





Cardiovascular System
Cardiology




Solution: pain on effort/stress? → stable;
Extra Information / Pictures:
Solution: left shoulder, arms, abdomen, neck
Extra Information / Pictures:
Solution: 1. Pericardial pathology 2. Aorta dissection 3. Pulmonary embolism 4. pneumonia, pleuritis 5. MI 6. Gastric, pancreatic, cholecystic, esophageal origin 7. Rheumatic pain (elderly)
Extra Information / Pictures:
⇒ PATHOLOGIES OF FOLLOWING ORIGIN:
cardiac, pulmo + upper gastro
Solution: sharp pain, superficial, ↑with motion/breathing, friction rub
Solution: uninfluenced by position, breathing, medication
Solution: usually ↓ pain more dominated by dyspnea + hypotension
Solution: - Lab - EKG rest - Stress EKG - Holter EKG - in really unsure cases: angiography or angioCT - Echography
DDx ⇒ Pericarditis, pulmonary embolism, aorta dissection
Solution: 1. Heart failure 2. Respiratory origin 3. Effort dyspnea (anemia/fat)
Solution: edema + hypotension
Solution: 1. Echo → systolic + diastolic performance & structural disorders(valve, pericardial, congential, dilation, dyskinesia) 2. EKG 3. Chest Xray → cardiomegaly 4. Stress testing → NYHA classification for effort dyspnea 5. Lab → BNP
Solution: false, there are a lot of other reasons
Extra Information / Pictures:
“Palpitations are differently perceived by patients, they being able to describe rapid heartbeats or heart rhythm irregularities. Irregularities are perceived like sudden pauses in cardiac activity, eventually followed by a strong precordial beat or at the level of throat vessels, usually due to increased preload and contractility following atrial or ventricular extrasystole with increased systolic output. Palpitations may appear without rhythm disorders, within the above mentioned hyperkinetic syndromes but also in case of precordial muscular fasciculation that may result in palpitations (especially in patients with necrosis or hypocalcemia) so suggestive for rhythm disorders. Of course, pulse palpation or auscultation quickly make diagnosis.”
Solution: 1. Lab 2. EKG (rest) + Holter EKG 3. Echo → Underlying cardiac disease for arrhythmias
Extra Information / Pictures:
Certain circumstances → endocavity electromstimulation may trigger arrhythmias
- Edema
- Skin color (cyanosis?)
- Veins (jugular, collaterals, varicosis)
- Pulse palpation (heart rhythm, irregular/high/low...)
check cardiac impuse → in hemodynamic overload + HF it is displaced
- Physiologic → P2 after A2 during INSPIRATION
- Wide → P2 even later than A2 in physiologic split on INSPIRATION → in RBBB, Pulmonary stenosis
- Fixed → P2 after A2 INSPRIATION INDEPENDENT → in ASD
- Paradoxial → A2 after P2 → On INSPRIATION P2 gets delayed and moves closer to A2 → "paradoxical" elimination of the split → LBBB
⇒ 📷
early diastole (after S2)
→ ↑ filling pressure
in Mitral+Triskuspid regurgitation
in HF
in VSD (l-r-shunt)
(esp in dilated ventricles)
late diastole (before S1)
↑ Atrial pressure
Left atrium must push against stiff LV wall (i.e. LV hypertrophy)
Aortic → Aortic stenosis → systolic
Pulmonic → Pulmonic stenosis + Atrial septal defect → systolic
Erb point → Pulmoniary + Aortic regurgitation → diastolic
Tricuspid → systolic: tricuspid regurg. + ventricular septal defect // diastolic: triscuspid stenosis
Mitral → systolic: mitral regurgitation/proloapse // diastolic: mitral stenosis
SAD → syncope, angina, dyspnea
holosystolic high-pitched blowing 📷
- post-MI
- LV dilaion
RV dilation
holosystolic harsh at tricuspid 📷
BEAR
Bicuspid aortic valve
Endocarditis
Aortic root dilation
Rheumatic fever
opening snap (OS) → rumbling mid-late diastolic murmur 📷
MR, TR, AR, MS (late sequella)
(double murmurs are mainly due to rhematic fever)
patent ductus arteriosus
(Note: Double murmurs are seperated from each another by a clear sound; continous are not seperated)
T
(even more: almost all patient with MI present with EKG abnormalities)
- Contractibility of ventricles
- EF
- diastolic function
- Valves
- Doppler → siginifance of the lesions (valves)
- Doppler shunts
- aneurysm
- pericarditis
- ........
- Also check for PAD (Aorta, carotids, renal a., etc.)
transesophageal or intravascular (during angio)
cardiomegaly
lung abnormalities secondary to HF (congestion, hypertension, pleural effusion)
- detection of angina (unstable)
- exercise capacity in dg. of HF → NYHA class 📷
detection of arrhythmia
→ if Holter doesnt detect → endocavitary electrophysiology or electrostimulation or loop recorder
detection of:
AV conduction abnormalities + sinus node diseases
- Diagnosis of ischemic cardiopathy + PAD → shows stenosis, occlusion, collaterals
- Mandatory prior interventional or surgical revascularization
- PTCA + stent
(percutaneous transluminal coronary angioplasty)
scintigraphy, MRI, PET
nope, not for heart
but for PA stenosis, aneurysm, dissection
- Echo
- Angio
- MRI
(Note: Echo is better for function of left ventricle but not for RV-functin; Angio + MRI also for RV)
detection of unstable artherosclerotic plaque
(+ viable myocardium)
- CV RF
- Lipids
- Gluc (fasting)
- Cardiac markers
- Trop + CK-MB
- BNP (in ac+chronic HF)
- Liver + Renal markers + Electrolytes
- INR + D-Dimer (=coagulation + fibrinolysis)
- Crea + Urine exam
- Na + K
- CRP (endocarditis)
- chronic wall stress → endothelial dysfunction
- invasion of inflammatory cells
- Adhesion of platelets → release cytokines + PDGF
- PDGF → migration+prolif of SMC & differentiation of fibroblasts→myofibroblast
- Inflammation of vessel wall
- Macrophages + SMC
- Calcification of the intimima
- Plaque rupture → exposure of collagen → thrombus formation → occlusion or thrombus migration
→ ingestion cholesterol (from oxidized LDL) ⇒ FOAM CELLS ⇒ FATTY STREAKS
→ production of ECM(collagen) → fibrous plaque (atheroma)
→ Mp also produce proteinases for breakdown of ECM→ minor stress = rupture of fibrous cap
20%
<40
Tg
normal <150
very high > 1000
- lipid transport facilitation
- activation LCAT, LPL + hepatic Tg lipase (HTGL)
- binding to surface receptors
LDL levels
- Smoking
- Dyslipidemia (↑LDL+Tg; ↓HDL)
- ↑BP
- DM
- Obesity
- Diet
- ↓Exercise
- ↑alcohol consumption
- CHD → PH or FM
- Age
- Gender (↑male)
- asymptomatic + >40y
- Ø FOR PATIENTS WITH:
- DM
- Familiar Hypercholesterolemia
- CVD
- CKD
- LDL > 190
Low Risk | Moderate Risk | High Risk | Very High Risk |
CVD* | |||
- | - | ≥1 Major RF:
Cholesterol >310 or BP >180 or LDL>190 | ≥ 3 Major RF** |
- | Young*** + DM duration <10year (no other risk factor) | DM duration >10y (w/o OD) AND any ↑RF | DM AND OD/Major RF **
OR T1DM duration >20y |
SCORE <1% | SCORE 1-5% | SCORE 5-10% | SCORE > 10% |
- | - | Moderate CKD (GFR 30-60) | Severe CKD (GFR<30) |
FH (+ Ø other RF) | FH AND any ↑RF |
*CVD = AMI, ACS, revascularization procedure, stroke+TIA, aortic aneurysm, coronary/carotid plaque on imaging
**Major Risk factor
***Young = T1DM<35y or T2DM <50y
lifestyle + Øsmoking
2,5-5h/week moderate exercise OR 30-60min most days
low → <116
moderate → <100
high → <70 + ↓≥50% from baseline
very high → <55 + ↓≥50% from baseline
(CKD + FH are automatically high or very high)
<140 (<130 - if tolerated + <70years)
statins (up to highest tolerated dose)
high risk + LDL <70
high risk + LDL 100-70 → BUT DRUG TREATMENT CAN BE CONSIDERED
LDL <70 BUT CONSIDER DRUG THERAPY!
high + LDL >100
very high + LDL >70
MI
- high potency statin at highest dose tolerated
- add Ezetemib
- add PCSK9 inhibitor
F → only ↓absorption of biliary (+dietary) cholesterol
give ezetemib + lower-dose statin
“The 2013 ESH/ESC Guidelines established also: Isolated systolic hypertension is classified (grade 1, 2, and 3) according to the same systolic BP values indicated for systolic-diastolic hypertension.”
“Optimal BSP < 120 and DBP < 80 mm Hg Normal SBP 120-129 and/or DBP 80-84 mmHg High normal SBP 130-139 and/or DBP 85-89 mmHg”
Check out risk factors, PH + FH of CV diseases
- Family history (gene mutations) + PH
- Hypertension + CV diseases
- Dylipidemia
- DM
- Lifestyle
- smoking
- diet
- obesity
- sleep apnea
- 🧠brain → headache, blurred vision, TIA, motor/sensory defects
- ❤️heart → palpitation, angina, dyspnea, ankle edema
- 🥐kidney → thirst, polyuria, nocturia, hematuria
- 🔴 arteries → cold extr., intermittent claudication
- Brain → murmurs carotid, motor+sensory defect
- Retina → fundoscopy abnormalities
- Heart → apical impulse, arrhythmia, ventricular gallop, crackles (rales) , periph. edema
- Periph. arteries → ↓pulses, cold extremities, ischmemic skin lesion
- obesity
→ identify RF, exclude secondary HT + identify end-organ damage
Routine
- Gluc (RF)
- Lipid profile (RF)
- crea + GFR (renal functin
- Uric acid (renal function)
- K+ (renal function)
- Urinanalysis (renal function)
- Hb + Hct (bleeding)
- Echocardiogram 📷
- Carotid ultrasound
- Quantitative proteinuria (if dipstick test is positive)
- Ankle-brachial blood pressure index
- Fundoscopy
- Glucose tolerance test (if fasting plasma glucose > 5.6 mmol/L (100 mg/dL))
- Home and 24h ambulatory blood pressure measuring (Fig.3)
- Pulse wave velocity measurement (if available)
“
→ see pharma (indication + contraindication)
- classic non-pharmacological
- ACEi/ARBs
- CCB
- Diuretics (thiazide, furo, spirono)
- BB
- second line drugs
- alpha 1 blocker
- alpha 2 agonist
- Rilmenidine (imidazoline type II agonist) → least side effect of #2 line (due to imidazole selectivity)
BP target: <140
- Statins ( target LDL <100)
- Low dose aspirin (if CV history, Afib)
- Glycemic control (target fasting-Glu ≤108; HbA1c <7%)
- Methyldopa + clonidine
- labetalol
- nifedipine
- magnesium sulphate i.v. (prevention of eclampsia)
- hydralazin iv.
T
bilateral upper masses on physical exam
→ confirm with US
Urine test: Protein, Erys, Leukos
Serum crea
T
1 or multiple stenoses at level of extra-renal arteries
- elderly → artherosclerotic
- young (esp. Female’s)→ fibromuscular dysplasia
- sudden onset HT
- worsening
- difficult to treat
- abdominal bruit → later radiation
- Hypokalemia
- ↓renal function
- Douplex US #1 line
- CT angiography
- MRI angiography
1,5cm
- Thiazides + CCB/BB
- add-on: ACEi/ARBs (if unilateral renal a. stenosis!)
- Balloon angioplasty + stent
- surgical revascularization
- Men-2 📷
- Hippel-lindau disease
- neurofibromatosis type 1
- familiar paragangliomas
measure urinary catecholamines + metanephriens
if only slight elevated but highly suggestive:
⇒ clonidine suppression test

- MRI #1
- CT
- occasionally US
- Laroscopically (surgical) excision
- PRIOR to surgery: ALPHA + BETA BLOCKER! + correction of fluidloss
#1 Adrenal hyperplasia (70%)
#2 Adrenal adenoma (30%)
rare: adrenal Ca + aldosteronism sensitive to glucocorticoids
- clinic: refractory BP
- Hypokalemia
- fludrocortisone suppression test

- measure aldosterone + renin
- CT + MRI
- Adenalectomy (laparoscopically)
- PRIOR TO SURGERY: Spironolactone or eplerenone
24h urinary cortisol excretion (>110mmol)
→ confirmed by small-dose or overnight dexamethasone suppresion test
→ normal results = exclusion of cushing
- contraceptives
- steroids
- NSAIDS
- cocaine + amphetamines
- ...
upper airway collapse (i.e. obese)→ respiratory arrest (reccurrent) → ↓SpO2% + ↓↓intra-thoracic pressure, sympath activation → periph vasoconstriction

apnea → sympathetic activation, oxidative stress, inflammation & endothelial dysfunction ⇒ ↑BP
- daytime somnolence
- unrefreshing sleep
- chocking episodes during night
- nicturia
- personality changes + irritability
- ↓concentration
- ↓Libido
Polysomnography
- CPAP
- Weight loss
- smoking cessation
children + young adults
- midsystolic murmor over chest+back (might become continous)
- ↓femoral pulse (but radial pulse is not ↓!)
- ↑BP at upper limb + ↓BP lower limbs (ankle-brachial index)
Stenting +/- continue hypertensive drugs
Concurrent with low or unmeasurable pressure in the lower limbs, hypertension may persist following correction or stenting, especially in adults. This is due to hemodynamic and vascular effects, necessitating the continuation of antihypertensive treatment in many patients.
BP >180/130 + OD
- LVF (congestive) + unstable angina
- encephalopathy + subarachnoid hemorrhage
- fundoscopy → hemorrhages, pappiledema, excudates
- signs of congestive HF + cardiac enlargmenet
- oligura + azotemia (RF)
- Nausea + vomiting (Gi dmg)
- microangiopathy hemoylsis (hematologic dmg)
↑BP (esp diastolic >140)→ esp. leads to HT signs in the eye (fundoscopy)
! most dangerous: encepahlopathy + RF
- ↓Preload
- 🌊Furosemide
- 🌀 Nitroprusside + Nitro
- ↓Afterload (+HR)
- 🎺Labetalol
- 🍦Nicardipine
- HR
- Wallstress → Afterload + Preload

- Contractility
Mitral regurgitation → ↑P in LA → Pulmonary Hypertension + Edema → RV hypertrophy → RV dilation → tricuspid regurg. → RA dilation
→ 📷
#1 🪕 IHD (due to ↓functional tissue, ↑scarring (↑stiffening) + remodeling)
#2 🫀Cardiomyopathy (primary i.e. hypertrophic)
#3 🏮HT → LV hypertrophy (secondary)
Other causes:
- other cardiomyopathy
- valvular diseases
- Arrhythmias (afib, ventricular premature beats)
- hyperdynamic circulation (thyrotox, anemia)
- drugs + alcohol
Congestive syndrome
Low output syndrome
Congestive syndrome
- ↑JVP (Jugular venous pressure)
- pulmonary edema + pleural effusion → dyspnea, orthopnea, noctural dypnea, cough w/ frothy sputum, ↑urination at night → bi-basal crackles/aka rales
- periph. edema
- ascitis + tender hepatomegaly
- heptojugular reflux
- tachycardia + Heartsound 3+4
- cyanosis (central+periph)

Low cardiac output syndrome
- Fatigue
- Pallor
- ↓weight + oliguria
- ↓SBP + ↑DBP
- Cerebral symptoms (memory + cognitive impairment)
- Lab
- EKG
- chest X-ray
- Echo
- stress echo, nuclear cardiology, cardiac MRI, catheterization
- Standard blood test: CBC, Kidney marker, Liver marker
- BNP → ddx pulmonary pathology for edema
- Thyroid marker





HFrEF (<40%)= systolic heart failure +- LV dilated
Diagnosis of Heart Failure with Reduced Ejection Fraction (HF-REF) requires three conditions to be satisfied:
- Symptoms typical of heart failure
- Signs typical of heart failure
- Reduced left ventricular (LV) ejection fraction
HFpEF (>50%) = diastolic HF (hypertension-assoc. LV hypertrophy or primary cardiomyopathy)
Diagnosis of Heart Failure with Preserved Ejection Fraction (HF-PEF) requires four conditions to be satisfied:
- Symptoms typical of heart failure
- Signs typical of heart failure
- Normal or only mildly reduced LV ejection fraction with LV not dilated
- Relevant structural heart disease (LV hypertrophy/left atrial enlargement) and/or diastolic dysfunction”
Heart failure is categorized into several types based on left ventricular ejection fraction (LVEF). These types include:
- Heart failure with reduced ejection fraction (HFrEF): LVEF < 40%
- Heart failure with preserved left ventricular ejection fraction (HFpEF): LVEF > 50% (also known as diastolic heart failure): This type is commonly seen in elderly hypertensive patients and those with primary cardiomyopathies such as hypertrophic, restrictive, and infiltrative cardiomyopathies.
- Heart failure with mid-range ejection fraction (HFmrEF): LVEF between 40% and 50%
- Right ventricular systolic dysfunction (RVSD): This refers to the impaired function of the right ventricle.
- Chronic Cor Pulmonale: This is a condition characterized by right ventricular enlargement and dysfunction due to chronic pulmonary hypertension.
Signs & Symptoms of HF
↓
ECG, Xray, Natiuretic peptide → cardiac disease?
↓ abnormal
Echo
↓ abnormal
Assessment: type of dysfunction, etiology, degree, precipitation factors
↓
Tx
- Øsmoking
- physical activity (20-30min walking 3-5x week; 20min cycling at 70-80% peak HR 5x/week)
- Diet
🥇
- ACEi/ARB (Ramipril/Valsartan) + ARNI
- Beta-blockers (Metoprolol, carvedilo, bisoprolol, Nebivolol)
- Diuretics
🥈
- Spironolactone
🥉
- Digoxin
- Ivabradine (SA node inhibitor)

- Bridge to transplantation
- Patient not considered for transplantation (alternative)
- End organ failure (irreversible) → renal+liver
- mechanical valves
- severe aortic regurgitation
- metastasis
- coagulation + bleeding disorder
→ 📷
- mitral valve repair
- triscupid anuloplasty
- heart transplant → esp. if VO2 is <10ml.kg/min

- Stage A: High risk + no symptoms:
- Risk factors
- Treat hypertension, diabetes, dyslipidemia (pharmacological
- Stage B: structural heart D + no symptoms:
- ACEi / ARBs
- Stage C: structural heart D + previous/current symptoms
- ACEi/ARB
- BB
- Diuretics
- Spironolactone
- Ivabradine (↓SA node)
- Cardiac resynchronization if LBBB
- Stage D: Refractory symptoms
- Inotropes (i.e. Digoxin, Dobutamine, Milrinone)
- LVAD
- transplantation

- Preload reducers
- i.v. Furosemide
- i.v. Nitro
- Spironolactone
- Afterload reducers (if Øhypoperfusion !)
- Dobutamine
- ↓BB + ACEi!

