
Table of content
- Orthopedics
- ⛲ Basics of osteoarticular traumatology
- 🤸🏽♀️Shoulder girdle injuries
- 🦾 Humerus fractures
- 💪🏽 Elbow and forearm injuries
- 🗼Spine injuries
- 🥣 Pelvic injuries
- 🦿Femur fractures
- 🧎🏽♂️Knee and distal lower limb injuries
- 👵🏽 Osteoarthritis and bone tumors
- 👶🏽 Pediatric Orthopedics
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6

Orthopedics
⛲ Basics of osteoarticular traumatology
break in the continuity of a bone → partial or complete
A sprain is an injury of ligaments without a permanent loss of the normal relationships in the joint.
A dislocation is an injury of ligaments with a permanent loss of the normal relationships in the joint. 📷
trauma, stress fracture, pathological fracture
- Direct trauma (e.g., an ulnar fracture caused by a direct blow)
- Indirect trauma (e.g., a fall on the outstretched hand fracturing the radial head)
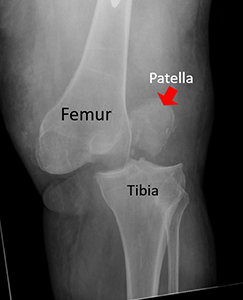
- Muscular pull (e.g., patellar fractures produced by sudden violent contractions of the quadriceps)
Stress or fatigue fractures are produced by repetitive stress (ex. fibular fractures in athletes)
Pathological fractures are produced by minor trauma on an poor quality bone. Severe osteoporosis, tumors, metabolic conditions, and congenital conditions may weaken bone.
- Closed or Open
- Complete or imcomplete 📷
- Displaced or Undisplaced
- In displaced fractures the original trauma, the muscle pull and the gravity force produce changes in the location of the bone fragments
- In undisplaced fractures the bone fragments have not changed their normal location
- Number of fragments: Simple(2 fragments), Wedge (3frag) or Comminuted (>3 frag)

- Weird Angle (Alignment) 📷
- Shortening 📷
- Rotation 📷
- Apposition 📷
This refers to a disturbance of the normal longitudinal axis of the fragments. The fragments are angled.
Shortening is produced by the overlapping of the fragments.
The distal fragment may rotate on the proximal one about the longitudinal axis of the bone.
Relation of two fracture fragments lying rather next to each other instead of in end-to-end contact is termed "apposition."
imperfect alignemnt + rotation is more harmful than imperfect apposituion
- trauma history? → heigth? assoiated injury?
- no trauma? → pathological?, stress fracture?
- Fracture specific:
- Loss of continuity of bone
- abnormal mobility
- no transmitted movement
- crepitus
- Signs of trauma:
- swelling,
- bruising,
- pain,
- tendernes,
- loss of function
- Neurovascular abnormalities
- 6 P's: (1) Pain, (2) Poikilothermia, (3) Paresthesia, (4) Paralysis, (5) Pulselessness, and (6) Pallor.
- Recap-time, Pulse, skincolouration, poikilothermia
- paresthesia/paralyis?

- Xray
- CT → comminuted fx, unclear fx, intra-artricular fx
- MRI → ST-involvment, spinal injury, ligament injury
PAIN MANAGEMENT, IMMOBILIZATION, COVER OPEN FRACTURE
- Splinting → prevents further damage + limits pain
- Analgesics
- Cover open fractures with cleanest material available
- Measures to limit pain and prevent further damage by excessive movement of the fragments.
- Splinting of the limb is a simple and effective method.
- Adequate doses of analgesics should be administered early, provided that there are no contraindications.
- Open fractures should be covered with the cleanest available material.
yes ofc
- hemorrhagic (vascular penetration)
- neurogenic → due to pain

⇒ GIVE VOLUME/TRANSFUSION
A fracture of a long bone may be associated with considerable blood loss, up to 1.5 liters in the case of a fractured femur. In cases with multiple fractures, hemorrhagic shock may be present. Neurogenic shock due to pain may also be present. Such cases require urgent transfusion with blood or plasma expanders.
reduction + immobilization → union → function
- Reduction
- Immobilization/fixation
- achievement of union
- restoration of function
restore normal anatomy
Displaced Fracture & Dislocation
→ restoration of normal anatomy
- in minimal displaced where function of the limb may be restored → otherwise you wanna reduce
- children
- Closed
- without incision, but traction
- quicker union
- less infection
- might be used till surgery
- Open
- surgical
- slower union
- more infections
- when closed failed or when open reduction is indicated in a specific injury

=CLOSED REDUCTION
immobilization via:
- CRIF → see relative stabilty → IM nails, K-wires

or other immobilization devices:
- plaster casts, splints
- slings
- orthosis (brace, splint)
Plaster casts are used in treating fractures that do not need surgical treatment. Usually a splint is used at the beginning, and lately it is completed to a circular plaster.
=OPEN REDUCTION
OPEN Reduction Surgical procedure Direct visualization Touch the fracture Instruments used
CLOSED Reducton External manipulation Don't see the fracture Don't touch the fracture No surgical instruments Xray visualization
- internal: pins, wires, screws, plates + IM nails
- external fixation devices: 📷

external fixation devices: used to surgically fix the fracture site when the fracture is open and internal fixation is not indicated.

surgical
Not at all my friend, totally rigid
intra-articular
No, it heals through direct/primary healing (see below)
conservative or Intramedullary nails

yeees
diaphyseal
Yes, because it heals through indirect/secondary healing (see below)
Aspect | Absolute Stability | Relative Stability |
Micromovement | No micromovement in the fracture site (rigid) | Micromovement in the fracture site |
Surgical Approach | Achieved through surgery (open reduction) | Often treated with IM nails |
Fracture Type | Often in intra-articular fractures | Often in diaphyseal fractures |
Healing | No callus formation (direct/primary healing) | Heals through callus formation (indirect/secondary healing) |
varies widely → depends on location, type, patient...
in general:
cortical bone → 12 weeks (3month)
spongy bone → 6 weeks (1,5month
After external or internal fixation, time is necessary for the achievement of union. This varies widely and differs between fracture sites, fracture types, and patients. However, as a general rule, cortical bone needs 3 months to heal, and cancellous bone requires six weeks. Children require about half as long as adults.
early mobilization → exercise + physical therapy after union
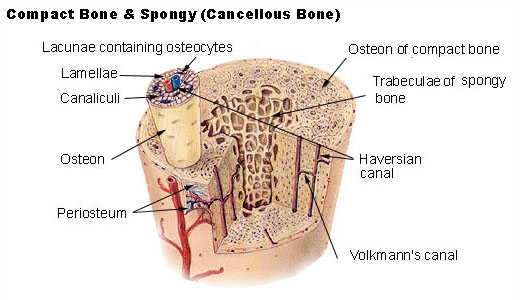
- Secondary = Indirect (with hematoma formation) 📷
- Non surgical (conservative) treatment → relative stability in fracture site
- The impact produces the hematoma.
- The induction stage: Within hours of the injury, fibroblasts from the adjacent tissues enter the hematoma. These cells are stimulated by various activating factors.
- The inflammatory stage: Activated fibroblasts transform the hematoma into granulation tissue.
- The stage of soft callus formation: Fibroblasts undergo metaplasia, transforming into collagenoblasts, chondroblasts, and later osteoblasts. Collagen, cartilage, and bone are produced and deposited in a disorganized manner. This is known as woven bone. The callus becomes firm and can be felt as a mass.
- The stage of consolidation by mature bone production: The soft callus is replaced by lamellar bone.
- The stage of bone remodeling: Excess callus is removed, and the bone resumes its normal or nearly normal shape. The medullary canal is recanalized. The bone structure is modified in response to mechanical stress.
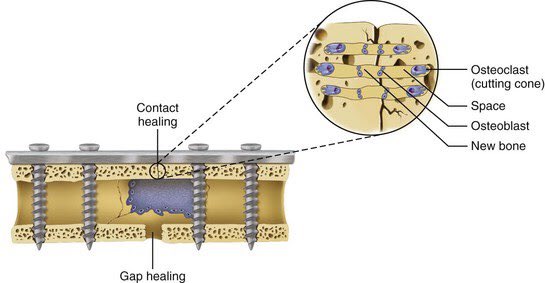
- Primary = Direct (without hematoma formation)
- Surgical - absolute stability in fracture site
screws 📷

- Irreducability
- Open fracture
- Associated injuries of structures in vincinity
- Infection
→ Compartment syndrome
→ Neurovascular injuries (might lead to limb ischemia)
→ Visceral injury
→ ST injury → crush injuries

