
Table of content
- Gastroenterology
- 💥 Abdominal pain and Dyspepsia
- 🍤 Gastro-Esophageal diseases
- 💩 Chronic Diarrhea, Celiac Diseases, IBS, Constipation
- 🔥 Inflammatory bowel disease
- 🩸 Upper and Lower GI Bleeding
- 🍄 Diverticulosis, Polyposis and Colo-Rectal Cancer
- 🍑 Liver Pathologies
- 🎋 Biliary Tree Pathologies
- 🧽 Pancreas Pathologies
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6
Gastroenterology
💥 Abdominal pain and Dyspepsia
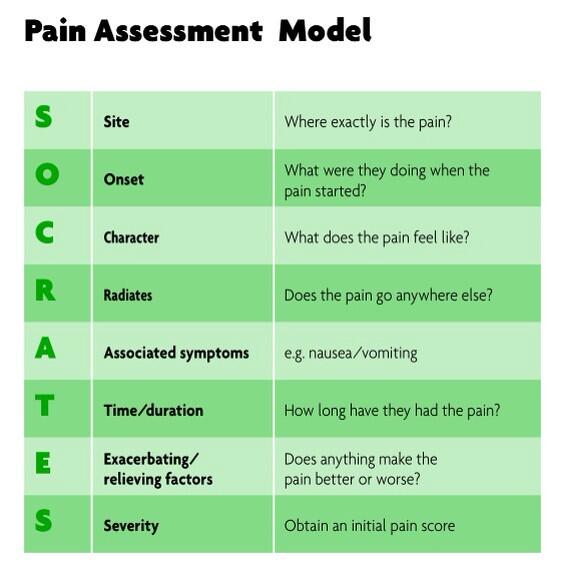
SOCRATES 📷
*associated symtpoms: nausea, vomiting, diarrhea, constipation, fever, weight loss, genitourinary symptoms?
*character: burning, colicky, stabbing, persistent etc.
- PMH
- Medication (i.e. NSAIDs)
- Alcohol, smoking (+other risk factors)
- Travel history
- MI
- Pancreatitis (chronic + acute)
- Peptic ulcer diseases (gastric + duodenal)
- GERD
- Gastritis/Gastropathy
- Functional dyspepsia
- Gastroparesis
- Biliary tree disorders







- Splenomegaly
- Splenic infarct
- Splenic abcess
- Splenic rupture



Biliary
- Biliary colic
- Acute cholecystitis
- Acute cholangitis
- Sphincter of Oddi dysfunct.




Hepatic
5. Acute hepatitis
6. Perihepatitis
7. Liver Abscess
8. Budd-Chiari snd.
9. Portal v. thrombosis




eating 🍰 (before or after)
- upper GI discomfort /pain related to eating
- early satiety
- postprandial ballooning /bloating
- retrosternal heartburns
- regurgittation
- dysphagia
- eructations
- nausea + vomiting
- GERD
- Esophageal syndrome
- Dyspeptic syndrome - Ulcer type
- Dyspeptic syndrome - Dysmotility type
- Dyspeptic syndrome - mixt type
- GERD → heartburn + regurgitation
- Esophageal syd. → dysphagia + odinophagia
- Dyspeptic syd.
- ULCER → epigastric pain (burning, related to eating)
- Dysmotility → Early satiety, plenitude, postprandial bloating, nausea+vomiting
- Mixt → both
- Organic = Inflammation, infection, neoplasm
- Motility = Esophageal MD, Gastro-paresis
- Functional dyspepsia


NSAIDs
iron
K+
Digoxin
ABs
- HP
- Giardia lamblia (lel)
- DM
- Thyroid
- Hyper.PTH
- Addisons
- Uremia





→compare sketchies
- >45y
- dysphagia + odynophagia
- Family history of upper GI neoplasm
- alarm symptoms: weight loss, anemia, loss of apeptite
- no response to empirical therapy
- functional chest pain
- functional heart burn
- reflux hypersensitivity
- Globus
- Functional dysphagia


presence of dyspeptic symptoms:
- PDS (post-prandial distress syndrome): early satiety + postprandial fullness
- EPS (epigastric pain syndrome): epigastric pain + burning
- absent of organic disease (after EGD, H.pylori test+treatment + after alarm feature evaluation)
Psychiatric (anxiety, depression, panic) → they might be the cause
- symptoms present in last 3 month
- onset at least 6month earlier
young woman
🍤 Gastro-Esophageal diseases
Benign gastro-esophageal diseases
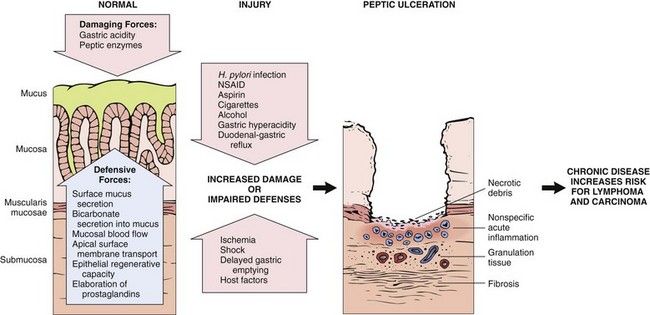
- Gastropathy - mucosal injury w/o inflammation
- Gastritis - mucosal injury w/ inflammation
loss of parietal cells 📷
- acute H.Pylori Gastritis
- Other infective gastritis (bacteria, virus, fungi, parasites)
- Acute non-infective gastritis
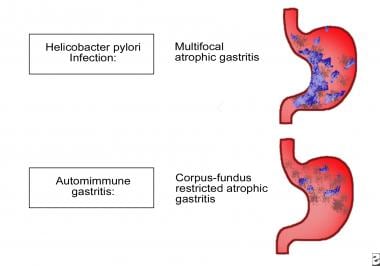
Type A (autoimmune) → Body fundus
Type B (H.P. related) → Antral predominant (multifocal)
Types AB (environmental) → Antral-body
Chemical (reflux) gastritis → Antral-body predominant
Chronic Gastritis: (Sydney classification)
- Non-atrophic: H. pylori
- Atrophic: H. pylori, dietary, environmental factors, autoimmunity
- Chemical: NSAIDs, Bile
- Radiation: Radiation injury
- Lymphocytic: Celiac disease, drug
- Eosinophilic: Food allergies
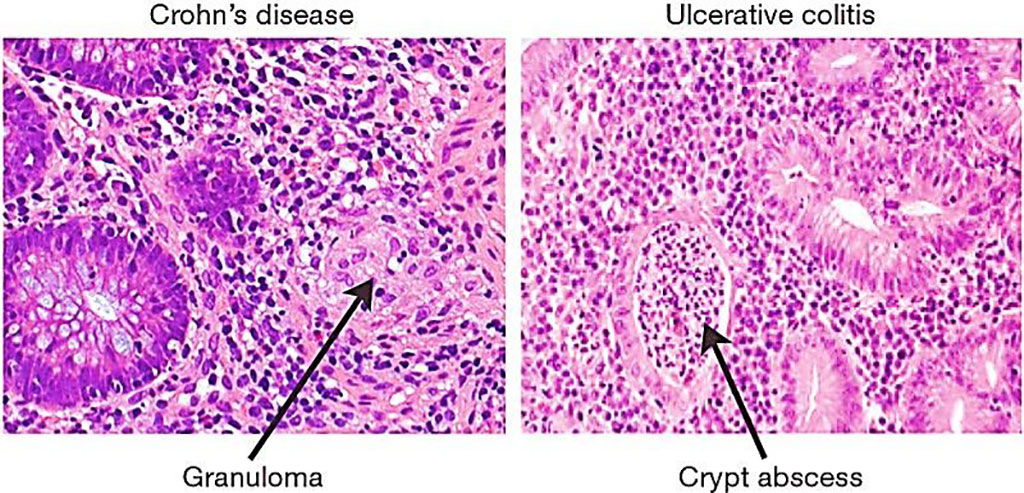
- Non-infectious granulomatous: Crohn's disease, sarcoidosis
- Other infectious gastritides: Bacteria, viruses, fungi, parasite
Acute gastritis: (Sydney classification)
- Hemorrhagic/Erosive → Alcohol, NSAIDS, shock/pysiological stress
- Non-erosive → H.Pylori caused
- NSAIDs
- H.pylori
- alcohol
- acute stress (ICU patients→ on ventilator >48hrs)
- bile
- cocain
- ischemia (i.e. due to cocain)
- trauma
- food poisoning
- 🔥burning epigastric pain
- +/- nausea + vomiting
- might improve or worsen with eating
🧯NSAIDs (oral +systemic!)
→ hemorrhagic, erosions + ulcer 📷
- Stop NSAID
- PPI
- Misoprostol (PG-analogue)
chronic form → acute complications
Non-Invasive:
- Urease breath test
- Stool Ag
- Blood Ab (serology)
Invasive - Endoscopy:
- Biopsy → Urease testing
- Biopsy → Histology
- Culture + AB sensitivity testing
Invasive - Endoscopy Testing Methods | Non-Invasive Testing Methods |
Biopsy Urease Testing | Urea Breath Test (UBT) |
Specimens from biopsies → immersed in a solution with urea and an indicator for pH → If H.Pylri present = breakdown of ureas into ammonia ⇒ ↑pH ⇒ color change | H. pylori’s urease: break down urea yielding isotope-labeled carbon dioxide and ammonia → detected by breath test |
Histological Examination | Stool Antigen Assay |
Tissue samples from antral region + body → microscopy → visibility of H.Pylori | H. pylori antigens in fecal matter = marker of active infection |
Culture and Sensitivity Analysis | Serological Testing |
↑ specificity
but H.Pylroi = hard to culture (↓ sensitivity) | Detects IgG antibodies against H. pylori.
Lacks local validation → less useful in clinical settings |
- Triple therapy or Quadruple therapy (if triple failes)
→ 4-6weeks: PPI + Amoxi + Clarithro (alternative metronidazole)

- Different toxicities of medications
- Relative costs of each medication and regimen
- Emergence of antimicrobial-resistant bacteria
- Level of patient compliance
- Non-invasive tests after 4 weeks.
- Stop PPI (Proton Pump Inhibitor) for 2 weeks before testing.
“Intestinal type gastric carcinoma” = AdenoCA!
- Begins in childhood
- Superficial mononuclear inflammation and acute neutrophilic inflammation
- Gastric antrum and fundus
atrophic gastritis → loss of mucous glands → immature glandular glands (goblet-cell-like) → intestinal metaplasia → gastric AdenoCa
Iron, Ca, Mg, Zinc
Ab → gastric glands, parietal cells, intrinsic factor → glandular atrophy, Achlorhydria + Inflammation
- Hyperplasia of G-cells → Hypergastrinemia
- pernicious anemia (loss of intrinsic factor)
- Cobalamin deficiency
- iron def. anemia
Adenocarcinoma + Carcinoid tumor
other AI
- hashimotos, addisons, etc
insidious + slow progress (aka sneaky MF 🐀)
- Hematologic → Megaloblastic Anemia
- GI → Megaloblastosis of GI-epithelium → malabsorption → Anoxrexia (mod. weight loss)
- Neurologic manifestations → Demyelination, axonal degeneration, neuron death → Peripheral paresthesia, Ataxia, Sphincter disfunction, Mental function disturbances
- UGI endoscopy → Biopsy+Histology
- Auto-Ab → Anti-instrisic factor, Anti.parietal cell
- Gastrin levels
Gastric cancer! → EGD every 3-5y
B12 replacement
- incompetent pyloric sphincter
- abnormal duodenal motility
metaplastic atrophic gastritis in ANTRUM
similiar effects on mucosa like NSAIds
EGD
- lifestyle
- weight reduction
- dont eat + lie down
- PPI
- Prokinetics (move the shit quickly from stomach to duodenum)
- baclofen → ↑ LES tone (in case of reflux into esophagus??)
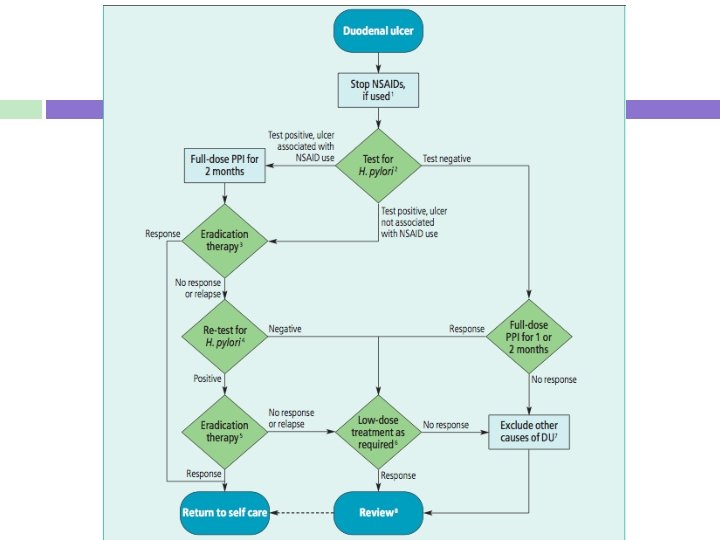
Duodenal Ulcer
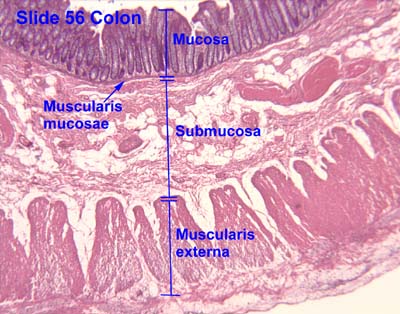
break in superficial epithelial cells → penetrations to Muscularis Mucosae 📷
most common location - #1 duodenum
lesser curvature
F: rarly the case
H. Pylori
(1) H. Pylori (2) Zollinger-Ellison Syndrome (gastrin secreting gastrinoma) (3) NSAID usage
smoking does not cause ulcers but can exacerbate symptoms
70% = majority
(1) Epigastric Pain = most common (2) Heartburn = 50% of the time
- Nausea
- Pain radiation to back (DDx pancreatitis)
- Bloating + distension
- Fatty food intolerance
Gastric = worse with meals Duodenum = better with meals
(1) Dysphagia + Odynophagia* (2) Vomitting (persistent)* (3) Iron-deficiency anemia (4) weightloss (5) Family History (6) >55 years old with new-onset dyspepsia (7) chronic GI bleeding (8) Epigastric mass
(1) Urease Breath Test (2) Stool Antigen Test
Acid Suppression (PPI) + 2 Antibiotics (clarithromycin + amoxycilin or clarithromycin + metronidazole)
Prescribe a PPI 1-2 month
Remove the offending agent
EGD 📷
Perform a biopsy
Biopsy of Antrum
(1) Zollinger-Ellison-Syndrome (2) Hypercalcemia
(1) Elevated Gastric Acid (2) Multiple Peptic Ulcers (3) Gastrinoma
F → continue PPI but Ø AB
(if H.Pylori found → add AB)
12 weeks
PPI Therapy or H2-antagonists
- 🩸 Hemorrhage
- ↖️ Penetration → into adherent underlying tissue (i.e. pancreas)
- ➡️ Perforation → peritonitis
- 🕸️Fibrous stricture → pyloric stenosis
- 🦀Malignant transformation
Surgery
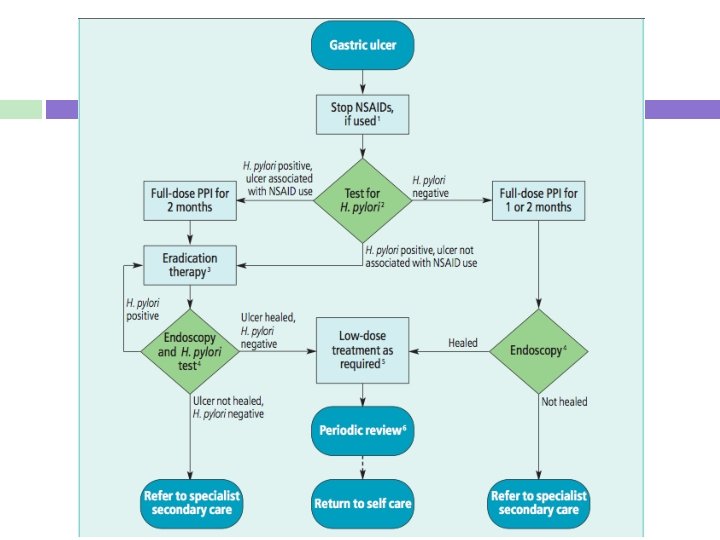
NSAID induced: 2 month PPI → then eradication
non-NSAID related: directly eradication
- Reflux/Regurg/Acid Brush
- Retrosternal Burning Discomfort (heartburn)
- Epigastric Pain (postprandial)
- Assoc. laryngeal irritations
- Chronic Cough
- Wheeze (if bronchial)
1) Obesity only
Lower Esophageal Sphincter Dysfunction (open too often or for too long)
→ gatric distension (delayed emptying)
→ gastric pressure (obesity)
- ↑LES opening
- Hiatus Hernia
- ↑Pressure
- Obesity
- Pregnancy (+estrogen effects)
- Substances (↓LES tone)
- Caffeine
- Smoking
- Alcohol
- Chocolate
- Nitrates
- Calcium Channel Blockers
Fat COPS have GERD.
- Eating
- Laying flat
- PPIs (omeprazole)
- H2 antagonists (ranitidine)
- Dysphagia
- Odynophagia
- Weight Loss (unexplained)
- Anemia (unexplained)
- GI bleeding (Melena, Hematochezia)
- High Risk for Barrett's Esophagus
- Failure of PPI trial
- Family Hx
- long GERD>5 years
- old Age>50
- Obese
- Smoking
False - symptoms can wake patients at night (night cough too)
Antacids
EGD
(+Barium swallow)
A)
- EGD
- biopsy
B) both every 3 years (lecture says 3month lel)
non→3years (4x a year)
low grade → 6-12month (2x - 1x a year)
- refractory or atypical🚩 GERD
- therapy for esophageal strictures
esophagectomy
- Impedance pH monitoring of the esophagus
- Manometry - r/o esophageal motility disorders
pH gets pH, number of reflux episodes, how high up reflux extends, and how long the episodes last. Gives you a DeMeester Score
- GERD non-responsive to PPI
- Extra-esophageal GERD symptoms
DONT GIVE PPI if no acid reflux
The impedance-pH monitoring test assesses the relationship between the patient's symptoms and acid reflux, nonacid reflux, or no reflux.
→ The test determines if the symptoms are associated with any type of reflux.
- Erosive Esophagitis → Strictures
- Barrett's → Adenocarcinoma
- Hemorrhage
!not all patients have esophageal injury! = non erosive GERD
take a biopsy
- Chronic GERD
- Infectious (HSV, CMV, Candida - HIV Pts)
- Pill esophagitis
- Eosinophilic Esophagitis
manometry or barium swallow
Immunocompromised (i.e. HIV patients)
- Nissen Fundoplication (360 wrap)
- Toupet Fundoplication
- Dor Fundoplication