- Sit patient upright
- high flow oxygen
- Nitrates i.v. (until BP <110) Øin low BP
- Furosemide
→ consider CPAP + opiates (cave: resp. depression)
→ if refractory: inotropic agent + mechanical ventilation + intraortic balloon pump. 📷
→ can be given monotherapy or with BB
⇒ RATE CONTROL
- New onset Afib + ischemia
- afib + Symptoms of pulmonary congestion
- afib + Symptomatic hypotension
- RVR (Rapid ventricular rate)
↓output + pulmonary congestion ⇒ myocardial ischemia

Right heart failure w/ systemic congestion due to primary lung pathology
Signs of systemic congestion: ↑JVP, Leg edema, Hepatomegaly
not in rest only on physical activity
- sympathetic overstimulation
- HF
- endocrine disorder (thyroid)
- resp. failure
Artrial flutter (2:1)
PSVT (no p-waves)
non-sinus stimulus
asymptomatic OR
brief early aprupt heartbeat - pause - followed by a stronger beat
usually no pathological significance (if no afib)
- anxious → BB + sedatives
- >20% extrasystoles on 24h holter → class Ic (Flecainide, Propafenon) or ablation (pulm. veins)

rapid atrial non-sinusoidal acitvation
rate 150-250/min (>150)
Palpitations (suddenly begin + stop and can last sec-hours)
if >200:
chest pain (ischemia due to high demand)
acute HF → syncope (low output syndrome due to ↑HR)
- Re-entry AV-node: dual slow or fast pathyway (aka AVNRT)
- accessory pathways (orthodromic vs. antidromic)
- pathologic foci in the atrium

- No p-waves (overlapped by QRS or T)
- Narrow 150-200/minute QRS tachycardia
→ 📷
preexitation (foci) 📷
but other can be as well → do electrophysiology
some ventricular transmission blocked (usually every second) → atrial tachycardia with block
→ 📷
retrograde p 📷

#1 Vagal + Adenosine
stable → Rate (BB, Verapamil) or Rhythm control (Amiodaron, IC: Propafenone, Flecainide)
unstable → shock
⇒ Ablation for definite prophylaxis
vagal m. = carotid massage, blowing in a syringe in laying position when patient is blowing with high pressure → elevate legs, eye pressure, induce vomiting
Do that when PSVT is frequent → within less than 3 month
Step 1: AV node blockers (BB or non-dihydropyridines CCB (Verapamil, Diltiazem)
Step 2: Class IC (Propafenone, Flecainide) or Class III (Sotalol)
Step 3: Amiodaron
Step 4: Ablation
(ablation can also be done as step 1)
rapid non-sinus activation 200-350 BPM
due to macro-reentry betw. tricuspid + vena cava (classic: counterclockwise; can also be clockwise)
due to ↑intra-atrial pressure, ischemia or inflammation
- right heart damage
- HF + ↑BP
- pulmonary diseases
- heart surgery (scars circuit not normal curcuit)
- sick sinus syndrom (tachy-brady)
- thyrotox
- etc.
- rapid rate palpitation
- refractory to valsalva (+ adenosin )
- symptoms depending on underlying heart diseases (i.e. HF, thromboemolic)
- 2:1 (or 3:1, 4:1) transmission of p-waves
- if 1:1 transmission → Vfib → sudden cardiac death
- F-waves 250-300/min + high amplitude + wide base
- negative in inferior leads + pos. in V1 in counterclockwise
- reverse in clockwise
- if counterclockwise: saw-tooth
- QRS narrow regular (or irregular); rate = 100-150
Treatment: Acute:
- For unstable patients with hypotension, congestive heart failure, or angina, electrical cardioversion is recommended.
- For stable patients, chemical cardioversion (e.g., amiodarone) should be considered along with rate control (e.g., beta-blockers).
- In both cases, anticoagulation is necessary, similar to atrial fibrillation.
Long-term:
- Antiarrhythmic medications are commonly used.
- Radiofrequency ablation via catheter, especially targeting the cavotricuspid isthmus, may be performed. 📷
- RATE CONTROL = BB, NDHP-CCB, Digoxin
- RHYTHM CONTROL
= Amiodarone, Class Ic, Ibu+dofetilide OR
electrical cardioversion (if unstable) OR
Long term = ablation
- Anticoagulation (if >48h after onset, BEFORE cardioversion) → for 3 weeks
- TEE (Transesophageal Echocardiography)
⇒ same as afib
directly ablation
non-sinus rapid chaotic activation of atria
BPM 350-600
ATRIAL FIBROSIS due to
- ↑intra-atrial p
- inflammation
- ischemia
- valvular diseas, congenital diseases, aterial hypertension, cardiomyopathies, congestive heart failure , after heart surgery
paroxysmal not longer than 7 days
persistent in first 3-12 month
permanent >12 month
microcircuit around pulmonary vein
→ no proper atrial contraction due to too rapid stimulation → ↓output by 25-30%
High heart rate 120-180 BPM
→ most of f-waves are blocked by Av-node
thromboembolic
- paroxysmal → sudden palpitations onset with variable duration
- persistent + permanent → reduced palpitation but increase with effort
- fatigue + ↓effort capacity , dizziness
- dyspnea
- LVF + acute pulmonary edema
- decompensation of pre-existing HF

Echo or TEE → thromboembolic risk
- Unstable → Shock
- Stable
- Rate control (AV blocking agents=BB, CCB, Digoxin) or Amiodarone
- Rhythm control (Class I, III or electrical shock (to overdrive stimulation))
- ablation
↓(if conversion to sinus)

STEP 1: RATE CONTROL (BB, CCB, Digox)
STEP 2: Ablation (compare: can be #1 for aflutter)
+ anticoagulation
Aflutter prevention → rhythm control (Class IC or III) or directly ablation +- BB +- Anticoagulant
choice depends on STRUCTURAL heart disease:
if no structural ⇒ Class IC preferred
if structural → Class III
Alternative for both: Ablation
- TEE (for direct cardiversion)
- If >48h → oral anticoagulants for 3-4 weeks then conversion
aka ventricles cant handle without atrial contraction
⇒ AV-node ablation + PACE MAKER
can occur in healthy + in every cardiac diseases → more freq. in: post-MI arrhythmia, dilated cardiomyopathy, HF
ventricular origin
F - usually not
ONLY IF → frequent, systemized or in runs (see later)
ASYMPTOMATIC OR
palpitation
Pause after VEs (feels like heart stopped) → then strong post-extrasystolic beat after pause
→ check pulse! → VEs + pause can be felt
- wide QRS >120ms
- ST + T waves reversed to ST+T from normal QRS complex
- refractory phase after extrasystole → postextrasystolic compensatory pause = distance pre-post extrasystolic QRS = 2x normal RR interval
- Isolated or systematized:
- Monotope or polytope (aka polymorphic(complex) /monomorphic aka multiple foci vs one focus). 📷

no treatment needed
TREATMENT IF FREQ. OR COMPLEX (couplets, runs, polytopes=complex)
→ i.v. lidocaine (post-MI VE)
→ BB
→ amiodarone
LONG term → IC, II, III
>25% VEs (24 holter) → ↑dimension of LV → ↓EF
antiarrhytmics or ablation
≥3 VE with a rate > 100/min
- idiopathic
- underlying heart disease
- ACS +post MI
- intox
- myocarditis
- cardiomyopaty
- HF
T
- no symptoms (sometimes in idiopathic)
- low cardiac output syndrome (systolic HF) (fatigue, pale, signs of underperfusion etc)
- ventricular failure +- cardiogenic shock
- trigger Vfib + cardiac arrest (structural heart disease)
- sudden onset of palpitations
- congestive HF
- +/- pulmonary edema
sustained >30s
unsustained <30s
⇒ can also be seen on EKG
100-180 BPM
- hemodynamically stable
- Amiodaron
- BB
- (Lidocaine in ischemic VT)
- hemodynamically unstable
- electrical shock
- (consider bridging with i.v. amiodarone, lidocaine or procainamide)
= pulseless ventricular tachycardia
HR ca. 200 BPM + NO periph. pulse
aka cardiocirculatory arrest
Shock + CPR
NON-SUSTAINED:
- BB (+/- amiodarone) → except. non-sustained with no structural HD
SUSTAINED:
- Step: treatment underlying diseae (i.e. ischemia → revascularization)
- Step: Class III, IC, Ib
- Step: If EF <35% → ICD
- Step: Ablation can be considered (esp. in idiopathic)
III Amiodarone, Sotalol IC Propafenone, Flecainide IB Mexiletine
Also Beta blocker is recommended
regular 200-250 BPM
→ quickly evolves towards Vfib!!!
CPR
→ after resuscitation - prevention:
- antiarrhythmic drugs (Amiodarone, BB)
- if episodes of Vfib → ICD
- etiological Tx → myocardial revascularization / catheter ablation
T
- idiopathic fibrosis of conduction system
- IHD
within AV (and above His) → suprahisian/intranodal
within His (and below AV) → infranodal
intranodal
Intranodal blocks, which involve interruption of impulse transmission within the atrioventricular (AV) node, have a better prognosis compared to infranodal or infrahisian blocks. Intranodal blocks allow for a "escape" rhythm with a rate of 45-50 beats per minute, which is sufficient for the patient to remain awake and engage in regular activities. On the other hand, infranodal or infrahisian blocks result in a ventricular escape rhythm with a rate of 10-30 beats per minute, which can lead to long pauses and a higher risk of asystole and death.
I° → all p transmitted, PR>200ms (22 in eledery)
II°
- intermittently ommited
- Mobitz I → PR intervals get progressively longer → suddenly one p wave not followed by QRS
- Mobitz II → PR-waves stays the same suddenly no QRS after one p
- 2:1 → only every second p followed by QRS
- advanced → ≥2 p-waves are not transmitted
III° → complete dissociation (R-R distance + P-P distance is REGULAR)


- I + IInd degree with intermittently blocked → asymptomatic
- II° 2:1, advanced II° + III° → regular/irregular rhythm (palpitation)
- Auscultation → ↓HR <40-50
- Systolic BP ↑ (compensatory vasoconstriction)
- LVF
- ↓Output: ↓effort capacity + effort syncope
- Congestion: worsening of underlying heart failure
Mobitz 1 → intranodal
Mobitz 2→ infranodal
2:1 → intranodal (QRS narrow); infranodal (QRS wide)
→ low junctional rhythm(from AV node 40/min) or ventricular escape rhythm (below AV node 10-30/min)
asystole → Adam stokes syndrome syncope/death Bradycardic ventricular arrhythmias
- I° + II° Mobitz I → no therapy
- II° Mobitz II risk for complete heart block → temporary or permanent pacing
- II° 2:1 → temporary or permanent pacing / atropine if intranodal (narrow QRS)
- III° → permanent pacing (except congenital heart block→adapted)
⇒ or drugs if you cant do pacing or for bridging (Adrenaline, Noradrenaline, Dopamine; atropin when intranodal)
single or dual
single → RV or RA
dual → RV + RA
depression/absensce of pulse formation from sinus sode
→ might also exist with AV-block (bi-nodal)
→ sometimes cause SVT
idiopathic, ischemic or fibrosaaaa
→ See av block
#1 idiopathic degeneration or ischemic heart diseases
#other (inflamm, drugs, cardiomyopathy)
sinus node dysfunction = excessive vagal tonus
- ↓effort capacity + effort syncope
- → might lead to asystole + sudden death
- → bradycardia-tachycardia syndrome → SVT alternating with bradycardia → cardiac + periph ischemia + acute heart failure
- Pulse <40-50 irregular or regular
- ↑Systolic BP (compensatory)
- Sinus bradycardia: 📷
- <50 BPM; <40 = suggestive for SSS
- Sinus Pauses. 📷
- Atrial fib + low ventricular rate (in case of simultaneous AV node imparment - binodal impairment) 📷
- Permanent sinus arrest - junctional/ventricular escape rhythm 📷

- Bradycardia-tachycardia syndrome 📷→ alternating bradycardia with episodes of atrial tachycardia/SVT → Permanent cardiac pacing necessary
stress or atropine test → DDx SSS vs node dysfunction due to ↑vagus tone
→ if SSS HR will not exceed 90 BPM under stress + atropine
- HR >40 + asymptomatic → follow up
- If pauses >3s + symptomatic bradycardia/syncope → permanent pacemaking
- symptomatic → emergency drugs / pacemaking
- Drugs or shock for tachycardic episodes
- or ablation/electrophysiology
- drugs: Atropine, Adrenaline, Noradrenaline, Dopamine
reflex, orthostatic hypotension + cardiac

Reflex → inapproriate sympathetic response
Orthostatic → chronically impaired sympathetic function
20 mmHg in systolic or a 10 mmHg drop in diastolic blood pressure within 3 minutes of standing
Drug which ↓Volume or ↑vasodilation + neurogenic causes (primary, secondary)
arrythmias
sick sinus
AV block
As a general rule, the more severe forms of acquired AV-block, such as Mobitz I block, "high grade" AV block, and complete AV block, are closely associated with syncope. These conditions are characterized by disturbances in the conduction of electrical signals between the atria and ventricles of the heart.
structural heart diseases
- Anemnesis: circumstances, history, onset, way of falling, end of the attack, etc.
- BP
- carotid sinus massage if >40y → cartoid sinus syndrome
- Echocardiography → structural heart disease
- ECG → arrhythmic suspected
- Holter
- Loop recorders
- implantable recorders
- electrophysiological study
- orthostatic challange (lying-stand; tilt test)
- Exercise stress test → exercise induced syncope is suspected → also diagnostic if Mobitz II or III° AV block without syncope
- Coronary angiography → Ischmia suspected
- Psychiatric drug evaluation → drug-induced suspected
- Neurological exam → primary vs. secondary autonomic failure (sec = DM, amyloidosis)
ventricular pause >3s and/or ↓BP >50
sick sinus → suspect when <50BPM in rest
BBB → ecg
Tachycardia → ecg + palpitation
≥ 20mmHg from baseline or < 90mmHg
→ Cerebrovascular disorder → subclavian steal. 📷
- EDUCATION (avoid trigger, recognize prodromal symptons, manoeuvers)
- TRAINING: TILT-Training 📷, HEAD up tilt sleep etc.
- cardiac pacing if tilt-induced cardioinhibitory response (HR<40 or asystole)
CORRECT HYPOVOLEMIA
- hydration + adequate salt intake
- adjunctive: fludrocortisone (mineralcorticoid → ↑BP+Volume)
mainly pacemaker
ablation
ICD
- aortic stenosis + myxoma→ surgery
- underlying process → infarction or pericardial tamponade
- hypertrophic cardiomyopathy → ICD
most severe form of LV failure
BP <80 for >30min
↑LV filling pressure (pulmonary capilly wedge >18)
80% STEMI
→ other causes: mechanical defect or RV-infarction
↑LV-filling pressure
↓Output
↓BP
hypoperfusion → cold, acidosis, oliguria
mitral regurgitation + other mechanical lesion
NE
- unstable + angiography is done
- refractory to drugs
- refractory ischemic pain
LVAD → until new heart transplant
systolic <100
diastolic <65
- Idiopathic
- Orthostatic hypotension
- Secondary
- Cardiovascular diseases: myocardial infarction, acute myocarditis, constrictive pericarditis, valvulopathies.
- Endocrine diseases: thyroid insufficiency, suprarenal insufficiency.
- Neurological disorders.
- Infections.
- Toxic agents.
- Psychotherapy
- physical treatment
- adequate fluid + salt (hypovolemic)
- fludrocortisone (orthostatic)
- Norepinephrin septic shock/hypotension
Coronary ischemia causes abnormalities in electrical activity (electrocardiographic ischemic abnormalities; rhythm disorders), heart function (systolic or diastolic dysfunction), and chest pain. These manifestations are associated with coronary artery disease and have clinical implications.
Coronary ischemia can result in various electrocardiographic changes indicating myocardial ischemia. These changes may include ST-segment depression or elevation, T-wave inversion, or pathological Q waves. These findings help diagnose myocardial infarction and guide management.
Systolic or diastolic dysfunction can occur due to coronary ischemia. Systolic dysfunction impairs heart muscle contraction, reducing stroke volume and cardiac output. Diastolic dysfunction involves impaired ventricular relaxation or increased stiffness, affecting filling and ventricular compliance.
Chest pain, known as angina, is a common symptom of coronary ischemia. It is described as a pressure-like or squeezing sensation in the chest that may radiate to the left shoulder, arms, abdomen, or neck. Prompt recognition and management of chest pain are crucial for preventing complications and ensuring optimal outcomes.
70%
at what point angina occurs during stress test
estimate the double product = HR x syst. BP when ST depression occurs on stress test
= index of myocardial oxygen consumption ⇒ estimation of mortality risk
- only during exercise or emotional stress
- Ø during rest
- 1-10min (depending on when exercise stopped) → alleviated at rest
- alleviated by sublingual Nitroglycerin
- radiation (neck)
- Levine sign 📷
sinus tachycardia
T → except. sinus tachycardia
- Class 1: ordinary physical activity → angina during exertion (strenuous, sudden or prolonged)
- Class 2: slight limitation ordinary activity. Angina during fast walking or climbing stairs. After large meals, cold, emotional stress
- Class 3: marked limitation. angina walking a normal pace
- Class 4: Invalidating angina, unable to perform any activity without discomfort. Angina may be at rest → transition to unstable angina
inverted t-wave
but 50% → normal ekg
ST-depression 📷→ for pos. dg: ≥1mm
+/- Inverted T-waves
≥1mm depression for at least 1min
+/- angina
- Coronary Angiography:
- exclude → CT coronary angiography (in atypical symptoms + low probability)
- coronary angiograph → diagnostic + severity assessment
- echo → contractility abnormalities during ischemic periods
- prove → scintigraphy (myocardial)
- lifestyle
- ACEi/ARbs (in all)
- Aspirin 75mg (#2line: Clopidogrel 75mg) (all symptomatic patients)
- Statins (all symptomatic patients)
#1 line BB
#2 add LAN + Nitroglycerin patches
#3 add CCB (DHP or NDHP CCB)

#4 add Ivabradine
#5 add Metabolic medication (trimetazide, ranolazine etc)
- Class III-IV + low ischemic threshhold (double product <15.000) + drug refractory symptoms
- severe events
- all patients survived cardiac arrest
- severe ventricular arrhythmia
- post-infarction angina
bare metal stents or #1 drug eluting stents
severe ischemia + angia with low ischemic threshhold
STEMI → overlapping trombus on unstable plaque → occlusion → myocardial necrosis
NSTEMI → overlapping trombus on unstable plaque → Ø complete occlusion → Ønecrosis or minor subendocardial necrosis
T
- Thrombus
- O2 demand/supply mismatch
- MI death W/o Necrosis enzymes
- Iatrogenic MI
Intraluminal thrombus is formed on the atheroscleroto plaque wich can be ruptured cracked eroder or discecred
Embolism or coronary spasm, potension, arrhythmias with haemodynaric instability, severe anemia
Death occurred before necrosis enzymes were reacted or dosed, but there were signs.
Type 4a: Myocardial infarction caused by percutaneous coronary intervention (PCI) Significant increase in necrosis enzymes is 3-20 times if already elevated, accompanied by symptoms of ischemia, additional ECG alterations, new imaging of myocardial kinetics disorders, or angiographic detection of a complication related to PCI.
Type 4b: Myocardial infarction caused by stent thrombosis.
Type 5: Myocardial infarction caused by coronary artery bypass graft (CABG) surgery. Significant increase in necrosis enzymes 10 times, accompanied by additional ECG alterations.
- severe angina
- at rest
- >1h
- Ø influenced by nitro
- radiation
- painless is diabetic elderly
- diastolic + systolic HF
- might be asymptomatic
- dyspnea
- pulmonary edema
- cardiogenic shock
- palpitation → sinus tachycardia, premature beats, SVT
- Autonomic symptoms: Sweating, agitation, palor, cold
Category | Conditions |
Cardiovascular | Acute coronary syndromes, Severe aortic stenosis, Obstructive hypertrophic cardiomyopathy, Acute pericarditis, Dissection of the aorta |
Pleuropulmonary | Acute pulmonary embolism, Pneumonia, Pleurisy, Pneumothorax, Malignancies |
Gastrointestinal | Hiatal hernia, Gastroesophageal reflux disease, Gastric/duodenal ulcer, Pancreatitis, Biliary colic |
Parietal - thoracic | Some cases of acute abdomen, Intercostal radiculopathies, Cervical Herpes Zoster, Shingles (requalitates to Intercostal Herpes Zoster), Tietze's syndrome |
Psychic | Anxiety disorders |
I → Absence: ØCrackles ØS3
II → Mild: Crackles lower half only, S3
III → Moderate (pulmonary edema): Crackles upper chest
IV → Severe: Cardiogenic shock


V1-6
LAD → V1-4 (6)
LXC → I, aVL
D2+3
aVF
ST depression + high R in V1, V2
V1-V3
- Myoglobin (but less specific than trop)
- Troponin I + T >0,2 = necrosis confirmed
- CK + CK-MB
F - not mandatory → dont delay angiography because of that!
- ↓LV contractility + Dyskinesia (systolic reverse movement of an area)
- Complications
- Thrombus
- Aneurysm (dilation + later wall thinning)
12h → asap
T
- Reperfusion therapy → 🥇PCI or fibrinolysis(when PCI Ø available <2h)
- Drugs ⇒ MONAAS BH
- General measures: Nitrates, analgesics, O2, morphine
- Dual platelet: Ass + Tica
- Heparin/Enoxaparin
- Adjuvant:
- Statins,
- BB (if ØHF),
- ACEi


