





Pediatric surgery
Gastro-intestinal
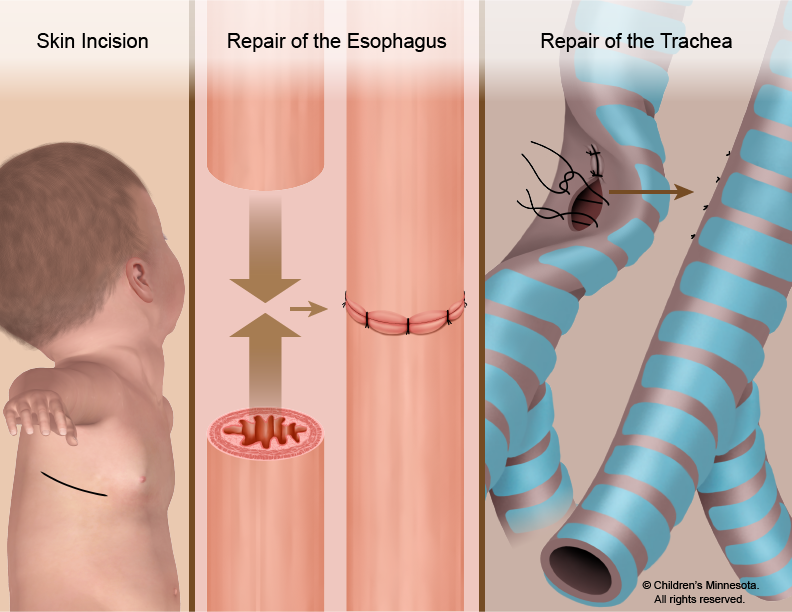
a variable length of the mid-portion of the oesophagus is missing 📷
Gross & Vogt Classification ⇒ 📷
A: isolated Esophagel atresia (EA) without Treacheal Esophageal Fistula (TEF) (5-7%)
B: EA with proximal TEF
C: EA with distal TEF (80-90%) = 🥇most common
D: EA with proximal and distal TEF
E: TEF without EA (4%)
Vertebral Anomalies
- Hemivertebrae
- Butterfly vertebrae
Ano-Rectal Anomalies
- Imperforate anus
- Anal atresia
Cardiovascular Anomalies
- VSD (Ventricular Septal Defect)
- ASD (Atrial Septal Defect)
- Tetralogy of Fallot
- PDA (Patent Ductus Arteriosus)
Tracheo-Esophageal Anomalies
- Tracheo-Esophageal Fistula (TE Fistula)
Renal Anomalies
- Hydronephrosis
- Renal agenesis
- Horseshoe kidney
- Hypospadias
- Undescended testis
Limb Anomalies
- Hip dysplasia
- Polydactyly
- Syndactyly
- Club hand
- Erythrodactyly
- Ø gastric bubble in prenatal ultrasound
- Polyhydramniosis (amniotic fluid can Ø be absorbed by babies digestive tract → excessive amount of fluid in amniotic sac)
- distension of the prox Esophagus
- 💦 due to ↓ saliva swollowing:
- excessive salivation
- mucus comig out of mouth/nose
- 🫁respiratory distress (because of fistula)
Diagnosis should be made BEFORE feeding, otherwise the milk might enter the lungs via the fistula ⇒ ⚠️ aspiration pneumonia
before first feeding: try to pass catheter throu the mouth ⇒ wont pass beyond 9 cm if atresia
- bronchoscopy
- Xray
- Chest radiography
- limb radiography
- Sono
- Echocardiography
→ VACTERL
- Chest radiography: vertebral/rib anomalies can be seen, poss. asp pneumonia, absence of GI air
- Sons: kidney/uretral anomalies
- ECho: heart malformations
- NO oral feeding
- aspiration of upper Esophagela pouch
- O2
- avoid crying → tends to fill the stomach with air→ risk for regurgitation
- transveres incision on 4. ICS
- intra and extrapleural approach of eosophagus
- TEF identifie and exposed ⇒ closed with absorbable transfixion sutures
- end-to-end eosophageal anastomosis
- classic complications → anastomotic leak
- 🚇 (esophagus)
- Reflux
- EO dismobility
- 🫁
- recurrent TEF
- Tracheomalacia

- Diagnosis is typically straightforward and may even be suspected prenatally.
- The prognosis can be influenced by associated anomalies and prematurity.
- Postoperative complications often occur.
- Preoperative management plays a crucial role in preventing aspiration pneumonia.
- If a neonate experiences respiratory distress, it should raise suspicion of Esophageal Atresia (EA).
nope, its an aquired disease, that occurs 3-8 weeks after birth
its the most common cause of non-bilious vomiting in infants → 1/800-1000 birth

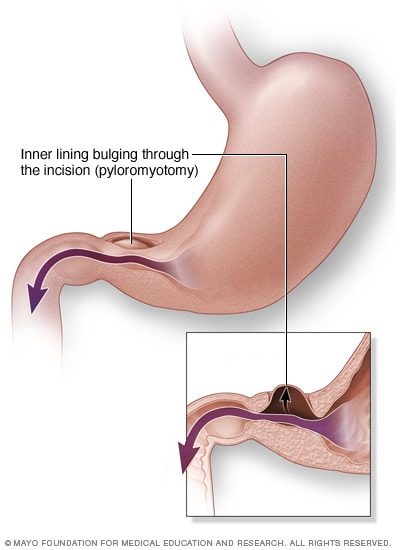
⇒ 📷
a hypertrophy of the circular smooth muscle of the pylorus

→ narrowing of the pyloric channel → obstruction
nobody knows (idiopathic)
→ a theroy suggest NO (nitric oxide) lack in the pylocir muscle
(NO usually leads to relaxation of smooth muscles)
hiatel/inguinal herias
- non bilious vomitung 2-4 weeks after birth → vomit begins 1 day after meal
- child seems to be hungry

- constipation
- weight loss, failure to thrive
- sometimes blood in the vomit → esophagits due to vomiting
- dehydration → decreased urinary output
- gastic contractions visibly moving across the epigastrium

