





Cardiology

= chapter genetic + birth defects
- Genetic (Trisomy 21, Turner)
- Environmental (Teratogens, maternal exposure, infection (rubella))
Eisenmenger’s syndrome (R-L shunt) 📷 = CYANOSIS
The left-to-right shunt will raise pulmonary artery pressure → pulmonary hypertension (PH) develop (Initially reversible, then becomes irreversible) [+ RV hypertrophy]
→ When pulmonary vascular resistance exceeds the systemic one → the direction of flow becomes right-to left (Eisenmenger's syndrome) 📷
- Cyanosis
- Stroke + Brain abscess
- HF
⇒ Hypoxic spells (periods of central cyanosis) 📷
→ Squatting for shunt reversal



Etiology:
🧬 genetic + 🏭 environmental
Patho:
- classic (L-R→🫁PHT→RVH + Eisenmenger(R-L))
- ØLV invovlement ‼️
Classification
- Size ⇒ small vs. large
- Location: 📷 Mainly: Ostium Secundum (75%), Ostium Primum (20%) , Sinus venosus defect (5%)
Etiology:
genetic
associated with fetal alcohol syndrom and down syndrom
Patho:
- classic (L-R→🫁 PHT→RVH + Eisenmenger(R-L))
- ↑Volume + pressure overload of RV compared to ASD

- LV 🌊 volume overload + ❤️🔥 HF

Classification
- Size ⇒ small (<1cm → irrelevant) vs. large (>1cm → relevant)
- Number ⇒ single vs. multiple
- Location: 📷
Mainly: Muscular & Perimembranous
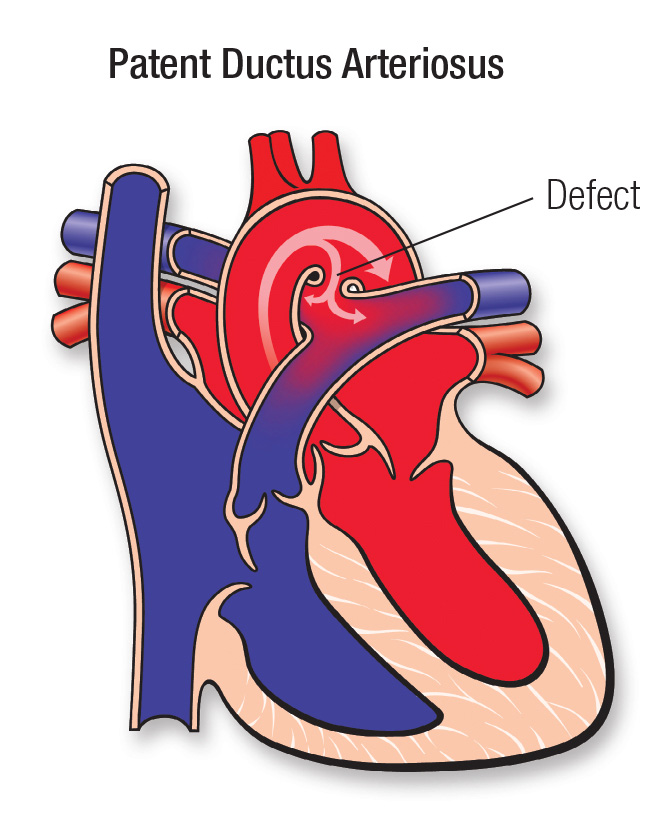
Etiology:
🕝 preterm, 🗑️ rubella, genetic
Patho:
⇒ 📷
- 🫁 Pulmonary HT → Eisenmenger’s
- ❤️🔥 HF
Classification
- Size ⇒ small (self-limited) vs. large (relevant)
- small → asymptomatic
- large → decreased exercise tolerance, failure to thrive
- 🩺auscultation
- Systolic murmur (functional pulmonary stensois)
- Second sound (split)
- signs of pulmo congestion + low output


