





Emergencies
an elevated body temperature due to change in the hypothalamus, >38°
hyperthermia is caused by physical mechanisms, such as excessive internal heat production due to exercising, malignancies, dehydration, what so ever
pyrogens
Exogenous pyrogens: eg induced through microbial organisms → parts of cellwall (Liposaccharide)
Endogenous pyrogens: → increase the hypothalamic set point!
- IL1/IL6
- TNF alpha
- cytokines
- fever with local signs
- fever without a source
- fever with unknown origin
fever with localizing sigs:
- signs of localized infections in physical exam and history
fever without a source (of infection):
- lasting ≤ 1 week, without explanation after history and examination
fever of unknown origin
- >1week, without localizing signs, no explaination after evaluation
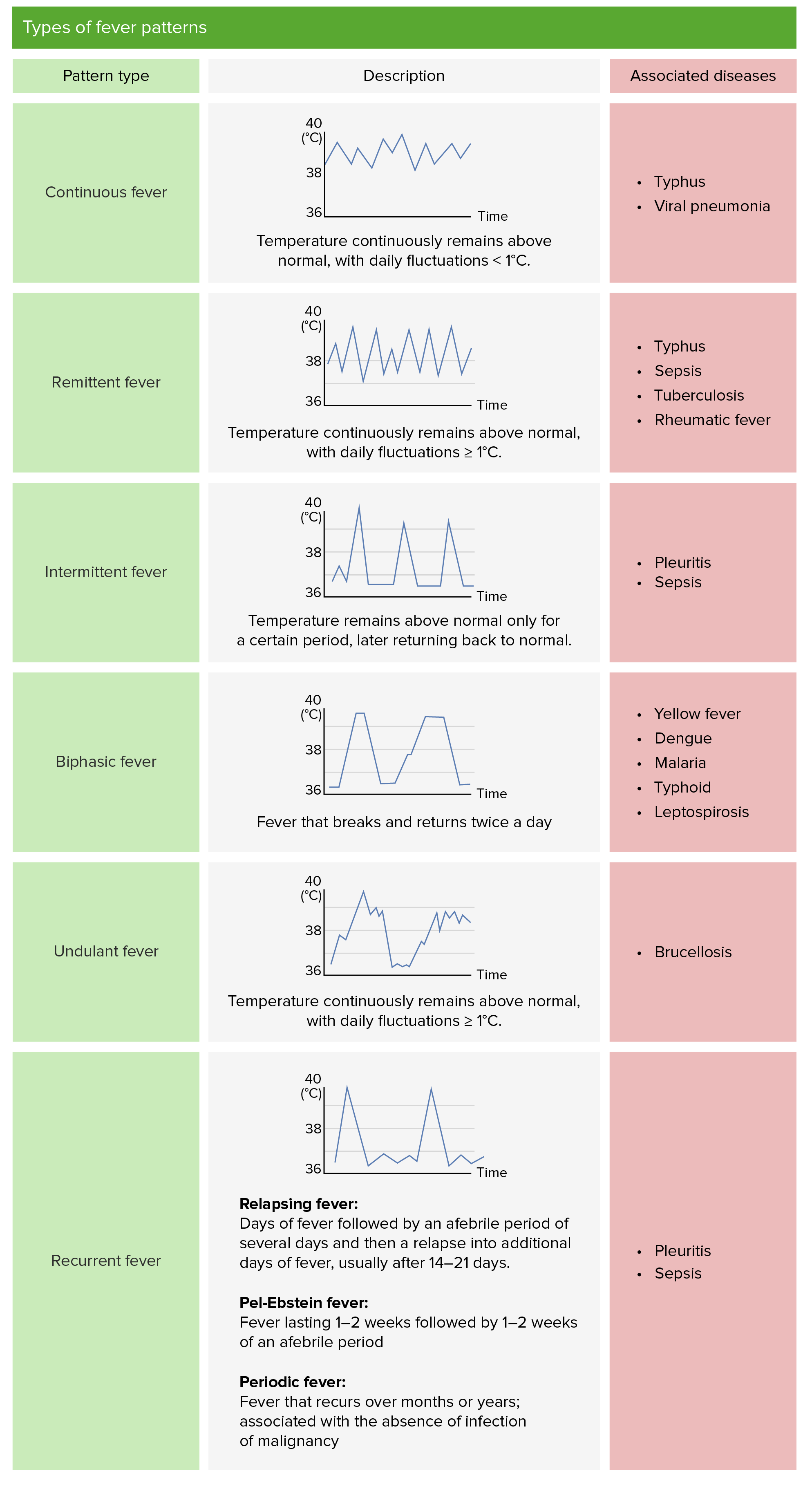
⇒ 📷
- continuous fever (above normal through day, fluctuation <1°C)
- remittend fever ( fluctuating >1°C in 24h but never normal)
- intermittend fever (normal temp periods)
- recurrent/relapsing fever (short febrile episodes between days of normal temo)
- Undulent/wavy fever (like recurrent but smaller variation + low grade fever insted of normal periods)
- hydration and general measures
- anti-pyretic treatment