- hypertrophied pylorus is palpable, feel like an olive 🫒
→ before examination tha stomache needs to be emtied! (NGt)
- non bilous vomiting beginning from week 3-8
- palpable pyloric tumor
- visible gastric waves
- US
- Upper GI contras examination
- Lab
- pyloric muscle thicening 3.4 mm. (premature) 4mm in infants
- pyloric channel length > 16 mm
elongated pyloric channel
METABOLIC ALKALOSIS DUE TO HCL LOSS → coz vomiting al the time
- high bicarbonate
- hypokalemia
- hypochloremia
- dehydration
Other causes for non billious vomiting
- Overfeeding
- MIlk allergy
- Obstruction
- pyloric spasm
- reflux
- maltrotation
- duodenal obstriction
- paralytic
- metabolic disorders
- sepsis
- central nervous problems
treat dehydration and stop oral feeding to prepare for operation
- vomiting → persistent after 4 days→ incomplete myotomy/perforation
- HPS (Hypertrophic Pyloric Stenosis) is the most frequent cause of nonbilious vomiting in previously healthy infants aged 2-8 weeks.
- Managing hydroelectrolyte and acid-base imbalances is crucial and necessitates preoperative attention.
- The triad of HPS includes an enlarged, palpable pylorus, forceful white vomiting, and visible gastric waves on the abdomen.
- Ultrasonography (US) offers gold-standard criteria for diagnosing HPS.
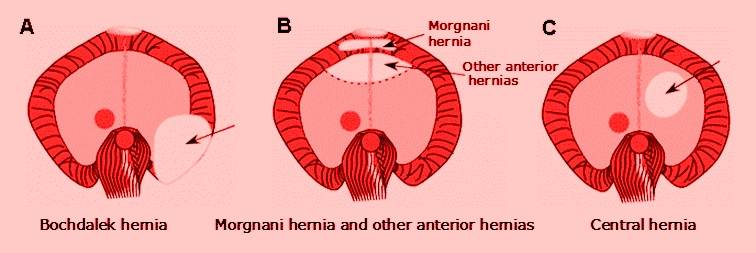
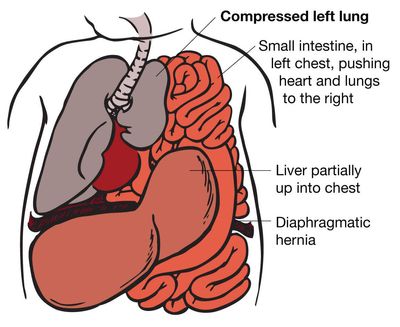
herniation of abdominal content through a diaphragmatic defect
bochdalek hernia (poeterolateral)
Impaired development and/or fusion of embryonic structures (pleuroperitoneal membrane) → defect in the diaphragm persists during development of fetus→ displacement of abdominal contents into the pleural cavity → compression of lung → pulmonary hypoplasia
mortality directly related to lung hypoplasia complcations
retrosternal hernia
pentalogy: omphalocele, inferior sternal cleft, ectopia cordis, anterior CDH, diaphragmatic pericardial defec
in 20%, most common cardial
most are born with respiratory distress (blue baby)
- tachypnea
- grunting respiration
- chest retractons
- cyanosis
⇒📷
- auscultation:
- diminished breath sounds on side of hernia
- deviated heart siunds
- bowl sounds on the affected hemithorax
- increased anterioposterior thoracic diameter
- echogenic mass
- absent intrathoracis gastric bubble
- mediastinal shift
- intrathoracic liver
- chest Xray:
- loops of air filled intestine within the thoracic cavity, absence of intestine in the abdominal cavity
- mediastinal shift
US → to check for other anomalies
(Cantrell pentalogy)
- acute GI symptoms → due to rotation and fixation
- cystic adenomaid malformations of the lung
- Intralobar sequestration
- Pleural effusion
- hyaline membrane disease
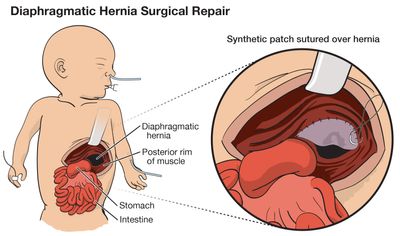
⇒ 📷
- cardioresp stabilization
- intubation, nasogastric tube
- operative approach through subcostal incision on affected side
- organs are pulled back into the abdominal cavity
- primary repair of the diaphragm defect (if too big, flaps might be needed)

survival rate ariund 50-60%
🌯gastroesophageal reflux as a long term problem
📈failure to thrive, growth retardation, 🚧bowl dismotility
- The most prevalent form of Congenital Diaphragmatic Hernia (CDH) is the postero-lateral left diaphragmatic hernia, also known as Bochdalek orifice.
- The prognosis and outcome are largely influenced by the extent of lung hypoplasia.
- There is a high mortality rate in the perinatal period.
- Approximately 10% of cases are detected beyond the perinatal period.
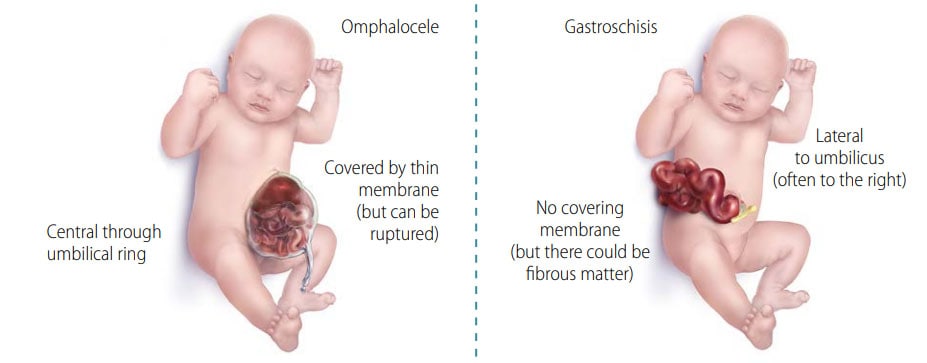
gastroschisis ans omphalocele
herniation of abdominal wall content through an abdominal anterior wall defect at the base of the umbilical cord
at the base of the umbilical cord, the herniated organs are covered by a membrane 📷
- other cranial fold defects
- anterior congenital diaphragmatic hernia, heart anomalies, defect of the pericardium, and sternal cleft, resulting Cantrell pentalogy
- bladder extrophy
- chromosomal abnormalities
- heart defects
- prenatal diagnosis via US
- large membrane covered bulge in the umbilical region
- larger than 5 cm → giant omphalocele
- small defect, less than 4 cm, only midgut → hernia of umbilical cord
- the sac can contain loops, somach, liver,spleen, large bowl
- umbilical cord is attached to the sac
- inner pertoneal layer
- outer amnion layer
the heart is in the sac through a defect in the pericardium and the central part of the diaphragm (plus sternal defect and heart defect)
when the omphalocele is ruptured →makes it difficult to distinguish from gastroschisis
- nasogastric tube to decompress bowl and stomach
- rectal examination, meconium evacuation
- oxygen
- antibiotocs and Vit K
- monitoring
- sac os prepared with antiseptic solution
- cord detached
- operative closure
- goal should be fascial closure
- if that isnt possible → skin should be closed over the viscera
- sometimnes flaps are needed
Grob technique → sac get painted with antiseptic solution when operative closure is not possible
- in primary closure: ventilation assistance
- monitoring of intraabdominal pressure via a central venous line → perenteral nutrition
herniation of abdominal content through a defect of the abdominal wall 📷
- young maternal age
- alcoholism and cigaretts during pregnancy
>10% of gastrochisis children present with other anomalies
- most common anomalies associated:
- chromosomal abnormalities are rare
- often respiratory problems and premature birth
→ small bowel atresia

- diagnosed via US 12-14 weeks after gestation → bowel loops floating in the amniotic cavity
- defect right to the umbilicus → 1-4 cm diameter
- defect is seperated from the base of the umbilical cord
- untestines are dilated → covered by a fibrin peel, NO OVERLYING MEMBRAINE

Well you pretty much see it right after birth 🌝
⇒ prevent fluid loss (large exposed surface), resp support, temp preservation → place baby after birth in a “plastic drawstring bowel bag” 📷
ASAP after birth → the longer you wait, the mor edematous the loops will becom → more difficult to replace
- primary closure, somtimes flaps are required
survival rate 80-90%, associated conditions are cause of morbidity and mortality
- Both omphalocele and gastroschisis are congenital malformations that can lead to significant morbidity and mortality.
- Omphalocele is often linked to heart and chromosomal anomalies.
- Gastroschisis is commonly associated with bowel atresia and perforation.
an aquired inflammatory disease affecting the gut of newborns
- prematurity
- enteral feeding
- perinatal events causeing hypotension, hypovolemia, hypoxia
- patholocig bacteria growth
sudden change in general status, signs of physiological instability in orally fed children
no, clinical findings inlude:
general:
- lethargy
- temperature instability (aka fever)
- apnea
- hypoglycemia
abdominal:
- distension
- tender
- vomiting/diarrhea
- rectal blood
- abdominal tenderness
- palpable bowl loops
- edema
- erythema

Stage I: suspected NEC
- lethargy, distended abdomen
- Nausea & vomiting
- bradycardia, apnea
Stage II: proven NEC →local peritonis
- Stage I +
- bloody stools
- Visible bowel loops lacking peristalsis
Stage III: Advanced→ perforated peritonitis + sepsis
- multiple organ failure
- sepsis,
- perforation
- pneumoperitoneum



