







Radiology I
- Radiology I
- ⛲ General 🔒
- 🦴 Musculoskeletal system
- 🥐 Urinary system 🔓
- 🥣 Retroperitoneum, Pelvis, Breast 🔓
- 🚑 Emergency Radiology 🔒
- 👶🏽 Pediatrics 🔒
- 🛡️ Radiation Biology & Protection 🔒
⛲ General 🔒
🦴 Musculoskeletal system
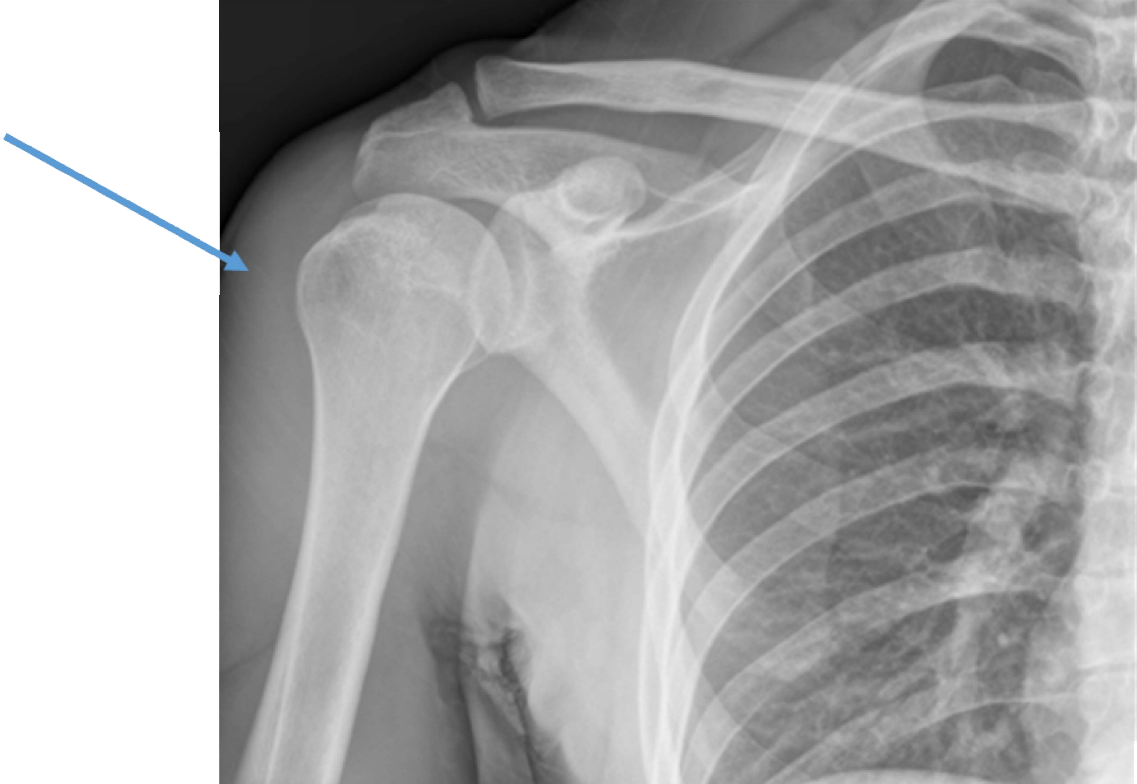
xray
- Epi, meta, diaphysis
- Cortical + medullary part
- Bone alignment in joint + joint space
- bone + joint lesions
{kind=link}
nopedidope
trauma (esp. soft tissue involvement) + tumor
evaluate vertebral fractures → also reconstruction for surgeon
contrast into jointspace → xray 📷, CT, MRI
{kind=link}
not really used nowaday
shoulder, rotator cuff
oseochondral bodies, cartilages, joint
{kind=link}
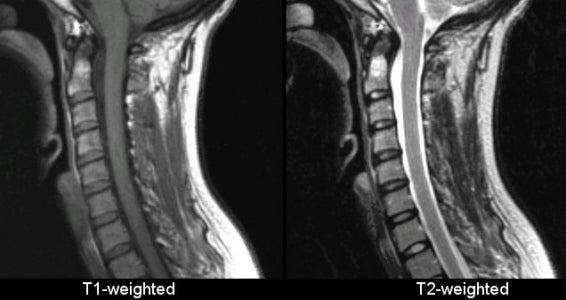
- joint spaces, cartilage
- ST in great accuracy
- BONE EDEMA (only with MRI) → early diagnsis of RA, inflam/autoimmune disease
hyperintense
compact bone, air
{kind=link}
Primary
- turning of connective & cartilaginous tissue into bone - imature bone
Secondary
- destruction & remodelling - adult bone
{kind=link}
skull + face
connective membrane → bone in a centrifugal manner (spreading from inside to outside)
{kind=link}
{kind=link}
PTH, VitA, Cortisone, Calcitonin (in high dose), low P-Calciuminput, immobilization, acidosis
Somatotropin, Insulin, Vit D, Andro/estrogen, calcitonin, Vit C, excess P+Ca, incr. water input, Stasis
medullary canal, compact bone at the periph. 📷
{kind=link}
spongious central
cortical in the periph
nope, only in pathological conditions (see later)
joint spaces or growth plates(betw. epi+dia)
PLASIA (hyper-,hypo-,aplasia/agenesis)
anostosis
hypostosis - osteolysis
hyperostosis - osteosclerosis or periostosis
also more radioopague due to more cortical bone
oedostosis = focal balooning
central destruction + periph. periostosis
Loss of mineral content, protein matrix intact

can be generalized, regional or localized
second most common diseases, after arthrosis/osteoarthritis
→ mainly spine
Axial skeleton, pelvic bones, proximal long bones
- incr. transparency - only obtainable when 30-50% mineral loss
- cortical thinning → incr. central canal diameter
- Abnormal trabeculation:
→ loss of spongy bone blades + hypertrophy of the remaining

{kind=link}
"glass bones"
severe thinning → same transparency as soft tissue around
{kind=link}
inc. transparency + hypertrophy of the remaining spongy bone plates
{kind=link}
{kind=link}
nerve dmg → distal atrophy → spotted osteoporosis on xray
trauma → nerve injury
- progressive pain
- swelling
- atrophy distal to trauma
{kind=link}
trauma, palsy, inflammatory diseases (rheumatoid arthritis)
- whole bone
- spotted on bone (öike algoneurodyst)
- BAND
- subcortical osteoporosis
{kind=link}
“bands” of bone thinning running from left to right covering the area over and around the joints. in between normal (not thinned) bone.
