
Table of content
- Medical Imaging
- 🏴☠️ Conventional GI Radiology
- 🔊 Ultrasound in digestive pathology
- ⚛️ CT in digestive pathology
- 🧲 MRI in digestive pathology
- ☢️ Nuclear medicine
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6

Medical Imaging
🏴☠️ Conventional GI Radiology
- assessment of movements of GI-T
- post-op assessment Morphology+dynamic
- chronic GI-T diseases
- !perforation
- !occlusion
- recent GI-hemorr, acute digestive D, pregnancy
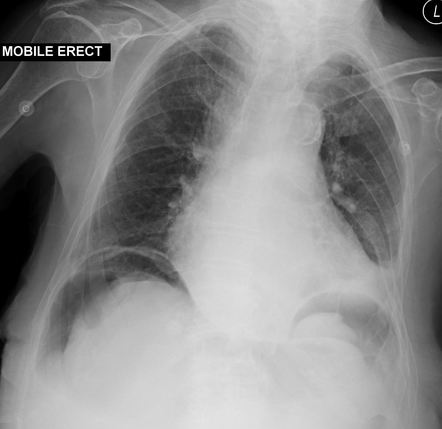
- Pneumoperitoneum
- Before contrast! → performation or obstruction??
- suspected contraindications for contrast xray: Bowel perforation, Bowel occlusion → diff. mechanical + paralytic → where is the mechanical obstruction?
- quick diagnosis of perforation or obstruction
- othercomplication
air → expands subdiaphragmetic 📷
cholecystitis, apendicitis, Ulcer, pancreatitis, diverticulitis
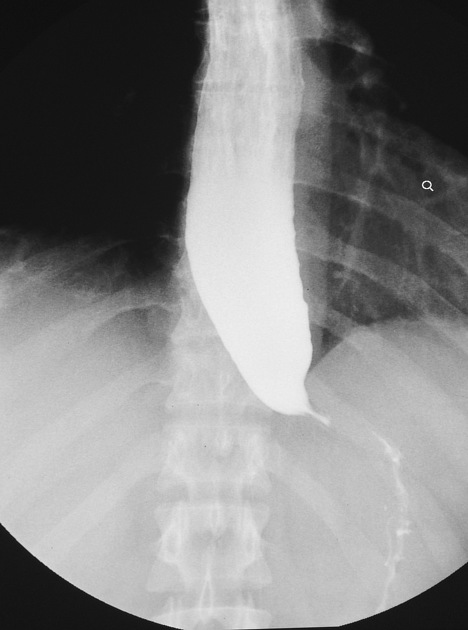
failure to relax of LES, hypertonic at rest
no primary persistaltic waves in lower 2/3
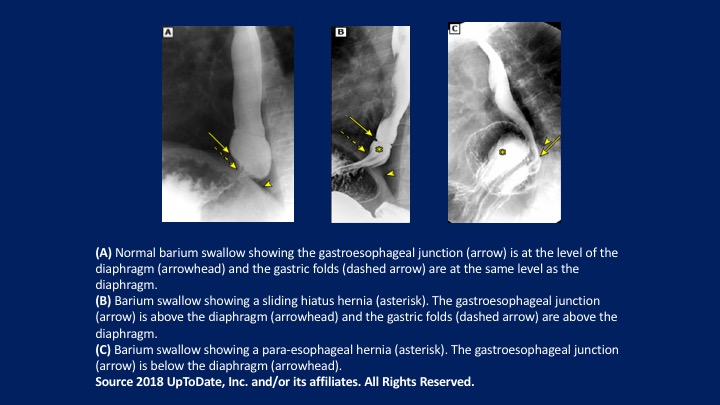
- bird beak appearach
- no gas bubble in stomach
- dilated esophagus (megaesophagus)
- lengthenic of the esophagus
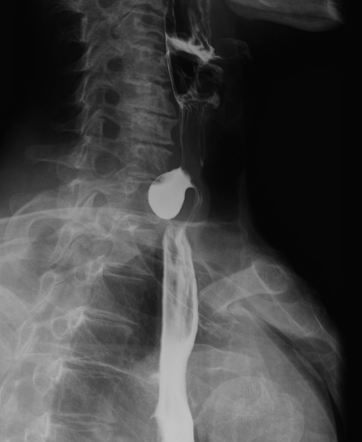
Features | Benign Stenosis 📷 | Malignant Stenosis 📷 |
Relation with the long axis | Axial, symmetrical | Usually excentric |
Junction with the normal esophagus | Progressive, smooth tapering | Abrupt, "overhanging margins" |
Length of stenosis | Spreads in length | Usually under 6 cm in length |
Contour of stenosis | Esophagitis = irregular initially; later = regular | Irregular, can contain ulcerations and lacunar images |
Localization | Above a physiological narrowing | Anywhere |
Suprajacent dilation | Always present, depends on duration | Light or Moderate |
Number of stenoses | Unique, rarely multiple | Unique |
Criterion | Benign Gastric Ulcer 📷 | Malignant Gastric Ulcer 📷 |
Localization | Lesser curvature (vertical) | Antral region |
Size | Under 1 cm | Over 2 cm |
Shape | Round/oval | Irregular |
Contour | Smooth | Irregular |
Convergence of Folds | The folds converge till the border of the ulcer (benign relief) | The folds end abruptly at some distance from the ulcer (malignant relief) |
Structure | Homogeneous | Inhomogeneous |
Relation with the Gastric Border | Passes the gastric border | Doesn’t pass the gastric border (embedded ulcer) |
Depth | More deep than wide | More wide than deep |
Carman Ulcer | Absent | Characteristic for ulcerated cancer |
Hampton Line | Present 📷 (thin, sharp, lucent line that traverses the orifice of the ulcer) | Absent |
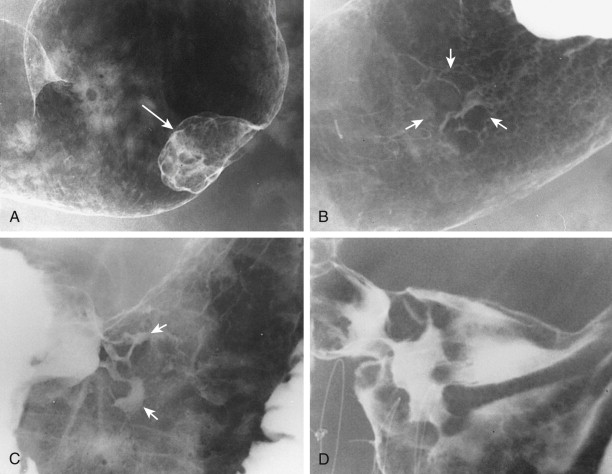
ulcerated, polypoid, infiltrative (+fungating)
infiltrative = linits plastica (=”leather bottle”, “scirrhous CA”) 📷
Characteristic | Malignant Stenosis | Benign Stenosis |
Relation with the Stomach Axis | Axial | Eccentric, towards the lesser curvature |
Length | Long | Short |
Contour | Irregular, rigid walls | Smooth, flexible walls |
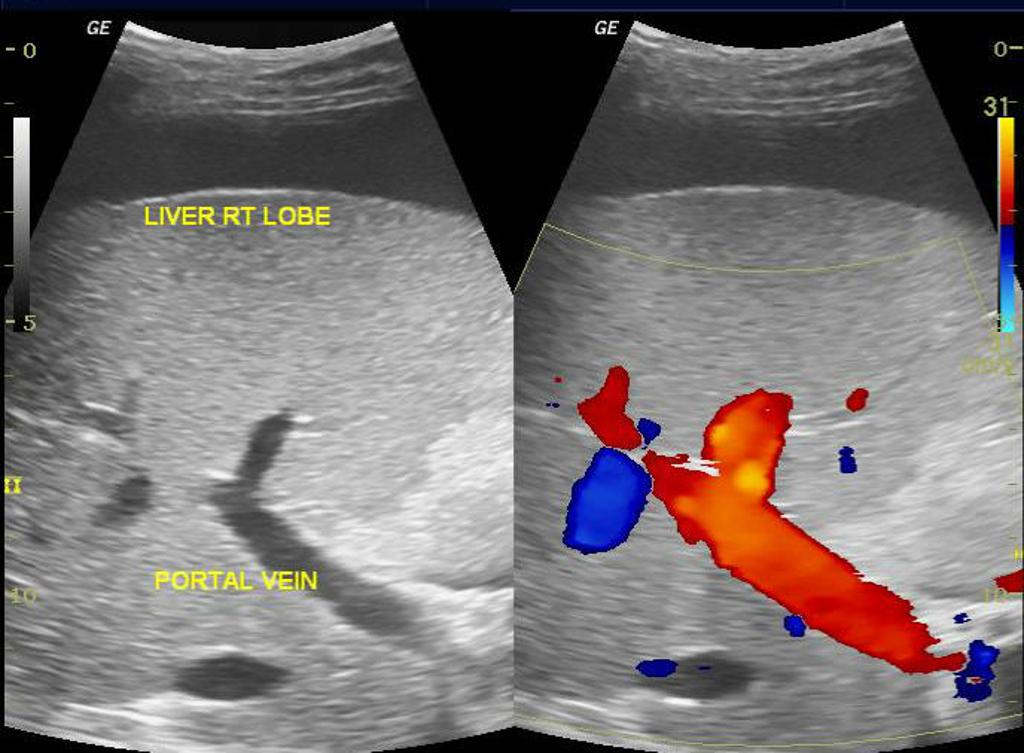
🔊 Ultrasound in digestive pathology
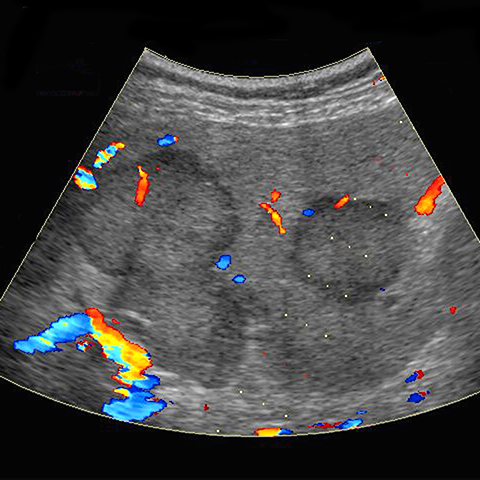
- red towards
- blue away
- green turbulent
vascularization without directiong
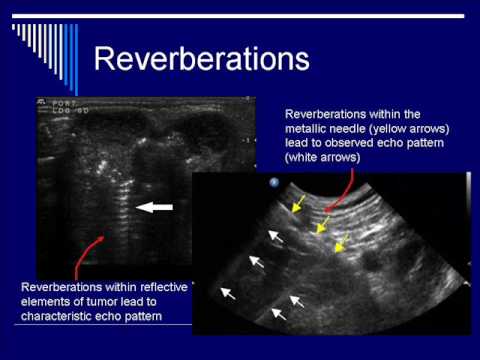
vibration of the transducer destroy the liphophilic layer of the contrast
- other things then vessels/capillaries are not filled(necrosis, cyst,..),
- vessel in a lesion are filled slower then in the normal parenchyma
no, eliminated by respiration
how strechable is tissue?
prostate cancer
right/middle/left hepatic vein
No doppler signal 📷
- inc. echogenicity (compare kidney)
- rounded borders (irregular margins)
- hepatomegaly (exceed upper liver pole)
→ may lead to fibrosis → cirrhosis
Chronic hepatopathy does not have a specific ultrasound aspect. In patients with chronic viral hepatitis B or C infection, hepatic steatosis is a frequent histological finding, occurring in more than 50% of cases.
The ultrasound findings in chronic hepatitis include:
- Hepatomegaly (the lower border of the liver exceeds the upper pole of the kidney).
- Steatosis (increased echogenicity of the liver compared to renal parenchyma).
- Liver with rounded borders.
- Increased diameter of the right lobe of the liver (normally less than 16 cm).
These findings suggest developing fibrosis and may indicate the possibility of malignant transformation, such as hepatocellular carcinoma.
