




Onco Surgery
🍈 Breast Cancer
false - Lymph
superficial + profound plexus
BRCA 1, 2
↑RISK FOR BC
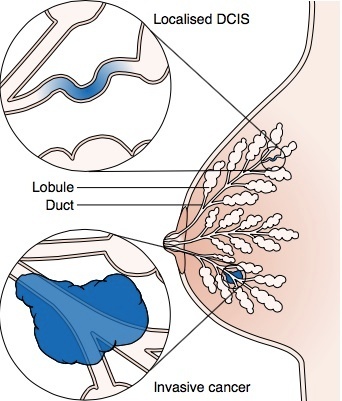
“Sclerosing adenosis (SA) is a benign proliferative condition of the terminal duct lobular units characterized by an increased number of acini and their glands. It manifests as multiple small, firm, tender nodules, fibrous tissue, and variable microcysts within the breast.”
- atypical ductal, lobular hyperplasia 📷
- in situ lobular carcinoma
- ALCOHOL
- OBESITY + HIGH FAT DIET
- CONTRACEPTIVES
- HORMON REPLACEMENT

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- surgical (after 2 uncertain punctures)
- excisional (small lesions that cant be punctured)
other reasons: technical reasons, microcalcification without mass on US, No opage center just distorsion, refusal
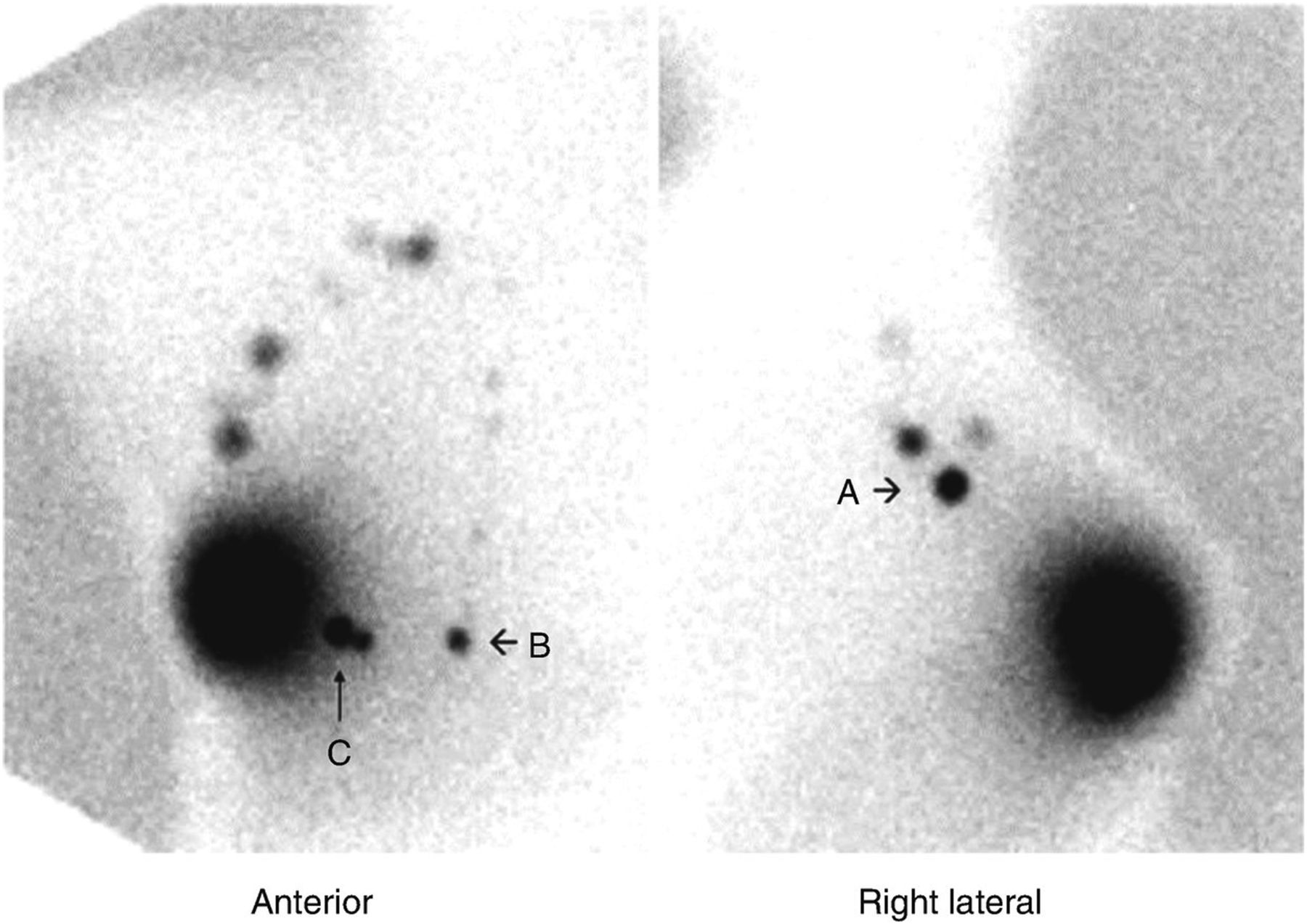
sentinel lymph node 📷
{kind=link}
{kind=link}
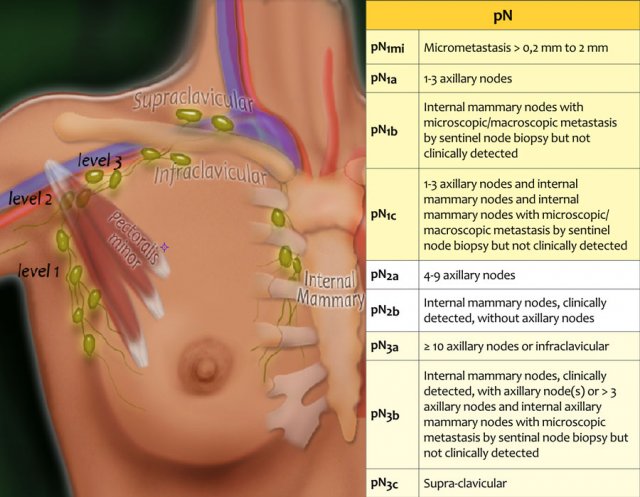
axillary, internal mammary, infraclavicular, supraclavicular 📷
{kind=link}
lung, liver, brain, bones 📷
:max_bytes(150000):strip_icc()/stage-4-breast-cancer-429891-01-4aaaca2549c1417fa0f6af12f99fc8f6.png){kind=link}
Check everything for mets
- Chest X-Ray
- abdomino-pelvic US,
- Bone radiographs+/- scintigraphy, (if bone pain)
- CT scan of skull (if neurological symptoms)
- any other suggested by specific symptoms
CA 15-3
- Liver function
- ALP
- Renal function
Lymphoscintigraphy 📷
{kind=link}
conversion to operability, inflammatory carcinoma, breast preservation, sensitivity testing of primary tumor chemotherapy