Arthritis, tumor, infection
bone tissue + density lost
→Loss of mineral content
→Proteic matrix is destroyed as well (not in osteoporosis)
no proteic matrix → no bone healing
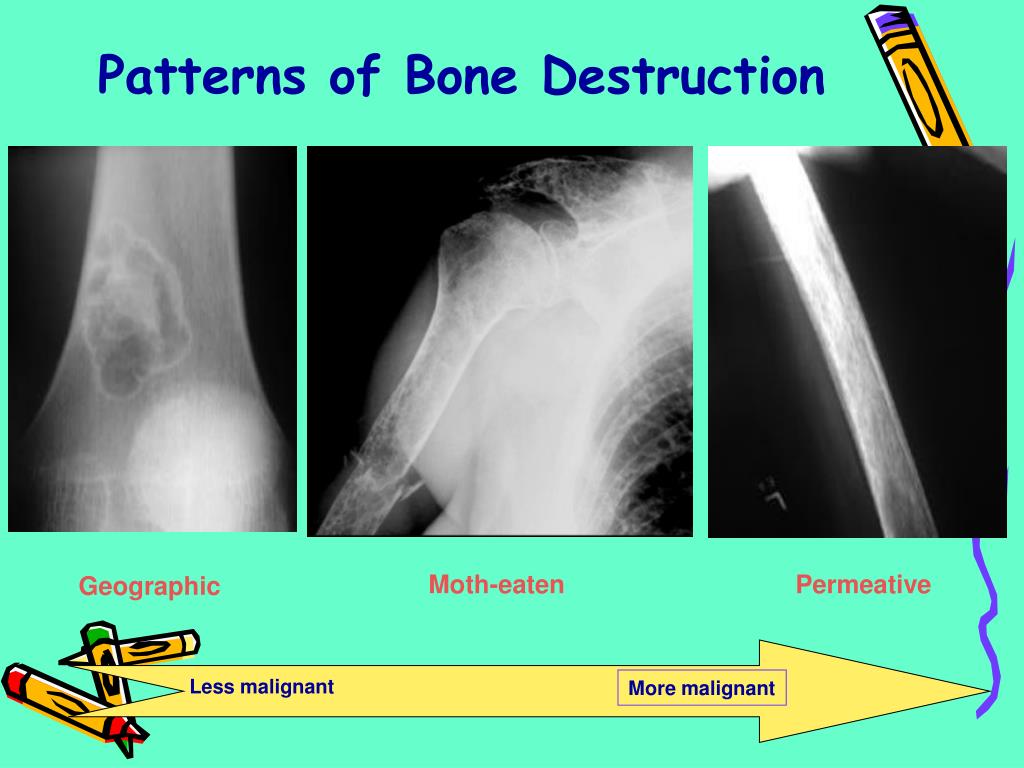
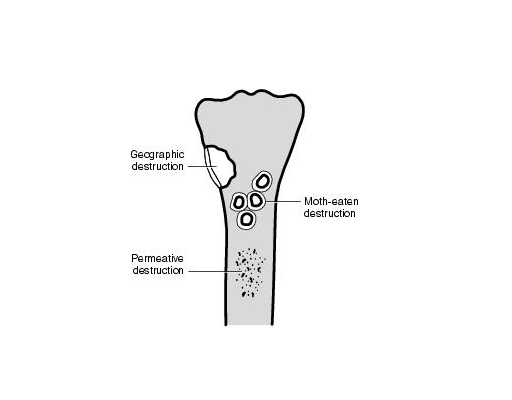
Attrition (wear) Erosion Caries
superficial = compact bone deep = spongy
{kind=link}
well circumscribed
- multiple small lesions
- blurred margins
- tendency to merge
agressive process → metastasis, osteomyelitis
{kind=link}
{kind=link}
{kind=link}
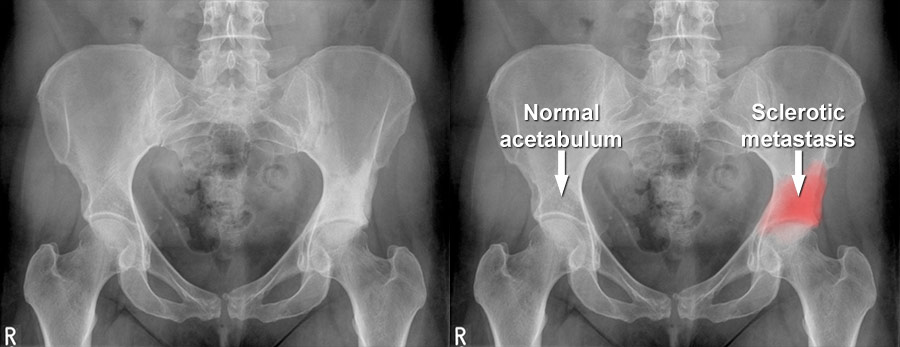
prostate cancer metastasis
snowball
{kind=link}
{kind=link}
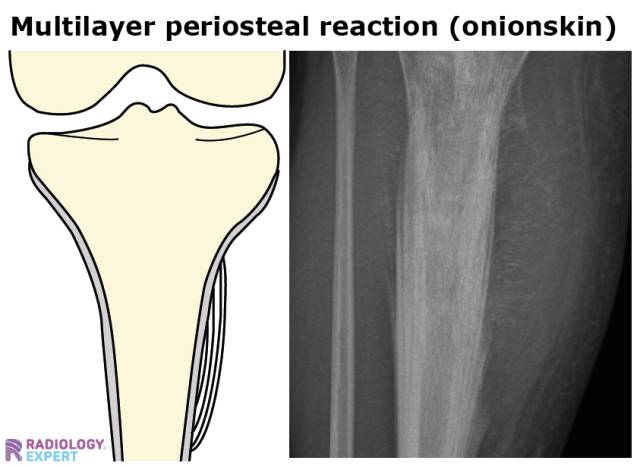
bone produced by periosteum → hyperostosis
only diaphysis + metaphysis → not at epiphysis
infections + tumor
benign
infections + malignant tumors
heterotopic = bone production where it shouldnt be
originate in bone next to any joint, where capsule inserts
{kind=link}
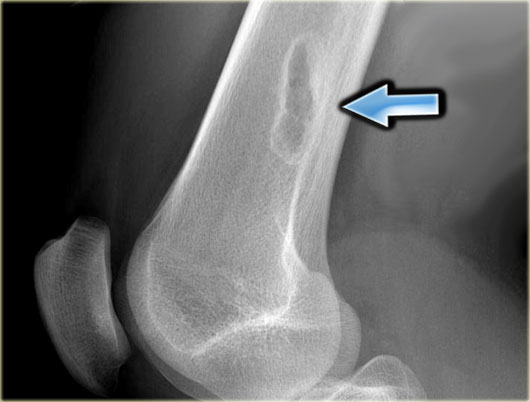
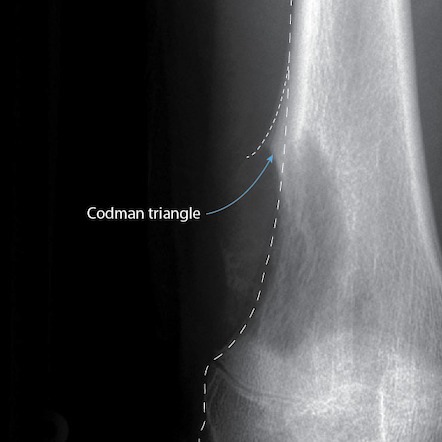
- Triangle: base-bone, tip -distally
- Covered by cartilage (not seen on xray)
- may form Bridges between bones
degenerative osteoarticular diseases ⇒ Arthrosis
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
epiphysis
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tissue of Origin | Benign | Potentially Malignant | Malignant |
Bone | Osteoma, Osteoid Osteoma, Osteoblastoma | - | Osteosarcoma |
Cartilaginous | Chondroblastoma | Chondroma, Osteochondroma | Chondrosarcoma |
Connective | Fibroma, Myxoma | Giant cell tumor (mieloplaxe) | Fibrosarcoma |
