




Pulmonology
- high BP
- recent surgery
- cataract glaucoma
- epilepsy
- acute respir. infection
- general pulmonary diseases
- cardiac diseases (acute or chronic)
- recent use of bronchodilators
RV + TLC
dilator → salbutamol
constrictor → methacholine/histamine
max amount of that can be expeled after max. inhalation
VC = TV+ERV+IRV
TV (tidal volume) 0,5 - 0,8 l = 15%VC 0 B • inspiratory reserve volume 1,5 - 21 = 60%VC expiratory reserve volume 1,2- 1,5l = 25%VC

FVC = amount of air that can be forcibly exhaled from your lungs after taking the deepest breath possible, as measured by spirometry.
FEV1 = The volume of air that can be forced out in one second after taking a deep breath, an important measure of pulmonary function
⇒ FVC + FEV1 represent big airways
FEF25-75% = Volume exhaled between 25% from FVC until eliminating 75%
FEF 50% = Volumen exhaled at 50% from FVC
⇒ FEF25-75 + FEF50 represnet small airways
Tiffneau = FEV1/FVC
min. 6sec
- COPD
- Asthma
- Cancer
- Check FEV1 first! → most important value: FEV1 + TIffneau decr → obstruction;
- in obstructive syd. small airways obstructed first (FEF50+ FEF25-75)
→ FEV1 for severity
Parameters | Normal Values | Light | Moderate | Accentuated | Severe |
FVC | >80% | 80-60% | 60-40% | 40-30% | <30% |
FEV1 | >80% | 80-60% | 60-40% | 40-30% | <30% |
TI | >70% | 70-60% | 60-40% | 40-30% | <30% |
FEF50% | >80% | 80-60% | 60-40% | 40-30% | <30% |
- pulmonary fibrosis
- pneumoconiosis
- others.
(mixed syndr) → check TLC to classify as restrictive pattern (TLC low) → Pletismography
→ note Tiffneau can be normal in restrictive pattern
Parameter | Normal values | Light alteration | Moderate alteration | Accentuated alteration | Severe alteration |
TLC
FEV1
FVC
FEF50
PEF | >80% | 80-60% | 60-40% | 40-30% | <30% |
FEV1/FVC | >70% | 70-60% | 60-40% | 40-30% | <30% |
RV | <125% | 125-145% | 145-175% | 175-200% | >200% |
hyperinflation → COPD (irrev.) or Asthma (rev.)
→ restrictive syndrome
or patient doesnt perform test correctly
- dg of asthma (DD vs. COPD)
- sprimetry showed: obstruction in small airways (FEF50 dec.) + obstructuctive ventilatory dysfunction (FEV+TI decr.) + hyperinflation (RV inc)
FEV1 incr >12% + FEF >25%
FEV1 incr. with 200ml
Bronchodilator Test | Positive | Negative |
Reversible Obstruction | Irreversible Obstruction | |
Asthma Crisis | COPD | |
Criteria | FEV1>12%, FEF 50%>25%, FEV1 increases with 200 ml | FEV1<12%, FEF50%<25% |
when spirometry is normal but pat. expirience dry cough at specific situations (work)
- bronchial hyperreactivity → only present at work space
- (nonspecific) asthma
→ confirms etiology/connection to occupation
nonspecific (methacholine) + specific (suspected agent at work)
- FEV1 < 60%
- pregnancy
- rib fracture
- recent surgery
- infection
- severe cardiac diseases
- glaucoma
FEV decr > 20%

🏮 Bronchiectasis
- due to alteration muscular + elastic componnent of the bronchial wall (mainly due to infammation) → fibrosis of the parenchyma
→ irreversible dilatiotion >2mm of medium sized bronchi
Cycles of bronchial inflammation 📷 → mucous plugging → BRONCHIECTASIS (= abnormal + permanent dilation of bronchi). For Bronchiectasis to happen, it requires the combination of: Local infection or inflammation PLUS inadequate secretion clearance or airway obstruction or impaired defenses of host
→. 📷
- chronic infection
- enzyme activation
- inflammation
- broncho-pulmonary infections
- bronchial obstructions
- congenital anatomical defects
- states of Immunodeficiency → agammaglobulinemia
- Hereditary defects

