
Table of content
- CMF Surgery
- 🔎 Clinical examination
- 💥 Trauma: Oral and maxillofacial
- 🧫 Infection: Oral and maxillofacial
- 🦷 Odontogenic maxillary sinusitis
- 💦 Salivary gland pathology
- 👻 Benign Tumors: Oro-maxillo-facial and cervical
- 🦀 Malignant Tumors of the oro-maxillo-facial
- 👶🏽 Congenital malformation and anomalies
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6

CMF Surgery
🔎 Clinical examination
lab + imaging
- Volume and contour modifications: Changes in the size and shape of a region.
- Color modifications: Alterations in normal pigmentation, either hyperpigmentation or depigmentation.
- Consistency modifications: Changes in the texture or firmness of tissues.
- Pathological mobility: Abnormal movement of teeth, mandible, tongue, etc.
- Functional alterations: Abnormalities in salivation, such as asyalia, hiposyalia, and hypersyalia.
- Temperature modifications: Inflammation or ischemia leading to changes in temperature.
- Pain: Spontaneous or stimulated discomfort.
EXTRA- & INTRA-oral exam
frontal + profile 📷
- symmetry + color
- catural creases
- labial + palpebral fissure
- radio (upper,middle, lower)
- obvious deformation
- inflammation, fistula, ulcer
- trauma: abrasion, hematoma, wounds
- neuromuscular diseases ⇒ #1 facial nerve impairment
- psychiatric
- structural changes → Soft tissue (ST) & skin deformity
jaw bones, nasal pyramid, orbit, maxillary sinus, mandible
- retroauricular
- preauricular
- parotid
- buccal
- submandibular
- submental
- cervical
- superfic., ANT to SCM
- superfic., POST to SCM
- deep, jugular LN
- supraclavicular
benign → soft, pain + movable
malignant → firm, Øpain, fixed
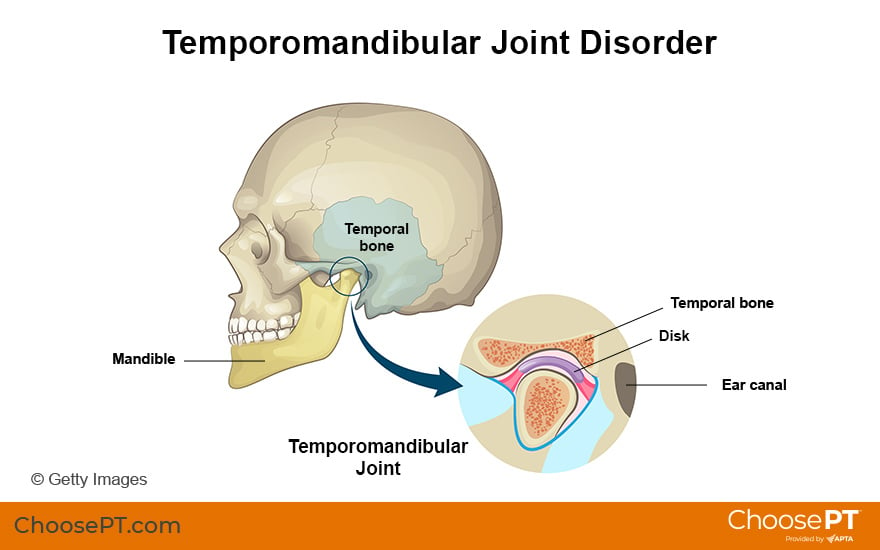
- Amplitude (Trismus, constriction, TMJ ankylosis)
- Lateral deviations
- Obstacles ("Steps") mandibula
Trismus → inflammatory reflex contraction of jar
constriction → scarring (Øinflammatory)
TMJ ankylosis → in children; leads to mandible hypoplasia
💥 Trauma: Oral and maxillofacial
- Bruise (subcut or submucosa hemorrhage → but Øbreak in ST)
- Hematoma (blood accumulation from hemorrhage of deeper or bigger vessel)
- Seroma (lymph accumulation; often post-surgical complication)

- Muscle Trauma → Muscle weakness or Muscle crushing
- mainly resorbed
- fibrosis → encapsulation
- infection → abcess
- cool packs
- compressive dressing (if too big)
- hematoma puncture/incision
- AB prophylaxis
- Pain killers
superficial lesion, only involving dermis+epidermis
"STOP the FALT ACTIoN"
- Size
- Tissue integrity (tissue loss, no tissue loss)
- Other lesions (isolated/combined/associated)
- Penetrating natural cavity (penetration, non-penetrating)
- Flaps (with pedicle or without)
- Wound age (freh, old)
- Location (extra-oral, intra-oral)
- Topographic region (one, multiple)
- Traumatizing agent → cut, laceration, contusion, bitten, shoot, etc.
