





Epidemiology
🎗️ Basics of Epidemiology
Standard precautions= Minimum measures to prevent and limit healthcare-associated infections, applied to all patients regardless of the patient's suspected/confirmed status.
Examples of precautions:
Hand hygiene, protective equipment, safe injection practices and handling of medical equipment, respiratory hygiene and cough etiquette.
1. 📖 Knowledge about
1.1 Disease + Exposure
1.2 Environment → food, water, blood safety
2. 👁️ Surveillance ⇒ Recognition + Identification → reported by primary healthcare worker (passive disease reporting)
“There can also be cases which meet laboratory criteria but not clinical criteria/with unknown clinical criteria”
⇒ clinic + epidemiology = probable ⇒ clinic = possible
- LABORATORY CRITERIA (Antigen ➕ → rapid test or PCR)
- CLINCAL CRITERA (cough, fever, shortness of breath, anosmia or dysgeusia)
- EPIDEMIOLOGICAL CRITERA (close contract past 14d; working in contitution with confirmed case)
- RADIOLOGICAL CRITERIA
3. ❌ Neutralization of carrier ⇒ limit transmission, Tx.+ education
4. ✋🏼Pathogenic transmission prevention (disinfection, rodent control)
5. 💉 Active immunization
6. 🎓 Health education (+promotion)
- Dgx (confirmed, probable, possible)
- Isolation
- +/- Patient notification / Hospitalization (i.e. meningococcal menigitis)
- Epidemiological outbreak investigation (collect + process indiv./general data ⇒ epidemilogical, etiological, prognosis (outbreak liquidation plan))
- Measure in
- Counseling + Public information
5.1 Environment of cases (disinfection)
5.2 Prevention in close contract(surveillange, vaccine, chemoprophylaxis)
🚬 smoking
🍷 alc
🍔 overnutrion
😮💨 Stress
15-49y
consumption of 4-6 units per day or 28-42 per week is risky, and above these limits affect health
(women = half the values)
- 500 ml of lager beer is equivalent to 2 units.
- 125 ml of wine is equivalent to 1.5 units.
- 175 ml of wine is approximately 2 units.
- 25 ml of spirits is equivalent to 1 unit.
HEAVY episodic drinking: >6 standard drink (≥60g) on 1 occasion / month
Protection | Promotion |
Legislation + Control
(prices, alc content, minimum,age, etc) | Education + Programms |
Warning labels | |
Replacement with low alc. content (Less hazardous drinking ) |
- Descriptive studies: Studies of distribution (among people, places and time) and frequency of risk factors and diseases.
- Analytical studies: Studies of causative factors, host characteristics and environmental exposures that influence disease occurrence.
- PCR
- Electrophoresis
- Blotting (macromolecule)

→ Pathogenesis ⇒ New standards for descriptive studies (↓Heterogeneity)
➕ PROS | ➖ CONS |
↑Se + Sp | mixed culture! → Too specific → clinic must support ?? |
Fast results | Expensive (but cost efficient) |
- Prevention of transmission ⇒ quick Dgx
- Source identification + Virulence ⇒ Prognosis
- Accurate + Fast Dgx → i.e. if highly infectious pathogen (brucella, francisella)
- Difficult culture
- Non-culturable → 🦠 viruses (EBV, HBV)
- 🐌 Fastidious (slow growing) → TB, Legionella
- ↓ Amount of pathogens → HIV, CMV
Segregation studies→ recessive/dominant 📷

Linkage studies→ part of chromosome 📷

Associated studies→ Alle of gene 📷
Genetic epidemiology: Studies the role of genetics in determining diseases in families and in the population, as well as their interplay with environmental factors. Uses strategies like segregation studies (pattern of inheritance: Recessive/dominant), linkage studies(which part of chromosomes are involved) and associated studies(which allele of which gene is associated).
- 3️⃣ Trisomies ⇒ 21,13,18
- 🐌 Cystic fibrosis
- 👵🏼 Alzheimer
- Early onset(30-60 years old)
- Late onset(>60 years old) → chromosome 19
Chromosomes:
→ 1 (presenilin 2 mutation) → 14 (presenilin 1 mutation)
→ 21 (amyloid precursor protein mutation) are involved.


Cancer molecular epidemiology: Utilizes biological markers to study disease progression and identify environmental and genetic factors involved in cancer development. Factors include environmental (place of residence, lifestyle, occupation, exposure) and genetic (age, race, sex, ethnicity, family history, genetic "susceptibility" genes).
- Relatives with breast cancer at <50 years old,
- family history of breast/ovarian cancer,
- women in the family with cancer in both of the breasts,
- cancer in a male relative,
- and family history of other gland-related cancers(pancreatic, colon and thyroid).
💉 Immunization & Chemoprophylaxis