→ RV-infarction → fluid + Ønitro

⇒ 📷
Absolute Contraindications | Relative Contraindications |
- History of intracranial hemorrhage | - History of chronic, severe, uncontrolled hypertension |
- Primary or metastatic intracranial neoplasia | - Significant hypertension at presentation |
- Ischemic stroke in the last 3 months (except within 4.5 hours) | - Ischemic stroke in the history within 3 months |
- Dissection of the aorta | - Other intracranial conditions not listed as absolute contraindications |
- Active bleeding or bleeding diathesis (except menstrual bleeding) | - Pro oncology cardiopulmonary resuscitation within 2 minutes or trauma |
- Significant head trauma within the last 6 months | - Major surgery during the last 3 weeks |
- Intracranial or intraspinous surgery within the last 2 months | - Recent internal bleeding (within the last 2-4 weeks) |
- Severe uncontrolled hypertension unresponsive to medication | - Uncomplicated vascular puncture |
- Previous treatment with streptokinase within the last 3 months | - Pregnancy |
- Active peptic ulcer | |
- Oral anticoagulant treatment |
<40%
venodilation → ↓preload → ↓O2 demand
Complication | Occurrence | Description |
Cardiac arrhythmia | First few days and within the first 24 hours post-MI | Important cause of death before reaching the hospital |
Postinfarction fibrous pericarditis | 1-3 days | Friction rub |
Papillary muscle rupture | 2-7 days | Postero-medial papillary muscle rupture ↑ risk from posterior descending artery. Severe mitral regurgitation. |
Interventricular septal rupture | 3-5 days | Macrophage-mediated degradation → VSD → ↑ O2 saturation and pressure in RV |
Ventricular pseudoaneurysm formation | 3-14 days | Free wall rupture contained by adherent pericardium or scar tissue; ↓ CO, risk of arrhythmia, embolus from mural thrombus |
Ventricular free wall rupture | 5-14 days | Free wall rupture → cardiac tamponade. LV hypertrophy and previous MI protect. Acute form leads to sudden death. |
True ventricular aneurysm | 2 weeks to several months | Outward bulge with contraction ("dyskinesia"), associated with fibrosis. |
Dressler syndrome | Several weeks | Autoimmune phenomenon resulting in fibrinous pericarditis |
LV failure and pulmonary edema | Occurs secondary to other complications (timing depends on them) | Due to LV infarction, VSD, free wall rupture, papillary muscle rupture with mitral regurgitation. |
- Arrhythmias:
- Ventricular arrhythmias
- Premature ventricular beats
- Ventricular tachycardia
- Ventricular fibrillation
- SVT
- Brady arrhthymias (Sinus bradycardia + AV-block)
- LBBB
- LVF + pulmonary edema
- Revascularization
- furosemide
- Nitrates
- standard measures → oxygen, morphine, mechanical ventilation
- ↓ afterload (or ↑afterload if Cardiogenic shock (Killip IV))
- ACEi
- NE or dobutamin if BP<90
- (Revascularization)
- NE, dobutamin, dopamin
- Volemic support
- Intra aortic balloon pump
- ECMO (extracorporal membrane oxygenation)
- (LVAD)
- Free wall rupture
- Mitral regurgitation (papillary muscle rupture)
- Interventricular septum perforation
- Morphine + mechanical suppoirt
- diuretics
- Nitro
- inotropic durgs
- Pericarditis
- relapsing chest pain (mimic re-infarct)
- friction rub
- echocardiography
- LV true aneurysm
- ACEi
- anticoagulation
- aneurysmectomy (in selected cases)
- LV thrombosis*
- LV pseudoaneurysm
- Extension of ac. MI*
- Post-infarction angina*
no treatment mandatory → just monitor
→ except: R-on-T phenomenon or non-sustained VT → lidocaine/amiodarone
electrical cardioversion
(if cannot be applied or bridging: lidocaine/amiodarone)
→ after sinus rhythm restored → continue with BB+amiodarone
defibrillation
if HR > 100BPM
BB
if hemodynamically instable →electrical cardioversion
BB (+/- amiodaron) if stable
unstable → shock
atropin + tempary pacing
suprahisian → Atropin
infrahisian → pacing
T
→ new onset LBB + chest pain = considered STEMI
30%
hemopericardium + percardial tamponade
→ emergency surgery if hemodynamic stabilization is not obtained with drugs!
only analgesics + anti-inflammatory drug when pain severe
the apex
intraventricular "regurgitation" → ↓output → LVF
→ might also lead to Vtach + Vfib
The 4 A’s

oral anticoagulation 2-3month
Echo → communication aneurysm + pericardium
(pseudoaneurysm = left ventricular free wall ruptured contained by adjacent pericardium)
ECG + enzymes (Esp. CK-MB)→ identical treatment to first time
- lifestyle (classic like angina)
- physical rehabilitation (↑exercise capacity)
- drugs
- Dual antiplatelet (at least 1y)
- “adjuvants of acute MI “
- High dose statins
- ACEi
- BB
unstable angina
non-Q MI
unstable angina → pain at rest but Ø↑enzymes (=Ø necrosis)
NSTEMI → ↑enzymes
T
→ NSTEMI with necrosis
→ unstable w/o necrosis
- Unstable angina out of progressively worsening stable angina (longer duration)
- de-novo angina out within first month of stable angina (1month exercitional angina) → ↑↑risk for MI
- Secondary rest angina = stable plaque + ↑Oxygen demand (↑HR, acute. HF) → precipitate rest angina
like stable angina
in de-novo → monitoring + coronary angiography! (if worsening or refractory)
- intense + prolonged pain (strong nerve-ending stimulation
- ↓syst+diastol. performance (in the ischemic area)
- ↓contractability
- ↓EF+Output
- rhythm disorder + cardiac arrest
- angina at rest (+during minimal physical exertion)
- broader irradiation of pain than stable angina
- >10-15min
- ↑HR (mild) during minimal exercision+emotional stress
- signs of LV failure
- dyspnea + orthpnea
- vegetative symptoms (palor, sweating)
- SINUS arrhythmia → palpitation
- most cases also: prematue VB, Vtach, Vfib
- ↑BP (anxiety + pain)
stable 1-10min
unstable/NSTEMI >10-15min
STEMI >60min
T
TROPONIN
↑ → NSTEMI confirmed
normal → unstable angina
- when Troponin is ↑ for confirmation
- extend of necrosis
- In re-infarcts
- Echo → LV performance, contractability (global +segmental), diastolic function ⇒ all affected by signif. ischemia
- Coronary angiography
- first day for high risk
- next few days for medium risk
- in low risk: stabilization → exercise stress test → if positive with high-risk criteria → coro
NAAS BH
- Dual anticoagulation (Ass + Tica)
- i.v. unfract. Heparin or Enoxaparine or Fondaparinux
- Nitates (sublingual, LAN, Nitro patches, iv. nitro) → pain control, if not enough add other analgesic i.e.opioids
- BB → max. tolerated dose (200mg metoprolol)
- if contraindicated → NDHP-CCB instead
- or add DHP-CCB if BB+LAN not enough
- ACEi
- Statins (Atorvastatin 80mg)
- in NSTEMI
- in medium + high-risk unstable angina
- in low-risk + positive stress test (with high-risk criteria)
consider aorto-coronary bypass
- 12month dual platelet
- NOAKs if dilated LV, afib or ↑risk for ACS
- BB
- ACEi
- Statins
- Nitrates if still angina
rest angina
→ usually morning (acidosis)
→ exposure cold
→ usually no pain during exertion
T
ST-elevation >1mm
prinzmetal = spontanous + promt resolution of ST elevation after pain relief (usually <15min)
F they can (including Vfib)
normal
Coronary angiography → Ø lesion + provocation test
(or angioCT)
F → anti-ischemic drugs → BUT: Ø BB!!
Coronary dilators
⇒ 🍦DHP CCB + 🌀 Nitrates
siginif. coronary lesions → angina on exercition
+transient superimposed spasms → ↓angina threshholt + sometimes chest pain at rest
ST depression → RESOLVE during pain → appear again after pain relief
- Idiopathic (familiary genetic factor)
- ischemic (post-MI)
- viral → esp. coxsackie (see myocarditis)
- Valvular
- Toxic esp. alcohol
↓contractability → ↓EF<40% (systolic dysfunction) → ↓output+↑pressure into atrium
→ secondary diastolic dysfunction → congestion (until pulmonary edema+RVF) → mitral/trikuspid regurgitation (can also be other way around see etiologies)
classic systolic heartfailure (+diastolic → late)
- can be asymptomatic for a long time
- exercise capicity ↓
- effort dyspnea
- Low cardiac output syndrom
- noctural paroxysaml dypnea
- acute LV failure, sudden cardiac death
- pulmonary edema (diastolic failure)
→ See systolic heart failure
- Signs of hypoperfusion (low cardiac output syndrome)
- sinus tachycardia (almost always)
- mitral regurgitation (always)
- Ventricular gallop (S3)
- Echo doppler
- diastolic diameter ≥60mm
- ↓EF<40%
- if <35% → severe
- Global hypokinesia (in ischemic → segmental)
- Mitral + tricuspid regurgitation
- diastolic dysfunction
- Enlarged left atrium + right heart (due to secondary diastolic dysfunction)
- Afib + Atrial thrombosis (due to secondary diastolic dysfunction)
- Chest X-ray
- Cardiothoracic index ≥0.55 = diagnostic (if <0.50 = exclusion)
- pulmonary congestion
- Pulmonary hypertension
- Pleural effusion
- Kerley A+B lines
- EKG
- SVT - Afib
- Ventricular arrhythmias
- extrasystoles
- Vtach
- Vfib
- Negative T-waves (might be seen)
- LBBB → ↓output even further → CRT
- Exercise stress testing + 6min walking test
- BNP → always elevated
- also check crea (serum)
- Radioisotope ventriculography (scinti)
- EF
- estimation of diastolic dysfunction
- MRI
- Myocardial biopsy
diagnosis
prognosis
monitoring

Cardiac output assessment of RV
exclusion of other secondary causes
bad as shit → ≥50% 5y mortality
(favoured by same risk factor correction as HF)
alcohol cessation → regression of symptoms in 6m
revascularization of hibernating myocardium
HF-algorithm + ICD + Transplant
- Like HF-drugs: ACEi, BB, diuretic, spirono
- If Afib present → digoxin
- if EF ↓ + QRS >130ms → CRT (atriobiventricular or biventricular)
- If Ventricular arrhythmias → ICD → if not possible amiodaron
- if EF <35/30 (30=mandatory)
- Heart transplant
- CV rehabilitation
Hypertrophy → diastolic dysfunction +/- ventricle outflow obstruction
→ ischemia

Mainly idiopathic
1/3 familiar
T
- non-obstructive (non-septal)→ eqally distributed hypertrophy (like in HT). 📷
- obstructive → assymetrical hypertrophy of interventricular septum 📷 → subvalvular aortic stenosis (septum bulges into aortic outflow tract) → drag effect aspiration of mitral valve → ant. mitral valve in systole (SAM) 📷→ more stenosis
severity of asymmetric hypertrophy
abnormal relaxation
severe, restrictive pattern, pseudonormalization
during exercise
(sinus tachycardia → ↓diastolic pressure → more obstruction of the outflow)
↑in LV diastolic pressure + LVH + Myocardial ischemia
obstructive hypertrophic (but the other one as well to lesser degree)
- ↑HR → ↑interventricular septum contractility → ↑obstruction
- ↓LV volume → more obstruction
Low output during exercise + congestion + arrhythmias

- exercise syncope
- exercise cerebral ischemia
- exercise angina pectoris
- acute LVF → ac. pulmonary edema
- Rhythm disorders
- PB
- non-sustained tachycardia → vfib → sudden cardiac death
- afib
TTTT!!!
restore sinus rhythm as qucik as possible
- systolic ejection murmor (in obstructive type)
- ↑during exercise (due due ↑HR )
- mitral regurgitation murmur
- S4
↑HR (exercise)
fails to increase
T - echo
- hypertrophied walls → ↓ventricular lumen
- hypertrophied asymetrical septum
- mitral regurgitation
SAM
(Systolic anterior movement)
- LVH
- Left atrial hypertrophy (bifid p-wave)
- Afib + ventricular arrhythmias
- sometimes pathologic Q + T-inversion (signs of ischemia)
pulmonary congestion
LVH
- provoke exercise induce syncope
- arrhythmia screening → if malignant ventricular arrythmia → surgery or ICD
- clinically manifest angina
- surgery is needed (screening for artherosclerosis)
genotype screening
minimal
medium
high
- Positive FH SCD

- PH:
- syncope
- malignant arrhythmias
- exercise hypotension
- severe LVH (>30mm)
- ↑Filling time (BB/NDHP-CCB + Disopyramide/amiodaron)
- treatment of septal hypertrophy
- ICD for ventricular arrhythmias
- Treatment of Afib → Cardioversion, Ablation, anticoagulation

In severe or refractory cases, surgical treatment (septal myectomy) or DDD pacing (with initial stimulation of the right ventricle, resulting in paradoxical movement of the interventricular septum during systole and a reduction in the degree of subaortic dynamic stenosis with decreased left ventricular outflow tract obstruction) can be considered. An alternative to surgery is alcohol septal ablation, which involves the infusion of pure alcohol into a major septal branch of the left anterior descending artery (LAD), inducing a localized "septal infarction" that leads to a reduction in the thickness of the interventricular septum and the degree of systolic obstruction. 📷
amiodarone
Like heart failure but:
- Digoxin contraindication
- Diuretics: caution (risk for hypotension)
- ACEi + Nitrates: caution!
heart transplantation
- diastolic dysfunction
- ventricular stiffness
- EF >40%
- non-infiltrative: myocardial fibrosis (+/- endocardial fibrosis)
- myocardial infiltration
- amyloids
- fatty infiltration in obese
- (or other compounds)
- elevated ventricular pressure → pulmonary + systemic congestion (but no dilation of chambers)
- signs of systolic heart failure with exertion (↑HR → ↓output → ↓EF)
- tachyarrhythmias
- conduction disorder
- sick sinus syndrome
- AV-block
- For a long period: moderate ↓exercise capacity
- later: moderate congestive symptoms
- discrete periph. congestion (hepatomegaly, limb edema)
- Moderate cardiac output syndrome → during stress/exertion
- sinus tachycardia
- S4
- DIASTOLIC DYSFUNCTION RESTRICTIVE PATTERN (doesnt really relax)
- mitral regurgitation
- TRICUSPID REGURG. + MODERATE PULMONARY HT
- dilated IVC + hepatic congestion
- ↑wall thickness in infiltrative type might be seen (ventricular hypertrophy mimicking)
- normal chamber
- EF>40%
(look-a-like on echo)
EKG → in amyloidosis Ø signs of hypertrophy!
- BBB
- AV-block
- Ventricular arrhythmias
Excluding other cardiomyopathy forms (hypertrophic + dilated)
⇒ restrictive: normal cardiothoracic index (<0,5) + moderate pulmonary congestion
(dilated: ↑index; hypertrophic: ↑ pulmonary congestion)
→ underlying diseases (amyloidosis + fatty infiltration) → but only efficient for minority
- small dose Diuretics + ACEi (+BB)
- Antiarrhythmics
- Pacemaker for bradyarrhythmias (esp. AV block)
- heart transplant (severe)
genetic diseases → FH!
Replacement myocytes with fibro-fatty tissue → dilation of RV + arrhythmias (can be severe: Vfib)
- inverted T-wave on ant. leads (V3+4)
- Arrhythmias
- Ventricular arrhythmias (#1 - 60%)
- Vfib
- non-sustained
- sustained
- extrasystoles
- SVT (20%)
- BBB
→ 📷
- dilated right ventricle
- Diffuse hypokinesia
- (depressed LV function)
MRI or myocardial biopsy
Symptomatic
- antiarrhythmics
- if severe: ICD
- most cases: Heart transplant in the end
VIRAL
- adeno-virus
- coxsackie virus
- cytolomegavirus
- influenza (often subclinical)
Viruses have shared similarities with myocytes → Antibodies → directed against myocytes → over time: dilation cardiomyopathy
→ systolic HF
- Sinus tachycardia (due to inflammation)
- Ventricular extrasystoles (inflammatory foci)
- rarely: T-wave inversion (diffuse ischemia )
- Systolic HF + signs
- exercise dyspnea
- infection signs
- sinus tachycardia
- fever
- asthenia, fatigue
- palpitations (sinus tachycardia + VEs)
- pulmonary + periph congestion signs
normal sized ventricle + ↓EF ⇒ suggestive for severe myocarditis
(or dilation + ↓contraction)
↑BNP (dilation)
↑Trop
CRP (infection)
- clinical symptoms (infection + low output + congestion)
- heart abnormalities (functional or structural) in the absence of ischemia
- nuclear MRI
- myocardial biopsy
(at least 2 positive criteria needs to be fulfilled to make positive diagnoses.)
- BB
- anti-inflammatory drugs
- corticosteroids
- if arrhythmia → consider amiodaron
- if HF → ACEi + diuretic
- Interferon + immune modulation therapy
- (L)VAD
- Heart transplant
inflammatory auto-immune disease insufficently undersotood
caused by Group A Streptococcal (GAS) pharyngitis
<25y
AB against M protein of GAS + Streptolysis O
→ M-protein = similar structure myocardium → AB against Myocarditis (endocarditis, pericarditis,) skin, joints
⇒ Aschoff nodules (granulomas) = hallmark
⇒ valvular vegetation
⇒ pancarditis: myocarditis, endocarditis, pericarditis
⇒ endocarditis dominant → scarring of valves → stenosis + regurgitation (mainly mitral + rarely aortic)
Major (JONES)
- Joints + migratory arthralgias
- O = Pancarditis (after 2-3weeks)
- Nodules (Aschoff)
- Erythema marginasum
- Sydenham chorea
Minor
- PR prolongation (I° AV-bl)
- fever
- athralgia
- acute phase reactants (ESR, CRP, Leukos)
2 Major OR 1 Major + 2 Minor
strep proof (AB or throat swab)
arthritis → infective + reactive + rheumatoi polyarthritis,
carditis → previous valvular heart diseass, mitral prolapse, congenital heart disease
chorea → epilepsy + other neurologcal disorders
1-3 weeks
- mitral (+aortic regurgitation) → (new onset) regurgitation murmor
- myocarditis → dyspnea
- pericarditis → precordial pain
- rhythm disorders → palpitations
- ↓intensity S1
- Sinus tachycardia
- 1° AV-block ( minor criteria)
- Inflammatory markers:
- CRP
- ESR
- Fibrinogen
- throat culture + antistreptolysin O
untreated → sequelae → infective endocarditis + valvular stenosis
oral penicillin within the 10 days
- anti-inflammatory drugs
- for -caridits
- steroids (<1mg/kg/day)
- aspirin/NSAIDs for pericaditis
- for arthritis
- aspirin (100mg/kg/day)
- symptom control → stop treatment for 1-2 weeks then continue 2-3 weeks (half doses)
- steroids can also be considered (<1mg/kg/day)
- bed rest
- hospitalization
- if HF or mitral regurg → HF treatment (acei, diuretics, small dose BB)
- chorea → sedatives
- degenerative valvular disease (#1)
- rheumatic fever
- functional valvular cardiomyopathy (dilative)
- congenital valvular diseases
- hypertrophy (stenosis) + dilation (V overload)
- diastolic + systolic HF
- thrombosis
- infective endocarditis
- rhythm disorder (esp. Afib + VEs)
effort
- Time of onset (congetial = early; young =rheumatic; old = degenerative)
- history of rheumatic fever (strep throat)
- + cardiomegaly → cardiomyopathy
Echo → confirm, severity, hemodynamic, treatment planing
- EKG
- Chest Xray → enlargered heart chamber + cardiothoracic index → pulmonary congestion + HT
- Coronarography in all patient >40(m)/50(f) if surgical correction is indicated → screening for ischemic cardiopathy (→ bypass if posiitive)
- Exercise stress → NYHA class → prognosis + treatment monitoring
→ atrial + ventricular hypertrophy → arrhythmias → ischemic cardiopathy
infective endocarditis prophylaxis
- 🥇degenerative: calcification of aortic valve (esp . bicuspid valve)
- rheumatic (usually with aortic regurgitation + mitral stenosis) → commissural fusion (+/- calcification)
- congenital (bicuspid → might become calcified)
LVH → diastolic dysfunction → LV diastolic failure (pulmonary congestion + ↓effort capcity)
→ systolic dysfunction if stenosis progresses → cerebral ischemia + effort angina (esp. during exercise)
- systolic murmor + systolic ejection click
Crescendo-decrescendo systolic murmur with soft S2
weak pulse with delayed peak (parvus et tardus)

- ↓effort capacity
- tachycardia during effort
- ↓BP proportional to stenosis
- only slight ↑ in effort test
- ac. LVF (dias)
- pulmonary edema
- later systolic dysfunction
- pulus parvus et tardus (diminished + ↑slowly) → in aortic stenosis
- S4 (hypertrophy)
- LVH
- Left Atrial hypertrophy
Hypertrophy + pulmonary congestion
- Left ventricular hypertrophy + ↑wall thickness
- normal size
- ↑/n contractility
- surface area <1,5cm2 +/- calcification
- transvalvular gradient + aortic velocity
- Diastolic dysfunction in severe stenosis
>10mmhg (transvalvular gradient)
(if >20 = regurgitation)
velocity >4m/s + gradient ≥40mmHg
OR
surface area <0.5cm2
⇒ severe

rheumatic fever
...congenital... degenerative...
- Ø🏋🏼♀️ Sudden strenuous exercise
- 💊drugs
- symptomatic
- Nitro patches + Diuretics
- BB
- ACEi
- rheumatic → AB prophylaxis
- ⏩ ↑ symptomatic/↑severity on echo
- 🔪 surgical valve replacement
- 🖍️ interventional valve replacement (comorbidities)
- transcatheter aortic valve replacement/implantation (TAVR aka TAVI)
- balloon dilation - for short-term bridging



often associated with aortic stenosis (enlarged degenerative aorta +- aneurysm)
- Degenerative (valve ring fibrosis + dilated and rigid aorta)
- Functional aortic regurgitation (dilated ring or proloapse cusps)
- Rheumatic (fuse + retract; with aortic stenosis)
HT, Marfan, syphillis, ankylosis spondylitits,
⇒ early: ↓DIASTOLIC ARTERIAL PRESSURE + Volume overload with later systolic HF
Volume overload → enlarged left ventricle + hypercontractility (+/- hypertrophy (eccentric))
→ high systolic flow /normal output
→ ↓diastolic arterial pressure (due to backflow) → ↓coronary flow → effort angina
→ left ventricular systolic dysfunction → (exhaustion) ↓output → tachycardia + hyperkinesia
- diastolic murmur
- ↓effort capacity
- ↓diastolic BP
- effort angina
- acute LVF (syst)
- syncope + ↓BP(dias)
- tachycardia
- pulsus celer et altus (high arterial pulsation - wide pulse pressure)
<60 + <40
🦇Echo:
- ↑LV size +- Hyperkinetic heart
- Mitral Diastolic flutter