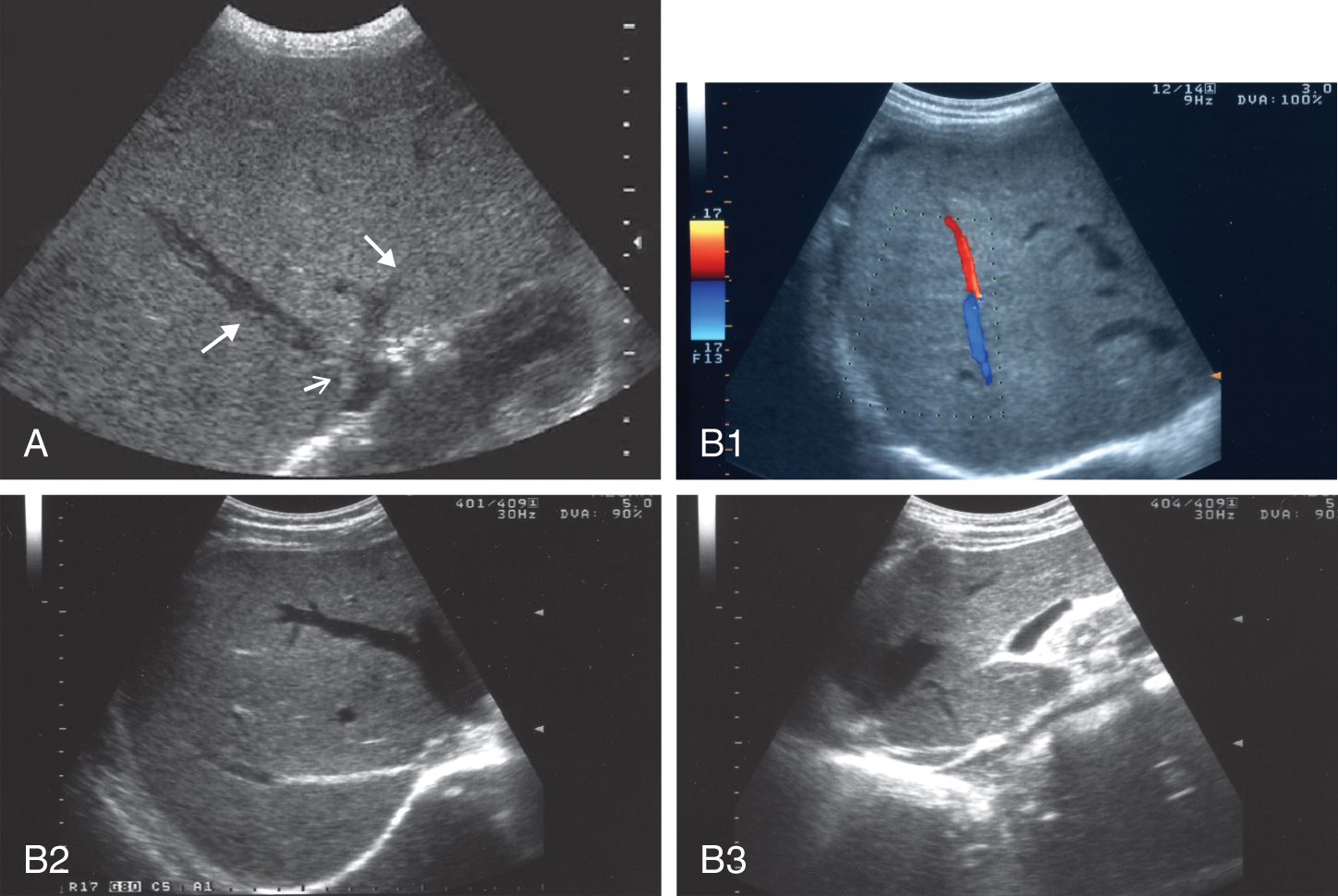
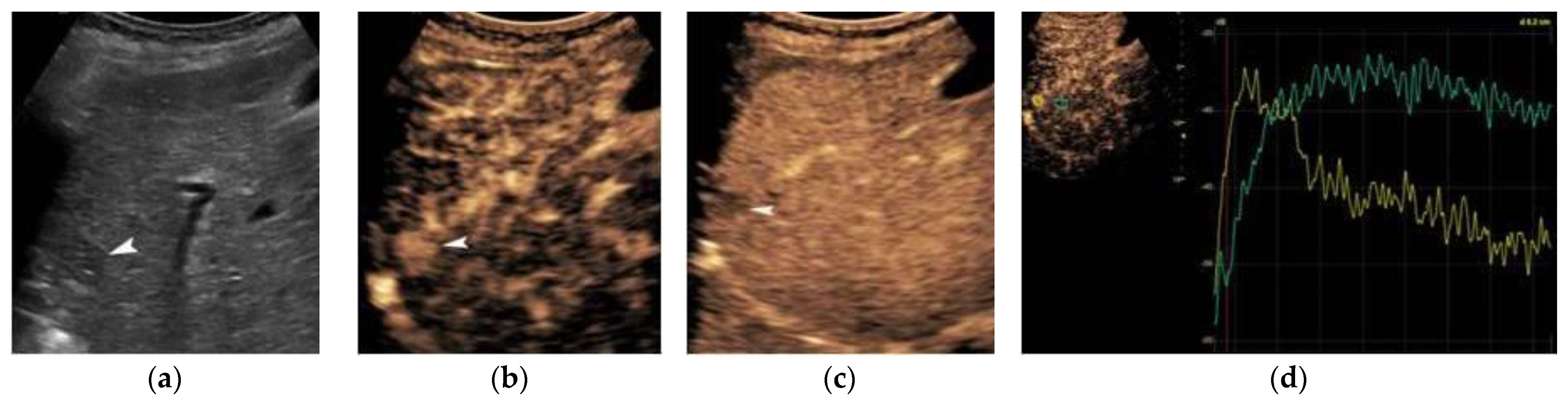
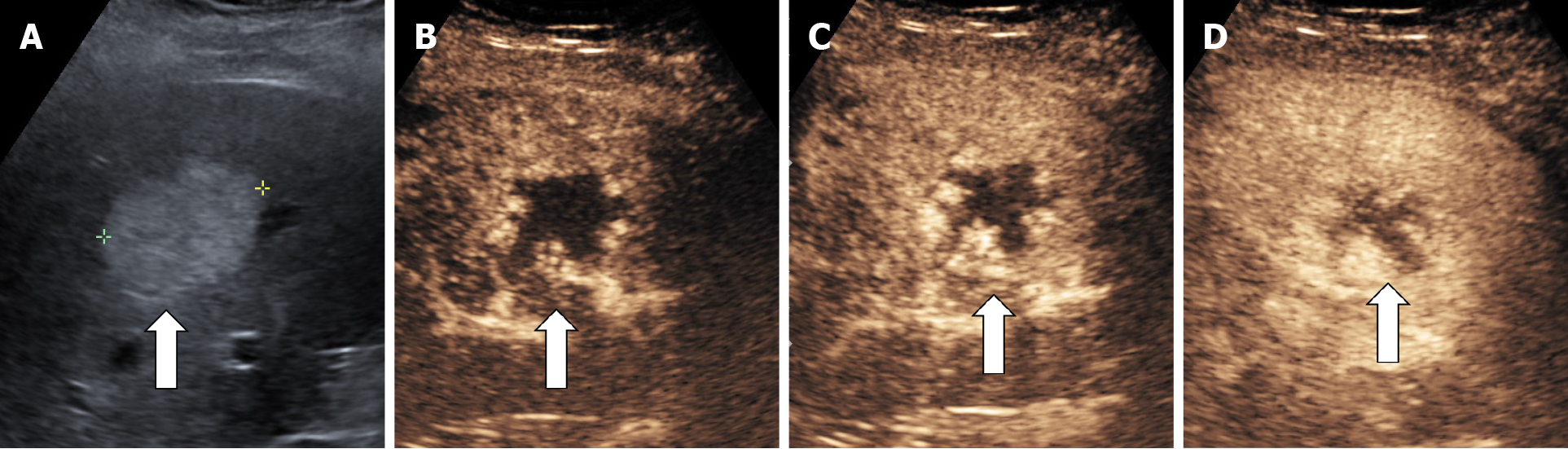
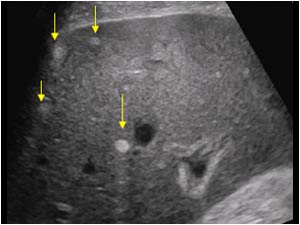
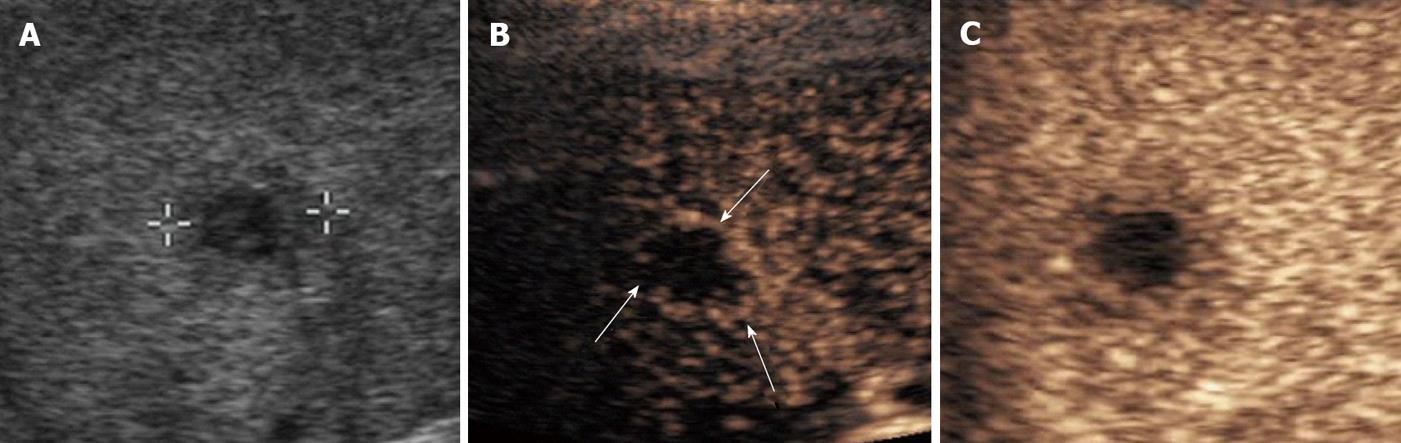
hepatocellular carcinoma
Contrast (CEUS)→ HCC has a lot of blood supply
- arterial: early enhancement
- portal: parenchyma enhanced as well
- later: wash" out
- enhances early → than quick wash out
HCC=early enhancement
cirrhotic nodule=enhanced together with liver parenchyma
normal blood clot doesnt have blood supply
HepC , Alcohol
- liver becomes more echogenic → no portal vein differentiation possible
- portal veins are usually differentiated due to their hyperechoic walls, → no differentiation possible
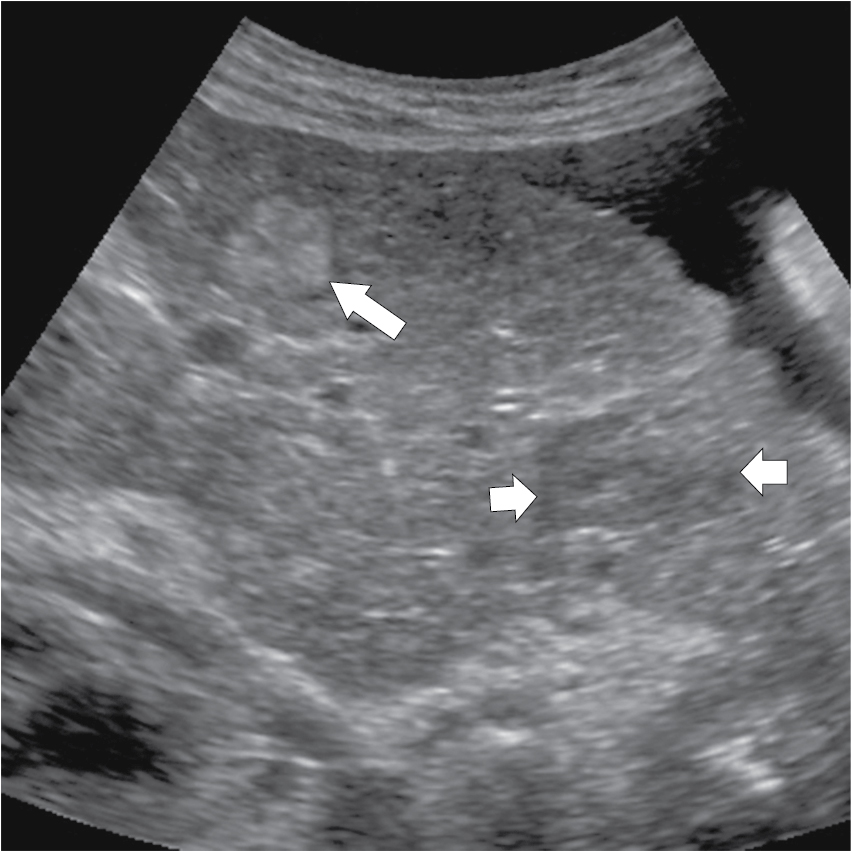
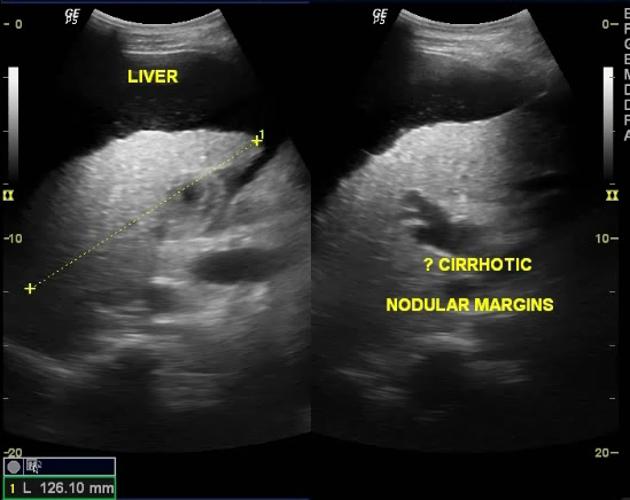
- heterogenous ecotexture (nodular micro/macro),
- +/- attenuation(due to fibrosis),
- no good deliniation of vessel (compression by the nodules),
- nodular contour/irregular margins,
- hepatomegaly or atrophy(when fibrotic tissue contracts)
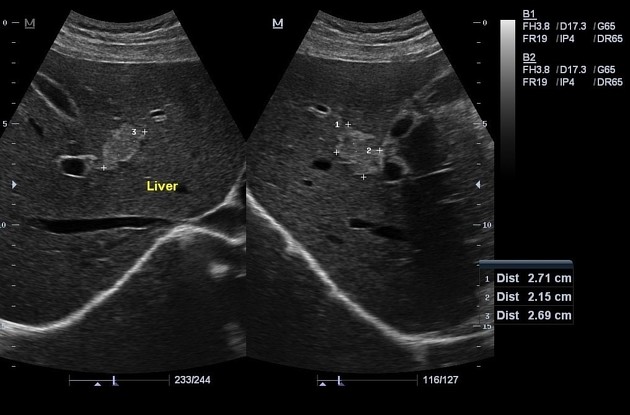
- Portal HT (portal vein enlargement >12mm 📷, collaterals dilated)
portal HT / enlargement(>12mm)
- Inhomogeneous Echotexture: Normal liver has a fine, ordered appearance which is disturbed in cirrhosis, becoming irregular with mixed echogenic dots.
