
Table of content
- Thoracic Surgery
- 💨 Pneumothorax
- 💥 Thoracic trauma
- 🧫 Pleural empyema
- 🌊 Malignant pleural effusion
- 🦀 Lung cancer
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6

Thoracic Surgery
💨 Pneumothorax
- Primary spontaneous pneumothroax (PSP)
- spontaneous
- Ø primary pathology
- <45y
- Contralateral lung normal on Xray
- Secondary spontaneous pneumothorax (SSP)
- pre-existing pathology
- pulmonary symptom preceeding PT
- >45y + smoker
- contraleteral lung with Xray abnormalities
- Iatrogenic → THoracocentesis, transbronchial biopsy, CVC, Barotrauma
- Post-traumatic
- Catamenial

- PT during pregnancy
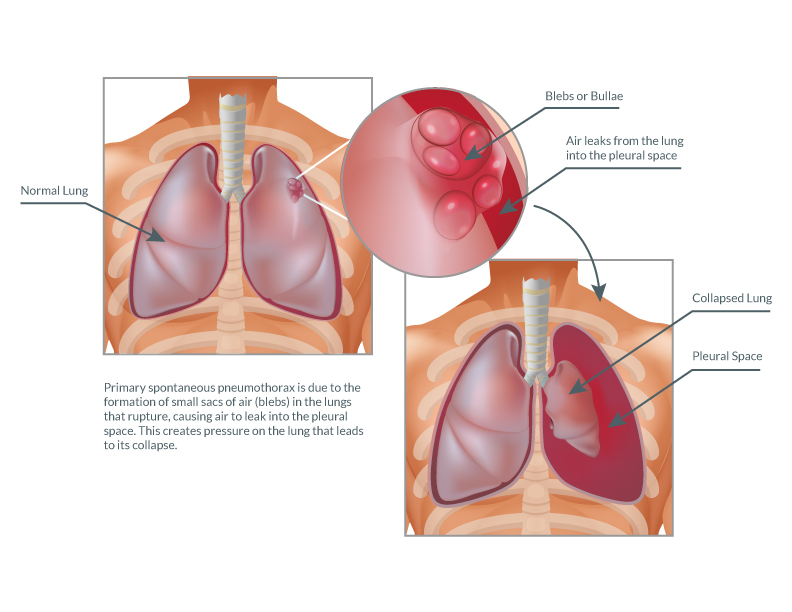
- Pulmonary blebs are small subpleural thin-walled air-containing spaces, not larger than 1 or 2 cm in diameter (with the precise limit varying by source).
- Their walls are less than 1 mm thick.
- If they rupture, they allow air to escape into the pleural space resulting in a spontaneous pneumothorax.
- Blebs are a very common finding in otherwise normal individuals. They are often found in young patients. They are more common in thin patients and in cigarette smokers 1
SSP → ↑mortality, more difficult treatment, longer hospitalization
- COPD/emphysema
- lung cancer
- Pneumonia
- lung fibrosis
⇒ but every lung disease can cause SSP
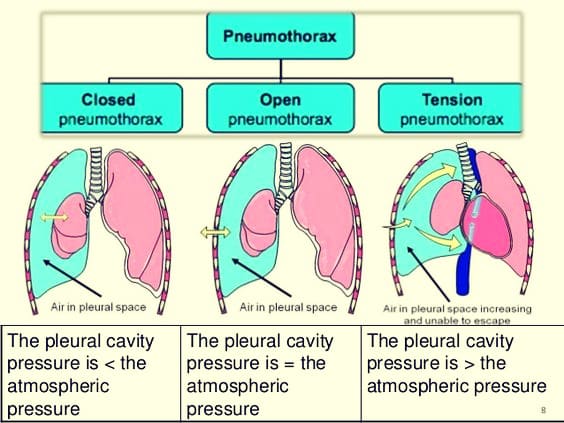
- Closed 📷
- #1
- small lesion visceral pleura
- mostly benign evolution
- Open ("sucking chest wound) 📷
- open penetrating trauma
- severe respir. insuff.
- Tension pneu 📷
- Freq. in SSP, posttraumatic or barotrauma (i.e. scuba diver)
- Severe cardio-circulatory failure (mediastinal shift)
- Tension pneumothorax:
- Disruption of visceral pleura, parietal pleura, or tracheobronchial tree
- One-way valve mechanism, allowing air to enter the pleural space on inspiration but not exit on expiration
- Progressive accumulation of air in the pleural space, leading to increasing positive pressure within the chest
- Collapse of the ipsilateral lung and compression of the contralateral lung, trachea, heart, and superior vena cava
- Angulation of the inferior vena cava
- Impaired respiratory function, reduced venous return to the heart, and decreased cardiac output
- Hypoxia and hemodynamic instability
T
T
- smoking
- age
- sex
- constitutinal size (skinny+ tall)
- Pleuritic pain → sudden onset
- Dyspnea (progressive)
- Cough (non-productive)
- Physical exam:
- Signs of unilateral air accumulation
- ↓/absent breath sounds
- Percussion: Tympanism/Hyper-resonance
- Tracheal deviation
- Subcutaneous emphysema
- Tachycardia+tachypena + hypotension (obstruct. shock), distended neck veins ⇒ tension P.