serum sickness if 6-12d after; if before: accelerated serum reaction **Arthus → also Type 3 hypersens.
F ! ⇒ Ø contraindication
“1. There are no contraindications to simultaneous administration of most vaccines.
2. Minimum intervals and ages: Vaccine doses should not be given at intervals less than the minimum intervals or earlier than the minimum age. Best response to vaccines is in childhood being diminished in the elderly.”
- Administration site:
- Infants up to 12 months: Anterolateral thigh
- Older children: Deltoid
- Routes:
- IM (90°) or
- SC (45°)
- Multiple vaccinations are done at different sites (2-4cm apart)
Feature | 🧬 Live attenuated vaccines | ☠️ Inactivated vaccines |
Definition | Bacteria/viruses are rendered non-pathogenic using genetic manipulation, laboratory culture serial passages, and replication after injection | The agents are inactivated using heat or chemicals |
Immune response | Humoral and cellular
(replicates after injection → latency) | Only humoral
primary response: 7-10d → IgM + G later (minimum limit: after 2-6 weeks) |
Lifelong immunity | Yes, usually | Several doses needed |
Side effects | ↑MORE common | ↓LESS common |
Preperation/Constituents |
DNA Vaccines
RNA Vaccine
Corpuscles (live/inactivated) | Suspension fluid(sterile water or saline± proteins), preservatives, stabilizers, antibiotics(never penicillin!), and adjuvants(aluminum salt to enhance the immune response but it can cause local irritation)- |
🧬 LIVE
- 🦠VIRUSES:
- MMR
- Vaccination given to staff in units with high exposure to rubella/measles, units with obstetrics-gynecology services, neonatal-pediatric units, ENT, and CVD units.
- Vaccination should be given to staff members >25 years old, unvaccinated with absent/uncertain history of measles/rubella.
- Staff members with rash appearance should be excluded from service for 5 days (rubella infectiousness decreases 5 days after the rash onset).
- Influenza intranasal - complex (also inactivated - I.M.)
- Polio - complex
- Varicella
- Varicella zoster (chickenpox) vaccination is recommended for specific groups:
- People in contact with newborns
- Pregnant women
- Immunocompromised individuals
- People from infectious diseases hospitals
- Post-exposure vaccination within 3-5 days after exposure for:
- People with immunodeficiency
- Individuals not vaccinated or with incomplete vaccination
- It is a live attenuated vaccination administered subcutaneously.
- Two doses should be given, 4-8 weeks apart.
- Rotavirus
- 🧫 BACTERIA
- BCG - monovalent
- 🍄 FUNGI (rarely - Candida)
Measles and rubella prevention:
Influenza vaccine: Administered annually during the flu season, particularly for high-risk individuals.
☠️ INACTIVATED
- 🧪 (toxins)
- Diph
- Tetanus
- 🦠VIRUSES:
- Hep A+ Hep B
- Influenza (i.m.)
- Polio
- Rabies
- 🧫 BACTERIA
- capsulated (polysachhardies)
- subunit/whole (acellular)
→ S.pneu, N.mening, H.Influenza B
→ pertussis (DTP)
Recommended Age | Vaccine Type | Notes |
First 24h - 7d | Hepatitis B immunization (Hep B) | Initial protection measure. |
At birth | BCG vaccine | Prevents severe forms of tuberculosis. |
2 months (2mo) | DTPa-VPI-Hib-Hep. B | Combined vaccine for multiple diseases. |
Pneumococcal conjugate immunization | Shields against pneumococcal infections. | |
4 months (4mo) | DTPa-VPI-Hib-Hep. B | Booster dose for sustained immunity. |
Pneumococcal conjugate immunization | Second dose for enhanced protection. | |
11 months (11mo) | DTPa-VPI-Hib-Hep. B | Continuation of vaccination schedule. |
Pneumococcal conjugate immunization | Additional dose for long-term immunity. | |
12 months (12mo) | MMR (Measles-Mumps-Rubella) | Essential vaccine for common childhood diseases. |
5 years (5yo) | MMR (Measles-Mumps-Rubella) | Booster to maintain immunity. |
5-6 years (5-6yo) | DTPa-IPV (Acellular Diphtheria-Tetanus-Pertussis) | Follow-up dose for extended coverage. |
14 years (14yo) | dTpa (Adult form of DTPa) | Updated formulation for teenagers. |
- 🤧 Allergy → vaccine component
- ❌ Sev. illness
- 🧠Encephalopathy
- 🦯 ↓ Immunity ⇒ ØLIVE vaccines
- HIV (MMR can be given!)
- Pregnancy (traveling safe: between 18-24w; week 20: DTP booster; influenza whenever; ØBCG vaccine if mother took steroids in T1/T2 for >2w)
- 🆎 Recent blood products