- Complexity (light, serious→immediate life threatening)
- Wound thickness (superficial, deep→function impairment)
- Infections (yes, no)
- Number (single multiple)
MANDATORY:
- Pain → dissapears after 10-12h → re-appears if infected
- Bleeding
- Loss of continuity
OPTIONAL:
- anesthesia + paralysis
- salivary fistula (external)
- Hypersalivation
- Orostoma (inside oral cavity →outside)
GENERAL:
- airway obstruction
- secondary complication
- shock
- infection → abscess, erysipel
- late: scars → jaw constriction, loss of tissue
- ABC → serious complication (i.e. shock)
- Treatment of serious injuries → cerebral, abdominal, thoracic
- CMF Wound treatment → cleaning, debridement, dressing
- Analgesics, AB, Tetanus vaccine
- Reduction+ immobilisation of fractures
- Suture (directly (primary sututre), delayed (3-4d), secondary (older then 20d), plastic repair (after 6m))
Dental abnormalities
- malposition
- fragile
- hyper/hypo calcificiation
- decays
- periodontal disease
direct
indirect (by antagonists teeth)
mastication (foreign body)
extraction
- subluxation - slightly mobile → observation
- luxation with intrusion → extraction / observation
- luxation with extrusion → extraction
- avulsion → leave it (Øreplantation)
- fissures of enamel or dentin without loss of substance → Ø treatment
- pentrating into pulp📷 (complicated) → dental treatment
- Horizontal: cervical, median or apical 📷
- cervical + median → extraction
- apical → apicocectomy 📷
- Vertical 📷→ extraction
Apicocectomy is typically done under local anesthesia, and an incision is made in the gum to access the root. The damaged portion of the root is then carefully removed, and the area is thoroughly cleaned and sealed to prevent further infection. Finally, the gum is stitched back into place to promote healing. The goal of an apicoectomy is to save the tooth and alleviate any pain or discomfort caused by the root fracture.
periodontal lesion (peridontal disease stage 3 or 4 📷) → no mobility + pain at percussion → Øtreatment
analgesics
AB
Oral hygiene
HIV-Tetanus prophylaxis
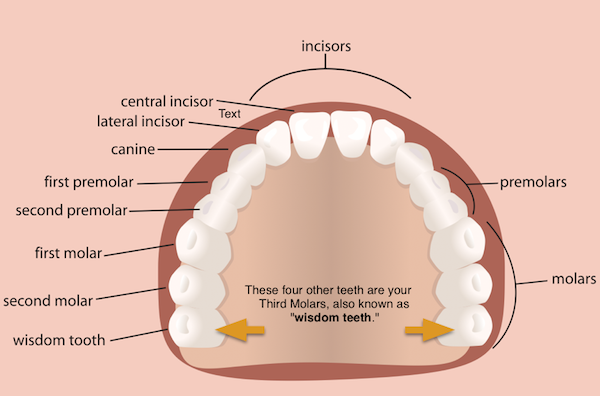
- Median (btw. central incisors)
- Paramedian (betw. incisor + cainine)
- Lateral (canine - third molar)
- Angle (after thrid molar)
- Ramus
- Condylar apophysis
- Coronoid apophysis
- non-specific fracture signs
- edema
- bruising/hematoma
- abrasion + wound
- deformations + discontinuity
- abnormal movement
- anesthesia
- crepitus
- trismus (occlusion on bite exam)
- ↓movement transmission to TMJ
- Le Bourg maneuvers
- intraoral damage: interdental spacing, mucosa bruise, hematoma, mobile teeth
- saliva w/ blood
- Median → Harmonia movement betw. incisors → minimal secondary dysplacement (due to symetrical muscle force)
- Paramedian → Fracture line, displacement: prox. segment goes down, distal sigments goes up
- Lateral → displacement (distal↑, prox↓), hemorrhage (artery involvement), hematoma of the floor → pushing tongue back → dysphagia, cant close mouth properly (occlusion modification)
- Angle → If in front of muscl insertion (displacement as above ⇒ occlusion modified), if in the area of muscle insertion →Ødisplacement
- Ramus → swollen parotid, pain, trismus (cant open mouth), frontal disocclusion → prox segment goes up, distal goes medially (two step occlusion), ↓sensitivity (inf damage alveolar nerve (D’alger)
- Condylar → TMJ pain, preauricular pain, ear bleeding, ear pain
- Coronoid → concom. zygomatic fracture, cant open mouth (Trismus), no occlusion
all muscles pull back → tongue pulled back as well into pharynx → asphyxia
Transmission of force: condylar
CT
callus in 4weeks
immediate: shock, hemorrhage, nerve damage
secondary (later): ST infection, bone-infection (osteomyelitis, osteitis), sepsis
Late: delayed consolidation, ankylosis of TMJ📷, constriction of the mandible , pseuoarthrosis
reduction + fixation
“ATP”
- Alveolar fracture → loose teeth, bleeding gums + lip echimosis, moving alveolar process
- Tuberosity fracture (after dentral extraction) 📷
- Hard palate fracture
Le Fort 1:
- brusing lips, jugal vestibule, paltine
- transverse mobility
- pain when pressing on vestibule 📷
Le fort 2:
- big edema
- bilateral echymosis
- epistaxis
- maxillary mobility (when palpate next to nose)
- infraorbital nerve anesthesia

Le fort 3:
- higher edema
- orbital: edema, conjunctival echymosis, infraorbital hematoma, ex-/en.opthalmus, diploplia
- maxillary mobility
- front-open bite (dislocation whole midface)

- Intermaxillary dysjunction (mid-saggital fracture) 📷
- Paramedian fracture
- Mixed Fractures
- Complex fractures (comminuted)
crackle master
- cheek hypoastesia
- bone crackles
- gaseous crackles
- lower eyelid bruising
- hematoma
- bone deformity
- clinic
- complementary exams (visual field etc)
- CT ❗
- MRI for CNS, nerves + eyeball
- Immediate → shock, hemorrhage etc.