- monitoring
- decompression of GI tract (NG Tube)
- IV nutrition
- fluids + AB
→ until recovery of complete peristalsis
just before perforation or necrosis 🤡
stabelized patient, but lets face it, thats unrealistic if your facing necrosis or perforation
only resect perforated or necrotic tissure
saline lavage
malabsorption, short bowl syndrom, delayed development
- Diagnosis and the timing of management remain challenging to determine.
- There is significant morbidity and a high mortality rate associated with this condition.
- In the initial stages, conservative treatment is typically preferred, but if pneumoperitoneum occurs, laparotomy is needed.
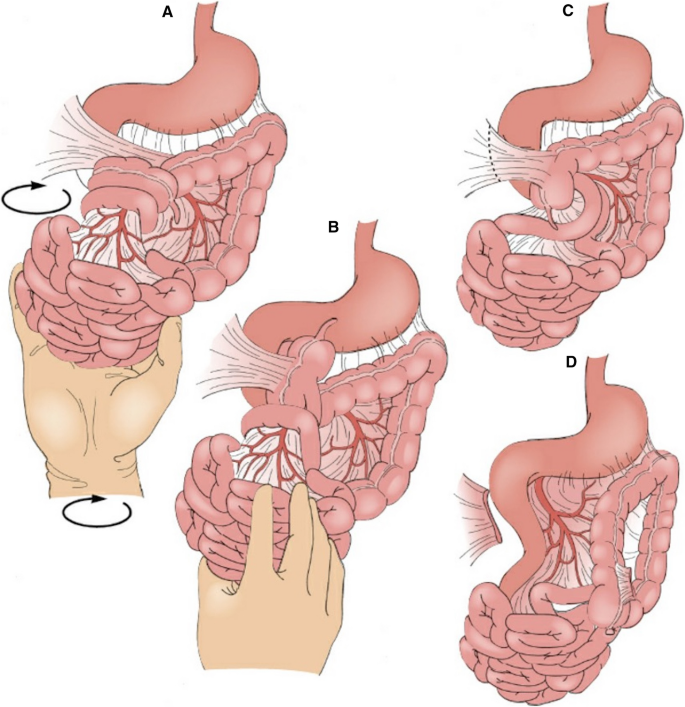
rotational anomalies of the intestine, used to describe nonrotation, incomplete rotation, errors of intestinal fixation
non-rotation:

A twisting of an intraperitoneal loop of intestines around its mesentery, which causes strangulation of the blood supply and mechanical bowel obstruction → “catastrophic” complication of malrotation
- >2yrs of age
- chronic vomiting
- intermittent colicky
- constipation
→ lymphatic and venous obstruction
- sudden onset
- bilious vomiting in aprev. healthy infant
- complete int. obstruction→intestinal ischema, abdominal distension
- hypovolemia and shock
- bloody stools
- met acidosis
- in neonates and infants
- extrinsic compression of the duodenum
- abdominal pain
- vomiting
- plain abdoinal xray
- contrast radiography

- US
- Abdominal CT
Xray:
- distended bowl loops
- air fluid levels → non specific
US:
- vascular flow with doppler
CT:
- whirlpool sign (twisted bowel) 📷
volvolus is a surgical emergency! 📷
- treat hypovolemia, dehydration and electrolyte loss
- nasogastric tubre for decompression
- parenteral AB
LADD procedure: 📷
- Untwist the bowel in a counter-clock wise direction
- Divide Ladds band (peritoneal band that cause extrinsic duodenal
- Straighten the duodenum
- Broaden the mesentery
- Remove the appendix (to prevent problems of diagnosis)
- Establish a non-rotation configuration placing the small bowel on the
- Cecopexy and duodenal fixation sutures are no longer necessary, since
obstruction)
right side of the abdomen with the duodenum along the right side of the abdominal wall and place the cecum and colon in the left quadrant
studies proven that they can cause later volvulus
- Malrotation is a congenital condition that is challenging to diagnose and can lead to chronic midgut volvulus, acute midgut volvulus, and duodenal obstruction.
- The most severe complication of malrotation is midgut volvulus, which constitutes a genuine emergency due to the risk of bowel ischemia and necrosis.
invagination of intestine into the lumen of the adjacent distal intestine, most frequent between 2 month -2 years of age, most common cause for intestinal obstruction 📷
two peaks in incidence: autum and spring→ increase of viral gastroenteritis and upper respiratory tract infections during these times
- <10% have a recognizable lesion as a cause→ so its idiopathic

- The intussusceptum usually arises in the distal ileum and passes through the ileo-cecal valve into the colon 📷
intussusception progresses → distension of the entrapped small bowl → compression of the mesentery, venous congestion, arterial flow impairment → bowl wall edema → bowl necrosis and perforation → peritonitis
- sudden onset
- colick abdominal pain
- pain followed by vomiting (initially non-bilious = non-complete obstruction)

- vomiting is followed by passage of bloody mucus stool
→ complete triad of vomiting, bloody stool and colic is only seen in 1/3 of patients
Currant jelly stool:
Dark red stool resembling currant jelly 📷 may be noticed in the passed stool or during a digital rectal examination, typically as a late sign.
→ mixture of sloughed mucosa, mucus, and blood. It often indicates longstanding invagination with bowel ischemia.
sausage shapes mass in the right upper abdomen
emptiness in the right lowe quadrant (dancers sign) → coz terminal ileum ind ileo cecal valve moved up
- Gastroenteritis
- rectal prolaps
- meningitis
- nasogastric tube (prevent aspiration)
- central line (Tx dehydration)
- AB therapy
enema → straight catheter is insterted, sometimes enema reduction of the invagination is sucessful (70-80%)
#1 air enema
#2 saline or water-sol. contrast
indicated :
- if enema redution fails

- peritonitis
- lead point supicion
procedure:
- milking technique: pushing on the apex of intussusceptum, rather than applying proximal traction, which is forbidden, due to the risk of perforating ischemic bowel.
- then inspection for vitality of the bowls
- if necrotic → resection
complete obsturction/absence
T
Trisomy 21
failure of recanalization of the duodenal lumen in the dirst week of gestation
3 different types
Type 1
- Type 1:
- mucosal diaphragmatic membrane
- intact muscle wall
- proximal duodenum dilated, distal part narrowed
- Type 2:
- short fibrous cord connecting the two ends of the atretic duodenum
- intact mesentery
- Type 3:
- complete seperation of the two ends
- annular pancreas 📷

- cogenital heart disease
- malrotation
- genito-urinary anomalie
- anorecrtal
- polyhydramniosis
- fuild filled stomache (sono)
- dilated duodenum (Sono)
- onset of vomiting after a few hours (billous)
- Dehydration
- If unrecognized → ulcer + aspiration pneumonia

- feeding intolerance
- NO abdominal distension (actually might be present)
- meconium passage might be possible (esp if only stenosis) but delayed
atresia will be diagnosed rather quickly because no passege at all possible, while a stenosis might be tolerated for a while
- Abdominal Xray (pot. contrast)

- Ultrasound
- Endoscopy
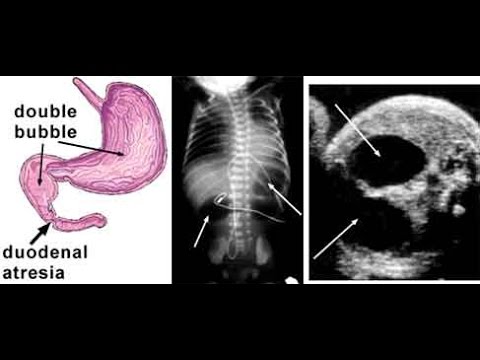
- double bubble sign in Xray
- dilated stomach in Sono, absence of air distally (to obstruction)
- Pyloric stenosis
- small bowel stresia/stenosis
- meconium ileus and peritonitis
- midgut volvulus
- extrinsic duodenal obstruction
- nasogastric tube for decompression
- central actheter line for parenteral nutrition
- if a thin web is the reason for obstruction (seen in type 1) → cautery
- Bypass
- duodeno-duodenostomy
- duodeno-jejunostomy
- right upper quadrant incision or midline longitdinal
- exploration
- right colon and hepatic flexure are mobilized
- obstruction bypass is created → side to side anastomosis
- diamond shaped incision is preferred
- in annular pancreas → DONT resect the ring tissue! ALso suitable for anastomosis