- asymptomatic if small
- decrease exrcise tolerance and heart failure symptons if severe
- dyspnea
- systolic murmur (functional pulmonary stenosis+ holosystolic-shunt Murmor)
- compensatory: tachycardia + tachypnea
- bounding pulse, prominent suprasternal and caroit pulsation

small → asymptomatic
large PDA
- pulmo overload
- dyspnea
- Respiratory tract infections
- heart failure symptoms
- tachypnea, tachycardia
- continuous heart murmur (left intraventricular)
- bounding pulse (notice: bounding pulse might be found in VSD+PDA)
- suprasternal carotid pulsations
- eisenmerger → cyanosis
- all can be asymptomatic → imaging necessary
- Clinical picture depends on Phase and is similar for all:
- Signs of congestive HF + low output syndrome including compensatory tachycardia (esp. in VSD +PDA
- Systolic murmur
- PDA+VSD: bounding pulse
- If eisenmenger (shunt reversal) → central cyanosis

- 🩺History + physical exam
- investigations
- 🔉 echo
- ☢️ chest xray
- 🔌 ECG
=goldstandard
- estimates size and location
- and RV (right ventricular) and PA (pulmonary artery) pressure can be stimated
pulmo hyperemia + right heart enlargement:
- cardiomegaly

- pulmo congestion: large main pulmonary artery


same as ASD
- location/size/number of VSD
- RV and PA pressure
- cardiomegaly
- pulmo congestion: increased pulmonary vascular markings

- right ventricluar hypertrophy
- + left heart volume overload!:
- left ventricluar hypertrophy signs
- Left atrium dilation
- size, location
- RV and PA
- direction and magnitude of shunt through PDA
- normal or cardiomegaly with LAE und LVE
- pulmo congestion:
- MPA visible
- pulmonary vascular markings
- normal
- or LVH and RVH in large PDA

in all cases Eisenmerger syndrom

- 🎶 arrythmia (coz of the bundle branch block)
- 🧫 infective endocarditis (flow alterations)
- 🫁pulmo V-overload:
- Pulmonary hypertension
- resp infections
- Eisenmenger
- ♦️ paradox embolism

- ❤️🔥heartfailure in large VSD
- 🧫infective endocarditis
- 🫁 pulmo overload
- Pulmonary HT
- ♦️paradox embolism

- ❤️🔥heart failure
- 🧫infective endocarditis
- 🫁pulmo overload
- pulmonary HT
- recurrent pneumonia
- all cause complications due to
- 🫁overload
- 🧫endocarditis


- ASD → 🎶Arrythmia

- VSD + PDA → ❤️🔥HF
- ASD + VSD → ♦️paradoxic emboli
- Endstage = Eisenmenger
→ generally: small VSD, PDA and ASD might close spontaneously and don’t necessarily need treatment
in severe cases: sUrgERy
what exactly?

- 💊 medical Tx (❤️🔥, 🧫. prophylax, ❌🏋️♀️)
- Percutaneous or surgerical Tx closure
- ASD + VSD ⇒ percutaneous expanding device or patch
- PDA ⇒ percutaneous coils/occluder or ligation + INDOMETHACIN

