






Oncology & Radiotherapy
🎗️ Cancer Basics 🔒
Carcinogenesis, Trials, Epidemiology (Onco), AND Precursors (RT) are fused in this topic
- Cancerogenesis
- Etiology
- Epidemiology & Clinical trials
🧩 Dg-Workup & Tx-Evaluation
⇒ direct=mass vs. indirect=other cancer signs
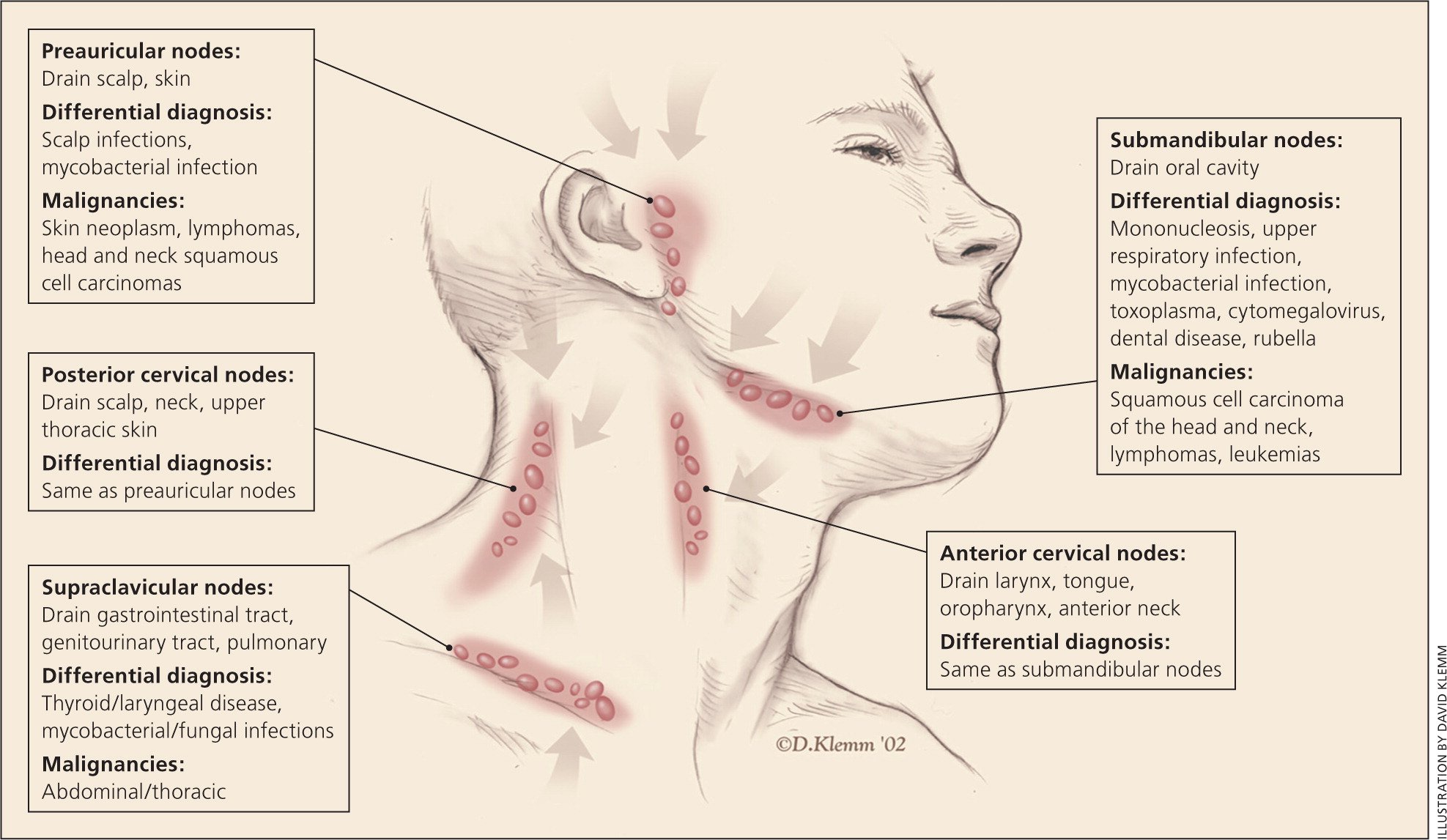
- direct signs → see/feel T, N (or M)
- indirect signs → see/feel effect of cancer
- bleeding,
- discharge,
- compression,
- neurologic signs
- B-symptoms,
- paraneoplastic synd.