pain, pallor, pulselessness, paresthesia, paralysis and poikilothermia
- fat from bone marrow → fat embolism
- Thrombosis: DVT, PE esp. lower limb
- infections: sepsis, pneumonia, UTI
- crush syndrome
- nonunion (esp in diaphyseal fx due to bad blood supply)
- delayed (esp in diaphyseal fx due to bad blood supply)
- Mal-union (esp. in metaphyseal fx with good blood supply; surgery indicated if function impaired)
- crossunion (mainly pediatric)
- osteosclerosis of the bone end
- closed marrow cavity
- Hypertrophy/atrophy of the fragments 📷
Avascular bone necrosis → bone collapse
articular fracture or mal-union
→ Joint stiffness
Pathological ossification
⇒ RESTRICTED MOBILITY
Gustillo Anderson classific.
- Type I: Wound < 1 cm 📷
- Type II: 1-10 cm 📷
- Type III A: > 10 cm, high energy, adequate tissue for coverage, includes segmental / comminuted fractures even if wound <10 cm, farm injuries are automatically Gustillo III 📷
- Type IIIB: Extensive periosteal stripping and requires free soft tissue transfer 📷
- Type IIIC: Vascular injury requiring vascular repair 📷
- first aid: dressing + splinting
- AB → Cephalosporin → 5-7days
- Tetanus prophylaxis
- Debridement + cleaning -
- Stabilization
Open fractures require early surgical treatment:
- Enlarge the wound if necessary.
- Excise crushed skin and soft tissues.
- Thoroughly wash the wound with saline and remove foreign material.
- Remove small fragments of bone unattached to soft tissues.
- Perform delayed closure by suturing or grafting if severe contamination is present.
I + II
I, II, IIIa
IIIb+c
Don't worry we gonna go through each of them in more detail in each topic. So feel free to skip that when you are reading this the first time. Just use for recap. 😎
- Allman - medial/middle/distal
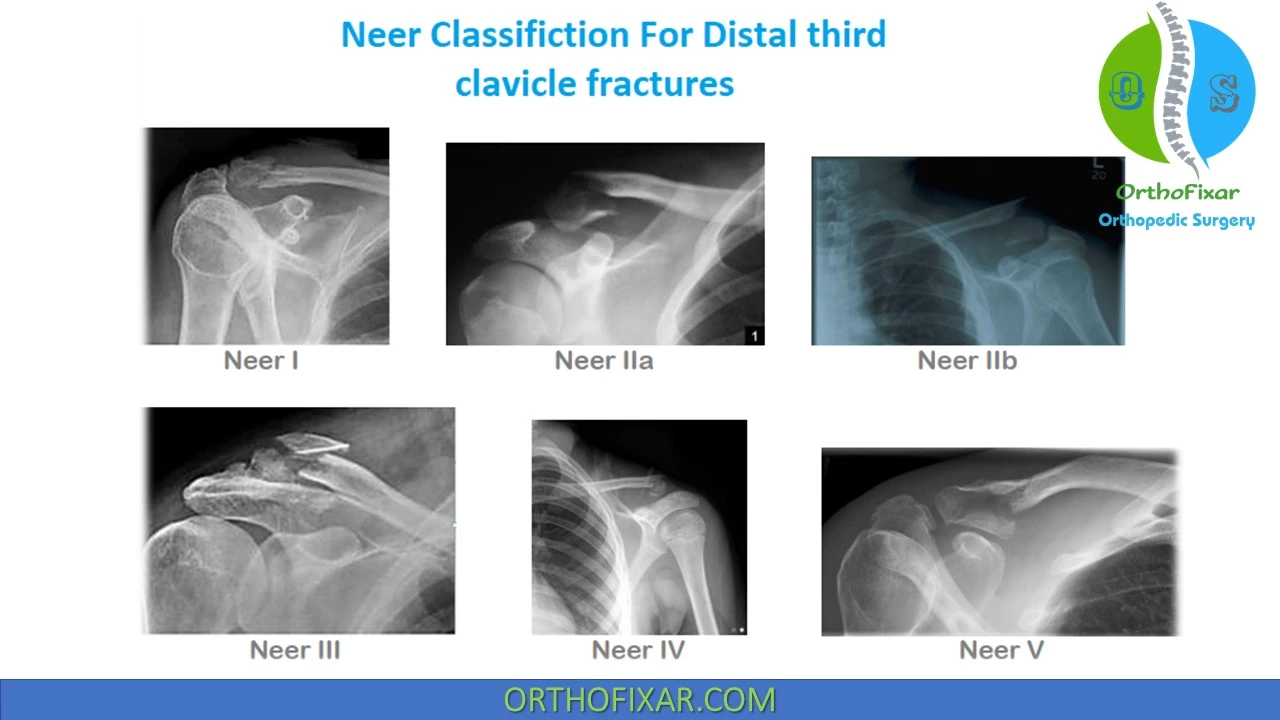
- Neer - distal classification
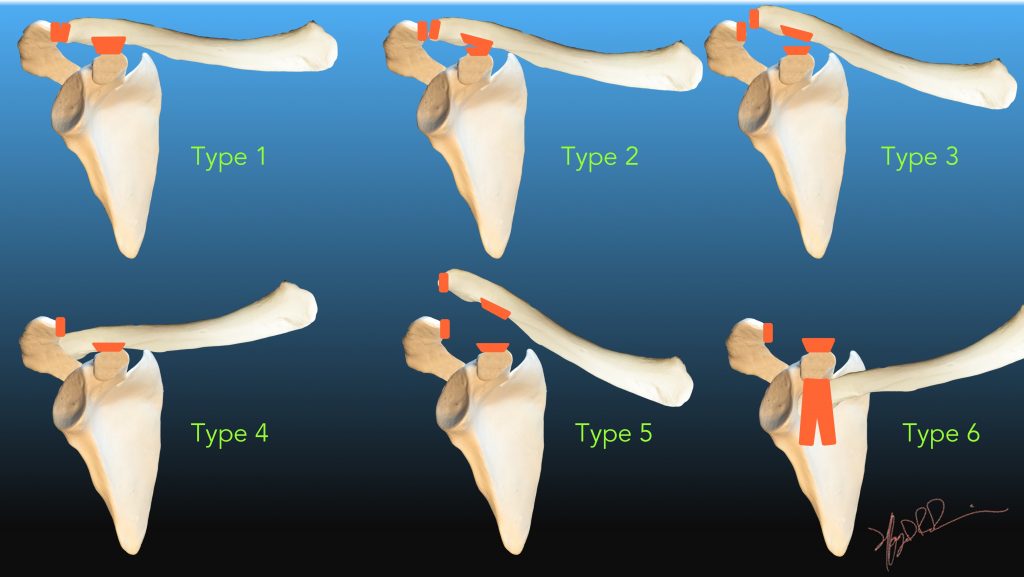
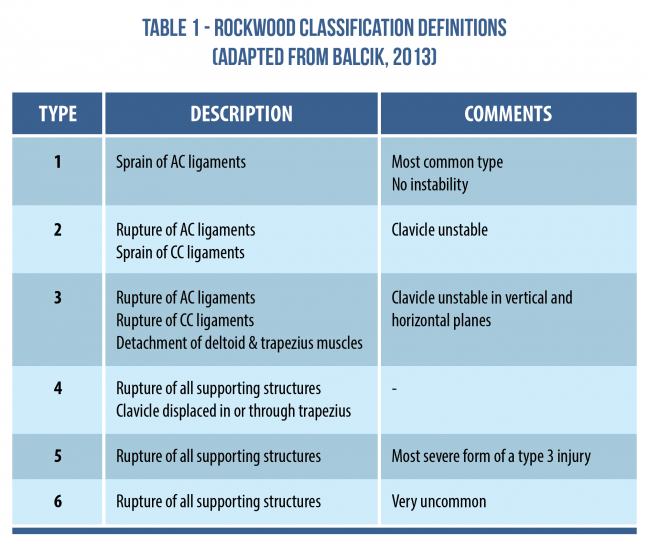
Rockwood
Neer
yes →
- Supra condylar
- Intercondylar
- Both
- Epicondylar
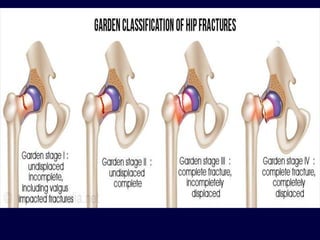
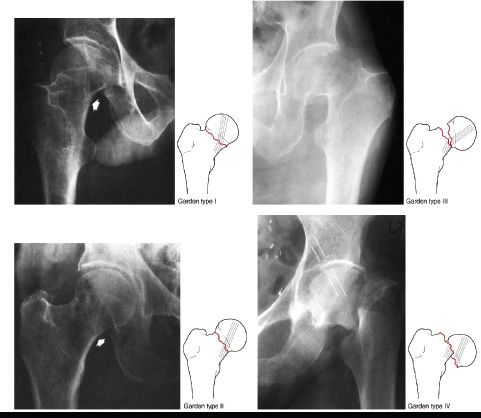
Garden
Schatzker
Description | Treatment | Exception (when the other one?) | Specific technique names |
|---|---|---|---|
Clavicle Fx | Conservative | complication, >2cm, comminuted, under skin, bilateral | Dessault: nondisplaced, Watson Jones: displaced, surgery: see exception |
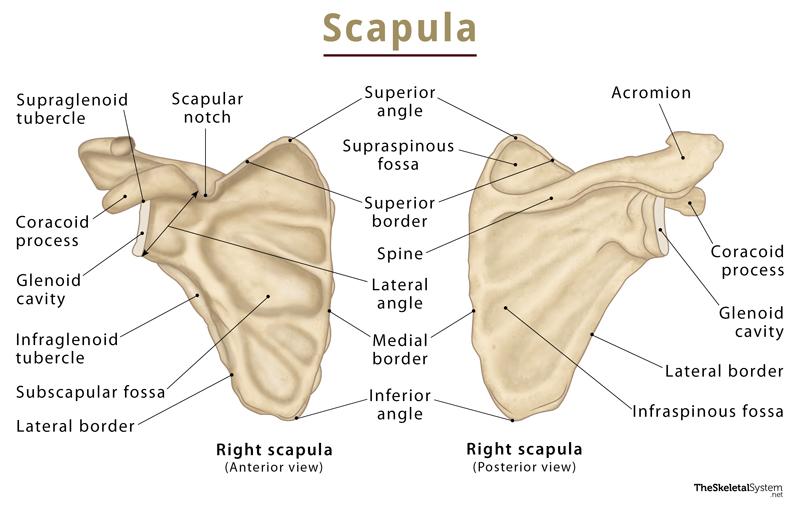
Scapula Fx | Conservative | glenoid, acromial fx | |
AC dislocation | Surgery | type I, II (,III if <2cm) | Tight rope, hook plate, k-wire, plates screws, tendon graft reconstruction |
Shoulder dislocation | Conservative | associated fx, old,recurrence | Hippocratic, Traction-countertraction, Kocher |
Prox. Humerus Fracture | Conservative | displaced, 2-3p → ORIF, CRIF; 4p → arthroplasty | cons.: Dessault; ORIF: philos-plates |
Humeral shaft fx | Conservative | complication, severely displaced, radial n. palsy >6w | U-slab → hanging cast or Sarmiento |
Distal humerus fx | Surgery | nondisplaces, no articular involvement, old | |
Elbow dislocation | Conservative | ||
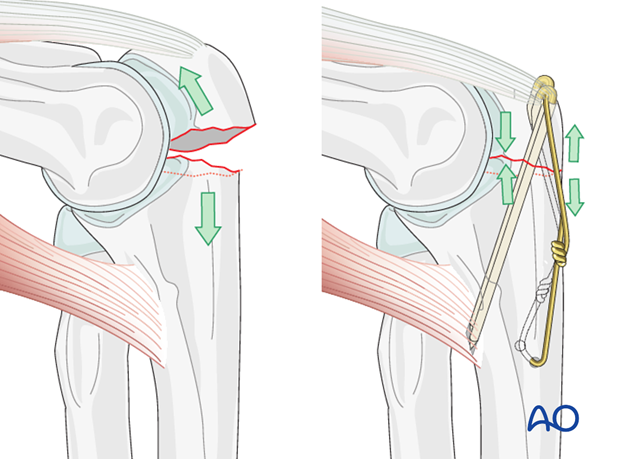
Olecranum Fx | Surgery | non displaced, non-comminuted, no articular involvement | Tension band, plates +screws |
Radial head Fx | Conservative | displaced, comminuted, intra-articular | |
Forearm fx | Surgery | isolated radius or ulnar fx + nondisplaced | |
Distal radius fx | Conservative | severely displaced, intra-articular, open, not reducable, high demanding patient | |
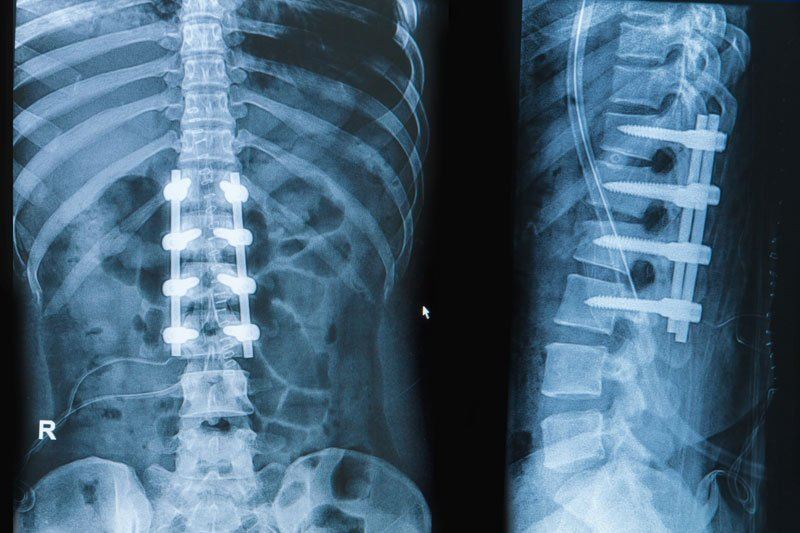
Spine fx | Conservative | highly unstable, neurologic risk | Spinal orthosis Spine fusion |
Pelvis fx | Surgery | stable, pat. can bear weight | |
Hip dislocation | Conservative | associated fx, fragments, >6h | Allis reduction maneuver |
Prox. Femoral head fx | Surgery | no exception, high risk pat. | I+II→IF, III→reduc.+IF,IV→athroplasty |
Femor. trochanteric fx | Surgery | old, high op-risk pat. | sliding screw, gamma nail, artroplasty |
Femoral shaft fx | Surgery | - | ORIF, Gamma (CRIF) |
Distal femoral fx | Surgery | nondisplaced, not intratricular | |
Patella fx | Conservative | cant extend, complications, displaced, comminution | Cylinder cast; CRIF, ORIF, tension band |
Knee sprain | Conservative | when full lig. rupture | RICE, orthesis |
Tibial plateaufx | Conservative | hard displaced, hard depressed, intra-articular, complications | |
Tibial shaft | Conservative | displacement, comminution, ankle involement, spiral fx | |
Ankle sprain | Conservative | tendon rupture, associated fx | RICE, orthesis |
Ankle fx | Conservative | displaced, not isolated |
🤸🏽♀️Shoulder girdle injuries
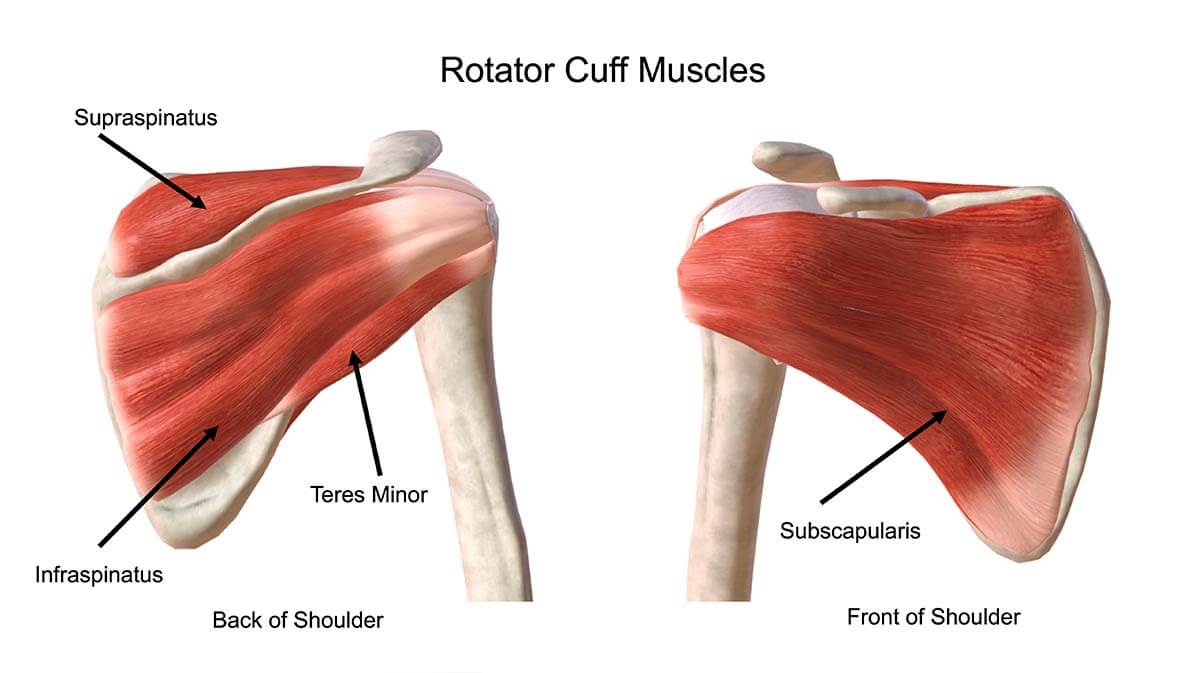
- Supraspinatus. This holds your humerus in place and keeps your upper arm stable. And helps lift your arm.
- Infraspinatus. This is the main muscle that lets you rotate and extend your shoulder.
- Teres Minor. This is the smallest rotator cuff muscle. Its main job is to assist with rotation of the arm away from the body.
- Subscapularis. This holds your upper arm bone to your shoulder blade and helps you rotate your arm, hold it straight out and lower it.
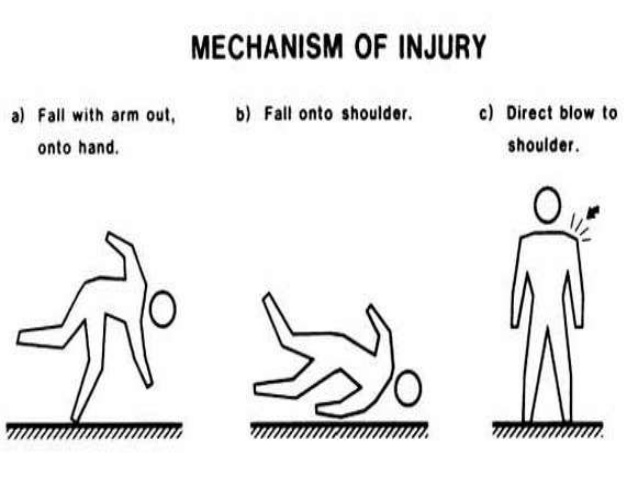
indirect + direct
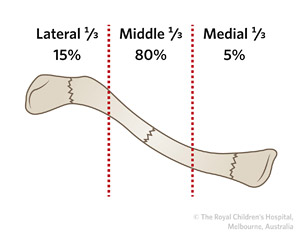
Group | Location |
1 | Midshaft (middle 1/3rd) |
2 | Later (distal 1/3rd) |
3 | Medial (proximal 1/3rd) |
classic
- displaced/undisplaced
- simple/comminuted
- open/closed
- ...etc → see classic classification
Type | Characteristics |
I | - stable → no surgery
- Minimal displaced, lat. to CC-lig
- T+C lig. are intact |
IIa | - unstable
- displaced, medial to CC lig
- T+C lig intact |
IIB | - unstable
- displaced, betw. + T+C lig
- T intact, C not intact |
III | - stable
- intra-articular AC-joint
- T + C intact |
IV (= pediatric fx) | - stable
- sup. displacement of medial to CC
- T +C intact, physeal fracture |
V | - unstable
- comminuted, med. clavicular displacement, inf. segment attached to CC-lig
- T + C intact |
Physeal fracture occurs in the immature skeleton of children
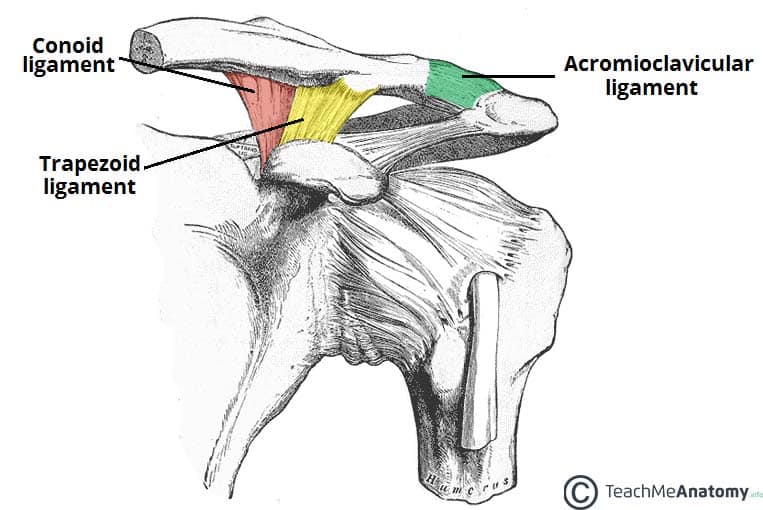
CC Lig: coracoclavicular ligament = T+C lig
T lig: trapezoid ligament
C lig: conoid ligament
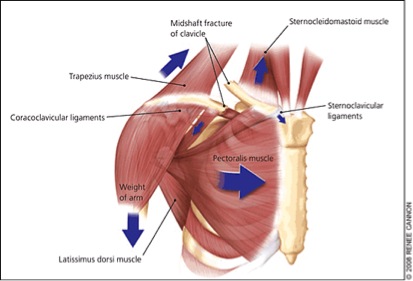
- tenting of the overlying skin → SCM pull medial fracture segment upwords
- shortening of the shoulder → due to pectoralis pull (pulls scapulohumeral segment medially → pulls lateral fracture segment medial too)
- elevation of the AC joint → due to CC ligament rupture
(coracoclavicular ligament = trapezoid ligament + conoid ligament)
open fracture, brachial plexus lesion, vascular lesions, pneumo/hemopneumothorax
acessing neurovascular status, pulmonary auscultation
⇒ 6 P's:
pain, pallor, pulselessness, paresthesia, paralysis and poikilothermia
brachial plexus lesion→dysfunction of distal nerve
subclavian artery involvement →Weak pulses
symptoms of pneumo/hemopneumothorax (very rare)
COMPARTMENT SYNDROME!
>2cm shortening → functional abnormality
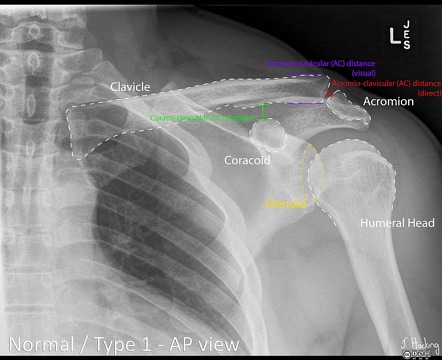
X-Ray
AP
CT / MRI
- Underlying secondary disease (e.g. osteomyelitis, tumor,etc.)
- ST-involvement
- severe vascular involvement
conservative treatment, almost all of them
only in fully nondisplaced fractures → otherwise further displacement with dessault bandage (all nondisplaced middle, medial, lateral)
in displaced fractures
4 weeks

- almost all distal → only conserv. if they are not competely non-displaced
- Clavicle is shortend >2cm (bad functional outcome)
- severe comminuted fx
- open fracture
- bilateral
- no closed reduction possible
- neuro-vascular abnormalities
- lesion is immediate under the skin
- polytrauma
- aestetic reasons (big callus formation)
- patients in coma

