
Table of content
- Diabetology
- ⛲ Basics
- 🍬 Diabetes Mellitus
- 🐡 Non-diabetic Hypoglycemia
- 🐷 Metabolic Syndrome, Obesity & Nutrition
- 🧈 Dyslipidemias
- 🧶 Hyperuricemia
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Diabetology
⛲ Basics
Non-communicable diseases
Disease that is:
- non-transmittable
- multifactorial
⇒ i.e. cancer
"Non-communicable diseases is a diseases, caused due to multiple causes and are not passed or transmitted directly or indirectly from person to another by any agency" E.g: Cancer etc "Non-communicable diseases (NCDs), is a diseases which are not passed from person to another" E.g: Cancer etc
- CV-D
- DM
- COPD
- Cancer
Risk factors:
smoking, faules schwein, harmful drinking, excess salt + general unhealthy diet
→ HT, Overweight/obesity, Hyperglycemia, Hyperlipemia
- dont smoke
- dont eat shit
- sport
- dont drink (too much) alc
- Effective interventions targeting shared risk factors can largely prevent chronic diseases, including heart disease, stroke, type 2 diabetes, and cancer.
- Eliminating the major risk factors could prevent approximately 75% of heart disease, stroke, and type 2 diabetes, as well as 40% of cancer.
- Shared risk factors that should be addressed include tobacco use, unhealthy diet, physical inactivity, and harmful use of alcohol.
- Diabetes mellitus
- Obesity
- Dyslipidemia
- Metabolic Syndrome
Multifactorial cause:
Environmental factors (smoking, unhealthy diet), sedentary lifestyle, genetic, stress
- individual: decr. lifeexpectancy + quality
- epidemiologic: obesity, diabetes + CV-D epidemic
- economic, social: incr. costs, decr. productivity + incr. discrimination
screening! → early detection
symptoms occur when chronic complications already present
CV Risk
- Hyperglycemia
- HBP
- Dyslipidemia
- Smoking
- hypercaloric diet (+other unhealthy diet)
- sedentary lifestyle
- excessive alcohol consumption
- male gender
- age >45 in men, >55 in women
- family history of premature CV diseases <55 men, <65 women
T1DM without end-organ damage, patients with end-oran damage are already at high risk
score chart 📷 = risk of fatal CVD
🍬 Diabetes Mellitus
defect of insulin secretion and/or insulin action
→ chronic hypergylcemia w/ disturbances in fat, carbohy, prot metabolism
→ microvascular → retinopathy, nephropathy, neuropathy
→ macrovascular → CV, cerebrovascular, PAD
<110 mg/dl
<140 mg/dl
Basal: > 126 mg/dl
2h OGTT > 200 mg/dl
Random > 200 mg/dl
Fasing plasma gluc < 126 mg/dl
AND
OGTT between 140 - 200 mg/dl
>6,5% → diabetes
6-6,5% → prediabetes - increased risk,prevention important!
- DM yes/no
- What Type
- Micro and macrovascular complications
- comorbidities
- CV risk
- 4-P→ Polydypsia, Polyuria, Polyphagia, poundloss
- weight loss
- weakness
- irritability
- ketoacidosis → nausea+vomiting
- dehydration
- fruity breath - Kussmaul
- nausea, vomiting, abdominal pain
- altered neurological state, coma
explanation later
- C-peptide
- Auto-ABs
- plasma glucose levels (fasting, postprandial, noctural)
- HbA1c
Additionally:
- Crea + Albuminuria/ Proteinuria
- Lipidprofile
- Full blood count
- thyroid hormones
- other autoimmune disease marker!
inflammatory! (adipokines)
- C Reactive Protein
- Fibrinogen level
- Liver enzymes: aminotransferases, gamma-GT
- Uric acid
- prior meal + snack
- prior to exercise
- when low Gluc is suspected + after treating low Gluc
- prior to critical task (driving etc.)
⇒ 📷
Type 1:
After initial presentation, honeymoon period often occurs where glycemic control can be achieved with little or no insulin treatment (residual cells still able to produce insulin). Once these cells destroyed→ complete insulin deficiency
Type 2:
Early on, glucose tolerance remains normal despite insulin resistance (B cells compensate with increased insulin production) with time: Insulin resistance and compensatory hyperinsulinism continue ⇒ cells are unable to maintain the hyperinsulinemic state which results in glucose intolerance and DM
Type 1:
Insulin
Type 2:
- Lifestyle modification
- Non-insulin anti-hyperglycemic agents → metformin should be the initial antihyperglycemic agent of choice. Additional agents to be selected on the basis of clinically relevant issues, such as glucose lowering effectiveness, risk of hypoglycemia, and effect on body weight
- Insulin therapy
Type 1: DKA if severe
Type 2: HHS, DKA if severe
- increased risk for spontaneous abortion and congenital malformations
- Macrosomia (big boiii 👶🏼)
- overweight/obese
- mother >35y
- multiparity (also prior signs of GD → macrosomia, fetal mortality)
- history of IFG or IGT
- excessive weight gain (during first 6month of pregnancy)
- PCOS
high risk before week 24 → negative → repeat week 24-28
moderate risk → week 24-28
- DM in pregnancy
- Gestational DM
Random Gluc >200 → check FPG or A1C → if FPG>126 or A1C>6.5% = diabetes mellitus in pregnancy
ONE of:
fasting >92
1h plasma gluc > 180
2h plasma gluc > 153
during pregnancy weeks 24-28
- Proinsulin consists of two chains, A and B, which are connected by a polypeptide called C-peptide. 📷
- Insulin is activated upon the release of C-peptide during secretion. 📷
- C-peptide is an indicator of endogenous insulin secretion and is produced in equimolar amounts with insulin.
- C-peptide has a lower clearance than insulin.
GLUT-2
>90 mg/dl
- Activation of glucosensor at PG > 90mg/dl
- Closure of ATP-dependent K+ channels
- Opening of voltage-dependent Ca++ channels
- Depolarization
- Insulin secretion is initiated by the transport of glucose into pancreatic cells via glucose transporters GLUT2.
