







Occupational Medicine
- Occupational Medicine
- ⛲ Introduction 🔒
- 🌬️ Work-related Asthma
- 🏭 Pneumoconiosis 🔒
- 🧪 Toxicology 🔒
- 💪🏽 Musculoskeletal Disorders 🔒
- 🪖 Physical Hazards 🔒
⛲ Introduction 🔒
🌬️ Work-related Asthma
inhaled Allergen → IgE Ab→ histamine release
- Bronchial hyperresponsiveness (fast+severe bronchoconstriction)
- Bronchial Inflammation → mucosal edema + SM contraction
- Bronchial obstruction
- Bronchospasm
- Edema
- incr. mucus production
Obstruction is reversible in asthma
→ spontaneously or with inhalator
work agent (direct occupational exposure)→ asthma
CLEAR RELATIONSHIP, no other cause
exacerbation of pre-existing nonoccupation asthma due to work-trigger
exacerbated or caused by work agent
a term that includes OA + WAA
- sensitizer-induced → immunological mechanism → exposure to sensitizing agent → occurance after a period of time
- high MW (molecular weight)→ animal or plant origin
- low MW → chemicals
- irritant-induced (no latency)→ direct trigger of airways-nerves + dmg epithelium → begins directly
→ ammonia, chlorin, ...= potent irritant
(in the past: Reactive airway dysfuction syndrome)
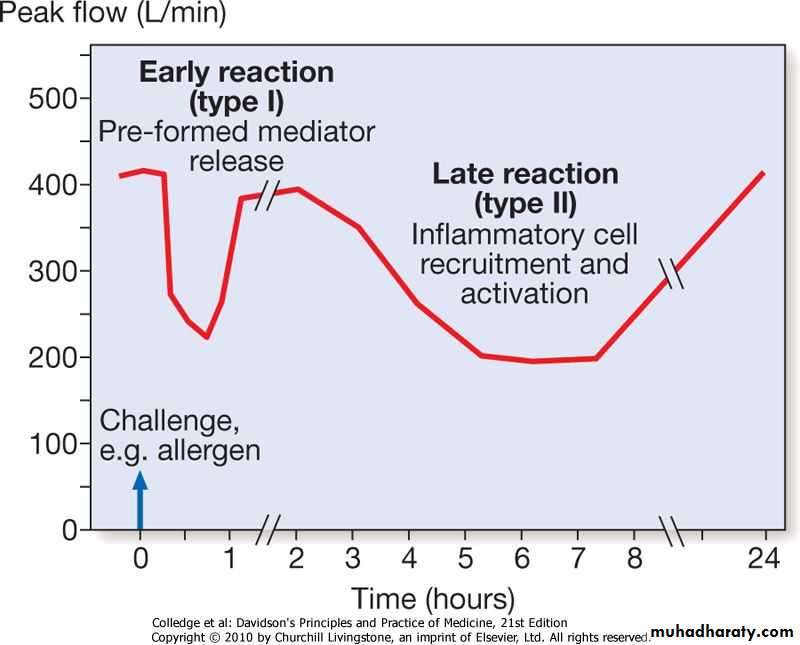
- early response(min)→ mastcell + IgE→ histamine → self limited
- late response(4-8h) → Ly, Np, Eo + IgG → persistent obstruction → beta-ago!
- dual response= both
{kind=link}
- wheezing
- dyspnea
- cough
- chest tightness
- concomitant eye+upper resp. tract symptoms
- Xray + spirometry normal (if no acute attack)
- NSHR - nonspecific hyperresponsiveness → trigger asthma attack with histamine→ decr FEV1 → pos decr. of FEV>20%
- Bronchodilator- test → give b2-agonist (salbutamol, albuterol, etc.) → what's the effect on FEV1 → if signif. incr. (≥12%, ≥200ml inc.) → positive
HISTORY!
