is present d) Unilateral dysphagia is a symptom
CDE (2 stages, young)
malignancy (+other ulc. anginas)→ take biopsy!
- AB → Penicillin + >Metronidazole
- oral hygiene
- topical disinfectants
F - can be in immunocompromised + non-immunocompr.
infectious mononucleosis
→ but EBV manifest more often as pharyngitis
children
ELISA → Anti-CMV IgM
(or complement fixation test)
children
Vesicular + ulcerative lesions
→ lips
→ tongue
→ gums
(only occasionally oropharyngeal mucosa)
HERPES ZOSTER PHARYNGITIS = unilat painful vesicles
dys/odynophagia
fetid odor
↓general health
Same as vincents angina:
- false membranes
- necrotic ulcer (bleed)
lab
- High dose AB
- steroids
- blood transfusion
like mononucleous +anemia
- signs/symp of anemia
- generalized lymphadenopathy
- spleno/hepatomegaly
- ulcero-necrotic lesions
- leukemic infiltration:
- hypertrophic gingivo-stomatitis
- tonsillar enlargment
classic hema lab for leukemia
AB + steroids





- Inspection: Severe long-standing obstruction can lead to the development of the characteristic "adenoid face," which is characterized by a narrow and pale facial expression, a dumb expression, an open mouth, and sunken eyes.📷
- Palpation: Cervical lymphadenopathies may be observed.
Q. The main symptoms in adenoid hypertrophy are:
A. Nasal obstruction
B. Chronic oral breathing
C. Mucopurulent rhinorrhea
D. Recurrent episodes of epistaxis
E. sensorineural hearing loss

- Tuberculosis
- Syphilis
- Rhinoscleroma
- Leprosy



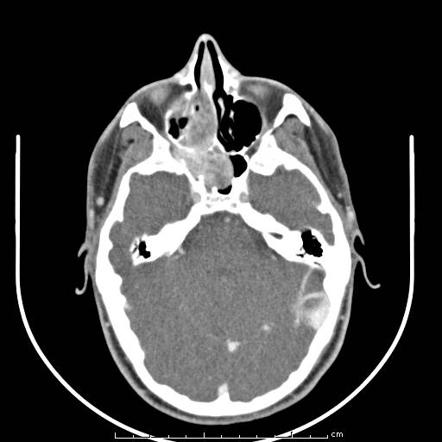
sphenopalatine foramen: 📷
CT: 📷
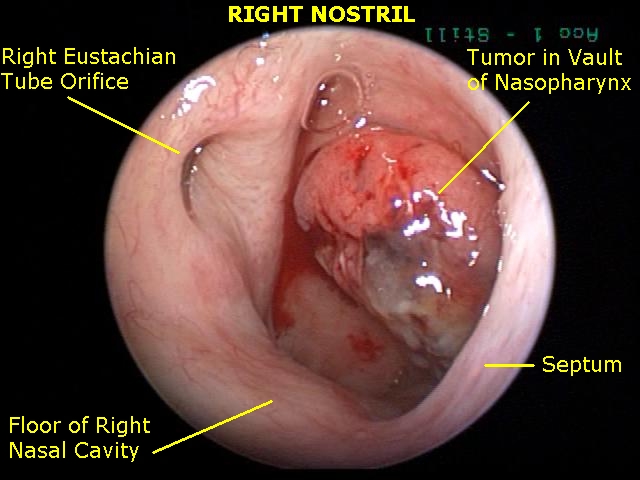
Q. A 14-year-old boy, complaining of nasal obstruction, nasally distorted speech, mucopurulent rhinorrhea, and unilateral right hearing loss with insidious onset. Parents report recurrent episodes of severe epistaxis. Which of the following is the most likely diagnosis?
A. Inverted papilloma B. Chronic invasive fungal rhinosinusitis C. Nasopharyngeal angiofibroma D. Nasopharyngeal carcinoma E. Wegener's granulomatosis
Q. The following statements about Nasopharyngeal angiofibroma are false:
a) infiltrating b) severe epistaxis c) biopsy should be performed d) highest incidence is 25-40 years of age
ACD = false
EBV
- upper neck mass
- ear: unilat conductive hearing loss (eustachian tube impairment)
- nose: obstruction, discharge, bleeding
- Neuro (i.e. cranial nerve palsies)
→ NO reffered Otalgia!!