Dysphagia (wrapped up too tight during surgery)
- Refractory to PPI BID (doesn't work) or:
- Don't want to
- can't take PPI
- complications
- Barret's Esophagus (complication of GERD)
- Esophageal Strictures (complication of GERD)
- Extra esophageal (Chronic Cough, Wheeze, Laryngitis)
T
- Assessment of esophageal emptying
- Presence and type of hiatal hernia 📷
- Motility disorders
- Stricture or distal mucosal ring
- Presence, cause, height, and persistence of the reflux
- Quit smoking
- Avoid alcohol consumption
- Achieve weight loss if necessary
- Consume small meals
- Wear loose-fitting clothing
- Avoid lying down for at least 3 hours after eating
- Elevate the head of the bed by placing blocks of wood under the bedposts (using extra pillows will not suffice)
- Hematemesis
- Cough, aspiration pneumonia
- Tumor affecting the recurrent laryngeal nerve
- Fistula between esophagus and air-tracts
- Dysphagia
- Odynophagia
- Weight loss, undernutrition
- Pain
- Regurgitations
- mainly direct invasion
- lymphatics (downward direction)
- rarely blood (liver, lung, bone, brain)
Malignant gastro-esophageal diseases
- Type A Gastritis Feature: Pernicious anemia, atrophic gastritis (achlorhydria)
- Family history
- Previous gastric resection
- Chronic peptic ulcer
- HP infection
- Smoking + Alkohol
- japanese
- nitrates + preserved food
[gastric ulcer]
Diffuse gastric adenocarcinoma in the submucosa
- occult GI bleeding (melena)
- nausea, abdominal pain
- Weight loss
- Anemia (iron def)
- Dysphagia (in prox)
- Colonic obstruction (spread)
- Ascitis
- Jaundice
- Blumers Shelf (mets in douglas pouch on DRE)
- Virchow node
- Sister mary joseph node
- Krunkenberg tumor
💡MERKE: AdenoCa or linitis plastica
- Intestinal Gastric Ca
- arises from of intestinal metaplasia
- polypoid or ulcer
- Diffuse Gastric Ca aka Linitis plastica
- infiltrates deep → no mass → spread in gastric wall
- mixed morphology
Early: mucosa+submucosa (T1 any N) → curable
Advanced: Muscularis → Type III + IV incurable
False - take multiple (upto7) biopsies of both suspicious and normal gastric mucosa
- Early superficial mucosa lesion can be missed
- no DD betw. benign + malignant ulcer
linitis plastica (”leather bottle” stomach)
(1) CT chest, abdo, pelvis or PET for distant mets (2) Laparoscopy →indicated: >T1, without stage VI disease (3) Endoscopic Ultra Sound
False - unresectable
Often mets at time of diagnosis - peritoneal seeding, invasion to surrounding structures, and distant mets
surgery
- Preoperative staging
- Nutritional deficiencies screening and consideration of nutritional support
- Symptomatic control
- symptomatic anemia: Blood transfusion
- Hydration
- Prophylactic antibiotics
- ABO and crossmatch
- Inquiry about current medications and allergies
- Smoking cessation
Locoregional (stage I-III) disease
- Potentially curable
- Multidisciplinary evaluation and consideration of surgery
Advanced (stage IV) disease
- Palliative therapy
- Longer survival and better quality of life with systemic treatment
- no proven benefit in treatment of curable cancer
- post-operative radiotherapy may decrese recurrence
- used for reduction of tumor bulk in palliative care
Total gastrectomy with reconstruction (see later)
Partial gastrectomy with reconstruction (see
Lymphadenectomy
- Remove distal part of esophagus
- Remove proximal duodenum
- remove greater+lesser omentum (to remove lymphnodes)
- remove LN
⇒ Roux-En-Y = Esophagojejunostomy 📷
- Duodenal stump leakage complications
- Secondary bleeding
- Nutritional deficiency (long term complication)
- Peritoneal + pleural effusion
- gastric outlet obstruction
- bleeding
- intrahepatic jaundice
- history
- ulcer relieved by antacids, cancer not
- ulcer periodic, cancer consistent
- cancer symptoms not assoc. with eating
- Gastric ulcer
- Other gastric neoplasm
- Gastritis
- Gastric Polyp
- Chrons (?)
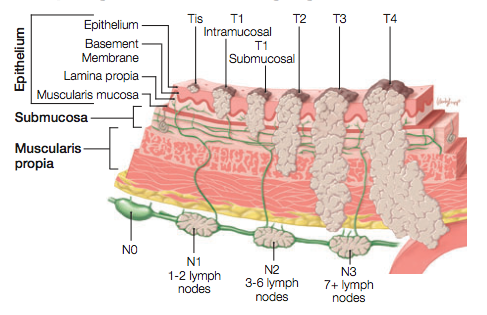
[depth of invasion] and presence of absence of [regional LN involvement]
- Lymphoma → might arrise from chronic gastritis
- similar presentation to gastric Ca
- +periph. adenopathy, splenomegaly, abdominal mases
- Dg: EGD, barium xray, CT FNAB
- Tx: surgery:total or partial, splenectomy; adjunct radio + chemo
- GIST - Gastrointestinal Stromal Tumors
- =leiomyoma+leiomyosarcoma
- from cells of cajal
- inccidental finding on endoscopy or barium
- endoscopic biopsy not helpful →mucosa normal
- small tumors → wedge resection
- larger → gastrectomy
- Barium esophagography
- CT (Contrast-enhanced computed tomography)
- MRI (Magnetic resonance imaging)
- EUS (Endoscopic ultrasonography)
- PET (Positron-emission tomography)
surgical resection at early stage
(1) Progressive dysphagia (solids first→DD achalasia) (2) Weight Loss (3) Retrosternal Chestpain (4) Hoarsness (voice)
(5)vomit /regurgitation
6) aspiration pneumonia
esophageal strictures
Early esophageal Ca leasion are present as [polypoid] lesions or coalescents [plaques] or [nodules]
EGD
biopsy
Squamous Cell Carcinoma
(1) Smoking (2) Alcohol (3) Nitrosamines (smoked/cured meats) (4) Hot Tea (5) chronic dysphagia
(6) Radiation
Der Plummer Vinson Tylos hängt am Strick deshalb kriegt er Achalasia
- Plummer-vinson synd.
- Tylosis
- Achalasia*
- Esophageal stricture* + diverticula


