




Plastic surgery
🥞 Covering methods for tissue defects
- septo-cutaneous arteries (most important)
- musculocutaneos arteries (thin)
- direct cutaneous arteries (seldom)
→ Subepidermal, dermal, subdermal plexus
- Morphilaxy aka Regeneration → replacement with identical tissue (i.e. liver)
- Epimorphosis aka Real Scarring → fibrous tissue
→ but only relative difference, any wound = scar
dermis
- when removed → good looking
- next 4-8weeks → hard +elevated, red + itchy = hyperplasic stage
- after → discolored, flatten, soften, stop itching
sun exposure
- Hyperthrophic = spontaneously reduce in 2-3y
- Cheloid = no tendency to reduction, might even worse → Presotherapy, Steroid injection into cheloid scar (Øcreams❗), Radiotherapy

- Superficial vs. deep
- simple vs complex
- minimal vs large
- with vs without skin defection
- shape regular vs odd
- clean vs poluted
- mechanism cut, contusion..
- Asepsy + repeated chemical wound cleansing
- Wound excision as rigurous as possible, conserving as much important anatomic elements as possible
- Decompression incision, fasciothomy, fasciethomy, evacuation hematomas, foreign bodies, bone fragments, hemostasis
- repair of injured anatomical elements + defect covering (immediate of active delayed emergency: 24-72h)
- without tension
- treads maintain borders in contact
- not to many treads
- Free full thickness skin grafts

- Full thickness island grafts (Burows grafts)

- Free split skin grafts (ollier-tiersch)
- thin (0.3-0.45mm)
- medium (0.3-0.45mm)

autograft -self
heterograft - others
grafts: only few cutaneous elements + no vascularization (thats why they are planted into vascular bed)
flaps: contain a vascular network (to ensure survival)
full thickness
(functionality is superior + no real donor site (bc. can just be sutured up, also better cosmetic outcome)
free split skin graft (→ donor site cant really be sutured up when that large thats why Øfull thickness)
if possible → full thickness
if too large → split
Granular surface → always with split
→ esp thigh, buttocks
- small grafts → scalpel
- Dermatome 📷


