





Gastroenterology
Aspect | Gastroesophageal Reflux (GER) | Gastroesophageal Reflux Disease (GERD) |
Definition | Involuntary passage of gastric contents into the esophagus, with or without regurgitation and vomiting. | Reflux of gastric contents causing troublesome symptoms and/or complications. |
Frequency | Occurs several times per day in normal infants, children, and adults. | Frequency is not specified but implies more troublesome or frequent episodes due to the term "disease". |
Duration of Episodes | Most episodes last less than 3 minutes. | Duration is not specified, but disease status implies that it could be more prolonged or severe. |
Symptoms | Causes few or no symptoms, physiologic. | Causes troublesome symptoms and/or complications, pathologic. |
Time of Occurrence | Occurs in the postprandial period. | Time of occurrence is not specified, could be anytime due to the chronic nature of GERD. |
Factor | A: Transient Relaxations | B: Lower Esophageal Sphincter Pressure | C: Impairment of Protective Mechanisms |
Description | Relaxations of the lower esophageal sphincter, not associated with swallowing, allowing gastric contents to flow into the esophagus. | The pressure fails to increase during a sudden rise in intraabdominal pressure or is chronically reduced, involved in a small number of patients with reflux episodes. | Involves several mechanisms including: insufficient clearance of the esophagus, delayed gastric emptying, abnormalities in epithelial restitution and repair, decreased neural protective reflexes, and hiatal hernia. |
Mechanism | Functional | Functional | Both functional and anatomical |
Outcome | Allows reflux | Allows or fails to prevent reflux | Compromises esophageal defense, contributing to reflux and damage |
Causes of esophagitis:
- Gastrosophageal reflux disease
- Eosinophilic esophagitis
- Infections a. Candida albicans b. Herpes simplex c. Cytomegalovirus
- Crohn disease
- Vomiting, bulimia
- Pill-induced (tetracycline, potassium chloride, ferrous sulfate, non-steroidal anti-intammator medications
- Graft versus host disease
- Caustic ingestion
- Post sclerotherapy/banding
- Radiation/chemotherapy
- Connective tissue disease
- Bullous skin diseases
13.Lymphoma
Infants:
Digestive:
- “Expulsion response”
- Regurgitation (esp. post-prandial)
- Vomiting
- Feeding difficulties
- refusal
- crying during feeding
Extradigestive:
- Respiratory infections / irritation
- Aspiration pneumonia
- Laryngitis (stridor + hoarseness)
- Bronchitis (wheezing)
- cough
- Neuro-, developmental + sleeping disorders
- Sandifer-Sutcliffe syndrome
- failure to thrive

Older children:
Digestive:
- “Expulsion response”
- vomiting (+regurgitation)
- hematemesis (🚩)
- Classic signs of GERD:
- heartburn,
- epigastric/retrosternal pain,
- dysphagia
- dental errosion
Extra-digestive:
- Asthma
(chronic cough + recurr. bronchial obstruction)

- 🤮Abnormal vomiting
- billious
- forceful vomiting
- onset > 6month
- 🩸Bleeding
- hematemesis
- hematochezia
- 💩Lower GI symptoms
- Diarrhea / Constipation
- Abdominal tenderness / distension
- 🔥systemic infectious signs
- fever + lethargy
- HSM (hepatosplenomegaly)
- 🤧Atopic history
- 🧠Neuro + 📈developmental signs
- Failure to thrive
- bulging fontanel
- macro- / micro-cephaly
- seizures



- Prognosis = excellent
- non-pharma Tx usually enough
- Symptoms usually disappear after 8-10m
- If refractory GERD ⇒ Complications:
- Strictures
- Barrett’s (if severe+chronic) → AdenoCa
Complications: Stricture + Fistulas
- Infectious
- Bacterial (i.e. H.P.)
- Viral, fungal, parasites
- Non-Infectious
- Auto-immune (i.e. celiac, eosinophilic)
- Genetic/Metabolic (i.e. diabetic, uremic)
- Vascular (PHT)
- Chemical (NSAIDs, steroids, bile reflux)
- Physical (i.e. radiation)
- Unknown (i.e. crohns)
a. Bacterial Pathogens: Include Helicobacter pylori, Helicobacter heilmanni, Mycobacterium tuberculosis, and Mycoplasma pneumonia.
b. Viral Agents: Mention CMV (Cytomegalovirus) and Herpes simplex.
c. Fungal Microbes: Address Candida albicans.
d. Parasitic Organisms: Highlight Anisakis simplex and Giardia lamblia.
Immune mechanisms (1) Celiac disease (2) Eosinophilic gastritis (3) Autoimmune gastritis (4) Henoch-Schonlein purpura (5) Polyarteritis nodosa (6) Graft versus host disease

MACRO: 📷
⇒ Antrum inflammation
- erythema, edema, exudate
- erosions / ulcer
- nodules
→ bleeding
MICRO:
- inflammatory infiltrate + activity
- Atrophy of gastric glands + intestinal metaplasia
- HP density

- Signs of gastric irritation
- epigastric pain
- vomiting → thoracic pain
- weight loss
- Bleeding (ulcer/erosion)
- hematemesis
- melena
on the long run you can get aplastic anemia du to B12 deficency caused by the reduced intrinsic factor production in the stomach due to the inflammation or iron def anemia due to chronic bleeding
- Organic cause
- Other GI pathology
- Distal esophagitis
- Peptic ulcer
- Pancreatitis
- Hepatitis
- Cholecystitis
- Cholelithiasis
- Diabetes
- Henoch-Schonlein purpura (corrected spelling)
- Crohn's disease
- Appendicitis
- Intussusception
- Mesenteric adenitis
- pain: pneumonia, kidney patho, menstruation
- Functional cause (i.e. IBS)
(1) Conditions Causing Epigastric Pain:
(2) Conditions Causing Right Upper Quadrant Pain:
(3) Other Conditions to Consider:
a. Irritable bowel syndrome. b. Functional dyspepsia. c. Abdominal migraine. d. Childhood functional abdominal pain.


⇒ 📷
- Bleeding (due to ulcer)
- gastric outlet obstruction (acute: edema; chronic: fibrosis)
- vomiting → dehydration → RF (renal failure)
- HP ⇒ MALT (+AdenoCa)
↑freq + ↑fluidity + ↑volume compared to individual “normal”
(WHO = ≥3 loose/liquid stools / day)
Acute ≤14d
Chronic >14d
inflammation of the gastric and intestinal mucosa
💩👄fecal oral route (direct or vehicle-born (food, water))
Infants | Children | Adolescents | |
Acute gastroenteritis | Viral > Bacterial > Protozoal | Viral > Bacterial > Protozoal | Viral > Bacterial > Protozoal |
Food poisoning | --- | + | + |
Extraintestinal infection | UTI, Pneumonia, Sepsis | UTI, Pneumonia, Sepsis | --- |
Postantibiotics | + | + | + |
Dietary errors | + | --- | --- |
- GI-Infection:
- Rota 🥇
- Noro
- adeno + astro
- 🧫 bacteria
- Classics: E.coli, salmonella+ shigella, C.diff, staph aureus
- Campylobacter
- Vibrio cholerae
- Yersenia enterocolitica
- 🪱 parasites
- giardia lamblia
- entamoeba histolytica
- cryptosproidum
- Others:
- 🧪 Food poisoning
- 🕵🏼 other infection focus (UTI,pneumonia, sepsis)
- drugs ⇒ AB 💊
- 🥦 diet errors+ food intolerance +
- 🔪surgical causes (intussusception, apendicitis etc.)
- ♾️ Intial chronic diarrhea (IBD, celiac)
#1 🦠

self limited (🦠)
3-7d
- promotion of breast feeding
- preventention of malnutrition (adequate caloric intake)
- hygiene
- immunization - Rota, cholera
- probiotics for children on oral AB
- <14days? acute vs. chronic diarrhea
- watery vs inflammatory (bloody)
- 🚰 hydration, 🧂electrolyte, 🧪AB status?
- Etiology?
- Complications?
↓
↓
↓
USUALLY 🦠 → Øno work-up needed
if inflammatory or severe ⇒ stool testing⇒ Pathogens?
↓

