





Endocrinology & Nutrition
malnutrition = too much/less nutrtion ⇒ undernutrition OR overnutrtion
WHO: malnutrition = energy-demand missmatch (of nutrients)
- Primary (↓intake)
- “Incorrect preparation of formula (too diluted, too concentrated)
- Unsuitable feeding habits (food fads, excessive juice)
- Behavioral problems affecting eating
- Poverty and food shortages
- Neglect
- Disturbed parent-child relationship
- Mechanical feeding difficulties (or motor dysfunction, congenital anomalies, central nervous system damage, severe reflux)”
- Secondary
- ↓Intake secondary (anorexia, oral intake restriction, cancer)
- ↑Losses (malabsorption)
- ↑Needs/metabolism (chronic disease (infection+cancer), trauma, hypoxemia)
- Defective utilization
→ Behavioral factors (child+parent), social factors, environmental factors


hypoxemia:

(genetic (trisomies) , congenital infections, metabolic disorders (i.e. storage dis.))
Acute <3m ⇒ wasting = ↓weight / height
Chronic >3m ⇒ stuntung = ↓height / age
Acute + chronic ⇒ underweight = ↓weight / age
- ↓🍗Protein reserveres
- ↓🫀CV-capacity
- ↓❤️ Bradycardia + ↓BP
- ↓circulation effects: (+ due to loss of micro nutrients i.e. iron + proteins):
- 🐻❄️ PALE skin (or hyper-/hypo-pigmented)
- DRYNESS
- 👁️ dry, pale conjunctiva
- 👄 angular stomatitis, cheilitis
- ↓🫁 capacity
- ↓🤏🏼Micronutrient:
- 👅 glossitis (b12, iron def.)
- 🥄 spoon-nail + dull sparse hair (iron def anemia, nutrtient, vitamin)
→ 💪 Muscle wasting → weakness + skeletal deformities

→ 🧊 Hypothermia (↓metabolic rate)
→ 💦 edema (Kwashiorkor)

→ 💫 ↓wound healing
→ 🧠 neurologic delay
→ 🍑 Hepatomegaly (↓lipoprotein production)
→ 🦷 enamel mottling, delayed eruption
- 🦠Infections (sepsis , pneumonia, gastroenteritis)
- 🧊Hypothermia (due to infection or ↓metabolic rate)
- ↓🍬 Hypoglycemia (due to sev. fasting or sepsis)
- ❤️🔥 HF (due to bradycardia)
- ⏰ Developmental (+cognititve) delay → 🧠 + 📈
- Kwashiorkor
- Antropometric measures
- wasting (weight/height) → acute
- stunting (height/age) → chronic
- less clinical significance: weight/age
- Identify Age and Sex:
- Determine the child's age group (0-23 months or 24-59 months) and gender (boy or girl).
- Measure children aged 0-23 months or less than 87 cm in length (lying down).
- Measure children aged 24-59 months or taller than 87 cm in height (standing up).
- Locate Height/Length:
- Find the figure on the chart that corresponds to the child's length (0-23 months) or height (24-59 months). This is usually located in the left column.
- Identify Weight Range:
- Move horizontally to the right from the figure you found to locate the weight range that includes the child's weight.
- Determine Nutritional Status:
- The label at the top of the column containing the weight range will indicate the child's nutritional status.
- Look for associated changes
- ↓Albumin
- ↓Micronutrients (Iron, zinc, Iodine, Vitamin A, folic acid)
- ↓Lymphos (Immunodeficiencies)
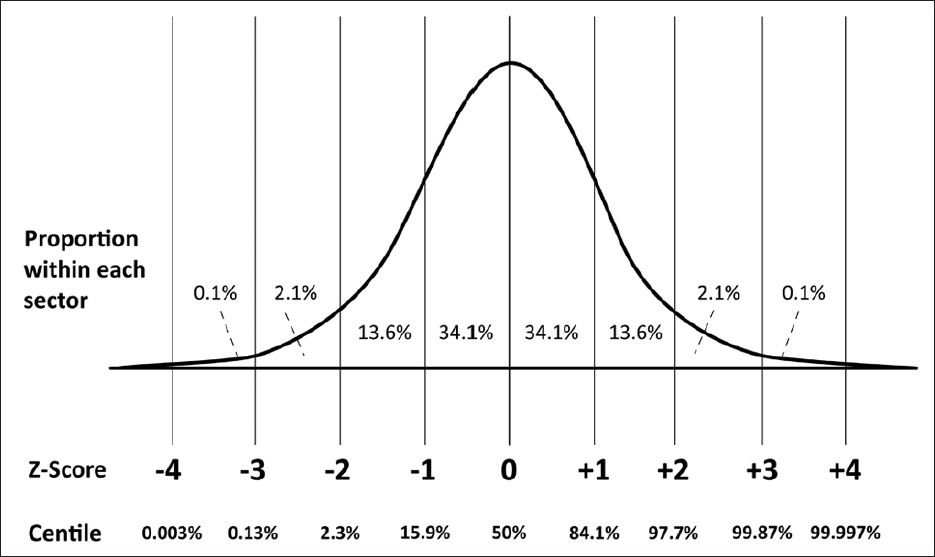
⇒ SEVERITY for ACUTE malnutrition:
(weight/height = wasting)
z-score <(-3) = severe acute malnutrition
z-score <(-2)📷 = moderate acute malnutrtion
{kind=link}
z-score = (X*-m)/SD; *=height, weight or BMI (⇒ in this case: weight in graph for same age + same height)
MODERATE
⇒ ↑ by 25 kcal/kg/day more than daily recommended for age
⇒ food rich in micro-nutrients (iron, zinc, VitA, essential fatty acids)
SEVERE
PHASE 1 - STABILIZATION phase (week 1)
CORRECTION of:
- 🌊 dehydration + acid-base