{kind=link}
{kind=link}
{kind=link}
Pedicle vs Island flap
Pedicle Flap → a flap which is left attached to the original site by a narrow base of tissue to provide a blood supply during grafting
Island flap → incised on all borders → no cutaneous attachments between the skin of the flap + adjacent skin of the donor site. The Donor and receiver site share the vascular pedicle of the flap
Free flap → tissue and its blood supply (artery and vein) are surgically removed from one part of the body and transferred to another area of the body (no connection donor + receiver site)
- Local → immediate proximity
- Regional → same region but Ø very close
- Locoregional → donor site at one region, receptor at another anatomical level
{kind=link}
- Direct skin system - random + axial
- Musculocutaneous -perforates
- Fasciocutaneous - perforates
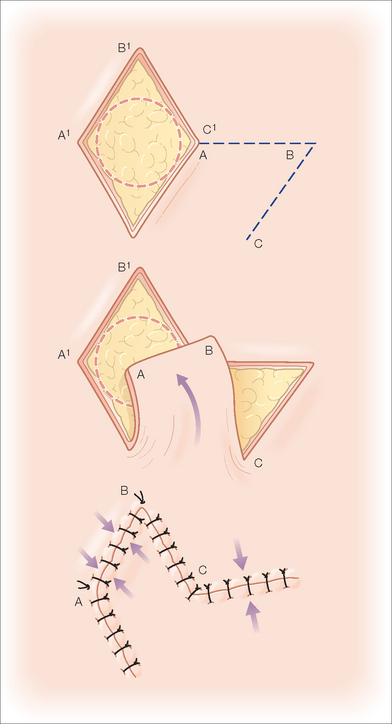
- Rotation transposition 📷
- Elimination of fat tissue
- Bandage
- vascular insufficiency
- necrosis
- infection
- hematoma
- seroma
- Øidentifiable vascular source
- supplied by random vessels
- cant survive unless length/width ratio 2:1
to release tension caused by contractile scars (i.e. finger contraction)
{kind=link}
{kind=link}
direct artereies are running axial to flap → can be extended (in with+lenght) 📷
{kind=link}
- pedicle
- island
- microsurgerical free transfer
{kind=link}
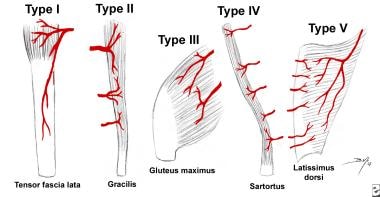
Type 1: one vascular pedicle
Type 2: one dominant and at least one minor pedicle
Type 3: 2 dominant vascular pedicles
Type 4: multiple similar sized pedicles (segmental)
Type 5: one dominant and multiple secondary segmental pedicles→ complete harvesting with significant skin part
{kind=link}
free fasciocutaneous flap from forearm
radial artery can be the only blood supply for the hand!
easy harvest nice caliber, thin, fine, can include bone, tendon, nerves
free flap (small skin island) from back of the foot with central cutaneous vein
venous + included superf. nerve = neurocutaneous flap
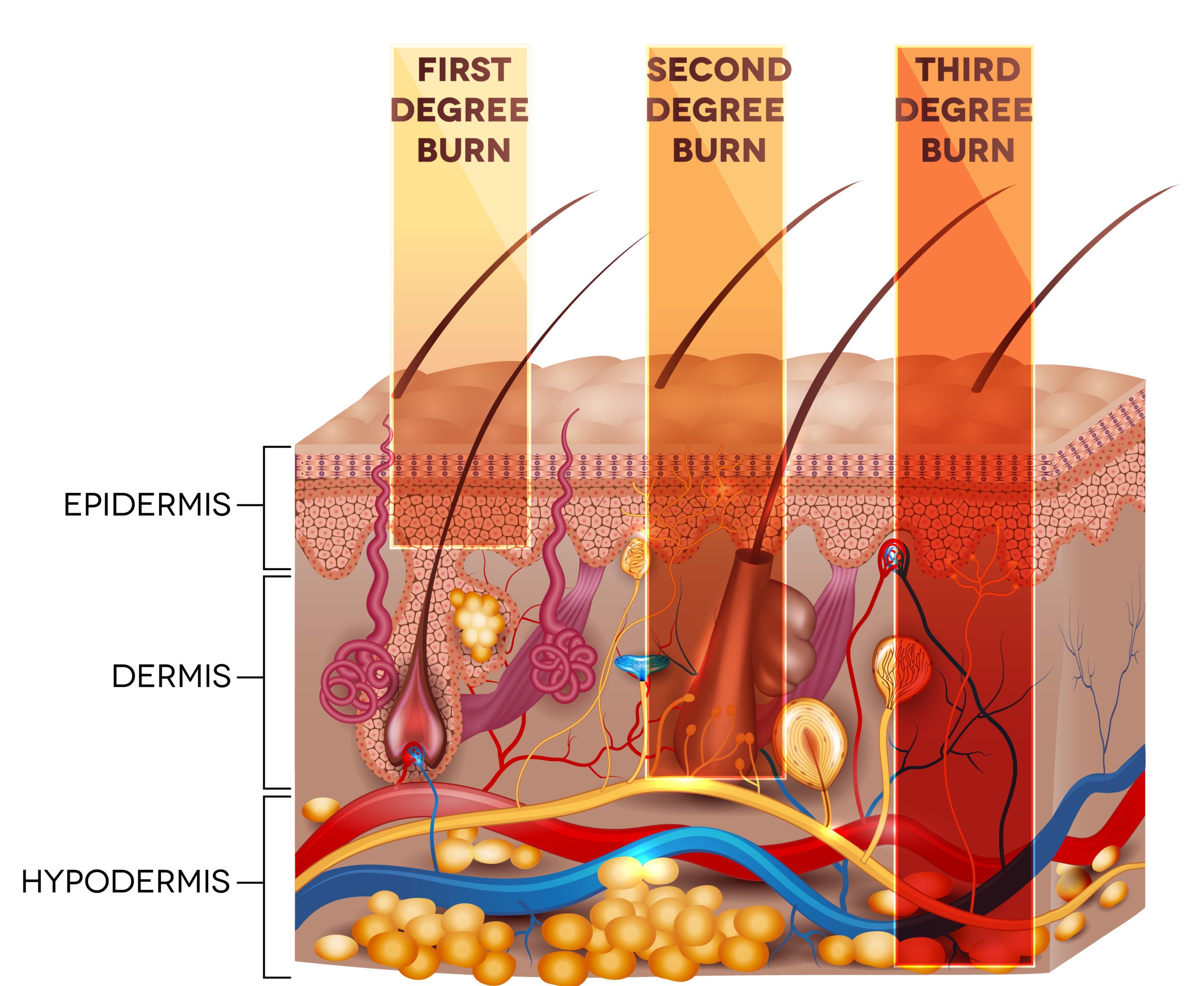
📛 Burns
- heat burns→ liquids, hot solids, flame→ closed space burns
- chemical burns→ corrosive substances
- electrical burns
- ACTH → ↑Mineralcorticoids
- ADH
- beta-endorphins
- catecholamins
- TSH
- cortisone
- glucagon
catabolic hypermetabolism:
- ↑endogenous glucose synthesis
- proteic hypercatabolism
- serotonine
- kinins
- prostaglandins
- necrolides
- leukocyte release
suppression→makesbody prone to endogenous or exogenous infection
- impairment of cilliary function
- decreased chest wall compliance
- increased airway resistance
tubular necrosis due to increased hemo and myoglobin
- decreased output
- decreased central venous pressure
- stasis
- increased permeability for infectious agents
- anemia
- hemolysis
- acidosis
{kind=link}
{kind=link}
{kind=link}
{kind=link}
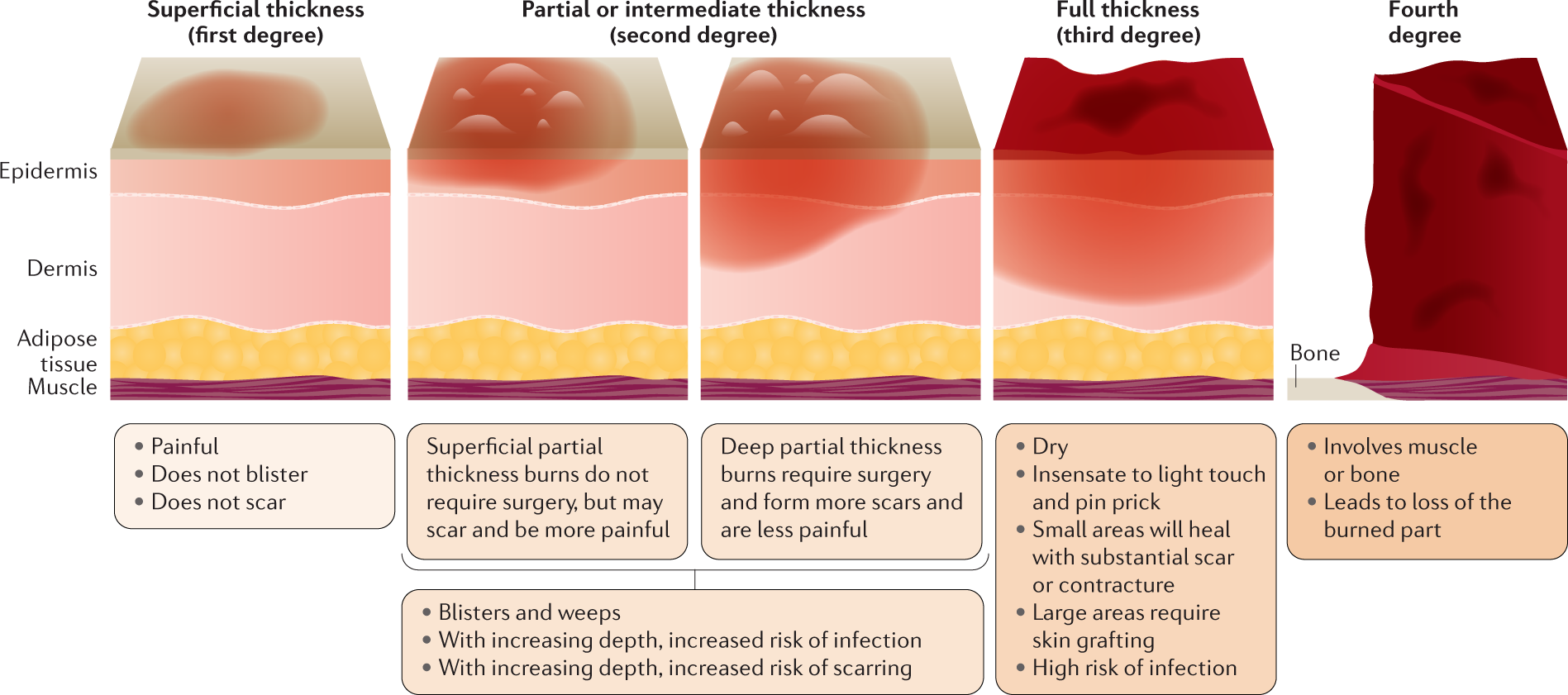
involves outer epidermis layer→ 7 days for healing
involves epidermis to basal layer; clear blister with painful pink dermis→ 14 days for healing
involves entire epidermis and part of dermis; blood in blisters→ 21 days for healing
destruction of entire epidermis and dermis; no residual cells to repopulate→ no spontaneous healing
burn shock
dysmetabolic, high aggression period; second degree should be healed, third degree should be with granulation tissue
surgery→ to cover substance defects
- extinguish fire
- drop cloths, rings etc
- cool out the tissues but avoid hypothermia!
- chemicalburns→ maybe washing out with saline
- tetanus prophylaxis
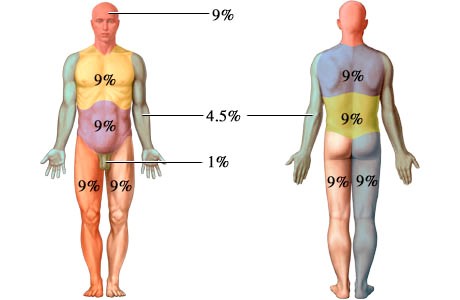
- surface and depth evaluation
- resuscitation, cervical immobilisation
- lesions of airway→inspiration trauma (hoarseness of voice, burn in mouth)
- thorax lesions
- unconscious patient (CO intox?)
- re-evaluation of patient (surface+depth + prognosis index)
- neurologic test Lab, blood gases, radiologic evaluation
- iv fluids
- monitoring
just remember some of them
- III degree
- inhalation
- burn >20% body surface (>10% if <10y or >50y)
- at specific locations
- Electrical + Chemical burn
- comorbidities
- homeless