- 🚰🧂Fluid + electrolyte correction
- Route: enteral (or parenteral)
- Volume → see dehydration
- volume replacement depending on severity
- exception: maintainence fluid = given by Early refeeding (age-appropriate →breast-/formula-milk or BRAT diet📷)
- First 10 kg of body weight = 100 mL/kg/day (= 4 mL/kg/hr).
- Second 10 kg of body weight = 50 mL/kg/day (= 2 mL/kg/hr).
- Each additional 10 kg of body weight = 20 mL/kg/day (= 1 mL/kg/hr).
- Composition → oral rehydration (add low amounts of salt + gluc in water) →see dehydration below
- Rate → correct in 4-6h ⇒ if vomiting give teaspoons
- Symptomatic:
- Anti-diarrheals
- Racecadotril (↓secretion)
- Smecta (absorbant → absorbs toxins, germs + coats intestinal mucosa)
- Probiotics (↓duration of diarrhea)
- anti-emetics ⇒ ondasetron
- Zinc (in developing countries)
- 💊AB ⇒ usually Ø indicated (viral + self-limited)







⇒ !!Loperamide contraindicated

⇒ indication: known bacteria, or travel (cholera), bloody diarrhea (child >2y)

Malabsorption - cant transport across membrane
maldigestion - cant break down nutrients
- Maldigestion:
- Biliary + pancreatic:
- 🍯 CF
- 🎋 Cholestasis
- 🧫 Bacterial overgrowth
- 🐮 Lactase deficiency (lactose intolerance can also be secondary due to malabsorption!)
- 🔪 Ileal resection
- Primary malabsorption:
- 💩 post-gastroenteritis
- 🤧 food allergy (i.e. 🐮 milk PROTEIN intolerance)
- 🍞 celiac disease & IBD
- 🪱giardia
- 🔽 short bowel synd.
- 💊 drugs (antineoplastics)
- 🧬 genetic

Age | Infant | Child | Adolescent |
🐮
post.-infec lactase def.
Cows milks proteins
Lactose intolerance |
✅
✅
- |
✅
-
✅ |
-
-
✅ |
🍎 Excessive fruit juice | ✅ | ✅ | |
🍞 Celiac | ✅ | ✅ | |
🍯 Cystic fibrosis | ✅ | ||
🪱 Giardiasis | ✅ | ✅ | |
🧱 IBD | ✅ | ✅ | |
😟 IBS | ✅ | ✅ | |
Anorexia nervosa | ✅ | ||
AIDS enteropathy | ✅ | ✅ |

- edema (↓oncotic p)
- muscle wasting + weight loss
⇒ Stool test: fecal alpha1 antitrypsin
⇒ suggestive for celiac disease (or other mucosal disorder)
- watery diarrhea (osmotic)
⇒ Stool test:
- pH <5.5 (due to bact. fermentation)
- Reducing sugars in stool (lactose, fructose, maltose, galactose)
⇒ Breath hydrogen test:
(production of hydrogen by bact. fermentation)
>20 → carbohydrate malabsorption
- steathorrhea + weight loss
- ADEK deficiency
- rickets (D)
- bleeding (K)
⇒ Stool test:
- spot fecal fat stain 📷
- Quantitative fecal fat/72h ⇒ total excretion (>5g/24h) + coeffic. of absorbtion*
Coefficient of absorption = [(fat ingested - fat excreted/fat ingested] x 100.
- ↓wound healing
- ↓taste
- acrodermatitis 📷

- anemia (megaloblastic)
- glossitis
- tetany

- paresthesia
- Initial workup - if malabsorption suspected:
- consequences of malabsorption?
- growth?
- chemistry panel: liver (inc. albumin + bili), electrolytes
- What type of diarrhea?
- inflammation lab → ESR+CRP
- stool exam + occult blood testing
- Cause for diarrhea / malabsorption?
- Disease - Screening test:
- IBD panel
- Celiac + IgA panel
- CF (blood + sweat)
- Malabsorption studies
- Blood screening - malabsorption:
- Iron, VitB12, folate studies
- ADEK studies
- Stool test for malabsorption (antitrypsin, fat (stain + quant), pH)
- Additional exams needed to confirm?
- Endoscopy + biopsy
- imaging (pancreas, liver)
→ + Hydrogen breathtest for carbs
- Fruit excess
- IBS

- Lactose intolerance
sweat test + → CF
if - → biopsy:
→ villous atrophy? → celiac
→ lymphangiectasis
→ normal = abeta-lipoproteinemia
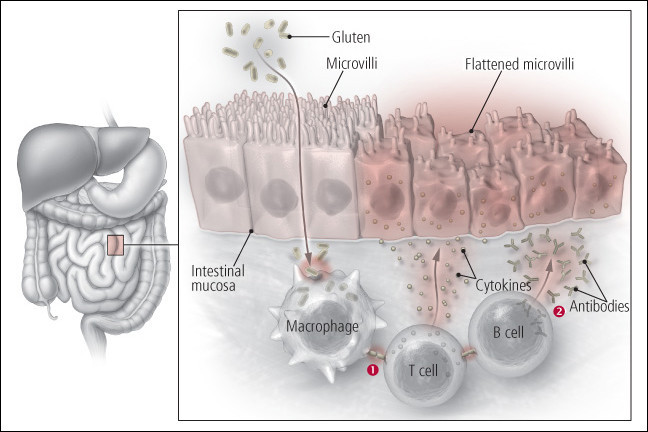
HLA-DQ2 + -DQ-8
→ HLA encodes MHCII → presentation exogenous peptide to Antigen-presenting-cells
The body's immune system reacts to gliadin, a component that can dissolve in alcohol and is present in gluten. When individuals consume gluten-rich food, tissue transglutaminase, an enzyme, becomes active, altering the structure of gliadin in the gluten proteins. This modified gliadin then activates specific T cells that instigate prolonged intestinal inflammation. This inflammation is responsible for epithelial injuries, which are evident by villous atrophy, crypt hyperplasia, and a diminished brush border. Such changes hinder the efficient absorption of nutrients, leading to malabsorption symptoms.
- chronic / recurrent diarrhea (watery or fatty)
- abdominal distension
⇒ children: short, delayed puberty, failure to thrive
⇒ weight loss (also due to ↓appetite)
- Total IgA (↓)
- anti-TG2(Anti tissue transglutaminase IgA)
- EMA-Ab (Anti-endo-mysial)
- AGA-Ab (Antigliadin)
- HLA typing DQ2+DQ8
- lymphocytes infiltration (intra-epithelial)
- Crypt hyperplasia
- Villous atrophy
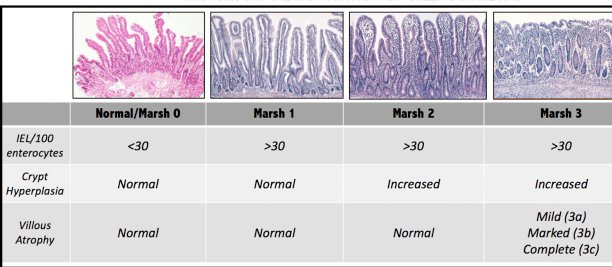
MARSH CLASSIFICATION: 📷
Type 1 ⇒ infiltrative (intra epithelial lymphocytes >25/100 enterocytes)
Type 2: crypt hyperplasia
Type 3 (a,b,c,): Villous atrophy (a,b,c = varbiable severity)