- Routine
- MMR
- DTP
- Hepatitis B
- Varicella
- Influenza (anual)
- COVID
- Variables: Attack rate in vaccinated (ARV) and non-vaccinated (ARNV), reduction rate of AR in vaccinated and non-vaccinated, and vaccination effectiveness (VE).
- VE (%) = (ARNV - ARV) / ARNV
- RR = ARV / ARNV
- EV (%) = (1 - RR) x 100
- Errors in VE calculation can be due to factors that increase ARNV (resulting in overassessment of EV) or factors that increase ARV (resulting in underassessment of EV).
- Quick estimation: The ARV and ARNV are unknown, but the proportion of vaccinated cases (PVC) and proportion of vaccination population (PVP) can be calculated:
- PVC = [PVP - (PVP x EV)] / [1 - (PVP x EV)]
Can be with antibiotics, antivirals, antifungals and others(aspirin to prevent strokes; anticoagulants to prevent MI)
Monoetiological Infections | Plurietiological Infections | |
Source (Microorganism) | Exogenous
(eg influenza, scarlet fever
meningococcal meningitis,
tuberculosis) | Exogenous and esp. endogenous |
Transmission Risk of diseases | Medium or high | |
Administration | Rate and doses = same as normal Tx
→ but with shorter durations | According to varied individualized schemes, often in combination with active and/or passive immunoprophylaxis |
Use | Individual use or in population groups | Pre or peri-interventional (surgery), single dose or short duration |
Resistance | Only for microorganisms that do Ø develop resistance to antibiotics |












Cause | Timing | Drug and administration | Indication | Ø recommended |
Meningococcal infections | ASAP/within 24 hours | -🪓Ceftriaxone
-🌷Ciproflox
- 🔫Rifampine | High-risk contacts
high-risk contacts (household, nursery school, people directly exposed during patient resuscitation or transportation) as well as in outbreaks or clusters (only for high-risk contacts too, unless authorities decide to provide chemoprophylaxis for everyone). | Not recommended for low-risk patients (casual contact, indirect exposure) |
Whooping cough | For unvaccinated contacts exposed to a confirmed case within 21 days of cough onset. | - 🦅Macrolides
- 🥚TMP/SMX | Unvaccinated contacts | |
Influenza | Within 48 hours of exposure. | 👩🏼⚕️ Oseltamivir | High-risk unvaccinated contacts | Recommended only for high-risk unvaccinated exposed people. |
Traveler’s diarrhea | Not usually given for healthy travelers, depends on the risk at the destination. | 💩Rifaximin can be used for immunocompromised people or travelers with short travels/sport competitions. | Immunocompromised people or travelers with short travels/sport competitions | |
GAS tonsillar-pharyngitis | Penicillin G | Confirmed cases and contacts with symptoms of pharyngitis | Ørecommended in families or collectives because of the low transmission risk. | |
Prevention of infections before/after splenectomy | At least 2 weeks before surgery | 💉 Vaccine:
- S.pneu
- N.mening.
- H.influenza | ||
Diphtheria | - ✏️ Penicillin G single dose or
- 🦅 erythromycin for 7-10 days | Carriers should be treated, and close contacts should be given a booster vaccine | ||
Malaria | Annual |
-👸🏼mefloquine
-🚴🏼doxycycline
-🧛🏼♀️atovaquone-proguanil | ||
Endocarditis | High-risk patients: Valvular prosthesis/intracardiac devices, history of endocarditis, unsolved congenital cyanotic heart malformations, heart transplants with residual valvopathy.
Intermediate-risk patients:
- Mitral prolapse,
- bicuspid aorta,
- calcified aortic stenosis.
🦷 *Procedures/Damage:
Gingival and endodontic manipulation and oral mucosa perforation. (Øimplants) | Dental implants aren’t associated with an increased risk, and they are not contraindicated even in high-risk patients.
Chemoprophylaxis isn’t recommended in respiratory tract, GIT, urogenital and soft tissue procedures. | ||
Surgical procedures | The antimicrobial agent should be chosen carefully. The risk of C. Difficile diarrhea after antibiotic prophylaxis should always be considered. | Primary prophylaxis (prevention of initial infection), secondary prophylaxis (prevention of relapse/reactivation of a pre-existing infection), and eradication (elimination of the pathogen).
Prevention of surgical wound infections (SSIs), without side effects affecting the patient’s normal flora. | ||
🪝 Pathologies
- Coronary heart disease (IHD, MI, Percutaneous Coronary Intervention, Coronary Artery Bypass Grafting)
- Stroke (cerebrovascular disease)
- Peripheral arterial disease (PADI)
- Hypertension
- Deep vein thrombosis and pulmonary embolism
- Older age
- Male gender
- Family history of CVD
- Ethnicity
“Systolic pressure rises with age throughout life in Western populations, whereas diastolic pressure plateaus in late midlife and decreases thereafter”
- 🚬Smoking
- ≤ 3 drink = protective

