






Pediatrics
- Pediatrics
- 🧸Childcare & Pediatric Anamnesis and Physical exam 🔒
- 🫁 Respiratory system 🔒
- 🫀 Cardiology 🔒
- 💩 Gastroenterology 🔒
- 🎡 Endocrinology & Nutrition 🔒
- 🧬 Genetics & Birth defects 🔒
- 🥐 Nephrology
- 🩸 Hematology 🔒
- 🐉 Immunology & Rheumatology 🔒
- 🚑 Emergencies🔒
- 🪚 Pediatric surgery 🔒
🧸Childcare & Pediatric Anamnesis and Physical exam 🔒
- 👶🏽Pediatric anamnesis & Physical exam
- 📈Growth & Development
- 🍼 Nutrition & Feeding
🫁 Respiratory system 🔒
- 🧣 Acute Pharyngitis
- 🫒 Acute Adenoiditis
- 🎙️ Acute Laryngitis
- 🚇Acute (tracheo-)bronchitits & bronchiolitis
- 🧫Pneumonia
- 🗣 Asthma
- 🐌 Cystic fibrosis (Mucoviscidosis)
🫀 Cardiology 🔒
- 🔉 Heart murmors
- 👶🏼 Congenital heart diseases
- 🧫 Infective endocarditis (IE)
- 🫀 Cardiomyopathies
- 🎒 Pericarditis
- 🥁Cardiac arrhythmias
- 💢 Hypertension
💩 Gastroenterology 🔒
- 🌯 GERD & Esophagitis
- 🍤 Gastritis
- Gastroenteritis - Acute diarrhea
- Malabsorption - Chronic diarrhea
- IBD
- 🥴 Recurrent abdominal pain - Functional disorders
- 🪠 Constipation & Fecal incontinence
- 🧪 Liver biochemical test
- 🌼 Jaundice
- Chronic Hepatitis B
- Chronic Hepatitis C
- Autoimmune Hepatitis
- Wilson disease (hepatolenticular degeneration)
🎡 Endocrinology & Nutrition 🔒
- 🍔 Malnutrition & Obesity
- 🦴 Rickets
- 🍬 Type 1 Diabetes Mellitus
- 🦋 Congenital Hypothyroidism
- ⛺ Congenital Adrenal Hyperplasia: 21-Hydroxylase deficiency
- 🐥 Short stature
🧬 Genetics & Birth defects 🔒
- Clinical genetics
- ❌ Chromosomal abnormalities
- 🧬 Inborn errors of metabolism
- 🍷 🦠 Birth defects
🥐 Nephrology
Retrograde flow of urine:
bladder ⇒ Ureter + kidney
#1 Primary = short intramural ureter
⇒ Short intramural ureter → vesicoureteric junction (VUJ) fails to close completely during bladder contraction → VUR
(**normal VUJ ❗)
#2 Secondary = obstruction → ↑pressure
- anatomical (i.e. stenosis, post. urethral valves)
- functional (neuro / muscular)
- inflammation (UTI / cystitis / stones)
Grade | Reflux into | Dilation ureter + pelvis |
1 | Ureter | Ø |
2 | Ureter + pelvis | Ø |
3 | Ureter + pelvis | mild |
4 | Ureter + pelvis | mod. |
5 | Ureter + pelvis | sev.
(hydroneph, calyces + tortuosity of ureter) |
- asymptomatic
- Pyelonephritis → renal scarring → RF

{kind=link}

see → UTI
inflammation of glomeruli
⇒ mainly due to immun-complexes
⇒ NOT due to infection!
focal → some glomeruli affected
diffuse → all glomeruli affected
Segmental → part of glomerulus affected
global → entire glomerulus affected
- Hematuria (The urine looks smoky, and tea or cola colored.)