- total parenteral nutrition is continuied
- nasogastric output monitored
oral feeding after a few day, when nasogastric tube output is clear
- up to 90%
- most death associated woth other anomalies
- Duodenal atresia: Type 1 is the more common variant.
- Duodenal stenosis can be challenging to recognize.
- Approximately 85% of patients will experience bilious vomiting within the first few hours after birth.
- A pathognomonic sign is the presence of a double-bubble appearance.
- Surgical treatment is required.
- About 30% of patients with duodenal atresia present with Down syndrome, and they often have associated heart malformations.
Jejunum and ileum —> Jejunu-ileal atresia/stenosis the most common congenital anomalies causing intestinal obstruction in neonates
atresia! 95%
T
distal ileum
Grosfeld classification
- Type 1:
- mucosal atresia, intact bowel wall, intact mesentery
- Type 2
- blind end seperated by a fibrous cord, intact mesentery, normal bowl length
- Type 3
- Type 3a 🥇
- blind ends, seperated by a V shaped defect, shortened bowl length, proximal not peristaltic segment → most common Type!
- Type 3b
- christmas tree deformity: proximal atresia near the ligament of Treitz, large mesenteric defect, fore shortened bowel.
- The blood supply of the distal bowel is supplied in a retrograde fashion by arcades from ileocolic, right colic or inferior mesenteric arteries
- Type 4
- multiple atresias, string of sausages appearance
- polyhydramnios
- dilated small bowel loops
- bilious vomiting after attempted feeding

- abdominal distension
- respiratory distress
- most newborns fail to pass meconium
- jaundice

- abdominal X ray
- the further distal the atresia, the more apparent the abdominal distension → the greater the number of distended loops
- constast enema
- abdominal US
- Xray: few air-fluid levels, no further gas beyond the atresia
- enema: microcolon/level of obstruction, position of the cecum, possible anomalies of intestinal rotations
- Meconium Ileus
- Hirschprung
- Colon atresia
- Maltotation and midgut volvulus
- adynamic ileus
- sepsis
- hypothyroidism
- meconium peritonitus
- narotic addition in the mother
- dehydration signs
- aspiration pneumonia
- perforation of proximal small bowel → peritonitis
orogastric tube is placed → fluid ans electrolyte repletion
- right UQ, transveres supraumbilical incision
- abdominal exploration
- resection of the affected bowl
- side to side anastomosis
- distal bowl should be evaluated for atresia by saline solution passage

- temporary enterostomy (4-8 weeks)
- parenteral nutrition until bowl function is restored
- in cae of ileostomy → feeding as soon as stoma function is noticed
overall survival 80%
- increased mortality in type 3b
- biggest complication is short bowl syndrome after surgery → failure to thrive
- Diagnosing small bowel atresia can be challenging, as it may resemble other causes of neonatal obstruction.
- The main clinical findings include vomiting, abdominal distension, and a failure to pass meconium.
- The most significant long-term complication is the development of short bowel syndrome.
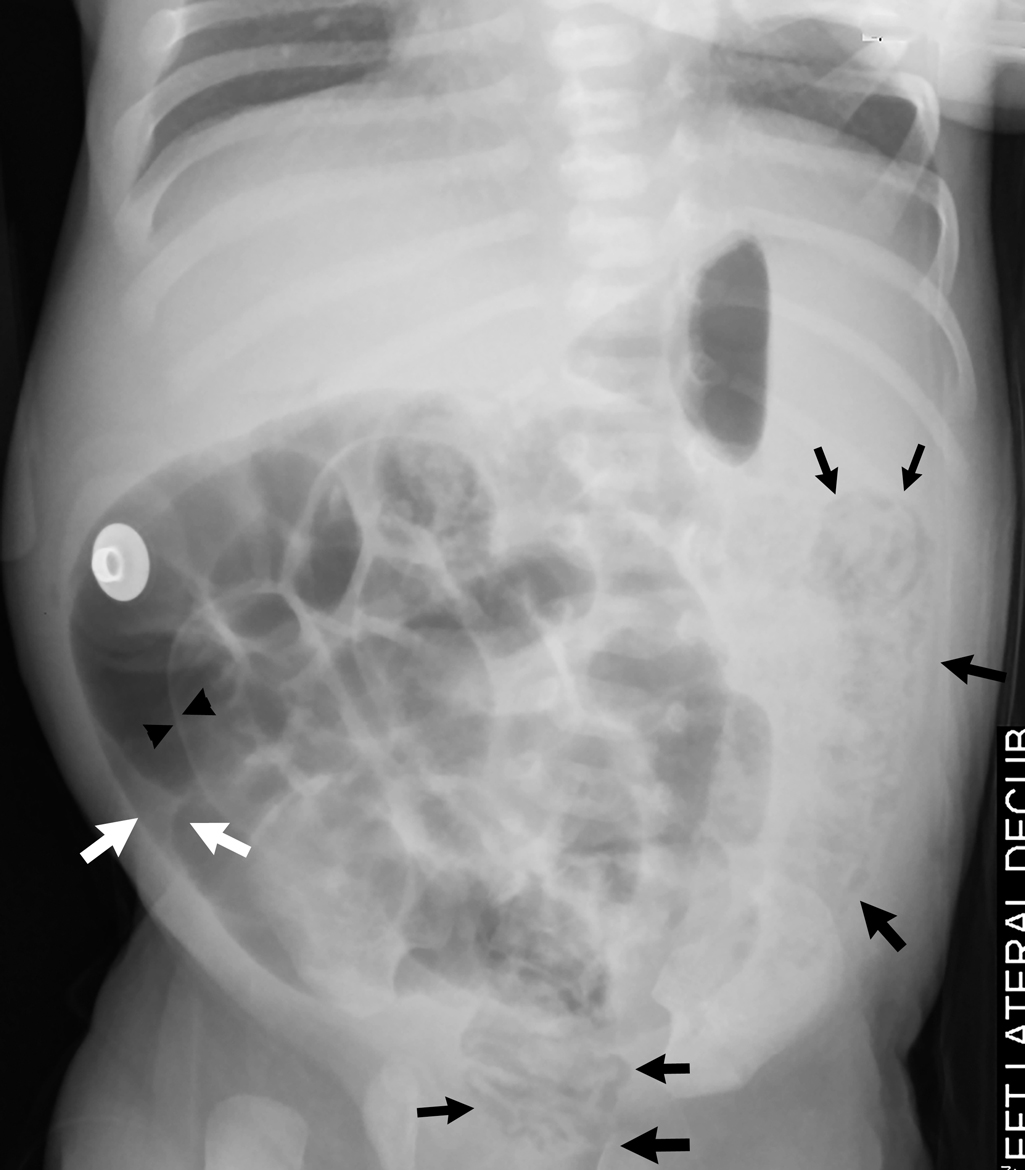
a small bowel obstruction at the terminal ileum, caused by very thick intraluminal meconium
cystic fibrosis
(CF)
inguinal hernia,
hydrocele,
cryptochidism