plates and screws
CRIF
intramedullary nail, percut. k-wires
severe chest trauma
Location + displacement
- not really specific
- pain
- associated injury symptoms
- shoulder instability
classic
(Xray, ct, mri (ST)
- associated injury complication
- shoulder instability
- scapular dyskinesis
conservative
- Majority of fractures require immobilization in a sling for 6-8 weeks.
- Rehabilitation is necessary after immobilization.
- acromial fx
- glenoid fx (with glenohumoral instability)
floating shoulder: fracture scapula + clavicle
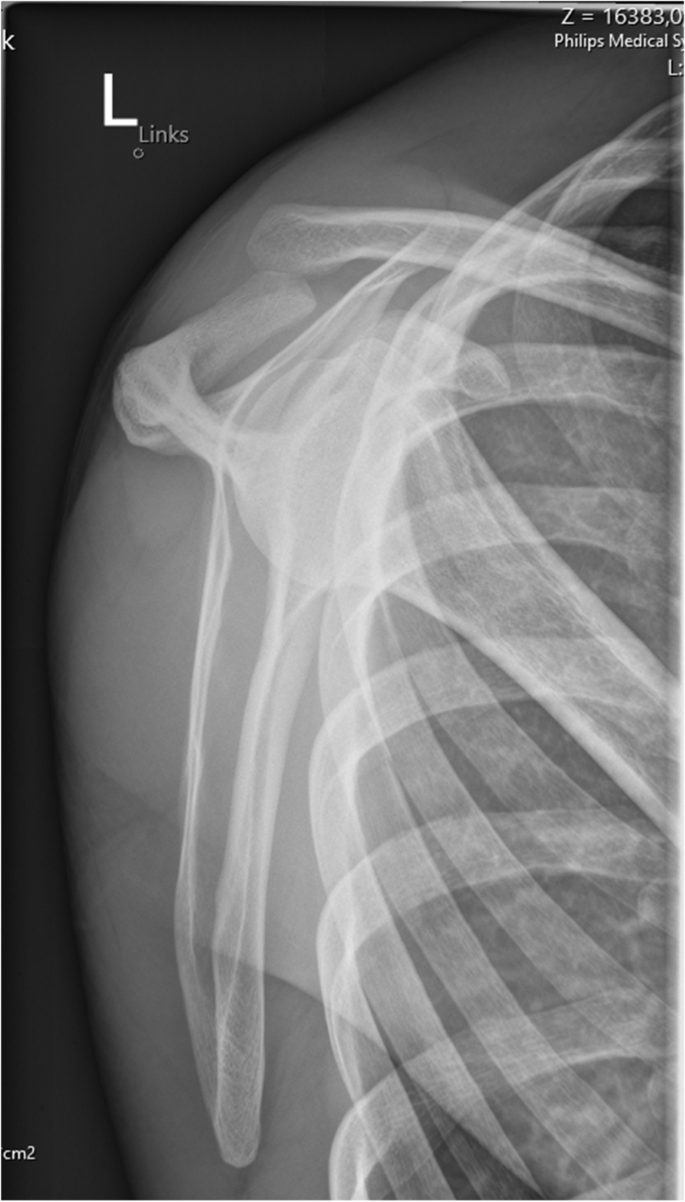
= shoulder separation due to traumatic injury to AC joint → disruption of AC ligament and/or coracoclavicular ligaments 📷
coracoclavicular ligament = conoid + trapezoid
AP + LeftRight stability/ horizontal motion stability
sup-inf. stability/ vertical movement stability
indirect or direct trauma like clavicle fracture
press downs step ladder → if it pops backs → piano!
- step ladder sign = step-like elevation 📷
- piano key sign = A maneuver used to determine injury to the coracoclavicular ligament, whereby a downward pressure is applied on the distal end of the clavicle. The result is positive if the clavicle pops up after release of the downward pressure.
⇒ in type 3+5
- AC assessing → check AP (horizontal) stability
- CC assessing → check SI (vertical) stability
- piano key + step ladder sign
- AC joint tenderness
- pain + other classics
Depends on severity of displacement (see above)
⇒ type I, II
+/- III (if <2cm displaced)
CONSERVATIVE → immobilization with sling + RICE 📷
- acute type IV, V or VI injuries
- acute type Ill injuries in laborers, elite athletes, patients with cosmetic concerns
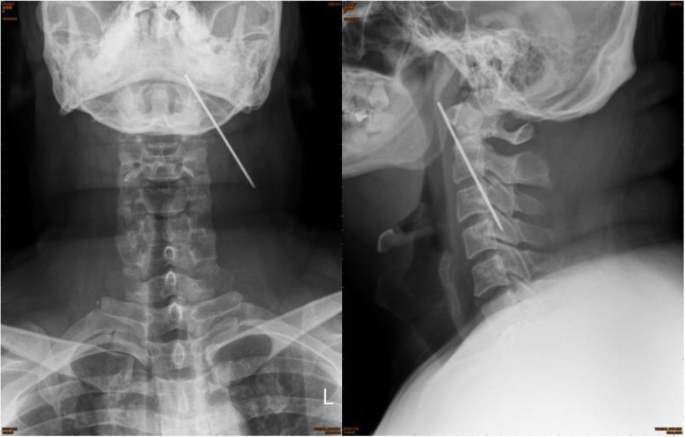
Kirschner wire 📷
when dislocated (not in severe dislocation)
through acromial process into clavicle → bend them at external end
very cheap, but still allows micromovent → not in severe dislocations
K wires haven't been taken out →rupture of one wire → migration+ dislocation into neck possible
you dont have to take it out :)
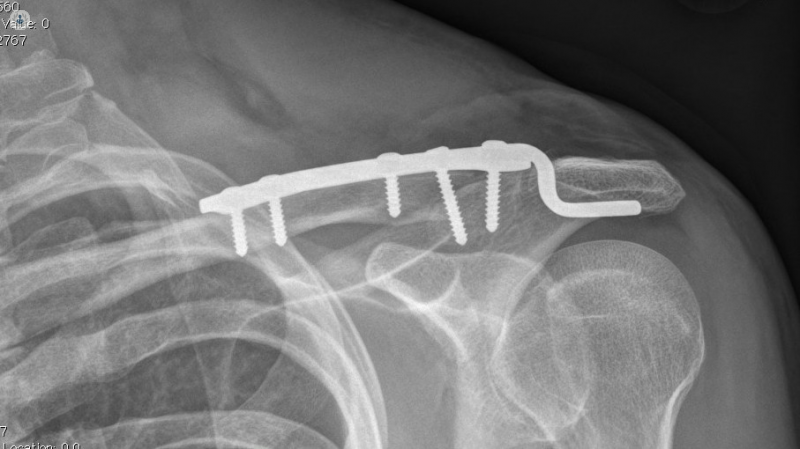
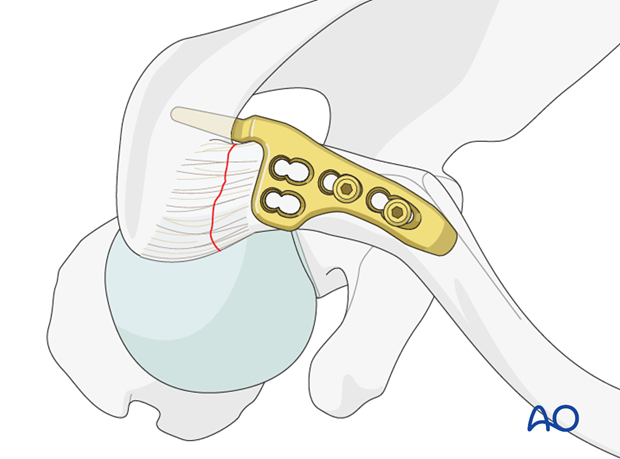
- Hook in the way of AC ligament
- Hook goes not through acromium(like K-wire), but under it→ every abduction irritates the rotator cuff and might cause it to tear
- lenght of the hook is not variable
screw through clavicle + coracoid process
if untreated → necrosis of the ligament → can't "bend" them back with the types of treatment above
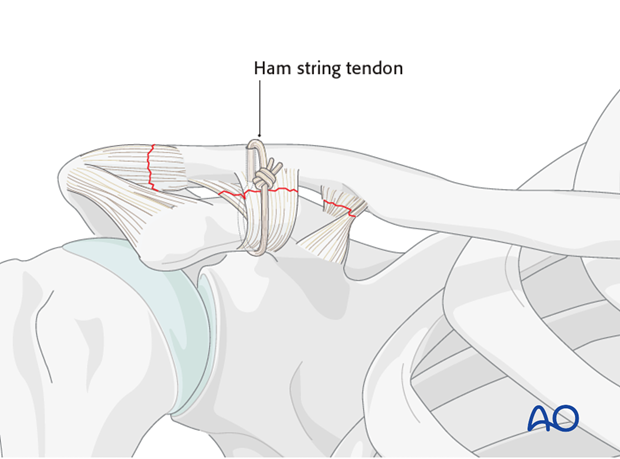
Reconstruction by harvesting tendon graft 📷
→ e.g. from gracilis, quadriceps
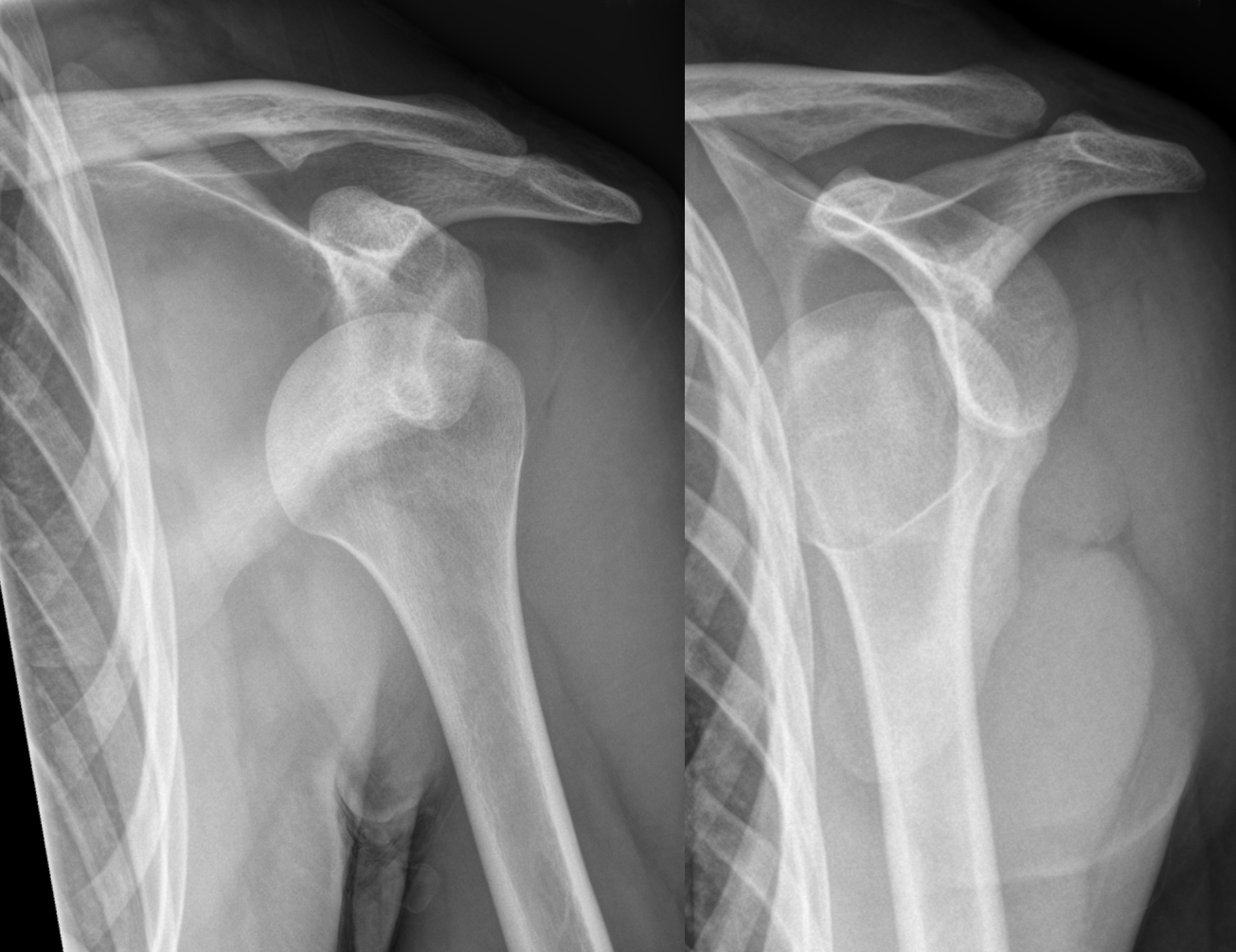
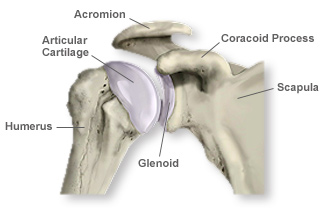
The shoulder dislocation (more accurately termed a glenohumeral joint dislocation) involves separation of the humerus from the glenoid of the scapula at the glenohumeral joint.
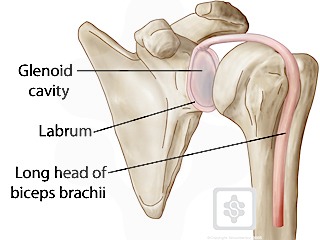
The glenoid is a saucer-shaped extension of the scapula. Its shape means that it offers limited bony support to the joint. The glenoid is augmented by the cartilaginous labrum with additional support from the joint capsule, surrounding ligaments and the muscles of the rotator cuff. The labrum, capsule and ligaments tend to be stronger in younger patients.
around glenoids 📷 → stabilizes it
where did the humerus go?
→most of the cases anterior
Anterior (80-90%) Posterior Inferior Superior
Anterior (compare hip dislocation: most common post.)
indirect trauma, violent muscle contraction(e.g.epilepsy)
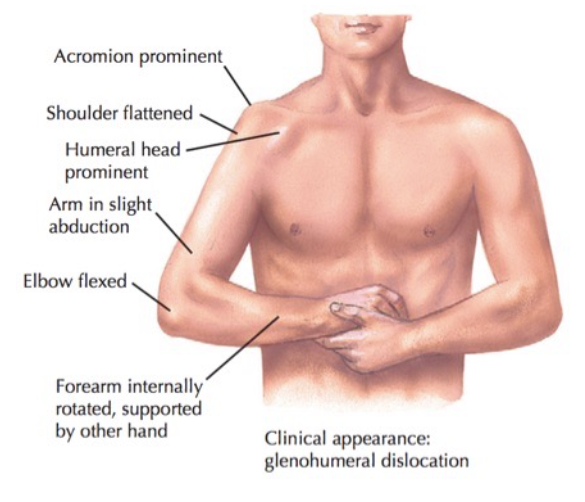
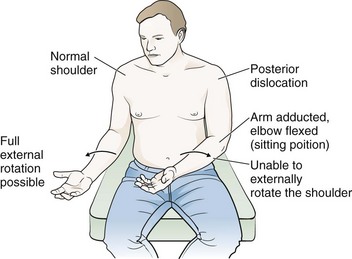
- Flexing + abducted arm
- Internal rotation of forearm
- Acromium prominent > not round anymore but 90degree
- Humeral Head ant. visible
- Deltopectoral grove Not und palpable
- Supported by other hand #
- pain
- Pain, arm abduction, forearm sustained.
- Palpation: under acromion-deltopectoral groove.
ant. dislocation: 📷
- humerus not in glenoid cavity anymore, not same acromi-humoral relationship anymore,
- internally rotated
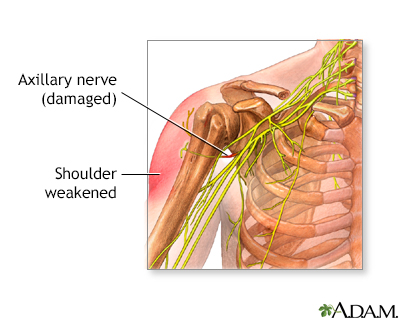
associated soft tissue injuries
- NeuroVascul. dmg (axiliar + brachial plexus others nerves)
- irreducibility
- associated fractures (e.g. tuberosity fractures)
- open dislocation
- associated cuff tear
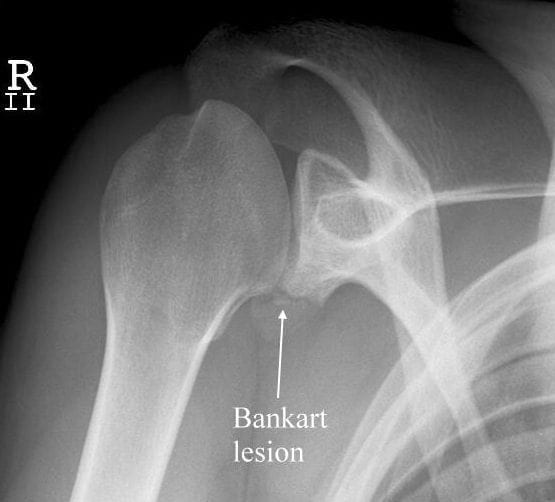
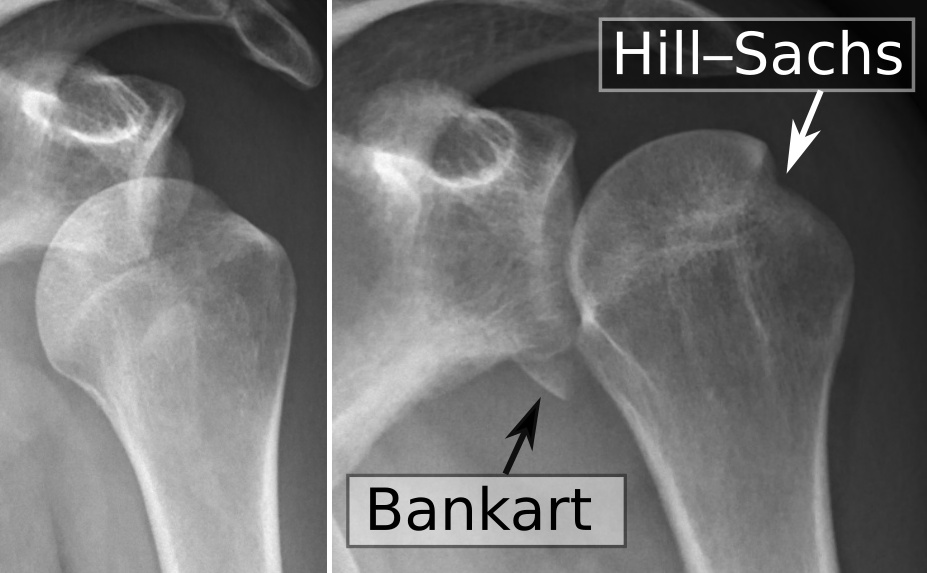
- bankart, bony bankart, Hill Sachs
- instability (e.g. after trauma)
- osteoarthritis
- adhesive capsulits (frozen shoulder) 📷
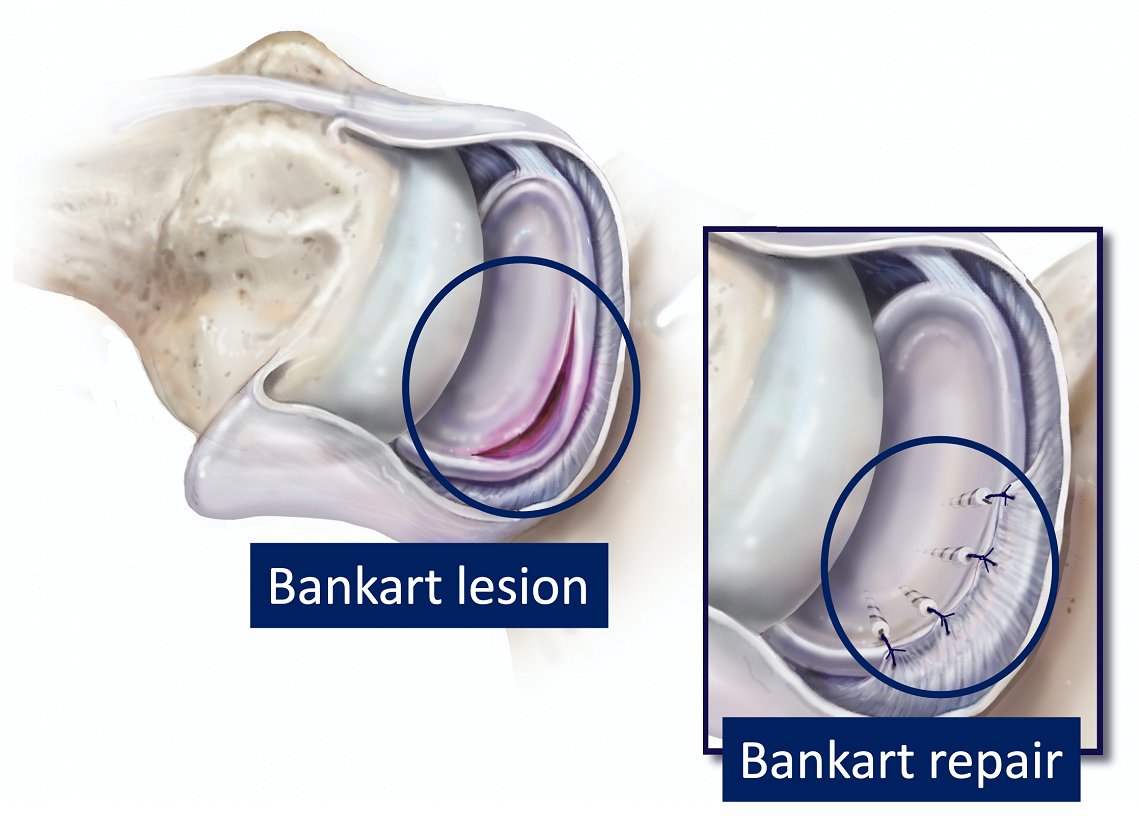
part of glenoid bone is broken off, but still attached to the labrum 📷


