
Table of content
- Occupational Medicine
- ⛲ Introduction
- 🌬️ Work-related Asthma
- 🏭 Pneumoconiosis
- 🧪 Toxicology
- 💪🏽 Musculoskeletal Disorders
- 🪖 Physical Hazards
Member Resources
 Year 4
Year 4 Year 5
Year 5 Year 6
Year 6

Occupational Medicine
- where did you work before?
- special shifts? night?
- operations carried out by colleagues that have an impact on health status (e.g. dust, noise, paint vapour)
- Most important: accessing risk factors!
- physical:
- noise
- radiation:
- ionizing: gamma → medical staff, airport staff, metal processing
- non-ionizing: UV → agriculture, lifeguards, road workers
- vibration → hand-arm, total body
- in lecture: microclimate
- esp. dyes + dusts
- metals
- organic solvent
- fibrogenous powers: silicogenes + asbesteos → pneumoconiosis
- non-fibrogens: textilles, cereals → allergic/irrtating efect → asthma, COPD
- Fungi, bacteria, viruses, parasites
- posture (prolonged standing, vicious positions)
- sustained heavy weight (max. 10kg female/ 20kg men)
- repetitive movement
- visual-pc operators
- welders (sweat cataract)
- cold <15°C
- warm >35°C
- incr./low humidity (normal 50-70%)
2. chemical
3. Physical-chemical
4. Biological
5. Ergonomical (Osteo-musculo-articular) + neuro-psycho-sensory overload
6.Microenvironment
- Personal Protection → mask, glasses, helmet, overalls, boots with protective caps
- Collective Protection → lighting, ventilation, toilet, proper handling of dining areas
incapacity for work greater than 3 working days
(a) accidents resulting in temporary incapacity for work of at least 3 calendar days; (b) accidents resulting in invalidity; (c) fatal accident; d) collective accidents, when at least 3 people are injured at the same time and for the same reason.
extra-work conditions
To interpret X-ray findings of silicosis and asbestosis, the lungs are divided into three areas: RU, RM, RI; LU, LM, LI.
- In silicosis, opacities typically appear in the middle areas,
- in asbestosis, opacities are more commonly seen in the inferior areas.
- conc. of small opacities in affected zones of the lung
- based on comparison with standard radiographs
0 ⇒ absent small opacities (/less opacities than 1)
1 ⇒ few small opacities
2 ⇒ more than few (moderate conc.)of opacities
3 ⇒ most numerous opacities
Category and Subcategories
- 0
- 0/-
- 0/0
- 0/1
- 1
- 1/0
- 1/1
- 1/2
- 2
- 2/1
- 2/2
- 2/3
- 3
- 3/2
- 3/3
- 3/+
rounded + irregular opacities
p → diameter up to 1.5mm
q → 1.5-3mm
r → 3-10mm
s → width up to 1.5mm
t → 1.5-3mm
u → 3-10mm
yeeee
Category A: longest dimension of one opacity OR sum of several large = 1-5cm
Category B: longest dimension of one opacity OR sum of several large = >5cm but less not exceeding equiv. area of right upper zone
Category C: longest dimension of one opacity OR sum of several large = exceeding equiv. area of right upper zone
p=1,5 mm | s=1,5 mm |
q=1,5-3 mm | t=1,5-3 mm |
r=3-10 | u=3-10 |
A=1cm-5 cm | |
B=opacities 5 cm, not over the right upper zone | |
C=1 or more the are over the right upper zone |
atherosclerotic aorta
coalescence of small opacities
bullae
cancer
calcification in small pneumoconiatic opacties
abnormality of cardiac size or shape
cavity
emphysema
eggshell calcification of hilar or mediastinal lymph nodes
rib fx (acute or healed)
enlargement of non-calcified hilar or mediastinal lymph nodes
mesothelioma
pleural thickening of an interlobar fissue
tuberculosis
other diseases or signif. abnormality
- 0/1, 1/0 the patient is no longer able to work with silica dusts
- 1/1 the patient is entitled to a compensation (Romania)
- 2/2 the patient is entitled to a compensation (Germany)
- high BP
- recent surgery
- cataract glaucoma
- epilepsy
- acute respir. infection
- general pulmonary diseases
- cardiac diseases (acute or chronic)
- recent use of bronchodilators
RV + TLC
dilator → salbutamol
constrictor → methacholine/histamine
max amount of that can be expeled after max. inhalation
VC = TV+ERV+IRV
TV (tidal volume) 0,5 - 0,8 l = 15%VC inspiratory reserve volume 1,5 - 21 = 60%VC expiratory reserve volume 1,2- 1,5l = 25%VC

FVC = amount of air that can be forcibly exhaled from your lungs after taking the deepest breath possible, as measured by spirometry.
FEV1 = The volume of air that can be forced out in one second after taking a deep breath, an important measure of pulmonary function
⇒ FVC + FEV1 represent big airways
FEF25-75% = Volume exhaled between 25% from FVC until eliminating 75%
FEF 50% = Volumen exhaled at 50% from FVC
⇒ FEF25-75 + FEF50 represnet small airways
Tiffneau = FEV1/FVC
min. 6sec
- COPD
- Asthma
- Cancer
- Check FEV1 first! → most important value: FEV1 + TIffneau decr → obstruction;
- in obstructive syd. small airways obstructed first (FEF50+ FEF25-75)
→ FEV1 for severity
parameters | Normal values | light | moderate | accentuated | severe |
FVC | >80% | 80-60% | 60-40% | 40-30% | <30% |
FEV1 | >80% | 80-60% | 60-40% | 40-30% | <30% |
TI | >70% | 70-60% | 60-40% | 40-30% | <30% |
FEF50% | >80% | 80-60% | 60-40% | 40-30% | <30% |
- pulmonary fibrosis
- pneumoconiosis
- others.
(mixed syndr) → check TLC to classify as restrictive pattern (TLC low) → Pletismography
→ note Tiffneau can be normal in restrictive pattern
Parameter | Normal values | Light alteration | Moderate alteration | Accentuated alteration | Severe alteration |
TLC
FEV1
FVC
FEF50
PEF | >80% | 80-60% | 60-40% | 40-30% | <30% |
FEV1/FVC | >70% | 70-60% | 60-40% | 40-30% | <30% |
RV | <125% | 125-145% | 145-175% | 175-200% | >200% |
hyperinflation → COPD (irrev.) or Asthma (rev.)