Lungs
Esophageal Adenocarcinoma
(1) Barret's Esophagus/GERD (2) Smoking (3) Obesity
(1) Liver (2) Peritoneum
(1) CT - mets, node (2) PET (Positron Emission Tomography - esp for abdominal lymph nodes + distant mets)
3) Laparoscopy/Thoracoscopy → best N-Accuracy
4) EUS for local invasion
5) MRI (why? → see later)
- Eccentric or circumferential wall thickening > 5 mm
- Peri-esophageal soft tissue and fat stranding
- Dilated fluid- and debris-filled esophageal lumen proximal to an obstructing lesion
assessing invasion of:
- trachea + bronchi
- aorta
- pericardial
same Se+Sp as CT
fat plane📷
Endoscopic Ultrasound (EUS) → T-Stage 📷
Dgx modality | T Accuracy (%) | N Accuracy (%) | M Accuracy (%) |
CT | 49-60 | 39-74 | 85-90 |
EUS | 76-92 | 50-88 | 66-86 |
Thoracoscopy/Laparoscopy | - | 90-94 | - |
distant mets
- Lower than T2N0M0 (1) Esophagectomy
- Higher than T2N0M0 (1) Neoadjuvant Chemotherapy (2) Esophagectomy
- Chemoradiation
Chemoradiation alone (surgery = technically challenging)
Postoperative Chemotherapy
Ivor-Lewis = Thoracic Anastamotic leaks Transhiatal = Cervical Anastamotic leaks
(1) Sepsis (2) Mediastinitis (3) Chylothorax
(1) Dyspnea (2) Distant Breath Sounds (3) Dullness to Percussion (4) Elevated Triglyceride Levels (>110 mg/dL) in pleural fluid
Xray
(1) Opacification of Hemidiaphram (2) Blunting of Costophrenic Angle
(1) Tube Thoracostomy (drain) (2) Surgical Thoracic Duct Ligation
Paliative esophageal stent placement → 1 month after chemoradiation
Um den Boy offen zu halten und Verbindungen nach Außen zu begrenzen.
- malignant esophageal stricture → surgery not possible, contraindication chemoradiation
- extrinsic compression (from lung/mediastinal tumor)
- Tracheoesophageal fistulas
- Esophageal perforation
- malignant reoccurance
2cm above + below the tumor
instruct patient to eat only soft food, ↓appetite, no peristalsis in the stent-portion, esophgram next day
- T in situ
- T1 Intramucosal + submucosal
- T2 invading muscularis propia
- T3. penetrating serosa/adventitia
💩 Chronic Diarrhea, Celiac Diseases, IBS, Constipation
≥3 stools/day and/or loose or liquid stools
Acute → <2w
Persistent → 2-4w
Chronic → >4w
small
- IBS
- IBD
- malabsorption synd
- chronic infection
- Watery
- Osmotic
- Secretory
- Inflammatory
- Fatty
- Motility disturbance
- Ingestion poorly absorbed osmotically active substances (i.e. laxatives w/ Mg, Phosphate)
- Carbohydrate malabsorption (i.e. fructose malabsorption, dissacharidase def., lactose intolerance)
⇒ condition that ↑ secretion of Cl or HCO3 or ↓Na absorption
- Bacterial toxins (↑secr)
- Endocrinopathies (Secretory neuroendocrine tumor [Gastrinoma, VIPoma] or Hyperthyroidism/Adrenal insuff)
- Congenital chloridorrhea (absent ion transporter)
- Malignancies (ie. Colon cancer, Lymphoma)
- Post-cholecytectomy (bile-salt diarrhea)
- Idiopathic
⇒ dmg to mucosa → ↓absorption/↑secretions
- IBDs
- Ischemic colitis
- Diverticulitis
- Radiation colitis
- Infectious
- Bacterial infection: Invasive (TB, Yersenia); C.Diff
- Ulcerating Viral: CMV, HSV
- Parasites (invasive): Amebiasis
- Maldigestion
- Pancreatic insuff
- Inadequate luminal bile acid conc. (i.e. in primary biliary cholangitis)
- Malabsorption
- Mucosal Diseases → Celiac, Whipple
- Short bowel synd.
- Post-resection diarrhea
- Mesenteric ischemia
- Bacterial overgrowth (bile salt deconjugation)
⇒ ↓contact food-products with mucosa due to Hypermotility
→ Hyperthyroidism, dumping synd
→ Post vagotomy and post-sympathetcomy
→ diabetic neuropathy
noctural bowel movement = organic
abnormal weight loss, fever, bleeding → organic
osmotic → better;
secretory → not better
Any AB
bacterial overgrowth
- Acid reducing agents (PPIs, H2-blocker)
- Mg laxatives/antacids
- NSAIDs
- ABs
- colchicine
- Furosemid
- Metformin
- orthostatic changes??
- Fever?
- Bowel sounds?
- Distension, tenderness, masses?
- DRE
- systemic signs (hyperthyroidism, skin, joint abnormalities, edema)
- bloating + flatulence
- bulky stools
- weight loss
- ADEK deficancy
- Anemia
- Coagulopathy
- Osteopenia
large
- blood
- mucus
- pus
- fever
- small volume
- CBC → Anemia, Leukocytosis, Eosinophila?
- Fluid + Electrolyte balance (chemistry screening)
- Inflammatory markers (CRP, Fibrinogen)
- Thyroid hormones
neoplasm + parasitic infections
- occult bood
- WBC
- Fat? → Sudan stain
- Fecal culture
Hydrogen breath test
“Hydrogen breath tests are based on the principle that bacteria metabolize carbohydrates, resulting in the production of hydrogen gas.” Humans never produce hydrogen gas, only bacteria can.
- correct fluid + electrolytes
- Etiological:
- Diet restrictions
- Opiates
- Bile acid resins
- Clonidine (in diabetic diarrhea)
- Octreotide (i.e. in VIPoma, chemoT induced, Aids-related diarrhea)
- DM1
- + familiy history
- Down syndrom
- Turner synd
- Selective IgA def.
- Classic: GI
- Atypical: Non-GI
- Asymptomatic
- Silent
- Latent
- chronic / recurrent diarrhea (watery or fatty)
- abdominal distension
- anorexia
- weight loss
- at 6-24month typical age of presentation
⇒ children: short, delayed puberty, failure to thrive
- Malabsorption symptoms: Vit deficiency, iron def. anemia, osteoporosis
- Dermatologic: dermatitis herpetiformis
- Dental: Enemal hypoplasia
- Silent: no/minimal symptoms, damaged mucosa, pos. serology
- Latent: no symptoms, no damaged mucosa, +/- pos. serology
HLA-DQ2 + -DQ-8
→ HLA encodes MHCII → presentation exogenous peptide to Antigen-presenting-cells
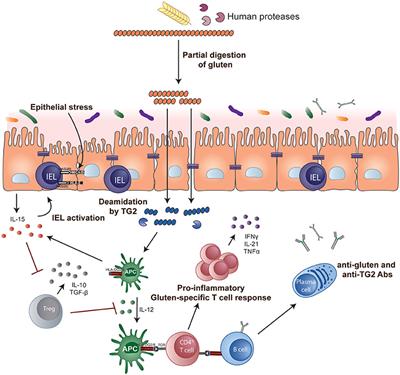
- Gluten-containing food consumption → Gliadin peptides release (upon partial digestion).
- Gliadin peptides → Deamidation by tissue transglutaminase (tTG) → Increased affinity for HLA-DQ2/DQ8 molecules on antigen-presenting cells (APCs).
- Gliadin-HLA complex on APCs → Activation of CD4+ T-helper cells in lamina propria → Release of pro-inflammatory cytokines.
- Cytokines & intraepithelial lymphocytes → Intestinal epithelial damage.
- Resultant Morphological Changes:
- Intestinal inflammation → Villous Atrophy.
- Compensatory mechanism → Crypt Hyperplasia.
- Damaged enterocytes → Loss of Brush Border.
- Loss of Brush Border & Villous Atrophy → Malabsorption Syndrome.
- Total IgA (↓)
- tTG-IgA(Anti tissue transglutaminase)
- AGA-Ab (Antigliadin)
- EMA-Ab (Antiendomysial)
- HLA typing DQ2+DQ8
- Villous atrophy
- Crypt hypertrophy
- Cuboid epithelium
- Intra-epithelial lymphocytes
- Lamina propria with Lp + Plasmocytes
Type | Description |
Type 0 | Preinfiltrative - normal mucosa |
Type 1 | Infiltrative - IEL more than 20/100 enterocytes |
Type 2 | Hyperplastic - Lieberkuhn crypt hyperplasia |
Type 3 | Flat destructive - villous atrophy (partial; subtotal; total) |
Type 4 | Atrophic hypoplastic (all components of small bowel mucosa involved) |
strict, life-long gluten-free diet
predni/AZA in acute flairs
→ see extra GI symptoms :
- Malabsorption symptoms:
- Vit deficiency → osteoporosis+ steatorrhea
- iron def. anemia,
- children: short, delayed puberty, failure to thrive
- Dermatologic: dermatitis herpetiformis
- Dental: Enemal hypoplasia
- Fertility porblems
- Gluten ataxia
- Lymphoma + AdenoCa
Whipples → check PCR + PAS positiv Macrophages → just give AB
undigested lactose (i.e)
→ ↑osmotic pressure → ↑ fluid secretion
→ ↑bacterial fermentation → ↑organic acids(↑osmotic drive) + ↑gases (bloating+flatulence)
⇒ ↑stool volume, ↑fluid → ↑motility+↑transit time → loose stool + malabsorption of fat
T.whipplei
Tropheryma whipplei
farmers + exposed to soil+animals
↓ability of Mp to degradate pathogenes or particles
diarrhea + steatorrhea
weight loss
CNS + cardiac problems
artralgia
- PCR postitive for T.Whipplei
- PAS-positive Mp 📷
AB-therapy for 1year
- abdominal pain (≥1x/week during previous 3month) associaten with ≥2 of the following
- change in stool frequ. + form
- Related to defacation (often reliefed)
- no organic cause
- IBS-D (diarrhea predominant)
- IBS-C (constipation predominant)
- IBS-M (mixed diarrhea and constipation)
- IBS-U (unclassified; symptoms cannot be categorized into one of the above three subtypes)
- CBC (anemia, inflammation)
- Metablic panel
- Stool examination (parasites, pathogens, leukos, toxins)
- Hydrogen breath test (excl. bacterial overgrowth + lactose+fructose intolerance)
- tTG-Ab + biopsy in IBS-D
- Thyoid markers
- Calcium (excl. HyperPth
- ESR + CRP
- antispasmotics
- anti-diarrheal
- anti-depressants + psychological therapy
- probiotics
< 3 stools passed / week
+/- other signs:
- Reduced quantity of stools
- Increased consistency of stools
- Difficult defecation
- Feeling of incomplete evacuation
type 1-3 📷
- Transport
- Hypotonia (i.e. diabetes, anticholinergics, ↓K)
- Hypertonia (spastic, i.e. vagal hypertonia)
- Evacuation mechanism
- Absent impulse for defecation (i.e. rectal dysmotility)
- Laxatives abuse → loss of defecation reflex
- Retention mechanism
- Megacolon
- Megarectum
- Obstructive mechanism
- Colorectal + Anal stenosis (i.e. Crohns, tumors)
- Hirschsprung's D (absent ganglions)
- Resudual deficit mechanism
- Diet: low fiber + rich refined carbs → reduced content → ↓movement stimulation
- Habitual aka primary idiopathic
- Symptomatic aka secondary
- elderly
- woman
- sedentarism
- diet (↓fiber, ↓liquids)
- Drugs (opiates, anticholinergics, antispastics)
- nervous + mucle dmg in colon +rectum
- Endocrine/metablic: Hypothyroidism, diabetes, ↓Ca, ↓K
- Neurologic: Hirschsprung; MS, parkinson
- Collagen disease, vasculitis, myopathy (i.e. scleroderma, dermatomyositis)
- lead intox
- reflex from distance (ulcer)
- Reduced Lumen: tumors, hemorrhoids, prolaps, IBD, diverticultis
- Inflammation: colitis, sigmoiditis, rectitis
- IBS
- Diverticulosis
- Anal fissures, hemorrhoids, prolapse
- occlusion (due to fecaloma in eldery)
- Abdominal hernias
- Endoscopy
- Radiology
- Measure colonic transit time
- Defecography (MRI)
- Anorectal manometry
- Diet + Lifestyle!!
- Laxatives (irritant, osmotic, bulk-forming, emollients)
- Prokinetics (Misoprostol)
- Prebiotics
- Surgery ( if obstruction)
🔥 Inflammatory bowel disease
10-15% of IBD = Ø criteria for UC/ CD
jews
20-40y
not really understood ⇒ combination of genetic, environmental + microbial factors
- Dysregulated and ↑immune response against commensal bacteria
- uncontrolled inflammation
- ↓suppression of inflamation
→ imbalance pro+ anti-inflammatory mediators
- Genetic: Chrons with NOD2 gene
- Pathogens (GI-pathogens i.e. Measles, Mycobacterium, Paramyxovirus)
- Stressors (Diet, smoking, AB, Drugs, stress)
active smoke → protective factor in UC
Chrohns → risk for disease + less responsive to treatment + more recurrence
UC - pANCA
Chrons - Anti-Saccharomyces cerevisiae (ASCA Ab)
- Anemia → iron, B12, Anemia of chronic disease
- Inflammatory
- Leukocytosis
- ↑CRP, ESR, Fibrinogen
- Thrombocytosis + Fibrinogen → Thrombosis
Endoscopy (or Endoscopic video capsules)
US
MRI + CT
Barium
3x
- Bloody diarrhea
- Abdominal pain ⇒ LLQ
- Abdominal cramp
- Extraintestinal
- low-grade fever
- Skin lesion (erythema nodusum + pyoderma gangrenosum)
- Uveitis
- Arthritis
- primary sclerosing cholangitis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
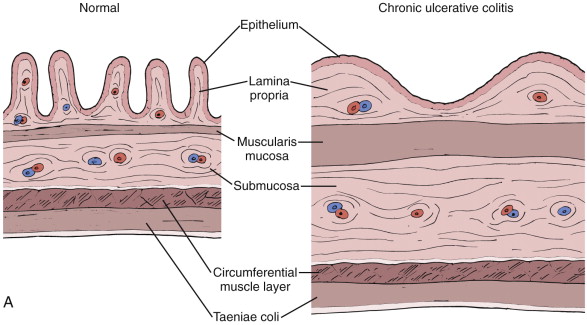
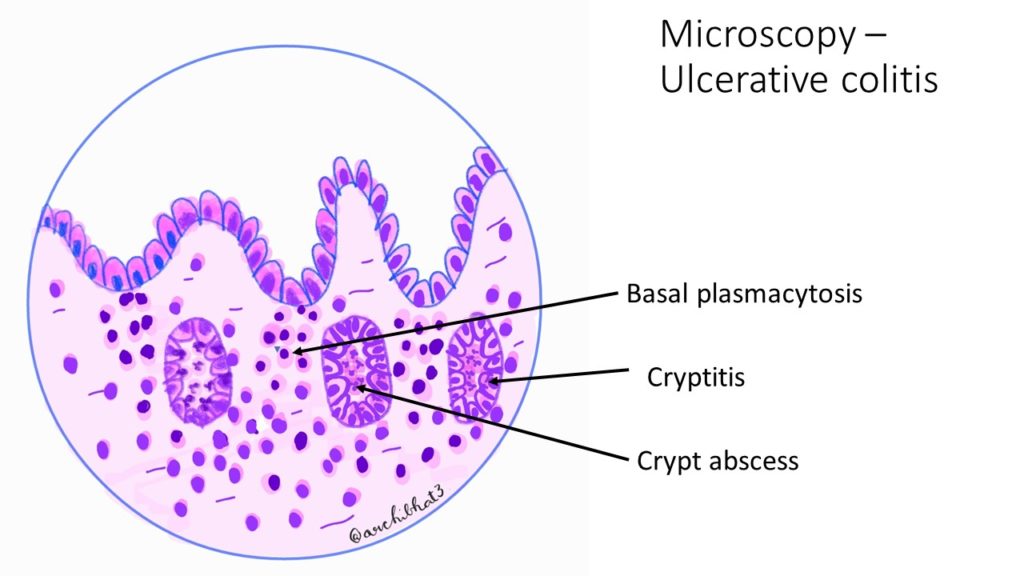
only mucosa + submucosa 📷
{kind=link}
{kind=link}
{kind=link}
- 🎱 Toxic megacolon
- 🩸sev. Hemorrhage (uncontrollabe)
- 🦀Colorectal cancer
- 🕸️Stricture
→ Sepsis
🌝Corticosteroids + 💊ABs
🔪surgery
C. difficile infection
"Lead pipe" appearance 📷
Involves rectum & Spares anus
Elective protocolectomy
- Diarrhea (non bloody - maybe occult)
- abdominal pain ⇒ often RLQ
- perianal skin patches + anal fistula or perianal abcess
- loss of weight
- →colicy + relieved by defacation
- Fever
- Rectal bleeding + Anal ulcer
- nausea, epigastric pain (in stricture)
anywhere in GI tract (Mouth to anus)
most often terminal ileum
transmural (all)
{kind=link}
{kind=link}
nope, recurrence after resection
cancer (colorectal + SMALL BOWEL)
fistulas
obstructing strictures
peri-anal abcess
unresponsive (refract)
- resection (to treat obstruction i.e.) → doesnt reduce recurrance risk!
- Strictureplasty 📷 → to treat obstructions esp.
🌝 steroids (budesonide or predni) + 🔰5ASA
Small bowel obstruction
(1) Bowel wall edema (2) "String sign"📷
{kind=link}
Incision & drainage (+ antibiotics)
Crohn's - occult blood UC - frank flood
Colovesical fistulas 📷
{kind=link}
Malabsorption
- Arthritis + Ankylosing spondlitis (back pain, does not parallel disease activity!)
- Erythema nodosum 📷 + pyoderma gangrenosum 📷
- PSC (primary sclerosing cholangitis) - esp UC
- Uveitis + Hyperemia of Sclera + conjunctiva (parallels D activity)
- kidney stones
- Gall stones
- ↑LFT (due to PSC, malnurtrition, sepsis)
- Venous thrombosis
- Angular cheilitis - esp Crohns due to iron def
- Mouth ulcer - crohns
CD
Crohns
CD
Crohns
Crohns
Crohns
UC
Crohns associated with recurrance
UC
Crohns
{kind=link}
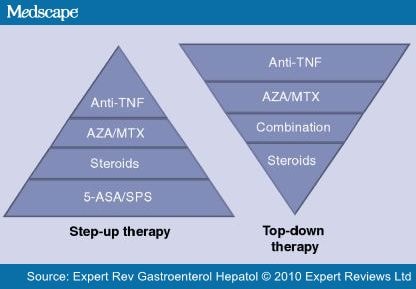
- 5-ASA (amnisalicylate aka mesalazine)
- steroids (prednisone, budesonide, hydrocortisone)
- Immunosuppressants (AZA,MTX)
- Biologicals (infliximab, natalizumab, ustekinumab)
in ACTIVE UC/Crohn’s:
- 5-ASA
- +- steroids (predni in UC, bude in Crohns)
- +- biological (#1 Infliximab in both; natalizumab & ustekinumab: alternative in crohns)
- +- Immunosuppressants (Cyclosporin in UC, MTX in Crohns)
- +- AB (in crohns, Øin UC)
in MAINTENANCE UC/Crohn’s:
- 5-ASA
- +- infliximab
- +- Immunosuppressant (#1 AZA in both; MTX: alternative in crohn’s)
Every 1-2years after 10years
Every year after 20y
🩸 Upper and Lower GI Bleeding
Stool guaiac test
slow pace - low volume bleeding
UPPER GI
(but can also be small intestine/colon if slow pace)
colonic origin
also UGI with large volume or high pace
might be bright or dark
- Peptic ulcer
- Gastroesophageal varices
- Erosive esophagitis/gastritis/duodenitis
- Neoplasm
- Aortoenteric fistula (rare, cant afford to miss!)
- Mallory weiss tear
- Dieulafoy's lesion
- Vascular ectasia
- Diverticulosis
- IBD
- neoplasm
- infectious or ischemic colitis
- hemorrhoids
- post-polypectomy
- Angioectasis
- Dieulafoy
- prior GI + or family history
- NSAIDs
- Liver disease
- Vascular disease
- Radiation exposure
- Vitals (ABC) ⇒ early fluid resucitation reduced mortality!!!!
- Abdominal tenderness
- Rectal examination
- description of blood
- masses / hemorrhoids
- Skin + oral (hereditary hemorrhagic telangiectasis)
an acute GIB
- Age <50
- Melena
- BUN/CREA ration ≥ 30! (blood gets reabsorbed → ↑urea)
- DD Hematochezia from UGIB vs LGIB → aspiration
- Coffee grounds bleeding (less severe/inactive bleeding)
- negative aspirate is not helpful: 20% with neg. aspirate have UGIB!
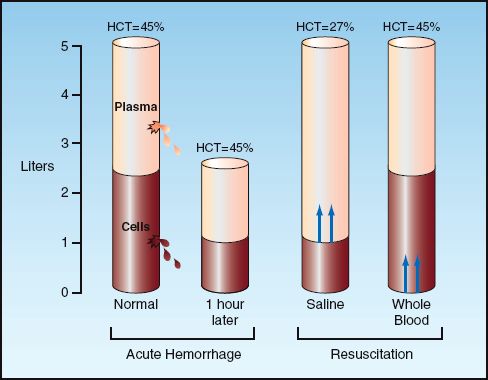
NO, initial Hct can be misleading → Hct stays the same with loss of whole blood (until re-equilibration) 📷
{kind=link}
≤7
Weigh risks / benefits of reversing anticoagulation (Assess degree of coagulopathy) → Vitamin K - slow acting, long-halflife → FFP - fast acting, short-halflife → RBC transfusion
Predictors of mortality in UGIB:
rockall scoring system: 📷
{kind=link}
{kind=link}
low risk UGIB will not likely requre endoscopic hemostasis
- Facilitate clot formation (i.e. VitK, FFP)
- PPI
- dg
- risk stratification
- hemostasis therapy
- endoscopic stigmata (high bleeding risk or active bleeding)
- recent hemorrhage
!80% resolve spontanously
{kind=link}
low rebleeding-bleeding rates
Flat pigmented IIc
Clean base III
- inject Epinephrin
- Thermal electrocoagulation
- Hemoclips
!combined therapy superior to mono-T
- low risk: oral PPI + fed
- Endoscopic therapy: PPI infusion for 72h
- Determine HP status
restart aspirin as soon as bleeding resolved
(not dying = more important than rebleeding)
high
- Severity of liver D → child pugh score
- ↓Platelets <88k
- Splenomegaly
- Platelet count/Spleen diameter(mm) ratio <909
"variceal"
Vasoconstrictor therapy*
Antibiotics*
Resuscitation*
ICU
Endoscopy*
ALternative aka rescue therapies (TIPS)*
Betablocker*
Reduce splanchnic blood flow
→ Terlipressin
→ Somatostatin
→ Octreotide
Bacterial infection: in 66% of patients with cirrhosis and variceal bleed → Prophylactic antibiotics → decr. incidence of bacterial infection
⇒ significantly reduces early rebleeding
Ceftriaxone IV Alt: Norfloxacin po
excessive fluid → ↑↑portal pressure → ↑↑bleeding
asap after resuscitation (withing 12h)
⇒ Band ligation 📺
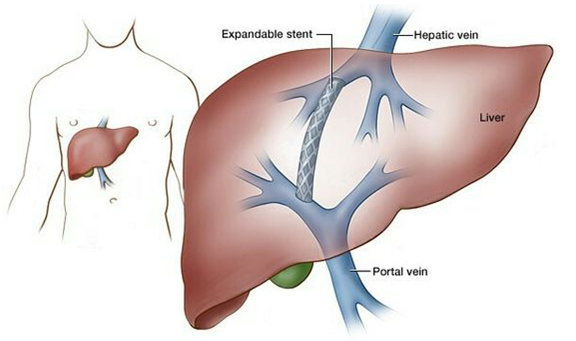
TIPS (Transjugular intrahepatic portosystemic shunt) 📷
{kind=link}
esp in high risk patients → within 24-72h
esp. in gastric variceal bleeding
Sengstaken-Blakemore Tube 📷
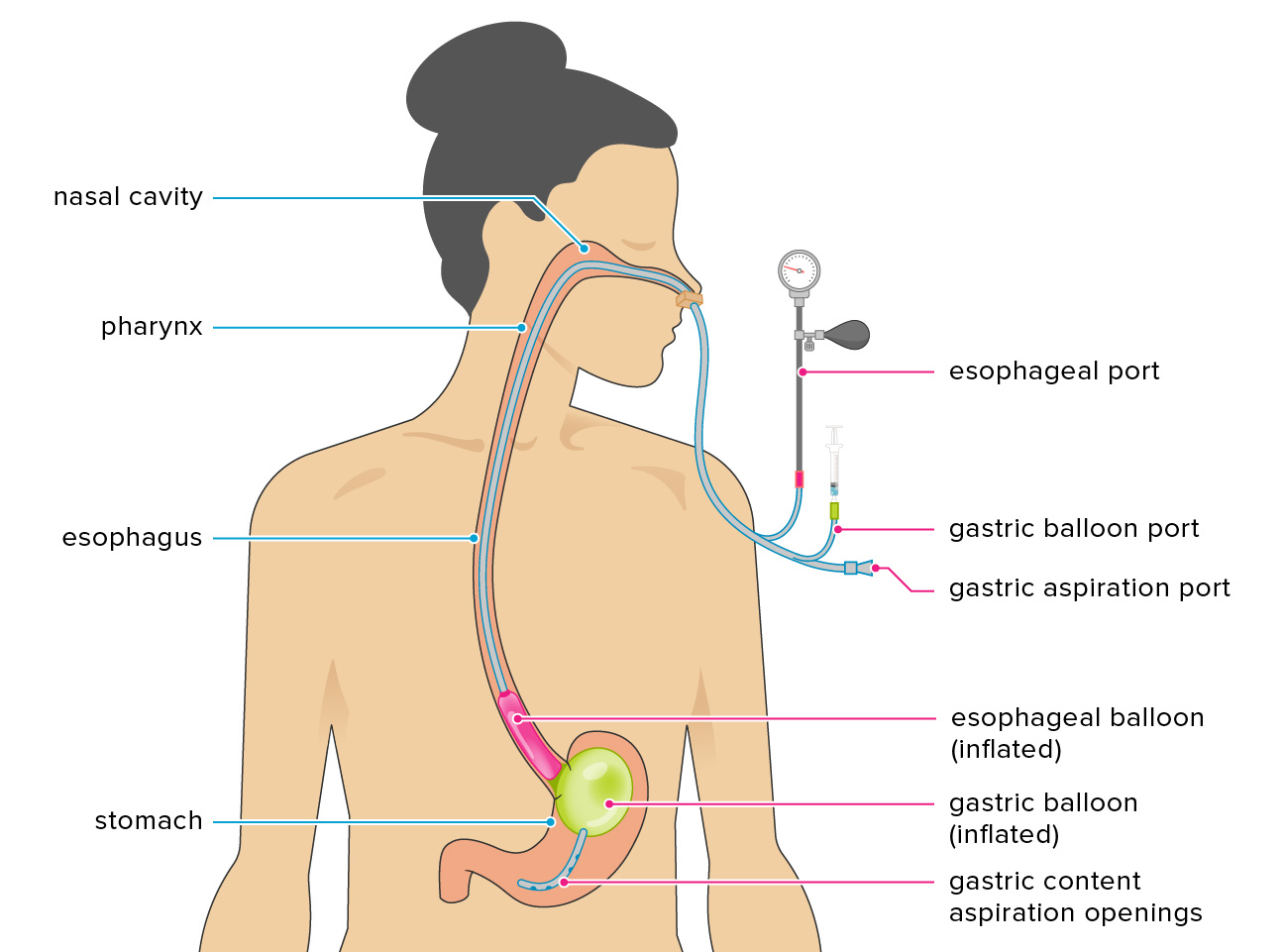{kind=link}
→ compression gastric variceals
!but only temporary → high complication rate (aspiration, necrosis, perforation)
!airway protection needed!
Self expanding metal stent 📷
{kind=link}
after acute bleeding resolved
→ ↓splanchnic vasoconstriction + ↓cardiac outbut → ↓risk for recurrent hemorrhage
Colorectum
UGIB
10-15% of patients with presumed LGIB actually have upper GIB in the end
Diverticulosis
Div: large volume, painless
collitis: small valume, pain, diarrhea
- Hemodynamic unstable: HR>100, SBP<115, Syncope (each counts 1 factor)
- nontender abdomen
- aspirin use
- >2 active comorbiditis
- bleeding during first 4h of evaluation
⇒ Interpretation:
- 0 factors: ~6% risk
- 1-3 factors: ~40%
- >3 factors: ~80%
- age
- intestinal ischemia
- comorbiditis
- secondary bleeding
- coagulopathy
- hypovolemia
- transfusion required
- male
true, 80% (like UGIB)
6-12h
similiar UGIB → identify stigma → therapy
- colonoscopy after resolution of bleeding + bowel prep
- angiography in massive bleeding
rapid "purpe" preg aka bowel prep → colonoscopy within 1h after clearance
- cant be stabilized
- cant be prepped for bowel
- had colonoscopy but failure to localize/treat bleeding
- localize active bleeding
- hemodynamically stable patient
- might be used with tagged RBC scan
- others failed
- Shock/Hypotension
- >6U PRBCs transfused
🍄 Diverticulosis, Polyposis and Colo-Rectal Cancer
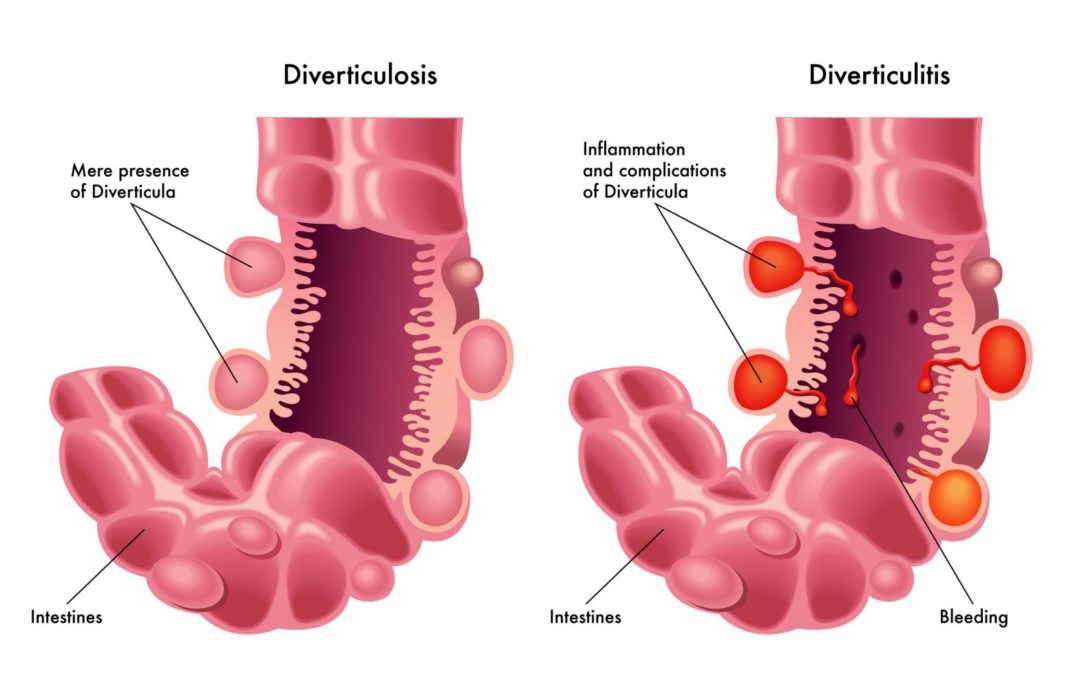
Mucosal and submucosal herniation: Abnormal protrusion of the mucosal and submucosal layers of the intestinal wall → Passing through the muscular layer of the intestinal wall. 📷
{kind=link}
desc. colon + sigma
- Strength of intestinal wall
- Pressure gradient between the colonic lumen and the peritoneal cavity.
- Advanced age
- Constipation
- Increased consumption of meat + other Western diet (low intake of fiber)
- Obesity, sedentary lifestyle
{kind=link}
- asymptomatic
- pain - left iliac fossa
- bloating (defecation favors)
- incomplete evacuation sensation
- constipation / diarrhea
- mucus
- rope sign
- Colonoscopy
- CT
- US
- Abdominal radiography: Barium enema 📷
- inflammation → diverticulitis
- perforation → peritonitis
- fistulas*: colo-vesical, colo-vaginal
- stenosis*
- hemorrhage
- complication treatment
- diet rich in fibers
- laxatives
- antispasmodics
- probiotics
proliferation of mucosa → small, well-circumscribed mass protrude into lumen
{kind=link}
{kind=link}
left colon
Adenomas = Adenomatous polyps 📷 ⇒ Adenocarcinoma
{kind=link}
Genetic + male, age, obesity, smoking
- fettes schwen (high fat diet, obesity, ↓exercise, ↓fiber-diet)
- smoking + alkohol
{kind=link}
villous + serrated(high risk not be detected)
tubular (75%)
young - distal colon
elderly - proximal colon
- most asymptomatic
- bleeding (Hemotochezia+melena) → evtl. iron def. anemia
- diarrhea or consitpation

