
Table of content
- CV surgery
- ⛲ Basics
- 🫁 Pulmonary embolism
- 🎒 Pericarditis
- ⛵ Cardiac valve surgery
- 🪕 Ischemic cardiopathy
- 👶🏽 Heart defects in neonates and infants
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6

CV surgery
⛲ Basics
mitral → systolic
aortic → diastolic
mitral → diastolic
aortic → systolic
- Take the blood from the vein → venous canulla into right (atrium) appendix or 2 canula into SVC + IVC or into Internal jugular vein
- blood → venous resorvoir
- resorvoir → main pump → into heat exchanger

- heat exchanger → oxygenator
- oxygenator → aortic canula: usually into desc. aorta or femoral, axillary, common carotid
- sucker → suck out blood from operation field → into resorvoir
- vent → theres still blood from the lungs go to the left ventricle → blood accumulates there → distension → needs to be sucked out → into resorvoir
- cardioplegia →to protect from ischemia → slow down metabolism → cool down + cardioplegia solution (stop the heart)→ canula into asc. aorta → push solution → aortic valve will close → solution into coronary arteries (⚠️alert: in aortic stenosis solution will go into ventricle → open aorta + operate valve; when also coronary stenosis → canula directly into coronary sinus (veins)=retrograde cardioplegia)
Cardioplegia solution:

heparin (nice monitoring → aPTT, and reversible→protamin)
at beginning of surgery → Hemodilution to let the blood flow freely into tubes
- stop cardioplegia solution + declamp aorta → washes out cardioplegic solution → starts by itself
- artificial pace-maker
- defibrillator if fibrillation happens
🫁 Pulmonary embolism
DVT
Virchow Triad → endothelial lesion, stasis, hypercoagulability
- venous stasis:
- hypercoagulable state
- immobilization
- trauma/surgery
- pregnancy + oral contraceptives
- malignancies
- massive pulmonary E
- acute pulmonary infarction
- PE without infarction
- repetetive pumonary embolism → pulmonary HT
- Dyspnea
- Hypoxia
- Pain
- shock: ↓BP, periph vasocon., ↑HR, ↑RR
→ pallor, sweating, oliguria
- S3 = ri. ventricular gallop (RVF)

- palpable impulse at left 2nd ICS (RVF → shift of PMI)

- systolic murmor in inspiration at left sternal margins (triscupid regurgitation)
- hemodynamic parameters
- degree of cardiac damage
- degreee of prev. Cardio-pulmo. damage
- location of obstruction
acute: embolus too small to cause shock or pulmonary HT → but enough to block significant parts of the lung → necosis → inflammation → pleural involvement
- pleuritic pain (=increases at inspiration) → ↓movement of the hemothorax + pleural friction + signs of pleural effusion,
- dyspnea
- hemoptysis
repetetive small embolus (see point 4.) into lungs → no symptoms but closure of a lot of pulmonary arteries → ↑pumonary resistance → pulmonary HT
hypertrophic right ventricle → dilates after time (cant compensate anymore) → chronic right heart failure:
- jugular distension
- palpable impulse at left 2nd ICS (RVF → shift of PMI)
- systolic murmor (triscuspid regurgitation)
- ascitis + hepatomegaly
- lower limb edema
- MI (troponin, ECG)
