





Respiratory System
T ”average incidence of common cold according to age:
- 3-8 episodes/year in toddlers
- 2-4 episodes/year in adults”
2-3w
Clinical presentation:
- signs of Infection: classic Pharyngitis:
- Clinical exam: Hyperremia + Congestion 📷
- Symptoms + Signs:
- dysphagia, odynophagia (sore throat)
- 🦠Specific viral signs
- cough (dry)
- Assoc. rhinitis + laryngitis
- Rhinitis: rhinorrhea + nasal obstruction + sneezing 📷
- laryngitis: dysphonia
- Diarrhea
- if adenovirus → conjunctivits
- +/- fever (if present LOW-grade)
- Special viral + pedi: (esp if <6y)
- Irritability
- Feeding difficulties ! (nasal obstruct. / odynophagia)
- +/- ↑LN


⇒ usually Ø other systemic manifestations (digestive, LN, exanthem)
Criteria | Infants | Older Children (≥6 years) |
Onset | Often presents with fever | Symptoms include dry nasal passages and scratchy throat |
Clinical Manifestations | Varied symptom presentation | Less variability in symptoms |
Nasal Inflammation Symptoms | Nasal discharge common | Nasal obstruction is more prominent |
Fever | More frequent occurrence | Less frequently observed |
Behavioral Changes | Irritability and restlessness are more common | Less commonly irritable or restless |
Feeding and Sleeping Patterns | More likely to have difficulties | Fewer difficulties with feeding and sleep |
Lymph Node Enlargement | More commonly observed | Less commonly observed |
Etiology: (RACI) - rhinovirus (30–80%), - coronaviruses (≈ 15%) - influenza viruses (10–15%) - adenoviruses (5%) - others
CLINICAL DIAGNOSIS:
- Rhinitis signs
- Pharyngitis signs
- Minimal/Ø systemic signs (fever, headache, myalgia)
- Exclusion of DDx
- bacterial pharyngitis
- Measles + Pertussis (common cold = prodrome)
- Any other respiratory infection w/ common cold = prodrome
- DDx rhinitis → allergic, vasomotor, etc.
- Normal: Self-limited after 5-7d (adults) / 10-14d (infants)
- Bact. superinfection / spread
- Asthma exacerbation
- Fever → Seizure

viral = symptomatic Tx:
for <6y:
- Odynophagia + other pain + fever ⇒ NSAIDs / paracetamol / Novalgin
for ≥12y (OTC drugs)
- Nasal obstruction ⇒ decongestants + de-obstructing methodes (inhalation, nasal aspiration, intra-nasal saline)
- Rhinorrhea ⇒ hydration, H1 blocker
- Cough ⇒ anti-tussives (i.e. Codein)


→ if bacterial superinfection (i.e. otitis media, sinusitis, pneumonia) ⇒ AB
infants / small children:
- Dehydration
- Vomiting + alimental refusal
- High fever
Clinical presentation:
- 🧣Signs of Infection:
- Clinical exam: Hyperremia + Congestion (+ pus) 📷
- Symptoms + Signs:
- Pharyngitis:
- like viral: dysphagia, odynophagia (sore throat)
- petechia (on pallate) 📷
- Tonsillitis
- 🧫Specific signs of bacterial infection:
- PUS
- HIGH Fever
- ↑LN
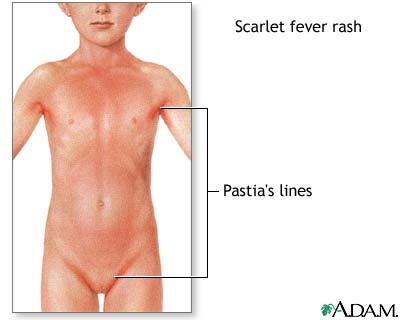
- Exanthem (⇒scarlet fever) aka scalantiform rash 📷
- Ø viral symptoms! (Øcough, Ørhinorrhea, Ø hoarseness)
⇒ Etiology: Strep. pyogenes (aka beta hemolytic GAS)

Acute viral tonsillopharyngitis: children <5 years and young adults Acute GAS tonsillopharyngitis: children aged 5-15 years; rare in children aged < 2years
Centor score
The Centor score is a clinical prediction tool used to estimate the probability of a streptococcal infection in patients with a sore throat.
A score of 0-1 is considered low risk, 2-3 is moderate risk, and 4-5 is high risk.
- The score is calculated based on the presence or absence of four clinical criteria: fever, tonsillar exudates, tender anterior cervical lymphadenopathy, and absence of cough.
- Another criteria used in the score is the patient's age, with younger patients (<15 years old) being assigned a higher point value. This is because streptococcal infections are more common in younger individuals. Specifically, patients under 3 years old are assigned 1 point in the Centor score.
- Each of these criteria is assigned a point value, and the total score is used to estimate the likelihood of a streptococcal infection.
🦠viral sign + ↑LN
Decreased appetite