immerditely at birth
- abdominal sitension
- failure to pass meconium
- feeding intolerance
- bilious vomiting
- volvulus
- ischemia
- bowel necrosis
- perforation → Meconium peritonitis
(Can present Intra-Uteral or post natal)
- intraabdominal clacifications
- peritonitis signs
- erythema
- edema
- sepsis
- abdominal distension → can cause resp distress
- non bacterial peritonitis
- during intrauterine life
- result of bowl perforation and peritoneum contaminoation wth mecomiun
→ superinfection can occur after birth due to GI colonialization
Visualization of obstructive ileus + peritoneum
- X ray of admonen
- US
- contrast enema
Xray: 📷
- dilated air filled loops with air fluid levels
- soap bubble appearance in terminal ileum (neuhauser sign)
US:
- air filled bowel loops
Other causes for obstruction in newborns
- small bowl atresia
- malrotation/vovlvolus
- hirschsprung
- microcolon on contrast enema 📷 →Small bowl atresia/hirschsprung
- suction rectal biopsy → hirschsprung diagnosis
CF diagnostic workup
in uncomplicated MI
use of hyperosmolar water soluble radiopaque solution (Gastrografin) to drag water into the bowel lumen and soften the meconium → easier to pass
or warm saline enema
+- decompression + AB
in complicated MI or failure of non operative treatment
- enterostomy → either try to milking/irrigation to push distally or evacuation through enterostomy
- temporary stoma → irrigations
- bowel resection (esp in complicated)
- When encountering a newborn with bowel obstruction, it's essential to consider conditions such as Hirschsprung's disease, ileal atresia, meconium ileus, meconium plug syndrome, and volvulus.
- A water-soluble contrast enema serves as both a diagnostic and potential therapeutic tool, particularly in cases of meconium ileus.
- If the enema fails to relieve the obstruction, a laparotomy becomes necessary.
- Meconium ileus is almost always associated with cystic fibrosis, necessitating genetic testing to rule out this condition.
persistence omphalo-mesenteric canal (aka vitelline duct)📷
contains all layers of small intestine
ectopic tissue → most often gastric mucosa + parietal cells
when complications occur
rarely (5%) symptomatic
- Bleeding
- Bowel obstruction (due to volvulus, intussusception )
- pain
- vomiting
- abdominal distension
- Ac. diverticulitis (older children)→ Perforation
- abdominal pain
- nausea + vomiting
- fever
- ↑Leukos
- Ulcer (on ectopic gastric mucosa)
T
stenosis at diverticular head → stasis → diverticulitis
Bleeding → for DD with bleeding from other source
symptomatic diverticulum
- peritonitis
- occulusion
- profuse bleeding
PPI or H2-blocker
ulcer bleeding from ectopic mucosa
last 80-100cm of ileum
(note: to be sure, <60cm is the most common distance
Fecaloids or lymphoid hyperplasia(due to viral infect) → obstruct appendix (CLOSED LOOP OBSTRUCTION) → secondary bacterial infection
other causes : undigested seeds, pinworm infection
obstruction → continous secretion of appendiceal mucosa → ↑intraluminal pressure → distension → pain
→ rapid multiplication of local appendix bacteria → edema, hyperemia, pentration through mucosa = catarrhal appendicitis
→ spreads to serosa + peritoneum(locally) → Pain illiac fossa → Mc-burney's +
→ phlegmonous phase → enlarged congested, purulent fluid on serosa + thickend mesoappendic
→ compression arterial blood flow → necrosis = gangrenous appendicitis
⇒ perforation
→ appendicular abcess,
→ appendicular block,
→ diffuse peritonitis (Rebound tenderness)
VERY RARE IN NEONATES!
if occurs → CF or Hirschprungs
sudden or progressive and ↑Intensity (esp with effort)
epigastic/periumbilical → 4-6h: RLQ
⇒variations= but can also be periumbilical, right flank, right hypochondrium or pelvis
first sub-febrile (<38°)
→ hours-days → perforation or abcess → 38.5-39.5°
- constant anorexia
- nausea + vomiting (vomiting doesnt relieve nausea)
- fever+pain
- Right illiac fossa tenderness
- Mc Burney's point 📷
- Blumberg's sign = rebound tenderness (irritation perietal peritoneum)
- Rovsing's sign - palpation LLQ → pain RLQ 📷
- Psoas sign 📷
- Obturator sign 📷
- Voluntary + involuntary guarding(peritoneal irritation)
- Grassmann Mendel's (Bell sign)
- Antalgic position
- Cutaneous hyperesthesia
children
→ 🦪 Meckels + Intussiception
→ 💩gastroenteritis + IBD
→ 🥐UTI, hydronephrosis, pyelonephritis, stones,
→ pancreatitis, pneumonia
→ trauma / tumor
- Appendicular block (= appendiceal mass)
- Appendicular abcess
- Diffuse peritonitis
→ adhere to cecum,ileum, omentum (3days after onset) due to inflammation+fibrosis
→ AB-therapy→ regression (after 7-10d)
→ after 4-6month appendectomy
→ might develop into abcess or generalized peritonitis:
→ transformed from appendic. block
→ AB + drainage (percut or laparotomy)
→ later appendectomy
→ due to direct perforation, or abcess perforation
→ peritoneal lavage, drainage + AB
→ later Appendectomy
- young: underdeeloped omentum to block perforation → fast generalized peritonis
- LAB:
- Leukos ↑
- Urine analysis → DDx kidney patho (ex. Urosepsis)
- US → thickend (>6mm diameter), peri-apendiceal fluid, DDx genital+urinary pathologies
- CT → if US Ø conclusive
⇒ “target” sign of appendicitis 📷
Either classic or laproscopic appendectomy
classic →McBurney incision
laparoscopic → 3 trocars
- intraperitoneal examination
- free appendix from cecum
- ligation + transection mesoappendix
- ligation + transection of appendix base
- remove appendix + close wound
generally good when correct + early Dg
(watch out in neonates + immunocompromised → ↑sepsis-risk)
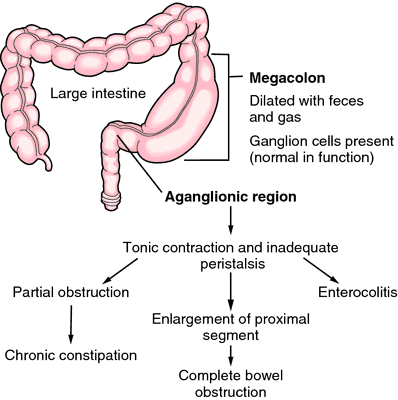
defection caudal migration of parasympathetic neuroblast (from neural crest to distal colon)
→ absent Meissner + Auerbach plexus:
→ beginning at anorectal line upwards (usually involving rectosigmoid region)
↓
⇒ uncoordinated motility ⇒ ↓motility
⇒ spastic contraction → stenosis / functional obstruction
⇒ Dilation prox. to aganglionic segment ⇒ !possible megacolon
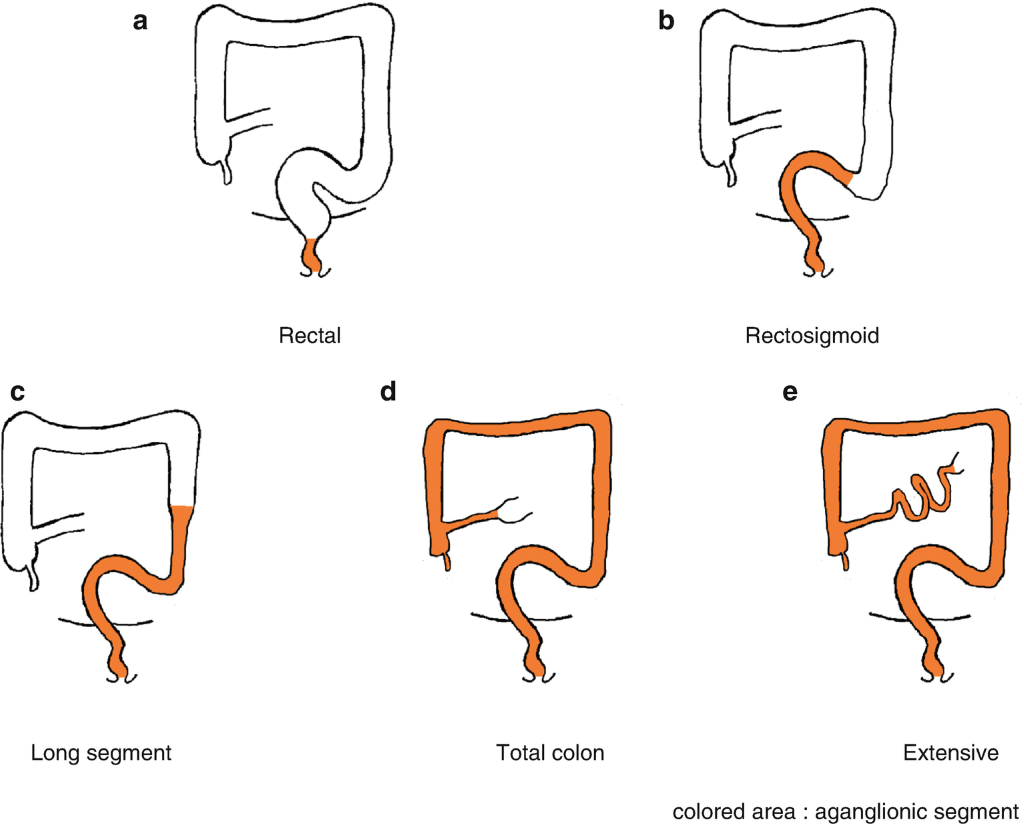
Types:
- Ultrashort (rectal)
- Short (Rectosigmoid)
- Long segment
- Total colonic
- Extensive
Ultra-short segment: limited to distal rectum (below pelvic floor + anus) Short segment: limited to rectosigmoid region (🥇 80% of cases) Long segment: involvement of distal colon until splenic flexure (10% of cases) Total colonic: entire colon affected (<10% of cases)
- DISTAL OBSTRUCTION SIGNS
- Delayed passage of meconium (>48h)
- DRE SIGNS
- tight sphincter (spastic contraction)
- empty rectum (no stool passage)
- squirt sign (explosive release of stool + air after finger removal)
Meconium is passed in the first 48 hours in 99% of healthy term newborns → If no stool passed→ exclude Hirschsprung!
→ Distal intestinal obstruction = abdominal distension + bilious vomiting
- other causes of obstruction:
- atresia
- meconium ileus + plug in
- hypothyroidism + uremia
- Xray: 📷
- narrow distal colon segment (with ↓air)
- dilated proximal segment
- Ano-rectal manometry → absent relaxation reflex of internal sphincter after streching rectum
- Biopsy = definite Dgx
- suction rectal biopsy
- full thickness
distal obstruction
⇒ workup with: Barium enema → localize + determine lenght of transitional segment 📷


