





Family Medicine
⛲ Generalities of Family Medicine
primary
Q) Which of the following statements regarding general practice are TRUE: a. It is viewed as a model of primary care. b. Less than 1/3rd of medical students were looking for residencies in family medicine. c. It is based on small units, able to operate on the scale needed to meet changing population needs. d. The shortage of family doctors is not responsible for people who have no timely access to healthcare e. have to change to rise to the challanges of an ageing population.
ABE
GP | Specialist |
EXCLUDES serious D. | CONFIRMS serious D. |
Tolerate uncertainty: Manage patient with UNDIFFERENTIATED SYMPTOMS | investigate until DIAGNOSIS |
LOW INCIDENCE of serious disease
(general population) | HIGH INCIDENCE of serious diseases
(selected patient population) |
Q) By their activities, family physicians: a. Manage patients with undifferentiated symptoms b. Explore the possibility seeing a preselected population of patients c. Exclude the presence of serious disease d. Tolerate uncertainty e. Explore the probability of seeing patients from a population with a relatively low incidence of serious disease
ACDE
- Changed way of work
- ↓ small “solo” practices ⇒ ↑ groups of GP practices
- reference frameworks
- Guidelines introduction
- New health care services
⇒ ↓accessibility in rural areas (country-side)
⇒ ↑investment in medical equipment for point of care tests
→ palliative + non-pallative → home- + institution-care
- 🚬 Smoking
- 🍺 alcohol
- 🛋️ physical inactivity
- 🍕unhealthy diet
- 🧠 (social isolation + loneliness)
35%

< 33% (1/3) ⇒ shortage of family doctors

❗ this was a question in the exam
- Dgx-Error (delayed or missed)
- Tx-Error (delayed or inappropriate)
Causes:
- physician’s behavior
- poor communication + coordination betw. health care professionals

- Tiredness, stress, and overwork
- Lack of appropriate management plan
- Not accepting limitations in expertise
- Not respecting patient wishes, even when contrary to professional judgment
- patient’s behavior
- Poor patient-doctor relationship
- Delayed presentation
- Nonadherence to medical recommendations
- Therapeutic non-compliance in serious illnesses (e.g., chronic alcoholism, mental diseases)
- Lack of family support
⇒ for INSURED people → classic shit you can think of
- Acute and subacute diseases care
- Medical emergencies
- Chronic diseases management
- Pregnancy and child healthcare
- Preventive care, including risk factors evaluation for asymptomatic individuals and specific prevention through vaccinations
- Services related to potentially endemic and epidemic diseases
- Dental care for children only
- Surgical interventions (excluding plastic surgery)
- Procedures and techniques enabling complementary studies certificates
- General ultrasonography
- Geriatric and palliative care
- Complementary medicine, such as homeopathy, acupuncture, and phytotherapy
⇒ for NON-INSURED people
- 🚑emergency
- 🤰pregnancy + 👶child healthcare
- 🦠endemic-epidemic related services
- 💉mandatory vaccinations
⇒ for FOREIGNERS
⇒ SAME as MINIMAL but Ø 👶CHILD HEALTHCARE!!

- Violence: includes physical violence, verbal abuse towards doctors, practice staff, or other patients; violence or threatening behavior by non-registered household members;
- Crime and Deception: deliberate deceit to obtain a service or benefit, obtaining drugs under false pretenses, use of the doctor to conceal or aid criminal activity, stealing from practice premises
⇒ immediate removal and police notification
(i know, stupid question but relevant for exam)
- Costly Tx
- Old Age
- Disagreement with the patient’s view

- direct contact to FAMILY + ENVIRONMENT
- higher practice satisfaction for family doctor
→ INFORMATION: socio-economic background + conflicts in family, toxins + other RF
- ↓ DIAGNOSTIC equipment
- Patient records
- Stethoscope
- Sphygmomanometer
- Otoscope and ophthalmoscope
- Sterile specimen cups
- Thermometer
- Tongue depressors
- Urine dipsticks
- Glucometer
- Laptop
- Patient education materials
- Scale
- Emergency medication: furosemide, metochlopramid, diazepam, adrenaline, hydrocortisone succinate, glucose and other relevant medications
- Oral medication: captopril, nitroglycerin, paracetamol, ibuprofen, tramadol, prednisone, salbutamol spray, and other necessary medications
- Needles, syringes, and sterile wipes disinfectant
- DISTANCE that has to be traveled
- OTHER PEOPLE → difficult history + exam
- payment → depends on insurance

Equipment:
- Emergency situations, especially in rural areas, where transportation to the doctor is difficult
- Acute illnesses requiring immediate attention
- Exacerbation of chronic diseases that
⇒ make it challenging for the patient to visit the doctor ⇒ in city → emergency; country side → family foctor has to visist
- 👶 Newborn
- Advise mother: nutrition & hygiene
- Physical exam
- Medical file preparation
- 👵🏽 Elderly + moving difficulty
- Evaluate health station
- Adjust Tx plan
- 🕰️Chronic patient with Tx NON-compliance
- Improvement of symptoms
- Financial
- Neglect
→ visit soon after discharge
Reasons:
⇒ Step 1: call the patient; Step 2: home visit
- Provide terminal care
- Grief support and pronouncement of death
- Family assistance (medical & emotial) - before, during & after death
Indications:
- Poor compliance
- Excessive use of health care resources
- Polypharmacy evaluation
- “At risk” patient → evaluate home environment for (signs of abuse, neglect, social isolation)
- Coping with chronic problem →e.g. Cognitive impairment & Incontinence
- Assess need for nursing home
After major illness/surgery:
- Evaluating coping behaviors of the patient and family members
- Assessing the effectiveness of the home health care plan
= Assessment of Functional activity:
Assessment of 💅🏼 SELF-CARE (ADL) + 🍳 INSTRUMENTAL (IADL) activities of daily living
- Assessment of the activities of daily living (ADLs) including bathing, transfer, dressing, toileting, feeding, and continence.
- Evaluation of the instrumental activities of daily living (IADLs) such as using the telephone, administering medications, paying bills, shopping for food, preparing meals, and doing housework.
Assess:
- State of nutrition
- Eating behavior (e.g. food preferences)
how is the patient living?
safe neighborhood?
Assessment of
- SOCIAL SUPPORT SYSTEM
- Availability of EMERGENCY HELP from family members
- Caregiver’s needs
Evaluation of medication-plan / Medication storage place:
⇒ interactions?
⇒ compliance?
⇒ “doctor shopping?”
⇒ OTC drugs and herbal remedies?
- Physical exam
- Teach patient self-monitoring (BP, Gluc)
- Correlation of home vs in-practice measure
environment= comfortable + safe? ⇒ correct RF
religious objects? 📷
→ ask about spirtuality + sense of physical/emotional health
Home health agencies → meet the patient together with them
🔍 Symptom-based Workup
(chronic cough hypersensitivity syndrome)
“Recently, the term chronic cough hypersensitivity syndrome has been proposed as a label for chronic cough, owing to the fact that the underlying abnormality leading to chronic coughing is an abnormally sensitive cough reflex”
cough >8w (>2m)
Acute cough: < 3 weeks in duration
Subacute cough: 3-8 weeks in duration
Chronic cough: > 8 weeks in duration
MOST COMMON ETIOLOGIES:
lung cancer 🦀
- (🥇) Upper airway cough syndrome (UACS)
- Asthma
- GERD
- Non-asthmatic eosinophilic bronchitis (NAEB)
- chronic cough
- airway eosinophilia (>3% in sputum)
- absence of airway hyperresponsiveness
previously referred to as postnasal drip syndrome (PNDS)

characterized by:
→ normal pulmonary function and normal bronchoprovocation challenge testing
More details later… (DDx)
ANAMNESIS:
- Frequency? (recurr., permanent, etc)
- Character? (sputum? amount+characteristics of sputum?)

- Time of appearance? (night, morning, evening?)
- other Symptoms? (vomiting, dyspnea+syncope etc)
- Trigger? (position, exercise, cold air, eating)
→ Cough exacerbated by exercise and at night = characteristic of cough-variant asthma

- 🅱️ -symptoms
- 🚬smoking
- >45y + new cough/change in cough
- 55-80y + 30 pack years
- 🫁Signs of lung cancer
- abnormal respiratory exam / Xray
- Hemoptysis
- dyspnea (during night + rest)
- recurr. pneumonia
- Signs of other cancer location
- 🍤 gastric -> vomiting
- 🧣 pharyx/larynx → Dysphagia + hoarseness

6th 📷
T
According to studies:
- 2 or more causes in 18 - 62 %
- 3 causes in up to 42 %

🚬 Environmental
(smoking, pollution, dust, ↓humidity)
🫁 Respiratory
- UACS (upper airway cough syd): chron. Rhinitis + Sinusitis ( allergic, non-allergic, non-allergic with eosinophilia, occupational, post-infectous, irritant, vasomotor)
- obstructive sleep apnea
- chronic inflammation or tumor:
- pharynx
- larynx:
- trachea
⇒ also post-infectious (i.e. post-covid)
Should be considered when cough persists after URT infection → self-limited (may persist sometimes for months)
- bronchi: chronic BRONCHITIS
- Asthma, COPD,
- non-asthmatic eosinophilic,
- bronchiectasis
- LUNG
- lung cancer
- TB,
- PLEURA
- pneumoconiosis
Characterized by eosinophilic inflammation bronchi. Symptoms include cough, wheezing, dyspnea. Sputum eosinophilia is a characteristic finding. Good response to corticosteroids. Ø obstruction or airway hyperresponsiveness (unlike in asthma and COPD)

🎡Extra-respiratory
- 🫀 cardiac congestion
- 🤢 GERD
- 💊 Iatrogenic (ACEi)
- 😵💫psychogenic




Children | <30y | >30y |
MSK:
Costochondritis + Chest wall injury | MSK | CV:
ACS, AoDissection |
GERD | GI | |
Precordial catch syndrome | Pulmonary | Pulmonary:
PE, Tumor |
Psychogenic | Psychogenic |

Site - where is the pain?
Onset - what where you doing when the pain started?
Character - stabbing, dull, ache, pressure, tearing, ripping?
Radiation - arm, shoulder, jaw?
Associations ⇒ Symptoms + Signs pointing towards DDx (see DDx in details below)
Time course - when did it start? have it changed since then? (Sudden, acute, chronic, recurr)
Exacerbation/Relieving factors - what makes it worse/better? (Exercise, rest, palption?)
Severity - 1-10?
- Exclude ACS 🫀
- Exclude 🚩
- Consider other DDx
↓
↓

1️⃣p ⇒ Ø-ANGINAL + m>40 or f>60 ⇒ INTERMEDIATE
2️⃣p ⇒ ATYPICAL + all m or f>50 ⇒ INTERMEDIATE
3️⃣p ⇒ TYPICAL ⇒ HIGH risk
Three key clinical features:
- Location: Is the pain pre-sternal or substernal?
- Aggravating factors: Is it exacerbated by exertion?
- Alleviating factors: Is it relieved by rest or nitroglycerin?
Number of Characteristics | Classification | Risk for CAD |
3 | TYPICAL ANGINA | High risk for CAD (in all age groups) |
2 | ATYPICAL ANGINA | Intermediate risk for CAD |
- In women older than 50 years | ||
- In all men | ||
1 | NON-ANGINAL chest pain | Intermediate risk for CAD |
- In women older than 60 years | ||
- In men older than 40 years |
“The clinical decision rule for identifying patients with chest pain caused by Coronary Artery Disease (CAD) involves assessing the presence of five characteristics”:
- Age > 55 years in men; > 65 years in women
- Known CAD or cerebrovascular disease
- Pain not reproducible by palpation
- Pain worsens during exercise
- Patient expresses concern that the pain may be cardiogenic
→ each = 1 point
Interpretation:
- A score of 0-1 indicates a low risk for CAD.
- A score of 2-3 suggests a moderate risk for CAD.
- A score of 4-5 indicates a high risk for CAD.


Tamponade:
- BECKS triad

- Cardiogenic shock
- Pulsus paradoxus (↓BPsys during INSPIRATION)


- sharp chest pain
Pericarditis:
- sharp chest pain
- friction rub
- 🔔 pain get BETTER when leaning FORWARD
- ECHO
- XRAY
- EKG
- tamponade: electric alternans 📷
- pericarditis: ST-elevation without mirror changes
QRS complexes alternate in height Occurs when the heart swings in front and backwards within a large fluid-filled pericardium (swinging changes heart vector)
Tamponade → Pericardiocentesis
Pericarditis → NSAID / Colchicine




- primary (spont.)
- secondary (pre-existing lung D.)
- Trauma
- iatrogenic
- TENSION PNEU 🚩

- 🔥 fever
- 🌬️cough +/- sputum
- 💨dyspnea
- 🩺Focal signs:
- 🧰 chest pain

Ø [FEVER] ⇒ but new onset [MENTAL CONFUSION]


CLASSIC GERD PRESENTATION
- Retrosternal heartburn (background pain) + Regurgitation
- Dysphagia + Odynophagia (these are actually alarm symptoms!)
- Chronic Cough + Wheeze ⇒ after/during meal
Ø exercise response
Ø radiation
- Dysphagia + Odynophagia
- B-symptoms: Weight Loss (unexplained) + ↓appetite
- “bleeding” related
- Anemia (unexplained)
- GI bleeding (Melena, Hematochezia)
- Failure of PPI trial
- Repeated vomiting (more indicative for gastric cancer)
EMPIRIC PPI TRIAL:
💊 Pantoprazol OR Esomeprazol: 4 WEEKS, 40mg - 0mg - 20mg


↓
if:
+ Response ⇒ GERD
if:
Ø Response ⇒ Refer to gastroenterologist (EGD, manometry, motility, 24h ph)

iatrogenic injury (endoscopy)
- 🧣DYSPHAGIA
- 🧰 Chest pain (retrosternal)
- RADIATES → BACK
- 🤮 Vomiting
- 📸 MEDIASTINAL SIGNS: Subcutaneous emphysema + mediastinal crepitus
- 🔥 fever
- 🫁 dyspnea, tachypnea, tachycardia
- 🆘 features of organ dysfunction
- CNS: altered mental status
- Cardiovascular failure: hypotension
- Respiratory failure: symptoms of ARDS (acute respiratory distress syndrome)
- Liver failure: jaundice
- Coagulopathy - disseminated intravascular coagulation - petechia, purpura
- Kidney failure: oliguria
- ⇒ ⚡ septic shock!