→ all basically predispose to inflammation / infection
- infiltration of inflammatory cells
- fibro-cartilaginous tissue destruction
- systemic neovascularisation→ hemoptysis
- metaplasia→ mucocilliary dysfunction
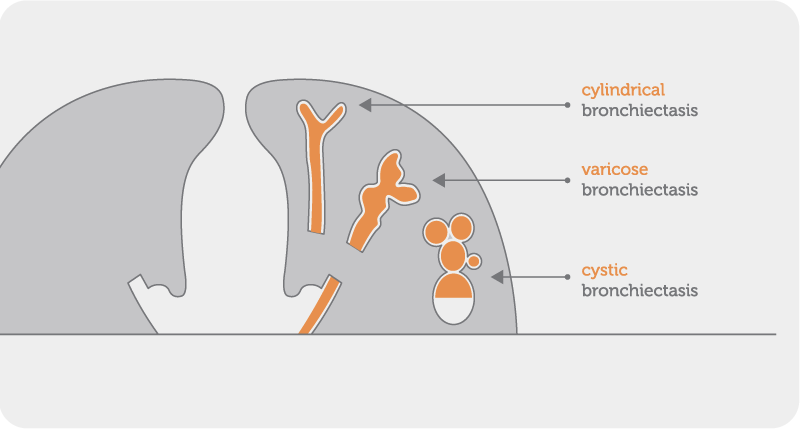
- cylindrical or tubular→most common → uniformily dilation+end appruptly
- varicoid→ resemble varicose veins
- saccular (cystic) → dilation increases towards lung periphery → terminal portion = 🎈-like
- localized
- generalized
- respiratory signs + symptoms regarding etiology
- Dyspnea
- Cyanosis
- right heart failure
- rales
- Cough
- purulent sputum
- minimal/no sputum (dry, blank sputum) → TBC
- periods of stability + periods of superinfection
- Hemopytsis
- Hippocratism (nail clubbing)

signs of infection
- severe alteration of general condition
- weight loss
- lack of appetite
- fever
- increased sputum with significant lung burden
- respiratory degradation
Findings: (?)
- bronchial dilatations→ morphology analysis 📷 (cylindrical vs cystic (aka saccular) vs varicose)
- exact location→ diffuse vs localized
- thicker bronchial wall
- signet ring sign 📷 → increased bronchial diameter of affected bronchus in comparison to adjacent bronchi
- absence of bronchial calibre decrease
- mucous plugs
F
- bacteriological examination → S.pneumona, H-influenza, S.aurus, pseudomonas
- Mycological examinations→ Aspergillus?
- Acid-Fast examination→ TB?

- Point of bleeding
- Quantity of secretion
- Identify tumors, foreign bodies, stenosis etc
- Biological samples (bronchial aspirate)
Highlights an obstructive ventilatory dysfunction

hypercapnia
- sweat test→ CF
- Protein immunoelectrophoresis
- Seric immune deficiencies→ systemic
- obstrutive
- Intrabronchial foreign bodies
- malignancy
- infections
- active TB
- pulmonary mycoses
- Lung abscess
difuse form → multiple complations
- infections
- Superinfection repeatetly
- pneumonia, abscess
- hemoptysis
- bronchial hyperresponseiveness
- Respiratory insuff
- Cor pulmonale + pulmonary hypertension
- emphysema + pneumothorax
- secondary amyloidosis
How do you treat each?
- lifestyle (stop smoking)
- track and treat ENT/ dental infectious foci
- vaccinations→ Influenza, Pneumococcus, Pertussis, Haemophylus influenzae and MEasles
- physiotherapy
- postural drainage
- breathing techniques
- autogenic drainage
- mucolytics
- saline nebulazation
- bronchodilators (prior to nebulization)
⇒ 20-30min 2x day
- AB in superinfection
- clinical picture or antibodies suggestive
- purulent sputum alone is Ø a indication!