A child or infant presenting with a fever >38C (axillary or rectal) without a readily identifiable source on history and/or physical examination (<1w)
- duration
- path. past (PM& FH)
- travels
- immunization
- Decr 🧠activity – lethargy
- poor perfusion &cyanosis
- hypoventilation/hyperventilation
- it’s indicated in assessment of febrile children up to 36 month
- “how toxic is the child?” → predicts serious infections
Assessment Criteria | Normal
(Score = 1) | Moderate Impairment
(Score = 3) | Severe Impairment (Score = 5) |
Cry | Strong OR Ø cry | Whimper OR sob | Weak cry moan |
Reaction to stimulation | Cries briefly OR content | Cries, stop and then cries again | Persistent cry OR hardly respond |
State | Awakens easily | Difficult to awaken, drowsy | Not arousable OR falls to sleep |
Color | Pink | Pale extremities OR acrocyanotic | Pale Cyanotic mottled |
Hydration | Eyes, skin, and mucosa - moist | Eyes, skin - normal Dry mouth | Sunken eyes Dry skin Dry mucous membranes |
Response | Alert, smiles | Alert OR brief smile | Ø reaction |
Score | Interpretation | Prevalence of Serious Illness |
6 - 10 | Healthy | 2.7% |
11 - 15 | Moderately Ill | 26% |
> 16 | Toxic | 92.3% |
bacteria:
- Listeria
- B strep
- Ecoli
🍺💩🩸🧠
- CBC
- Infectious parameters
- blood cultures, Urin analysis, stool analysis and culture
- LBP

ampicilin and cefotaxime/genta
- goru B streps
- PMH
- pneumokokken🫐
- Haemophilus🔻
- Menigokokken🍒
rochester criteria
Ø signs of infection:
Clinical criteria - No prior illness - Well appearing infant - Full term birth
Laboratory screen - WBC normal (5,000 to 15,000/uL) - Band neutrophils <1,500/pL - If diarrhea is present, fecal WBC <5/high-power field - Urine WBC < 10/high-power field
AB: Ceftriaxone or observation without AB
observation*:

ampicillin and gentamicin OR ampicillin and cefotaxime
(Same)
- PMH
- pneumokokken 🫐
- haemophlus🔻
- meningokokken 🍒
- salmonella ❗
Evaluation , 24h follow up

- if all cultures negative → monitoring and observation (antipyretics)
- if positive: parenteral AB
- antipyretic treatment, 48h reevaluation
evaluation → ampicillin and cefotaxim/genta


PMH
- pneumokokken🫐
- haemophilus🔻
- meningoikoken🍒
persisting fever
- PMH (Pneumokokken, Hemophilus, meningokokken) is most common etiology
- AB-Tx indicated if infection proven or high probability
- Give Ampicillin + Gentamycin/cefotaxime
- Antipyretics if Fever >39
bacteria in the blood of a febrile child without sepsis signs and no focus of infection
can cause serious illnesses like meningitis, osteomyelitis, sepsi, pneumonia…
- Pmh
- pneumokokken 🫐
- Haemophilus 🔻
- meningokokken 🍒
- salmonella ❗
- Children between 6 and 36 months.
- Signs of infection
- Temperature >39°C.
- WBC >15,000/mycroL.
- Elevated neutrophil count, ESR, CRP.
resolves spontaneously sometimes
but you give AB:
- Amoxicillin
- 2nd or 3rd gen cephalosporin
- A single dose of ceftriaxone 50-75 mg/kg is superior to oral antibiotics treatment
- Resolve fever
- Clear bacteremia
- Prevent meningitis
> 38.3°C (100.9°F) lasting for > 3 weeks (in book >1 week) with no clear etiology despite appropriate diagnostics (Øsigns, symptoms, paraclinic)