The pain is characterized by the following features:
- It is not squeezing or oppressive in nature.
- It is localized on the left or median-left part of the chest wall.
- It is well-localized on the chest wall.
- It occurs without exercise.
- It is influenced by movement or posture.
- It can be reproduced by palpation.

Tx:
🍯 “honey approach in children” = IBU 🔫 ”pump-approach in adults” = steroids + sulfasalazin
Q. Which of the following are characteristic for costochondritis: a. It is particularly common in children (2-6 years old). b. The hallmark of costochondritis is tenderness to pressure over the costochondral joint. c. frequently caused by viral illness or by frequent coughing. d. It is often accompanied by difficulty in breathing. e. It may last for several months.
BC

- Fibromyalgia (FM) is a neurosensory disorder characterized by chronic musculocutaneous pain.
- Etiology and pathogenesis are not fully understood, and there is no identifiable inflammation causing symptoms.
- Patients often have functional symptoms (fatigue, unrefreshing sleep, morning stiffness) and a history of psychiatric disorders.
- Physical examination reveals characteristic tender points over multiple areas with no signs of inflammation.
- Laboratory tests show normal findings.
- Treatment involves lifestyle changes and multidisciplinary pain management.
- Anti-depressants (SSRI/SNRI, TCA)
- CBT: Cognitive behavioral therapy



SSRIs include:
- 🥇 Preferred:
- Fluoxetine (brand name: Prozac)
- Sertraline (brand name: Zoloft)
- Others
- Citalopram (brand name: Celapram)
- Escitalopram (brand name: Escicor)
- Fluvoxamine (brand name: Faverin)
- Paroxetine (brand name: Aropax)
SCREENING QUESTIONS:
- 2 questions to screen for panic disorder:
- "In the past 6 months, have you ever had an attack when all of a sudden you felt frightened, anxious, or very uneasy?"
- "In the past 6 months, have you ever had an attack when for no reason your heart suddenly began to race, you felt faint, or you couldn't catch your breath?"
- In primary care, this brief questionnaire has high sensitivity (94%-100%) and negative predictive value (94%-100%) for excluding panic disorder.
- However, it has low specificity (25%-59%) and low positive predictive value (18%-40%), requiring further assessment for a positive result.
→ A positive response to either question is a positive screen.
- 2 questions to screen for depression:
- "During the past month have you often been bothered by feeling down, depressed, or hopeless?"
- "During the past month have you often been bothered by little interest or pleasure in doing things?"
→ A positive response to either question is considered a positive screen for depression.

- Dyspnea is characterized by conscious breathing
- It is uncomfortable but not painful
- Breathing effort is perceived as insufficient
- Described as a "lack" of air or a sensation of oppression related to breathing
- 🎗️ CAUSE
- ⏱️ TEMPORAL (acute, continous, subacute, paroxistic intermitt., recurrent)
- 🏃🏻♂️ relation to EXERCISE (induced vs. rest)
- 🌬️
- Respiratory FREQUENCY (tachy vs brady-expiratory vs. brady-inspiratory)
- Breathing RHYTHM (regular vs. irregular (i.e. Kussmaul, Cheyne stokes, Biot’s) 📷
- 🧘 POSITION (platipnea, trepopnea, hypopnea, orthopnea)
- Dyspnea worsens when standing, but improves when sitting down.
- Associated with
- neurological diseases.
- pneumectomies.
- hemo-pulmonary congestive syndrome.
- shortness of breath that is alleviated by lying on one side.
- Assoc. with:
- congestive heart failure
- various pleuro-pulmonary and mediastinal conditions.
- shallow → pleuritic chest pain
- noctural paroxistic, patient has to stand up
- assoc. with:
- Hypertensive and ischemic heart diseases
- Mitral-aortic valve injuries
- Unstable COPD
- Gastroesophageal reflux
- Diaphragmatic paralysis
- Degenerative neurological diseases
Plati:
Trepo:
Hypo:
Ortho:
- 🫁 Respiratory
- ❤️ Heart
- 🦴 MSK
- 🥐 GI
- ⚡ Neuro + Neuromuscular
- 🤪 Psych
- 🩸 Blood changes (metabolic, intox, hema)
![[Crab icons created by Icongeek26 - Flaticon]](https://images.spr.so/cdn-cgi/imagedelivery/j42No7y-dcokJuNgXeA0ig/acd61734-0f76-4167-886e-46bb0603e7f2/SCR-20221106-pld/w=1920,quality=90,fit=scale-down)
- anaphylaxis + foreign body aspiration,
- epiglottitis, croup,
- cancer
COPD, Asthma
pneumonia,
++ Lung cancer
- pneumothorax, hemothorax
- pleural effusion, pleuritis,
- restrictive lung diesease
- PE,
- pulmonary HT

- Coronaries:
- ACS + MI
- CAD
- Arrhythmias
- “Pan-Carditis”
- Pericardium:
- Tamponade
- Pericarditis
- Myocardium:
- Myocarditis
- Cardiomyopathy
- Endocardium:
- Valvulopathies
- (Congestive) HF
→ acute & chronic
![[Crab icons created by Icongeek26 - Flaticon]](https://images.spr.so/cdn-cgi/imagedelivery/j42No7y-dcokJuNgXeA0ig/8c15b4f0-d9fc-43fb-abb2-c5b967978ca5/SCR-20221106-qii/w=1920,quality=90,fit=scale-down)
1 Rib fracture + flail chest
2 pain
(3 severe deformities → kyphosis)
![[Crab icons created by Icongeek26 - Flaticon]](https://images.spr.so/cdn-cgi/imagedelivery/j42No7y-dcokJuNgXeA0ig/ee4841b2-40f5-4526-af75-00cd99b053b5/SCR-20221106-qk2/w=1920,quality=90,fit=scale-down)
1 GERD + obesity
![[Crab icons created by Icongeek26 - Flaticon]](https://images.spr.so/cdn-cgi/imagedelivery/j42No7y-dcokJuNgXeA0ig/77eb6fc0-ad20-40d6-a2f1-229a0382dd37/SCR-20221106-qlt/w=1920,quality=90,fit=scale-down)
- ⚡Neuro (UMN, LMN)
- UML (upper motor neuron lesion)
- Stroke
- spinal cord injury
- MS, ALS
- LMN (lower motor neuron lesion)
- Guillain-barre
- 💪 Neuro-muscular
- Myasthenia gravis
- diaphragmatic paralysis
![[Crab icons created by Icongeek26 - Flaticon]](https://images.spr.so/cdn-cgi/imagedelivery/j42No7y-dcokJuNgXeA0ig/557ce640-b61e-41f8-bac5-8b0a56d64df1/SCR-20221106-qqe/w=1920,quality=90,fit=scale-down)
- panic attack
- anxiety + somatization

![[Crab icons created by Icongeek26 - Flaticon]](https://images.spr.so/cdn-cgi/imagedelivery/j42No7y-dcokJuNgXeA0ig/faaa1ec2-8c33-4097-b297-bb7a68bdc0ff/SCR-20221106-qwh/w=1920,quality=90,fit=scale-down)
metabolic+endocrine
1 metabolic acidosis (incl. diabetic acidosis)
2 thyrotoxicosis
intox
3 salicylate + organophosphate poisoning
4 CO poisoning
hema
5 anemia (+ hypoxia)
![[Crab icons created by Icongeek26 - Flaticon]](https://images.spr.so/cdn-cgi/imagedelivery/j42No7y-dcokJuNgXeA0ig/ecc33c19-9192-41bc-b565-ad8cffcbd29f/Untitled/w=1920,quality=90,fit=scale-down)
dyspnea + palpation+ syncope
- 🎵 arrythmia (i.e. paroxistic tachycardia)
- PE
dyspnea + palpitations only
- valvulopathy
- PANIC attacks
- respiratory infection:
- URT: epiglottitis, laryngitis
- LRT: bronchitis, pneumonia
- sepsis
- Auto-immune → vasculitides
- tumor
- TBC
- PE
- pneumonia
- bronchiectasis

![[Crab icons created by Icongeek26 - Flaticon; Timer icons and Alarm clock, Freepik - Flaticon]](https://images.spr.so/cdn-cgi/imagedelivery/j42No7y-dcokJuNgXeA0ig/731f87d1-cc26-4aab-945a-75f8a8645e77/Neue_Zeichnung_2/w=1920,quality=90,fit=scale-down)
- Subacute dyspnea (onset of days-weeks)
- Paroxysmal intermittent dyspnea (related to certain times in a day, possible after exercise)
- Special form - recurrent dyspnea may indicate paroxysmal tachycardia or a complete intermittent atrioventricular block.
Characteristic | Inspiratory Bradypnea | Expiratory Bradypnea |
Type of Bradypnea | Slow and incomplete | Short and sufflating in-breath followed by a longer, strenuous, and noisy expiration |
Primary Feature | Difficulty in inspiration | Prolonged expiration |
Common Causes | Mechanical upper airway obstruction | Bronchial patho: asthma, Chronic bronchitis, Obstructive emphysema |
Breathing Pattern | Difficulty in taking in air | Difficulty in expelling air |
A
- open airway
B
- inspection (RR (>40 🚩), rhythm, accessory muscles)
- stridor? (🚩)
- auscultation (🚩Øbreathsound)
- pulse-oxi ↓🚩
C
- vital signs (BP↓🚩, HR, pulse)
- cyanosis 🚩
- auscultation (arrhythmia🚩)
- chest trauma?
D
- mental status? ↓🚩
- CLASSIFY dyspnea
- Exclude life-treatening conditions 🚩 + decide if ViTAL RISK (CV instable)
- Respiratory rate > 40 respirations per minute
- Cyanosis
- Reduction of oxygen saturation in the blood (e.g., examination of lips, gums, nails, hair)
- Low blood pressure
- Altered mental state
- Hypoxia (when Astrup parameters can be determined)
- Arrhythmias with vital risk
- Stridor and effort to breathe with no visible chest movements (suspicion of upper airways obstruction)
- Arterial hypotension and unilateral respiratory sounds (suspicion of compressive pneumothorax)
- Upper airway • Angioedema + Anaphylaxis • Deep neck infections • Foreign body aspiration
- Pulmonary • PE • Asthma / COPD exacerbation • Tension pneum • Diffuse alveolar hemorrhage • ARDS
- Cardiac • Acute coronary syndrome • Acute heart failure / flash pulmonary edema • Arrhythmias • Acute valvular dysfunction • Tamponade
- Other • Stroke • Diabetic ketoacidosis
- Anamnesis + exams for other DDx
Signs indicating vital risk in a patient:
- General measures (O2, position, comfort, improving environment)
- Ensure well-ventilated rooms
- Maintain suitable room temperature
- Monitor humidity levels
- Administer oxygen therapy as required
- Use continuous treatment for acute dyspnea
- Employ intermittent or long-term oxygen therapy for chronic dyspnea
- Enhance patient comfort through proper positioning
- Facilitate postural drainage
- Provide soothing massage
- Offer distractions such as music or reading
- Create a peaceful atmosphere
- Foster supportive relationships in the patient's surroundings
- Symptomatic (depending on pathology)
- Etiological Tx ⇒ ❕only partially applicable in family practice
- Bronchospasm: Administer oxygen therapy following protocols, use beta-adrenergics, and consider mild sedatives.
- Bronchial obstruction: Encourage oral hydration, prescribe mucolytics, administer oxygen therapy, and use beta-adrenergics.
- Pleural or pericardic effusion: Utilize diuretics and administer oxygen therapy.
- Hypoxia: Verify upper airways and provide oxygen therapy.
![[Crab icons & Süßigkeiten Icons & Baby Icons, by Freepik - Flaticon]](https://images.spr.so/cdn-cgi/imagedelivery/j42No7y-dcokJuNgXeA0ig/4befdb6a-3bc6-4200-ae71-d4292d82141b/SCR-20221102-q5l/w=1920,quality=90,fit=scale-down)
“vomit island 🌈🏝️🤮“
- 🚧 obstructive (GOO, ileus, volvolus, strangulated hernia, pyloric stenosis, tumor, achalasia)
- 🏗️ non-obstructive “functional”
- 🔥 inflammatory (appendicitis, pancreatitis, cholecystitis, gastritis, hepatitis, peritonitis)
- 🦠infectious
(GERD, IBS, Peptic ulcer)
(Gastroenteritis ⇒ viral, bacterial + toxins, food poisoning)
- ↑ ICP
- 🎾 mass (i.e. tumor)
- ❌stroke:
- ischemic
- hemorrhagic (trauma)
- 🦠infection (menigitis, encephalitis)
- 👂🏼Vestibular pathology
- Meniers
- infectious (vestib. neuritis, labyrhntitis)
- tumor (schwannoma)
- ⚡Migraine
- Psych
• Anorexia nervosa • Anxiety • Depression • Bulimia nervosa
- 🦀 Radio + chemo
- 🌸 Digoxin + (other anti-arrhythmics)
- 🌈 Opioids
- 🍺 Ethanol
- 🧪 Toxins: Arsenic, organophosphates/pesticides, ricin
- NSAIDs, AB, Anticonvulsants
- Inferior MI
- endocrine:
- 🤰pregnancy
- 🦋thyroid + parathyroid
- 📐 adrenals
- metabolic:
- 🍬 DKA
- 🥐 Uremia
- 🍤 → 🚧 + 🔥 (obstruction // pancreatitis, peritonitis)
- 🧠 → ❌ + 🦠 (stroke // menigitis, encephalitis)
- 💊 → Toxins + Drugs
- ❤️ → MI
- 🍬 + 📐 (DKA // Adrenal crisis)
- Check + correct Complications (dehydration, Acid-Base, electroly)
- Etiologly: Search + Tx
- Empiric Tx (anti-emetics)→ if Ø Etiology found
ILEUS