strict, life-long gluten-free diet 📷
cancerrrrrrr 🦀
↓
Lymphoma + AdenoCa
impaired function and structure of intestinal tissue (i.e. villous atrophy ⇒ diarrhea + malabsorption
villous atrophy, deep crypts, short microvilli, damaged brush border
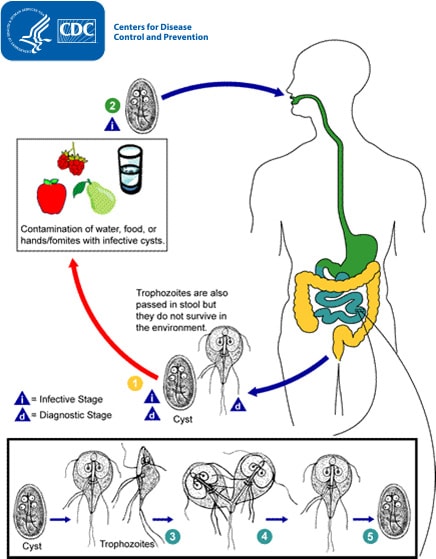
- Incubation: 1-3w
- Asymptomatic or acute illness:
- Diarrhea
- watery
- signs of bact. overgrowth → distension + flatulence
- other signs: cramps, vomiting+nausea
NON-SPECIFIC:
→ Øblood (Øinvasion)
- persistence symptoms→ chronic diarrhea, steatorrhea, malabsorption, weight loss, failure to thrive
→ esp. if hypoglammaglobulinemia
#1 Metronidazol (or alternative)
- if pregnant or immunodef. in household → prevention in family members
#2-line drugs: furazolidone, albendazole, paromomycin, and quinacrine.
Non-pharma → hygiene
Lactase deficiency → unabsorbed carbohydrates
⇒ signs of carbohydrate malabsorption → colon: bacterial fermentation (flatulence+acidic ph) → osmotic diarrhea + sugars in stool
- Congenital complete lactase deficiency (rare as shit)
- Primary adult type hypolactasia (physiological decline with age)
- Secondary = MUCOSAL DMG
Fewer than 50 cases have been reported worldwide
⇒ celiac, infection, inflammatory, allergic
Lactase = localized at brushborder on villi: 📷

(production of hydrogen by bact. fermentation**)
a. Lactose Administration: Patients receive a dose of lactose (2 g/kg) orally following an overnight fast.
b. Lactase Deficiency and Fermentation: In cases where lactase is deficient or reduced at the brush border membrane, unabsorbed lactose undergoes fermentation by colonic bacteria, leading to the production of gases, including hydrogen (H2).
c. Positive Test Criteria: A test result is considered positive for lactose malabsorption if there is an increase of 20 parts per million of H2 above the baseline level.
d. Potential False-Negatives: It's important to note that this test can yield false-negative results in patients with a predominant population of non-hydrogen-producing bacteria in their gut and in cases where there is a recent history of antibiotic usage.
+ Breath test OR +Lactase activity in biopsy
↓dairy products → ↓Ca2+ ⇒ rickets / osteomalacia
- DIET:
- Lactose free
- infants: lactose free formula
- yogurt with live cultures generally tolerated
- Ensure Ca2+ intake
- LACTASE SUPPLEMENTATION
(allergic) immune reaction on cow or soy protein (might be IgE or non-IgE mediated)
⇒mucosal damage
- <1y
- CLASSIC ALLERGIC REACTION: (minutes after ingestion)
- 💪🏼: urticaria, eczema, angioedema
- 💩: dysphagia, pain, nausea+vomiting, bowel habit change, occult blood loss
- 🫁: rhinorrhea, wheezing, cough
- STOOL: bloody mucus-streaks 📷
→ but appear healthy
- Allergy test:
- specific IgE (cow-milk)
- Skin prick test
- Øperiph. eosinophilia!
- Complications → iron def. anemia?
- Biopsy
Should be performed in patients with otherwise unexplained significant and persistent gastrointestinal symptoms, failure to thrive, or iron deficiency anemia.
Nearly all of these infants lose their sensitivity to the offending protein by 1 year of age.
⇒ after 1y of age = everything gucci 👍
- Avoid protein
- bottle fed → switch to hydrolzed protein formula
- if persistent bleeding → amino-acid based formula
- breast fed → mother should stop eating soy + dairy products
- Iron def. anemia Tx

non-IgE mediated syndrome
⇒ severe shock-like reaction + metabolic acidosis
- abdominal pain
- diarrhea
- extraintestinal manifestation
- fistulas
- abcesses (intra-abdominal + ani-perineal)
- occlusion
terminal ileum
but can appear anywhere
⇒ transmural involvement
- erythema + friability
- involvement of all layers (in longitudinal section)
- multiple apthous + longitudinal ulcer → cobblestone appearance
- fibrosis of the lesions → stenosis
- thickend wall + mesentery (also enlarged lymphnodes + expansion of fat )
- fixed adhesion betw. intestinal loops ⇒ developtment of fistulas within them → abcesses + duodeno-/jejuno-colic shunts (→ malabsorption)
- alternation with normal segment = skip lesions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- 💥Pain (⇒RLQ)
- 💩Diarrhea
- 🩸Iron deficiency anemia → due to occult bleeding (gross blood if colon involvement)
- ⚖️ Weight loss ⇒ 📈 failure to thrive (growth)
- +- 🔥fever
- 🐚 Peri-anal → inflammation, fissures, fistula
- 👄 Mouth → apthous ulceration + gingival hyperplasia
→ persistent + severe

