






Pharmacology I
- Pharmacology I
- 🧑🏽🔬 New Drugs and Clinical Trials 🔒
- 🚁 Peptic Ulcer Treatment
- 🍤 Gut Pharmacology 🔒
- 🍑 Hepatitis Treatment 🔒
- 🧈 Dyslipidemia and Obesity Treatment 🔒
- 🩸 Anticoagulants, Anti-Platelet Drugs and Thrombolytics 🔒
- 🐼 Anemia Treatment 🔒
- 🌊 Diuretics and ADH 🔒
🧑🏽🔬 New Drugs and Clinical Trials 🔒
🚁 Peptic Ulcer Treatment
Chief aka peptic cells
Parietal cells
Parietal via HCl
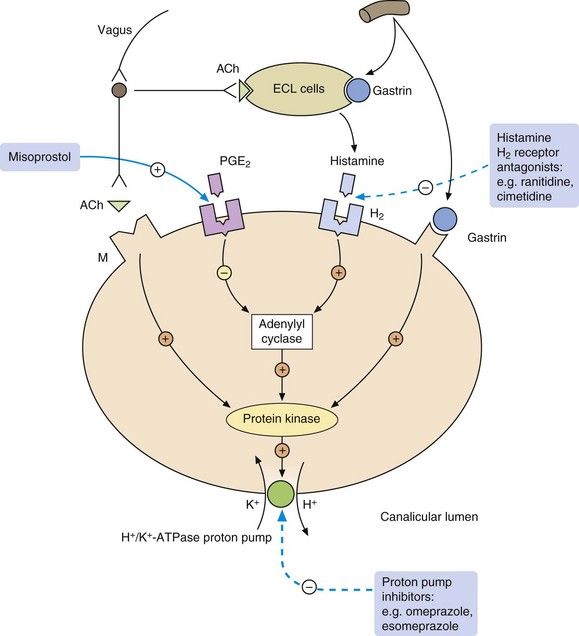
- PGE2 [+PGI2] (synthesis by gastric mucosal cells aka Mucus-neck-cells) → mucus and bicarbonate
- protective coat against HCl
- G-cells
- Stimulates HCl secretion (directly on H+/K+ ATPase and indirectly by stimulating Histamine releasing cells)
ECL cells (Entero-Chromaffin-like cells) → on Parietal H2-R → HCl secretion
Intrinsic factor → VitB12 binding+absorption
vagus stimulation
→ ACh on M3-R of parietal cells + entochromafin cells(Histamin release)
→ Stimulate GRP of G-cells → Gastrin
Somatostatin (released by D cells) 📷
{kind=link}
pH<3
PGE2 + PGI2(Prostacyclin)
{kind=link}
Gastrinoma (Zollinger-Ellison syd.)