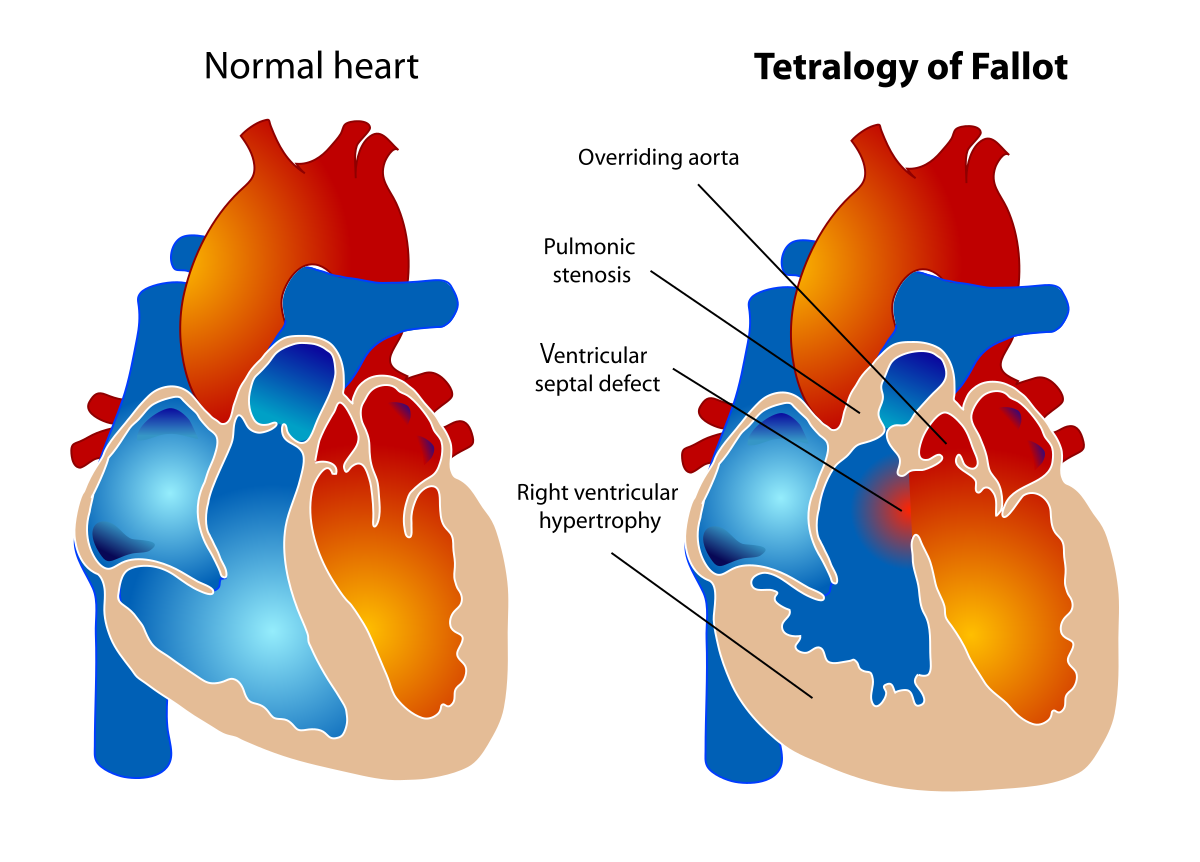
⇒ 📷
- pulmonary stenosis
- → right ventricular hypertrophy
- VSD
- overriding aorta
The term "Overrding Aorta" refers to a specific malposition of the aorta in connection with a high-septum defect in a congenital heart defect:
The main artery, which usually originates in the left ventricle, is shifted to the right in the phenomenon of the riding aorta, thus riding over the hole in the heart septum, and thereby receiving blood from both ventricles.
- 🧬genetic (sporadic)
- associated with deletion of ❌chromosome 22
- malformationas in general associated with 🍷maternal alcoholism during pregnancy
left to right shunt due to VSD → right ventricular outflow obstruction → increased pressure in the RV → RV hypertropy and right left shunt → deoxygenated blood from RV can get into systemic circulation immediatly coz of overriding aorta → cyanosis and hypoxic spells with squatting
- tachy- + dyspnea on exertion
- hypoxia
- feeding difficulties and failure to thrive
- cyanosis, clubbing of fingers and toes
- systolic murmur
- Polycythemia

RVH & less blood in lungs
- boot shaped shilouette 📷→ hypertrophy, right atrial enlargement
- reduced pulmonary vascular markings

- RVH signs
- axis deviation bcs of hypertrophy
- pressure gradient due to obstruction can be measured
- VSD can be identified
- overriding aorta can be seen
- hypoxia 🧙🏻♂️
- cyanosis becomes more severe
- hypoxic spells
- infective endocarditis 🧫
- brain abscess (septic embolism)
- ♦️ embolism → strokes


- surgery → complete repair of the defects
- Hypoxic spells:
- oxygen
- reversal of shunt → knee chest position
- ↓pulmo obstruct → propranolol
- correct acidosis → bicarbonate



- genetic
- assocuated with alcoholism of the mother
- diabetes
- rubella
- but the real cause is unknown
⇒ 📷
- anatomical reversal of pulmonary artery and aorta → two seperate circulations, without any exchange of blood between them
- so the only chance, oxgenated blood can get into the body circulation is via a septal defect or PDA
- cyanosis at birth
- dyspnea and feeding difficulties
- tachypnea
- cyanosis
- systolic murmur (VSD)
- Heart failure signs (esp. RV - HF)
- unresponsive hypoxemia if ASD/VSD/PDA close → death
SEVERE HYPOXEMIA
- egg shaped heart 📷