#1 Endoscopic polypectomy 📷
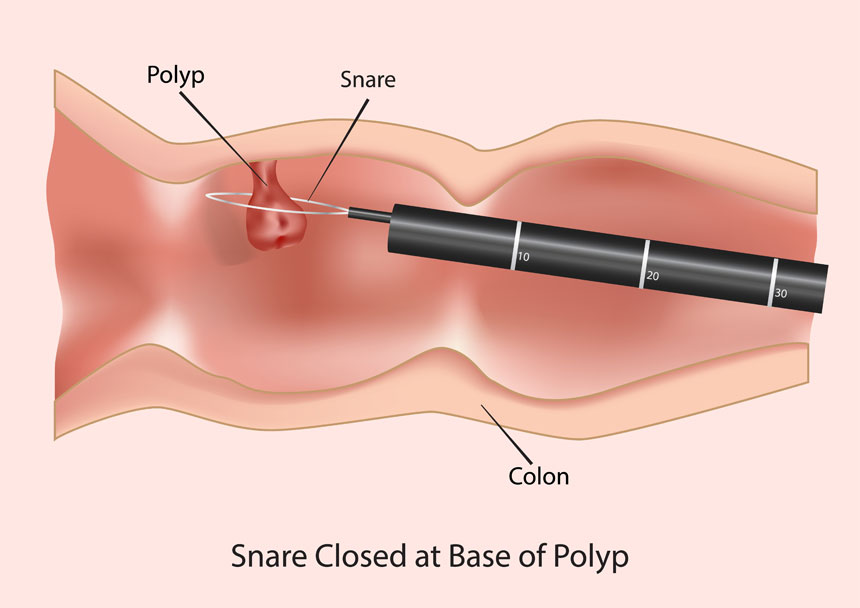{kind=link}
alternatives: mucosectomy or endoscopic submucosal dissection
Surgery (open)
- small <5mm
- no cellular atypia
- no malignancy risk
hyperplastic + adenomatous polyps
high malignancy risk
juvenile aka retention polyps → excess lamina propria
Poly peutz yegers → SM network, normal lamina propria
Inflammatory polyps → granulatuion tissue, in chronic inflammatory D
- Familiar adenomatous polyposis
- Peutz-Jeghers synd → also perioral hyperpigentation + extraintestinal malignancy
- Colon+Rectum - 95% malignancy
- Gastric - no malignancy
- Duodenal - 60-90% malignancy
- duodenal carcinoma (periamullary)
- jejunal + ileal adenoma (rare carcinomas)
- Hypertrophy of retinal pigmented epithelium
- Cancer in Thyroid, liver, bilary tree, pancreas, CNS, adrenals
- proctocolectomy → ileo-anal anastomosis or ileostomy
- subtotal colectomy → ileo-rectoanastomosis
- endoscopic polypectomy
- surgical resection
- NSAID → regression
90% if dg early → screening!
bullshit environmental factors (diet, smoking, alk, microbiotic flora)
→ eat your fucking fibers
IBDs, herditary non-polyposis colorectal cancer (HNPCC), FAP
⇒ 📷
>96%!
- polypoid (exophytic)
- ulcerated infiltration
- stenosis
- Epithelial cell hyperproliferation
- Aberrant crypts
- Small tubular adenoma with mild dysplasia
- Large, (tubulo)villous adenoma, high dysplasia
- Cancer
before splenic flexure 📷
{kind=link}
50y
beginning at 50y:
- colonoscopy → every 10y
- flexible sigmoidoscopy every 5 years
- combined annular iFOBT + sigmoidscopy 5y
- occult blood test annually
- If high risk (i.e. familiar risk) → 10 years earlier than dg auf relative → 5 year recurrance
FAP → starting from 10y old ⇒ sigmoidscopy every year!
HNPCC → 20-25y old ⇒ colonoscopy every 1-2y
after 8y of evolution - every year
- polyp>1cm
- multiple adenomatous polys >3
- high grade dysplasia
every 3-6 month!
{kind=link}
{kind=link}
→ still long time asymptomatic
→ pain
→ blood loss
→ diarrhea / constipation
→ change in stool appearance
→ weight-loss + asthenia + fever (alarm symptom)
Feature | Ascending colon | Transverse | Sigm+descending | Rectal cancer |
Anemia | x | x | ||
Hematochezia | x | x | x | |
Pain | RUQ | Epigastric+periumbilical | when defacating | |
Fever | x | |||
Weight loss | x | |||
Subocclusion synd | +/- | x | x | x |
Diarrhea/Constipation | x | x | ||
Appearance change | pencil-stool | x | ||
Perforations | x | x | ||
Fistulas | ||||
Tenesmus | x |
- #1 surgery → removal of segment, peritumoral lymph, liver mets, screening!
- chemo
- radio
🍑 Liver Pathologies
- hepatomegaly
- splenomegaly
- jaundice
- ascitis
- varices
- ↑AST+ALT
- ↑Bili
- Cholestasis marker
- ↓Thrombos