- Glucose is then phosphorylated and converted into glucose-6-phosphate through glycolysis, which inhibits ATP-dependent K+ channels.
- Inhibition of ATP-dependent K+ channels leads to membrane depolarization and the opening of calcium channels.
- Calcium influx stimulates insulin secretion.
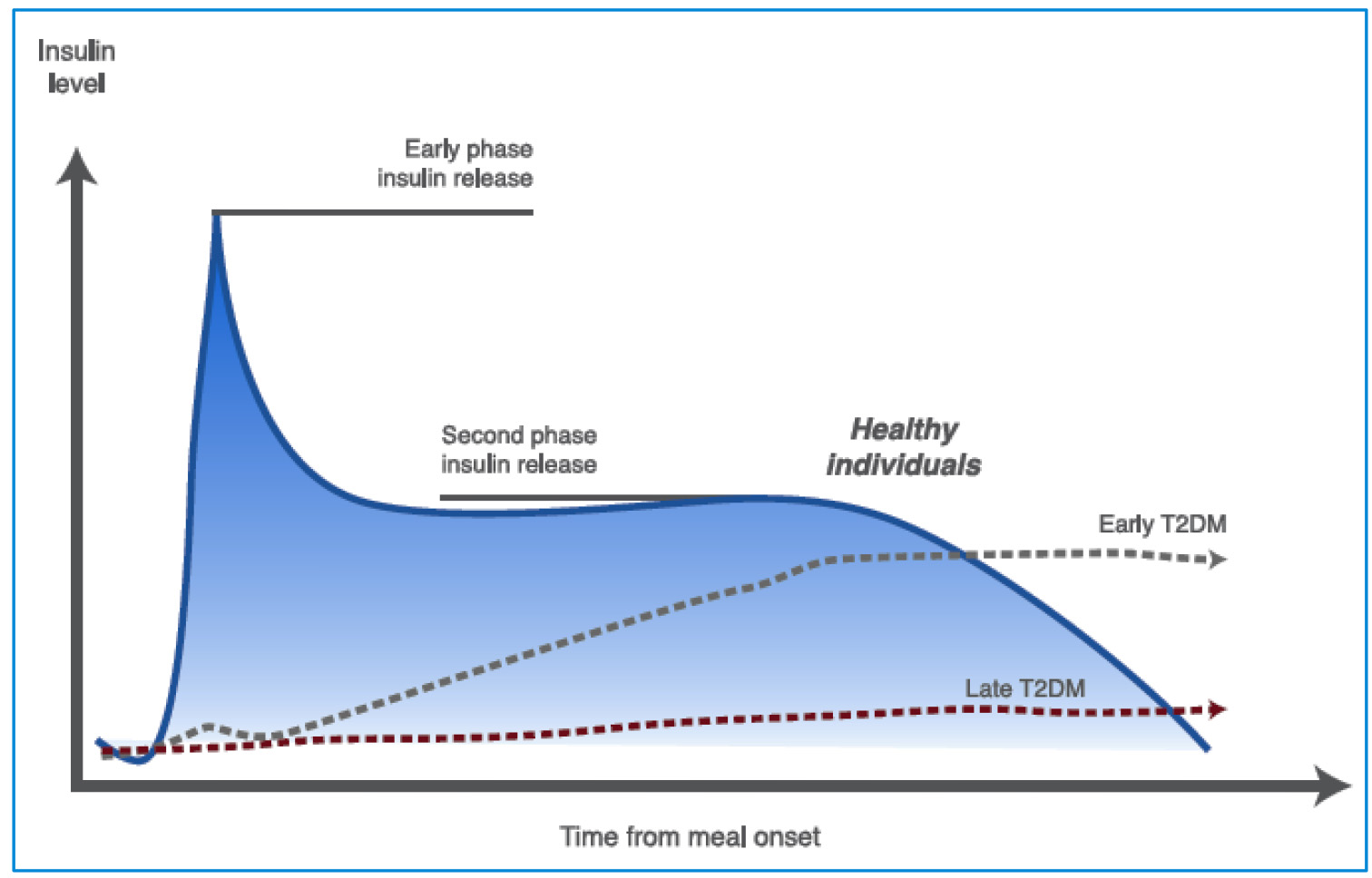
- Normal insulin secretion:
- Very rapid first-phase insulin secretion
- Lower, sustained rate of insulin secretion that stops abruptly at the end of glucose infusion
- Impaired glucose tolerance:
- Loss of first-phase insulin secretion
- Much higher rate of insulin secretion than in a normal person, which persists after glucose infusion has ended
- Overall, insulin resistance is much higher in impaired glucose tolerance.
ANABOLIC
- GLUT-4 activation→ Glucose uptake+ glucose oxidation
- glycogen synthesis
- lipogenesis+antilipolytic
- amino acid uptake + protein synthesis
- anti-apoptotic effect
- DNA synthesis
- Islet cell autoantibodies (ICA)
- insulin autoantibodies (IAA)
- glutamic acid decarbocylase ABs (GAD65)
- thyrosine phosphatases IA2 + IA2beta
- viral infection
- Cow's milk antibodies
- Environment?Pollution?