- 💥pain + 🎈distension
- preceeds 🤮vomiting!
Pain:

- 🩺↓ or ↑ bowel sounds
- if tumor → weight loss
GASTROPARESIS + GOA


🎈 bloating + 💦succussion splash, ⏰🤮late vomiting + early satiety
- GERD signs: retrosternal pain, reflux,..
- ulcer → gnawing pain, related to eating (depending if duodenal or gastric)
- epigastric pain/tenderness → pancreatitis or ulcer
- pancreatitis → radiates back

- right upper + aprupt onset → cholecystitis
- jaundice → hepatitis
- fever
- diarrhea
- +/- bloody (bacterial)
- myalgias, malaise, headache → viral
⇒ ❗ DEHYDRATION + AB + ELECTROLYTES
FND + cranial nerve signs
headche, stiffneck (menigitis)
vertigo (vestibular)
cyclic
calluses on dorsal finger 📷 → self infuced vomiting (bullemia)
signs of depression + anxiety
- squeezing chest pain / pressure
- dyspnea
- autonomic signs..
- etc…
- heat intolerance
- ↑metabolic function (HR, BP, peristalsis, etc)
- graves → myxedema + exopthalmos
- goiter
- 🤒fever
- ❤️ → arrhythmia + hypotension → shock
- 🧠 altered mental status
- nausea/vomiting
- 🌊 fluid
- 🎺BB
- Symptomatic: Beta-Blocker → Propranolol, atenolol
- 🌝 steroids

- 🚫Thyroid-hormone synthesis blocker
- Methimazole → generally prefered because not hepatotoxic, but teratogenic (MethMatzle)
- PTU (propyl-thio-uracil) → in pregnancy, hepatotoxic but not teratogenic, and in Thyroidstorm because block periph. conversion T4→T3. 🔫
hypotension ⇒ shock
(precipitated by stress [i.e. infection, surgery])
if chronic insuff → weakness, anorexia, orthostasis, weight loss, fatigue
- fluids
- steroids: hydrocortison/dexamethasone
- signs of DM (3 P’s)

- coma
- acidosis
⇒ 🏥 !!
Insulin
Volume replacement
Correct Acid-base + electrolytes
DOTAA
- Duration
- Onset
- Timing related to..
- Appearance of vomit
- Assoc. symptoms + signs
(acute/chronic)
(aprupt, acute, insidious)
(before eating, directly after, hours after
(undigested food, partially digested, bile, feculent, large volume).
(see above)
- CBC
- Inflammatory
- Electrolytes + AB
- Enzymes: Liver, pancreas
- Pregnancy test !
- tox screen if suspected
- thyroid hormones, adrenal hormones, ketone-bodies, uric acid
- Xray → obstruction
- US → inflammation
- EGD → pyloric + ulcer
- +/- barium
- manometry
- MRI / CT
- echo + ekg
- Ondasetron (5-HT3 Antagonist)
- Metoclopramide + Haloperidol + Phenotiazine (D2-Antagonist)
- Scopolamine (Anti-cholinergic)
- Antihistamines
- Aprepritant (Neurokinin-1-Rezeptor-Antagonisten)
- PREVENTION: Scopolamin ⇒ Scopoderm patch 1,5 mg
- phenothiazine
- antihistamines
Prevention of travel sickness: Scopoderm patch (1.5 mg) ➡️ helps with nausea, vomiting, vertigo ➡️ apply 6 hours before journey or the evening before ➡️ provides up to 72-hour protection.
Aprepritant + Ondasetron + Dexamethasone!
OR
Metoclopramide + Dexamethasone
haloperidol, benzos
extrapyramidal signs
dystonia (continuous spasms and muscle contractions), akathisia (may manifest as motor restlessness), parkinsonism characteristic symptoms such as rigidity, bradykinesia (slowness of movement), tremor, and tardive dyskinesia (irregular, jerky movements)
both: drowsiness
anticholinergic: dry mouth visual disturbance
prenatal vitamins → may ↓ severity of n+v
- ginger
- Ø iron supplement
- if persistant vomiting:
- PPI (Omeprazol/Rabeprazol) or
- H2-blocker (Ranitidine)

- Metoclopramide
- Ondasetron
- if morning sickness ⇒ DICLEGIS (=Doxylamine (antihistamine) + Vitamin B6 (pyridoxine)
>5% weight over 6-12m

- 🦀 cancer
- 🦠
- 🧀 TBC
- 🦠HIV
- 🪱GI-parasites
- 🍤 GI
- 💩IBD
- 🧈Fatty stools disorders
- celiac
- chron. pancreatitis
- 🛡rheuma diseases (i.e. vasculitides)
- surgery (bariatric)
- 🤪 Psych
- ❤️ + 🫁 + 🥐
- HF,
- chronic obstructive pulmonary,
- renal
- 🦋 + 🍬 + 📐 thyroid, DM type 1, adrenal
- 💊
- Urinary
- 🍬 diabetic drugs
- 🌊 diuretics
- GI
- 💩 laxatives
- 🦋 thyroid hormones
- 🚬 Abuse drugs: amphetamines, nicotine
- 🎭 Antidepressants, ⚡️anticonvulsants
- 👨👩👧 social
“Significant unintentional weight loss in the setting of type 2 diabetes, in the absence of causative medications, may arouse suspicion of a comorbidity such as infection or a pancreatic tumor.”
- 🤪
- 🍤 (celiac, IBD, cystic fibrosis)
- young-🦀 (leukemia, lymphoma)
- 🦀
- 🍤
- ❤️
- 🦀
- 🦠
- (+rheuma + vasculitides)
- hemoptysis + cough → lung cancer
- dysphagia → laryngx, pharynx, esophagus
- abdominal pain → gastric
- rectal bleeding → colo-rectal
- Lower urinary tract signs → prostate

- pelvic pain → ovarian cancer (+bloating)
- neurologic → brain cancer
- B-symptoms
- cough + hemoptysis
(in celiac, IBD, pancreatitis)
- 💥abdominal pain
- 💩diarrhea
- appearance:
- 🩸bloody stools → IBD, parasites
- 🧈 fatty floating → celiac, pancreatitis
- 🥶 - HYPOTHERMIA
- ❤️ ↓ - BP, HR, Arrythmia, cardiomyopathy
Correct weight + electrolytes
❗cave: SLOWLLLLLY ⇒ re-feeding syndrome due to correction of ↓K, ↓PO, ↓thiamine

- 🩸CBC,
- 🥐 Renal marker, urinalysis, elektrolytes
- 🍑Liver function including albumin
- Endo: 🦋TSH, 🍬gluc
- 💩GI: stool (heme) test
- 🦀 Cancer-screening
→ if signs for colon cancer →colonoscopy
Colonoscopy indications = colon cancer signs: → unintentional weight loss, anemia, heme-positive stools or gross rectal bleeding, abdominal pain, or change in stool caliber.
- PSA + Inflammatory markers
- Xray lung (mass, lymphadenopathy)
- US + CT Abdomen (cancer)
- old (>80y),
- anemia (Hb<10),
- ↑inflammatory marker (leukos, ESR, LDH, ALP)
other characteristics of NORMAL liver:
- Elastic consistency
- Smooth surface
- Absence of pain at palpation
usually fully covered by ribs
- Percussion
Start below the breast at the midclavicular line. Percuss as you move downwards and note the sound change of the transition from lung (resonant) → liver (dull). Continue until the sound changes again after the inferior margin of the liver.
- Liver scratch test
stethoscope → placed below xiphoid process of sternum
scratch midclavicular line downwards.
A scratch can only be heard over the liver
- US
Liver on US >16cm in midclavicular line
when palpable ✋🏽
- normal spleen does Ø exceed the costal margin
- palpable spleen = pathological.
- Physiological
- occasional norm-variant
- Riedel’s lobe 📷
- Relaxed/thin abdominal muscles
- ⬇️ Pushed down liver
- Low diaphragm (emphysema, asthma)
- Subdiaphragmatic injuries (abscess)
- pleural effusion


1. ↓OUTPUT (cyanosis, oliguria) 2. CONGESTION (↑JVP + hepato-jugular reflux, lower limb edema, dyspnea) → EXERCISE-INDUCED liver pain

RECENT | LONG-TERM | |
surface | smoth + eleastic | stiff + rounded margins |
palpation | painful | less painful |
hepato-jugular reflux | present | absent |
special features | Tx → REGRESSION
of hepatomegaly | Jaundice + Splenomegaly |
*hepatojugular reflux 📷

- Echo
- Chest-Xray
- Uneven enlargement (caudal)
- smooth surface
- pain
- Øhepato-jugular reflux
- +”liver signs”
- Cirrhosis (except last stage)
- Hepatitis
- Viral
- Drug-induced
- auto-immune
- EBV
- 🧈 LIPIDS
- Alcoholic liver disease
- NAFLD + NASH
- smooth surface
- Øpainful
- signs of cause
- ↑Cholestasis marker
- ↑Lipids
- abnormal OGTT
- also take liver marker + function test
- 🍞 GLYCOGEN (DM)
- 🤍 AMYLOIDOSIS
- 🔳 IRON + COPPER (hemochromatosis, hemosiderosis, wilsons)
- GRANULOMAS (TBC+sarcoidosis)
NAFLD = Nonalcoholic fatty liver disease NASH = Nonalcoholic steatohepatitis

Causes: - DM2 + Obesity - Toxins + Drugs - Chronic diseases (IBD+TBC)

anorexia, nausea, asthenia, transit disturbances, sub-jaundice, paresthesia (alcoholism, diabetes)


1.2 Gaucher’s
- HCC
- Leukemia + lymphoma

- Mets
- cystic disease, congenital liver fibrosis
- ascending → respiratory
- inferior → jaundice + ascitis (compression bile duct + portal v.)
- posterior → push liver forwards
- ant → isolated hepatomegaly, irregular, firm, surface
- central → uniform hepatomegaly, smooth surface+ normal consistency
- Lab → n/↑eos 🍒
- Xray → calcification + bulging of diaphragm
- US + CT → location, daugther vesicles, detached membrane

⇒ usually secondary to liver cirrhosis
⇒ PH? (lithiasis, cholecystitis?)
⇒ family history?? (familial cholestasis)
- 🍠 SPLENOMEGALY plus
- 🍑 CLASSIC LIVER SIGNS
- jaundice
- ascitis
- varrices + bleeding
- inflammatory signs: fever + ↑LN
LIVER + BILIARY MARKER
- 🪵 Liver cell marker (AST, ALT, LDH, iron)
- 🏭 Liver functional markers (Albumin, prothrombin (INR)+coagulation factors, cholinesterases)
- 🎋 Cholestasis markers (ALP, GGT, Bili→blood+urine)
GENERAL INFLAMMATORY:
- 🔥 Inflammatory markers (ESR, CRP, Leukos)
left shoulder
HYPERFUNCTIONAL spleen → faster blood cell removal→ pancytopenia
Patho: spleen overactive → cells removed faster from blood than normal → ↓ of cell lines, possible cytopenia (pancytopenia, leukopenia, anemia, and thrombocytopenia) → reactive bone marrow hyperplasia
⇒ Signs of anemia, thrombocytopenia, leukopenia


(increased splenic activity)
sickle cell, spherocytosis, thalassemia

- Spleen moderately enlarged and soft
- Sensitivity to palpation
- Clinical infectious signs: shivering, fluctuating or plateau fever, altered toxic septic general state
- Identification of the entry port and potential suppurative foci
- Diagnosis established with hemocultures
- others
- Bacterial endocarditis
- Tuberculosis (TB)
- Malaria
- Leishmaniasis
- Trypanosomiasis
- AIDS (Acquired Immunodeficiency Syndrome)
- Viral hepatitis
- Syphilis
- Splenic abscesses
- Disseminated histoplasmosis
- 🦢 Rheumatoid Arthritis (RA) ⇒ Felty’s syndrome🎅🏼 📷

- 🐺 Lupus
- 🏮 Immune hemolytic anemia + thrombocytopenia
- 🦀
- Lymphoma + Leukemia
- primary tumors
- mets
- 🛢️ benign
- COMPENSATORY (extra-medullary) HEMATOPOESIS
- BM malignancy
- iron-def. anemia / chronic hypoxia
- Gaucher
- amyloidosis

OTHER CAUSES
- ⚰️ sarcoidosis
- ❓ Idiopathic/Isolated
- 🐼 iron-def anemia
- 🦋 thyrotoxicosis




- 🦀TUMOR of SURROUNDINGS
- Parietal tumor (solidarized with the abdominal wall)
- Tumors of:
- stomach
- left colic flexure
- left kidney
- adrenal gland
- tail of the pancreas
- omentum
- peritoneum
- 🍠 SPLEEN
- normal variant
- displaced spleen (retro-splenic tumor)
- 🍑 HYPERTROPHIC left LIVER lobe 📷
- hema workup
- lab
- BM (bone marrow)
- Imagistics
- laparoscopy (if poly-adenopathy)
US, Xray, CT, scinti

