







Orthopedics
- Orthopedics
- ⛲ Basics of osteoarticular traumatology🔒
- 🤸🏽♀️Shoulder girdle injuries🔒
- 🦾 Humerus fractures
- 💪🏽 Elbow and forearm injuries 🔒
- 🗼Spine injuries 🔒
- 🥣 Pelvic injuries 🔒
- 🦿Femur fractures 🔒
- 🧎🏽♂️Knee and distal lower limb injuries 🔒
- 👵🏽 Osteoarthritis and bone tumors🔒
- 👶🏽 Pediatric Orthopedics 🔒
⛲ Basics of osteoarticular traumatology🔒
- Generalities of OA traumatology
- Classifications
- Diagnosis
- Treatment
- Healing
- Complications
- Open fractures
- All classifications
- Overview: Treatment according to localization
🤸🏽♀️Shoulder girdle injuries🔒
- Clavicle fracture
- Scapula fracture
- Acromio-clavicular dislocation
- Gleno-humoral dislocation
🦾 Humerus fractures
growth plate
- more often affected then anat˝˝omical → weaker
- average neck-shaft angle is 135°
surgical neck • represents the weakened area below head • more often involved in fractures than anatomic neck • average neck-shaft angle is 135 degrees
Muscles
- pectoralis major displaces shaft anteriorly and medially
- supraspinatus, infraspinatus, and teres minor externally rotate greater tuberosity
- subscapularis internally rotates articular segment or lesser tuberosity
2:1
- Osteoporotic elderly (low energy falls)→on outstretched arm
- in young individual (high energy trauma): might also have associated Soft tissue + neurovascular injuries
{kind=link}
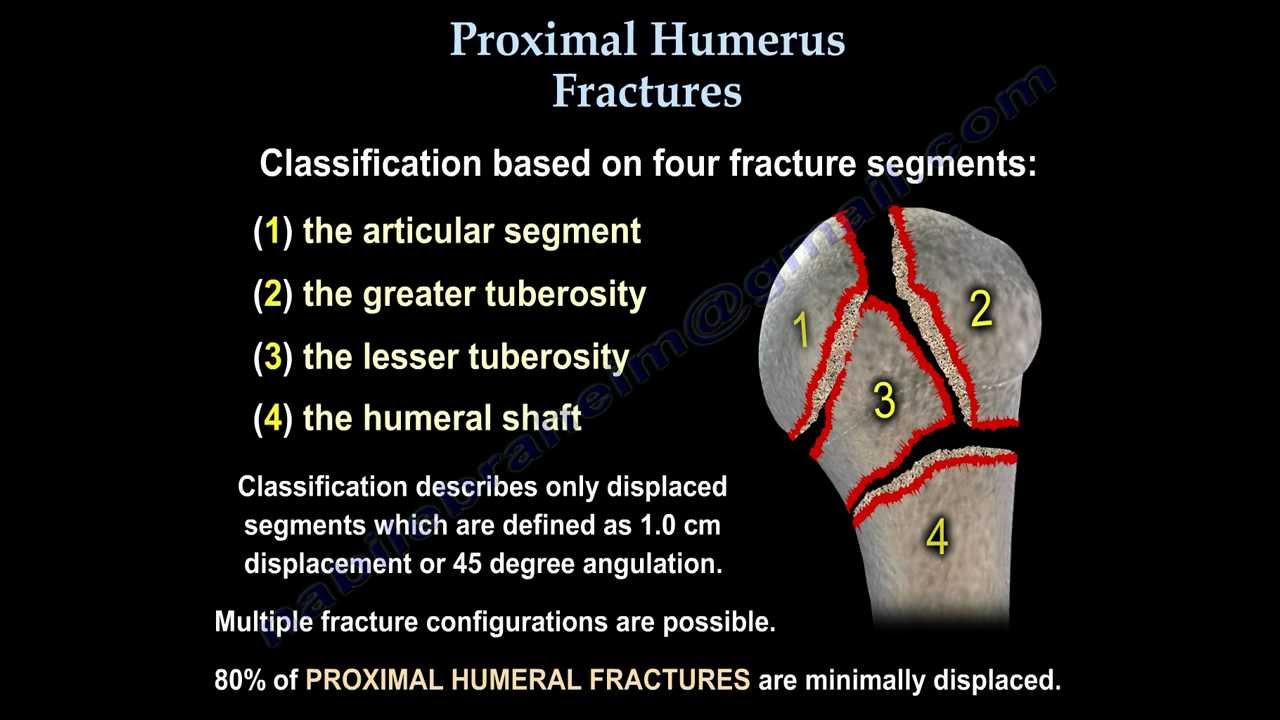
→ 4 parts of prox. humeral fracture
{kind=link}
- if one part displace → 2 part fracture
- if 2 displaced → 3 part
- if 3 displaced → 4 part fracture
- dislocation
No/minimal displacement = 1 part fracture 📷
muscles pull up → rotator cuff muscle
{kind=link}
gr. tuberosity displaced
humeral head more then >45° change if you compare to diaphysis
- Pain
- Decreased motions
- Extensive ecchymosis
NeVas exam ⇒ axillary nerve injury most common
- Sensory loss lat shoulder
- Abduction + ext. Rotation not possible (deltoid, teres minor)
{kind=link}
most of the cases xray: AP + scapular view
CT: prepare for surgery, see more detailed view if unclear on xray (head-split fracture? Head or gr. tuberosity uncertain?), intraarticular comminution
MRI: any rotator cuff injury or other soft T damage?