- history or signs of liver disease
- Heartfailure/COPD symptoms+signs
- alcohol/drug history
- symptoms of infection
- history or signs of malignancy (spread)
- weight loss/anorexia
- sexual contact/blood transfusion/tattoos
- Hemolysis / hemolytic anemia
- Massive hematomas
- Spherocytosis

- deficit in conjugation
- hepatocyte destruction
- failure in excretion
- Conjugation: Neonatal, Gilbert, Cringler-Najjar
- Destruction: acute + chronic liver D
- Excretion: acute Hep, primary biliary cholangitis, sepsis, Dubin-johnson
- pancreas Ca
- Cholangio carcinoma

- chole(doco)lithiasis

- Ampulloma
→ less bile salts
- Steatorrhea (+pale stools)→ malnutrition, diarrhea, ↑cholesterol
- Vit ADEK def
- vision
- osteomalaciy
- muscular asthenia
- coagulation
- onset → progressive vs sudden
- pain
- medication / alcohol
- fever + weight loss
dark urine + pale stool
Courvoisier's sign:
- palpable enlarged gallbladder
- mild jaundice
⇒ cause is unlikely gallstones → 🦀 gallbladder / pancreas malignancy!
- Bili (conj+unconj)
- Cholestasis marker (ALP + GGT)
- ALT + AST (hepatocytolysis synd?)
- CBC: RBC, Leukos, Coagulation!
- Cholesterol (↑in cholestasis)
US → DD intra- vs extra-hepatic
more sensitive in:
- bile duct obstruction
- small pancreatic cancer
→ biopsy possible
{kind=link}
{kind=link}
check the liver!

evaluation hepatic + pancreatic tumor
Pre: Portal vein thrombosis
Hepatic: Cirrhosis
Post-hepatic: Budd-Chiari syd (obstruct. of venous outflow) + RHF

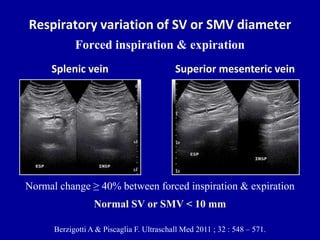
- Change in diameter + ↓flow velocity +- portal flow reversal = Pathognomonic
- backflow changes
- ↑SMV + ↑SV + collaterals
- spleen size (10-12mm=normal)
- ascites
40% 📷
{kind=link}
lack of respiratory variation!
↑resistance by liver + porto-systemic shunt → ↓Velocity
portal flow reversal 📷
{kind=link}
large collateral vessel
- para-umbilical
- spleno-renal
- hemorrhoids
{kind=link}
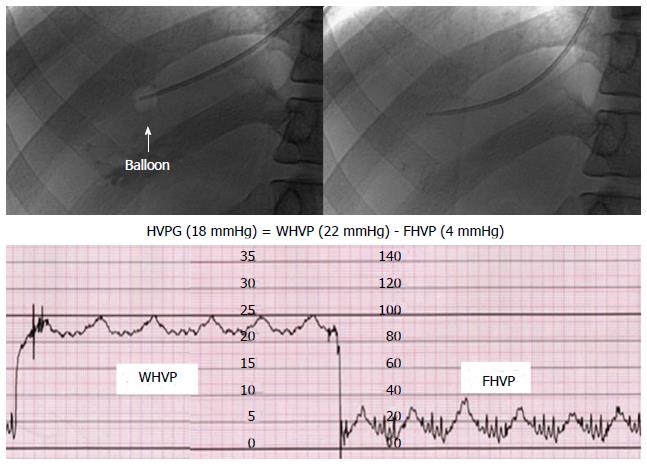
HVPG (hepatic venous pressure gradient) ≥ 5mmHg = portal HT → if >10mmHg = clinically significant portal HT
HVPG = gradient betw. WHVP + FHPV = pressure gradient PV+IVC
WHVP = wedged hepatic venous pressure ⇒ hepatic sinusoidal pressure → 📷 catheter in hepatic vein → occludes it → measure proximal stasis blood flow (reflective of pressure in sinusoids)
{kind=link}
FHPV = free hepatic venous pressure
- hypercoagulability state
- myeloprolif neoplasm
- defic. in endogenous anticoagulants (protein C+s, antithrombin III)
- idiopathic
- local
- inflammation
- pancreatitis
- hypercoagulability
- esp due myeloproliferative neoplasms,
- endogenous anti-coagulants def
- local: secondary budd chiari → tumors or hepatic cysts
- idiopathic
Anticoagulant
→ 3-6 month in local + idiopathic
→ unlimited in hypercoagulability
- 🍑Liver disease (acute + chronic)
- Cirrhosis
- Alcoholic hepatitis
- Acute liver failure
- budd-chiari
- cancer
- ❤️HF
- 🦀Cancer (liver, peritoneal)
- 🥐 Nephrotic syd
- 🦐 Pancreatitis
- PARACENTESIS!!
- Cell count + DDs specific
- Albumin + proteins total
- Culture
>1 g/L ⇒ Portal HT related
- Cirrhosis/severe hepatitis
- Chronic hepatic congestion (right heart failure, Budd-Chiari)
- Massive liver metastases
- Myxedema
<1 g/L ⇒ Non-Portal hypertension related
- Peritoneal carcinomatosis
- TB
- Pancreatic disease
- Serositis
- Nephrotic syndrome
- salt restriction (no added salt, avoidance of pre-prept food) ⇒ 90mmol Na / day (<2g/day)
- Diuretics (esp. Furosomide-Spironolactone-combination)
- Therapeutic paracentesis: Use intravenous albumin paracentesis.
- TIPS: Consider in appropriate patients with no contraindications, as it may provide a transplant-free survival advantage.
- Liver transplantation: Should be considered in every case, as the development of ascites in patients with cirrhosis is associated with a 50% 2-year mortality.
During the procedure, a large volume of fluid is removed from the abdominal cavity using a needle and catheter, and it is replaced with an equal volume of intravenous albumin solution. This helps to prevent complications such as hypovolemia and electrolyte imbalances. The procedure is typically performed under sterile conditions and with the guidance of ultrasound or other imaging techniques.
Also Na excretion! → 24h urinary Na excretion
if random urina Na/K ration >1 ⇒ >78mmol/day excretion
- ↑AST+ALT
- Jaundice
- INR > 1.5
- Encephalopathy
- no chronic liver disease
- Encephalopathy?
- Transjugular liver biopsy → exclude cirrhosis, alcohol-induced, malignancy
- Contraindications for emergency transplant?
- Viral (Hepatitis, CMV, HSV, Dengue) ⇒ inflammatory markers
- Wilson → young, hemolytic anemia, ↑bili/ALP ratio, kayser-fleischer, ↑copper
- Autoimmune → ↑↑ALT+AST, antibodies, histology!
- Malignancy ⇒ history, ↑ALP, tumor markers
- Drugs/Toxins:
- Paracetamol → ↑↑↑AST+ALT, ↓bili, RF+Acidosis
- Chemo, Anti-TBCs
- Vascular:
- Budd Chiari → pain, ascitis+hepatomegaly, loss of portal flow on US
- Ischemia (hypoxic hepatitis)⇒ ↑↑↑AST+ALT, ↑LDH, ↑Crea
- Pregnancy? → HELLP, Fatty liver of the pregnancy, Pre-eclamptic rupture
- Alcohol abuse
- Viral hepatitis
- Acute bacterial infection
- GI bleeding
- iatrogenic: TIPS + Large-volume paracentesis
- 40%→no identifiable precipitating factor
- Acute decompensation of cirrhosis (ascitis, encephalopathy, GI bleeding, bacterial infection)
- high short term mortality ≥15%
- Organ failure → defined by SOFA score ⇒ Clif-sofa-score
⇒ ACLF 1: single organ failure
⇒ ACLF 2: 2 organ failure
⇒ ACLF 3: 3 organ failures
53%
35%
cell injury + inflammation
>6month
- Hepatocyte lesion
- Balooning degeneration
- Necrosis
- interface necrosis/hepatitis
- lobular
- bridging necrosis
- Regeneration
- Inflammatory cells in portal + intralobular space
- Bile duct injury
- Fibrosis
- Portal
- Central
- Perisinusoidal
{kind=link}
{kind=link}
{kind=link}
- spotty hepatocyte necrosis
- Apoptotic hepatocytes on periportal areas → monoculear cells around
progressive fibrosis Limiting plates → enlarged portal tracts → fibrous extension → portal-portal or portal-central fibrous bridging
{kind=link}
30-60d
areas where HepB is common: birth, blood during childhood
areas where HepB is uncommen: i.v. drugs, sex
healthcare worker: blood transfusion, dialysis
⇒ transmission only via blood or body fluids
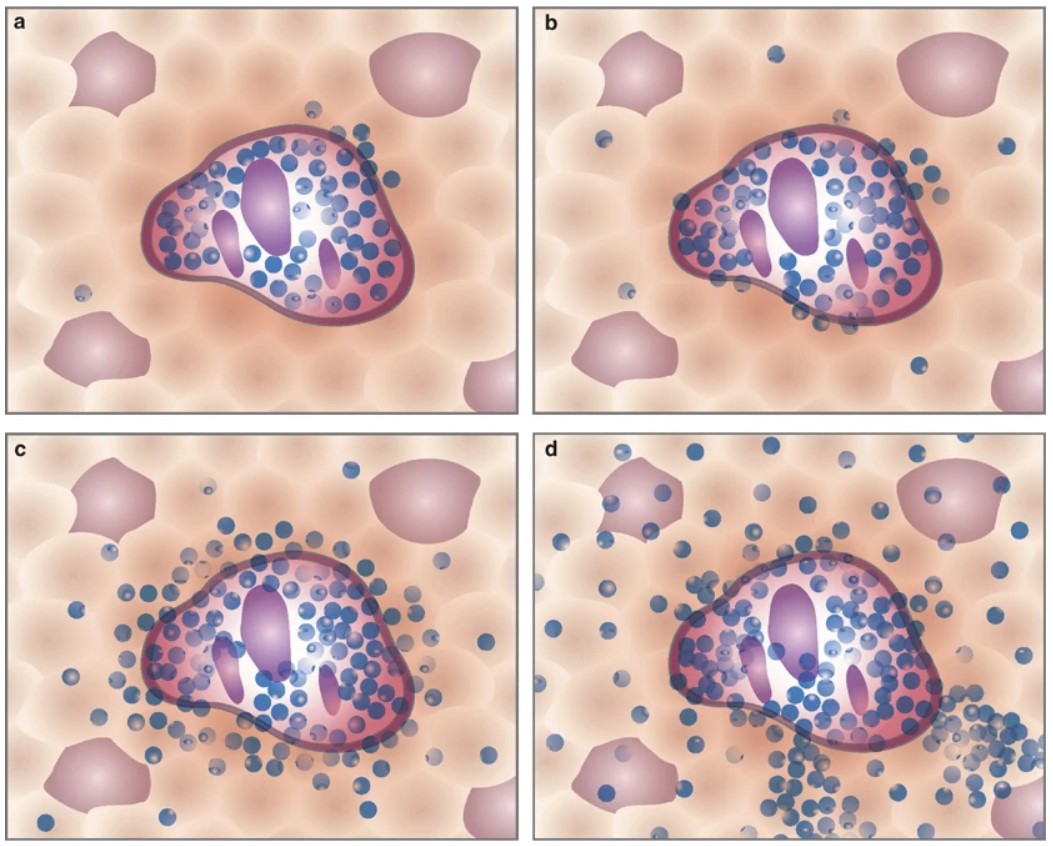
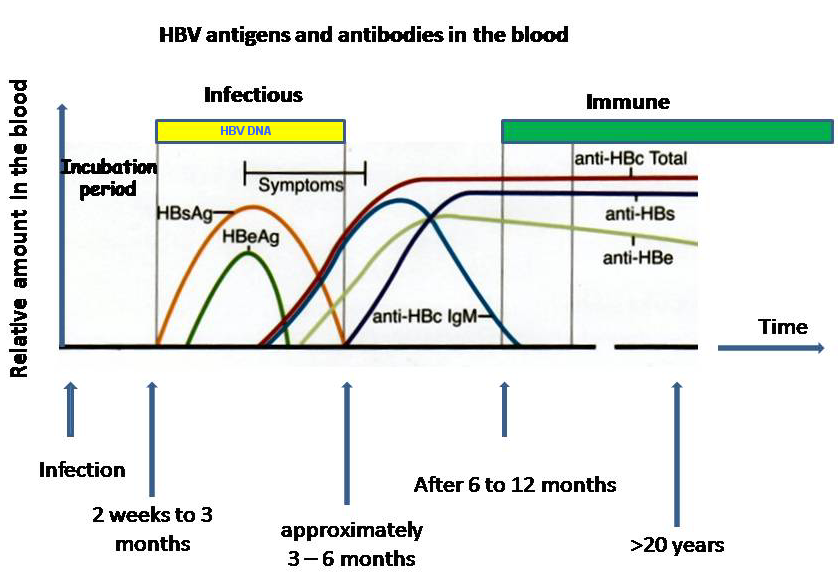
HBs → in the blood, presence of infection, first detectable Ag
Hbc → not in blood
Hbe → shortly after Hbs, ↑viral replication + ↑infectivity
{kind=link}