gr. tuberosity fracture: 📷

- Xray
- Full neuro-vascular assessment
- give proper analgetic/anesthesia therapy
99% closed nonsurgical reduction
turn into ASD then reduce with other methods
immobilization with dessault bandage 📷
- associated fractures
- old dislocation (4w)
- + recurrent dislocation (esp. in young patients → very high chance!)
- closed reduction doesn't work /impossible
a procedure to prevent recurring anterior shoulder dislocations due to instability in the back (anterior) of the shoulder.
→Arthroscopy suturing of labrum to glenoid 📷
🦾 Humerus fractures
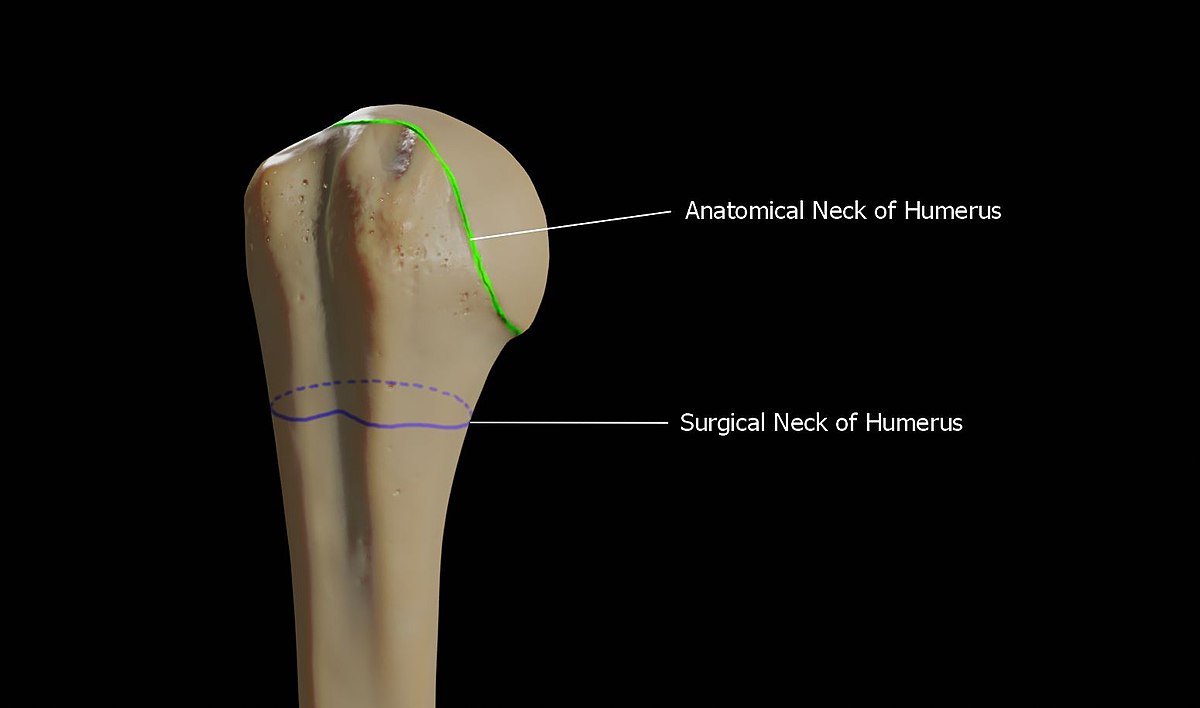
growth plate
- more often affected then anat˝˝omical → weaker
- average neck-shaft angle is 135°
surgical neck • represents the weakened area below head • more often involved in fractures than anatomic neck • average neck-shaft angle is 135 degrees
Muscles
- pectoralis major displaces shaft anteriorly and medially
- supraspinatus, infraspinatus, and teres minor externally rotate greater tuberosity
- subscapularis internally rotates articular segment or lesser tuberosity
2:1
- Osteoporotic elderly (low energy falls)→on outstretched arm
- in young individual (high energy trauma): might also have associated Soft tissue + neurovascular injuries
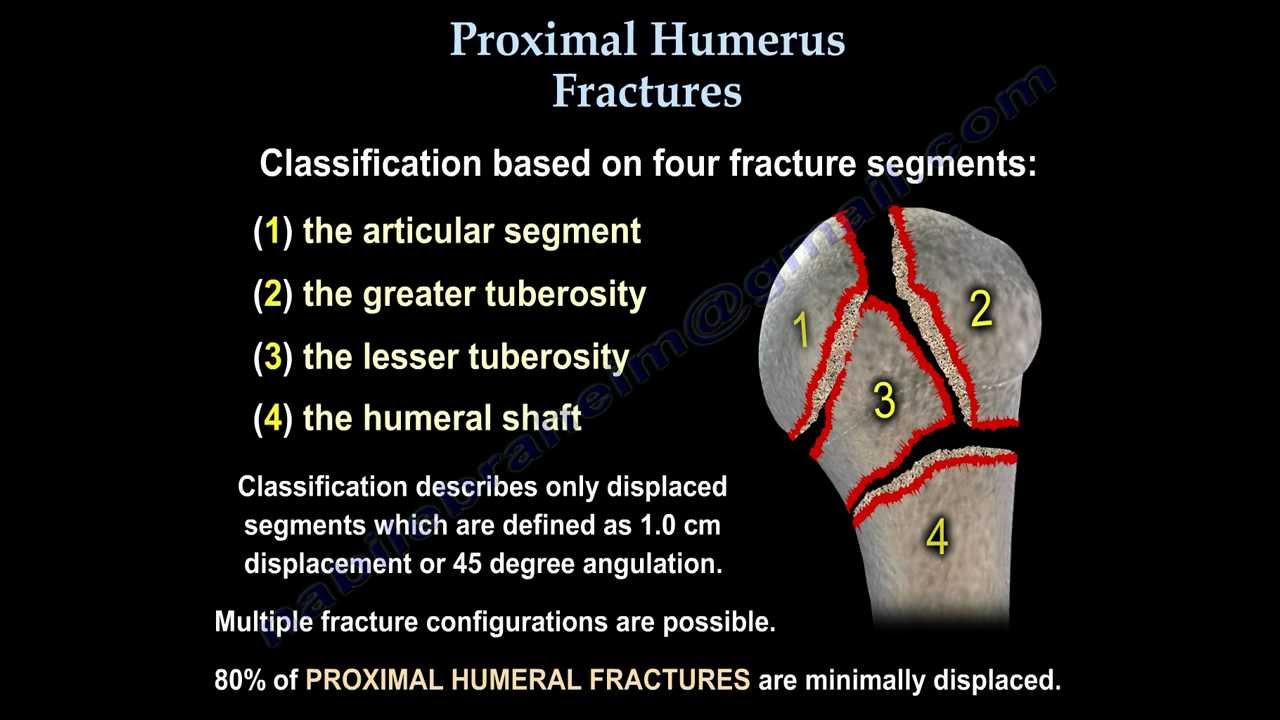
→ 4 parts of prox. humeral fracture
- if one part displace → 2 part fracture
- if 2 displaced → 3 part
- if 3 displaced → 4 part fracture
- dislocation
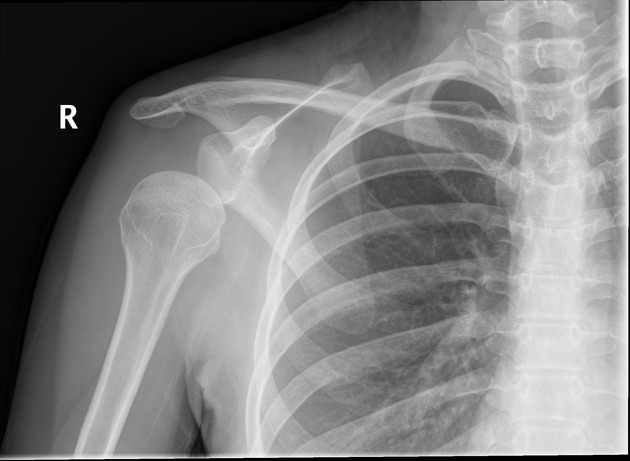
No/minimal displacement = 1 part fracture 📷
muscles pull up → rotator cuff muscle
gr. tuberosity displaced
humeral head more then >45° change if you compare to diaphysis
- Pain
- Decreased motions
- Extensive ecchymosis
NeVas exam ⇒ axillary nerve injury most common
- Sensory loss lat shoulder
- Abduction + ext. Rotation not possible (deltoid, teres minor)
most of the cases xray: AP + scapular view
CT: prepare for surgery, see more detailed view if unclear on xray (head-split fracture? Head or gr. tuberosity uncertain?), intraarticular comminution
MRI: any rotator cuff injury or other soft T damage?
- 70-80% of prox. humerus fracture
- 2-4 weeks of immobilization
- nondisplaced (<1cm; <45°) = 1 part fx
- use extra-fixation (Dessault bandage) if you think the patient is not gonna be compliant
- Also you might consider this in older patients with more severe surgical neck fracture (2 part fractre)! → risk too high
head preserving treatment
- 2-3 parts fracture (less than 4) , esp. in younger individuals
- percutaneos pinning (K-wires) 📷
- philos-plates: open reduction
- CRIF: intra-medullary nail 📷 + k-wires: closed reduction → small incision sup. to the humerus → introduction of IM nail → nail through 5cm incision ⇒ stabilizes extremly good but is hard to place (needs a lot of xrays) + might damage rotator cuff
- ORIF: philos-plates 📷 : Holes in the plates: rotator cuff muscles can be re-attached here
ball + socket reverse 📷 → deltoid muscles will act like the rotator cuff
only in old people
- screw cut-out: screws come out + scratch glenoid 📷
- avascular necrosis
- nerve injury during surgery
- malunion / nonunion
- Rotator cuff injury
- Arthritis
- Infection
- other classics
Indirect/direct trauma
classic fracture signs
• Pain localized to the fracture site • Redness and swelling • Limb deformity • Palpable step-off or gap • Bone crepitus • Ecchymosis • Possible neurovascular compromise below the site of injury • Possible signs of an open fracture
Nope just the usual
→ classic simple, comminuted, wedge, etc...
- simple
- wedged
- comminuted
- displaced or undisplaced
- closed or open.
- Early
- open fracture
- vascular damage
- Late
- delayed union
- non-union
- mal-union
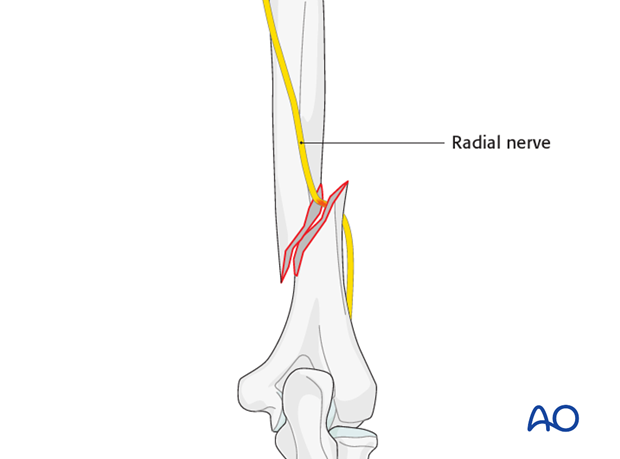
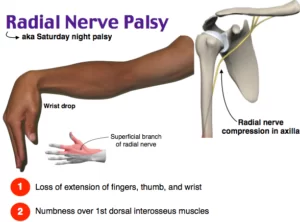
Fall hand
dorsal part sensitivity loss
no dorsiflexion possible
→ general rule: surgery only when hard displaced
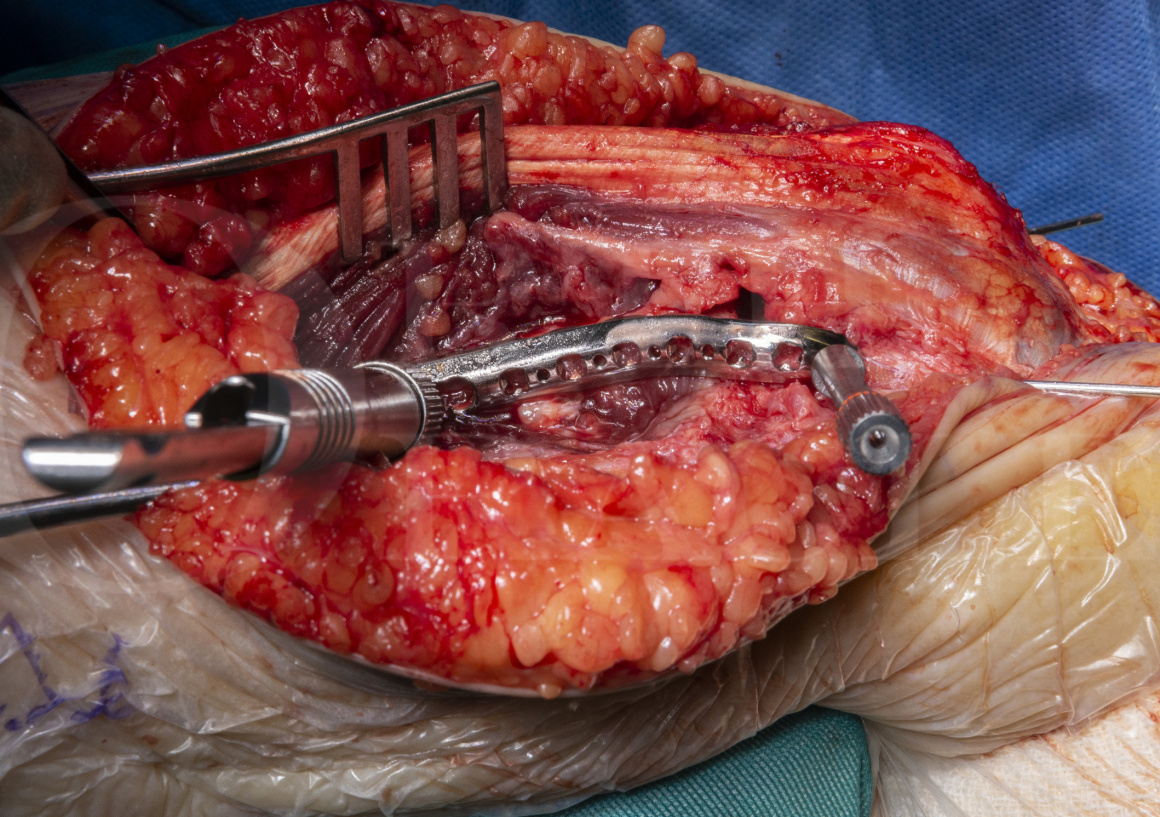
SURGICAL TREATMENT:
ORIF 📷
vascular involvement/compartment/open/polytrauma fracture → surgery
→ radial nerve palsy AFTER 6 weeks→ conservative most of the time due to temporarly nerve palsy
in really long, displaced shaft fractures:
CRIF with IM-nails 📷
closed reduction with minimal invasive fixation
(right pic: intramedullary not deep enough→ will scrape acromial process)
→ intraarticular fractures need ORIF!! (with plates + screw)
- anatomical reduction of articulation, stable internal fixation ⇒ ORIF
- early ROM and rehabilitation
- mainly operative
- undisplaced
- probably without articular involvement
- Eldery + comminuted
⇒ Casts for 3 weeks
💪🏽 Elbow and forearm injuries
- radial head in radial notch of ulna
- radius main articulation with hand
- ulna main articulation with humerus
→ PRONATION + SUPPINATION = rotational movement
- Fall on outstretched arm
- most often posterior or posterior-lateral (med, lat, ant,post)
- convergent=radius+ulna move in same direct
- divergent=humerus goes inbetween radius+ulna (more severe)
- xray 📷
- clinical
- Palpation the olecranum
- Forearm is in slight flexion
Answer is revealed after next question
Early
- nerve damage
- vascular damage
- associated fractures
- instability
Late
- joint stiffness
- myositis ossificans.
- recurrent dislocations