- secondary → infections
- Late → vicious bone consolidation, maxiallary retrognathism, speech+chewing abnormalities, fistulas
- ABC - emergency treatment (shock, bleeding, asphyxia)
- AB
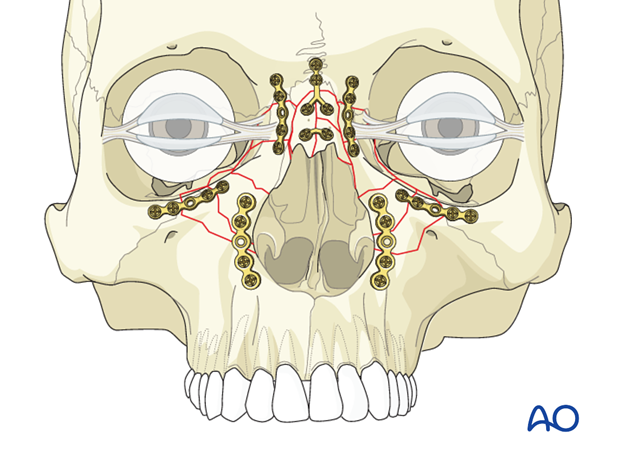
- Reduction + Fixation (emergency or definitive orthopedic or surgical) ⇒ in general micro-screws + -plates
- Treatment of sequella: diplopia + facial asymetry
→ in general: personalized implant + plastic surgery
🧫 Infection: Oral and maxillofacial
- Dental + peridontal lesions
- Dental treatment complication (i.e. teeth extraction)
- osteomyelitis
- infecticted salivary gland lithiasis
- jaw tumors
- Pharyngeal + tonsillar infections
- foreign bodies
- anesthesia complication
- Acute cellulitis
- Abcess
- Diffuse suppuration = Phlegmon = ludwigs angina
- Acute cellulitis: reversible, slight celsius signs (swelling, congestion, erythema), slight alteration general condition
- Abcess: pus, painful swelling, general condition alteration (tachycardia + fever, malaise)
- Phlegmon/ludwigs angina: hard + diffuse swelling, streched skin+ membranes, cyanosis, septic general condition
Ø pain
Ø general condition alteration
- Determination severity (of infection)
- Immunocompromised❓ (hospitalization vs. ambulatory)
- CT❗(esp. if deep)
- Surgical treatment
- Medical treatment → AB
- Follow-up
T
- buccal swelling near affected tooth
- masicatory dysfuntion (↓function)
- General inflammatory signs:
- fever
- pain (spontaneous or on palpation)
- swelling + edema of ST
- Complications: spread of infection → i.e. orbital abcess
- maxillary cyst
- maxillary tumor
- furuncle
- Incision + drainge
- Medical treatment (esp. AB)
- Treatment of the tooth the causes the abcess
- lower molars
- infected salivary gland lithiasis
- acute submandibular adenitis
- extension from neigboring spaces
- Tooth pain lower molar (if tooth related) → cant palpate lower edge of mandible
- intense pulsating pain (spont+palpation) → irradiate in ear
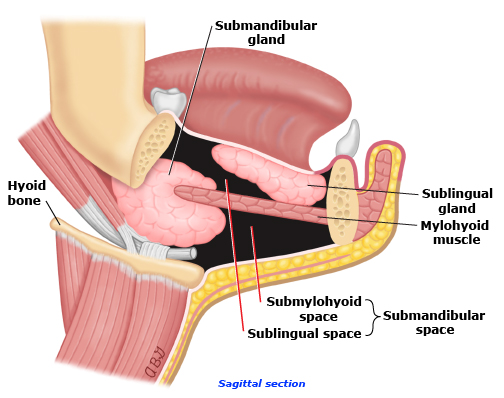
- Swelling post. 1/3rd of mandible 📷 📷
- celsian signs (congestion, erythema, swelling)
- Trismus (impaired opening of mouth)
- Inflamed floor of the mouth (ipsilateral) → painful palpation
- Functional impairment: of mastication, swallowing + phonation, hypersalvation
- ↓general state: Malaise fever + musclar pain
- Lymphadenitis (can also be cause)+ specific lymphadenitis (i.e. TBC, Syphilis)
- Submandibular sialadenitis (Ø trismus)

- mandible tumors
- Perimandibular, Sublingual, submental abcess
- Floor of the mouth Ludwigs angina
- actinomycosis


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- inflammation from (upper) wisdom teeth or after wisdom teeth removal
- anesthetic punctures (septic puncture)

- sperad from neighboring spaces (i.e acute sinusitis)
- Onset:
- acute hemicranial pain
- trismus
- fever, malaise
- After the previous signs:
💉 PUNCTION → leave the needle there (marks collection)
also allows the drainage of pus → send to lab → Antibiogram
{kind=link}
{kind=link}
{kind=link}
carotid a. (int+ ext), vagus n., pharyngeal nerve→ transmission into mediastinum + base of the skull
Spread from:
- Tonsillitis (most freq)
- Dental infection (lower third molar)
- Neighboring spaces
- Tonsillitis: sore throat, odynophagia, swelling
- Dysphagia
- Trismus
- unilateral swelling of pharyngeal lateral wall + soft palate 📷
- stenosis pharyngeal isthmus (opening back of mouth into throat) → asphyxia