→ restrictive syndrome
or patient doesnt perform test correctly
- dg of asthma (DD vs. COPD)
- sprimetry showed: obstruction in small airways (FEF50 dec.) + obstructuctive ventilatory dysfunction (FEV+TI decr.) + hyperinflation (RV inc)
FEV1 incr >12% + FEF >25%
FEV1 incr. with 200ml
Bronchodilator Test | Positive | Negative |
Reversible Obstruction | Irreversible Obstruction | |
Asthma Crisis | COPD | |
Criteria | FEV1>12%, FEF 50%>25%, FEV1 increases with 200 ml | FEV1<12%, FEF50%<25% |
when spirometry is normal but pat. expirience dry cough at specific situations (work)
- bronchial hyperreactivity → only present at work space
- (nonspecific) asthma
→ confirms etiology/connection to occupation
nonspecific (methacholine) + specific (suspected agent at work)
- FEV1 < 60%
- pregnancy
- rib fracture
- recent surgery
- infection
- severe cardiac diseases
- glaucoma
FEV decr > 20%

20-20.000 Hz
500-3000 Hz
lowes perceived 0db
abover 120-140 (150) → pain + possible hearing loss
- transmission hypoacusia ( air lower than bone diagram, bone diagram in normal limitis)
- neurosensory hypoaccusia (bone + air equally low)
- mixed (air lower bone, but bone below normal limits
determine where minimum intensity (sound pressure) perceived on the various frequencies (125-8000Hz)
physiological hearing loss → indivdualized table by age group
Age | 125 | 250 | 500 | 1000 | 2000 | 4000 | 6000 |
20-29 | 0 | 0 | 0 | 0 | 0 | 3 | 5 |
30-39 | 5 | 5 | 5 | 5 | 6 | 14 | 16 |
40-49 | 7 | 7 | 7 | 8 | 8 | 21 | 25 |
50-59 | 10 | 10 | 12 | 12 | 13 | 29 | 32 |
60-69 | 14 | 14 | 15 | 19 | 24 | 40 | 48 |
70-79 | 18 | 19 | 23 | 24 | 31 | 47 | 59 |
80 | 22 | 23 | 27 | 33 | 39 | 56 | 66 |
vibration fog → diapason
high → does not affect life at first
earplugs + headphones
permanent decr. of threshhold to a freq. 4000Hz >30db after correction
→ neurosensorial hypoacusis if bone line is similar
bilat + symmetrical (+-10db)
>25db at freq. 500, 1000, 2000 Hz (after correction)
bilat + symetric
- oven + dust+ coal → recurrent bronchitis → pneumonia → lung cancer
- chimney-swweps carcinoma: testicular (skin) cancer caused by soot (Ruß) → can be prevented easily by washing or special cloths
- chemo + radiotherapy → protective meassures for workers! (gloves, masks)→ they might cause skin + bone cancer + leukemia
- PVC → liver angiosarcoma
- chlorine gas → carcinogenic!
- ABS (plastic material)
- Arcylonitrile → lung cancer
- Butadiene → carcinogenic in mice
- Styrene → poss. carcinogenic
- wood dust → ethmoid cancer
- glue (benzene) → leukemia
- chromium → lung cancer, nasal septum perforation + ulcer
- alcohol → cancer mouth, pharyn, esophagus, larynx, liver
- asbestos → malignant mesothelioma, lung cancer , mediastinal cancer
- Chimney sweeps (soot, smokes, gas with polycyclic aromatic hydrocarbons (PAHs) - carcinogenic liver, lung, esophagus
- PAH also in asphalt (tar)
⛲ Introduction
Hazard - anything that can cause harm - potential to harm
Risk - chance smb harmed by hazard - likelihood of harm
{kind=link}
- physical
- chemical
- biological
- ergonomical
- psychological
- Physical: noise, vibration, radiation, temperature, etc.
- Chemical: metals, SiO₂, organic solvents, polymers, etc. (70,000 chemicals used - 12,000 tested)
- Biological: viruses, bacteria, parasites
- Ergonomical: posture, repetitive motions, heavy weight lifting, working schedule, etc.
- Psychological: inter-personal relationships
- controlled
- health
- uncontrolled
- fatigue
- occupational illnesses and injuries
- work-related and work-aggravated disease
- illness: (long term) direct consequence of risk factor exposure
- injury: accident, acute violent injury/poisoning during work or on the way to or from the workplace → >3days can't work (not minor cuts etc)
- “Occupational illness = health impairment occurred as a consequence of practicing a specific job, caused by exposure to physical, chemical or biological risk factors or by physical or mental stress
- Occupational injury = violent body injury or acute body poisoning which occurs during work activity or in the way to/from the workplace and determines more than 3 days away from work, permanent handicap or death”
- work-related: common diseases (HT, ischemic heart diseases, chronic respiratory diseases, peptic ulcer, MSK..) ⇒ multifactoral etiology (only some of them are occupational risk factors!)
- “Work-related illness = common disease, multifactor etiology, with some occupational risk factors
- Work-related illnesses: arterial hypertension, ischemic heart disease, chronic non-specific respiratory diseases, peptic ulcer, low back pain and other musculoskeletal diseases, neurosis and other neuro-psychiatric disorders”
1. muscoloskeletal
2. neurological diseases
3. respiratory diseases,
4. disease of sensory organ
⇒ 📷
{kind=link}
WARP
Work - Cause or aggrevation factor for complaint/diseases?
- What's your job?
- Do you think there's a relation?
- Symptoms different at work vs. at home?
- Any present or past exposure?
- Coworkers similar symptoms?
- Occupational physician at workplace?
Activities - complaint/Disease = consequence for activities at work?
Refferal - should I refer to occupational physican or other specialist?
Prevention - Can I do smth. to prevent complaint/disease?