- Xray #1 → pleural line is moved more medially and lateral part shows Øvascular signs 📷
- US → intens. pleural reflex + recurr. ecchos (A-line); loss of Sea shore sign → bar code sign; 📷
- CT → Underlying cause of SSP, esp in TRAUMA❗, DDx with emphysem bulla or ruptured pulmonary cyst
if tension p → mediastinal/tracheal deviation
Acute:
- reexpansion of the lung
- prevention of recurrence
Observation and Aspiration
- classic treatment fails
- P. recurrence
- persistent P.
- prolonged air leaks (> 5 days)
- tension P.
- bilateral P.
- professions at risk (pilot, diver)
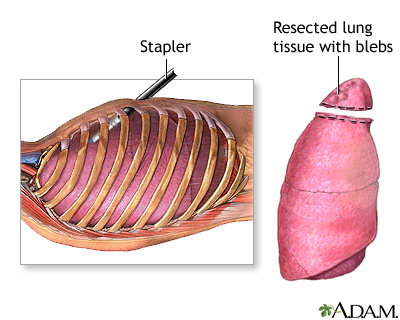
- need for pulmonary biopsy
atypical resection of affected lung and partial parietal pleurectomy (VATS or thoracotomy(open) 📷
severity of symptoms
💥 Thoracic trauma
optimal time frame in which treatment can bring signif. benefit in patients w/ severe trauma
- lesion most lethal should be treated first
- absence of a definitive diagnosis should not delay the initiation of the needed treatment
- detailed anamnesis is not necessary for the initial evaluation of patients
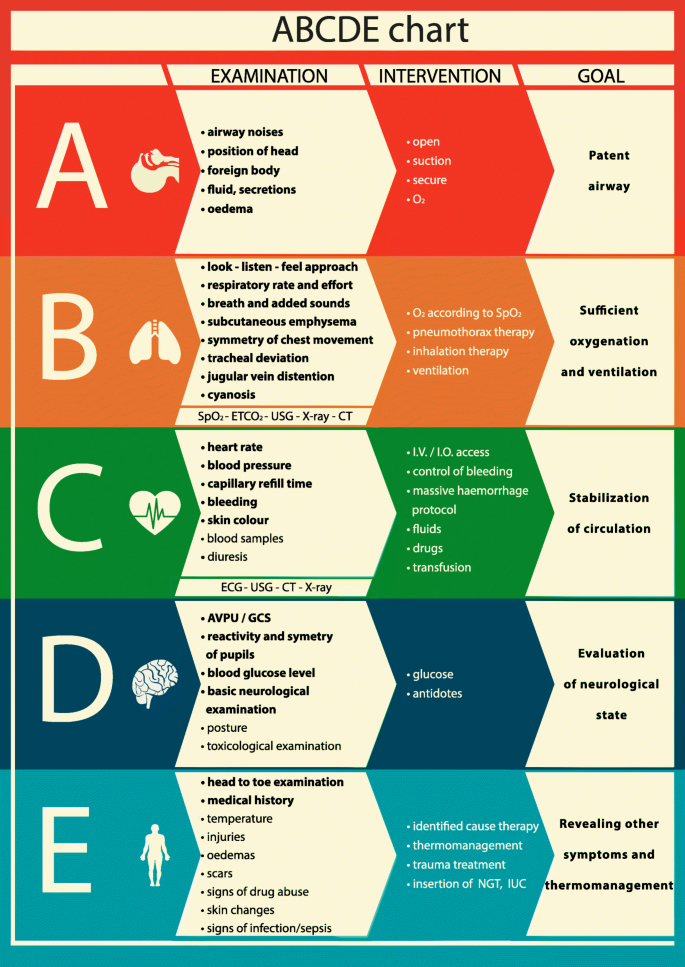
hypoxia
- airway control (tubus)
- thorcocentesis (aspiration)/chest tube
- Airway obstruction
- Tension pneumothorax
- Open pneumothorax
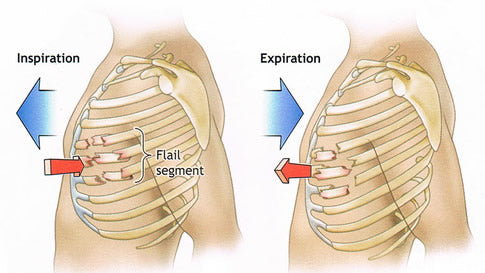
- Flail chest + lung contusion
- Massive hemothorax
- Cardiac tamponade
- Asphyxia:
- Foreign body aspiration
- Larynx trauma
- Sternoclavicular luxation → post dislocation of medial clavicle
- Rupture trachea or main bronchi
- inspection oral cavity + pharynx
- aeric sounds at the level of etiology (nose, trachea, lung)
- clavicular dislocaiton
- Cyanosis
- Dysphonia
- Pneumomediastium + Subcutaneous emphysem
- removal foreign body
- conitomy (cricotyroidotomy) 📷
- clavicle repositon
(ventil mechanism = can only go in but not out)
Rip frature + lung injury → Lung surface
Pentrating wound + Inaapropriate occlusion after open PT → Chest wall
- lung collapse (complete)
- mediastinal shift
- compression contralateral lung
- reduction blood inflow into heart
⇒ cardiogenic shock ("obstructive shock")
- SHOCK: dyspnea, tachycardia, hypotension
- contralateral shift trachea
- ↓/absent breathing sounds + lack of resp. movement
- distended hemithorax (ipsilateral)
- venous distension
- cyanosis (late)
penetrating trauma
Severe respiratory insufficiency
→ "Pendelluft" if wound >2/3x tracheal diameter
= paradoxial breathing pattern: lung → small on insipration; larger on expiration
- #1 (initial Tx): partial close with sterile foil fixed only on 3 sides (functions as a external valve) 📷
- #2 (follow up Tx): chest tube in pleura + occlusive wound dressing