- Chronic heart failure + acute pulmonary edema
- Aortic + Mitral stenosis
- pericarditis + temponade
- Dilated cardiomyopathy
- ARDS (acute respiratory distress syndrome)
- Other forms of shock (DD with massive emboli)
- pulmonary Angiography #gold-standard
- AngioCT
- ECG
- Doppler US→ Detection DVT
- Echocardiography (not for dg just to check heart)
- Xray
- Scintigraphy (tells perfusion at the level of lungs)
- Anticoagulant → Heparin (unfractionated or LMWH) → bolus + perfusion; Rivaroxaban, Warfarin (long-term) → give heparin for 3month + correct risk factors; if cant correct → for life
- Thrombolytics → if hemodynamically unstable + Ø bleeding risk; and if high risk patient (see score) without hypotension with low risk for bleeding
Embolectomy → CPB + open pulmonary artery (evacuate from there) → in massive PE when contraindication for thrombolytics or become unstable
→ if migrated in small branches → you cant take them out
→ Not indicated in low risk PE; + in submassive PE with minor right ventricular dysfunction (high surgery risk)
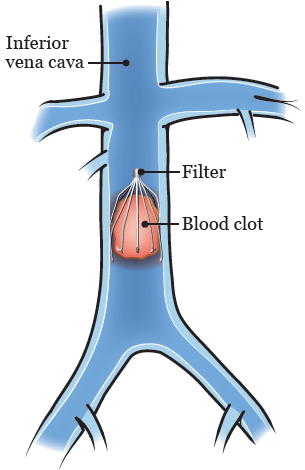
Caval filters 📷(filter into IVC → block embolus) → indication: DVT with contraindication to anticoagulants, after massive PE (survived but another episode will be fatal), recurrent pulmonary embolism
🎒 Pericarditis
- MI
- viral + bacteria + TBC
- uremia
- neoplasm
- trauma + post-op
- diffuse inflammatory infiltrate
- ↑vascularization
- +/- pericardial effusion
- appearance: brown, serous, fibrous, hemorrhagic, white (lymph), purulent
- self limited
- a lot of liquid → tamponade
- recurrent
- become chronic
viral - self limited - regress in 1-2w
bacteria + neoplastic → fatal without treatment
- +/- inflammatory syndrome
- +/- pericardial effusion → dry or exudative
- pain during inhalation (dry) sudden or progressively
- radiation neck/epigastrum
- Pericardial friction → superficial murmor when patient inhales
- disappears when liquid accumulates in pericardial sack
- pain
- dyspnea + tachycardia
- signs of compression (dysphagia, dysphoina, cough)
- fever / subfebrile
- altered general state
- muffled heart sounds
- cardiac tamponade = BECKS TRIAD 📷 (if rapid accumulation of liquid) → ventricles cant fill during diastole → esp ↑of right ventricle p → pushes septa towards left → shock → orthopnea, edema, dilated jugular veins
DRY
EXUDATIVE
- ecocardiography #goldstandard → liquid, heart affection
- CT + MRI
- xray → cardiomegaly
- Pericardial punction → diagnostic (etiology) + treatment (decompression)
- Lab: inflammatory markers: CRP, Leukos, ↑fibrinogen, ESR
Drugs:
- Analgesics
- Anti-inflammatory drugs
- AB (if bacterial)
- cytostatics (if neoplasia)
- tuberculostatics (TBC)
Surgical:
- Pericardial punction (US guided)
- if Ø possible → Surgical drainage → minimal pericardiotomy (at xyphoid process)
- idiopathic (most common)
- viral or infective pericarditis
- TBC
- truama
- Connective tissue disease
- post-radiation
hypodyastolic cardiac insufficiency
→ hepatic insufficiency
→ renal insufficency
→ venous insufficiency
- slow progression