→ might be severe + noctural
- Incomplete reabsorption of bile salts (impaired ileum , can’t absorb bile) → colon → electroly + water influx→ diarrhea ⇒ cholesthyramine
- Bacterial infection ⇒ AB tetracyclin or metronidazole
- Fistulas → duodeno-/jejuno- colic → shunting of absorption → undigested bolus into colon → diarrhea ⇒ surgery
- Extensive colon involvement → colon mucosa damage (structural) → ↓water+electrolyte reabsorption → osmotic diarrhea ⇒ 5-ASA + steroids
- Joint disorders (i.e. ankylosing spondylitis)
- Skin:
- Erythema nodosum
- pyoderma gangrenosum
- (Red) Eye: Uveitis + Keratoconjunctivitis
- Fistulas (bladder, vagina etc) + Abcesses
- Bile- + kidney-lithiasis ⇒ pyelonephritis + cholestasis
- Ureteral stenosis
- vascular: hypercoagulability
Ulcer perforation → usually Øfree into peritoneal cavitiy BUT inside blocks of adhesions → Abcesses → Fistulas: entero-peritoneal, entero-vesical, recto-vaginal, ano-perineal and more(see later)
terminoileitis or resection of ileum → ↓bile salt reabsorption → ↑cholesterol (relative) + ↓bilesalts in bile → lithogenic bile
terminoileitis or removal of illeum → ↓FFA reabsorption → FFA bind Ca2+ → ↓free Ca2+ to bind oxalate → ↑Natrium-oxalate (soluble) → absorbed by colon → hyperoxalemia → oxalic lithiasis
right ureter
sclerotic-inflammatory progress in terminal ileum + ceco-asc. colon
hydronephrosis
anti-inflammatory therapy → associated with active phase
🩸 BLOOD
- ↓Albumin (due to malnutrition+inflammation)
- Anemia (iron def) ⇒ CBC, Hb, MVV
- Inflammatory markers → ↑ESR, ↑CRP
- liver + renal marker
- SEROLOGY ⇒ ASCA (suspicious for crohns)

💩 STOOL
- Infection?
- culture (shigella, salmonella, etc)
- toxin test for C.Diff
- Giardia workup (antigen + microscopy)
- Inflammatory fecal markers: calprotectin + lactoferrin
- positive family history
- ↓Body weight + underdeveloped child
- Abdominal pain (most often RLQ)
- Diarrhea
- peri-anal disease
- +-fever
- extra-intestinal
Physical exam:
- Pallor? (anemia)
- Weightloss?
- Inflammatory mass (painful) in right iliac fossa
- fistulas/abcesses peri-anorectal
- extraintestinal manifestations (skin, joint, eye, bile+kidney stones, hydronephrosis)
Check Lab
🩸 BLOOD
- ↓Albumin (due to malnutrition+inflammation)
- Anemia (iron def) ⇒ CBC, Hb, MVV
- Inflammatory markers → ↑ESR, ↑CRP
- liver + renal marker
- SEROLOGY ⇒ ASCA (suspicious for crohns)
💩 STOOL
- Infection?
- culture (shigella, salmonella, etc)
- toxin test for C.Diff
- Giardia workup (antigen + microscopy)
- Inflammatory fecal markers: calprotectin + lactoferrin
- UC (location, bloody diarrhea, +paraclinical investigations)
- Lymphoma
- TBC
- Appendicitis, intussiception + meckels
- DDx for other signs of crohns
- Colonoscopy
- MRI (/CT)
- US
→ Normal lower colon + rectum
→ Cobblestone-appearance: Extensive longitudinal + transversal ulcers delimiting edematous mucosa
→ BIOPSY❗→ granuloma

→ stenosis, abcesses, wall thickening
→ Radiological DDx with lymphoma
histological confirmation → granuloma
Endoscopic OR Imaging evidence of:
- small bowel involvement
- biopsy = granuloma
- severe peri-anal disease (fissure, fistula, abscess)
- iron (+B12+ folic acid) replacement
- caloric supplements or parenteral nutrition
Sulfasalazine (📷→ 5-ASA) + Steroids
{kind=link}
active phases
(oral / iv (severe) or enema if recto-sigmoid inflamm)
- Steroids failed
- long term treatment required (+5-ASA is not enough)
⇒ Immunosuppressiva: AZA, 6-MP
⇒ MAbs / biologic: Infliximab → alternative: Adalimumab
AB! → metronidazole
- Loperamide
- If due to removal of ileum → Cholestyramine
- If due to bacterial infection → metronidazole
steroids + NSAIDs
- unresponsive to drug Tx
- Stenosis
- Perforation
- Bleeding
(+abscess+fistula, emergencies (toxic megacolon, fulminant colitis)
nope freq. recurrance after resection
{kind=link}
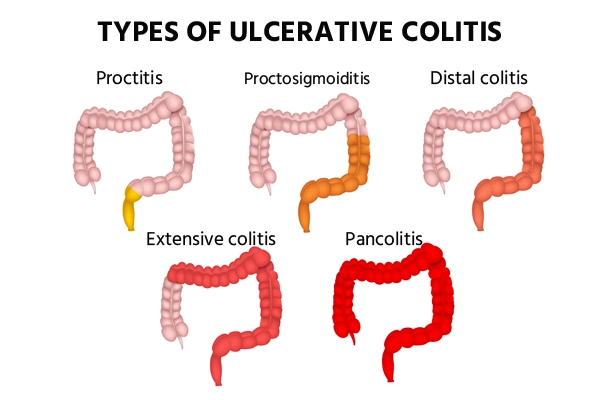
- proctitis (rectum)
- (proctosigmoiditis)
- left (distal) colitis
- (extensive colitis)
- pancolitis
only mucosa + submucosa
features of both IBDs (Crohns +UC)
⇒ about 10% of children affected
more severe + extended lesions (the more colon involvement + the more severe lesions ⇒ the more symptoms
- 💥 pain LLQ
- tenesmus - pain during defactation
- 💩diarrhea
- 🩸rectorrhagia (proctitis, proctosigmoiditis, pancolitis [↑severity])
- ⚖️ weight loss GROWTH USUALLY NORMAL
- 🔥 +-fever
⇒severe anemia + dehydration (esp. in pancolitis due to ↑↑diarrhea+bleeding)
- 💪Skin lesion (erythema nodusum + pyoderma gangrenosum)
- 🦴 Arthritis - evtl. ankylosing spondylitis
- 🐍 primary sclerosing cholangitis + Autoimm. hepaptitis
- 👁️ Uveitis + keratoconjunctivitis
- vascular: thromboembolic
- crohns
- infection (gastroenteritis)
- carbohydrate intolerance
- Allergic (i.e. protein intolerance)
- Hirschsprung
- Celiac
- drugs
TTTTTTTT 📷
{kind=link}
septic shock
- tachycardia
- fever
- hypotension
- abdominal distension
- signs of perioneal irritation (perforation/abcess)
⇒ early detection of free air in peritoneal cavity (=perforation)
- Xray
- US
- CT
- Leukos
- radioloy: "empty abdomen" + dilation 📷
- signs of inflammation: altered state, fever, ↑Leukos, tachycardia
1. ↑body T (by 3 tens of degree - under steroid therapy)
2. colic pneumatosis (intramural gas) 📷
{kind=link}
local smooth muscle hypertrophy
(Øsclero-fibrotic)
- Hemorrhage → anemia
- long term → AdenoCa
Colonoscopy
- Erythema
- Granular mucosa (sandpaper like) → later nodular + friable
- pseudoinflammatory polyps
- hemorrhagic, ulcerated, stenosis
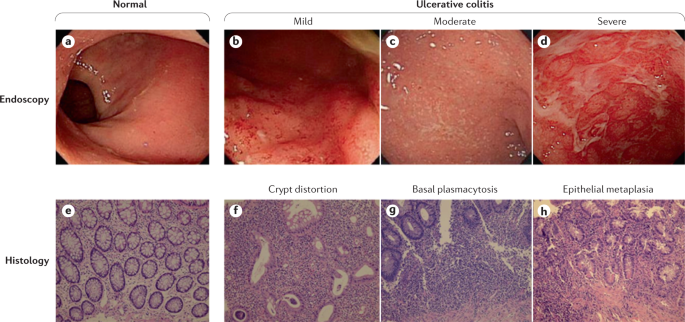{kind=link}
- skip lesions
- Øpseudo-polyps
- cobblestone
- Cryptitis (Np infiltration) + abcesses
- inflammatory cells in lamina propria
- depletion of goblet cell mucin
- lesions limited to mucosa or submucosa
🩸 BLOOD
- ↓Albumin (due to malnutrition+inflammation)
- Anemia (iron def) ⇒ CBC, Hb, MVV
- Inflammatory markers → ↑ESR, ↑CRP
- liver + renal marker
- SEROLOGY ⇒ pANCA (suspicious for crohns)
💩 STOOL
- Infection?
- culture (shigella, salmonella, etc)
- toxin test for C.Diff
- Giardia workup (antigen + microscopy)
- Inflammatory fecal markers: calprotectin + lactoferrin
- Bloody diarrhea → ≥2weeks negative stool cultures
- Endoscopy features + (→ diffuse continous mucosal inflammation, rectum → colon )
- BIOPSY features+: Features of AKTIVE + CHRONIC inflammation in all biopsies
Like crohns
🥇 5-ASA + Steroids(active period)