→ Øganglions + ↑AchE
- Hirschsprungs-associated enterocolitis
- Fecal incontinency
- Urinary dysfunction (bladder + urethra compression due to megacolon)
⇒ toxic megacolon (pain, fever, foul-smelling + bloody diarrhea)
⇒ ⚠️ risk of sepsis + perforation(→peritonitis)
- iv fluids
- nasogastric decompression
- broad spectrum AB (prevent toxic megacolon)
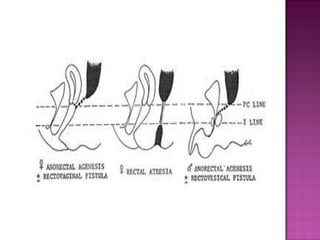
Males | Females |
Perineal fistula | Perineal fistula |
Recto-urethral fistula (Bulbar, prostatic) | Recto-vestibular fistula |
Recto-bladder neck fistula | Persistent cloaca |
Rectal atresia | Rectal atresia |
Imperforate anus without fistula | Imperforate anus without fistula |
Down syndrome
>50% have one or more abnormalities
- ❤️cardiovascular defects
- 💩GI defects
- 🎍Vertebral anomalies (hemisacrum)
- 🥐🥜Genito urinary anomalies
- Gynecologic anomalies
Cardiovascular defects: PDA, ASD, VSD, Fallot tetralogy, transposition of great vessels Gastrointestinal anomalies: duodenal obstruction, esophageal atresia, Hirschprung's disease Vertebral anomalies: hemivertebrae, hemisacrum, myelomeningocele Genito-urinary anomalies: vesicoureteric reflux, renal agenesis, renal dysplasia, hypospadias, cryptorchism Gynecologic anomalies: bicornuate uterus, uterus didelphus, vaginal septum, vaginal atresia
recto perineal fistula
recto urinary fistula
- Upside-down Xray aka Wangensteen-Rice 📷 (after 24 h, before rectum is collapsed) –> evaluate for hemisacrum (–>MRI)
- US and ECG to see other abnormalities
Postbone at least 24h to identify fistulas (give the meconium time to pass)
But if urethral: protective colostomy & delay surgery 3–4 month

– Iv fluids
– AB
– nasogastric decompression
anoplasty
Give AB & Dilation schedule (prevents stenosis)
good bowl control can be achieved in 75% of patients
- strictures – constipation, megasigmoid
- Fecal incontinence
- Anorectal malformations (AMR) are highly complex defects that require various types of management and can lead to different outcomes.
- Surgical repair should be delayed by at least 24 hours to allow for the identification of fistulas.
- In girls with AMR, the most frequently observed finding is rectovestibular fistula.
- In males with AMR, the most common finding is rectourethral fistula.
T
T
- in children are intra-abdominal organs (liver and splee) are exposed beyond the thoracic cage, less protected → vulnerable to traumatic external forces
- The abdominal wall musculature is less developed in children, and less able to protect abdominal content
- Compared with adults, the diaphragm is more horizontal and the liver and spleen are more anterior and less protected by the ribs, which are easily compressible, crushing the organs underneath
- Retroperitoneal structures such as kidneys and pancreas lie only a short distance away from the anterior abdominal wall in thin children, making them prone to injuries
- The liver occupies a relatively large percentage of the abdominal cavity, further exposing it to injury
- direct blow (esp if crushed betw force and spine)
- Dilaceration GI-tract
frequent causes are:
- pedestrian hit, car crash, lab belt injuries
- bike accidents → handlebar/pushed off
- falling
- skiing/other sports
- agression+abuse
cullens sign/turner sign 📷→ intraabdominao/retroperitoneal injury
- pain and tenderness LUQ → radiating in the left shoulder
- Bleeding signs
- abdominal distension
- tachycardia (shock)
- rib fractures
- pain → right shoulder
- tenderness
- Bleeding signs
- abdominal distension
- pallor
- high mortality and eraly mortality
- Pain
- abdominal pain
- lower back pain
- hematuria
- difficulty urinating
in lab belt injuries
- blood from the urethra/gross hematuria
- intraperitoneal fluid
- absence of voiding (anurie?)
→ mesenteric avulsion, enterostomy, bowel transection
easily be missed, no clinical findings sometimes
rare
- handle bar injuries (crashes pancreas against vertebral column)
- asymptomatoc until destructive effects of enzymes
- raised derum amylase
- acute pancreatitis management
- FAST US
- CT
- Peritoneal lavage
- Laparoscopy
- in hemodynamic stable children
- blunt injuries
penetrating injuries
continued blood loss → hemodynamic instability
peritonitis
middle abdominal incision
- Control of active bleeding
- Suture repair or partial resection of injured organ
- Organ specific:
- 💩
- Protective ileostomy or colostomy
- Attempts of splenic salvage (wrapping of the damaged organ)
- Ureteral stenting, percutaneous nephrostomy
- Selective embolization
- Foley catheter drainage for small bladder injuries (contusion)
- Pyloric exclusion or gastro-jejunostomy for severe duodenal injuries
- many ingested objects lodge at the cricopharyngeal muscle
- Objects larger than 2 cm and longer than 3 have difficulties traversihg the pyloric chanel
small stony concretion which may form in the stomachs/GI trackt → often made of vegetable matter/hair → can cause obstruction
- often unrecognized
- if eosophagus obstructive:
- sudden onset of couching
- restrosternal pain
- drooling
- poor feeding
- chocking
X ray
Abdominal US
CT
- #1 observation 24-48h
- most object don’t have to be removed exept sharp/magnets/batteries
- open laparotomy and manual extraction
- bezoars endoscopical elimination
- tissue necrosis from electrical discharge
- toxin release (mercury poisoning)
- direct caustic injury → severe local complications:
- esophageal perforation
- Fistula
- trachea-esophageal fistula
- aortoesophageal fistula → lead to mediastinitis, hemorrhagic shock and sudden death
emergency endoscopy 🔦
(Like bezoars)
- Ingestion of foreign bodies (FBs) in children often goes unnoticed and may remain asymptomatic.
- However, ingestion of batteries can lead to very severe complications, including a significant risk of mortality.
Uro-genital
- abnormal location + size of urethral meatus
- associated with other anomalies of penis
⇒ on ventral surface of penis proximal to end of glans
(can be located from glans to scrotum to perineum)
⇒ very small