- Etiology signs
- HT
- Associated aortic stenosis → rheumatic
- ↑aortic size → degenerative + Marfan
⇒ Aortic regurgitation severity (I-IV degrees)
Pressure half time <400ms = severe aortic stenosis

→ do surgical correction!!
- EKG - LAD + atrial hypertrophy
- Chest xray → enlarged LV, dilated aorta (+- pulmonary cong)
- Stress test → NYHA
- mild - moderate → drug (esp. prevent rheumatic)
- ACEi + vasodilators (Øin severe!!)→ ↓degress of regurg
- BB small doses (if hyperkinetic)
- Diuretics → ↑exercise capacity or in diastHF
- EF <50% or severe symptomatic (diasBP <40mmHg) or PHT<400ms)→ surgical correction
- if functional secondary to aortic root dilation(marfan) → aortic root prosthesis

RARE PATHOLOGIES BECAUSE MAINLY CAUSED BY RHEUMATIC FEVER WHICH IS RARE
(congenital, mitral ring calcification→main regurg)
Diastolic (+ systolic) HF
→ LA pressure → pulmonary HT → RV systolic dysfunction
→ thrombi
→ afib
→ ↓LV output (esp. exercise output)
- esp young woman (rheumatic)
- ↓effort capacity
- congestive heart failure → signs of pulmonary + systemic cong.
- bloody sputum (during exercise + respiratory infection)
- if severe: low output during rest → ↓systolic BP ↑diastolic BP → ↓pulse pressure, tachycardia + cold extremities

- thromboembolism
- diastolic murmor with opening snap
- ↑S1 intensity
- S2 delayed (pulmonary HT)
<2 cm2 + >2 mmHg
(rule of 2 in mitral stenosis; aortic: <1,5cm2 + >10mmHg)
- Mitral valve abnormalities
- surface area <2cm2 + transmitral gradient ≥2mmHg
- calcifications of mitral valve (importance: surgical vs. interventional)
- anterior diastolic movement (in M-mode)
- enlarged LA
- thrombus (confirm with TEE)
- Signs of diastolic failure
- ↑pulmonary artery pressure
- Tricuspid regurgitation + RV hypertrophy
→ Normal LV: normal size + normal contraction
- LA hypertrophy
- RV hypertrophy
- Afib
↑LA size
pulmonary congestion + pulmonary hypertension
- Diuretics
- BB (↓HR → ↑filling time)
- Afib:
- Digitalis + BB if afib
- anticoagulation: Warfarin (→ history of thromboembolsim or afib)
Indications for surgery + interventional:
- Severe stenosis: Mitral surface are <1,5cm2 + gradient ≥10mmg
- Complications: history thromboembolism or HF
→ Ø severly calcified → interventional (balloon dilation)

→ severly calcified → valve replacement (mainly biological)

- functional → enlargement LV + 🥇systolic dysfunction (dilation)
- Cardiomyopathies (restrictive, dilative, hypertrophic)
- Ischemic → rupture papillary (+chordate tendinae)
- endocarditis: bacterial +rheumatic → perforation (or retraction)
- Degenerative → calcification mitral ring in eldery
- Idiopathic (mainly hemodynamically insignificant)
V OVERLOAD of Left ventricle (like aortic regurg)
→ enlarged LA
→ afib
→ thrombosis = rare due atrial "washing"
→ pulmonary congestion (more than aortic reg) → LV failure + pulm edema → RV failure
→ low output esp in severe (less than aortic regur)
- holosystolic murmur
- Congestion
- assoc. with LV dilation signs→ Low output + ↓exercise capacity + compensatory tachycardia
- rarely thromboembolism
- S3 (↑ventricular filling)

EKG:
- Afib
- LAD
- often absent in degenerative etiology
- LV hypertrophy (eccentric) after 5-10y of disease
Xray:
- Enlarged LA+LV (compare to mitral stenosis → only LA!! DDx)
- Enlarged pulmonary artery + pulmonary congestion
- ↑LV diameters (dilation +/- hypertrophy; +/-hypercontractily)
- if hypocontractile → functional etiology (systolic HF or dilative cardiomyopathy)
- ↑LA diameter
- Mitral valve
- color Doppler → regurgitant flow
- Posterior systolic movement (post+ ant leaflet) on M mode
- Mitral ring calcification (degenerative)
- Associate valvular leasions (bacterial endocarditis)
- Pulmonary hypertension + ↑RV size + tricuspid regurg
2.5mm beyong ring line
- reduce afterload (↓aortic regurgitations): i.e. ACEi
- congestion → diuretics + Nitrates
- BB → in hyperkinetc
measure LV dimension + LV EF
→ If systolic diameter >45mm + EF <60% → indication for surgical correction
🔪Surgical (gold standard):
- valve Reconstruction (reinsertion of chordae or special valve patches)
- valve replacement
🖍️ Interventional → function etiology + critically ill ⇒ mitral clip

rheumatic fever (often together with mitral stenosis)
2mmg
(like mitral stenosis)
- congestive signs
- afib
- low exercise capacity
- tricuspid opening snap + diastolic murmur
- S1 incr. intensity
RA Hypertrophy (or biatrial)
RA hypertrophy + normal RV !!!
enlarged RA
- Enlarged RA (normal RV)
- Inversion tricuspid E+A (A↑↑) wave or even plateau aspect of diastolic flow (severe cases or with afib)
- gradient ≥2mmgh
- Rarely atrial thrombosis (high washing)
right heart catheterization
MAINLY SYMPTOMATIC → DIURETICS
cave with BB → ↑diastole → diastolic flow & ↓inotropic
rarly surgical valve replacement / valvulotomy
- MAINLY: functional from hemodynamic overload (volume or pressure)
- pulmonary HT
- Iatrogenic: Pacemaker with RV trans-tricuspid electrode
- Degenerative: tricuspid apparatus fibrosis
- rare: bacterial endocarditis (IV drug user → S.Aureus), carcinoid syndrome, rheumatic, RV infarct
- CONGESTION
- later: ↓RV output → ↓LV output
- ↓exercise capcity
- Right sided heart failure signs → systemic congestion
- Regurgitation murmurs (systolic) → tricuspid +/- mitral
→ ↑JVP, hepatomegaly, periph. edema
- EKG → RV + RA hypertrophy
- Chest xray → right side heart enlargment , pulmonary hypertension
- enlarged RV + RA
- Regurgitant flow on color doppler (+continous+pulse)
- paradoxical movement interventricular spetum
regurgitant flow penetration + regurgitant flow surface area
UNDERLYING DISEASE!!!
treat left heart disases + pulmonary diseases!!
Right HF → diuretic + ACEi (cave: with BB)
rarely surgery: valvuloplasty/prothesis
- Mainly congenital (monocuspid valve)
- Left-right shunt → functional stenosis = normal valvular area but ↑gradient
P overload RV → diastrolic + later systolic dyfunction
→ Right heart failure → global heart failure (↓exercise capacity during childhood + syncope + chestpain during exercise)
systolic murmur (+click)
↓S2 intensity
EKG → RV hypertrophy
xray → enlarged right heart + Øpulmonary congestion! (except if caused by shunt)
- RV hypertrophy + dilation of RV
- paradoxial septal movement
- tricuspid regurgitation (secondary)
>10mmHg
(LIKE AORTiC stenosis)
gradient >40mmHg
(LIKE AORTIC STENOSIS!!)
ballon valvuloplasty
backflow
- mainly: functional due to pulmonary HT
- bacterial endocarditis

Volume overload → right sided heart failure
- underlying diseases + pulmonary HT!
- right heart failure →congestion
- diastolic murmur
- ↑S2 intensity
EKG → RV + RA hypertrophy
Xray → pulmonary hypertension + enlarged pulmonary artery , +/- right heart enlarged
- regurgitant flow
UNDERLYING DISEASE → pulmonary HT
already damaged
- Formation of nonbacterial thrombotic endocarditis (NBTE) due to damage of valve (i.e. rheumatic fever)
- Bacteremia (from mucosal trauma i.e. dental, gut, etc)
- Adherence bacteria to NBTs → increase in vegetation size
- Extension of infections to surroundings (valve ring, myocardium, etc)
- Embolization (septic/non-septic)
acute → marked toxicity + progress over days/weeks, tend to valve-destruction + metastatic infection (emboli)
subacute → mild/mod. toxicity + progress over weeks/month, Ømetastatic infection
S.aureus
S. pneumonie
Stepcocc A-G
Hemophilus influenza


- history infective endocarditis
- structural valve disease;
- mitral prolapse,
- rheumatic fever,
- aortic valve disease,
- congenital
- prosthetic heart valve
- iv drug use
- HIV, dialyiss, poor dental hygiene, pregnancy
mitral + aortic
→ drug use: tricuspid!

Fever Roth spots Osler nodes Murmur Janeway lesions Anemia Nail-bed hemorrhage Emboli
- Congestive heart failure
- Inflammatory signs + fever
- including non-specific inflammatory signs (sweat, weightloss, fatigue..)
- Hematogenous seeding of infection → splenomegaly (esp. subacute) + hypergammaglobulinuria
- Embolization (esp. left sided S.aurus)→ infection + infarction of other organs
- Antibody-complexes
- Regurgitation murmor (new onset or changing preexisitng)
- Petechia
- Splinter-hemorrhage
- Janeway lesions
- Roth spots aka oval retinal hemorrhages
local destruction → distortin/perforation of valves(regurgitation), rupture of c. tendinae, perforations/fistulas, valvular stenosis
→ glomerulonephritis → RF
→ Osler nodules
→ rheumatologic manifestations
F → usually not audible
- At least 3 blood cultures
- Inflammation markers (CRP, anemia, leukos, ESR)
- Urin-analysis (proteinuria, hematuria)
(might be culture negative if previously treated with ABs)
- Check for 🛡️CONDuCtion ABNORMALITIES ⇒ new AV-block or BBB suggests perivalvular invasion
- pericarditis? → myocardial abscess!
Do normal echo first → if complication suspected or if negative transthoracic echo → do TEE
- Vegetations (upstream side)

- Regurgitation
- complications
- New partial dehiscence of prosthetic valve
- Abscess + fistula
- pericardial effusion
- Xray → cardiomegaly, congestive heart failure, nodular infiltration
- multislice CT (abcess + pseudoaneurysm)
- MRT (cerebral consequences)
- Nuclear imaging (periph. emboli)
Major: Cultures + Echo
Minor: Clinical + Cultures not meeting major
Diagnosis for IE!
→ 2 major criteria
→ OR 1 major + 3 minor
→ OR 5minor

Native → Vanco + Genta Prosthetic → add cephalosporins (3/4gen)

susceptebility testing → give specific AB
- prosthetic valve endocarditis
- refractory congestive HF (due to severe valve dysfunction)
- complications
- large vegetations (>15mm; or >10mm+embolsim or regurgitation/stenosis)
- perivalvular extension (failed AB treatment)
- abcess
- uncontrolled infection
- fungal endocarditis + multiresistant germs
- prosthetic valve
- previous IE
- Congenital HD
⇒ esp . in Dental procedures!!!! (give Amoxi)
L-R-shunt → higher output of RV → pulmonary HT → RV dilation → R-L shunt → cyanosis + Low cardiac output (↓exercise capacity + ischemia)
→ pulmonary HT → remodeling of pulmonary artery → ↑resitance → irreversible (closue of shunt is not useful anymore)
→ Volume overload → RV failure
- central cyanosis + hypoxemia→ Eisenmenger + R-L
- ↓growth
- hypoxic spell (cerebral symptoms)
- squatting + clubbing of fingers
- Fatigue
- Decrease exercise capacity (both shunt types)
- Precordial thrill + systolic murmors (holosystolic)
- Tachycardia (V overload)
- Palpitation + arrhythmias (volume + hypox)
LVH or RVH
BBB
arrhythmias
- cardiothoracic index (↑in volume overload)
- enlarged chambers
- pulmonary hypertension
- increased pulmonary flow vs
- increased resitance type
- Boot shaped heart→ Teratology of Fallot
#most important
- shunts
- regurgitation + stenosis
- pulmonary hypertension
- Systolic + diastolic performance
- systemic + pulmonary EF
- Ratio between them → severeity
→ DDx high flow vs. resitance
- only in complex congenital heart disease (Fallot etc)
- check oxygenation in all chambers
- Hb + Hct (polycythemia)
- PaO2 + PaCO2 + SpO2 (eisenmenger)
- BNP + Nt-proBNP (hf)
- Exercise stress (capacity)
- Holter (arrhythmias)
- biopsy (myocardial in arrhythmogenic RV cardiomyopathy)
⇒ 📷
- ostium secundum (at area of f. ovale) #🥇mostcommon
- ostium primum (at mitral valve)
- sinus venousus
- coronary sinus ASD
if large → no shunt (same pressure)
if small → L-R-shunt → pulmonary flow ↑→ resitance + RV/RA dilation→ eisenmenger
- asymptomatic or late onset
- no murmur of defect ! (low gradient, unlike in VSD=high gradient)
- signs of ↑pulmonary fluid volume
- exertional dypnea
- recurr. resp. infection (fluid)
- signs of low output
- fatigue
- syncope (low output)
- palpitation (compensatory tachycardia)
- murmur of functional pulmonary stenosis (high flow)
- S2 split (fixed during inspiration)
- stroke (paradox. embolism)
- xray → cardiomegaly (dilation right chamber)
- Echo → defect, RA + RV enlargement, colored flow
- TEE in sinus venosus type
- EKG → right axis deviat, RBBB due to V overload (rSR' in V1)
all patient but esp Qp/Qs >1.5
- surgery:
- small/moderate defects → sutured
- large → patches (synthetic or autologous pericardium)
- percut. transcatheter: Umbrella
L-R shunt → ↑pulmonary flow → ↓output + LV overload → pulmon. resistance ↑→ eisenmenger
- Xray → defects, cardiomegaly, dominant pulmonary artery, pulmonary vasculature ↑
- Echo → defects, color doppler flow, calculation of Qp/Qs flow ratio →gradient accross VSD + prediction of RVF

- Angio → pressure gradient, abnormal oxygen saturation, estimation pulm. pressure+resistance
- EKG → LVH or RVH
patent ductus → shunt from aorta into pulmonary artery → pulmonary hypertension → Left side overload
no specific symptoms or signs
→ continous murmur on pulmonary area
- ECHO!!
- enlarged LA + LV
- color flow aorta + pulmonary a.
- vizualisation of ductus
- Calculate Qp-Qs ratio (is always ↑↑)
- EKG → LVH + LAH
- Xray → pulmonary HT

- interventional closure devices
- surgical lagation + cutting of ductus
→ early during life in all patients!!
T → turns into R-L shunt (↓pulmonary flow)
F → murmur from shunt diminished due to reverse of shunt
- VSD
- Overriding aorta (takes some blood from Right heart)
- subpulmonary stenosis
- →RV hypertrophy
⇒ R-L shunt → classic eisenmenger
systolic thrill
systolic murmur (pulmonary v.)
septal defect murmur
- EKG → RVH
- Xray → RVH, ↓pulmonary circulation, boot shaped heart (Coeur en sabot)
- Echo → defect, pulmonary stenosis , overriding aorta
- dacron patch. 📷
- put aorta on left side
- +/- surgical correct pulmonary stenosis
→ 📷
downward displacement tricuspid → RV↓size + RA↑Size + pulsating → tricuspid regurgitation → ↓cardiac output + exercise tolerance
- systolic murmur (tricuspid regurg.)
- central cyanosis + respirory failure esp. during exercise
- palpitations + arrhythmias
- Xray → dilated ri. atrium + ↓pulmonary circulation
- EKG → RA hypertrophy (RAH) + RBBB + WPW associated + arrhythmias
- Echo → Difference insertion mitral valve vs tricuspide ≥8mm, ↑RA, ↓RV, pulsation in RA, tricuspid regurgitations
usually symptomatic (arrhythmias, lifestlye etc.)
sometimes tricuspid prosthesis but low results
stenosis of desc. aorta → LV hypertrophy + ↑growth of upper parts of the body and ↓growth of lower parts
↑increase arm BP + ↓leg BP
- EKG → LVH
- Chest xray → enlarged LV + notching ribs
- Echo → LVH, pressure gradient measure in desc. aorta, narrowing of aorta, turbulent color flow
>10
40
angioplasty +/- stenting
less than 2 weeks
- Chest pain
- worse during inspiration + lying down
- better with sitting up + leaning forward
- Friction rub
- Fever
- differentiated from pleural rub which is modified by inspiration
- friction rub best heard when patients sits up and leans forward
- 3 phases of friction rub
- atrial systolic rub
- ventricular systolic rub
- early diastolic rub
idiopathic→ undiagnosed viral (Coxsackie A+B)

Viruses→ Coxsackie A+B, echovirus→ presents as short 1-3 self-limited weeks
Bacteria→ mainly steptococcus + gram negative → from pulm extension, hematogenous spread, abscess, endocarditis→ can lead to purulent pericarditis with poor prognosis (constrictive pericarditis also rather common)
Tuberculosis: consider in all instances with slow course (especially risk areas)→ test for acid-fast bacilli→ RIPE therapy (high mortality, still)
Others→ fungi, parasites
AUTOIMMUNE
- Rheumatic fever
- SLE
- Rheumatoid arthritis
- Scleroderma
- Sarcoidosis
- Uremia in RF → Øtypical ST-elevation → dialysis
- Hypothyroidism
- Cholesterol pericarditis
- Pericarditis directly after MI (within 24h) → Persistent pos. T-waves >48h or premature T-wave inversion → high dose Aspirin
- Dressler syndrome (2-3weeks after) → pulmonary infiltrates + large pericardial effusion → NSAIDs
- Cancer → antioncotics + AB
- Drugs
- Penicillin
- Procainamide
- hydralazin + methyldopa
- Irradiation
- Postpericardiotomy syndrome → give ass or NSAIDs
→ classic chest pain DDx
- Aortic Dissection
- Coronary Artery Vasospasm
- Esophageal Rupture
- Esophageal Spasm
- Gastritis, Acute
- Myocardial Infarction
- Peptic Ulcer Disease
- Pulmonary Embolism
- Inflammatory
- Leucocytosis
- increased ESR abd CRP
- cardiac biomarkers (DDx with myocarditis)
- blood/viral culture
- kidney + thyroid
- BUN and Crea
- thyroid markers
- tuberculin test/ acid-fast staining/ rheumatoid factor / antinuclear antibodies / anti-DNA /
Stages: 📷
Stage 1: Presents with diffuse, concave, upward-oriented ST elevation accompanied by upright T waves and depressed PR segment. Stage 2: Following stage 1, the ST segment returns to baseline, followed by flattening of the T waves. Stage 3: In this stage, inverted T waves are observed. Stage 4: ECG returns to normal in weeks to months after the acute episode. T wave inversion may persist indefinitely, especially in cases related to tuberculosis or uremia.
Electrical alternans 📷 → beat-to-beat variability of QRS voltage due to effusion
- MI: early repolarisation→ no progression through stages and uncommonly associated with PR depression
- Ømirror/reciprocal changes (only in MI Øin pericarditis(except aVR))
- ST segment in pericarditis is concave
- ST segment elevation/ T wave ratio >1/4 in V6
maybe enlarged cardiac silhouette (”leather bottle”) 📷 → if pericardial effusion
→ 📷
- echo free space→effusion
- clots/ fibrin inside
- hyperechoic and thickened Pericardium
- #1 🧯NSAIDs (i.e. indomethacin 300-800mg/day) OR Aspirin #2 add Colchicine🌱 #3 🌝Glucocorticoids
- if autoimmune→ #1 Glucocorticoids 60mg/day
rate (speed) of accumulation of fluid
→ Rapid accumulation of pericardial fluid may cause elevated intrapericardial pressures even with small amounts of fluid, while slow accumulation of fluids (even up to 2 l) may not elicit symptoms.
acute and chronic
- Chest pain
- BECKS TRIAD (if tamponade)
- Low output → syncope, palpitation (↑HR)
- Tachycardia + Tachypnea
- weakend periph. puls + pulsus paradoxus (↓BP >10mmgh on insipration)
- cyanosis
- Congestion → dyspnea + cough
- hepatojugular reflux + hepatosplenomegaly
- ↓breath sounds (pulmonary edema)
- edema