immune reaction → cytotoxic T lymphocytes
- Hbe +; chronic HBV infection
- Hbe+; chronic HepB
- Hbe -; chronic HBV infection: inactive carrier!
- Hbe-; chronic HepB
- Hbe-; Resolved HBV infection
1-4
1+2
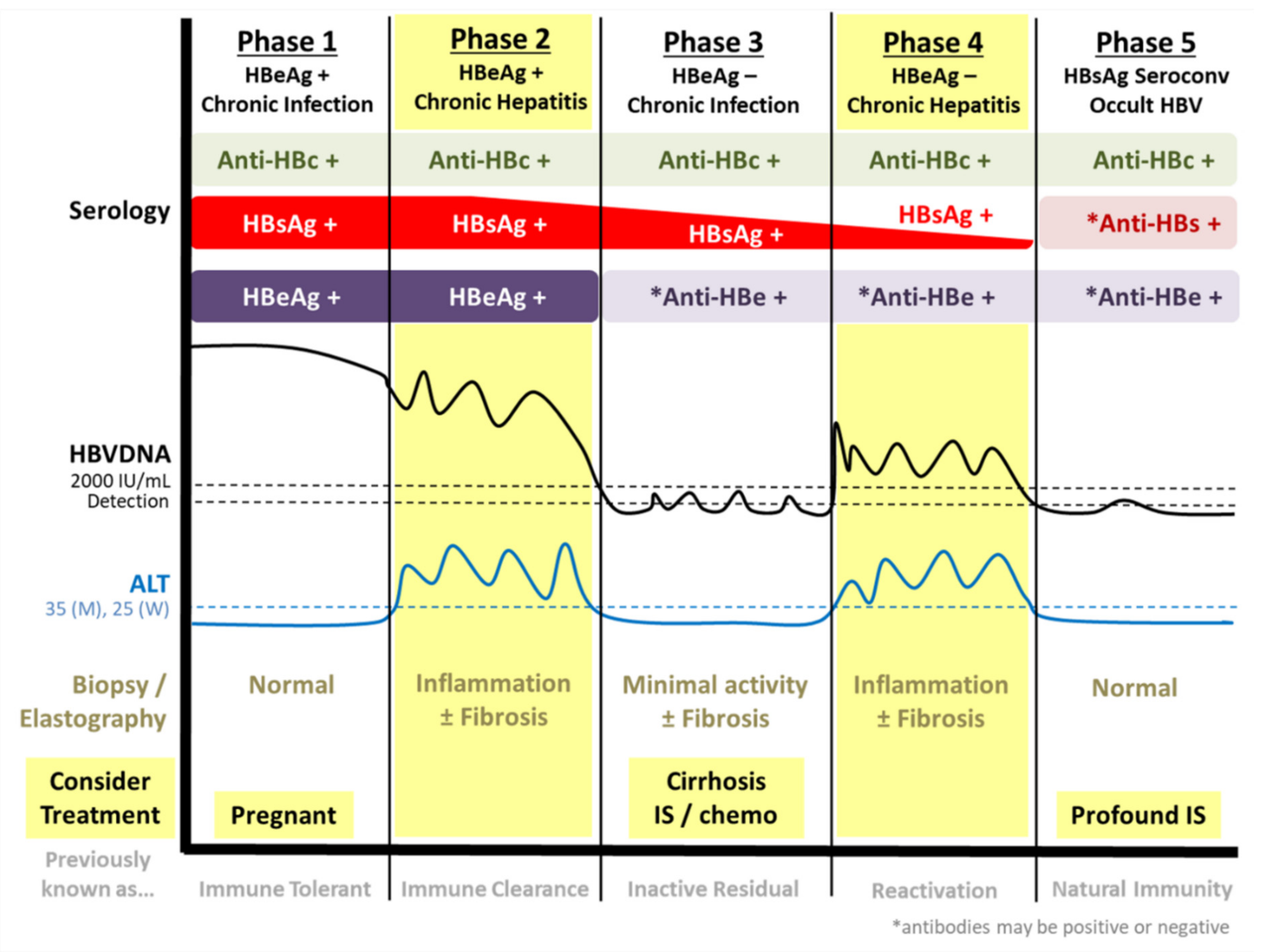{kind=link}
2+4
→ !necroinflammation + fibrosis on biopsy!
2+4
{kind=link}
immune patients, resolved disease
either after natural infection or vaccination
Immune due to natural infection | HBsAG (-)
Total anti-Hc (+)
anti-HBs (+) |
Immune due to vaccination | HBsAG (-)
Total anti-Hc (-)
anti-HBs (+) |
Acute | HBsAg (+)
Total anti-HBc (+)
IgM anti-HBc (+)
anti-HB (-) |
Chronic | HBsAg (+)
Total anti-HBc (+)
IgM anti-HBc (-)
anti-HB (-) |
2+4! when AST is incr + active inflammation
fibroscan (elastography)
- PegIFNalpha
- Entecavir
- Telbivudin
- Tenofovir
- Adefovir
- Lamivudin
- simultanous infection with HepB (coninfection)
- or superimposed in chronic HepB or HepB carrier (superinfection)
- liver failure
- liver cancer
- liver cirrhosis
👍🏿
SUPERinfection
(rarely in coinfection)
- Anti-HD AB (igm + igg)
- Immunohistochemical staining → HD-Ag
- PCR → RNA-HDV
- vaccine!!! against HepB
- pegIFNalpha
- myrcludex B

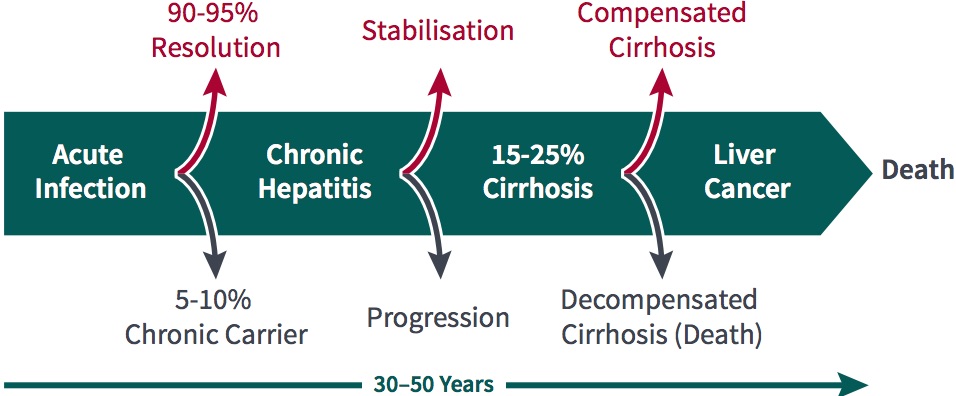
80%
false: NO digestive symptoms
“Early on chronic infection typically has no digestive symptoms - arthralgias, paresthesias, myalgias, pruritus, sicca syndrome, sensory neuropathy”
lymphocytes
7
T
- blood-blood: i.v. drugs, medical equipment, needle sticks
- during birth
joiint, muscle +skin
- Arthralgias + Myalgias
- Pruritus
- Paresthesias
- Sicca synd

- hepatic encephalopathy
- Portal HT
- ascitis
- varcieal bleeding
- Porphyria cutanea tarda

- Glomerulonephritis (membranoprolif)
- thrombocytopenic purpura
- Raynauds
- cryoglobulinemia
- etc.
- CBC Leukos
- AST+ALT
- check necro-inflammation activity (biopsy) + fibrosis (fibrotest)
- HCV genotyping! + quantitative RNA assay
- screen for coinfection with HIV+HBV
- screen for alcohol + drug abuse
- extrahepatic manifestations (see before)
- Rapid development to fibrosis + cirrhosis
- ↑risk for LF, HCC + mortality
- avoid toxic drugs + alcohol
- vaccination HepA+B
- US surveillance (for HCC) if cirrhosis
not at high risk of dying from other causes.
Genotype + Cirrhosis(+/-)
NS5B polymerase inhibitors
NS5A protease inhibitors
NS3 protease inhibitors
Sofosbuvir + valpatasvir
12w
1+4
renal impairment
not in decomp cirrhosis!!
- unknown causes (might be triggered by virus or drug)
- like viral hep
- continuing hepatocellular inflammation + necrosis
- tends to progress to cirrhosis
- +- associated with other AI disease
↓
🍑 variable liver presentation
- most patient: insidous onset
- non-specific: fatigue, anorexia etc
- insidious to fulmunent
- cirrhosis + hepatic failure
🐉 Extra-hepatic autoimmune signs of:
→ i.e. arthritis, vasculitis, nephritis, Coombs, anemia, rash, thyroiditis
⭐to sum it up ⇒ classic symptoms of ↑toxins + PHT
- URQ discomfort
- mild pruritus
- anoxrexia
- myalgia
Classics:
- Hepatomegaly
- jaundice
- Splenomegly
- Spider angioma
- Ascitis
- Encephalopathy
- ↑AST+ALT
- ↑ALP + ↑Bili
- ↑IgG (and other IgGs)
- Antibodies
- antinuclear Ab (ANAs)
- Smooth muscl Ab (SMAs,)
- Liver-kidney microsomal type 1 Ab (LKM1)
- anti-liver cytosol 1 Ab (Anti-LC1)
- anti-soluble liver antigen (anti-SLA)
Lick my 1 (LKM1) anus (ANA) smoothly (SMA) + lick 1 (LC1) slowly (SLA)
{kind=link}
{kind=link}
→ evaluates Ab, IgG, histology, presence of viral hepatitis
- active disease
- advanced fibrosis/cirrhosis
Initially Predni → AZA/6-MP (maintaince) → evtl. stop AZA when remission archieved → if relapse start again with predni 🔁
⇒ many require lifelong immunosuppressive therapy and cant stop AZA
Test for thipurine methyltransfere (TPMT) deficiency!!
→ ↑toxcicity
- normal AST+ALT
- normal IgG
after 2nd relapse → predni or AZA, evtl. liver transplant
every 3month for 1 year → then every 6month
primary biliary cirrhosis
cirrhosis only in late stage!!
woman
cholestasis
biliary epithelial cells
Pruritus, Fatique, RUQ-pain
early → normal
advanced:
- Hepatomegaly + Splenomegaly
- Hyperpigmentation
- Jaundice
- Xanthomas + Xanthelasmas
Sicca syd.: Dry eye + mouth
also might occur in HepB + C
- ALP + GGT
- ALT + AST
- Cholesterol
- cirrhosis progression → ↑Bili, ↑PT, ↓albumin
- portal HT → Thrombocytopenia
- IgM (! compare IgG in AI)
- HDL
AMA - antimitochondrial antibody → in 95% with PBC, very specific!!
ANA - 20-50%
(notice AI hepatitis → SMA + PBC → AMA)
= autoimmune cholangitis
- Ursodeoxycholic acid
- Corticosteroids+immunisupressive, MTX, Cyclosporin → might improve biochemical + histological findings
- Antihistamines, Cholestyramin → pruritus treatment
- Plasmapheresis
Liver transplant
- NAFL
- NASH
- HCC
- AFLD
- Drug-induced fatty liver disease
- HCV-associated fatty liver
= secondary NAFLD
- pure steatosis
- Steatosis + mild lobular inflammation
{kind=link}
→ Fibrotic NASH → Cirrhosis → HCC
(Steatosis → ROS → lipid peroxidation → hepatocyte necrosis → stellate cells: fibrosis/cirrhosis)
obesity + DM2 - metabolic syndrome
F → multiple organs likely to be involved (adipose tissue, pancreas, gut, liver)
T
T
Associated with:
- Severity of NAFLD progression to NASH
- Presence of advanced fibrosis
- Development of HCC (Hepatocellular Carcinoma)
- patients with Insulin-Resistance + metabolic synd
- also vice versa!! (pat. with NAFLD → screen for metabolic synd
secondary causes + alcohol intake
US
Fibrotest + elastography (fibroscan)
T
Liver biopsy
→ essential for Dg!
NASH = Steatosis + Hepatocyte ballooning + lobular/portal inflammation
NAFL = Steatosis + ONE lobular/portal inflammation OR hepatocyte balloning
{kind=link}
Check liver enzymes: if normal → follow up in 3-5y (US + liver enzymes)
Serum fibrotests

slowly
CVD!
“Screening of the cardiovascular system is mandatory in all individuals with NAFLD because CV complications frequently dictate the outcome”
Lifestyle & Diet
- Energy restriction: Implement calorie restriction of 500-1,000 calories per day.
- Weight loss target: Aim for a 7-10% reduction in body weight.
- Long-term maintenance approach: Adopt a strategy to sustain weight loss in the long run.
- Fructose intake: Avoid consuming foods and drinks that contain fructose.
- Alcohol intake: Limit daily alcohol consumption to below 30 grams for men and 20 grams for women.
- Macronutrient composition: Opt for low-to-moderate fat and moderate-to-high carbohydrate diets. Consider low-carbohydrate ketogenic diets or high-protein diets.
- Physical activity: Engage in 150-200 minutes per week of moderate-intensity exercise in 3-5 sessions. Include resistance training to improve musculoskeletal fitness and metabolic factors.
- Coffee consumption: No restrictions for liver health.👍🏽
none 🤡
off label:
- Antioxidants (vit E)
- Lipid-lowering agents
Bariatric surgery
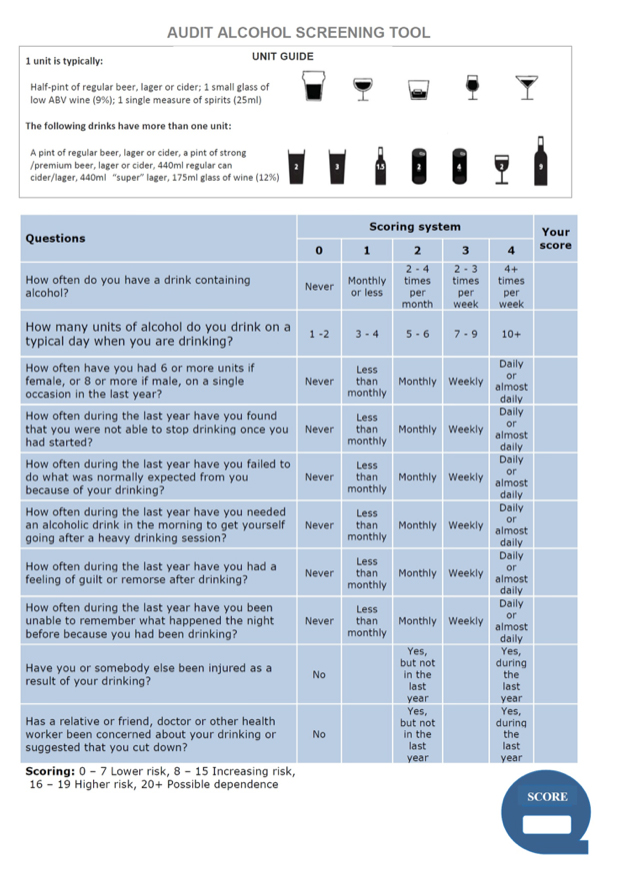
≥2 woman
≥ 3 men
men: 15 standard drinks/week or > 5 on occasion
women: 8 standard drinks/week or > 5 on occasion
AUDIT 📷
{kind=link}
Steatohepatitis → Cirrhosis (incl. decompesantions)→ HCC
- comorbidities
- obesity + metabolic syndrome🐷
- chronic viral Hep 🦠
- Alcohol 🍺
- genetics 🧬
- bilater parotid hypertrophy