- ≥3 drinks (4-6U/d or 28-42/w ; = harmful → ❤️: BP, arrhythmias, myocardial dmg → 🩸hypercoagulability)
- 500 ml of beer is equivalent to 2 units
- 125 ml of wine is equivalent to 1.5 units
- 175 ml of wine is approximately 2 units
- 25 ml of spirits is equivalent to 1 unit
- 🐽 Metabolic:
- 🍔 Unhealthy diet
men → 2x
women → 4x
- Anger
- Anxiety
- Depression
- Hostility
- Type A behavior
- POPULATION approach:
- public health approach
- target = population
- Community-wide interventions
- Behavior modification
- Influence the distribution of risk factors in a population
- Modest changes in risk factors lead to substantial reduction in the cumulative population risk of CVD in a community
- Small benefits to each individual
- HIGH RISK approach: clinical management; target = individual
- Identify individuals at high risk
- Implement targeted behavioral or pharmacological interventions
- Achieve the greatest risk reduction in individuals
(i.e. Initiate lipid profile starting at 20 years of age, Repeat lipid profile every 4-6 years)
Disease, Condition, or Risk Factor | Recommendations |
Cerebrovascular Diseases | - Auscultation for carotid bruits. |
- Elicit a history of transient ischemic attack. | |
- Screening for hypertension and smoking. | |
Coronary Artery Diseases | - Strongly recommended screening for hypertension and smoking. |
High Blood Cholesterol Level | - Periodic measurement of total serum cholesterol starting at 20 years of age, repeated every 4-6 years, and in the elderly. |
Hypertension | - Blood pressure should be measured regularly in all adults starting at three years of age and older. |
Peripheral Artery Disease | - Screening for risk factors, especially for smoking. |
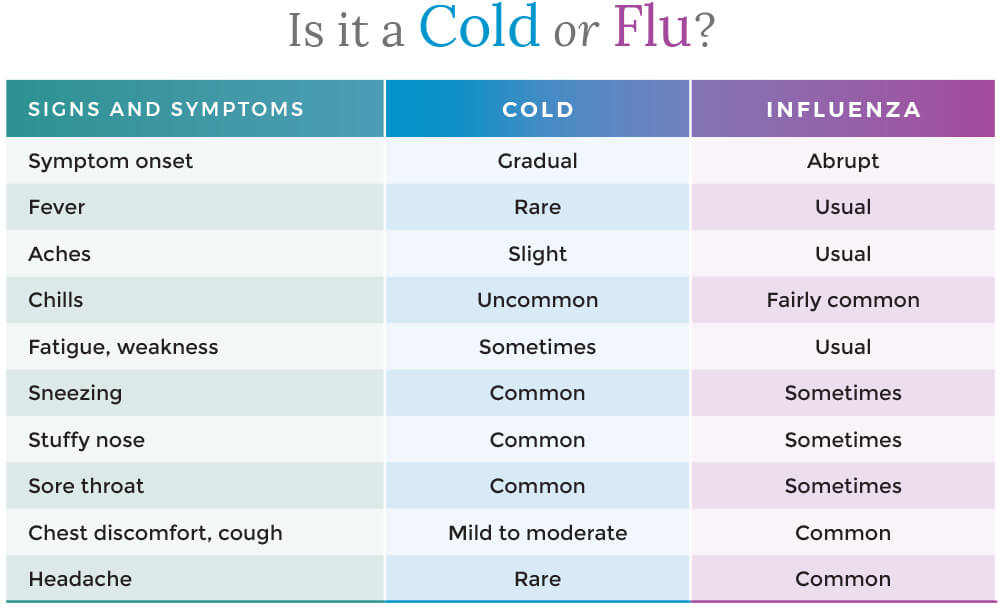
- Influenza viruses are classified into four types: A, B, C, and D.
- Types A and B are responsible for seasonal epidemics of influenza, while type C causes mild respiratory illness and type D primarily affects animals.
⇒ A causes ENDEMIC + PANDEMICS (Ag drift + shift) ⇒ B only ENDEMICS (Ag drift only)

Antigenic DRIFT = point mutation Antigenic SHIFT = segments shared → new formation
- 🫁 Respiratory: croup, bronchiolitis, primary influenza pneumonia – early (12-24 h), severe, hemorrhagic alveolitis with ARDS !
- mild interstitial prominence
- to poorly defined, 1- to 2-cm patchy areas of consolidation
- to extensive airspace disease due to hemorrhagic pulmonary edema
- cavity formation suggests bacterial superinfection with Staphylococcus
- pleural effusion is rare and usually represents bacterial infection
- characteristic appearance of ARDS: multifocal bilateral air-space opacities, in a predominantly perihilar and lower zone distribution = ground-glass opacity
- differential diagnosis includes: infection (common complication of ARDS), cardiogenic pulmonary edema, differentiation can be impossible in some cases
- causes of ARDS include: trauma, septicemia, hypovolemic shock, fat embolism, near-drowning, burns, viral pneumonia (influenza, SARS-CoV2, VZV), pancreatitis, oxygen toxicity, disseminated intravascular coagulopathy
- ARDS mortality is high, around 50%
- many survivors develop chronic lung disease, with damaged lung healing by fibrosis
- 🧠 Neurological: neuritis, 🐻 Guillain-Barre sd, transverse myelitis, encephalitis, cranial nerves palsies
- ❤️ Cardiac: myocarditis, pericarditis
- 💪🏼 Myositis, rhabdomyolysis (> in children, > with type B)