- Nodules: Presence of both micro-nodules (less than 3mm) and macronodules (greater than 3mm). The latter are regenerative nodules that are benign and have a well-defined appearance similar to the surrounding liver tissue.
- Surface and Architecture Changes: Irregular and nodular liver surface along with a loss of normal vascular structure within the liver.
- Liver Lobe Changes: Atrophy of the left and right lobes and hypertrophy of the caudate lobe are common in advanced cirrhosis.
- Portal Hypertension: Evidenced by an enlarged portal vein and reduced speed of blood flow within it.
- ascitis
- atrophy
- irregular, nodular, inhomogenous
- portal HT → HSM, porto-systemic shunts, ascitis

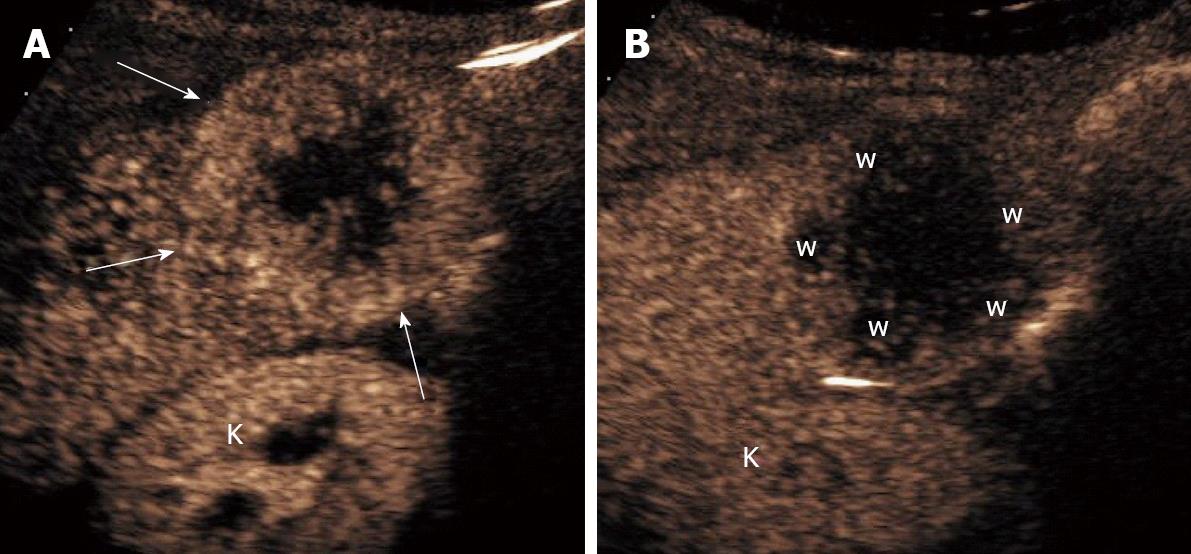
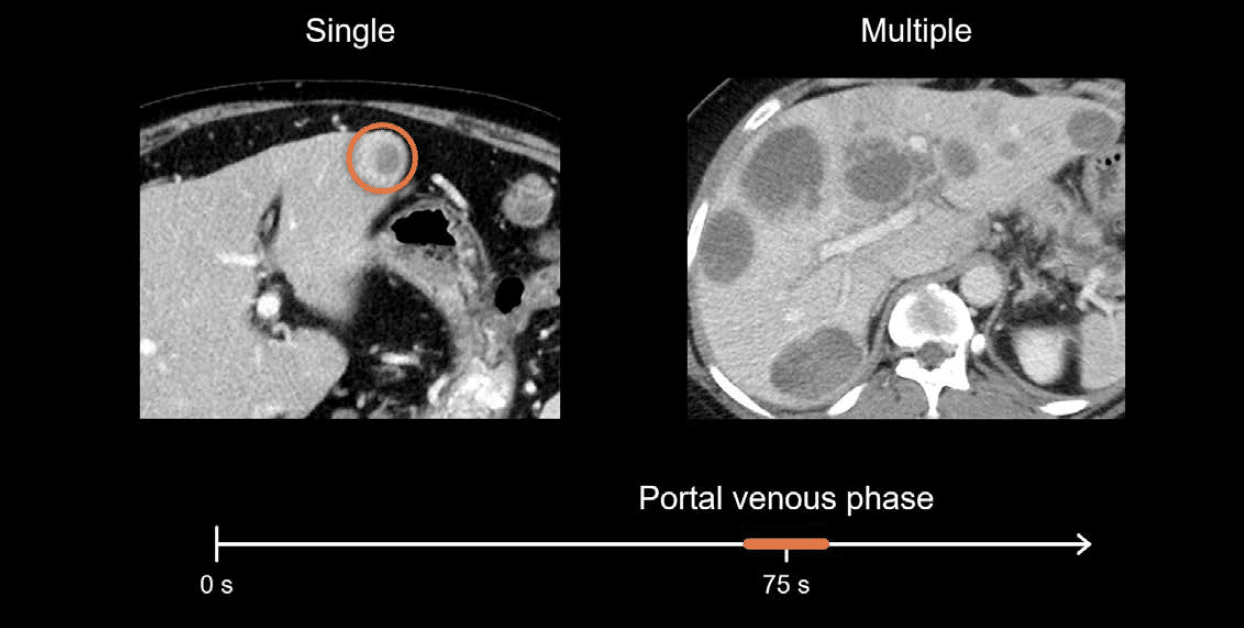
metastasis! → complementary exam needed
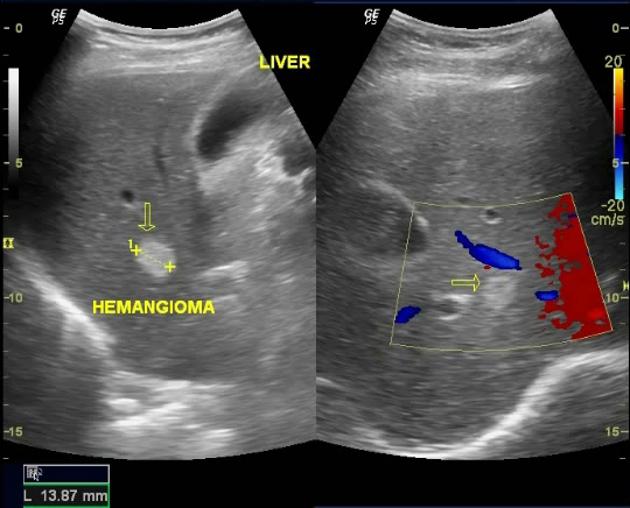
rim enhance in portal/late phase (no washout → see video)
from periph → central region
regular periph. enhancement;