MSDS
material safety data sheet
Sources of information
- MSDS (Material Safety Data Sheet)
- Example: Diversey Nocolok Flux MSDS.pdf
- https://fscimage.fishersci.com/msds/10421.htm
- Employer (Safety Engineer)
- Poison Control Centers, Government Agencies, Academic Institutions
- Worker’s Compensation Insurance Carriers
- Occupational Physicians and Industrial Hygienists
- Medical Libraries
- Online Databases
🌬️ Work-related Asthma
inhaled Allergen → IgE Ab→ histamine release
- Bronchial hyperresponsiveness (fast+severe bronchoconstriction)
- Bronchial Inflammation → mucosal edema + SM contraction
- Bronchial obstruction
- Bronchospasm
- Edema
- incr. mucus production
Obstruction is reversible in asthma
→ spontaneously or with inhalator
work agent (direct occupational exposure)→ asthma
CLEAR RELATIONSHIP, no other cause
exacerbation of pre-existing nonoccupation asthma due to work-trigger
exacerbated or caused by work agent
a term that includes OA + WAA
- sensitizer-induced → immunological mechanism → exposure to sensitizing agent → occurance after a period of time
- high MW (molecular weight)→ animal or plant origin
- low MW → chemicals
- irritant-induced (no latency)→ direct trigger of airways-nerves + dmg epithelium → begins directly
→ ammonia, chlorin, ...= potent irritant
(in the past: Reactive airway dysfuction syndrome)
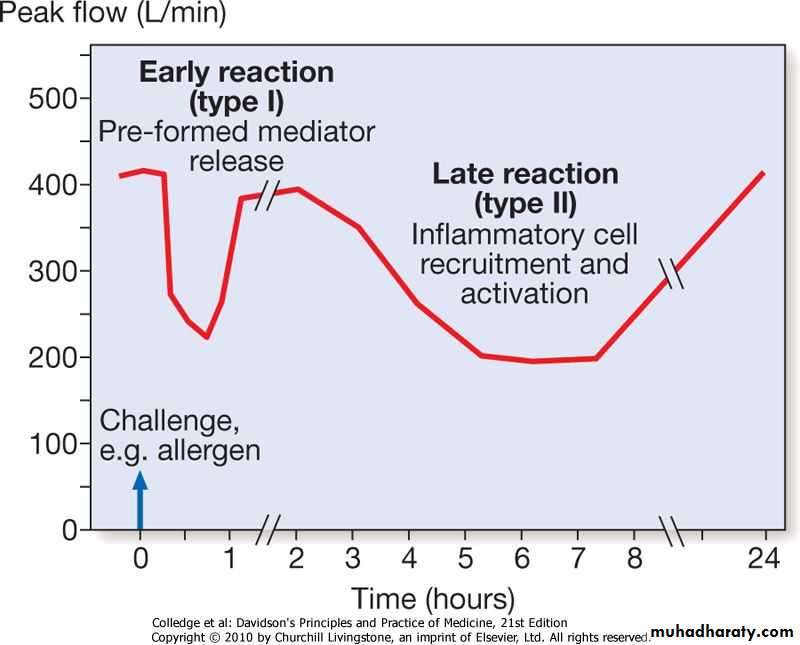
- early response(min)→ mastcell + IgE→ histamine → self limited
- late response(4-8h) → Ly, Np, Eo + IgG → persistent obstruction → beta-ago!
- dual response= both
{kind=link}
- wheezing
- dyspnea
- cough
- chest tightness
- concomitant eye+upper resp. tract symptoms
- Xray + spirometry normal (if no acute attack)
- NSHR - nonspecific hyperresponsiveness → trigger asthma attack with histamine→ decr FEV1 → pos decr. of FEV>20%
- Bronchodilator- test → give b2-agonist (salbutamol, albuterol, etc.) → what's the effect on FEV1 → if signif. incr. (≥12%, ≥200ml inc.) → positive
HISTORY!
Diagnostic criteria:
- symptoms only at/regularly after work
- improve on day off
- progression over week
- improve after change of work environment
Specific inhalation challange test (SICT) = gold standard → exposure to expected allergen
→ but expensive, special equipment, has to be in the laboratory
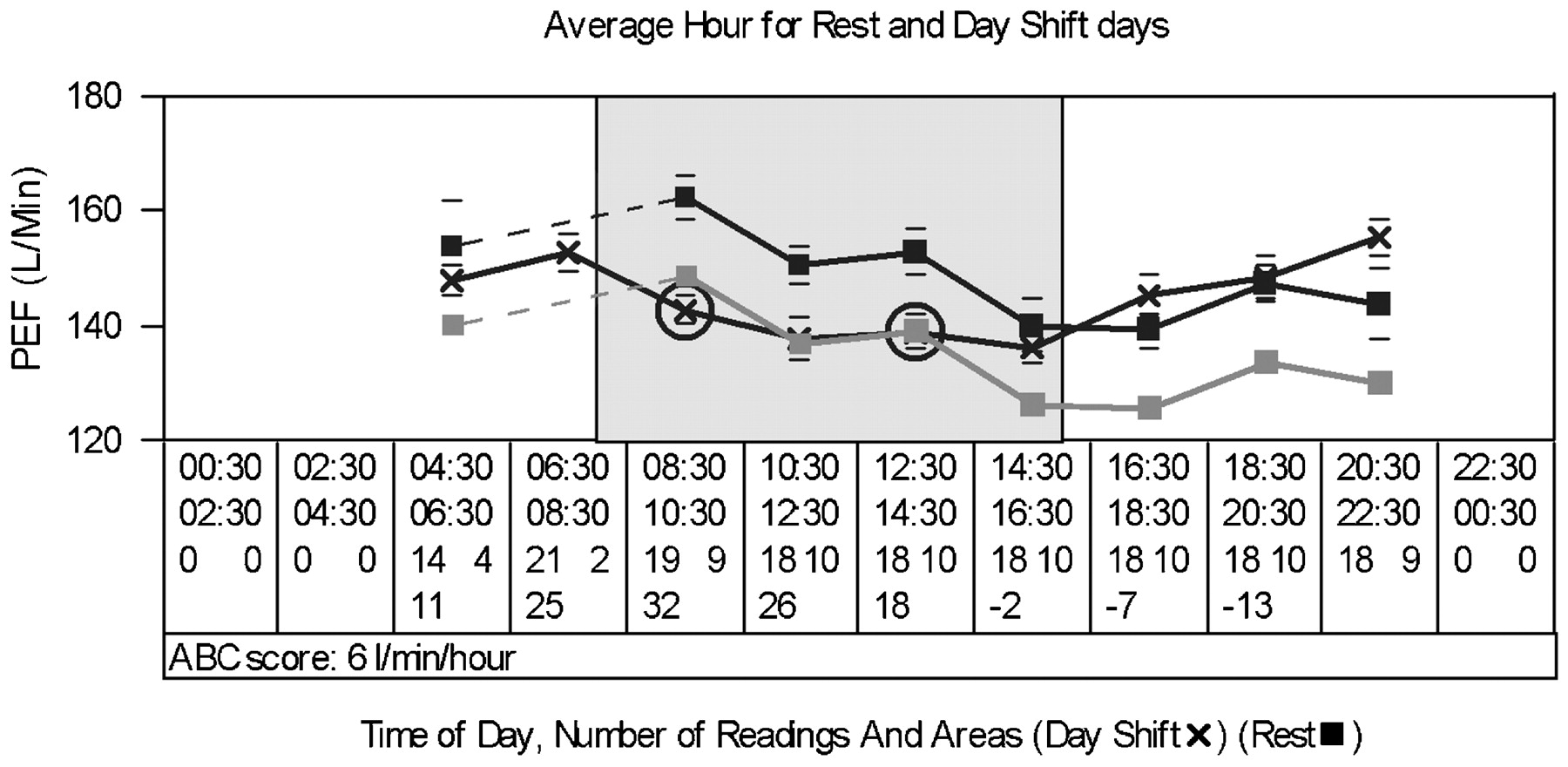
→ bring equipement to workplace → Across-work-shift spirometry(workplace challange)
→ but compared to SICT cant identify the specific agent + you need to send lab workers to the work place (good for large companies)
⇒ SERIAL RECORDING of PEFR(peak expiratory flow rate) 📷 is used most of the time → uses peak flow meter 📷 → patient can do that by himself and write a diary - 4x/day
{kind=link}
{kind=link}
→ allergen skin test + serological test (RAST,ELISA) might also be used in identifying the specif. allergic agent but they dont confirm the asthma dg.
- beta agonist (salbutamol)
- steroids
- O2
- Antibiotics
- ipratropium bromide