⇒ Influenza-virus pneumonia (primary)


- Infection of respiratory tract
- Sinusitis + Otitis
- Bronchitis
- Pneumonia (S.AUREUS!) / bronchopneumonia
- toxic shock syndrome (TSS) frequently reported during last epidemics due to some modifications of colonization and replication of toxins producers staphylococci induced by A and B viruses
- pregnancy severe evolution, double lethality teratogenic potential
- Exacerbation of underlying chronic diseases - COPD, asthma, cystic fibrosis (=risk groups → vaccination!)
- Influenza A, B viruses/ VZV + salicylates
- Acute encephalopathy + fatty degenerative liver failure
- Affects frequently children as well as other ages
- Other viral / atypical bacterial
- Covid-19
- Common cold
- Respiratory infections with adenoviruses, RSV, enterov, parainfluenza viruses
- Atypical pneumonia (Mycoplasma, chlamydia, legionella)
- Other disease’s onset with respiratory catarrh: measles, varicella
- Systemic infections
- Systemic disease’s onset: leptospirosis, brucella, typhoid fever
- Flu-like infectious diseases: TB, HAV, sepsis
- Influenza can be diagnosed through laboratory tests, including
- rapid antigen tests,
- PCR (viral Ag detection)
- Ø SEROLOGY!
-
viral culture. - Clinical evaluation and epidemiological factors (SEASONAL) are also taken into consideration for diagnosis.
- ✳️ Identification of groups of risk for severe forms, complications
- 🛏️Supportative
- Isolation
- Bed rest
- Diet
- Medication differentiated according to clinical forms – common/complicated/severe
- 💊Antivirals
- Protein
M2inhibitors:Amantadine, Rimantadine⇒ #not anymore! - NA inhibitors: Oseltamivir (Tamiflu), Zanamivir, Peramivir – iv, Favipiravir
- Endonucleases inhibitors: Baloxavir
- FAVIPIRAVIR (Avigan)
- Laninamivir (Inavir)
- Peramivir (Rapiacta, Peramiflu)
- Endonucleases inhibitors: Baloxavir
- severe forms: 🌝steroids


- High-risk groups: Children under 2 years old, adults 65 years and older, pregnant women (up to 2 weeks postpartum), residents of nursing homes and long-term care facilities.
- Medical conditions: Asthma, neurological and neurodevelopmental conditions, chronic obstructive pulmonary disease (COPD) and cystic fibrosis, heart disease (including congenital heart disease, congestive heart failure, and coronary artery disease), blood disorders (such as sickle cell disease), endocrine disorders (such as diabetes), weakened immune system (due to diseases, medications, or HIV/AIDS), kidney disorders, liver disorders, metabolic disorders, extreme obesity (BMI of 40 or more).
Complications of the flu include:
- Pneumonia
- Bronchitis
- Sinus infections
- Ear infections
- Worsening of chronic medical conditions, such as heart disease, asthma, or diabetes
- In rare cases, the flu can lead to respiratory failure, sepsis + multiorgan failre
Basic measures: 📷
ANNUALLY SEASONAL INFLUENZA 💉VACCINATION
→ IM (inactivated) quadrivalent → Intra-nasal (live attenuated) [! in pregnancy]
every person ≥6 month should get vaccination
- Antiphagocytic activity, Internalization, Invasiveness
- M protein
- major GAS virulence determinant
- atypical superantigen
- Adherence factors
- hyaluronic acid capsule also antiphagocytic
- Persistence and invasiveness
- Fibronectin binding protein
- Extracellular products
- Streptolysin O, streptokinase
- Streptococcal pyrogenic exotoxins (erythrogenic toxins SPEs)
- scarlet fever
- 11 serologically distinct superantigens
- low-molecular-weight exoproteins
- T cell activation ~1000x normal immune response leading to inflammatory cytokine release and shock
Clinical presentation:
- 🧣Signs of Infection:
- Clinical exam: Hyperremia + Congestion (+ pus) 📷
- Symptoms + Signs:
- Pharyngitis:
- like viral: dysphagia, odynophagia (sore throat)
- petechia (on pallate) 📷
- Tonsillitis
- 🧫Specific signs of bacterial infection:
- PUS
- HIGH Fever
- ↑LN
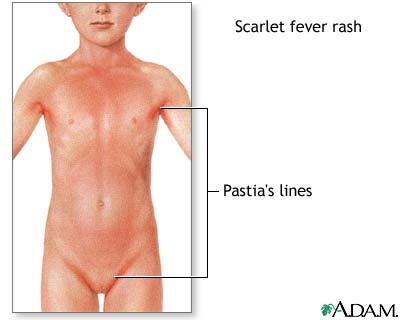
- Exanthem (⇒scarlet fever) aka scalantiform rash 📷
- Ø viral symptoms! (Øcough, Ørhinorrhea, Ø hoarseness)
⇒ Etiology: Strep. pyogenes (aka beta hemolytic GAS)