↓
#2 Immuonosupressive (AZA, 6MP, ..)
#3 Biologics (Infliximab)
- Elective:
- before-mentioned medical treatment fails
- Malignancy or dysplasia (low or high grade)
- Emergency:
- Toxic megacolon
- Perforations
- Hemorrhage (↑↑) - requir. transfusion
- Organic causes
- Functional causes
≥3 attacks of pain in 2 month
causes activity restriction
Øorganic cause found

- visceral hypersensitivity
- altered GI motility
hypersensitivity → pain
motility:
↑ - diarrhea
↓ - constipation (→bloating, nausea)
should be avoided 🤡
{kind=link}
- FH for organic GI disease → IBD, celiac, peptic ulcer
- persistent:
- pain (RUQ + RLQ)
- vomiting
- inflammatory signs → unexplained fever, noctural diarrhea
- IBD signs → arthritis, peri-rectal disease
- failure to thrive: weight loss, growth, delayed puberty
- Functional dyspepsia
- IBS
- Abdominal migraine
- Function abd. pain not otherwise specified
Diagnostic criteria (ROME IV) for…
≥1 of the following 4 for ≥ 4 days / month (every week) :
- Signs of Postprandial distress syndrome
- Postprandial fullness
- Early satiety
- Signs of Epigastric pain syndrome
- Epigastric pain / burning Ø relieved by defecation
→ assoc. with bloating, nausea, belching
- can Ø be explained fully by organic cause
ABDOMINAL PAIN ≥4x/month
PLUS
≥1 of the following:
- pain related to defecation (i.e. relieved)
- changed BOWEL HABITS:
- frequency (i.e. diarrhea)
- change in form (i.e. diarrhea)
PAROXYSMAL INTENSE PAIN
- ≥2 episodes of INTENSE paroxysmal pain (midline, peri-umbilical OR diffuse)
- lasting ≥1h
→ episodes seperated by month
PLUS
≥2 of the following (each symptome count 1)
- non-specific Upper-GI sign: anorexia, nausea, vomiting, pallor
- Sign of classic migraine: headache, photophobia
≥4x / month + includes ALL:
- ØTHE OTHER: Criteria for other functional D Ø met
- Pain Ø only related to physiologic events (eating, menses)
- cant be explained by organic cause
(might be episodic or continous)
Treatment of..
- Avoidance of gastric iritants: ØNSAIDS + Øaggravating food
- epigastric pain synd. → PPI / H2-blocker
- postprandial distress synd → prokinetics
- if persistent symptoms ⇒ anti-depressives (i.e. TCA)

🥴 psychological Tx + lifestyle (🍿diet,🏄🏼♂️exercise)
“In irritable bowel syndrome confirmation of the diagnosis, explanation of pain experience and reassurance are very important”
- Avoid trigger
- When freq ⇒ prophylactic tx (i.e. sumatriptan)
- defecation <2x/week
- hard, large, dry stool
- painful bowel movement + withholding behavior
- +- fecal incontinence
stool into other place than toilet
AFTER 4y of age
- Organic cause
- GI → malformations, Hirschsprungs
- metabolic,
- neuropathic,
- drugs,
- CF + others
- Functional constipation
(a) Imperforate anus (b) Anal stenosis (c) Anterior displaced anus



Other (1) Connective tissue disorders (scleroderma) (2) Heavy-metal ingestion (lead) (3) Botulism (4) Cow's milk protein intolerance (5) Cystic fibrosis (6) Sexual abuse
- Organic cause ⇒ ↓spincter control - direct or neuromuscular: Anorectal surgery, neuro (spinal + CNS cause), muscular
- Functional cause
- Primary: Non-retentive (Øconstipation) fecal inconctinence
- Secondary to functional constipation
T
avoid defecation → ↑stool retention → ↑H2O absorption → hard stool (fecal mass) → progressive loss of rectal sensitivity → pain (when hard stool passes) → anal sphincter spasm → loss of sensivity (+loss of urge to defecate) ⇒ fecal incontinence
- INFANTS: change breast milk → formula/solid food
- TODDLER: acquiring toilet skills → try to control bowel movements → pain (psycholog. association)
- SCHOOL CHILDREN: avoid defecation during school
T - in 50%
“A positive family history has been found in 50% of constipated children, and a higher concordance has been described in monozygotic than dizygotic twins.”
- FAILURE TO THRIVE
- ABDOMINAL DISTENSION
- BLOOD in stool
- NEURO signs
- general neuro signs
- Absent reflexes → anal wink + cremaster
- lower extremities: weakness + ↓muscle tone
- signs of spina bifida:
- lack of lumbosacral curve
- sacral dimple with hair
- midline pigment abnormalities
- sacral agenesis
- asymmetry of buttocks
- signs of hirschsprungs
- tight empty rectum +abdominal fecal mass
- gush of liquid+air on withdrawel of finger
- signs of malformation → i.e. ant. displaced anus
≥2 of the following:
- ≤2 defecations / week (child ≥4y)
- ≥1x fecal incontinence / week (child ≥4y)
- Fecal mass in rectum (DRE)
- History of:
- excessive rentention (posturing or volitional)
- painful hard bowel movement
- large stool (obstruct toilet)
volitional*:

ALL of the following ⇒ age ≥4y !
- Fecal incontinence (defecation into inapproriate places)
- Øevidence of fecal retention (constipation)
- Øexplained by other cause
- Lab → depending on organic cause suspected
- DRE + Anal manometry
- Imaging: US + Xray (+-enema), MRI (spine)
- Biopsy → hirschsprung
- metabolic workup
- thyroid function (metabolic)
- Electrolytes
- Fecal incontinence
- Hemorrhoids (excessive straining)
- Fistulas
- Dilation → rectal prolapse+ulceration, intussusception
→ UTI
- Disimpaction
- p.o. - PEG (polyethylene glycol), mineral oils
- enema
- suppositories - glycerine
- older children → bisacodyl suppositories
- Maintenance Tx (for several month)
- NON-PHARMA:
- Diet - ↑fluid, fibers & whole grains
- Behavioural changes
- Biofeedback training
- PHARMA:
- Osmotic laxatives - PEG, lactulose, etc.
- Lubricants - mineral oil ⇒ Øin infants ❗
- Stimulant laxatives - Senna, bisacodyl ⇒ Øin maintenance ❗
“(1) Fruit juices (prune, pear, apple juices). (2) Whole grains, fruits, and vegetables. (3) Constipating foods should be reduced or eliminated: bread, pasta, potatoes, fried, greasy foods, corn, rice, foods that contain a high level of sugar and dairy products (ice cream, cheeses, cow milk).”