- Local spread
- 2)👂🏼 Otitis media 📷+ Mastoiditis
- 3) 🎛️ Sinusitis 📷
- 4) 💪🏼 Necrotizing fasciitis 📷
- 5) Pneumonia 📷
- Systemic complications
- Pharyngitis signs + non-specific inflammatory
- +- GI signs
- 3) ⛑️ Auto-immune
- Rheumatic fever 📷 (JONES)
- PANDAS: neuropsychiatric disorder

aka “streptococcal bacteremia”
1. TOXIC Shock-signs(i.e. ↓BP+fever) + Exanthem (measle-like) 2. Evolution: - skin desquamation - multi-organ failure ☠️
erythrogenic toxin
(makes you red 👹)
5-15 years (like GAS)
(max 5-9y)
Antitoxic antibodies against pyrogenic exotoxines → lifelong protection (you only get it once in a lifetime)
2-3 days (1-7d)
Starts on 👹 face (SPARES PERIORAL! = Filatov mask)
↓
⇒ spreads rapidly over entire body ⇒ GENERALIZED (measle-like) → TEXTURE: “ 🧽 SANDPAPER” (micropapules) → +- pruritus
↓
3) ⇒ after generalization ⇒ becomes more insense around skin folds: “🍝 PASTIA’S LINES”
↓
4) DESQUAMATION: ❄️ flaking of the face → after 1w: ✋🏼desquamation on hand 📷
→ 🩸hematuria → RF ⇒ 🥐 ↓GFR → 💳 ↑Crea

*patho
Indication for AB Tx? ⇒ high probability strep infection?
- + rapid antigen test
- GAS clinic + Øviral signs
↓
- AB Tx
- <27kg: p.o. - 250mg - 3x/d - 10days
- >27kg: p.o. - 500mg - 3x/d - 10days
- allergy → macrolide
- abscess → incision,drainage + Penicillin + Clinda
- non-compliant →i.m. Benzathine pencillin G single dose
- recurr. → Clindamycin / Amoxi-clav / Cefuroxim
- NEVER Tetracycline + Sulphonamide!!!
#1 ✏️Penicillin V / Amoxi
#2 Amoxi
#3 special situations:

- symptomatic Tx (NSAIDS, paracetamol, local tx)
- Sipping cold or warm beverages
- Gargling with warm salt water

local:
- LIKE VIRAL:
- Dehydration
- Vomiting + alimental refusal
- High fever
- failure of p.o. AB-Tx ⇒ i.v. in hospital
VIRAL:
- common cold (pharyngitis +/- nasopharynx / larynx) (rhino, corona, influenza, adeno)






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Liver markers
- Leukocytosis (INVERSION: ↑Lymp + Monos)
- Monospot Test (paul bunnel)
- Identifies heterophile antibodies resulting from EBV exposure using red blood cells (RBCs) sourced from sheep or horses.
- A sample of the patient's serum undergoes mixing with sheep/horse RBCs for testing.
- A positive outcome shows a cross-interaction between heterophile antibodies and RBCs from sheep/horses, leading to clumping.
- A negative outcome indicates the absence of heterophile antibodies, resulting in no clumping reaction.
- The test boasts an approximate specificity of 100% and a sensitivity rate of 85%. There's no need for added evaluation if results are positive.
- Serology (IgM)
Monospot Assessment

- Symptomatic Tx (anti-inflammatory + steroids if severe)
severe means 1 of the following:

- Avoid physical exercise! (esp. contact sport → risk of splenic rupture)
NO Penicilin/Amoxi 🤡
{kind=link}
{kind=link}
BACTERIAL:
- GAS pharyngitis
unilateral pharyngitis !!!
- ulceration + necrotizing pseudo-membrane on one tonsil 📷
- halitosis
- ↑LN (+fever)
{kind=link}
{kind=link}
bacterial overcrowding due to:
- poor oral hygiene
- malnutrition
- AB → Penicillin / Erythromycin + Metronidazole
- oral hygiene
- topical disinfectants
- Viral
- Bacterial (GAS or golden quartett)
GAS = Group A streptococcus