- fatigue (lower blood volume ejected into circulation)
- congestion:
- dyspnea
- dilated jugular v
- hepatomegaly + ascitis + icterus
- edema lower limbs
- Xray → eggshell appearance if calcification
- Echocardiography → pericardial thickening + dilation IVC
- CT + MRI
- Lab: ESR, liver function
- symptomatic - medical
- curative surgery: subtotal pericardectomy

⛵ Cardiac valve surgery
- LV hypertrophy
- low cardiac flow
when effort:
- angina
- dyspnea
- syncope
- death
- pulsus parvus et tardus 📷
- systolic ejection murmor
- diminished BP in systoly
- ECG → LV hypertrophy
- Ecocardiography #most important
- xray → calcification
- coronarography → for planning of surgery (most of patient are old and often have coronary diseases)
depends on valvular lesions, specific symptoms, ventricle function, comorbities
- symptomatic = surgery
- asymptomatic with severe stenosis + ventricular dysfunction/ventricular tachycardia/hypertrophy(>15mm septum), orrifice <0.6cm2) = surgery
- moderate stensosis, in patient which also receive operation on asc. aorta or coronary artery = surgery
replacement aortic valve (Øpossible to repair)
→ under CPB
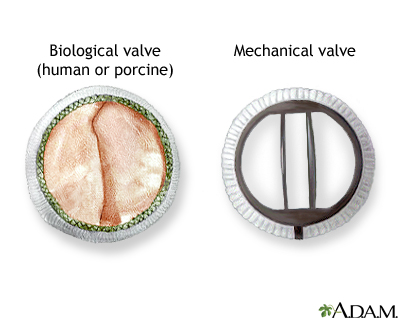
→ open aorta → replace valve with mechanical/biological valve (with stent or stent-less)📷
Mechanical: Østrucural defect, but anticoagulant for indefinite time
Biological: Øanticoagulation, but ↑rate of structural defects (over time)
Aortic valve cant close properly → backflow during diastole from aorta to ventricle → ↑blood volume in ventricle
- endocarditis
- Rheumatism
- Aortic dilation: dissection or collagen diseases
- trauma
- Inflammatory disease
- Bicuspide aortic valve
- endocarditis (i.e. due to rheumatic fever)
- aortic dissection
- trauma
- ventricle is not adapted to that much volume
- ↑hypoxia of coronaries
- hypertrophy of ventricle → dilation → mitral insuff → pulmonary congestion (esp when complicated)
- angina
- dyspnea (effort)
- asthenia
- ↑pulse pressure (↓diastolic)

- diastolic murmor 4th ICS
- ECG → LV hypertrophy
- Ecocardiography #MVP→ valvular modification
- Doppler → regurgitation
- Xray → dilated heart + asc. aorta
- CT + MRI
- Endocarditis prophylaxis
- Vasodilators + ACE inhibitors ⇒ ↓after-load
- symptomatic with severe. aortic insufficience + EF>60(normal)
- severe aortic insuff + normal EF, but progressive ventricular dialtion
- symptomatic/ asymptomatic dysfunction of LV
- Thromboembolism - esp with mechanical valve → anticoagulation
- Thrombotic blocking of mechnaical valve
- Hemorrhage
- Valve
- Endocarditis on valve prothesis
- Valvular dysfunction
- Hemolysis
Endocarditis is a life-threatening inflammation of the inner lining of your heart's chambers and valves (endocardium). Might be associated with splenic vein thrombosis (palpate spleen)
inflammatory vegetations at the valves
T
- early(<2m): high mortality, dysfunction of prosthesis → AB broad spec (Vancomycin+Rifampicin + Gentamicine)
- Late (>2m): sub-acute
1.5x
- Rupture
- Aortic insufficiency
- Ischemia (myocardia, cerebral, visceral, periph)