AST + ALT
AST:

ALT:

(high sensitivity +low specificity ⇒ esp. AST → also expressed in heart, muscles, kidney, pancreas, RBC etc,)
GLDH (Gluthamatdehydrogenase)→ liver cell specific, in very severe damage elevated!
- Albumin (↓ in chronic liver failure)
- Pseudo-Cholinesterase (↓ in chronic liver failure)
- Enzyme produced by the liver
- can hydrolyze several choline-based esters (i.e. muscle relaxants succi)
- ↓ serum levels in: cirrhosis or organophosphate pesticide exposure.
- Prothrombin time (quick) (↓ in ACUTE liver failure)
- Bili
- ALP (also ↑ in liver disease, rickets, pregnancy)
- GGT

(also ↑ in renal failure, pancreatitis, etc; marked ↑↑in alpha 1 antitrypsin + biliary atresia)
Ammonia (↑in acute + chronic advanced; also in porto-systemic shunt, urea-cycle enzyme defects)
FIBROtest or FIBROspect
hyaluronan
“
- Single serum biochemical markers: hyaluronan.
- Multiparameter tests (>20 tests are described): a. Fibrotest incorporates 5 biochemical markers: haptoglobin, bilirubin, GGT, apolipoprotein A-1, and a2-macroglobulin b. FIBROSpect II incorporates 3 biochemical markers: hyaluronate, tissue inhi- bitor of metalloproteinase 1, and a2-macroglobulin.”
- viral serology
- metabolic (+ genetic) test
- auto-immune test (auto-antibodies etc.)
Property | Direct Bilirubin (Conjugated) | Indirect Bilirubin (Unconjugated) |
Solubility | Water soluble | Fat soluble |
Excretion | Excreted in urine | Not excreted in urine |
Urine Appearance | Urine dark | Urine not dark |
Blood-Brain Barrier (BBB) | Does not cross BBB | Can cross BBB |
Kernicterus | Does not cause kernicterus | Can cause kernicterus |
{kind=link}
yellow discoloration → skin, sclera, mucous membranes due to ↑bili
(visible when total bili is >2mg/dl (children/adults) or >5-7 (newborns))
Hyperbilirubinemia (>2(-7))
PLUS
unconjugated: indirect >80% AND direct <2mg/dl
conjugated: direct ≥20% OR direct >2 mg/dl
- ↑destruction of RBC (fetal hemoglobin)
- Immature liver UDP-glucuronosyltransferase (↓conjugation capacity)
- ↑enterohepatic bili circulation (↑uptake of unconjug. bili)
⇒ ↑↑ UNCONJUGATED BILI
- preterm or low gestational weight
- acidosis (binding of H+ to alb → ↓carring capacity for unconj. bili)
- hypoxia
- sepsis
- hemolytic anemia
Physiologic jaundice | Pathologic jaundice | |
Onset | >72h | <24h |
Total bili | ↑ | ↑↑ (>12-15mg/dl)** |
Bili type | unjonj | conj >2 mg
(can also be unconjugated) |
Rise (unconjugated) | ↓<5mg/dl/day
(<0,5 / hour) | ↑>5 mg/dl/day
(>0,5 / hour) |
Persistence | < 1w (term)
<2w (premature) | >1w (term)
>2w (premature) |
**preterm>15; term breast >14; term formula >12
- 🌼Unconjugated
- 🐣 Physiologic (hemolysis + ↓conjugation)
- Pathologic
- Prehepatic
- 💔Hemolysis (sepsis, blood incompatibility i.e. Rh sensitization)
- 📛 Sepsis
- 🩸Hemorrhage (cephalhematoma)
- Non-hemolysis/hemorrhage:
- 🤱 Breastfeeding / breastmilk jaundice
- 👽 Cringler Najjar (🍑 intra-hepatic)
- 📦 Conjugated
- 🍑 Intra-hepatic
- 🦠 hepatitis
- idipathic
- viral
- bacterial (sepsis, UTI)
- 💨 metabolic: alpha-1 antitrypsin, CF
- 🧬 genetic (Alagille synd)
- 🎋 Extra-hepatic
- biliary atresia
- biliary cysts

Breastfeeding:

Breastmilk




- 🌼 Unconjugated
- Pathologic
- 🌶️ Pre-hepatic
- 💔 Hemolysis (i.e. hemolytics anemia)
- 🩸Hemorrhage
- 🍑 Intrahepatic (🧬genetic)
- 👽 Cringler Najjar (↓conj)
- ISOLATED UNCONJUGATED hyperbili
- ØSIGNS of OTHER causes
- Øhemolysis
- Øhepatocellular disease
- normal liver histo
- molecular GENETIC testing
- 🪨Gallstones
- 💊Drug-toxicity (drugs that require glucoronidation)
- 📦 Conjugated
- 🍑 Intra-hepatic
- 🦠 hepatitis
- toxic (drugs, alc, toxins) + autoimmune
- viral (hep ABCDE, EBV, CMV, HSV)
- bacterial (sepsis, UTI)
- 🧬genetic: 🚬 Dubin Johnson + 🚁Rotor
- 💨 metabolic: alpha-1 antitrypsin, CF + wilson
- 🎋 Extra-hepatic
- classic biliary pathologies (stone, cystitis, cyst, sclerosing cholangitis, stricture)
genetic autosomal dominant disease → gene: UDP-glucuronyltransfera → ↓conjugation ⇒ ↑UNCONJUGATED bili
onset: during/after puberty
jaundice ⇒ intermittend + exacerbated by stress (fasting, dehydration, hemolysis, etc)
→ ↑during stress ⇒ during fasting ⇒ ↑≥1,4mg/dl = suggestive
⇒ ↓with phenobarbital