- Definite tx: surgical wound closure
acumulation of blood in pleural cavity
>1500ml or >1/3x blood volume of patient
- pentrating wound with great vessel injury or lung hilum
- closed trauma with internal injuries secondary to fracture (→ aortic rupture)
- Hypovolemia (↓BP, ↑HR, collapse jugular vein)
- Lung collapse (↓/absent breath sound, hypoxia)
- Dullness
- mediastinal shift (→evtl associated tension pneu❓❗)
- Tension pneu
- Endotracheal tube in right main bronchus
→ tympanism (eig. hyperresonance)
→ tracheal/mediastinal shift
→ distension involved hemithorax
- Large chest tube
- if >1500ml blood → emergency thoracotomy
- also in persistent blood loss
- if no ↑in Hb despite transfusion
- penetrating injury
- esp betw. mid axillary line or betw. the two scapulae (heart, great vessel or lung hilum injury)
- acute: fixation of flail chest with compressive bandage 📷
- definite:
- internal pneumatic stabilization with mechanical ventilation
- osteosynthesis (surgical repair)
PARADOXIAL MOVEMENTS 📷 → “Pendelluft”, inefficient ventilation, mediastinal movement
lung contusion
paradocial chest wall movement
(can be less evident due to pain → superfic. breathing + antalgic position)
pentrating trauma
BECKS TRIAD:
- jugular distension
- hypotension
- muffled heart sound
other:
- Kussmaul sign: ↑jugular pulse during insipration
- ↑CVP
- ECG abnormalities
tension pneu
Echocardiography
→ (e)FAST 📷
- pericardicentesis = percut. pericardial drainge
- cardiac surgery
🧫 Pleural empyema
pus in the pleural cavity
(also known as purulent pleural effusion or pyothorax)
- Primary purulent pleural effusion: hematogenous spread
- Secondary = parapneumonic pleural empyema
- Infection neigboring organ → pneumonia + lung abcess
- subphrenic abscess
- posttraumatic (open trauma)
- iatrogenic: thoacocentesis
community aquired: s.pneumoniae, Staph, G-, anerobic
nosocomial: MRSA, Pseudomonos, Fungi etc.
- Age < 60 years
- Predisposition for aspiration: stroke, alcoholism, neurologic diseases
- Predisposition for infections:
- Poor oral hygiene, Drug abuse, Immunodeficiencies (HIV, Diabetes, malignancies)
- Chronic disease
- Cardiovascular diseases
- Liver cirrhosis
classic inflammation
- Exudative stage
- Fibrino-purulent stage
- Organized stage
- general clinical signs are predominant
- pleural fluid is an exudate
- sterile
- LDH <1000 UI/L
- ph + gluc = normal
- local signs become evident
- pleural fluid is turbid/ purulent
- increased proteins and LDH >1000 UI/L
- ↓ph + ↓gluc
- general signs diminish
- pus
- pleural thickness reaches 2-3cm
- collapsed and fixed lung
- narrowed intercostal spaces
- fever
- dypnea
- cough chest pain
- ↓chest wall movement of affected side + ↓breath sounds
- narrowing ICS
- dullness (percussion)
- Other effusions:
- Hemothorax
- Chlyothorax
- Malignant pleural effusion
- Transudative pleural effusion
- Giant lung abcess
- TBC
- Pleural mesothelioma
Thoracocentesis
→ Turbis effusion or pus
→ bacterial evidence
LDH >1000 U/l
Leukos > 500/mm3
↓ph+gluc
- children: repeated thoracocentesis
- Chest tube
- lavage
- fibrinolysis
- Stage 1: Thorcoscopic debridement
- Stage 2: VATS pleural decortication 📷