diameter
- Marfan (collagen disorders)
- Aortic dissection (chronic)
- aortic valve pathology (impaired blood flow in aorta)
- remove asc. aorta → vascular prosthesis 📷
- or remove asc. aorto together with aortic valve (if stenosis present)
- if aortic root dilated (ie. in marfan) → remove asc aorta, aortic root + valve → aortic valve prosthesis+ vascular + root prosthesis = Bentall-DeBono operation 📷
- or same as Bental-DeBono but valve sparing
classic RFs
- smoking
- HT
- Cholesterol ↑
- arteriosclerosis
- diabetes
rupture of aneurysm
- asymptomatic
- history of HT + smoker
- nausea + vomiting
- pulsatile abdominal mass
- pain (vetebral body erosion) → post. irradiation
- if ruptured:
- acute pain
- hemorrhagic shock: Hypotension + shock
- pulsatile mass
F → 80%❗
hemodynamic stabilization (i.v. fluids)
- symptomatic
- asymptomatic:
- if diameter 4-5cm young, low risk, good life expectancy
- if diameter 6-7, elderly or very high risk
dying patient not responding to CPR
- perforated organ
- mesenteric artery occlusion
- MI
- PE
- acute pericarditis
- renal colic
- lumbo-sacral nerve irritation/lesion
🪕 Ischemic cardiopathy
arteriosclerosis
Smoking
high cholesterol
diabetes
obesity
MI (due low blood flow → obstruction)
- Angina pectoralis → stable (pain with effort) or instable (at rest)
- MI
- Sudden death
- acute pericarditis
- myocarditis
- valve diseases
- Aortic dissection
- PE
- GI causes (hiatal hernia, GERD, cholecystic, acute pancreatits)
- pneumothorax
- Effort test
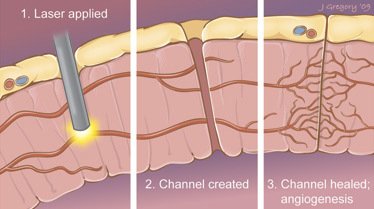
- Coronary angiography 📷 → stenosis + obstruction, also Left ventricle function (hypo-,dys- or akinesia) + collaterals
- intravascular US
- Intracoronary doppler
- ECG only modified in MI
- reduction of risk factors: stop smoking, Hypertensive drugs, Statins, exercise, diet
Anti-platelets:
→ Aspirin
BP lowering:
→ Nitrates
→ Beta-blockers
→ ACE inhibitors
→ Ca channel blocker
Cholesterol lowering:
→ Statins

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- #1 Left Internal mammary artery (aka internal thoracic)
- Right internal mammary artery
- internal Saphenous vein
- alternative: radial artery, external saphenous v
after 1y already 20% thrombosed
25% after 5y
50% after 10y
use both internal mammillary artery + gastroepiploic
(=modern shit + Øreally freq. used)
🐙 Octopus(sy) 📷
{kind=link}
heart not stopped → no complications like with CPB
but anastomotic technique is not so perfect like with CPB → thats why you use octopus
- MI (rare after CPB)
- Stroke
- acute renal insuff
- infection
- etc
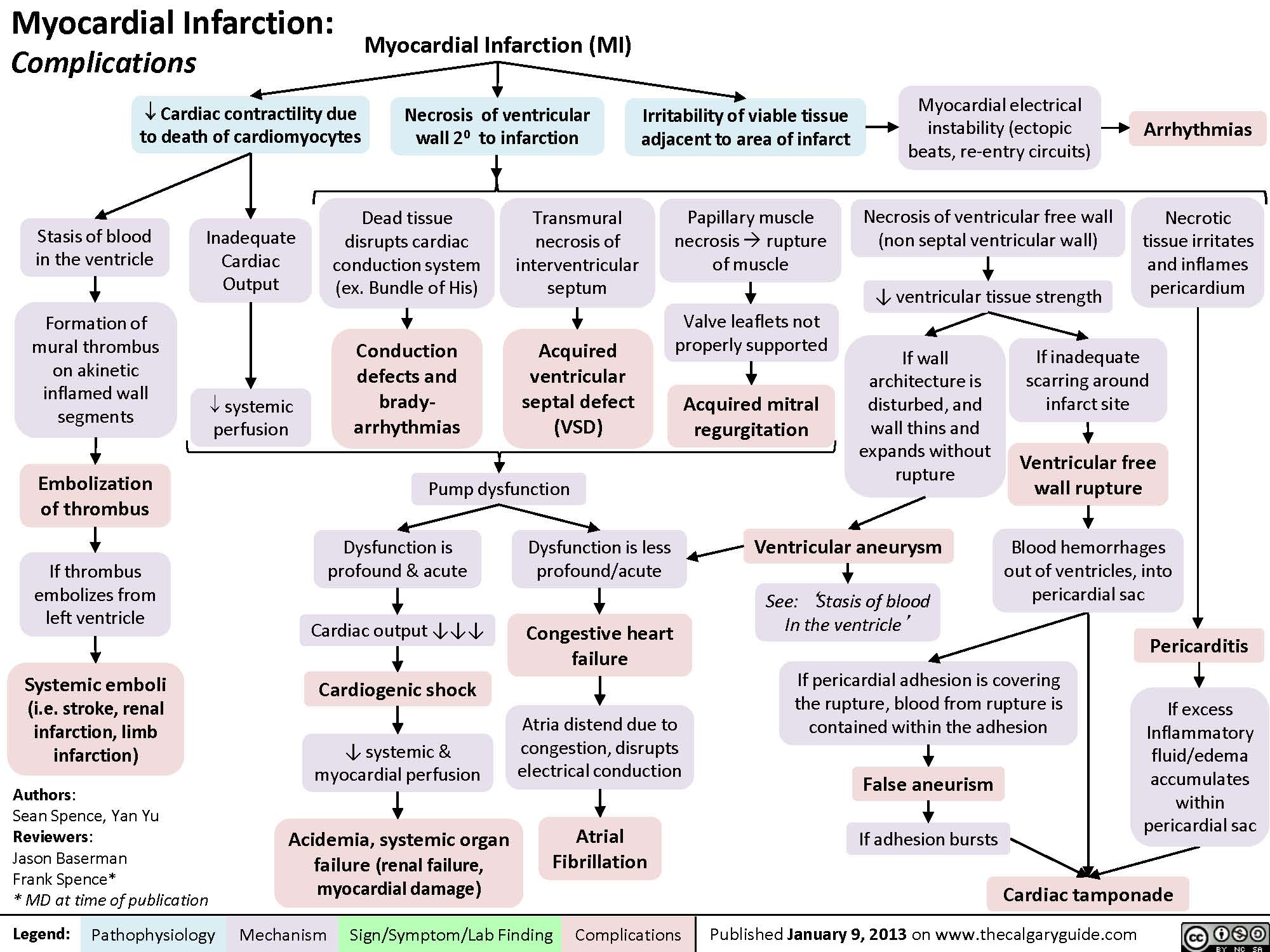
the 4 most imporant are:
- aneurysm
- mitral insuff
- VSD (Ventricular-Septal defect)
- free rupture left ventricle
{kind=link}
Complication | Occurrence | Description |
Cardiac arrhythmia | First few days and within the first 24 hours post-MI | Important cause of death before reaching the hospital |
Postinfarction fibrous pericarditis | 1-3 days | Friction rub |
Papillary muscle rupture | 2-7 days | Postero-medial papillary muscle rupture ↑ risk from posterior descending artery. Severe mitral regurgitation. |
