






Endocrinology
- Endocrinology
- ⛲ Hormones Overview 🔒
- 🫒 Pituitary Gland Disorders 🔒
- 🦋 Thyroid Gland 🔒
- 💠 Parathyroid Gland 🔒
- 📐 Adrenal glands
- 🍆 Reproductive System 🔒
‣
⛲ Hormones Overview 🔒
‣
🫒 Pituitary Gland Disorders 🔒
- Basics
- Precocious Puberty
- Constitutional Delay in Puberty + Absent Sexual Infantilism
- Adenohypophysis
- Pituitary tumoral syndrome
- Neurohypophysis & Diabetes insipidus
- Acromegaly and Gigantism
- Hyperprolactinemia (Prolactinoma)
- Pituitary insufficiency
‣
🦋 Thyroid Gland 🔒
- Basics
- Thyroid Function Tests
- Goiter
- Thyroid Nodule and Cancer
- Thyroiditis
- Thyrotoxicosis & Hyperthyroidism
- Hypothyroidism
‣
💠 Parathyroid Gland 🔒
‣
‣
‣
‣
‣
‣
‣
‣
‣
‣
‣
‣
TRY this topic 🏎️
↓
‣
📐 Adrenal glands
‣
‣
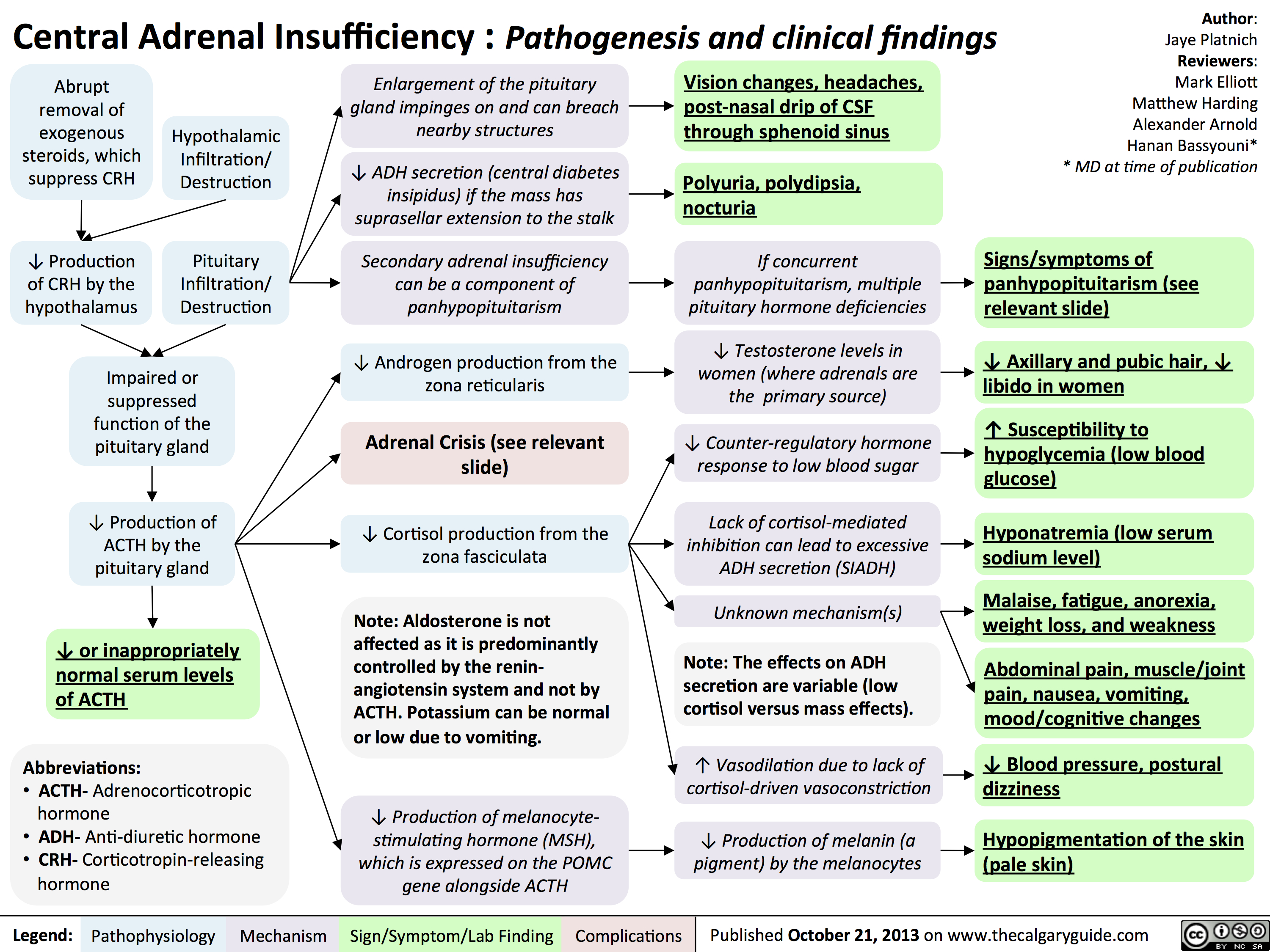
- External → adrenalectomy, chronic corticosteroid Tx
- Destructive internal process
- Autoimmune (most common) → Sporadic, Autoimmune polyendocrine, familial
- Metastasis (SMLungCa, Breast Ca)
- Infection
- Waterhouse-Friderichsen syndrome (meningococcal septicaemia)
- Tuberculosis + other infections
- Genetic - Congenital (adrenal hyperplasia → 21-hydrox-def) ⇒ see later extra!!