- 🧂electrolytes (Ca, Mg, K)
- 🦠 infection
PHASE 2 - REHABILITATION phase (week 2-6)
⇒ 🥗 ORAL FEEDINIG: 100kcal/kg/day
→ if <80 kcal/kg/day ⇒ nasogastric tube

⇒ start 🔗 IRON TX

PHASE 3- FOLLOW-UP phase (after week 6)
⇒ 🥗 FEEDING (ad libitum) → to catch up growth

⇒ ⚡ stimulation: emotional + sensory
- follow up during pregnancy + supplements if needed
- monitor growth of children
- promote breastfeeding + adequate feeding
- timly complementary
- hygiene
- correct micronutrtients
- endemic areas: parasites tx + rehydration (if high diarrhea region)
→ i.e. give Vitamin A + iron supplements (also to young children)
weight below 5th percentile OR weight/age curve falls below 2 major percentiles
→ if below 2 ⇒ mild FTT, if below 3 → severe FTT
→ see causes for malnutrition
organic FTT → secondary to disease
non-organic FTT → psychosocial factors
- HISTORY
- Dietary history?
- PMH + FM?
- Development?
- Psychosocial problems?
- trigger?
- child-parent interaction?
- PHYSICAL EXAM
- Organic cause? → dysmorphic features, other features of underlying disorder
- Signs of child abuse?
- Malnutrtion severity + complications?
- LAB:
→ usually Ø needed ⇒ consider workup for organic cause
organic FTT → Tx of underlying etiology
non organic ⇒ multidisciplinary approach:
- health visitor + home nurse
- pediatric dietician
- ↑energy intake strategies:
- concentrated formulas / ↑caloric food
- make it nice: variety or food, include plesant taste fats
- behavioral adjustment
- eat at regular times + with other family member
- encouragement + Øforcing strategies
- 🥇Primary obesity (≥95%)
- Genetic: Parental obesity
- Hypercaloric diet
- ↓Physical acitivty → ↑Sedentary behaviour
- other (Socioeconomic status, maternal factors, infection, sleep deprivation, environment
- 2️⃣Secondary obesity (<5%)
- 🎡 Endocrine
- hypothalamic-pituitary lesion
- Hypothyroidism
- Cushings
- GH deficiency
- hyperinsulinism
- 💊 Drugs
- steroids
- insulin
- contraceptives
- anti-epiletics + anti-psychotics
- 🧬 Genetic
- Single gene disorder (i.e. leptin defic.)
- syndromes
- genetic obesity syndromes ⇒ prader-willi
- chromosomal abnormalities ⇒ Down, turner, klinefelter
maternal factors:

- Clinical picture? (fat child)
- History?
- Anthropometric measurements ⇒ severity? (overweight, obese) (if <2y ⇒ use weight/lenght; >2y ⇒ use BMI / age)
- Abdominal vs. generalized obesity? ⇒ risk of complications? (+ etiological hints) (waist + hip circumference & height)
↓
(FH, growth + development, diet, activity, drugs)
↓
Age Group | Normal | Overweight | Obese | Grades of Obesity |
0-2 years
(weigh-for length) | ≥97th percentile | >99.9th percentile | Risk of overweight: >85th percentile | |
2-18 years
(BMI, percentile) | 5 – 84.9th percentile | 85 – 94.9th percentile | ≥95th percentile | Severe obesity: ≥99th percentile |
Adults
(BMI, kg/m2) | 18.5 – 24.9 BMI | 25 – 29.9 BMI | ≥30 BMI | Class I: 30 – 34.9, Class II: 35 – 39.9, Class III: ≥40 |
↓
Measurement | Abdominal (Android) Obesity | Generalized (Gynoid) Obesity |
Waist Circumference | ≥90th percentile | <90th percentile |
Waist/Hip Circumference Ratio | ≥1.0 in boys, ≥0.8 in girls | <1.0 in boys, <0.8 in girls |
Waist/Height Ratio | ≥0.5 | <0.5 |
Complications | More common | Less common |
↓
- Etiological workup:
- primary vs. secondary?
- Assoc. symptoms of secondary causes: hypothyroidism, cushing, hyperglycemia
- Lab:
- Metabolic profile: lipid, gluc, insulin, liver function
- depending on etiology:
- thyroid
- cortisol levels
- others
Characteristic | Primary Obesity | Secondary Obesity |
Prevalence | ≥95% of cases | <5% of cases |
Family History of Obesity | Common | Uncommon |
Mental Function | Normal | Often mentally impaired |
Stature | Tall (usually >50th percentile) | Short (usually <5th percentile) |
Physical Examination | Otherwise normal | Associated stigmata |
Bone Age | Normal or advanced | Often delayed |
*mentally impaired → genetic syndrome?, **stigmata → dysmorphism, hirsutism, abdominal obesity, sexual development, etc.
- 🫀 CV →HT, heart hypertrophy, arrythmias, Ischemia
- 🧈 metabolic → DM, ↑blood fats
- 🎡 endocrine → precocious puberty, irregular menses, gynecomastia
- 🫁 respiratory → obstructive sleep apnea, asthma
- 💩 GI → GERD
- 🍑 & 🎋 & 🍤 liver + biliary + pancreas → fatty liver, bile stones, pancreatits
- 💪 skin → yeast infection
- 🧠 neuro + psychosocial → HT (pseudotumor cerebri+migraine) + psychological problems
#🥇 NON-PHARMA
- Diet modifications → Stop light diet plan
- Eating habit modification
- Exercise
Quality | Green Light Foods | Yellow Light Foods | Red Light Foods |
Calories | ↓ | ↑ | ↑↑ |
Fiber | ↑ | ||
Fat | ↓ | ↑ | ↑ |
Nutrient | ↑ | ↑ | ↑ |
Sugar | ↑ |
Green Light Foods | Yellow Light Foods | Red Light Foods | |
Types | Fruits, Vegetables | Lean meats, Dairy, Starches, Grains | Fatty meats, Fried foods, Sugar, Sugar-sweetened beverages |
Green Light Foods | Yellow Light Foods | Red Light Foods | |
Quantity | Unlimited | Limited | Infrequent or Avoided |
“b. Do not eat due to boredom, anger or frustration. c. Do not eat directly from the tray. d. Do not eat fast. e. Do not skip meals. f. Do not eat at fast food restaurants (McDonalds,...).
Recommended: a. The child should eat in a room devoid of amusement. b. The child/adolescent should pay attention to hunger and fullness during a meal. c. Food will be served in small plates (to limit the portion size) and will be cut into small pieces. d. Food will be eaten only at meal times. e. Meals will be served along with other family members. f. All family members should adopt the same healthy eating habits.”
↓
#🥈: PHARMA → 💊 Orlistat (if >12y !)