Acute viral tonsillopharyngitis: children <5 years and young adults Acute GAS tonsillopharyngitis: children aged 5-15 years; rare in children aged < 2years
Centor score
The Centor score is a clinical prediction tool used to estimate the probability of a streptococcal infection in patients with a sore throat.
A score of 0-1 is considered low risk, 2-3 is moderate risk, and 4-5 is high risk.
- The score is calculated based on the presence or absence of four clinical criteria: fever, tonsillar exudates, tender anterior cervical lymphadenopathy, and absence of cough.
- Another criteria used in the score is the patient's age, with younger patients (<15 years old) being assigned a higher point value. This is because streptococcal infections are more common in younger individuals. Specifically, patients under 3 years old are assigned 1 point in the Centor score.
- Each of these criteria is assigned a point value, and the total score is used to estimate the likelihood of a streptococcal infection.
- Local spread
- 2)👂🏼 Otitis media 📷+ Mastoiditis
- 3) 🎛️ Sinusitis 📷
- 4) 💪🏼 Necrotizing fasciitis 📷
- 5) Pneumonia 📷
- Systemic complications
- Pharyngitis signs + non-specific inflammatory
- +- GI signs
- 3) ⛑️ Auto-immune
- Rheumatic fever 📷 (JONES)
- PANDAS: neuropsychiatric disorder

aka “streptococcal bacteremia”
1. TOXIC Shock-signs(i.e. ↓BP+fever) + Exanthem (measle-like) 2. Evolution: - skin desquamation - multi-organ failure ☠️
erythrogenic toxin
(makes you red 👹)
5-15 years (like GAS)
(max 5-9y)
Antitoxic antibodies against pyrogenic exotoxines → lifelong protection (you only get it once in a lifetime)
2-3 days (1-7d)
Starts on 👹 face (SPARES PERIORAL! = Filatov mask)
↓
⇒ spreads rapidly over entire body ⇒ GENERALIZED (measle-like) → TEXTURE: “ 🧽 SANDPAPER” (micropapules) → +- pruritus
↓
3) ⇒ after generalization ⇒ becomes more insense around skin folds: “🍝 PASTIA’S LINES”
↓
4) DESQUAMATION: ❄️ flaking of the face → after 1w: ✋🏼desquamation on hand 📷
→ 🩸hematuria → RF ⇒ 🥐 ↓GFR → 💳 ↑Crea

*patho
Indication for AB Tx? ⇒ high probability strep infection?
- + rapid antigen test
- GAS clinic + Øviral signs
↓
- AB Tx
- <27kg: p.o. - 250mg - 3x/d - 10days
- >27kg: p.o. - 500mg - 3x/d - 10days
- allergy → macrolide
- abscess → incision,drainage + Penicillin + Clinda
- non-compliant →i.m. Benzathine pencillin G single dose
- recurr. → Clindamycin / Amoxi-clav / Cefuroxim
- NEVER Tetracycline + Sulphonamide!!!
#1 ✏️Penicillin V / Amoxi
#2 Amoxi
#3 special situations:

- symptomatic Tx (NSAIDS, paracetamol, local tx)
- Sipping cold or warm beverages
- Gargling with warm salt water

local:
Acute diarrhea = ≥3 watery/loose/decreased consistency stools per day lasting less than 2 weeks
🦠+🧪 EARLY Onset Diarrhea | 🧫 LATE Onset Diarrhea | |
Onset | <6 hours after eating | 1-2 days after eating |
Causes | - 🧪 Toxin-induced food poisoning
- 🦠 Viral | 🍤 Enterobacteriaceae:
Salmonella, E.Coli, Shigella, Yersinia enterocolitica, Campylobacter jejunii,
+ Listeria monocytogenes |
Symptoms | Predominant 🤮 vomiting ⇒ rapid dehydration,
Ø/↓ fever | 💩Diarrhea predominant,
🔥 fever,
abdominal pain,
+- vomiting |
- 🍤 gastric acidity
- ⏩ motility
- 🧫local immunity + flora
flora:

Developed Countries | Developing Countries |
Travelling | Lack of drinking water |
Immunosuppression | Contaminated food |
PPI treatment | Poor hygiene |
Elderly | Overcrowding |
Prolonged antibiotic treatment (C.Diff) | Inefficient education |
Breastfeeding (protective) |
Transmission | 💩👄Fecal-Oral (contaminated water, food, hands, atropods)
↑↑in viral ( aerosol spread) |
Entry site | Oral cavity |
Multiplication | Intestines |
Elimination | Feces, Blood, Oral secretions |
- 🚿 REHYDRATION (oral / iv) → continue breastfeeding
- Ø
Antibiotics⇒ exception: invasive or ↓immunity