Vascular | Hemangioma, Aneurysmal cyst | - | Angiosarcoma |
Reticuloendothelial | - | - | Ewing Sarcoma |
Hematogenous Marrow | - | - | Plasmocytoma |
Adamantine | Adamantinoma | - | - |
- multiple myeloma
- chondrosarcoma
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- facial sinuses (esp. frontal sinus)
- or surface of skull
- opacity
- bell clapper appearance (”hanging on a pedicle”)
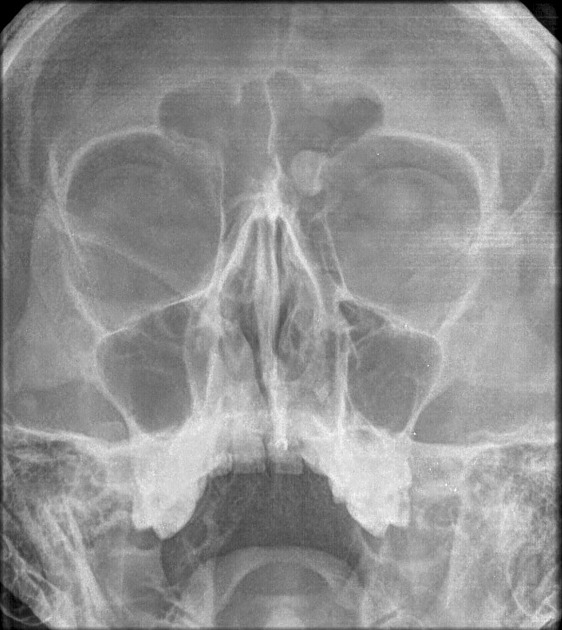{kind=link}
osteoma located in left frontal sinus just next to the left eye (bell clapper appearance → hangs on pedicle)
{kind=link}
{kind=link}
{kind=link}
Cartilaginous origin:
mature hyaline cartilage in medullary cavity
long bones
- enchondroma →in medullary canal
- Ecchondroma →on surface of bone
- multiple enchondromatosis → greater chance for malignancy
{kind=link}
{kind=link}
{kind=link}
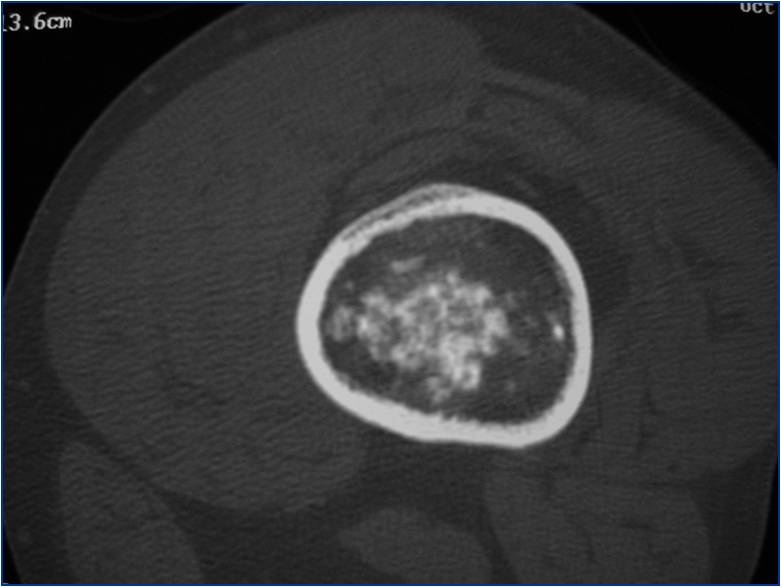
hypodense fat, less hypodense cartilage, central calcification
still hypodense - osteolytic parts (actually no fat like on the image)
and more hyperdense cartilage
with most hyperdense calcifications
{kind=link}
Cartilage nodules grow from periostum
45% of all benign TU
metaphysis close to epiphysis
when they are multiple
{kind=link}
{kind=link}
{kind=link}
Metaphysis long bone
Around knee away from elbow (=distal femur+prox. humerus)
osteolytic, osteogenic, mixed
- diffuse or localized destruction
- cortical osteolysis cortical bone destroyed
- ST swelling
- Malignant periostosis (Codman triangle, spiculated)
{kind=link}
- bone matrix assessment
- tumor extent
- staging - metastasis in other organs?