- he said: "acutally completely avoid exposure when asthma has developed in sensitizing-induced forms!"
- further lung function + monitoring
→ reduction only in irritant-induced forms
- Diisocyanates - coating, insulation, furniture - irritant mechanism + second. sensitizing mechanism
- Vegetable dust - cotton, → Byssinosis =monday syndrome (1-2 after return to work - milder on work-offdays)
- Metal salts - Platinum, Nikkel, Kobalt - electroplating, jewelry-making - Platinosis = asthma + rhinitis + urticaria
- Acid anhydrides - curing + hardening agents
- Wood dust - plicatic acid
- animal derived (high molecular weight)
- chemicals
- wheat
- latex
- dust
- vapour + fumes
Hypersensitivity pneumonitis is not relevant for the exam.
🏭 Pneumoconiosis
- interstital lung diseases after inhalting mineral dust - restrictive lung disorder
Types:
- collagenous (silicosis + asbestosis)
- non-collagenous (less severe collagen fiber proliferation and reticulin fiber proliferation instead → not so much destruction) - i.e. coal workers pneumoconiosis
→ collagen fiber proliferation in interstitium
<5 micrometer → respirable fraction
SILICA
- silica in crystalline form in rocks,sand
- burned silicates (800°C)
Inhalation of silicon dioxide (silica) in crystalline form (rock, sand) or silicates burned at high temperatures (over 800°C)
“I found (foundries) sand (sandblasting) on my (mining) window sill (silicosis)!”
- miners (gold)
- sandblasters + tunnel drillers
- foundry works
Occupations: miners (gold mines), sandblasters, foundry workers, tunnel drillers, quarry workers, stone carvers, ceramic workers, silica flour production workers
alveolar Macrophages take up silica particles in the alveoli → migrate into interstitium → can't destroy the particles → release cytokines → activate fibroblast + recruit Monocyte-Mp → collagen production + macrophageal alveolitis
⇒ 📷
{kind=link}
A silicotic lesion can be observed in the lung of a coal miner, displaying distinctive characteristics of a silicotic nodule. These features include an amorphous center with collagen fibers arranged in concentric patterns. It is important to note that the nodule is surrounded by coal dust. (coal dust + silica dust = double fuck)
⇒ 📷
{kind=link}
- chronic = classic, most common - ≥10y
- subacute/accelerated - 2-5y
- Acute - month
→ the more acute the more severe the exposure concentration
- upper + middle areas bilateral small opacities+(without affecting the apex)
- calcification of hilar lymph nodes → egg-shell calcification 📷
progressive massive fibrosis (PMF)
→ coalescence of small nodules → large fibrotic masses
- similar to chronic but:
- shorter exposure time
- great exposure conc.
- Progressive massive fibrosis more frequent!
rare
filling of alveolar spaces → starting from hilar lymphnode → to external areas (butterfly wing like) 📷
{kind=link}
nope ☠️
history of exposure + xray → confirms dg
xray → classification of radiography of pneumoconiosis (LAB!!)