- 💉 PREVENTION
- source/risk factor control
- surveillance
- IMMUNIZATION (rota, cholera, measles)
- preformed → 🍢S.Aureus
- formed in intestine → Chlostridium ssp. ⇒ 🤖 Botulinum + 🏍️ Perfringens
🍤 Enterobacteriaceae: G - bacilli ⇒ FACULTATIVE ANAEROBES






- local
- rectal prolapse
- intussusception
- toxic megacolon
- systemic:
- sepsis
- seizures
- glomerulonephritis + reactive arthritis
- HUS



- 🔬microscopy + Gram stain
- 🧫 Culture (stool + blood)
- 🔰 +-serological (elisa, agglutination test) + PCR
- US for DDx (appendicitis)
bipolar staining (safety-pin appearance) 📷
- 🤺 Aminoglycosides,

- 🌷Fluros,
- 🦑 Cephalos 3rd,
- 🧻🥚TMP-SMX





fecal oral (poor sanitation → gets into food)
Tx:
- 🚿 REHYDRATION
- AB (🚴🏼♂️Doxy/🌷Fluro/🦅Macrolide)
- Prevention in endemic areas: Vaccine (Dukoral, shanchol)
Special forms:
C. difficile infection causes toxic megacolon through the action of its toxins, particularly toxins A and B. These toxins cause damage and inflammation to the colon lining, leading to ulcerations and erosions. As the inflammation worsens, it can result in the colon becoming dilated and distended, leading to the development of toxic megacolon. The toxins also impair the function of the smooth muscle of the colon, which can contribute to the development of megacolon. Overall, the exact mechanism by which C. difficile causes toxic megacolon is not fully understood, but it is believed to be related to the toxins' impact on the colon's inflammatory response and smooth muscle function.
- Recurrent = easier but chronic evolution
- ↑ sensitivity tests: GDH (with EIA) or PCR (toxin)
- ↑specifictiy: Toxin (with EIA)
- Toxin detection / determination
- detection → EIA
- determination → PCR
- C.diff detection
- glutamate dehydrogenase = GDH test → EIA
cultureonly in research

#2 ORALLY 👄 ⇒ 🚇 Metronidazol (only in non-severe forms) if FULMINANT: ⇒ 🚌 Vanco oral 👄 PLUS 🚇 Metronidazol I.V. 🌀 if RECURRENT: ⇒ 🔄 switch ABs or ⏰ give Vanco longer (additive rifaximine and fecal transplant can also be considered)
*newer guidelines propose 🦊 Fidoxamicin as #1 Tx
Fidoxamicin:


more details → see infectio
- Food-born botulism (adults → preformed) - Intestinal botulism (mainly infants → “floppy baby” syndrome) - Wound botulism
- appropriate preparation of canned food and fish,
- avoiding honey in infants.