Q. The main clinical presenting patterns in nasopharyngeal cancer are:
A. An upper neck mass B. Unilateral conductive hearing loss C. Referred otalgia D. Nasal obstruction, epistaxis E. Cranial nerve palsies
Initial: nasopharyngoscopy + biopsy
Work-up:
Extend? → MRI/CT
EBV? → Check for Antibodies
Serologic tests for EBV: Detection of IgA antibodies to EBV (anti-VCA, anti-EA titres)
#1 Curative RT
advanced? → RCT


post-cricoid cancer
(assoc. with a history of Patterson-Kelly-Brown synd)

Q. *The only head and neck cancer site which is characterized by a higher incidence in women is: A. Piriform sinus cancer B. Tonsillar cancer C. Supraglottic cancer D. Postcricoid cancer E. Soft palate cancer

Everything (except Tx) is same as tonsillar SCC
#1 Surgery + adjuvant RT
advanced → RCT
- Squamous cell carcinomas (75-95%)
- Other malignancies: minor salivary gland tumors
- Treatment: radiotherapy, chemotherapy, surgery
- Functional outcomes: varible, significant hyponasality of speech, nasal food regurgitation
- Rare occurrence
- Poor prognosis
- Treatment options: radiotherapy, chemotherapy
#1 “Lumb in the throat”
→ gets worse with saliva swallowing BUT food swollowing is normal
Øweightloss or other symptoms
often assoc. with cancerophobia
malignancy
GERD
- Tranquilisers + Anxiolytics
- PPI (GERD)
Q. Treatment of pharyngeal paresthesias consists of:
A. Tranquillisers B. Anxiolytics C. NSAIDS D. PPI E. Topical disinfectants
stabbing pain in palatine tonsil + base of tongue
Rule out malignancy
Carbamazepine + Symptomatic
(similar to trigeminal neuralgia)
dysphagia
SALIVA CANT FLOW INTO STOMACH
→ drooling, nasal regurg, choking, throat clearing, wet voice
- Myogenic
- Myasthenia gravis (+dysphonia)
- Neurogenic
- Central
- Stroke
- Parkinsons
- nerve specific
- Demyelinating syndrome: MS, Guillain-Barre
- Periph. nerve lesions
- Infections: Polio, Diphteria
🪗 Larynx

special form of acute laryngitis in young children (6m-3y)
viral infection (RSV) → subglottic edema → airway obstruction
- Signs of upper airway obstruction
- Dyspnea (during night)
- Stridor
- Inspriatory retraction (of suprasternal + supraclav. ST)
- Barking cough
- Normal voice + swallowing
Q. The main symptoms in acute edematous subglottic laryngitis are:
- A. Dyspnea and stridor
- B. Throat clearing
- C. Barking cough
- D. Drooling
- E. Quite normal voice
A,C, E (the other answer are referring to motor disorders / epiglottitis)
- O2
- Drugs that ↓ edematous obstruction
- Steroids
- Epinephrin (nebulized)
- broad spec. AB (prevent superinfection)
- last resort: Intubation/tracheostomy

→ see pharyngeal Dyphteria
upper airway obstruction
Classic anaphylaxis
- Epinephrin
- Steroids
- Antihistamines
- Last resort: Intubation/tracheostomy

