







Gastroenterology
- Gastroenterology
- 💥 Abdominal pain and Dyspepsia 🔒
- 🍤 Gastro-Esophageal diseases 🔒
- 💩 Chronic Diarrhea, Celiac Diseases, IBS, Constipation 🔒
- 🔥 Inflammatory bowel disease (IBD) 🔒
- 🩸 Upper and Lower GI Bleeding
- 🍄 Diverticulosis, Polyposis and Colo-Rectal Cancer 🔒
- 🍑 Liver Pathologies 🔒
- 🎋 Biliary Tree Pathologies 🔒
- 🧽 Pancreas Pathologies 🔒
💥 Abdominal pain and Dyspepsia 🔒
🍤 Gastro-Esophageal diseases 🔒
Benign gastro-esophageal diseases
Malignant gastro-esophageal diseases
💩 Chronic Diarrhea, Celiac Diseases, IBS, Constipation 🔒
🔥 Inflammatory bowel disease (IBD) 🔒
- Crohn’s
- Ulcerative colitis
🩸 Upper and Lower GI Bleeding
Stool guaiac test
slow pace - low volume bleeding
UPPER GI
(but can also be small intestine/colon if slow pace)
colonic origin
also UGI with large volume or high pace
might be bright or dark
- Peptic ulcer
- Gastroesophageal varices
- Erosive esophagitis/gastritis/duodenitis
- Neoplasm
- Aortoenteric fistula (rare, cant afford to miss!)
- Mallory weiss tear
- Dieulafoy's lesion
- Vascular ectasia
- Diverticulosis
- IBD
- neoplasm
- infectious or ischemic colitis
- hemorrhoids
- post-polypectomy
- Angioectasis
- Dieulafoy
- prior GI + or family history
- NSAIDs
- Liver disease
- Vascular disease
- Radiation exposure
- Vitals (ABC) ⇒ early fluid resucitation reduced mortality!!!!
- Abdominal tenderness
- Rectal examination
- description of blood
- masses / hemorrhoids
- Skin + oral (hereditary hemorrhagic telangiectasis)
an acute GIB
- Age <50
- Melena
- BUN/CREA ration ≥ 30! (blood gets reabsorbed → ↑urea)
- DD Hematochezia from UGIB vs LGIB → aspiration
- Coffee grounds bleeding (less severe/inactive bleeding)
- negative aspirate is not helpful: 20% with neg. aspirate have UGIB!
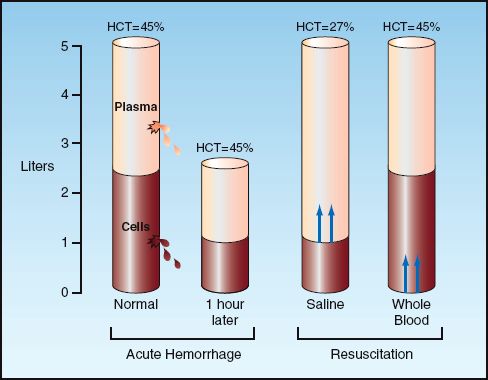
NO, initial Hct can be misleading → Hct stays the same with loss of whole blood (until re-equilibration) 📷