- detect tumor (feel/see)
- Suggestive special signs? → aditional exam needed
→ if neg. → further dg-workup (imaging, lab)
- RF? → FH, Lifestyle, Diet, Environment/profession, etc.
- Main symptoms?
- Pre-neoplastic conditions/lesions? (polyps, leucoplasia, CIN, Barrets)
- Lab
- Imaging
- MRI
- CT
- US
- PET
- scinti
⇒ tumor resence? size? spread (local, regional, distant)?
- Endoscopy
- FNA → cytology
- Biopsy → histo + special tumor characteristics
STANDARDIZATION FOR:
- Tx-decision + evaluation/response
- Prognosis
- size
- invasiveness (adj. structures)
- number of involved structures
superficial → clinical exam
partially accessible to palpation → imaging and/or intrstrumental
deep → imaging!
- number (single vs. multiple)
- size
- location (regional vs. extra-regional)
- mobility (fixed or non-adherent)
- breast+ENT → Palpation
- deep → Imaging
>[1]cm in [short] axis.
Abdomen + Thorax
{kind=link}
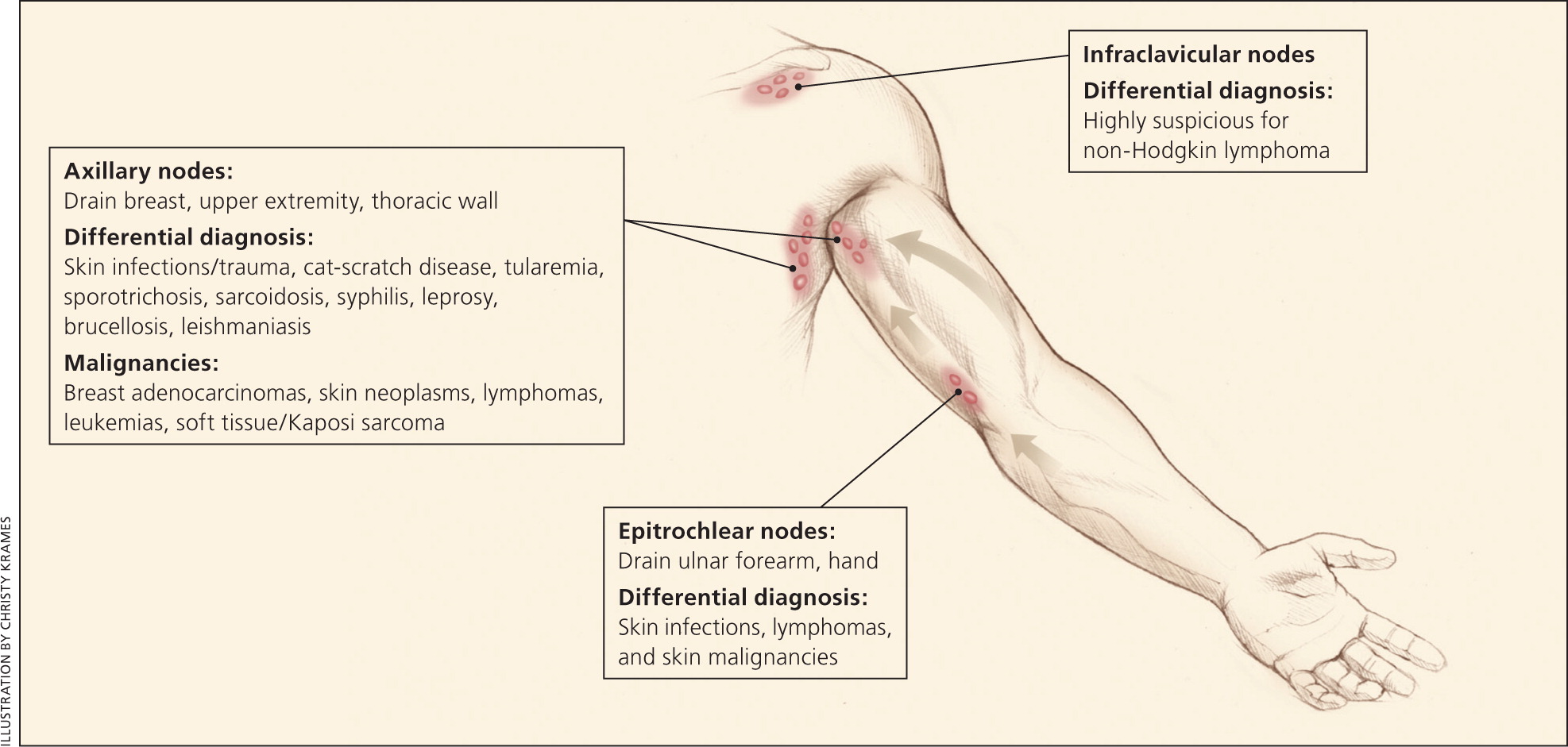
axillary 📷
{kind=link}
- male, white, >40y
- Generalized lymphadenopathy (≥2 regions)
- Lymphadenopathy ≥4-6w* (Øreturn to baselike after 12w)
- B-Symptoms
- supraclavicular location
- Lungs
- Liver
- Bone
- Brain
- distant LN (extra-regional LN)
Notice that CT catches almost everything → order scinti if bone involvement suspected
MRI for brain
CT | MRI | US | Xray | Scinti/PET | |
Lung | ✅ | ✅ | |||
Liver | ✅ | ✅ | ✅ | ||
Bone | ✅ | ✅ | ✅ | ||
Brain | ✅ | ✅#1 | |||
distant LN | ✅ | ✅ | ✅ |
F → does not modify
pathological TNM after chemo/RT
TNM after recurrance
less advanced
clinical stages (0-IV)
0 = in situ
1 = small tumor (Ø N,M + Ø BM invasion)
2 = local/regional extension minimum (BM invasion)
3 = local/regional extension important (LN +)