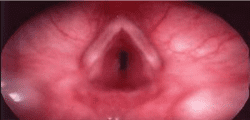
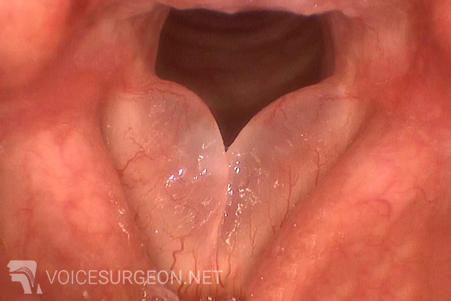
Reinke's space: 📷
Q. *A 52-year-old woman presents to your office with a chronic dysphonia. She describes her voice as low-pitched, often in the masculine range, and it started gradually one year ago. The patient is a long-term smoker and works in a noisy environment. The most likely diagnosis is…
A. Vocal polyp B. Vocal nodules C. Glottic cancer D. Reinke's edema E. Leukoplakia
red type → erythema, edema+swelling, secretion
white type → leukoplakia

- Grade I: Hyperplasia and/or keratosis with or without mild dysplasia
- Grade II: Moderate dysplasia
- Grade III: Severe dysplasia, carcinoma in situ without infiltration of the basement membrane
- immunocompromised (HIV, chemo)
- prolonged steroid + AB use
- Radiotherapy
ANTI-FUNGALS
nystatin or fluconazole
(severe: amphotericin)
- Tuberculosis
- Syphilis
- Rhinoscleroma
→ see Wegener’s nose
laryngitis + subglottic granulomatous ulcers
→ see Sarcoidosis nose
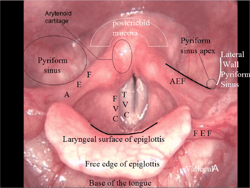
supraglottis
(non-caseating epitheloid granuloma)






Q. The main clinical characteristics of glottic large cell cancer are:
A. Early diagnosis B. Dysphonia is the first alarm symptom C. As tumor bulk increases, a typical raspy, hoarse voice appears D. High incidence of lymph node metastasis E. Upper airway obstruction develops in advanced disease
ABE
Q. A 55-year-old male patient presents to your ENT Department with a diagnosis of squamous cell carcinoma of the right vocal cord. The tumor is located at the junction between the anterior one-third and the posterior two-thirds of the vocal cord. The vocal cord exhibits mobility. Which two therapeutic options would be most appropriate?
A. Total laryngectomy B. Curative radiotherapy C. Frontolateral partial laryngectomy D. Endoscopic cordectomy E. Concurrent chemoradiotherapy
BC
cricoid cart. + thyroid gland
upper airway obstruction
glottis or recurr. laryngeal n.
surgery +/- adjuvant RT ⇒ thyroid isthmectomy
⇒ partial/total thyroidectomy
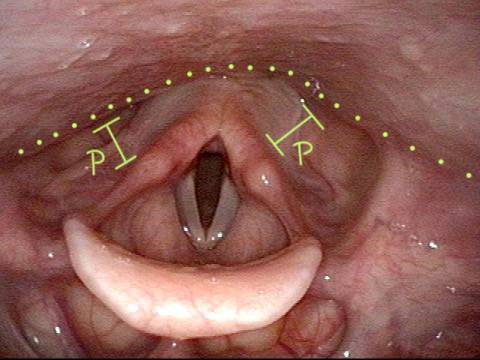
- unilateral
- bilateral
- acute
- chronic
thyroid gland surgery
- unilat → hoaresness + breathing voice
- bilat acute → acute airway obstruction
- bilat chronic → subtle airway obstruction → dypnea + insp. stridor + reccurr. URT infection (⇒ might lead to acute airway obstr. when infection present)
(bilat. voice = normal/mild)
CONSERVATIVE
- unilat → symptomatic (NSAIDs, steroids, voice rest, speech Tx)
- chronic bilat → treat episodes of URT infection! (Ab, steroids, NSAIDS)
SURGERY
Unilat
→ medial vocal fold augmentation
→ medialization thyreoplasty
Bilat:
Q. Main surgical procedures for bilateral vocal cord palsies are:
- A. Temporary intubation/tracheostomy
- B. Medialization thyreoplasty
- C. Myotomy of the crycopharyngeal muscle
- D. Posterior endoscopic cordotomy
- E. Endoscopic arytenoidectory
ADE (B→unilat; C→deglutiotion disorders: see slide 153 larynx)
24h to prevent subglottic stenosis
- Freq suction + local toilet of wound
- cuff of tube inflated as short as possible (prevent tracheal mucosa damage)
- AB, analgesics, mucolytics
- Immediate:
- bleeding, embolism,
- apnea → cardiac arrest;
- local dmg (cricoid, recurr. laryngeal, esophag)
- Intermediate (within 4 w)
- tube displacement/obstruction with secretion
- infections
- fistula
- pneumothorax/-mediastinum
- Late:
- Stenosis
bronchi
(mainly right main bronchus)
⇒ only 8% in larynx
- Hoarseness (/aphonia)
- cough → barking/croupy
- Signs of airway obstruction
- inspiratory stridor
- cyanosis
- dyspnea
- wheezing
- Endoscopy (laryngoscopy, bronchoscopy) or surgery
- acute: hits betw. shoulder blades, Heimlich 📷
- intubation/tracheostomy if needed
👂🏼 Ear