Interventricular septal rupture | 3-5 days | Macrophage-mediated degradation → VSD → ↑ O2 saturation and pressure in RV |
Ventricular pseudoaneurysm formation | 3-14 days | Free wall rupture contained by adherent pericardium or scar tissue; ↓ CO, risk of arrhythmia, embolus from mural thrombus |
Ventricular free wall rupture | 5-14 days | Free wall rupture → cardiac tamponade. LV hypertrophy and previous MI protect. Acute form leads to sudden death. |
True ventricular aneurysm | 2 weeks to several months | Outward bulge with contraction ("dyskinesia"), associated with fibrosis. |
Dressler syndrome | Several weeks | Autoimmune phenomenon resulting in fibrinous pericarditis |
LV failure and pulmonary edema | Occurs secondary to other complications (timing depends on them) | Due to LV infarction, VSD, free wall rupture, papillary muscle rupture with mitral regurgitation. |
👶🏽 Heart defects in neonates and infants
⇒ see later❗
- Without Shunt
- valve malformation
- coarctation aorta
- Left-to-right shunt
- PDA
- SD
- ASD (atrial septal defect)
- VSD (ventricular septal defect)
- AVSD (atrio-ventricular septal defect)
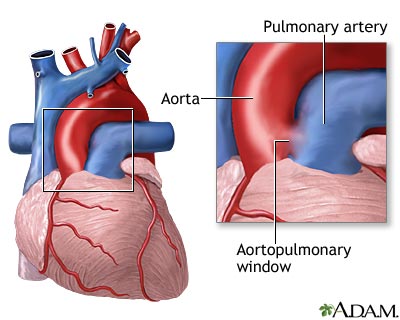
- aorto pulmonary window
- Right-to-left shunt
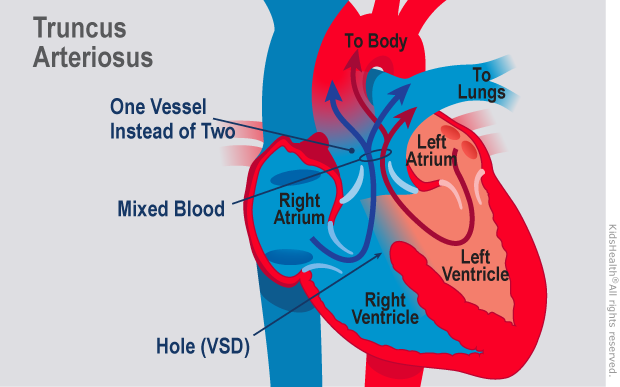
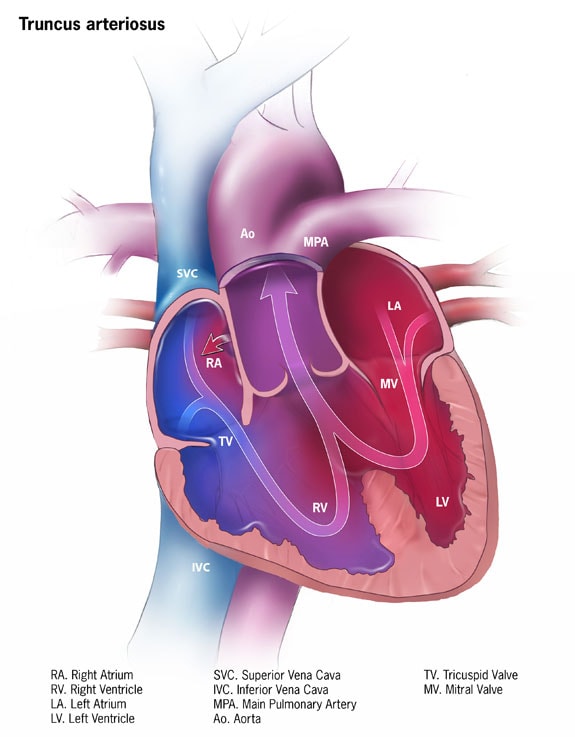
- truncus arteriosus
- TGA
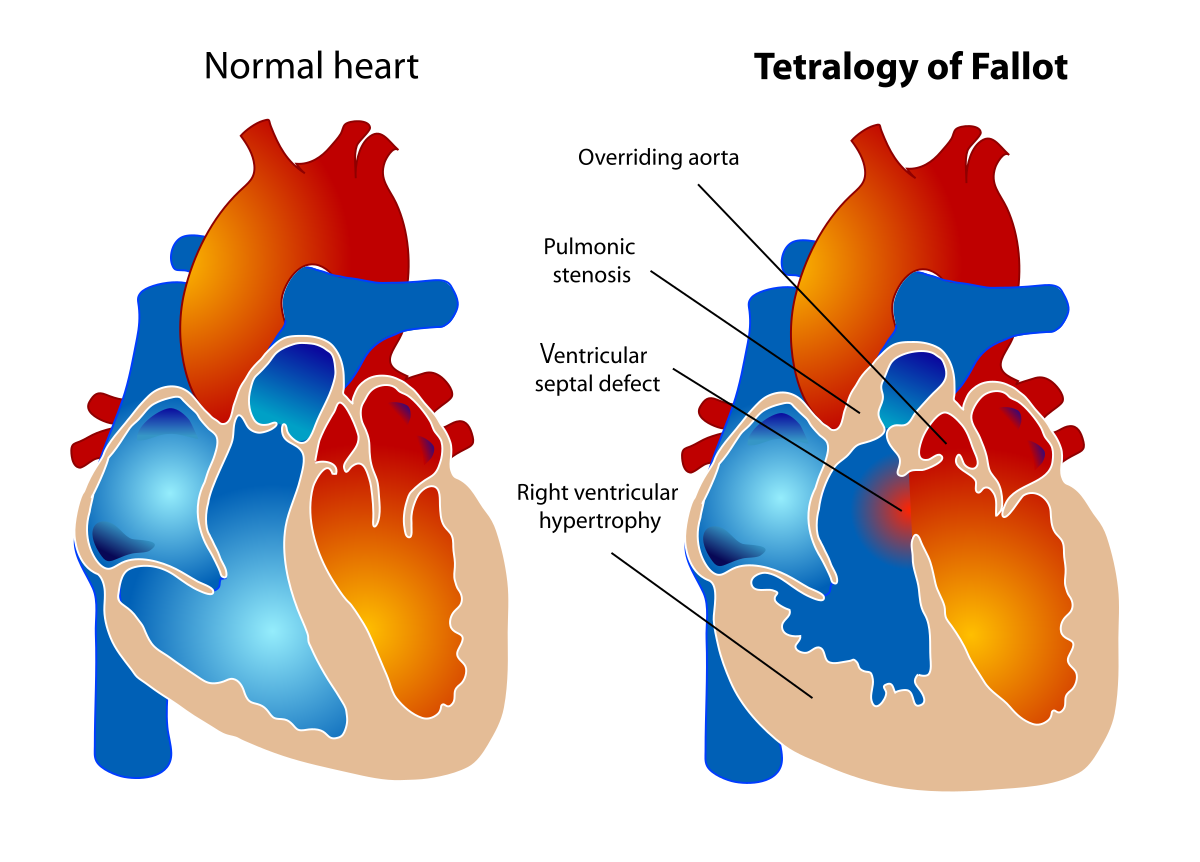
- TOF
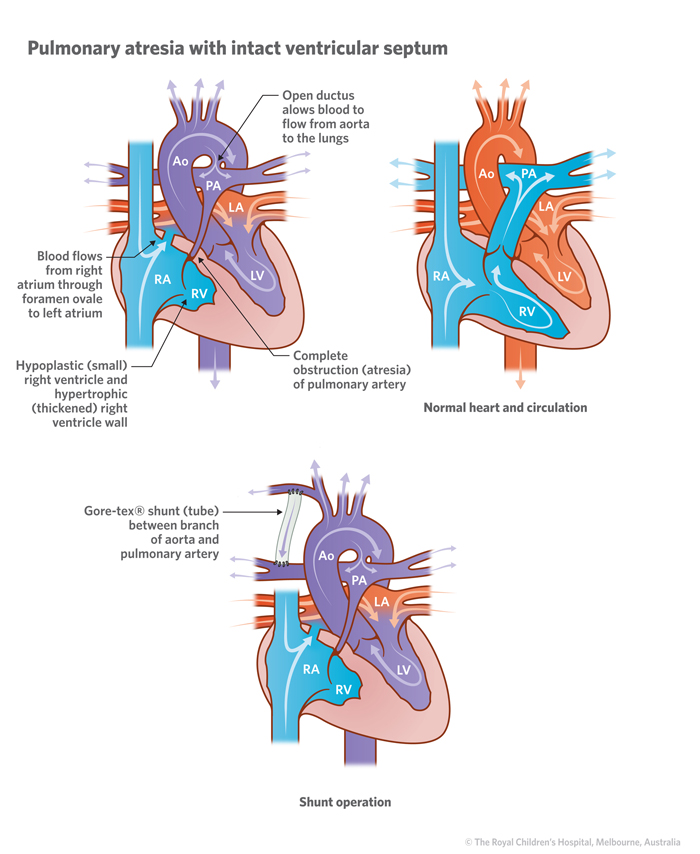
- Pulmonary atresia +- septal defect
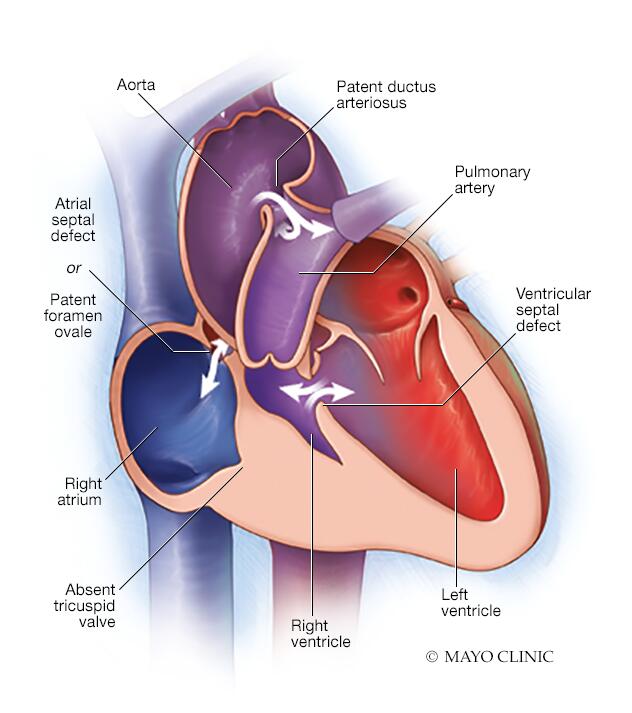
- triscupid atresia
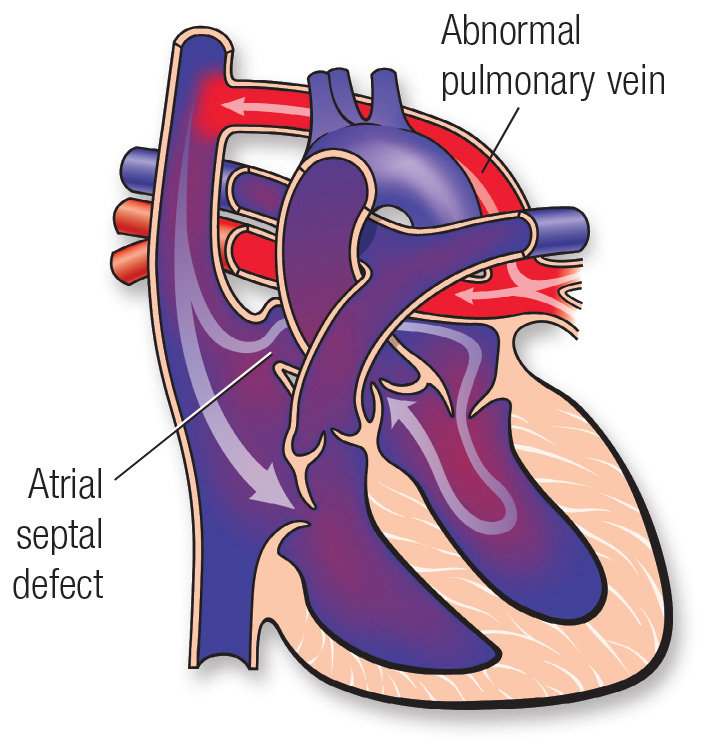
- total anomalous pulmonary drainage
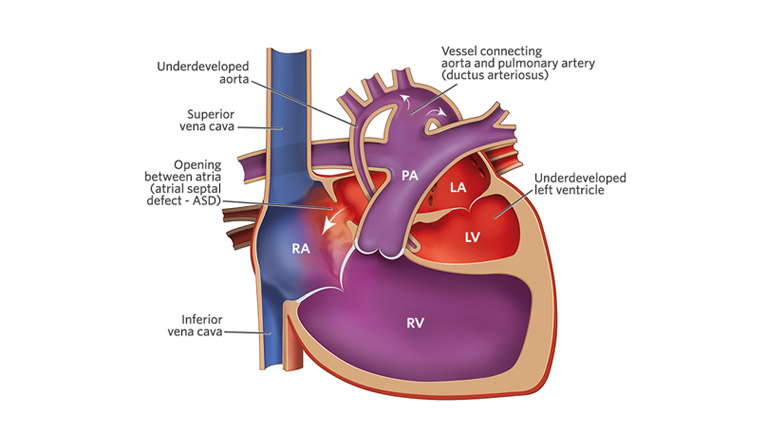
- Hypoplastic left heart syndrome








xray
ECG
echography
MRI + CT with catheterization
endocarditis
RV hypertrophy + pulmonary HT 📷 → cyanosis + hypoxemia
{kind=link}
- reactive polycythemia, hyperviscosity + coagulopathy
- thrombosis
- mental + physical growth impairment
- death ( due to hypercyanotic episodes aka "hypoxic spell")
Septal defect (AVSD/VSD) → Left-to-right shunt → pulmonary HT → right ventricle hypertrophy → reversing of shunt: right-to-left-shunt → pulmonary circulation is "skipped" → hypoxia
Heart-Lung transplant
percutaneous (less complications+no scarrs, +ØCBP)
or surgical
{kind=link}
communication aortic isthmus + bifurcation pulmonary artery
i.e. polypnea
directly after dg (severe symptomatology present)
- depends on angiographic type
- only betw 3-7(10)mm (Ølarger, Øsmaller)
- children over 6kg
- Large non-restrictive ductus
- in newborns + prematures
- if assoc. with severe CHF
- Large ductus >7mm
- Second defect with surgery indication
- Medicine (ibuprofen)
- Catheter-based procedures
- Surgery
symptomatic (regardless of age)
1y
paradoxical

- central (oval fossa defect) 📷
- non-central margins >5mm
- circumference <30mm
- all non-central types(see below) 📷
- thin margins
- central >30mm
patch on defect → continous suture
Amplatzer device → 2 umbrellas
Video: Paradoxical embolism + Amplatzer device:
{kind=link}
- perimembranous defects