ringer lactat
1/2 fluids from the first day, colloids can be added
hyperproteic, hypercaloric food, vitamins, oligoelements
ABs, Antacids
- cool out (not hypothermia❗)
- wound cleaning
- topical desinfectants (in III degree)
- special dressings (tegaderm 📷, opsite) (not on face→just topics)
- early excision and grafting → deep + large (>30% Surface Area)
- tangential excision 📷→ use dermatome
- excision to fascia 📷 → only in full thickness burns and wound infections, or failed first skin graft
- seriate excision → well delimitate burns, repeat every week until all the whole region is grafted
Tangential excision: The term refers to the removal of the necrotic surface of a burn by taking repeated parallel slices using a skin graft knife, as opposed to using a scalpel to excise burned skin and subcutaneous tissue together.
- regarding healing-process:
- late healing
- hypertrophic, retractable scar
- itching
- multiorgan failure
- ulcerations + Marjolin ulcer
- Aggressive ulcerating squamous cell carcinoma that occurs in previously traumatized, chronically inflamed, or scarred skin.
- Commonly associated with chronic wounds: including burn injuries, varicose veins, venous ulcers, ulcers from osteomyelitis, and post-radiotherapy scars.
Marjolin's ulcer:
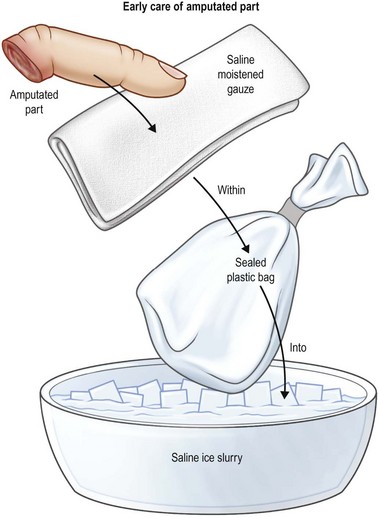
🌱 Re-plantation
functional rehabilitation
re-attachment of a completely severed limb
<1/8 circumference
reattachment of a partially amputated limb segment
>1/8
complete amputation→ two teams needed
incomplete amputation with partially preserved venous-lymphatic drainage→ saves time
amputation by clean cut
- avulsion
- crush
- torsion
24 hours at 4°C
- thumb
- multiple fingers
- hand
- wrist
- forearm
distal to TFS insertion (flexor digitorum superficialis)


