





Nephrology
Retrograde flow of urine:
bladder ⇒ Ureter + kidney
#1 Primary = short intramural ureter
⇒ Short intramural ureter → vesicoureteric junction (VUJ) fails to close completely during bladder contraction → VUR
(**normal VUJ ❗)
#2 Secondary = obstruction → ↑pressure
- anatomical (i.e. stenosis, post. urethral valves)
- functional (neuro / muscular)
- inflammation (UTI / cystitis / stones)
Grade | Reflux into | Dilation ureter + pelvis |
1 | Ureter | Ø |
2 | Ureter + pelvis | Ø |
3 | Ureter + pelvis | mild |
4 | Ureter + pelvis | mod. |
5 | Ureter + pelvis | sev.
(hydroneph, calyces + tortuosity of ureter) |
- asymptomatic
- Pyelonephritis → renal scarring → RF


see → UTI
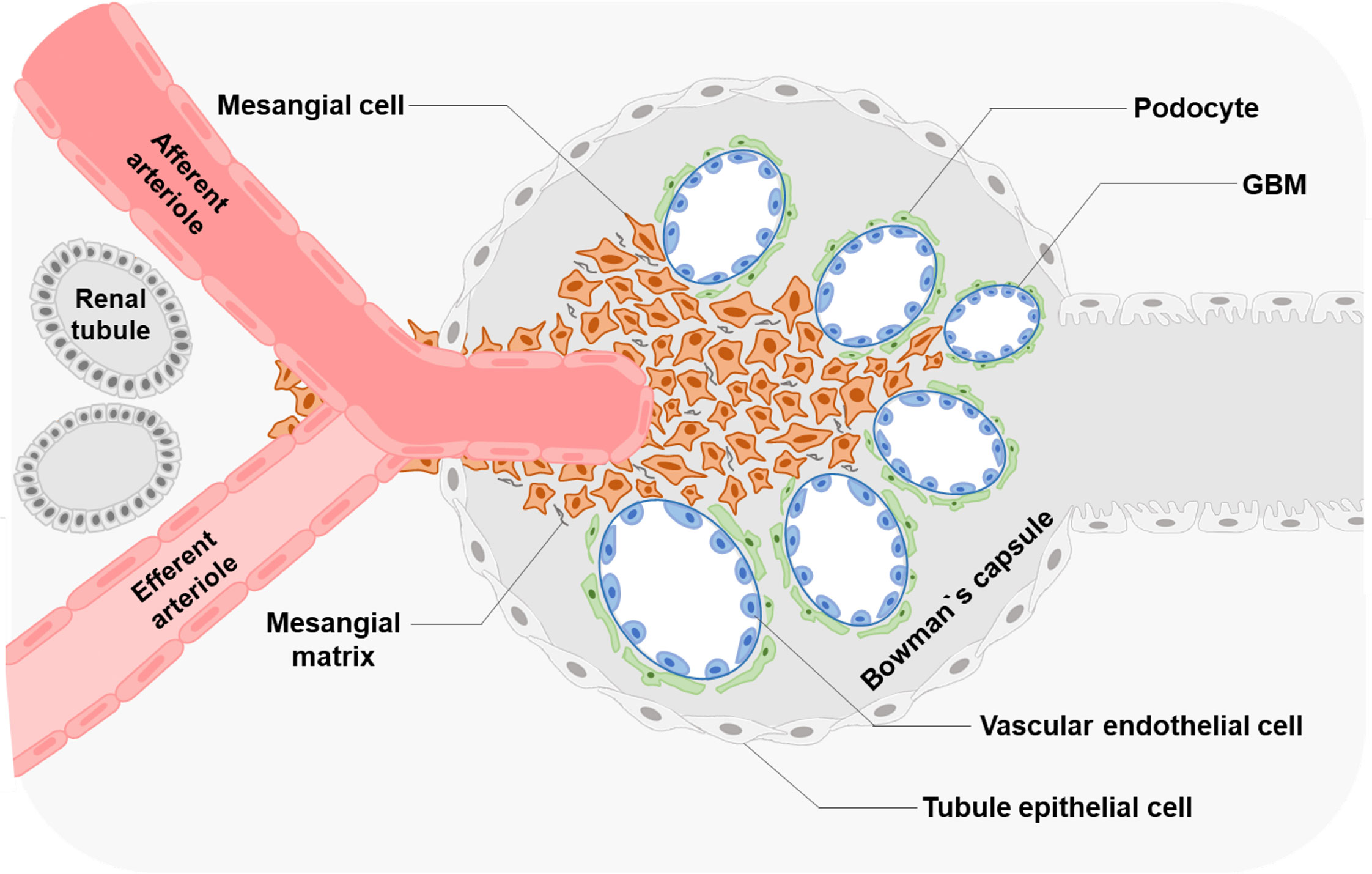
inflammation of glomeruli
⇒ mainly due to immun-complexes
⇒ NOT due to infection!
focal → some glomeruli affected
diffuse → all glomeruli affected
Segmental → part of glomerulus affected
global → entire glomerulus affected
- Hematuria (The urine looks smoky, and tea or cola colored.)
- Salt-retention ⇒ ↑BP + edema
- +/-Oliguria
+ Pyuria
- persistent proteinuria AND/OR hematuria
- RF within years
end stage RF within weeks
prior GAS infection (URT, skin) → Ag-Ab complex → deposition in glomeruli → Complement activation (↓C3) → Inflammation (acute GN)→ glomeruli damage → hematuria and other signs acute GN
F - only when indications are met (see later)
Unknown cause → IgA Immunoglobulin deposition in mesangial cells 📷
ØSystemic disease! (i.e. Henloch-Schönlein, SLE)
Probable mechanism: The synthesis of an increased number of defective IgA antibodies, often triggered by mucosal infections such as respiratory tract and gastrointestinal infections, leads to the formation of immune complexes that deposit in the kidney, resulting in glomerulonephritis.
T
(APSGN = secondary)
T
(histo findings → see later)
Disease | Post-infectious | Acute nephritic | RF |
APSGN | 1-6 WEEKS | ✅ | Acute RF |
Berger | 1-2 DAYS | ✅ | Rare - Acute RF,
→ progression end stage RF within 20-25y |
*acute nephritic sy = acute GN = hematuria, ↑BP, edema, oliguria
APSGN:
- child >3y (max inc. 5-15y)
- 1-6 w after GAS
- 50% asymptomatic
- Acute nephritic syndrome
- Acute RF (50%?)
- rare: nephrotic sy
Berger:
- (max. inc. 10-35y)
- VARIABLE PRESENTATION/EVOLUTION
- Recurrent (isolated) gross hematuria
- 1-2days after URT / GI infection
- assoc. with loin pain
- Persistent microscopic hematuria / proteinuria
- Acute nephritic syndrome
- CRF
- rare: acute RF, nephrotic sy