children → secondary to otorrhea
Impetigo → crust removal, AB-steroid ointment
Erysipel → Penicillin
Ramsey Hunt syndrome
→ neuralgia (painful)
→ faciel nerve palsy
→ vesicles
- Ear irrigation
- Curretage / Suctioning
- Ceruminolytics

Q. Which statements are true for otomycosis:
A. Presence of masses B. Tragal tenderness C. Aural fullness D. Clotrimazol is indicated E. Flavus is the etiological cause
ACDE







Q. Main complications of simple chronic suppurative otitis media are: A. Facial nerve palsy B. Diffuse extemal otitis C. Labyrinthine fistula D. Acute exacerbations
BD (AC = acuteSOM)
Q. *Etiological agents of simple chronic suppurative otitis media are: A. Streptococcus pneumoniae, Haemophilus influenza, Strep pyogenes B. Pseudomonas aeruginosa, Staph Aureus, Proteus C. Aspergillus flavus, Aspergillus niger
B


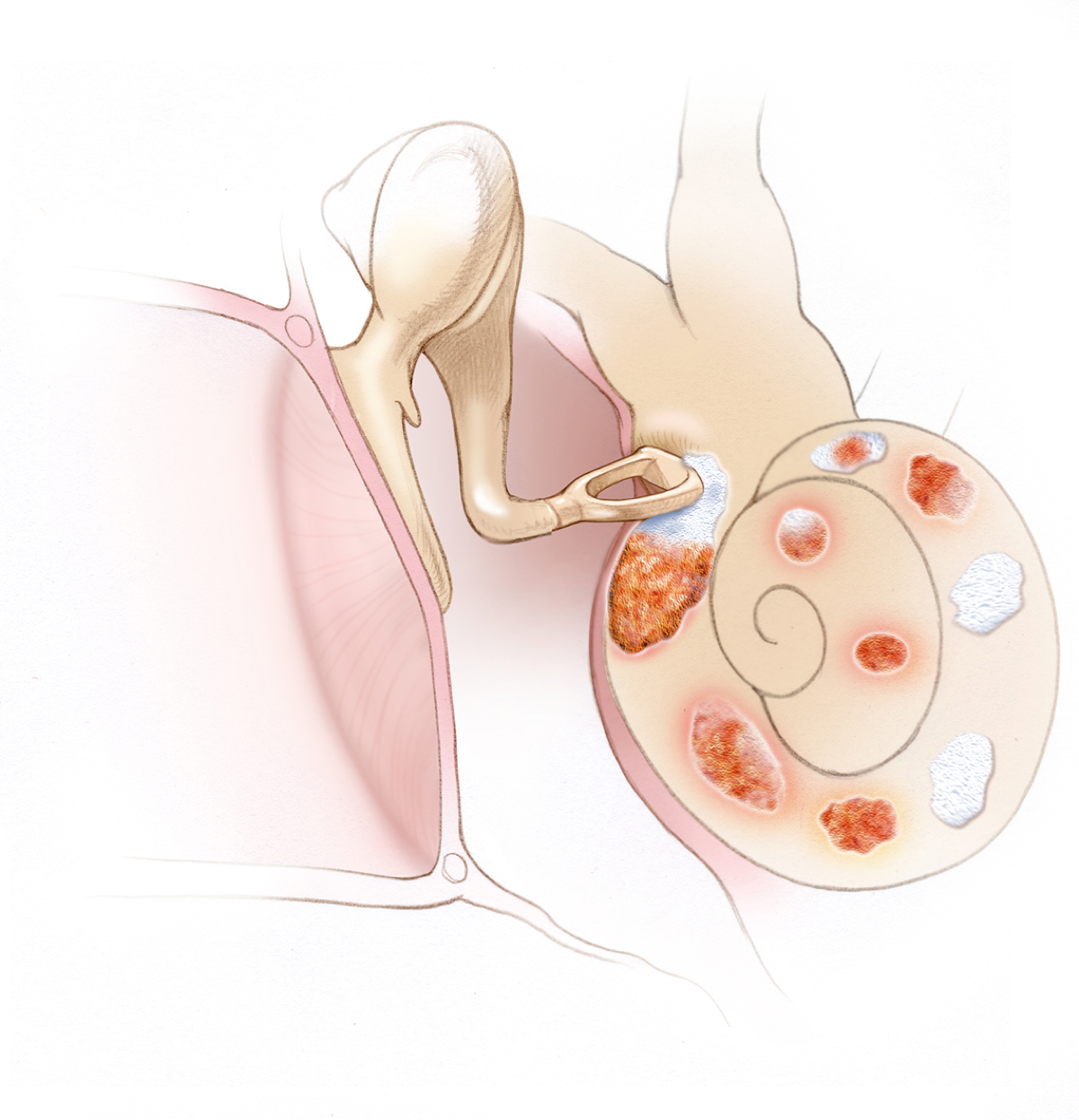