- Nociceptive pain:
- 🗡️ Somatic pain → sharp/localized
- Musculo-skeletal 🦴 💪🏼
- Vascular 🩸 (artery + vein)
- Visceral pain → dull/diffuse
- 🪞 Referred (radiated, mirrored) pain
- 🔥 Neuropathic pain → burning
- Central
- Peripheral
- Sympathetic
- 🗡️ + 🔥 Mixed (nociceptive + neuropathic)
- 🤪 Psychogenic
(bone, joint, peri-articular; muscle, skin)
⇒visceral ORGANS (i.e. ❤️)
- somatic → 🔪 localized + sharp
- visceral → diffuse, dull +- radiation + autonomic signs
- neuropathic → intermittend / permanent + 🔥 burning OR aching, numb, stabbing, shock-like
+ NEURO-SIGNS (sensory,motor, reflexes)
+/- 💦 autonomic changes in sympath. (vasomotor+sweating, trophic changes)
+/- 🧦 distal hypesthesia (periph)
- somatic → 🔪 localized + sharp
- visceral → diffuse, dull +- radiation + autonomic signs
- neuropathic → intermittend / permanent + 🔥 burning OR aching, numb, stabbing, shock-like
+ NEURO-SIGNS (sensory,motor, reflexes)
+/- 💦 autonomic changes in sympath. (vasomotor+sweating, trophic changes)
+/- 🧦 distal hypesthesia (periph)
- Fracture
- Articular
- if DEGNERATIVE: MECHANICAL pain → ↑use+palpation ↓rest
- if INFLAMMATORY: INFLAMMATORY pain → ↑rest ↓use+NSAIDs
- if GOUT: tophi + ↑uric acid
- Peri-Articular
→ HISTORY: trauma, osteoporosis, malignancy (primary+mets)?
→ PAIN: MECHANICAL ↑use/stress + ↓rest (immobilization)
→ Xray
→ PAIN:
→ RESTRICTED movement (stiffness) + joint SWELLING
(tendinitis, bursitis)
SAME as ARTICULAR pain (more mechanical) BUT Øswelling + restriction
- + Muscle weakness
- Pain = Cramps
- ↑Use + PALPATION (”mechanical-like”)
- ⇒ Muscle work-up: check CK, EMG, biopsy, MRT

⛲ Leriche-Fontaine Classification:
STAGES:
- Øsymptoms → incidental findings
- Claudication
- >200m
- <200m + ↓daily activites
- Rest pain - IMPROVES with legs down (declining position)

- Rest pain - ØIMPROVE with legs down + TROPHIC changes

Clinic + ABI
Ankle-brachial pressure index (ABI) ratio betw. systolic ankle BP & systolic brachial BP:
Normal ABI = 0,9-1,3 PAD < 0,9 Calcified blood vessel (non-compressible) >1,4
- unilateral
- swelling, edema
- pain (deep muscle cramps)
- ØSigns of arterial P’s - only pain
- warm

- Homan’s + 📷
Homans: Calf pain on dorsiflexion
Other signs: Meyers signs (compression calf → pain); Payr sign (pressure on sole → pain)
- signs of PE (rarely)
dyspnea, chest pain, dizziness/weakness, tachycardia, hemoptysis
- signs of chronic venous insufficiency (varices + heavy legs)
Doppler US
*PCA
Patient-controlled analgesia → machine that give opioids when you press a button
- Neuropathic-pain → Anticonvulsants + antidepressants + steroids

- Spasticity → Muscle relexants

(+biphosphonates in bone mets)
↓
- 2. Etiological Tx
🦴 Joint pain
- pain
- swelling
- ↓function
- stiffness
- muscle fatigue
- 🔥Inflammatory
- 🗼Spondyloarthritis: Ankylosing spondylitis, IBS-related, Reaktive arthritis (Chlamydia/GI)
- ⚰️Sarcoidosis
- 🦠 HepB+C & Rubeola
- (👵🏼Degenerative)
- 🍋Metabolic → Gout
- 🦋Endocrine
- Hyper-/Hypo- thyroidism/parathyroidism
- DM
- 🦀Neoplasm
- leukemia, myeloproliferative tumors
- paraneoplasm (clubbing)
- 🩸Blood diseases
- RBC abnormality (thalasemia, Hb) → capillary obstruction
- Hemophilia → intra-articular bleeding
INFLAMMATORY | DEGENERATIVE | |
morning STIFFNESS | >30min (↑↑) | <30min (↑) |
PAIN | ↑Rest (+night)
↓Use + 🧊 COLD | ↑Use
↓Rest + 🥵 HEAT |
🗼spondyloarthritis → reiters + ankylosing spondylitis, IBD

REACTIVE = NO GERMS in joint aspirate
MIGRATING (from one joint to another) + BIG PERIPHERAL joints (KNEE)
⇒ symmetrical or assymetrical
⇒ Ø destruction
⇒ ARTHRITIS reflects ⇒ activity of BOWEL INFLAMMATION

- acute / subacute arthritis PROCEEDES acute HEPATITIS
- DISAPPEARS after onset of JAUNDICE
⇒ PHALANGEAL joints 📷 (Polyarthritis)

- intermittend OR permanent
- assymetric joint pain
- myalgia + fever
- +/- associated with PAN (polyarteritis nodosa) 📷
polyarthritis + tenosynovitis + SMALL joint synovitis
⇒ POOR response to NSAIDS → Tx of hepatitis instead
- men or post-menopausal woman, with RF:
- drinker
- obese
- stress
- Sudden onset MTP
- Tophi 📷
- Kidney stones
- Lab: ↑Uric acid (blood + urinary)

⇒ RED, SWOLLEN, TENDER
+ fever
Colchicine
or NSAIDs / steroids
hypo → morning stiffness
hyper → myopathy (muscle weakness) + shoulder periarthritis
visceral (mainly 🫁 lung)
ASSOCIATED with LUNG CANCER +other lung patho
Hypertrophic osteoarthropathy, known as Pierre-Marie-Bamberger syndrome, is characterized by clubbing of the fingers 📷due to bone surface and soft tissue calcification (periosteal reaction with new bone formation)
🐣 Pediatrics
- <1000g / below 3SD or <28w
- Life-threatening disease (pathologies) after birth
- Respiratory distress syndrome (SD) requiring respiratory support
- EUN (ulceronecrotic enterocolitis)
- BPC (chronic pulmonary disease)
- Apnea and bradycardia in newborns with bilirubinaemia > 20 mg/dl
- Newborns requiring transfusion
- Abnormal neuro exam
- twins
- alcoholic mother
SD = standard deviation 📷
⇒ In the first 48h after discharge if
- newborn stayed <48h in hospital
- preterm
- complications
⇒ after 3-5d after discharge if newborn stayed >48h in hospital
- General INSPECTION
- SYSTEM + ORGAN exam
- ANTROPOMETRIC MEASUREMENTS
- hearing loss + retinal detachments
- Cystic fibrosis
- PKU
- Endocrine (🦋hypothyroidism + 📐hyperplasia)
- hemoglobinopathies
- others
- appears early
- gets worse
- classic shit
- Jaundice: Appears within 24 hours of birth and intensifies.
- Fever: Temperature of 37.8 degrees Celsius in preterm infants.
- General influenced state: Child's overall condition is affected.
- Poor feeding/excessive sleepiness: Preterm baby has difficulty feeding properly and experiences excessive sleepiness.
⇒ MALFORMATION/deformation?
⇒ NUTRITIONAL status?
⇒ Respiratory movement? / Distress signs?
⇒ SKIN
- COLOR: CYANOTIC? JAUNDICE? PALLOR?
- LESIONS? milias, erythema toxicum, mongoloid spots, nevus, vascular patch
⇒ Body position + movement?
- Skin, mucosa, subcutaneous tissue, lymphatics(see general inspection)

- Chest malformations? (pectus excavatum/carinatum, intermamillary distance)
- 🩺 ⇒ 🫁 + 🫀
- femoral a. pulse; if ↓ = coarctation?
- normal conditions: diastasis recti 📷
a > 2 cm separation of the right and left rectus abdominis muscles resulting in protrusion of abdominal organs on straining
- excessive distension
- malformations? (ophalocele, gastroschisis, hernia)
- ✋🏼 Palpation

Back:
- Neuro tube defect sings? (skin discoleration, hemangioma, hairs)
- esp sacral insepection 📷
Extremity:
- movement: symmetrical, equal amplitude?
- syndrome signs? (syndactylsis, crease)
- check for hip instability
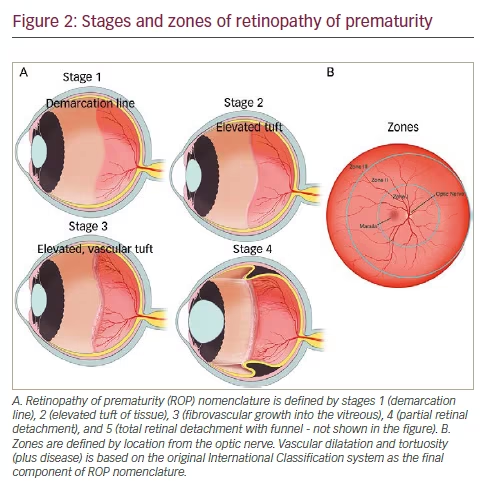
retinopathy
defined by → localization, extension + stages 📷
The condition is characterized by three parameters: localization (3 concentric zones around the optical disc), extension (correlated with the clock), and stage (ranging from 0 to 5, representing retinal vascularization and detachment).
- premature
- birth complications
- Hypoxia at birth
- Neonatal DR with oxygen therapy (FiO2 > 40%)
- Mechanical ventilation
- Intraventricular cerebral hemorrhage
- Hyperbilirubinemia or prolonged jaundice
- Neonatal sepsis
- Anemia of prematurity
- Necrotizing enterocolitis
- Neonatal shock with dopamine treatment
- FM
- TORCH

- Genetic syndromes
- Craniofacial defect
- abnormalites
- trauma
- Lenght + Weight
- Circumference
- Head
- Chest
1) Gestational age (GA):
Term | Weeks |
Late preterm | 34 weeks to <37 weeks |
Moderate preterm | 32 weeks to <34 weeks |
Very preterm | <32 weeks |
Extremely preterm | <28 weeks |
2) Weight (absolute + percentile)
Low birth weight (LBW) | Very low birth weight (VLBW) | Extremely low birth weight (ELBW) |
< 2500 g | 1500 - 2499 g | < 1000 g |
OR
LBW = below 10th percentile: 📷
ChrAge =

⇒ growth + development evaluation
⇒ made for weight, height + headcircumference
Corrected age is the premature baby’s chronological age minus how many weeks or months early they were.
Corrected age helps with tracking premature baby growth and development.
Ex: Child who got delivered 20 weeks ago but was born at 30 weeks GA (10weeks early preterm)⇒ corrected age = 20-10 = 10 weeks
- small (↓height) or big (obesity)
- too young/old (<20 OR >35)
- chronic disease (thyroid, asthma, mental)
- amniotic abnormalties (placenta previa, hydraminos, membrane rupture)
- drug abuse (alc, ciggs, drugs)
6 million (5,9) / year 2015 ⇒ 16.000 daily
1st week of life
1st hour
T
1500g (LBW)
VLBW+ELBW
⇒🍼 mother milk +⚡️ fortifiants
fortifiants:

15g / kg / day
immuno
nutrition
psycho + development
- Immunoglobulin transfer
- Optimal nutrient mix
- Emotional bonding
- 24/7 availability
- Reduced risk for several types of cancer (benefit for mother)
FFFFFFF ⇒ give it according to CHRONOLOGICAL AGE
(corrected age + weight of infants are not respected)
after birth/1m (again after 6m)
- Hep B → depends on birthweigh (>2000g → after birth, <2000g → can be done 1m after)
- The administration of the hepatitis B vaccine in the maternity hospital varies based on the mother's status, birth weight, and newborn's weight.
- If the newborn weighs below 2000g, the first dose of hepatitis B vaccine can be delayed until 1 month after birth.
- If the newborn weighs over 2000g, the first dose of hepatitis B vaccine is given on the first day of life.
- BCG
2month (every 2 month)
- Rota
- Diptheria, Tetanus, Pertussis
- Hemophilus influenza B
- Pneumococcal (conjugate vaccine)
- Polio (inactivated polio-virus vaccine)
1y
- Influenza (yearly)
- Mumps, measles, rubella
- varicella
- hep A
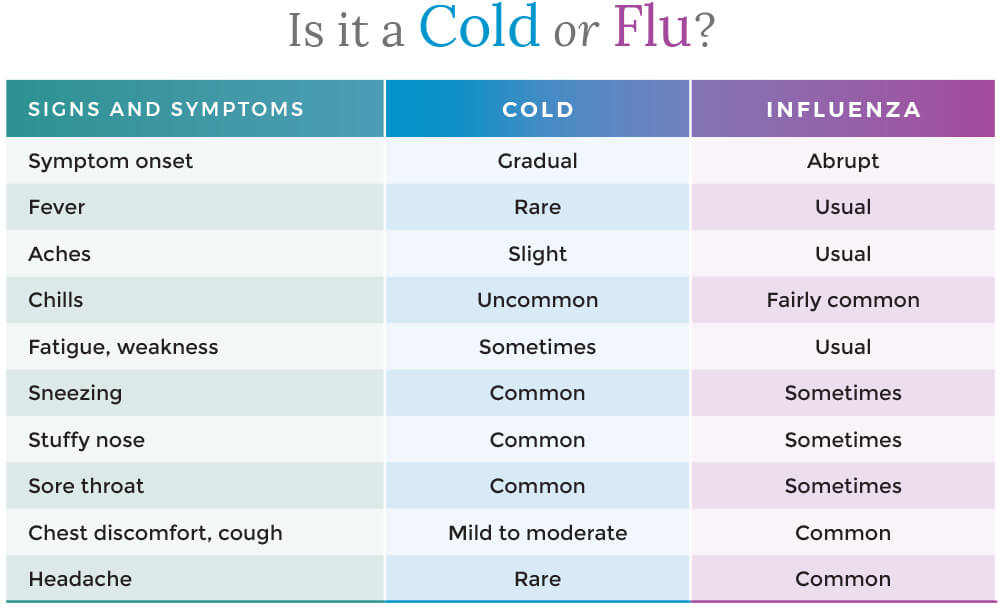
Children <6 years of age have in average 6-8 colds/years with a typical symptom duration of 14 days
🧫 1) BACTERIAL
Clinical presentation:
- 🧣Signs of Infection:
- Clinical exam: Hyperremia + Congestion (+ pus) 📷
- Symptoms + Signs:
- Pharyngitis:
- like viral: dysphagia, odynophagia (sore throat)
- petechia (on pallate) 📷
- Tonsillitis
- 🧫Specific signs of bacterial infection:
- PUS
- HIGH Fever
- ↑LN
- Exanthem (⇒scarlet fever) aka scalantiform rash 📷
- Ø viral symptoms! (Øcough, Ørhinorrhea, Ø hoarseness)
⇒ Etiology: Strep. pyogenes (aka beta hemolytic GAS)