- Classic signs of Hepatitis (Hepatomegaly, jaundice, dark urine, pale stools, bleeding, neuro, etc)
- “Rheuma”-Prodrome:
- PN (polyarteritis nodosa)📷
- GN (membranous + membrano-proliferative)
- Rash (pruritic)
- Arthralgia/Arthritis
- Fever
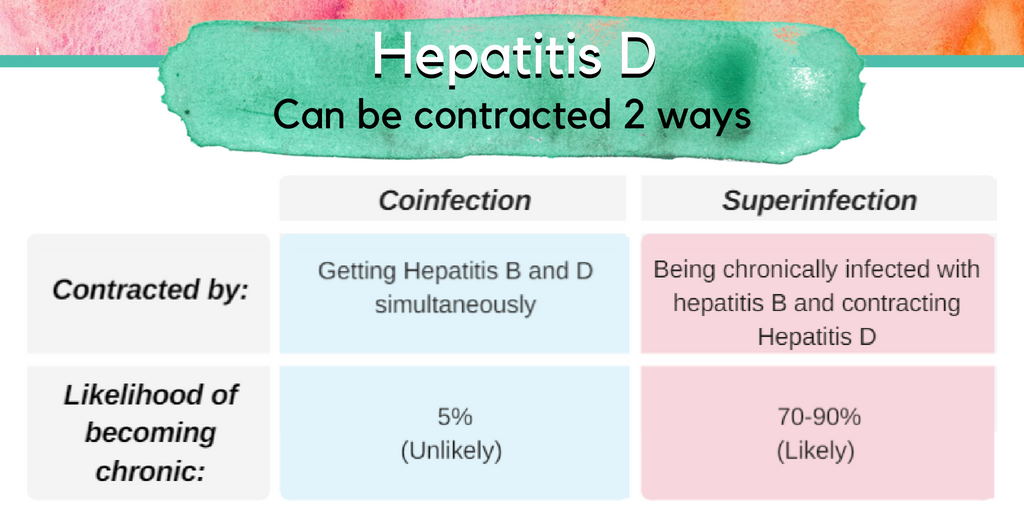
- ⇒ 🦛 HepD (co-infection or superinfection)
- 🕰️ CHRONIC HEPATITIS ⇒ 🦀 HCC
- adults ⇒ rarely (5-10%)
- 🐣 NEWBORNS ⇒ very common! (90-95%)
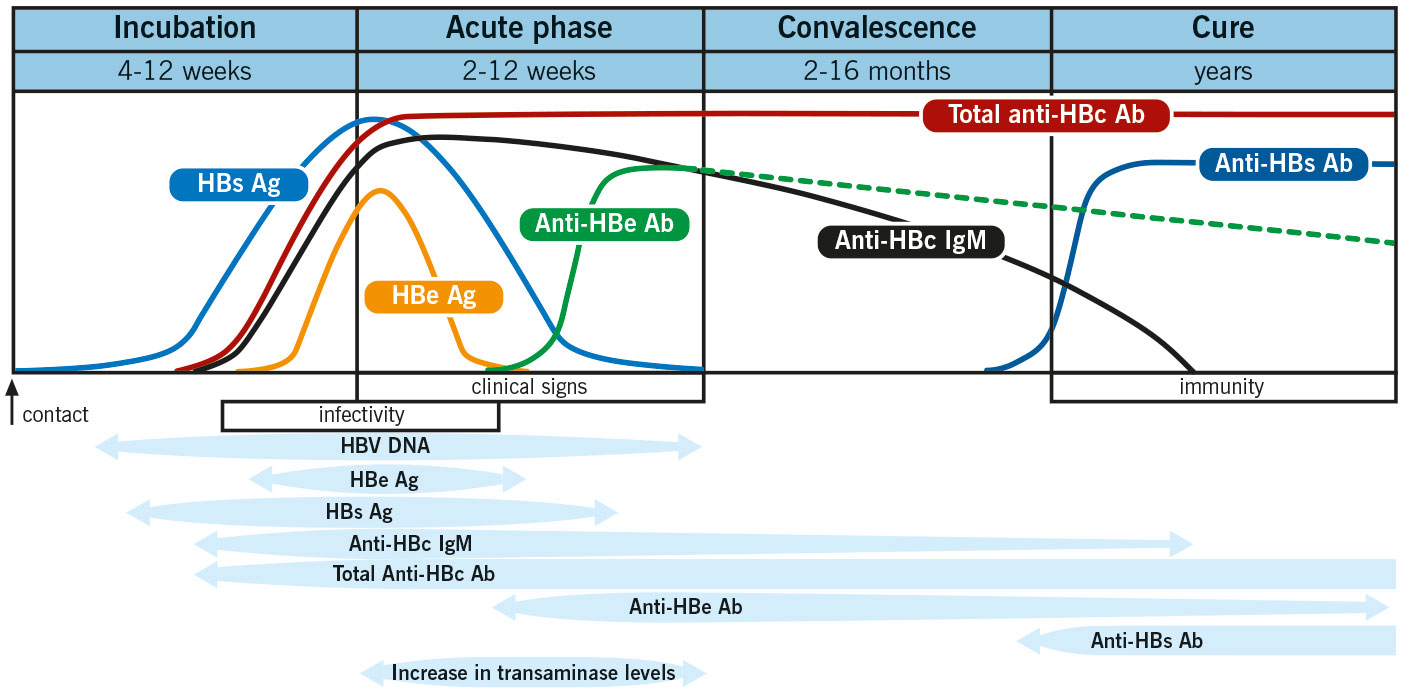
- The onset of acute hepatitis B is typically insidious.
- Clinical manifestations of acute infection vary depending on age.
- Jaundice is less common in children under 5 years old (less than 10%) and more common in older children and adults (30%-50%).
- Most cases of acute hepatitis B (approximately 70%) are either subclinical or anicteric.
- Severe fulminant forms of acute hepatitis B occur in a small percentage of cases (0.1-0.5%).
- The majority of adults with acute hepatitis B (90-95%) experience complete recovery, characterized by clearance of hepatitis B surface antigen (HBsAg) and production of anti-HBs, indicating future immunity against the infection.
- Screening for acute infection:
- If positive: detemine transmissibility
- Acute vs. chronic (persistence)
HBsAg + anti-HBc IgM
HbeAg + HBV DNA
anti-Hbc IgM vs IgG

THERAPEUTIC ALTERNATIVES:



die Ente spielt Klavir (Entecavir) und das Lamm telefoniert(2x = bi) mit Hudini (Lamivudin + Telbivudin)

- Interferons
- Bulevirtide
- Lonafarnib
On the 🧑🏼🌾 Loner-farm (Lonafarnib) lives only the 🐂 bull D in wires that are tight (Bulevirtide) . (Bull is lonely = HepD needs another virus (HepB)

- 🙅🏼 Mainly ASYMPTOMATIC
- or 🍑 CLASSIC LIVER SIGNS
complications:
- 🕰️ CHRONIC (65-70%)⇒ cirrhosis + HCC
- ❄️ Cryoglobulinemia




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}