- subaortic
- but onto central fibrous body
- juxta-arterial defects
- beneath conjoined arterial valves
- muscular defects
- entirely enclosed in muscular septum
larger VSD → early + severe
smaller VSD → later + less severe
symptoms: CHF, failure to thrive, ↑PAP, valvular defects
- muscular defect 📷
- perimembranous → generally not by interventional treatment: only when bigger distance to aortic + tricuspid valve
- juxta-arterial
- perimembranous
patch + suture
- Severe CHF first weeks of life + no response to drugs
- multiple muscular defects + shunts and severe CHF or PHT
- large defects with severe PHT (reversibility of PHT uncertain)
pulmonary artery banding 📷→ band around pulmonary artery → stenosis → protection of lung
also give viagra (treat pulmomary HT) [#no joke]
Viagra (aka sildenafil), helps with pulmonary hypertension by dilating the blood vessels in the lungs. It works by inhibiting phosphodiesterase type 5 (PDE5), which is responsible for breaking down cyclic guanosine monophosphate (cGMP). By inhibiting PDE5, Viagra increases the levels of cGMP, which relaxes and widens the blood vessels in the lungs, reducing pulmonary hypertension and improving blood flow.
after 1y meassure pulmonary pressure + surgically correct if possible
triscuspid + mitral → fuse: common orifice → insufficent valve 📷
{kind=link}
COMPLETE defect
- Regardless of age: if severe clinical symptoms
- betw. 3-6month: If well tolerated
PARTIAL defects
- Regardless of age: if severe clinical symptoms present,
- Betw. 3-6month: If important pulmonary hypertension is present
- < 5y: If well tolerated
acutally <5years is not true → nowadays: operate every defect before age of 1
- 1 patch on each ASD + 1patch on VSD 📷
- or common patchu
- reconstruction mitral+bicuspid valve
< 3month: if severe PHT assoc. with one of:
- multiple VSD
- parachute mitral valve 📷
Parachute mitral valve (PMV) is a congenital valvular anomaly in which all the chordae tendineae of the mitral valve are attached to a single papillary muscle.
pulmonary artery banding
{kind=link}
Aortopulmonary window (AP window) is a congenital heart defect characterized by a communication between the ascending aorta and the pulmonary trunk (more prox than PDA)
at time of dg
(this shunt is big like a motherfucker)
- ØRepair at all (→ pulmonary banding + viagra instead)
- PVR ≥8 wood units
- PVR/SVR > 0.7
- Postpone repair
- Qp/Qs < 1,5

PVR = pulmonary vascular resistance, SVR=systemic vascular resistance; Qp= pulmonary flow; Qs=systemic flow
correct abnormalities:
- infection free
- optimal heart failure tx
- anemia free
- optimal nutritional status
CPB + Surgical repair using patch closure 📷
{kind=link}
is the preferred treatment and should be done early to avoid the development of pulmonary hypertension. Pulmonary hypertensive crisis can complicate the immediate postoperative care
- myocardial failure (post CPB)
- hemorrhage
- post-OP pulmonary HT crisis
- surgery related complication → AV block (suture into his bundle) + hoarse voice (disection recurr. laryngeal n.)