{kind=link}
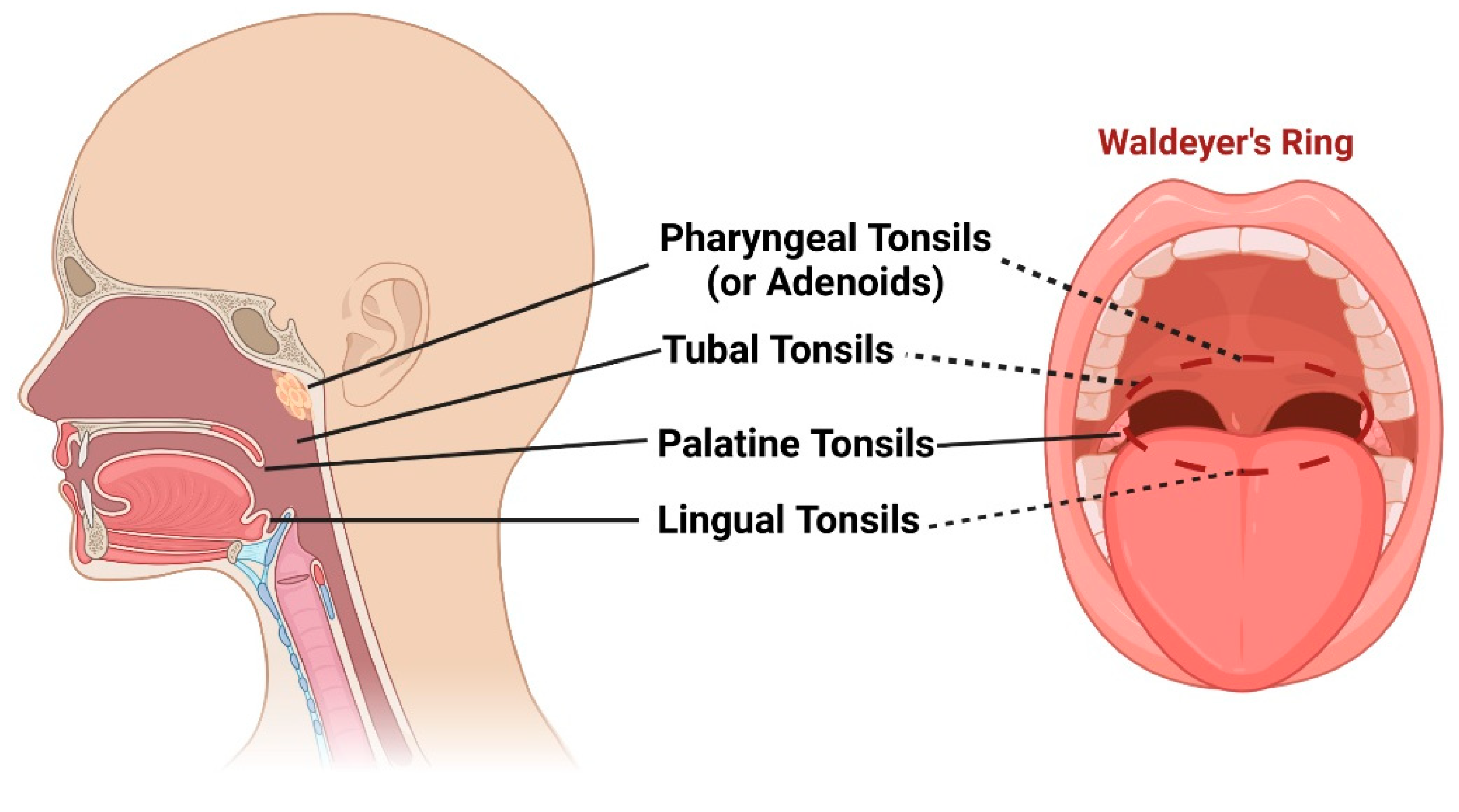
⇒ PHARYNGEAL TONSILS / ADENOIDS
- hypertrophy
- congestion + edema
⇒ POST. nasal obstruction (eustachian tube blocked)
Pharyngeal (Luschka’s) tonsil → hypertrophied (lymphoid tissue) + congested/secretion 📷
{kind=link}
(fiberoptic) nasal endoscopy → post nasal cavity → entire rhinopharynx filled with mass (=gold standard but not mandatory for dgx)
Clinical presentation of ACUTE adenoids
- Nasal obstruction
- Eustachian tube obstruction →frequent Otitis media (effusion + suppurative)
- Adenoid face (in evolution) 📷 📷
- Adenoid facies, associated with persistent nasal obstruction
- Upper lip dysfunction, linked to chronic nasal obstruction
- Constricted upper dental arch, often observed in this condition
- Rearward positioning of the mandibular incisors
- Elongated anterior facial height, a characteristic feature
- Narrow or "V"-shaped maxillary arch, typical in such cases
- Mandible with posterior rotation, a common observation
→ Persistent rhinitis (>10d)
→ mucupurlent rhinorrhea → ant + POST.(drip→ Cough ) → Fever
→ oral breathing → halitosis , in evolution: sleep apnea
⇒ conductive hearing loss (in evolution)
📷 = Waldeyer’s ring
{kind=link}
Other causes for rhinorrhea
- Common cold <10d
- Sinusitis >10d
Clinical Manifestation | Common Cold | Adenoiditis | Sinusitis |
Nasal Congestion | Present (+) | Present (+) | Present (+) |
Mucopurulent Rhinorrhea | Present (+) | Present (+) | Present (+) |
Cough | Present (+) | Present (+) | Present (+) |
Duration of Symptoms | <10 days | >10 days | >10 days |
- AB (if bacterial)
- Penicillin
- Cephalosporin
- Topical Tx (intra-nasal): saline solution +/- AB
→ Duration: durations of symptoms + 1 week
- Tx of otitis media ⇒ myringotomy + grommet 📷