no, but the risk is increased
Risk of DM type 1 in offspring:
- Maternal T1DM: 2-3%
- Paternal TIDM: 5-6%
- Both parents with T1DM: 30%
genetic predisposition + triggering factors → progress. beta-cell destruction → ABSOLUTE insulin deficiency
OBESITY →
- Insulinresistance→ increased hepatic glucose production, decreased muscular+adipocyte uptake
- beta-cell dysfunction→ can't keep up with the IR→ decreased secretion due to depletion
- genetic susceptibility, obesity, sedentary lifestyle
increased lipolysis and FFA flux due to hungrrrry cells 🍖 (cant get gluc into cells)
- increased hepatic glucose production because the cells are hungrrrrry
- decreased uptake of muscles and adipocytes
lipotoxicity, glucotoxicity→ beta cell dysfunction
absulute insulin deficiency DM1
gluc cant get into cell → no energy → incr. in ketonbodies instead
LACK OF INSULIN OR STRESS
- interruption insulin treatment
- unadjusted insulin to CH intake
- 1st presentation (not diagnosed yet)
- Acute MI
- infection
- dehydration
- keton breath
- acidotic breath - Kussmal
- abdominal pain, nausea, vomiting
- altered mental state, coma
- ketonuria + plasma ketons
- fluid → i.v. NaCl (when Gluc low enough around 200 → switch to i.v. dextrose/gluc 5%)
- K-correction → in low K no insulin only fluids!!! when corrected or high K → insulin + fluid
- insulin (regular): 0.1U/kg bolus initally → than infusion 0.1U/kg/h
- Bicarbonate in severe acidosis (ph<7)
- Treatment of specific etiology
- Hyperglycemia (impaired uptake, incr. gluconeogenesis+glycogenolysis) → polyuria, water+electroly loss, polydipsia
- Incr. lipolysis → incr. FFA in blood → hepatic ketogenesis → ketonuria + pulmonary excretion
- Potassion depletion → incr. catabolism due to proteinolysis
relative insulin defic. DM2
often precipitated by stress (MI, spesis, stroke, drugs, trauma)
- hyperglycemia (750)
- Severe dehydration → Hypotension, tachycardia, dry skin
- Polyuria + Polydypsia
- Progressive alteration conciousness + coma
- pH + ketonbodies in acidosis in ketoacidosis (high anion gap)
- high osmolarity + extremely incr Gluc in HHS
same as DKA but without bicarbonate 📷
- fluid→ i.v. NaCl (when Gluc low enough <300 → switch to i.v. dextrose/gluc 5%)
- K → no insulin when HypoK!
- insulin
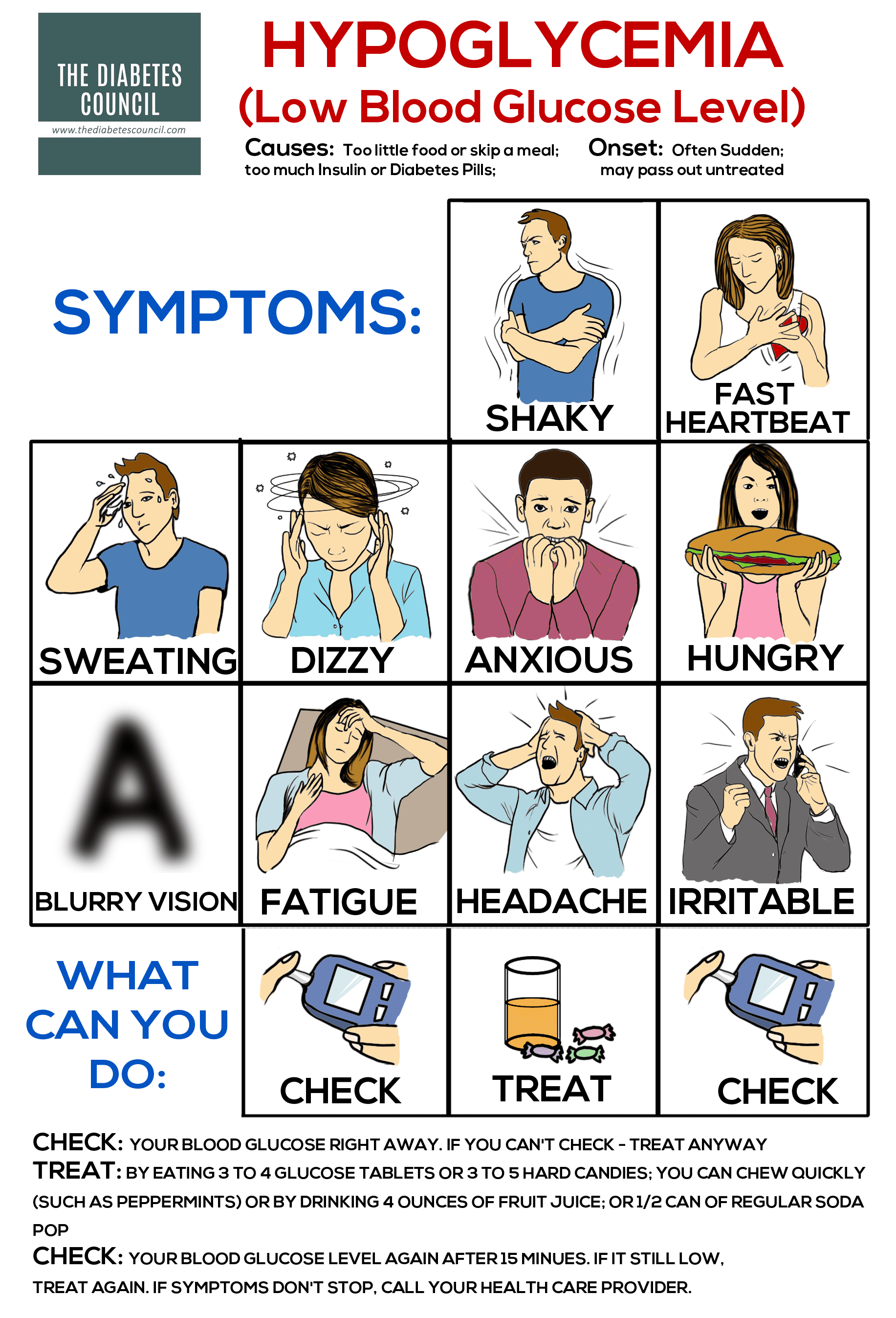
<70
- Symptoms of hypoglycemia (Confusion, Irritation, Stupor, Mood alternation, Syncope)
- Low blood glucose values (<70 mg/dl)
- Resolution of symptoms after glucose intake
- Autonomic Alarm symptoms → due to catecholamines
- neuroglycopenic symptoms
- others
Autonomic symptoms | Neuro symptoms | Other symptoms |
Sweating | Dizziness | Hunger |
Trembling | Drowsiness | Blurred vision |
Tachycardia | Confusion | |
Nausea | Personality changes | |
Difficulty speaking | ||
Weakness | ||
Headache | ||
Impaired judgement | ||
Seizures | ||
Coma |
- too much insulin
- physical activity
- impaired gluconeogenesis (alcohol)
- rapidly absorbed carbohydrates (juice)
- glucose i.v.