Method of urine collection
| Diagnostic threshold
|
Midstream girls
| 100,000 CFU/mL
10,000-100,000 FU/mL - repeat culture
|
Midstream boys
| 10,000 CFU/mL
|
Catheter
| 10,000 CFU/mL
1,000-10,000 CFU/mL - repeat culture
|
Suprapubic aspiration | Any number of CFU |
does Ø influence natural history ⇒ can be given to prevent spreading
Renal replacement therapy / kidney transplantation
Yes, but slow progression also nicht so schlimm lel
- IgA
- membranoproliferative GN
- chronic evolution (vs. self-limited)
- ↓ASLO (vs. ↑ALSO)
- More common with NEPHROTIC sy
- (both ↓C3 + gross hematuria)
Henoch-Schönlein purpura (IgA vasculitis)
(+benign familiar hematuria)
Parameter
Oliguria Macroscopic hematuria Elevated creatinine Hypertension Low C3 Proteinuria Microscopic hematuria
Duration
7-10 days 1-3 weeks 3-4 weeks 4-6 weeks 6-8 weeks 3-6 months 1-2 vears
Q. Which of the following statements about the evolution of acute post-streptococcal glomerulonephritis are true? a. disappearance of macroscopic hematuria in 1-3 weeks b. normalization of blood creatinine level in 3-4 weeks c. normalization of C3 level occurs in 6-8 weeks d. proteinuria disappears after 2 years of evolution e. disappearance of microscopic hematuria in 1-1.5 years
- Pure nephrotic sy.
- Impure nephritic-nephrotic sy.
→ nephrotic proteinuria (+++)
→ Hypoalbuminemia → Edema (+weight gain)
→ pure nephrotic + sings of glomerular inflammation (hematuria, ↑BP, ↑BUN)
Typical Features | Nephrotic Syndrome | Nephritic Syndrome |
Onset | Insidious | Abrupt |
Edema | ++++ (anasarca) | ++ |
Blood Pressure | Normal | Raised |
Jugular Venous Pressure | Normal/low | Raised |
Proteinuria | ++++ | ++ |
Hematuria | May/may not occur | +++ |
Red Blood Cell Casts | Absent | Present |
Serum Albumin | Low | Normal/slightly reduced |
in nephrotic edema starts periorbital; DDx in nephritic = gravity dependent-edema (legs first)
⇒ 📷