Acute viral tonsillopharyngitis: children <5 years and young adults Acute GAS tonsillopharyngitis: children aged 5-15 years; rare in children aged < 2years
Centor score
The Centor score is a clinical prediction tool used to estimate the probability of a streptococcal infection in patients with a sore throat.
A score of 0-1 is considered low risk, 2-3 is moderate risk, and 4-5 is high risk.
- The score is calculated based on the presence or absence of four clinical criteria: fever, tonsillar exudates, tender anterior cervical lymphadenopathy, and absence of cough.
- Another criteria used in the score is the patient's age, with younger patients (<15 years old) being assigned a higher point value. This is because streptococcal infections are more common in younger individuals. Specifically, patients under 3 years old are assigned 1 point in the Centor score.
- Each of these criteria is assigned a point value, and the total score is used to estimate the likelihood of a streptococcal infection.
<3years:
- 👃🏽 nasal congestion
- 🤒 low grade fever
- 🟢 cervical ↑LN
<1year:
- 🍔 ↓ appetite
- 🤒 low grade fever
- 👨👨👦👦 older siblings/contact with GAS
- Local spread
- 2)👂🏼 Otitis media 📷+ Mastoiditis
- 3) 🎛️ Sinusitis 📷
- 4) 💪🏼 Necrotizing fasciitis 📷
- 5) Pneumonia 📷
- Systemic complications
- Pharyngitis signs + non-specific inflammatory
- +- GI signs
- 3) ⛑️ Auto-immune
- Rheumatic fever 📷 (JONES)
- PANDAS: neuropsychiatric disorder

aka “streptococcal bacteremia”
1. TOXIC Shock-signs(i.e. ↓BP+fever) + Exanthem (measle-like) 2. Evolution: - skin desquamation - multi-organ failure ☠️
erythrogenic toxin
(makes you red 👹)
→ 🩸hematuria → RF ⇒ 🥐 ↓GFR → 💳 ↑Crea

*patho
The incubation period of diphtheria is 2-4 days.
- ONSET: It has an insidious onset with sore throat and mild pharyngeal inflammation.
- A diagnostic feature is the 'wash-leather' elevated greyish-green membrane on the tonsils, called a 🧁 pseudo membrane. 📷
- ❤️ Tachycardia, despite modest fever, is a sign of myocarditis.
- 🌕 Neuropathy
→ The pseudo membrane has a well-defined edge, firm and adherent, surrounded by a zone of inflammation. It can extend to the larynx, trachea, or bronchia → airway obstruction.
⇒ 🐂 Swelling of the neck ('bull-neck') 📷 ⇒ 🟢 tender enlargement of the lymph nodes may occur.
There are three types of diphtheria:
- 🧣Pharyngeal diphtheria: Insidious onset of exudative pharyngitis. Exudate spreads to form adherent, malignant “pseudo membrane”: removal of the membrane reveals a bleeding, edematous mucosa. It can lead to respiratory obstruction and death by asphyxiation. Fever is not high, but the patient appears toxic.
- 🎙️ Laryngeal diphtheria: Either an extension of pharyngeal form (often) or the only site involved (rarely). Symptoms include mild fever (with little absorption of toxin), dyspnea, hoarseness, and a barking cough. The pseudomembrane can lead to airway obstruction, coma, and death.
- 💪🏼 Cutaneous diphtheria: Skin infections are quite common in the tropics and are probably responsible for the high levels of natural immunity found in these populations. Skin infections may be manifested by a scaling rash or by ulcers with clearly demarcated edges and pseudomembrane. 📷
- ↑Inflammatory markers
- ↓Plts
- severe cases: Damage of heart tissue ⇒ ↑LDH, CK, proteinuria
⇒ CULTURE (naso-pharyng. swab) ⇒ Löfflers ⇒ SMEAR + GRAM stain
The treatment for diphtheria should begin once appropriate swabs have been taken, before waiting for microbiological confirmation. Strict isolation should be used as pseudo membranes are highly contagious.
Antitoxin and antibiotics should be used for the neutralization of free toxin, elimination of further toxin production, and to control local infection.
Diphtheria antitoxin is produced in immunized horses. It will not neutralize toxin that is already fixed to tissues but will neutralize circulating toxin. Early use will prevent the progression of the disease. The earlier, the better.
For moderate disease ⇒ 16.000-40.000-100.000 U i.m. mild cases ⇒ 4.000-8.000 U.
Antibiotics like penicillin/amoxicillin or macrolides (erythromycin) should be used for two weeks to eradicate the bacteria and prevent further toxin production.
- Gram negativ Bacilli:
- Fusiform bacilli,
- Bacteroides ssp
- Spirochets (Treponema, Borrelia)
bacterial overcrowding due to:
- poor oral hygiene
- malnutrition
- AB → ✏️ Penicillin + 🚃 Metronidazole
- oral hygiene
- topical disinfectants

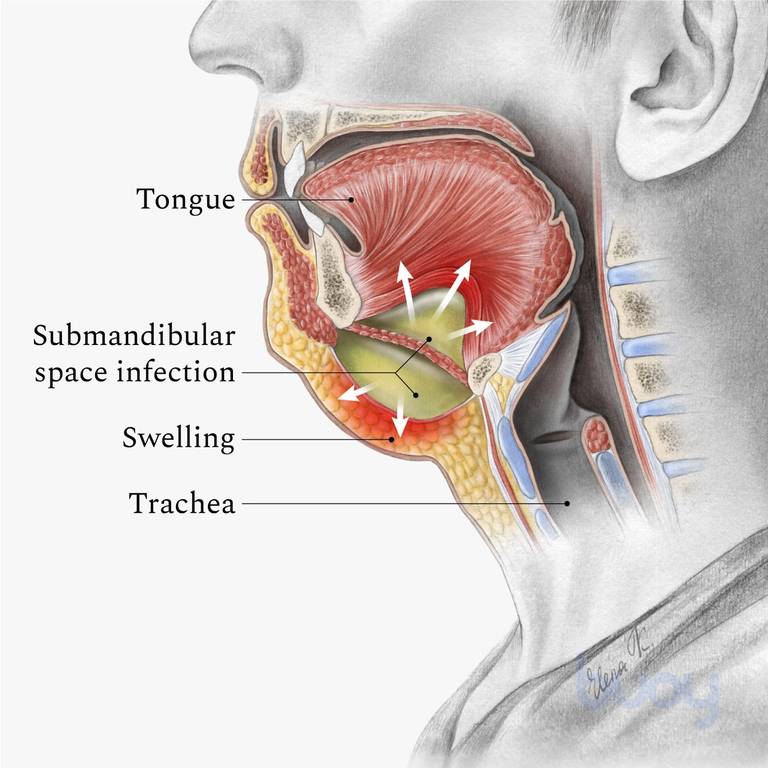
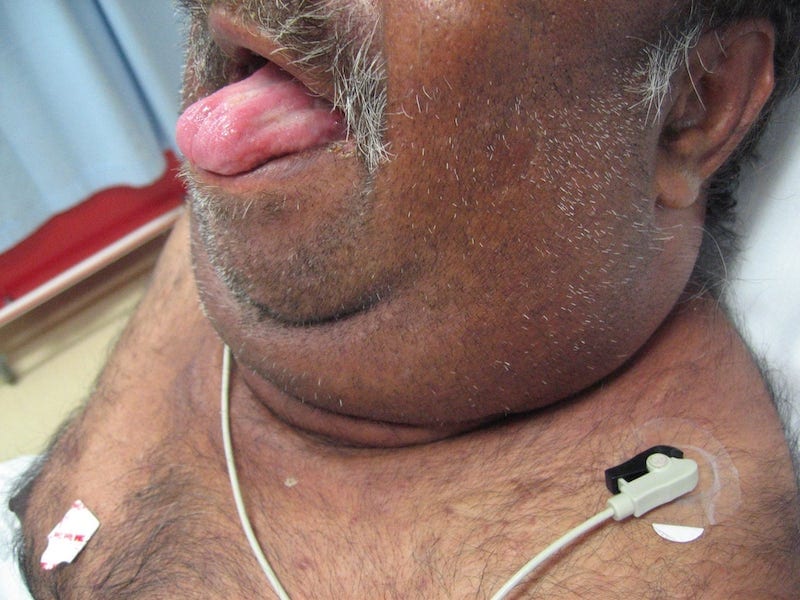
- Bilateral “wood-like” swelling
- double chin appearance
- Tongue protrusion (airway obstruction)
- Fever
- ØLN + ØAbscess
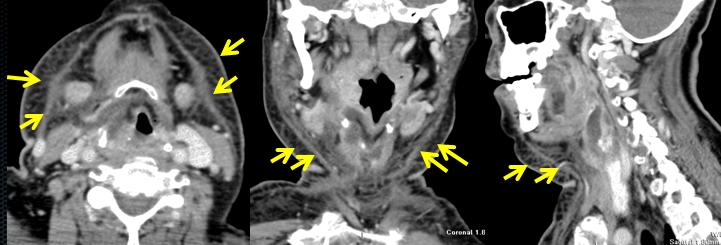
1) CT 📷
2)🩸 Blood + 💉 Needle aspiration ⇒ 🧫 CULTURE
🔪 SURGERY + 💊 AB

- Arcanobacter haemolyticum
- Pathogen: Arcanobacter haemolyticum
- Similar to GAS pharyngitis
- Occurs in adolescents and young adults
- Clinical features:
- Pharyngeal erythema and exudate
- Fever
- Cervical lymphadenopathy
- Distinguishing feature: Rash (>50%)
- Scarlet fever-ish
- Macular/maculopapular
- Involves distal extremities, typically extensor surfaces
- Spares palms and soles
- Rarely causes severe infections (e.g., pneumonia and pyomyositis)
- Can be a confecting agent

- 🎿 WALKING PNEUMONIA: M. pneumoniae + C. pneumoniae
- young adults <30y
- xray worse than clinical symptoms (=”walking pneumonia”)
clinical differentiator: history of recurrent pharyngitis
→ Patchy infiltrates on xray
⇒ Tx Macrolides
→ also causes walking pneumonia
🦠 2) VIRAL


Clinical presentation:
- signs of Infection: classic Pharyngitis
- Clinical exam: Hyperremia + Congestion
- Symptoms + Signs: dysphagia, odynophagia (sore throat)
- 🦠Specific viral signs
- 🌬️ cough (dry)
- ↕️ Assoc. rhinitis + laryngitis
- 👃🏼Rhinitis + sinusitis: rhinorrhea + nasal obstruction + sneezing sinus pressure
- 🎙️ laryngitis: dysphonia
- 💩 Diarrhea (nausea, vomiting)
- if adenovirus → conjunctivits
- +/- fever (if present LOW-grade)
Special viral + pedi: (esp if <6y)
- Irritability
- Feeding difficulties ! (nasal obstruct. / odynophagia)
- +/- ↑LN
⇒ usually Ø other systemic manifestations (digestive, LN, exanthem)
Criteria | Infants | Older Children (≥6 years) |
Onset | Often presents with fever | Symptoms include dry nasal passages and scratchy throat |
Clinical Manifestations | Varied symptom presentation | Less variability in symptoms |
Nasal Inflammation Symptoms | Nasal discharge common | Nasal obstruction is more prominent |
Fever | More frequent occurrence | Less frequently observed |
Behavioral Changes | Irritability and restlessness are more common | Less commonly irritable or restless |
Feeding and Sleeping Patterns | More likely to have difficulties | Fewer difficulties with feeding and sleep |
Lymph Node Enlargement | More commonly observed | Less commonly observed |
Etiology: (RACI) - rhinovirus (30–80%), - coronaviruses (≈ 15%) - influenza viruses (10–15%) - adenoviruses (5%) - others
CLINICAL DIAGNOSIS:
- Rhinitis signs
- Pharyngitis signs
- Minimal/Ø systemic signs (fever, headache, myalgia)
- Exclusion of DDx
- Non-infectious rhinitis → allergic, vasomotor, etc.
- Influenza
- bacterial pharyngitis
- Measles + Pertussis
- Any other respiratory infection w/ common cold = prodrome
Self-limited after 1w (adults) / 10-14d (infants)

- Influenza viruses are classified into four types: A, B, C, and D.
- Types A and B are responsible for seasonal epidemics of influenza, while type C causes mild respiratory illness and type D primarily affects animals.
⇒ A causes ENDEMIC + PANDEMICS (Ag drift + shift) ⇒ B only ENDEMICS (Ag drift only)