- muscle wasting + malnutrition
- Dupuytren's signs 📷

- symmetric periph neuropathy

- gynecomastia

- spider angiomas
- ↑GGT
- ↑AST + ALT
- AST/ALT ratio >1

- ↑MCV

US → steatosis, cirrhosis, portal HT
Elastography (aka Fibroscan) >13.1kPa → cirrhosis
Fibrotest, ASH test (see biochem)
Maddrey → Bili + INR
⇒ Suggests which patients with alcoholic hepatitis may have a poor prognosis and benefit from steroid administration.
Lille → Bili, INR, Renal markers, Age, Albumin, Change in bili from day 0-7 ⇒assesses response to steroids
Score | Bilirubin | PT/INR | Creatinine/Urea | Leucocytes | Age | Albumin | Change in Bilirubin from Day 0 to 7 |
Maddrey | + | + | - | - | - | - | - |
MELD | + | + | + | - | - | - | - |
GAHS | + | + | + | + | + | - | - |
ABIC | + | + | + | - | + | + | - |
Lille | + | + | + | - | + | + | + |
disulfiram (Antabuse)
Losartan
=Alcoholic steatohepatitis, when drinking isnt stopped
- inflammation signs (fever, leucocytosis)
- AST/ALT>2
- jaundice
- malnutrition
- +/- cirrhosis + ascitis
- Predni ufffn nacken (↑survival)
- Alternatives:
- Pentoxifyllin - prevention hepatorenal synd.
- Infliximab → alert: evtl. infections
- N-acetycystein - prevention HRS
- Enteral nutrition
- Transplant
mutation in the ATP7B gene which encodes for Copper-Transporting ATPase → ↓ceruloplasmin + ↑free copper → ↓biliary excretion → accumulation in liver, eye, kidney, CNS (basal ganglia).
liver D or neuropsychiatric manifestations
commonly 5-35y
only biochemical abnormalities → cirrhosis + ALF
T
- Rapidly progressive RF
- Coagulopathy
- Encephalopathy
- ALP/total bili ration <4
- AST/ALT ratio >2
- mild ↑AST+ALT
- Hemolytic anemia (coombs neg aka not due to antibodies)
Steatosis
T
- ↓Ceruloplasmin
- 50% Kayser-Fleischer
- ↑Liver copper
- ↑free copper
- Dysarthria
- Ataxia
- Tremor
- Parkinsonism
- Dystonia
- Cognitive, behavior + psychiatric impairment
- ↑Ca (urine) → nephrolithiasis + nephrocalcinosis
- Fanconi synd
- Ceruloplasmin
- Copper in serum and 24h urinary Copper excretion
- hepatic copper concentration after taking biopsy.
- On MRI/CT a typical sign in the basal ganglia is "Face of the giant panda" sign 📷
- Genetic testing reveals abnormality in ATP7B.
→ Histological findings might be conclusive for Steatosis, Fibrosis, Cirrhosis or ALF.
Cholestasis
heptic copper >4 micromol/g dry weight
{kind=link}
- D-penicillamine → chelating agent to detoxify tissue
- Chelation with zinc salts (interference with absorption)
- low copper diet
⇒Monitor the compliance!
In acute liver failure you wanna consider any type of dialysis, plasma pheresis or plasma exchange.
Worst case liver transplant if chelation fails in ALF + decomp cirrhosis
Wilsons appears due to a mutation in the ATP7B gene which encodes for Copper-Transporting ATPase → ↓less ceruloplasmin + ↑free copper → ↓biliary excretion → accumulation in liver, eye, kidney, CNS (basal ganglia).
Most common presentation is with liver disease or neurpsychiatric symptoms. Liver damaged ranges from only liver markers incr. → cirrhosis, most important presentation is with Acute liver failure or cirrhosis. Neurological manifestations involves dysarthria (cant speak properly), ataxia, Dystonia, Parkinsonism, Tremor + Cognitive impairment. Occular manifestations are Kayser-Fleischer ring. Renal abnormalitites are due to ↑Ca → Nephrolithiasis + nephrocalcinosis. Heart + pancreas might also be involved.
Biochemical markers in acute LF are an AST/ALT ratio >2, a Coombs-negative anema, ALT/total bili ration <4. In Cirrhosis you find ↓Ceruloplasmin+↑Copper.
Diagnosis is made by checking the Ceruloplasmin, Copper in serum and 24h urinary Copper excretion, measuring the hepatic copper concentration after taking biopsy. Histological findings might be conclusive for Steatosis, Fibrosis, Cirrhosis or ALF. On MRI/CT a typical sign in the basal ganglia is "Face of the giant panda" sign. Genetic testing reveals abnormality in ATP7B. A scoring system takes 7 things into consideration: Kayser-Fleischer, Neurologic, Ceruloplasmin, Coombs-neg hemolytic anemia, Liver Copper, Urinary copper + Mutation analysis. Score ≥4 is considered a safe dg.
Treatment is with D-penicillamine which is a chelating agent to detoxify tissue, Chelation with zinc salts(interference with absorption), and a low copper diet. Monitor the compliance! In acute liver failure you wanna consider any type of dialysis, plasma pheresis or plasma exchange. Worst case liver transplant if chelation fails.
Iron overload due to HFE mutation (esp. C282Y). Typically presentation ≥40y.
- Liver: Hepatomegaly, ↑AST+ALT, Fibrosis/Cirrhosis, HCC;
- DM (atypical)
- Bronzed skin
- Heart: dilated cardiomyopathy, HF, conduction disturbances (arrthymias);
- Hypopituitarism → Hypogonadism + Hypothyroidism
- Cognitive + neurologic abnormalities
- ↑Infections
- Porphyria cutanea tarda
- Clinical manifestations (above) that cant explained otherwise
- + family history
↑Ferritin, ↑iron + ↓TIBC
MRI might reveals heterogenous iron in the liver and neoplastic lesions.
CT is not very sensitive and might show and ↑liver density
- evidence of iron overload without HFE mutation;
- signs of cirrhosis;
- Ferritin >1000 and/or ↑AST+ALT.
Phlebotomy if Ferrtin >1000nl/ml
Chelating agents
<50 mg/l
There should be NO restrictions in meat, dont take Vit with extra iron; be aware that oxalate ↓ iron absorption and VitC ↑the absorption.
DM, HF, Cirrhosis, HCC
Iron overload due to HFE mutation (esp. C282Y). Typically presentation ≥40y.
Clinical manifestation can be fatigue and pain or more organ specific: with liver damage and hepatomagaly and signs of cirrhosis and HCC, damage to the heart which lead to dilated cardiomyopathie, arrhthmias and evtl. HF, atypical DM, Hypopituitarism and associated features, CNS involvement, bronzed skin and a ↑rate of infections. Porphyria cutanea tarda might also be present. Non-specific biochemical markers are high Ferritin, high iron + ↓TIBC.
MRI might reveals heterogenous iron in the liver and neoplastic lesions. Liver biopsy should be done in if theres evidence of iron overload without HFE mutation; signs of cirrhosis; Ferritin >1000 and/or ↑AST+ALT. CT is not very sensitive and might show and ↑in liver density
Treatment is with Phlebotomy if Ferritin >1000 ng/ml; target is a Ferritin of <50 mg/L. Dont forget to monitor for cirrhosis + HCC and maybe consider liver transplant.
There should be NO restrictions in meat, dont take Vit with extra iron; be aware that oxalate ↓ iron absorption and VitC ↑the absorption.
Most common causes of death are HF, Cirrhosis, DM + HCC.
{kind=link}
Hepatic:
- Hepatitis - viral or AI
- ALD + NAFLD
- Wilson hemochrom
- Drugs Toxins
Hepato-biliary: Chronic cholestasis: PBC + PSC
Posthepatic: obstructions → i.e. budd-chiari, CHF
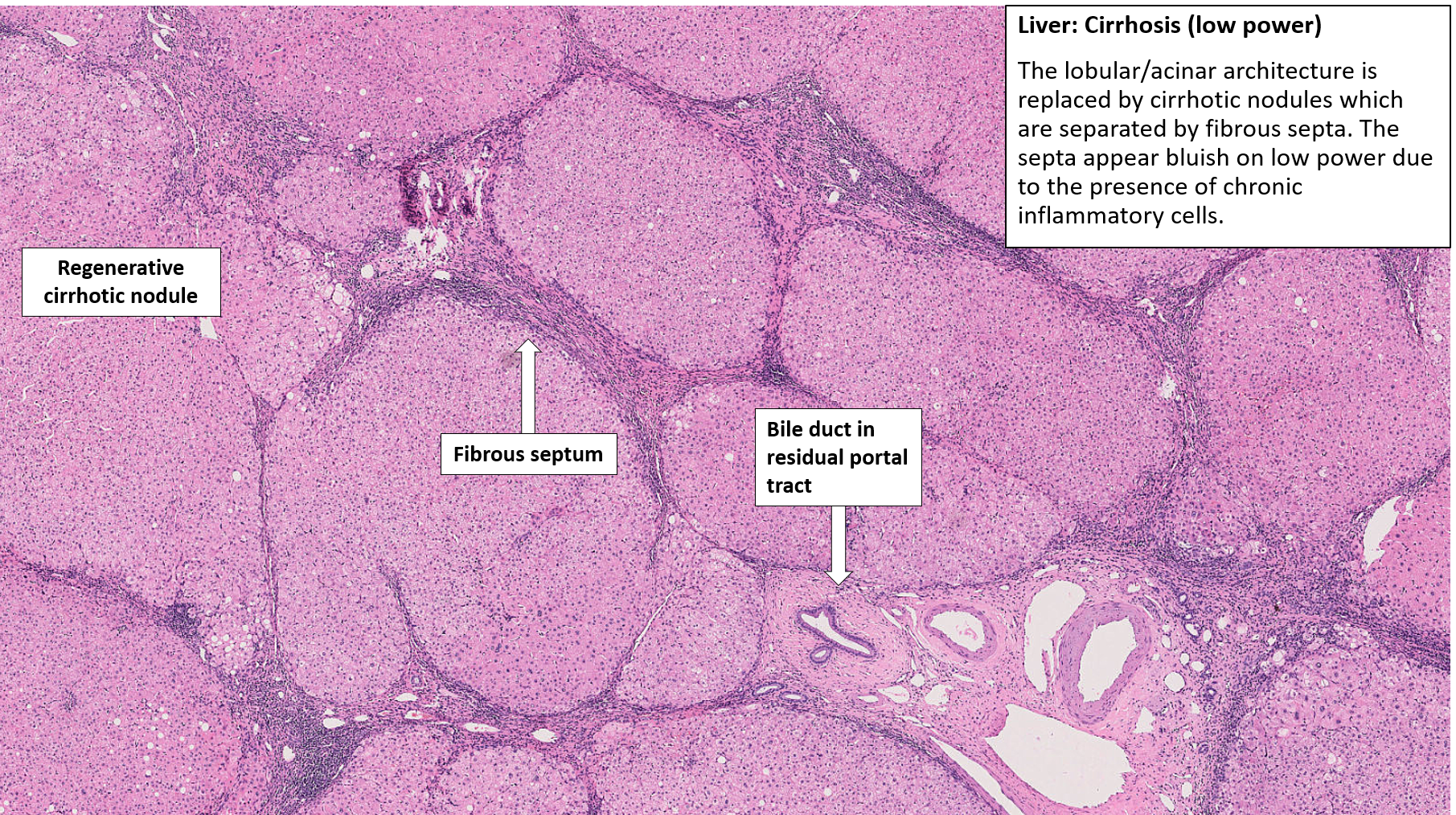
- macro + micro nodular
- Portal biliary or postnecrotic
portal - alcohol
hepatitis → viral or AI
fibrogenesis
- ↑intrahepatic resitance (fibrosis, vasoconstrictors, NO deficiency(intrahepatic))
- ↑portal venous flow (splanic dilation due to ↑NO)
- ↑resistance to collateral circulation
10mmHG - 12mmHG
12mmhg
- periph. vasodilation → RAAS → Na+H2O reabsorption
- Increase in sinusoidal pressure
- bacterial translocation
- Constipations (↓transit→overpopulation)
- ↑permeability of intestinal mucosa (hypoxia)
E.Coli, Klebsiella, Streptococcus
encephalopathy(due to worsening of liver failure), kidney failure
↑ammonia + other toxic metabolits → ↑GABA synthesis + ↑no. of benzodiazepin ligands
trigger factors:
- SBP
- Anemia (bleeding)
- TIPS
- Dehydration + Hypokalemia (!Diuretics)
- Hypoxia
- constipation
- drugs
→ vasodilation (probably due to toxins) → shunt formation → perfusion-ventilation missmatch → hypoxia (→evtl. secondary vasoconstrition: pulmonary HT)
⇒ (chronic) liver disease, hypoxemia, intrapulmonary shunts
hypoxia is worse in orthostatism because gravity → blood into lIver lobes → increase blood at the level of shunts
cardio-pulmonary disease
Peripheral vasodilation (esp. splanchnic) → RAAS + ADH → renal vasoconstriction → ↓renal blood flow + ↑Na reabsorption
- 40% asymptomatic
- asthenia + fatigue
- derma changes
- spider angioma
- palmar erythema
- Jaundice
- Encephalopathy (Asterixis)
- Ascitis (abdominal pain)
- Digestive hemorrhage
- Splenomegaly
- Hepatopulmonary synd
- Hepatorenal synd.
- bleeding (↓coagulaton factors+thrombos)
- Hepatic hydrothorax
- hypogonadism + gynecomastia (↓estrogen clearance)
- pancreatitis (esp. in alcoholics)
- reflux esophagitis ( ↑NO due to bacterial toxins which are not cleared by the liver)

- gastritis + ulcers (due to portal HT)

- steatorrhea + Gallstones (both due to ↓secr. of bile acids)
Portal HT → splenic pooling → splanchnic arterial vasodilation → ↓volume → RAS activation
→ ↑ADH → ↓Na
→ ↑Aldosteron → ↓K
- ↓Albumin
- ↑INR/PT
- ↑Bili
- AST/ALT >1
- Cholestatic markers → ALP, GGT, 5nt
- ↓Hb
- Inflammatory syndrome (i.e. in SBP)
- Crea
Palpation left hepatic lobe
splenomegaly
- Encephalopathy
- Ascitis → SBP + Hepatorenal synd.
- Splenomegaly + Thrombocytopenia
- Digestive hemorrhage
- Fever
- Confusion
- Abdominal pain + tenderness
- jaundice
- size of the liver (small)
- HCC
- Signs of Portal HT
- portal diameter (also SMV, SV)
- collaterals
- portal flow
- thrombosis
check for esophageal + gastric varices
→ ligation of varices or sclerotherapy
non-selective beta blockers (nadolol, propranolol)
- ascitis - at onset assessment
- suspicion of SBP
- unexplained encephalopathy
- release pressure
- renal insuff
HVPG assesment with catheter⇒ see above
- decompensated cirrhosis
- imaging (CT) + scincti already dg. (didnt mention it before but can be used too)
- Liver pretretment (??)
- cytology (+culture of fluid)
- PMN >250/mm3
MRI + CT
- anuria /oliguria
- hyperosmolar urine (↑Na excretion)
- ↓Na elimination after diuretics
- ↑crea-urinary/blood-ratio
- Liver disease
- Blood creatinine levels increasing by ≥ 0.3 mg/dL within two days or rising by over 50% from the starting level.
- No enhancement in kidney function following fluid replacement using albumin for a minimum of two days and a minimum of 48 hours excluding diuretic use.
- Urine output of less than 0.5 ml/kg.
- Reduced urine sodium concentration (below 10 mmol/L).
{kind=link}
{kind=link}
- Child A: 40%
- Child B: 60%
- Child C: 85%
Stage 1:
- low attention
- irritability
- tremor
- depression
- normal EEG
Stage 2:
- Sleepiness (+sleep disturbances)
- ↓Memory
- Behavior change
- Asterixis
- Ataxia EEG
Stage 3:
- confusion + disorientation
- amnesia
- Hypo-reflexia
- Nystagmus
Stage 4:
- Coma
- Mydriases
- No response to stimuli
- Glasgow coma
- Conn encepathlopathy index
- other neuropsychitric test
- Asterixis
- NH3 arterial
Type 1:
- ↑crea by 100% to >2.5mg/dl
- or 50%↓ in Crea-clearance to <20ml/min
- high mortality!
Type 2:
- Crea >1.5mg/dl
- better prognosis
- Antiviral → HepB+C
- Vaccination (HepB)
⇒ Reduced progression of cirrhosis + ↓risk for HCC
- Withdrawl alcohol
- Loose weight
AI → predni
cholestasis → ursodeoxycholic acid
nope
2-3y
repeat in 1-2y
primary prophylaxis with nonselective betablockers or band ligation
TIPS
- Volume recusitation
- AB prophylaxis (Cetriaxone)
- Prevention of Hepatic encepahlopathy → lactulose, rifaximin
- Vasoconstrictors: terlipressin, somatosatin, ocreotide
- Endoscopy (within 12h) → Ligation or glue injection
→ secondary: NS-beta-blockers, repeat band ligation, TIPS (if rebleeding), Liver transplantation
- vasoconstrictors → but ↑intrahepatic resistance
- (vascons + vasodil) → ↓intrahepatic resistance
Treatment | Splanchnic Flow | Intrahepatic Resistance | Portal Pressure |
Vasoconstrictors | ↓↓ | ↑ | ↓ |
Vasodilators | - | ↓ | ↓ |
Vasoconstrictors and Vasodilators | ↓ | ↓ | ↓↓ |
TIPS
Treatment | Splanchnic Flow | Intrahepatic Resistance | Portal Pressure |
Vasoconstrictors | ↓↓ | ↑ | ↓ |
Vasodilators | - | ↓ | ↓ |
Vasoconstrictors and Vasodilators | ↓ | ↓ | ↓↓ |
Endoscopic treatments | - | - | - |
TIPS/surgical shunt | ↑ | ↓↓↓ | ↓↓↓ |
- Na + water restriction
- Diuretics (Furo+Spironolactone)
- Paracentesis
- → TIPS or peritoneum-venous shunts (esp. in refractory cases)
paracentesis → protein loss + hypovolemia
diuretics → encephalopathy
- responds to diuretics
- no infection
- no kidney damage
- untreatable with diuretics (side effect)
- diuretic resistance
- kidney dmg to post-paracentesis hypovolemia (RAAS→ Water+H2O retention)
→ repeated paracentesis + albumin or other macromolecules
→ TIPS
→ Peritoneo-venous -shunt
encephalopathy
ABs!
- Cephalos: Cefotaxime
- Amoxi-Clavu
→5days
Albumin
- correct precipitating factors
- lactulose
- rifaximin
- ↓protein intake
- oxygen therapy
- oxygen
- ascitis correction
- liver transplant
hepatopulmonary syndrome = triad of liver disease, hypoxemia, and intrapulmonary shunting (vasodilation of pulmonary vessel)
- Na restriction + Diuretics (Furo+Spirono)
- Albumin
- Dopamine (or NE, octreatide)
- TIPS
- Liver translant
- reducting of PT + variceal bl
- ascitis
- hepatorenal
- Large regenerative nodule
- Low grade dysplastic nodule
- high grade -"-
- Small HCC
- early HCC
- progressed HCC
- PV
- Hepatic vein
- IVC
- intrehepatic bile ducts
- refractory ascitis (see above)
- Gelb wie n simpson (deep jaundice)
- worsen encephalopathy
- UGIB
- Cholestasis
- ↑Liver markers (AST,ALT, ALP,GGT)
- alpha fetoprotein
- inflammatory + ↑viral markers
- des-gamma-carboxiprotrombin (abnormal protrombin)