Adenotonsillectomy, or surgical excision of adenoids, is indicated for:
- Chronic/recurrent otitis media in children
- Chronic/recurrent sinusitis
- Severe symptomatic nasal obstruction (e.g., obstructive sleep apnea)
gucci 👍
(duration = 7d)
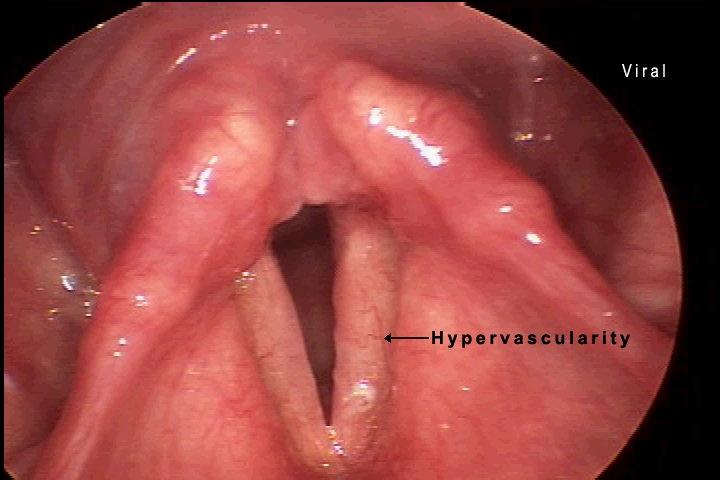
Acute (simple) laryngitis
Laryngoscopy: 📷
{kind=link}
Etiology: COMMON COLD (VIRAL)
Patient: older children!
- viral infection signs

- LARYNGEAL signs
- hoarseness
- BARKING COUGH (seal-like)
- ØAIRWAY obstruction
- assoc. / prodrome nasopharyngitis
(Østridor, Ødyspnea, Ørespir. distress)
= self limited (1w)
⇒ Symptomatic Tx (hydration, inhalation, avoid irritants, vocal rest)

*Signs of respiratory distress → 📷
*Tripod → 📷
{kind=link}
SUBGLOTTIC:
VIRAL → mainly: Parainfluenza virus 📸 (less common RSV 🪦 or others)
Inflammation + edema ⇒ 📷 narrowed subglottic area (obstruction)
{kind=link}
⇒ more severe in smaller children (small larynx→ edema more impact of luman narrowing)
Clinical Indicator | Mild Severity | Moderate Severity | Severe Severity |
Stridor | Observable when agitated | Notable at rest | Present at rest (occasionally biphasic) |
Tachypnea | Absent | Mild presence | Moderate to severe |
Retractions | Absent | Mild to moderate | Severe |
Mental Status | Restlessness upon disturbance | Restless without disturbance | Lethargy |
- Viral → pneumonia, bronchiolitis
- bacterial → pneumonia, bronchiolitis, tracheitis, otitis media
- dehydration
- <0,5y
- moderate / severe
- poor oral intake / dehydration
- Toxic + high fever ⇒ DDx bacterial (membranous + epiglottitis)
- steroid refractory
- Øpossible at home
- other obstructive laryngitis
- other causes for airways obstruction
- abscess (peritonsillar, retropharyngeal)
- foreign body
- angioedema
- external compression
- other causes for laryngeal irritation
- GERD
- congenital anomalies
Non-inflammatory subglottic edema
contraction of larynx muscles
⇒ triggers/RF = laryngeal irritants: allergic, viral, adenoids, GERD, FH
- Membranous bacterial croup (Chevalier Jackson laryngo-tracheo-bronchitis)
- Diptheria
(Staph aureus)
SUPRAGLOTTIC:
- Acute epiglottis
→ 🅱️ Hemophilus influenza B
Pathology | Clinical Course | Stridor (Intensity) |
Viral Croup | Self-limited disease; worse at night | Yes (mild to severe) |
Spasmodic Croup | Short duration; recurrences | Yes (moderate to severe) |
Membranous Croup | More rapid deterioration compared to viral croup | Yes (moderate to severe) |
Epiglottitis | Rapidly progressive; respiratory arrest can occur within hours | Yes (often not severe) |
‼️ be careful with them → stress → trigger airway obstruction
contraction of laryngeal muscles or aspiration of saliva → apnea → resp. arrest
⇒ only performed when airways secured
⇒ in epiglottitis: only performed on ICU!!
NOT COMPULSARY!
LAB:
- Deyhydration?
- Oxygenation? (SpO2)
- Inflammatory lab?
PARACLINICAL: (usually Ø recomm. in viral)
⇒ Xray
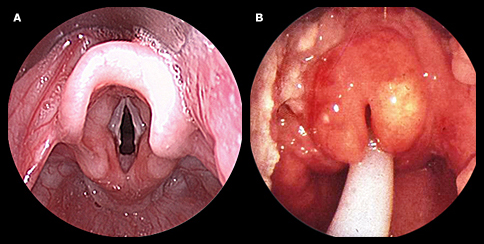
⇒ laryngoscopy 📷(+oropharyngoscopy)
{kind=link}
left picture = viral croup
right picture = epiglottitis