+classic pulmonary symptoms esp. in PMF! → dypnea, decr. V, hypox
esp. in PMF:
- Chronic bronchitis
- Cor pulmonale
- Carcinoma (crystalline silica = carcinogenic)
- TBC + atypical mycobacteria
- fungal (crptococc, blastomycosis, coccidiodomycosis)
NO TREATMENT KNOWN
- prevention
- whole-lung lavage in ACUTE
Prognosis:
- good if removed from exposure
- bad in PMF+ACUTE form
chrysotile (90%) = white asbestosis
resistance master
- insulation materials
- roofing materials
- textile (heat resistance clothing)
- friction material (brake lining)
- cement
- mining
- fiber type + size
- exposure intensity + duration
- SMOKING 🚬
!long lateny
- Asbestosis >2microm in lenght
- Mesothelioma >5microm
- Lung Cancer >10microm
note: asbestosis may lead to mesothelioma or lung cancer as a long-term complication
lung cancer >15y after exp
mesothelioma >30y after exp
phagocytosis of fibers → cytokines + ROS → fibroblast proliferation → collagen esp. in pleura
- history with exposure
- dynspnea + unproductive cough
- bibasilar crackles (esp. posterolat)
- Pulmonary Function test
- decr. FVC, FEV1 + TLC- restrictive impairment
- Decr. DLCO (diffusion capacity carbon monoxide)
- Imaging
→ combination suggest interstitial lung diseases
NO TREATMENT
- surveillance
- smoking cessation
🧪 Toxicology
absorption, distribution, metabolism, excretion
3.5 half-lives
- battery manufacturing
- lead metal industry
- ceramic (tableware)
- drinking water
- paint (toys, walls)
- gas
- ammunition
- mining
- construction (sound, vibration attenuation, radioactive shielding)
ingestion or inhalation
- inhibition enzyms heme synthesis (ALA dehydratase + ferrochelatase) → inc. Protoporphyrin + ALA in RBC 📷

- free fraction → brain, kidney, liver, skin, muscles, placenta
bone matrix deposition
half-life 5-10years
- GI → lead colic (severe pain), tarry stool, constipation, general GI-symtoms
- variable CNS symtoms (headache, confusion, coma, seizures)
- renal failure in severe cases
- hypochromic Anema with basophilic strippling 📷

- Reticulocytosis (regenerative anemia)
- Incr. Protoporphyrin + ALA
40-80 microgram/dl
- 🧼 keep it clean
- clear eating areas
- shower + clean work clothes
- 🛡️ Personal protective equipment: use resp. protection (mask), coveralls, gloves, protective shoes
- 🩸 check blood lead levels
- remove from exposure
Chelation therapy
- oral Succimer
- +/- i.v. CaNa2EDTA (calcium disodium edetate)
- Neutropenia
- Rebound Elevation of lead after treatment
- GI
- Rashes
- kidney dmg (CaNa2EDTA)
aka Quecksilber
- seefood (like in minamata → "Minamata disease")
- manufacture control instruments, thermometers, batteries, barometers, electrical devices
- alkyl mercury in grain fumigants
- jewelry
- taxidermy (tiere ausstopfen)
- Felt industry ("mad as a hatter)
- Dentistry - amalgam (teeth filling)
mainly by vapor inhalation
(poorly absorbed by GI-tract except alkyl compounds)
- pulmonary symptoms (cough, dyspnoe, inflammation of airways(oral cavity))
- chemical pneumonitis (cyanosis, tachypnea, edema)
- renal failure (inital diuresis)
- neurolgic symptoms (see chronic)
- Neuropsychiatric
- change in personality
- anxiety, memory loss, emotional lability
- progressive hand tremor
- head tremor + ataxia
- distal paresthesias
- hallucinations + dementia
- Others
- oral cavity inflammation
- blue pigmentation of teeth + gum
- excessive sweating + skin eruptions
- xray: infiltrated in chemical pneumonitis
- proteinuria in renal injury
- Mercury level in blood and urine:
- >0.01mg/l in blood
- 50-150 microgram/g crea in urine → subtle NS + renal effects (normal <10microg/g crea)
- >500 microg/g urea severe NS+renal effects
- control of industry
- proper ventilation + resp. protection
- proper handling + disposing
- medical surveillance (neurologic exam, monitoring mercury levels)
- treat renal + resp symtoms
- Chelation therapy:
- i.m. dimercaprol (BAL)
- oral: Penicillamine
dissolve other substances → organic (hydrocarbon-based)
→lipid soluble
mainly inhalation (→incr. retentation rate with physical labor)
can also enter percutaneous bec. lipid soluble aspect → check gloves+clothing if it might run under it,
- lipid rich (CNS, liver,fat)
- large blood flow (heart, skeletal m.)
- placenta cross + breast milk!
→ exhalation (primary) or urine
half-life vary widely but a lot very short → take samples directly after work(week)(minute - days)
- 20% of occupational dermatitis caused by organic solvents due to lipid solubility
- most common mechanism: mainly washing hands with solvents
- acute: erythema + edema
- chronic: dry + cracked eczema 📷 → +/- bacterial infection
- therapy: corticosteroids + emollients
- prevention: esp. education
- anestetic, depressive (due to lipid solubility)
- like being drunk
= drinking alcoholic beverages (headache, nausea, vomiting, dizziness, light-headedness, vertigo, disequilibrium, slurred speech, euphoria, fatigue, sleepiness, weakness, irritability, nervousness, depression, disorientation, confusion, loss of consciousness, death).
- chronic toxic encephalopathy
- personalality, mood change, impaired intellectual function, decr. short term memory + psychomotor → Swedish Q16 questionnaire 📷 for long-term solvent-exosed workers
- sympathetic symptoms
- symmetric, ascending, sensorimotor neuropathy
- trigeminal nerve anesthesia
- color vision decr.
- decr. of olfactory funct.
→ slowly ascending numbness, paresthia, weakness
→ decr. sensation + strenght
→ depressed distal reflexes
- “Carbon disulfide, hexane, and methyl n-butyl ketone are toxic substances used in industrial settings.