lupus/JIA/sarcoidosis/VAsculitis/Kawasaki

leukemia/lympoma
- resp/UTI/bone/joint
- rare:
- toxoplasmosis
- lyme disease
- malaria
- viral (EBV;CMV;HIV)
- abscess
- osteomylitis
- duration
- travel
- pets
- drugs
- immunization
- pathological oast
- General:
- lymphadenopathie
- skin examination
- rashes/jaundice
- Resp, cardio and abdomen
- hepatosplenomegaly
- new murmurs
- Joint swelling
- Head:
- Eye exam
- uveitis (always sign for rheumatic shit going down)
- conjuctivitis
- Oral cavity examination!
- CNS
- meningitis
- focal neurologic deficit
basically everything, coz your clueless
- infectious
- CBC
- blood smear

- cultures
- serum test (Viruses)
- urinary analysis
- US 🫀+ abdomen
- CT, MRI
- Lymphnode biopsy
- stool culture
- bone marrow exam
- tuberculin test
depends on your final diagnosis, but empirical AB administration (according to book)
Amboss says: (basically the exact opposite👀 → only in very severe cases)
- Febrile seizures
acute or chronic inability of the respiratory system to maintain gas exchange → leads to failure of oxygenation (PaO2 of < 60 mmH) and failur of decarbonization (PaCO2 of > 50 mmHg)
a clinical syndrome of acute respiratory failure, signs associated with difficult, labored or uncomfortable breathing
- abnormal breathing rhythm, speed, amplitude, pattern
- Tachypnea/bradypnea/apnea
- Irregular rythm of breathing
- hyperpnea
- seasaw movements
- orthopnea
- nasal flaring
- chestwall retractions
- head bobbing
- Grunting+Gasping
- tripod position


ARDS is a severe inflammatory reaction of the lungs to pulmonary damage and respiratory distress simply the signs of diffictult breathing
Hypoxia means low o2 delivery to the tissue
hypoxemia means low oxygen saturationof Hb (low SaO2)
obstructive, restrictive resp disease and disease affecting gas transfer
can be cause by:
- Hypoxemia (Less O2)
- Less O2 in
- low athmospheric O2
- 🫁respiratory failure
- ventilation perfusion mismatch
- diffusion disorder
- hypoventilation
- shunt
- 👶🏽right left shunt congenital heart defects (less lung perfusion)
- abnormal Hb (less O2 binding/quantitative decreased binding capacity)
- 🐼Anemia (Less Hb)
- 🩸Shock (Less blood)
- histotoxic hypoxia (eg cynide poisoning; less uptake)



- decreased Co2 elimination
- hypoventilation
- primary
- compensatory (metabolic alkalosis)
- severe ventilation perfusion mismatch
- increased Co2 production
- fever, sepsis, seizure
- metabolic acidosis

- cyanosis in late stages
- sweating (diaphoresis)
cyanosis appears, when the HbH (unsaturated Hb) concentration is higher than 5g/dl in the capillary blood
the blood turns blue, as the light absorption spectrum of unsaturated Hb is in a bluisher area as the absorption of saturated blood, which is more red
- dyspnea, resp distress
- tachypnea
- hyper/hypotension
- arrythmia
- tachy/bradycardia
- confusin/altered mental status
- anxiety/restlessness
- seizures
- coma
- flushed skin
- sweating
- Dyspnea, resp distress
- apnea
- Hypertension
- tachycardia
- restlessness
- tremor/ataxiasomnolence
- slurred speech
- coma
↓PaO2 (<60) + normal/↓ PaCo2
↓PaO2 and ↑ PaCo2
- Increasing O2 delivery to the cell
- reducing O2 demans
- Increasing Co2 removal
- decreasing Co2 production
- increasing O2 delivery by:
- reliving the obstruction (A)
- increase ox concentration (give O2 +- intubation)
- increse ventilation (mask-bag, Cpap or mechanical)
- reduce O2 demand by:
- reducing breathing work
- reduce met demand (tret infection/fever/termal changes)