Antigenic DRIFT = point mutation Antigenic SHIFT = segments shared → new formation
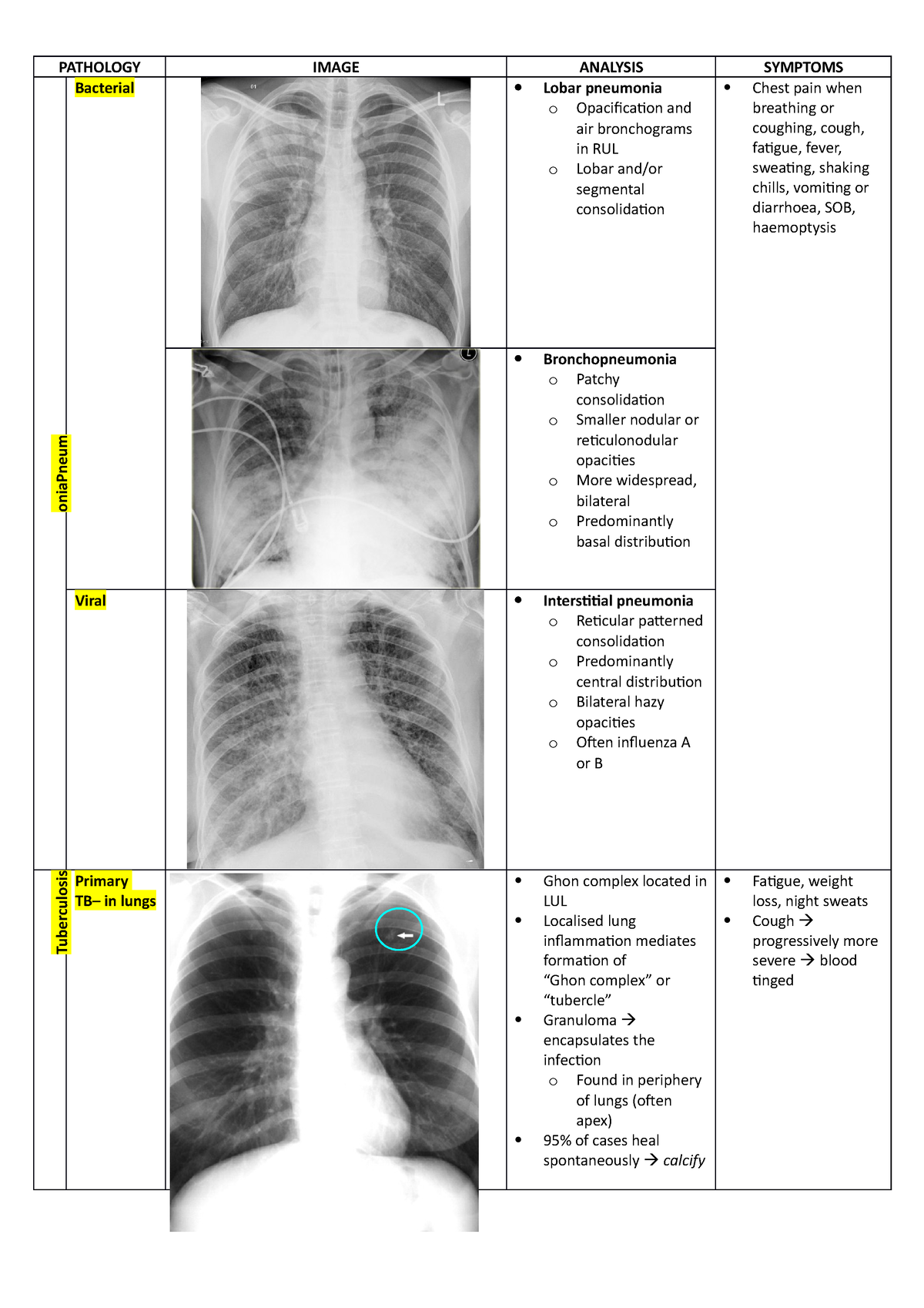
- 🫁 Respiratory: croup, bronchiolitis, primary influenza pneumonia – early (12-24 h), severe, hemorrhagic alveolitis with ARDS !
- mild interstitial prominence
- to poorly defined, 1- to 2-cm patchy areas of consolidation
- to extensive airspace disease due to hemorrhagic pulmonary edema
- cavity formation suggests bacterial superinfection with Staphylococcus
- pleural effusion is rare and usually represents bacterial infection
- characteristic appearance of ARDS: multifocal bilateral air-space opacities, in a predominantly perihilar and lower zone distribution = ground-glass opacity
- differential diagnosis includes: infection (common complication of ARDS), cardiogenic pulmonary edema, differentiation can be impossible in some cases
- causes of ARDS include: trauma, septicemia, hypovolemic shock, fat embolism, near-drowning, burns, viral pneumonia (influenza, SARS-CoV2, VZV), pancreatitis, oxygen toxicity, disseminated intravascular coagulopathy
- ARDS mortality is high, around 50%
- many survivors develop chronic lung disease, with damaged lung healing by fibrosis
- 🧠 Neurological: neuritis, 🐻 Guillain-Barre sd, transverse myelitis, encephalitis, cranial nerves palsies
- ❤️ Cardiac: myocarditis, pericarditis
- 💪🏼 Myositis, rhabdomyolysis (> in children, > with type B)

⇒ Influenza-virus pneumonia (primary)


- Infection of respiratory tract
- Sinusitis + Otitis
- Bronchitis
- Pneumonia (S.AUREUS!) / bronchopneumonia
- toxic shock syndrome (TSS) frequently reported during last epidemics due to some modifications of colonization and replication of toxins producers staphylococci induced by A and B viruses
- pregnancy severe evolution, double lethality teratogenic potential
- Exacerbation of underlying chronic diseases - COPD, asthma, cystic fibrosis (=risk groups → vaccination!)
- Influenza A, B viruses/ VZV + salicylates
- Acute encephalopathy + fatty degenerative liver failure
- Affects frequently children as well as other ages
- Other viral / atypical bacterial
- Covid-19
- Common cold
- Respiratory infections with adenoviruses, RSV, enterov, parainfluenza viruses
- Atypical pneumonia (Mycoplasma, chlamydia, legionella)
- Other disease’s onset with respiratory catarrh: measles, varicella
- Systemic infections
- Systemic disease’s onset: leptospirosis, brucella, typhoid fever
- Flu-like infectious diseases: TB, HAV, sepsis
- Influenza can be diagnosed through laboratory tests, including
- rapid antigen tests,
- PCR (viral Ag detection)
- Ø SEROLOGY!
-
viral culture. - Clinical evaluation and epidemiological factors (SEASONAL) are also taken into consideration for diagnosis.
- ✳️ Identification of groups of risk for severe forms, complications
- 🛏️Supportative
- Isolation
- Bed rest
- Diet
- Medication differentiated according to clinical forms – common/complicated/severe
- 💊Antivirals
- Protein
M2inhibitors:Amantadine, Rimantadine⇒ #not anymore! - NA inhibitors: Oseltamivir (Tamiflu), Zanamivir, Peramivir – iv, Favipiravir
- Endonucleases inhibitors: Baloxavir
- FAVIPIRAVIR (Avigan)
- Laninamivir (Inavir)
- Peramivir (Rapiacta, Peramiflu)
- Endonucleases inhibitors: Baloxavir
- severe forms: 🌝steroids


- High-risk groups: Children under 2 years old, adults 65 years and older, pregnant women (up to 2 weeks postpartum), residents of nursing homes and long-term care facilities.
- Medical conditions: Asthma, neurological and neurodevelopmental conditions, chronic obstructive pulmonary disease (COPD) and cystic fibrosis, heart disease (including congenital heart disease, congestive heart failure, and coronary artery disease), blood disorders (such as sickle cell disease), endocrine disorders (such as diabetes), weakened immune system (due to diseases, medications, or HIV/AIDS), kidney disorders, liver disorders, metabolic disorders, extreme obesity (BMI of 40 or more).
Complications of the flu include:
- Pneumonia
- Bronchitis
- Sinus infections
- Ear infections
- Worsening of chronic medical conditions, such as heart disease, asthma, or diabetes
- In rare cases, the flu can lead to respiratory failure, sepsis + multiorgan failre
Basic measures: 📷
ANNUALLY SEASONAL INFLUENZA 💉VACCINATION
→ IM (inactivated) quadrivalent → Intra-nasal (live attenuated) [! in pregnancy]
every person ≥6 month should get vaccination
incubation period: 5 days
contagious: 2 days before symptoms
- 🧣 URT VIRAL signs (”influenza like”)
- cough + sore throat
- congested nose (+- taste dysfunction)
- fever, muscle aches, fatigue, headache
- assoc. GI symtoms
- 🫁VIRAL PNEUMONIA signs (see below)
- dyspnea +- wheezing + cough
- assoc. URT (⇒ see “1.” ↑)
→ more common: young → a + b; elderly → c + d
- 🥍 RAPID-Ag or PCR
- Lab:
- Inflammatory markers?
- Lymphocytes?
- Thrombocytes?
- LDH?
- Liver, renal?
- Imaging ⇒ CT (or Xray) ⇒ GROUND GLASS OPACITIES: BILATERAL + PERIPHERAL 📷
Stage | Characteristics |
Asymptomatic or presymptomatic infection | Positive virologic test for SARS-CoV-2 (ie, NAAT or antigen test) but no symptoms consistent with COVID-19 |
Mild illness | ØLUNG, only URT + systemic:
Varied symptoms (eg, fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste or smell) but no shortness of breath, dyspnea, or abnormal chest imaging |
Moderate illnes | LUNG, but Ø severe
SpO2 ≥ 94% and lower respiratory disease evidenced by clinical assessment or imaging |
Severe illness | LUNG severe
Severe hypoxemia (SpO2 < 94%, PaO2/FiO2 < 300 mm Hg, respiratory rate > 30 breaths/min, or lung infiltrates > 50%) |
Critical illness or organ failure | ORGAN FAILURE / SEPTIC SHOCK
Respiratory failure, septic shock, and/or multiorgan dysfunction |
In a multivariate analysis comparing 16 critical COVID-19 cases with 310 asymptomatic, mild, or severe cases, the following predictors of increased disease severity were identified:
- Older age (P = 0.002)
- Lymphocyte declines correlated with high levels of IL-6 and IL-8 in patients exhibiting severe/critical disease.
- ↗️ symptomatic
- 🌝 corticosteroids systemic + other immunomodulator (IVIG, JAK-inhib)
- 🦠 anti-viral ⇒ 🐏 remdesivir + 💧convalescent plasma
Remdesivir:
A nucleotide analog → inhibits RNA synthesis. Has been shown to have in vitro activity against SARS-CoV-2. Its clinical efficacy is not well understood.

Convalescent plasma:

(Prevention = Vaccination)
- persistent cough
- fatigue














- ⛄3) Irritative pharyngitis

*Signs of respiratory distress → 📷
*Tripod → 📷
SUBGLOTTIC:
VIRAL → mainly: Parainfluenza virus 📸 (less common RSV 🪦 or others)
Inflammation + edema ⇒ 📷 narrowed subglottic area (obstruction)
⇒ more severe in smaller children (small larynx→ edema more impact of luman narrowing)
Clinical Indicator | Mild Severity | Moderate Severity | Severe Severity |
Stridor | Observable when agitated | Notable at rest | Present at rest (occasionally biphasic) |
Tachypnea | Absent | Mild presence | Moderate to severe |
Retractions | Absent | Mild to moderate | Severe |
Mental Status | Restlessness upon disturbance | Restless without disturbance | Lethargy |
- Viral → pneumonia, bronchiolitis
- bacterial → pneumonia, bronchiolitis, tracheitis, otitis media
- dehydration
- <0,5y
- moderate / severe
- poor oral intake / dehydration
- Toxic + high fever ⇒ DDx bacterial (membranous + epiglottitis)
- steroid refractory
- Øpossible at home
- other obstructive laryngitis
- other causes for airways obstruction
- abscess (peritonsillar, retropharyngeal)
- foreign body
- angioedema
- external compression
- other causes for laryngeal irritation
- GERD
- congenital anomalies
Non-inflammatory subglottic edema
contraction of larynx muscles
⇒ triggers/RF = laryngeal irritants: allergic, viral, adenoids, GERD, FH
- Membranous bacterial croup (Chevalier Jackson laryngo-tracheo-bronchitis)
- Diptheria
(Staph aureus)
SUPRAGLOTTIC:
- Acute epiglottis
→ 🅱️ Hemophilus influenza B
Pathology | Clinical Course | Stridor (Intensity) |
Viral Croup | Self-limited disease; worse at night | Yes (mild to severe) |
Spasmodic Croup | Short duration; recurrences | Yes (moderate to severe) |
Membranous Croup | More rapid deterioration compared to viral croup | Yes (moderate to severe) |
Epiglottitis | Rapidly progressive; respiratory arrest can occur within hours | Yes (often not severe) |
‼️ be careful with them → stress → trigger airway obstruction
contraction of laryngeal muscles or aspiration of saliva → apnea → resp. arrest
⇒ only performed when airways secured
⇒ in epiglottitis: only performed on ICU!!
NOT COMPULSARY!
LAB:
- Deyhydration?
- Oxygenation? (SpO2)
- Inflammatory lab?
PARACLINICAL: (usually Ø recomm. in viral)
⇒ Xray
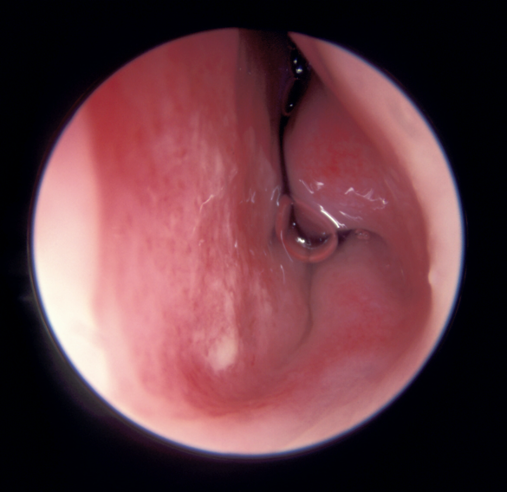
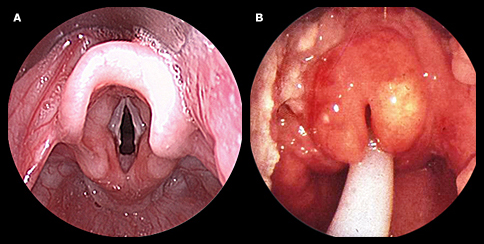
⇒ laryngoscopy 📷(+oropharyngoscopy)
left picture = viral croup
right picture = epiglottitis