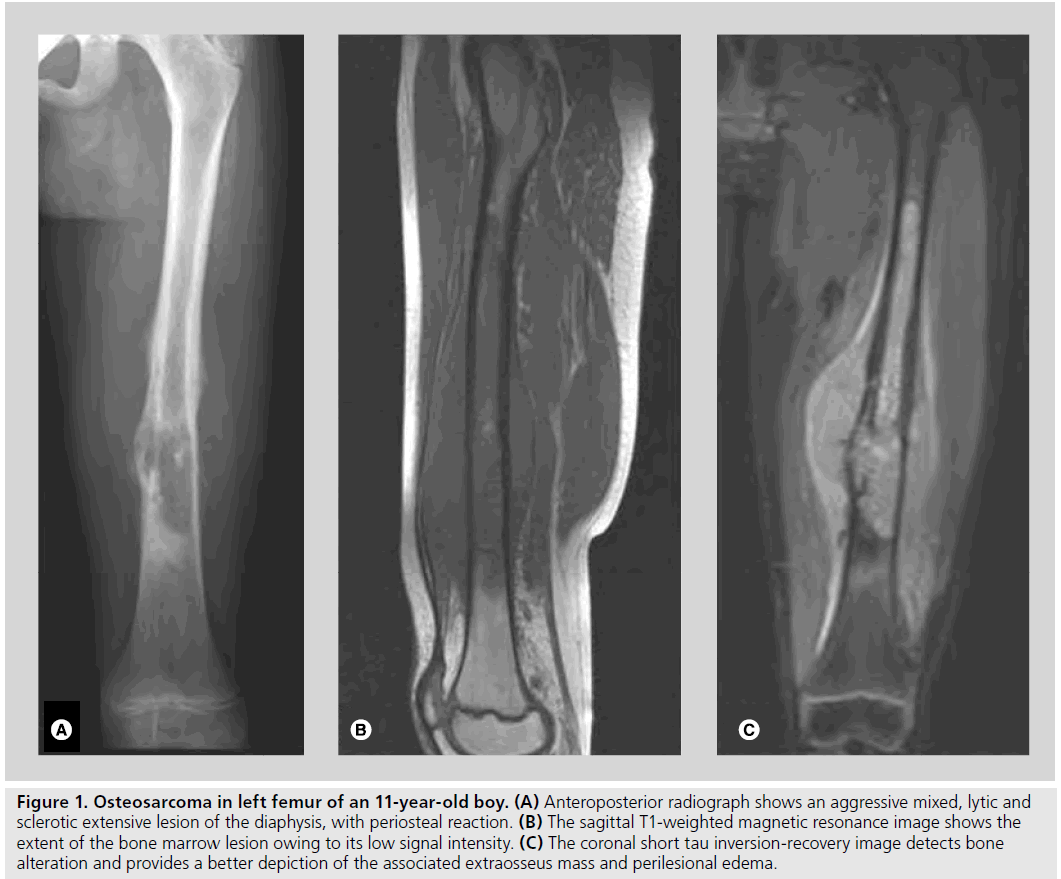{kind=link}
shows more clearly the extension in the central canal + soft tissue
{kind=link}
- malignant periostosis (spur or spicules)
- ST invasion
- sunburst / lighthouse in the fog (not necessarily)

evaluation bone matrix, invasion
central - in central canal
peripheral
illiac bone > proximal femur > prox. humerus > distal femur
{kind=link}
{kind=link}
extension
differentiation with osteosarcoma → messure cartilage → >2,5cm → chondrosarcoma
plasma cells, bone marrow
→ most frequ. malignant primary bone tumor
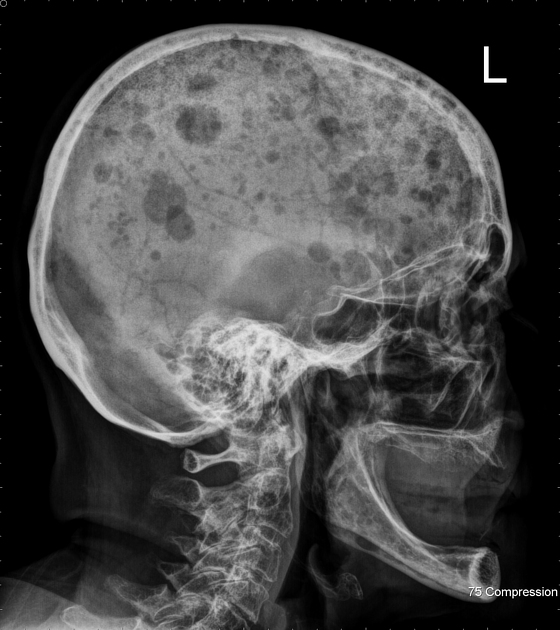
hematopoietic sites → vertebra, ribs, iliac, femur, skull
Bence-Jones-Proteins , proteinuria
{kind=link}
{kind=link}
{kind=link}
spine, pelvis, ribs, skull, prox long bones
{kind=link}
vertebral sagging - wedge shaped → leads to spinal canal compression
also all other forms of mottled, permeative..