Trastuzumab→ in HER2 positive cancer
TOGETHER WITH CHEMO

- hormonal therapy
- chemo
{kind=link}
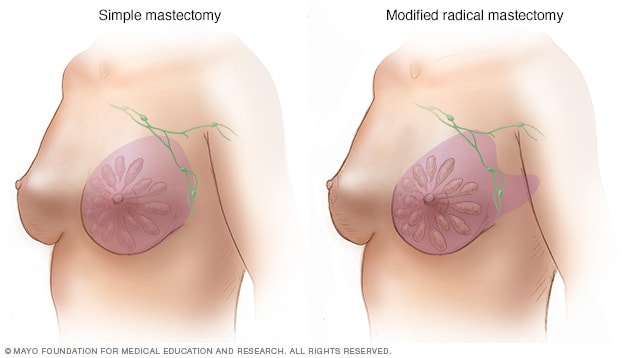
lumpectomy, wide excision, quadrantectomy (all breast-conserving) and mastectomy
with oncolocic margins
{kind=link}
{kind=link}
dye 📷
{kind=link}
adjuvant therapy
RADIOTHERAPY MANDATORY IN CONSERVATIVE TREATMENT
homonal, chemo, trastuzumab
periodic controls at 3 months in the first 2 years
→at 6 months in the next 3-5 years,
→then annual controls;
- anamnesis and objective examination;
- ippsilateral mammography and contralateral at 1 year;
- in the case of symptomatic or pathological changes at the objective examination→ targeted additional examinations