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
F → pretty common (1 out of 250-300 births)
- 🥜Testi shit: Inguinal hernia + undescended testicle
- 🧬 Intersex state (genetic disease) → assoc. with undesc. testicle, micropenis, bifid scrotum ⇒ genetic tests + karyotyping
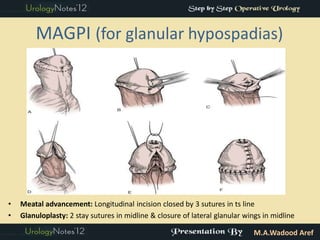
- Placing meatus on tip of glans
- New uretra that reaches meatus
- Glans-plastic: Form symmetric cone-shaped glans
{kind=link}
{kind=link}
{kind=link}
CLASSIC COMPLICATIONS
- early:
- bleeding
- infection
- late:
- fistula,
- stenosis (meatus + urethra)
- persistent chordee
⇒ complication may require multiple surgical corrections
BUT delay surgical corrects until 6m after initial surgery
(try to complete surgical corrections until 2-3y of age to prevent psychological problems)
at age 2-3

- Hypospadias is a frequently encountered condition in boys.
- Although proximal hypospadias is rare, it poses greater treatment challenges.
- The primary objective of surgical repair is to achieve a straight penis with the urethral meatus positioned at the tip of the glans.
- Management should be personalized and tailored to the specific anatomical type.
inability to retract the foreskin over the glans
⇒ 📷
{kind=link}
PHYSIOLOGICAL
normal adhesion betw. prepuce + glans → almost all become retractable by age of 3-4y Ø scarring, infection, trauma, or inflammation.
PATHOLOGICAL → due to SCARRING of prepuce
- True phimosis (scarred preputial orifice) → rare in first year of life
- Paraphimosis 📷
- Recurrent infections: Balanitis (glans) + Posthitis (prepuce)
- Balanitis xerotica obliterans

indications = Complications
⇒ Tx = circumcision
Trueee, bilateral in 15%
{kind=link}
{kind=link}
interuterine torsion of the spermatic cord → atrophy at the time of birth
but spermal cord ending blindly into inguinal canal → proof, that it was there
inguinal hernia (patent inguinal canal )
abdominal wall abnomalies (gastroschisis, bladder extrophy…)
Hypospadias
- identify the lowest position the testis will stay in without undue tension

- inguinal swelling → testis/hernia
- Abdominal, perineum and femoral region need to be checked for ectopic testis
→ to identify the position of undescended testis (Esp if non palpable)
- US (abdominal and inguinal)
- CT
- MRI
- laparoscopy
- anorchia
- retractile testis
- vanishing testis
- sexual differentiation disorder
- surgery (orchidopexy)
- at 6 month
- for palpable testis with adequate vessel length
- procedure: 📷
- incision over inguinal external ring
- testicular mobilization
- obliteratin of the processus vaginalis
- passage of the testis without tension into puch in the scrotum
- If high inguinal or Intra-abdominal
- Can’t be placed in scrotum bc too short vascular pedicule
- Multistage orchidopexy + collaterals
- testicular torsion (non-fixed)
- Infertility
- Testicular cancer
- An undescended testis is detected in approximately 3-5% of full-term male newborns.
- Undescended testes are at a higher risk for malignancy and may experience impaired spermatogenesis.
- In over 90% of cases involving undescended testes, a patent processus vaginalis is present and must be ligated during orchidopexy.
- Laparoscopy is a valuable tool for locating nonpalpable undescended testes.
{kind=link}
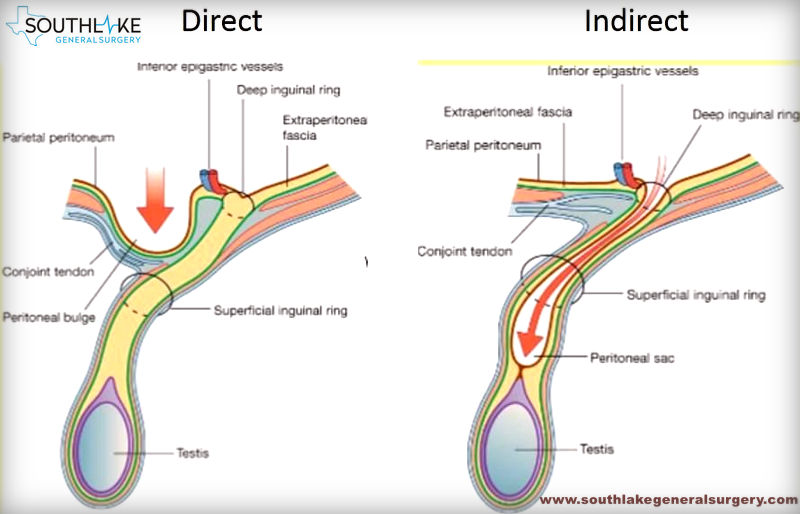
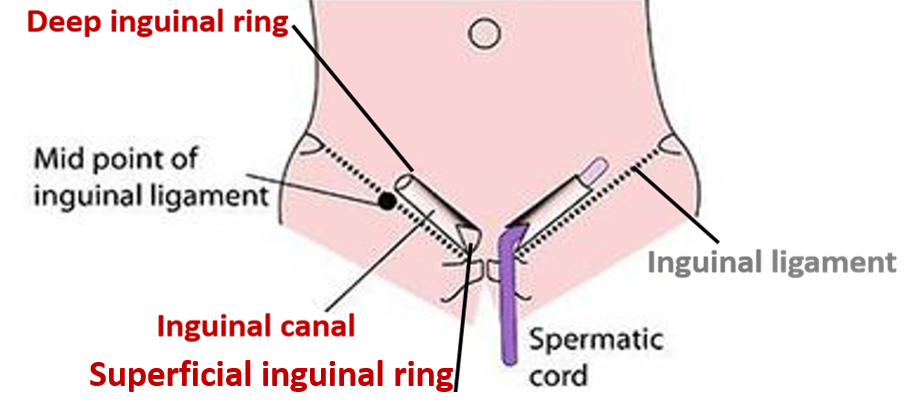
indirect → protrusion of abdominal/pelvic contents through deep (external) inguinal ring of inguinal canal
direct → protrusion of abdominal/pelvic contents through post wall of inguinal canal
indirect
F ⇒ typical patient is a male infant
(male:female = 10:1)
{kind=link}
{kind=link}
communicating hydrocele (descends into testicle → bowel loop is filled with peritoneal fluid ) 📷
{kind=link}
- Prematurity
- Undescended testis
- Abdominal wall disorders Gastroschisis / Ompahlocele
- Cystic fibrosis (+meconium ileus)
- Ascitis
- Connective tissue disorder
Groin swelling/mass (at deep inguinal ring)
- intermittent swelling
- ↑ in size when ↑intra-abdominal pressure
- ↓ in size when relaxed
- +/- extending into scrotum/labium: communic. hydrocele → transilluminates (”shines through”)📷
- communicating hydrocele → size changes depending on activity + posture
- non-communicating hydrocele → Ø influenced by activity

- Typically clinical diagnosis
- US
Other types of pathologies of theeeese nuts 🥜:
- reactive hydrocele
- varicocele
- testicle tumor
- testicular torsin
- scrotal traumatic hematoma
+ femoral hernia
strangulation / Incarceration 📷
{kind=link}
first year of life
If you aren't able to push the hernia back in, the contents of the hernia can be trapped (incarcerated / irreducible) in the abdominal wall. An incarcerated hernia can become strangulated, which cuts off the blood flow to the tissue that's trapped A strangulated hernia can be life-threatening if it isn't treated.