- Osteoporosis
- Metastasis
- Trauma
- Staph aureus (75 %)
- Streptococci; other germs
hematogenous
direct seeding → open fracture /iatrogenous
contiguity = soft tissue infection → penetration
not very symptomatic. fever, pain
basically nothing
Increased soft tissue opacity Thinning of adipose tissue
- periostosis
- focal bony lysis
- evtl .peripheral sclerosis
- osteoporosis
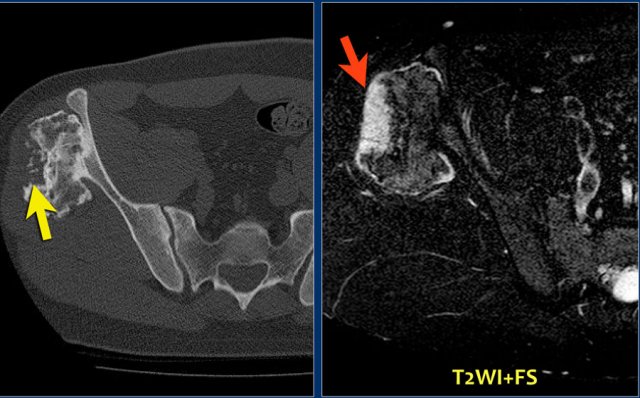
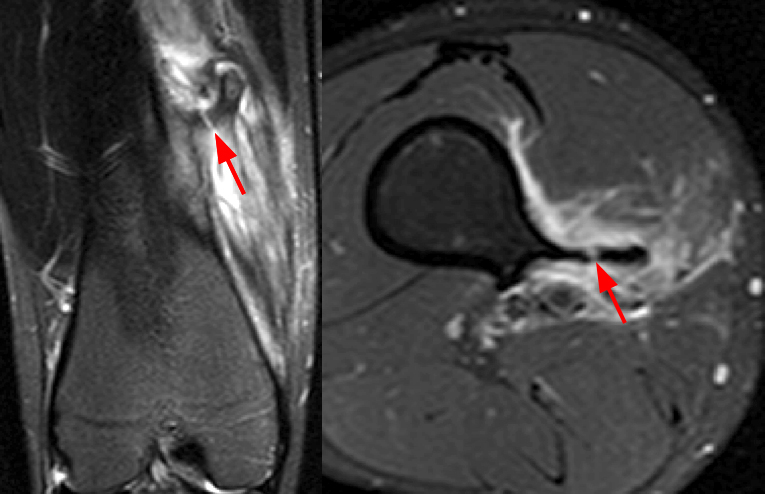
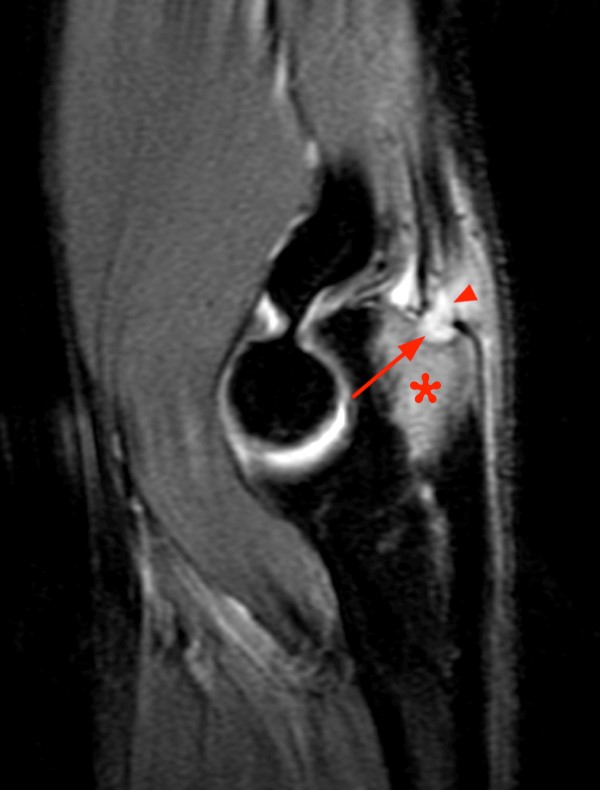
MRI + US to assess the softtissue
- edema in soft tissue + bone marrow (hypoT1, hyperT2)
- incr. uptake Ga uptake due to infection
- soft tissue edema = paraosseous hyperT2
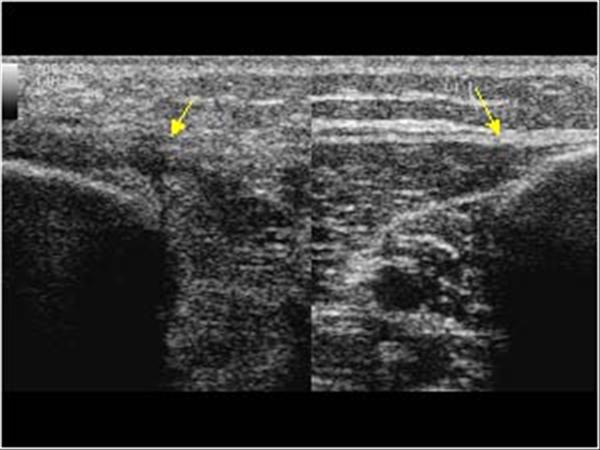{kind=link}
edema, periosseos abcessess, periostosis
{kind=link}
- sequestrum is characterist for chronic
- single bone, single place
- → only METAPHYSIS + DIAPHYSES
- NEVER EPIPHYSIS NOR JOINTS
- Triad: Osteosclerosis, Periostosis, Hyperostosis ⇒ very characteristc for chronic osteomyelitis
Mainly for better imaging of sequestration
- Sequestration
- Cortical thickening
- Fistulae - fistulography
- Soft tissue abscess (+- contrast)
{kind=link}
Bone Whitlow
Softtissue infection → extends to the bone → destroys periostum (Surface osteolysis)→ Then into bone: osteolysis
{kind=link}
→ because periosteum gets destroyed: NO PERIOSTOSIS
- extension to joints → septic arthritis
- pathological fracture + healing
- Limb deformity (shortening)
- if next to growthplate → stimulation of the growthplate → paradoxical lengthening
{kind=link}
mainly staph., pseudomonas (gas bubbles on ct)
hematogenous direct contiguity
- General: Hematopathies, diabetes, cancer, chronic renal failure, immune deficit, drug abuse.