- Steroids
- epinephrine
- humidified air
- intubation + ventilation
- hydration + O2
Mild Croup:
- Manage anxiety in infants.
- Utilize cool mist inhalation.
- Position infant in upright posture for sleep.
- Encourage cool air inhalation during colder months.
- Administer Dexamethasone:
- Effective in reducing airway inflammation within 6 hours.
- Available as oral syrup, IV, or IM.
Moderate to Severe Croup:
- Hospitalization is necessary for severe cases.
- Use inhaled racemic epinephrine:
- Efficient in reducing airway inflammation; faster than Dexamethasone.
- Apply Dexamethasone.
- Offer humidified air or oxygen when needed.
- Administer IV fluids to counteract dehydration.
- Intubation is vital when there's a risk to the airway (occurs in less than 3% of severe croup cases).
Note: Intubation can be challenging in severe croup due to narrowing of the subglottic region. An anesthesiologist's assistance is crucial.
- Rapidly improves without Tx (<1h)
- Symptomatic
- Cold night air
- Humidified air


- Single therapy often suggested with a third-generation cephalosporin (examples include cefotaxime, ceftriaxone) or a beta-lactam combined with a beta-lactamase inhibitor (such as ampicillin/sulbactam, amoxicillin/clavulanate, piperacillin/tazobactam).
- If there's a penicillin allergy in patients, opt for a fluoroquinolone like levofloxacin.
- To counteract MRSA, consider adding an antibiotic with anti-MRSA properties, e.g., vancomycin or clindamycin.
- Intubation in Severe Croup:
- Intubation is indicated when airway compromise is imminent.
- This procedure is required in less than 3% of infants with severe croup.
- A noteworthy point is the difficulty of intubation in severe croup due to subglottic narrowing. It emphasizes the importance of having an anesthesiologist present during the process, indicating the complexities and potential challenges of this procedure.
child presenting with stridor + respiratory distress
↓
- laryngeal signs? → croup → recurrent/Øprodrome → pseudocroup →common cold prodrome → croup → viral croup prodrome + high fever → membranous (also respect age; <3y ⇒ 0,5-3y - viral croup+pseudo; 0.5-7 - epiglottitis)
- muffled voice + drooling/dysphagia + Ø cough + high fever? → epiglottitis
↓
[SKIP Lab + Paraclinical exams to Ø aggrevate respiratory distress!!]
↓
Tx:
- pseudocroup → usually ØTx needed(symptomatic → humidified air, cold air at night
- Rest → steroids, epinephrine, humidified air, intubation + ventilation, hydration + O2
- epiglottitis + membranous croup → AB (Amoxi/Cephalorsporine)
“aka crepitations”
MAINLY VIRAL! 🦠
bronchitis: parainfluenza 📸; influenza A+B 👯♀️; others
others: common cold viruses + RSV
bronchiolitis: RSV 🪦 (rare bact.: myocoplasma pneumonia or other respiratory viruses)
- Vaccination Influenza A+B
- Pavilizumab (montly injection before RSV season)
- Infection control measures
- hand hygiene
- prevent cross-infection with other infants in the hospital (isolate infants with bronchiolitis)
- avoidance of tobacco smoke exposure
- encouragement of breastfeeding at least in the first 6mo of life

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Asthma
- Bronchiolitis obliterans

{kind=link}
{kind=link}
F → valuable!
⇒ Dg: PLEURAL effusion +pneumonia( consolidation, interstital pneumonia)
⇒ DDx: pneumothorax, atelectasis, cysts, tumors

CLINIC:

PARA-CLINIC:

{kind=link}

🏥 when:
- <6️⃣Ⓜ️ Age ≤ 6 months.
- 🚨 Severe OR complicated pneumonia.
- 🕰Associated chronic diseases
- ❌Failure to respond to initial ambulatory antibiotic treatment.
Tx:
⇒ 💊 supportive treatment + AB
Typical: 🎸amoxicillin p.o./ampicillin iv. OR Cefotaxim i.v.
Atypical: 🦅Macrolides p.o. OR i.v. (Clarithro, Azithro)
Setting | Patient Age | Bacterial Pneumonia | Atypical Pneumonia |
Ambulatory | 6 months - 4 years | First line: Amoxicillin PO Alternative: Amoxicillin-clavulanate PO | First line: Azithromycin PO Alternative: - |
≥5 years | First line: Amoxicillin PO Alternative: Amoxicillin-clavulanate PO Atypical pneumonia cannot be excluded: Beta-lactam PO + Macrolide PO | First line: Azithromycin PO Alternative: Clarithromycin PO | |
In hospital | - Immunized with Hib and PCV
- LOW resistance of S. pneumoniae | First line: Ampicillin IV Penicillin G IV Alternatives: Ceftriaxone IV Cefotaxime IV Atypical pneumonia cannot be excluded: Beta-lactam IV + Macrolide IV or PO Suspicion of CA-MRSA: Vancomycin IV or clindamycin IV | First line: Azithromycin PO or IV Alternatives: Clarithromycin PO Final height reached, macrolide intolerance: Levofloxacin IV or PO |
- NOT immunized with Hib and PCV
- HIGH resistance of S. pneumoniae | First line: Ceftriaxone IV Cefotaxime IV Alternative: Levofloxacin IV Suspicion of CA-MRSA: Vancomycin IV or clindamycin IV | First line: Azithromycin PO or IV Alternatives: Clarithromycin PO Final height reached, macrolide intolerance: Levofloxacin IV or PO |
- 🔥 Infection
- GI (Gastroenteritis)
- Extra-GI (UTI, strep throat, pneumonia)
- 🚧 constipation
- 😭 Colic w/ hypertonia
- Flushed face
- Occasional circumoral pallor
- Distended and tense abdomen
- Legs drawn up on the abdomen
- Cold feet
- Clenched fingers
- Stiff, tight, and extended arms
- Flexed elbows
- Arched back
- others: ruptured ovarian cyst, mesenteric lymphadenitis, adominal migraine

Features of hypertonia in infants with colic:
- 🚗 Trauma
- 🔥 Inflammation
- Appendicitis
- Necrotizing enterocolitis
- 🚧 Obstruction
- intussusception
- volvolus
- hernia
- adhesion (post-surgery)
- 🙋🏽♀️ adolescents pathology:
- peptic ulcer disease
- ectopic pregnancy
ACUTE = < 2weeks
💩 DIARRHEA ⇒ ↑stool freq (>2x than usual)
⇒ +/- 🤮vomiting / 🌡️fever /💥 abdominal pain
- Infection:
- 🥇 = 🦠: NORO + ROTA
- or 🧫 / 🪱
- Food poisoning 🧪
- Antibiotics 💊
- food intolerance 🥛
- surgical causes (intuss, append.) 🔪
- Intial chornic diarrha (IBD, celiac) 💩

- Diarrhea = non-bloody 💩
- vomiting 🤮
- fever 🌡️
- abdominal pain 💥
- irritable / tired 💤
- headache + myalgia 💪🏼
Complications:
- dehydration, 🐪
- Acidbase, 🧪
- electrolytes disturb, 🍌
- carbohydrate intolerance 🥛
→ if severe: seizures + death
Clinic suggestive for NORO:
- Age > 2️⃣ years
- 💉 history of ROTA-vaccination
- ☀️ spring + summer
⇒ STOOL tests (i.e. ROTA Ag-detection → ELISA)
- Fluid + electrolyte correction
- Route: enteral (or parenteral →if severe)
- Volume → Replacement + Maintenance
- volume replacement depending on severity
- exception: maintainence fluid = given by Early refeeding (age-appropriate)
- Give 10ml/kg for each diarrheic stool + 2 ml/kg for each vomiting episode
- Composition → oral rehydration (low salt + gluc)
- Rate → correct in 4h with teespoons (=5ml every 1-2min )
- Symptomatic:
- Anti-diarrheals ⇒ Racecadotril, Smecta
- anti-emetics ⇒ ondasetron
- Probiotics (↓duration of diarrhea)
- AB ⇒ usually not indicated (viral + self-limited)

(Loperamide contraindicated)

- 🐣 Child-specific cause
- young (<6m) / small (<8kg)
- underlying diseases
- 🧫 Bacterial clinic
- high fever
- bloody diarrhea
- 🐪 Dehydration problem
- dehydration= mod-severe
- prologend diarrhea (>7d)
- Oral rehydration Tx fails
- CV-instability
- 👨👩👦 Social causes


(double click to zoom)
{kind=link}
⇒ assoc. signs
NEPHROTIC + NEPHRITIC (see below)
- Edema secondary to heart failure in a child with diaphoresis, dyspnea on exertion, and/or history of heart disease.
- Acute urticaria and angioedema after exposure to allergens in a child with a history of food allergies.
- Liver failure/disease or protein loss enteropathy indicated by a history of jaundice, growth failure, steatorrhea, or abdominal pain.
- Nephrotic syndrome indicated by progressive weight gain, periorbital edema, and minimal systemic signs.
- Chronic kidney disease presenting with edema, anorexia, and growth deficit in a child.
- Turner syndrome in a newborn girl with edema of the hands and feet, short neck, nail dysplasia, ogival palate, and short 4th metacarpal.
inflammation of glomeruli
⇒ mainly due to immun-complexes
⇒ NOT due to infection!
- Hematuria (The urine looks smoky, and tea or cola colored.)
- Salt-retention ⇒ ↑BP + edema
- +/-Oliguria
+ Pyuria
end stage RF within weeks
prior GAS infection (URT, skin) → Ag-Ab complex → deposition in glomeruli → Complement activation (↓C3) → Inflammation (acute GN)→ glomeruli damage → hematuria and other signs acute GN
F - only when indications are met (see later)
Unknown cause → IgA Immunoglobulin deposition in mesangial cells 📷
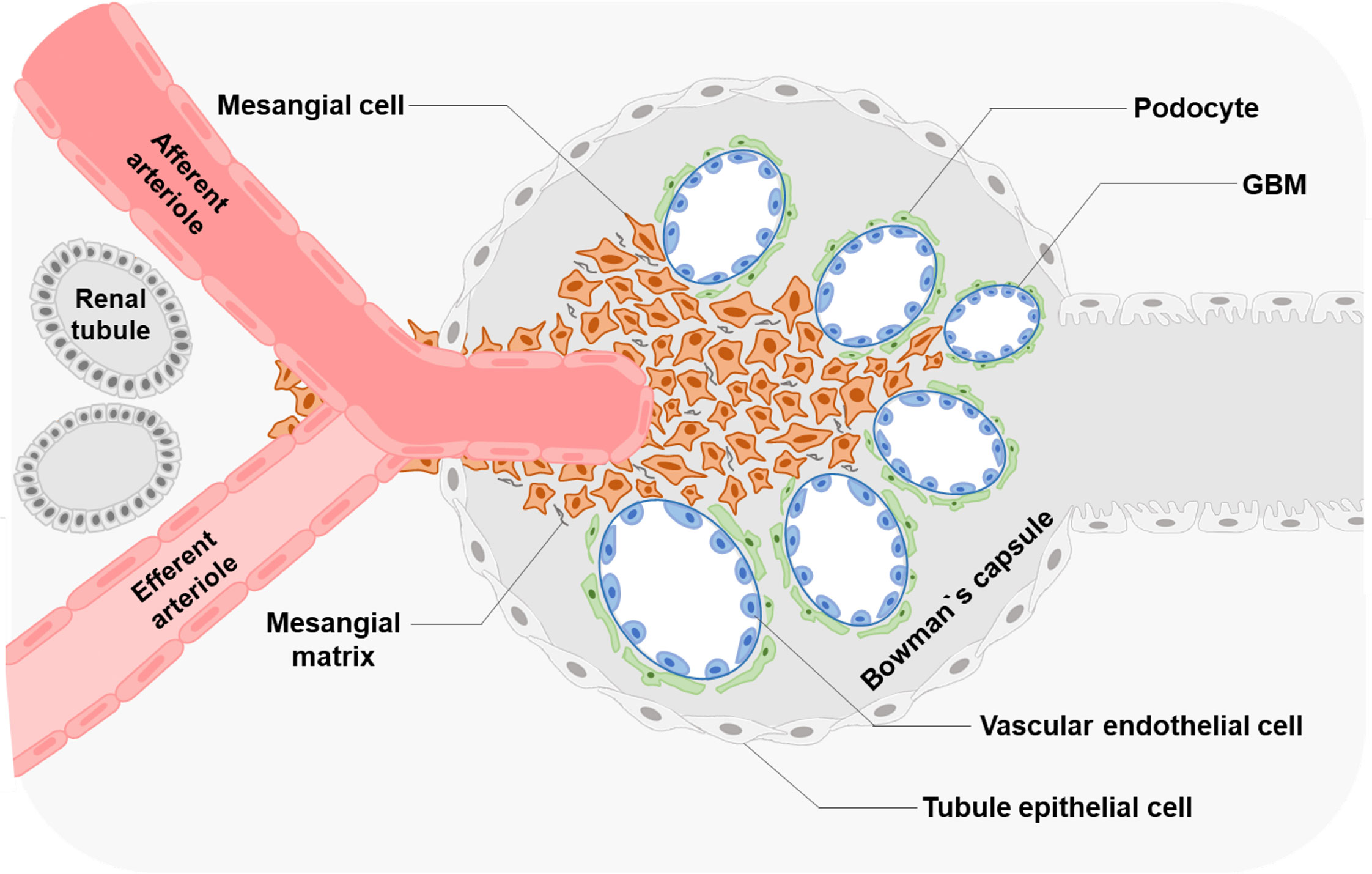{kind=link}
ØSystemic disease! (i.e. Henloch-Schönlein, SLE)
Probable mechanism: The synthesis of an increased number of defective IgA antibodies, often triggered by mucosal infections such as respiratory tract and gastrointestinal infections, leads to the formation of immune complexes that deposit in the kidney, resulting in glomerulonephritis.
T
(APSGN = secondary)
T
(histo findings → see later)
Disease | Post-infectious | Acute nephritic | RF |
APSGN | 1-6 WEEKS | ✅ | Acute RF |
Berger | 1-2 DAYS | ✅ | Rare - Acute RF,
→ progression end stage RF within 20-25y |
*acute nephritic sy = acute GN = hematuria, ↑BP, edema, oliguria
APSGN:
- child >3y (max inc. 5-15y)
- 1-6 w after GAS
- 50% asymptomatic
- Acute nephritic syndrome
- Acute RF (50%?)
- rare: nephrotic sy
Berger:
- (max. inc. 10-35y)
- VARIABLE PRESENTATION/EVOLUTION
- Recurrent (isolated) gross hematuria
- 1-2days after URT / GI infection
- assoc. with loin pain
- Persistent microscopic hematuria / proteinuria
- Acute nephritic syndrome
- CRF
- rare: acute RF, nephrotic sy