- ↑pulmo volume: pulmonary vascular markings
same as TOF
⇒ RVH

- visualization of transpositons 📷
- transposition: PA emerges from the LV and aorta arises from the RV.
- Proximal segments of the great arteries run parallel
- Aorta is placed anterior and to the right of the pulmonary artery.
- Communication shunt: VSD, ASD, PFO, PDA (otherwise ☠️)
- heartfailure ❤️🔥
- death ☠️
- 💊 mediacal:
- prostaglandin infusion to keep PDA open
- heart failure tx: inotropic agents + diuretics
- 🔪 surgery: arterial switch in first 2 weeks if Ø VSD
- 🎈Cardiac catheterization and balloon atrial septostomy 📷
inotropos:

- multifactorial
- genetic
tricuspid valve is displaced into the ventricle towards the hearts apex → RV atrialization →reduced RV function and tricuspid regurgitation → hypolasia of the RV and dilation of the RA ⇒ “RV atrialization”
⇒ Bulging of the large sail-like anterior tricuspid leaflet into the RV → RVOTO → ↑ right heart pressure → ↑ flow through the patent foramen ovale → right-to-left shunt → cyanosis
→ reduced cardiac output and increased pressure in RA
→ right left shunt through ASD/PFO 📷
→ pulmonary perfusion via PDA + depending on RVOTO
classic +
- cyanosis, heartfailure in neonates
- dyspnea and palpitations
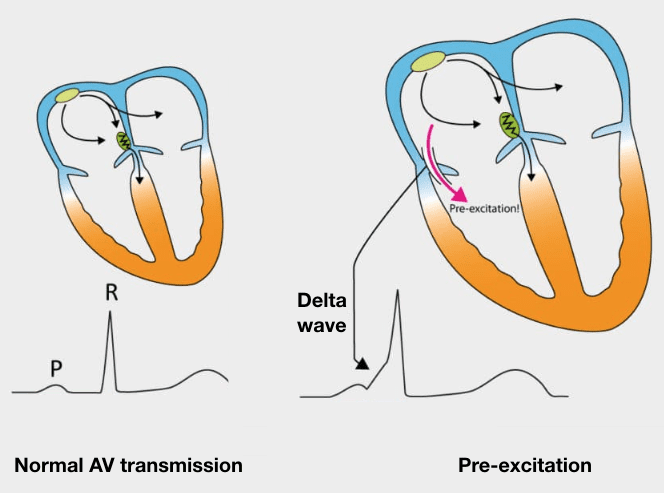
- SVT (supraventric. tachycardia)→ ebstein anomaly is associated with Wolf-Parkisnon-White syndrome

- hypox ⇒ cyanosis, clubbing of fingers/toes
- systolic murmurs (tricuspid regurg + shunt)
- HF signs
- triple/quadruple rythm
- displacement of the tricuspid valve, regurgitation (Duplex)
- RA enlaregd, RV small
- conduction shizzl
- RBBB
- first degree AV block
- WPW
- RA dilatation
- cardiomegaly 📷
(balloon shape)
- ❤️🔥RV and LV dysfunction
- heartfailure
- 🎶 SVT ass eith WPW
- 🧫infective endocarditis
- ♦️paradoxal embolism (stroke and abscess)
- medical: prostagalndin E1 to maintain PDA open
- low output ❤️🔥HF Tx : Ionotropic aganets (i.e. Digox preffered)
- 🧫endocarditis prophylaxis
- 🧪correct metabolic acidosis
- Surgery
- 🔪repair/replacement of valve and ASD closure 📷

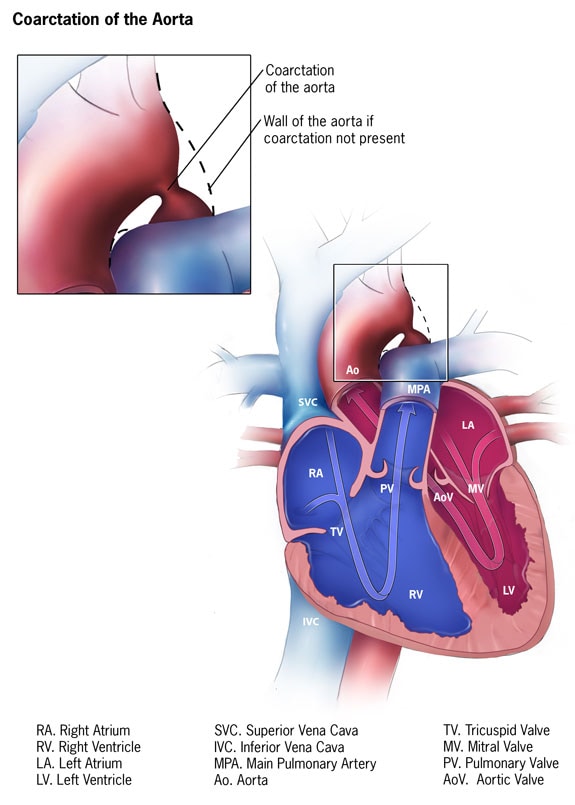
⇒ 📷

can be asymptomatic or signs of ↓perfusion
- poor weight gain
- ciculatory shock sogns
- weakness
- >20 mmHG BP difference between arms