- contralateral deviation uvulua + pharygeal wall (towards healthy part)
- painful palpation + stiffness of pharygeal wall
- signif. poor general condition: malaisa, ↑↑fever, tachycardia, headache
- Ø really extra-orally signs
- might spread to submandibular space
- Ludwig Angina (bilateral)
- Submandibular abscess (can also be a complications; but if DD no signs of pharyngeal involvement)
- Tumors (benign, malginant) of pharygeal space

Depends on location → CT with contrast or MRI ❗
- Endo-orally: only small mucosa incision + then blunt dissection into collection (be really really careful: feel for palpation (inner carotid artery❗) [only possible if in ant. part]
- Exo-orally #preferred
- Submandibular incision
- Retro SCM incision
- Pre SCM incision
- Drainage tubes
- Lavage with antiseptics
- AB (first broad-spec; later accord. antibiogram)
- NSAID, rehydration, perenteral feeding
⇒ depending where is most oft the collection present
- Dental infections
- 3rd molar infections
- Impaired immunity
{kind=link}
{kind=link}
- swelling sublingual (like roosters crest📷) space → spreads through buccal floor into: sublingual contralateral + submandibular 📷
- Øsigns of acute inflammation
- hard consistency cervical tissue
- no/high fever(usually no fever→bc. ↓immunity; fever when already septic )
- ↓↓general condition (tachycardia, ↓BP, , anemia)
- purple mucosa
- Functional abnormality: swallowing, respiratory, specific phonation(severe sore throat), hypersalivation, halitosis
⇒diffuse swelling → tongue backwards (+cant really close mouth)
⇒ Øappetetite + dysphagia +dyspnea
- sublingual abcess (most often etiology, but also as single abcess unilateral)
- submental + submandibular absces (unilat)
- Infection salilithiasis (check CT, mainly unilateal)
- acute lymphadenitis
- wide bilateral exo-oral incision of submental + submandibular spaces (open all spaces, also lat. pharygeal + sublingual) + drainage 📷
- evtl perform tracheostomy first (Ødo it when lower part is involved)
- Wide debridement
- Lavage with antiseptics
- AB (broad spectrum, later accor. antibiogram)
- NSAID, rehydration, parenteral feeding
- All spaces* (also involves the fascial spaces ) are involved but only on one side → check all spaces to decide which treatment 📷
- also severely altered general condition
- same signs + symptoms
spaces: temporal, orbital, cheek, submandibular, later cervical, retromolar perimandibular, lateral phargygeal
- oral + intratemporal infection (can also be etiology of hemifacial ludwigs angina)
- tumor (orl + infraorbital)
- Incision + drainage (exo- + intra-oral incision)
- Lavage
- AB
- NSAID, rehydration, parenteral feeding
depleted immunity of the patient
- polymorphic bacteria
- trauma
(again only in altered health conditions)
Ludwigs angina
skin tumor
- Debridement of necrotic tissue (necrectomy)
- lavage with antiseptic solutions
- wound bandage
- AB (broad-spec)
- General status correction (Rehydration, proteins parenteral + enteral coloric intake)
- plastic treatment after 6month (if survives)
- dento-peridontal infection
- oral mucosa infection
- tonsil infection
- pyoderma, acne (any kind of infection that is in the drainage of the lymph node)
{kind=link}
{kind=link}
- Submandibular abscess
- ac. submandibular sialolithiasis
- tumor
- Incision + Drainage with tubes (or rubber blades)
- AB
- NSAIDS
- General status correction (rehydration etc.)