{kind=link}
≤7
Weigh risks / benefits of reversing anticoagulation (Assess degree of coagulopathy) → Vitamin K - slow acting, long-halflife → FFP - fast acting, short-halflife → RBC transfusion
Predictors of mortality in UGIB:
rockall scoring system: 📷
{kind=link}
{kind=link}
low risk UGIB will not likely requre endoscopic hemostasis
- Facilitate clot formation (i.e. VitK, FFP)
- PPI
- dg
- risk stratification
- hemostasis therapy
- endoscopic stigmata (high bleeding risk or active bleeding)
- recent hemorrhage
!80% resolve spontanously
{kind=link}
low rebleeding-bleeding rates
Flat pigmented IIc
Clean base III
- inject Epinephrin
- Thermal electrocoagulation
- Hemoclips
!combined therapy superior to mono-T
- low risk: oral PPI + fed
- Endoscopic therapy: PPI infusion for 72h
- Determine HP status
restart aspirin as soon as bleeding resolved
(not dying = more important than rebleeding)
high
- Severity of liver D → child pugh score
- ↓Platelets <88k
- Splenomegaly
- Platelet count/Spleen diameter(mm) ratio <909
"variceal"
Vasoconstrictor therapy*
Antibiotics*
Resuscitation*
ICU
Endoscopy*
ALternative aka rescue therapies (TIPS)*
Betablocker*
Reduce splanchnic blood flow
→ Terlipressin
→ Somatostatin
→ Octreotide
Bacterial infection: in 66% of patients with cirrhosis and variceal bleed → Prophylactic antibiotics → decr. incidence of bacterial infection
⇒ significantly reduces early rebleeding
Ceftriaxone IV Alt: Norfloxacin po
excessive fluid → ↑↑portal pressure → ↑↑bleeding
asap after resuscitation (withing 12h)
⇒ Band ligation 📺
TIPS (Transjugular intrahepatic portosystemic shunt) 📷
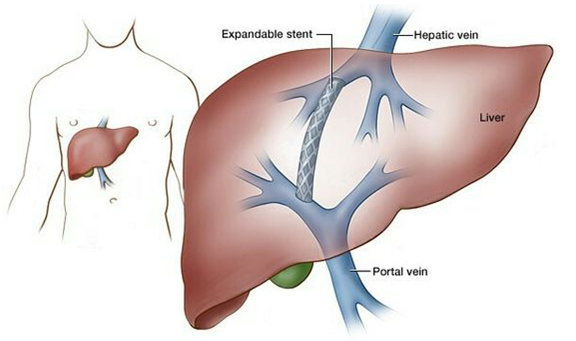{kind=link}
esp in high risk patients → within 24-72h
esp. in gastric variceal bleeding
Sengstaken-Blakemore Tube 📷
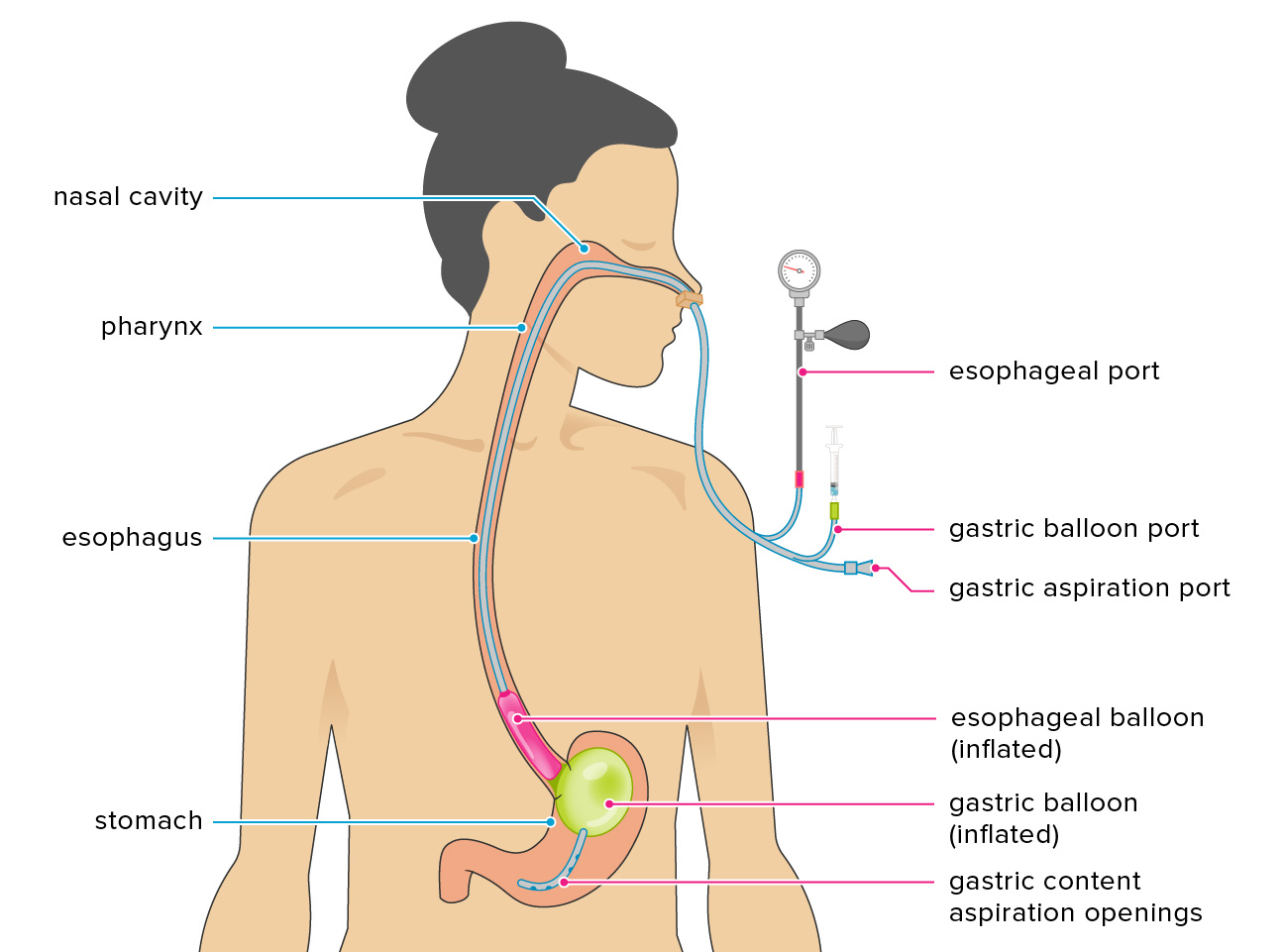{kind=link}
→ compression gastric variceals
!but only temporary → high complication rate (aspiration, necrosis, perforation)