- Steroids
- epinephrine
- humidified air
- intubation + ventilation
- hydration + O2
Mild Croup:
- Manage anxiety in infants.
- Utilize cool mist inhalation.
- Position infant in upright posture for sleep.
- Encourage cool air inhalation during colder months.
- Administer Dexamethasone:
- Effective in reducing airway inflammation within 6 hours.
- Available as oral syrup, IV, or IM.
Moderate to Severe Croup:
- Hospitalization is necessary for severe cases.
- Use inhaled racemic epinephrine:
- Efficient in reducing airway inflammation; faster than Dexamethasone.
- Apply Dexamethasone.
- Offer humidified air or oxygen when needed.
- Administer IV fluids to counteract dehydration.
- Intubation is vital when there's a risk to the airway (occurs in less than 3% of severe croup cases).
Note: Intubation can be challenging in severe croup due to narrowing of the subglottic region. An anesthesiologist's assistance is crucial.
- Rapidly improves without Tx (<1h)
- Symptomatic
- Cold night air
- Humidified air


- Single therapy often suggested with a third-generation cephalosporin (examples include cefotaxime, ceftriaxone) or a beta-lactam combined with a beta-lactamase inhibitor (such as ampicillin/sulbactam, amoxicillin/clavulanate, piperacillin/tazobactam).
- If there's a penicillin allergy in patients, opt for a fluoroquinolone like levofloxacin.
- To counteract MRSA, consider adding an antibiotic with anti-MRSA properties, e.g., vancomycin or clindamycin.
- Intubation in Severe Croup:
- Intubation is indicated when airway compromise is imminent.
- This procedure is required in less than 3% of infants with severe croup.
- A noteworthy point is the difficulty of intubation in severe croup due to subglottic narrowing. It emphasizes the importance of having an anesthesiologist present during the process, indicating the complexities and potential challenges of this procedure.
child presenting with stridor + respiratory distress
↓
- laryngeal signs? → croup → recurrent/Øprodrome → pseudocroup →common cold prodrome → croup → viral croup prodrome + high fever → membranous (also respect age; <3y ⇒ 0,5-3y - viral croup+pseudo; 0.5-7 - epiglottitis)
- muffled voice + drooling/dysphagia + Ø cough + high fever? → epiglottitis
↓
[SKIP Lab + Paraclinical exams to Ø aggrevate respiratory distress!!]
↓
Tx:
- pseudocroup → usually ØTx needed(symptomatic → humidified air, cold air at night
- Rest → steroids, epinephrine, humidified air, intubation + ventilation, hydration + O2
- epiglottitis + membranous croup → AB (Amoxi/Cephalorsporine)
Features / Structures | Bronchi/Trachea | Bronchioles |
Epithelium | Pseudostratified ciliated columnar epithelium (important for mucociliary clearance) | Simple ciliated columnar epithelium |
Special Cells | Goblet cells (associated with Cough + rhonchi) | - |
Support Structure | Cartilage (C-shaped hyaline cartilage rings in the trachea and elastic cartilage plates in the bronchi) | Enclosed by smooth muscle |
Other Structures | Annular ligaments of trachea (horizontal fibrous bands that join the tracheal cartilage rings together), Smooth muscle, Seromucous glands (secrete mucus), Basal cells | Terminal bronchioles have simple ciliated cuboidal epithelium & are surrounded by smooth muscle |
MAINLY VIRAL! 🦠
bronchitis: parainfluenza 📸; influenza A+B 👯♀️; others
others: common cold viruses + RSV
bronchiolitis: RSV 🪦 (rare bact.: myocoplasma pneumonia or other respiratory viruses)
- Vaccination Influenza A+B
- Pavilizumab (montly injection before RSV season)
- Infection control measures
- hand hygiene
- prevent cross-infection with other infants in the hospital (isolate infants with bronchiolitis)
- avoidance of tobacco smoke exposure
- encouragement of breastfeeding at least in the first 6mo of life