- Local: Rheumatoid arthritis, osteoarthritis, trauma, microcrystal arthritis, neuroarthropathy.
can be in any joint
Most Frequent:
- Hip in kids
- Knee in adults
- SI or sternoclavicular in diabetes, HIV, drug abuse.
normal
{kind=link}
- effussion intraarticular
- periarticular osteoporosis
- joint space narrowing
- blurred cortical bone, erosion → subcondral bone destruction
- +/- osteomyelitis
- ankylosis (rare endstage)
not really used
only when we are uncertain about Rx or to guide interventional procedures
soft tissue mass with gas bubbles → abcess+pus+gasforming germs (anerobic e.g.chlostridium)
{kind=link}
{kind=link}
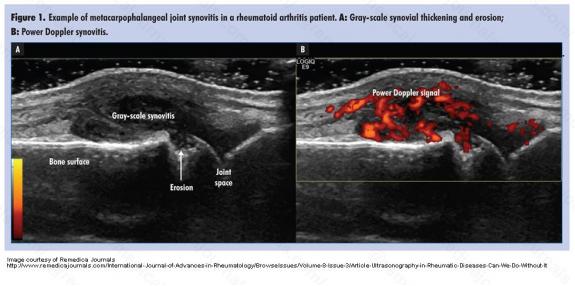
- fluid effusion
- thickenend synovial membrane
- due inflammation but not infection → autoimmune
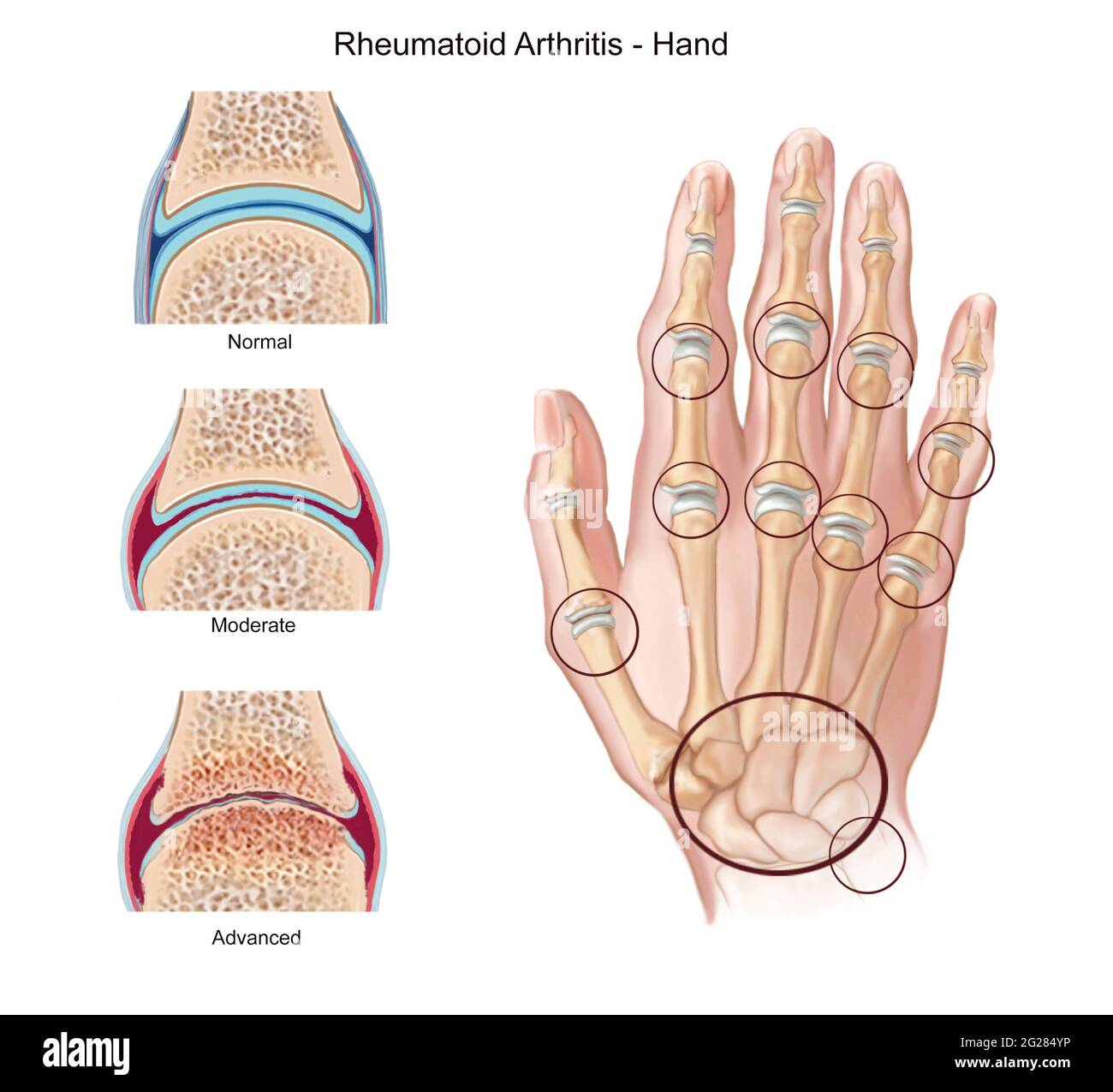
- Mainly in the hand: involve small joints of extremities
- systemic diseases
Female 3:1 Male
{kind=link}
- bilateral (might be unilateral in beginning)
- ALMOST NEVER DISTAL INTERPHALANGEAL JOINT
- MCF: 85%
- Carpal: 80%
- PIPh: 75%
- Classic: symmetric (unilateral in early stages)
- Early: MCP, distal RUD, RC
- Late: PIP, IC
- DIP almost never involved!
Location:
- morning stiffness
- pain
- swelling → swelling of further joints
- swelling is BILATERAL
- typical xray
- nodules
- positive rheumatic factor
mccarpal, prox. interphalangeal, etc..
NOT distal interpahlangeal joints!