- Breast MRI may be indicated in young patients with dense breasts and genetic / familial predisposition - discussion in CDT;
- for patients undergoing hormone therapy with Tamoxifen, an annual gynecological consultation is recommended
- for patients undergoing hormone therapy with aromatase inhibitors, periodic evaluation of bone density is recommended;
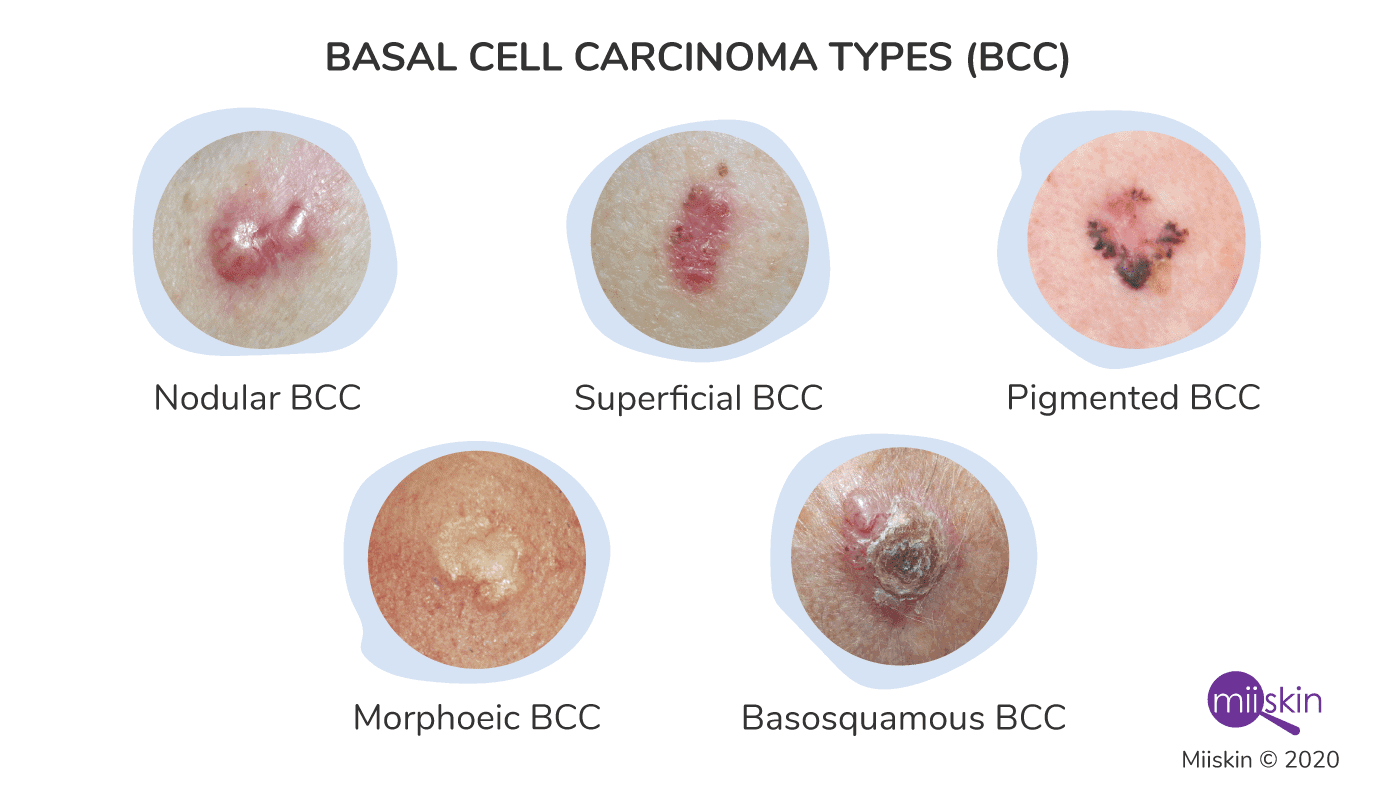
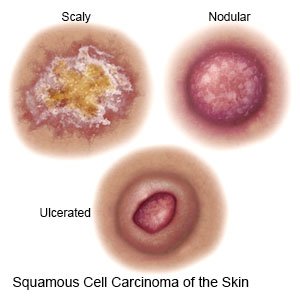
☀️ Skin Cancer
{kind=link}
{kind=link}
{kind=link}
Anamnesis, Clinic, Biopsy
FNA
complete resection with maximal preservation of function and cosmesis; patient preference must be taken into consideration
surgical, RT, CT
- excision
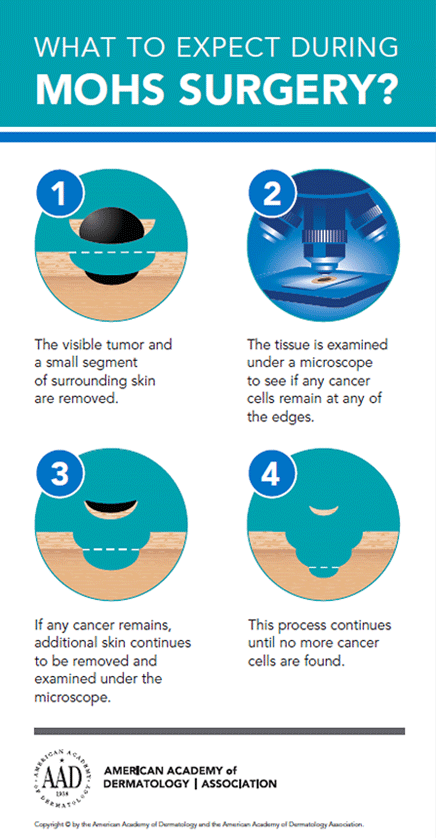
- Mohs surgery
- Curretage + cautery
- Topical treatment: Cryotherapy, laser