- infections (Ig loss)
- Relative Hypovolemia (due to ↓Albumin)→ ARF → Anemia (↓EPO)
- Thrombosis + ↑CV-Risk[ArtScl] (comp. Increase in fibrinogen + lipoproteins)
- Growth failure

minimal change disease
(max. incidence = 1-7y) ≤ 10 y → 90% of cases
≥ 10y → 50%
pure NS + normal renal function
→ nephritic components might be present
= Minimal change unlikely ⇒ DDx exclusion
- Age <1y OR >10y
- Impure NS
- ØResponse to steroids
- Frequ. relapses / CRF
- ↓C3 / ANA

- Steroids! ⇒ classification accoring to response
- Nephrotic syndrome sensitive to steroid therapy
- Nephrotic syndrome resistant to steroid therapy
- steroid dependent
- frequently relapsing
- Edema Tx
- Diet
- Sodium restriction
- NORMAL protein intake ❗
- Human albumin if
- albumin (serum) < 1,5g/dl OR
- anasarca (sev.+ generalized)
- ØDiuretics (predni has best “diuretic” effect)
- respiratory distress / GI symptoms
- after human albumin
- Ø response for predni
- Complications Management
- Infectious Tx (vaccination, + infection tx if occurs)
- DVT (mobilize, avoid hypovolemia, Øanticoagulation rountinely)

→ should be followed by iv diuretics
⇒except:
vaccination: pneumococcal + chickenpox
Hodkin's lymphoma → inc. cytokines
- VUR
- Obstruction: Disruption urinary flow
- foreign body (catheter, ureteral stent, nephrostomy)
- Neuro-muscular: neurologic bladder + sphincter abnormality
G- → E.coli, Enterobacter, Proteus
G+ →Enterococc(Klebs, Pseudomonas), StaphAureus
*most common - assiciated with infection outside hospital, others are nosocomial
- Neisseria gonorrhea
- clamydia
- staph + strep
dipstick (leukoC-esterase, nitrit)
Systemic signs | Specific signs | |
Pyelonephritis | High grade fever
Nausea + vomiting | Flank pain (giordano) |
Cystitis | low grade fever | -Dysuria
- urgency, freq, incontinence
- suprapubic discomfort |
Urethritis | Dysuria (+/- discharge) |
⇒ check for UTI in febrile child with unknown source
- URINALYSIS:
- Dipstick: Nitrite + WBC esterase
- Microscopy: bacteria + WBC
- URINE CULTURE → interpretation depends on sampling methode used!
- Sample from mid-stream → Dg = 2 pos. cultures
- Sterile collecting plastic bag → for exclusion → needs 3. or 4. for confirmation
- Bladder catheterization
- Suprapubic bladder aspiration
Method of Urine Collection | Diagnostic Threshold |
Midstream in voiding girls | 100,000 CFU/mL
10,000-100,000 CFU/mL - repeat culture |
Midstream in voiding boys | 10,000 CFU/mL |
Catheter | 10,000 CFU/mL
1,000-10,000 CFU/mL - repeat culture |
Suprapubic aspiration | Any number of CFU |
- Positive culture
- Positive dipstick (Nitrates / Pyuria)
- Positive clinic ⇒ FEVER +/- other signs of UTI (see above)
PLUS
PLUS
- US
- US + contrast = urosonography
- VCUG
- Cystoscopy
- Scinti
- Uro-MRI