OR
BARITRIC SURGERY:
→ if ≥13y + BMI >40 + complications + failed #1 for 6month
- 👀 early recognition
- 🥗 Promoting healthy eating pattern
- “Promotion of breastfeeding for at least the first 6 months of life.
- Regularly scheduled meals and snacks.
- Age-appropriate portion sizes for meals and snacks.
- Healthy food choices (foods with low energy density).
- Children should never be forced to eat when they are not willing.
- Children should not be punished during mealtimes with regard to eating.
- Foods should not be used as rewards.
- Interactions during meals should be pleasant and happy.”
- 🏃🏽♂️ ↑Physical acitivty
{kind=link}

Vitamin D | PTH | Calcitonin | |
Stimuli for Secretion | ↓ Serum Ca²⁺, ↓ Serum HPO₄²⁻, ↑ PTH | ↑ Serum Ca²⁺, ↑ 1,25(OH)₂D, ↑ FGF-23 * | ↑ Serum Ca²⁺ |
Intestine | ↑ Absorption (Ca²⁺, HPO₄²⁻) | ↑Absorption (via 1,25(OH)₂D) | ↓Absorption? |
Bone | Complex Effects on Ca²⁺ and HPO₄²⁻ | ↑ Release (Ca²⁺, HPO₄²⁻) | ↓ Release (Ca²⁺, HPO₄²⁻) |
Kidney | ↑ Reabsorption (Ca²⁺, HPO₄²⁻) | ↑ Reabsorption Ca²⁺, ↓ Reabsorption HPO₄²⁻ | ↓ Reabsorption (Ca²⁺, HPO₄²⁻) ** |
Serum | ↑ Ca²⁺, ↑ HPO₄²⁻ | ↑ Ca²⁺, ↓ HPO₄²⁻ | ↓ Ca²⁺, ↓ HPO₄²⁻ ** |
Notes:
- * FGF-23 = fibroblast growth factor-23; effects include ↓ tubular reabsorption of HPO₄²⁻ and ↓ formation of 1,25(OH)₂D.
- ** Effects with pharmacological doses.
↓Ca AND/OR ↓Phosphorus
⇒ deficient mineralization of cartilage including growth plates (rickets) / osteoid (osteomalacia)
Rickets | Osteomalacia | |
Defect | 1) Deficient mineralization of growth plate | 1) Deficient mineralization of osteoid |
Location | Metaphyses | Other sites of bone formation (↑ bone turnover or intramembranous bone formation) |
Cell Affected | Chondrocyte | Osteoblast |
Consequence | Accumulation of cartilage | Accumulation of osteoid |
Age | Occurs only in growing organisms (children) | Can occur at all ages (children and adults) |
Association | Children with rickets also have osteomalacia | Adults with osteomalacia do not have rickets |
Rickets/Osteomalacia | Osteoporosis | |
Mechanism | Deficient mineralization | Insufficient formation or increased resorption of bone tissue |
Bone Mass | ↓ | ↓ |
Bone Mineral Density | ↓ | ↓ |
Microarchitecture | Normal | Disrupted |
Mineralization | ↓ | Normal |
Bone Mineral/Bone Matrix Ratio | ↓ | Normal |
Risk of Fractures | ↓ | ↓ |

- Calciopenic rickets (secondary ↓Phosphate)
- Primary calcium deficiency (↓intake)
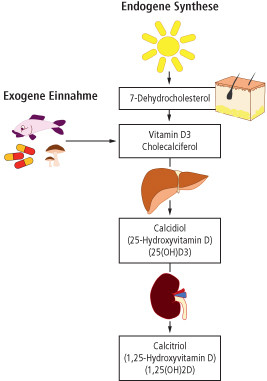
- ↓ Vitamin D-related
- Deficiency (↓intake / ↓sun)
- Malabsorption (i.e. CF, biliary, celiac)
- Enzymes (liver + renal)
- End-organ resistance
- Phosphopenic ricket (primary ↓Phosphate)
- Renal loss of phosphate
liver:

kidney:

(i.e. due to genetic, Fanconi, tumor-induced, renal tubular acidosis)
bone biopsy ⇒ but not really used!
{kind=link}
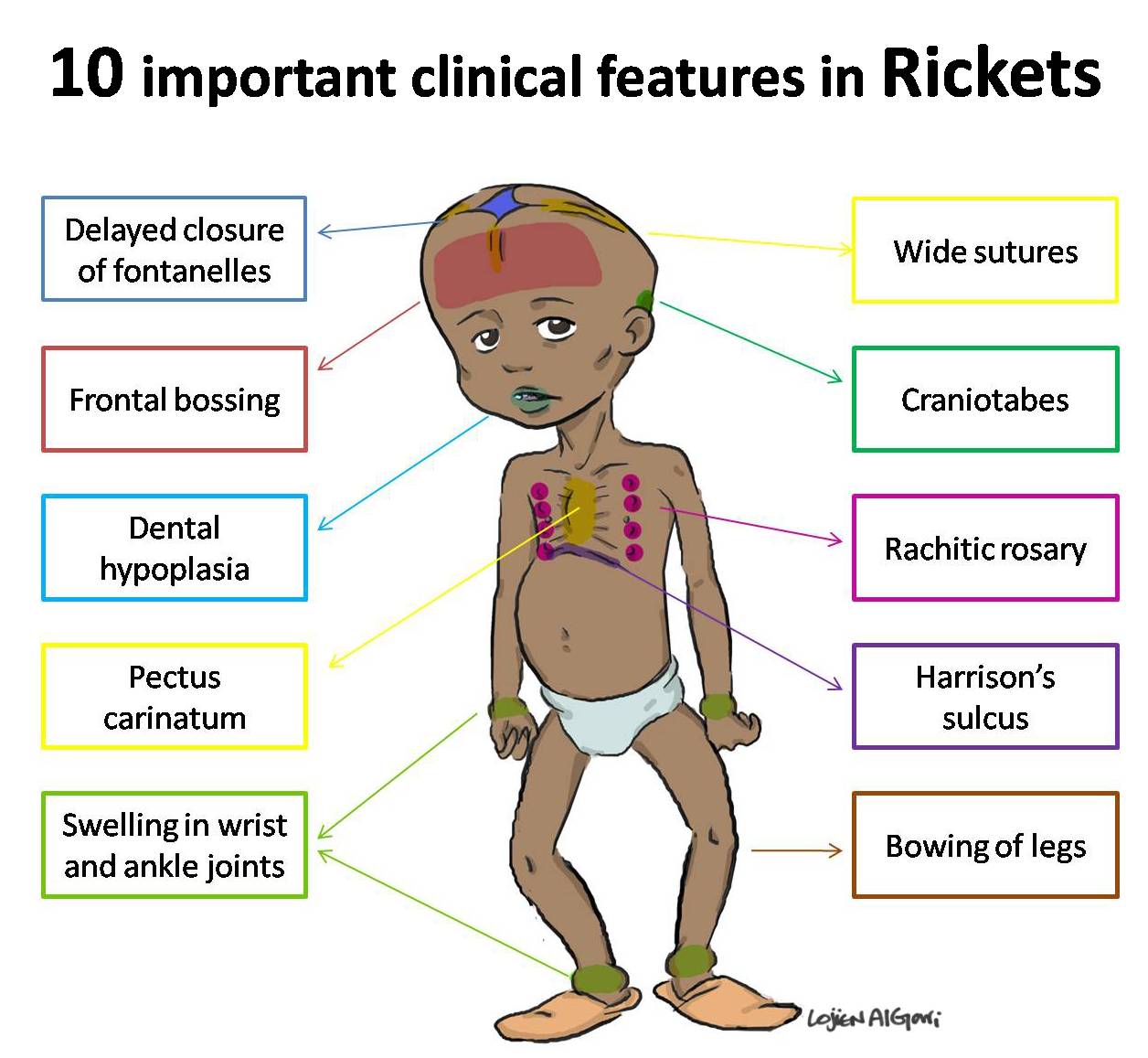
Additional clinic:
- ↓Ca signs = Chwostek+ Trousseau📷 , muscle spasms
- ↓VitD signs = infections, ↑ICP, Muscle tone/weakness → ↓motor development
- Failure to thrive (→ decreased growth)
muscle tone/weakness:



Biochemical Marker | Stage 1 | Stage 2 | Stage 3 |
Calcemia | ↓ | ↓ | ↓ |
Phosphatemia | N (PTH compensates) | ↓ | ↓↓ |
Alkaline Phosphatase | ↑ | ↑↑ | ↑↑↑ |
PTH | ↑↑ | ↑↑↑ | ↑↑↑↑ (compensated) |
25(OH)D | ↓↓ | ↓↓↓ | ↓↓↓↓ |
1,25(OH)2D | N | ↑ | ↑/N/↓ |
- 🦠 Infections → 🫁Pneumonia + 🩸Anemia
- 🐦 chest deformities → 🫁 Atelectasis
- ↓🍦 (Ca) →🧣 Laryngospasm + 🫀- arrhythmia, HF, cardiac arrest
- 🦴 - fractures
Vitamin D + Calcium
+ prophylaxis
Ca >8 mg/dl | Ca <8mg/dl | |
Calcium | p.o. | i.v., followed by p.o. |
Vitamin D | directly | 48h after i.v. calcium |
genetic + environmental trigger → autoimmune response → production specific antibodies → destruction of pancreatic beta cells → absolute insulin deficiency
HLA-DR3 + -DR4
childhood onset <20y (technically at any age)
bimodal peak: 4-6y and 10-14y
- acute (infants) - days 🚨 ⇒ severe dehydration!
- intermediate (#1) - weeks
- slow (children+teens) - months
Onset Type | Commonality | Age Group | Symptom Development | Associated Symptoms | Weight Loss |
Acute | Common in infants | Infants | Rapid, within a few days | Severe dehydration | - |
Intermediate | Most common | - | 2-8 weeks | Symptoms of DM (polyuria, polydipsia, polyphagia) | - |
Slow | Common in children and teenagers | Children and Teenagers | Progressively over months | Severe fatigue, significant weight loss | 5-10 kg |
Cause Number | Hypoglycemia Cause |
1 | Missed/delayed meals |
2 | Excessive exercise or lack of blood glucose monitoring after exercise |
3 | Excess of insulin (too high dose) |
T



DM | Impaired Glucose Tolerance | Impaired Fasting Glucose | Normal | |
Fasting Glucose | ≥126 | <126 | 110-125 | <110 |
Random Glucose | ≥200 | --- | --- | --- |
2-Hour Glucose after OGTT | ≥200 | 140-199 | <140 | <140 |
HbA1c (%) | ≥6.5 | --- | --- | 4-6 |

Short term: Diabetic keto acidosis and hypoglycemia (>60-65mg/dl)
long term: diabetic retinopathy, neuropathy, nephropathy, coronary artery disease

Severity of DKA: (a) Mild: pH <7.3 or HCO3 <15 mmol/L. (b) Moderate: pH <7.2 or HCO3 <10 mmol/L. (c) Severe: pH <7.1 or HCO3 <5 mmol/L.
- Self monitoring → diary
- Ambulatory monitoring → Gluc + HbA1c

→ intermittend or continous (s.c. sensor)

Age (years) | Pre-meal Glucose (mg/dL) | HbA1c (%) |
<6 | 100–180 | 7.5–8.5 |
6–12 | 90–180 | <8 |
>12 | 90–130 | <7.5 |
higher gluc + HbA1c levels are accepted in children
⇒ 📷
{kind=link}
T
Prognosis
- Treatment within 14d of life → normal intellectual development
- Treatment after 14d of life → progressive loss of IQ points
- TSH newborn-screening (before day 14) ⇒ ↑TSH?
- Genetic counseling in genetic forms
{kind=link}
Persistent:
- Primary: Thyroid patho ⇒ ↑TSH + ↓ T4
- dysgenesis (ectopia, aplasia, hypoplasia)
- dyhormogenesis (defective genes for thyroid-proteins involv. in biosynthesis)
- Secondary: TSH, TRH deficiency/resistance ⇒ ↓TSH + ↓T4
Transient:
- Maternal cause:
- Iodine def.
- Antithyroid-drugs
- Antibodies (i.e. anti-TSH-Receptor)
- Idiopathic