- increasing CO2 removal by:
- decresing ventilation-perfusion mismatch
- increasing ventilation
- decreasing CO2 production by:
- decresing Carbohydrate load
- treatment of fever/infectins/met acidosis
Infants: ⇒ tachypnea
→ worse during feeding + diaphoresis,
→ poor feeding/↓weight gain
Older: ⇒ dyspnea + edema (puffy eyelids, swollen feet )
🎠Ross Heart failure classification: 📷
→ Mainly depending on grade of respiratory distress
classic
Echo, EKG, xray, cardiac marker (BNP)
- Positive inotropic (↑contractability)
- negative chronotropic + dromotropic (↓SA + ↓AV)
- positive batmotropic (→automatism in cardiac tissue → Atrial or V arrhythmias🚨)
- Positive tonotropic (↑Tonus + ↓size of the heart→better oxygen consumption)
inhibits Na+/K+- ATPases in cardiomyocytes → Increased intracellular Na+ levels→ reduce the efficacy of Na+/Ca2+ exchangers → higher intracellular Ca2+ concentrations.
⇒ the force of contraction becomes stronger (positive inotropic effect)
- ❤️🔥worsening of HF ❗
- ECG:
- sinus bradycardia,
- AV-Block (↑PR-interval)
- Arrythmias → ventricular + SVT
- 💩 GI: nausea + vomiting, diarrhea
- 👁️ visual disturbance (objects appear yellow) + restlessness/fatigue
- stop digitalis
- Tx of arrhythmias(i.e. lidocaine, propanolol) + block (atropin)
- Correct predisposing factor (i.e. ↓K, renal disease, cardiac disease)
- Antidigitalis Antibody ⇒ Fab fragments
- 🌊 Diuretics
- 💠 ACEi
- 🧨 Nitrates
- 🚣🏽 Hydralazine
- General measures: O2, sedation, salt+ fluid restritction
Inadequate supply of O2 ⇒ demands of vital organs not met (inadequate organ perfusion and tissue hypoxia)
A. Hypovolemic shock
- Severe gastroenteritis
- Blood loss
- Burns
- Diabetes mellitus or insipidus
B. Cardiogenic shock
- Heart failure: acute myocarditis, cardiomyopathy
- Arrhythmias
- Obstructive: cardiac tamponade
C. Distributive shock
- Sepsis
- Anaphylaxis
Pre-Shock
compensated, non-progressive shock
appears IMMEDIATELY after triggering event
Compensatory mechanisms only:
- Peripheral vasoconstriction
- 💪 🧊 cold + clammy + ↓recap
- may be absent in distributive shock ❗
- ❤️ ↑HR
- 🥐 Oliguria
Shock
decompensated, progressive shock
- ✨ ↓BP
- Hypoperfusion →🍼 Lactic acidosis (high AG metabolic acidosis)
⇒ 🧠 Altert mental stage
⇒ DIC
⇒ worsening tachypnea
End-organ dysfunction
irreversible shock
ORGAN FAILURE due to ISCHEMIA, INFLAMM. MEDIATOR + REPERFUSION INJURY
- 🧠 - autonomic dysfunction
- 🧠 - ↓/↑ activity
- ⇒ ❤️ - ↓↓output
- ⇒ 🫁 ⇒ ARDS ⇒ micro-thrombi
- ⇒ 🥐 ⇒ ischemia, oliguria, ↑↑RAAS + tubular necrosis
- ⇒ 🍑 ⇒ ischemia ⇒ ↑transaminases
- ⇒ 🍤 ⇒ ischemia ⇒ translocation of gut bacteria ⇒ septic shock
- ⇒ 🩸 (coagulation) ⇒ DIC + Thrombocytopenia
Phase: | ☀️Warm shock
(early) | 🧊 Cold shock
(late) |
HR | ↑ | ↑ |
Extremities | warm | cool |
Skin | flushed | pale
↑capillary refill |
Pulses | bounding | diffic. to palpate |
Mental state | altered | altered |
Urine output | ↓ | ↓ |