US
low likelihood of HCC
→surveillance: US every 3 month → no growth in 1-2y → US every 6 month
→ 2 imaging techniques (i.e. CT+, MRI+, CEUS): arterial enhancement + washout
⇒ treat as HCC
! if not typical on imaging ⇒ biopsy(FNA)
- arterial enhancement + washout on 1 imaging techniqie
- OR AFP>200 ng/ml
⇒ treat as HCC
! if not typical on imaging ⇒ biopsy
- bleeding
- seeding
nice rhyme 😎
- inoperable patient
- assessment of:
- tumor biology
- prognosis
- rupture → bleeding (intraperitoneal)
- Thrombosis → PV, HV, IVC
- Obstructive jaundice (bile duct invasion)
- colon + stomach invasion
- mets : pulmonary +spine
- Hypoglycemia

poor → average 6m survival
- Resection
- Chemo or radioembolization (TACE / TARE)

- Percutaneous ablation:
- Ethanol injection = PEI
- Radiofrequence ablation = RFA 📺
- Sorafenib→ multikinase inhibitor, prolongs survival

BCLC staging system : (Barcelona-Clinic Liver-Cancer)
0 = Very Early stage, Child-Pugh A → Single <2 cm, carcinoma in situ
Child-Pugh A-C
A - early stage → Single or 3 nodules <3 cm, PS 0
B - intermediate → Multinodular, PS 0
C - advanced → Portal invasion, N1, M1, PS 1-2
D = terminal stage, Child-Pugh C
Child-Pugh A
No portal HT
Bili<1mg/dl
- mets
- Child-Pugh B+C
- PHT
- Bili>1
Milan Criteria:
- single tumor <5cm (stage 0)
- ≤3nodules each ≤3cm(=stage A)
- no extrahepatic disease (0+A)
means stage 0 and stage A (without extrahepatic manifestation
- BCLC 0-A
- RFA
- <5cm
- PEI
- <2cm
- recurrance after surgery
- residual tumor after chemoembolization
{kind=link}
contrast imaging - CEUS, CT, MRI,
AFP
Multikinase inhibitors → i.e. Sorafenib
→ ↓cell division, prolif., angiogenesis
- Vaccine HepB
- IFN therapy in HepC
imaging methods, esp often incidentally discover via US
T
mets
{kind=link}
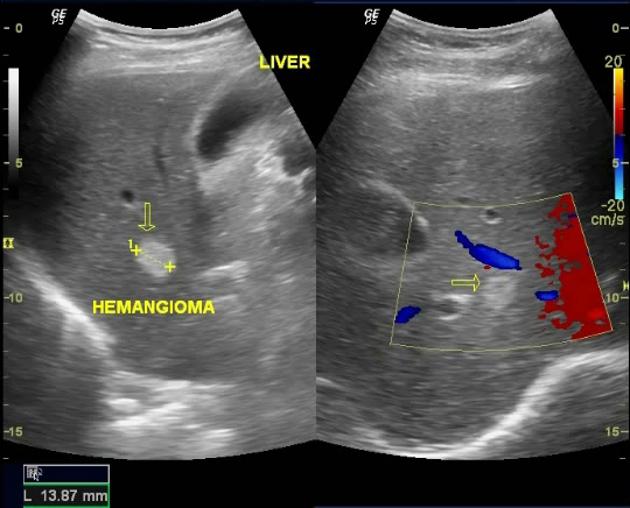
- bright (hyperecho)
- inhomogenous
- reduced Doppler
young females on contraceptives
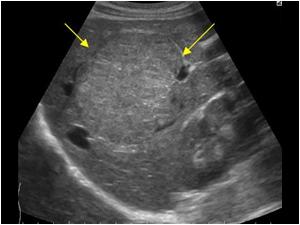
{kind=link}
- dark (hypoecho)
- homogenous
biopsy
!!bleeding
T
MRI
(you might also consider CEUS)
biopsy to exclude malignancy
{kind=link}
Large nodule mimicking regnerative cirrhotic nodule
compression of sourrounding → pain
imaging: CEUS, Doppler, CT
⇒hypervascular
{kind=link}
{kind=link}
T
hematogenous pathway
- asymptomatic: incidental discoverd
- pain
- fever
- jaundice
- Liver failure
- multiple, irregular 📷
- tumor markers
- ALP+GGT ↑ (if jaundice)
- chemo
- RF laser ablation
- Resection
- Palliative care
🎋 Biliary Tree Pathologies
hemolysis + liver disease
bacterial infection
cholangitis
cholecystitis
→ compromised vascular suppls → gangrene+abcess
F → woman 2:1 men
obese + middle age
- nausea
- episodes of biliary colic
- ↑with fatty meals
- Murphy sign → cholecystits
- signs of infections: fever, tachycardia
- jaundice if CBD obstr.
- Pancreatits (look for Cullen + Grey turner signs)
- cholangitis (look for charcot triad +Raynauds pentad (mental status change + hypotension)
Prolonged fasting
- CBC
- Electroyltes
- ↑AST+ALT
- ↑ALP, GGT
- ↑Bili
- Lipase, Amylase
US
→ also info about: bile duct, liver, pancreas, cholecystis
- xray → porcelain gallbaldder(heavy calcification) →↑ risk gallbladder cancer
- CT scanning → but only when invest. abdominal pain without specific localizing symptoms or signs
HIDA scan
- symptomtic gallbladder-disease
- prophylactic only in:
- porcellan gallbladder
- gallstones >3cm
gallstone → inflammation behind it
( may be caused by infective agents in immunocompromised)
Acalculous cholecystitis
- RUQ / epigastric pain → sudden, stead, ↓over 12-18h
- radiation infrascapular
- Fever
- RUQ guarding
- vomiting
- palpaple bladder
- jaundice (consider also choledocholithiasis)
- WBC
- AST+ALT
- ALP+GGT
- Total bili
- Amylase + Lipase*
- X-ray: may reveal radiopaque gallstones (15% of cases)
- HIDA Scan: helpful for obstructed cystic duct, reliable if bilirubin < 5mg/dL
- Ultrasound: useful for visualizing gallstones
Alles was sich entzünden kann
- perforated ulcer
- pancreatitis
- liver: hepatitis, abcess
- pneumona
- appendicitis
- MI
- Antibiotics
- Analgesics
- cholecystectomy (adviced-high recurrance rate)
- (total parenteral nutrition??)
Stones in CBD
→ cholangitis!
- Pain (RUQ)
- Fever
- Jaundice
- All classics
- US
- CT
- MRI
- MRCP
- EUS
- Percutaneous transhepatic cholangiography (PTC)
- ERCP
- Laparaoscopic cholecystectomy
- ABs (ciproflox)
→ papillotomy
→ stone extraction
diffuse inflammation biliary tract → fibrosis → strictures
young men 20-40
IBDs → esp. UC!
HLA
AIDS
- progressive obstructive jaundice
- ↑ALP
→ mailaise, pruritus, anorexia, dyspepsia
A marked increase in serum autoantibody levels occurs in patients with PSC as well, with antineutrophil cytoplasmic antibodies (ANCA) in 87%, anticardiolipin (aCL) antibodies in 66%, and antinuclear antibodies (ANA) in 53%. It has been reported that PSC and IBD have overlapping yet distinct genetic architectures
- Malabsorption Vit ADEK
- Osteoporosis.....
ERCP+ MRCP
- corticosteroids
- broad spectrum Ab → esp. episode of acute bact cholangitis
- Ursodeoxycholic acid
- ERCP → in bileduct stenosis → stent
cirrhosis + clinical decompensation
stones
- surgery for biliary disasese
- chronic cholecystitis with salmonella typhi
- polyps >1cm
- large stones
- procelain gallbladder
- weird panceraticobiliary ductal junction
at confluence of hepatic duct
=KLATSKIN TUMOR
65%
distal extrahepatic bile duct
(rest intrahepatic bile duct )
- Courvoisier Sign
- RUQ pain → raditation in back
- weight loss
- fever, chills (if cholangitis)
- jaundice
- pruritus
- anorexia
- Hepatomegaly
obstruction markers, liver markers, CA19.9 (also for pancreates Ca)
- ↑conj bili
- ↑ALP + GGT
- ↑Cholesterol
- CA 19-9
- (evtl ↑ALT+AST)
classics (US, CT, MRI) + MRCP
good 80%
→ drops hard when more extensive
10%
- surgery + chemo
- stenting
- analgesics
intrahepatic choleangioCa
🧽 Pancreas Pathologies
- irrev. progressive destruction parenchyma due to autodigestion → glandular artrophy, inflammation, fibrosis
- pancr. insufficiency (exo+endocrine)
- chronic pain
- calcification
{kind=link}
Most important: alcohol, reccurent acute pancr., obstruction
genetic form: either mutation in genes of Trypsinogen or Trypsinogen inhibitors
🍷🍺
👍🏾
- continous pain (epigastric)
- malabsorption syd → steatorrhea (when 90% of parenchyma destroyed after 10-20y)
- weight loss
- Vit ADEK + B12 def.
- diabetes (latest, after 20y)
- !risk of hypoglycemia
→ radiates to the back, left costal margin, interscapulohumeral
→ esp. after alcohol intake + eating
→ relieved by bending forward
T
classics + EUS + MRCP
- xray
- US + endoscopic US (EUS)
- CT
- MRI
- MRCP
calcifications 📷
{kind=link}
EUS 📷
- duct dilation + wall
- strands
- cysts >2mm (major assessment: relationshiop, maturation)
- calcifications
Cholangio-MRI
treatment! → stone extraction, duct dilation + stent insertion
acute pancreatitis
{kind=link}
- ↓Fecal elastase 1 activity → confirms that steatorrhea is due to pancreatic lipase insufficiency
- D-xylose

- steatocrit
- pancreatolaurly
- OGTT
- Glucose
- Glycosuria
might be ↑ in exacerbation
- GGT → if obstructive
- ↑Ca+TGs
- Macrocytic anemia, low Ca → alcoholic etiology
- ↑gamma-globulin
- eosinophilia
- Anti-lactoferrin, anti carbonic hydrase
CEA, CA19-9 ("tip aufn po")
- Cystic fibrosis gene
- trypsin inhibitor gene
- trypsinogen gene

T
POPSI FC
- Compression/Stenosis
- CBD obstruction → jaundice, pain
- duodenal obstruction
- colon stenosis
- Pseudocysts → imaging + ↑urinary amylase
- might infect, rupture, fistula

- Pseudoaneurysm
- due to autodigestion of arterial wall or erosion by pseudocyst
- might lead to hemorrhagic shock
- Splenic vein thrombosis → gastric variceal bleeding
- Infarction of adjacent tissue
- Fistula → might produce pancreatic ascitis, pleural effusion or pericarditis
- Pancreatic cancer
- ulcer
- cancer
- biliary tree pathology
IBD, Celiac
pancreatic cancer!!
! imaging + tumor markers + biopsy
nope, high mortality after 7-10y of evolution
!stop smoking+alc → ↓progression
- avoid alc, coffee, smoking
- lower fat consumption
- antioxidants
DOS OPA
- Drainage of pseudocyst
- endoscopic, surgical, percutaneous
- remove obstruction: tumor, inflammation
- → ERCP or surgery
- i.e. stone extraction, dilation, stent(stenosis), sphincterotomy
- extracorporal shockwave lithotripsy
- Splenectomy in splenic vein thrombosis
- Octreotide → ↓secretion stimulation
- Pancreatin (lipase substitution)
- Analgesics + denervation
- Duodenal obstruction → wipple
- dont forget to treat hyperparathyroidism if exist
I GET SMASHED 📷 : most important: Gallstone, ERCP
{kind=link}
PANCREAS 📷 : Most important: parenteral feeding, analgesics, fluid resuccitation, stone extraction
{kind=link}
Complication: Pseudocyst, Hemorrhage, Fat necrosis, Bacterial superinfection, Sepsis & multiorgan failure
Lab: Amylase, Lipase, Hct, (Tg, Ca)
Imaging: US, CT, MRCP
old, 60-80y
- chronic pancreatitis (on the setting of ductal hyperplasia)
- hereditary + tropical pancreatitis
- ↑caloric intake, cooked meat +fish
- smoking
- DM (also vice versa)
- genetic: family history, hereditary pancreatitis, peutz-jeghers, ocogene mutation,
75% head of pancreas
- ductal strucutre different degree of differentiation
- desmoplastic reaction (fibrous tissue)
- invasive af!!
- !Peritoneal invasion
- vessel: PV, SV, SMV etc.
- regional lymph nodes
- nearby organs
Stage 1: T1/2N0M0 → only pancreas
Stage 2: T3N0M0 → expansion to nearby organs
Stage 3: Any TN1M0
Stage 4: AnyT+N M1
- Pain
- Radiation to back (visceral retroperitoneal pain)
- Somatic pain according to location
- Jaundice
- Pruritus
- Courvoisier sign
- weight loss
- diabetes
- GI bleeding → invasion
- Trousseau syndrome → thrombophlebitis
- nausea
- palpable tumor
- ascitis
- CEA + CA 19-9
- ↑Gluc
- Cholestasis markers
- inflammatory or anemic synd.**
- hypoecho (dark like a motherfucker)
- detect if >1.5-2cm
- Double duct sign (wirsung + CBD dilation)
- ascitis
- invasion
- mets
dg + staging!
1
also best to assess resectability
- tumor staging
- vascular invasion
- biopsy
- collect pancreatic juice for cytology
- biopsy
- DD: chronic pancreatis vs cancer
Laparoscopy → peritoneal micromets
PET → DD chronic pancreati
FNA
with US, CT, EUS or ERCP guidance
- acute pancreatitis
- peritonitis
- pancreatic fistula
portentiall resectable lesions!!
risk of seeding
> 40% show capsule invasion, lymphatic, venous and perineural extension
T
- The identified lesion should be less than 1 cm in size, confined to the ductal epithelium, and without invasion into the parenchyma.
- Diagnostic procedures such as ERCP and ductal biopsy are recommended to confirm the diagnosis.
- The condition is curable with a success rate of 100%.
- obstructive jaundice → CBD obstructions
- gastric outlet obstructions
- Mets (esp liver)
- etc....
- chronic pancreatitis
- cystadenocarcinoma
- pancreatic lymphoma
poor
- radical surgical
- deuodenopancreatectomy
- resection tail+body
- total pancreatectomy + duodenum, spleen, stomach, omentum
- palliative surgical (most patients)
- biliary stents → resolve obstructions
- duodenal stents
- alcoholization of nervous plexus (pain)
- chemo + radio → additionally to surgery
- Cystadenocarcinoma → good survival with surgery
- Epithelial neoplasm
- solid
- papillary
- Intracanally tumory
- papillary
- mucinous
- Acinar carcinoma