- glucagon (subcutaneos or intranasal)
- Level: Alert-value: Gluc 54-70; pat can recognize the symptoms + can solve them by himself
- Level: Clinically signif. <54 → pat. still concious but might ask for help from another person
- Level: Severe → Person cant react (sev. cognitive impairment)
Condition | Hyperglycemic Coma | Hypoglycemic Coma |
Case History | Gradual onset over several days | Swift onset within minutes |
Anteceded by excessive urination and increased thirst (polyuria-polydipsia) | Anteceded by autonomic and neuroglycopenic manifestations | |
Physical Examination | Dehydrated epidermis | Perspiration |
Lowered blood pressure | Elevated heart rate (tachycardia) | |
Respiratory difficulty (Kussmaul respiration) | Elevated systolic blood pressure | |
Presence of acetone in breath | Convulsions | |
Deep coma, yet undisturbed | Coma with restlessness |
- Microvascular complications ("specific"):
- diabetic retinopathy
- diabetic nephopathy
- diabetic neuropathy
- Macrovascular complications:
- chronic heart disease
- cerebrovascular disease
- peripheral artery disease
- Mixed complications:
- diabetic foot
- erectile dysfunction
- Others
- hyperglycemia
- dyslipidemia
- HT
- obesity + metabolic syndr.
- insulin resistance
- incr FFA
- oxidative stress
- glycosylation of arteries
⇒ endothelial dysfunction
⇒ vasoconstriction, inflammation, thrombosis
⇒ atherogenesis → macro + microangiopathy
- genetic
- age
- personal history
- lifestyle → diet, smoking, sedentary, psychosocial stress, depression
dg. of exclusion!
peripheral neuropathy in the setting of DM without other causes
peripheral → motor + sensory
autonomic
Neuropathy Type | Presentation |
Peripheral Sensory Neuropathy | Sensation alterations (paresthesias) like tingling or itching, neuropathic pain, radicular pain, and sensory loss manifesting as numbness or reduced tactile perception. These symptoms are bilateral, symmetric, and often include diminished perception of vibration and pain/temperature, primarily in the lower limbs but can also affect the hands. There may be a reduction in ankle reflexes. Entrapment syndromes, such as carpal tunnel, may be the initial manifestation, potentially leading to neuropathic ulceration of the foot. |
Motor Neuropathy | Characterized by less frequency compared to sensory neuropathy, there is delayed motor nerve conduction and muscle weakness or atrophy. It may affect a single nerve trunk (mononeuropathy) or multiple (mononeuritis multiplex). Some motor neuropathies may resolve spontaneously within 6 to 8 weeks. Conditions include reversible cranial neuropathies such as III (ptosis/ophthalmoplegia, pupil sparing), VI (abducens paralysis), and VII (Bell's palsy). Diabetic amyotrophy is associated with pain, weakness, and wasting of hip flexors or extensors. |
Autonomic Neuropathy | Presents with postural hypotension, increased heart rate (tachycardia), and a decreased cardiovascular response to the Valsalva maneuver. Gastrointestinal manifestations include gastroparesis, alternating diarrhea and constipation. Urogenital complications encompass urinary retention and erectile dysfunction. |
Clinical features of autonomic neuropathy
- Cardiovascular Resting tachycardia Orthostatic hypotension Silent myocardial ischemia, congestive heart failure and sudden death
- Gastrointestinal Gastroparesis Diarrhea, Constipation
- Genitourinary Bladder dysfunction Erectile dysfunction Sexual dysfunction in women
- Sudomotor dysfunction Hypohidrosis / distal anhidrosis
- Pupil abnormalities
- hypoglycemia unawareness, lack of reaction to hypoglycemia
Stage 0/1: No clinical neuropathy
- No signs or symptoms
Stage 2: Chronic painful neuropathy
- Burning / tingling pain
- Decreased / absence of sensitivity
- Decreased / absence of osteotendinous reflexes
Acute painful neuropathy
- Diffuse pain, including in the trunk
- Hyperesthesia
- No signs on examination of the peripheral nervous system
Painless neuropathy with decreased / no sensitivity
- Absence of symptoms or numbness
- Painless lesions
- Reduction / absence of sensitivity and reflexes
Stage 3: Late complications of clinical neuropathy
- Leg ulcers
- Neuropathic deformities (Charcot osteoarthropathy)
- Non-traumatic amputations of the lower limbs
Charcot osteoarthopathy = fracture of foot bones without pain
oxidative stress
hyperglycemia → ↑ROS & impaired antioxidant defenses → oxidative stress → vascular & neuro dysfunction/degeneration
every year
5years after dg in DM1
→ for both polyneuropathy + autonomic
- sensory
- reflex
- motor strenght
- Monofilament screening
- vibration (tuning fork)
- nerve conduction measurements (EMG, etc.)