{kind=link}
Surgical, RT +/- CT
lymphatic spread→ Adenopathy→ FNA/biopsy→ Lymphadenectomy +/- RT
CT
{kind=link}
red, fleshy noddules, aggressive (Lymph and distant mets)
- sun exposure (like the others) + immunosuppression
PET-CT
(also MRI + CT might be useful)
- wide excision, 1-2cm margins
- mohs surgery,
- biopsy→ staging and ggf. lymphadenectomy
- adjuvant radiotherapy
- +/- chemo(if stage IV)
fibroblasts (sarcoma)→malignant
{kind=link}
F -
LN mets = 1%
Distant Mets = 4-5%
Clinic→ biopsy/surgery→ Dx
large excision, Mohs technique, Radiotherapy (adjuvant)
highest risk
- Congenital Nevi
- Dysplastic Nevus syndrome
sun and UV exposure
- race (white,black)
- familial predisposition
- personal history
- predisposing diseases (Xeroderma pigmentosa)
A = Asymmetry
B = Border (irregular border with indistinct margins)
C = Color variation (new changes in pigmentation or variations in pigmentation within the same lesion)
D = Diameter > 6 mm
E = Evolving/enlargement (new lesion or a lesion that changes in size, shape, or color over time)
F = Family history

- non-healing injury
- new melanic lesion
- redness, itching, pain
- bleeding or fluid leakage from nevus
:max_bytes(150000):strip_icc()/what-is-melanoma-514215_final-01-3b091d9a68074ba7b5a1cb6d8287cf92.png){kind=link}
excisional (1-3mm margins) → parallel to lymphatics
or incisional (for facial or large congintal nevi)
- cTNM (clinic+imaging+histo)
→ histo lymphatic and metastases check→
2. pTNM
wide excision (Mohns only in minimal invasive as alternative)
dependent on the Breslow score: 1-2 cm
Breslow Thickness | Margin |
<1mm | 1 cm |
1-2mm | 1-2 cm |
>2mm | 2 cm |
0.5cm
Mohns surgery, RT, imiquimod (immune response modifier)
older
<8mm
slective lymphadenectomy
sentinel node aka sentinel ganglion
pT2-T4: tumor thickness >1mm and/or ulcer
pT1b (if >0.75mmm)
pT1a with RF → varicouse vein,MI, ulceration
Imaging with US for baseline staing
Primary Tx: ultrasound surveillance or complete lymph node resection plus adjuvant therapy
Surgery
intralesion injection (i.e. IFalpha, IL-2)
systemic treatment (chemo)
- limited lesion → surgical resection
- Disseminated → systemic treatment (chemo)
💪🏽 Soft Tissue Tumors
under mask of benign tumors (wo/ pain)
aggressive→ metastases, relapses
- hereditary retinoblastoma
- Li-Fraumeni Sdr.
- Neurofibromatosis
- Gardner sdr., FAP
- ionizing radiation
- chronic lymphedema
- injuries
- chemicals
- mass in any region of body
- asymptomatic
biopsy→ sarcoma, type, grade
- Core needle biopsy,
- excisional biopsy → for T<3cm+clinically benign
- incisional biopsy
Imaging (CT, US, MRI,angiog.)→ invasion of neighbouring tissues→ OPERABILITY
T1→ <5cm
T2→ 5-10 cm
T3→ 10-15 cm
T4→ >15cm
Surgery
radiotherapy = complementary role for local disease control
chemotherapy = control of distant mets / neoadjuvant role in multimodal treatment
- complete eradication R0
- minimizing recurrence risk
- ensuring best functionality
- improving overall survival
- improving quality of life
→ What R resection (R0,R1,R2) is achieved which each technique?