- Symmetric, ascending, mixed sensorimotor neuropathy
- Trichloroethylene - trigeminal nerve anesthesia
- Acquired color vision disturbances - toluene, styrene
- Disturbances of olfactory function - long-term painters”
- upper airway irritation (esp. formaldehyde)
- asthma+COPD exacerbasion + RADS (react. airway dysfunc. syd) =irritant induced asthma
- !special: phosgene gas exposure from welding of metal parts that were treated previously treated with chlorinated hydrocarbons→ acute pulmonary edema
{kind=link}
- "cardiac sensitization" → incr. sensitivity to arrthymogenic effect of epineph
- identifiedy due to cases of sudden death from worker exposed to toluene from glue, trichloroethana in spot remover → arrhytmia induced
- if not death → dizziness, palpitation, faint, low BP, irregular pulse
- ECG + physical normal at rest! ⇒ holter monitor during exposure
hepatotoxicity → acute hepatic necrosis (paint products (2-nitro-propane)+ carbon tetrachloride)
- mainly asymptomatic
- abormal liver function test (ALT+AST)
→ DD: alcoholic, inf. hepatitis
- ingestion etyhlene glycole → oxalic acid deposition (ethylene glycol-anti-freeze) → Acute renal failure (ARF)
- exposure halogenated hydrocarbons (carbon tetrachloride) →halogenated hydrocarbons(carbon tetrachloride) → Acute tubular necrosis (ATN) → ARF
note: carbon tetrachloride(halogenatied hydrocarbons)=, liver + renal failure)
chlorinated hydrocarbons → pulmonary edema(acute)
- mainly due to benzene + chlorinated hydrocarbons = carcinogenic
- glycol ethers → hemolytic + hypoplastic anemia
- ⇒ weakness, fatigue, bleeding infections
- reduction in the 3 cell lines
- hypo- or hyperplastic bone marrow
→ aplastic anemia → leukemia
note chlorinated hydrocarbon also in pulmonary edema
→ see also movie
- benzene +chlorinated hydrocarbons→ leukemia
- halogenats hydrocarbons → hepatocellular Ca in mice
- solvent-mixture → synergistic effect: incr. rate of different cancer types
- indirect: incr. skin absorption of other carcinogens
- cross placenta → malformations + abortions
- dec. fertility
- "fetal solvent syd" → hypotonia, retardation, poor postnatal head grwoth
- incomplete burning of carbon-based fuels → garage workers, petroleum refinery, furnace jobs, firefighters
- methylene chloride vapor (mainly from industrial emission)
CO avidly binds to hemoglobin → carboxyhemoglobin (COHb)→ ↓oxygen carrying capacity & ↓ release of oxygen from Hb
⇒ 📷
{kind=link}
⇒ 📷
{kind=link}
- headache
- drowsiness
- breathing rate abnormalities (dyspnea + tachpnea)
- blurred vision
- unconciousness, death
30% COHb = moderate to severe symptoms;
50% = can be lethal;
(4-7%)<10%
- CO alarms
- proper ventilating
- combustion (burning) engines outdoor
- remove!
- give O2
- hyperbaric chamber
- colorless liquid (or gas when mixing with acid)
- bitter almond odor (often odorless)
- precursor to many chemical compounds ranging from polymers to pharmaceuticals.
- high potentcy + rapid onset of toxicity
{kind=link}
inhalation, ingestion, dermal, (i.v)
- metal plating operation
- extraction silver + gold ores

- plastic production
- electroplating + metallurgy
- Nitroprussid - drug in hypertensive crisis (NO oxide release)
{kind=link}
blocks aerobic mitochondrial metabolism: binds to ferric iron in cytochrome oxidse → anerobic metabolism → lactic acidosis
low level:
- dypnea (+ initially hyperpnea)
- mild CNS (headche, dizzy, confusion)
- GI
high level:
- loss of conciousness
- seizures
- resp. depression + cardiac arrest
- death
thiocyanate in urine
(in blood only forensically ☠️)
- avoid mixing cyanide salts with acid → turns into gas
- avoid skin contact
- Nitrites (triggers methemoglobin → combines with cyanide → cyanmethemoglobin (sparing cytochrome oxidase)
- Sodium thiosulfate (cyanite → thiocyanate→renal excr.)
- hydroxocobalamin (→cyanocobalamin (VitB12))
1) Nitrate + Oxyhemoglobin ⇒ Methemoglobin
2) Methemoglobin + Cyanide ⇒ Cyanmethemoglobin
💪🏽 Musculoskeletal Disorders
overuse
- muscles
- bone
- ligaments, tendon, cartilage
- nerves
- too heavy load - for short time
- lighter load - but for a too long time (also most of work time)
3. verly light load - repetetive (incr. frequency)(cashiers)
4. incorrect posture - long time
5. no load - monotonous repetive movement (keyboard)
6. Static contraction (load) - no movement 📷
{kind=link}
7. Muscle inactivity - poor physical cond., joint instability + motor incoordination
8. Vibration (hand-arm / whole body)
Neck Tension Syndrome
awkward posture
static contraction (computer)
{kind=link}
- holding a load over shoulder (loading/unloading)
- holding vibration (drilling in mining, construction)
- repeated flexion + abduction >60° (automobile mechanics, swimmers, basketball)
- pain → radiates in upper limb
- contraction (tension)
- functional impairment → dec. act+pass mobility
- xray → nothing
- MRI + US !