⇒ Toronto-Score:
- glycemic control
- pain-killers
- surgery of the ulcers
- special shoes
- drugs for GI symptoms + erectile dysfunction
In diabetology, treatment and management strategies include tight glycemic control, medications for neuropathic pain syndromes, foot care education, interventions for orthostatic hypotension, treatment for gastroparesis, and options for erectile dysfunction.
besides neuropathy also macro+ microangiopathy contribute to the formation
Neuropathy + Feet deformity → Foot at risk + Trauma → Foot ulcers (+infections)
- hard excudate
- macular edema
- hermorrhage (dot+blot)
nonproliferative → microaneurysm, dot+blot + leakage + retinal ischemia
proliferative: ischemia → neovascularization → vitreous hemorrhage → RD + Neovascular glaucoma
- gylcemic, HT, lipid control
- laser therapy, Anti-VEGF
- Optimal glycemic control (delays onset, decreases progression), lipid management, blood pressure controlsmoking cessation
- Annual follow-up visits with an optometrist or ophthalmologist examination through dilated pupils regardless of symptoms
- The frequency of follow-up should be adjusted based on the severity of retinopathy
albuminuria and in the end CKD
III → microalbuminuria (30-300mg/24h)
IV → albuminuria (>300mg/24h)
V → CKD → Progressive decline in renal function
Stage | Diagnosis | Characteristics |
I & II | Subclinical | Normal albumin excretion rate; |
III | Incipient DN | Albuminuria 30-300mg/24h or 20-200mg/l |
IV | Overt DN | Albuminuria >300mg/24h or >200mg/l |
V | DN + CKD | Progressive decline in renal function |
Normal albumin excretion rate « 30mg / 24h or < 20mg/l
→ Albuminuria
→ nephrotic sediment
→ Electrolyte abnormalities
→ Abnormalities identified by histology or imaging
→ GFR <60
KDIGO 2012 📷
According to GFR + ALbuminuia
Cardiovascular, PAD, Cerebrovascular
macrovascular + microvascular, lesion of myocardium + autonomic neuropathy (heart)
- lifestyle (diet, alcohol, smoking, sedentary)
- HT
- Dyslipidemia
- Poor glycemic control
- abdominal obesity
- metablic synd., insulin resistance
- albuminuria
- afib
- Depression
- Alzheimer
- HT
- Dylipidemia
- UTI
- Obesity + Metabolic syndrome
- Hyperuricemia
around 6,5%/<7%
80-130 mg/dl
< 145 mg/dl
<140/80mmHg → 130/80mmHg would be noice
<175 mg/dl
<100 mg/dl
<55 mg/dl
cLDL= TG- HDL- (TG/5) (in mg/dl)
<150 mg/dl
females→ >40mg/dl
males→ >50 mg/dl
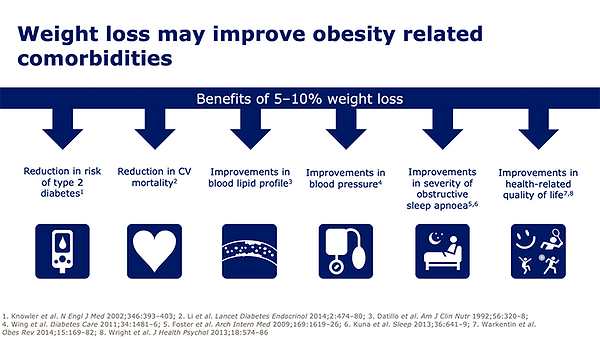
10-15% weight loss over the next 3-6 months
= complete clinical management of diabetic patient
- Therapy→ Lifestyle, Medication, Bariatric Surgery
- Education
- Monitoring
- Evaluation- annual
- healthy eating patterns→ nutrient dense foods in appropriate portion sizes
- address individual needs
- maintain pleasure of eating
20-25 kcal/kg/KG
Mediterranean 📷→ rich in monounsaturated fatty acids, omega-3 (fish)
sodium reduction <2,300 mg/day
saturated fat, cholesterol, trans-fat
Patient compliance→ Patient education is very important
psycho-social care
physical activity
children → 60min per day
Aduls → 150min / week
- Encourage children with diabetes or prediabetes to engage in at least 60 minutes of physical activity daily.
- Advise adults with diabetes to perform at least 150 minutes per week of moderate-intensity aerobic physical activity spread over 3 days with no more than 2 consecutive days without exercise.
- Encourage adults with type 2 diabetes to perform resistance training twice per week.
- low-glycemic Carbs should be eaten
- no artificial (free) sugar (<10% of total energy)
- no processed foods→ often with sugar
- high fiber→ Veggies
- low trans-fats and saturated fats
- high unsaturated, polyunsaturated fats→ fish, coconut oil, nuts, seeds
- omega-3
avoid carbohydrate sources high in protein
< 2.300 mg
- only moderate
- patient education→ delayed hypoglycemia
- attitude towards DM and Tx
- Depression assessment
- cognitive impairment in older patients
decreased mortality, better glycemic control, improved lipid profile, improved quality of life
10-15% in the first 3-6 months
- exercise
- diet
- obstetric surgery→ most superor glycemic control
- medication→ Glucosidase inhibitor

💊 Pharmacotherapy DM
- sc, iv
- Insulin pumps
Basal→ Long-Acting
prandial→ rapid-Acting
Glargine aka Lantus
Detemir aka Levemir
NPH (InsumanBasal, Humulin N)
regular
Human Insulin→ Insuman Rapid, Humulin Regular, Actrapid
Humalog, Apidra
Insuman Comb, Mixtard (+ all other with “mix” in the name)

Basal→ thigh
Rapid→ belly
- Fasting BG
- preprandial BG
- postprandial BG
- HbA1c
SMBG→ self monitoring blood gluc
CGM→ continuous monitoring
According to ADA Guidelines 2014, patients on MDI or insulin pump therapy should perform self-monitoring of blood glucose (SMBG) before meals, snacks, bedtime, exercise, when suspecting low blood glucose, after treating low blood glucose, and before critical tasks like driving.
- Preprandial: 95 mg/dL
- 1-h postmeal: 140 mg/dL
- 2-h postmeal: 120 mg/dL
- lifestyle (diet, physical activity)
- Drugs
- Basal Insulin + Bolus
- Metformin
- Gluc + US monitoring
- Implement dietary modifications and encourage regular exercise, such as walking.
- Ensure strict monitoring of blood glucose levels, with measurements conducted four times daily.