- Quantitative = arousal / responsiveness
- Alert - normal response
- Lethargy - difficult staying awake, responds easy to any stimuli
- Obtundation - stimulation → delayed answer
- Stupor - only reaction to repeated painful stimuli
- Coma - complete unresponsiveness
- Qualitative = “content” of mental function
- Delirium (acute confusional + agitated state) - fragmented attention, conc. + memore
Ø perception
Ø reactivity
PLUS autonomic troubles
(⇒corneal + pupillary reflex might be preserved)
- External causes:
- Trauma
- Infections
- Tox
- Internal causes:
- Metabolic
- Ischemia (vascular path, hypoxia)
- Space occupying lesion (tumor)
- Epilepsy
- CNS Damage (ext. or int.) - aka “NEUROLOGIC“ COMA
- diffuse cortical,
- midbrain, dienchephalon (thalamus),
- reticular system (brainstem)
- Systemic: metabolic, toxins
⇒ ASSYMETRICAL COMA (see exam findings)

⇒ SYMMETRICAL COMA
Unresponsive patient
↓
ABC
↓
- FND?
- Intracranial hypertension?
- REFLEXES: Pupils: Light reflex? (fixed mydriasis) Vestibulo-ocular reflex: Dolls eye? Caloric ?


→ Cerebral herniation?


{kind=link}
{kind=link}
{kind=link}
Dolls eye:

Caloric test:

{kind=link}
↓
ETIOLOGY SEARCH:
- trauma signs?
- fever? (infect)
- seizure signs? → tongue bite
- metabolic signs?
- intox signs?
- pre-existing neuro disease?
→ smells? → skin changes? →sweating? tremor?
ETIOLOGY?
- EMERGENCY CT → IF FND! (hemorrhage?)
- MRI: structural, infection?
- Lab-Screening:
- INFECTION: CBC + inflammatory lab
- consider CSF analysis
- consider blood cultures
- METABOLIC: liver function, BGA, Guc, Elektroly, urea, crea
- TOX-screening (urine)
- Fundoscopy (ICP?)
- EEG (seizure suspected)
- stabilize vital function (like in shock)
- etiological Tx
- prevention of coma complications