- systolic murmur (stenosis)
- direct signs of ↓perfusion
- pallor (reduced blood flow after obstruction)
- oliguria/anuria (Ø blood for 🥐 kidneys→ Ø diuresis)
- circulatory shock and acidosis
- weak peripheral pulses
- tachypnea, dyspnea
- LV failure
- ↓perfusion (distal)
- renal failure
- ↑perfusion (prox)
- hypertension → intracranial hemorrhage
- infective endocarditis
- recoarctation

genetic
dysplastic valve (bicuspid)
- asymptomatic (in mild - moderate)
- ↓output
- exercise intolerance, chestpain syncope
- HF
- systolic ejection murmur
- ↓output
- weak peripheral pulse
- HF signs
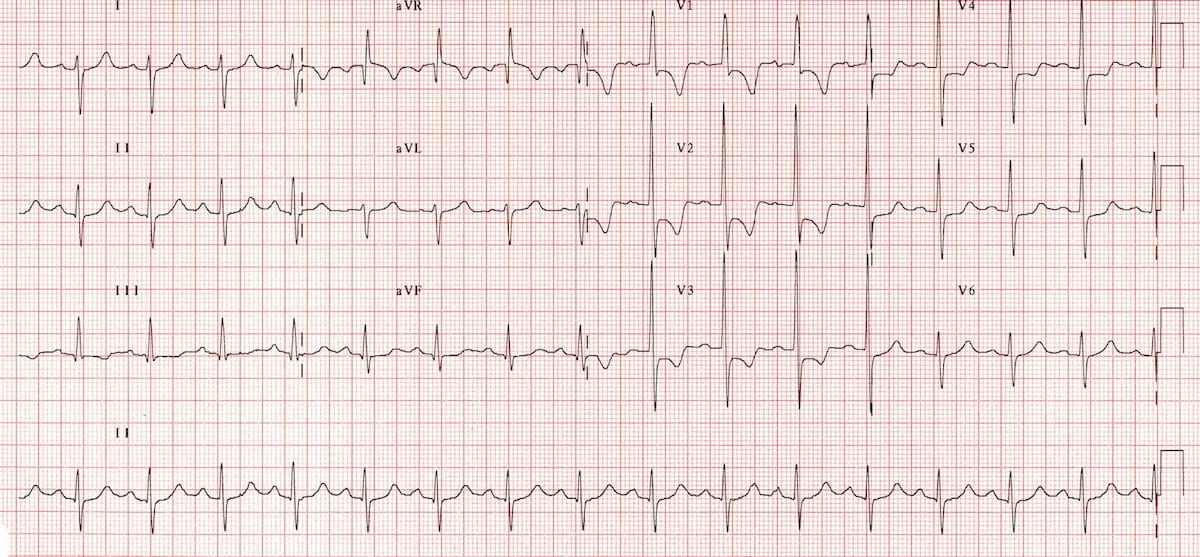
- 🧠mental retardation +🧝 elf facies if supra-valvular aortic stenosis (williams synrome) 📷
- Confirmatiotion of aortic stenosis = pressure gradient estimation
- LOCATION
- bicuspid aortic valve
- subaortic membrane
- narrowing supravalvular As
- normal heart size/cardiomegaly
- +-pulmonary venous congestion

- if valvular: dilated post-stenotic ascending aorta
- normal/LVH
- Heartfailure, + syncopes → death
- endocarditis
- Aortic regurgitation (=double trouble)
- medical:
- Prostaglandin
- HF treatment
- endocarditis proph.
- O2
- Surgical:
- Complete valve repair: valvuloplasty, valvulotomy, myectomy
- Palliative repair: balloon dilatation.