- first episode (fever / pyelonephritis)
- US suggestive for PN / cystitis
- all children <6m
⇒ if abnormality on US, weak urinary flow, FH of VUR ⇒ VCUG
- Pyelonephritis:
- Cystitis:
Ampicillin + Gentamycin OR 3rd gen Cephalos
→ 10-14d (2x)
Penicillins(Ampi,Amoxi) OR Cephalos
→ 5-7d
CLASSICS
- <3m
- Complications
- Toxic appearance
- Dehydration + vomiting
- can Ø be treated at home (low compliance, parents...)
Indication:
- PN during infancy
- Recurrent UTI
- Immuno-compromised
⇒ TMP/SMX (if >2m!!)
→ other: nitrofrantoin, amoxi

⇒ give 50% of standard dose of AB
kidney scars → HT + end-stage RF
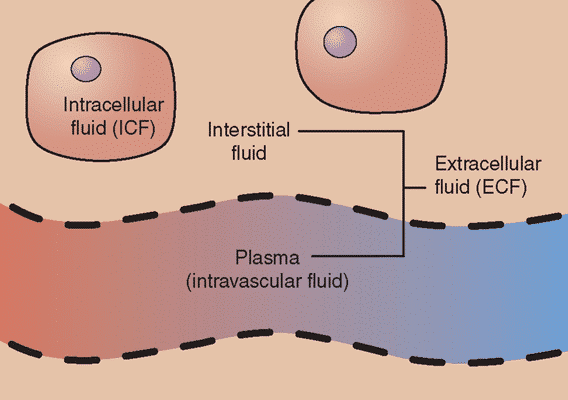
F:
TBW + ECF ↓
ICF ↑
Component | Newborn | 12 months | 12 years | Adult Male | Adult Female |
Total Body Water (TBW)
→ ↓ w/ age | 79% | 65-70% | 60-65% | 60% | 55% |
Intracellular Fluid (ICF)
→ ↑ w/ age | 35% | 40-45% | 40-45% | 40% | 35-40% |
Extracellular Fluid (ECF)
→ ↓ w/ age | 44% | 25-30% | 25% | 20% | 15-20% |
- fluid intake + losses (for etiology & clue of severity)
- micturition
- weight loss (for easy calculation of severity)
- ↓Intake (→ hypernatremic/-tonic)
- increased Losses: diarrhea, vomiting, renal, sweating (CF, fever)
- Translocation (3rd spacing): edema, burns, paralytic ileus (i.e. hirschsprung)
- Weight method: Volume-deficit (L) = initial weight (kg) - illness weight(kg)
- Clinical:
5-10-15 = 50-100-150 ml/kg
(if <1y = 3-6-9)
Grade | Mild | Moderate | Severe |
Volume Deficit (Infants) | 5% (50 mL/kg) | 10% (100 mL/kg) | 15% (150 mL/kg) |
Volume Deficit (Older Children) | 3% (30 mL/kg) | 6% (60 mL/kg) | 9% (90 mL/kg) |
Clinical Signs: Tears | Present | Reduced/absent | Absent |
Clinical Signs: Eyes | Normal | Sunken | Very sunken |
Clinical Signs: Skin Touch | Normal | Dry | Clammy |
Clinical Signs: Skin Elasticity | Pinch retracts immediately | Pinch retracts slowly (tenting) | Pinch retracts very slowly |
Clinical Signs: Buccal Mucosa/Lips | Moist/dry | Dry | Very dry/cracked |
Clinical Signs: Anterior Fontanelle | Flat | Soft | Sunken |
Clinical Signs: Respiratory Rate | Normal | Normal/increased | Increased |
Clinical Signs: Respiratory Amplitude | Normal | Deep | Deep |
Clinical Signs: Heart Rate | Normal | Slightly increased | Increased |
Clinical Signs: Pulse Amplitude | Normal | Weak | Feeble/impalpable |
Clinical Signs: Capillary Refill Time | <2 seconds | 2-3 seconds | >3 seconds |
Clinical Signs: Blood Pressure | Normal | Normal/low | Low |
Clinical Signs: Diuresis | Normal/mild decrease | Oliguria | Severe oliguria |
Clinical Signs: Mental Status | Alert, restless | Drowsy | Drowsy, lethargic, obtunded |
if in doubt classify in the more severe grade
- Intracellular dehydration = thirst, dry mucous membranes, hyperthermia, anorexia