- 🎩 CLASSICS
- slowed vital functions:
- 🧊 hypothermia
- ❤️↓HR
- 🚧 constipation + feeding diffuculties
- Skin changes:
- 🌼prolonged physiological jaundice
- dry, pale skin
- myxedema
- +/- 🧣Goiter (in dyhormonogenesis, Ø in dygensis)
- → 🎙️ laryngeal compression (horse, stridor, respir. distress)
- 🐥↓growth + 🧠 psychomotor
- → disproportional stature
- → ↓activity, hypotonia, mental retardation
- 💀Cranio-facial features
- Large fontanelles
- Facies
- → macroglossia 👅
- → coarse facial features 📷
- Positive Diagnosis (LAB)
- Newborn screening: ↑TSH
- Symptomatic → ↑TSH + ↓ T4
- Etiological Diagnosis
- US + Scinti→ dygenesis? large?(dyshormogenesis)
- Xray → bone age
- Gene mutations → familiy recurr. risk?
L-Thyroxine p.o. lifelong (synthetic T4)
- Clinic: Physical + psychomotor development

- Lab: T4 + TSH
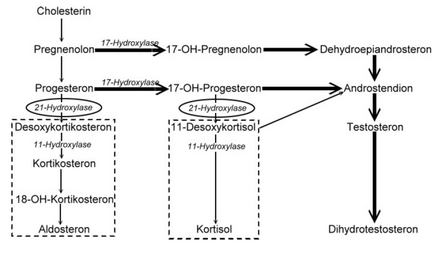
autosomal recessive disorder → 21-hydroxylase deficiency 📷
{kind=link}
⇒ ↓ steroids (cortisol) (+↓Mineralcorticoids (Aldosterone) in salt-losing type)
⇒ ↑Androgens ⇒ virilization
= male seccondary characteristics occur (hirsutism, deep voice, ↑muscles)
↓steroids
→ ↑ACTH → Adrenal hyperplasia
→ ↓growth

male external genital + female internal genital (UTERUS + OVARIES)
T → 85%
(and/or clitoromegaly)

Occurs at 1-4 weeks of age
↓🧂mineralcorticoid deficiency
- Hypotension, High K+. low Na+
↓steroids
- 😴Fatigue + lethargy
- 💩GI: nausea, vomiting, diarrhea → dehydration
- Weight loss + anorexia
- ❤️CV: hypotension → shock, cardiac arrhythmias, death

other signs of virilization
→ menstrual abnormalities
→ precocious puberty
→ acne + hirsutism
→ infertility (anovulation)
- Lab
- Hormones (see table types above)
- Salt-loosing: ↓Aldosteron → ↓Na + ↑K + metabolic acidosis
- ↓Steroids → ↓Gluc
- Imaging
- CT adrenals
- US + Urogenitography → internal organs
- Hand Xray → bone age
- Genetic analysis
metabol. acidosis:

- Correct electrolytes + acidosis
- Hormone supplementation:
- steroids → Hydrocortison p.o. physiological dose (↑in stress)
- mineralcorticoids → Fludrocortison p.o. + salt
- Surgery → ext. genitalia correction
- Psychosocial
stress = surgery, febrile illness, multiple trauma,..
- new born screening
- prenatal dgx
- corionic villi sampling
- amniocentesis
height <3rd percentile (>2 (1.9) SD/z-score) for age,sex,ethnicity
OR height percentile < target height base on parents height
Target height:
In boys = (Father's height + Mother's height + 13 cm) / 2 In girls = (Father's height + Mother's height - 13 cm) / 2
height curve crosses lower percentile lines
OR
↓height velocity (=growth rate):
if normal height: height velocity/bone age <3rd percentile
if short height: height velocity/bone age <25 percentile
proportionale → limbs proportionate to trunk (i.e. familial short stature)
disproportinate → LIMBS disproportionate SHORT to trunk (i.e. skeletal dysplasia)
- Lower body segment = Symphysis pubis to the floor.
- Upper body segment = Height - Lower body segment.
⇒ Calculate U/L ratio
Normal average values: newborn = 1.7; 2 years = 1.4; 10 years = 1.0.
- Genetic (parents height)
- Nutrition
- Hormones:
- Thydroid
- GH + IGF-1
- Androgens + Estrogens
- non-pathologic:
- familial short stature
- Constitutional growth delay
- pathologic:
- syndromes:
- Turner
- Laron
- Down
- skeletal dysplasias
- 💨 CF