T → since invention of AB
mandible + maxilla
Cortical + spongy bone
T
- fractures
- dento-parodonal infection
- surgical procedures
- sudden onset
- rapid spread to sourrunding area
- lower lip anesthia (Vincent D'alger sign)
- osteo-periosteal thickening + pain (will go away when fistula develop)
- dental mobility
- inflamed oral mucosa
- alter general condition + fever + Øappetitie
- Incision + Drainage of ST abscess
- Lavage with antiseptics
- Sequestrectomy (because it will lead to more abscesses)
- Local AB (gentamicin)
- AB (broad spec with bone conc)
- Hyperbaric oxygen 📷
- affected mandibular development(in young)
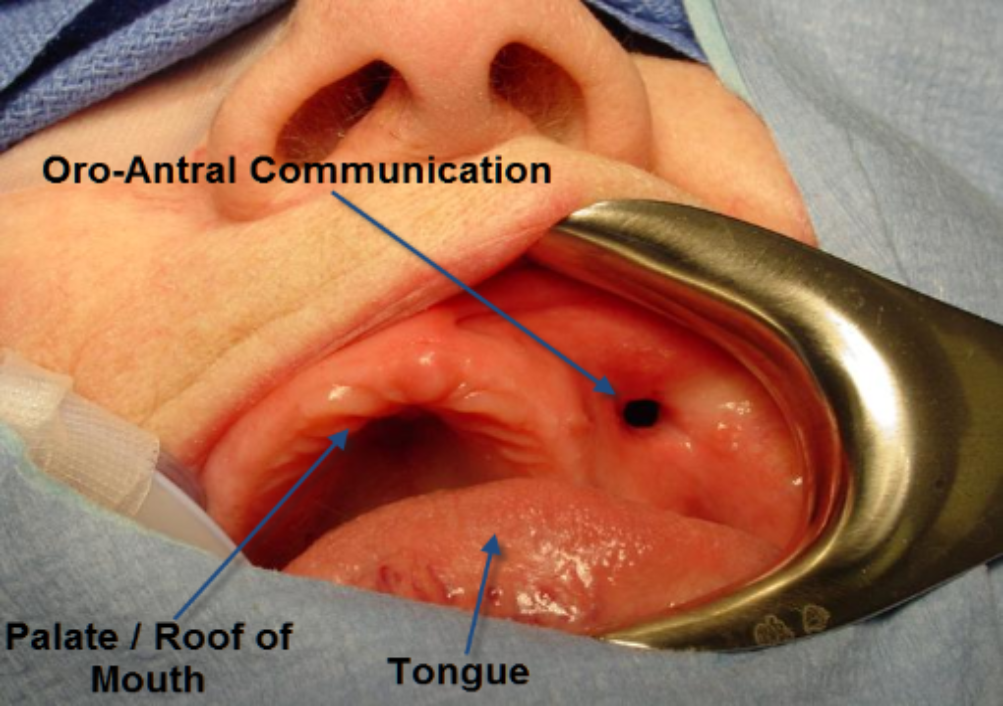
- bone defect with intra-oral or oro-antral (maxillary sinus) communications
- mandibular constriction
odontogenic (tooth) + pharygeal abscess (latero-pharyngeal)
(any abcess can lead to septic mediastinits❗)
Staphilococcus
- Septic shock
- fever +Oligura + Tachycardia + diaphoresis +agitation
- Dysphagia + Dyspnea
- ASthenia
- Chest pain
- Trismus
- productive cough
{kind=link}
{kind=link}
- wide incision + drainage of all affected cervical region (open the whole fucking neck) 📷
- Debridement of necrotic tissue (uni or bilateral)
- AB (first broad spec (Meropenem, Vanco, Metronidazole) later accord antibiogram)
- General correction
thoracotomy 📷
{kind=link}
- Arrhythmia
- septic shock
- erosion of carotid artery
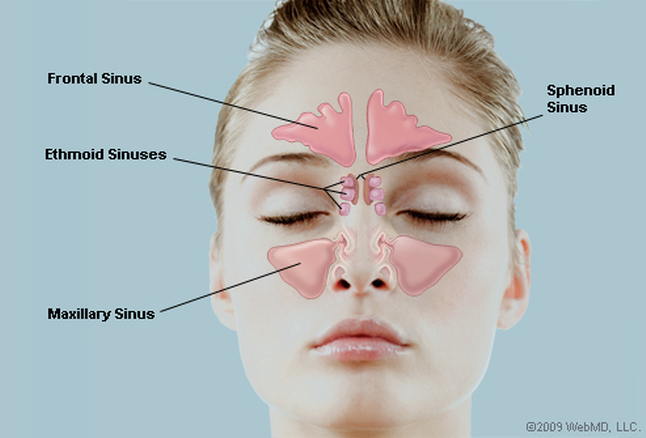
🦷 Odontogenic maxillary sinusitis
{kind=link}
Inflammation of the mucosa lining the paranasal sinuses
→ due to viral, bacterial infections, or allergic reactions.
- Chronic rhino-sinus inflammation
- nasal polyps (obstructive)
- Sept diviation
- Molar + Premolar teeth pathologies near the sinus (periodonitis, pockets)
- Osteitis
- Tumors
- Treatments damage
- Foreign bodies + Dental implants
- Triad:
- Dental pain → intraorbital pain → ↑↑in pain when bending over
- Subjective cacosmia (abnormal sense of smell)
- purulent rhinorrhea
- Others:
- Congested skin
- pain at palpation
- nasal obstruction + congestion
- tension infraorbital region
- fatigue + fever
- Sinusitis after URT infection

- chronic exacerbates maxillary sinusitis
- purulent rhinitis (Øsinus)
- maxilly cyst, intrasinusal cyst
- osteomyelitis (maxillary)
- dental tumor
- carcinoma
- Odontogenic sinusitis + Øoral-antral communication → endoscopic drainage and extraction +extraction tooth
→ if endoscopic not sucessfull → Caldwell-Luc radical antrostomy (trans-os drainage)📷
{kind=link}
2. Odontogenic sinusitis with oral-antral communication
- Antrostomy + closure of communication
- NSAID, AB
- Nasal decongestants + fluidifiers
T
directly or repeatend acute maxil. sinusitis
- Diffuse pain, headache
- Purulent rhinorrhea
- Subjective cacosmia (subjective perception of foul or unpleasant odors)
{kind=link}
{kind=link}
- surgical dental extraction
- cyst or tumor surgery
- accidental injuries
- infections (nonspecific or more specific i.e. TBC)
- Endo-oral orifice → alveolar ridge, vestublar, invisible
- after 4-6w after extraction → might be invisble + epithelialized but maxillary polyp can protrude through it
- VALSALVA sign (compress nose + blow air → fluid leaking out the orifice
- fluid backflow thorugh nostril
- air from sinus into nose
- nasal voice
- spontanous healing
- chronic sinusitis +/- ac. sinusitis
- Protetic treatment: after maxillectomy or in relapsing communications
- Comunication orifice plasty (when clean + w/o secretion )
- no hard blowing of nose
- AB + NSAIDs 7days
- decongestants
💦 Salivary gland pathology
the skin
- #1 Traumatic (penetrating)
- abscess of partoid gland
- Sialolithiasis (complicated with abscess + fistula)
- TB
- Tumor
- Surgery
- small orifice with erythematous halo
- on path of main salivary duct or directly from parenchyma 📷
- salivary discharge
- catheterization fistula duct
- Sialography or Fistulography (contrast + xray)
when trauma in this area → prophylactic treatment: suture Stenon duct📷; drain tube
curative:
- Atropine → ↓in salivary secretion
- Restricting mastication
- Compressive bandage on gland
- Cauterization (of fistula tract)
- Surgical plasty of fistula
removal of entire gland
inflammation of the epithelium of the salivary glands