Direct
feel fracture line of the elbow (palpation) + xray
- Early: open
- Late: • mal-union • non-union • joint stiffness • elbow osteoarthritis
- Pain with pronation/supination
- xray: 📷
- undisplaced/ minimally displaced → conservative 2w plaster cast
- displaced/comminuted → surgery
Direct/indirect
2 Plane (AP+LL), always elbow + wrist
Classic
- simple, wedged or comminuted
- displaced or undisplaced
- close or open
- one bone both bones/ one bone+the other dislocated
compartment syndrome!!! most commonly happening in the forearm
passive strech of the arm → severe pain
classic
- Early: • open • neurovascular injury • compartment syd
- Late: • mal-union • non-union • joint stiffness • elbow osteoarthritis
- ORIF
- plate + screw 📷 → surgical
- Anatomic reduction, mainly by compression forces
- Displaced/dislocation
- always if ulna + radius broken
3-4month (with conservative 2-3month)
conservative only if isolated radius/ulna + nondisplaced
⇒ otherwise always surgery
Enjoy the video + try to answer the questions :)
Fracture Prox. Ulna (Cubital) + dislocation radial head 📷
Mechanism: Indirect or direct trauma
Type | Percentage | Description |
Type I | 60% | Fracture of the proximal or middle third of the ulna with anterior dislocation of the radial head (most common in children and young adults) |
Type II | 15% | Fracture of the proximal or middle third of the ulna with posterior dislocation of the radial head (70 to 80% of adult Monteggia fractures) |
Type III | 20% | Fracture of the ulnar metaphysis (distal to coronoid process) with lateral dislocation of the radial head |
Type IV | 5% | Fracture of the proximal or middle third of the ulna and radius with dislocation of the radial head in any direction |


Radial Head dislocation - closed reduction
ORIF ulnar fracture (plate+screws)
Resection radial head
- Emergency department: Closed reduction of radial head dislocation.
- Trauma department: Open reduction and internal fixation (ORIF) of ulnar fracture using plates and screws.
- Old unreduced: Resection of radial head.
Yeaaaa, another one:
Distal radius fracture + dislocation distal radio-ulnar joint (DRUJ) 📷
- ER+children→ closed reduct
- TraumaDep: ORIF
- Old unreduced: resection of ulnar head
- Persistent dislocation ulna
- Radius malunion
- Joint stiffness
- Interosseous n. Syndrome
not really, radius is important here. Ulnar is import in ellbow joint
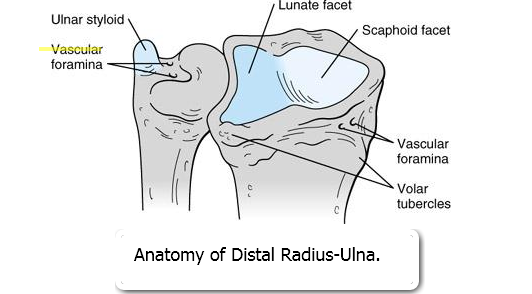
Usually produced by indirect trauma • low energy, fall on outstretched hand • high energy accidents
broken fragment of the radius tilts upward and radially 📷
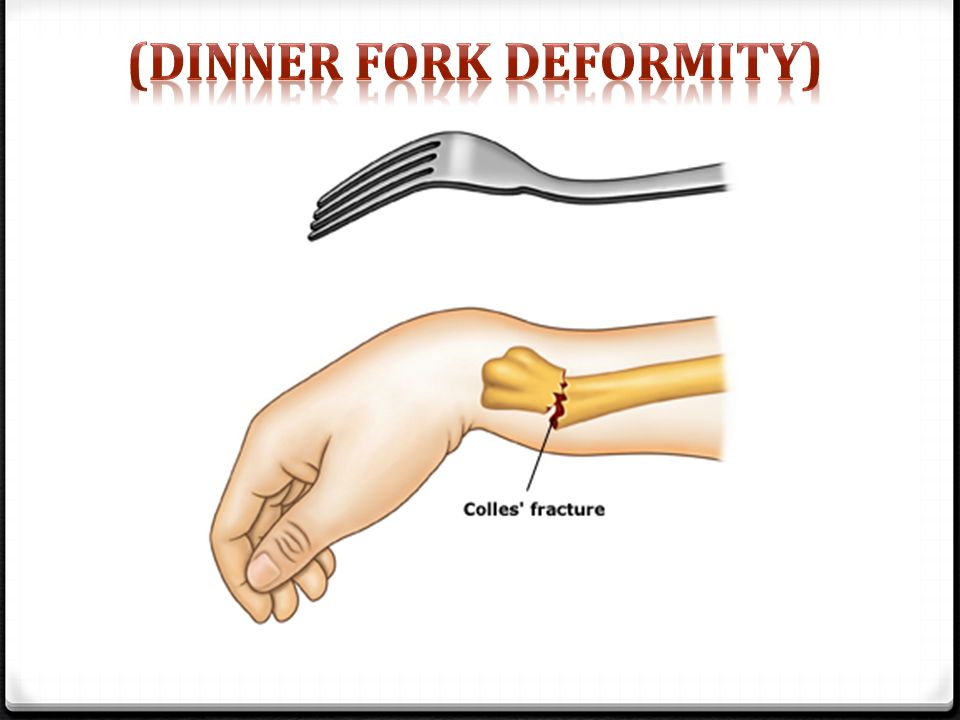
Classic: Pain, tenderness, swelling, bruising, Deformity
fork deformity 📷
Xrays (AP+ Lateral) 📷 CT scan
- Undisplaced
- Displaced
- Anatomical closed reduction (no internal fixation)
- For low demanding patients
→ cast 4-6w followed by rehab
early:
- open fx
- associated fx (scaphoid)
- compartment
late:
- malunion, nonunion
- carpal tunnel sy
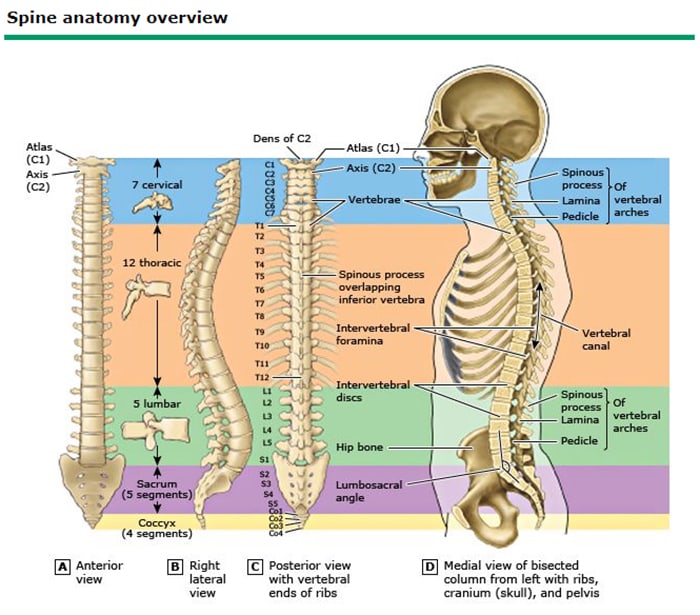
🗼Spine injuries
- Support the mass of the body/head and withstand external forces.
- Allow for mobility and flexibility to absorb energy and protect against impact.
- Protect the spinal cord, nerves, and the vertebral artery in the cervical area.
- Trunk muscles & ligaments act on individual vertebrae for postural control and spinal stability.
Cervical (+thoracic) + lumbar
in trauma mainly:
- C1-C2 + C5-C6
- T11-12, L1-2
- The cervical spine is dominated by flexion-extension motion with axial rotation and lateral bending also in the upper region.
- The thoracic region is characterized by the rib cage and experiences little motion relative to the cervical and lumbar regions.
- The lumbar region has considerable lateral bending in the middle, with great flex-ext in the LS motion segment, minimum rotation due to facet joint orientation.
- Greater mobility in the cervical and lumbar segments leads to greater stresses in those areas and therefore a clinically-noted increase in pain reporting and injury.
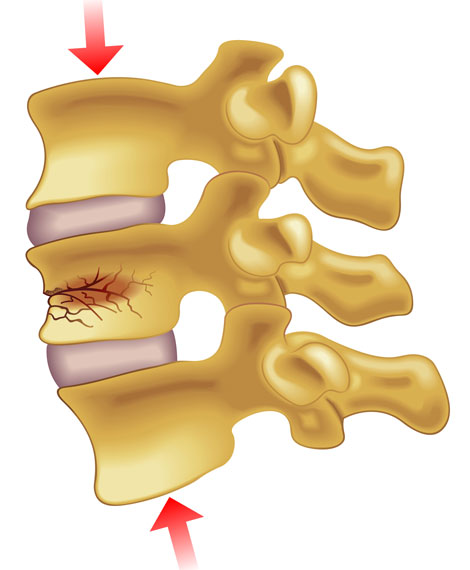
- high velocity 📷
- or osteoporosis fractue (low energy)
cervical
- Hyperextension injury - serious injuries
- Rotation injury
comminutive 📷
nerve damage

nothing special
Xray, CT, MRI
conservatively → spinal orthosis 📷
yes but only if there is no neurologic damage
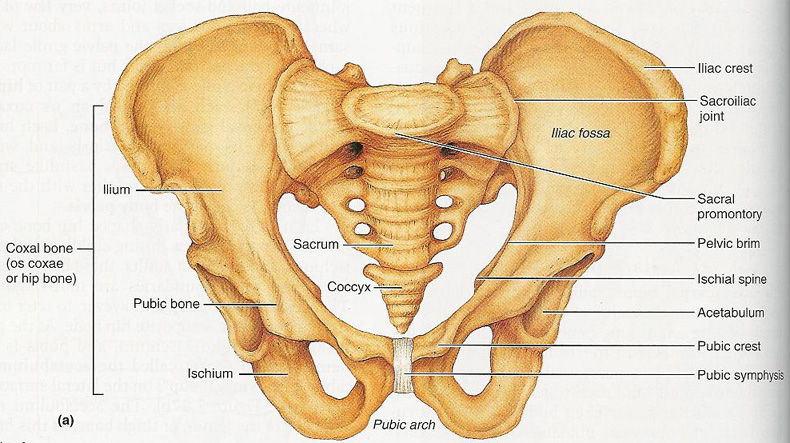
🥣 Pelvic injuries
- weight transfer: upper axial skeleton → lower libs
- muscle + lig. attachement
- protective: abdominal + pelvic viscera
- low energy - osteoporosis
- high energy - direct or indirect
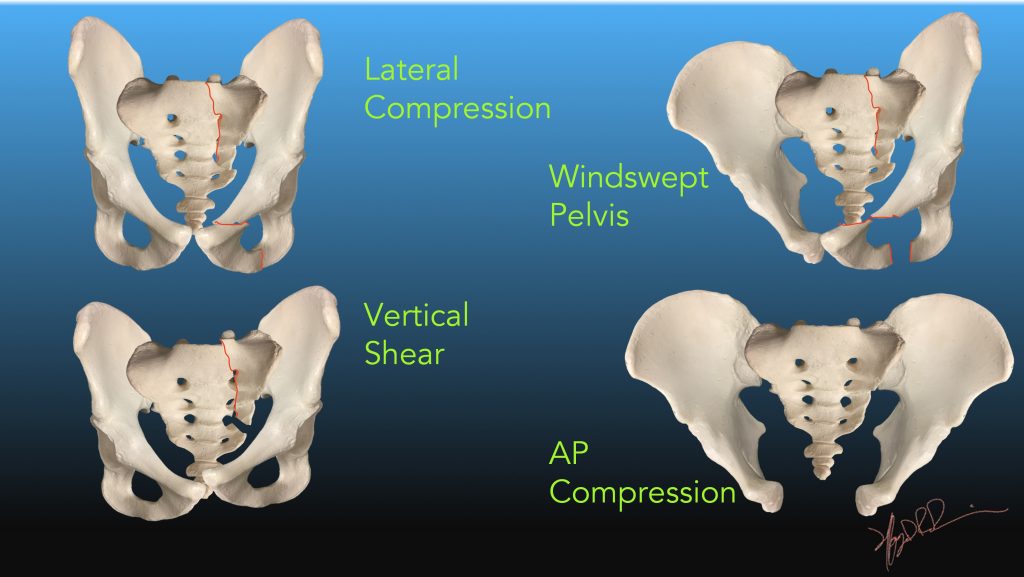
Lateral compression (overlapping pelvis)
50% 📷 → shit
aka. what can happen if get hit by a car or if someone kicks you in your pubic bone?
- Chest injury in up to 63%
- Long bone fractures in 50%
- Sexual dysfunction up to 50%
- Head and abdominal injury in 40%
- Spine fractures in 25%
- probably not walking → inability to bear weight#
- hardcore pain
- evtl. reduced stability by applying force on each iliac crest
- evtl. abnormal lower extremity position
- ext. rotation (uni/bilateral)
- limb-length discrepancy
- Scrotal, labial, or perineal hematoma, swelling, or ecchymosis
- Flank hematoma
- Lacerations of perineum
- Degloving injuries (Morel-Lavallee lesion)

- lumbosacral plexus injury
- gross hematuria
- rectal exam → sphinctertone + sensation
- vaginal or rectal hemorrhage

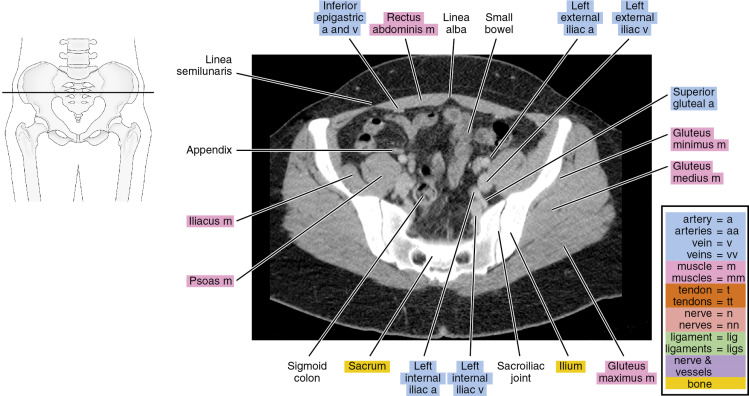
better + clearer evaluation
→ esp. for post. ring
- Routine part of pelvic ring injury evaluation.
- Better characterization of posterior ring injuries.
- Helps define comminution and fragment rotation.
- Visualize position of fracture lines relative to sacral foramina.
- shock
- urinary tract + visceral injury
- degloving injury
- open fracture → !!50% mortality ☠️
classic
- osteoarthritis
- chronic instability
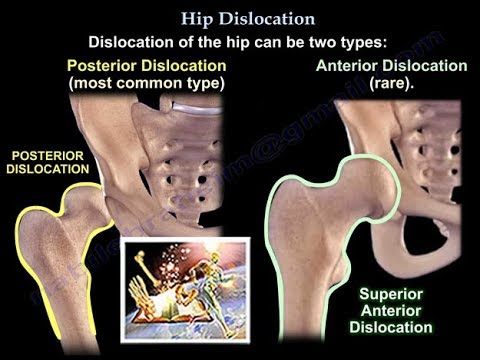
young patient, high engery → dashboard injury
Hip joint is a super stable one
- simple vs. complex
- anatomic classification
- simple → no fracture, only dislocation
- complex → fracture + dislocation
- post dislocation → "dashboard injury"
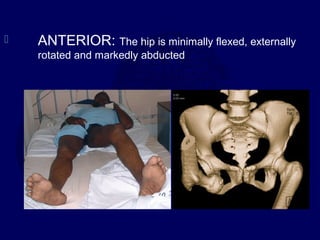
- ant. disloation → due to abduction + ext. rotation trauma → "Rape"-trauma
- inferior vs. superior
Posterior dislocation (90%):
- Occurs with axial load on the femur, typically with the hip flexed and adducted.
- Axial load through the flexed knee (dashboard injury).
- The position of the hip determines the associated acetabular injury.
- Increasing flexion and adduction favor simple I.
- Associated with osteonecrosis, posterior wall acetabular fracture, femoral head fractures, sciatic nerve injuries, and ipsilateral injuries (up to 25%).
- Anterior dislocation:
- Associated with femoral head impaction or chondral injury.
- Occurs with the hip in abduction and external rotation.
post. dislocation
- Post. dislocated? → usually seen on APview
- Lesser trochanter visible → internal rotated!
- Check femoral head for fracture line before closed reduction
- within 6hrs
- in ant + post. dislocation
- Contraindication: FEMORAL NECK FRACTURE
Allis maneuver 📷
- irreducible with conservative
- incarcerated fragments
- dalyed presentation (>6hrs)
- Associated fractures → ORIF