👉🏽
Reminder: primary = adrenal patho; secondary = hypophyseal patho; tertiary = hypothalamic patho
{kind=link}
‣
👉🏽
{kind=link}
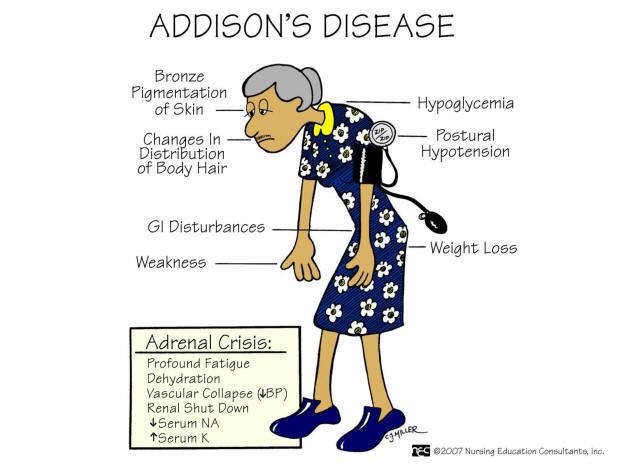
- Hyperpigmentation (sun exposed + pressure, new scars, buccal+gums after skin)
- Fatigue, Weakness, Weightloss
- orthostatic Hypotension (pos- Schellong test)
- GI-disturb: nausea, vomiting, abd. pain
- Arthralgia
- emotional instability, depression, irritability
- loss sec. hair in woman
- others (related to autoimmune e.g. vitiligo)
- Clinic of HypoNa, HyperK, metab. azidosis
- salt craving (due to Na-loss)
‣
- measure serum Cortisol + ACTH → if high ACTH + low Cortisol = primary; if low ACTh = central/secondary
- ⇒ cosyntropin (rapid ACTH-stimulation) test if uncertain i.e. in partial primary → if cortisol <500 → Adrenal insuff (normal <550) ⇒ !doesn't mean its primary! → can be secondary or iatrogenic too (due to adrenal atrophy) ⇒ only tells you that you have hypoadrenalism
‣
- HypoNa, HyperK
- low Gluc
- inc. BUN + Crea ⇒ Volume-depletion
- Anemia + Eosinophilia
- high Renin, high ADH
- ECG → low voltage, ST-modific.
‣
⇒ What's the etiology?
- Adrenal Autoantibodies → Anti-21-hydroxylase, Anti-17-hydroxlase 📷
- CT
- serological+Mibi test (i.e. tuberculosis)
→ enlarged + Calcification → tuberculosis, metastasis
→ small + atrophic → chronic autoimmune
‣
- life long Glucocorticoids → Hydrocortisone, Prednisone
- Mineralcorticoid in primary → Fludrocortisone
- DHEA (Dehydroepiandrosteron) - esp. in female
- enough sodium intake!
- etiological Tx → Infektion, Autoimmune, Cancer etc.
‣
everything should return to normal
- symptoms should disappear + hyperpigmentation should improve
- !overtreatment → cushings
- check Cortisol day curves + ACTH
- Fludrocortison → Electrolytes, BP, Plasma-Renin should be normal
‣
- ↑ Dose of steroids during (Stress, surgery, illness)
- minor stress →incr. 3x3
- major stress (surgery) → up to 200-300mg/day
- pat education: “Don’t miss a dose!”
‣
- Hypotension, volume depletion, shock, coma
- hyperpyrexia
- CNS depression sympt
- GI symptoms like chronic
- hypoglycemia
- weakness + muscle cramps
‣
- Addison + stress (infection, surgery, trauma, dehydration)
- Bilateral acute adrenal hemorrhage (Waterhouse-Friedrichsen syd.)
- Congenital adrenal hyperplasia
‣
draw blood → send to lab
Tx: immediate start with Hydrocortison i.v. + Saline + Gluc i.v.
→ don’t wait for lab results before starting Tx
‣
- low Cortisol
- HypoNa, HyperKa, metabolic azid.
- Hypoglycemia
- Eosinophilia
- Urea+ Crea
‣
search for etiology!
→i.e. infection?
‣
👉🏽
{kind=link}
- Congenital Adrenal Hyperplasia🔒
- Cushing's Syndrome 🔒
- Hyperaldosteronism 🔒
- Pheochromocytoma and Paraganglioma 🔒
‣
🍆 Reproductive System 🔒
‣
Female Reproductive System Disorders
- General
- Hypogonadism (Ovarian Insufficiency)
- Menopause
- Polycystic Ovarian syndrome
- Turner Syndrome
‣
Male Reproductive System Disorder
- Male Hypogonadism
- Klinefelter Syndrome