Endothelial damage

⇒ initial nidus ⇒ colonization ⇒ formation of vegetation
⇒ valvular damage (HF) + Extracardiac (septic emboli + immuncomplexes)
surgical or transcatheter ❤️interventions. (⇒ iatrogenic)
- FUNGI (aspergillus + candida)
- BACTERIA
- Enterococci (esp. E. faecalis)
- Strep Viridans (dental 🦷procedures)
- Staph Aureus (!assoc. with invasive 🔪 procedures)
- Hemophilus
- others
AB prophylaxis in high risk patients before dental procedure (🦷)

FEVAH FROM JANE
- 🔥Fever + B-sympt
- 🩺 Changing heart murmor
- Extra-cardiac:

- 🫀
- Destruction of valve / chordae tend.)
- 🎶 Conduction patho (block, arrhythmia)
- ☠️ Septic embolus
- 🧠 stroke, seizure, abscess
- 🫁 PE (if right sided or abnormal connection)
- 🎾 abscess (spleen, kidney)
→ Valvular insuff. → ❤️🔥 HF

⇒ DUKE CRITERIA: 📷


MAINLY VIRAL (parvo, adeno, herpes, EBV, CMV) →Coxsackie and Chagas as well!
other causes: immune, collagen deposition d., drugs/toxins
Phases:
- direct viral injury
- immune response
- recovery / fibrosis (⇒ HF + DCM)
⇒ inflammatory infiltrate → necrosis of myocardium (Øischemic)
⇒ immunohistochemical (IHC): Antibodies (in tissue biopsy)
- Asymptomatic
- 🫀
- signs of HF → dyspnea, chest pain, tachycardia, syncope, hemodynamic compromise, sudden cardiac death
- Arrhythmia (foci)
- EKG:
- 🎶 ↑HR: sinus tachycardia
- arrythmias / block
- ☠️ necrosis: ST/T changes
- Echo:
- Motion: hypokinesia, (global / segmental)
- +/- pericardial effusion
- Lab - Enzymes: Trop + CK/CK-MB
- Others:
- Cardiac MR (edema/hyperemia, necrosis)
- Biopsy → IHC analysis


usually without sequella
⇒ few patient: DCM, HF, death

Hospitalization
↓
Conventional ⇒ HF Tx (symptomatic Tx)
(diuretics, ACEi/ARBs, BB)
↓
Non-conventional/specific ⇒ antiviral / immunosuppression
(interferon beta + antiviral, IVIG, Immunosuppressives)
myocardial disorder (→ small areas of degeneration/necrosis/fibrosis) → LV chamber dilation → systolic dysfunction ⇒ ending in congestive HF

- Idiopathic (+ Genetic)
- myocard dysfunction
- Myocarditis
- Neuromuscular dystrophies
- ischemic (post-MI)
- Valvular
- Toxic (i.e. doxorubicin)

- Signs of systolic dysfunction (↓exercise capacity, acute left ventric. failure [LVF])
- Signs of congestive HF (dyspnea, edema)
- assoc. disease signs
- arrythmias ***
- ECG → LV enlargement? → sinus-tachycardia + ST changes? (myocarditis) → arrythmias
- Echo → ↓EF (systolic dysfunction) + Dilation
- Cardiac markers: NT-proBNP 📷 ⇒ HF?
- others: cardiac MR + screening studies
- Symptomatic
- HF Tx ⇒ diuretics/ACEi + Inotropic agents (digoxin)
- If arrhythmias → anti-arrhythmic
- L-carnitine 🥕
- Anti-thromb. Tx (stasis = ↑thromb risk)
- transplant

- unexplained LV hypertrophy
- ØLV chamber dilation (DDx DCM)
- diastolic dysfunction (abnormal relax.) +/- ventricle outflow obstruction
- in children: Ventricular hypertrophy = septal wall thickness ≥ 2-3x normal SD (age+sex adjusted)

→ ischemia
Mainly ❓ idiopathic
1/3 familiar /🧬 genetic:
- syndromes (i.e. noonan sy.)
- metabolic inborn errors (=worst prognosis)
- 🛣️ non-obstructive → eqally distributed hypertrophy (like in HT)
- 🚧 obstructive → assymetrical hypertrophy of interventricular septum → subvalvular aortic stenosis (septum bulges into aortic outflow tract) → drag effect aspiration of mitral valve → systolic ant. movement of mitral valve (SAM) → more stenosis ⇒ 📷