- Stage 3: Open surgery + pleural decortication
🌊 Malignant pleural effusion
Pleural effusion with malignant cells in pleural liquid or pleural tissue
F - it present in 50% of metastatic malignancies
🫁 Lung cancer, 🍈 Brest cancer, Other malignant tumors, Lymphoma
→ other exudative effusion
→ other effusion due to malginancies (=paramalignant effusion)
- Atelectasis due to lung cancer
- Pulmonary infarction
- Chylothroax (Lymphoma)
- Transudative effusion (hypoproteinemia assoc. with cancer)

- Oberservation → in asymptomatic with know etiology for a short time (recurrence/progression is the rule)
- Thoracocentesis (us-guided)→ symptom relief + cytologic exam → but high recurrance rate in 4w → in SCLC, lymphoma + breast cancer (sensitive to chemo) & patient with reduced life expect.
- Pleurodesis with talc
a. insufflation(thoracoscopic) OR
b. slurry(tube) → reduction of recurrance,
throacoscopic: confirms dg+drainage → indicated: life exp >1month

- Indwelling pleural catheter → catheter with multiple orfices at intrapleural end → spontaneous pleurodesis
→ indicated: trapped lung, altered general condition, reduced life exp.


"air or germs introduction"
- pneumothorax
- empyema
<1.5l at one sitting
OR until symptoms (dypnsea, cough, chest pain)
- infection
- catheter obstruction/displacement/deterioration
- tumor growth along catheter canal
🦀 Lung cancer
- NSCLC: Non-small cell lung cancer
- AdenoCa
- SCC
- large cell undifferatiated carcinoma
- SCLC: Small cell lung cancer
25-30% (every 3rd to 4th)
- smoking (85%)
- Asbestos
- Radon
- Diesel
SCC → male
Adeno → female
→ Adeno is more common in total
Squamous carcinoma | Adenocarcinoma | Large cell carcinoma | Small cell carcinoma | |
M (%) | 50.9 | 30.3 | 9.9 | 9.9 |
F (%) | 24.9 | 58.1 | 9.7 | 7.3 |
SCC:
- smoker
- central: lobar/segmental bronchi (2/3 of cases)
- keratinisation
- endoluminal → obstructive symptoms
- slow growth, late mets
- SCC-specific IHC (cytokeratin, p40,p63)

AdenoCa:
- non-smoker
- peripheral
- columnar epithelium/acinar/glandular cells
- AdenoCa-specific IHC (Napsin A, TTF-1)
- smoke assoc.
- centrally or periph
- IHC: 80% Adenoca-IHC, 20% SCC-IHC
- histology: hyperchromic nucleus
- almost exclusively in smokers
- centrally
- IHC: neuroendocrine markers
- early distant + LN mets
- poor prognosis → manly Ø operable
- Histo: monomorphic, small cells, few cytoplasma
- smoker❓
- asbestos exposure❓
- Symptoms❓ (see below)
- B-symptomatic → fever, night sweats, weight loss, fatigue
- hemoptysis (🚩)
- dyspnea
- chest pain
- endoluminal obstruction
- endocrine imbalance aka paraneoplstic syndrome.
- SIADH
- hypercalcemia
- Cushings
- thrombophlebitis migrans
- etc.
Serum: ↑Na ↓Osmolarity Urine: ↑Osmolarity

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- ESR
- CBC
- GGT + ALP
- calcium
- LDH
- Percutaneous biopsy (US/CT guided)
- *EBUS-TBNA → LN puncture
- Mediastinoscopy 📷
- Toracoscopy → Biopsy (primary tumor, LN, pleural)

lymphnodes
large tissue biopsy
- Histologic type: NSCLC (non-small cell lung cancer) vs. SCLC (small cell lung cancer)
- Tumor stage: Assessment using the TNM system
- Functional reserves / life expectancy: Evaluation of the patient's overall health and prognosis
I+II
IIIA
IIIB
IV (↓number of mets)
- IV
- IIIA → bulky+multilevel
- IIIB, IIIC
open thoracotomy
in stage 1 NSCLC (<5cm, >2cm distance to bronchus)→ VATS thoracoscopy (lobectomy)
Lobectomy:
- anatomical resection
- minimally-invasive approach
- without rib spreading
- video system
- NSCLC
- stage I
- diameter <5cm
- >2cm distance to lobar bronchus (CT)
- PET-CT → suspected N+ → EBUS/Madistinoscopy