→ DD: metastasis

- large, heterogenous, poorly defined hyperechoic mass
- +- tumoral thrombosis
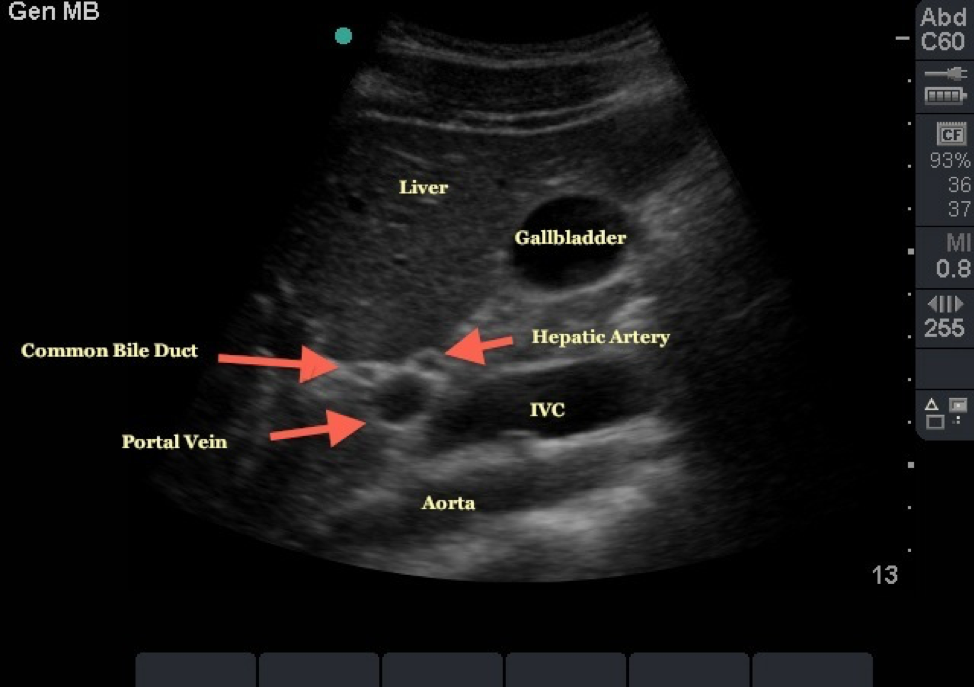
- swollen walls→"double contour sign"
- wallthicknes 4-10mm
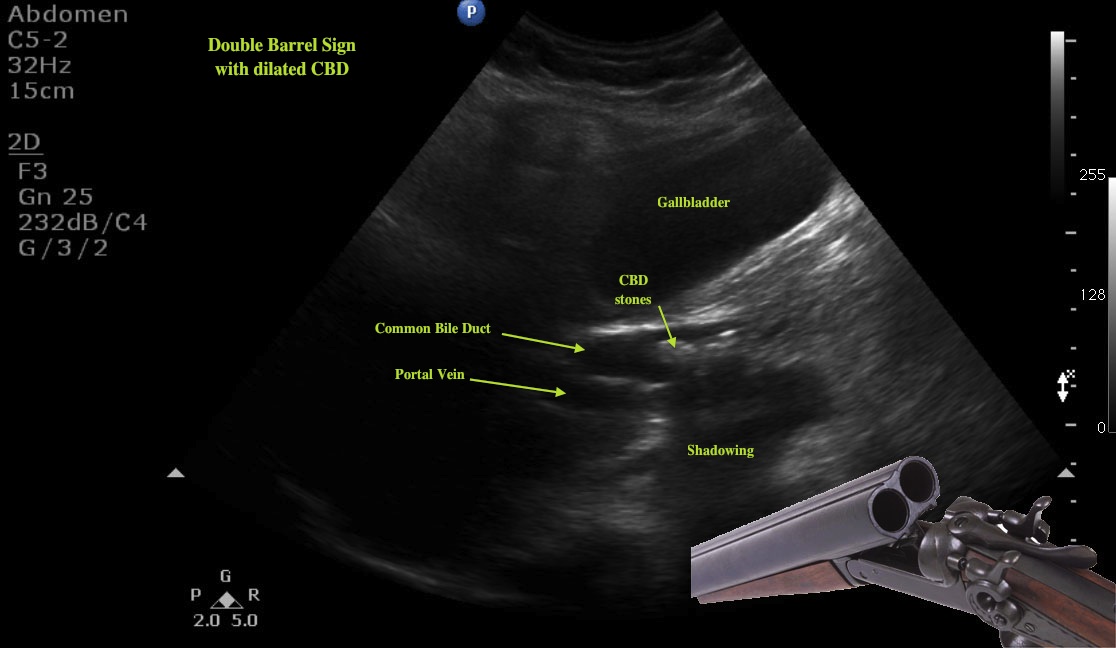
- stones withing lumen (w/ post. shadowing)
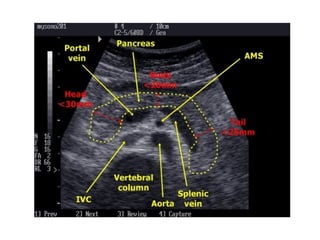
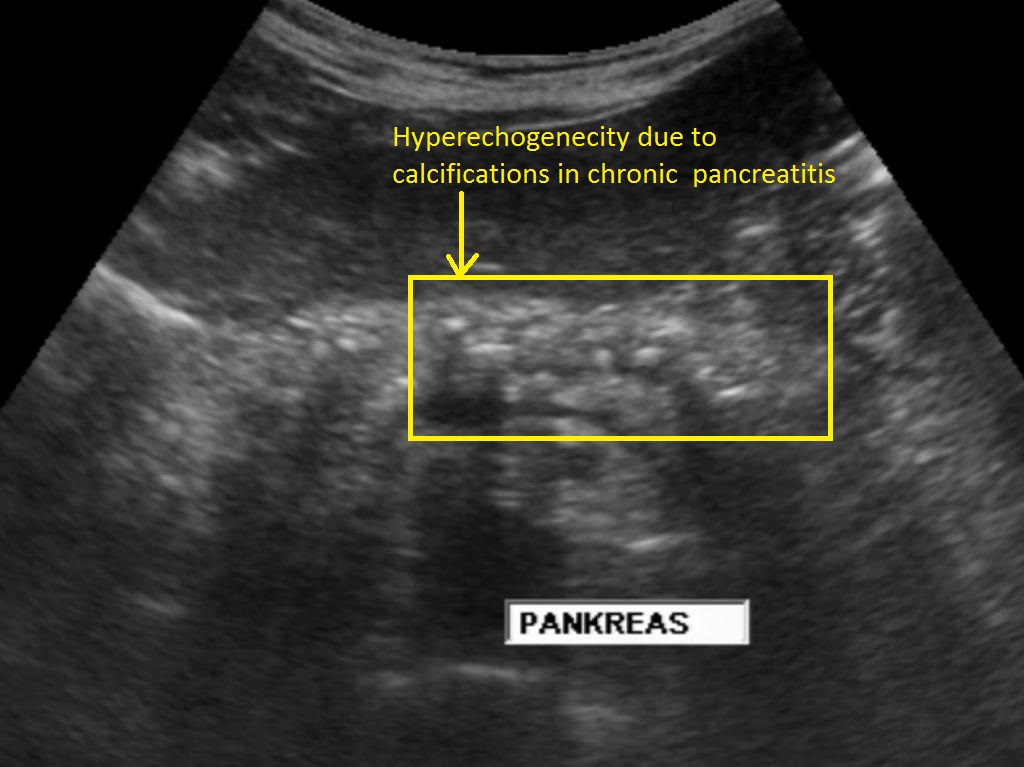
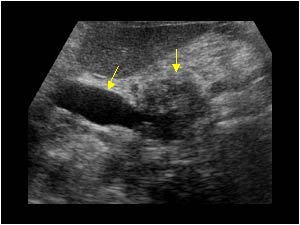
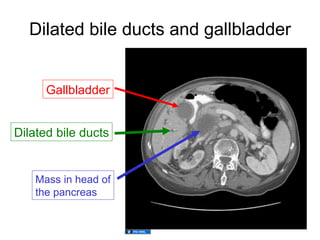
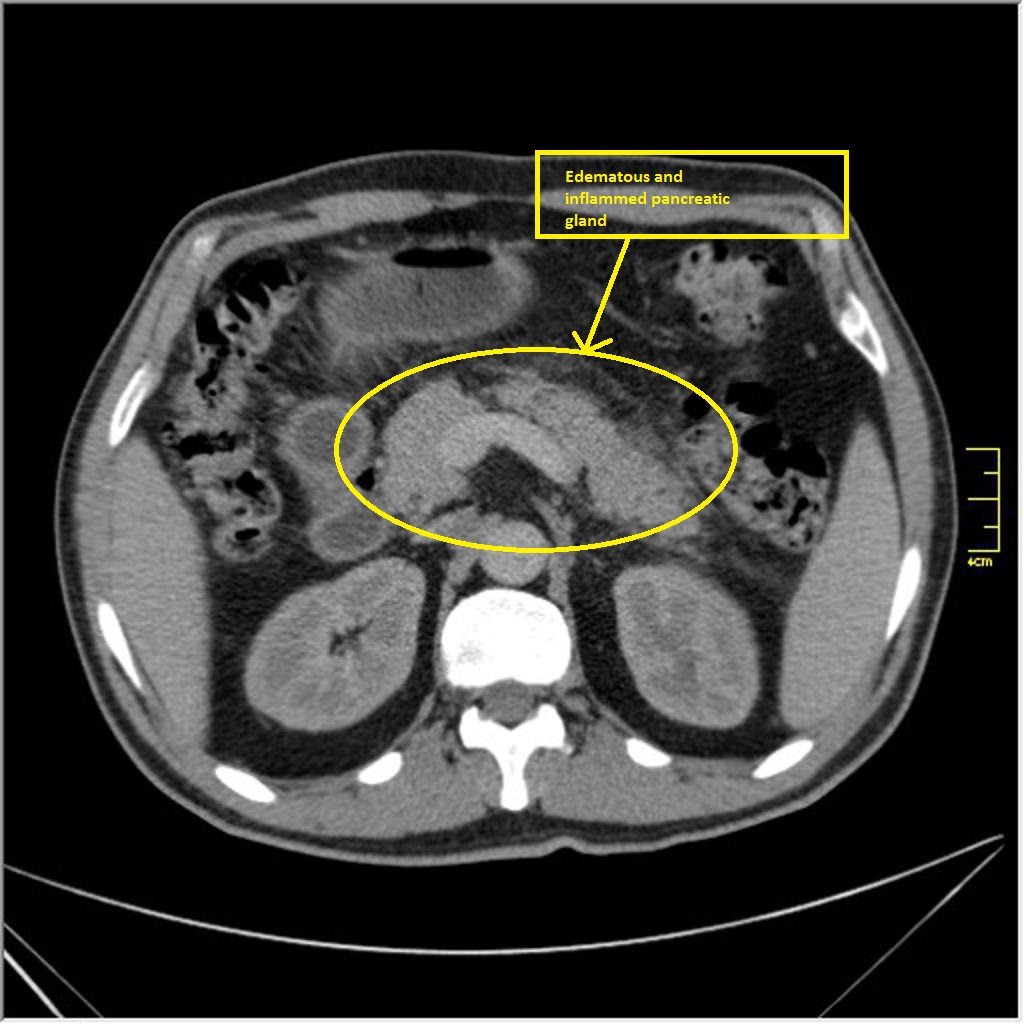
- enlarged
- more hypoechoic than normal (edema)
- irregular borders
- peripancreatic fluid → spread through peritoneum
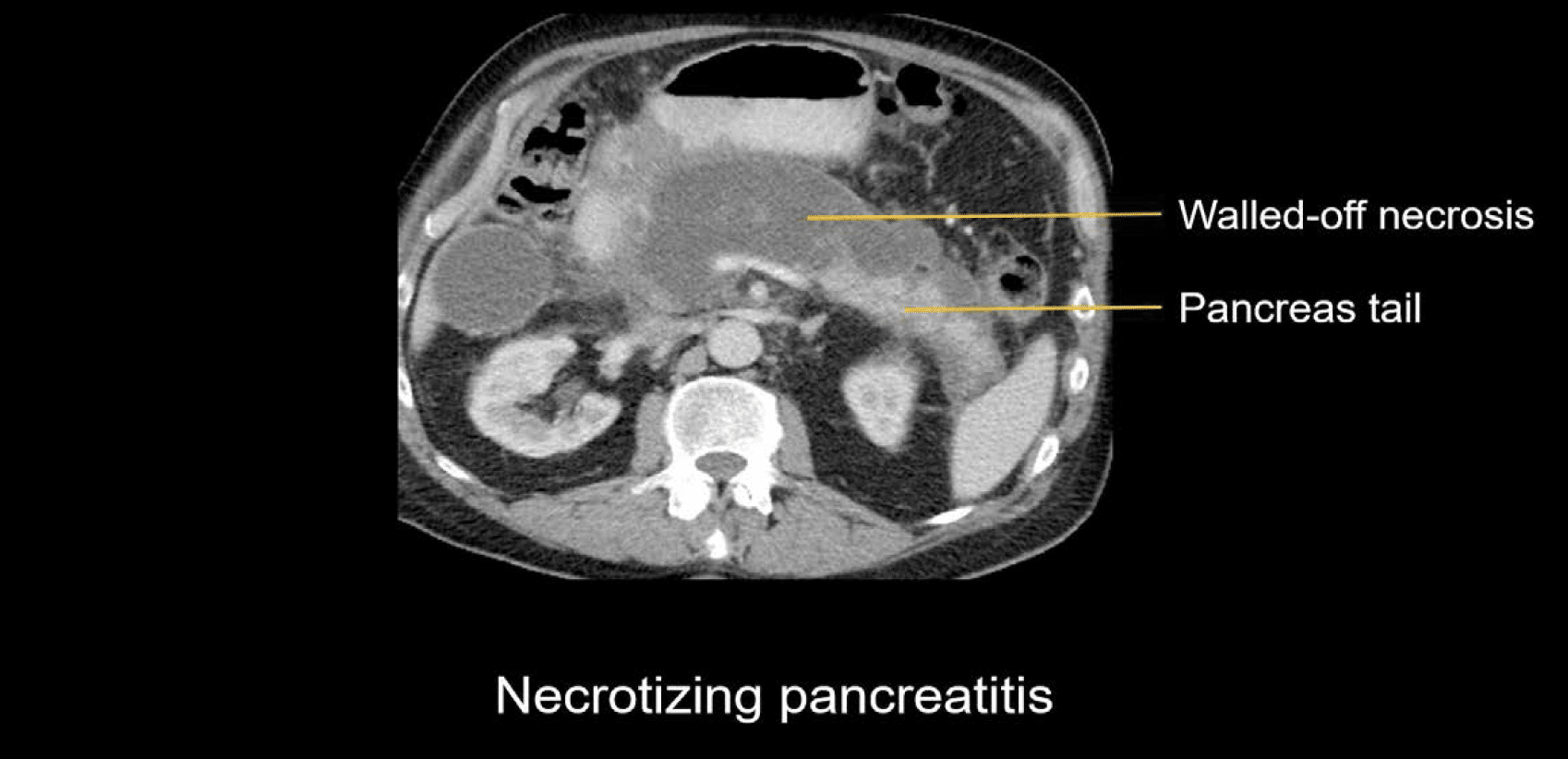
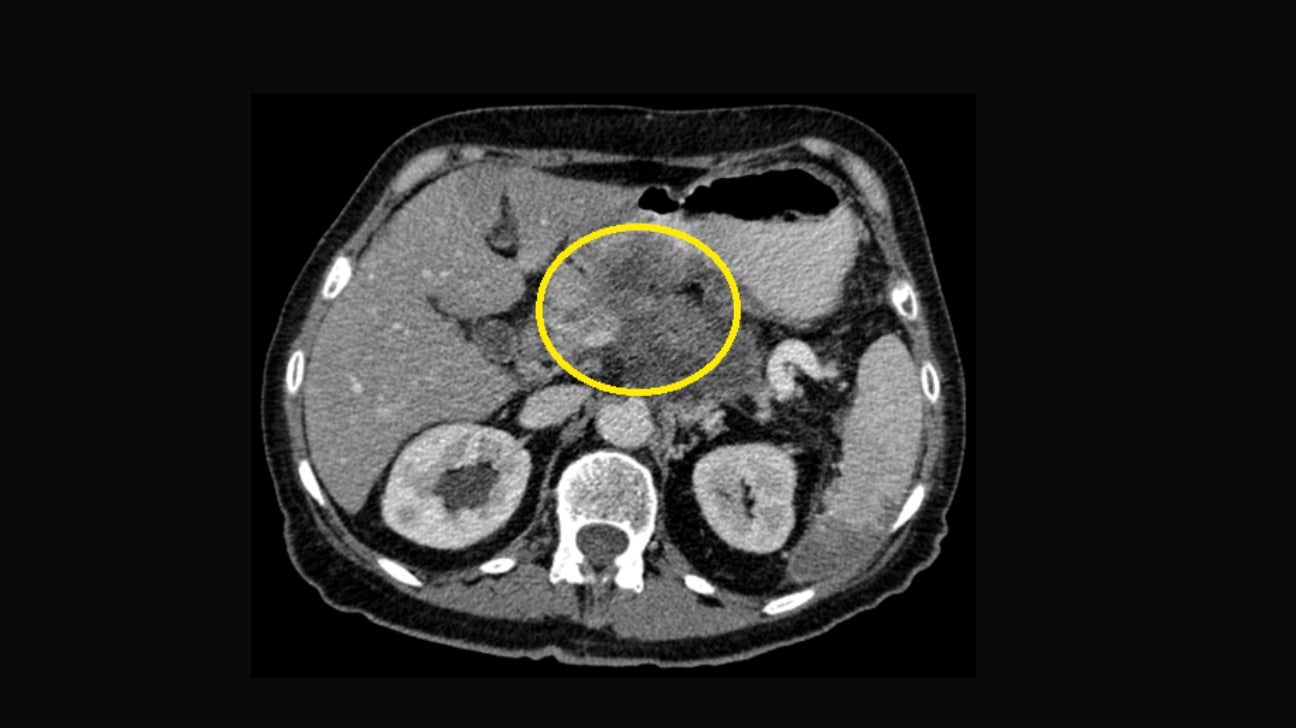
- due to pancreatic enzymes (after episode of acute pancreatitis)
- well deliniated
- debris inside (hyperechoic debris inside)
- rim hyperemia on DOppler
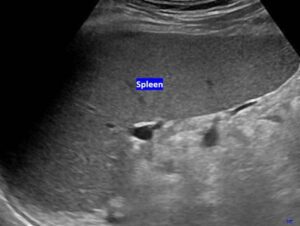
- The liver appears homogeneously moderately echogenic, resembling the sonographic appearance of the liver.