- ❤️🔥HF:
- ⬇️ low output syndrome → chest pain(ischemia→ sudden cardiac death), syncope
- 🚰 congestion
- 🎵 Arrythmias
- ↑HR → ↑interventricular septum contractility + ↓ filling time → ↑obstruction
- ↓LV volume → more obstruction
severity of asymmetric hypertrophy
⇒ 〰️ ECG + 🦇 ECHO
- HF (↓HR + decr. afterload) + Arrhythmia ⇒ 🎺BB + 🍦CCB = 👍
- ØDIURETICS ❗
- 🔪Septel myectomy (if severe + obstructive HCM)
Incessant (continous): >4-6w but <3m; Øremission
Recurrent: symptom free ≥4-6w
Chronic: >3m
- Echo
- Parvo (B19)
- Herpes (type6)
- Coxsacke
⇒ other less common causes: bacteria, fungi, parasites autoimmune, neoplastic
- Precordial pain
- Pericardial friction rub
- ECG changes
- pericardial effusion (sometimes)
↑ in inspiration + supine
- cardiac tamponde
- constrictive pericarditis (panzerherz)
- Spread → assoc. Myocarditis
≥ 2 of the 4:
- Clinic:
- Precordial pain
- Pericardial friction rub
- Echo → Effusion
- typical ECG changes (↑ST, ↓PR)
ACUTE:
Hospitalization
↓
NSAIDS (1-4w) + Colchicine 🌺
RECURRENT: immuno (AZA, IL1-antagonist, IVIG)
CHRONIC: Pericardiocentesis/pericardectomy ( in constrictive pericarditis)
ASYMPTOMATIC OR
palpitation
Pause after VEs (”skipped beat) → then strong post-extrasystolic beat after pause
→ check pulse! → VEs + pause can be felt
- different morphology
- wide QRS >120ms
- ST + T waves reversed to ST+T from normal QRS complex
- Monotope or polytope (aka polymorphic /monomorphic aka multiple focis vs one foci) 📷
- Isolated or systematized:
- refractory phase after extrasystole → postextrasystolic compensatory pause = distance pre-post extrasystolic QRS = 2x normal RR interval

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Benign | Malignant | |
Cause | stress (i.e. fever) | structural |
During exercise | disappears | increases |
Multifocal (polymorphic) | - | ❌ |
≥2 in a row (≥bigeminus) | - | ❌ |
occurs on preceding T-wave | - | ❌ |
- benign → ØTx
- malignant:
→ correction of organic disease
→ anti-arrhythmics ⇒ lidocaine, amiodaron
rapid atrial non-sinusoidal acitvation
rate 150-250/min (>150)
- Re-entry AV-node: dual slow or fast pathyway (aka AVNRT)
- accessory pathways (orthodromic vs. antidromic)
- pathologic foci in atrium
Palpitations (suddenly begin + stop and can last sec-hours)
if >200:
chest pain (ischemia due to high demand)
acute HF (if persistent for 48-72h)→ syncope (low output syndrome due to ↑↑HR)
{kind=link}
{kind=link}
#1 Vagal + Adenosine
stable → Rate (BB, Verapamil) or Rhythm control (Amiodaron, IC: Propafenone, Flecainide)
unstable → shock
⇒ Ablation for definite prophylaxis
{kind=link}
Normal: <90 percentile
Pre-HT: >90 percentile OR BP>120/80
HT: ≥95 percentile
Stage 1 ≥95 + 5mmhg
Stage 2 ≥99 + 5mmhg
- Primary HT → Dg of exclusion
- mild HT
- 🍿 overweight & FH+
- Secondary HT:

- 🚫 Asymptomatic
- 🧠 Headache, visual, seizures
- 👃🏼epistaxis
- 🫀 palpitations, tachycardia, chest pain
- 🥐 Renal workup:
- Lab:
- BUN, crea, uric acid, electrolytes
- renin + aldosterone
- urine: culture + urinanalysis
- Imaging:
- US
- scinti
- 🥇 Metabolic → 🧈 Lipid profile
- 👁️ Eye Workup: → fundoscopy
- Other organ evaluation: 🫀 + 🌶️
- non-pharma (classic)
- Drugs: classics
- TX OF ENDORGAN DMG
→ diuretics, BB, ACEi/ARBs, CCB