- bacteria from mouth (pneumococcus, staph)
- Virus: Mumps, Herpes, Cocsacki
- Catarrhal
- Suppurative
- Gangrenous
- Catarrhal → inflamm infiltrate, enlarged gland, painful, fibrous viscious saliva
- Suppurative → microabscess, pus in gland + duct which is also excreted📷, enlarged, pain
- Gangrenous → necrosis, parotid inflammation, skin congestion+necrosis+ulcer, facial n. damage, altered general condition
prophylactic: supression of etiology, hygiene, stimulation saliva secre: pilocarpine
curative:
- AB systemic + inject into gland(with proteoloytic enzymes)
- masage of gland
- if necessary: incision + drainage
F → most often in submandibular gland, but parotid also possible
- Salivary Colic: migration calculus → distension (intense pain w eating) → "salivary phantom tumor" → disappears few hours postprandially
- Salivary Abscess: usually after colic → pain, fever, mastication + swallow difficulties → Rooster's crest + purulent secretion Wharton's duct
- Salivary "tumor" → repeated infection → fibrotic transformation → enlarged, harded, only slightly painful

- submandibular abcess,
- sublingual abscess
- submandibular adenitis
lesion + perforation of accessory (minor) salivary gland
F → children + young
- Paramedian lower lip
- buccal
- usually taken out - because recurrance
- also can heal + evacuate spontaneously
chronic obstruction accessory gland → cystic dilation of excretory duct of
also often recurrance → take it out (surgical excision together with accessory gland)
Ranula 📷
{kind=link}
- sublingual
- submandibular
(both =bisac)
surgical excision together with sublingual gland
- mixed tumor
- of major+minor salivary gland
higher than in major
T
- nodular
- painless
- well-demarcated
- mobile
- rapid growth
- accentuation of skin vessels
- facial nerve paresis
- positive lymphnodes
- pain
- altered general condition
- adenocarcinoma
- glandular cyst
- Surgical excision: Parotidectomy but ↑recurrance risk → take adequate margins
- Superficial paritoidectomy (if sup. parotid lobe)
- Deep Paritoidectomy (if deep lobe)
- preserve the facial nerve
Warthin tumor
- parotid gland
- submandibular gland
- palate
- PLGA (Polymorphous low grade adenoca)
- NOS (Not other specified; only adenocarcinoma can be specified)
T
F → can be of any grade
- nodular onset
- pain
- facial nerve paresis
- infiltratative growth
- rapid increase in size
- lymphadenopathy
F → 50% survival at 5y
radical surgery of primary tumor + lymph mets
- radiation when indicated
- superfiical parotidectomy when low grade + superficial lobe
- total parotidectomy when deep lobe
- neck dissection when LN mets, tumor >4cm, high grade, invading
- also resection of strucutre in continuity (skin, muscles, bones)
mucoepidermoid carcinoma
T - general 5y survival is 80%
T → ↑mets to regional nodes → 5y surial than only 5%
myasthenia gravis
nerves
T
T
Uncertain cause
- bilateral parotid gland enlargement 📷
- soft + non-tender
- if mild → Ø treatment
- if gland disfigured → partial parotidectomy
Sjörgen syndrome

Sicca symptoms:
- dry eyes
- dry mouth
- parotid gland enlargement
extraglandular:
- atralgia + myalgia
- GI abnormalities
- neuronal abnormalities
- RTA (renal tubular acidosis), pericarditis, pulmonary HT
- Ocular symptoms
- Oral symtpoms
- Ocular signs (Schirmer test 📷)
- Oral signs → abnormal sialography
- Histo → lymphocytic sialoadenitis
- Auto-Antibodies (Anti-SSA or Anti-SSB)
symptomatic treatment (curative is Ø possible)
- topical therapy
- cyclosporing for dry eyes
- steroid
- rituximab (if primary Sjögren synd)
- parotid enlargement (uni-bilat)
- ↓salivary flow
- Øeye involvement (lacrimal gland)
- Lymphoma
- Adenocarcinoma
- symptomatic for salivary flow
- alpha interferon
- subtotal partidectomy in tumor-like appearance
lungs
0.5-15%
- parotid painless welling (uni or bilat)
- ↓salivary flow
- clinic
- radiology
- histology (non-caseating granuloma)
- steroids
- Immunosuppressiva (MTX, AZA)
👻 Benign Tumors: Oro-maxillo-facial and cervical
- pre-exisitng problem will affect/is affected by treatment
- oral lesion might by due to systemic disease
- duration
- change in size
- change in appearance (i.e. lump → ulcer)
- Associated symptoms: pain, swelling, dysphagia, LN swelling etc.