- It is slightly smaller and more echogenic, with a more homogeneous texture.
- The splenic vessels are not visible within the splenic parenchyma.
- Long axis above 12-13 cm
- Short axis over 6 cm
- The spleen becomes larger than the left kidney
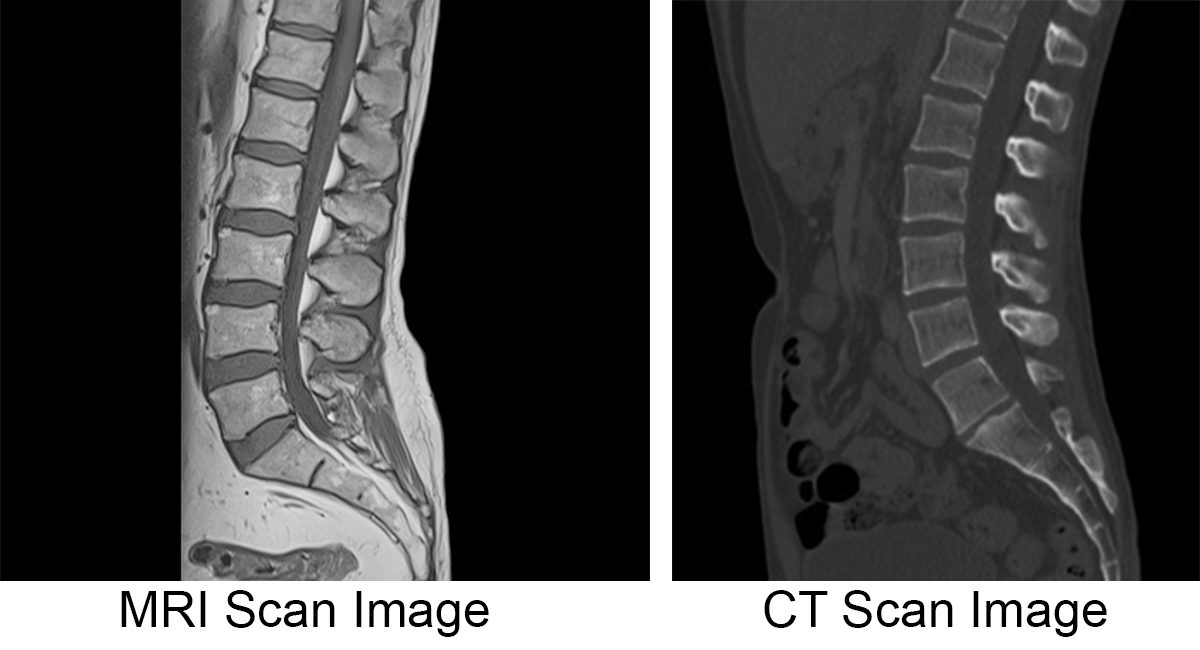
⚛️ CT in digestive pathology
not really, doesn't really display the chronic characteristics (like the eco texture you can see on US)
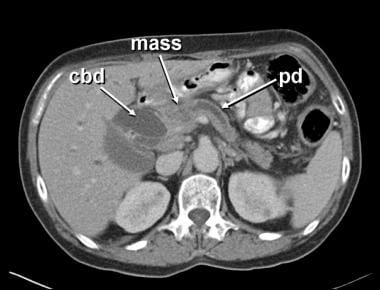
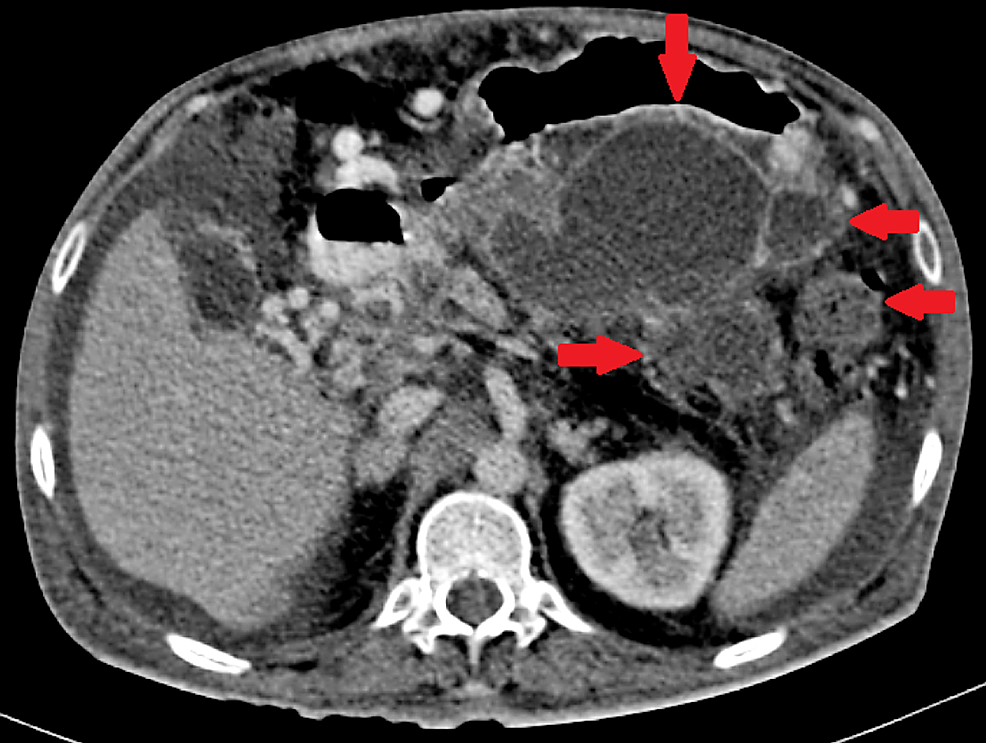
- cyst vs. solid ⇒ content = water or living/necrotic tissue
- contrast enhancement



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
endoscopy
give osmotic agents (Fortrans)→ pulls water into bowel → natural contrast (hypodens)
i.v. contrast → hyperdens walls
fortrans in the evening before → water enema on CT table
{kind=link}
{kind=link}
{kind=link}
→ rather use colonoscopy
{kind=link}
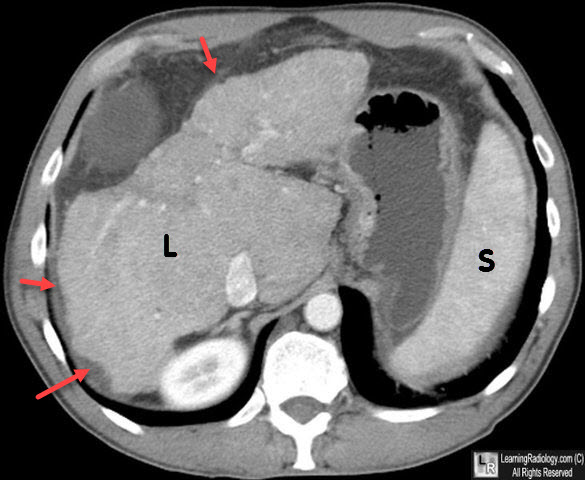
- trauma → hematoma?