{kind=link}
- Asthma
- Bronchiolitis obliterans

{kind=link}
{kind=link}
F → valuable!
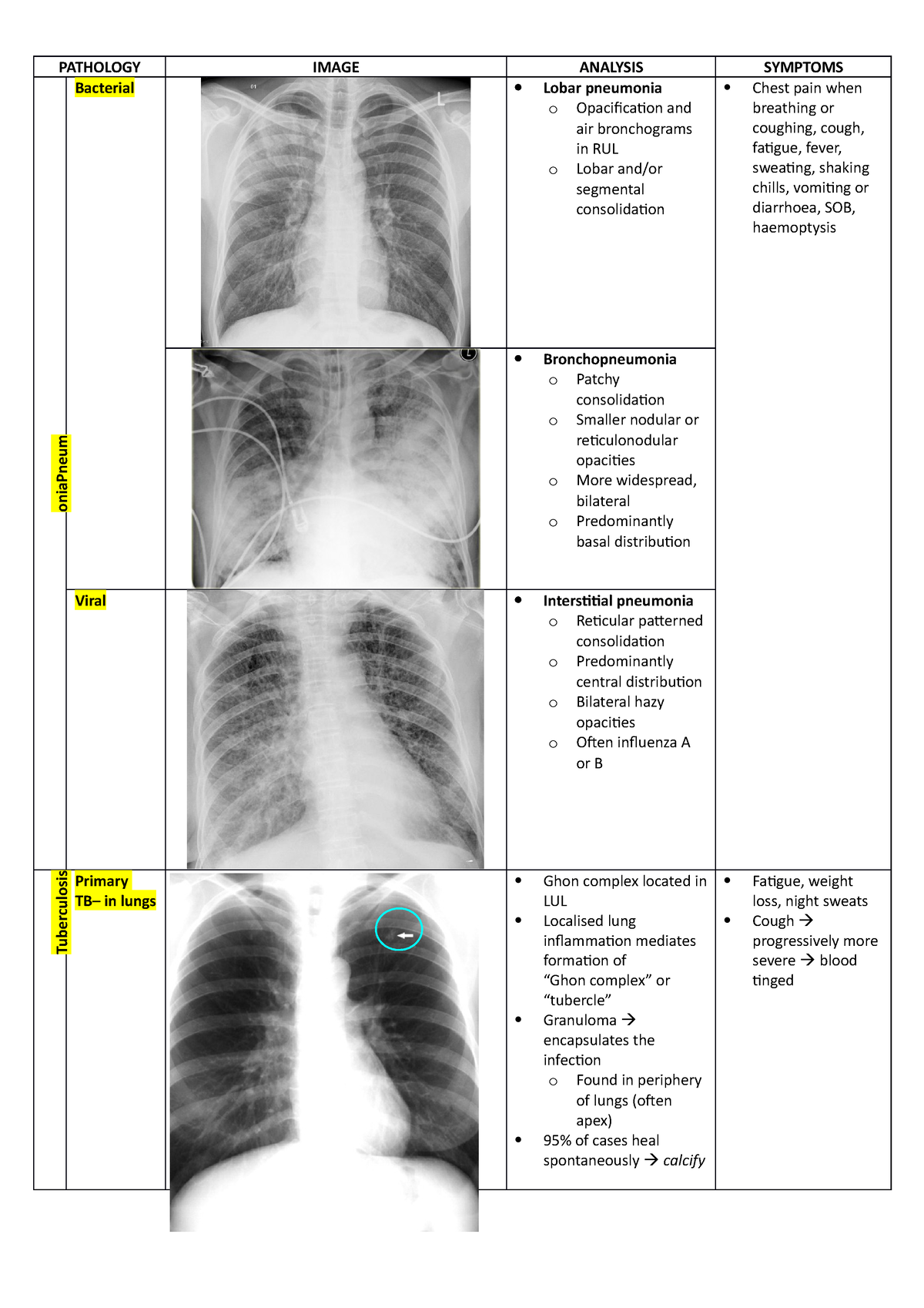
⇒ Dg: PLEURAL effusion +pneumonia( consolidation, interstital pneumonia)
⇒ DDx: pneumothorax, atelectasis, cysts, tumors

CLINIC:

PARA-CLINIC:

{kind=link}

🏥 when:
- <6️⃣Ⓜ️ Age ≤ 6 months.
- 🚨 Severe OR complicated pneumonia.
- 🕰Associated chronic diseases
- ❌Failure to respond to initial ambulatory antibiotic treatment.
Tx:
⇒ 💊 supportive treatment + AB
Typical: 🎸amoxicillin p.o./ampicillin iv. OR Cefotaxim i.v.
Atypical: 🦅Macrolides p.o. OR i.v. (Clarithro, Azithro)
Setting | Patient Age | Bacterial Pneumonia | Atypical Pneumonia |
Ambulatory | 6 months - 4 years | First line: Amoxicillin PO Alternative: Amoxicillin-clavulanate PO | First line: Azithromycin PO Alternative: - |
≥5 years | First line: Amoxicillin PO Alternative: Amoxicillin-clavulanate PO Atypical pneumonia cannot be excluded: Beta-lactam PO + Macrolide PO | First line: Azithromycin PO Alternative: Clarithromycin PO | |
In hospital | - Immunized with Hib and PCV
- LOW resistance of S. pneumoniae | First line: Ampicillin IV Penicillin G IV Alternatives: Ceftriaxone IV Cefotaxime IV Atypical pneumonia cannot be excluded: Beta-lactam IV + Macrolide IV or PO Suspicion of CA-MRSA: Vancomycin IV or clindamycin IV | First line: Azithromycin PO or IV Alternatives: Clarithromycin PO Final height reached, macrolide intolerance: Levofloxacin IV or PO |
- NOT immunized with Hib and PCV
- HIGH resistance of S. pneumoniae | First line: Ceftriaxone IV Cefotaxime IV Alternative: Levofloxacin IV Suspicion of CA-MRSA: Vancomycin IV or clindamycin IV | First line: Azithromycin PO or IV Alternatives: Clarithromycin PO Final height reached, macrolide intolerance: Levofloxacin IV or PO |
Inducer →
- Genetic
- Environmental
Inflamm →
↑responsive →
+TRIGGER (allergens, infect, exercise, cold air, ..)
Clinic
Wheezing, Dyspnea, cough, chest tightness
Characteristic | Early Asthmatic Response
(Hyperresponsive/allergic) | Late Asthmatic Response
(inflammatory) |
Onset | 5 - 60 min | 3 - 4 hr |
Duration | 60 - 120 min | Up to 24 hr (or more) |
Mechanism | Bronchospasm | Inflammation |
Mediators Involved | Histamine, leukotrienes,... | Cytokines, leukotrienes,... |
Cells Involved | Mast cells | Eosinophils, T cells |
Prevention & Tx | Salbutamol | Steroids |
⇒ 📷
{kind=link}
{kind=link}
Classification ⇒ Controlled?
Age | Criteria (in the past 4 weeks any of): | WELL controlled | PARTIALLY controlled | UNCONTROLLED |
Children 6-11 | >2x daytime symptoms/week
Any night waking?
>2x Reliever needed? *
Any activity limitation? | None | 1-2 criteria | 3-4 critera |
Children ≤5 | >1x daytime symptoms/week (few min.)
Any night waking/coughing?
>1x Reliever needed?*
Any activity limitation? | None | 1-2 criteria | 3-4 critera |
*Excludes reliever taken before exercise

- psycho-social
- often in hospital + Ø in school
- psychologic impact
- ↓ Lung function
- Short stature (due to asthma/steroids)
Mutation CFTR gene ⇒ autosomal recessive transmission ⇒ abnormal CFTR ⇒ absence of chloride channels

↓
In sweat glands: 📷
{kind=link}
inability to reabsorb Cl- ⇒ ↓Na+H2O reabsorption ⇒ ↑NaCl in sweat
Chloride channel transports chloride from lumen into cell
Other exocrine glands (GI, lungs, billiary etc): 📷
{kind=link}
⇒ inability to secrete Cl- into lumen ⇒ ↑Na +H2O reabsorption ⇒ ↑Viscosity of mucus ⇒ blockage of passages ⇒ chronic inflammation + remodeling (i.e. bronchiectasis, pneumonia in lungs ⇒ COPD)
→ ↑ Na+ reabsorption →↑ transepithelial potential difference between interstitial fluid and the epithelial surface (relevant for dgx)
↑Na in cells → negative charge of epithelial surface → ↑transepithelial potential difference (in healthy individ: Na stay on epithelial surface → positive charge of surface → ↓transepithelial potenial difference)

GI (common in children)
- Intestine:
- Obstruction ⇒ pain, distension, palp. mass
- Meconium ileus (in newborns)
- rectal prolapse (rare)
- Pancreas:
- Pancreatitis
- Exocrine insuff
- Malabsorption → failure to thrive
- Vit ADEK malabsorption
- Steatorrhea + diarrhea
- Abdominal distension
- CFRD (endocrine) - late
- Hepatobiliary
- Obstruction:
- cholecystolithiasis, cholestasis
- biliary cirrhosis + portal HT
- ↓Albumin

initally: hyperviscous secetion block pancreatic duct → pancreatic enzymes dont reach duodenum + self destruction of exocrine pancreas → enzyme deficiency