⇒ Obstructed hernia: intermittend pain
⇒ signs of mechanical bowel obstruction (sudden pain, vomiting, abdominal distension, constipation)
⇒ Strangulation📷 constriction of internal/external ring → cuts blood supply off (venous + lymphatic)
⇒ swelling of viscera ⇒ arterial compromise: gangrene + perforation of viscera (bowel, ovarian torsion+necrosis)
⇒ male: testis vascular compromise ⇒ testicular atrophy
⇒ female: ovarian torsion + necrosis ⇒ immediate surgery when ovaries are in hernia sac!! ⚠️
⇒ late signs: shock, blood in stool. peritonitis
- Inguinal hernia ⇒ Always Surgery
- laproscopic
- ligation of hernia sac
- in boys: take care of spermatic cord ⚠️
- hydrocele:
- <1y → resolves spontaneously (90%)
- >1y → surgery
- strangulated hernia:
- complications (signs of shock + peritonitis) ⇒ surgery
- Øischemic viscera signs ⇒ manual reduction
→ soon after Dgx (in premature wait until 2kg body weight)
→ if fails ⇒ surgery
- Recurrance of hernia
- Injury
- Spermatic cord (vas deferens) injury
- Testiscles
- swelling → resolves spontaneously
- testicular atrophy (if compromised blood supply)
- hematoma
- Bowel injury
- A hydrocele may resolve within the first year of life. However, if a fluid collection persists beyond one year, it indicates communication between the peritoneal cavity and the processus vaginalis, necessitating surgical intervention.
- Strangulation of a hernia is more frequent during the first year of life and can result in signs of intestinal obstruction.
- If an ovary is found within the hernia sac in girls, it requires immediate surgical attention.
{kind=link}
extravaginal torsion ⇒ perinatal period
intravaginal torsion = abnormal testicular fixation to /tunica vaginalis (bell-clapper deformity) ⇒ older childern

⇒ interruption of blood flow to testis + epididymus
⇒ 📷
{kind=link}
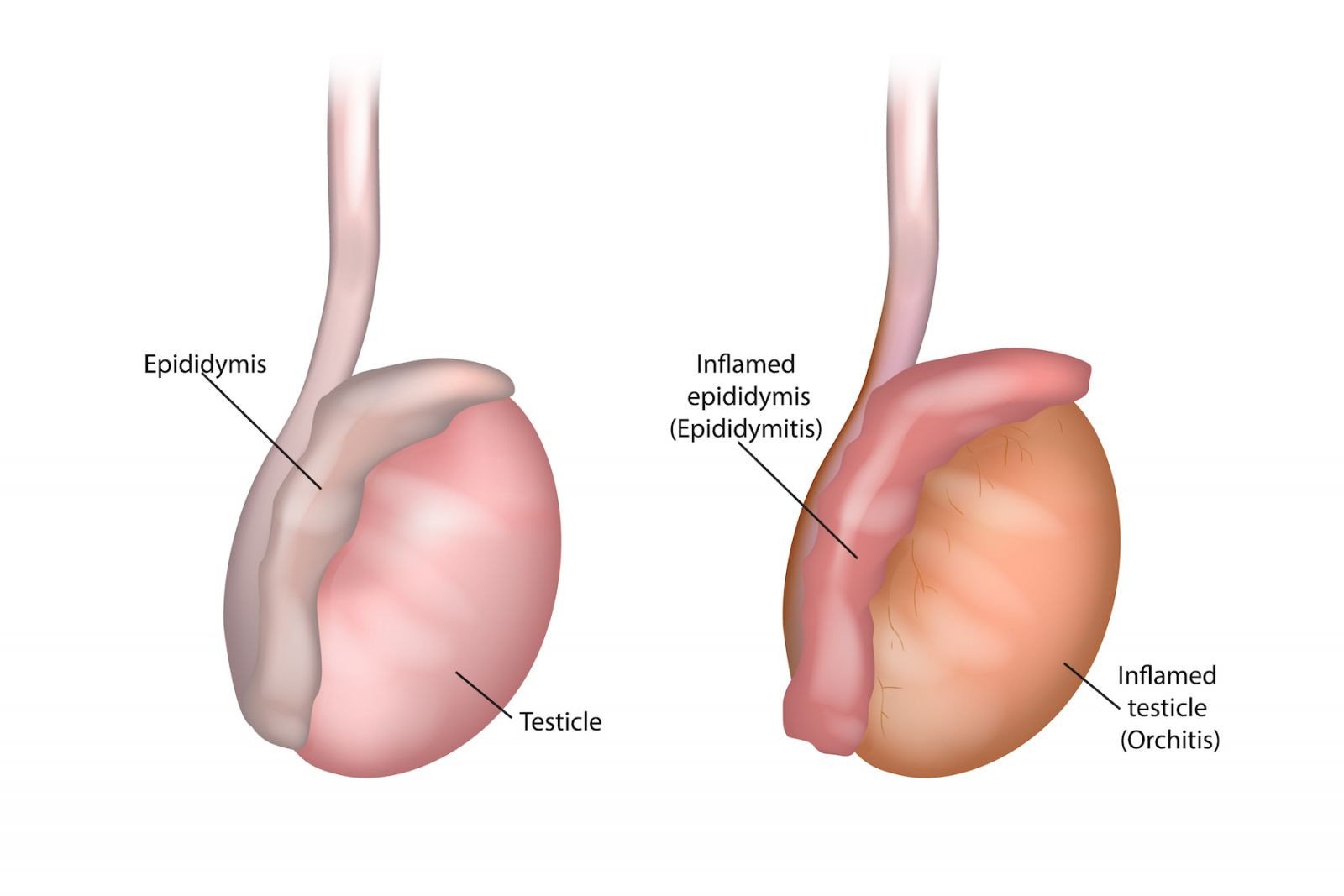
sexually active → chlamydia + gonorrhea
non-sexually active → urinary tract abnormality ⇒ reflux into vas deferens ⇒ chemical epiditimitis
uncommon in infants + young children ⇒ if present assoc. with 🦠 infectection (mumps)

Testicular torsion | Appendix torsion | Epididymitis | Orchitis | |
🎈 Scrotum | ↑size + tender
- elevated testis (diffic. palpate) | ↑↑size +tender
- tender mobile nodule in scrotum
+- blue dot sign 📷(necrosis) | ↑size + tender | tender
erythema + FEVER
|
🎇 PAIN | sudden
(might be abdominal - DDx appendicitis)
→ less apparent after necrosis occured (2d) | - ↑ w/ movement
(tend to not move)
- less intense than testicular | develop slowly (several hours/days) | ? |
🤮 vomiting | ✅ | ❌ | ||
🥜 cremaster reflex | ABSENT
(elevated scrotum) | normal | ||
✈️ Associations | secondary hydrocele (↑↑size) | - sex-acitve: DYSURIA + urethral discharge
- Øsex: assoc. with excessive straining during urination | MUMPS (or other viral infection |
⇒ look for testicular torsion
DOPPLER US
SURGERY → scrotal exploration:
Detorsion ⇒ look for viability based on color
if necrotic ⇒ remove
⇒ check contralateral side → bell-clapper deformity?
→ contralateral orchidopexy if:
- perinatal period (extra-vaginal)
- bell-clapper deformity (intravaginal)
orchidopexy:

- Symptomatic: Bedrest + analgetics
- prophylactic AB
→ if resistent pain or testicular torsion cant be excluded ⇒ surgical exploration + appendix removal
mild symptoms → oral antibitics
= viral ⇒ bed rest +observation
- If there is any uncertainty in excluding the diagnosis of testicular torsion, immediate scrotal exploration is necessary.
- Prompt diagnosis and treatment of testicular torsion are crucial for preserving the testicle and its role in endocrine function and fertility.