- Resection (in refectory cases)
- Also when in lower lobes (eg. TB)
- Arterial embolization may be used in massive Hemoptysis
- Even lung transplant in severe cases
🍏 Lung abscess
inflammatory circumscribed focus (nidus) which evolves towards necrosis and excavation→ bronchorrhea
- primary→ pneumonia, bronchoaspiration, PE
- secondary→ bronchial obstruction
- Aspiration of oropharyngeal content→ states of unconciousness, deglutition disorders, Obstruction, Ileus, Vomiting, ENT/Dental Interventions
- Hematogenous dissemination
- Pre-existing lung diseases→ischemia,necrosis
- Immune deficiencies
- Infected thorax wounds
- #1 by direct inhalation - bronchial
- check for obstruction!
- parenchymal
- hematological dissemination (vasculary)
- point of entry→ ENT/ Dental/ CUtaneous
- non-specific: fever, asthenia, weight loss
- cough
- purulent
- fecal-smelling (anerobe)
topographic stability of auscultatory signs during daily auscultation
- Building-Up phase/ Closed fester→ Pneumonia signs
- Vomica phase→ exhibition of purulent, fetide and abundant sputum, fever decreases
- Open fester phase→ alteration of general condition between periods of fever and abundant sputum with no fever/small amounts of sputum
Findings?:
- Cultures
- Sputum examination→ collect before starting AB Tx ‼️
- Biohumoral→ Leukocystosis, Procalcitonin, Glycemia
⇒ 📷
- hydroaeric levels.
- soft wall
- irregularity in hydroaeric levels in various examinations
- drainage bronchus (more visible on CT)
⇒ 📷
in any lung or pleural abscess→ to identify bronchopulmonary tumor
- excavations of existing:
- no history of aspiration
- no fever and sputum
- no answer to ABs
- CXR
- cavity progresses towards center→ necrosis
- irregular walls
- Cytologic examination of sputum
- Fibrobronchoscopy + biopsy→ if non-conclusive→ Thoracotomy
- infectious:
- Sputum (aspergillus +)
- CT or xray ⇒ 📷
- meniscal (”c-shaped) picture
- pre-exisiting cavities
⇒ 📷
→occupational exposure
upper lobes
caverna. 📷
microscopy + culture (BK+)
pre-existing cavities
→ evacuated hydatid cyst, emphysema air pockets
→ no inflammation signs around
→ suspect in animal breeders (aka farmer fut)
→ ANTIBODIES IN SERUM
- gas bubble (stomach) + fluid levels
- double heart border
endoscopy or barium swallow
- asphyxating of vomica
- systemic spread
- septicemia→ brain, renal abscesses, DIC
- local spread
- contralateral pneumonia
- Hemoptysis
- Pleural empyema
- becomes chronic
- Bronchiectasis
- Infection Tx→ rapid, early, long-term
- Areal/ Causative treatment
after acute phase is over
- chronic lung abscess, non-responging to AB Tx>3 months
- irreversible obstruction
- abscess >6cm
- Hemoptysis
- Empyema
- bronchiectassis
- retractile plachypleuritis → restrictive resp. failure
🪱 Hydatid cyst
Echinococcus granulosus
⇒ 📷
rupture or fissure of the hydatic cyst → anaphylaxis
asymptomatic for along period→ random discovery on CXR
- persistent dry cough
- hemoptysis
- thorax pain
hematopoietic expectoration, Urticaria up to anaphylaxis
hydatid vomica
- dullness, decreased breath sounds
- pleural effusion
- manifestations of other locations (hepatosplenomegaly, abdominal mass)
- CERTAINTY Dx: parasitological examination (scolex,hooks?) of puncture
- cystic formation with latent growth
- persons from edemic area with contact to dogs/sheep 🐕 🐑
- suggestive clinical signs
- suggestive paraclinical examinations → AB + eosinophilia
puncture:

- eosinophilia
- non-specific inflammatory syndrome
- detection of serologic ABs
- Common Hydatid cyst. 📷
- liquid-like opacity, homogenous, well limited, with soft walls, surrounded by viable lung parenchyma, round « cannon ball » shaped, singular
- Fissured Hydatid cyst 📷
- pneumocystic image, meniscus sign (like aspergillus abcess)
- Ruptured hydatid cyst into the bronchi. 📷
- horizontal hydroaeric level, undulated, « floating membrana » aspect, pathognomonic, double contour sign. If the cyst was evacuated – image of an aeric cavity, with thin walls, segmental or lobar collapse
- Ruptured cyst into the pleura - hydropneumothorax. 📷
- aspect of floating membrane and vesicle
if neoplasm suspect → DDx
- if round → abscess, TBC, tumur
- meniscal → aspergillioma (,hematoma)
- if fluid-air level → abcess
- multiple → metastasis
- juxta-mediastinal → Aortic aneurysm + mediastinal mass
- juxta-periatel → abscess, hematoma, tumor
- cavity like → bubble, pneumatocele
T
- fissure + rupture (in bronchi or pleura=
- compression → ventilatory disorders
- Superinfection
- Rib erosion
- Surgery
- removal of cyst in 1 block (+residual cavity) → avoid rupture
- “PAIR”
- ALBENDAZOLE

- pleural + diaphragm
- hepatic + splenic
- mediastinal + cardiac + pericardial
⚰️ Sarcoidosis
systemic inflammatory disease with unkown cause characterized by organ infiltration with epitheloid granulomas and immune giant cells (tuberculoid granulama) without caseous necrosis

T 😵💫🚬
- exposure to one or more antigens (i.e. mKatG protein from TBC)
- preparation and presentation by APC
- Lymphocyte transformation into Treg and Th1 (CD4 T-Lympho)
Th1

- cell recruitment
- granuloma formation
pulmonary fibrosaaaa
- asymptomatic (60%) → often incidentally discovered on xray
- cardiac syncope (direct infiltration→ restrictive; or cor pulmonale)
- respiratory + see later
- low grade fever
- neuropathy
- dry syndrome
interstitial syndrome:
- persistent dry cough→ main respiratory sign!
- exertional dyspnea

- chest pain
- hemoptysis (search for aspergillosis)
auscultation → normal or crackles

25% of patients with Sarcoidosis exhibit skin findings
- mild fever
- erythema nodosum
- lymphadenopathy - stage 1
- arthralgia
- tuberculin allergy
(MNEMONIC: MELAT)
→ classic case of sarcoidosis
- prompt Sarcoidosis Dx→ no need for histological Dx of Sarcoidosis
- excellent prognosis 👍
- infiltrative cardiomyopathy (restrictive)
- Myocarditis
- Pericarditis
- Conduction disorders
EKG
Echo
Cardiac MRI
50%
→ 📷
- Uveitis
- Dry syndrome (lacrimal gland affected)
- Retinitis
- Conjunctival nodules
- meningitis
- polyneuritis (i.e. facial nerve → facial paralysis 📷)
- psychiatric disorders
- dementia
- seizures
Granulomatous hepatitis
→ ↑transaminase + evtl ↑cholestase
• Hypothalamo-epiphyseal • Parotid glands • Lacrimal glands • salivary glands
- neprhocalcinosis
- Urolithiasis
→ due to increased active Vitamin D

- specific granulomatous interstitial disease (renal infiltration)
Arthralgias→ knee and ankles
infiltration
- myositis
- chronic atrophic myosystis
- diagnosis
- prognosis
- follow-up
upper + posterior (stage 2 is middle + upper)
- retraction → hilum + bronchovascular distortion → honeycomb
- diaphragmatic traction
- emphysema (scar)
aspergillus
T
→ 📷
- diffuse subpleural nodule distribution
- along bronchial-vascular axis→ predominate in upper parts
- peribronchovascular thickening
Prognosis
- restrictive/ mixed syndrome
- early decrease in DLCO
- bronchial hypersensitivity→may be present
- ABG→ hypoxemia in exercise
- 6-minute walking test

- normal or with fungus
- whitish granules→ suggestive of tracheal and proximal bronchial mucosa