- Genetic /idiopathic & Congenital(+perinatal)
- Genetic
- 5-20y
- Øother neuro signs
- FH+
- congenital = malformation
- infancy / early childhood
- structural (gross abnormalities / features of underlying disease)
- head trauma ( young + old) + tumor → compressive hemorrhage
- strokes, degenerative disease (old)
- Metabolic
- immune / infection
(DM, Elektrolytes dysbalance, waste product accumulation (kidney), nutritinal def., phenylketonuria, intox / withdrawl)
provoked → immediate preceeding cause
unprovoked → unknow etiology OR pre-existing (progressive) cause
ANY OF THE FOLLOWING:
- ≥2 seizures (unprovoked/reflex) >24h apart
- 1 unprovoked seizure and similar recurrance risk as “1.”
- EEG abnormalities (inter-ictal)
- Neuro-exam abnormalities
- seizure during sleep
- Symptomatic secondary cause (tumor, prior CNS infection)
epileptic seizures ≥5min (for tonic-clonic)
(Øconciousness in this time aka generalized)
Status epilepticus is a seizure that lasts ≥ 5 minutes or a series of seizures in rapid succession without full neurological recovery in the interictal period
Focal (unilateral → may spread) | Generalized (bilat) | |
Origin | Single hemisphere | Both hemisphere |
Awareness | aware or impaired | Ø |
Symptoms | Motor (↑/↓)
Non-motor (sensory, cognitive, autonomic) | Motor (Tonic clonic or other motor)
Non-motor |
- clonic: sustain rhythmic jerking (automatism movement - i.e. lip smacking, automated movements)
- unilat. body
- may spread prox. (”jacksonian march”)
- tonic: ↑tone (sec-min)
- atonic: ↓/Ø muscle tone
- myoclonic - short brief single / series of muscle contraction (jerks)
- hyperkinetic: irregular large amplitude (”chorea-like”)
- automatism: repeating automatic actions
Øtonic-clonic
- Sensory (somatosensory, visual, auditory, olfactory, gustatory, vestibular)
- Cognitive → cortical symp (aphasia, agnosia, memory, hallucination, alexia, etc)
- Emotional (everything imaginable; unapproriate bursts of laughter)
- Autonomic
(cardiac, GI, cutaneous, respiratory, urination, lacrimation, etc)
- Tonic-clonic (”grand mal”) - 1-3min
- Tonic (w/ expiratory sound in beginning)
- Atonic → brief ”drop attack” or unilateral sagging (seconds-min)
- Myoclonic → brief (seconds) jerk
- Epileptic spasms → on awakening sudden brief flexion, extension or mixed proximal + truncal muscles
Øhyperkinetic + Ø automatism
- Typical absence
- abrupt onset + offset of conciousness-loss (5-10(15) sec)
- multiple times a day
- memory impaired (retrograde)
- +/- assoc. features
- +/- minor clonic movement (twitching) of face + eye muscles
- +/- automatisms
- Øpost-ictal phase
- Atypical absence
- Less abrupt onset + offset
- Less loss of conciousness
- ASSOCIATED w/ loss of muscle tone (head, trunk, limb)
- Myoclonic absence
- jerks → shoulder + arms
- with tonic abduction → lifting of arms during seizure
(i.e. starring with variable loss of conc.)
→ history taking from observing person + patient!
- Before:
- trigger? (syndrome?)
- aura? (Ø in generalized)
- During:
- duration of seizure? etc
- trauma during seizure?
- ↓/Øconciousness? (awarness, memory, response, sense of self)
- After:
- UMN signs ? (FND, aphasia) →structural
- classic postical?
→ talk + response + comprehend? retrograde amnesia? autonomic?
- look for trauma
- Aspiration? → SpO2 + auscultation
- CV workup (ECG → rhythm+ rate, pulse, BP, prolonget QT? carotid murmors?)
- Neurowork-up: diffuse vs. focal? (see below) ⇒ assymetries (face, pupillary)
⇒ aphasia? ⇒ pronator drift
⇒ Babinski might be + (normal)
- EEG
- Background: asyymetry + slowing
- Interictal phase → Spikes, sharp waves, spike-wave-complex 📷
- Sleep deprivation provocation
- MRI → structural abnormality?
- Lab (gluc, tox, electrolytes, CBC)
- fever/infection? → Lumbar puncture
- others
A group of paroxysmal, reversible, neurological symptoms that typically precede an attack of migraine or seizure and vary in intensity and duration.
⇒ Aura can manifest with a multitude of symptoms: e.g., visual (e.g., flashing lights, scotoma), motor (e.g., paresis), somatosensory (e.g., paresthesia), vestibular (e.g., dizziness), vocal (e.g., aphasia), or olfactory (e.g., hyperosmia) symptoms.
NON-EPILEPTIC SPELLS:
- Febrile seizures !!🤒
- tremor
- DDx: loss of conciousness ⇒ vasovagal, arrhythmias, autonomic dysfunction
- Aural: migraine
- motor: TIA
- psychological disorders
{kind=link}
Focal (unilateral → may spread) | Generalized (bilat) | |
Origin | Single hemisphere | Both hemisphere |
Awareness | aware or impaired | Ø |
Symptoms | Motor (↑/↓)
Non-motor (sensory, cognitive, autonomic) | Motor (Tonic clonic or other motor)
Non-motor |
- clonic: sustain rhythmic jerking (automatism movement - i.e. lip smacking, automated movements)
- unilat. body
- may spread prox. (”jacksonian march”)
- tonic: ↑tone (sec-min)
- atonic: ↓/Ø muscle tone
- myoclonic - short brief single / series of muscle contraction (jerks)
- hyperkinetic: irregular large amplitude (”chorea-like”)
- automatism: repeating automatic actions
Øtonic-clonic
- Sensory (somatosensory, visual, auditory, olfactory, gustatory, vestibular)
- Cognitive → cortical symp (aphasia, agnosia, memory, hallucination, alexia, etc)
- Emotional (everything imaginable; unapproriate bursts of laughter)
- Autonomic
(cardiac, GI, cutaneous, respiratory, urination, lacrimation, etc)
- Tonic-clonic (”grand mal”) - 1-3min
- Tonic (w/ expiratory sound in beginning)
- Atonic → brief ”drop attack” or unilateral sagging (seconds-min)
- Myoclonic → brief (seconds) jerk
- Epileptic spasms → on awakening sudden brief flexion, extension or mixed proximal + truncal muscles
Øhyperkinetic + Ø automatism
- Typical absence
- abrupt onset + offset of conciousness-loss (5-10(15) sec)
- multiple times a day
- memory impaired (retrograde)
- +/- assoc. features
- +/- minor clonic movement (twitching) of face + eye muscles
- +/- automatisms
- Øpost-ictal phase
- Atypical absence
- Less abrupt onset + offset
- Less loss of conciousness
- ASSOCIATED w/ loss of muscle tone (head, trunk, limb)
- Myoclonic absence
- jerks → shoulder + arms
- with tonic abduction → lifting of arms during seizure
(i.e. starring with variable loss of conc.)
- Generalized epilepsy
- = generalized seizure type
- typical findings: EEG (interictal/inctal)
- FH+ ?
- types: Childhood Absence Epilepse, Juvenile Absence Epilensy, Juvenile Myoclonic Epilepsy, Generalized Tonic-Clonic Seizures Alone
- Focal epilepsy
- = focal seizure type
- typical findings: EEG (interictal)
- structural cause? (→ imaging!!)
- Combined (both)
- general + focal seizure type
- typical EEG findings for both
- Cause: Syndrome (Dravet + Lennox)
WEST SYNDROME (starts after 3-12m) - general poor prognosis, Tx: vigabatrin/benzos
- Spasm
- ↓Development
- EEG: Hypsarrytmia (severe chaotic brain activity) 📷
- ≥2 seizures (in <24h)
- 1 unprovoked + 1 of the following:
- EEG abnormalities (inter-ictal: epileptic form)
- Symptomatic secondary cause (tumor, prior CNS infection)
- Neuro-exam abnormalities
- seizure during sleep
- FH+
avoid triggers
- sleep
- avoid drugs+alcohol
- ↓stress
- others
caution in dangerous situation
- driving
- swimming/bathing
psychological