- Salt-retention ⇒ ↑BP + edema
- +/-Oliguria
+ Pyuria
- persistent proteinuria AND/OR hematuria
- RF within years
end stage RF within weeks
prior GAS infection (URT, skin) → Ag-Ab complex → deposition in glomeruli → Complement activation (↓C3) → Inflammation (acute GN)→ glomeruli damage → hematuria and other signs acute GN
F - only when indications are met (see later)
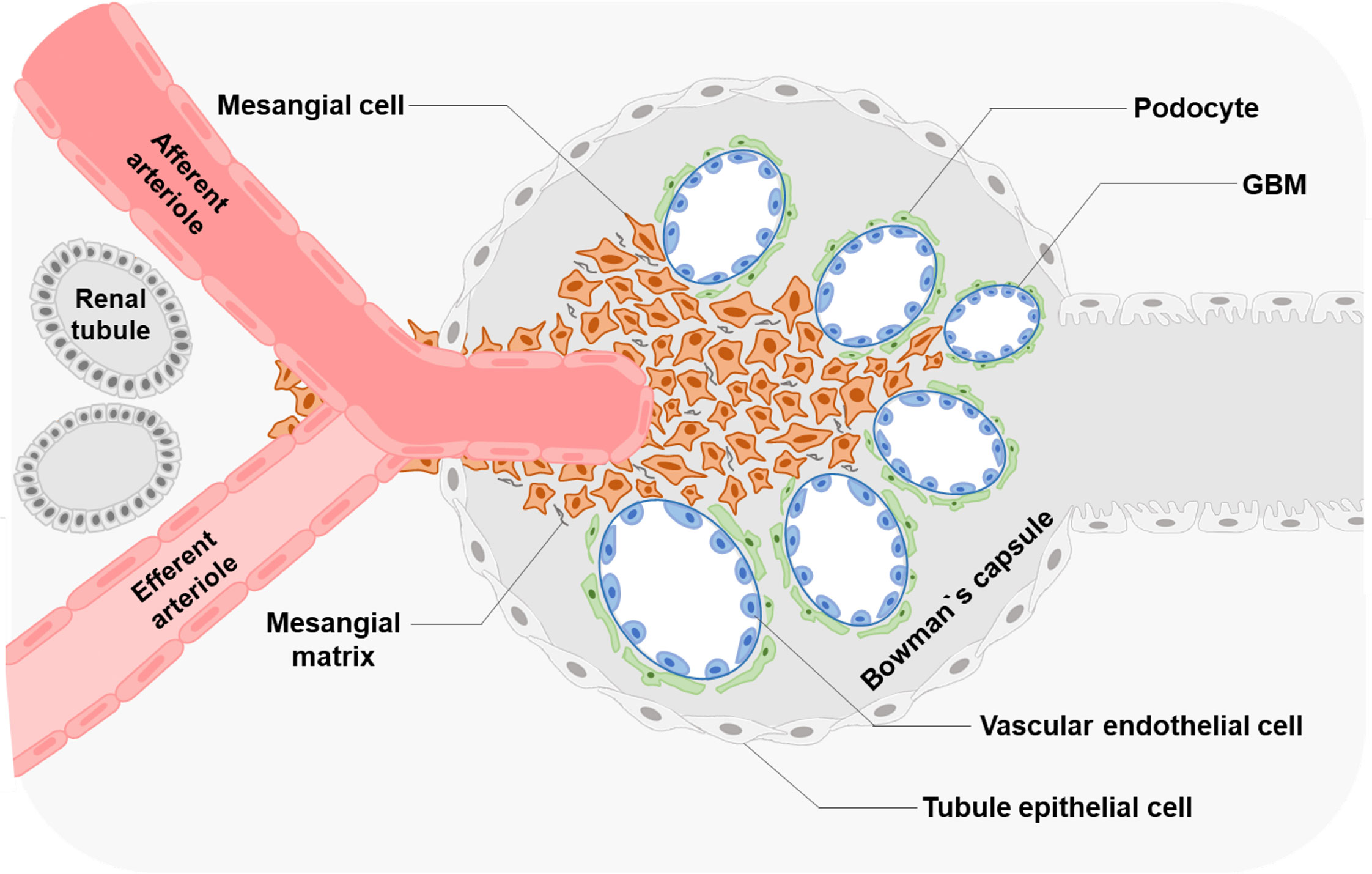
Unknown cause → IgA Immunoglobulin deposition in mesangial cells 📷
{kind=link}
ØSystemic disease! (i.e. Henloch-Schönlein, SLE)
Probable mechanism: The synthesis of an increased number of defective IgA antibodies, often triggered by mucosal infections such as respiratory tract and gastrointestinal infections, leads to the formation of immune complexes that deposit in the kidney, resulting in glomerulonephritis.