- cirrhosis, acute hepatitis,
- infectious diseases
- hematologic disorders
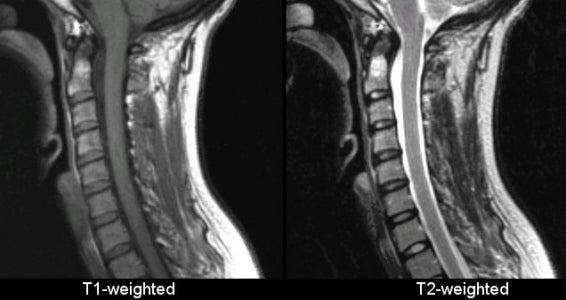
🧲 MRI in digestive pathology
{kind=link}
{kind=link}
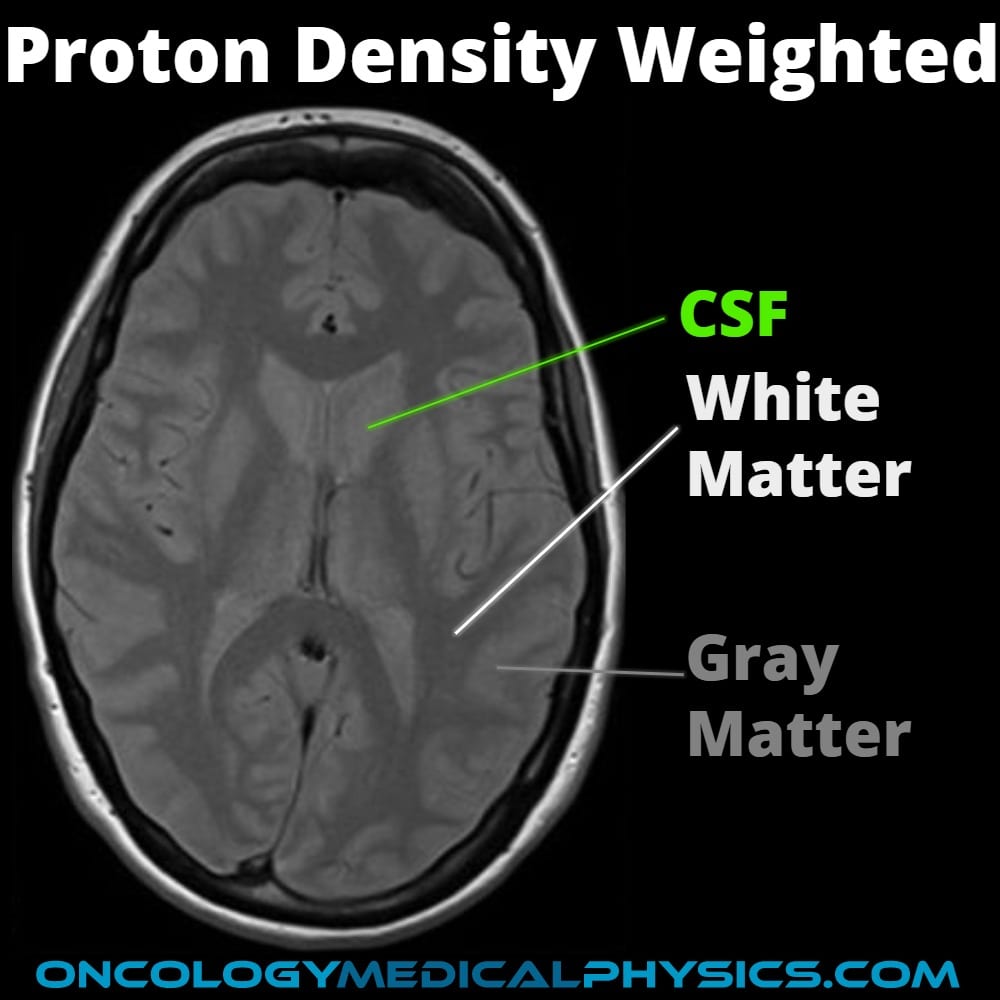
muscles are very dark on T2 (due to high iron contect),
fat is only less hypersignal than water but more hypersignal than muscles tissue
![[📷]](https://www.researchgate.net/publication/352362398/figure/fig3/AS:1034125062447104@1623566036656/Axial-images-of-lower-extremity-MRI-A-Axial-T2-weighted-image-T2-TSE-RST-TRA-showing.png){kind=link}
{kind=link}
HYPOINTENSE
also no signal is send back because it is moving
- Contrast (in T1)
- Subacute hematoma (both)
- → becomes darker as the hematoma becomes older
{kind=link}
{kind=link}
- vascular extend evaluation
- Uptake time (higher uptake + quicker washout in malignant lesion)
- extrahepatic diseases
Gadolinium
→ Hypersignal T1
→ Hyposignal T2
kidney → nephrotox
ARTERIAL PHASE
T1: compare to portal vein: cancer: early uptake; biliary metabolism: later uptake
early uptake → disproportial vascularization compared to portal vascularization
normal biliary metabolism take contrast up after 10-20min, malignancies → low bililary metabolism → very dark after 20min
{kind=link}
{kind=link}
{kind=link}
2-5min
gradually loses contrast
- Hemangioma → "wash in" begins here
- HCC → arterial early enhancement; inhomogeneous "wash out" hyposignal (in venous +late phase)→ evtl. with capsular hypersignal
- Cyst → no contrast uptake at all (compare to fluid in CSF)
- Adenoma → native T1: dark, Contrast → early uptake
- Focal nodular hyperplasia: Hyperintense in arterial phase with black scar tissue inside
- Metastasis: Hypersignal halo surrounding hyposignal lesion in arterial phase
- Abscess: Septa, fluid, necrotic tissue → no strong enhancement; compare also clinical picture
Fe (iron)
hyperintens on T2
dg of malignant metastasis → hypersignal on T2 [📷]
![[📷]](https://pubs.rsna.org/cms/10.1148/rg.296095515/asset/images/medium/g09oc20g10b.jpeg){kind=link}
Primovist
hyperintense
no → CT mainly
similiar to ERCP but MRCP is not invasive
magnetic resonance coleangiopancreaticography
ONLY FLUIDS ARE WHITE, everything else is black
→ bile duct obstruction
{kind=link}
biphasic → T2 hypersignal content with dark walls 📷 (pic “A”)
☢️ Nuclear medicine
functional (regarding metabolism)
- We are continously exposed to radiation → Bananas, cosmic, terestrial (radon)
- Nuclear medicine doesnt equal nuclear clouds
- it is less ionizing than CT
Spontaneously→ to form stable configurations Radioactive decay is a random and spontaneous nuclear process in which an unstable parent nucleus transforms into a more stable daughter nucleus through the emission of particles or gamma rays.
gamma rays
{kind=link}
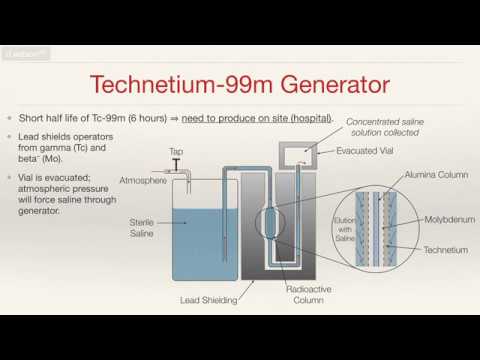{kind=link}
- labeled with radioisotope (Techneticum)
- Are organ specific
- Tc-99m-DTPA (diethylene-triamine-pentaacetate) = renal; dynamic
- Te-99m-DMSA (dimercaptosuccinic acid) = renal; static
- Tc-99m-MDP (methylene diphosphonate) = bone
- is a beta and gamma emmiter
- because of its beta emmision, it is now seldom used diagnostic studies(whereI-123)is prefered) and is mainely used for therapeutic indications
Gamma-camera 📷
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Different parts work together to provide images of a variety of organs, using a wide range of radiopharmaceuticals.
- Detectors contain collimators and a sodium iodide crystal that scintillates when gamma or X-ray photons interact with it.
- A scintillation is a flash of light.
- Photomultiplier tubes convert light into energy and amplify the signal.
- The signal is sent to a computer.
- This information is manipulated by electronics in the detector and the controlling computer to generate the image we see.
- The scintigraphic image is the spatial distribution of the radiopharmaceuticals at the organ or system level.
{kind=link}
{kind=link}
Static: one picture after certain time (after reached max conc in target organ) → morphological (esp for scarring)
dynamic: multiple pic after 5,10,15sec,.. → functio-morphological 📷
{kind=link}
The different types of acquisitions used in medical imaging are as follows:
- Dynamic: These acquisitions are performed sequentially, capturing a series of images over a period of time. This allows for the visualization of physiological processes or the uptake and distribution of radiotracers in real-time.
- Static: These acquisitions involve capturing planar or whole-body images at a single time point. They provide a snapshot of the radiotracer distribution in the body, allowing for the detection of abnormalities or changes in specific areas.
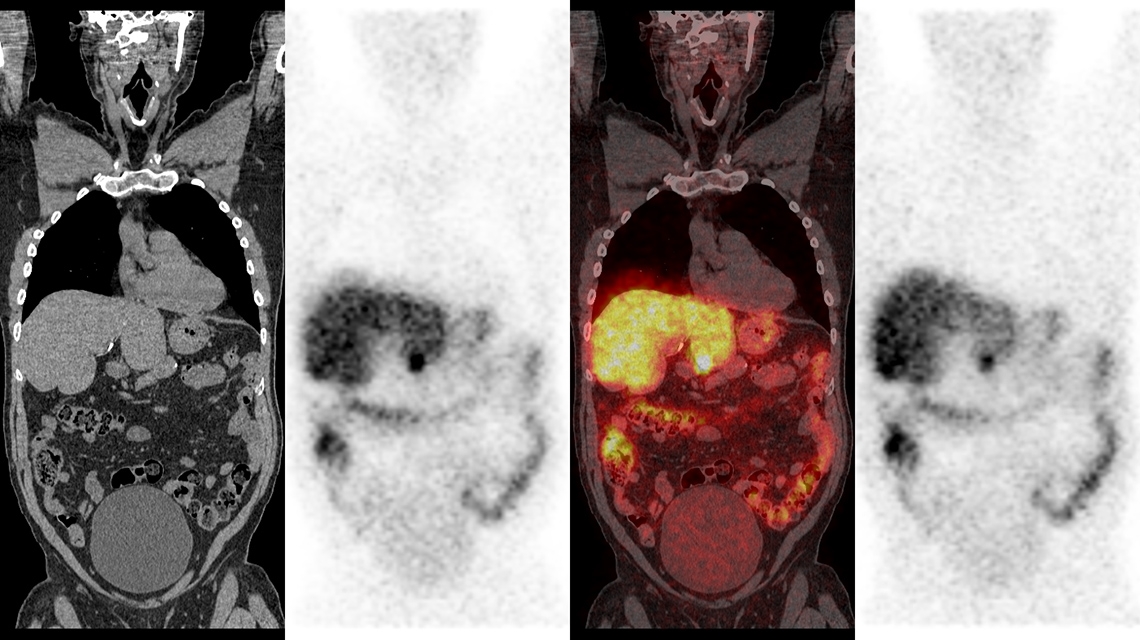
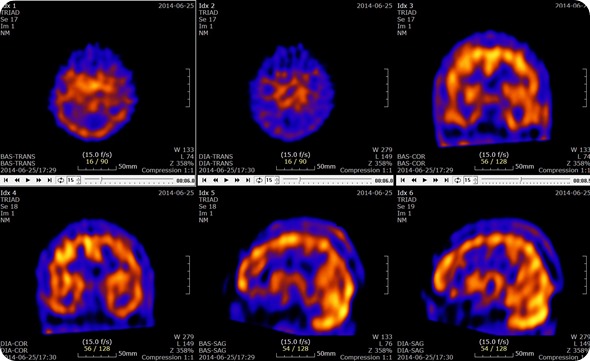
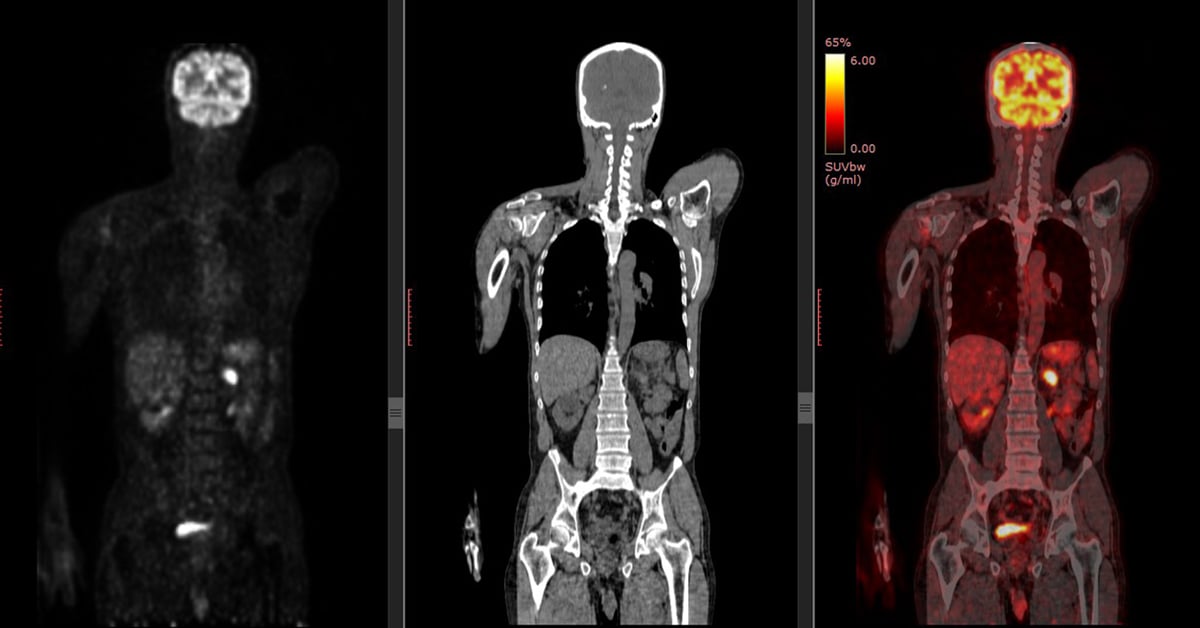
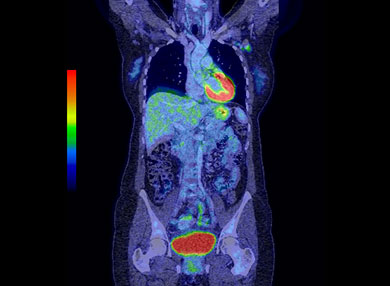
- Tomoscintigraphy: This category includes Single-Photon Emission Computed Tomography (SPECT), Positron Emission Tomography (PET), and Gated SPECT. These techniques involve the use of specialized cameras to capture three-dimensional images of radiotracer distribution in the body. They provide detailed information about the location, extent, and function of various organs and tissues.