- NITRIC OXIDE
- ventilatory support
- pulmonary vasodilator drugs
{kind=link}
- pulmonary stenosis
- → right ventricular hypertrophy
- VSD
- overriding aorta
- The term "Overriding Aorta" refers to a specific malposition of the aorta in relation to a high septal defect in a congenital heart defect.
- The aorta, which usually originates from the left ventricle, is displaced to the right
- The aorta rides over the hole in the septum, receiving blood from both ventricles.
- various presentation: cyanosis, hypoxic spell or acanotic
- US
- Angiography + catheterization (if needed)
ToF after pallative treatment of pulmonary HT (angiography is needed here)
3-6month → before: do palliation (systemic-pulmonary shunt)
{kind=link}
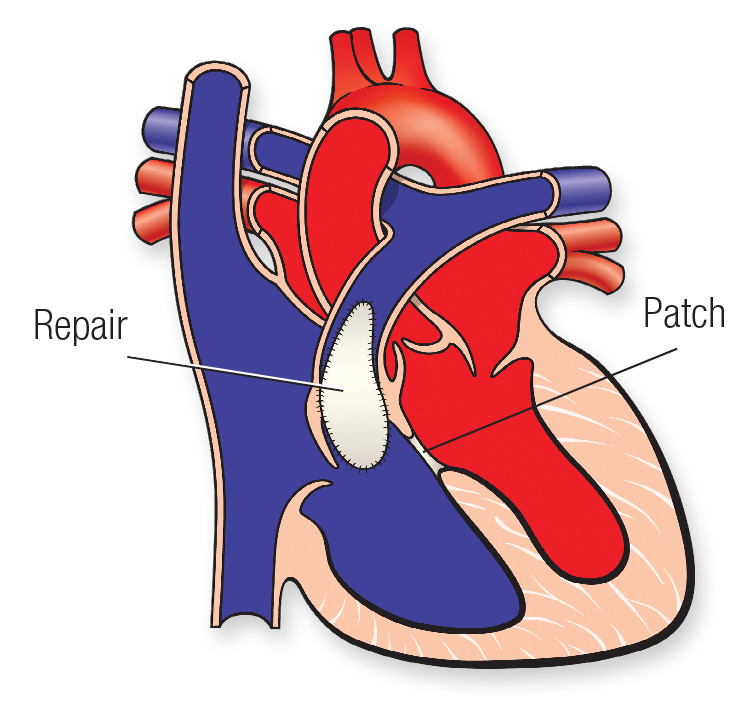
- Resect pulmonary stenosis
- Close VSD with patch (tilt slightly to the right so overriding aorta will be on the left side)
Drugs:
- critically ill → PG
- hypoxic spells → vasopressor + systemic-pulmonary shunt(=palliative treatment in r-l-shunt ) 📷
{kind=link}
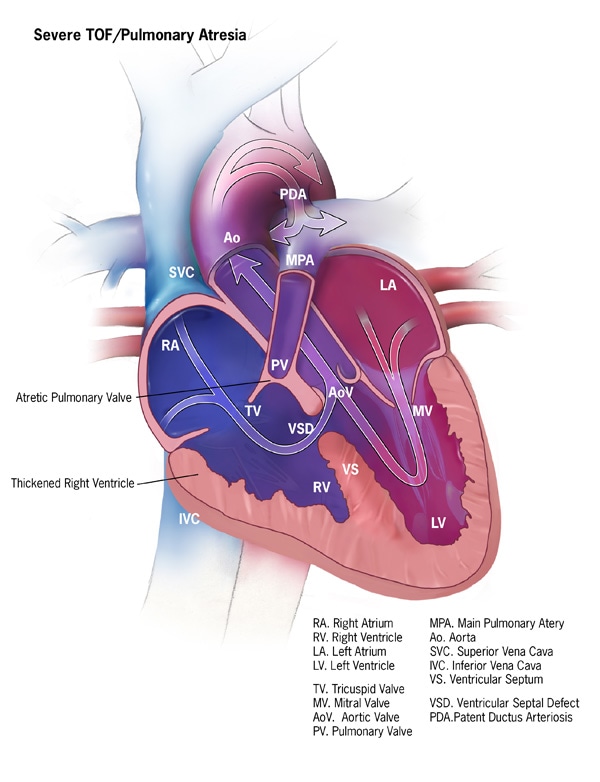
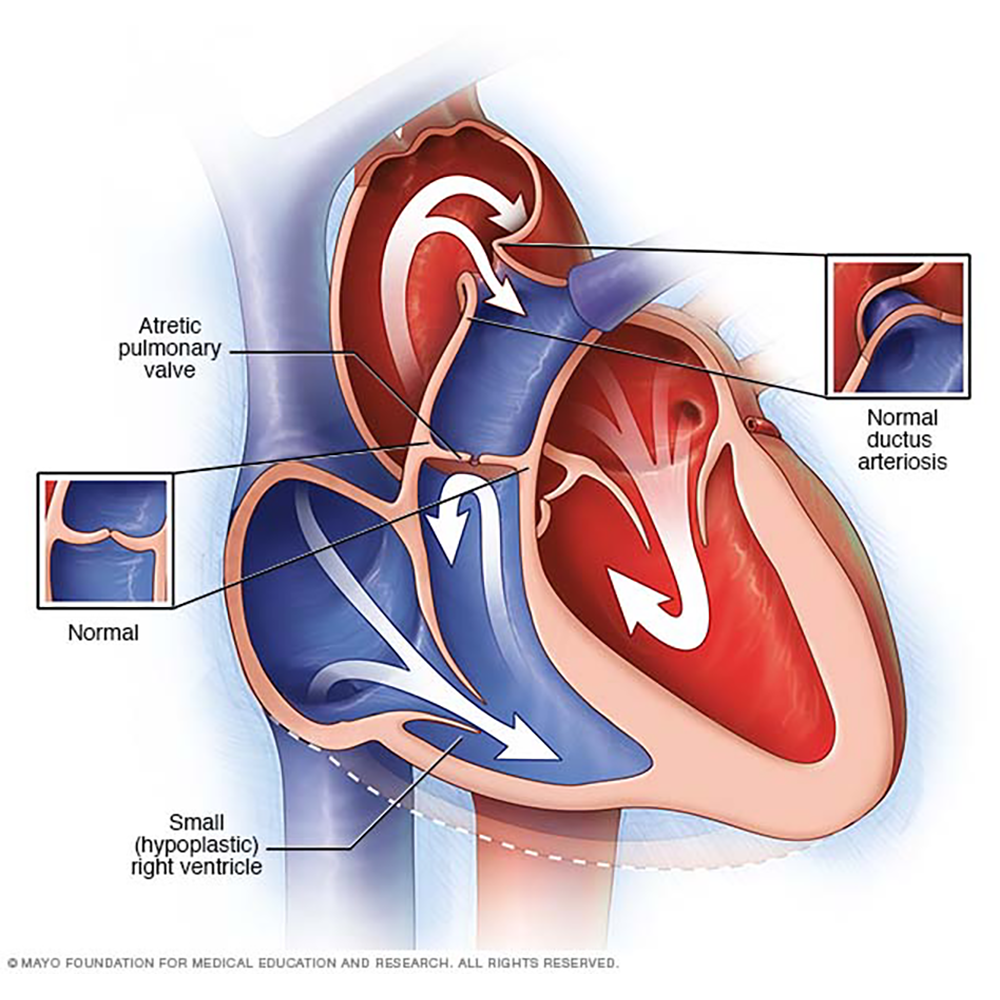
Same as Tetralogy of Fallot but instead of pulmonary stenosis
⇒ pulmonary atresia

→ blood supply to the lungs by PDA
angigraphy + cathetherization
CT
biventricular repair:
- pulmonary valvotomy (cut into Pulmonary valve)
- right ventricular outflow tract reconstruction
- patch the septal defect
PGE1
{kind=link}
{kind=link}
{kind=link}
Aorta connected to right ventricle
pulmonary artery connected to left ventricle
⇒ oxygenated blood recirculates in the lung
⇒ unoxygenated blood recirculated in system
→ patient only survives if PDA, ASD or VSD
first weeks of life (otherwise RIP ☠️)
- PGE1
- if ASD not large enough → enlarge it: balloon arterial septostomy
- Arterial switch operation: cut both arteries + reverse distal ends + moves coronary arteries from the left root of the aorta to the root of the pulmonary artery which is now connected to the aorta 📷
{kind=link}
{kind=link}
{kind=link}