- Osteoarthritis
- Femoral head avascular necrosis
- sciatic n. injury
- recurrent dislocation
🦿Femur fractures
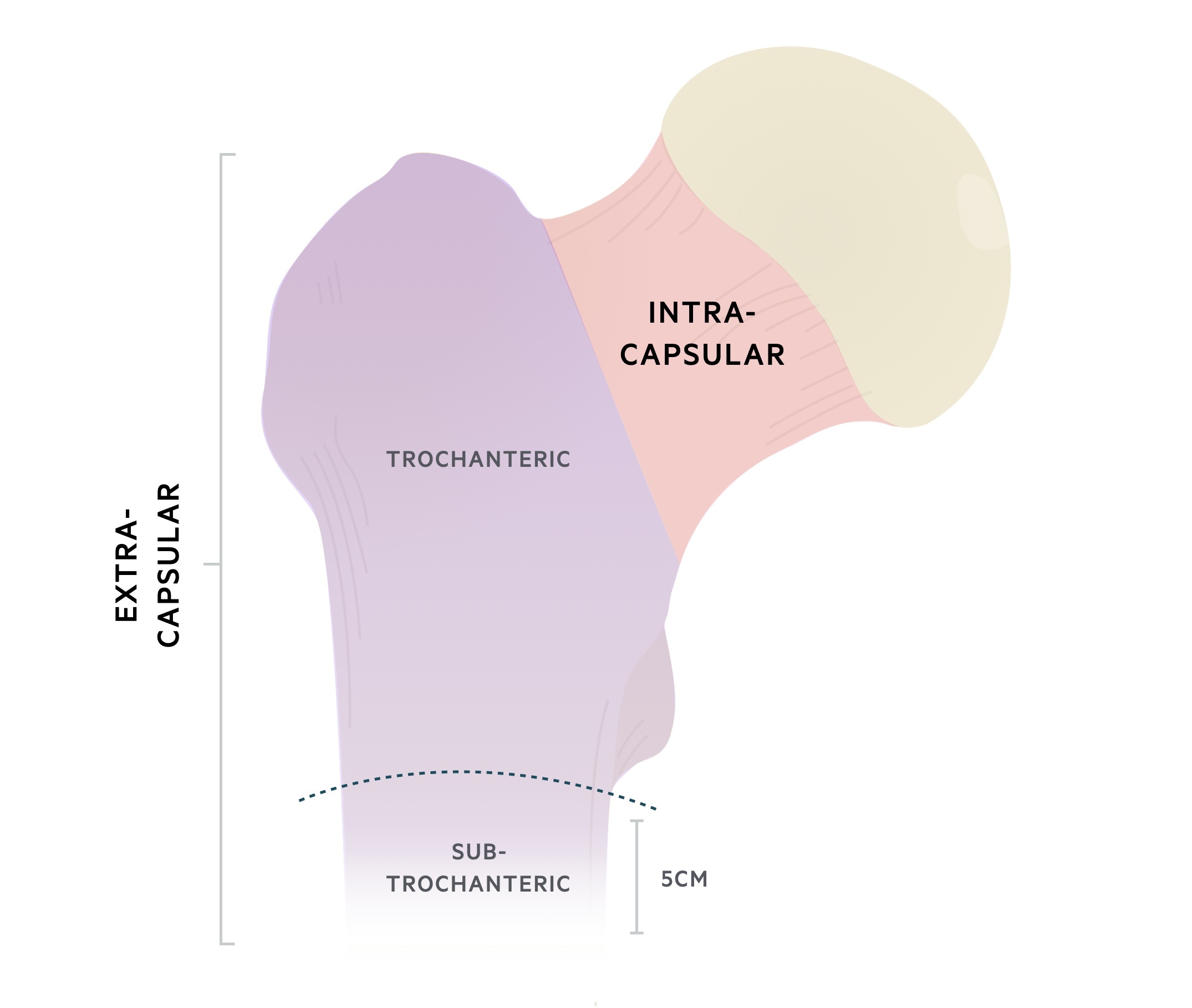
intracapsular 📷
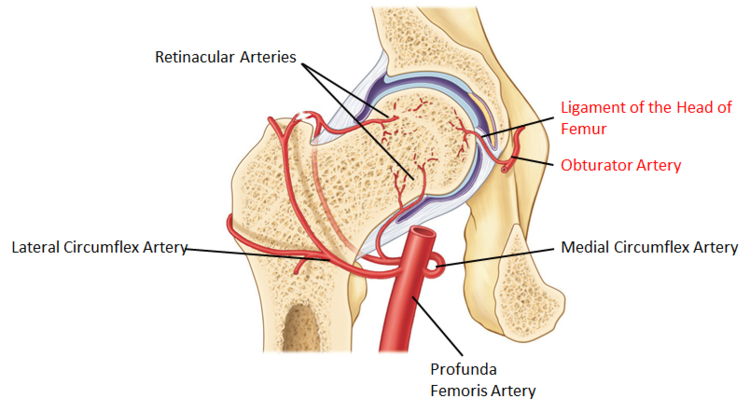
Avascular necrosis

The main problem is the blood supply of the femoral head. 📷 Two of the most important blood sources, the capsular vessels and the medullary vessels are affected by the fracture. The third source of blood supply (the ligamentum teres) is not enough to maintain the viability of the femoral head if the other two sources have been destroyed.
low energy - osteoporotic elderlies (90%)
→ in young; only in high energy trauma
femoral shaft fracture
Treat neck fracture before shaft fracture!
→ look for possible neck fractures if you find a shaft fracture to exclude it before treating
💀 death → high mortality prognosis!
- slight point groin pain
- pain along medial thigh + knee
entire hip pain
- no deformity
- minor discomfort with hip motion (active + passive)
- percussion pain over greater trochanter
- ext. rotation
- abduction
- shortening
DD: ant. hipdislocation
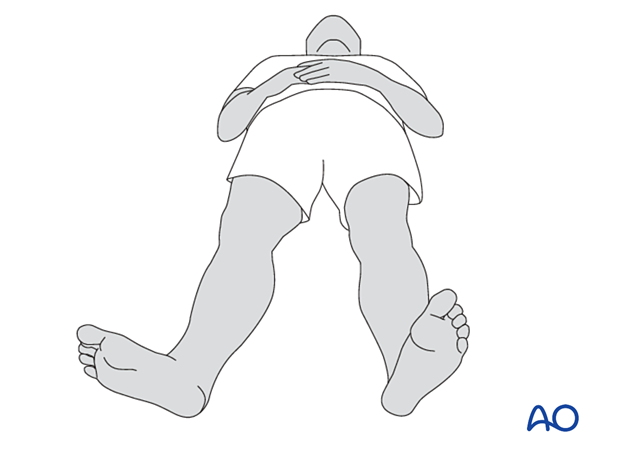
- X-ray
- AP
- Internal rotation AP hip is best for defining fracture type
- Cross-table lateral 📷
- Full-length femur
- CT
- Helpful in determining displacement and degree of comminution in some patients
- MRI
- Helpful to rule out occult fracture
- Not helpful in reliably assessing viability of femoral head after fracture
never 🤡
fixed in situ with pins or screws
reduced and fixed with screws
in patients <35y → try screws
classic complications that are associated with elderly hosptalized patients undergoing surgery:
- infection
- DVT + Pulm. embolism
- pain
- pneumonia
- decubitus
- UTI
- etc.
- non-/mal-union
- femoral head avascular necrosis
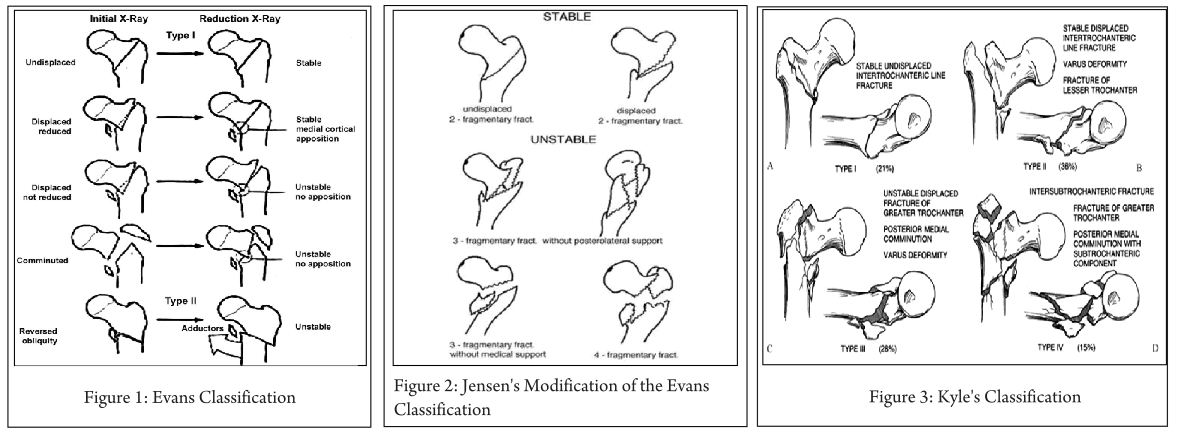
extracapasular
- high energy in young
- low energy in osteoporotic elderly
pain + functional loss
same as displaced neck but apperently adduction instead of abduction
→ shortening, ext. rot., adduction
- Radiographs
- Recommended views
- AP pelvis
- AP of hip, cross table lateral
- Full-length femur radiographs
- CT or MRI
- Useful if radiographs are negative but physical exam consistent with fracture
- MRI useful to evaluate intertrochanteric extension with isolated greater trochanteric fracture patterns
- patient at high periOP mortality
→ pneumona, UTI, decubitus, DVT

- sliding → only in stable intertrochanteric fractures
- Gamma can be used in other types too:
- Stable fracture patterns
- Unstable fracture patterns
- Reverse obliquity fractures
- 56% failure when treated with sliding hip screw
- Subtrochanteric extension
- Lack of integrity of femoral wall
- Associated with increased displacement and collapse when treated with sliding hip screw
- Increased risk of lateral wall fracture with decreasing lateral wall thickness
- Equivalent outcomes to sliding hip screw for stable fracture patterns
- Use has significantly increased in the last decade
Indications:
Outcomes:
- severe comminuted fract.
- osteoporosis
- if others fails
- early: classic elderly hospital post-surgery complications late: mal+non-union
→ notice: no avascular necrosis
high energy injuries
→ fracture of variable severity: simple, wedged or comminuted, displaced or undisplaced, closed or open.
- classic (shaft) fracture symptoms

also see complication femoral neck
- Early complications • open fracture • vascular or nerve damage • fat embolism
- Late complications • mal-union • delayed and non-union • knee stiffness
- surgical → even for undisplaced → without internal fixation they might get displaced
- IM gamma nails - CRIF
- plates + screws - ORIF
- external fixation in open fractures

- below metaphysis-diaphysis junction
- until articular surface of condyles
classic
high energy → young
low energy → old, osteoporotic
significant displacement of the fracture

nothing special
Early complications • open fracture • vascular or nerve damage Late complications • mal-union • delayed and non-union • knee stiffness, secondary arthritis
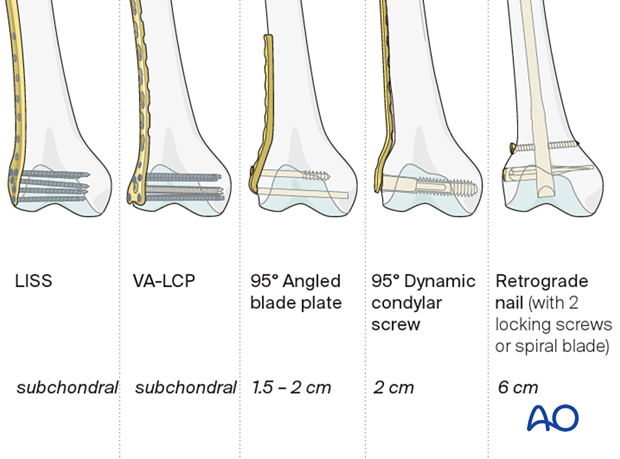
conservative 📷 - undisplaced fracture
Undisplaced fractures are rare and can be treated conservatively, using a plaster cast for six veek, touch down weight bearing six more weeks and progressive weight bearing afterwards.
- ORIF or IMnails
- plate screws
- articular surface → anatomical reduction
🧎🏽♂️Knee and distal lower limb injuries
- direct impact - Fall or dashboard injury
- indirect eccentric contraction of quadtriceps
- patella sleeve fracture 📷 → in pediatrics
- Overview
- patellar sleeve fractures are a rare injury seen in children between 8 and 12 years of age characterized by separation of the cartilage "sleeve" from the ossified patella
- most fractures are displaced and require treatment with open reduction and internal fixation
- Epidemiology
- incidence
- <1% of pediatric fractures
- accounts for >50% of patella fractures in children
- demographics
- more common in males (5:1)
- occurs in children 8-12 years old
- when patellar ossification is nearly complete
- Pathophysiology
- mechanism of injury
- indirect injury caused by powerful contraction of the quadriceps muscle applied to a flexed knee
- pathoanatomy
- separation between the cartilage "sleeve" and main part of the patella and ossific nucleus
- femoral neck fract.
- acetabular fract. post. wall
- knee dislocation
- non-displaced vs. displaced
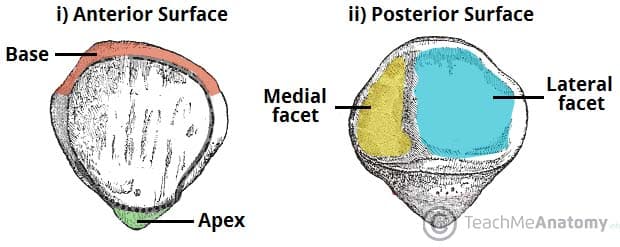
- According to fracture site + no. of fragments 📷
- transverse
- pole / apex
- vertical
- osteochondral (fracture in the facet area; associated with patella dislocation)
- comminuted (stellate)
- unable to extend
- history descripes possible trauma mechanism as above
- abnormal palpation of patella
- hemarthrosis
- retinaculum disrupted 📷
AP. ah ah never never
CT → complication +stress fx
MRI → child with normal xray cant extend

- extension possible
- non-/minimal displaced
- vertical fracture
early ROM if you compare it to ORIF
Casts 📷 (brace + cylinder) + go for full weight bearing
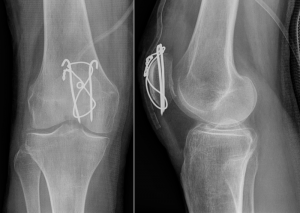
preserve patella whenever possible 🙏🏽
- K-wire complications: migration, ST-compromis
- loss of reduction in osteoporotic bone
- osteonecrosis
- infection if open
- knee pain
- non-union etc
- stiffness
G1: minor sprain, periarticular streched
G2: moderate sprain, ligaments partially torn
G3: severe sprain, ligaments torn
- sprain → lig. injury
- strain → muscle injury
- tear → tendon injury