protective if normal
- HP associated
- Zollinger-Ellison sdr.* associated
- NSAID induced
- stress induced (esp. on ICU)
- non-Zollinger-Ellison, non HP
- 🚬 (smoking)
- family history
- NSAIDs
- Corticosteroids
- Stress
- Zollinger-Ellison
- Non-erosive esophagitis
- Erosive esophagitis
- Barret's esophagus (metaplasia)
→ Decr. HCl (Acid supression)→ antisecretory drugs + antacids
→ incr. mucosal defense mechanism → mucosa protective drugs
→ eradication HP
→ lifestyle modification
- symptoms relieve
- Healing
- Risk reduction of complications
- Prevent recurrance
Acid suppressing drugs
- Antisecretory agents
- PPIs
- H2 Antagonists
- M-cholinolytic agents
- Antacids
Mucosal protecting agents
- Sucralfate
- Bismuth
- Prostaglandin analogues
surgery of LES
- irreversible blocking H+/K+ ATPase
- prodrug → systemic absorption → parietal cells→ leaves parietal cells → prodrug is activated in low pH (in lumen of parietal cell canalliculi) → binding to proton pump
"Meine eso Oma reitet auf nem Panter mit ner Lanze in der Hand + einem Raben auf der Schulter"
-"prazol"
- ome-
- ezome-
- panto-
- lanzo-
- rabe-
rebound acid hypersecretion 🥴
- enteric-coated capsules+tablets+microgranules → absorbed in bowel
- i.v. ()
- 30-60 min before first meal of the day
"all except rrrrrrabe 🐦"
ome, esome, panto, lanso -prazole
- Liver CYP450
- Renal excretion (Lansoprazol also stool)
18 hrs
renal + hepatic failure
genetic polymorphism (CYP450 enzyme activity)
Highest variations - omeprazole, lansoprazole, pantoprazole Lowest variations - rabeprazole
- usually well tolerated
- Low 2+ Cations: → Decreased Mg2+, Ca2+, Fe2+
- Clostridium difficile diarrhea
- pneumonia (community acq. + nosocomial)
- nonspecific-GI-symtoms: nausea, constipation, diarrhea
- Hypergastrinemia might lead to GI-tumor development *
- mask gastric cancer symptoms *
- Kidney diseases → ARF, CRF, AIN*
- skin eruptions
- cardiac conduction disturbances
- reduced absorption ampicillin and ketoconazole
- reduced VitB12 absorption
- inference with warfarin, cyclosporin
- Gastric + duodenal peptic ulcer
- GERD
- HP triple therapy
- zollinger ellison snd (first line)*
- Maintainance therapy* → lowest dose! (reduce ulcer recurrance + in GERD with severe symptoms)*
- Prophylactic in chronic NSAID use *
- Heartburns (OTC) (ome, lanso, esome)
same efficiancy when equivalent doses (aka angepasste dosis)
"Nase Reh"
- 20mg/day (can be increased to 40mg/day after 4 weeks)
- 4 weeks
- 20mg/day (can be increased to 40mg/day after 4 weeks)
- 4-6 weeks
4-8 weeks, same dose as ulcer

Omeprazole, Esomeprazole
"Hepatic master"
Omeprazole (+Dexlansoprazole)

20mg/day → can be incr. to 40 in severe cases
- coated tablets (10,20,40mg)
- i.v. 40mg (powder)
- 20-40mg coated tablets
- i.v. 40mg (powder)
→ lower variability of hepatic metabolism
→ prolonged T1/2
→ reduced dosage in hepatic failure needed!
Zollinger Ellison syd → ↑dose(160-240mg/day)
40 mg/day- one dose
Ayyyy, much rather used in GERD + erosive esophagitis
“PPIs at standard doses for eight weeks relieve symptoms of GERD and heal esophagitis in up to 86 percent of patients with erosive esophagitis. There are no major differences in efficacy among PPIs and no consistent increase in symptom resolution or esophagitis healing rates between different doses or dosing regimens of PPI therapy”
"esophagitis master" → Lange Lanze für den langen esophagus
PPI is the boss (compare sketchy)
{kind=link}
→ less Acid secretion (reduced stimulation by HIS)
→ reduced stimulation by Ach + Gastrin
→ reduced pepsin
- Ulcer (gastric + duodenal)
- prevention of stress ulcers (pre-OP)
- GERD
acutally same as with PPI
vierrrrrrr
duodenal ulcer 4 weeks
gastric ulcer 4-6 weeks
As a result of stronger acid suppression as compared with H2RA, PPI use results in faster control of peptic ulcer disease symptoms and higher ulcer healing rates [24-26]. PPIs are also more effective in preventing nonsteroidal anti-inflammatory drug (NSAID)-induced gastroduodenal toxicity and in healing gastroduodenal ulcers associated with NSAIDs when they cannot be discontinued
less efficient
tolerance develops
(stinkt ab)
75% uffff
→ single maintenance dose (→only 15% relapse)
Cimetidine
orally
i.v. (+i.m.) possible as well → in gastric bleeding or preoperative to prevent stress ulcer
only dose reduction in altered renal function (50% reduction in severe renal failure)
can be used in hepatic failure
passes through placenta + excreted in breast milk
gucccci
- general GI shizzl: nausea, vominting, diarrhea
- Gynecomastia, galactorrhea erectile dysfunction
- CNS shizzl: confusion, somnolence
- rare: hypergastrinemia
NO endocrine effects
poor CYP450 inhibition
Famotidine (40 mg/day in active ulcer)
Inhibits CYP450!