!airway protection needed!
Self expanding metal stent 📷
{kind=link}
after acute bleeding resolved
→ ↓splanchnic vasoconstriction + ↓cardiac outbut → ↓risk for recurrent hemorrhage
Colorectum
UGIB
10-15% of patients with presumed LGIB actually have upper GIB in the end
Diverticulosis
Div: large volume, painless
collitis: small valume, pain, diarrhea
- Hemodynamic unstable: HR>100, SBP<115, Syncope (each counts 1 factor)
- nontender abdomen
- aspirin use
- >2 active comorbiditis
- bleeding during first 4h of evaluation
⇒ Interpretation:
- 0 factors: ~6% risk
- 1-3 factors: ~40%
- >3 factors: ~80%
- age
- intestinal ischemia
- comorbiditis
- secondary bleeding
- coagulopathy
- hypovolemia
- transfusion required
- male
true, 80% (like UGIB)
6-12h
similiar UGIB → identify stigma → therapy
- colonoscopy after resolution of bleeding + bowel prep
- angiography in massive bleeding
rapid "purpe" preg aka bowel prep → colonoscopy within 1h after clearance
- cant be stabilized
- cant be prepped for bowel
- had colonoscopy but failure to localize/treat bleeding
- localize active bleeding
- hemodynamically stable patient
- might be used with tagged RBC scan
- others failed
- Shock/Hypotension
- >6U PRBCs transfused
🍄 Diverticulosis, Polyposis and Colo-Rectal Cancer 🔒
- Diverticolosis
- Polyps and polyposis of the colon
- Colo-Rectal cancer
🍑 Liver Pathologies 🔒
- Basics
- Jaundice
- Portal Hypertension
- Ascitis
- Liver failure
- Chronic viral hepatitis
- Autoimmune hepatitis
- Primary biliary cholangitis
- Non-alcoholic fatty liver diseases
- Alcoholic liver disease
- Wilson's diseases
- Hemochromatosis
- Liver cirrhosis
- Hepatocellular carcinoma
- Benign Liver Tumors
🎋 Biliary Tree Pathologies 🔒
- Cholelithiasis
- Acute Cholecystitis
- Choledocholithiasis and Cholangitis
- Primary sclerosing cholangitis
- Choleangiocarcinoma
🧽 Pancreas Pathologies 🔒
- Chronic pancreatitis
- Pancreatic cancer