- Initiate insulin therapy if dietary modifications alone are insufficient to achieve glycemic control.
- Administer metformin and glyburide as alternative options for patients who refuse insulin therapy.
- Conduct regular ultrasound examinations to assess fetal development.
- Consider inducing delivery at weeks 39-40 in cases of poor glycemic control or the presence of complications.
- Anti-hyperglycemic medication:
- Oral medication
- Non-insulin injected medication
- Insulin
- Anti-hypertensive medication
- Lipid lowering medication: Statins, fenofibrate
- Aspirin
- Chronic complications medication
Metformin, 2g/day
SGLT-2 Inhibitors
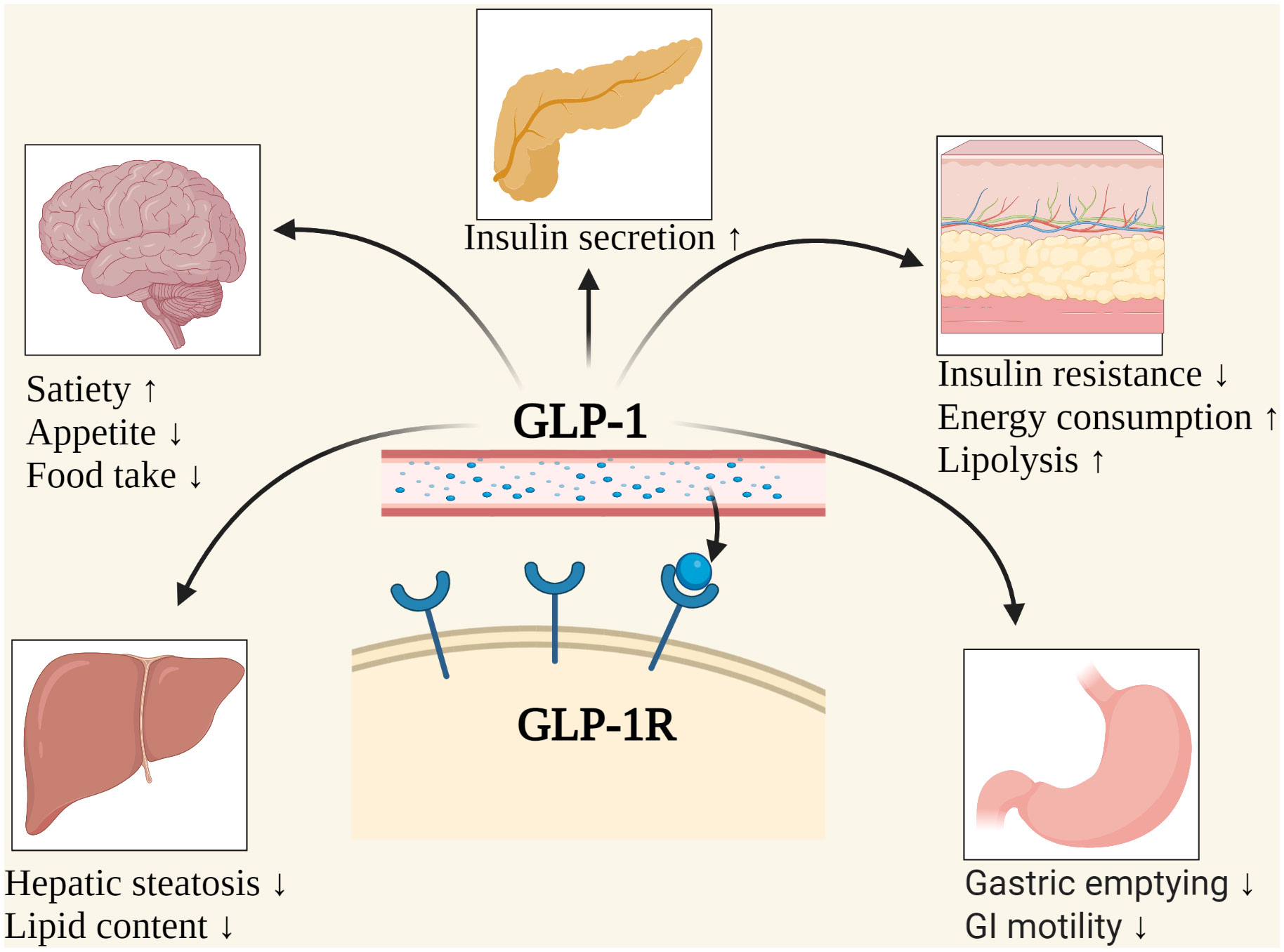
GLP-1 (incretin mimetic)
→ mechanism: see comment
Dapagliflozin
Empagliflozin
Canagliflozin
polyuria
phenomenon that oral glucose elicits a higher Insulin response than iv Glucose due to gut-derived GLP-1 in healthy individuals
- increases postprandial insulin release
- decreases glucagon release
- slows gastric emptying
- inhibits food intake
- increased insulin sensitivity
- decreased hepatic glucose production
- CARDIOPROTECTIVE
- Liraglutide
- Dulaglutide
- Semaglutide
Dipeptidyl peptidase 4, enzye which catabolyzes incretins (GLP-1)
inhibition of DDP4→ increased levels of GLP-1
- DPP-4 inhibitors increase insulin release and decrease glucagon levels in a glucose-dependent manner.
- Incretin levels are increased and prolonged by DPP-4 inhibitors.
- The effect of DPP-4 inhibitors on insulin release and glucagon levels is dependent on glucose.
- DPP-4 inhibitors have a glucose-dependent mechanism of action.
- DPP-4 inhibitors have a glucose-dependent effect on insulin and glucagon.