R2
R1
R0
R0
{kind=link}
LSS = Limb sparing Surgery
in contrasto to Amputation
rarely used nowadays
- tumors that cannot be resected otherwise (large, low degree, symptomatic)
- no metastases
- with possibility of long-term rehabilitation
internal, ant + post compartment of thigh



complete tumor excision with at least 2cm safety margins
bones, vessels, nerves in the way
wide excision and Radiotherapy
ERT (external)

Brachytherapy (intra-operative)

N1 (but N+ in only 3% of STS)
plastic surgery → Flaps
(more details → see plastic surgery)
thoracic surgery + follow up + repeated resection
- Thoracic surgery is crucial in the treatment of metastatic melanoma in the lung.
- Follow-up and repeated resections have the potential to save 25-30% of patients.
- Surgical persistence is rewarded by achieving favorable outcomes for patients with incurable disease.
🔪 Oncological Surgery
- general health
- comorbidities
- surgery type + technical complexity
- Anesthesia type
- Aspiration biopsy → FNA (cells + tissue fragments)
- Needle biopsy (core of tissue)
- Incisional (segments)
- Excisional (entire tumor)
small wedge resection
excision of the entire suspected tumor with little/Ømargin
contamination of new tissue planes
placement of radiopaque clips → mark spots for delivery of radiation therapy
- conveniently removable needle tracks/scars
- extremity incision longitudinally → easier removal + closure later
- Avoid contamination new tissue
- Perfect hemostasis (tourniquet) during biopsy to avoid hematoma (can lead to tumor spread)
- dont use the same instruments when exploring potentially uncontaminated areas (because otherwise there will not be a "potentially")
→ no spread
- definitive surgical treatment for primary cancers
- surgery to reduce severity of disease
- surgical resection of metastases (with curative intent)
- treatment of oncological emergencies (hemorrhage, perforation, destruction vital organs, etc.)
- palliation surgery (i.e. relief obstruction: gastric/intestinal bypass, intestinal stoma; feeding tubes)
- surgery for reconstruction and rehabilitation
- Polyposis coli
- Familial colon cancer
- Ulcerative colitis
- Multiple endocrine neoplasia types 2 and 3
- Familial breast cancer
- Familial ovarian cancer
single site
consequence of laparoscopic oncological procedures with uncertain reason
recurrence of tumor at the small wounds created for the transabdominal placement of ports used to pass instruments or retrieve specimens
→ use a specimen bag
Despite some controversies in the literature, it appears that aerosolization caused by pneumoperitoneum, tumor manipulation, and tumor burden are important factors for the development of port site metastases To eliminate the effects of pneumoperitoneum, gasless laparoscopy has been recommended, but port site metastases have been reported even under these conditions
provides:
biopsy, + lavage-cytology❗
staging
and treatment
in ONE single procedure
- retroperitoneal adenopathy
- peritoneal carcinomatosis
- mesenteric tumor
- early gastric cancer (T1-2,N0,M0)
- palliative → i.e. gastric bypass
advanced = open surgery
equally
laparoscopy
open
(distal pancreas + selected neuroendocrine tumors might be resected with laparoscopy)
detection + treat of small mets (otherwise missed by imaging)
→ RF ablation
even major hepatectomy can be performed with laparoscopy (if experienced)
open
↑incidence of port-site mets
laparoscopic
open prefferd, but laparoscopic is good alternative → also standard approach dor dg of adnexal masses