- Hybrid imaging: These acquisitions combine nuclear medicine techniques with other imaging modalities such as Computed Tomography (CT) or Magnetic Resonance Imaging (MRI). Examples include SPECT/CT, PET/CT, SPECT/MR, and PET/MR. By combining functional and anatomical information, these hybrid imaging techniques offer enhanced diagnostic capabilities and improved accuracy in the evaluation of various diseases and conditions.
none
high → finds the smallest shit
low → if we find something we need further techniques (e.g. CT) do evaluate what it is (primary tumor, metastasis, etc)
- Tumors - primary (benign, malignant)
- Secondary (metastasis)
- Infections - osteomyelitis, septic arthritis, diskitis
- Trauma
- Surgery - joint prosthesis
- Metabolic bone disease
- Unexplained musculoskeletal pain
organspecific diphosphosphonate:
MDP (Tc-99m methylene diphosphonate) for bone
others: HDP, HMDP and DPD,..
- osteoblastic activity
- blood flow
→ metastasis
→ esp. in osteosclerotic cancer (osteolytic cancer lacks these characteristics)
maginification of the image
{kind=link}
- bones visualized
- symmetrical uptake
- kidney + urinary bladder can be seen
- are the bones individual visualized + not blurred?
- is everything symmetrical when you draw a vertical midline?
- You should always see the kidney + bladder + soft parts
(sometimes processed/masked on the computer→so absence could be normal)
normal, just growthplates
- focal uptake: metastasis
- "Cold" zone: blue spot lacks uptake → either osteolytic metastsis which is - osteoclasitic activity (¬ sclerotic), or metal plate after neurosurgery
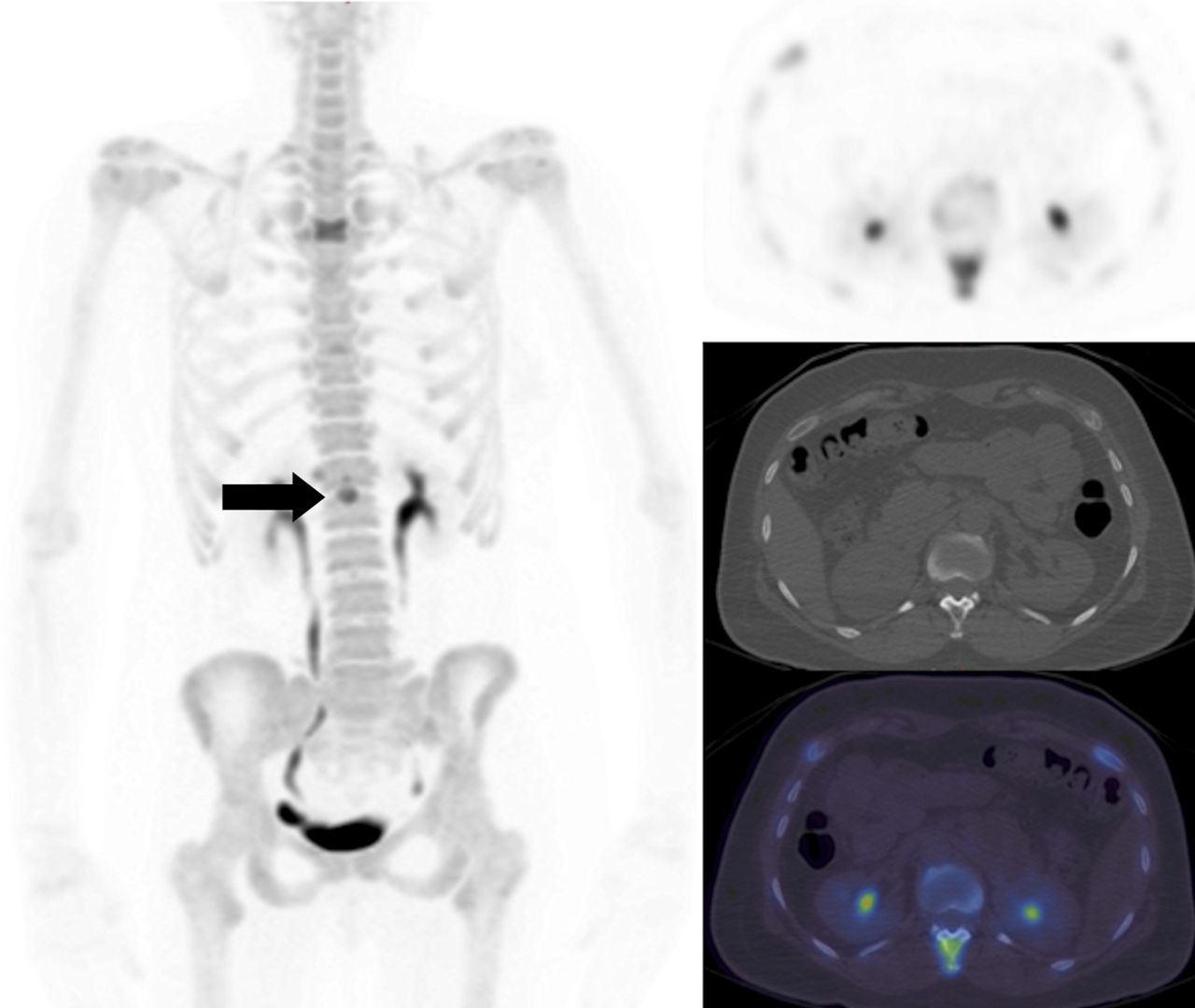
- Hyperscan/Superscan: symetrical:
- Diffuse intense skeletal uptake with reduced renal visualization - high tumor load (cancer of the prostate or breast).
- MDP accumulates in numerous bone lesions to such an extent that there is little available for renal excretion.
⇒ 📷: we cant see the kidney, urinary bladder and soft-tissue, high bone tumor uptake → prob. general carcinomatosis!, tumor spread is so severe that is takes up all the contrast.
{kind=link}
- multiple focal lesion
- incr. MDP uptake
- randomly asymmtric distributed, but around axial skeleton
hematogenous
- after breast + prostate cancer therpapy
- higher uptake in metastassis after chemo → good sign pentru ca osteoblastic response, bone healing
fracture → imagine fracture line → should be at the 2 sides of the fracture
{kind=link}
- Hypertrophic Pulmonary Osteoarthropathy (HPOA) is characterized by the abnormal proliferation of the skin and the periosteal formation of new bone at the distal ends of long bones.
- Primary HPOA, 5% of cases ⇒ genetically inherited
- secondary HPOA, 95% ⇒ paraneoplastic syndrome. It is most commonly associated with advanced stages (III or IV) of adenocarcinoma lung cancer.
Secondary HPOA can also be linked to other conditions such as mesothelioma, renal cell carcinoma, gastrointestinal cancers, melanoma, thymic cancer, nasopharyngeal cancers, and Hodgkin lymphoma.
metastasis 📷
{kind=link}