- classic → pain, swelling brusing
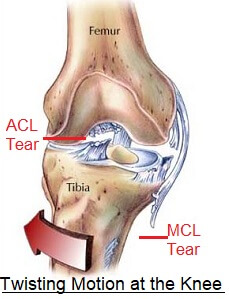
- instability signs:
- Lachman test
- Anterior drawer test
- Pivor shift test
⇒ instability signs for ACL tear:
all of em
xray, US, ct, mri
- associated fracture
- compartment syndrome due to associated fractures
- instability
- stiffness: arthosis, arthrofibrosis, septic arthritis
functional treatment
→ physio + reha
conservative → immobilization
- RICE (Rest, Ice, Compression, and Elevation)
- Orthesis
conservative or surgical
→ usually ligament reconstruction
- old lady with osteoporosis
- wild male 40y (Midlifecrisis) → high energy trauma → motorcycle or sport
- Lateral split - valgus + axial force - young
2. Lateral split + lat. compression - valgus + axial - osteoporotic
3. lat. compression - axial force
4. Medial split or compression - varus or axial - greater forces than before
5. med + lat. split +/- medial + lateral compression
6. med + lat complex fracture , seperated from diaphysis - diverse forces
- classics
- Pain, swelling, bruising
- Deformity, functional impairment
- Crepitus, valgus, varus instability (abnormal mobility)
- Evaluation of the soft tissues to determine whether a compartment syndrome is present
- Neurovascular status
- varus vs valgus instability
50% → meniscus + cruciate lig injury
- displacement 4-10mm
- depression ≤ 5mm
much depressed, much displaced, complications
absolute:
- open
- compartment sy
- vascular inj
relative:
- displaced fractures (bicondylar, medial, lateral) → esp. when joint instability
- joint is not deformed + stable
- Anti-edema → joint aspiration + RICE
- Debridement of open injury
- Fasciotomy in compartment sy
- Traction
- External fixation in closed fract.
noting special
- compartment sy
- neurovascular injury; including DVT
- infections
- swelling wound healing problemds
- stiffness, osteoarthosis
- instability
- angular deformities
- collapse, malunion
crazy lifestyle male 🏍️👱🏽♂️
High-speed lifestyles with motor vehicles, snowmobiles, and motorcycles, as well as the growing popularity of extreme sports, contribute to the increasing occurrence of tibial shaft fractures
- indirect torsional injury → spiral fx
- fibula fx at different levels
- Tscherne grade 0 / I (ST-injury)
- direct → wedge / oblique, comminution
- fibula fx at same level
- ST injury! → Tscherne II/III
- open fx
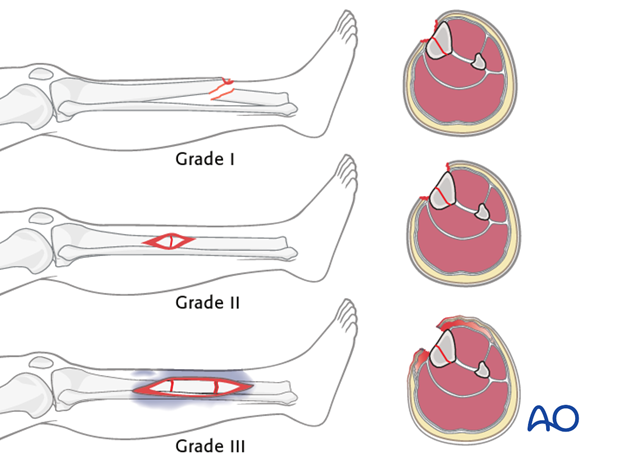
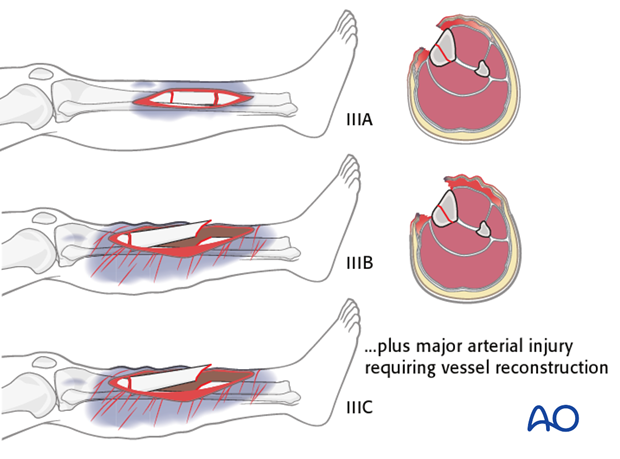
⇒ Oestern & Tscherne classification:
Grade | Tissue Injury ⇒ 📷! |
1 | minimal skin laceration |
2 | skin laceration, local circumferential contusions to muscle/skin, contamination |
3 | extensive skin contusion: major neurovascular damage, compartment syd |
4 | subtotal and complete amputations |
classic
- Variability in the intensity of pain experienced
- Compromised capacity to load-bear on the limb affected
- Manifestations of deformity, aberrant motility, and crepitus are evident
- Incidence of accompanying injuries is notable in tibial fractures
- Evaluation of neurovascular integrity in the affected limb is critical
- Inspection of the overlying skin is warranted
- Vigilance for open wounds or color modifications is necessary
- Gustillo Anderson classification for open fractures
- Type A - Unifocal fractures
- Type B - Wedge fractures
- Type C - Complex fractures
- Each subdivided into 3 subgroups
A=2 fragments, B=3 frag, C= >3frag.
- Xray AP/LL
- knee + ankle must be included
- CT if:
- intra-articular
- spiral distal tibia fx → exclude post. malleolar fracture 📷
- compartment sy
- NV-damage
- open fx
classic
- infection
- non-union
- malunion
- delayed
stable + contraindic for surgery → conservative
>than minimal displaced → surgery → ORIF,CRIF,Ext.fixation
- Conservative management
- Fractures that are stable with negligible displacement
- Criteria precluding surgical intervention
- Surgical approaches
- Open Reduction and Internal Fixation (ORIF) utilizing plates and screws
- Closed Reduction and Intramedullary Fixation (CRIF) with an IM nail
- Provision of stability via external fixation
quick debridement + irrigation within 6hours
→ !incr. infection rates
A pilon fracture, is a fracture of the distal part of the tibia, extending to articular surface at the ankle joint ⇒ if articulation is not involve it's called distal tibial fx
Soft-tissue injury (high energy) 📷
ext. fixation first
- axial forces
- low - high energy → high energy = talus into tibial plafond 📷
→ articular + metaphyseal injuries
- classic fracture signs: pain, deformity, swelling, skin, crepitus, cant bear weight
- enormous blister (bulla) + ST swelling 📷
- ST → necrosis, skin loss, skin infection
- Bony → Pin track infection, Osteomyelitis, Avascular necrosis, malunion, arthritis

- loosening or breaking of metal
- infection
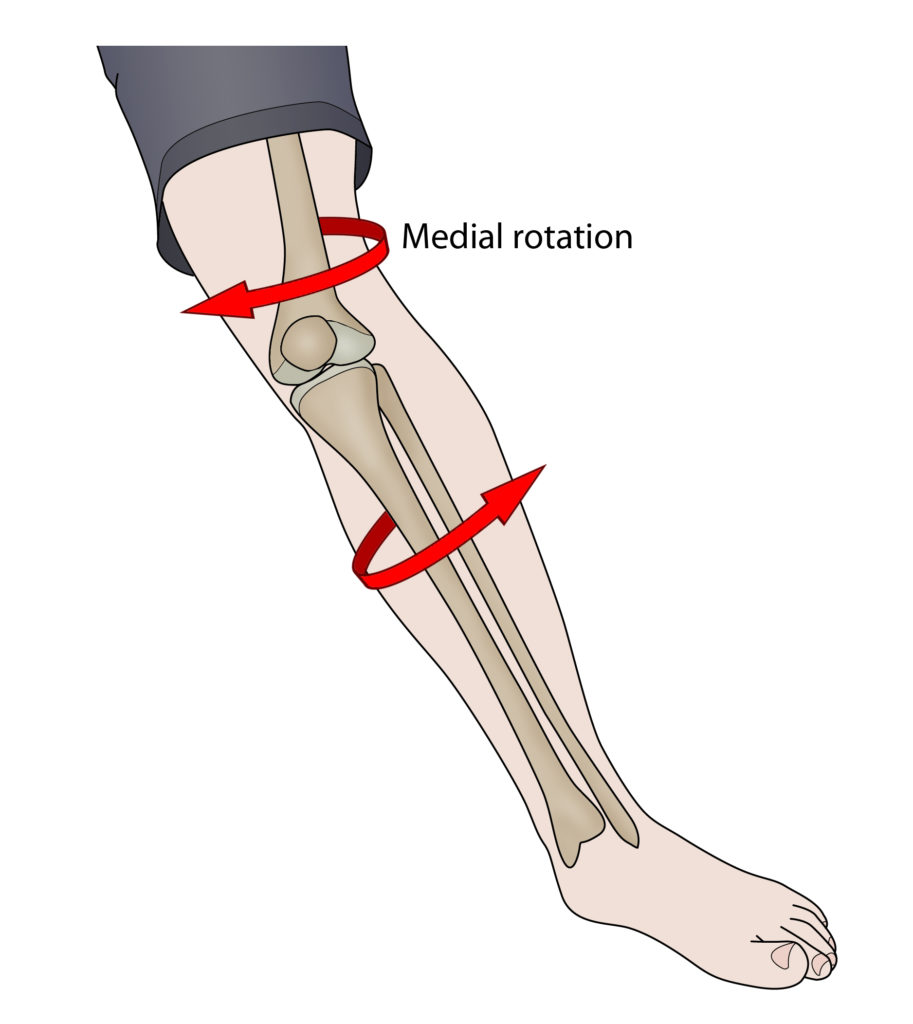
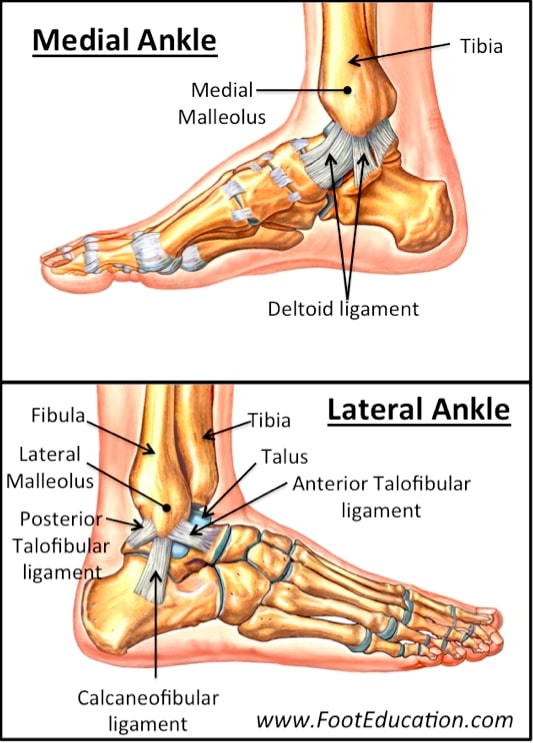
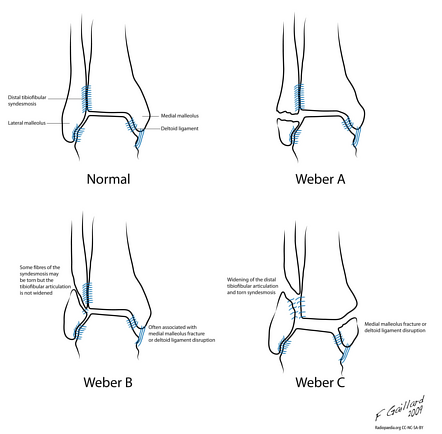
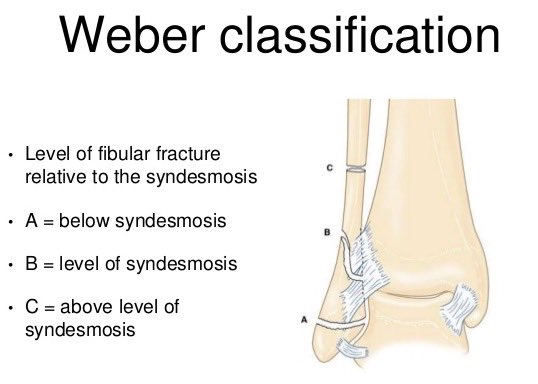
misstep(inversion), sport (eversion), twisting
deltoid lig. 📷
→ high ankle sprain → tibio-fibular ligament
same as knee sprain
- variable - depending on severity
- classic: pain, swelling, buising, redness, warmth, restricted ROM
- instability signs
→ ant. drawer test, talar tilt test 📷
- incr. distance tibia + talus
- incr. dist. tibia + fibula
- associated fractures
- ST-damage
- ankle instability + stiffness (arthritis)
- chronic pain
- swelling
- nerve dysfunction
according to severity could be:
- functional + phsyiotherapy
- conservative: RICE 📷 + orthesis
- surgery: IF
higher forces applied compared to sprains • Vehicle related injuries • Sport related • Indirect trauma (missteps) • Direct trauma (Impact from a heavyweight) • Twisting injury • Stress fracture
classic
- Pain, swelling, bruising, tenderness to touch
- Deformity, functional impairment
- Crepitus, abnormal mobility
- Instability signs (same as sprains)
- Neurovascular status
- Soft tissue damage evaluation
Complications | Early | Late |
Vascular | Vascular injuries | - |
Nerve | Nerve injuries | Nerve dysfunction |
Soft Tissue | Soft tissue damage/swelling | - |
Infection | Infection | - |
Thrombosis | Deep vein thrombosis | - |
Stability | - | Ankle instability |
Mobility | - | Stiffness |
Bone Healing | - | Mal-union |
Pain | - | Chronic pain |
Arthritis | - | Arthritis |
- pain
- anti-edema
- traction
- debridment if open
- external fixation
nondisplaced/minimal displaced isolated med./lat/post
others
- talar displacement/shift
- displaced medial, lateral + post
- bimalleolar + bimalleolar-equivalent
- fracture dislocation
- open
- debridement
- evtl ext. fixation instead of ORIF
👵🏽 Osteoarthritis and bone tumors
Arthrosis
hip, knee, spine
woman after 45
male before 45y
- post-trauma
- avascular necrosis
- mechanical abrasion
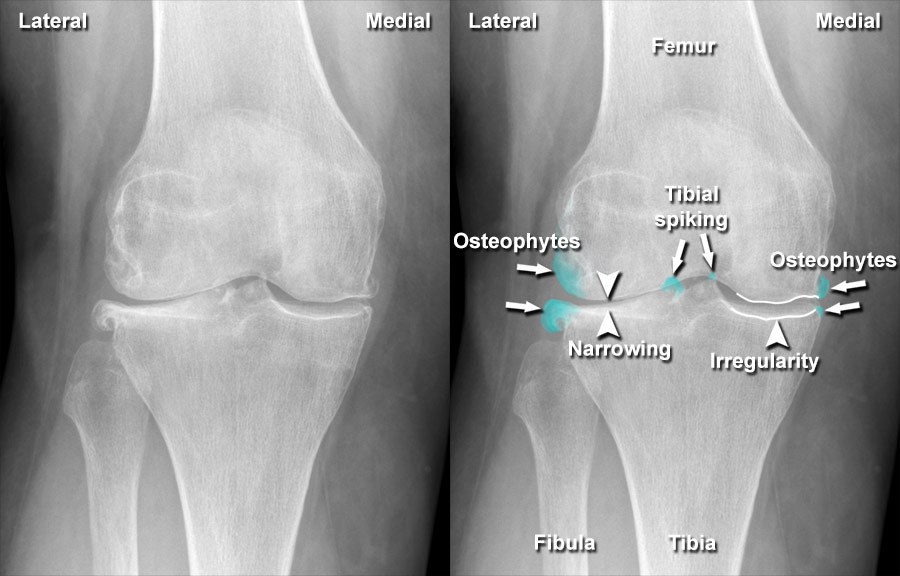
- Joint space narrowing → no ankylosis
- subchondral osteosclerosis, and evtl. osteoporosis
- Osteophytes assymetric
- Cysts
Synovitis → Joint effusion
US or MRI
nope
coxarthrosis 📷
- gradual onset → pain
- functional imparment
- stiffness
- swelling
- deformity
- crepitus
→ symptomatic
- analgesic
- incr. ROM
- inc. muscle strenght
- NSAID
- steroids
- visco supplements

- walking aids
- physical therapy
- life style changes - weight loss..


- DVT
- Infections
- Dislocations + Loosening
- Peri-protetic fractures
- Antithrombotic + AB prophylaxis
- give sufficient fluids
- pain medication
- elastic stockings
- physical therapy
- pain
- mass
- fractures
- abnormal xray
giant cell tumor 📷
chondroblastoma
- ewing sarcoma - young
- histocytosis - adults
- fibrous dyplasia (popcorn appearance 📷)
Metastasis or Myeloma (MM)
Characteristic | Benign Features | Malignant Features |
Margins | Well-marginated | Ill-defined zone of transition |
Reactive Bone Formation | Surrounding rim of reactive bone | Periosteal reactive new bone formation |
Cortical Involvement | Cortical expansion rare | Frank cortical destruction |
- extension 📷
- detection of metastasis
- has actually replaced CT
- size, extend, anatomical relationship 📷
Scinti to determine lesion activity and possible bone metastasis 📷
- Bone forming: osteoid osteoma, bone island
- Cartilage lesions: chondroma, osteochondroma
- Fibrous lesions: nonossifying fibroma, fibrous dysplasia
- Cystic lesions: unicameral bone cyst, aneurysmal bone cyst
- Giant cell tumor
- Chondroblastoma
- Osteoblastoma
- Chondromyxoid fibroma
- Osteosarcoma
- Chondrosarcoma
- Ewing sarcoma
- Multiple myeloma
- Metastatic carcinoma
👶🏽 Pediatric Orthopedics
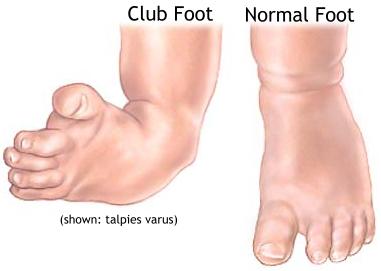
Congenital clubfoot
CAVE
Cavus, Adduction, Varus, Equinus 📷
- stuck in plantar flexion of the ankle
- no dorsiflexion possible;
- contraction achilles tendon
- post. capsule of ankle
medial strucutres of soft tissue are contracted → medial deviation (supination) in horizontal plane
medial rotation in transv. plane → also due to contr. of medial ST
→equinus localized in ankle
→ cavus localized in forefoot
C <130°
A <180°
V <180°
E >90°
calf hypertrophy due to fibrosis
- posterior fold
- medial fold
- skin desquamation
clinical or prenatal ultrasound
- "packing"/positional clubfoot 📷
- neurogenic CF 📷
- arthrogrypotic 📷
- progressive muscular dystrophy CF 📷
- post-traumatic 📷





positional: right after birth contracted, but no fibrosis, etc. returns to normal, is still flexible, resolves spontaneously with stretching sessions
Neuromuscular diseases = increased impulses→hypertonus of the muscles , e.g. cerebral palsy→flexion of other muscles
arthrogriposis = syndromic foot of clubfoot (not idiopathic), multiple congenital malformation in joints
post-traumatic clubfeet, after complex fracture
spina bifida
maternal smoking
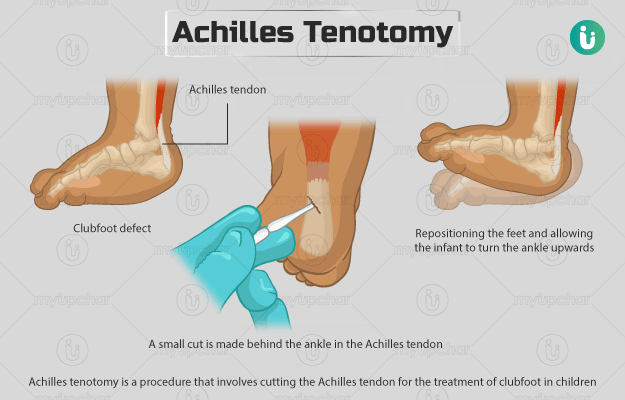
ponsetti
cavus, varus + adduction, then TAT for equinus correction 📷

after 3 weeks of plaster correction of the others → TAT → then 3 weeks plaster immobilization
correction + prevention
Orthoses: Denis-Brown 📷

relapse of treated clubfoot
→FOLLOW UP until growth complete
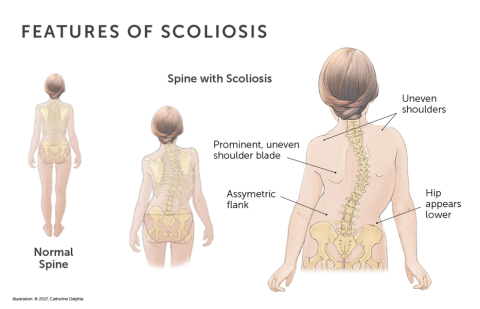
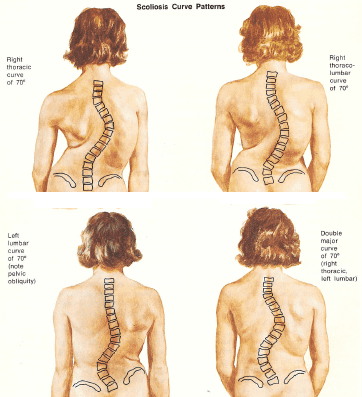
Adolescent idiopathic scoliosis
- lat. deviation of spine
- rotation of vertebra bodies
before puberty, without obvious cause
- hereditary
- environmental (mother >26y)
- intense growth periods → get taller + develop IV disc assymetric → scolliosis → loose height again
- muscular hypertension (not regarding BP, but the muscle tension → pull the spine)
- Neurologic defect (deficient postural control)
- Structural scoliosis: A fixed lateral (sideway) curve of the spine. Structural scoliosis often occurs from unknown factors without reference to other physical problems (idiopathic scoliosis). It tends to affect girls during adolescence. Structural scoliosis can also be part of a syndrome or disease.
- Nonstructural scoliosis involves a temporary change of spinal curvature. This is caused by an underlying condition such as a difference in leg length, muscle spasms, or inflammatory conditions, (e.g. appendicitis), which may produce muscle spasm. Correcting the underlying problem treats this type of scoliosis
Patient erect: double curve (right thoracic, left lumbar)
Bending to left: thoracic curve increased; lumbar curve uncoiled (or reversed), indicating suppleness. Lumbar curve is nonstructural and minor
Bending to right: lumbar curve increased; thoracic curve persists, indicating rigidity. Thoracic curve is structural and major
- structural vs nonstructural
- DD with other scoliosis (esp. congenital → formation, segmentation abnormalities )