- Pure nephrotic sy.
- Impure nephritic-nephrotic sy.
→ nephrotic proteinuria (+++)
→ Hypoalbuminemia → Edema (+weight gain)
→ pure nephrotic + sings of glomerular inflammation (hematuria, ↑BP, ↑BUN)
Typical Features | Nephrotic Syndrome | Nephritic Syndrome |
Onset | Insidious | Abrupt |
Edema | ++++ (anasarca) | ++ |
Blood Pressure | Normal | Raised |
Jugular Venous Pressure | Normal/low | Raised |
Proteinuria | ++++ | ++ |
Hematuria | May/may not occur | +++ |
Red Blood Cell Casts | Absent | Present |
Serum Albumin | Low | Normal/slightly reduced |
in nephrotic edema starts periorbital; DDx in nephritic = gravity dependent-edema (legs first)

- infections (Ig loss)
- Relative Hypovolemia (due to ↓Albumin)→ ARF → Anemia (↓EPO)
- Thrombosis + ↑CV-Risk[ArtScl] (comp. Increase in fibrinogen + lipoproteins)
- Growth failure

minimal change disease
(max. incidence = 1-7y) ≤ 10 y → 90% of cases
≥ 10y → 50%
pure NS + normal renal function
→ nephritic components might be present
try steroids (no biopsy first)
- Oral prednisone: dose of 60 mg per day (maximum 60 mg/day)
- after remission (Ømore proteinuria) → for 30 days with the same dose → then “wear off”
→ response → steroid sensitive
→ Øresponse → steroid resistant → biopsy:
⇒ foot process effacement 📷or other glomerulopathies (DDx)
{kind=link}
- Steroids! ⇒ classification accoring to response
- Nephrotic syndrome sensitive to steroid therapy
- Nephrotic syndrome resistant to steroid therapy
- steroid dependent
- frequently relapsing
- Edema Tx
- Diet
- Sodium restriction
- NORMAL protein intake ❗
- Human albumin if
- albumin (serum) < 1,5g/dl OR
- anasarca (sev.+ generalized)
- ØDiuretics (predni has best “diuretic” effect)
- respiratory distress / GI symptoms
- after human albumin
- Ø response for predni
- Complications Management
- Infectious Tx (vaccination, + infection tx if occurs)
- DVT (mobilize, avoid hypovolemia, Øanticoagulation rountinely)

→ should be followed by iv diuretics
⇒except:
vaccination: pneumococcal + chickenpox
- 🍑 LIVER
- congenital disease
- Deficiency in Alpha-1 antitrypsin-DAAT
- Cystic fibrosis
- Wilson's disease
- infections (Hep)
- 🎋 BILIARY
- Biliary atresia
- Allagille syndrome (deficit in the development of intralobular bile ducts)
- ❤️ congenital heart malformations
- ⭕ blood vessel
- vasculitis
- antiphospholipid syndrome
- hyperviscosity
- contraceptive pill
- nephrotic
- cancer
- 🛌 immobility
- obesity
- Lymphedema prae-cox (most common) 📷
- Congenital
- Milroy
- Aagenes
- Turner+Down, Noonan
- Late
- Lymphedema prae-cox = Meige disease (77 to 94%)
- Onset at puberty
- More common in females
- Edema of the foot and leg
- Congenital lymphedema (6 to 12%)
- Present before the age of 2 years
- Small number of lymph vessels
- Hypo/hyperplasia and fibrosis of the lymph nodes
- Assoc. disorders:
- Milroy's disease
- Bilateral lower extremity edema immediately after birth
- Relatively stationary evolution
- Mutation in the gene encoding VEGFR-3
- Aagenaes syndrome
- Congenital lymphatic hypoplasia and recurrent cholestasis
- Lymphedema typically occurs in the feet of infants
- Turner Syndrome, Noonan Syndrome, Down Syndrome
- Late lymphedema (11%)
- Typical onset after 35 years
- Cancer and its treatment
- Infections: filariasis, nematodes (Wuchereria bancrofti is the most common cause)
- Autoimmune diseases: Sarcoidosis, Idiopathic juvenile arthritis, Crohn's disease
⇒ 📷
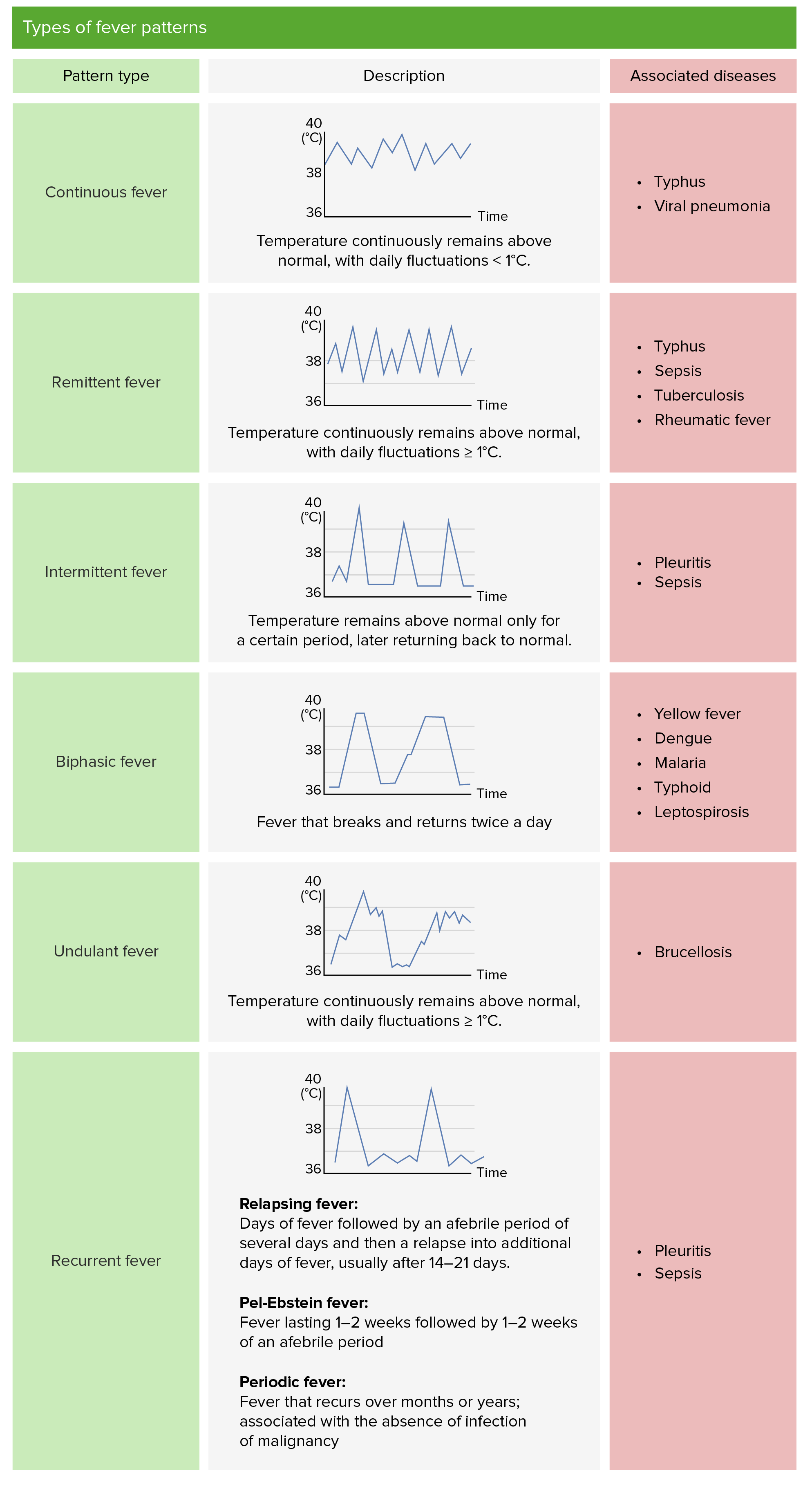{kind=link}
- continuous fever (above normal through day, fluctuation <1°C)
- remittend fever ( fluctuating >1°C in 24h but never normal)
- intermittend fever (normal temp periods)
- recurrent/relapsing fever (short febrile episodes between days of normal temp)
- Undulent/wavy fever (like recurrent but smaller variation + low grade fever insted of normal periods)
OTHER TYPES OF FEVER:
- Habitual fever: slightly higher temperatures than normal in clinically healthy individuals
- Septic fever: diurnal variations, accompanied by profuse sweating and chills, associated with septicemic syndromes
- Catheter fever: secondary to invasive procedures such as cystoscopy or catheterization, caused by transient bacteremia
- Psychogenic fever: due to emotional stimulus, transient in nature
- Fever in irregular system diseases, endocarditis, abscesses, necrotizing pneumonia, septicemia
- Prodrome: Asthenia, headache, chills, myalgia, arthralgia
- Standing Phase: Warm skin wheal, tachycardia, tachypnea, profuse sweating
- Defervescence: Normalization of fever, reduction in tachycardia and tachypnea
- Infection:
- 🦠 → URTi (i.e. EBV) + GE
- 🧫 → meningitis, OM, pneumonia, TBC, UTI, endocarditis, sepsis etc.
- 💉 Post-Vaccination → hour-days

💊 ⇒ see below for more details

- Classics
- CBC
- 🔥 Inflammatory markers (ESR; CRP)
- 🫁Lung → Chest Xray
- 🟡 UTI → Urine workup (dipstick, microscopy, culture, antibiogramm)
- 💩 GE → GI workup (Ag-test, stool microscopy, culture, occult blood test)
> 38°C lasting for > 3-4 weeks with Ø clear etiology despite appropriate diagnostics (Øsigns, symptoms, paraclinic)

- Classic FUO → fever >3w, dgx uncertain after 3 consultations
- Neutropenic FUO → classic + neutropenia (<500)
- FUO assoc. with HIV → fever >4w, +HIV history
- nosocomial FUO → in hospital, Øsigns on admission, dgx uncertain after 3 consultations
- 🦠🧫 Infection
- ENT: pharyngitis-esp EBV!, sinusitis, OM(+complications)
- Pulmo: Pneumonia, TBC
- Other
- 🛡️ Inflammatory (Auto-immune)
- Rheumatic fever → EKG + ASLO
- Juvenile idiopathic arthritis ⇒ INTERMITTENT fever
- SLE
- 🦀 Neoplasia
- Leukemia (low grade, irregular)
- Lymphoma (undulant + recurr.)
- Neuroblastoma
- Other
- 🧠 CENTRAL origin → infection, drugs, trauma (resorption)
- Prolonged fever due to drug allergies induced by antibiotics
- Impaired thermoregulation causing prolonged hyperthermia due to cocaine use
- Prolonged febrile syndrome accompanying trauma with hematoma, massive necrosis, and burns over large areas
- Periodic fever → recurrent
- Familial Mediterranean Fever (FMF):
- Autosomal recessive disease
- Associated with arthritis
- Important to differentiate from Rheumatic Arthritis (RAA)
- Marshall Syndrome:
- Characterized by the acronym PFAPA (Periodic fever, oral thrush, pharyngitis, and cervical lymphadenopathy)
- Occurs periodically, and the child may appear clinically healthy without fever during symptom-free intervals.

CNS infection, endocarditis, hepatitis, cholecystisis, UTI, etc.

- Fever (>38°C) +Seizure
- Short (<15min) but they can also be longer
- Benzos → Diazepam
- i.v. - 0,5mg/kg/dose
- rectally
- Fever Tx (Anti-pyretics+ cold wraps)
Temp >41°C
Hyperthermia PLUS end-organ failure signs
Signs of end-organ failure
- 🧠 - ↓conciousnes, convulsion, tremor
- 🫁 - tachypnea
- ❤️ - ↑HR, ↓BP, cyanosis
- 🥐 - anuria
Both: Fever Tx + 🏥 hospitalization
- Lower the child's temperature by removing clothing and giving a general bath with water that is 1-2°C cooler than the child's temperature.
- Administer antipyretics such as Paracetamol, Ibuprofen, or Algocalmin.
if heatshock ⇒ Tx of complications
see also ⇒ non-pharma Tx
see ⇒ Chest pain (adults)