- tissue sampling (biopsy)→ of granulomas in parenchyma
- Bronchioalveolar lavage (BAL)
CD4/CD8 >3,5
Mediastinoscopy
= 100% dg
- ACE↑ → good for monitoring (correlates with disease activity)
- Vit D → ↑Ca, hypercalciuria, phosphatemia
- CBC → lymphopenia (bone marrow invasion)
- CRP
- electrophoresis (proteins, gammaglobulins)
in granuloma = malfunctional lymphocytes → leads to allergy to tuberculin
- Ophtha
- ECG + echo
- liver function test
- renal function test
- HIV
- biopsy of skin lesions, periph. lymphnodes, salivary glands + liver
scinti
- history
- granulamos + histo evidence
- rule out other
- ≥2 organs involved
(Lofgren syndrome)

- Mediastinal Lymphadenopathy (DD with stage 1)
- Lung parenchyma diseases (DD with stage 3)
- pulmonary fibrosis
- other granulomatous diseases (Infections, Pneumoconiosis, Immunodeficiency)
- Pulmonary hypertension
- Cor Pulmonale
- Risk of pyogenic superinfection
- Risk of Colonisation of aspergillosis
- Hemoptysis
- Pneumothorax
- Blindness
- pericardial/neurological affection→ life threatening
- Liver damage+ Facial skin lesions→ significant sources of morbidity
Glucocorticoids
- Immunosuppression→ Methotrexate, Aza, Anti-TNF-alpha
- Anti-malarial Tx (Hydroxychloroquine)
→ every 3-6month
- classic clinical exam
- CXR, CT
- ECG
- Specific enzymes (ACE)

🪘 Tuberculosis
- m. tuberculosis
- m.bovis
- m.africanum
- NMT (non mycobacterium tuberculosis)
Mps phagocytose Bacteria → TB-bacteria inhibit protome maturation + fusion with lysosome → intracellular SLOW multiplication of bacteria (intercellular) → Granuloma formation around macrophage → lung collapse+dissemination or healing: calcification + firbosis → re-activation: pumonary dissemination → caverns with ↑immune response → dissemination = milliary tuberculosis (hematogenous spread)
PRIMARY TB | primary infection |
Latent | Øsigns of active TB; state of constant immune response stimulation via TBC antigens |
Active | Signs of active TB after first-time exposure |
REACTIVATION TB | secondary infection |
Signs of active TB after reactivation or reinfection |
- Healthcare workers
- Traveling to TB endemic areas
- Others • Migration from countries with high TB incidence • Close contact of patient with active TB infection / Crowded living conditions • Homeless
Immunosuppressied people (HIV, DM, chronic disease, transplant, immunsuppresiva, old)
Lifestyle (smoking, alcohol, iv drug, malnutrition)
Prexisting lung disease (COPD, silicosis)
Øresponse to AB
HIV+
- peritoneal
- larynx
- hepatosplenic
Typically asymptomatic !!!
But can have:
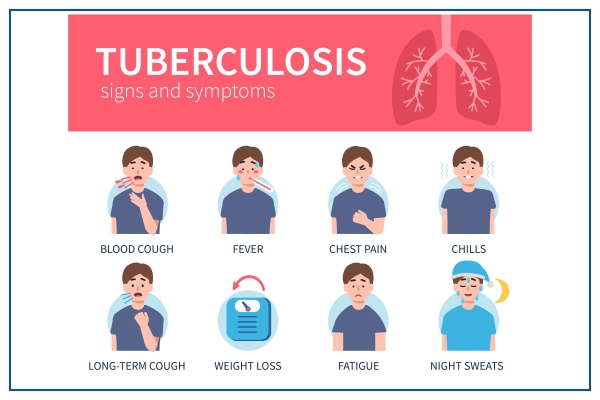
- Systemic
- Low-grade fever with night sweats
- Weight loss (often severe)****
- Decreased appetite
- Malaise
- Pulmonary
- Persistent Cough with purulent sputum that is occasionally blood-streaked (hemoptysis)
- dyspnea
- Pleuritic chest pain
- Percussion
- Dullness over areas of consolidation
- Hyperresonance over areas of cavitation
- Auscultation
- Amphoric breath sounds over areas of cavitation
- Rhonchi aka wheezing
- Crackles
- Diminished breath sounds over areas of consolidation (or pleural effusion)

- Lymphadenopathy (i.e. axillary LN)
- Hepatosplenomegaly
- On Xray → i.e. lungs: multiple small nodules
PDD → Mycobacterium TB antigens