reduced metabolism of other drugs → toxic-effect:
- oral anticoagulants
- theophylline
- alprazolam
- tricyclic antidepressant
"Rami (Daka) aus Nizza ist ein famous Rockstar"
- Cimetidine (800mg)
- Ranitine (300mg)
- Nizatidine (300mg)
- Famotidine (40mg)
- Roxatidine (150mg)
before bedtime 😴 (PPIs 30-60 min before 1st meal)
in general half the dose
i.e 150mg Ranitidine
- tolerance (already relevant after 3 days of treatment)
- rebound acid hypersecretion → to prevent progressively reduce dose + consider antacids
weak bases → neutralize gastric acid → incr. pH + reduced pepsin activity
- duodenal ulcers! → healing + symptomatic (pain)
- poor efficacy in esophagitis + gastric ulcer
nonsystemic (neutralize acid → insoluble salts)
systemic (absorbed systemically → metablic alkalosis i.e. sodium carbonate)
ORAL
- chewable tablet (chew for max effect)
- powder
- suspension
after eating (1-3hours after) + before sleep
Antacids on empty stomach -short effect (30') Food in the stomach - may prolong the effect to 4-5 hours
- peptic ulcer
- intermittend symptoms GERD
- Heartburns
- frequent administration required
- no correlation symptoms - ulcer healing
- take drugs 2 hours after antacids, otherwise reduced absorption
- thyroid hormones, allopurinol, iron salts, -azoles → need acidic environment for absorption → reduced absorption
- reduced absorption tetracyclin (+some fluros)
aluminium compounds*
magnesium compounds*
calcium carbonate
*(most used)
- aluminium hydroxide
- aluminium carbonate
- aluminium phosphate
- GI shizzl: constipation, nausea, vomition
- phosphate deficiency after prolonged treatment (binding + incr. stool elimination)
Aluminum CHOPS
C-onstipation
H-ypophosphatemia
O-steodystrophy
P-roximal muscle weakness
S-eizures
high conc → osteodystrophy, prox myopathy, encephalopathy
(CHOPS)
alzheimer
5-30ml / dose
"Love-Möse mit Aluminium-Helm" (läuft aus, deswegen mL)
Mg hydroxide, carbonate oxide, trisilicate,
hydroxide → rapid + short action
oxide → reaction with water → hydroxide
trisilicate → slow + prolonged action
carbonate → weak + prolonged
laxative (esp. Mg-hydroxide)
might also produce toxic effects!
"remember, all = caution in kidney-impairment"
Mg-carbonate ⇒ Rennie
Mg-carbonate + Mg-Trisilicate ⇒ Dicarbocalm
rapid + prologed
anti-diarrheeeeeea effect 💩
- rebounds hypersecretion*
- hypercalcemia → renal stones
- constipation
Ca-carbonate trinkt auch Tee mit Norbi + Noah
1-2g/day
- =synthetic PGE1 analog
- reduced acid secretion (esp. food-stimulated, little basal)
- cytoprotective via incr. local circulation + incr. mucus + Bicarbonate production
{kind=link}
- in combination with NSAID treatment to prevent peptic ulcer (prophylaxis)
- also in NSAID induced peptic ulcer treatment (but rather PPI)
- 0,2mg x4 /day as as long as NSAID treatment in prophylaxis
- 0,2mg x4 /d or 0,4x2 in Ulcer treatment
- contraindicated in pregnancy!