- Intracellular hyperhydration: refusing fluids, moist mucous membranes, brain (dizzy, lethargic, seizure)
Dehydration-type | Iso-tonic (#1) | Hypo-tonic | Hyper-tonic |
Serum Na | n | <130 | >150 |
Cause |
-losses (Øsweating)
-translocation | -hypernatremic fluid loss (i.e. CF)
-dehydration only treated w/ water | -↓intake
-hypotonic fluid loss
(sweating, D. insipid.) |
ECF / ICF | ↓↓ depending on duration (see table→ first ECF then ICF | ECF ↓↓↓
ICF ↑ | ECF ↓
ICF ↓↓ |
Physical exam | extracellular + intracellular dehydration | - extracell. dehydration
- intracell. hyperhydration | -MILD extracell. dehy
- intracell. dehydration
→ neuro! (UMN, ↓conciousness) |
Duration of Dehydration | ECF Loss | ICF Loss |
< 3 days | ↓↓ 80% | ↓ 20% |
≥ 3 days | ↓ 60% | ↓↓ 40% |
Example: Infant with fluid loss of 1 L of recent onset (<3 days). ECF loss = 1 L x 0.8 = 0.8 L ICF loss = 1 L x 0.2 = 0.2 L Distribution of fluid loss: total fluid loss = 0.8 L from ECF + 0.2 L from ICF
- ↓K? → EKG!, signs of ileus or paresis w/ ↓reflexes?
- ↓Ca? → tetany?
- Acid base disturbance?
- Renal function? (BUN, crea, diuresis, etc)
enteral → oral + NG-tube
parenteral → iv
- Deficit → Assess severity (weight method or clinical → 1% dehydration = 10 mL/kg volume deficit)
- Maintenance:
- First 10 kg of body weight = 100 mL/kg/day (= 4 mL/kg/hr).
- Second 10 kg of body weight = 50 mL/kg/day (~ 2 mL/kg/hr).
- Each additional 10 kg of body weight = 20 mL/kg/day (~ 1 mL/kg/hr).
- Ongoing losses → Measure diuresis, stools, vomiting
- diarrhea → 5-10 ml/kg/each diarrheic stool
weight methode:

Holliday-Segar method (not for ages<14 days):
alternative: basal calorie method or body surface area method
example:
infant + 10kg + clinical signs of moderate dehydration + no ongoing losses
⇒1 L volume deficit (10x 10ml / kg)
⇒ maintenance: 40 ml/h / 1000ml/day
⇒ if diarrhea: give 50-100ml/stool

Example:
Na-deficit ⇒ correct Na lost from ECF
Na-deficit = Volume deficit (severity) x ECF loss proportion x Na in ECF (Na x ECF loss)
Lab → Na in serum
ECF → Clinical exam + Severity assessment
From these 2 parameter ⇒ estimate Na in ECF
- isotonic + hypotonic (corrected in 24h) → first 8hr: 1/2 of deficit correction → next 16h: other 1/2
- hypertonic: (corrected in 48h)
→ first 24h: 1/2 free water correction → next 24h: other 1/2
- 🚨SHOCK ⇒ NaCl 20 ml/kg IV BOLUS
⇒ maintenance: constant rate over 24h
every 8h ⇒ clinic, intake/losses, lab
- route of rehydration
- volume of fluid to be administered
- composition of fluid administered
- rate of administration (ml/h)
- respiratory compensation quickyl within hours (PaCO2 alterations through breathing)
- metabolic compensation within days (renal alterations)
Na - (Cl + HCO3)
= 8-12 in children
= 8-17 in infants

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
HCO3 loss ⇒ diarrhea, Renal tubular acidosis
Cl will replace → ↑Cl-
- Elektrolytes +AB-parameters
- Mudpiles screening
- Renal markers (RF?)
- Gluc (DM?)
- Ammonia, Lactate?
- Tox screening (salicylate, methanol, ethanol)
- Urine: pH, ketones, gluc, ammonia
⇒ Aniongap calculation
⇒ ↑K → acute; ↓K → chronic (normal glomerul. function)
- Etiological Tx
- Consider Sodium-Bicarbonate in severe acidosis