- 70-80% of prox. humerus fracture
- 2-4 weeks of immobilization
- nondisplaced (<1cm; <45°) = 1 part fx
- use extra-fixation (Dessault bandage) if you think the patient is not gonna be compliant
- Also you might consider this in older patients with more severe surgical neck fracture (2 part fractre)! → risk too high
head preserving treatment
- 2-3 parts fracture (less than 4) , esp. in younger individuals
- percutaneos pinning (K-wires) 📷
- philos-plates: open reduction
- CRIF: intra-medullary nail 📷 + k-wires: closed reduction → small incision sup. to the humerus → introduction of IM nail → nail through 5cm incision ⇒ stabilizes extremly good but is hard to place (needs a lot of xrays) + might damage rotator cuff
- ORIF: philos-plates 📷 : Holes in the plates: rotator cuff muscles can be re-attached here
{kind=link}
ball + socket reverse 📷 → deltoid muscles will act like the rotator cuff
{kind=link}
only in old people
- screw cut-out: screws come out + scratch glenoid 📷
- avascular necrosis
- nerve injury during surgery
- malunion / nonunion
- Rotator cuff injury
- Arthritis
- Infection
- other classics
Indirect/direct trauma
classic fracture signs
• Pain localized to the fracture site • Redness and swelling • Limb deformity • Palpable step-off or gap • Bone crepitus • Ecchymosis • Possible neurovascular compromise below the site of injury • Possible signs of an open fracture
Nope just the usual
→ classic simple, comminuted, wedge, etc...
- simple
- wedged
- comminuted
- displaced or undisplaced
- closed or open.
{kind=link}
{kind=link}
- Early
- open fracture
- vascular damage
- Late
- delayed union
- non-union
- mal-union