10 IU
4 IU
- Sulfonylureas (block K+ channels in beta cells → ↑insulin-secretion)
- Glinides (block K+ channels in beta cells (other binding position than sulfonylureas) → ↑insulin-secr)
- Glitasones (activate PPARy in nucelus of cells → incr. gluc uptake by cells)
- Alpha-glucosidase inhibitors (blocks carb-cleaving enzymes in small intestine → decr. post-prandial gluc)




- Statins
- Fibrates
- Omega-3
- PCSK-9 inhibitors
- secondary prevention → aspirin
below 190
below 150
cLDL= Cholesterol- LDL- (Triglycerides/5)
below 100
below 50
females: above 40
males: above 50
<130/80 mmHg
→ RAAS-inhibitors (ACEI or ARB)
🐡 Non-diabetic Hypoglycemia
- denutrition, malnutrition, eating disorders
- Endocrine diseases: Adrenal insuff., pituitary dysfunction, thyroid diseases
- renal failure
- hepatic failure
- severe infections
- extrapancreatic tumor
- Insulinoma
- stomach surgery
- hemodialysis
- sustained physical activity
- transient neonatal hypoglycemia - resolves in 3-5 days
- persistent (recurrent) hypoglycemia - doesnt resolve in 5-7 days
- biochem (high insulin+C-pep; low Gluc)
- Localization: CT, Octreoscan (scinti[labeled somatostatin analog], endoscopic or intraoperator US)
- mild-moderat: 15-20 mg carbohydrates
- severe→ iv glucose and/or glucagon
- Diazoxide (K+ channel blocker)→ 10-25 mg/kg/day
- Ocreotide (Somatostatin analog)→ 1-20 mcg/kg/day
- tumor removal
🐷 Metabolic Syndrome, Obesity & Nutrition
JUST READ THE LECTURE + SEE ABOVE:
- Lifestyle + Nutrition
Mediteranean diet 📷
A food is considered functional if it positively affects one or more specific bodily functions, going beyond basic nutritional benefits, and is relevant to improving health, well-being, and disease risk reduction.
Diabetology focuses on the health benefits of live microorganisms, such as lactic acid bacteria and bifidobacteria, which can lower cholesterol and blood pressure, improve immune function, prevent infections and colon cancer, reduce allergies and inflammation. Yoghurt consumption can also improve mineral absorption, help with irritable bowel syndrome and colitis, prevent gastrointestinal infections, and reduce oxidative stress.
Fibers → ↑ activity of intestinal flora
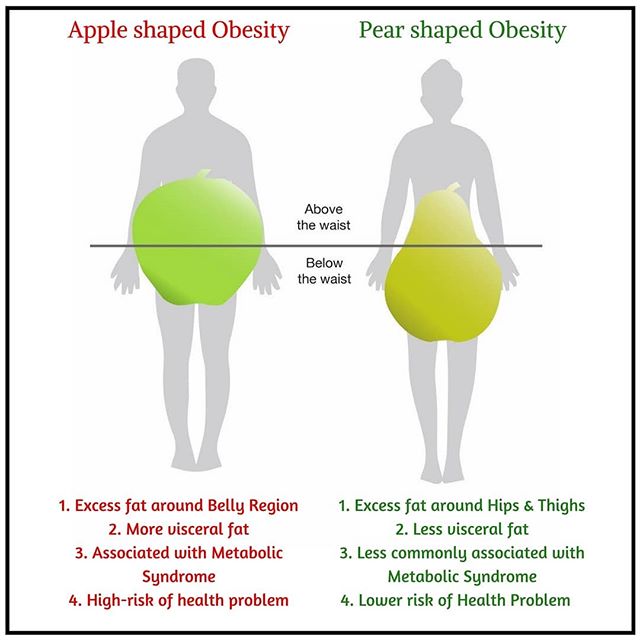
- abdominal obesity
- aterogenic dyslipidemia (high TG, low HDL)
- Gluc intol + insulin resistance
- HT
- Prothrombitic + proinflammatory state
- endothelial dysfunction
- Non-alcoholic fatty liver disease (NAFLD)
- Albuminuria
woman> 80 cm, men > 94 cm
>130/85 mmHg
>150 mg/dl
male < 40mg/dl
female < 50mg/dl
>100 mg/dl
at least 3
- Lifestyle optimization (diet+physical activity)
- weight loss and maintenance
- BP control
- lipids control
- DM2 prevention
excessive fat accumulation
men >25% and
woman >30% Body fat
- BMI calculation: BMI = Weight (kg) / Height (m^2)
18,5-24.9
25-29,9
30-34,9
35-39,9
>40
- abdominal (”male”)
- gluteo-femural (”female”)
⇒ 📷
polygenic factors (group of genes) → incr. susceptibility of weight gain
- adipose tissue distribution+accumulation
- BMR determination and its response to physical activity
- caloric intake+food selection
FTO gene (fat mass and obesity associated genes)
- Prader-Willi Syndrome
- Bardet-Biedl Syndrome
- Leptin deficiency/ Resistance
- adipocytes
- enterocytes (small intestine)
arcuate nucleus of hypothalamus → inhibit hunger → diminishes fat storage in adipocytes
Leptin resistance
- genetic
- metabolic (energy intake>expenditure)
- behavioural
- environmental
resetting of the body weight ''set point'' at an increased value
- Thyroxin
- Cortisol
- Ghrelin
- Leptin
- Insulin
- GLP-1
- (PYY, Amylin, ,CCK)
- metabolic syndrome
- T2DM
- Dyslipidemia
- Hypertension
all these above → CHD + CV-disease
- NAFLD
- PCOS
- female and male hypogonadism
- Gallbladder disease
- Gout
- CKD
- obstructive sleep apnea
- obesity hypoventilation Sdr.
- Asthma
- Osteoarthritis
- GERRRRD
- Immobility
B"ECKE"
- colon
- kidney
- esophagus
- endometrium
- (postmenopausal breast)
- Antropometry→ weight, BMI, waist circumference etc.