- erosion → osteoporosis
- joint alignment changes. luxation + ankylosis
{kind=link}
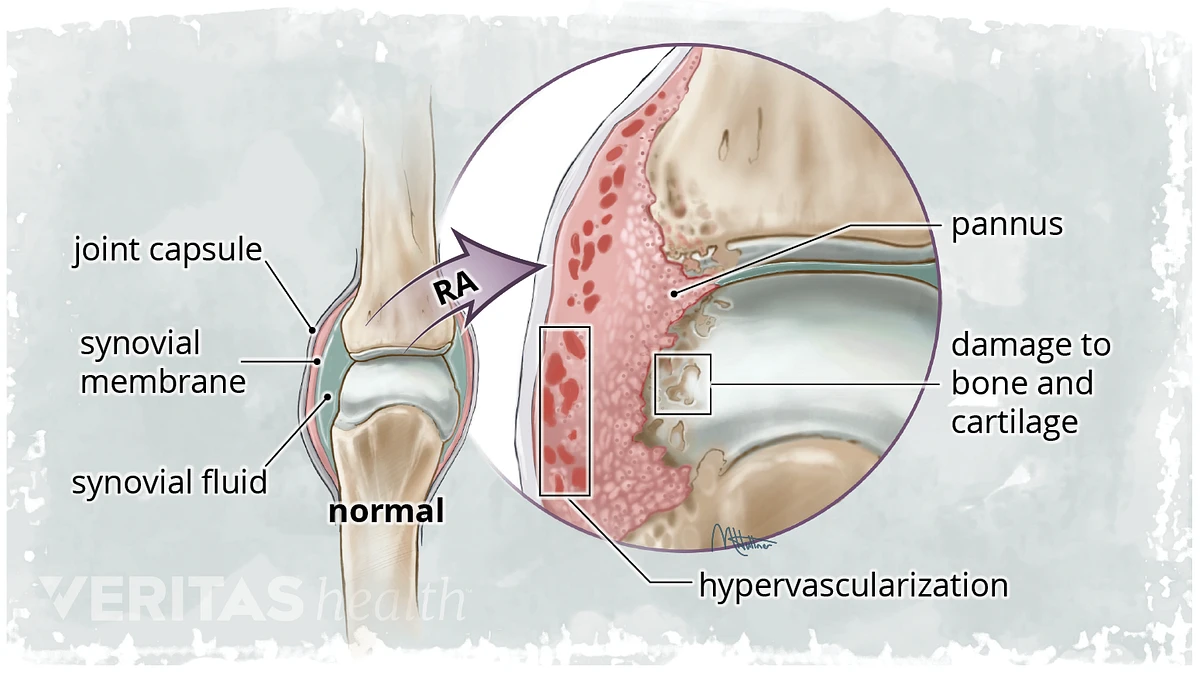
synovial membrane swells → hypertrophy
→ fills the joint space = panus
synovium fills joint space, at the insertion points of the capsule the bone is partially not covered by cartilage → direct contact
→ destroys bone + cartilage
→luxation+subluxation
→ ankylosis
swelling SM→erosion → band osteoporosis → false widening → ankylosis → ulnar deviation
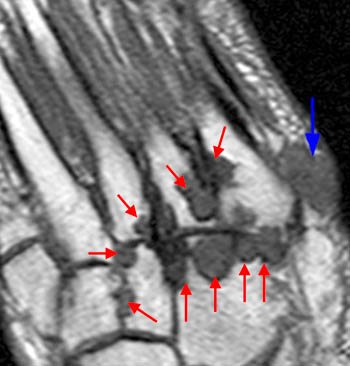
- early: ST swelling
- Erosions:
- early → superficial loss of cortical bone →dot-dash pattern 📷
- erosions at the margins of the bone → "mouse ears" 📷 at basis of phalanges (not at tip)
- subchondral progression → "pen in cup" 📷 carpal bones
- osteoporosis
- early: band osteoporosis 📷
- late: diffuse
- Cartilage destruction:
- early: false widening of joint space
- then destruction + join space narrowing+ankylosis
- subchondral cysts
- malalignment in advanced stages
→ leads to:
→ulnar deviation
{kind=link}
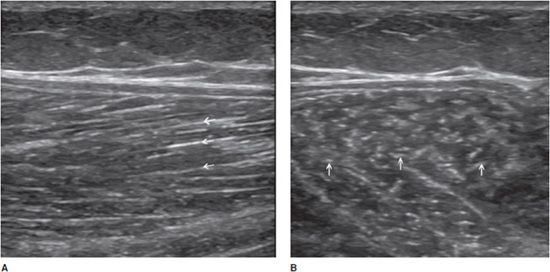
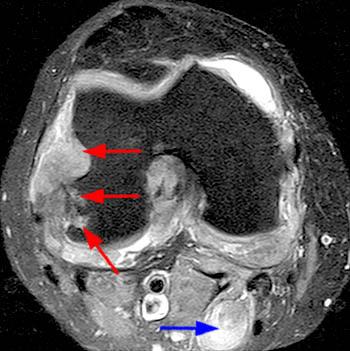
- fluid effusion in joints
- panus
- erosions
- rheumatoid nodules
- doppler
usually not used ⇒ images
- Panus
- Effusion
- Bone edema
- Erosions
- Cysts
- Tendons
- Contrast
x-ray bruder
MRI + US in early stages (when not visible on xray)
Follow up: US, maybe with contrast → synovitis, effusion
lung, pleura, pericardium,
- "Rheumatoid lung
- Rheumatoid lung nodules
- Pleural effusion
- Pericarditis
Remember: It's basically the opposite of RA
{kind=link}
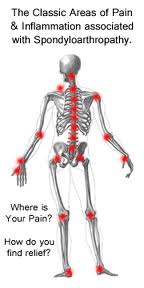
Inflammatory arthropathy + enthesopathy

syndesmophytes, bilateral sacroilitis + calcaneal enthesopathy
axial: spine + sacroilitis
young male (20-25y)
- pain at rest, pain is progressive
- esp. noctural pain
- bilateral
- sensitivity on pressure
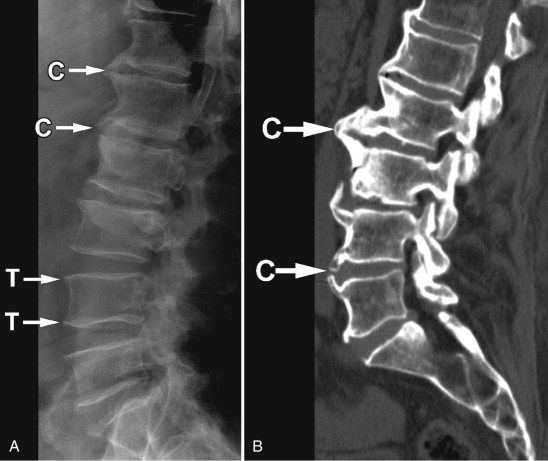
- Spine
- Syndesmophites → Bamboo stick
- shiny corners → osteolysis → square vertebrae
- Calcifications of other ligaments (interspinate + yellow lig)
- → tramline + dagger sign
- Bilateral Sacroiliitis


→associated with subchondral osteosclerosis
→erosions + false widening of joint space
→ bone bridges, narrowing of js
→ ankylosis
{kind=link}
calcanean enthesitis
spikes on the calcaneus due to ossificiation of the insertion of the longitudinal plantar lig. → auaaaa
{kind=link}
- lumbar pain > 3mo, not released by rest
- pain stiffness chest - limit mobilitlty spine + breathing
- the 2 xray signs
MRI → edema + bone swelling
CT or MRI
male 20:1
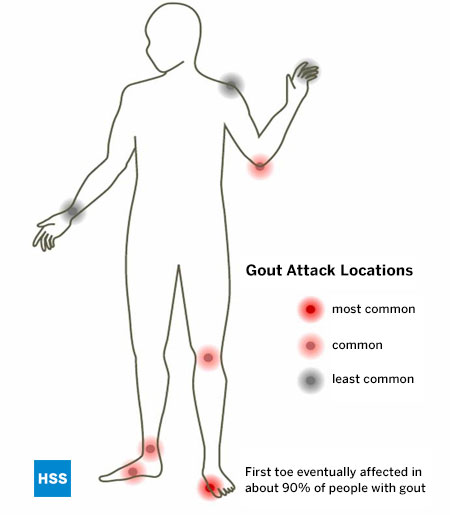
Hyperuricemia → uric acid in ST, cartilage, bone, esp. synovial membrane → inflammation → panus → destruction (like rheumatoid arthritis but compare location + soft tissue)
- Soft tissue swelling → if no tophi → MRI
- Tophi →density in ST 📷
- Bone erosions intraarticular 📷
- most often in lower extremity esp. metarsophalangeal (MTP)
- more frequent in the small joints
- could be anywhere!