none🤡
→ no specific Tx necessary
physiologic (day ≤ 2-4), peak total bili<12

breastfeeding (day ≤ 7), peak total bili >12
→ ↓intake → ↓bowel movement/stasis → ↑entero-hepatic uptake of bili
breast milk: (day >7)
- with ↑beta-glucuronidase → deconjugation of bilirubin in bowel → ↑entero-hepatic uptake
- unidentified factor → inhibit conjugation
Tx:
breastfeeding → eat more / supplement with formula
breast milk → continue breastfeeding (consider hydrolyzed formula / phototherapy in severe cases)
- Unconjugated vs. conjugated
↓
Unconjugated: hemolytic anemia? hemorrhage? hemolysis? reabsorption / genetic?
Conjugated: patho workup
→ US (liver + biliary)
→ liver + biliary markers → infectious workup
→ metabolic + genetic workup
- phototherapy
- transfusion (ABO match + Rh negative)
- IVIG
>6month
peri-portal inflammation + extension → hepatocyte necrosis → fibrosis → nodules (regeneration) ⇒ cirrhosis ⇒ HCC
⇒ ↓Hepatic function
⇒ Portal HT + Cholestasis
{kind=link}
- 🦠 Viral: Hep B,C,D
- 🛡️ Autoimmune
- 🔰 Autoimmune hepatitis
- 🐍Primary sclerosing cholangitis → assoc. w/ IBD
- 🧬 Genetic:
- 👁️ Wilson
- 💨 CF (biliary)
- Alpha1-antitrypsin deficiency
- 💊Drug-induced
- ❓ Idiopathic
(Isoniazid, NSAIDs, alpha-methyldopa, etc.)
- 🏭 ↓Function.
- ↑Bili → 🌕 Jaundice + pruritus
- ↑Ammonia → 👼 encephalopathy
- 🩸 coagulopathy → brusing + petechia
- hepatomegaly
- 🎋 Cholestasis signs
- 🧈 fat malabsorption signs
- ↓Vit ADEK
- rickets +coagulopathy
- malnutrition
- muscle wasting
- ↓growth + development
- loss of fat stores
- ⚪ pale stool + dark urine
- 🌊 portal HT signs
- Ascitis
- Varices
- Splenomegaly
- Hepatorenal syndrome
- Other: 🕸️ spider nevi, ✋clubbing+ liver palms

- Liver + Biliary markers:
- ALT + AST
- Bili
- ALP
- PT + INR
- Albumin
- ETIOLOGICAL WORKUP (see later)
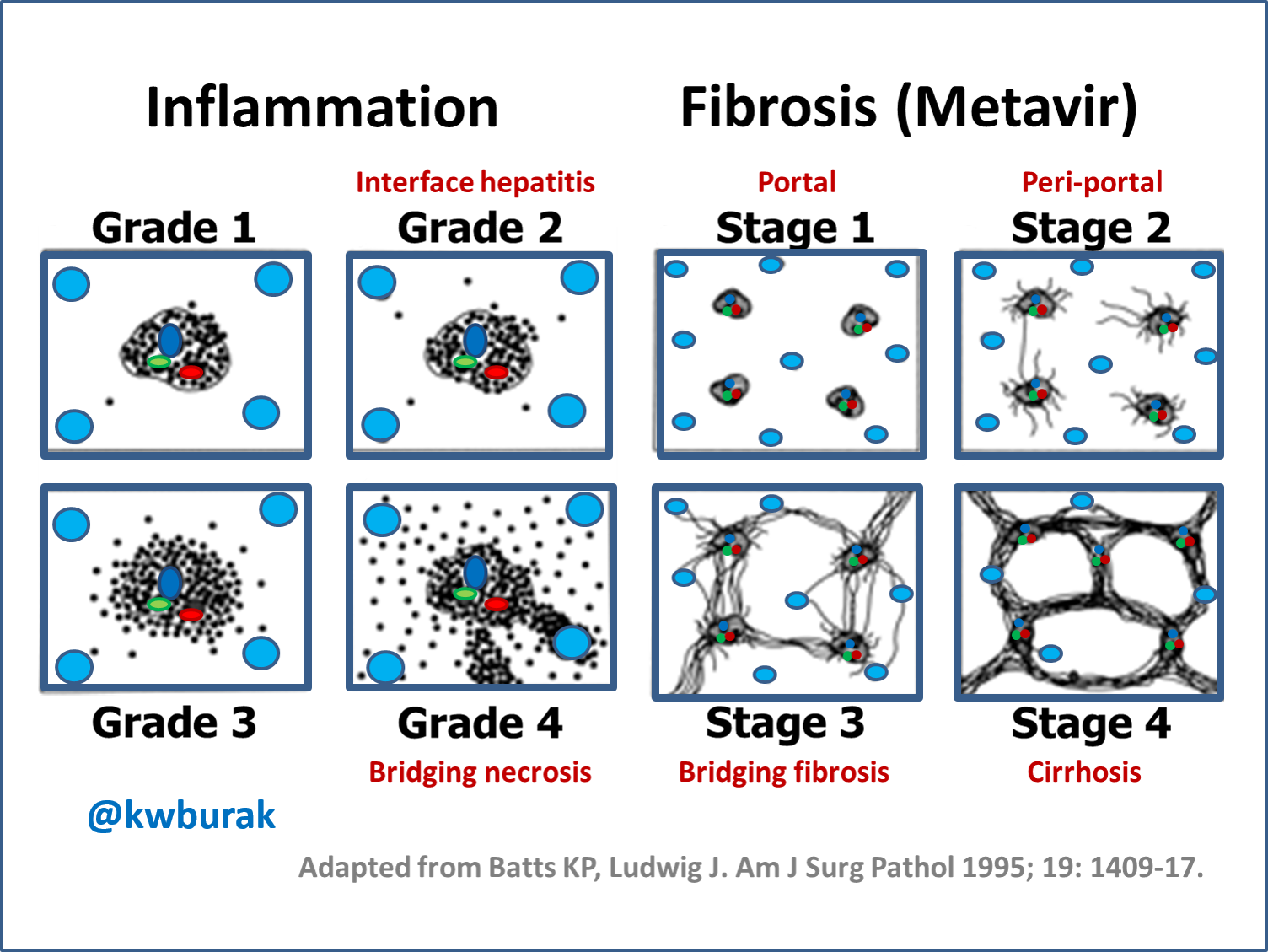
Stage 0 | Ø fibrosis |
Stage 1 | portal fibrosis |
Stage 2 | portal fibrosis + septa (periportal) |
Stage 3 | bridging fibrosis |
Stage 4 | cirrhosis = nodules |
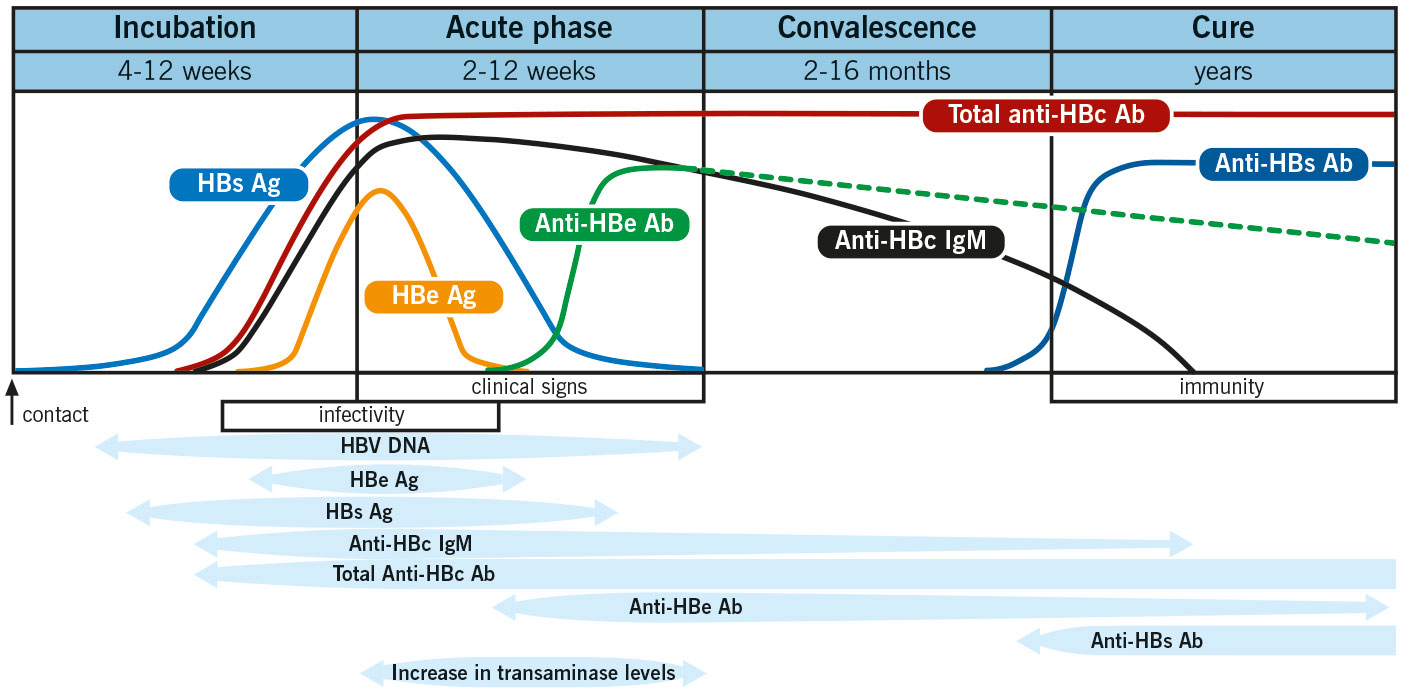
Chronic hepatitis (≥6m) due to persitent HBV infection
= HbsAg in serum for ≥ 6month
>persistent infection with Ønecrosis+Øinflammation
↑Transaminases x10
OR x2 compared to previous level
- Mother-child-transmission ⇒ children infected during birth have a 90% ↑risk of becoming chronic HBV carrier !
- sexual
- blood: drugs, needle,transfusions
1-6month
→ markers (HbsAg) become positive after that period
- Subclinical hepatitis
- Symptomatic hepatitis → unspecific symptoms (pain + fatigue)
- rare: liver failure → hepatomegaly, jaundice, hematemesis etc..
- ☠️ Cirrhosis, liver failure, HCC
- simultaneous 🦠HepD infection
- 🧊 cryoglobulinema, 🍎 polyarteritis nodosa, 🥐GN
ALT
↑protrombin time / INR (>1,5)
{kind=link}
- Screening for acute infection:
- If positive: detemine transmissibility
- Acute vs. chronic (persistence)
HBsAg + anti-HBc IgM
HbeAg + HBV DNA
anti-Hbc IgM vs IgG
- Undectable HBV DNA → ↓replication
- HbeAg + HBsAg seroconversion
- Normalization of ALT