- proximal 1/2 of arm
- multiple amputations levels
Polytrauma
= all relative indications
- multiple amputation levels
- proximal 1/2 of arm
- single fingers proximal to tfs insertion
- avulsion
None 👏🏿
difficulty to assess muscle-tendon insertion
→ diseases with negative vascular implications
- diabetes
- renal failure
- peripheral vascular disease
- connective tissue disease
retraction, inefficient, difficult to obtain drainage and vascularisation
- revascularisation
- cover the defect
- include vascularised elements (tendons, nerves, bones)
- increased comfort
warm ischemia >32° C.
cold ischemia <5-10° C.
→ optimal preservation conditions: 5-10°C

{kind=link}
two teams→ one for amputated segment, one for the stump
- abundant washing
- fasciotomy + excision
- identification and isolation of important anatomical elements
- osteosynthesis
- extensor and flexor tendon suture
- artery suture
- venorrhaphy
- skin suture
also neurorrhaphy
- Osteosynthesis
- Artery suture
- Extensor tendons suture
- Flexor tendons suture
- A second artery suture
- Venorrhaphy (sodium bicarbonate washing)
- Skin
- ↑vascular suture tension
- vascular suture in injured vessel wall
- sutured vessel compression
- bandage
- immobilisation- plaster cast
- position- postural drainage
- vasodilators
- anti-coagulants
→ Heparin dependent on patient and trauma
- venous congestion
- ischemia
- infection
- hematoma
- seroma
- partial necrosis
→ pseudoarthrosis, stiff joints
- Osteitis +vicious bone consolidation
- cold intolerance
- early start
- long standing
- complete
another finger for the thumb or toe to finger transfer