hereditary diseses → disorderded bone resorption/deposition in endochondral layer of the bony labyrinth(=otic capsule)
- Genetic predisposition: otosclerosis is more common in Caucasians and less common in Asian and black populations.
- Gender: Women have a higher likelihood of developing otosclerosis compared to men.
- Familial aggregation: There is evidence of familial clustering in otosclerosis cases, potentially related to defects in the COL1A1 gene.
- Measles virus infection: Measles RNA has been detected in fresh footplate specimens of otosclerosis patients, and higher levels of anti-measles antibodies have been found in perilymph during stapedectomy.
- Autoimmune disease: Autoimmunity to type II collagen or a related antigen may be involved in otosclerosis.
- Hormonal factors: Pregnancy can sometimes accelerate the progression of otosclerosis.
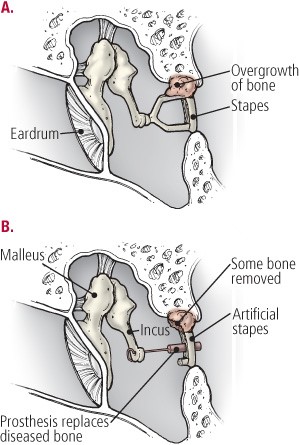
⇒ fixation of stapes footplate to oval window
⇒ conductive (later mixed) hearing loss
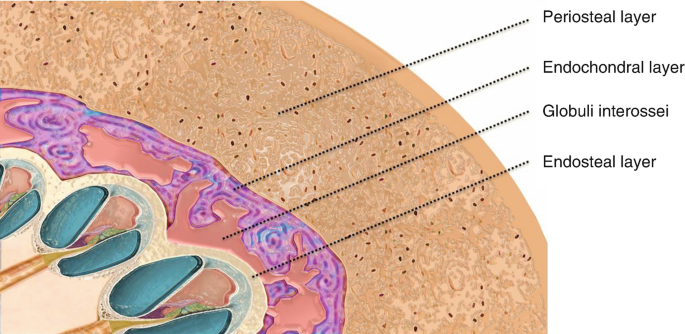
The bony labyrinth (otic capsule) has three layers: 📷
- inner endosteal,
- middle endochondral
- outer periosteal
- mainly woman 20-30y
- Slow progressive hearing loss (uni- or bilat)
- Tinnitus
- Vestibular symptoms
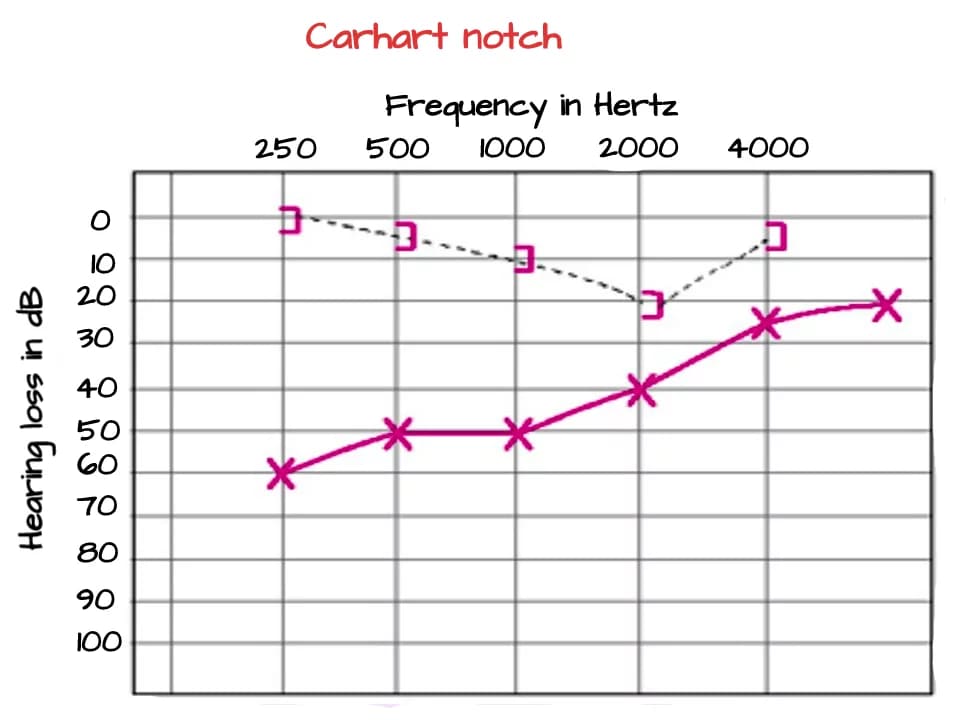
⇒ 70% mixed / 30% conductive
Q. Hearing loss in otosclerosis might be:
A. Conductive B. Sensorineural C. Mixed D. All of the above
AC
NORMAL!
NORMAL! (type A)
- A = normal
- As = stiffened tympano-ossicular system
- Ad = disarticulation
- B = middle ear effusion, tympanic membrane perforation, or impacted cerumen
- C = negative middle ear pressure
CT
- Otitis media
- Trauma of ossicular chain
- Tympanosclerosis
- Malleolus head fixation
- Other bony diseases: Osteogensis imperfecta, paget, sup. semicircular canal dehiscensce
air-bone gap <20 dB