2 seizure free years
- Ketonic diet
- Vagus n. stimulator (refr. FOCAL)
- Surgery
- resection of focus (pot. curable)
- partial resection of region to prevent spread(palliative)
- esp in MESIAL TEMPORAL LOBE EPILEPSY !!
>5min OR ≥2 discrete seizures w/ incomplete conciousness recovery
#1 Benzos (after 5min)
↓
#2 Anti-epileptics (25min later (after 30-40min))
Non-pharma: clear environment, put something under head, let him shake → after: lat. decubitus
- First seizure?
- trauma?
- dyspnea?
- Drug indication (≥5min, ≥2 seizure)?
- mainly normal children
- all drugs have teratogenic risk
- stick to monotherapy
- add-on: folate
{kind=link}

LOOK FOR CAUSE OF FEVER ‼️
- Lab
- <18m OR >18m + clinical suspicion ⇒ Lumbar puncture (meningitis?)
- Imaging + EEG
treat underlying cause (💊AB)
fever → antipyretics
if >5m (status epilepticus)→ benzos
Øanticonvulsants!

pathological state caused by a toxic substance
- mediactions (family)
- cleaning agents
- plants
- cosmetics
- too much paracetamol (→liver failure)
- lead
- antidepressants
- gases
- CO
- hydrocarbons
- caustic agents (acidic/alkaline)
- medications