T
(APSGN = secondary)
T
(histo findings → see later)
Disease | Post-infectious | Acute nephritic | RF |
APSGN | 1-6 WEEKS | ✅ | Acute RF |
Berger | 1-2 DAYS | ✅ | Rare - Acute RF,
→ progression end stage RF within 20-25y |
*acute nephritic sy = acute GN = hematuria, ↑BP, edema, oliguria
APSGN:
- child >3y (max inc. 5-15y)
- 1-6 w after GAS
- 50% asymptomatic
- Acute nephritic syndrome
- Acute RF (50%?)
- rare: nephrotic sy
Berger:
- (max. inc. 10-35y)
- VARIABLE PRESENTATION/EVOLUTION
- Recurrent (isolated) gross hematuria
- 1-2days after URT / GI infection
- assoc. with loin pain
- Persistent microscopic hematuria / proteinuria
- Acute nephritic syndrome
- CRF
- rare: acute RF, nephrotic sy

Method of urine collection
| Diagnostic threshold
|
Midstream girls
| 100,000 CFU/mL
10,000-100,000 FU/mL - repeat culture
|
Midstream boys
| 10,000 CFU/mL
|
Catheter
| 10,000 CFU/mL
1,000-10,000 CFU/mL - repeat culture
|
Suprapubic aspiration | Any number of CFU |
does Ø influence natural history ⇒ can be given to prevent spreading
Renal replacement therapy / kidney transplantation
Yes, but slow progression also nicht so schlimm lel
- IgA
- membranoproliferative GN
- chronic evolution (vs. self-limited)
- ↓ASLO (vs. ↑ALSO)
- More common with NEPHROTIC sy
- (both ↓C3 + gross hematuria)
Henoch-Schönlein purpura (IgA vasculitis)
(+benign familiar hematuria)
Parameter
Oliguria Macroscopic hematuria Elevated creatinine Hypertension Low C3 Proteinuria Microscopic hematuria
Duration
7-10 days 1-3 weeks 3-4 weeks 4-6 weeks 6-8 weeks 3-6 months 1-2 vears
Q. Which of the following statements about the evolution of acute post-streptococcal glomerulonephritis are true? a. disappearance of macroscopic hematuria in 1-3 weeks b. normalization of blood creatinine level in 3-4 weeks c. normalization of C3 level occurs in 6-8 weeks d. proteinuria disappears after 2 years of evolution e. disappearance of microscopic hematuria in 1-1.5 years
- 🦤 Nephrotic syndrome (NS) 🔒
- 🧃Urinary tract infection (UTI) 🔒
- 🚱 Dehydration
- 🆎 Acid-base disorders
- 💥 Acute kidney injury (AKI / ARF) 🔒
- 🕰️ Chronic renal failure 🔒
🩸 Hematology 🔒
- 🐼 Anemia
- 🎾 Acute lymphoblastic leukemia (ALL) & Lymphoma
- 🩸 Bleeding disorders
🐉 Immunology & Rheumatology 🔒
- 😶🌫️ Immunodeficiencies
- 🦿Poly-articular arthropathies - Connective tissue disorders
- 📯 Post-streptococcal
- 🌺 Vasculitis
🚑 Emergencies🔒
- Fever
- Respiratory failure
- Heart failure
- Shock
- Coma
- Seizures
- Seizures
- Acute intoxication
🪚 Pediatric surgery 🔒
- 🌯 Esophageal atresia (EA) and Tracheo-esophageal fistula
- 🍤 Hypertrophic pyloric stenosis (HPS)
- 🫁 Congenital diaphragmatic hernia
- 🧱 Congenital abdominal wall defects
- 🚒 Necrotizing entero-colitis
- ↪️ Malrotation & Volvulus
- 🚟 Intussusception
- duodenal atresia & stenosis
- Small bowel atresia & stenosis
- Meconium ileus & Peritonitis
- Meckel’s diverticulum
- Acute appendicitis
- 🦌Hirschprung’s disease (congenital aganglionic megacolon)
- Ano-rectal malformation
- 🤕 Abdominal trauma
- 🪀 Gastrointestinal foreign bodies
- Hypospadias
- Phimosis
- Undescended testis (Cryptorchism)
- Hernia & Hydrocele
- Acute scrotum