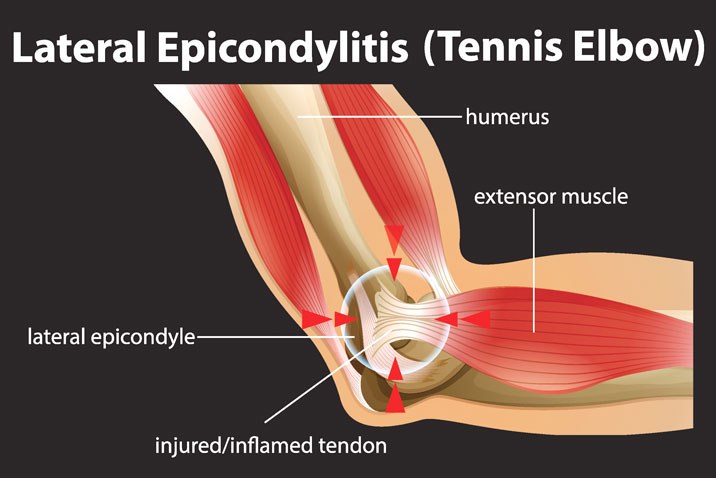
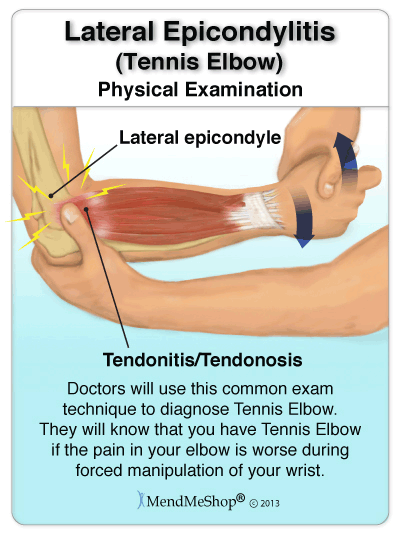
epicondylitis - tendons or periosteal inflamation at humeral epicondyle
- dorsal flexion, flexion, pronation, supination movement
- esp. when arm in extension
- construction, butcher,tennis player
tennis elbow 📷
{kind=link}
= lateral humeral epicondylitis
- pain with movement → esp. against resistance + with supination/pronation
- swelling, redness, heat (inflammatory signs)
- tender to compression
- US → thick tendon
⇒ 📷
{kind=link}
Pain, signs of inflammation, functional impairment gets better by activity and worse with rest
- inflammation tendon sheath + tendon in the wrist 📷
→ liquid in sheaths
winker + schnapper
- repetetive flexion-extension hand+fingers
- prehension thumb-other fingers repetitive pronation-supination
→ packers, fitters, crop pickers, tailors
firm tendon
pain, crepitus
- De Quervain tenosynovitis
- Trigger Finger
tendonsheats of long+short extensor & long abductor of thumb inflammed due to repetetive prehension movements (greifen) 📷
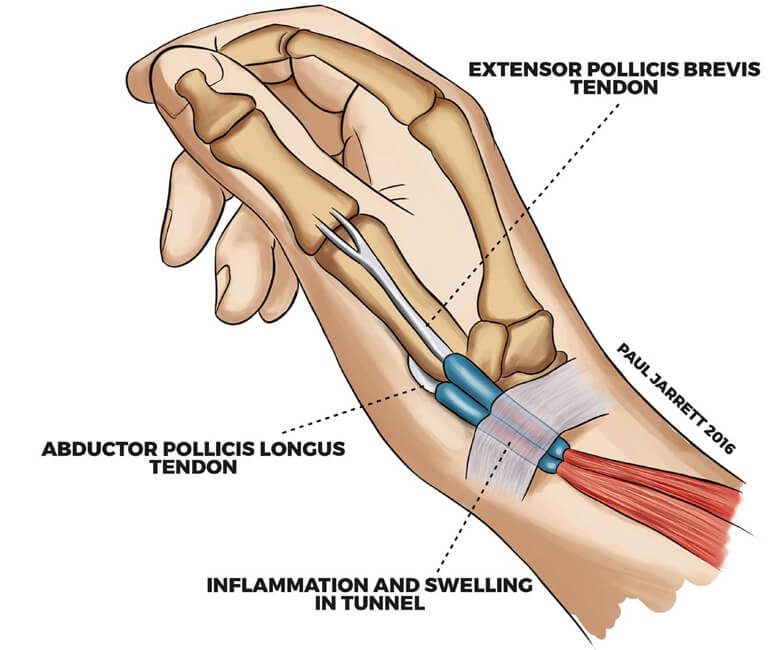{kind=link}
Finkelstein test 📷
{kind=link}
= stenosing tenosynovitis of flexor tendon of one finger
- flexing of prox IP-joint - when trying to extend a certain force is needed → sudden snap into extension
- Nodule at Metacarpal-phalangeal joint
repetetive hyperext + hyperflexion with flexed fingers
→ automobile assembling, packers, ..
{kind=link}
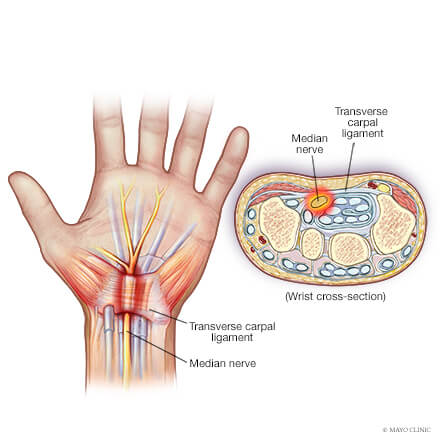
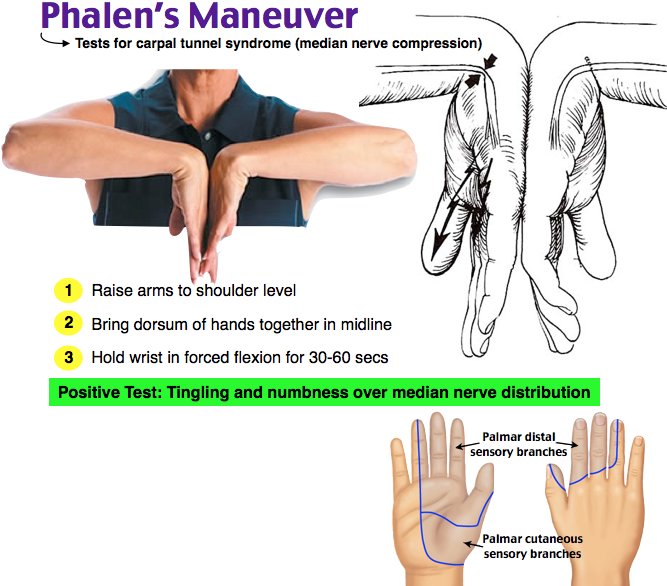
- carpal tunnel deliniated by carpal bone + transverse carpal lig
- contains median nerve + flexor tendons
→ overuse flexor tendon → inflammation → incr. P in carpal tunnel → pressure on median nerve → might lead to fibrosis + atrophy
- pain
- signs of inflammation (swelling, red, heat)
- paresthesia of finger 1-3
- worse at night
→EMG + Nerve conduction studies
{kind=link}
{kind=link}
acuet back pain
pain radiates into lower limbs - involvement of sciatic nerve
- heavy load
- lifting weights
- bendig + twisting
- long time static posture
→ but multifactorial!