→ see acute pericarditis
- pericardial tamponade
- suspected purulent effusion,
- recurrent effusions
- large effusions that do not resolve with treatment (refractory + large)
💉pericardiocentesis
(underlying disease Tx)
accumulation of fluid in percardium → ↓ventricular filling + ↓output (aka hemodynamic compromise)
- increased stifness of ventricle→ needs higher filling pressure (ventricle filling pressure > pericardial pressure)
- pericardial pressure > ventricular filling pressure →↓ output
- pericardial pressure = LV filling pressures→ further ↓output
rapid accumulation (even with small volume) → marked ↑ in pericardial pressure
slow accumulation (event with large volume) → adaptive stretching over time → ↓increase in pericardial pressure
- BECKS TRIAD (congestion, low output, muffled sounds)
- Pulsus paradoxus (fall of BP ≥10mmHg with inspiration)

- tachycardia (compensatory)
see acute pericarditis
PLUS anticoagulation
pleural effusion → fluid might travel into pericardium
- swinging of the heart in sac
- LV pseudohypertrophy (shift septum to the right)
- early diastolic collapse RV (free wall)
- late diastolic collapse RA
cardiomegaly→ water-bottled shaped heart 📷
- sinus tachycardia
- low-voltage QRS
- Electrical alternans 📷
- PR depression
—> suggestive but not diagnostic
compression coronary sinus (early)
- removal of pericardial fluid (💉pericardiocentesis)
- Medication→ positive 🔼 inotropes (Dobutamine) and adequate 💦volume expansion
- underlying disease Tx
- if hemodynamically unstable→ 🔪surgery
→pericardiectomy, pericardial window, slerosing of pericardium, creation of a pericardio-peritoneal shunt,
constrictive pericarditis with thickened fibrotic pericardium (due to scarring after acute pericarditis) → late ventricular filling problem
- restrictive cardiomyopathy
- diseases with ↑RV pressure
⇒ DDx via Echo, CT, MRT, invasive hemodynamic measurement
all of them;
most frequent→ viral, post-surgery and postradiation
SIGNS OF ↓Output + congestion + muffled sounds
- most commonly→ Dyspnae, Fatigue and Orthopnea
- congestion→ nausea, vomiting , GI pain (if liver and bowels are affected)
- CV findings:?
- elevated jugular venous pressure
- sinus tachycardia
- impalpable apical impulse
- distant/ muffled heart sounds
- pericardial knock
- Kussmaul sign
- peripheral edema


- early → might be absent
- late → muscle wasting, cachexia, signs of congestion (hepatomegaly + ascitis, jugular distension, pleural effusion)
- restrictive Cardiomyopathy→ exclude via history + CT/MRI/Echo
- congestive HF→ Echo
- RIght sided valvulopathies→ Echo
→ Echo but findings are non-pathognomic
- echodense pericardium
- ↑early rapid diastolic filling (E over A), mitral shows an opposite pattern to tricuspid
- signs of congestion dilated VC + liver veins
- tissue doppler→ to exclude restrictive Cardiomyopathy (myocardium only moves minimally in restrictive, in constrictive = normal)
- interventricular septal paradoxial movement
- atrial septal shifting to the left with inspiration→ pressure overload
- Lab → i.e. liver markers, BNP, inflammatory markers
- Xray → normal, evtl. pericardial calcifications + dilated IVC
- EKG → normal, evtl. persitent. inverted T from acute pericarditis + afib
- CT + MRI → thickness >3-4mm; calcifications, signs of congestions (dilated: VC, hepatic vein, RA)
- Right heart catheterization → ↑diastolic pressure + ↓systolic pressure
surgical pericardectomy
- Diuretics→ in early stages (improve congestion)→ CAVE low C-output
- Afib → Øno BB+CCB!! (comp. tachycardia)→ Amiodaron(?)
- underlying disease TB?→ RIPE-Therapy

Aortic Dissection (AoD) is a condition where the layers of the aorta separate due to a tear in the aortic intima. 📷 This tear exposes the diseased medial layer to the force of blood pressure, causing it to penetrate and cleave the aortic wall, creating a false lumen. 📷
Alternatively, AoD can begin with the rupture of vaso-vasorum, leading to the development of an intramural hematoma and subsequent intimal tear.
→. 📷
Type | Description | Recommended Treatment |
Type I | Dissection starts in the ascending aorta and propagates distally to include at least the aortic arch and typically the descending aorta | Surgery |
Type II | Dissection starts in and is confined to the ascending aorta | Surgery |
Type III | Dissection starts in the descending aorta and propagates most often distally | Nonsurgical treatment |
Type IIIa | Dissection is limited to the descending thoracic aorta | Nonsurgical treatment |
Type IIIb | Dissection extends below the diaphragm | Nonsurgical treatment |
→ 📷
The Stanford classification divides dissections into two categories based on the involvement of the ascending aorta:
Type A: Dissections that involve the ascending aorta, regardless of the site of origin. Surgical treatment is usually recommended for type A dissections.
Type B: Dissections that do not involve ascending aorta. Nonsurgical treatment is usually recommended for type B dissections.
acute <14 days
subacute 15-90 days
chronic >90 days
↑ aortic wall stress:
- Hypertension, particularly if uncontrolled
- Pheochromocytoma
- Cocaine or other stimulant use
- Weight lifting or other Valsava maneuver
- Trauma (e.g. fall, motor vehicle crash)
- Deceleration or torsional injury
- Coarctation of the aorta
aortic media abnormalities:
- Genetic: Ehlers-Danlos syndrome, Marfan syndrome (vascular form), bicuspid aortic valve, Turner syndrome
- Inflammatory vasculitis: Takayasu arteritis, giant cell arteritis
- Other: pregnancy, polycystic kidney disease
- Chest PAIN
- SUDDEN & severe onset
- TEARING (sharp, stabbing) character
- RADIATES → back
- pain located at site of rupture
- HTN + ASSSYMMETRIC BP + pulses
- ISCHEMIC syndrome (i.e. MI, stroke, renal, leg)
- RUPTURE → pleura (hemoptysis, dyspnea), peritoneum (shock), pericardium (tamponade)
- SYNCOPE
TEE (Øabdominal)→ intima flap + false lumen 📷
other: regurg + percardial effusion