- induration (hardening) at the injected place
- ≥10mm skin erythema
- HIV+ → ≥5mm

Tuberculinic conversion
TST conversion refers to the situation where an individual's TST result changes from “negative” (typically 0-4mm diameter induration) to “positive” (typically equal to or >10mm diameter induration) within a 24 month period.
BCG vaccination
sarcoidosis
immuno (HIV, malnutrition, Hodgkin)
infectious Mononucleosis
- interferon gamma release assay (IGRA) → also differentiate betw. BCG vaccination and true exposure to m.tuberculosis (skin test doesn't)
Gold standard diagnostic test
Used for drug susceptibility testing
Highest sensitivity
But takes long (10-14d) → liquid medium can be used for faster results but more expensive + generally not used
Löwenstein-Jensen
Used as an adjunct along with acid-fast staining and culture
High sensitivity
But expensive
bronchial endoscopy
→ can also obtain samples for ziel neelsen stain
- smear positive culture
- good clinical + radiologic evolution after treatment
≥2 positive smear sputum
≥1positive smear sputum + radiology suggestive
negative culture but radiology suggestive
INITAL PHASE:
R + I → 6month
P →2-month
Rifampin & Isoniazide (alone or in combination
- in the morning 1x/day
- intermittent (2-3 or weekly)
steroids → meningitis + pericarditis
surgery → TB complications + drug refractory
BCG vaccination
- hemoptysis
- pneumothorax
T
breaking of subpleural nodula into pleura
- xray → liquid
- Pleural liquid examination → Exsudate, culture, ADA, ↑Lymphos, stain
- pleural biopsy

- bacteriological monitoring
- liver markers: R + I + P = hepatotox
- hemoptysis
- Aspergilloma (residual cavitiy → hemoptysis)
- chronic respiratory failure
- extensive destruction of lung parenchyma
- fibrosis (of lung)
- bronchiectasis
benign
- athelectasis
- cavities
- fistula
- bronchiectasis
- atelectasis
- hemoptysis
- milliary TB
- TB menigitis
same as adults
rigidity of feet + hands
- Apathy
- Conjunctival blisters
- epidemological context
- exclusion of other etiologies
⇒ even if skin test negative → start treatment directly (DOTS) + dont wait for culture!
DOTS:

- high fever
- GI (vomiting, diarrhea)
- dypnea, cyanosis, respiratory dysfunction
→ occur in first weeks after primary infection
classic
- Xray → miliary aspect +- lymphadenopathy
- TST → can pe positive (rarely)
- history (epidemiological context)
- exclusion of other causes
T
- LN
- Pleueresia, peritonitis, pericatitis
- menigitis
rifampicin→ if protease inhibitor is used in HIV Tx
😴 Sleep Apnea
stop of airflow for <10 sec
reduction of flow <50%
number of apnea + hypopnea per hour
Criteria A, B or C
- A) excessive daytime sleepiness
- B) two criteria not explained by other factors
- daily snoring
- non-restorative sleep
- sensation of chocking during sleep
- difficulty concentrating
- daytime fatigue
- Nycturia→ >1/night
- C) AHI≥5
SSCCFN
pharynx→ anatomically "soft" structure→ collapses during night
false
- Obstructive → with persistent respiratory movements

- Central→ lack of central control (no persistent respiratory movement)
- excessive daytime sleepiness
- asthenia + morning headache
asthenia:

- cognitive impairment
- severe hypertension

Epworth Sleepiness Scale (ESS)
- frequent snoring
- noisy breathing breaks
- restless sleep
- Obesity?!
- Cervical and abdominal parameters
- BP measurement in both arms
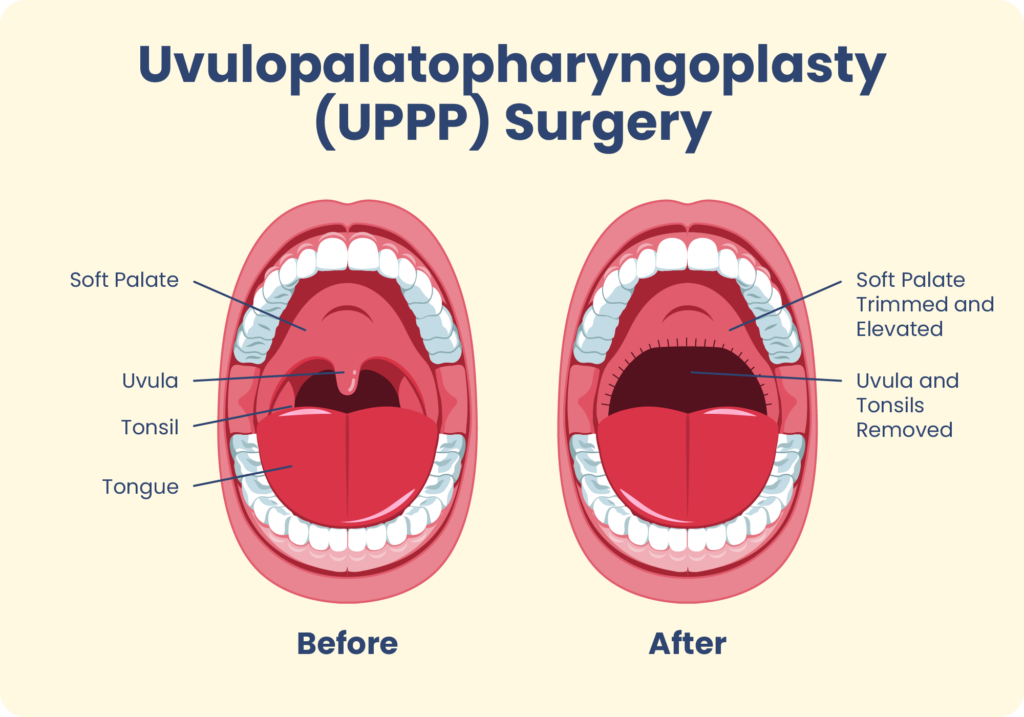
- ENT examination:
- retrognathia
- macroglossia
- hypertrophy soft pallate
- enlarged tonsills

- smoker/ ex-smoker
- Obesity
- respiratory symptoms
- COPD overlap
- SpO² <94%
- restrictive ventilatory effect
- Noctural oxymetry
- O2 saturation
- airflow (nasal canula)
- breathing effort (abdominal + thoracic sensor)
- HR (EKG)
- body position (sternal sensor)
- snorring (sound sensor)
polysomnography
F- out + inpatinets
TTTTTTT 👍🏻
- EEG,
- can analyse stages of sleep → hypnogram
- Electrical oculogram,
- EMG
- Leg movement (tibialis anterior)
F - only inpatients
- OSAS + associated non-respiratory sleep diorder
- unclear polygraphy + symptoms
- Chest X-Ray
- CV exam→ECG, Echo, Holter Ecg
- ENT examination
- Obesity assessment (check diabetes, lipid profile)
- depression
- sedative treatment
- poor sleep hygiene
- neurological condition (narcolepsy)
- Obesity hypoventilation syndrome
T
T
- sinus bradycardia
- sinus pauses <2 seconds
- tachycardic arrhythmias→ rare
DM2, metabolic synd, obesity
- pulmonary hypertension
- night hypoxemia
- alveolar hypoventilation
- depressive syndrome
- chronic fatigue (accidents due to decreased alertness)
- Ischemic Cardiopathy
- Cerebrovascular Complications
- classic shit→ less alcohol, dieting (surgery)
- watch out for hypnotic therapy
- counseling
positive airway pressure
continuous positive airway pressure→ steady pressure rate for both inhalation and exhalation
(no changes in pressure)

auto-adjustable airway pressure→ different pressure rates throughout the sleep
bi-level positive→ if CPAP doens't work
- severe SAHOS + high AHI
- severe SAHOS+ slight-moderate sleepiness
- SAHOS + CV-Riskfactors
- skin irritation - due to mask
- Rhinitis
- Eye irritation
- nasal + pharxy → dry mucosa
- mild OSA + obstructive anatomy
- if CPAP not tolerated
- patient doesnt want (little bitch)
- or not very good improvement
→ esp in mild OSA + normal-mild obese



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}