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
fluride
RULE OF 3
sudden (≤3days OR on awakening) sensorineural hearing loss:
→ ≥30dB in ≥ 3 cont. freq.
- Infections:
- viral
- bacterial
- vascular
- bleeding
- occlusion
- spasm
- hyperviscosity / sicklecell
- Trauma
- Tumors
- Autoimmune disease
- Neurological
- MS
- Psychogenic
→ might induced perilymph fistula! ⇒ vestibular symptoms
- Sudden unilat. hearing loss
- Tinnitus
- Vestibular symptoms (vertigo, nausea)
- History!
- Exclude others causes for hearing loss
- Hearing tests
- vestibular tests
- Etiological search:
→ compl. ENT-exam
→ tumor + neuro exclusion → MRI
→ Lab test (i.e. Inflamm, Auto-Ab, test for germs)
#1 Steroids
Systemic/intra-typanic
Supplementary:
- ↑cochlear blood flow (dextran, pontoxiphylin)
- Spasm? → CCB
- Anti-virals
- Vitamins (ABCE)
fluctuating unilat. hearing loss + VESTIBULAR SYMPTOMS
⇒ RULE OUT PERILYMPHATIC FISTULA → Tympanoscopy → Positive? → seal with connective tissue graft (harvested from ear lobule)
bilateral progressive sensorineural hearing loss that is related to aging
higher 📷
(1).png){kind=link}
Tinnitus
- Obtain a detailed and accurate history
- Perform a complete ENT examination
- Conduct a hearing assessment, including:
- Tuning-fork tests
- Pure-tone audiogram
- Speech audiometry
- Tympanogram
- Auditory brain-stem responses (ABR)
🦻🏻hearing aids (binaural) + 🗣️ psycholocial care
binaural = both ears
T
→ but assoc. with chronic noise
tinnitus
history + audiogram ⇒ 4k notch 📷
{kind=link}
tinnitus Tx → steroids + vasodilators
hearing aid
noise protection
hearing and/or vestibular function
- aminoglycosides
- cisplatin
T → bilat/symetric + progressive
T
T
(=assoc. vegetative vestibular symptoms)
- antioxidants + iron-chelaters
- Evidences support the protective effect of antioxidants and iron-chelators
- oxidative stress plays a role in ototoxicity
- hearing aid / cochlear implant
- vestibular rehabilitation
Remove the ototoxic agent?
- Labyrinthitis
- Bacterial labyrinthitis (otogenic, meningogenic)
- Viral labyrinthitis: occurs during the course of a viral upper respiratory tract infection, including the middle ear
- Mumps: associated with deafness in about 4% of adult cases of epidemic parotitis; often severe and usually unilateral; vertigo may also be present
- Otosyphilis: presents with symptoms similar to Meniere's disease, including recurrent episodes of vertigo lasting for hours and progressive sensorineural hearing loss (endolymphatic hydrops - abnormal increase in pressure of the inner ear fluid)
- Conventional 📷
- Implantable
- Bone anchored hearing aid (BAHA) 📷 ⇒ in mastoid
- The device used for treating bacterial otitis media consists of a microphone, an amplifier, and a transducer.
- The transducer, which can be electromagnetic or piezoelectric, is connected to one of the middle ear ossicles or cochlear windows.
- The challenge has been to develop a small yet powerful device that can fit within the middle ear cavity and provide the necessary amplification.
- Cochlear implant 📷→direct nerve-stimul.
- Brain stem implant 📷
OR Middle ear implants 📷
→ when conventional cant be done
→ if damaged cochlear structures
→ if damaged auditory nerve
- congenital
- aquired (infections, ototox)
genetic syndromes
(usher, alport, pendred)
- Hearing test
- Imaging
- Speech development evaluation
- Neuro + Optha exam
- genetic testing
hearing aids
surgery
→ if conductive OR severe sensorineural (cochlear implant)