4 = extra-regional (M)
- Brain tumor
- Endometrial + Cervix
- ST sarcomas
CLINICAL STAGING:
early stage → 0-IIb
locally advanced → IIIa-IIIc
metastatic → IV
TNM:
early stage → T≤2 N≤1 (OR T3N0)
locally advanced → T1/2 N2+; T3N+, T4N0, or N3
metastatic → M1
- History → how fast did the symptoms progress?
- Inflammatory signs (edema, congestion)
- Imaging → RECIST: measure size + progression of size
- Lab → monitor tumor markers
ECOG performance index scale
→ ask for:
weight loss? (+fatigue?)
physical acitivity? → walking, self-care
work capacity?
⇒ decides which Tx can be done

Local:
- Surgery
- RT
Systemic:
- Chemo
- Hormone
- Immuno + Targeted Tx
- Other (cryo, HIFU, RFA)
RO= ideal R1= microscopic residual disease R2= MACROscopic residual disease
- acute complications / toxicity
- tumor regression (RECIST)
- natural tumor history
- risk of recurrence
- Immediate post-tx → first control after 2month
- Maximum risk → 2m - 5y
- relative security → >5y
Year 1: every 3m (4x/y)
Year 2-3: every 3-6m (2-4x/y)
Year 4-5: every 6m-1y (1-2/y)
⇒ in lab:
year 1-2 = every 3m
year 3-5 = every 6m
- aggressiveness of tumor
- Tx-fails


☢️ Radiotherapy
survival
The abscopal effect is a hypothesis in the treatment of metastatic cancer whereby shrinkage of untreated tumors occurs concurrently with shrinkage of tumors within the scope of the localized treatment.
{kind=link}
🧱 Treatment 🔒
- 📛 Pain Therapy
- 🧪 Chemotherapy
- ☢️ Radiotherapy
- 🚧 Targeted Therapy, Immunotherapy & Hormonal Therapy
- 🥕 Nutrition in cancer
- DVT & PE
- Superior vena cava obstruction
- Spinal cord compression
- Intracranial Hypertension
- Metabolic Emergencies
- Hematologic emergencies
- Urological emergencies