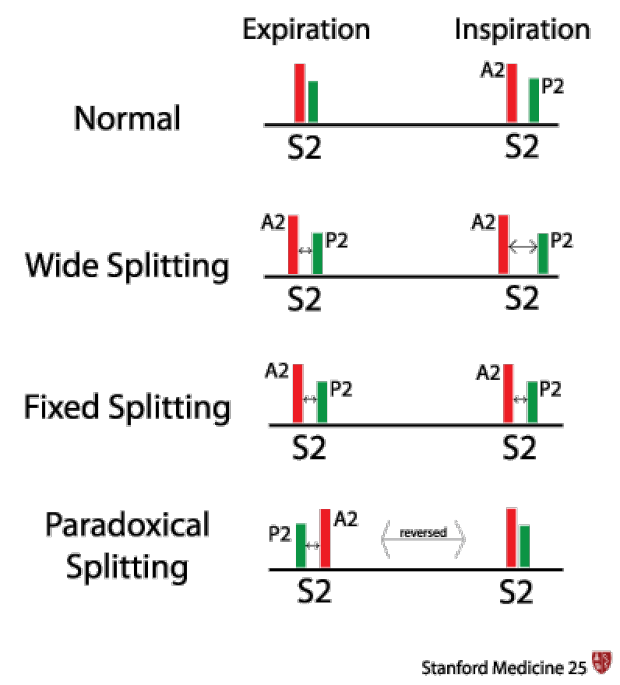{kind=link}
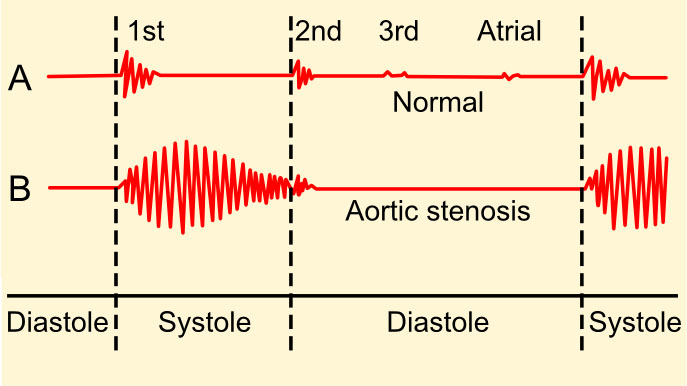{kind=link}
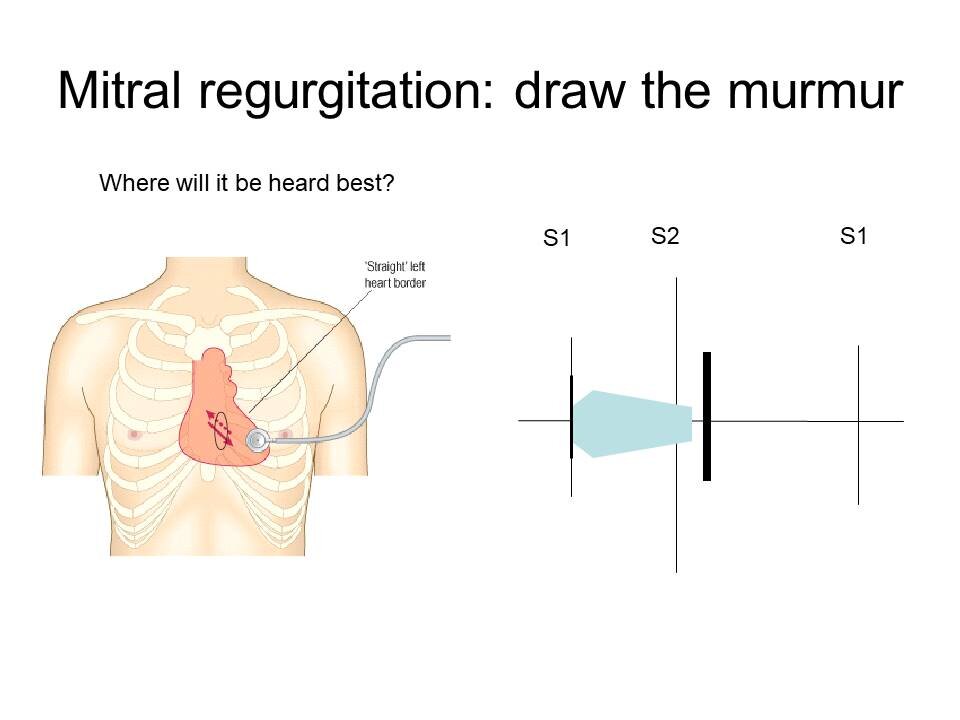{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
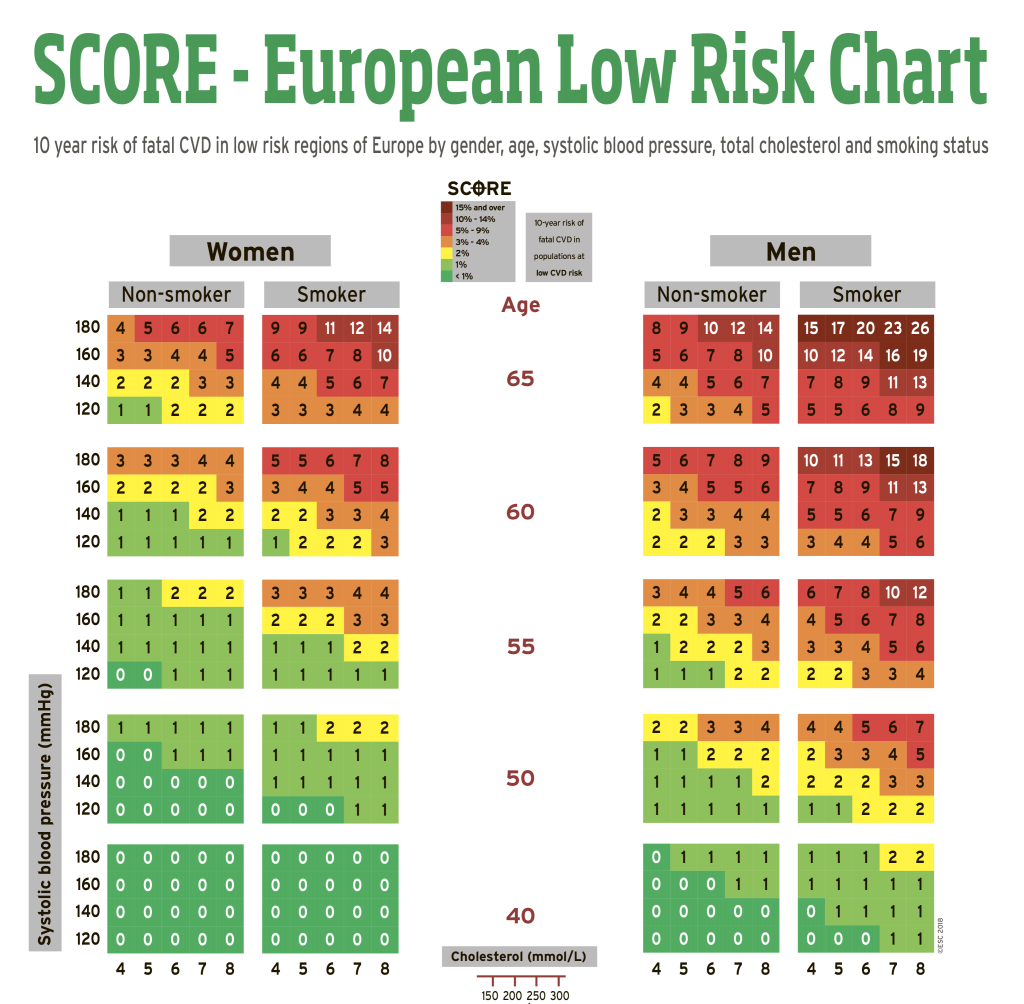{kind=link}
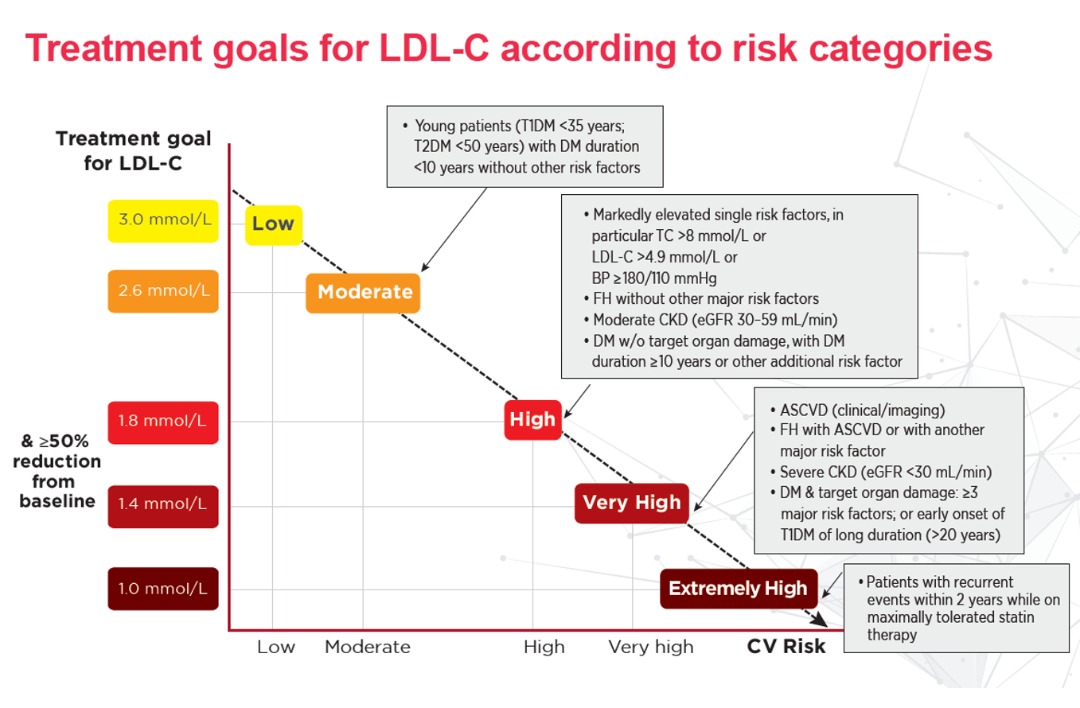{kind=link}
{kind=link}
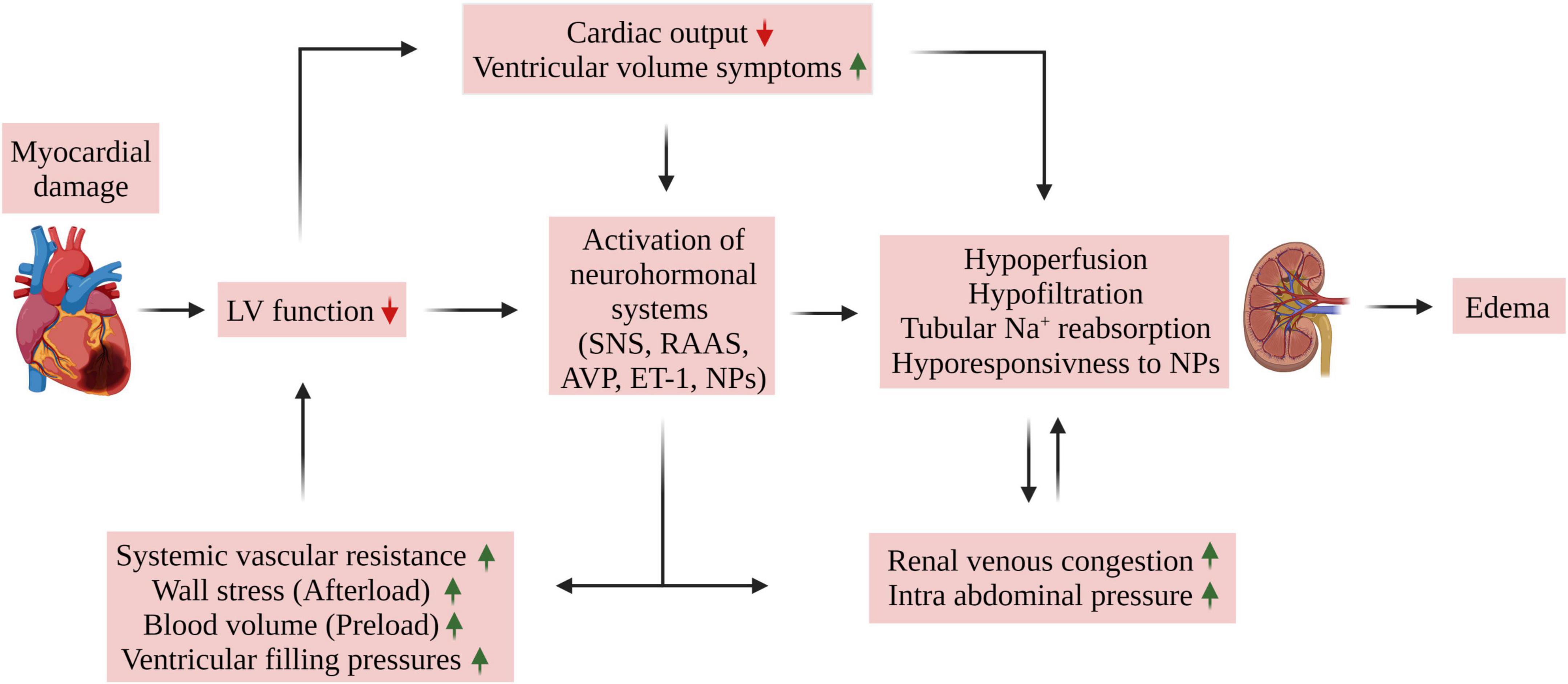{kind=link}
{kind=link}
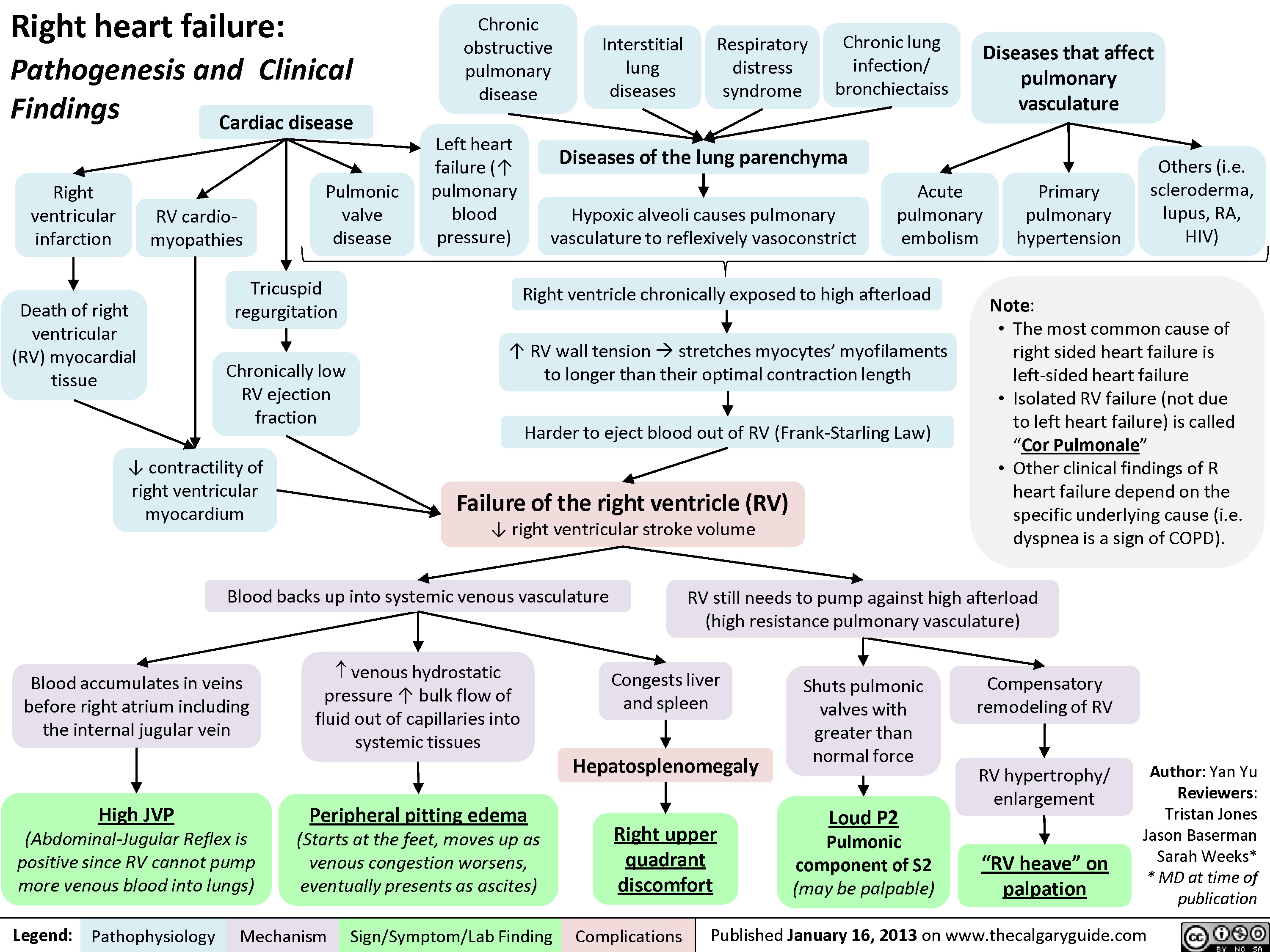{kind=link}
{kind=link}
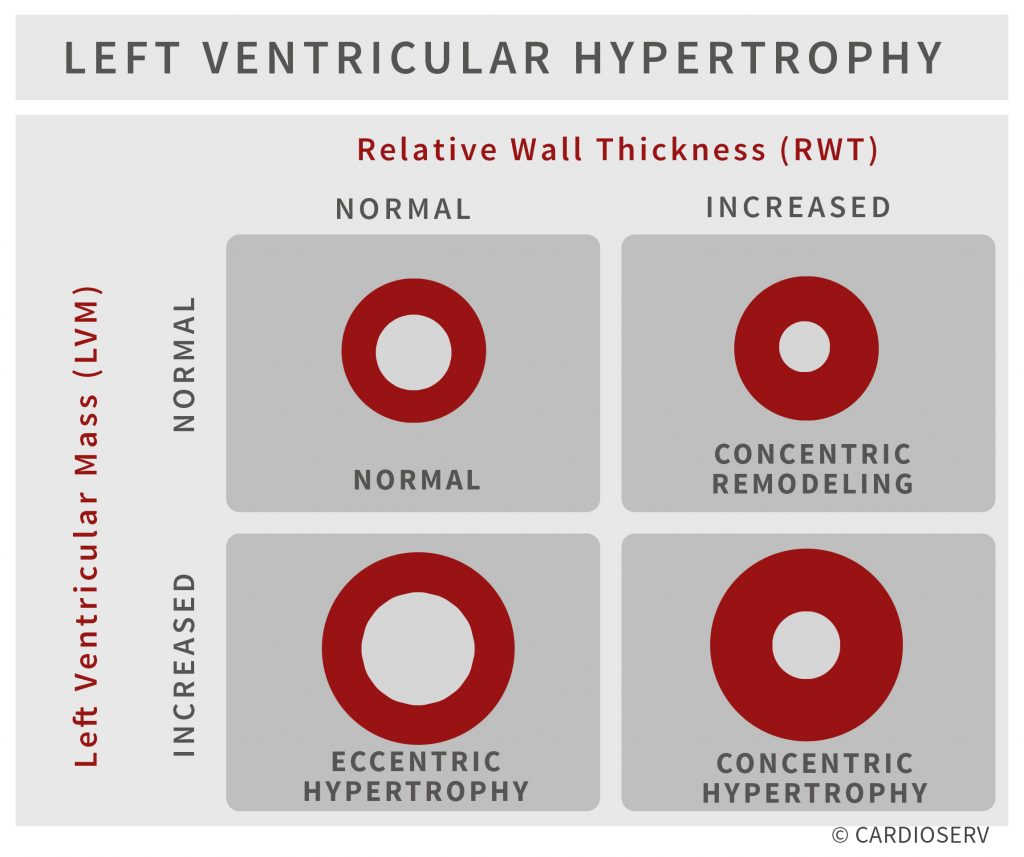{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
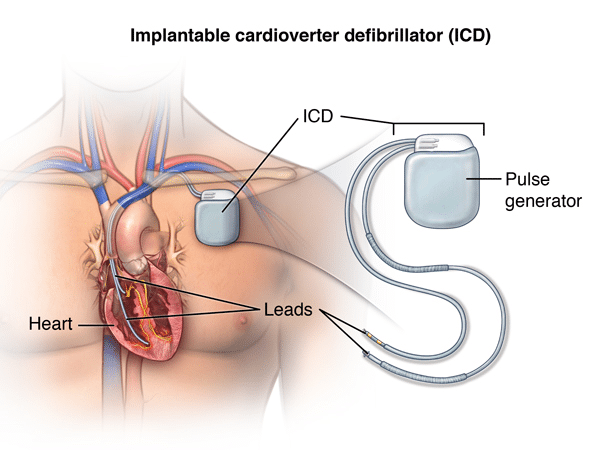{kind=link}
{kind=link}
{kind=link}
{kind=link}
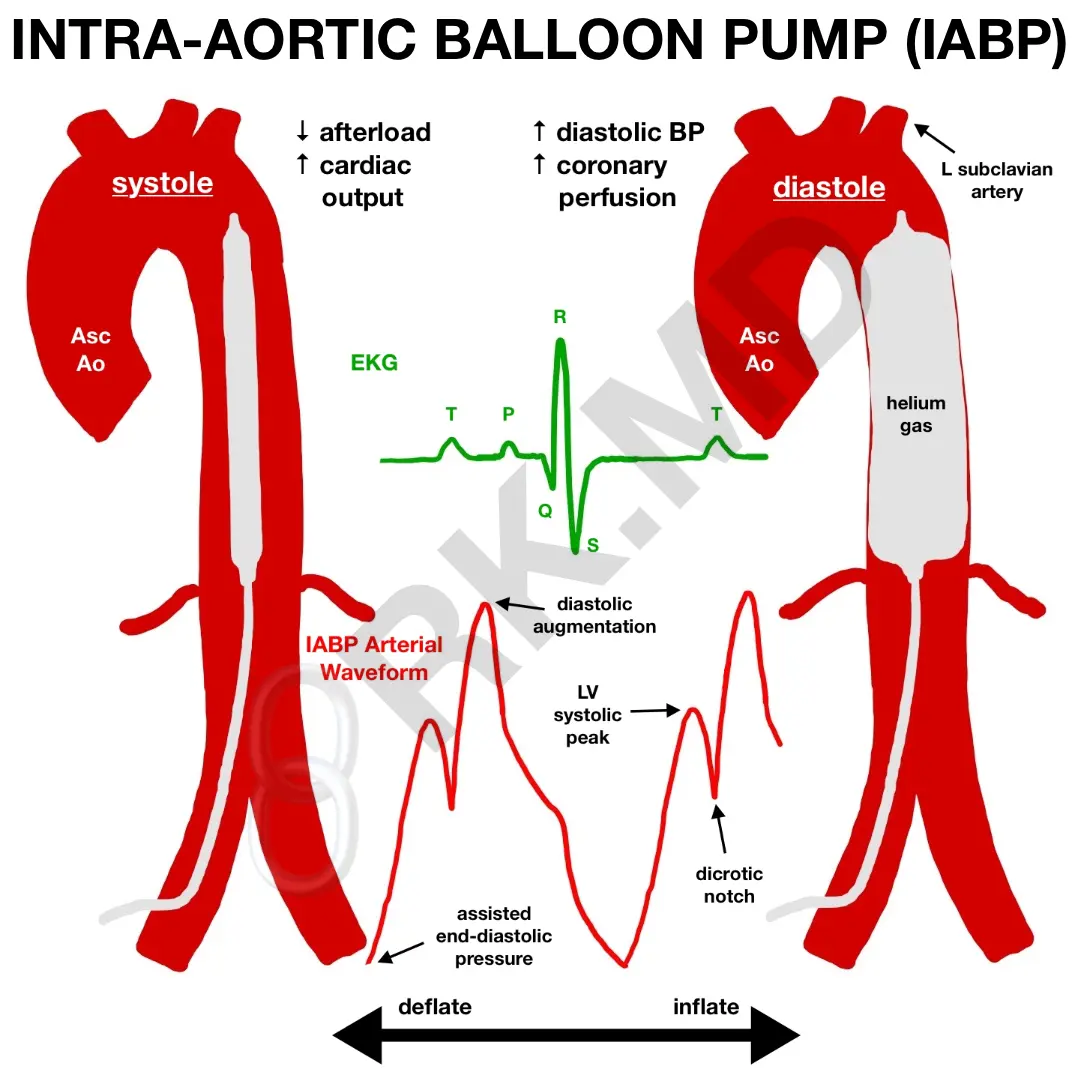{kind=link}
{kind=link}
{kind=link}
{kind=link}
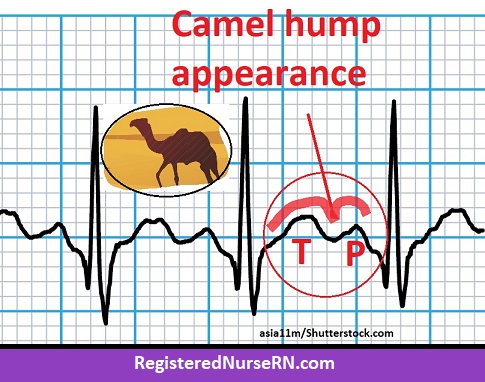{kind=link}
{kind=link}
{kind=link}
{kind=link}
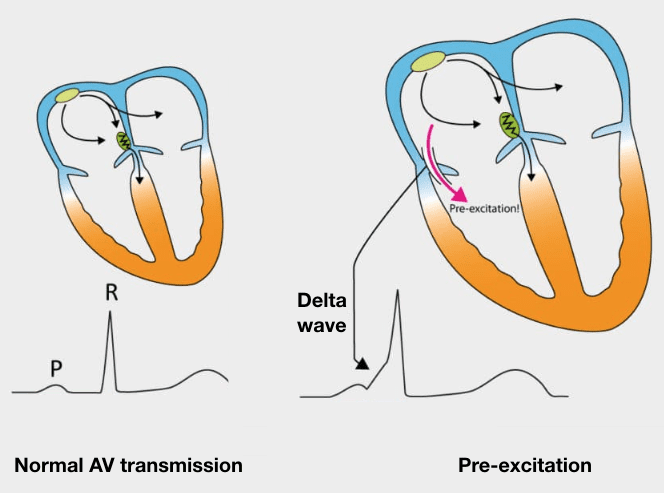{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
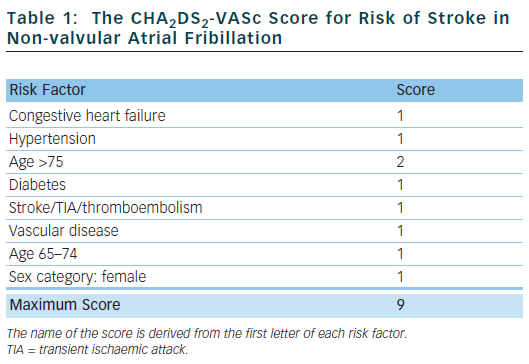{kind=link}
{kind=link}
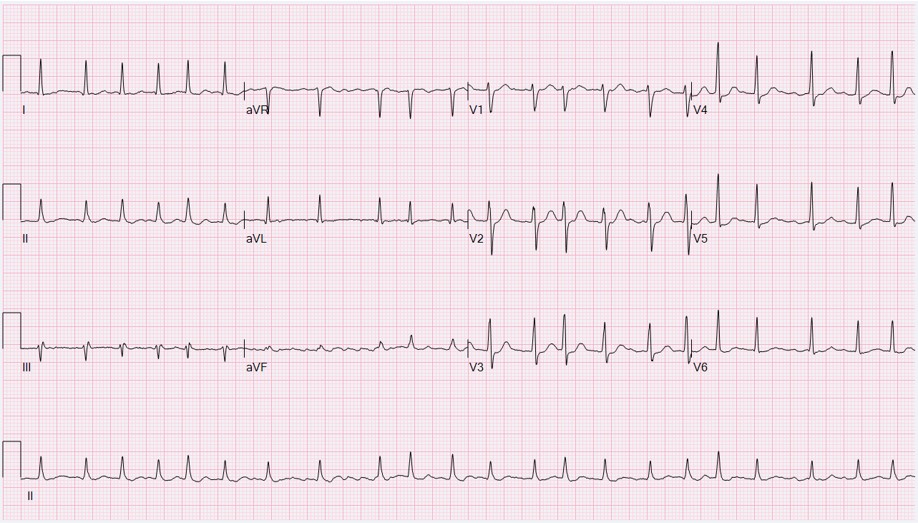{kind=link}
{kind=link}
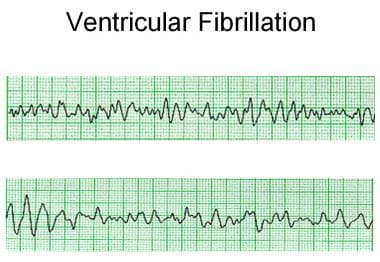{kind=link}
{kind=link}
{kind=link}
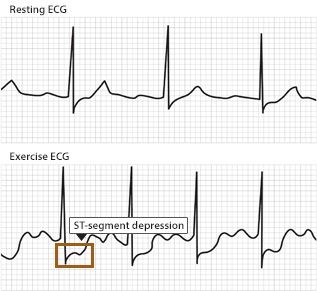{kind=link}
{kind=link}
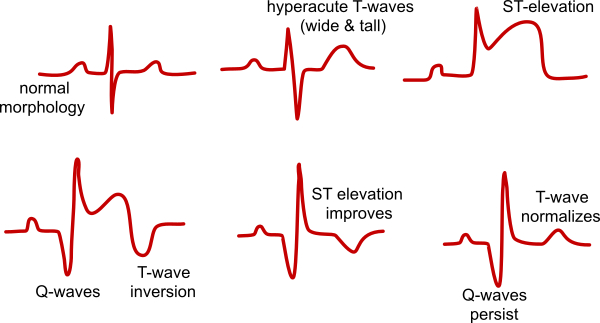{kind=link}
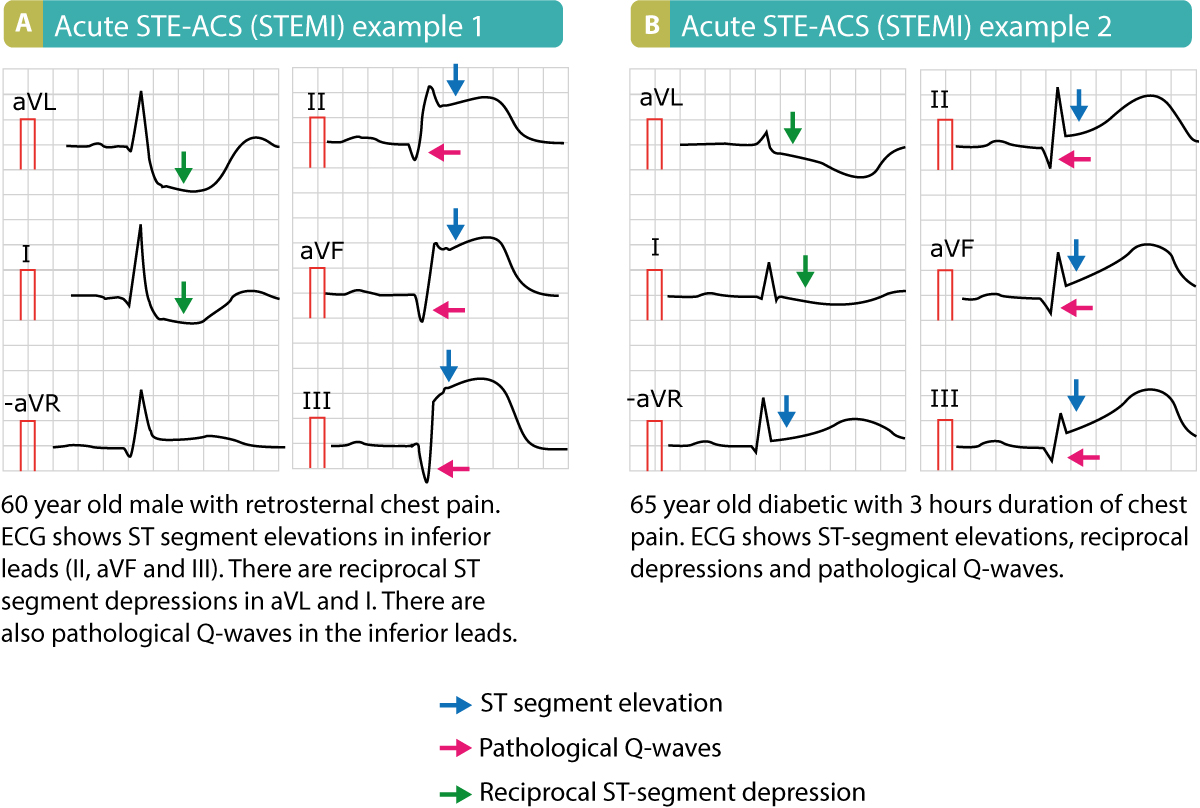{kind=link}
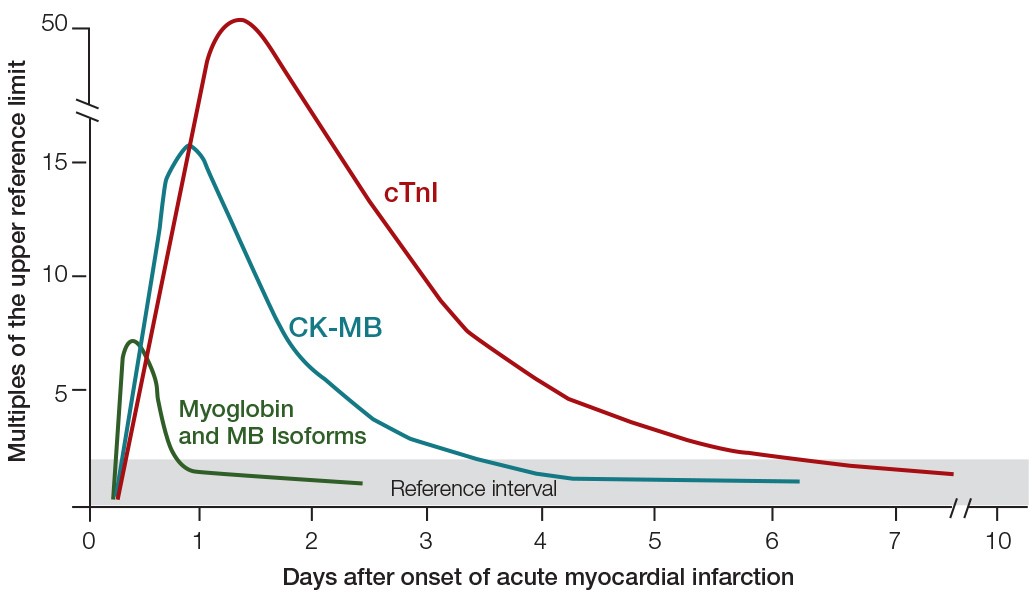{kind=link}
{kind=link}
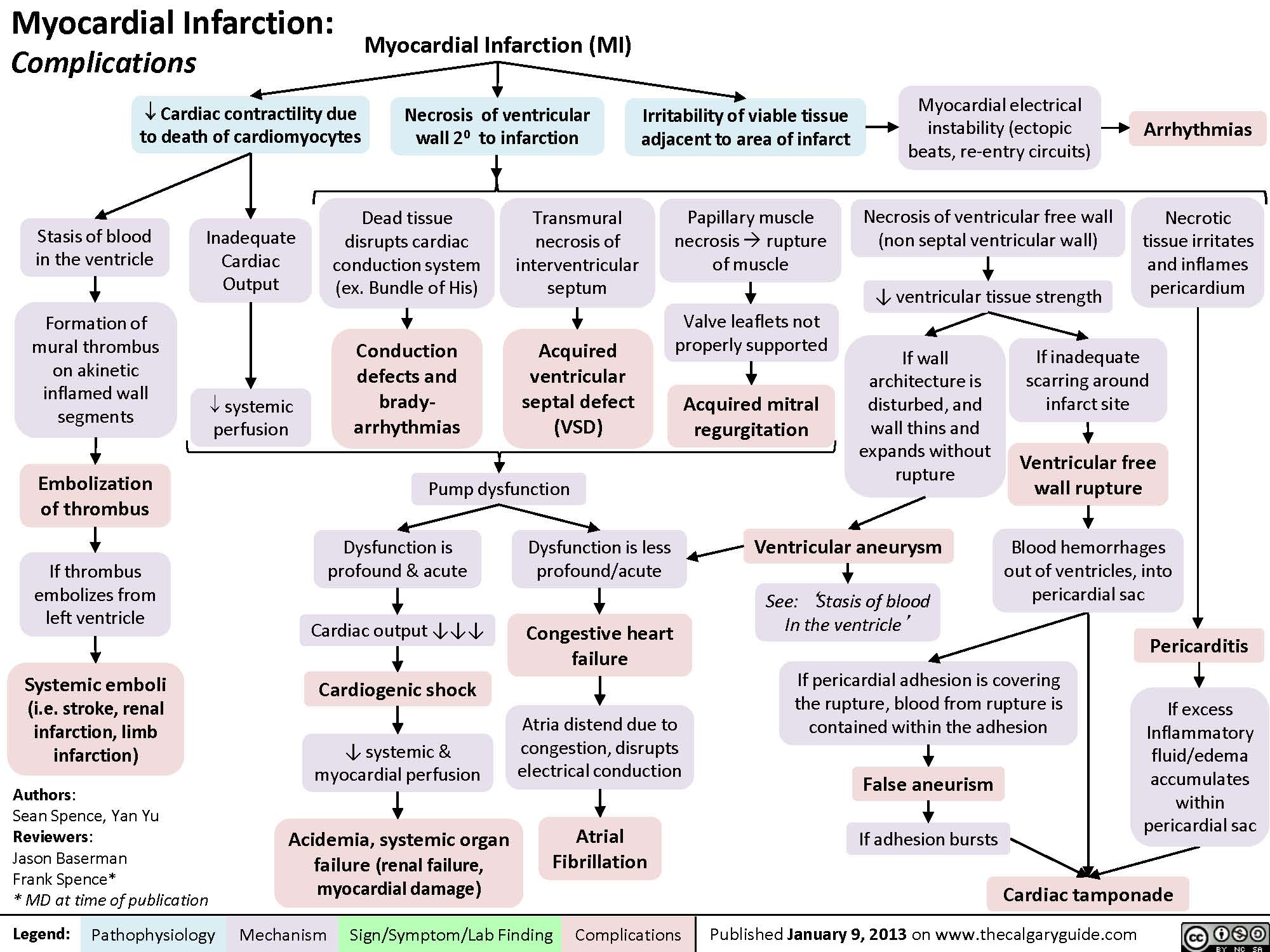{kind=link}
{kind=link}
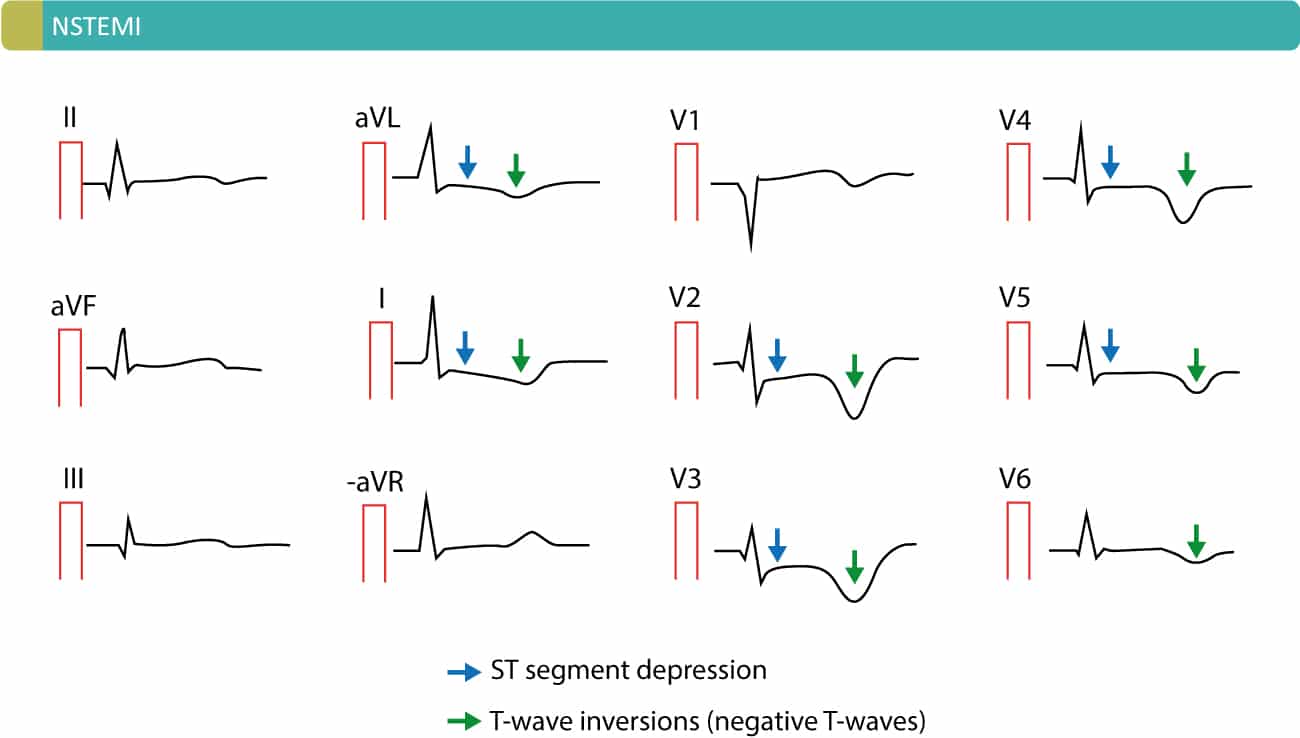{kind=link}
{kind=link}
{kind=link}
{kind=link}
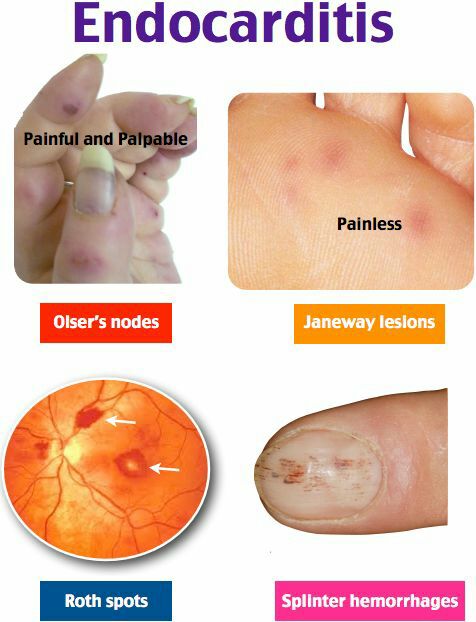{kind=link}
{kind=link}
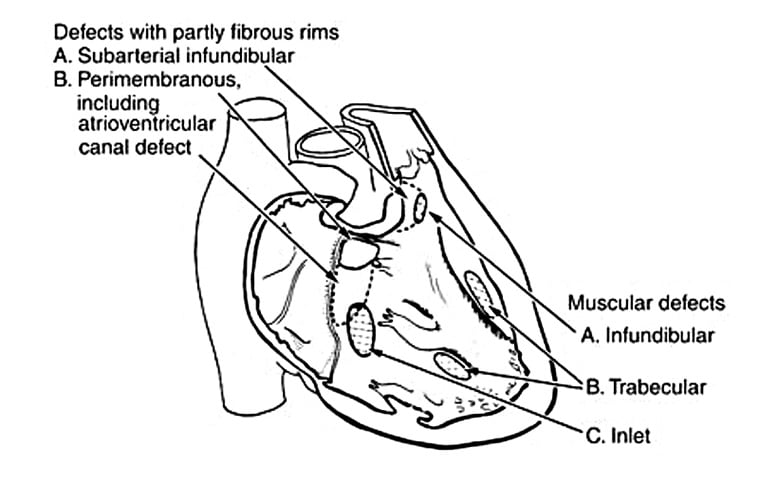{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
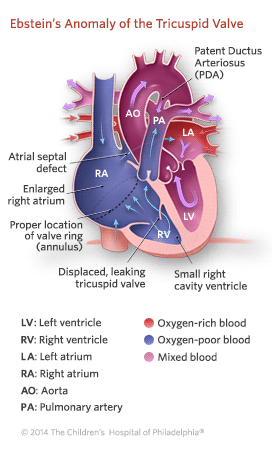{kind=link}
{kind=link}
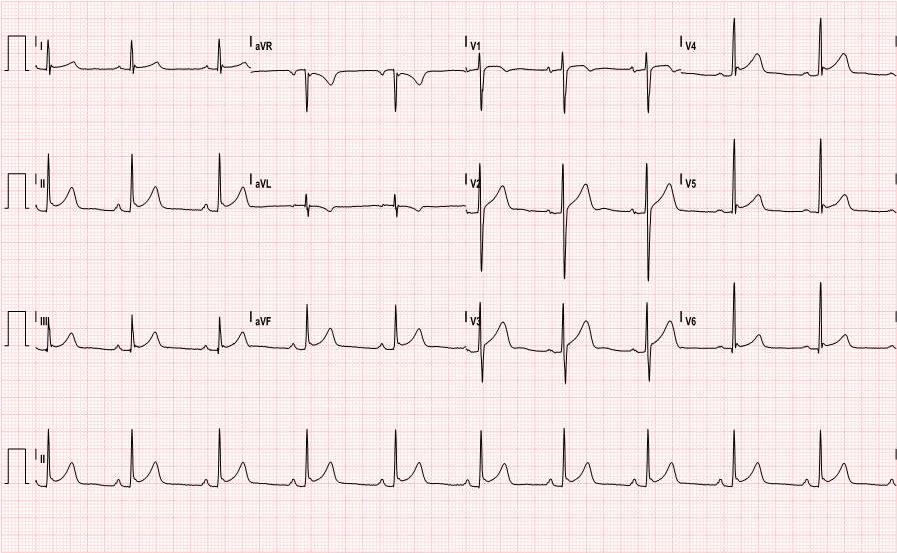{kind=link}
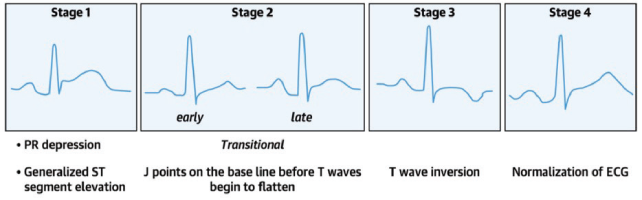{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
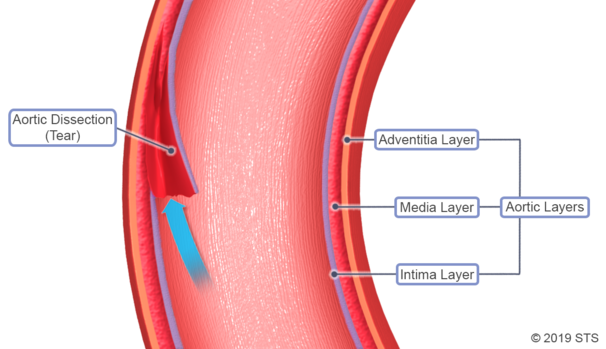{kind=link}
{kind=link}
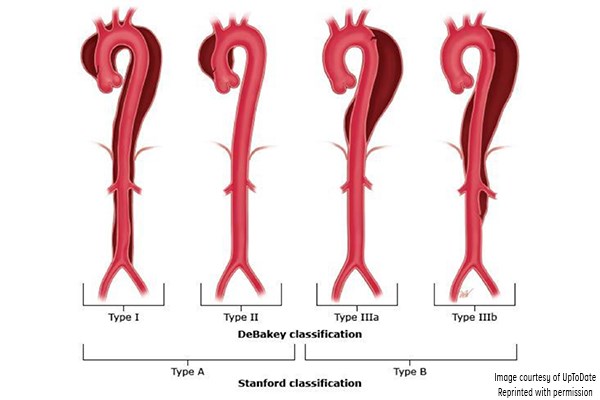{kind=link}
{kind=link}
{kind=link}
- Output + BP (+afterload if refract)
- Morphine
- if hypotensive → NE + volume expansion
#1 🎺BB (alternative: 🍦NDHP CCB)
→ if refractory → 💠ACEi or other vasodil.
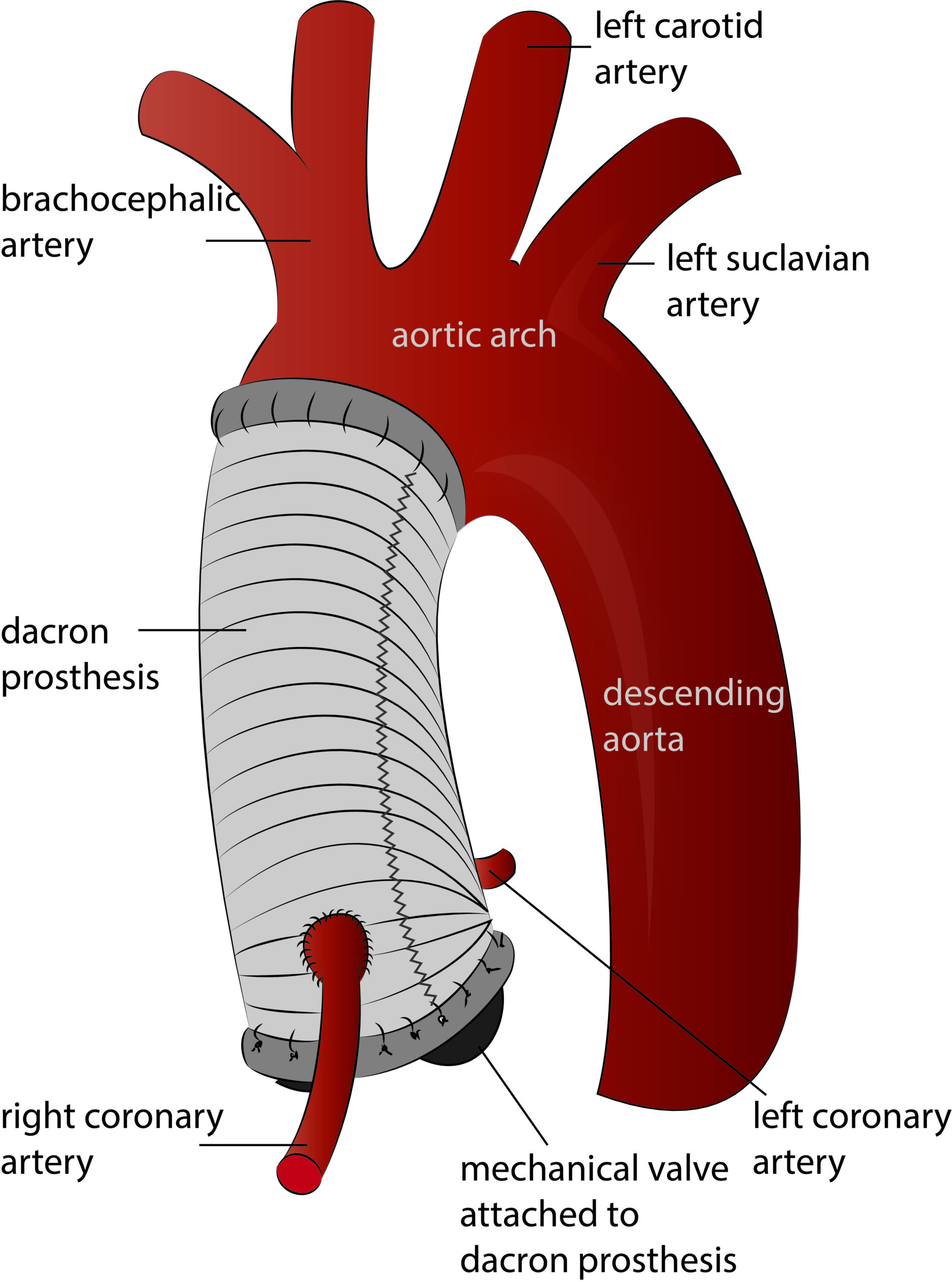{kind=link}
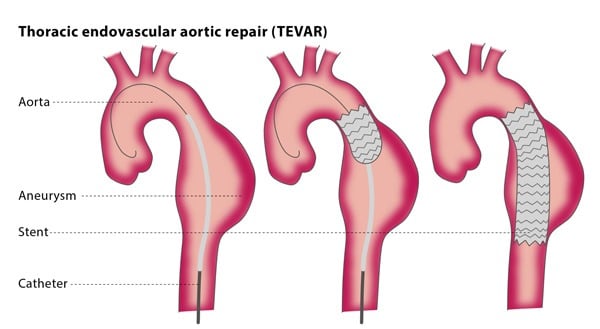{kind=link}
intramedial hemorrhage caused by vasa vasorum rupture (no evidence of communication with aortic lumen)
→ resolving of the Hematoma
→ conversion to classical dissection
→ rupture of the aorta
CT, MRI + TEE → thickened aortic wall 📷 + Ø flow within hematoma
{kind=link}
Type A → surgery
Type B → First BB → then TEVAR (or surgery)
→ 📷
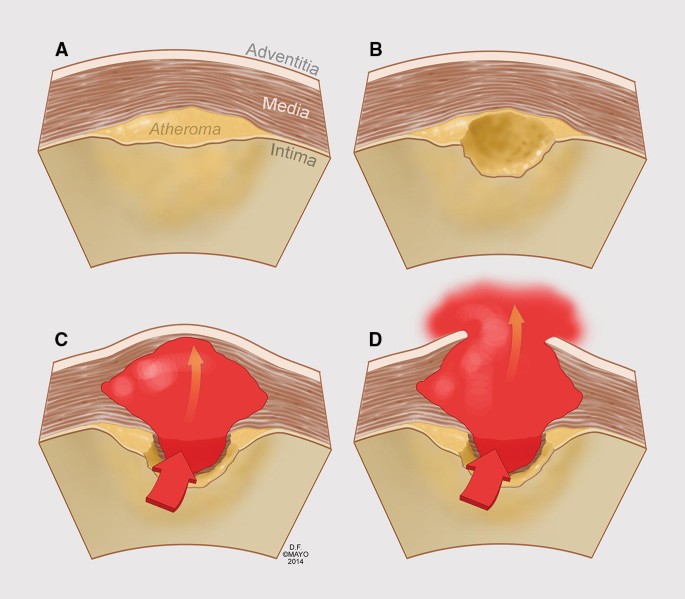{kind=link}
ulceration of an atherosclerotic plaque which penetrates internal elastic lamina → hematoma formation within media → rupture
(no formation of a false lumen)
dilated descending aorta+ left-sided or bilateral pleural effusions
aortography → contrast-filled pouch
(Øflap or false lumen)
prevent aortic rupture
progression to acute AoD
- recurrent + refractory pain
- Signs of soon rupture
- rapid growing ulcer
- periaortic hematoma
- pleural effusion
Type A → surgery
Type B → BB → then TEVAR or surgery
degenerative disease resulting in dilatation of aorta
- 50% assymptomatic
- Aortic valve regurgitation → HF
- compressive symptoms
- horseness
- stridor
- dyspnea
- dysphagia
- edema + red face
→ 📷
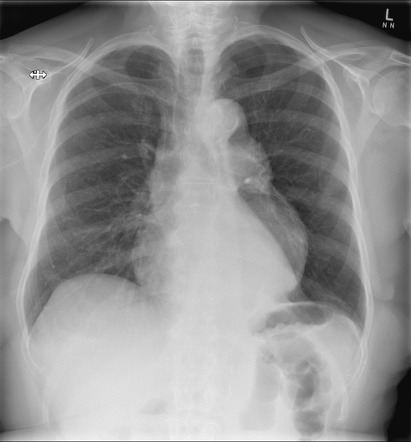{kind=link}
- enlarged aortic knob
- widening of mediastinal silhouette
- displacement of trachea from midline
the aortic root
- CT/MRI
- (Aortography- not longer used)
- aneurysm asc. aorta >5.5cm
- Marfan already at >5.0
- small aneurysm with:
- rapid expansion rate
- significant aortic regurgitation
- compressive symptoms
Descending thoracic aorta >5,5cm
- smoking cessation (🚬)
- lifestyle→ nutrition 🥗
- Anti-Hypertensive Tx→ BBs, ACEi/ARBs
- decrease CV-risk factors
- lipid profile optimization
T (much more common)
antero-posterior diameter >3 cm
ARTEROSCLEROSIS → inflammation aortic wall → degradation extracellular matrix
- Age is an important risk factor for abdominal aortic aneurysms (AAA), with the incidence rising rapidly after 55 years of age in men and 70 years of age in women.
- Smoking is also associated with the risk of AAA, with the duration of smoking being a contributing factor.
- Male gender, hypertension, and hyperlipidemia are other factors that have been linked to the development of AAA.
- Atherosclerosis is widely considered to be the underlying cause of abdominal aortic aneurysms, with the infrarenal abdominal aorta being the most commonly affected area.
T→ becomes symptomatic with herald expansion and impending rupture
{kind=link}
{kind=link}
- US
- CT / MRI
- aortography
size + time
F → mainly not indicated
⇒ only if >5.5cm (for woman >4.5)