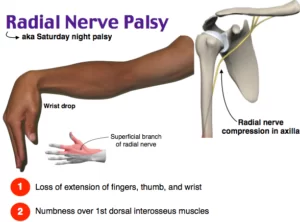
Fall hand
dorsal part sensitivity loss
no dorsiflexion possible
→ general rule: surgery only when hard displaced
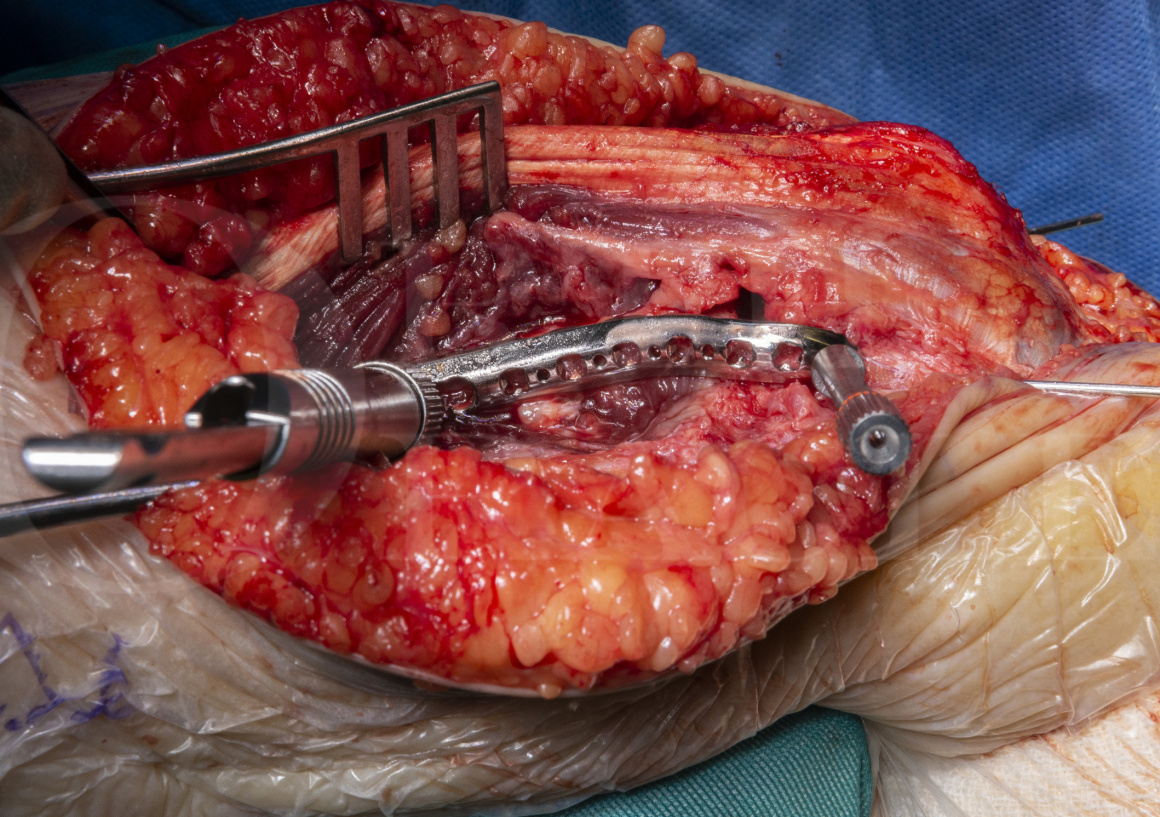
SURGICAL TREATMENT:
ORIF 📷
{kind=link}
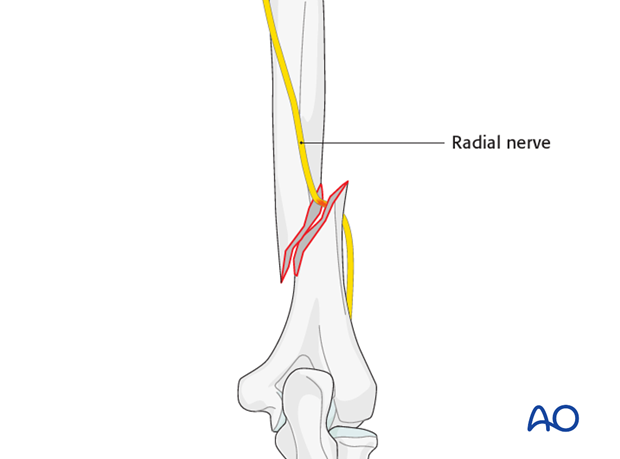
vascular involvement/compartment/open/polytrauma fracture → surgery
→ radial nerve palsy AFTER 6 weeks→ conservative most of the time due to temporarly nerve palsy
in really long, displaced shaft fractures:
CRIF with IM-nails 📷
{kind=link}
closed reduction with minimal invasive fixation
(right pic: intramedullary not deep enough→ will scrape acromial process)
{kind=link}
{kind=link}
→ intraarticular fractures need ORIF!! (with plates + screw)
- anatomical reduction of articulation, stable internal fixation ⇒ ORIF
- early ROM and rehabilitation
- mainly operative
- undisplaced
- probably without articular involvement
- Eldery + comminuted
⇒ Casts for 3 weeks
{kind=link}
{kind=link}
💪🏽 Elbow and forearm injuries 🔒
- Elbow dislocation
- Olecranon fracture
- Radial head fracture
- Forearm fracture
- Distal radius fracture
🗼Spine injuries 🔒
🥣 Pelvic injuries 🔒
- Pelvis fractures
- Hip dislocation
🦿Femur fractures 🔒
- Femoral neck fracture
- Trochanteric fracture
- Shaft fracture of the femur
- Distal femoral fracture
🧎🏽♂️Knee and distal lower limb injuries 🔒
- Patella fracture
- Knee sprain
- Tibial plateau fracture
- Tibial shaft fracture
- Pilon fracture
- Ankle sprain
- Ankle fracture
👵🏽 Osteoarthritis and bone tumors🔒
- Osteoarthritis
- Bone tumors
👶🏽 Pediatric Orthopedics 🔒
- Congenital clubfoot
- Adolescent idiopathic scoliosis
- Developmental dysplasia of the hip (DDH)
- Fractures in children