Cessation of 🥐-function (↓GFR) ⇒ Changes in urine-Volume + ↑BUN (+Crea)

pre-renal | intrinsic | post-renal | |
CLINIC | |||
🚫 oliguria /anuria | ✅ | ✅ | ✅ |
🚰 Blood volume | ↓ | ↑ | |
🌊weight gain + edema, HT | ✅ | ||
🍎 urinary retention? (full bladder) | ✅ | ||
🩸 hematuria | ✅
(painless) | ✅
(painful - urethral obstruc) | |
🧣 preceeding pharyngitis | ✅ (GN) | ||
💊 💪 drugs, poly-trauma | ✅ (ATN) | ||
🐉 fever, rash, joints | ✅ (AIN) | ||
💩 Diarrhea + pale | ✅(HUS) | ||
LAB | |||
⏰ BUN (Urea) | ↑ | ↑ | ↑ |
💳 Crea (→↓GFR) | ↑ | ↑ | ↑ |
🩸Hematuria | ✅
(nephritic sedim) | ✅ | |
🐻❄️Leucocyturia | ✅
(Pyelonephritis, TIN (eos)) | ||
🪀 Proteinuria | ✅ | ||
⏰/💳BUN/Crea ratio | >20:1 | <15:1 | >20:1 |
🧂FENa
| <1% | >2-3% (ATN/tubular) |
*FeNa=Fract. excr. of Na =The percentage of glomerular filtered sodium (Na) that is excreted in the urine in relation to filtered creatinine
- all → CBC, Electrolytes, BGA
- rest → depending on etiology suspected:
- Immunotest (C3, ASO, ANA) → if APSGN / SLE / membranoprlif
- US → obstruction, kidney size, renal a. stenosis
- Scinti → scarring (+renal function, outflow)
- Xray → stones
- Biopsy → indication: ⇒ RPGN, Non-strep AGN, unknown cause, ATN w/o improvement
- compare current + previous Crea levels 💳
- irreversible (chronic) vs. reversible (acute)
- Chronic clinical signs
- pre-existing illness
- weight + stature deficit
- uremic symptoms (pruritus, nausea, etc)
- small kidneys
- osteodystrophy
↑BUN | ↑Crea | |
AKI | ✅ | ✅ |
dehydration | ✅ | ✅ |
Drugs | ✅(Steroids) | ✅(ASS) |
↑Protein
(intake + catabolism+fasting) | ✅ | |
fever, sev. infections | ✅ | |
↑Muscle mass | ✅ | |
Rabdomyolysis | ✅ |
SIADH ⇒ normal BUN


- SEVERE
- hypervolemia
- Anuria
- acidosis
- hyperkalemia
- uremic complications (see above)
- HUS
- Drug overdose of filterable toxin (i.e. NSAID, aminoglycosides)
- ↓Proteins (uremia)
- ↓K
- ↓Fluid + Na (hypervolemia)
- Adequate calories
Aspect | Chronic Renal Failure (CRF) | Chronic Kidney Disease (CKD) |
Definition | Clinical condition resulting from various pathological processes, leading to renal disorder and insufficiency of kidney function. | Abnormalities of kidney structure or function present for over 3 months, with implications for health. |
- Malformation of the urinary system (reflux, hypoplasia)
- Acquired renal disease (GN, pyelonephritis, tubulointerstital nepropathy)
- hereditary renal disease (ie. Alport, PCKD, etc)
(Intrinsic or post renal)
Children >2y:
50,20,5
Stage | Crea clearance |
1: ↓renal function | 20-50 |
2: RF | 5-20 |
3: ESRD/Uremia | <5
(+ <%5 funct. glomeruli) |
Normal staging:
Stage | Description | GFR (mL/min/1.73m²) |
1 | Renal damage with normal or increased GFR | > 90 |
2 | Mild decrease in GFR | 60-89 |
3 | Moderate decrease in GFR | 30-59 |
4 | Severe decrease in GFR | 15-29 |
5 | End-Stage | < 15 or dialysis |
Initial assessment of albuminuria from morning urine can be conducted using the following methods:
- Albumin/Creatinine Ratio
- Protein/Creatinine Ratio
- Urinary Dipstick
dipstick + → ACR + → albuminuria/24h or proteinuria/24h
ACR: albumin to creatinin ratio
Kidney OUTAGES
hyperKalemia, renal Osteodystrophy, Uremia, Triglyceridemia, Acidosis (metabolic), Growth delay, Erythropoietin deficiency (anemia), Sodium/water retention
- 💩: (GI)
- Nausea + vomiting
- Øappetite
- uremic fetor (urine odor)
- 💪🏼: (skin)
- pruritus
- uremic frost (crystals on skin) 📷
- skin color: pallor (anemia) OR hyperpigmentation (yellow-brown)
- 🧠: (brain)
- encepahlopathy (→seizure, somnolence,coma)
- asterixis
- 🫀 (serositis)
- pericarditis
- pleuritis
- 🩸 (hema)
- Anemia (↑destruction RBC)
- Leuko dysfunction → ↑infections
- Platelet dysfunction → ↑bleeding
Exact cause is unknown. Hypotheses: Accumulation of histamine deposition of urate crystals , increased levels of parathyroid hormone , neuronal changes, and minor inflammatory reactions.
Uremic frost: uremia leads to high levels of urea secreted in the sweat → evaporation → crystallized yellow-white urea deposits on the skin.
yellow brown hyperpigmentation:

Stage | 1 + 2 | 3 |
V-overload/HT | mild (nocturia) | severe (evtl. HF) |
Uremia | 💩 + 💪🏼 | 🩸 + 🫀 + 🧠 |
Development | failure to thrive | retardation of puberty |
others | electrolyte dysbalance,anemia | osteodystrophy |
Stage 1+2
- mild V-overload → nocturia
- mild Uremia
- Fatique
- 💩 but Øbleeding ⇒ malnutrition
- 💪🏼 → pruritus + hyperpigmentation
- failure to thrive
- Elektrolyte imbalance signs
- cramps
- seizures (can also be due to uremia)
Stage 3
- sev. V-overload→ oligura + HT ⇒ can lead to HF
- sev. Uremia:
- 🫀 Pericarditis
- 🩸 → 💩bleeding + infection
- 🧠 → encephalopathy
- retardation of puberty
- 🦴 osteodystrophy
- Renal markers (↑↑urea, crea, uric acid)
- Elektrolytes + acid-base:
- ↓Ca + ↑Phosph+ALP (second. hPTH)
- Na ↓/n
- K ↑
- metabolic acidosis
- CBC (anemia)
- Proteins:
- ↓serum prot
- Albuminuria
- Urine exam
- albuminuria
- Casts (RBC, WBC, granular)
- Acanthocytes
→ calculate eGFR
confirmation:
dipstick + → ACR + → albuminuria/24h or proteinuria/24h
- History:
- renal/uro patho?
- recurr. UTI?
- GN?
- FH of PCKD
- perinatal complications?
- Clinical features of CKD
- ↓GFR
- ↑Crea + GFR for > 3 month
- Anemia (normochromic, normocytic)
- high PTH (due to low VitD→HypoCa2+→high PTH)
- Ultrasound → small kidney, hyperechoic
Aspect | Chronic Kidney Disease (CKD) | Acute Kidney Injury (AKI) |
History of renal disease | Yes | No |
Small kidneys on US | Yes (exceptions: DM, MM, Amyloidosis, ADPKD) | No / ↑ |
Anemia | Normocytic, normochromic | Variable |
HPTH | Yes | No |
- Diet:
- Adequate water
- Na
- Øedema+HT ⇒ n Na
- edema+HT → ↓Na
- tubular patho → ↑Na
- ↓K
- +/- ↓proteins
- Physical activity
- V-Overload (HT + HF) → diuretics, ACEi/ARBs
- Acidosis → i.e. Sodium bicarbonate
- Osteodystrophy → Vit D, Phosphate binders + ↓Phosphate diet
- Anemia → EPO or ESA (Øtransfusion)
ESA:

Stage 3 ⇒ ESRD
- Crea clearance <5
- severe V-overload (HF, HT)
- sev. Uremia (pericarditis, BM failure, neuropathy)