- B-symptoms: nausea, fever, anorexia, weight loss
- History reason for lesion → trauma, tooth-pain etc.
ABCDE 📷
{kind=link}
- location
- consistency
- borders
- color
- size + shape
- surface
- LN
- pulsation + fluctuation
- Ulceration
- ill-defined border, raised margins
- bleeding
- fixation
- LN enlargement, Øpain, firm, fixed
vascular endthelium prolif
- Bleeding and ulceration
- Ocular locations can lead to strabismus, amblyopia, and astigmatism.
- Cervical locations may cause airway obstruction.
- Multiple cutaneous and visceral hemangiomas can be observed.
- Tuberous → surveillance
- steroids
- Sclerosing agents injection
- Laser therapy
- Embolization
- Surgical excision (only in small, well defined - you can provoke severe hemorrhage ❗)
- (or embo + excision)
{kind=link}
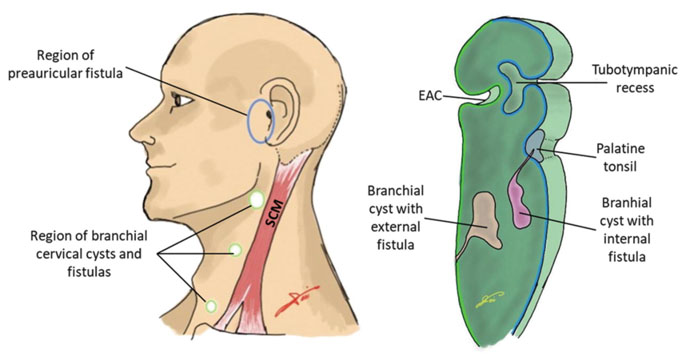
- congenital epithelial cyst - arise in child or young adult
- from failure of obiteration of second branchial cleft in embryonic development
- arise on lateral part of the neck (often submandibular, generall along SCM ant. border)
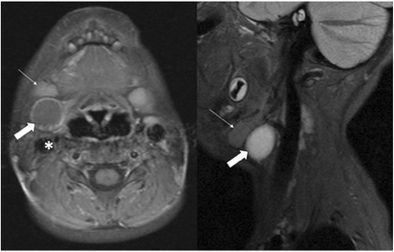
- solitary painless, non-tender 📷
- history of interemittend swelling + tenderness during URT infection (might be tender if secondary inflammation/infection)
→ evtl. mucoid purulent discharge into pharynx or skin (associated sinus tract)

MRI 📷
{kind=link}
often cholesterol crystalls inside the tumor❗
- metastatic carcinoma → cystic degeneration
- lymphoma
- paraganglioma
- infection
- mass effect → dysphagia, dyspnea, pain
- cosmetic
- acute infection (treat prior)
- general contraindication for surgery
🔪Cyst removal (surgical excision)
→ horizontal incision
F it is the most common congenital cervical cysts
Anomalous development + migration of thyroid gland
{kind=link}
average 6y
50% before 20
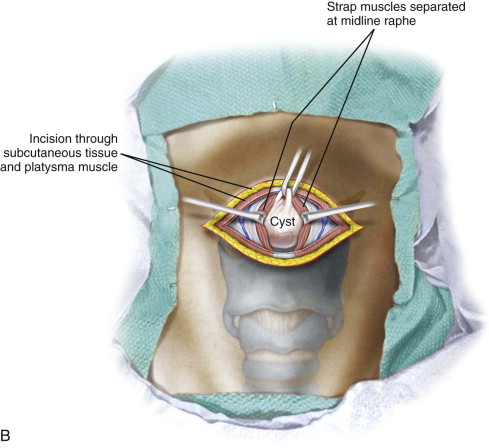
- asymptomatic palpable midline neck mass at the hyoid bone (or supra or infra-)📷
- moves with swallowing
- evtl. pain + dysphagia
clinically + US
normal thyroid tissue at usual location → thyroid scans + functional test
Sistrunk procedure: removal of cyst + central portion of hyoid bone (to ensure complete removal of tract)
{kind=link}
benign ondotogenic tumor of jaws
solid, cystic, mixed
Angle of mandible
- locally destruction + spread into ST → treat like a maligant tumor
- can undergo malignant transformation
facial or jaw bone deformities
F does not do that
Xray → "soap bubbles" 📷
{kind=link}
surgical
- curretage (scraping out) / enucleation (only tumor cells removed; other parts untouched)
- bone resection + reconstruction
🦀 Malignant Tumors of the oro-maxillo-facial
Mole: sharply-cicumscribed chronic lesion
- Simple: ØUnna(nevic) cells → Ømalignant transform
- Nevocellular: contain Unna cells → malign. transf
- Atypical/dysplastic: contain melanocytes → malignant transf.