- multiple or single
{kind=link}
in advanced stages
{kind=link}
{kind=link}
joint cartilage degeneration (aging) → joint changes → subchondral bone changes
- joint cartilage thinning → subchondral osteosclerosis
- osteophytes
- cysts
- osteoporosis
- Narrowing of joint space →but NEVER ankylosis
- Joint space narrowing → no ankylosis
- subchondral osteosclerosis, and evtl. osteoporosis
- Osteophytes assymetric
Synovitis → Joint effusion
US or MRI
nope
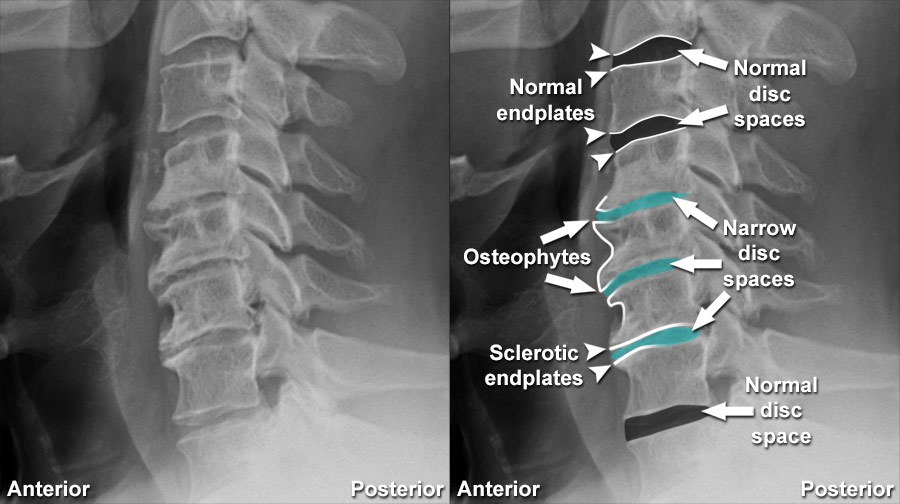
Spondylosis = ant. spine arthrosis = Discarthrosis
- Osteophytes→ first horizontal → then vertical → McNab osteophytes = huge uniting 2 neighboring vertebra
- narrowing, bulging, herniation (Schmorl) of IV-disc
- disc calcification
- "vaccum phenomen" (air inside disc)
- osteosclerosis
{kind=link}
osteo → assymetric + no fusion
synd → symmetric + fusion
Criterion | Osteophyte | Syndesmophyte |
Origin | On the vert. surface | In the vert angle |
Orientation | Perp. | Paral. |
Thickness | thick/parrot beak | thin/linear |
Fuses vert. | No | Yes |
Number | single/multiple | Multiple |
Symmetry | asymmetric | symmetric |
Significance | arthrosis | AS. |
Arthrosis of the hand in DIP joints 📷 → the one spared by RA
{kind=link}
coxarthrosis 📷
{kind=link}
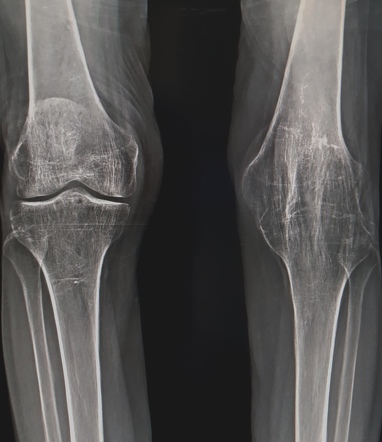
gonarthrosis 📷
{kind=link}
{kind=link}
arthritis
→ more details: see orthopedics
🥐 Urinary system 🔓
- Basics
- Morphological abnormalities - Syndrome of renal anomaly
- Stones
- Hydronephrosis
- Acute Pyelonephritis
- Chronic interstitial nephritis (pyelonephritis)
- Abcess
- Renovascular disease / Hypoxic kidney
- Syndrome of renal mass
- Small kidney syndrome
- Big kidney syndrome
- Syndrome of renal function loss
- General
- Bladder stasis
- Bladder content
- Bladder wall
🥣 Retroperitoneum, Pelvis, Breast 🔓
- Anatomy
- Adrenals
- Lymph nodes
- Fluid collections
- Uterus pathologies
- Ovary pathology
- Prostate
- Scrotum
- Sign + Symptoms
- Imaging techniques
- Imaging appearance
- Classification
- Breast cysts
- Fibroadenomas
- Ductal Ca
- Ductal Ca in situ (DCIS)
- Invasive ductal carcinoma (IDC)
- Lobular Ca
- Interventional diagnosis + therapy
🚑 Emergency Radiology 🔒
- MSK traumas
- Renal trauma
👶🏽 Pediatrics 🔒
- Musculoskeletal system
- Urinary system
- Hypertrophic pyloric stenosis
- Acute appendicitis
- Intussusception / Invagination