- exacerbates IBD!
- might cause diarrhea + abdominal pain
complex compound of aluminiumhydroxid (antacid) + saccharose-sulfate
activated by acidic pH
→ form a cross-linking →protective gel
→ also binds to proteins on ulcer-surface (albumin, fibrinogen) → formation of insoluble complexes
⇒ protection of gastric mucosa, reduced inflammation, favors healing
⇒ also incr. mucus secr. + stimulation of PG secr.
- esp. duodenal ulcer or gastric ulcer with biliary reflux
→ also reduced relapses + recurrances
- prophylaxis stress-induces ulcer in immune-compromised
- rectal ulcer, irradiation induced proctitis, oral mucositis
- esophagitis
- NSAID induced peptic ulcer
oral (tablet / suspension)
on EMPTY stomach (1h before meal) (passt perfekt zu PPI, niemals mit H2+Antacids)
- dont give with H2-antagonist + antacids
- theophillin
- quinolones
- digoxin
kidney insuff
- constipation (most common)
- vomiting
- dry mouth
- headache
- skin eruption
- similiar like sucralfate → precipitation in acid environment → coat ulcer + erosions with protective layer
- stimulation of PG secr.
- anti-HP! (antimicrobial)
orally (tablet/solution)
→ 1200mg/d [30min before breakfest or dinner] - passt auch super zu PPI
→ 600mg x2 or 300mg x4
⇒ take 1 month, then 1 month break!
- black stools
- nausea
- RF
- pregnancy
- not when already on antacids (also no milk)
"Die 2 schwarzen Schweine aus der Tonne (1200mg) nehmen nen dicker Biss (Bismuth) von der Miso-Suppe mit NSAIDs (ind.)und prosten (Misoprostol) nochmal vor dem Nachtisch (Sucralfate ,Saccarose-sulfate + aluminium-hydrox)". Schwangere mit IBD sollten nicht anstoßen. Der immune supressive Kidney boy isst den Nachtisch so gestresst, dass es ihm wieder hochkommt deshalb isst er n leckeren PPI + kriegt constipation, NSAIDs gibts leider nicht. Auch die Schweine haben keine Kidney + sind geschwängert"
- duodenal ulcer + gastric ulcer
- in pat. under chronic NSAID/aspirin treatment
- before starting NSAID treatment in patient with history of peptic ulcer
- after gastric bleeding → prevent re-bleeding
!notice: no influence on GERD

Triple T with Levofloxaxin (PPI, Amoxi, Levoflox) only 10 days
Triple T with Rifabutin (PPI, Amoxi, Rifabutin)
PPI
Amoxi day 1-5
Clarithro day 6-10
Metronidazole/Tinidazole Day 6-10
ALL 14 days!
exception: triple with levoflox, sequential therapy ⇒ 10d
- PPI standard dose x2 / d (see below)
- Amoxi 1000mg x2
- Clarithro + Metronidazole 500mg x2
- Levoflox 1000mg x2
- Rifabutin 25mg x2
- Bismuth subcitrate 120mg x4
- Tetracyclin 400mg x4
Esomeprazole 20mg 2x/day Or Lansoprazole 30mg 2x/day or Omeprazole 20-40mg 2x/day Or Pantoprazole 40mg 2x/day or Rabeprazole 20mg 2x/day
Check for HP after 4 weeks via UBT or stool-Antigens
only in complicated ulcers (gastric + duodenal)
→ non-complicated duodenal ulcer dont need maintance therapy
give H2-Antagonist
- NSAIDs
- steroids
- KCl
- Alcohol
prophylactic treatment with misoprostol
PPI
fixed dose combination naproxen + esomeprazole is available
- High risk = History of complicated ulcer or >2 risk factors
- Moderate risk = >65y, high dose NSAIDS, history uncomplicated U, anticoagulants/aspirin/steroid therapy
- Low = no risk factors
HP is an independent additonal risk factor!