







Gynecology, Obstetrics & Neonatology
🦪 Gynecology
- 🔃 Hormonal Physiology
- 👧🏼 Puberty
- 👵🏼 Menopause
- 👉🏼 Vaginal touch
- 📺 TRADITIONAL (natural) contraception
- 🚧 BARRIER contraception & SPERMICIDES
- ☂️ Intra-uterine device (IUD)
- 💊 Hormonal contraception
- ♀: 🥍 Tubular ligation (Sterilization)
- ♂: ✂️ Vasectomy
- 👩🏼🍼 Postpartum contraception
- ❌ Abortion (elective)
- 🏗️ Malformations
- ◀️ Pre-menstrual syndrome (PMS)
- 🍫 Endometriosis
- 🧺 Adenomyosis (”Internal” endometriosis)
- 👛 Pelvic inflammatory disease (PID)
- 🚱 - Amenorrhea (ØFLOW)
- ⚾ Lump
- 💦 Discharge (Leukorrhea)
- 🧧Sore / Wound
- 👅 Pelvic organ prolapse (POP) & urinary incontinency
- Most will clear infection within 12 months
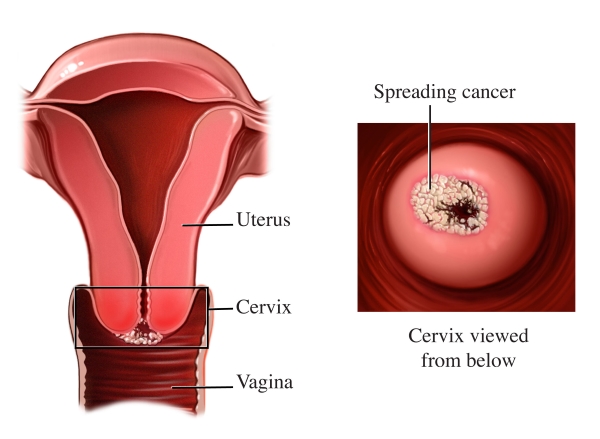
- Some will have infection persist ⇒ Cervical cancer:
- HPV 16: 50% of cases
- HPV 18: 20% of cases
- Others: HPV 31, 33, 45, 52, and 58
- Related to Sexual behaviour
- HPV infection or history of other STD
- sex at young age
- multiple partners
- Smoking
- Immunodeficiency
- Hormonal factors
Q. It isn't a risk factor for cervical intra-epithelial neoplasia (CIN) A. HPV infection B. Smoking C. Immunosuppression D. Hormonal factors E. High socioeconomic level
→ E) Low socioeconomic level (only listed for carcinoma; Ø CIN)
{kind=link}
{kind=link}

- Squamocolumnar junction
- Junction between squamous and columnar epithelium
- Endocervix: columnar epithelium
- Ectocervix: squamous epithelium
- Transformation zone
- SCJ moves from exposure to hormones
- TZ: area between original SCJ and new SCJ
- Most (95%) cancers arise here
Q. Which part of the cervix do cancerous lesions begin: a. Exocervix b. Endocervix c. Squamo -columnar junction d. External cervical ostium e. Internal cervical ostium
HPV testing (PCR) ⇒ identifies HPV-INFECTION (Øcellular changes)
PAP smear ⇒ epithelial CELL changes (Koilocytes) due to HPV 📷
{kind=link}
Bethesda system “Squamous intraepithelial lesions” (SIL) | Cervical intraepithelial neoplasia (CIN) | WHO | |
Atypical cells | ASC-US + ASC-H | Atypia | Atypia |
Low grade lesion
⇒ 📷 | LSIL | CIN 1 | Koilocytes |
High grade lesion ⇒ 📷 | HSIL | CIN 2 + 3 | Moderate / Severe dysplasia + CIS |
Invasive carcinoma | When passing BM | When passing BM |
- CIN1 (corresponds to mild dysplasia)
- CIN2 (moderate dysplasia) - anomalies are present in the 2 / 3 basal epithelium.
- CIN3 (severe dysplasia and intraepithelial cancer) - anomalies are present in all epithelial structure.
→ the anomalies described are present in 1 / 3 basal epithelium, maintaining a mature aspect in superficial layers
- 🩸BLEEDING → irregular/heavy menses or POST-COITAL Discharge → initially watery, then bloody
- ↔️ Signs of INVASION → pain (pelvic/back), bladder & bowel signs (dysuria , dyschezia)