0.1%
- known poisoning with known poison
- known poisoning with unknown poison
- unknown poisoning with unknown poison
clinical features of intox, importaint when you don’t know what your intoxicated with
anticholinergic means activation of the sympathicus → now the signs might be easier to remeber, as sympathicus makes you ready to fight or flee
- red, warm dry skin → hypertermia
- tachycardia
- hypertension
- seizures
- confusion, disorientation, coma
- ataxia, myoclonus
- hallucination
- delirium
- dry mouth
- mydriasis (large pupils)
- agitation
- mushrooms
- atropin
- Antihistamines
- Antiparkinson
- carbamazepin
- tricyclic antidepressants
cholinergic means, that the paraysympathicus is activated → rest and digest
- muscle weakness
- fasciculation
- paralysis
- confusion, coma
- urinary incontenence
- diarrhea, emesis
- bronchospasm
- miosis (small pupils)
- lacrimation
- excessive salivation
- sweating
- nicotine
- insecticides (Organophosphate pesticides poisoning)
- mushrooms
- tremor
- rigidity
- ophistotonus
- stiff neck
- oculogyric crisis

- trismus
- tongue protrusion
- Phenothiazides
- heloperidol
- metoclopramid
- fever
- tachycardia
- hyperpnea
- agitation
- seizures
- metabolic acidosis
- lethargyy, cona
salicylates

phenols
It is a methemoglobin former, neurotoxin, and irritant. Acute amounts of 1 to 4 grams (oral) can be lethal in adults. It serves as an auxiliary substance for the synthesis of numerous chemical compounds and pharmaceuticals, such as acetylsalicylic acid.
ONLY IN CONSULTATION WIT A TOXICOLOGIST
all of criteria need to be met:
- ER will be facilitated in 1 h or less, ingestion less than 90 minutes ago
- severe toxity risk
- no alternative treatment available
- ipecac will not affect the therapy in hospital
- no CI
- ingestions of caustics

- coma/seizure
- ingestion of things, that can induce coma/seizure quickly
- cardioresp maifestations

- Syrup of ipecac.
- Dishwashing liquid (3 tablespoons in a glass of water).

basically not recommended, only in toxic agents without alternative and 60 minutes after ingestion
- Ingestion of caustics, hydrocarbons.
- Previous esophagus or stomach surgery.
most effective technique in toxins that can be absorbed by activated charcoal
- metals (surprise)
- insecticides
- cyanide
- alcohols
- organic solvements
- hydrocarbons
→ funktioniert demnach eigentlich auch nicht so wirklich
- Intestinal obstruction/perforation.
- Altered mental status.
- Caustics, hydrocarbons.
1g/kg/dose → max 60g/dose in water/juice
- slowly absorbed substances
- substances not adequately absorbed by charcoal

The answer is always “active charcoal”
(&dialysis)
every 4-6 hrs
unprotected airways
abdominal problems (peritonitis/ileus)
- doesnt work too well, limited value in forced diuresis
- urinary alkalization helps to eliminate weak acids
- electrolyte disturbances
- patients with HF, RF,Pulm edema, cerebral edema
Dialysis + similar
- peritoneal dialysis, hemodialysis
- hemofiltration
- hemoperfusion
- exchange transfuion
whats the antidot againts…
O2!
(&hyperbaric chamber)
Vitamin C 🍋 IV
methylen blue IV 🔵
Atropin
naloxone
amyl nitrite and sodium nitrite followed by sodium thiosulfate
acetylcystein
- ABC
- treatment of renal failure, rsp failure, metabolic/ph/electrolyte disturbances
200mg/kg/dose in children

👃🐷 = 💀(major system)
75mg/kg/day in children for consecutive days
- 🤮Initial stage (0-24 hours)
- nausea, vomiting
- ❌Asymptomatic stage (24-48 hours)
- increased transaminases
- 🍑Liver stage (3-4 days)
- further increase in transaminases, progressive liver, failure, coagulopathy, renal failure
- 🏁Final stage (begins after 4-5 days)
- liver recovery or progression to complete liver failure → you die of inner bleedings (coagulopathy)
Signs of liver failure (&renal failure)
- hypoglycemia
- incr. transaminases and bili
- prolonged APTT and QUick
- BUN and creatinine increased
GI decontamination
Antidote: acetyl cystein