Skeletal abnormalities Gonadal dysgenesis Congenital cardiovascular defects
tissue insensitivity to growth hormone (GH) due to GH receptor mutation (leads to ↓ linear growth)
↓
Microcephaly Prominent forehead Saddle nose Hypoglycemia Delaved puberty
probably caused by selctive IGF deficiency
↓
Craniofacial dysmorphia Skeletal abnormalities Developmental delay Obesity
- ENDOCRINE CAUSES: (see all subtopics)
- 🦴Rickets + 🥐CKD (↓VitD)
- 🍬DM1
- 🦋Congenital hypothyroidism
- ⛺ Congenital adrenal hyperplasia
- 🐳GH deficiencies
- 🌝 ↑Glucocorticoids
- NON-ENDOCRINE CAUSES:
- 💩 malabsorption (IBD + Celiac)
- 🫐 Chronic hypoxia → anemia + CHD
- 🐉Rheuma + Immuno: JIA + Immunodef.

- Maternal substance abuse → esp. alcohol → smoking, cocaine,..
Intrauterine growth retardation = low birth weight + length! + Skeletal anomalies
- Psychosocial short stature (abuse)
Emotional deprivation/stress that involves neglect, abuse, or a poor relationship between the patient and caregiver
↓
• Poor growth or weight gain • Poor record of school attendance and medical care • Signs of child maltreatment • Clinical and radiographic signs of abuse
- Psychiatric → anorexia nervosa

⇒ 📷
{kind=link}
GH → IGF-1 synth. by liver
- IGF-1 binds to IGF + insulin receptors → cell growth + proliferation, inhibit apoptosis
- incr. secretion of Somatostatin → inhibit [neg. feedback]
- lipolysis
→ bone, cartilage, skeletal muscles, skin, ST, organs incr. in size
→ impaired glucose tolerance (due to action on Insulin-R)
Kidney:
- incr. reabsorption Phosphorus + inc. excretion Ca
- incr. Na + Water reabsorption
- ❓Idiopathic (congenital or acquired) ⇒ 🥇
- 🧠CNS
- congenital malformation
- acquired: secondary CNS lesions
- others:
- functional
- Amphetamine Tx



- ↓Height parameters
- Height <3rd percentile = short stature
- Height velocity/bone age <3rd (if still normal height)/25th(if short) percentile = failure to grow
- ↓Target height
- Consider DDx: Etiological Dg-workup for short stature
- Additional clinical findings suggestive for GH deficiency:
- Neonate:
- 🍬↓ - Gluc
- 💀↓ - microcephalus
- 🌼 hepatitis + prolonged jaundice
- Child:
- 🧠 - CNS history (PMH or FH)
- 🧄 - multiple pituitary hormone deficiency (Adenoma)
GH def = proportial + ↓height+velocity + ↓bone age

“In a child: cranial irradiation, head trauma, central nervous system infection, consanguinity or an affected family member, craniofacial midline abnorma- lities, signs indicative of an intracranial lesion, signs of multiple pituitary hormone deficiencies.”
GH deficiency → growth retardation (during childhood) Prolactin deficiency → Ø lactation after delivery FSH/LH deficiency → hypogonadism (hypogonadotropic hypogonadism) TSH deficiency → hypothyroidism ACTH deficiency → adrenal insufficiency
- Paraclinical workup:
- Xray → ↓ bone age
- Lab: ↓IGF (IGF-1 + IGF-BP3)
- GH stimulation test (2 positive tests)
Two different positive GH stimulatory tests; positive test = GH <10 ng/mL post- stimulation; stimuli: sleep, exercise, clonidine, arginine, insulin, glucagon, L-dopa, propranolol, glucagon, GHRH.
GH (somatotropin)
⇒ s.c./transdermal
- Hypersensitivity
- Acute or progressive disease
- acute critical illness
- active malignancy
- progressive intracranial lesion
- Closed epiphyses
- Renal transplant

Indicated in short stature due to:
- GH defic.
- Turner + other syndromes (noonan, prader-willi)
- non-pathologic: idiopathic, small for gestational age
- CKD BEFORE transplant
- HT (Na + Water reabs)
- fluid retention
- pseudotumor cerebri
- Insulin Resistance + lipolysis
- DM + pancreatitis
- bone, cartilage, skeletal muscles, skin, ST, organs incr. in size
- gynecomastia
- scoliosis
- Target height archiev
- ↓Growth rate (<2,5cm/y)
- Bone age >14/16 (f/m)
- Fused epiphysis (Hand wirst xray)
- serious SE
- refusal