ABCDE 📷
A - asymmetry (irregular surface)
B- Border - irregular
C- color + consitency → totally tarker or different colors
D- Dimension → brutal extension
E - Evolution + Extra (tenderness, bleeding, ulceration + pruritus)
- ↑likelyhood of malignant transformation
- cosmetic
surgical excision (see below)
- extensive surgical exision + LN dissection
- Interferon alpha
- Radiation +chemo
{kind=link}
{kind=link}
excision + plastic reconstruction (free skin graft, local + regional flaps)
→ if less predictive: chemo + radiotherapy
MOHS MICROGRAPHIC SURGERY 📷
{kind=link}

{kind=link}
- underlying bone
- perineural invasion
- reginal LN mets
- wide excision + reconstruction
- LN dissection (prophylactic or therapeutic)
- LONG TERM MONITORING❗ → ↑risk of recurrence + LN mets
erythoplakia + leuplakia (slightly raised)
(can also be spleckled leukoplaskia ) white patch on periphery of erythroplakia
Nerve+ear+tongue+tooth+pharynx+functional(trismus)+bleeding
- Nerve-damage: Paresthesia, Paresis, paralysis
- Otalgia (ear pain) → if tongue, floor, maxill. sinus lesion
- Odontalgia (tooth pain) → bone tumors
- Tooth mobility → bone tumors
- Glossodynia (burning mouth)→ tongue tumor
- Dysphagia → paryngeal tumor
- Spontaneous bleeding or when chewing
- Ankyloglossia (limited tongue movement)
- Trismus (limited mouth opening)
- clinic
- Toluidine-blue staining 📷
- Cytology
- Biopsy
- LN examination
- Imaging → MRI, CT, xray, US, scincti
- check tumor suppressor gene p53
- other tumor markers
- Ulcer or fissure (Øpain Ø healing)
- Nodular (later ulcerated)
- Proliferative - cauliflower
DESTRUCTION + INFILTRATION:
- Dental signs: pain, mobility, avulsion
- Eye signs: Orbital floor syndrome + post. orbital sydrome

- Extension infratemporal fossa: Trismus, pain, edema
- Nerve involvement: Pain, paresthesia, paresis, paralyis
- Functional impairment: Difficulties chewing, swallowing, moving tongue + jaw
- Adenopathy
- Distant mets + related symotoms
- B-symptoms
- Surgical incision (2cm margins)
- neck dissection
- reconstruction (i.e. fibula flap)
4. radio + chemo
5. others (cryotherapy, laser, immuno)
surgery + radiation (alone or combination)
advanced + recurrance
survival + minimum function impairment
options:
- limited partial resection
- subtotal maxillectomy + rhinotomy
- maxillectomia + orbital exenteration
- partial restection cranial base + dura mater
- resection; depends, can be:
- partial
- segmental (interruption continuity)
- asc. ramus resection
- condyle resection
- reconstruction
take care of the 🦷
→ oral cavity sanitation before start❗
👶🏽 Congenital malformation and anomalies
- Partial cleft
- Anterior: (involves primary plate)
- Incomplete: lip + nasal floor
- Complete: alveolus, lip + nasal floor
- Posterior: (involves secondary plate)
- Incomplete: soft pallate
- Complete: soft + hard pallate
- Total Cleft = ant + post. cleft
⇒ both can be unilateral or bilateral
{kind=link}
combination betw.
ant, post, complete, incomplete, unilat, bilat
{kind=link}
{kind=link}
Cleft assoc. w/ macrostoma → 📷
syndromic patients
FUNCTIONAL DISORDERS:
- sucking, swallowing
- chewing
- phonation
- middle ear function
→ with indersiciplinary team
- at 2 weeks: treatment planning, caries prevention, palatal plate📷 (to obturate the cleft)
- 3-6m: lip plasty (uni- or bilat
- 5-6m: auditory function test
- 12-18m: Soft+hard palate plasty
- 2y: surveillance of tooth eruption
- 3-4y: logopedic treatment (breathing exercises + occlusive consonant pronunciation)
- 5-6y: re-intervention lip, nasal floor, vestibular space, elongation columella📷
- 8-12y: secondary osteoplasty (with autogenous illiac crest graft)
- 8-14y: Intensification orthodontic treatment (calibration upper + lower arch, dental reposition) , speech therapy, osteodistraction
- 15y: nasal cartilage + nasal bone surgical correction
- 18y: Maxillary hypoplasia surgical correction
- 20y: correct of unfinish + final prosthetic treatment
- Prosthetic Surgery
- Surgical Orthodontics
- Speech Therapy
- Control of Auditory Function
- Psychology
{kind=link}
{kind=link}
- elevate nasal + sinus mucosa
- osteotomy (like leford I - 📷) - seperate maxilla from pterigoid process (alert: pterigoid-palatine vessels❗) → free-maxila → bring it in front
- splint on maxilla → bring in contact with mandible
- osteosynthesis (micro-plates + screws at zygomatic alveolar process + piriform apperature)
- bilateral sagital osteotomy on mandible → keep post part (with nerves + vessels) in place and push the anterior part laterally → free mandible → push post (max 13mm - risk of asphyxia
- osteosynthesis of mandible
{kind=link}