- Chronic (HBsAg>6month) & ≥1year
- persistent ↑ALT (>1,5x UNL or >60 IU/L)
- Moderate/severe inflammation / fibrosis
{kind=link}
{kind=link}
{kind=link}
- Acute: HCV infection (HCV-RNA in blood) + transaminase ≥ 10x + known to be negative last 6 month
- Chronic: HCV-RNA detectable for ≥6m
ØTx and
Ødetectable HCV-RNA by 2 negative test ≥6month apart
- during birth (vertical transmission)
- blood-blood: i.v. drugs, medical equipment, needle sticks
- (rare sexual - in comparison to HepC)
6
→ relevant for Tx
T
T
- Mainly asymptomatic ❗
- Non-specific: fatigue, anorexia
- signs of chronic liver disaese (aszitis, hepatomegaly, etc)
- EXTRA-HEPATIC manifestations
- 🧊cryo + 🥐GN
- ☀️ Porphyria cutanea tarda
- 👁️ Eye:
- Sialadenitis (sicca syndrome ; +dry mouth)
- Corneal ulcers
- 🟢 NHL (non-hodgkin lymphoma)
☠️ Cirrhosis, liver failure, PHT (portal hypertension)
(rare HCC)
- History of (possible) exposure
- drug use
- transfusion / transplant
- contaminated blood from doner
- needlestick
- peristent ↑ transaminases
- HIV infection (often HepC co-infections)
- Liver workup: AST, ALT, bili, albumin, CBC, PT/INR
- Serology:
HCV antibodies (6-8w after exposure) = active or past infections
HCV-RNA (1-2w after exposure) = active infection
3. Biopsy → before starting Tx + to rule out DDx
- HCV genotyping

≥6m positive HCV-RNA PLUS ↑Transaminases
OR
positive HCV-RNA PLUS chronic hepatitis on biopsy
- Persistent ↑Transaminases
- Progressive disease (fibrosis)
- +HCV-RNA + ≥moderation inflammation with bridging/portal fibrosis on biopsy
- Less advanced also Tx → prevent progression→ if ≥3y of age
Combination therapy: pegylated INF alpha + Ribavirin📷
{kind=link}
- unknown causes (might be triggered by virus or drug)
- like viral hep
- continuing hepatocellular inflammation + necrosis
- tends to progress to cirrhosis
- +- associated with other AI disease
↓
🍑 variable liver presentation
- most patient: insidous onset
- non-specific: fatigue, anorexia etc
- insidious to fulmunent
- cirrhosis + hepatic failure
🐉 Extra-hepatic autoimmune signs of:
→ i.e. arthritis, vasculitis, nephritis, Coombs, anemia, rash, thyroiditis
- ↑AST+ALT
- ↑ALP + ↑Bili
- ↑IgG (and other IgGs)
- Antibodies
- ANAs,
- Smooth muscl Ab (SMAs,)
- Liver-kidney microsomal type 1 Ab (LKM1)
- anti-liver cytosol 1 Ab (Anti-LC1)
- anti-soluble liver antigen (anti-SLA)
⇒ depending on antibodie results ⇒ different subtypes (2)
Lick my 1 (LKM1) anus (ANA) smoothly (SMA) + lick 1 (LC1) slowly (SLA)
- ↑Aminotransferases prodominent
- Exclusion of other DDx
- Histo+ → interface hepatitis (piecemeal necrosis w/ plasma cell rich infiltrate )
- Immunoreactivity: IgG + Antibodies

Initially Predni → AZA/6-MP (maintaince) → evtl. stop AZA when remission archieved → if relapse start again with predni 🔁
⇒ many require lifelong immunosuppressive therapy and cant stop AZA
⇒ worst case: liver transplant
autosomal recessive disorder
mutation in the ATP7B gene which encodes for Copper-Transporting ATPase (ATP7B2)→ ↓ceruloplasmin + ↑free copper → ↓biliary excretion → accumulation in liver, eye, kidney, CNS (basal ganglia).
{kind=link}
{kind=link}
- ↓Ceruloplasmin (serum)

- ↑Urinary copper (24h)
- Liver biopsy → ↑copper concentration
- EM → copper containing hepatocytic lysosomes
- MRI → for early lesion + 🧠

- copper chelating agents:
- Liver transplant
- zinc (↓GI uptake of copper)
⇒ D-Peniciliamine or Trientine