Respiratory (common in adults)
- Obstruction
- “COPD” with bronchiectasis
- emphysema → pneumothroax + cor pulmonale
- airway obstruction + hyperreactivity ⇒ wheezing + dyspnea
- Infections + Productive cough + hemoptysis (recurr infections→ damage to lung tissue)
- infants + childs → S.aureus
- Adults → Pseudomonas
- other common → S.pneumonia, H.influenz
- Chronic sinusitis (+/- polyps)
- Digital clubbing (chronic hypox)
bronchial obstruction + reccurr. infection → atelectasis, emphysema* → pneumothorax *emphysema → ↑pulmonary artery pressure → RV strain


Sweatglands
- salty sweat
- +/- electrolyte wasting
Urogenital
- UT-obstruction → nephrolithiasis, freq. UTIs
- Ø/↓ Fertility
- Men → infertile (but sterile)
- obstructive azoospermia (normal production of sperms)
- absent vas deferens
- Woman → ↓fertility
- Viscous cervical mucus can obstruct fertilization.
- menstrual abnormalities (i.e. amenorrhea)
- Delayed secondary sexual development
viscous mucus → obstruction of vas deferens formation during development
signs of DISTAL small bowel obstruction
- BILIOUS vomiting
- abdominal distension
- Ø meconium / stool
XRAY w/ contrast:
📷 ⇒ dilated bowel loops +- “soap bubble” appearance
{kind=link}

Tx:
- enema with contrast agent

- perforation (or volvulus)→ surgery
CLINIC
(🫁, 🍤, 🍑, 🎈🍆)
2 Sweat tests +
OR Family history +
PLUS
OR 2 CF mutations +
OR Neonatal screening +
OR Nasal transephithelial potential abnormal
⇒ DGx Algorithm: 📷
{kind=link}
- LUNG:
- Pulmonary function test (obstruct? (bronchiectasis), diffusion)
- Imaging: Xray + CT (hyperinflation, signs of bronchiectasis?)
- Sputum culture + sinus aspirates (if pneumonia suspected: typically = bilateral lobar consolidation)
- BGA (hypox?)
- ↓Albumin
- Aspergillus serology
- Pancreas
- ↓ Fecal elastase 1 (endocr.)
- OGTT (exocr.)
- Nutrition
- ↓Vit ADEK

Contraction Alkalosis (due to fluid loss via sweat)
- Sweat loss ⇒ ↓Na + ↓Cl
- Renal Na+Water resorption ⇒ ↓K+ + ↓H+

Lung fx preservation
- PHARMA
- high dose IBU (alternative: low dose Azithromycin)
- Bronchodilators (SABA, LABA)
- Mucolytics
- Hypertonic NaCl (nebulized)
- Dornase alfa (aerosolized)
- CFTR modulators ⇒ in combination therapy
- Lung transplant
- NON-PHARMA
- Airway clearance techniques (i.e. chest physio)
- Exercise

recombinant DNase: break down of extracellular in sputum ⇒ thinning of mucus
New therapy 🆕
Target = defects in CFTR protein
⇒ CFTR modulator have different targets for CFTR → can be combined
improves airway clearing, lung capacity & increases survival
Infections: Prevention + acute exacerbations
- Prevention:
- Consider AB eradication regimes (for Pseudomonas + MRSA)
- Long-term treatment with azithromycin may be used to prevent recurrent pulmonary infections.
- Pulmonary exacerbation: AB!
Pseudomonas: Tobramycin inhaled
MRSA: Vanco inhaled + oral ABs + Extrapulmonary eradication
S.Aureus → Vanco if MRSA, Naficillin if MSSA
Pseudomonas → i.e. Tobramycin + Ceftazidime (= 2 AB with different MOA)
Others: H.influenza→like pseudomonas; other G+→ like S.Aureus
Nutrition adjustments
- High energy diet
- ↑NaCl intake
- Supplementation:
- Pancreatic enzymes
- Vit ADEK
CF ⇒ ↑energy demand (high resting energy consuption, loss via malabsorption, ↑resp. demand
blood spot test (heal prick) in the first 24-48h 📷
{kind=link}
↓
Immunoreactive trypsinogen screening (IRT)
Mucus plug obstructs pancreatic duct → trypsinogen cant be converted to trypsin → ↑IRT
↓
confirmatory test if ↑ (i.e. sweat test)
alternative for IRT: molecular testing, PAP testing (Pancreatitis-assoc. protein)