- Lifestyle
- Biochemistry
- CV
- Co-morbidity (see questions before)
- Psycho-emotional
- Therapy→ lifestyle, behavioral, pharma
- Education
- Monitoring
- Evaluation
- Increased metabolic efficiency
- Changes in neuroendocrine signaling (e.g., reduced satiety signaling)
- Changes in neural responsivity to food cues (e.g., heightened reward-related or diminished inhibitory anticipatory responsivity)
- Changes in neural responsivity to food intake (e.g., decreased consummatory reward through habituation to the rewarding aspects of palatable food)
low-caloric diet
with an energy deficit of over 500 kcal/ day
(generally reduce carbs, fat, low-fibers + prefer low energy density food)
- avoid snacking and skipping of meals
- eat only in response to the hunger feeling
- eat slowly
- eat mindfully
- keep a food-diary
- exercise
BMI > 27 plus comorbidities or
BMI >30
- Gastric lipases inhibitors (Orlistat)
- Opioid antagonists→ Naltrexone
- GLP-1 agonist→ Liraglutide
- increase BMR→ Norepinephrine releasing agents (Phentemine)
🧈 Dyslipidemias
- Hyperlipidemia→ elevated Cholesterol and/or Triglycerides
- Dyslipidemia→ Hyperlipidemia plus decreased HDL
cLDL= Cholesterol- HDL- TG/5

if TG >400 mg/dl
HDL→ brings to liver ''good''
LDL→ brings to tissue and arteris ''bad''
=Protein component of lipoproteins
- structural→ ensures stability
- functional→ binding to receptors
"B stands for bad"
Apo-B→ main protein of LDL
Apo-A→ main protein of HDL
- Chol <190
- TG<150
- HDL male >40 female >50
- LDL <100
- genetic
- aggravated by lifestyle factors
mutation in gene coding LDL receptor
high CVR!!!! 20 fold increased risk of MI in men
- mild to moderate: 150-880 mg/dl
- severe: >880 mg/dl
- TG >500
- lipaema retinalis, eruptive xanthomas, hepatosplenomegaly
- increased risk for pancreatitis
- alcohol
- DM
- RF
- Hypercholesterolemia >300 mg/dl
- Hypertriglyceridemia >500 mg/dl
- palms and elbow xanthomas
- hypothyroidism
- obesity, metabolic syndrome
- diabetes
↑ TGs
normal or ↑ LDL
↓ HDL
- metabolic syndrome, DM2
- Insulin resistance
- Pt. with high to very high CV risk (CVD, DM, CKD, Chromic Inflamm, Hypertension)
xanthoma, xanthelasma, arcus cornealis
- age: males >40 females >50
- relatives of patients with severe forms of dyslipidemias and/ or premature CVD
(note: LDL is the primary goal in CVD prevention)
very high <55mg/dl
high <70 mg/dl
moderate <100 mg/dl
low <116 mg/dl
no smoking, diet, physical activity, body weight, blood pressure, DM-control, decr. alcohol
→ all have a pos. effect on lipid profile
- monounsaturated fats→ olive oil, avocado, nuts, egg yolk
- polyunsaturated fats→ vegetable and seed oils, linseeds, 🐟
- saturated→ animal fat butter, cream lard, coconut oil
- trans fats→ refined shizzle
- consume low-fat milk
- avoid salad dressings
- low-fat yogurt
- olive oil instead of butter
- bake,boil, steam veggies
- no excessive fast food
- cut visible fat of the meat
- consume less meat
- decrease total cholesterol, LDL, TG
- prevent plaques in arteries
- lower BP
- lowers risk for arrhythmia
statins
Mechnism: inhibition of HMG-CoA reductase→ lowers cholesterol de-novo synthesis→ higher cholesterol uptake by the liver by incr. LDL-R expression on hepatocytes
→ titration to max. tolerated dose
Ezetimibe
Mechanism: inhibits intestinal uptake of fat without lowering fat-soluble vitamin uptake
10 mg/day
→ can also be given as monotherapy if statins not tolerated
PCSK-9 inPCKShibitors
⇒ Evolocumab + Alirocumab
- Mechanism:
normal action PCSK-9 → inactivates LDL receptor on hepatocytes → less LDL into liver, more remain in blood
MABs→ inhibit PCSK-9 → decreased LDL-receptor breakdown
>880 mg/dl→ fibrates
>200 mg/dl
statins as first-line treatment
if LDL is within target: add Fenofibrate
🧶 Hyperuricemia

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
femals: <6
males: <7
70% via kidney
30% via intestines
patients with acidosis (i.e. diabetic ketoacidosis) → decr. tubular secretion
metabolic syndrome
- diuretic therapy
- diabetes insipidus
- CVD
- Obesity
- kidney failure (GFR <20)
- Hypertension
- Hypothyroidism
- Hyperparathyroidism
- tumor lysis syndrome
- preeclampsia,eclampsia
- gout→ monoarthritis, gouty tophy 📷
- urolithiasis→ flank pain, hematuria, nausea, vomiting
- patients with family history
- patients with DMT2, High BP, Obesity, Dyslipidemia
urea comes from protein catabolism (nitrogenous waste product)
uric acid→ purine metabolism
- uric acid
- CBC (malignancy, hemolysis, lead poisoning)
- electrolytes, urea, serum creatinine (abnormal in acidosis or renal diseases)
- Liver function tests (malignancy or metabolic disorder)
- Glycemia (DM)
- Lipid profile (dyslipidemia)
- Calcium and phosphate levels (hyperparathyroidism, sarcoidosis, myeloma, renal disease)
- TSH (hypothyroidism)
lifestyle
avoid meats poultry, fish, seafood, alcohol
NSAIDS, intra-articular Glucocorticoids
Colchicine
+lifestyle as in asymptomatic
- Probenecid→ increases excretion
- Allopurinol→ Xanthine oxidase inhibitor → inhibit production of uric acid
- prophylactic colchicine (acute lowering can precipitate an acute gout attack)
- +lifestyle
- allopurinol
- increase urin pH→ Potassium citrate, Sodium Bicarbonate
- adequate hydration
- +lifestyle