- Type I: short pulmonary trunk, gives rise to both pulmonary arteries
- Type II: Both pulmonary arteries arise separately close to one another from the truncus arteriosus.
- Type III: Both pulmonary arteries arise separately at some distance from one another from the truncus arteriosus.
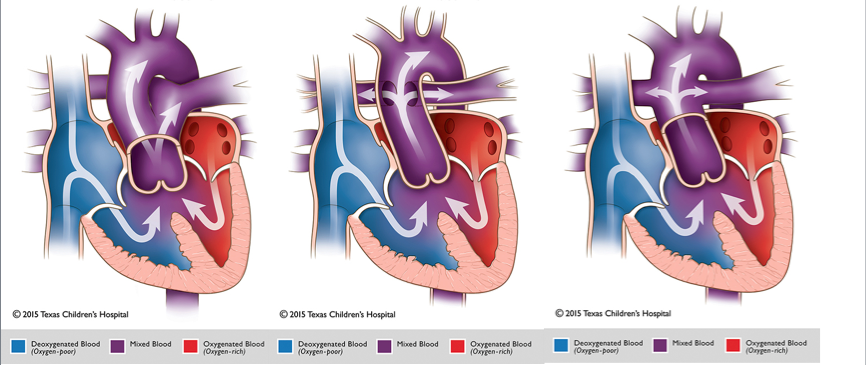
first 2 month of life (otherwise already untreatable pulmonary HT)
- Cut pulmonary arteries from aorta → leave common valve as aortic valve
- Homograft/or conduit-containing valve (=Rastelli procedure) from pulmonary arteries to RV 📷
- VSD close
{kind=link}
- Absent triscupid v. → no communication RA + RV
- hypoplastic right ventricle
- with VSD, ASD, PDA
- cyanosis (degree depending on VSD size)
- signs of diminished cardiac output (↓Ejection fraction, Hypotension, hypoxia)
- shock if obstruction to systemic blood flow
- PGE1
- atrial septostomy if communication is too small
- "Fontan" type circulation → anastomosis SVC + right pulmonary artery (later also IVC connected) 📷
{kind=link}
everything hypoplastic on the left side
hypoplastic aorta, aortic valve, left ventricle, mitral valve, left atrium
{kind=link}
{kind=link}
pulmonary veins do not connect normally to the left atrium. → drain into resorvoir in SVC or ICV → to the right atrium
communication via ASD → left atrium
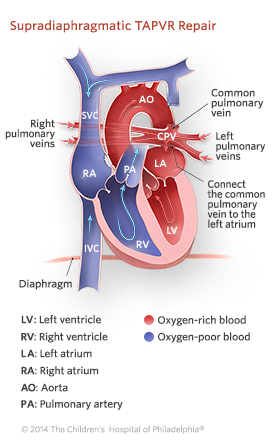{kind=link}
- Connect the resorvoir to left atrium (by anastomosis)
- Ligate communication to SVC/IVC
- Close ASD patch
The goal of surgery is to redirect pulmonary vein flow entirely to the left atrium. In patients with a supracardiac or infracardiac connection, the common pulmonary vein is opened wide and connected side to side to the left atrium. The foramen ovale is closed, and the ascending or descending vein is usually ligated. In a cardiac connection (to right atrium or coronary sinus), the atrial septum is resected partially and a new septum is surgically created, directing pulmonary veins to the left atrium
{kind=link}
{kind=link}