Diagnostic criteria:
- symptoms only at/regularly after work
- improve on day off
- progression over week
- improve after change of work environment
Specific inhalation challange test (SICT) = gold standard → exposure to expected allergen
→ but expensive, special equipment, has to be in the laboratory
→ bring equipement to workplace → Across-work-shift spirometry(workplace challange)
→ but compared to SICT cant identify the specific agent + you need to send lab workers to the work place (good for large companies)
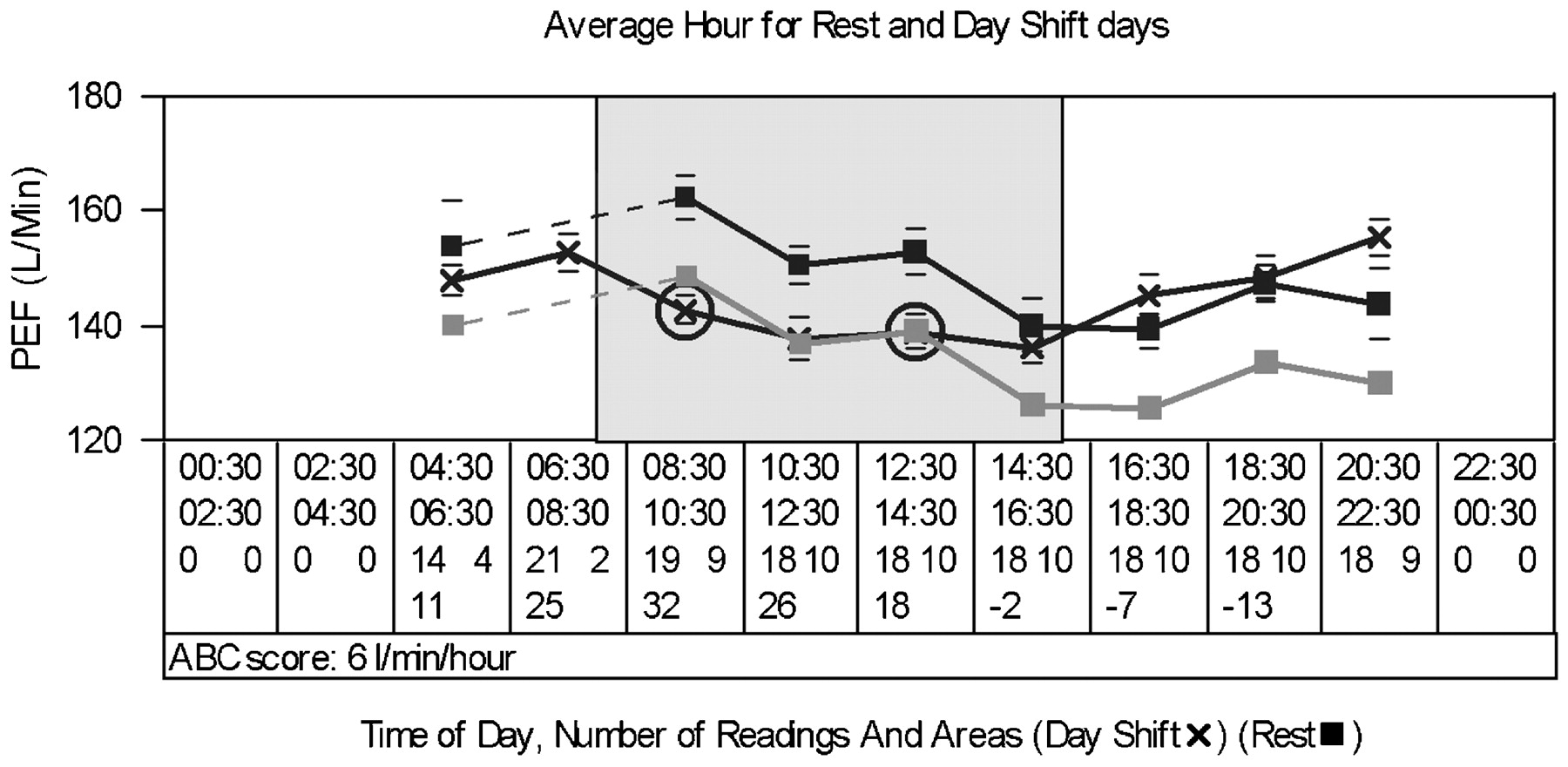
⇒ SERIAL RECORDING of PEFR(peak expiratory flow rate) 📷 is used most of the time → uses peak flow meter 📷 → patient can do that by himself and write a diary - 4x/day
{kind=link}
{kind=link}
→ allergen skin test + serological test (RAST,ELISA) might also be used in identifying the specif. allergic agent but they dont confirm the asthma dg.
- beta agonist (salbutamol)
- steroids
- O2
- Antibiotics
- ipratropium bromide
- he said: "acutally completely avoid exposure when asthma has developed in sensitizing-induced forms!"
- further lung function + monitoring
→ reduction only in irritant-induced forms
- Diisocyanates - coating, insulation, furniture - irritant mechanism + second. sensitizing mechanism
- Vegetable dust - cotton, → Byssinosis =monday syndrome (1-2 after return to work - milder on work-offdays)
- Metal salts - Platinum, Nikkel, Kobalt - electroplating, jewelry-making - Platinosis = asthma + rhinitis + urticaria
- Acid anhydrides - curing + hardening agents
- Wood dust - plicatic acid
- animal derived (high molecular weight)
- chemicals
- wheat
- latex
- dust
- vapour + fumes
🏭 Pneumoconiosis 🔒
- Basics
- Silicosis
- Asbestosis
🧪 Toxicology 🔒
- Basics
- Lead Poisoning
- Mercury Poisoning
- (Organic) Solvents
- Toxic Asphyxants (CO & Hydrogen cyanide)
💪🏽 Musculoskeletal Disorders 🔒
- Basics
- Occupational Risk factors
- Neck
- Shoulder
- Elbow
- Wrist and Hand
- Spine
- Hip
- Knee
🪖 Physical Hazards 🔒
- Basics
- Heat Stroke
- Heat Exhaustion, Heat cramps + Heat syncope
- Disorders caused by VIBRATION
- NOISE induced hearing loss
- Radiation