most probably due to fracture than metasis
osteolytic 📷
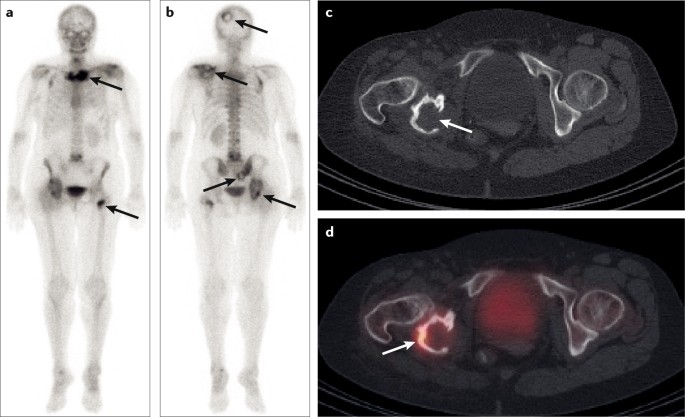{kind=link}
breast cc 📷
{kind=link}
SPECT/CT
high uptAKE 📷 → further diagnostic needed: Three-Phase Bone scan
{kind=link}
{kind=link}
PHASES: 📷 | TIME | IMPORTANCE |
FIRST PHASE: Radionuclide angiography phase/dynamic vascular flow phase | First 30 sec | Differences in vascularity to region. |
SECOND PHASE: Blood pool phase | At 5 min | Difference in blood flow and vascular permeability in bone. |
THIRD PHASE: Bone scintigraphy phase/osseous delayed static image | 2–4 hours later | Distribution of radioisotope in bone and metabolic activity of bone. |
still high uptake of the sourroung → osteoblast try to heal
no good → better other techniques
osteoid osteoma: double density sign/headlight in fog 📷
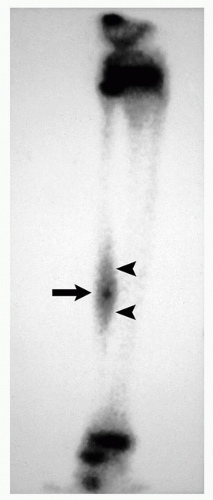{kind=link}
- avascular necrosis
- acute osteomyelitis also in prostetic evaluation - in all 3-phase positive
- Paget's diseases 📷
- Trauma
- sport trauma + joint diseases



- relative renal function
- goldstandard: upper UT-obstruction
- scarring after obstructive pyelonephritis
- dg renovascular HT
- Non-invasive examinations
- No side effects
- No need to stop eating
- Provides functional-morphological information
- Can perform pharmacological interventions (Captopril, Furosemide)
- dynamic = renography
- static
basal + diuretic
no → i.v. bolus → start direct
- Te-99m DTPA - glomerular filtration
- Te-99 MAG3 - tubular secretion
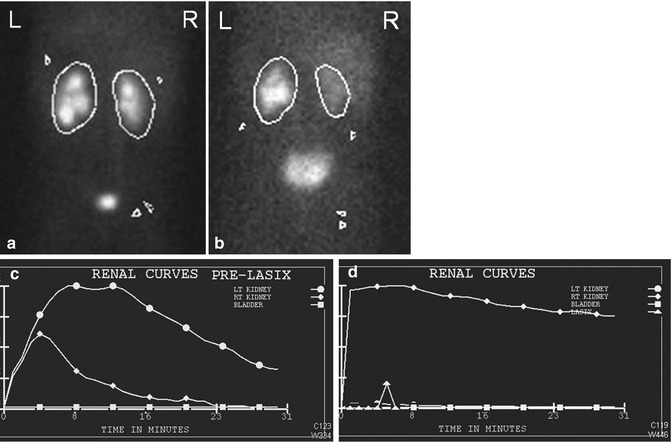
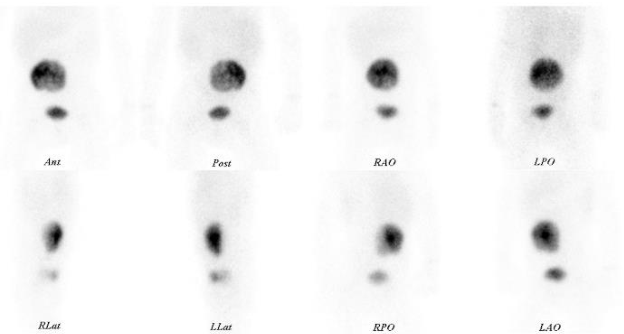
you have to mark the ROIs (regions of interest)
{kind=link}
x → time
y → measured radioactivity
Rise in the curve → progressive inflow of the tracer in the kidney = vascular phase
→ between min 2-5 → GF-phase (marked by the 2 yellow vertical lines)
⇒ then slow excretion phase
{kind=link}
the 3 segments/phases (see one question above)
gap between the 2 lines is not important
45-55%
→ dosage card: 📷
- Obstruction severity
- surgical strategy
- efficiency of surgical treatment
true obstruction vs. "Lappen"-Obstruction ⇒ furosemid → incr. urinary pressure → in true obstruction is will still not flow like a river
{kind=link}
basic renography + furosemid
→ wait 18min
⇒ rapid fall in curve → non obstructive

⇒ no/little fall → obstructive
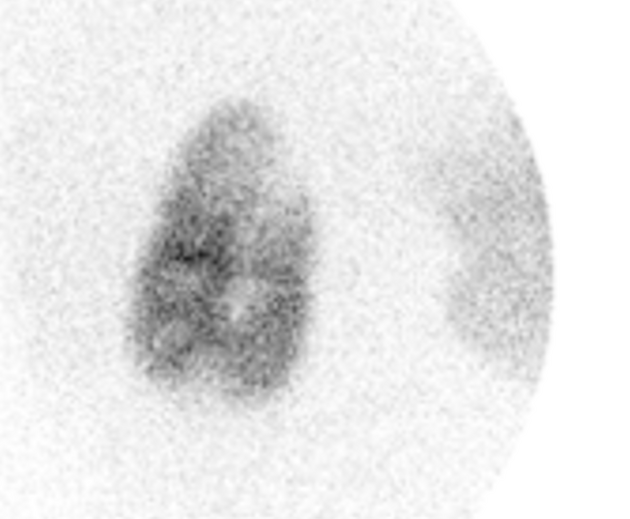
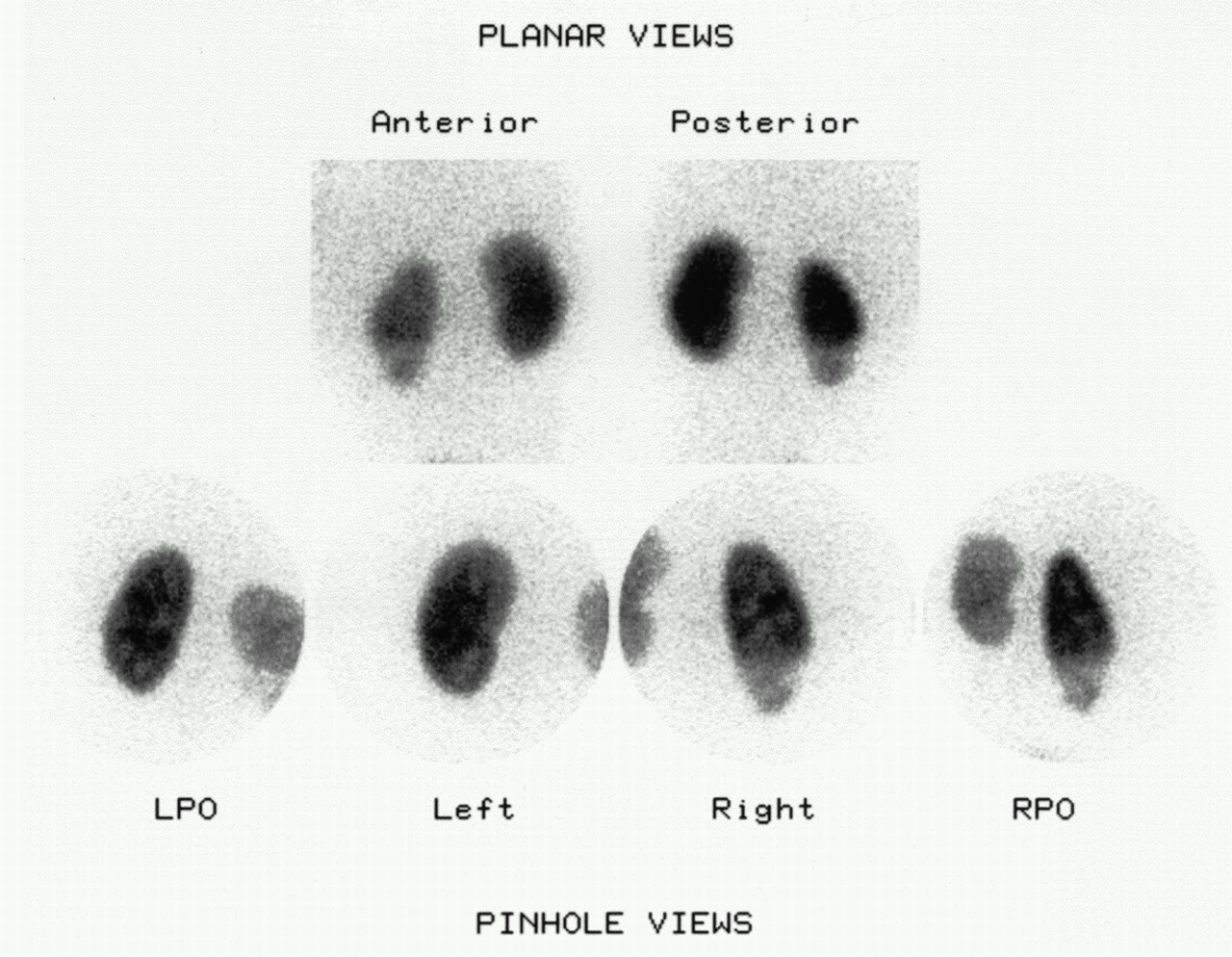
DMSA (fixed in the renal cortex)
diagnose renal scarring 📷 due to PN or reflux
{kind=link}
can also estimate relative renal function
{kind=link}
{kind=link}
{kind=link}
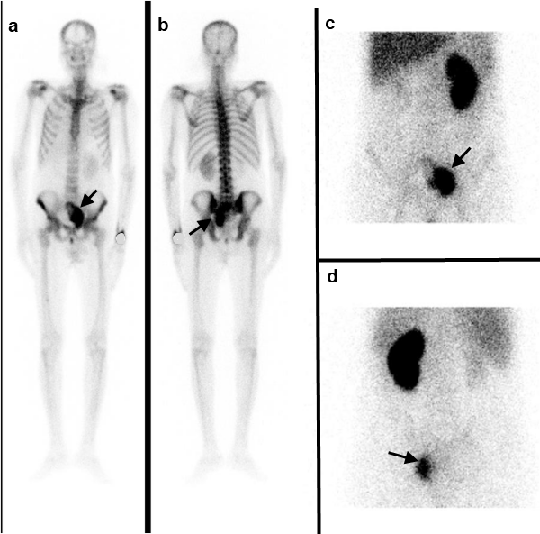
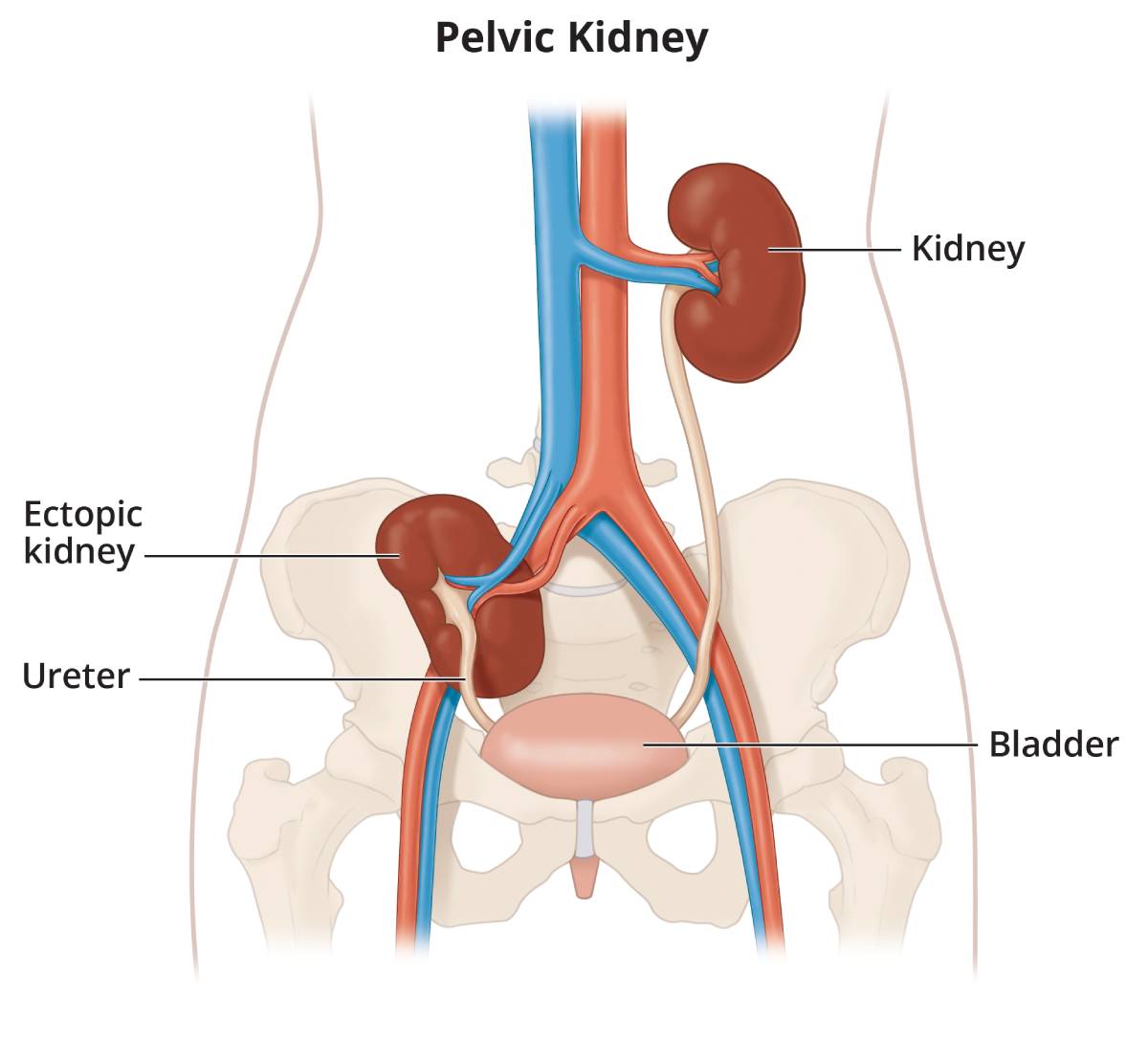
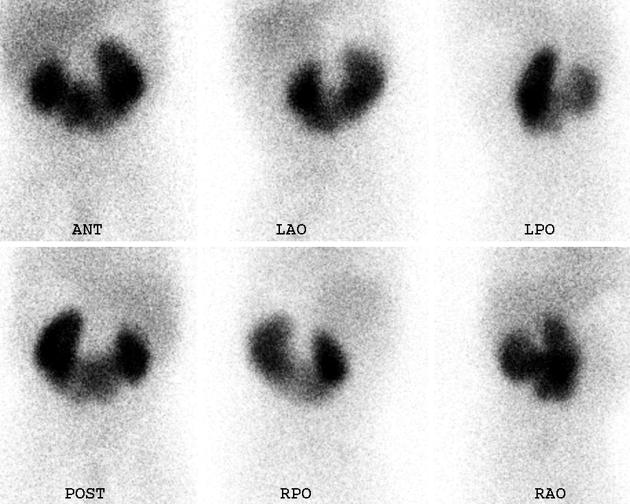
horseshoe kidney
{kind=link}
Vesicourethral reflux
multiple zones with no uptake in both kidney → smaller right kidney, with lesser uptake→ has probably suffered more (also 30%-70% split renal function)
{kind=link}
Pancake kidney → no scarring in this case

⇒ 📷
{kind=link}
1: little less uptake, little scars
2: less uptake, scar
3: smaller kidney, way less uptake
4: same as 3 + increased backgroud