Other Investigations to Evaluate Tumor Extension:
- Pulmonary X-ray
- Urography, cystography, cystoscopy
- CT scan, MRI
- Renal and hepatic scintigraphy
- Barium enema (Irigography), rectoscopy
- Lymphography
- small elongated tumors on the cervix (usually benign )
- might cause
- bleeding
- abnormal pap smear
- Tx: Polypectomy
Screening → normal, like non-pregnant (abnormal PAP ⇒ colposcopy); if last screening >1y → screen in first 6w of pregnancy Biopsy ⇒ only if high risk APPEARANCE (Raised masses, ulcerative lesions) Excision ⇒ only considered if INVASIVE CA (beyond BM) → delay Tx for non-invasive (CIN1-3, LSIL+HSIL) until 6w after birth (via C-section)

Carcinoma Type | Treatment Approach and Details |
Micro invasive carcinoma | - Diagnostic conization, followed by a conservative approach until birth; colposcopy every 2 months.
- Birth when fetal viability is reached
⇒ caesarean section
⇒ followed by total hysterectomy.
- In case of early diagnosis, patient may choose radiotherapy, followed by miscarriage. |
Invasive carcinoma | Patient choice is fundamental:
- Radical surgery with lymphadenectomy in the 1st trimester.
- C-section in 3rd trimester, followed by radical surgery. |
Advanced carcinoma | - Subtotal hysterectomy (abortion) + radiotherapy
- If Dgx close to birth:
C-section → followed by total hysterectomy + radiotherapy
|
- 🍫 Endometriosis
- 💪🏼 Fibromyoma (= Leiomyoma = Fibroid)
- 📍Endometrial Polyps
- 🧺 Adenomyosis
- ⚰️ Uterine sarcoma
- 📍Endometrial POLYPS
- 🦀Endometrial HYPERPLASIA & CARCINOMA
- 🎈Ovarian Cysts
- ✨ Ovarian neoplasia
- 🩸- Abnormal uterine bleeding (AUB)
- 💦 Sexuality & sexual dysfunction
🤱🏼 Obstetrics
- Physiological basics
- 🔎 History, Clinic & Dgx
- 1️⃣. Trimester screening
- 2️⃣. Trimester screening
- 3️⃣. Trimester screening
- 🧬 Aneuploidy screening
- 💉 Vaccination
- 🕷️ Teratogens
- 👀 Antepartum Fetal Surveillance
- 👫 Multiple Gestations
- ❌ Spontaneous ABORTION (Miscarriage)
- 🥀 ECTOPIC pregnancy
- 🥮 Gestational trophoblastic disease (GTD)
- 🎑 Placental detachment (Abruptio placentae, retroplacental hematoma)
- 🚪 Placenta praevia
- 🧶 Vasa praevia
- 👛 Uterine rupture
- 🍮 Cervical lesions + other non-obstetric
- ❌ Spontaneous ABORTION (Miscarriage)
- 🤢 Nausea & Vomiting
- 🍬 Diabetes mellitus (DM) & Gestational Diabetes (DGM)
- Gestational hypertension (GHT):
- Preeclampsia, Eclampsia & HELLP
- 🕯️ TORCH infections
- 🥐 Urinary infections
- 🍑 Liver & 🍤 GI
- 🦋 Thyroid (+other endocrine → pituitary, adrenal)
- 🫀Heart
- 🫁 Resp. (pneumonia, TBC)
- 🩸 Blood → Anemia + DVT
- 👶🏼 EMBRYO-FETAL pathologies during pregnancy
- ⭐ Identification & Stages
- 👶🏼 Fetal characteristics
- 💊 Induction & Analgesia
- 🚚 Methods of delivery
- 🚰 Rupture of membranes (ROM)
- ↑↓⏰ Pre- & Post-term pregnancy
- 🦠 Perinatal infections
- 🖥️ Fetal monitoring (intra-partum) & distress
- 🐛 Umbilical cord prolapse
- ✖️Dystotic delivery (= Abnormal labor patterns/”Failure to progress”)
- 💥 Trauma (maternal & fetal)
- 📯 Postpartum
🐣 Neonatology
- 📺
- ⛑️ Neonatal resuscitation