BBs
- #1 Arterosclerosis
- thrombosis + embolism
- vasculitis
- aortic coarctation
- diabetes mellitus 🍬
- smoking 🚬
- hypertension 🤯
- dyslipidemia 🧈
→ rest pain and intermittent claudication, the location relates to the site of the most proximal stenosis
walking distance, speed, and incline that precipitate claudication
- ↓ or absent pulse → location of stenosis
- bruits
- muscle atrophy
- chronic low-grade ischemia sign 📷
- hair loss
- thickened + brittle nail
- smooth + shiny skin
- subcutaneous fat atrophy of digital pad
- Ankle/Brachial Index→ cut-off <0,9 (<0,4 = severe)
- Treadmill exercise testing→ provides objective evidence of claudication
- Vascular ultrasound imaging→ plaque, colour flow disturbance
- Contrast angiography
- MRI/ CT
- Segmental pressure measurement 📷 → 20mmHg upper, 10mmHg lower extremity
2 fold
3 fold
- Risk factor lowering
- LDL <70
- smoking cessation
- HbA1c <6,5
- BP <140/90
- Antiplatelet therapy
- PDE3-inhibitors: Cilostazol (not in HF)
- Exercise rehabilitation programm
- Interventional/ surgery
- angioplasty + stent
- Surgery → bypass
occurs most frequently when 2 or more levels of the distal arterial tree are compromised by hemodynamically significant stenosis or occlusion
rest pain in forefoot + toes
ischemic ulcers + gangrene
- percutaneous interventions
- surgery (even amputation)
- Pain
- Pulseless
- Pallor
- Paresthesias
- Paralysis
when an arterial occlusion suddenly reduces blood flow to the arm or leg
- Ultrasound doppler
- MRT, CT, Arteriography → site of occlusion
- Analgesics→pain reduction
- Heparin (directly after diagnosis is made)
- Revascularisation therapy
- Percutaneous mechanical thrombectomy
- intraarterial thrombolytic therapy
- surgical revascularisation
! - indicated if viability of limb is threatened or when symptoms of ischemia persist
segmental vasculitis that affects distal arteries, veins and nerves
- rest pain
- digital ulceration
young persons who smoke
other autoimmune diseases (i.e. lupus)
- smoking cessation
- prostacyclin (Iloprost)
- Sympathectomy to decrease arterial spasm
idiopathic large vessel vasulitis in esp. young women affecting the aorta and its major branches
Signs:
- bruits
- high BP
- pulse asymmetries
Symptoms:
- Claudication
- active disease:
- visceral ischemia
- malaise myalgias arthalgias
- night sweats + fever
- Aneurysm aortic root
- renal artery stenosis
- cardiac + CNS vascular diseases
- aortic regurgitation
- high dose predni
- add on: Cyclophosphamide or Methotrexate (MTX)
- hypercoagulability
- stasis
- endothelial dysfunction
→ simply speaking: reduced blood flow → activation of coagulation + some endothelial defect
📷
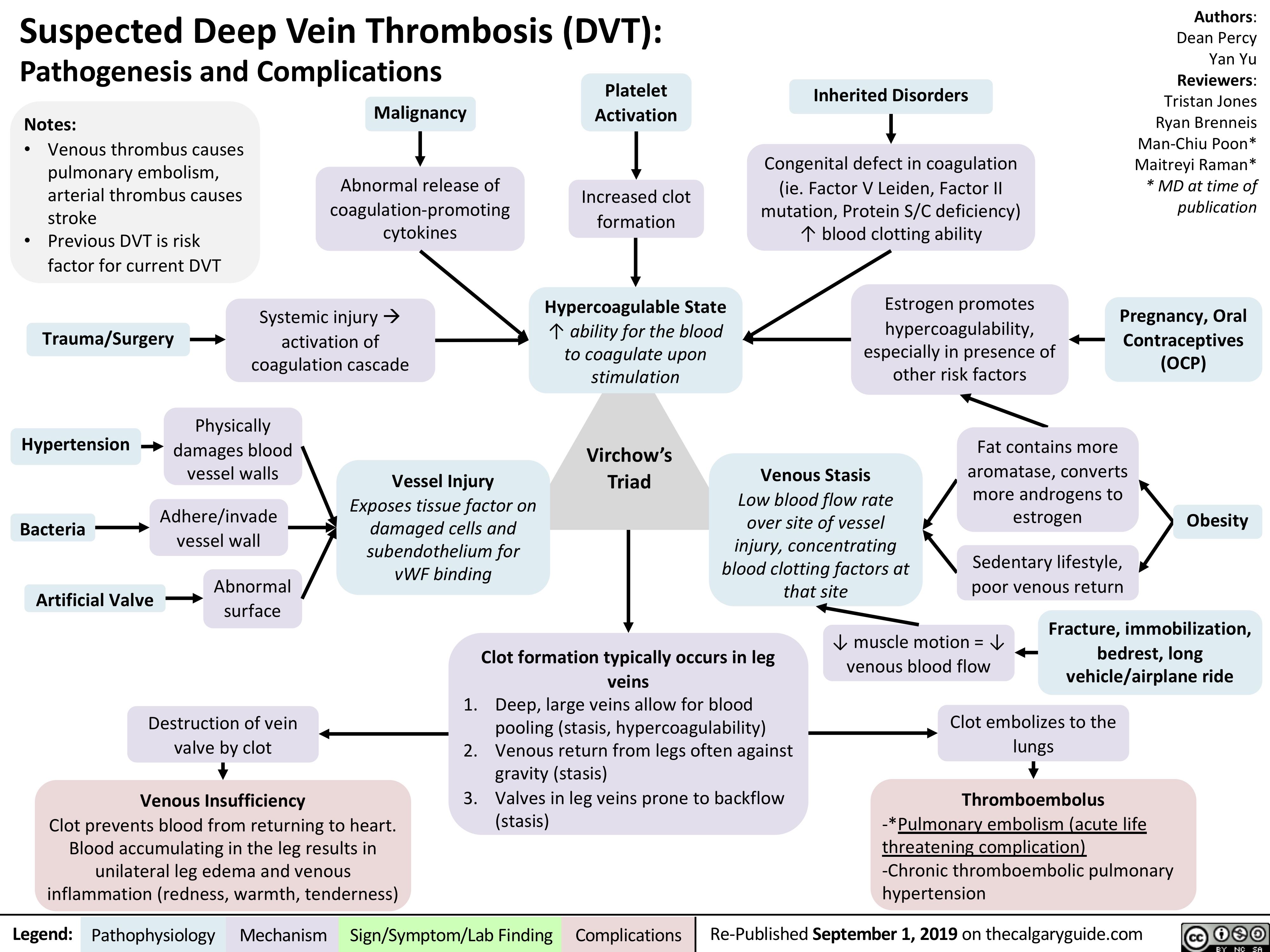{kind=link}
- Thrombus propagate proximally → obstruction + destruction of venous valves → chronic venous insufficiency (post-thrombotic synd)
- embolization
- unilateral edema
- leg pain or tenderness
- Unilateral edema
- tenderness in the calf muscles (meyer sign)
- Homans sign 📷
- Venous distension and prominence of the subcutaneous veins
- Low grade fever (high grade would be suggestive for different inflammatory process)
- Variable discoloration (most common purple)
- Warmth + erythema might also be present
- Phlegmasia 📷
- Phlegmasia cerulea dolens (cyanotic discoloration)
- Phlegmasia alba dolens (white inflammation)
massive ileofemoral venous thrombosis + arterial compression (and spasm)
→ pulse is absent (or diminished)
(mimics arterial occlusion) → but edema + distend vein