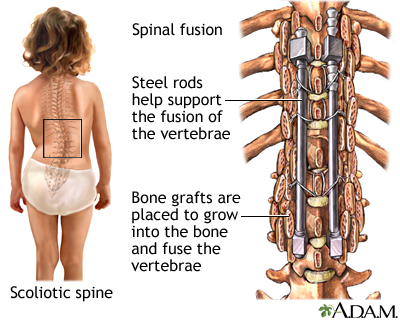
Cobb angle < 25 degrees → observation
corsett 📷, kinesitherapy
up to 50°
Developmental dysplasia of the hip (DDH)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
:max_bytes(150000):strip_icc()/what-is-rice-190446_FINAL-5bc5fcebc9e77c005135258d.png){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
secondary anatomical changes due to hip development deficiencies
- Morphological developmental changes are harmonious, hierarchized, and synchronous and start at the embryonic age of 4 weeks to 15 years.
- At the age of 8 weeks, the first cartilage model of the joint appears.
9:1 F/M
🤦🏽♀️
- genetic: Down-Sy, Turner sy, 43% in monozygotic twins
- mechanical: small uterus, abnormal fetus position, postural drainage
- Vitamine A + Folic Ac.
- Toxins: teratogenic substances + pesticides
Femoral head dislocates out of acetabulum ⇒ disproportionate growth → Østable joint
LABRUM, LIGAMENTUM TERES, & TRANSVERSE LIGAMENT HYPERTROPHY → SOCKET BECOMES "MORE SHALLOW" → FEMORAL HEAD does NOT FIT
- unequal leg lenght
- asymetric skin folds
- osteoarthrits
- waddling gait + limping
{kind=link}
performed in dorsal decubitus, 90° knee+hip, now ADDUCTION! → femoral head will exit posteriorly = dislocation → positive: dysplastic hip!
{kind=link}
normal hip
US, until the 4th month
{kind=link}
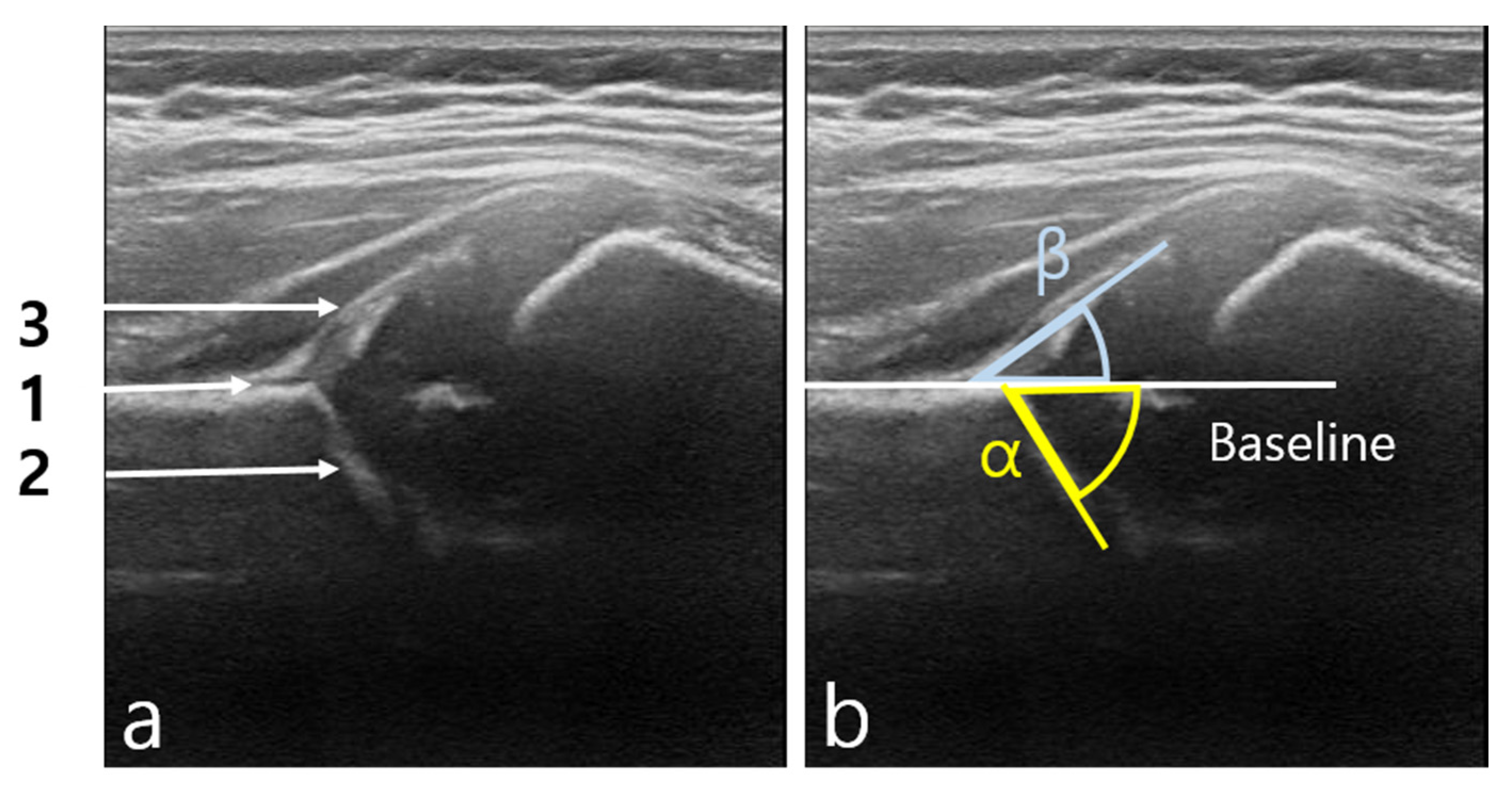{kind=link}
{kind=link}
alpha: between ileum + bony acetabulum roof
beta: betw. ileum + cartilagineous acetabulum roof
Dysplasia if:
alpha <60°
beta >55°
⇒ less stability of the femoral head in acetabulum
Stability:
⇒ the smaller alpha → the less place for the femoral head in the bony acetabulum
⇒ the bigger beta → the less is the femoral head hold in place by the cartilaginous acetabulum
- Cartilaginous covering line - from the apex of the acetabular bone through the labrum
{kind=link}
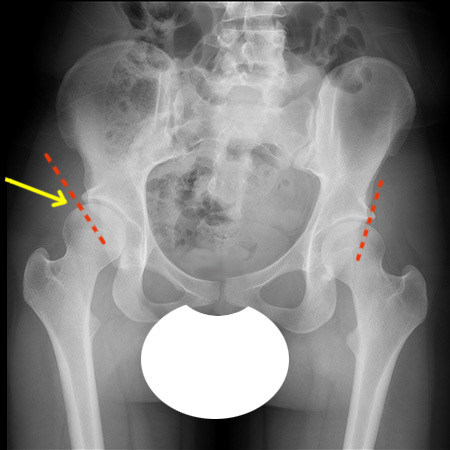
abduction devices 📷
{kind=link}
- aseptic necrosis femoral head
- coxa vara (x-legs) 📷
- osteomyelitis
- osteoporosis
- stiffness
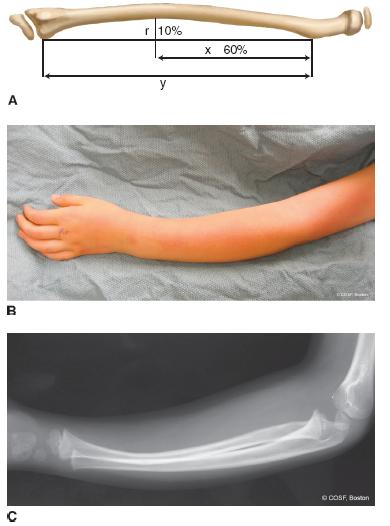
Fractures in children
{kind=link}
{kind=link}
- girl: 14-15 y
- boys: 16-17y
higher! tendons+ligaments are really elastic in children
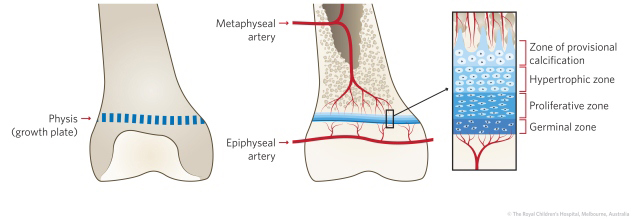
→ prone to growthplate fracture
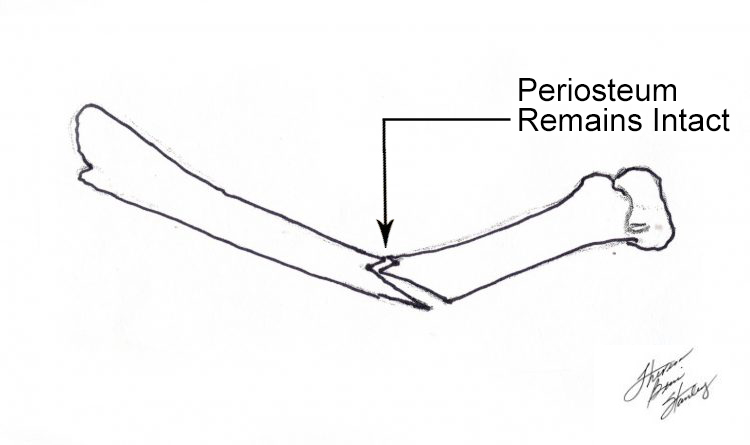
really thick
- stabilized the fracture
- helps in callus formation
- the younger the child, the better the autocorrection capacity (optimal: <8 years)
- Doesn't work when already full grown
- fertile growth plates are better: femur , tibia, prox. humerus, distal. radius
{kind=link}
{kind=link}
- bony crepitus
- abnormal mobility
- palpation: discontinouty of the bone
- Non-transmission of movement in distal distal
classic
- shock signs
- local trauma sign: St swell, edema, ecchymosis
- shortening + deformation of limb
- NV-lesions
- according location: diaphysis, metaphysis, growth plate, epiphysis
- complete / incomplete
- fragments / fracture ligns: wedge, spiral etc. (see below)
- open / closed
bending/compression → obliques fracture → brakes first on the convex side
direct force → transversal
spiral
high indirect force → wedge/3 fragment fracture
high direct/indirect → comminuted
- outside to inside (!infection)
- inside to outside
{kind=link}
{kind=link}
{kind=link}
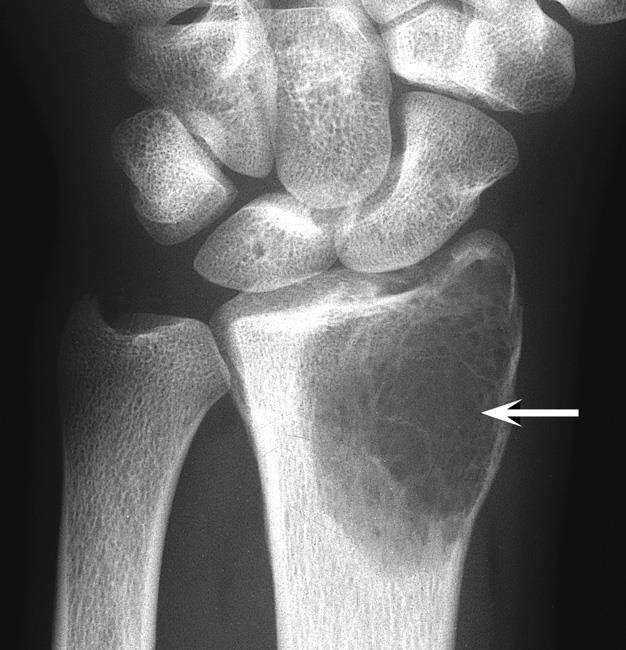
compression mechanism, fall on hand (i.e.) → compression of the bone → compression fracture (no fracture line)
Turn into complete fracture due to another fall
{kind=link}
- pain in forearm
- interior + exterior curve
- xray → incr. curvature but no fracture line
When an angulated longitudinal force is applied to a bone, the bone bends. Pediatric bones have a degree of elasticity and therefore, if the force is low and subsequently released, the bone returns to its normal position and no lasting evidence of that bowing is seen radiographically.
If the force is greater than the mechanical strength of the bone, the bone undergoes plastic deformation and when the force is released, the bone remains in its bowed position.
Microscopic examination of the bone reveals that there are microfractures along the concave border of the bowed bone, but these are not visible radiographically.
microscopic examination → microfracture
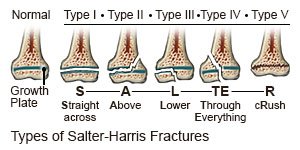{kind=link}
{kind=link}
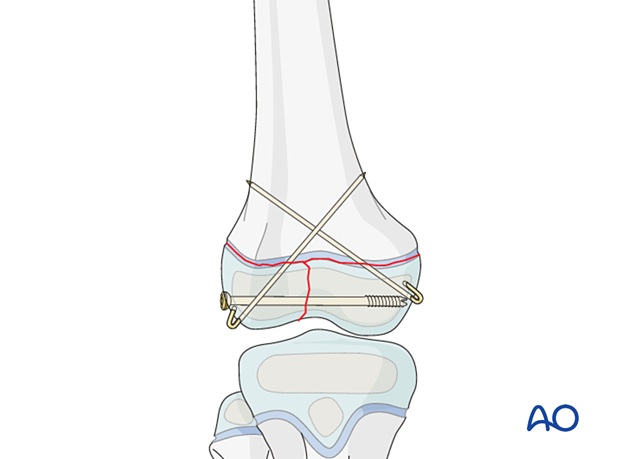
⇒ Surfical treatment: internal fixation → osteosynthesis for type 3+4
they are intraarticular type 3+4
RESTORE CONTINOUTY OF ARTICULAR CARTILAGE
no treatment might cause post-traumatic arthritis
→ other types (1,2,5) are treated orthopedically
xray
uS → newborns fx, superficial bones fx
CT: intraarticular fx, pelvis fx
MRI: spine fx
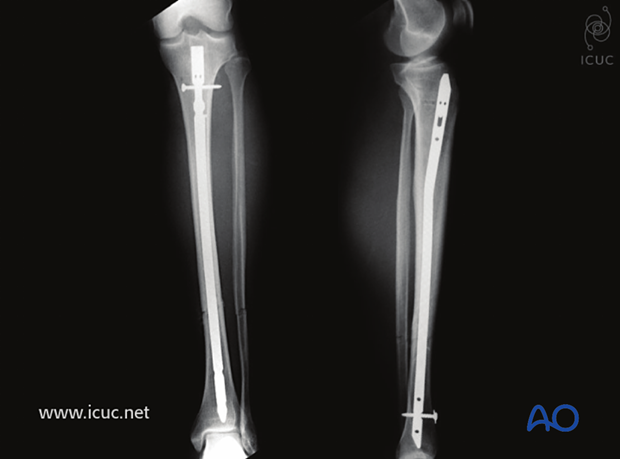
- usually orthopedic in children
- non-displaced → immobilize in plaster cast, xray → check if not compressed
- displaced → reduction (closed or open), than immobilization with plaster cast or osteosynthesis (surgical internal fixation)
- use anesthesia
- immobilize distal + proximal joint
- sometimes also more → femur fracture: also immobilize ankle joint
{kind=link}
{kind=link}
{kind=link}
classic
- NeuroVasc-lesion + compartment
- open fx
- osteomyelitis + osteonecrosis (femoral head)
- growth problems → esp. growthplate fx
- compartment
- late: mal/non-union + stiffness