- muscle contraction (tension)
- disc diseases (hernia, prolapse) → might lead to sciatica
→ MRI+surgery
- movement restriction
- heat (only in minor lesions)
- ice (anti-inflammatory + anti-swelling)
- Kinetotherapy
- steroids + NSAIDS
- surgery
- Hip
- Knee
🪖 Physical Hazards
hypothalamus
→ muscle tone
→ vascular tone
→ sweat glands
- indoor: steel, oven, glassblowers
- outdoor: construction, farmer
radiation - mainly (65% under normal condition)
!limited when sourrounding exceeds bodyT
evaporation (20% normal condition
→ important at excessive temperature
!limited by incr. humidity
important to prepare the body to exposure to incr. temperature
controlled exposure for shorter periods of time and incr. exposureT slowly
⇒ sweat at lower T, incr. sweat production, decr. salt in sweat, incr. plasmaV+cardiac output wh
extreme heat + low heat dissipation capability (elderly, children, ill)
exertional form → exercise in hot environment
- changes in mental status =hallmark
- coreTemp >41°C
- Hypotension (due to vasodilation)
- dry+hot skin (absence of sweating due to failure of thermoregulation)
conc urine + blood
decr. electrolytes
- hemoconc.
- conc. urine
- leukocytosis
- decr. electolytes
cool that MF down! 📷
{kind=link}
→ cool place, remove clothing, wet sheets/ice-packs/ice-water
- correct fluid + electroly.
- O2
- vital support (ABCDE)
- hypovolemic shock
- renal failure due to - rhabdomyolyis + hypovolemia
- cardiac failure
- respiratory distress
- hepatic failure
- body T normal/incr. but <40°C
- incr. heart rate
- moist skin
- THIRST
- less CNS symptoms
→ might develop into heat stroke if incr. T or decr. sweating
{kind=link}
SODIUM DEPLETION
- sweat losses only replaced by water
- during strenous muscle work → slow mainful spasm/contract. (1-3min)
- moist + cool
- hard → "billiard balls"
- cool environment
- i.v. salt solution or oral saline solution
cutaneous vasodilation → systemic + cerebral hypotension → sudden unconsciousness
occurs after strenous work (at least 2hr)
- cool + moist skin
- weak pulse
- BP<100mmHg
→ lay down, cool, liquids
whole body + hand-arm
- truck + bus driver
- heavy equipment operators
→ Freq <20Hz
Vibration sickness
→ gastrointestinal problems
→ decr. visual acuity + labyrinthine disorders
→ musculosceletal pain
→ HT
- demyelinating periph. neuropathy
- degeneration of hand+finger bones +joints
- excess CT deposition
- arterial wall muscl hypertrophy + microvasc. occulusion
→ vibration induced white finger disases (hand arm vibration syndrome) vasospasms = raynauds synd. (Freq 125-300Hz)
early: tingling + numb finger
white → blue (cyanotic) → red (react. hyperemia)
→ history + response to cold (thermography, finger BP, etc.)
- idiopathic raynauds disease
- other causes for second. raynauds synd:
- vasculo-occulusive
- CT disorders (SLE)
- thoracic outlet sy
- drug intox (beta-blockers)
- gloves
- work-rest schedule
- education about early signs
- no smoking
- shake hands or put in warm water
- Nifedipine (Ca-channel blockers)
- sympathectomy
- stop vibration exposure
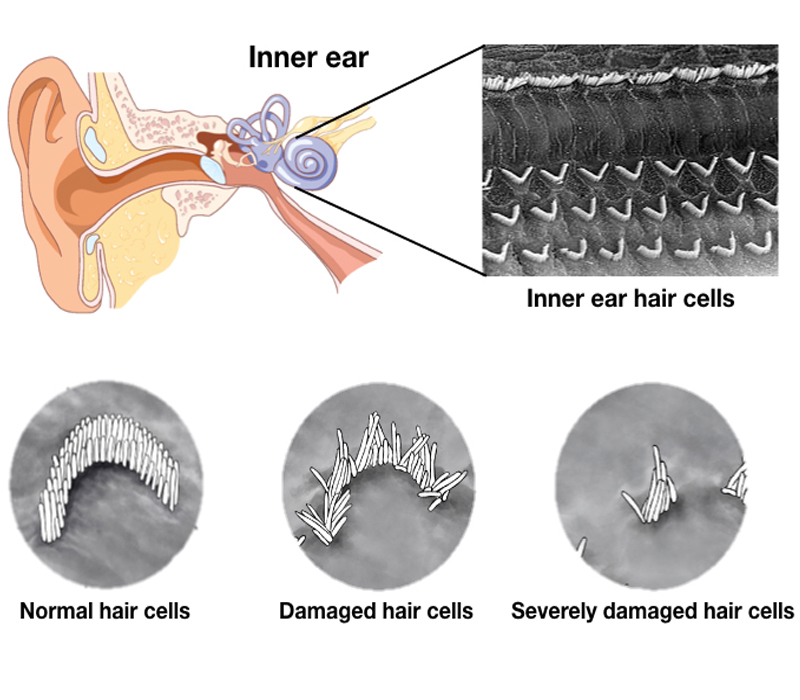
>85dB
only in early temporary threshold shift
- Initially, changes are potentially reversible (temporary threshold shift).
- Permanent threshold shift - no recovery (audiometric tests after a 12-24 hours recovery period).
→ 📷
{kind=link}
- gradual difficulty comprehending speech + high pitches voices
- Tinnitus intermitted/continous (exacerbated by noise)
{kind=link}
→ "4000Hz notch" 📷
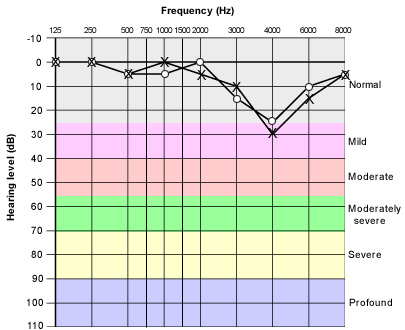{kind=link}
500-3.000Hz → affected in prolonged + late stage diseases
Probably not
hearing loss is usually bilateral + symmetric
exception call center
- monitor noise at workplace
- educate workers + control engineering+administration
- use hearing protectioin
- periodic audimetric evaluation
- no medical+surgic. treatment
- Remove → stabilization possible
→ only hearing amplification 📷
→otherwise: deafness
- Radiation