- Age
- Smoking
- Immobilization
- Pregnancy and the postpartum period
- Long plane or car trips (> 4 h) in the previous month
- Cardiovascular:
- Stroke
- Acute myocardial infarction
- Congestive heart failure
- Inflammatory:
- Sepsis
- Vasculitis, systemic lupus erythematosus, Behçet syndrome
- Ulcerative colitis
- Surgical/Injury-related:
- Major surgery
- Trauma or lower extremity fractures
- Central nervous system/spinal cord injury
- Burns
- Other Medical Conditions:
- Cancer
- Previous DVT
- Nephrotic syndrome
- Homocystinuria
- Polycythemia vera
- Thrombocytosis
- Antithrombin III deficiency
- Protein C deficiency
- Protein S deficiency
- Prothrombin 20210A mutation
- Factor V Leiden
- Dysfibrinogenemias and disorders of plasminogen activation
- D-Dimers→ if negative exclusiom
- Ultrasonography→ failure to compress the vascular lumen + Doppler
superficial vein thrombosis 📷→ venous mosaic, inflammatory signs, →hyperpigmentation+ulcer(if postthrombotic syndrom)
{kind=link}
- prevention of pulmonary embolism
- minimizing risk of postphlebitic syndrome
- Anticoagulation: NOAK or Warfarin+Heparin

- IVC filter
- if obstruction: Interventional: Ballon angioplasty + stent 📷 ; or surgery
complication, contrainidcation or failure of anticoagulation
→ In massive iliofemoral vein thrombosis → thrombolysis (or interventional is contraindicated)
- PE
- Bleeding (from anticoagulation)
- Chronic venous insufficiency
- Postthrombotic/post-phlebitic syndrom

- Phlegmasia cerulea dolens (cyanotic) 📷
small thrombi → can reach the small vessels more distally
- alveolar deadspace (some alveoli are Ø perfused but ventilated) → ventilation-perfusion mismatch → hypoxemia
- reflex bronchoconstriction → further hypoxemia +hyperventilation
- intrapulmonary shunt → collateral shunt blood from perfused alveoli to non-perfused alveoli (steal the blood for gas exchange) → further hypoxemia
- ↓cardiac output (less return) → further hypoxemia
reduction of cross-sectional pulmonary vascular bed→ increased vascular resistance→ right ventricular failure
→Detailed Patho: 📷
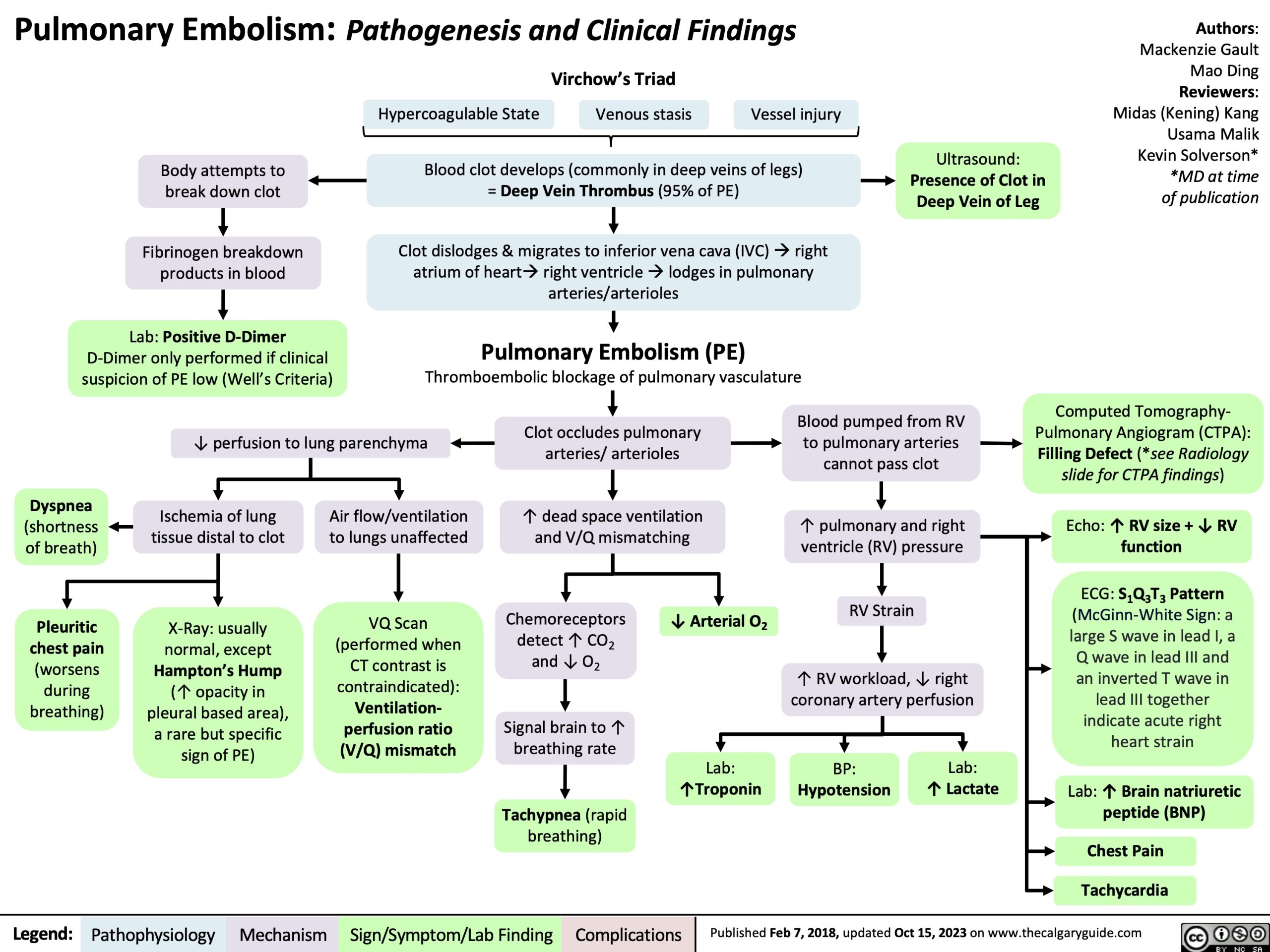{kind=link}
{kind=link}
peripheral occlusion of the pulmonary circulation
presents with→ acute onset pleuritic pain, dyspnea, and hemoptysis
Signs→ decreased excursion of the involved hemithorax, pleural friction rub pleural effusion may be present
non-specific, dypnea, substernal discomfort, tachypnea, tachycardia, crackles
- patients with repeated episodes over years→ eventually present with cor pulmonale
- widespread obstruction of the pulmonary circulation with clot→ progressive dyspnea, intermittent chest pain and cor pulmonale
- Other cardiac pathologies
- other shock types
- other respiratory diseases
- D-Dimer → exclude PE (not confirm)
- Heart marker:
- Troponin (right ventricular myocyte strech)
- BNP
- BGA: hypoxemia, hypocapnia, respiratory alkalosis
CT angiography
- central intravascular filling defect 📷 within the vessel lumen with sharp cutoff
- tracking of contrast material around the filling defect
- complete vascular occlusion
- peripheral wedge-shaped pleural-based opacification (pulmonary infarction). 📷
- pulmonary hemorrhage (ground-glass attenuation)
- chronic thrombi or recent recanalization
- ruling out other causes
- later stages:
- westermark sign (dilation pulm vessels + sharp cutoff)
- atelectasis
- others:
- pleural effusion (small)
- elevated diaphragm
- wedge shaped opacity
⇒ 📷
{kind=link}
RV dilation (+/- akinesia)
triscupid regurgitation
tachycardia→ most common
S1Q3T3-pattern 📷 → right sided heart strain
{kind=link}

- Sudden cardiac death + arrhythmias
- cor pulmonale
- obstructive shock
- Anticoagulation: NOAK / Warfarin + LMWH
- for 3 month if reversible risk factors
- for 6 month if reccurrent thrombosis + continued reversible risk factor
- lifelong if irreversible risk factor
- if massive PE or RVF ⇒ Thrombolytics
- surgical thrombectomy
- IVC Filters → see DVT

right ventricular hypertrophy and/or dilatation secondary to pulmonary arterial hypertension as result of pulmonary disease (parenchymal or vascular) from pulmonary artery origin to pulmonary veins entry into the left atrium
- #1 COPD
- other parenchymal lung/bronchial disease
- PE (recurrent + subclinical)
- idiopathic pulmonary hypertension
- Neuromuscular diseases (due to hypoventilation)
- Rib cage diseases (bone + obesity)
- Central respiratory depression (stroke + obesity)



THE FIRST 4
- COPD
- parenchymal lung diseases
- idipathic pulmonary hypertension
- PE
T 👍🏻
chronic Hypoxia→ chronic vasoconstriction and REMODELLING(structural changes) 📷 → increased smooth muscle cells→ even higher pulmonary hypertension
{kind=link}
50%
- first: Hypertrophy → compensation (of ↑afterload)
- moderate-severe pulmonary HT → Øno more compensation
- congestive syndrome
- ↓Output of RV → LV failure
atrial and ventricular arrhythmias 🥁
(classic shit)
poor af→ most people die within 5 years
>8

- severe respiratory failure
- intermittent infections
- rapid rhythm disorders
F → always present
decreased cardiac output (CO) and increased congestive syndrome
hypoventilation (hypercapnic) type
- ↑PCO2
- ↓PO2
- pulmonary disease→ cough,chronic spitting, rales, wheezing(COPD)
- respiratory failure→ decreased exercise capacity, cyanosis
- pulmonary arterial hypertension→ loud pulmonary S2, S4 and specific echo/CXR signs
- right sided heart failure→ dyspnea without orthopnea, congestive syndrome, tachycardia (sinus/afib) , global systolic heart failure (i.e. cerebral minderperfusion symptoms)
elevated PCO²→ peripheral vasodilator effect
decreased O²→ sleepiness, confusion, occasionally hypercapnic coma
ECHOOOO #classico
- RV enlargement
- RA enlargement→ is a rule!
- paradoxical septal motion
- tricuspid and pulmonary regurgitations
- LV→ usually normal in severe cases decreased LVEF
- signs of RV + RA hypertrophy

- arrhythmias
- record signs of underlying pulmonary disease
- record signs of pulmonary hypertension (pulm artery enlargement)
- occasionally RV enlargement can be seen
DDx ischemic cardiopathy and segmental hypoperfusion
- evaluation of RV performance (cant be done so good with echo)
- CT angiography → in suspected PE
→ not routinely used
pulmonary arterial hypertension of unkown cause (idiopathic)→ primary pulmonary arterial hypertension
mainly in women
spirometry
- blood gas
- coagulation→ hypoxic liver→ hypocoagulability

- Htc (↑in COPD → due to polycytemia)

respiratrory diseases with respiratory failure but without RV-failure signs
- underlying pulmonary disease
- pulmonary Hypertension
- right sided HF
classic stuff→ bronchodilators, ABs, if severe glucos
- continuous O² (18 hours per day)
- CCBs (CAVE→ cardio depressive→ RV failure risk)
- ACEi→ indicated in all right heart failure aptients
- i.v Nitrates→ lessens pulmonary arterial hypertension mainly when given iv.
- Prostacyclin→ especially in primitive pulmonary arterial hypertension
- Phosphodiesterase 5 inhibs→ Sildenafil (viagra)

- Bosentan (Endothelin 1 receptor blocker) MOST EFFECTIVE DRUG
remodelled vessel → ↑risk for thrombosis → further aggravation of pulmHT
→ NOAKs or Warfarin
polycythemia→ hypercoagulable state→anticoagulation
due to atrial/ ventricular enlargement→ arrhythmia risk→ anticoagultion
- in respiratory depression → diaphram pacing 📷
- cyphoscoliosis correction
Diaphragm pacing, (and even earlier as electrophrenic respiration), is the rhythmic application of electrical impulses to the diaphragm to provide artificial ventilatory support for respiratory failure or sleep apnea.
ACEi and Diuretics
CAVE: beta blockers→ risk for COPD exacerbation and HF
→ use beta 1 selective (best = Nebivolol [extra vasodilation effect])
always (if Afib or sinus rhythm)
CAVE→ proarrhythmic effects!
Arrhythmias but CAVE side effect→pulmonary fibrosis→only give for short time (few months)
- heart-lung transplantation (mainly in idiopathic pulmonary arterial hypertension)
- phlebotomy→ if polycythemia is present (i.e. in COPD)
- EXERCISE!! (promote that shit)
- low salt intake